PoTS; the King s approach. Dr. Nick Gall King s College Hospital London, UK
|
|
|
- Madison McKinney
- 6 years ago
- Views:
Transcription
1

2 PoTS; the King s approach 2017 Dr. Nick Gall King s College Hospital London, UK
3 The King s PoTS experience Appointed in 2004 Cardiac electrophysiologist Occasional patients with PoTS / IST Anticoagulant nurse was the first recognisable patient Impotent in dealing with the issues Paucity of UK services Little help as to what to do
")


4 Initial (on-going) battle against myths PoTS DOESN T EXIST They re just hysterical nurses

5 A neurocardiology MDT
6 So what did we do.. Ask the expert(s) at conferences Read the articles (written by the expert(s) at conferences) Treat the patients and see what happens Ask questions Why do you get migraines? How do I treat that? Why don t you get better?

7 At last.we ll know what to do now!?
8
9 Oh if only it were that easy! So, this is what I ve learnt! STEP 1: RECOGNISING YOUR PATIENT

10 It s not always that simple! The HR changes are unfortunately variable and are perhaps not the whole story

11 Did you know? Symptoms change from day to day, hour to hour.. Tested 8-9am, fasted, medication stopped >5 half-lives before
12 The world is not divided into normal, mad and PoTS! Normal Fainty people Mad Orthostatic intolerance PoTS POTS


13 The haemodynamic changes vary! THE CLASSICAL PATTERN
14 OI
")
15 Normal (?!)
16 Reflex syncope is not required for the diagnosis
17 Clinical features CORRECT DEMOGRAPHIC SYMPTOMS FOR >6/12 CARDIOVASCULAR SYMPTOMS UNEXPLAINED BY OTHER CONDITIONS OFTEN WORSE WITH POSTURAL CHANGE ASSOCIATED, VARIABLE NON- CARDIAC SYMPTOMS
18 You might have the right patient IF THEY VE GOT THE RIGHT SYMPTOMS AND A SUGGESTIVE TILT
19 Is this really our patient? STEP 2: LET S MAKE SURE WE RE NOT MISSING SOMETHING!

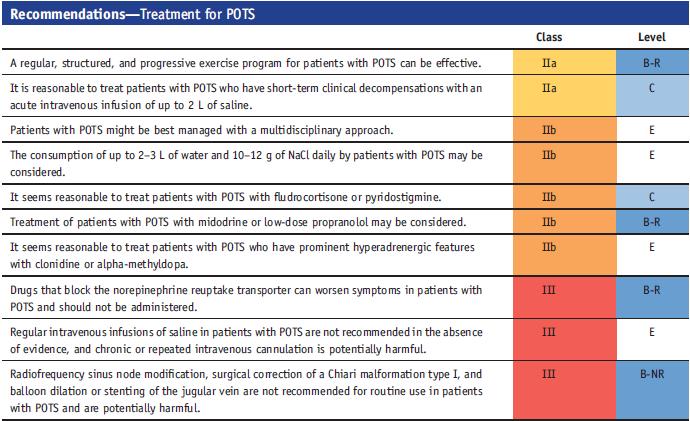
20 The guidelines will help us?! Tiny evidence base!
21 Our approach to testing is empiric and cardiological Tilt / active stand Echo 7 day Holter CPET Respiratory function tests

22 Holter the HR trend is helpful Persistently fast Spiky More normal
23 CPET Very complex investigation Good assessment of physiology overall, exclude other conditions Assessment of deconditioning Dysfunctional breathing
24

25 Respiratory function tests
26 Other things. BLOOD TESTS FBC, ESR, CRP U&Es, LFTs, TFTs, Glc CK Ferritin, B12, folate, Vitamin D (Coeliac, autoantibodies) EBV serology (Lyme serology)
27 Results AFTs Very complex Helpful where there is uncertainty e.g. Diabetes and hypermobility Cardiovascular reflexes: Resting cardiac vagal tone (CVT): was 6.2 units in the linear vagal scale (LVS) which is a normal vagal tone, (Normal range, units in the LVS). Resting heart rate: was 78.0 beats/min, which is a normal heart rate for this level of CVT. Breathing: there was normal breathing at the rate of 14.0 breaths/min. Deep breathing: CVT was 11.5 units and the maximum CVT was 14.4 units in the LVS indicating normal respiratory effect on CVT in the brainstem during deep breathing. Carotid massage: CVT increased by 5.8 units in the LVS showing a normal cardiodepressor effect (normal increase units), blood pressure (BP) changed by mmhg indicating a normal vasodepressor effect (normal drop mmhg). Baroreflex responsiveness in isometric exercise: was 1.85 ms/mmhg but 1.42 ms/mmhg was predicted from the patient s height, indicating a normal central gain of the baroreflex system. Phenylephrine injection test: there was no measurement. Valsalva s ratio: was 2.39 indicating a high Valsalva's ratio (normal range, ). Orthostasis: Cardiac response: showed an abnormally low response in a 30:15 ratio test. BP stability: was good, systolic BP varied by mmhg, normal variation is <25 mmhg. Mean supine arterial BP was 77.5 mmhg indicating normal supine BP (the normal range of supine mean arterial BP, mmhg). Orthostatic hypotension: Postural change in diastolic BP was mmhg. Therefore, no postural hypotension was detected. Sympathetic function in general: There was no test done for postganglionic damage. Control of resistance blood vessels in skeletal muscles during isometric exercise: showed normal muscle sympathetic tone. Cardioaccelerator function in isometric exercise: showed normal cardioaccelerator function. Blood pressure response to Valsalva s manoeuvre: BP change in phase IIe was 4.9 mmhg and in phase III was 9.9 mmhg showing evidence of normal venous return. BP change in phase IIi was 48.9 mmhg indicating raised splanchnic sympathetic tone. Cutaneous sympathetic function: Sudomotor function function Emotional sudomotor function was not assessed not assessed Vasomotor Thermoregulatory vasomotor function was Interpretation: The results show evidence of normal muscle sympathetic tone, normal cardioaccelerator function and raised splanchnic sympathetic tone in the deep targets of the sympathetic division of the autonomic nervous system. There was evidence of normal venous return to the heart. In the cutaneous targets, there was no sudomotor measurement and there was no vasomotor measurement. Postganglionic sympathetic fibres were not assessed for damage. In the parasympathetic division, there was normal vagal tone. Baroreflex system had a normal central gain and there was normal respiratory effect on the CVT in the brainstem during deep breathing. There were normal cardiodepressor and normal vasodepressor effects of the carotid reflex. Of the non-specific tests, there was no postural hypotension, a high Valsalva's ratio and an abnormally low response of the heart to standing upright. HR increased from 91 to 100 bpm and there were runs of Mayer type waves which were associated with her symptoms of icy legs and headache. Clinical Interpretation: Despite the relatively modest HR change with standing the Mayer type waves were convincing and were symptomatic. This is more the picture of dysregulation rather than a major autonomic neuropathy.
