Comprehensive Review of Clinical Laboratory Tests for Investigating the Etiology of Anemia in the Elderly.
|
|
|
- Fay Banks
- 6 years ago
- Views:
Transcription
1 Comprehensive Review of Clinical Laboratory Tests for Investigating the Etiology of Anemia in the Elderly. December 15, 2017 Dennis J Chapron MS, RPh Medication Safety Pharmacist Saint Francis Hospital and Medical Center Hartford, CT Dennis J Chapron reports no real or potential conflicts of interest relevant to this lecture. 1
2 At the conclusion of this knowledge based activity, the participant will be able to: Compare the kinetic vs the morphological approach for identifying the cause of anemia. Discuss the laboratories tests used to investigate and differentiate anemia due to nutrient deficiency, blood loss, hemolysis, chronic inflammation, renal failure and marrow failure. Describe the physiological mechanisms that maintain adequate nutrients for red cell production and how diseases and medications adversely affect these mechanisms. WHO Definition of Anemia In woman: hemoglobin concentration below 12 gm/dl. In men: hemoglobin concentration below 13 gm/dl 2
3 Hematocrit Approx 3 x Hgb Plasma Packed RBCs Anemia Severity Scale Mild anemia Hgb >10<12 Moderate anemia Hgb >8 10 Severe anemia 8 3
4 Estimated Anemia Prevalence in the Elderly Based on WHO definition 12% in those living in the community 40% in those admitted to the hospital 47% in nursing home residents Hematologica 2014;99:1127 Some Disorders Associated with a High Prevalence of Anemia in the Elderly Chronic upper and lower GI bleeding Chronic inflammatory disorders Heart failure Cancer Debility Chronic renal failure Unintentional weight loss 4

5 Anemia is Often an Important Sign of an Underlying Pathological Process Anemia is common in the elderly. Anemia impacts morbidity Anemia impacts mortality Am Fam Phys Sept
6 Anemia Morbidity/Mortality and QOL Anemia Disease M/M and QOL 6
7 Anemia and the Elderly Anemia in the elderly is due to a primary underlying disease and is not related to aging. Look for the problem behind the problem. Anemia: Problems in Diagnosis and Treatment Not recognized (not in problem list) Recognized but not investigated Recognized, investigated (at least partially), but failure to treat or considered not worth treating. Recognized, investigated and treated suboptimally 7
8 Types and Prevalence of Anemia Observed in Geriatric Populations Anemia of chronic inflammation 20% Iron deficiency anemia 17% Vitamin B 12 or folate deficiency 15% Chronic kidney disease 9% Kidney disease with inflammation 5% Unexplained anemia 34% NHANES III Blood 2004;104: Conceptual Views of Anemia Etiology 8
9 Kinetic Approach Steady-state [hemoglobin] PRODUCTION RATE [Hgb] = CLEARANCE DJ Chapron Kinetic Approach Bone marrow Nutritional PRODUCTION RATE [Hgb] = CLEARANCE Bleeding Hemolysis DJ Chapron 9
10 Hematology Basic Principles and Practices 2013 Chronic inflammation Hemolysis MDS/Ca EP Bone marrow RBCs Kidney Bleeding Iron, B-12, folate DJ Chapron 10
11 Reticulocyte Count (RC) Immature red cell released from bone marrow into the circulating blood and contains residual ribosomal RNA that can be stained with special dyes. Normal RC is about 1% (range %). Helps to define mechanism of anemia by defining the appropriateness of the bone marrow response to a low hemoglobin level. They are almost twice as large a mature erythrocytes and when present in increased numbers raise the MCV. Increased peripheral blood reticulocytes indicate increased marrow erythroid activity and a normal erythropoietin response. Increased reticulocyte counts indicate a high RBC turnover caused by either hemolysis or blood loss. RC is adjusted to the Hct yielding a value known as the reticulocyte index (RI). In anemic patients with chronic bleeding (with normal iron stores) or hemolytic disorders, the RI is 3% or greater. Anemias due to compromised red cell production, the RI is less than 3%, often in the range of 1.5% or less. RI = RC x Patient Hct /45% Kinetic Classification of Anemia Decreased production (Retics decreased) Stem cell and progenitor cell-based Aplastic anemia Pure red cell aplasia Leukemia Myelodysplastic syndrome Marrow infiltration Anemia of chronic inflammation Anemia of chronic renal failure Nutritional deficiency Vitamin B-12 Folate Iron 11
12 Kinetic Classification of Anemia Increased destruction (Retics increased) Intracorpuscular Membrane (hereditary) Enzyme deficicency (G6PD) Hemoglobinopathy (sickle cell) Extracorpuscular-immunological Autoimmune Alloimmune Extracorpuscular Acute / chronic blood loss Chemicals (oxidative stress) Hypersplenism Infectious Mechanical (heart valve) Chronic inflammation Hemolysis MDS/Ca EP Bone marrow RBCs Kidney Bleeding Iron, B-12, folate DJ Chapron 12
13 13
14 Morphological Approach Anemias According to Cell Size (MCV) Microcytic - MCV< 80 fl Normocytic MCV fl Macrocytic MCV > 100 fl MCV = mean corpuscular volume 14

15 Microcytosis Normocytic and Macrocytosis hypochromia normochromic Hillman and Finch 1985 UpToDate
16 Morphological Classification of Anemia Microcytic (MCV <80 fl) Iron deficiency (chronic blood loss) Anemia of chronic inflammation Thalassemias Sideroblastic anemias Aluminum toxicity Normocytic (MCV fl) Anemia of chronic inflammation Anemia of renal disease Acute blood loss Morphological Classification of Anemia Macrocytic (MCV >100 fl): Megaloblastic Folate deficiency Vitamin B-12 deficiency Medications Nonmegaloblastic Ethanol abuse Hypothyroidism Liver disease Primary bone marrow disease Reticulocytosis 16
17 Multiple Choice Question : A key component of the kinetic approach to anemia classification is: a. Mean corpuscular volume (MCV) b. Mean corpuscular hemoglobin concentration (MCHC) c. The reticulocyte response d. Nutritional indices including serum folate, vitamin B 12 and iron. 17

18 ECCO Anemia Statement JCDC
19 The Diagnosis of Anemia is Dependent on Laboratory Measurements Initial Testing Hemoglobin Hematocrit Complete blood count Red Cell Indices mean corpuscular volume (MCV), MCH mean hemoglobin (MCH), mean hemoglobin concentration (MCHC) Reticulocyte count Red Blood Cell distribution width (RDW) Examination of peripheral blood smear Complete Blood Count (CBC) CBC includes red cells, white cells and platelets. CBC helps to distinguish isolated anemia from pancytopenia or bicytopenia. 19
20 Red Cell Indices MCV mean cell volume, normal being fl. Accurately detects any general increase or decrease in red blood cell volume. MCH mean cell hemoglobin an excellent measure of the amount of hemoglobin in each individual red blood cell. Patients with IDA show significant reductions in the MCH. Normal value is pg MCHC mean corpuscular hemoglobin concentration. Not sensitive to disorders where Hgb production is defective, since such disorders are paralleled by reductions in cells size. Normal value is g/dl. Red Blood Cell Distribution Width (RDW) Normal RDW is % An index of the distribution of red cell volumes and is a mathematical representation of anisocytosis (variation in red cell size). Increases in RDW suggest the presence of a mixed population of cells (ex., microcytes with normal cells, or macrocytes with normal cells). 20
21 Iron Deficiency Anemia (IDA) The Diagnosis of Anemia is Dependent on Laboratory Measurements Initial Testing Hemoglobin Hematocrit Red Cell Indices mean corpuscular volume (MCV), MCH mean hemoglobin (MCH), mean hemoglobin concentration (MCHC) Reticulocyte count Red Blood Cell distribution width (RDW) Examination of peripheral blood smear 21
22 COMPREHENISVE LABORATORY EVALUATION OF ANEMIA Complete blood count (CBC) Hemoglobin/ hematocrit Red cell indices: MCV, MCH, MCHC Red blood cell distribution width (RDW) Peripheral smear Total reticulocyte count: absolute number or as a percentage: Serum [iron] Total iron binding capacity (TIBC) Percent transferrin saturation: (serum iron / TIBC) Serum [ferritin] Serum [folate] Serum [vitamin B-12], methylmalonic acid, homocysteine Serum [haptoglobin], [bilirubin (indirect)], [LDH] Serum [erythropoietin] Serum [transferrin receptors] Stool for occult blood Seminars in Nephrology
 Serum Fe --- Transferrin complex Bone marrow Fe/TIBC = %")
23 Seminars in Nephrology 2016 GI Fe absorption Serum Fe + Transferrin (TIBC) Serum Fe --- Transferrin complex Bone marrow Fe/TIBC = % saturation 23
24 Serum [Iron] ( ug/dl) as circulating transferrin bound iron. Serum iron levels are higher in the morning and levels should be determined on fasting AM samples. Total Iron Binding Capacity (TIBC) Transferrin is a circulating transport protein for iron. TIBC is a measure of the amount of iron that can be bound by transferrin and is equivalent to measuring the serum concentration of transferrin protein. Normal TIBC is ug/dl Transferrin saturation (T sat) is the ratio expressed as: serum iron/tibc x 100. Normal values are 25 45%. A transferrin level (mg/dl) can be converted to a TIBC (mcg/dl) by multiplying by TIBC levels are increased in IDA and normal or reduced in anemia of chronic disease (ACD). In IDA, serum iron is reduced while TIBC is increased yielding a low T sat. A T sat < 10 16% is often used as a cutoff for IDA. In iron overload (ex., hereditary hemochromatosis) T sat often approaches %. 24
25 T-SAT = Transferrin saturation Iron deficiency anemia [Fe] TSAT = IBC Serum Ferritin Normal levels in adult men and postmenopausal women are ug/l. A circulating iron storage protein that is proportional to body iron stores and primarily reflects hepatic iron stores. A very low ferritin is very specific for absolute iron deficiency (<15/20/30 ug/l). Serum ferritin may increase due to underlying inflammation. In the presence of inflammation serum ferritin can be high despite very low iron stores. In the presence of inflammation, a serum ferritin 100 ug/l may still be consistent with absolute iron deficiency. Massive increases in serum [ferritin] (>1000) are seen in patients with iron overload (hemochromatosis), hepatocellular disease, and malignancies. 25
26 Iron Deficiency Anemia Bone marrow Nutritional PRODUCTION RATE [Hgb] = CLEARANCE Bleeding Hemolysis Kinetic Classification of Anemia Decreased production (Retics decreased) Stem cell and progenitor cell-based Aplastic anemia Pure red cell aplasia Leukemia Myelodysplastic syndrome Marrow infiltration Anemia of chronic inflammation Anemia of chronic renal failure Nutritional deficiency Vitamin B-12 Folate Iron 26
27 Morphological Classification of Anemia Macrocytic (MCV >100 fl): Megaloblastic Folate deficiency Vitamin B-12 deficiency Medications Nonmegaloblastic Ethanol abuse Hypothyroidism Liver disease Primary bone marrow disease (MDS) Reticulocytosis Morphological Classification of Anemia Microcytic (MCV <80 fl) Iron deficiency Anemia of chronic inflammation Thalassemias Sideroblastic anemias Aluminum toxicity Normocytic (MCV fl) Anemia of chronic inflammation Anemia of renal disease Acute blood loss 27
28 COMMON CAUSES OF IRON DEFICIENCY ANEMIA Deficient diet (vegetarian, malnutrition) Decreased absorption (celiac disease, partial gastrectomy,) Increased requirements pregnancy lactation Blood loss gastrointestinal menstrual blood donation Hemoglobinuria (traumatic hemolysis from cardiac valve) ENDOSCOPIC LESIONS ASSOCIATED WITH OCCULT BLOOD LOSS ESOPHAGOGASTRODUODENOSCOPY (EGD) Esophagitis Gastric ulcer Gastritis Duodenal ulcer Duodenitis Carcinoma Vascular ectasia Adenomatous polyp COLONOSCOPY Adenoma Carcinoma Colitis Vascular ectasia (angiodysplasia) Ulceration NEJM 12/2/93 28
29 NEJM 1993;329:
30 Microcytosis Normocytic and Macrocytosis hypochromia normochromic Hillman and Finch