28 The tilt can help though..
29 Let s get the treatment started. STEP 3: MAKING A DIFFERENCE TO THE ORTHOSTATIC INTOLERANCE
30

31 Nonpharmacological therapy IT S NOT SEXY BUT NOTHING WORKS IF THEY RE NOT DOING THIS!! Consider proving it with a 24 hour urine collection for Na+ and volume: >2.5L >170mmol Na+ REMEMBER THE DIET
32 IV Saline (1L) Acutely Decreases Orthostatic Tachycardia G Jacob et al. Circulation 1997;96:
33 Exercise Study in POTS - Design Cardiac MRI Maximal Exercise Test Blood Volume Measurement 3 months of exercise training 45-min 60 Upright Tilt Screening 45-min 60 Upright Tilt Blood Volume Measurement Maximal Exercise Test Cardiac MRI
34 Exercise in POTS Focus on Aerobic Activity Some resistance training focused on thighs Exercise training in POTS: Must be Regular Every other day (4/week) 30min/session -> 45-60min/session NO UPRIGHT EXERCISES Rowing machines Recumbent Cycles Swimming o o o o o Increases fitness levels Increases blood volume Cardiac Remodeling Normalizes Sympathetic Activity Decreases Orthostatic Tachycardia Takes 4-5 weeks to start seeing benefits Qi Fu et al., JACC 2010;55:

35 Pharmacological therapy Does it really help? Very helpful; use with care Worth a go, at low dose Very helpful in some; split doses
36 Midodrine Decreases Orthostatic Tachycardia Jacob, G. et al. Circulation 1997;96:
37 Heart Rate (bpm) Change in Heart Rate (bpm) Propranolol 20mg lowers Orthostatic Tachycardia Standing HR Orthostatic Increase in HR 130 Propranolol Placebo 40 Propranolol Placebo P Drug <0.001 P Int < P Drug < Pre 1H 2H 3H 4H Time Post Dose 0 Pre 1H 2H 3H 4H Time Post Dose SR Raj et al. Circulation 2009;120:
38 Symptoms (a.u.) Propranolol Improves Symptoms Symptoms 26 Propranolol Placebo P Int = Pre 2H 4H Time Post Dose SR Raj et al. Circulation 2009;120:
39 Symptoms Score (a.u.) but less is more 0 Propranolol 20mg Propranolol 80mg P =0.041 Wilcoxon SR Raj et al. Circulation 2009;120:
40 Heart Rate (bpm) DDAVP+H 2 O reduces standing HR DDAVP+H2O Placebo P Time = P Drug = P INT = Pre 1H 2H 3H 4H Time Post Dose ST Coffin et al., Heart Rhythm. 2012;9:
41 Heart Rate (bpm) Change in Symptom Score (au) Acetylcholinesterase Inhibition Standing Heart Rate Symptoms 135 Pyridostigmine Placebo 5 Pyridostigmine Placebo P=0.001 P= P<0.001 P< P= Pre 2H 4H -15 Time Post Dose SR Raj et al., Circulation 2005;111:
42 Heart Rate (bpm) Symptoms Score (a.u.) SNRIs make it worse! C Orthostatic Change Symptoms: 0 to 2h 40 Atomoxetine Placebo Atomoxetine Placebo 20 P Int = P = Pre 1H 2H 3H 4H Time Post Dose -6-8 SR Raj et al., AAS Presentation (2010)
43 So what do I do? Midodrine first (2.5 10mg TDS) Ivabradine second (2.5 5mg BD TDS) Then think about something else Beta blockers if high functioning (low dose) Fludrocortisone (up to 200 mcg daily) Slow sodium ( mg TDS) Anti-histamines (Pyridostigmine etc - I don t prescribe drugs I can t spell.)
44 But what about all of the other stuff? STEP 4: ALL OF THE OTHER SYMPTOMS
45 Dysfunctional breathing respiratory physio
46 Gastroenterology Often complain of: Nausea / vomiting Bloating Pain Constipation / Diarrhoea Find a helpful gastroenterologist and look for gastroparesis, SIBO, colonic dysmotility Treat whatever you can! Medications, diet (various)
47 Urology Often complain of: Weak bladders Frequency, urgency, incontinence Recurrent UTI, pain Find a helpful urologist and look for a large, insensate bladder Timed and double voiding Antibiotics Catheters etc
48 Neurology / Sleep / Audiovestibular medicine Lots of headaches esp. migraines Migraine variant balance disorder Psychophysiological insomnia Reassurance needed: Neuropathic symptoms. MS. Chiari.
49 Rheumatology Hypermobility is very common Pain, clicky joints, stretch marks, easy bruising PoTS vs hypermobility Do we need to exclude an inflammatory arthritis? Find a helpful rheumatologist Try to refer to the hypermobility experts for pain management, specialist physio etc

50 Mast cell activation syndrome
 Empirical treatment (cetirizine,")
51 Mast cell activation syndrome Consider if allergies, rashes, pain Testing.. Try to find an expert (and let me know when you do ) Empirical treatment (cetirizine, ranitidine, Na+ cromoglicate etc)
52 Other stuff that comes up. STEP 4: DAY TO DAY MANAGEMENT
53 Pregnancy implications No clear suggestion of adverse consequences Symptoms may well get worse reassure Fludrocortisone and beta-blockade are OK Don t do anything differently on our account Standard analgesia and delivery in labour
54 Anaesthetic implications No adverse consequences Inform the anaesthetist that it is not a heart problem but is about managing the underfilled Lots of IV fluid TEDs Slow mobilisation Don t panic with the tachycardia
55 Other stuff LYME DISEASE SAY NOTHING WE WERE NEVER HERE I HAVE NEVER MET ANY OF YOU
56 What we really need is some sort of practical document. Perhaps with a UK focus.
57 To conclude: Recognise the patient by the symptoms more than the HR change Exclude other conditions Do the simple stuff extremely well Consider medications Treat the associated features Be honest and caring because we don t have all of the answers!
58 AND ON THAT BOMB- SHELL... THANK YOU FOR YOUR ATTENTION
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE
 IT S NOT THAT SIMPLE") POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME (POTS) IT S NOT THAT SIMPLE POTS Irritable heart syndrome. Soldier s heart. Effort syndrome. Vasoregulatory asthenia. Neurocirculatory asthenia. Anxiety neurosis.
Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST)
 and Inappropriate Sinus Tachycardia (IST)") Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST) Ahmad Hersi, MBBS, MSc, FRCPC Professor of Cardiac Sciences Consultant
Findings from the 2015 HRS Expert Consensus Document on Postural Tachycardia Syndrome (POTS) and Inappropriate Sinus Tachycardia (IST) Ahmad Hersi, MBBS, MSc, FRCPC Professor of Cardiac Sciences Consultant
Rehabilitation for Postural Tachycardia Syndrome (POTS)
") Rehabilitation for Postural Tachycardia Syndrome (POTS) Satish R Raj MD MSCI FACC FHRS FRCPC Associate Professor of Cardiac Sciences University of Calgary Adjunct Associate Professor of Medicine Autonomic
Rehabilitation for Postural Tachycardia Syndrome (POTS) Satish R Raj MD MSCI FACC FHRS FRCPC Associate Professor of Cardiac Sciences University of Calgary Adjunct Associate Professor of Medicine Autonomic
Exercise Training for PoTS and Syncope
 B 140 120 100 80 60 40 20 0 Blood Pressure (mm Hg) Blood Pressure Heart Rate 60 degree Head Up Tilt Time 140 120 100 80 60 40 20 0 Heart Rate (beats.min -1 ) Exercise Training for PoTS and Syncope C Blood
B 140 120 100 80 60 40 20 0 Blood Pressure (mm Hg) Blood Pressure Heart Rate 60 degree Head Up Tilt Time 140 120 100 80 60 40 20 0 Heart Rate (beats.min -1 ) Exercise Training for PoTS and Syncope C Blood
Syncope Update Dr Matthew Lovell, Consultant in Cardiology
 Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Syncope Update Dr Matthew Lovell, Consultant in Cardiology Definition of Syncope Syncope is defined as TLOC due to cerebral hypoperfusion Characterized by a rapid onset, short duration, and spontaneous
Pyridostigmine in the Treatment of Postural Orthostatic Tachycardia: A Single-Center Experience
 Pyridostigmine in the Treatment of Postural Orthostatic Tachycardia: A Single-Center Experience KHALIL KANJWAL, M.D.,* BEVERLY KARABIN, PH.D.,* MUJEEB SHEIKH, M.D.,* LAWRENCE ELMER, M.D., PH.D., YOUSUF
Pyridostigmine in the Treatment of Postural Orthostatic Tachycardia: A Single-Center Experience KHALIL KANJWAL, M.D.,* BEVERLY KARABIN, PH.D.,* MUJEEB SHEIKH, M.D.,* LAWRENCE ELMER, M.D., PH.D., YOUSUF
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE
 June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
June 8, 2018, London UK TREATMENT OF VASOVAGAL SYNCOPE Where to go for help Syncope: HRS Definition Syncope is defined as: a transient loss of consciousness, associated with an inability to maintain postural
Neurocardiogenic syncope
 Neurocardiogenic syncope Syncope Definition Collapse,Blackout A sudden, transient loss of consciousness and postural tone, with spontaneous recovery Very common Syncope Prevalence All age groups (particularly
Neurocardiogenic syncope Syncope Definition Collapse,Blackout A sudden, transient loss of consciousness and postural tone, with spontaneous recovery Very common Syncope Prevalence All age groups (particularly
A lady who can t stand up. Inter-Hospital Geriatrics Meeting Dr Man Shiu Piu NTWC
 A lady who can t stand up Inter-Hospital Geriatrics Meeting 26-8-2011 Dr Man Shiu Piu NTWC Madam Ho 89 years old Lives with family, walks with stick, ADL-I. Non-drinker Past health: Labelled IHD since
A lady who can t stand up Inter-Hospital Geriatrics Meeting 26-8-2011 Dr Man Shiu Piu NTWC Madam Ho 89 years old Lives with family, walks with stick, ADL-I. Non-drinker Past health: Labelled IHD since
Postural Orthostatic Tachycardia Syndrome:
 Postural Orthostatic Tachycardia Syndrome: A Case Presentation Interesting Cases from the Annals of Women s Heart Care I have no financial relationships or commercial interests to disclose that are relevant
Postural Orthostatic Tachycardia Syndrome: A Case Presentation Interesting Cases from the Annals of Women s Heart Care I have no financial relationships or commercial interests to disclose that are relevant
Desmopressin In The Treatment of Postural Orthostatic Tachycardia
 The Journal of Innovations in Cardiac Rhythm Management, 6 (2015), 2222 2226 DOI: 10.19102/icrm. 2015.061202 PHARMACOLOGICAL THERAPY RESEARCH ARTICLE Desmopressin In The Treatment of Postural Orthostatic
The Journal of Innovations in Cardiac Rhythm Management, 6 (2015), 2222 2226 DOI: 10.19102/icrm. 2015.061202 PHARMACOLOGICAL THERAPY RESEARCH ARTICLE Desmopressin In The Treatment of Postural Orthostatic
Note: At the end of the instructions, you will find a table which must be filled in to complete the exercise.
 Autonomic Nervous System Theoretical foundations and instructions for conducting practical exercises carried out during the course List of practical exercises 1. Deep (controlled) breath test 2. Cold pressor
Autonomic Nervous System Theoretical foundations and instructions for conducting practical exercises carried out during the course List of practical exercises 1. Deep (controlled) breath test 2. Cold pressor
Correspondence should be addressed to Shaista Safder,
 Gastroenterology Research and Practice Volume 009, Article ID 868496, 6 pages doi:0.55/009/868496 Research Article Autonomic Testing in Functional Gastrointestinal Disorders: Implications of Reproducible
Gastroenterology Research and Practice Volume 009, Article ID 868496, 6 pages doi:0.55/009/868496 Research Article Autonomic Testing in Functional Gastrointestinal Disorders: Implications of Reproducible
SYMPATHETIC STRESSORS AND SYMPATHETIC FAILURES
 SYMPATHETIC STRESSORS AND SYMPATHETIC FAILURES Any discussion of sympathetic involvement in circulation, and vasodilation, and vasoconstriction requires an understanding that there is no such thing as
SYMPATHETIC STRESSORS AND SYMPATHETIC FAILURES Any discussion of sympathetic involvement in circulation, and vasodilation, and vasoconstriction requires an understanding that there is no such thing as
Syncope Guidelines Update. Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon
 Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists,
Syncope Guidelines Update Bernard Harbieh, FHRS AUBMC-KMC Beirut-Lebanon New Syncope Guidelines Increase the volume of information on diagnosis and management Incorporation of emergency specialists, neurologists,
SYNCOPE. Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope
 SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
SYNCOPE Sanjay P. Singh, MD Chairman & Professor, Department of Neurology. Syncope Syncope is a clinical syndrome characterized by transient loss of consciousness (TLOC) and postural tone that is most
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Joining The Dots - EDS
 Joining The Dots - EDS Ehlers-Danlos Syndrome (EDS) named after physicians Ehlers and Danlos turn of 20th Century What is EDS? 2017 new classification -up to date encompasses 14 different individual genetic
Joining The Dots - EDS Ehlers-Danlos Syndrome (EDS) named after physicians Ehlers and Danlos turn of 20th Century What is EDS? 2017 new classification -up to date encompasses 14 different individual genetic
Wednesday September 20 th CMT Regional Study Day. Dr Colin Mason, Consultant DME, Addenbrooke s Hospital
 Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Wednesday September 20 th CMT Regional Study Day Dr Colin Mason, Consultant DME, Addenbrooke s Hospital Develop a structured approach to a patient presenting with a fall Risk stratify who can go home and
Syncope: Evaluation of the Weak and Dizzy
 Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
Syncope: Evaluation of the Weak and Dizzy William M. Miles, MD, FACC, FHRS Professor of Medicine Silverstein Chair for Cardiovascular Education University of Florida College of Medicine Disclosures Medtronic,
I Can t Think Properly Brian Fog & POTS
 I Can t Think Properly Brian Fog & POTS Satish R Raj MD MSCI FACC FHRS Libin Cardiovascular Institute of Alberta University of Calgary Autonomic Dysfunction Center Vanderbilt University School of Medicine
I Can t Think Properly Brian Fog & POTS Satish R Raj MD MSCI FACC FHRS Libin Cardiovascular Institute of Alberta University of Calgary Autonomic Dysfunction Center Vanderbilt University School of Medicine
Disclosures. Adult Postural Orthostatic Tachycardia Syndrome (POTS) Topics. Objectives. Definition/Terminology. Epidemiology 2/2/2017
 Topics. Objectives. Definition/Terminology. Epidemiology 2/2/2017") Disclosures Adult Postural Orthostatic Tachycardia Syndrome (POTS) Nothing to disclose (no financial or pharmaceutical affiliations) All discussed pharmacologic treatments are off-label Juan J. Figueroa,
Disclosures Adult Postural Orthostatic Tachycardia Syndrome (POTS) Nothing to disclose (no financial or pharmaceutical affiliations) All discussed pharmacologic treatments are off-label Juan J. Figueroa,
Gut involvement in PoTS an overview
 Gut involvement in PoTS an overview Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology Case Hx * 28 year old lady presents with a long hx of constipation
Gut involvement in PoTS an overview Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology Case Hx * 28 year old lady presents with a long hx of constipation
Tilt training EM R1 송진우
 Tilt training 2006.7.15. EM R1 송진우 Introduction North American Vasovagal Pacemaker Study Randomized, controlled trial Reduction in the likelihood of syncope by dual chamber pacing with rate drop response
Tilt training 2006.7.15. EM R1 송진우 Introduction North American Vasovagal Pacemaker Study Randomized, controlled trial Reduction in the likelihood of syncope by dual chamber pacing with rate drop response
Postural Tachycardia Syndrome and Hypermobility Syndrome
 Postural Tachycardia Syndrome and Hypermobility Syndrome Blair P. Grubb MD FACC Departments of Medicine and Pediatrics Health Science Campus University of Toledo Toledo, Ohio USA Over the years it became
Postural Tachycardia Syndrome and Hypermobility Syndrome Blair P. Grubb MD FACC Departments of Medicine and Pediatrics Health Science Campus University of Toledo Toledo, Ohio USA Over the years it became
Tilt Table Testing. Dr. Prateek Suri
 Tilt Table Testing Dr. Prateek Suri Background Syncope is very commonly seen in the population Among the various causes of syncope vasovagal syncope is the most common cause There is an absence of a gold
Tilt Table Testing Dr. Prateek Suri Background Syncope is very commonly seen in the population Among the various causes of syncope vasovagal syncope is the most common cause There is an absence of a gold
Contempo GIMSI Cosa cambia alla luce della letteratura in tema di terapia farmacologica
 Contempo GIMSI 2015-2017 Cosa cambia alla luce della letteratura in tema di terapia farmacologica Dott.ssa Diana Solari Centro Aritmologico e Sincope Unit, Lavagna www.gimsi.it POST 2 (Prevention of Syncope
Contempo GIMSI 2015-2017 Cosa cambia alla luce della letteratura in tema di terapia farmacologica Dott.ssa Diana Solari Centro Aritmologico e Sincope Unit, Lavagna www.gimsi.it POST 2 (Prevention of Syncope
INTRODUCTION POTS is: Poorly understood Rarely considered SIGNIFICANT morbidity Appropriate initial diagnosis & care will expedite management of POTS
 Learning objectives At the end of this presentation the learner should: Define POTS & identify the various etiologies of POTS Be able to differentiate POTS from other causes of orthostatic intolerance
Learning objectives At the end of this presentation the learner should: Define POTS & identify the various etiologies of POTS Be able to differentiate POTS from other causes of orthostatic intolerance
:{ic0fp'16. Geriatric Medicine: Blood Pressure Monitoring in the Elderly. Terrie Ginsberg, DO, FACOI
 :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
Setting up and running an effective Syncope Service
 Setting up and running an effective Syncope Service P Boon Lim Consultant Cardiologist and Electrophysiologist Clinical Lead Syncope Diagnostic Unit Imperial College Healthcare NHS Trust Hammersmith Hospital
Setting up and running an effective Syncope Service P Boon Lim Consultant Cardiologist and Electrophysiologist Clinical Lead Syncope Diagnostic Unit Imperial College Healthcare NHS Trust Hammersmith Hospital
ME Association Transcript Royal Society Conference: Understanding the neurobiology of fatigue
 ME Association Transcript Royal Society Conference: Understanding the neurobiology of fatigue September 2017 Professor Julia Newton, Newcastle University, UK Standing up for fatigue Abstract Fatigue is
ME Association Transcript Royal Society Conference: Understanding the neurobiology of fatigue September 2017 Professor Julia Newton, Newcastle University, UK Standing up for fatigue Abstract Fatigue is
Indications and Uses of Testing. Laboratory Testing of Autonomic Function. Generalized Autonomic Failure. Benign Disorders 12/30/2012.
 Indications and Uses of Testing Laboratory Testing of Autonomic Function Conditions of generalized autonomic failure Help define the degree of autonomic dysfunction and distinguish more benign from life
Indications and Uses of Testing Laboratory Testing of Autonomic Function Conditions of generalized autonomic failure Help define the degree of autonomic dysfunction and distinguish more benign from life
Faculty Disclosure. Sanjay P. Singh, MD, FAAN. Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion
 Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Faculty Disclosure Sanjay P. Singh, MD, FAAN Dr. Singh has listed an affiliation with: Consultant Sun Pharma Speaker s Bureau Lundbeck, Sunovion however, no conflict of interest exists for this conference.