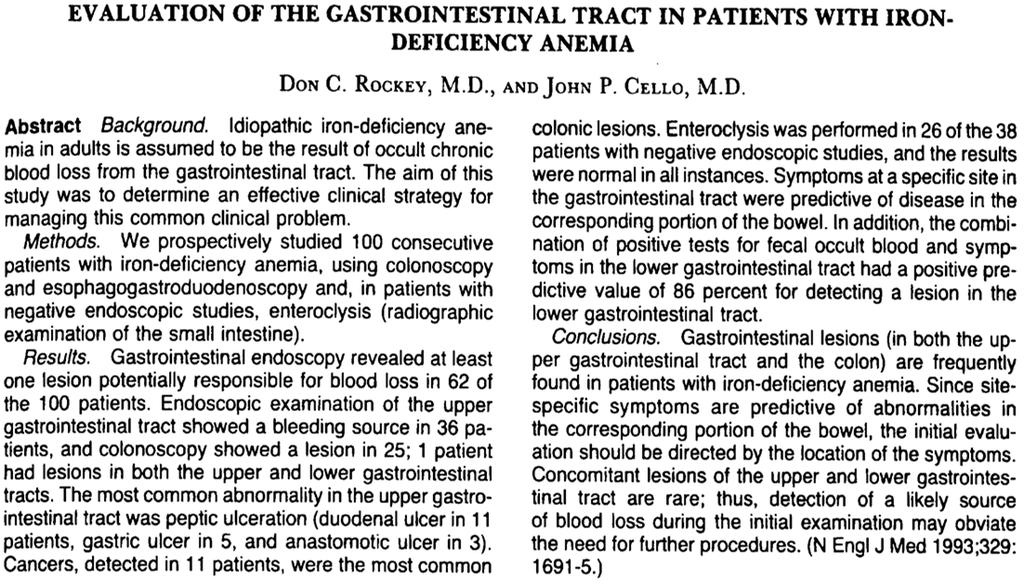
31 Normal RBCs, a single granulocyte and many platelets. Hillman and Ault 2002 Microcytosis with hypochromia, anisocytosis and poikilocytosis 31

 Schmaier")
32 12/1/2017 Normal erythrocytes Schmaier 2003 Iron deficiency anemia RBCs - micocytic and hypochromic (central pallor >1/3 diameter of cell) Schmaier


33 Severe microcytosis and hypochromia due to IDA Severe iron deficiency anemia Hillman and Ault
34 Iron Deficiency Anemia Case -1 Anemia Case-1 An 84 year old woman complains of not feeling well. She says she is having dizzy spells, problems with walking and cannot concentrate on certain tasks. These symptoms seem to have developed gradually over the last several months. 34
35 Anemia Case-1 This 84 year old woman has formidable problem and medication lists, which includes the following: 84 year old woman; her problem list: CAD (MI CABG) HTN Hyperlipidemia COPD GERD with hx PUD OA Hypothyroidism Depression OP 35
36 Medication List L-thyroxine 125 mcg qd Aspirin 81 mg qd Clopidogrel 75 mg qd Simvastatin 20 mg qd Escitalopram 10 mg qd Lansoprazole 30 mg bid Calcium carbonate 500 bid Metoprolol 50 mg bid Multivitamin 1 qd DOSS 100 mg bid Ipratropium/albuterol nebs tid Anemia Case -1 A complete blood count is obtained and reveals the following: Hemoglobin = 8.8 gm/dl Hematocrit = 27 % MCV = 70 fl ( fl) MCH = 22 pg/cell (26-34) MCHC 31 gm/dl (31-37) White blood cell and platelet cts - normal 36
37 Anemia Case 1 Classification Microcytic, hypochromic anemia Anemia case -1 A complete blood count is obtained and reveals the following: Hemoglobin = 8.8 gm/dl Hematocrit = 27 % MCV = 70 fl ( fl) Reticulocyte count = 0.5% ( %) Corrected as RI = 27/45 x 0.5% = 0.3% 37
38 Anemia Case 1 Classification Microcytic, hypochromic anemia Hypoproliferative Same 84 Year old woman Serum iron ( ug/dl) 14 TIBC ( ug/dl) 460 % saturation (25 45%) 3 Ferritin ( ug/l) 15 38
39 Anemia Case 1 Classification Microcytic, hypochromic anemia Hypoproliferative Iron indices indicate iron deficiency anemia Anemia Case -1 Stools are positive for occult blood 39
40 Anemia Case -1 Stools are positive for occult blood Is blood loss upper or lower GI tract? Anemia Case 1 Classification Microcytic, hypochromic anemia Hypoproliferative Iron indices indicate iron deficiency anemia Dx GI bleeding blood loss anemia, with PPI use lower GI bleeding may be more likely. Consider combined effects of aspirin, clopidogrel and escitalopram. 40
41 Temporal relationship between laboratory tests results and the evolution/stages of iron deficiency anemia 41

42 Hillman and Finch
43 Stages of Iron Deficiency Anemia Storage iron - Serum ferritin Serum iron - TIBC - Percent saturation Hemoglobin / Hematocrit Microcytosis / Hypochromia Anemia of Chronic Disease Anemia of Chronic Inflammation 43
44 Chronic inflammation Bone marrow Nutritional PRODUCTION RATE [Hgb] = CLEARANCE Bleeding Hemolysis DJ Chapron Chronic inflammation Hemolysis MDS/Ca EP Bone marrow RBCs Kidney Bleeding Iron, B-12, folate DJ Chapron 44
45 Anemia of Chronic Disease Occurs in patients with acute or chronic immune activation. Elevated pro inflammatory cytokines (esp IL 6) mediate the induction of hepcidin synthesis. Hepcidin inhibits intestinal iron absorption and the release of recycled iron from macrophages, resulting in iron restrictive anemia. Serum iron and transferrin levels are depressed as well transferrin saturation. This is referred to as a functional iron deficiency where iron stores are normal, but with a restricted iron availability in the bone marrow and a resulting reduced erythropoiesis. Elevated cytokines reduce erythropoietin production and inhibit bone marrow erythropoiesis. There is enhanced apoptosis of erythroid progenitor cells in the marrow Hematologica 2014;99:
46 Iron Restricted Anemia Any anemia where the bone marrow erythropoietic activity is reduced due to a restricted availability of iron in the bone marrow, either by true/absolute iron deficiency or functional iron deficiency. Absolute iron deficiency Iron deficiency anemia Hypoferremia [Fe] Anemia of Chronic Disease Decreased GI iron absorption and Increased iron sequestration by RES 46