Ivabradine in Inappropriate Sinus Tachycardia
 UNIVERSITA DEGLI STUDI DI MILANO I.R.C.C.S POLICLINICO SAN DONATO CENTRO PER LO STUDIO E LA TERAPIA DELLLE MALATTIE CARDIOVASCOLARI E. MALAN Ivabradine in Inappropriate Sinus Tachycardia Riccardo Cappato,
UNIVERSITA DEGLI STUDI DI MILANO I.R.C.C.S POLICLINICO SAN DONATO CENTRO PER LO STUDIO E LA TERAPIA DELLLE MALATTIE CARDIOVASCOLARI E. MALAN Ivabradine in Inappropriate Sinus Tachycardia Riccardo Cappato,
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope
 Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
Medicine Dr. Aso Lecture 9 Syncope and Pre-syncope SYNCOPE AND PRE-SYNCOPE Syncope:- sudden, transient loss of consciousness, due to reduced cerebral perfusion. The patient is unresponsive with loss of
An Interview with a Chiropractor
 An Interview with a Chiropractor Doctor Scott Warner took the time out of his busy schedule to talk to us about chiropractic medicine what it is, what it isn t, and why he chose it as a profession. What
An Interview with a Chiropractor Doctor Scott Warner took the time out of his busy schedule to talk to us about chiropractic medicine what it is, what it isn t, and why he chose it as a profession. What
Cardiology Services Bon Secours Hospital. Mary Buckley Staff Nurse Cardiology
 Cardiology Services Bon Secours Hospital Mary Buckley Staff Nurse Cardiology Overview Philosophy Cardiology Team Referral Criteria Electrocardiograph (ECG) 24/48 Hour Holter Monitor Event Monitors 24 Hour
Cardiology Services Bon Secours Hospital Mary Buckley Staff Nurse Cardiology Overview Philosophy Cardiology Team Referral Criteria Electrocardiograph (ECG) 24/48 Hour Holter Monitor Event Monitors 24 Hour
Department of Paediatrics Clinical Guideline. Syncope Guideline
 Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
Department of Paediatrics Clinical Guideline Syncope Guideline Definition Transient, self-limited loss of consciousness (TLOC), usually leading to falling. Onset is relatively rapid. Recovery is spontaneous,
START AUDIO. You re listening to an audio module from BMJ Learning.
 BMJ LEARNING PODCAST TRANSCRIPT File: FINAL medically unexplained symptoms.mp3 Duration: 0:16:13 Date: 20/02/2014 Typist: TC6 START AUDIO Recording: You re listening to an audio module from BMJ Learning.
BMJ LEARNING PODCAST TRANSCRIPT File: FINAL medically unexplained symptoms.mp3 Duration: 0:16:13 Date: 20/02/2014 Typist: TC6 START AUDIO Recording: You re listening to an audio module from BMJ Learning.
Syncope Guidelines: What s New?
 Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope Guidelines: What s New? Dr. Samuel Asirvatham Professor of Medicine and Pediatrics Mayo Clinic College of Medicine Medical Director, Electrophysiology Laboratory Program Director, EP Fellowship
Syncope: The Pediatric Patient
 Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Syncope: The Pediatric Patient Lindsey Malloy-Walton, DO, MPH, FAAP Division of Pediatric Cardiology Children s Mercy Hospital 2401 Gillham Road Kansas City, MO 64108 Phone (office): 816-234-3255 Email:
Orthostatic Hypotension
 Orthostatic Hypotension http://suntechmed.web4.hubspot.com/portals/41365/images/bloodpressuredoctor.jpg Orthostatic (postural) hypotension is an excessive fall in BP when an upright position is assumed.
Orthostatic Hypotension http://suntechmed.web4.hubspot.com/portals/41365/images/bloodpressuredoctor.jpg Orthostatic (postural) hypotension is an excessive fall in BP when an upright position is assumed.
AUTONOMIC NEUROPATHY- PREDICTION OF COMPLICATIONS AND ITS RELEVANCE TO ANAESTHESIA
 AUTONOMIC NEUROPATHY- PREDICTION OF COMPLICATIONS AND ITS RELEVANCE TO ANAESTHESIA Dr.R.Selvakumar.M.D.,D.A.,DNB Assistant Professor, Dept. of Anaesthesiology, Madurai Medical College, Madurai. The human
AUTONOMIC NEUROPATHY- PREDICTION OF COMPLICATIONS AND ITS RELEVANCE TO ANAESTHESIA Dr.R.Selvakumar.M.D.,D.A.,DNB Assistant Professor, Dept. of Anaesthesiology, Madurai Medical College, Madurai. The human
Key Words: Autonomic, syncope, orthostatic tachycardia, orthostatic hypotension,
 Update on the theory and management of orthostatic intolerance and related syndromes in adolescents and children. Julian M. Stewart Departments of Physiology, Pediatrics and Medicine New York Medical College,
Update on the theory and management of orthostatic intolerance and related syndromes in adolescents and children. Julian M. Stewart Departments of Physiology, Pediatrics and Medicine New York Medical College,
Guidelines Pediatric Congenital Heart Disease SYNCOPE
 Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
Guidelines Pediatric Congenital Heart Disease SYNCOPE www.kinderkardiologie.org/dgpkleitlinien.shtm Definition and Characteristics of Syncope temporary loss of consciousness and tonicity due to inadequate
POSTURAL TACHYCARDIA SYNDROME (PoTS)
") Information Booklet POSTURAL TACHYCARDIA SYNDROME (PoTS) www.potsuk.org info@potsuk.org 1 CONTENTS What is PoTS? What are the symptoms of PoTS? How is PoTS diagnosed? What causes PoTS? What can I do to
Information Booklet POSTURAL TACHYCARDIA SYNDROME (PoTS) www.potsuk.org info@potsuk.org 1 CONTENTS What is PoTS? What are the symptoms of PoTS? How is PoTS diagnosed? What causes PoTS? What can I do to
THE BEST TIME IS NOW.