47 J Clin Epi 1994; 47:23 47
 and a TSAT")
48 J Clin Epi 1994; 47:23 Anemia of Chronic Inflammation Biochemical and/or clinical evidence of inflammation Decreased serum iron Decreased iron binding capacity Normal iron stores (stainable iron in the bone marrow or elevated serum ferritin (> 100 ug/l) and a TSAT < 20% 48
49 T-SAT = Transferrin saturation Anemia of chronic disease [Fe] TSAT = IBC Iron deficiency anemia [Fe] TSAT = IBC Anemia of Chronic Disease (ACD) When anemia occurs in the presence of biochemical or clinical evidence of inflammation, the diagnostic criteria for ACD are a serum ferritin > 100 ug/l and a TSAT < 20%. If the serum ferritin concentration is between ug/l, a combination of absolute iron deficiency and ACD is likely. JCDC 2015 ECCO Consensus Paper 49
50 Tests used to detect Systemic Inflammation ESR (10 30 mm/hr) C-Reactive Protein (5-10 mg/l) Anemia of Chronic Disease Case 2 50
51 Anemia Case-2 76 year old man has complains of fatigue and a 10 lb weight loss. He is a smoker. His problem and medication lists, includes the following: Problem List Anemia Case 2 Chronic prostatitis Chronic urinary tract infections COPD Hypertension Peripheral vascular disease 51
52 Medication List Anemia Case 2 Lisinopril 20 mg qd Ipratropium inhaler 2 puffs qid Nitrofurantoin 50 mg at night Anemia Case -2 A complete blood count is obtained and reveals the following: Hemoglobin = 10.0 gm/dl Hematocrit = 30.0 % MCV = 82 fl ( fl) MCH = 27 pg/cell (26-34) MCHC = 31 gm/dl (31-37) White blood cell and platelet cts - normal 52
53 Anemia Case 2 Classification Normocytic, normochromic, anemia Anemia case -2 A complete blood count is obtained and reveals the following: Hemoglobin = 10.0 gm/dl Hematocrit = 30 % MCV = 82 fl ( fl) Reticulocyte count = 0.5% ( %) Corrected as RI = 30/45 x 0.5 =
54 Anemia Case 2 Classification Normocytic, normochromic, anemia Hypoproliferative Anemia Case 2 Additional Lab Tests Serum iron = 35 ug/dl ( ug/dl) TIBC = 220 ug/dl ( ug/dl) Tsat = 35/220 = 15.9% (25 45%) Serum ferritin = 200 ug/dl ( ug/dl) Serum creatinine 1.0 mg/dl ( mg/dl) Thyroid function tests = normal 54
55 Anemia Case -2 Tests used to detect Systemic Inflammation ESR (10 30 mm/hr) C-Reactive Protein (5-10 mg/l) Anemia Case 2 Additional Lab Tests Serum iron = 35 ug/dl ( ug/dl) TIBC = 220 ug/dl ( ug/dl) Tsat = 35/220 = 15.9% (20 45%) Serum ferritin = 200 ug/dl ( ug/dl) Serum creatinine 1.0 mg/dl ( mg/dl) Thyroid function tests = normal ERS = 80 mm/hr (10 30mm/hr) C reactive protein = 90 mg/l (5 10 mg/l) 55
56 Anemia Case 2 Classification Normocytic, normochromic, anemia Hypoproliferative Anemia of chronic inflammation Multiple Choice Question : Which laboratory test is NOT consistent with a diagnosis of anemia of chronic disease? a. Serum ferritin level of 15 ug/l (normal ). b. Total iron binding capacity of 220 ug/dl (normal ). c. Serum iron of 38 ug/dl (normal ) d. Suppressed reticulocyte count. 56
57 Combined IDA with ACD Patient with IBD and GI bleeding Case 3 Anemia of Chronic Disease (ACD) When anemia occurs in the presence of biochemical or clinical evidence of inflammation, the diagnostic criteria for ACD are a serum ferritin > 100 ug/l and a Tsat < 20%. If the serum ferritin concentration is between ug/l, a combination of absolute iron deficiency and ACD is likely. JCDC 2015 ECCO Consensus Paper 57
58 Differential Biochemical Diagnosis for IDA ACD Combined IDA/ACD IDA ACD Combined IDA / ACD Serum Ferritin (ug/l) <30 > C reactive protein Normal Elevated Elevated DJChapron 58
59 Anemia case-3 ACD with IDA A CBC reveals the following: Hemoglobin = 9.4 gm/dl Hematocrit = 28.2 % MCV = 78 fl ( fl) MCH 25 pg (26-34) MCHC 32 g/dl (31-37) Reticulocyte count = 1.5 ( %) Corrected as RI = 9.4/45 x 1.5 = 0.31% Peripheral smear normocytes with microcytes. Normal leukocytes WBC = 7,900/uL (4,500-11,000) Platelet Ct 300,000/uL (150, ,000) Anemia Case 3 Classification Mild microcytic, hypochromic, anemia Hypoproliferative Because of a dx of IBD, check for active inflammation and iron indices and stools for occult blood. 59
60 Case-3 - Combined IDA with ACD Serum iron ( ug/dl) 36 TIBC ( ug/dl) 270 % saturation (25 45%) 13 Ferritin ( ug/l) 65 ESR (10-30mm) 100 C-reactive protein (5-10 mg/l) 58 Stool positive for blood Anemia Case 3 Classification Mild microcytic, hypochromic, anemia Hypoproliferative Iron deficiency anemia with concurrent active inflammation and intestinal blood loss. 60
61 61
62 62
63 Hemolytic Anemia Bone marrow Nutritional PRODUCTION RATE [Hgb] = CLEARANCE Bleeding Hemolysis DJ Chapron 63
64 Chronic inflammation Hemolysis MDS/Ca EP Bone marrow RBCs Kidney Bleeding Iron, B-12, folate DJ Chapron Kinetic Classification of Anemia Increased destruction (Retics increased) Intracorpuscular Membrane (hereditary) Enzyme deficicency (G6PD) Hemoglobinopathy (sickle cell) Extracorpuscular-immunological Autoimmune Alloimmune Extracorpuscular Acute / chronic blood loss Chemicals (oxidative stress) Hypersplenism Infectious Mechanical (heart valve) 64
65 Common Causes of Hemolytic Anemias Intrinsic: (almost always inherited) Membrane defects Spherocytosis/elliptocytosis Hemoglobin defects: Sickle cell Thalassemia Metabolic defect: G6PD deficiency Extrinsic: membrane defects Autoimmune Oxidative drugs/chemicals SELECTED DRUGS THAT MAY CAUSE HEMOLYTIC ANEMIA PROMOTING RED CELL DESTRUCTION (HEMOLYSIS) IMMUNE MEDIATED ALPHAMETHYLDOPA PENICILLINS/CEPHALOSPORINS QUINIDINE OXIDATIVE ANTIMALARIALS NITROFURANTOIN PHENAZOPYRIDINE SULFONAMIDES 65

 and crescent-shaped")
66 Peripheral blood smear characteristic of intravascular hemolysis, with fragmented (schistocytes) and crescent-shaped (helmet) cells Schmaier

67 Degmacyte = bite cell 67

68 Heinz bodies Microscopically visible refractile intraerythrocyte hemoglobin precipitates (oxidized and denatured) that attach to the internal surface of the red cell membrane. Red blood cells containing Heinz bodies have a shortened survival, mostly due to splenic sequestration. They are found in patients with unstable hemoglobin's, thalassemias and G6PD deficiencies and drug induced oxidative stress. Heinz bodies 68

69 UpToDate 2017 Anemia Case-X A 78 year old man has just received intravesical therapy with mitomycin C for bladder cancer. Soon after he develops a very painful chemical cystitis that is substantially relieved by phenazopyridine 100 mg bid, which he is placed on chronically. Over the course of several weeks he complains of fatigue and shortness of breath. A routine CBC and electrolytes are ordered. 69
70 Anemia Case -X A complete blood count is obtained and reveals the following: Hemoglobin = 8.0 gm/dl Hematocrit = 24 % MCV = 110 fl ( fl) MCH = 32 pg/cell (26-34) MCHC = 33 gm/dl (31-37) White blood cell and platelet cts normal Electrolytes normal Anemia Case X Classification Macrocytic, normochromic anemia 70
71 Anemia case -X A complete blood count is obtained and reveals the following: Hemoglobin = 8.0 gm/dl Hematocrit = 24 % MCV = 110 fl ( fl) Reticulocyte count = 21% ( %) Corrected as RI = 8/45 x 21 = 3.7% Anemia Case X Classification Macrocytic (due to increased RC), with normochromic anemia Proliferative bone marrow response elevated reticulocyte index 71
72 Laboratory Tests That Assist in the Diagnosis of Hemolytic Anemia Serum Indirect Bilirubin concentration Serum Haptoglobin Level Serum LDH level Reticulocyte count Anemia case X Additional tests Bilirubin total = 4.0 mg/dl; 3.5 mg/dl indirect (normal total = mg/dl; approx 70% is indirect or unconjugated). Serum haptoglobin = 5 mg/dl ( mg/dl). Serum lactate dehydrogenase (LDH) = 1100 U/L ( U/L). Peripheral smear reveals bite cells and a special stain shows Heinz bodies. 72
73 Anemia Case X Classification Macrocytic, normochromic anemia Proliferative elevated reticulocyte index Peripheral smear with bite cells, special stain showing Heinz bodies, elevated serum LDH and indirect serum bilirubin and reduced serum haptoglobin are consistent with a hemolytic process. Prolonged phenazopyridine use is the source of the hemolytic process. 73
74 74
75 Multiple Choice Question Which set of laboratory tests is NOT consistent with a hemolytic anemia: a. Elevated reticulocyte index, presence of bite cells and an elevated serum total bilirubin b. Discovery of Heinz bodies, elevated serum lactate dehydrogenase and bite cells c. Elevated serum haptoglobin, reduced serum bilirubin and normal reticulocyte index d. Reticulocytosis, elevated MCV and an elevated serum indirect bilirubin Macrocytic Anemias B 12 and Folate 75



76 Microcytosis Normocytic and Macrocytosis hypochromia normochromic Hillman and Finch

77 UpToDate 2017 Normal neutrophil 77

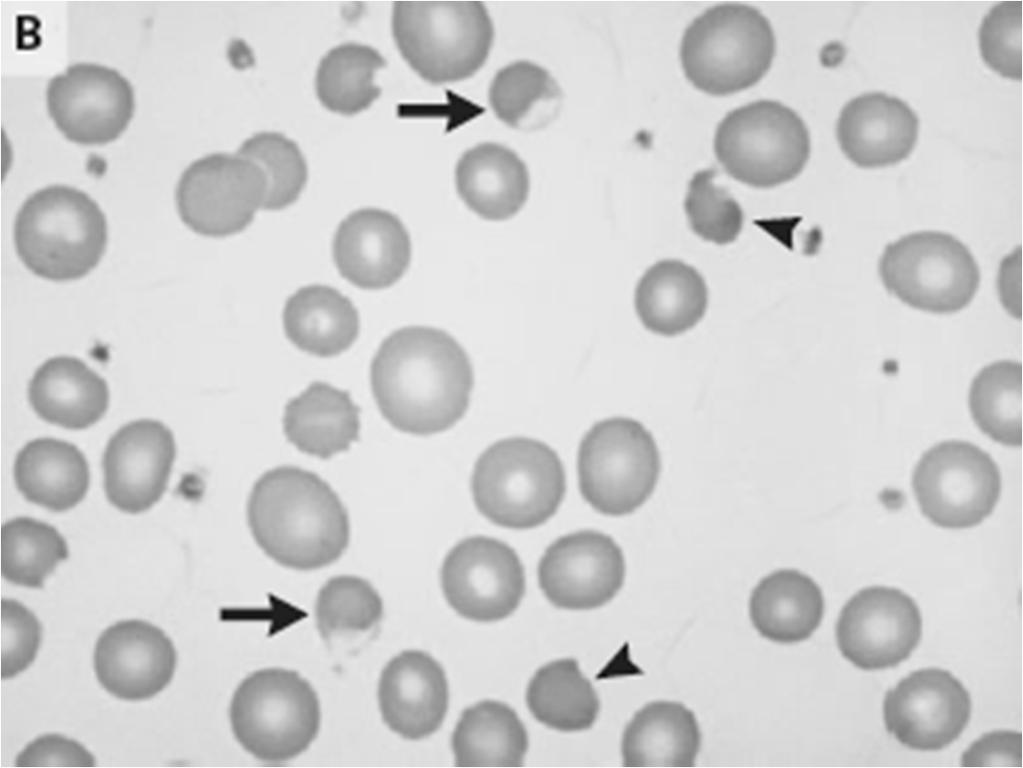
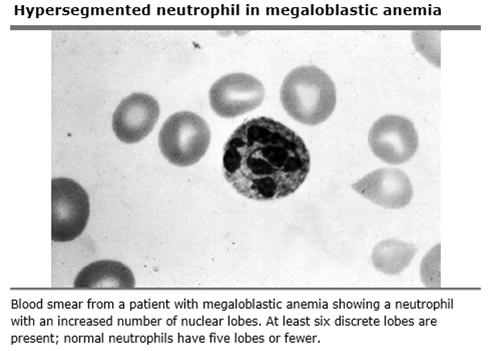
78 Hypersegmented neutrophils (contains five or more nuclear lobes) Hypersegmented Neutrophils 5 or 6 or more lobes or nuclear segmentation. Hypersegmentation of neutrophils is the first morphological change in patients with megaloblastic anemia. It is the last morphological change to disappear after appropriate treatment. Signal to investigate the cause of underlying megaloblastosis. 78
79 Macrocytic Anemias 2 types Megaloblastic: morphologic characteristics on peripheral smear include macroovalocytes (oval as opposed to spherical) and hypersegmented neutrophils (5 or more nuclear segments or lobes). Nonmegaloblastic: spherical macrocytes, absence of hypersegmented neutrophils. Hematological Features of Megaloblastic Anemia Due to Folate and Cobalamin Deficiency In severe cases MCV > 115 fl. White blood cell and platelet counts are often decreased. Marked changes in RBC size and shape (increased RDW) and on peripheral smear macro ovalocytes are common. Hypersegmentation of neutrophils; platelet morphology is normal. Nucleated RBCs can be observed on smear. Reticulocyte count is low. Serum LDH and indirect bilirubin levels may be elevated because of hemolysis of abnormally formed cells within the marrow. 79

80 Megaloblastic Anemia Result of a defect in DNA synthesis and repair due to a perturbation in thymidine synthesis. In the marrow, normal RBC nuclear development is disrupted with a lagging of nuclear behind cytoplasmic maturation. There is cell loss in the marrow because of ineffective hematopoiesis resulting in increased serum levels of lactic dehydrogenase and bilirubin. AFP
81 Morphological Classification of Anemia Macrocytic (MCV >100 fl): Megaloblastic Folate deficiency Vitamin B-12 deficiency Medications Nonmegaloblastic Ethanol abuse Hypothyroidism Liver disease Primary bone marrow disease Reticulocytosis 81
82 Laboratory Testing for Vitamin B 12 Deficiency A vitamin B 12 level < 200 pg/ml is strongly suggestive of B 12 deficiency. A vitamin B 12 level > 400 pg/ml generally rules out B 12 deficiency. Vitamin B 12 levels between pg/ml are considered borderline/high risk and require the addition of measuring MMA serum levels. Elevated MMA levels are considered the most sensitive and specific test for identifying B 12 deficiency. A low MMA serum level is strongly indicative of normal B 12 status. 82
83 Laboratory Testing for Vitamin B 12 Deficiency continued Vitamin B 12 deficiency due to pernicious anemia (an autoimmune disease) is diagnosed by the detection of circulating anti intrinsic factor antibodies (high specificity, but moderate sensitivity). 83

84 Biochemical Detection of Cobalamin Deficiency Serum cobalamin concentration ( nl pg/ml) < 400 pg/ml Elevated serum homocysteine concentration ( umol/l) >13 umol/l Elevated serum methylmalonic acid (MMA) concentration ( nmol/l) >350 nmol/l 84
 gastrectomy Competition for vitamin B-12 gut absorption (bacterial, medications) Pancreatic insufficiency (malabsorption) Decreased ileal absorption of vitamin B-12 surgical")
85 CAUSES OF VITAMIN B-12 DEFICIENCY Dietary deficiency (vegetarians) Decreased liberation from foodstuffs (achlorhydria atrophic gastritis)) Decreased production of intrinsic factor pernicious anemia (anti-if antibodies) gastrectomy Competition for vitamin B-12 gut absorption (bacterial, medications) Pancreatic insufficiency (malabsorption) Decreased ileal absorption of vitamin B-12 surgical resection Crohn's disease AIDS Transcobalamin II deficiency 85
86 Neurological Effects of Cobalamin Deficiency Nerve injury due to demyelination. Usually starts with painful paresthesias, in fingers and feet and is associated with problems in vibratory sense and proprioception. Weakness, gait ataxia and spasticity Somnolence, changes in affect and mentation, frank psychosis (megaloblastic madness) Neurological effects of cobalamin deficiency can occur in the absence of anemia or elevated MCV 86
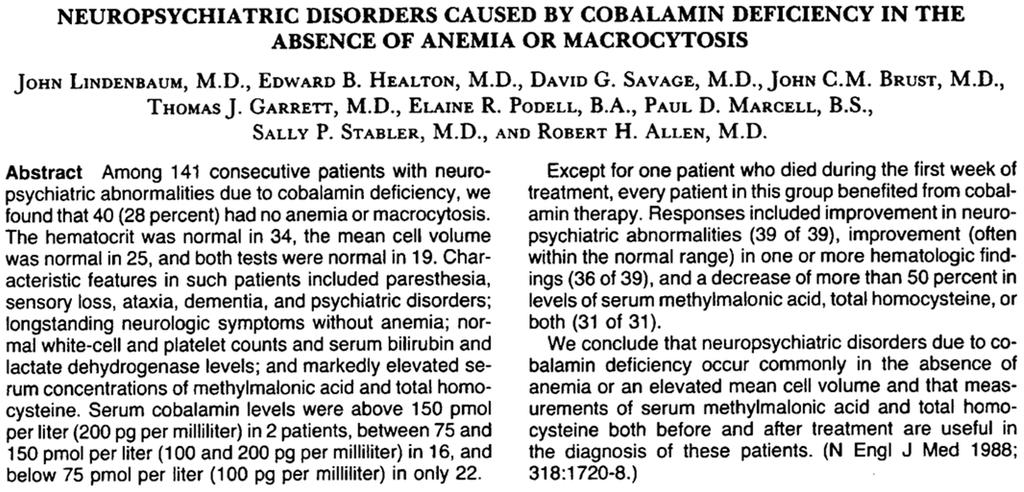
87 87
88 [Total vitamin B-12] = [Holotranscobalamin] + [Holohaptocorrin] Enters cells via specific receptors Inert Enters cells via specific receptors Active B 12 Deficiency results in elevated methylmalonic acid (MMA) and Homocysteine (HC) serum levels. MMA >350 nmol/l HC > 13umol/L Inactive B 12 Total Vitamin B 12 Concentration 88
89 Vitamin B 12 deficiency Case Z Case -Z SJ is a 84 year old woman who is concerned about progressive memory loss and decreased sensations in her right foot. Her medical history includes osteoporosis, hypertension, and hypothyroidism, which are well managed calcium carbonate 500 mg bid, alendronate 35 mg qwk, hydrochlorothiazide 12.5 qd and L-thyroxine 100 mcg qd. Neurologic examination reveals a MMSE of 23/30, decreased vibratory sensations in both legs, and an ataxic gait. 89
90 Anemia Case -Z A complete blood count is obtained and reveals the following: Hemoglobin = 11.5 gm/dl Hematocrit = 34.5 % MCV = 109 fl (80 100) MCH = 33 pg/cell (26-34) MCHC = 32 gm/dl (31-37) White blood cell ct = 4400/uL ( ,000) Platelet ct - 89,000/uL (150, ,000) Anemia Case Z Classification Macrocytic, normochromic anemia Low WBC and platelets counts 90
91 Anemia case -Z A complete blood count is obtained and reveals the following: Hemoglobin = 11.5 gm/dl Hematocrit = 34.5 % MCV = 109 fl ( fl) Reticulocyte count = 1.5% ( %) Corrected as RI = 11.5/45 x 1.5 = 0.38% Anemia Case Z Classification Macrocytic, normochromic anemia Low WBC and platelets Hypoproliferative anemia 91
92 Anemia case -Z A complete blood count is obtained and reveals the following: Hemoglobin = 11.5 gm/dl Hematocrit = 34.5 % MCV = 109 fl ( fl) Reticulocyte count = 1.5% ( %) Corrected as RI = 11.5/45 x 1.5 = 0.38% Peripheral smear mixed population of macroovalocytes and normocytes, with notable hypersegmented neutrophils. Anemia Case Z Classification Macrocytic, normochromic anemia Low WBC and platelets Hypoproliferative anemia Megaloblastic macrocytic anemia consider nutritional deficiencies. 92
93 Anemia Z Additional lab tests Serum vitamin B 12 and folate. Results Vitamin B 12 = 150 pg/ml ( pg/ml) Folate = 8 ug/l (>4 ug/l) Anemia Case Z Classification Macrocytic, normochromic anemia Low WBC and platelets Hypoproliferative anemia Megaloblastic macrocytic anemia consider nutritional deficiencies. Vitamin B 12 is abnormally low Dx vitamin B 12 deficiency. Determine etiology of Vitamin B 12 deficiency. 93
94 Anemia Z additional laboratory tests Anti intrinsic factor antibodies Patient is found to be positive for circulating anti intrinsic factor antibodies. Anemia Case Z Classification Macrocytic, normochromic anemia Low WBC and platelets Hypoproliferative anemia Megaloblastic macrocytic anemia consider nutritional deficiencies. Vitamin B 12 abnormally low Dx pernicious anemia 94
95 Vitamin B 12 deficiency Case ZZ Case ZZ SJ is a 84 year old woman who is concerned about progressive memory loss and decreased sensations in her right foot. Her medical history includes osteoporosis, hypertension, and hypothyroidism, which are well managed calcium carbonate 500 mg bid, alendronate 35 mg qwk, hydrochlorothiazide 12.5 qd and L-thyroxine 100 mcg qd. Neurologic examination reveals a MMSE of 23/30, decreased vibratory sensations in both legs, and an ataxic gait. 95
96 Anemia Case -ZZ A complete blood count is obtained and reveals the following: Hemoglobin = 12.5 gm/dl Hematocrit = 37.5 % MCV = 96 fl (80 100) MCH = 33 pg/cell (26-34) MCHC = 32 gm/dl (31-37) White blood cell ct = 6400/uL ( ,000) Platelet ct - 200,000/uL (150, ,000) Anemia Case ZZ Classification Neurological findings on physical exam suggestive of a possible vitamin B 12. Patient is not anemic and has a normal MCV. 96
97 Anemia case -ZZ A complete blood count is obtained and reveals the following: Hemoglobin = 12.5 gm/dl Hematocrit = 37.5 % MCV = 96 fl ( fl) Order serum vitamin B-12 level. Anemia ZZ Additional lab tests Order a serum vitamin B 12 Results Vitamin B 12 = 250 pg/ml ( pg/ml) 97
98 Anemia Case ZZ Classification Neurological findings on physical exam suggestive of a possible vitamin B 12. Patient is not anemic and a normal MCV. Serum vitamin B 12 levels are in the borderline/high risk range. Order a serum methylmalonic (MMA) acid level. Anemia ZZ Additional lab tests Results Vitamin B 12 = 250 pg/ml ( pg/ml). Methylmalonic acid = 800 nmol/l ( nmol/l). 98
99 Anemia Case ZZ Classification Neurological findings on physical exam suggestive of a possible vitamin B 12. Patient is not anemic. Serum vitamin B 12 levels are in the borderline/high risk range. Serum methylmalonic acid level (MMA) is elevated indicating a functional vitamin B 12 deficiency state. Multiple Choice Question : All of the following are common features of a significant vitamin B 12 deficiency except: a. Elevated serum homocysteine b. Hypersegmented neutrophils seen on a peripheral smear c. Macrocytosis d. A suppressed serum methylmalonic acid level. 99