 THE BEST TIME to tackle osteoarthritis knee pain IS NOW. 1. TAKE ACTION 2. Consider synvisc-one Synvisc-One (hylan G-F 20) is indicated for the treatment of pain in osteoarthritis (OA) of the knee in patients
THE BEST TIME to tackle osteoarthritis knee pain IS NOW. 1. TAKE ACTION 2. Consider synvisc-one Synvisc-One (hylan G-F 20) is indicated for the treatment of pain in osteoarthritis (OA) of the knee in patients
HRV in Diabetes and Other Disorders
 HRV in Diabetes and Other Disorders Roy Freeman, MD Center for Autonomic and Peripheral Nerve Disorders Beth Israel Deaconess Medical Center Harvard Medical School Control Propranolol Atropine Wheeler
HRV in Diabetes and Other Disorders Roy Freeman, MD Center for Autonomic and Peripheral Nerve Disorders Beth Israel Deaconess Medical Center Harvard Medical School Control Propranolol Atropine Wheeler
AUTONOMIC FUNCTION TESTING Clinical Applications and Examples
 AUTONOMIC FUNCTION TESTING Clinical Applications and Examples Alejandro Ortiz-Burgos, MD University of Miami, Internal Medicine 27 June 2006 1 The Autonomic Nervous System 2 ANS Overview ANS controls or
AUTONOMIC FUNCTION TESTING Clinical Applications and Examples Alejandro Ortiz-Burgos, MD University of Miami, Internal Medicine 27 June 2006 1 The Autonomic Nervous System 2 ANS Overview ANS controls or
Syncope and Cardiovascular Causes of Falls in Older People. Professor T. Masud Nottingham University Hospitals NHS Trust
 Syncope and Cardiovascular Causes of Falls in Older People Professor T. Masud Nottingham University Hospitals NHS Trust Faller 1 75 male, smoker, moderate alcohol intake Retired driving instructor At least
Syncope and Cardiovascular Causes of Falls in Older People Professor T. Masud Nottingham University Hospitals NHS Trust Faller 1 75 male, smoker, moderate alcohol intake Retired driving instructor At least
Understanding Congestive Heart Failure
 Understanding Congestive Heart Failure Your health care team offers this information to help you and your family cope with congestive heart failure. It defines congestive heart failure, discusses ways
Understanding Congestive Heart Failure Your health care team offers this information to help you and your family cope with congestive heart failure. It defines congestive heart failure, discusses ways
Orthostatic instability is an important co-factor and trigger of reflex syncope
 Orthostatic instability is an important co-factor and trigger of reflex syncope Artur Fedorowski 1,2, Philippe Burri 2, Steen Juul-Möller 2, and Olle Melander 1,2 1 Lund University, Sweden 2 Skåne University
Orthostatic instability is an important co-factor and trigger of reflex syncope Artur Fedorowski 1,2, Philippe Burri 2, Steen Juul-Möller 2, and Olle Melander 1,2 1 Lund University, Sweden 2 Skåne University
Patient Resources: Syncope
 Patient Resources: Syncope Overview Syncope is the medical term for fainting or loss of consciousness. Fainting can occur for a few different reasons. The autonomic (involuntary) nervous system helps to
Patient Resources: Syncope Overview Syncope is the medical term for fainting or loss of consciousness. Fainting can occur for a few different reasons. The autonomic (involuntary) nervous system helps to
Disclosures. Where We Are Going. My Goals for Giving This Talk. Diagnosis and Management of Dysautonomia in the Pediatric Population
 Diagnosis and Management of Dysautonomia in the Pediatric Population Disclosures David M Bush, MD, PhD Pediatric Cardiology/Electrophysiology Pediatric Cardiology Associates of San Antonio Adjunct Associate
Diagnosis and Management of Dysautonomia in the Pediatric Population Disclosures David M Bush, MD, PhD Pediatric Cardiology/Electrophysiology Pediatric Cardiology Associates of San Antonio Adjunct Associate
POTS. Putting the Puzzle Pieces Together. Artur Fedorowski MD, Assoc.Prof. FESC Skåne University Hospital in Malmö and Lund University Sweden
 POTS Putting the Puzzle Pieces Together Artur Fedorowski MD, Assoc.Prof. FESC Skåne University Hospital in Malmö and Lund University Sweden 1993 These patients were usually women who experienced an acute
POTS Putting the Puzzle Pieces Together Artur Fedorowski MD, Assoc.Prof. FESC Skåne University Hospital in Malmö and Lund University Sweden 1993 These patients were usually women who experienced an acute
How to Talk to Your Doctor About Psoriatic Arthritis
 How to Talk to Your Doctor About Psoriatic Arthritis Preparing for your Doctor s Appointment Psoriatic arthritis is a type of arthritis that often occurs with psoriasis of the skin, a condition that features
How to Talk to Your Doctor About Psoriatic Arthritis Preparing for your Doctor s Appointment Psoriatic arthritis is a type of arthritis that often occurs with psoriasis of the skin, a condition that features
Orthostatic Intolerance (OI) In the Young. (orthostasis = standing) (OI= Can t remain standing)
 In the Young. (orthostasis = standing) (OI= Can t remain standing)") Orthostatic Intolerance (OI) In the Young (orthostasis = standing) (OI= Can t remain standing) Gravitational Blood Distribution in Man and Beast Unconstrained Pooling Causes Rapid Loss of BP Circulatory
Orthostatic Intolerance (OI) In the Young (orthostasis = standing) (OI= Can t remain standing) Gravitational Blood Distribution in Man and Beast Unconstrained Pooling Causes Rapid Loss of BP Circulatory
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital
 Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
Syncope : What tests should I do? Boon Lim Consultant Cardiologist Clinical Lead for Imperial Syncope Unit Hammersmith Hospital The most important diagnostic test is History taking Why is history taking
 Ian Carroll MD, MS https://med.stanford.edu/profiles/ian-carroll CarrollCSFleak@gmail.com SIH and/or POTS? Disclosures No Conflicts of Interest This work is supported by the Considine CSF Leaks Fund Thank
Ian Carroll MD, MS https://med.stanford.edu/profiles/ian-carroll CarrollCSFleak@gmail.com SIH and/or POTS? Disclosures No Conflicts of Interest This work is supported by the Considine CSF Leaks Fund Thank
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect
 Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
Vasovagal Syncope and Bradyarrhythmias Mechanisms, distinguishing cause and effect Walid Saliba, MD, FHRS, FACC Director EP lab Director Atrial Fibrillation Center Department of Cardiovascular Medicine
 Original citation: Macdougall, Colin. (2009) Food intolerance in children (non-allergenic food hypersensitivity). Paediatrics and Child Health, Vol.19 (No.8). pp. 388-390. ISSN 1751-7222 Permanent WRAP
Original citation: Macdougall, Colin. (2009) Food intolerance in children (non-allergenic food hypersensitivity). Paediatrics and Child Health, Vol.19 (No.8). pp. 388-390. ISSN 1751-7222 Permanent WRAP
PRESENTED BY BECKY BLAAUW OCT 2011
 PRESENTED BY BECKY BLAAUW OCT 2011 Introduction In 1990 top 5 causes of death and disease around the world: Lower Respiratory Tract Infections Diarrhea Conditions arising during pregnancy Major Depression
PRESENTED BY BECKY BLAAUW OCT 2011 Introduction In 1990 top 5 causes of death and disease around the world: Lower Respiratory Tract Infections Diarrhea Conditions arising during pregnancy Major Depression
Patient Clinic Leaflet. chronic fatigue syndrome (CFS) myalgic encephalomyelitis or myalgic encephalopathy (ME)
 myalgic encephalomyelitis or myalgic encephalopathy (ME)") Patient Clinic Leaflet Basic information on your illness and the treatments we can offer you for chronic fatigue syndrome (CFS) also known as myalgic encephalomyelitis or myalgic encephalopathy (ME) Chronic
Patient Clinic Leaflet Basic information on your illness and the treatments we can offer you for chronic fatigue syndrome (CFS) also known as myalgic encephalomyelitis or myalgic encephalopathy (ME) Chronic
Augusto Morales, MD; Andreea I. Stoichita, MD; and Jessica D. Wharton, MD
 Original Research Orthostatic Intolerance and Other Autonomic Symptoms in Adolescents With Headaches Augusto Morales, MD; Andreea I. Stoichita, MD; and Jessica D. Wharton, MD From the Department of Pediatrics,
Original Research Orthostatic Intolerance and Other Autonomic Symptoms in Adolescents With Headaches Augusto Morales, MD; Andreea I. Stoichita, MD; and Jessica D. Wharton, MD From the Department of Pediatrics,
The Atrial Fibrillation Clinic in Llanelli. Dr Lena Marie Izzat Consultant Cardiovascular Physician
 The Atrial Fibrillation Clinic in Llanelli Dr Lena Marie Izzat Consultant Cardiovascular Physician Llanelli Multidisciplinary AF Clinic Went live January 2009 Based on the fact that Carmarthenshire has
The Atrial Fibrillation Clinic in Llanelli Dr Lena Marie Izzat Consultant Cardiovascular Physician Llanelli Multidisciplinary AF Clinic Went live January 2009 Based on the fact that Carmarthenshire has
the study to patients evaluated clinically by 2 of the authors (P.S., P.A.L.). Symptoms of orthostatic intolerance, aggravating factors, antecedent il
. Symptoms of orthostatic intolerance, aggravating factors, antecedent il") ORIGINAL ARTICLE POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME Postural Orthostatic Tachycardia Syndrome: The Mayo Clinic Experience MARK J. THIEBEN, MD; PAOLA SANDRONI, MD, PHD; DAVID M. SLETTEN; LISA M.