100 Medications and Vitamin B 12 Deficiency 100
101 101

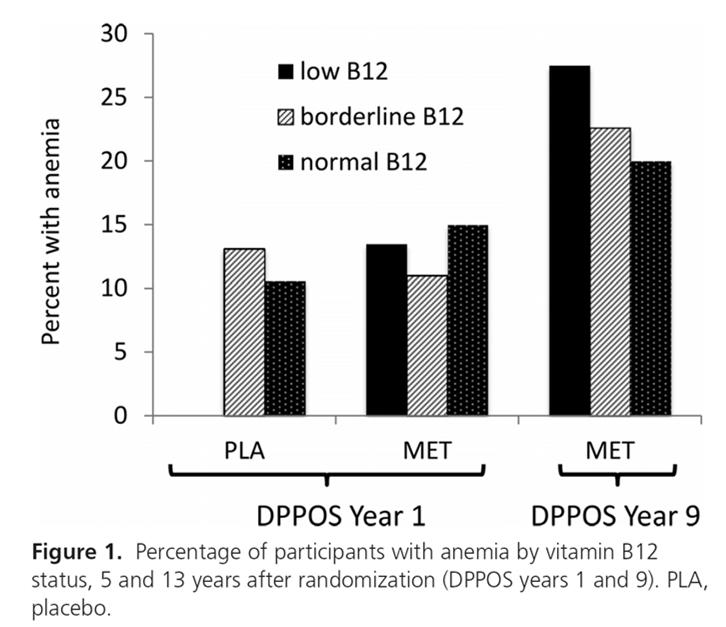
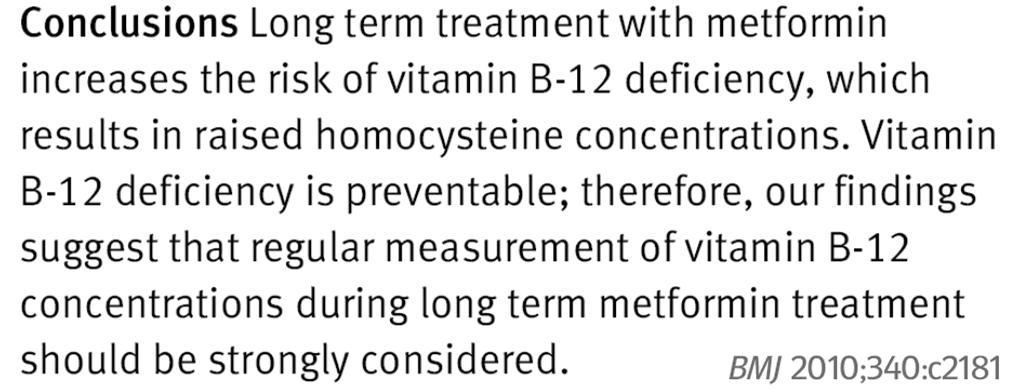
102 DM + Metformin DM No DM 102


103 Diabetes Mellitus Metformin Vitamin B-12 deficiency Peripheral Neuropathy 103
104 104
105 Diabetes Mellitus Metformin Vitamin B-12 deficiency Peripheral Neuropathy Proton Pump Inhibitors Diabetes Mellitus Metformin Vitamin B-12 deficiency Peripheral Neuropathy Proton Pump Inhibitors 105
106 Medications and Macrocytosis 106

107 Folate Deficiency 107
108 Laboratory Testing for Folate Deficiency A serum level less than 4 ug/l us indicative of folate deficiency. Borderline serum levels have been described as 4 8 ug/ml. A borderline level with an elevated plasma homocycteine level is indicative of a functional folate deficiency. Of note, plasma homocysteine levels are increased in B 12, folate and vitamin B 6 deficiencies. MMA serum levels are not effected by folate deficiency. RBC folate levels provide a time integrated folate level, whereas serum folate levels may be acutely influenced by recent dietary or multivitamin intake. Symptoms of folate deficiency are primarily due to anemia, but long term exposure to hyperhomocysteinemia may have adverse neurological and cardiovascular effects. Folate Deficiency Folate stores in the body are limited and last only a few months when intake/absorption is negligible. With the introduction of mandatory folic acid fortification in the diet in North America, folate deficiency is rare in this region. 108
109 Hillman and Finch

110 CAUSES OF FOLATE DEFICIENCY Dietary deficiency Decreased absorption Jejunal pathology Medications phenytoin sulfasalazine ethanol Increased requirements Chronic hemolytic anemia Pregnancy Exfoliative skin disease Compromised utilization: MTX,TMP Loss: dialysis 110
111 Nutr Rev 1988;46:
112 Nutr Rev 1988;46:320 Multiple Choice Question All of the medications with chronic use may be associated with hypersegmented neutrophils on a peripheral smear except: a. Metformin b. Omeprazole c. Phenazopyridine d. Sulfasalazine 112
113 Unexplained Anemia Patients with UA, by definition, do not have a well characterized anemia resulting from a single cause, such as iron or B12 deficiency. Unexplained anemia accounts for approximately one third of all anemia in individuals >65 years of age. Several theories have been put forward to explain the high rate of unexplained anemia in elderly individuals, including reduced pluripotent hematopoietic stem cell reserve, decreased production of hematopoietic growth factors, reduced sensitivity of stem cells and progenitors to growth factors, marrow microenvironment abnormalities, androgen deficiency, unrecognized CKD, undiagnosed myelodysplasia, or early stage ACD. 113
. EPO level is usually within normal limits but is low relative to the [Hgb]. Serious causes have been excluded (malignancy).")
114 Unexplained Anemia (UA) in the Elderly Routine investigation yields no apparent cause. Anemia is generally mild with Hgb of g/dl. Anemia is normocytic and hypoproliferative (low reticulocyte count/index). EPO level is usually within normal limits but is low relative to the [Hgb]. Serious causes have been excluded (malignancy). Bone marrow examination may be needed for transfusion dependent UA. Consider bone marrow examination for UA with macrocytosis, thrombocytopenia and neutropenia. Also consider (BME) if splenomegaly, bone pain, weight loss and fever and chills are present. Brocklehurst 2017 Chpt
115 115
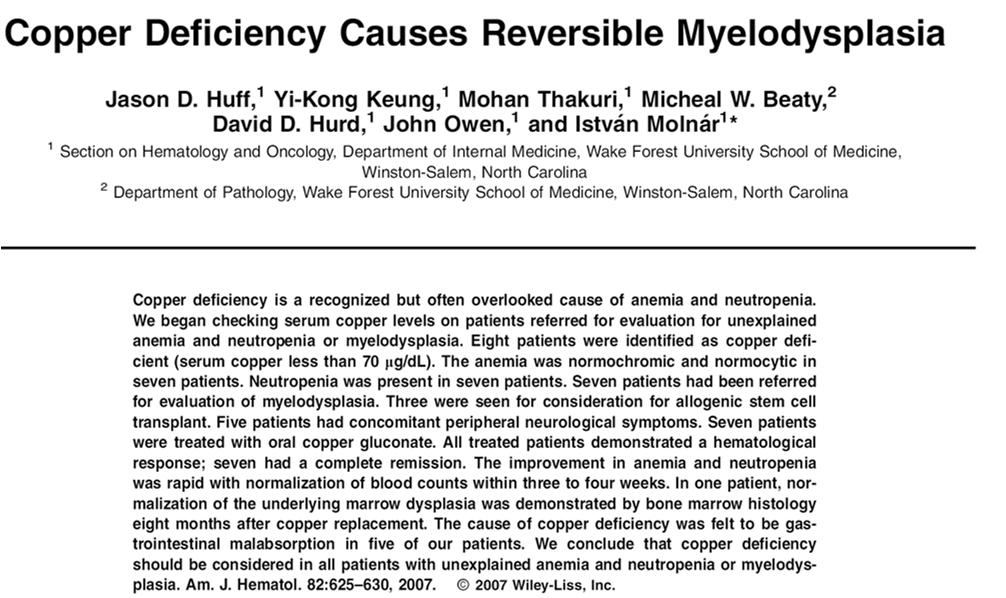
116 2 Other Disorders to Consider in the Elderly Patient with Unexplained Anemia both bone marrow disorders Myelodysplasia Multiple Myeloma Myelodysplasic Syndrome MDS 116
117 Myelodysplastic Syndrome with anemia MDS include a heterogenous group of disorders characterized by dysplastic (abnormal) changes within the bone marrow and impaired proliferation of one or more cell lines (erythroid, myeloid and megakaryocytic). It occurs primarily in older men, with a median age of occurrence of 76 yrs. 117
118 FAB Classification of MDS Refractory anemia Refractory anemia with ringed sideroblasts Refractory anemia with excess blasts Refractory anemia excess blasts in transformation Chronic myelomonocytic leukemia (CMML) FAB = French, American, British classification Anemia Case MDS Classification Macrocytic, normochromic anemia. Hypoproliferative/ineffective erythropoiesis. Leukopenia and thrombocytopenia. Bilobed leukocyte (Pelger Huet abnormality) on smear suggests myelodysplastic process. Consider bone marrow biopsy. Serum B 12, folate and iron studies are normal. 118
 Corrected as RI = 10.5/45 x 1.5 = 0.35% Peripheral smear mixed population of macrocytes and normocytes, with occasional bilobed cells (ie., Pelger-Huet anomaly).")
119 UpToDate 2017 Anemia case -MDS A CBC reveals the following: Hemoglobin = 10.5 gm/dl Hematocrit = 32 % MCV = 104 fl ( fl) MCH 32 pg MCHC 33 g/dl Reticulocyte count = 1.0% ( %) Corrected as RI = 10.5/45 x 1.5 = 0.35% Peripheral smear mixed population of macrocytes and normocytes, with occasional bilobed cells (ie., Pelger-Huet anomaly). WBC = 3,900/uL (4,500-11,000) Platelet Ct 99,000/uL (150, ,000) 119
120 Multiple Myeloma Multiple Myeloma (MM) Multiple myeloma (MM) is a neoplastic disease deriving from an abnormal proliferation of monoclonal plasma cells in the bone marrow and immunoglobulin or light chain overproduction that can cause end organ damage. MM is a disease of the elderly reflected by a median age at diagnosis of approximately 70 years, with 35 40% of patients being older than 75 years, and with the highest rates of diagnosis reported in the 80 to 89 year age group. MM accounts for approximately 13% for all hematologic malignancies and 20% of hematologic malignancy related deaths. The major hematological manifestation of MM is anemia due to decreased erythropoiesis as a result of marrow damage and a relative failure of the erythropoietin response to anemia. Rouleaux formation may be seen on the peripheral smear. 120