ORIGINAL ARTICLE POSTURAL ORTHOSTATIC TACHYCARDIA SYNDROME Postural Orthostatic Tachycardia Syndrome: The Mayo Clinic Experience MARK J. THIEBEN, MD; PAOLA SANDRONI, MD, PHD; DAVID M. SLETTEN; LISA M.
Pain Notebook NAME PHONE. Three Hole Punch Here Three Hole Punch Here. Global Pain Initiative 2018 Ver 1.0
 Pain Notebook Three Hole Punch Here Three Hole Punch Here NAME EMAIL PHONE Global Pain Initiative 2018 Ver 1.0 What is pain? Pain is a bad sensation that tells you something is wrong. Pain falls into two
Pain Notebook Three Hole Punch Here Three Hole Punch Here NAME EMAIL PHONE Global Pain Initiative 2018 Ver 1.0 What is pain? Pain is a bad sensation that tells you something is wrong. Pain falls into two
droxidopa (Northera )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
Presentation of transient loss of consciousness
 Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Presentation of transient loss of consciousness Definition of transient loss of consciousness Transient loss of consciousness: sudden onset, complete loss of consciousness of brief duration with relatively
Clinical Studies 129
 Clinical Studies 129 Syncope in migraine. The population-based CAMERA study Roland D. Thijs, 1* Mark C. Kruit, 2* Mark A. van Buchem, 2 Michel D. Ferrari, 1 Lenore J. Launer, 3,4 and J. Gert van Dijk
Clinical Studies 129 Syncope in migraine. The population-based CAMERA study Roland D. Thijs, 1* Mark C. Kruit, 2* Mark A. van Buchem, 2 Michel D. Ferrari, 1 Lenore J. Launer, 3,4 and J. Gert van Dijk
some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment
 some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment This booklet was created to help you learn about opioids. You probably have lots
some things you should know about opioids before starting a prescription an informational booklet for opioid pain treatment This booklet was created to help you learn about opioids. You probably have lots
Section 5 Treatment and health service provision
 Section 5 Treatment and health service provision Section 4: Experience of treatment Summary Treatments experienced The most commonly treatments reported were beta blockers (n=37; 74.%), followed by diuretics
Section 5 Treatment and health service provision Section 4: Experience of treatment Summary Treatments experienced The most commonly treatments reported were beta blockers (n=37; 74.%), followed by diuretics
Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP
 Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology GI involvement in autonomic dysfunction Conditions Diabetes
Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology GI involvement in autonomic dysfunction Conditions Diabetes
Managing the patient with episodic sinus tachycardia and orthostatic intolerance
 REVIEW ARTICLE Cardiology Journal 2014, Vol. 21, No. 6, 665 673 DOI: 10.5603/CJ.2014.0098 Copyright 2014 Via Medica ISSN 1897 5593 Managing the patient with episodic sinus tachycardia and orthostatic intolerance
REVIEW ARTICLE Cardiology Journal 2014, Vol. 21, No. 6, 665 673 DOI: 10.5603/CJ.2014.0098 Copyright 2014 Via Medica ISSN 1897 5593 Managing the patient with episodic sinus tachycardia and orthostatic intolerance
Shared Care Guideline
 Shared Care Guideline Midodrine for Orthostatic hypotension and neurocardiogenic syncope Executive Summary Update of Guideline following licencing of drug. The responsibility for initiating midodrine will
Shared Care Guideline Midodrine for Orthostatic hypotension and neurocardiogenic syncope Executive Summary Update of Guideline following licencing of drug. The responsibility for initiating midodrine will
Disorders of the Autonomic Nervous System: Part 2. Investigation and Treatment*
 NEUROLOGICAL PROGRESS Disorders of the Autonomic Nervous System: Part 2. Investigation and Treatment* J. G. McLeod, PPhil, FRACP, and R. R. Tuck, PhD, FRACP Autonomic function may be adequately tested
NEUROLOGICAL PROGRESS Disorders of the Autonomic Nervous System: Part 2. Investigation and Treatment* J. G. McLeod, PPhil, FRACP, and R. R. Tuck, PhD, FRACP Autonomic function may be adequately tested
Treatment of orthostatic hypotension in Multiple System Atrophy New Clinical Studies
 Treatment of orthostatic hypotension in Multiple System Atrophy New Clinical Studies Cyndya A. Shibao, M.D., F.A.H.A. Assistant Professor of Medicine Division of Clinical Pharmacology Disclosure Lundbeck
Treatment of orthostatic hypotension in Multiple System Atrophy New Clinical Studies Cyndya A. Shibao, M.D., F.A.H.A. Assistant Professor of Medicine Division of Clinical Pharmacology Disclosure Lundbeck
Neurogenic orthostatic hypotension: the very basics
 Clin Auton Res (2017) 27:39 43 DOI 10.1007/s10286-017-0437-3 EDITORIAL Neurogenic orthostatic hypotension: the very basics Horacio Kaufmann 1 Jose-Alberto Palma 1 Received: 7 June 2017 / Accepted: 8 June
Clin Auton Res (2017) 27:39 43 DOI 10.1007/s10286-017-0437-3 EDITORIAL Neurogenic orthostatic hypotension: the very basics Horacio Kaufmann 1 Jose-Alberto Palma 1 Received: 7 June 2017 / Accepted: 8 June
David Saperstein, MD Center for Complex Neurology.
 Patient Name: Patient DOB: Patient Phone: Patient Email: David Saperstein, MD Center for Complex Neurology Ph 602-900-94043354 Fax 602-391-2344 www.complexneurology.com I am pleased that you are seeking
Patient Name: Patient DOB: Patient Phone: Patient Email: David Saperstein, MD Center for Complex Neurology Ph 602-900-94043354 Fax 602-391-2344 www.complexneurology.com I am pleased that you are seeking
NEW PATIENT QUESTIONNAIRE For Dr Benoy Benny. Section 1: Today s Date: Date of Birth: Age:
 Baylor Physical Medicine and Rehabilitation NEW PATIENT QUESTIONNAIRE For Dr Benoy Benny Dear Patient: Please complete this questionnaire before you come for your appointment. Be sure to call us as soon
Baylor Physical Medicine and Rehabilitation NEW PATIENT QUESTIONNAIRE For Dr Benoy Benny Dear Patient: Please complete this questionnaire before you come for your appointment. Be sure to call us as soon
NEURO QUIZ 45 EHLERS DANLOS SYNDROME
 NEURO QUIZ 45 EHLERS DANLOS SYNDROME Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D START 1. Regarding
NEURO QUIZ 45 EHLERS DANLOS SYNDROME Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D START 1. Regarding
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare. Andrea Ungar, MD, PhD, FESC
 Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies. Falls can be classified into four main groups:
 What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
What are you trying to achieve? Falls Prevention, Assessment and Management Strategies Dr Adam Darowski Community: Falls risk assessment: Falls risk is 50% per year in 80yr population and higher in those
HOLEP (HOLMIUM LASER ENUCLEATION OF PROSTATE )
") HOLEP (HOLMIUM LASER ENUCLEATION OF PROSTATE ) What does the procedure involve? Removal of obstructing prostate tissue using a telescope and a laser. What are the alternatives to this procedure? Alternatives
HOLEP (HOLMIUM LASER ENUCLEATION OF PROSTATE ) What does the procedure involve? Removal of obstructing prostate tissue using a telescope and a laser. What are the alternatives to this procedure? Alternatives
Syncope By Remus Popa
 Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope By Remus Popa A 66 years old male is brought to the ED from a restaurant where he fainted while dining out with his family. He complained of nausea and stood up to go to the restroom but immediately
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018
 Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018") Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Syncope (From a Cardiologist s Perspective) Patrick Henderson, DO 118 th OOA Annual Convention Internal Medicine Specialty Track April 28 th, 2018 No financial disclosures to report Goals Formally define
Dysautonomia: Experience from a Large Single Center
 Dysautonomia: Experience from a Large Single Center David S. Cannom, M.D. Clinical Professor of Medicine UCLA School of Medicine Good Samaritan Hospital/Cedars Sinai Heart Institute September 13, 2018
Dysautonomia: Experience from a Large Single Center David S. Cannom, M.D. Clinical Professor of Medicine UCLA School of Medicine Good Samaritan Hospital/Cedars Sinai Heart Institute September 13, 2018
SUPRA PUBIC CATHETER(SPC)
") Suprapubic versus urethral catheter? When a long-term catheter to drain the bladder is advised, it can be placed in the urethra (water pipe) or suprapubically (directly into the bladder through the skin
Suprapubic versus urethral catheter? When a long-term catheter to drain the bladder is advised, it can be placed in the urethra (water pipe) or suprapubically (directly into the bladder through the skin
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
DECLARATION OF CONFLICT OF INTEREST The Management of Syncope remains a challenge: Clues from the History Richard Sutton, DSc Emeritus Professor of Cardiology Imperial College, St Mary s Hospital, London,
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST CARDIAC INVESTIGATIONS PAEDIATRIC & CONGENITAL SYNCOPE INVESTIGATIONS/QUESTIONNAIRE PROTOCOL Written Date: 2009 by Dr Duke, then updated by Dr Sarita Makam 12/4/2016
Baroreflex sensitivity and responses to the Valsalva manoeuvre in subjects with diabetes mellitus
 Journal of Neurology, Neurosurgery, and Psychiatry, 1976, 39, 178-183 Baroreflex sensitivity and responses to the Valsalva manoeuvre in subjects with diabetes mellitus T. BENNETT,' D. J. HOSKNG, AND J.
Journal of Neurology, Neurosurgery, and Psychiatry, 1976, 39, 178-183 Baroreflex sensitivity and responses to the Valsalva manoeuvre in subjects with diabetes mellitus T. BENNETT,' D. J. HOSKNG, AND J.
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1
 Lecture 14 Cardiovascular control mechanisms p. 1") BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
BIPN100 F15 Human Physiol I (Kristan) Lecture 14 Cardiovascular control mechanisms p. 1 Terms you should understand: hemorrhage, intrinsic and extrinsic mechanisms, anoxia, myocardial contractility, residual
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders
 C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
C1: Medical Standards for Safety Critical Workers with Cardiovascular Disorders GENERAL ISSUES REGARDING MEDICAL FITNESS-FOR-DUTY 1. These medical standards apply to Union Pacific Railroad (UPRR) employees
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
EVALUATION & MANAGEMENT OF AUTONOMIC DYSFUNCTION IN EDS (Transcript)
") The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
The Ehlers-Danlos Society P.O. Box 87463 Montgomery Village, MD 20886 USA Phone: +1 410-670-7577 The Ehlers-Danlos Society - Europe Office 7 35-37 Ludgate Hill London EC4M 7JN UK Phone: +44 203 887 6132
Atrial Fibrillation. A guide for Southwark General Practice. Key Messages. Always work within your knowledge and competency
 Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
Atrial Fibrillation A guide for Southwark General Practice Key Messages 1. Routinely offer pulse checks to patients at high risk of AF 2. Use the CHA 2 DS 2 VASc score to identify patients for anticoagulation
The symptom recognition and help- seeking experiences of men in Australia with testicular cancer: A qualitative study
 The symptom recognition and help- seeking experiences of men in Australia with testicular cancer: A qualitative study Stephen Carbone,, Susan Burney, Fiona Newton & Gordon A. Walker Monash University gordon.walker@med.monash.edu.au
The symptom recognition and help- seeking experiences of men in Australia with testicular cancer: A qualitative study Stephen Carbone,, Susan Burney, Fiona Newton & Gordon A. Walker Monash University gordon.walker@med.monash.edu.au
Warfarin PATIENT EDUCATION
 Warfarin PATIENT EDUCATION Information for patients taking warfarin Read this booklet to learn: What warfarin is and why you are taking it What blood tests you need to use warfarin safely How other medicines
Warfarin PATIENT EDUCATION Information for patients taking warfarin Read this booklet to learn: What warfarin is and why you are taking it What blood tests you need to use warfarin safely How other medicines
The recommended protocol is for all patients suffering from diabetes to have yearly foot checks. This was checking the foot pulses and doing
 Foot disease is a common long-term complication of diabetes. There are different types of foot disease caused by diabetes, but they all stem from a similar process. Raised blood sugar for a prolonged amount
Foot disease is a common long-term complication of diabetes. There are different types of foot disease caused by diabetes, but they all stem from a similar process. Raised blood sugar for a prolonged amount