121 UpToDate 2017 UpToDate
122 Any Questions? 122
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
Faculty of Medicine Dr. Tariq Aladily
 Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
HAEMATOLOGICAL EVALUATION OF ANEMIA. Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore
 HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
Microcytic Hypochromic Anemia An Approach to Diagnosis
 Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Evaluation of Anemia. Md. Shafiqul Bari Associate professor (Medicine) SOMC
 SOMC") Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
General Characterisctics
 Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Anemia General Characterisctics Definition: anemia is a decrease in red blood cells. Happens due to underproduction, increased destruction or loss of red cells. Diagnosis of anemia: Hgb < 135 (men) Hgb
Introduction and Approach to Anemia
 2 nd lecture in Hematology by Dr.Alaa Fadhil Alwan Introduction and Approach to Anemia Anemia is defined clinically as a blood hemoglobin or hematocrit value that is below the appropriate reference range
2 nd lecture in Hematology by Dr.Alaa Fadhil Alwan Introduction and Approach to Anemia Anemia is defined clinically as a blood hemoglobin or hematocrit value that is below the appropriate reference range
Types of Anaemias and their Management. S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014
 Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Anemia in the elderly. Nattiya Teawtrakul MD., PhD
 Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Anemia in the elderly Nattiya Teawtrakul MD., PhD Contents Definition of anemia in the elderly The impact of anemia in the elderly Etiology of anemia in the elderly Management of anemia in the elderly
Diagnostic Approach to Patients with Anemia
 J KMA Special Issue Diagnostic Approach to Patients with Anemia Seonyang Park, MD Department of Internal Medicine, Seoul National University College of Medicine E mail : seonpark@snu.ac.kr J Korean Med
J KMA Special Issue Diagnostic Approach to Patients with Anemia Seonyang Park, MD Department of Internal Medicine, Seoul National University College of Medicine E mail : seonpark@snu.ac.kr J Korean Med
Anemia In the Insurance Applicant What do the numbers mean?
 Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Susan Stegman, MD Medical Director AXA Equitable Life May 3, 2016
 Susan Stegman, MD Medical Director AXA Equitable Life May 3, 2016 Underwriting impact Anemia overview Classification of anemia Specific anemia topics Iron deficiency anemia Thalassemia Megaloblastic anemia
Susan Stegman, MD Medical Director AXA Equitable Life May 3, 2016 Underwriting impact Anemia overview Classification of anemia Specific anemia topics Iron deficiency anemia Thalassemia Megaloblastic anemia
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to the child with anemia. Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital
 Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor
 Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
(anemia) ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2
 ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2") ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
Interpreting the CBC. Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired
 Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES
 namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
Hematopoiesis, The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid.
 Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Case # 1. RBC Loss. CASE #1 (Continued) Blood Loss Is the Most Common Cause of Anemia. AGA Definition of Occult Blood Loss
 Blood Loss Is the Most Common Cause of Anemia. AGA Definition of Occult Blood Loss") Case # 1 A 42-yo woman with heavy menses presents with rectal bleeding. Except for pallor, exam is normal. HCT = 17.1% (normal, 36-48) HGB = 5.3 g/dl (normal, 12.0-16.0) MCV = 76 fl (normal, 82-98) RBC
Case # 1 A 42-yo woman with heavy menses presents with rectal bleeding. Except for pallor, exam is normal. HCT = 17.1% (normal, 36-48) HGB = 5.3 g/dl (normal, 12.0-16.0) MCV = 76 fl (normal, 82-98) RBC
Anemia 1: Fourth year Medical Students/ Feb/22/ Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor
 Anemia 1: Fourth year Medical Students/ Feb/22/ 2018 Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Kidney EPO O2 Sensor Blood vessel Definition: Anemia is operationally
Anemia 1: Fourth year Medical Students/ Feb/22/ 2018 Abdallah Awidi Abbadi.MD.FRCP.FRCPath Professor Email: abdalla.awidi@gmail.com Kidney EPO O2 Sensor Blood vessel Definition: Anemia is operationally
THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY
 THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY INTRODUCTION TO ANEMIA Third year medical students First semester 2018/2019 Dr. RBC DISORDERS Lecturer: Dr. Tariq Al-Adaily Email: TNALADILY@ju.edu.jo
THE UNIVERSITY OF JORDAN FACULTY OF MEDICINE DEPARTMENT OF PATHOLOGY INTRODUCTION TO ANEMIA Third year medical students First semester 2018/2019 Dr. RBC DISORDERS Lecturer: Dr. Tariq Al-Adaily Email: TNALADILY@ju.edu.jo
Deconstructing the CBC
 Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
LEC 6 Megaloblastic Aneamia
 LEC 6 Megaloblastic Aneamia Megaloblastosis is a generalized disorder involving most rapidly growing cells, such as gastrointestinal and uterine cervical mucosal cells. The etiology of megaloblastosis
LEC 6 Megaloblastic Aneamia Megaloblastosis is a generalized disorder involving most rapidly growing cells, such as gastrointestinal and uterine cervical mucosal cells. The etiology of megaloblastosis
Approach to Anemia PG CME
 Approach to Anemia PG CME 2014 2017 Vikram Mathews Haematology Department Christian Medical College Vellore Definition of Anemia Beutler et al. Blood 2006. Definition of Anemia WHO definition of anemia
Approach to Anemia PG CME 2014 2017 Vikram Mathews Haematology Department Christian Medical College Vellore Definition of Anemia Beutler et al. Blood 2006. Definition of Anemia WHO definition of anemia
Hematology Unit Lab 1 Review Material
 Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Hematology Unit Lab 1 Review Material - 2018 Objectives Laboratory instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Red cell disorder. Dr. Ahmed Hasan
 Red cell disorder Dr. Ahmed Hasan Things to be learned in this lecture Definition and clinical feature of anemia. Classification of anemia. Know some details of microcytic anemia Question of the lecture:
Red cell disorder Dr. Ahmed Hasan Things to be learned in this lecture Definition and clinical feature of anemia. Classification of anemia. Know some details of microcytic anemia Question of the lecture:
Chapter 2. ERYTHROPOIESIS and ANEMIA
 Chapter 2 ERYTHROPOIESIS and ANEMIA Red Cell Production The Production of red cells, known as erythropoiesis, is a developmental system fundamentally under genetic control but modulated and regulated by
Chapter 2 ERYTHROPOIESIS and ANEMIA Red Cell Production The Production of red cells, known as erythropoiesis, is a developmental system fundamentally under genetic control but modulated and regulated by
Nutritional anaemia. Dr J Potgieter Dept of Haematology NHLS - TAD
 Nutritional anaemia Dr J Potgieter Dept of Haematology NHLS - TAD Classification of anaemia Microcytic, hypochromic MCV < 80fl MCH > 27pg Iron deficiency Anaemia of chronic disease Thalassaemia Lead poisoning
Nutritional anaemia Dr J Potgieter Dept of Haematology NHLS - TAD Classification of anaemia Microcytic, hypochromic MCV < 80fl MCH > 27pg Iron deficiency Anaemia of chronic disease Thalassaemia Lead poisoning
Lisa B. Weissmann, MD
 Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
PATHOLOGY OF THE HEMATOLYMPHOID SYSTEM 1 AND 2 -INTRODUCTION TO ANEMIA - ANEMIA OF DECREASED PRODUCTION.
 PATHOLOGY OF THE HEMATOLYMPHOID SYSTEM 1 AND 2 -INTRODUCTION TO ANEMIA - ANEMIA OF DECREASED PRODUCTION. 1 ANEMIA Anemia is defined as decrease in the RBC mass, it usually is reflected by decrease in hemoglobin
PATHOLOGY OF THE HEMATOLYMPHOID SYSTEM 1 AND 2 -INTRODUCTION TO ANEMIA - ANEMIA OF DECREASED PRODUCTION. 1 ANEMIA Anemia is defined as decrease in the RBC mass, it usually is reflected by decrease in hemoglobin
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Symptoms and Signs in Hematology (2)/ 2013
/ 2013") Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
GP refresher course Anaemia. Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018
 GP refresher course Anaemia Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018 None Declarations WHO thresholds Hb (g/l) Children 0.5 5 yrs 110 Children 5 12 yrs 115 Teens
GP refresher course Anaemia Peter MacCallum Consultant Haematologist Barts Health NHS Trust London January 2018 None Declarations WHO thresholds Hb (g/l) Children 0.5 5 yrs 110 Children 5 12 yrs 115 Teens
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 93 A 24-year-old woman, who has recently arrived in Australia from Vietnam, presents for evaluation of abnormal menstrual bleeding. There are no abnormalities on examination. Results of investigations
QUESTION 93 A 24-year-old woman, who has recently arrived in Australia from Vietnam, presents for evaluation of abnormal menstrual bleeding. There are no abnormalities on examination. Results of investigations
Moath Darwish. Waseem Alhaj. Tareq Adely
 4 Moath Darwish Waseem Alhaj Tareq Adely Please refer to the slides for pictures. Iron deficiency anemia 1. Iron absorption and regulation a. only 10% of ingested iron are absorbed b. absorption of iron
4 Moath Darwish Waseem Alhaj Tareq Adely Please refer to the slides for pictures. Iron deficiency anemia 1. Iron absorption and regulation a. only 10% of ingested iron are absorbed b. absorption of iron
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED
 INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
INTERELATIONSHIP BETWEEN IDA AND VITAMIN D DEFICIENCY IS NOW ESTABLISHED Rationale for Combining Iron & Vit-D Vit D deficiency and Iron deficiency Anaemia the two most menacing disorders - are inter-related
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Approach to the abnormal CBC
 Approach to the abnormal CBC Robert T. Means, Jr., M.D. Hematology and Blood & Marrow Transplant Division University of Kentucky and VA Medical Center Lexington KY General Considerations Always repeat
Approach to the abnormal CBC Robert T. Means, Jr., M.D. Hematology and Blood & Marrow Transplant Division University of Kentucky and VA Medical Center Lexington KY General Considerations Always repeat
PNH Glossary of Terms
 AA Absolute neutrophil count Alendronate Allergen ALT Anemia Antibodies Anticoagulant Anticoagulation Antigen Antithymocyte globulin (ATG) Aplastic Aplastic anemia Band Bilirubin Blast cells Bone marrow
AA Absolute neutrophil count Alendronate Allergen ALT Anemia Antibodies Anticoagulant Anticoagulation Antigen Antithymocyte globulin (ATG) Aplastic Aplastic anemia Band Bilirubin Blast cells Bone marrow
Lisa B. Weissmann, MD
 Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
Lisa B. Weissmann, MD Anemia- Most common hematologic disorder Evaluation should be orderly Questions to ask Timing - new, old, rapidity of onset Isolated - only anemia, or other cell lines Size of cells
Does Morphology Matter in 2017
 Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Does Morphology Matter in 2017 ISLH May 2017 Kathryn Foucar Distinguished Professor Emerita kfoucar@salud.unm.edu Objectives Recognize unique RBC and WBC abnormalities in non-neoplastic disorders Learn
Assessing Iron Deficiency in Adults. Chris Theberge. Iron (Fe) deficiency remains as one of the major global public health problems for
 deficiency remains as one of the major global public health problems for") Assessing Iron Deficiency in Adults Chris Theberge Iron (Fe) deficiency remains as one of the major global public health problems for two reasons. It affects about one fourth of the world s population
Assessing Iron Deficiency in Adults Chris Theberge Iron (Fe) deficiency remains as one of the major global public health problems for two reasons. It affects about one fourth of the world s population
DOWNLOAD PDF MACROCYTOSIS AND MACROCYTIC ANAEMIA
 Chapter 1 : Macrocytic Anemia- Causes, Symptoms Treatment Macrocytosis is a term used to describe red blood cells that are larger than normal. Anemia is when you have low numbers of properly functioning
Chapter 1 : Macrocytic Anemia- Causes, Symptoms Treatment Macrocytosis is a term used to describe red blood cells that are larger than normal. Anemia is when you have low numbers of properly functioning
Management of anemia in CKD
 Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
Management of anemia in CKD Pierre Cochat, MD PhD Professor of Pediatrics Chair, Pediatrics & Pediatric Surgery Department Head, Center for Rare Renal Diseases Néphrogones Hospices Civils de Lyon & University
2. Non- hemolytic anemias 3. Normocytic Normochromic Normocytic Normochromic Blood loss. (MCV<80 fl) (MCV fl) (MCV>100 fl)
 (MCV fl) (MCV>100 fl)") Definition of Anaemia of Anaemias Approach for diagnosis of Red cell disorders any condition resulting from a significant decrease in the total body erythrocyte mass due to decrease of Hb and or RBCs Hemoglobin
Definition of Anaemia of Anaemias Approach for diagnosis of Red cell disorders any condition resulting from a significant decrease in the total body erythrocyte mass due to decrease of Hb and or RBCs Hemoglobin
Examination Tests from Pathological Physiology. Pavel Maruna et al. Reviewed by: Prof. MUDr. Emanuel Nečas, DrSc. Prof. MUDr. Jaroslav Veselý, CSc.
 Examination Tests from Pathological Physiology Pavel Maruna et al. Reviewed by: Prof. MUDr. Emanuel Nečas, DrSc. Prof. MUDr. Jaroslav Veselý, CSc. Authors: Prof. MUDr. Pavel Maruna, CSc. Doc. MUDr. Martin
Examination Tests from Pathological Physiology Pavel Maruna et al. Reviewed by: Prof. MUDr. Emanuel Nečas, DrSc. Prof. MUDr. Jaroslav Veselý, CSc. Authors: Prof. MUDr. Pavel Maruna, CSc. Doc. MUDr. Martin
Updates in the Management of Anemia in Cancer. Taylor M. Ortiz, MD May 19, 2017
 Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Updates in the Management of Anemia in Cancer Taylor M. Ortiz, MD May 19, 2017 Objectives Recall common causes of anemia in patients with cancer Understand risks/benefits of blood transfusion in patients
Dr. Hasan Fahmawi, MRCP (London), FRCP(Edin) Consultant Physician ANAEMIA
, FRCP(Edin) Consultant Physician ANAEMIA") Dr. Hasan Fahmawi, MRCP (London), FRCP(Edin) Consultant Physician ANAEMIA Definition Anaemia refers to a state in which haemoglobin in the blood is below the reference range appropriate for age and
Dr. Hasan Fahmawi, MRCP (London), FRCP(Edin) Consultant Physician ANAEMIA Definition Anaemia refers to a state in which haemoglobin in the blood is below the reference range appropriate for age and
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
An Oncologist s Approach to Anemia in Adults Christie J. Hilton, DO
 An Oncologists Approach to Anemia in Adults (There are not many updates) Christie Hilton DO POMA Winter Symposium 2019 Nemicolin Woodlands 8 Disclosures None 9 Objectives Define anemia Review the classification
An Oncologists Approach to Anemia in Adults (There are not many updates) Christie Hilton DO POMA Winter Symposium 2019 Nemicolin Woodlands 8 Disclosures None 9 Objectives Define anemia Review the classification
L4-Iron Deficiency Anemia (IDA) & Biochemical Investigations
 & Biochemical Investigations") L4-Iron Deficiency Anemia (IDA) & Biochemical Investigations 1 st Year-College of Medicine Hematology Module-Biochemistry Semester II Dr. Basil OM Saleh Objectives Identify stages in development of IDA
L4-Iron Deficiency Anemia (IDA) & Biochemical Investigations 1 st Year-College of Medicine Hematology Module-Biochemistry Semester II Dr. Basil OM Saleh Objectives Identify stages in development of IDA
Anemia defined. Challenging Case Studies in Laboratory Diagnosis: A focus on anemia
 Challenging Case Studies in Laboratory Diagnosis: A focus on anemia Margaret A. Fitzgerald, DNP, FNP-BC BC, NP-C, FAANP, CSP President, Fitzgerald Health Education Associates, Inc., North Andover, MA Family
Challenging Case Studies in Laboratory Diagnosis: A focus on anemia Margaret A. Fitzgerald, DNP, FNP-BC BC, NP-C, FAANP, CSP President, Fitzgerald Health Education Associates, Inc., North Andover, MA Family
Med Chem 535 ~ Diagnostic Medicinal Chemistry. Hematology ~ Erythrocytes (Red Blood Cells, RBCs)
") Med Chem 535 ~ Diagnostic Medicinal Chemistry Hematology ~ Erythrocytes (Red Blood Cells, RBCs) I. Tests A. Red Blood Cell Count (RBC)* B. Hemoblobin (Hb or Hgb)* C. Hematocrit (Hct)* D. Wintrobe Indices
Med Chem 535 ~ Diagnostic Medicinal Chemistry Hematology ~ Erythrocytes (Red Blood Cells, RBCs) I. Tests A. Red Blood Cell Count (RBC)* B. Hemoblobin (Hb or Hgb)* C. Hematocrit (Hct)* D. Wintrobe Indices
Avoiding Early Cancer Claims. Presentation #4. Hank George, FALU
 Avoiding Early Cancer Claims Presentation #4 Hank George, FALU Hematology and High Risk of Early Cancer Claims Mild Anemia in elders is underpriced by insurers most likely because of its high prevalence
Avoiding Early Cancer Claims Presentation #4 Hank George, FALU Hematology and High Risk of Early Cancer Claims Mild Anemia in elders is underpriced by insurers most likely because of its high prevalence
* imagine if the Hb is free ( e.g. hemolysis ) in the plasma what happens?
 in the plasma what happens?") In this lecture we will talk about Some characteristics of RBC. Erythrpoiesis : * During fetal & adult life. * its regulation. RBCs : - Appear under the microscope as circular,unnucleated and biconcave
In this lecture we will talk about Some characteristics of RBC. Erythrpoiesis : * During fetal & adult life. * its regulation. RBCs : - Appear under the microscope as circular,unnucleated and biconcave
Definition Aetiology
 Definition Anaemia is a fall in haemoglobin below the reference ranges for age and sex (adult female
Definition Anaemia is a fall in haemoglobin below the reference ranges for age and sex (adult female
Objectives. But first: What s in blood? Introduction. Overview: Erythrocytes. Erythrocytes, cont. 4/21/2016
 Objectives Nutritional Deficiencies That May Cause Anemia Lee Ellen Brunson-Sicilia, MHS, MLS(ASCP) CM 1. Discuss the role that various nutrients play in red blood cell formation. 2. List sources of nutrients
Objectives Nutritional Deficiencies That May Cause Anemia Lee Ellen Brunson-Sicilia, MHS, MLS(ASCP) CM 1. Discuss the role that various nutrients play in red blood cell formation. 2. List sources of nutrients
5/1/2017 DISCUSSION POINTS. Clinical Utility of Immature Cell Indices Beyond the Routine CBC John E. Donnelly BSN, RN
 DISCUSSION POINTS Importance of hematological immature cell indices Clinical Utility of Immature Cell Indices Beyond the Routine CBC John E. Donnelly BSN, RN Investigate the evidence for clinical utility:
DISCUSSION POINTS Importance of hematological immature cell indices Clinical Utility of Immature Cell Indices Beyond the Routine CBC John E. Donnelly BSN, RN Investigate the evidence for clinical utility:
HEMATOPOIESIS. HEMATOLOGY Introduction. Study of blood & its components Window of rest of body. Introduction
 HEMATOLOGY/ HEMATOPOIESIS Introduction HEMATOLOGY Introduction Study of blood & its components Window of rest of body 1 BLOOD Raison d etre Delivery of nutrients Oxygen Food Vitamins Removal of wastes
HEMATOLOGY/ HEMATOPOIESIS Introduction HEMATOLOGY Introduction Study of blood & its components Window of rest of body 1 BLOOD Raison d etre Delivery of nutrients Oxygen Food Vitamins Removal of wastes
ORIGINAL ARTICLE CLINICO PATHOLOGICAL REVIEW OF MEGALOBLASTIC ANAEMIA IN CHILDREN- A 7 YEAR PAEDIATRIC HOSPITAL EXPERIENCE
 CLINICO PATHOLOGICAL REVIEW OF MEGALOBLASTIC ANAEMIA IN CHILDREN- A 7 YEAR PAEDIATRIC HOSPITAL EXPERIENCE M.Ramani 1, D.Ranganath 2,O.H.RadhikaKrishna 3, K.Geetha 4, M.Keerthika 5, PujaDeshmukh 6, S.P.Krupani7,
CLINICO PATHOLOGICAL REVIEW OF MEGALOBLASTIC ANAEMIA IN CHILDREN- A 7 YEAR PAEDIATRIC HOSPITAL EXPERIENCE M.Ramani 1, D.Ranganath 2,O.H.RadhikaKrishna 3, K.Geetha 4, M.Keerthika 5, PujaDeshmukh 6, S.P.Krupani7,
Clinician Blood Panel Results
 Page 1 of 8 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
Page 1 of 8 Blood Panel - Markers Out of Range and Patterns (Pattern: proprietary formula using one or more Blood Markers) Blood Panel: Check for Markers that are out of Lab Range ***NOTE*** Only one supplement
11. An acute leukemia causing. 12. An adult patient presents with acute. 13. Anemia due to renal failure may be
 Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
Hematology Study online at 1. A 23 year old white female has weakness, fatigue and has developed a habit of chewing ice. What are the expected findings in regard to TIBC and Ferritin? 2. A 25 year old
NUTRITIONAL CARE IN ANEMIA
 االله الرحمن الرحيم بسم NUTRITIONAL CARE IN ANEMIA Nutrition Departement Faculty of Medicine University of North Sumatera Definition Deficit of circulating RBC associated with diminished oxygen-carrying
االله الرحمن الرحيم بسم NUTRITIONAL CARE IN ANEMIA Nutrition Departement Faculty of Medicine University of North Sumatera Definition Deficit of circulating RBC associated with diminished oxygen-carrying
Case Report A Puzzle of Hemolytic Anemia, Iron and Vitamin B12 Deficiencies in a 52-Year-Old Male
 Hindawi Publishing Corporation Case Reports in Hematology Volume 2013, Article ID 708489, 5 pages http://dx.doi.org/10.1155/2013/708489 Case Report A Puzzle of Hemolytic Anemia, Iron and Vitamin B12 Deficiencies
Hindawi Publishing Corporation Case Reports in Hematology Volume 2013, Article ID 708489, 5 pages http://dx.doi.org/10.1155/2013/708489 Case Report A Puzzle of Hemolytic Anemia, Iron and Vitamin B12 Deficiencies
ANEMIA Dr. Luke (Mike) Stapleton 5 Nov 2016
 Stapleton 5 Nov 2016") ANEMIA----101 Dr. Luke (Mike) Stapleton 5 Nov 2016 ANEMIA----101 Introduction Background, Incidence, Significance Basic definition: Disease vs Sign Classification: Morphology/Pathophysiology Pumping Iron
ANEMIA----101 Dr. Luke (Mike) Stapleton 5 Nov 2016 ANEMIA----101 Introduction Background, Incidence, Significance Basic definition: Disease vs Sign Classification: Morphology/Pathophysiology Pumping Iron
EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS
 EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY MORPHOLOGIC CHANGES IN PERIPHERAL BLOOD CELLS Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
NUTRITIONAL ANEMIAS K Y L I E P E T E R S O N & E M I L Y S T E W A R T S A O R I S A K I T A & M A R J O R I E M I L L E R
 NUTRITIONAL ANEMIAS K Y L I E P E T E R S O N & E M I L Y S T E W A R T S A O R I S A K I T A & M A R J O R I E M I L L E R ANEMIA Anemia: a deficiency in the size/number of RBC or the amount of hemoglobin
NUTRITIONAL ANEMIAS K Y L I E P E T E R S O N & E M I L Y S T E W A R T S A O R I S A K I T A & M A R J O R I E M I L L E R ANEMIA Anemia: a deficiency in the size/number of RBC or the amount of hemoglobin
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
ANEMIA & HEMODIALYSIS
 ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
Preferred Clinical Services for Leading Age Florida August 26-27, 2015
 DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 3, D CODES DISEASES OF THE BLOOD AND BLOOD-FORMING ORGANS AND CERTAIN DISORDERS INVOLVING THE IMMUNE MECHANISM Preferred Clinical Services for Leading
DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 3, D CODES DISEASES OF THE BLOOD AND BLOOD-FORMING ORGANS AND CERTAIN DISORDERS INVOLVING THE IMMUNE MECHANISM Preferred Clinical Services for Leading
APPROACHING TO PANCYTOPENIA
 APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
Objectives. But first: What s in blood? Introduction. Overview: Erythrocytes. Erythrocytes, cont. 4/10/2016
 Objectives Nutritional Deficiencies That May Cause Anemia 1. Discuss the role that various nutrients play in red blood cell formation. 2. List sources of nutrients involved in red blood cell formation.
Objectives Nutritional Deficiencies That May Cause Anemia 1. Discuss the role that various nutrients play in red blood cell formation. 2. List sources of nutrients involved in red blood cell formation.
Dr Anzo William Adiga
 Anemia Dr Anzo William Adiga +256777363201 anzoism2008@gmail.com Definition of Anemia Deficiency in the oxygen-carrying capacity of the blood due to a diminished erythrocyte mass. May be due to: Erythrocyte
Anemia Dr Anzo William Adiga +256777363201 anzoism2008@gmail.com Definition of Anemia Deficiency in the oxygen-carrying capacity of the blood due to a diminished erythrocyte mass. May be due to: Erythrocyte
Anemia and Polycythemia John W. Adamson, Dan L. Longo
 Section 10 Hematologic AlTERATions 1 77 Anemia and Polycythemia John W. Adamson, Dan L. Longo HEMATOPOIESIS AND THE PHYSIOLOGIC BASIS OF RED CELL PRODUCTION Hematopoiesis is the process by which the formed
Section 10 Hematologic AlTERATions 1 77 Anemia and Polycythemia John W. Adamson, Dan L. Longo HEMATOPOIESIS AND THE PHYSIOLOGIC BASIS OF RED CELL PRODUCTION Hematopoiesis is the process by which the formed
Indication of peripheral blood smear exmination:
 Indication of peripheral blood smear exmination: 1. For carried out differential WBC count. 2. For differential diagnosis of anemia. 3. For detection of parasites. 4. For diagnosis of leucemoid reaction.
Indication of peripheral blood smear exmination: 1. For carried out differential WBC count. 2. For differential diagnosis of anemia. 3. For detection of parasites. 4. For diagnosis of leucemoid reaction.
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE
 THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
THE KENYA POLYTECHNIC UNIVERSITY COLLEGE SCHOOL OF HEALTH SCIENCES AND TECHNOLOGY DEPARTMENT OF BIOMEDICAL LABORATORY SCIENCES AND TECHNOLOGY DIPLOMA IN MEDICAL LABORATORY SCIENCE END OF YEAR 1 EXAMINATION
Collect and label sample according to standard protocols. Gently invert tube 8-10 times immediately after draw. DO NOT SHAKE. Do not centrifuge.
 Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Iron deficiency anemia:
 بسم هللا الرمحن الرحمي Before we start: Dr. Malik suggested for the third immunity lecture to be a continuation for the hematology pharmacology. And he will discuss the drugs for treating leukemia and
بسم هللا الرمحن الرحمي Before we start: Dr. Malik suggested for the third immunity lecture to be a continuation for the hematology pharmacology. And he will discuss the drugs for treating leukemia and
Drop of Blood Unravels Mysteries. Prof. Salma Afrose Department of Hematology Dhaka Medical College
 Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
Drop of Blood Unravels Mysteries Prof. Salma Afrose Department of Hematology Dhaka Medical College Peripheral Blood Film (PBF) PBF is a laboratory workup that involves cytology of Peripheral blood cell
OBJECTIVES Define anemia and identify the appropriate diagnostic testing necessary to diagnose anemia Discuss various types and causes of anemia Discu
 ANEMIA Marjaana Krieger, MSN, RN, NP-C, AOCNP Advanced Oncology Certified Nurse Practitioner Department of Veterans Affairs/ VA Southern Nevada Healthcare System Hematology/Oncology/Infusion Clinic OBJECTIVES
ANEMIA Marjaana Krieger, MSN, RN, NP-C, AOCNP Advanced Oncology Certified Nurse Practitioner Department of Veterans Affairs/ VA Southern Nevada Healthcare System Hematology/Oncology/Infusion Clinic OBJECTIVES
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration
 Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016
 NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TEST PROGRAM Glass Slide - November 2016 Results from this proficiency test event are available at: http://www.wadsworth.org/regulatory/clep/pt/summaries SLIDE
Anemia in the Elderly
 #99081 Anemia in the Elderly COURSE #99081 5 CONTACT HOURS/CREDITS Release Date: 02/01/15 Expiration Date: 01/31/18 Anemia in the Elderly HOW TO RECEIVE CREDIT Read the enclosed course. Complete the questions
#99081 Anemia in the Elderly COURSE #99081 5 CONTACT HOURS/CREDITS Release Date: 02/01/15 Expiration Date: 01/31/18 Anemia in the Elderly HOW TO RECEIVE CREDIT Read the enclosed course. Complete the questions
HEAMATOLOGICAL INDICES AND BONE MARROW BIOPSY
 HEAMATOLOGICAL INDICES AND BONE MARROW BIOPSY HEMATOCRIT Hematocrit is a measure of the percentage of the total blood volume that is made up by the red blood cells The hematocrit can be determined directly
HEAMATOLOGICAL INDICES AND BONE MARROW BIOPSY HEMATOCRIT Hematocrit is a measure of the percentage of the total blood volume that is made up by the red blood cells The hematocrit can be determined directly
9/23/2018. Investigation of Hemolysis in the Clinical Laboratory. Objectives. What is hemolysis?
 Investigation of Hemolysis in the Clinical Laboratory Jason Anderson, MPH, MT(ASCP) Field Product Specialist Objectives 1. Define hemolysis. 2. Distinguish between intrinsic and extrinsic hemolysis 3.
Investigation of Hemolysis in the Clinical Laboratory Jason Anderson, MPH, MT(ASCP) Field Product Specialist Objectives 1. Define hemolysis. 2. Distinguish between intrinsic and extrinsic hemolysis 3.
The Irony of Anemia How to interpret the CBC
 Jaideep Shenoi MD Hematology Oncology Northwest Medical Specialities Tacoma, WA The Irony of Anemia How to interpret the CBC March 10 th, 2018 Disclosures: Advisory Board for Pharmacyclics, Janssen, Takeda,
Jaideep Shenoi MD Hematology Oncology Northwest Medical Specialities Tacoma, WA The Irony of Anemia How to interpret the CBC March 10 th, 2018 Disclosures: Advisory Board for Pharmacyclics, Janssen, Takeda,
Normal Development. Normal Development 10/16/2012. Hematopoietic and Lymph Node Pathology. Red Blood Cell Maturation & Anemias
 Hematopoietic and Lymph Node Pathology Normal Development Red Blood Cell Maturation & Anemias Normal Development Differentiation of Hematopoietic Cells 1 Bone Marrow Bone Marrow Bone Marrow, RBC Precursors
Hematopoietic and Lymph Node Pathology Normal Development Red Blood Cell Maturation & Anemias Normal Development Differentiation of Hematopoietic Cells 1 Bone Marrow Bone Marrow Bone Marrow, RBC Precursors
The LaboratoryMatters
 Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. Complete Blood Count This issue highlights: CBC, while ubiquitous, is an excellent diagnostic
Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. Complete Blood Count This issue highlights: CBC, while ubiquitous, is an excellent diagnostic
Updates for your practice August 2013 TLALELETSO. HIV & Anemia. Continued on Page 2
 dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
dates for your practice August 2013 TLALELETSO HIV & Anemia In this issue we review anemia and HIV. Medical professionals across all disciplines need to be alert to the hematological complications of HIV
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone