IMPAIRMENT RATING 5 TH EDITION MODULE III THE UPPER EXTREMITIES AND PAIN
|
|
|
- Marcia Stone
- 6 years ago
- Views:
Transcription

1 IMPAIRMENT RATING 5 TH EDITION MODULE III THE UPPER EXTREMITIES AND PAIN PRESENTED BY: RONALD J. WELLIKOFF, D.C., FACC, FICC In conjuction with:
2 The physical examination is the determining factor of a permanent anatomic impairment of the upper extremities. The physical examination MUST be accurate, objective, and well DOCUMENTED. Included in an impairment report the following should be considered: 1. Activities of Daily Living 2. Observations of the Examinee 3. Local and General Physical Examination 4. Appropriate Imaging Evaluation 5. Laboratory Tests 6. Photographic Record, if possible. A prior injury may be considered during an assessment of causation and, if included in the report, should be apportioned. Hand dominance should be considered if the examiner determines that it impacts on the Activities of Daily Living.
3 Once again, the impairment rating is based on the inability to perform, at least, one of the activities of daily living. For the purpose of today s program, we will touch on the subject of impairment of the hand and fingers briefly. Again, the medical evaluation is the basis for the determination of a permanent anatomical impairment. Everything that you do MUST be documented. THE DIGITS When evaluating the digits, it is important to remember that the hand is broken down into a number of parts: 1. Thumb 2. Index or Middle Finger 3. Ring or Little Finger It is important that you use the correct chart when evaluating a patient and assigning an impairment.
4 As previously mentioned, in the musculoskeletal section of the 5 th edition, you will first get a rating of the part examined. In this case the digit. HIERARCHY IN WHOLE PERSON CONCEPT FOR UPPER EXTREMITY AND HAND Thumb Index Middle HAND UPPER EXTREMITY Ring Little WHOLE PERSON So, the number you get for the appropriate digit must be converted to a number represented by a larger anatomic part.
5 FIGURE 2 1 HIERARCHY IN WHOLE PERSON CONCEPT FOR UPPER EXTREMITIES: UPPER EXTREMITY 100% WHOLE PERSON 40% 50% 60% 60% Introduction to the AMA s 6th edition of the Guides
6
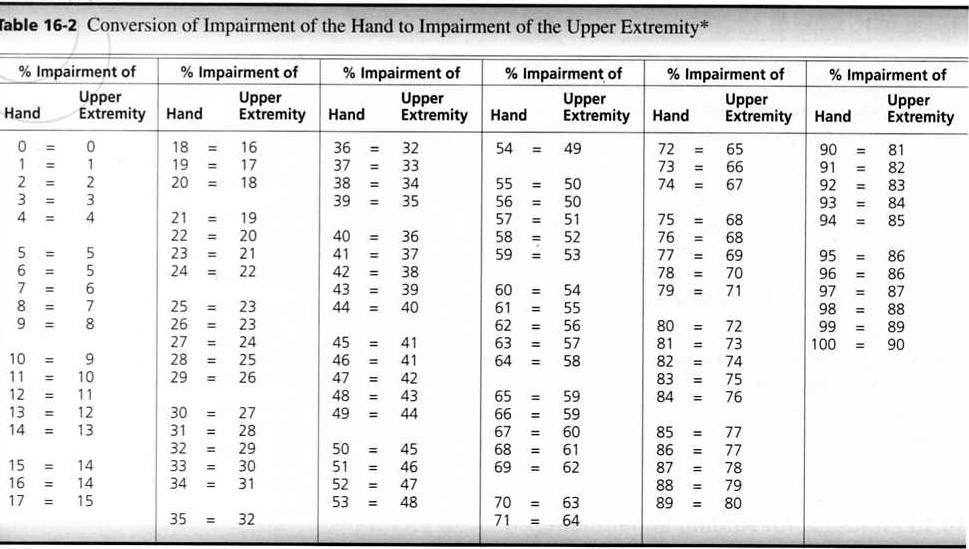
7 Using Table 16-1, you first combine the digit to the hand. EXAMPLE: A 40% impairment of the thumb converts to a 16% impairment of the hand. A 16% impairment of the hand converts to a 14% impairment of the upper extremity. A 14% impairment of the upper extremity converts to an 8% impairment of the whole person. EXAMPLE: A 40% impairment of the index finger converts to an 8% impairment of the hand. An 8% impairment of the hand converts to a 7% impairment of the upper extremity. A 7% impairment of the upper extremity converts to a 6% impairment of the whole person.
8 Introduction to the Upper Extremities The upper extremity is divided into 4 regions (distal to proximal): 1. Digits/Hand 2. Wrist 3. Elbow 4. Shoulder
9 THE WRIST The wrist functional unit represents 60% of the upper extremity function. 1. Flexion/Extension represents 70% of wrist function and 42% of upper extremity function. 2. Radial/Ulnar Deviation represents 30% of wrist function and 18% of upper extremity function.
10 Normal range of motion of the wrist is from 60 degrees extension to 60 degrees flexion. Procedure for measurement: Measure maximum active wrist flexion and extension angles from the neutral position..
11 When looking at the chart, row V represents the range of motion measured. Row IF represents the corresponding impairment of flexion. Row IE represents the corresponding impairment of extension. Note: Impairment values for angles falling between those listed may be adjusted proportionally. Add (IF) and (IE) to obtain the percent of upper extremity impairment
12 Normal range of motion of the wrist is from 20 degrees radial deviation to 30 degrees ulnar deviation Procedure for measurement: Measure maximum active wrist radial deviation and ulnar deviation angles from the neutral position.
13 When looking at the chart, row V represents the range of motion measured. Row IRD represents the corresponding impairment of radial deviation. Row IUD represents the corresponding impairment of ulnar deviation. Note: Impairment values for angles falling between those listed may be adjusted proportionally. Add (IRD) and (IUD) to obtain the percent of upper extremity impairment
14 THE ELBOW The wrist functional unit represents 70% of the upper extremity function. 1. Flexion/Extension represents 60% of elbow function and 42% of upper extremity function. 2. Pronation and Supination represents 40% of elbow function and 28% of upper extremity function.
15 Normal range of motion of the elbow is from 140 degrees flexion to 0 degrees extension Procedure for measurement: Measure maximum active elbow flexion and extension from the neutral position.
16 When looking at the chart, row V represents the range of motion measured. ELBOW JOINT Row IF represents the corresponding impairment of flexion. Row IE represents the corresponding impairment of extension. Note: Impairment values for angles falling between those listed may be adjusted proportionally. Add (IE) and (IF) to obtain the percent of upper extremity impairment
17 Normal range of motion of the elbow is from 80 degrees supination to 80 degrees pronation from the neutral position. Procedure for measurement: Measure maximum active elbow flexion and extension from the neutral position.
18 ELBOW ELBOW JOINT JOINT When looking at the chart, row V represents the range of motion measured. Row IS represents the corresponding impairment of flexion. Row IP represents the corresponding impairment of extension. Note: Impairment values for angles falling between those listed may be adjusted proportionally. Add (IS) and (IP) to obtain the percent of upper extremity impairment
19 THE SHOULDER The shoulder functional unit represents 60% of the upper extremity function. The shoulder has three units which add to the relative value. 1. Flexion/Extension represents 50% of shoulder function and 30% of upper extremity function. 2. Abduction/Adduction represents 30% of shoulder function and 18% of upper extremity function. 3. Internal/External Rotation represents 20% of shoulder function and 12% of upper extremity function.
20 The normal range of motion of the shoulder in flexion is 180 degrees. The normal range of motion of the shoulder in extension is 50 degrees. When combine together the flexion/extension unit represents 30% of the upper extremity range of motion. Once again the pie chart is set up like the wrist and elbow.
21 PROBLEM A patient has been seen in the office for 4 months. Based on a complete physical examination it has been determined that the patient has reached MMI with the following findings. R. Shoulder Flexion: 80 degrees R. Shoulder Extension: 20 degrees Using the chart to the right determine the impairment to the upper extremity.
22 R. Shoulder Flexion: 80 degrees R. Shoulder Extension: 20 degrees IF% = 7% UE IE% = 2% UE Since this is range of motion of a single joint, the numbers are added. 7% + 2% = 9% UE The final upper extremity rating, in this case, is 9% UE
23 ABDUCTION/ADDUCTION The normal range of motion of the shoulder in abduction is 180 degrees. The normal range of motion of the shoulder in extension is 50 degrees. When combine together the abduction/adduction unit represents 18% of the upper extremity range of motion. Once again the pie chart is set up like the wrist and elbow.
24 PROBLEM A patient has been seen in the office for 4 months. Based on a complete physical examination it has been determined that the patient has reached MMI with the following findings. R. Shoulder Abduction: 110 degrees R. Shoulder Adduction: 20 degrees Using the chart to the left determine the impairment to the upper extremity.
25 R. Shoulder Abduction: 110 degrees R. Shoulder Adduction: 20 degrees IABD% = 3% UE IADD% = 1% UE Since this is range of motion of a single joint, the numbers are added. 3% + 1% = 4% UE The final upper extremity rating, in this case, is 4% UE
26 INTERNAL/EXTERNAL ROTATION The normal range of motion of the shoulder in internal rotation is 90 degrees. The normal range of motion of the shoulder in external rotation is 90 degrees. When combine together the abduction/adduction unit represents 12% of the upper extremity range of motion.
27 Using the chart to the left determine the impairment to the upper extremity. PROBLEM: A patient has been seen in the office for 4 months. Based on a complete physical examination it has been determined that the patient has reached MMI with the following findings. R. Shoulder Internal Rotation: 10 degrees R. Shoulder External Rotation: 50 degrees
28 R. Shoulder Internal Rotation: 10 degrees R. Shoulder External Rotation: 50 degrees IIR % = 5% UE IER% = 1% UE Since this is range of motion of a single joint, the numbers are added. 5% + 1% = 6% UE The final upper extremity rating, in this case, is 6% UE
29 In discussing the shoulder, we have six distinct movements which all contribute to the functional unit of the shoulder. This patient has six distinct problems with the shoulder. 1. Right Shoulder Flexion: 80 degrees 2. Right Shoulder Extension: 20 degrees 3. Right Shoulder Abduction: 110 degrees 4. Right Shoulder Adduction: 20 degrees 5. Right Shoulder Internal Rotation: 10 degrees 6. Right Shoulder External Rotation: 50 degrees Using the appropriate charts, determine the final upper extremity rating for this patient. 80 (7) + 20 (2) (3) +20 (1) + 10 (5) +50 (1) = 19% UE
30 Using this chart, what would the whole person rating be, IF, this was the only finding? In this case the final whole person rating would be 11%. Take a look at 100% UE. Note: 100% UE cannot ever exceed 60% WP.
31 PERIPHERAL NERVE DISORDERS It is extremely important to arrive at an accurate, defensible diagnosis that your documentation, testing, and procedures can support. In the 5 th edition of the Guides, they address upper extremity impairments related to disorders of the spinal nerves (C5 to C8 and T1), the brachial plexus, and major peripheral nerves of the upper extremities. It also addresses the evaluation of specific conditions, including entrapment/compression neuropathy and complex regional pain syndromes (CRPS), which include CRPS I/reflex sympathetic dystrophy (RSD) and CRPS II/causalgia. Ratings based on peripheral nerve disorders are based on the anatomic distribution and severity of loss of function resulting from: 1. Sensory deficits or pain 2. Motor deficits and loss of power
32 It is important to remember that within each chapter there are a number of exceptions to each rule. Example: If restricted motion cannot be attributed strictly to a peripheral nerve lesion, such as would be the case in CRPS I/RSD, the motion impairment values are evaluated separately. Once the value is calculated it is then combined with the peripheral nerve system impairment value. IMPAIRMENT EVALUATION (MOTOR AND SENSORY) Besides range of motion, sensory and motor deficits are also ratable. If both are involved, then the two are rated separately and then the numbers are combined.

33 SENSORY IMPAIRMENT RATING (SIR) O U C H
34 SENSORY IMPAIRMENT RATING (SIR) FORMULA 1. Identify the area of involvement using the cutaneous or dermatome charts. 2. Identify the nerve(s) that innervate the area(s). 3. Determine the value of the nerve(s) that innervates the area of involvement (Spinal nerves, Brachial plexus, and major peripheral nerves. 4. Grade the severity of the sensory deficit or pain according to the grading classification. Use clinical judgment to select the appropriate percentage from the range of each grade. 5. Multiply the full value of the nerve by the degree of sensory deficit or pain.
35 The following example is taken from the AMA Guides, 5 th edition. Final Diagnosis: Reduced dislocation of the right shoulder to its normal anatomical position (as seen on x-ray). STEP ONE: Location: Identify the area of involvement using the cutaneous or dermatome charts. Some loss of muscle strength. While standing with the arm placed alongside the body and the elbow flexed, the individual could actively abduct and elevate the upper arm from 90 degrees to 180 degrees against gravity and slight resistance. Some hypesthesia of the skin over the lower two thirds of the deltoid muscle that did not interfere with activity.

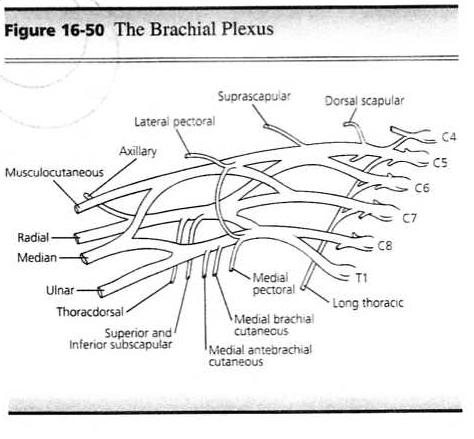
36 STEP TWO: Identify the nerve(s) that innervate the area(s). Cutaneous dermatome involved: Lateral brachial cutaneous nerve (terminal sensory branch of the axillary nerve).
37 STEP THREE: Determine the value of the nerve(s) that innervates the area of involvement (Spinal nerves, Brachial plexus, and major peripheral nerves. Severity of sensory deficit or pain: Grade 4. This was selected based on clinical judgment. Since the range for this for this grade is between 1% and 25%, a mid grade number was chosen to be 15%.
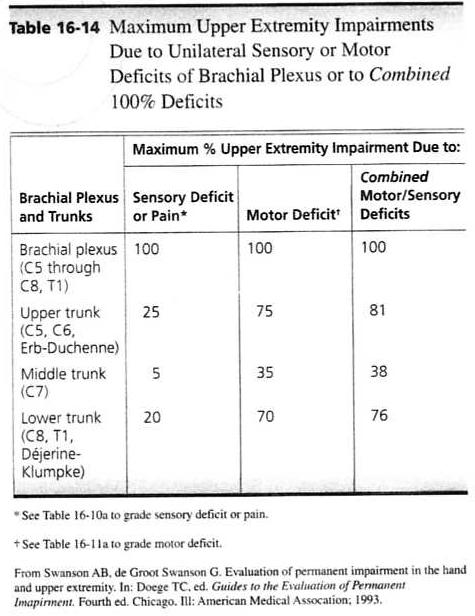
38 STEP FOUR: Grade the severity of the sensory deficit or pain according to the grading classification. Use clinical judgment to select the appropriate percentage from the range of each grade. Maximum upper extremity impairment resulting from sensory deficit of the sensory branch of the axillary nerve is 5%.
39 STEP FIVE: Multiply the full value of the nerve by the degree of sensory deficit or pain. Multiply the maximum upper extremity impairment for sensory deficit of the axillary nerve sensory branch (5%) by the severity of the sensory deficit (15%) to obtain the impairment of the upper extremity due to sensory deficit of the axillary nerve terminal sensory branch. 5% x 15% =.075%, which is rounded off to 1% UE.
40
41

42 MOTOR IMPAIRMENT RATING (MIR)
43 The AMA Guides addresses the loss of strength as a neurological deficit. Rules and precautions must be taken in order to rate the motor aspects appropriately. Muscle testing, including tests for strength, duration, repetition of contraction, and function helps evaluate the motor function of specific nerves. Testing should be performed both ACTIVELY and PASSIVELY, but, only the ACTIVE movement should be considered in the impairment.
44 The rating of loss of function due to loss of strength is dependent on two major factors: 1. Muscle Grade 2. Innervation of the nerve that goes to the muscle Muscle Grading is based on two principles: 1. Gravity (the ability to raise a segment of the body through its ROM against gravity). 2. Resistance (to hold its segment at the end of its ROM against resistance).
45 The Guides lists six muscle grades and assigns each a value. NOTE: In the 5 th edition, the rating scales now read 5 through 0 with 5 being considered normal and 0 indicating no contractibility. GRADE % MOTOR DEFICIT 5 Complete active ROM against 0 gravity with full resistance 4 Complete active ROM against gravity with some resistance Complete active ROM against gravity only, without resistance 2 Complete active ROM, with gravity eliminated 1 Evidence of slight contractability, no joint movement 0 No evidence of contractabilty 100 To be accurate, compare the affected and non-affected sides.
46 MOTOR IMPAIRMENT FORMULA (MIR) 1. Identify the motion involved, such as flexion, extension, etc. 2. Identify the muscle(s) performing the motion and the motor nerve(s) involved. 3. Grade the severity of the motor deficit of individual muscles according to the classification provided on the previous slide. 4. Find the maximum impairment of the upper extremity due to motor deficit for each nerve structure involved. 5. Multiply the severity of the motor deficit by the maximum impairment value to obtain the upper extremity impairment for each structure involved.
47 Using the same region as the SIR, an example of the MIR is as follows: Final Diagnosis: Reduced dislocation of the right shoulder to its normal anatomical position (as seen on x-ray). STEP ONE: Identify the motion involved, such as flexion, extension, etc. Motion: While standing with the arm placed alongside the body, and the elbow flexed, the individual could actively abduct and elevate the upper arm from 90 degrees to 180 degrees against gravity and slight resistance.
48 STEP TWO: Indentify the muscle(s) performing the motion and the motor nerve(s) involved. Muscle Performing the motion: Deltoid Motor nerve involved: Axillary
49 STEP THREE: Grade the severity of the motor deficit of individual muscles according to the classification provided. GRADE 5 Complete active ROM against gravity with full resistance % MOTOR DEFICIT 0 4 Complete active ROM against gravity with some resistance 3 Complete active ROM against gravity only, without resistance 2 Complete active ROM, with gravity eliminated 1 Evidence of slight contractability, no joint movement No evidence of contractabilty 100 In this case, the motor deficit is 4. A severity rating of 25% was selected on clinical judgment because of the severity of the weakness

50 STEP FOUR: Find the maximum impairment of the upper extremity due to motor deficit for each nerve structure involved.
51 STEP FIVE: Multiply the severity of the motor deficit by the maximum impairment value to obtain the upper extremity impairment for each structure involved. In this case, multiply the maximum upper extremity impairment for motor deficit of the axillary nerve (35%) by the severity of motor deficit (255) to obtain the impairment of the upper extremity due to motor deficit of the axillary nerve. 35% x 25% = 9%
52 We now have a patient who has a 1% UE impairment resulting from a SIR and a 9% UE impairment resulting from a MIR. 10% UE = 6% WP The two numbers have to be COMBINED. 1% C 9% = 10% UE
53 When multiple movements are affected in one joint due to loss of strength, each motion must be calculated separately and then the value for each movement COMBINED. EXAMPLE: Abduction and adduction of the right shoulder against gravity only. 1. Motion: Abduction of right shoulder 2. Muscle: Deltoid 3. Nerve: Axillary 4. Value of Nerve: 35% 5. Muscle Grade: 3 6. Summary: 50% of 35% = 17.5% or 18% UE
54 SUMMARY 1. Motion: Adduction of the right shoulder 2. Muscle: Pectoralis Major 3. Nerve: Pectorals (Anterior Thoracic) 4. Value of Nerve: 5% 5. Muscle Grade: 50% or 5% = 2.5 or 3% UE 18% (Adduction) C 3% (Adduction) = 20% UE (Combined Value Chart) FINAL ANSWER 20% UE = 12 WP
55 SPECIAL NOTE: When you have an entire extremity involved it is, based on experience, the conservative approach to use the value of a nerve only one time. Using the same nerve on multiple occasions for different movements may involve duplication. At times, the use of the lower end of the muscle grading scale may help to reduce the rating, if necessary. REMEMBER, give the patient what is due. HOWEVER, when rating an extremity the final impairment should not exceed the amputation rating. It would be very difficult to explain that to a judge or jury.


56
57 This section will help to identify pain that results from an illness or injury, and is included in an SIR, and that which is an autonomous process (chronic pain). This section of the AMA Guides focuses on those situations in which the pain itself is a major cause of suffering, dysfunction, or medical intervention. For the purposes of evaluation, pain is considered in this chapter is persistent, which is not to say that it is refractory to all treatment, but that is likely to be permanent and stationary. CONSIDER THE FOLLOWING: 1. It is difficult to provide an objective method for assessing chronic pain. 2. In chronic pain states, there is often no demonstrable active disease or unhealed injury, and the autonomic changes that accompany acute pain, even the anesthetized individual, are typically absent.
58 3. Pain, as defined by the International Association for the Study of Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage. 4. Pain usually includes the following concepts: a. Biological b. Psychological c. Social 5. Pain is influenced by cognitive, behavioral, environmental, and cultural factors. FIRST AND FOREMOST: PAIN IS SUBJECTIVE!
59 Think about this statement from E. Scarry To have great pain is to have certainty, to hear that another person has pain is to have doubt. Chronic pain as an extension of acute nociceptive pain is not valid. Chronic pain is defined as an evolving process in which injury may produce one pathogenic mechanism, which in turn produce one pathogenic mechanism, which in turn produces others, so that the cause(s) of pain change over time. Pain can exist without tissue damage, and tissue damage can exist without pain.
60 GENERAL THOUGHTS RELATING TO THE PRI: 1. it was decided that impairment ratings for pain disorders would not be expressed as percentages of whole person impairment. 2. the value of a qualitative assessment is that any identification of a significant pain component warrants additional consideration when interpreting impairment ratings used for allocation of medical resources, work placement, or financial compensation. 3. impairment ratings currently include allowances for the pain that individuals typically experience when they suffer from various injuries or diseases.
61 USING THE PAIN RELATED IMPAIRMENT (PRI) Organ and body system impairment rating does not adequately address impairment in several situations, as follows: 1. When there is excess pain in the context of verifiable medical conditions that cause pain. In this situation a patient has a verifiable, objective injury or illness. EXAMPLE: An individual with persistent lumbar radiculopathy following a lumbar diskectomy. Such an individual will usually have objective findings, including atrophy of the affected leg, muscle weakness, and MRI evidence of epidural scarring. An individual with these findings would receive an impairment rating of 10% on the basis of the DRE spine impairment rating system
62 Although the DRE rating is usually appropriate, some individuals with persistent lumbar radiculopathies report excess pain They report that their pain causes severe ADL deficits, suggesting a level of impairment greater than 10%. Procedures in this chapter can be used to assess this additional impairment and to classify it as mild, moderate, moderately severe, or severe.

63 2. When there are well-established pain syndromes without significant identifiable organ dysfunction to explain the pain. Individuals in this group have pain syndromes that are widely accepted by physicians based on the individuals clinical presentation but that are not associated with definable tissue pathology. In these individuals there is no measureable organ dysfunction. These individuals must have symptoms and signs that can plausibly be attributed to a well-designed medical condition.
64 If an examiner determines that an individual has a diagnosis that is not on the list, he or she may rate the individual s pain-related impairment if he or she is convinced that the diagnosed condition is well recognized and that the pain-related impairment is a consequence of the condition. REMEMBER: Be sure that you can support your opinion and provide a report that explains your decision.

65 3. When there are other associated pain syndromes. Use this chapter to evaluate pain-related impairment when dealing with syndromes with the following characteristics: a. They are associated with identifiable organ dysfunction that is ratable according to other chapters in the Guides. b. They may be associated with well-established pain syndromes, but the occurrence or nonoccurrence of the pain syndromes is not predictable; so that c. The impairment ratings provided in other chapters of the Guides do not capture the added burden of illness borne by individuals who have the associated pain syndromes.
66 When should you NOT use this chapter? 1. When conditions are adequately rated in other chapters of the Guides. 2. When rating individuals with low credibility. 3. When there are ambiguous or controversial pain syndromes Since the distinction between well recognized conditions and ambiguous or controversial ones is subtle, asking the following questions can separate the two: 1. Do the individual s symptoms and/or physical findings match any known medical condition? 2. Is the individual s presentation typical of the diagnosed condition? 3. Is the diagnosed condition one that is widely accepted by physicians as having a well-defined pathophysiologic basis?
67 If the answer to all three questions is yes, the examiner should consider the individual s pain-related impairment to be ratable. If the answer to any of the three questions is no, the examiner should consider the individual s pain-related impairment to be unratable. According to the Guides, if the determination is unratable, the examiner should still use the assessment protocol to determine the severity and impact of the individual s pain and report the results, noting that it is unratable. NOTE: What this actually does is take the burden of proof away from the examiner and merely states that the pain in unratable. No comment is made as to whether or not the individual actually has pain, or to the extent of that pain. Your are merely stating that it is not ratable under current standards. According to the Guides, it is more appropriate for the examining physician to describe the individual s pain-related impairment as unratable than to give a rating that cannot be supported by either scientific evidence or consensus.
68 An overview of the pain related impairment. Due to the nature of this type of rating, it differs significantly from the conventional rating system. The Process A. Evaluate the individual according to the body or organ rating system. During the examination informally assess the pain-related impairment. B. If the pain noted in the examination of the body part or organ system encompasses the pain experienced by the individual, then the rating of that body part or organ system encompasses that pain. C. If the individual appears to have pain-related impairment that has increased the burden of his or her condition slightly, the examiner may increase the percentage found in A by up to 3%.
69 D. It is important to do a pain-related impairment assessment in the presence of the following: 1. The individual appears to have pain-related impairment that is substantially in excess of the impairment determined in A. Or 2. The individual has a well-recognized medical condition that is characterized by pain in the absence of measurable dysfunction of an organ or body part.

70 Or 3. The individual has a syndrome with the following characteristics: a. it is associated with identifiable organ dysfunction that is ratable according to other chapters in the Guides ; b. It may be associated with a well-established pain syndrome, but the occurrence or nonoccurrence of the pain syndrome is not predictable; so that c. the impairment ratings provided in step A do not capture the added burden of illness borne by the individual because of his or her associated pain syndrome.
71 E. If the examiner performs a formal pain-related impairment rating, he or she may increase the percentage found in step A by up to 3%, and he or she should classify the individual s pain-related impairment into one of four categories: Mild Moderate Moderately Severe, or Severe. In addition, the examiner should determine whether the pain-related impairment is ratable or unratable. REMEMBER: This process is generally subjective and the examiner MUST support their conclusions.
72 Practical Steps in rating pain-related impairment: 1. Use of a questionnaire: This is part of a more extensive Questionnaire that may be found In the Guides. The scoring of the answers helps Identify whether the problem is Mild through Severe.
73 2. Assess whether the individual is at MMI. 3. Determine the severity of the pain. a. Visual Analog Scale b. Standardized Tests c. Numeric or box rating scale d. Discuss exacerbating or mitigating factors e. McGill Pain Questionnaire 4. Determine activity restrictions. a. Pain Disability Questionnaire (PDQ) b. Oswestry c. Roland-Morris 5. Determine the presence of emotional distress. a. Beck Depression Inventory b. Zung Depression Index c. Hamilton Self-Rating Scale for Depression
74 6. Determine if pain behaviors are present. a. A pain behavior is a manner in which an individual communicates information about their pain. b. It is important to be able to differential between someone who exaggerates and someone who is stoic. 1. The examiner should start the evaluation as they enter the room observing the way the individual sits, answers questions, etc. NOTE: So that this process may be as objective as possible (understanding that pain is subjective) the Guides has provided an assessment tool.
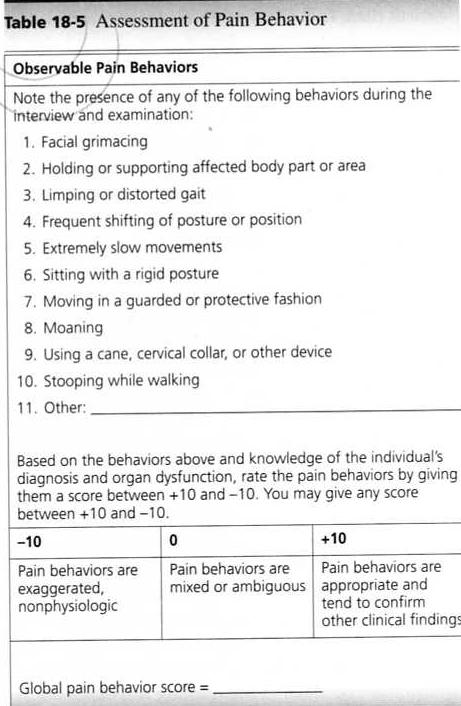
75
76 7. Credibility of the individual. Here is the question that you need to ask yourself before assigning a Pain-Related Impairment. Do the limitations that an individual describes and demonstrates accurately reflect the burden of illness he or she bears during everyday activity? NOTE: There are many factors that come into play when using this method of impairment rating. The rating itself will usually come under scrutiny as this is the most subjective form of evaluation.
77 NOTE: There are many factors that come into play when using this method of impairment rating. The rating itself will usually come under scrutiny as this is the most subjective form of evaluation. There are additional consideration to be concerned about, such as: 1. Psychogenic Pain 2. Malingering 3. Psychosomatic Pain 4. Etc. It is my suggestion that an examiner should use this method of impairment rating ONLY when absolutely necessary, and is defensible.
78
UNDERSTANDING PAIN RELATED IMPAIRMENT: CHAPTER 18 OF THE AMA GUIDES INTRODUCTION
 UNDERSTANDING PAIN RELATED IMPAIRMENT: CHAPTER 18 OF THE AMA GUIDES INTRODUCTION This course involves reviewing the following materials as well as Chapter 18 of the AMA Guides (5th Edition). The chapter
UNDERSTANDING PAIN RELATED IMPAIRMENT: CHAPTER 18 OF THE AMA GUIDES INTRODUCTION This course involves reviewing the following materials as well as Chapter 18 of the AMA Guides (5th Edition). The chapter
RECIPES FOR RATINGS !!! A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P.
 RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
IAIABC 2003 Upper Extremity Impairment Guides Part 3 of the Supplemental Impairment Rating Guides
 IAIABC 2003 Upper Extremity Impairment Guides Part 3 of the Supplemental Impairment Rating Guides Draft 11-03 IAIABC Executive Office 5610 Medical Circle, Suite 14 Madison, WI 53719 Phone: (608) 663-6355
IAIABC 2003 Upper Extremity Impairment Guides Part 3 of the Supplemental Impairment Rating Guides Draft 11-03 IAIABC Executive Office 5610 Medical Circle, Suite 14 Madison, WI 53719 Phone: (608) 663-6355
QME AMA Impairment Ratings (6hrs) ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars
 ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars") QME AMA Impairment Ratings (6hrs) ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars Instructions: Answer all questions and email answers to: marcusstrutzdc@gmail.com Please DO NOT scan tests or test
QME AMA Impairment Ratings (6hrs) ~ Glenn Crafts, DC ~ Back to Chiropractic CE Seminars Instructions: Answer all questions and email answers to: marcusstrutzdc@gmail.com Please DO NOT scan tests or test
Basic AMA Impairment Ratings for Chiropractors CE Exam 6 Hours ~ Back to Chiropractic CE Seminars
 Basic AMA Impairment Ratings for Chiropractors CE Exam 6 Hours ~ Back to Chiropractic CE Seminars Simply list your answers (write down letter choice only: in a NUMBERED vertical column and email to: marcusstrutzdc@gmail.com
Basic AMA Impairment Ratings for Chiropractors CE Exam 6 Hours ~ Back to Chiropractic CE Seminars Simply list your answers (write down letter choice only: in a NUMBERED vertical column and email to: marcusstrutzdc@gmail.com
Back To Chiropractic Continuing Education Seminars
 Welcome: Back To Chiropractic Continuing Education Seminars Basic AMA Impairment Ratings for Chiropractors: ~ 6 Hours This course counts as 6 Hours of CE for the Chiropractic Board of Examiners for the
Welcome: Back To Chiropractic Continuing Education Seminars Basic AMA Impairment Ratings for Chiropractors: ~ 6 Hours This course counts as 6 Hours of CE for the Chiropractic Board of Examiners for the
EVALUATING AMA IMPAIRMENT IN CALIFORNIA. Report Writing Mark Evans, DWC Rater
 EVALUATING AMA IMPAIRMENT IN CALIFORNIA Report Writing Mark Evans, DWC Rater What Makes a Good Report? Identifiers Patient name Claim number Date of injury Date of birth Occupation/duties Introduction/purpose
EVALUATING AMA IMPAIRMENT IN CALIFORNIA Report Writing Mark Evans, DWC Rater What Makes a Good Report? Identifiers Patient name Claim number Date of injury Date of birth Occupation/duties Introduction/purpose
Air splint exercises. THINGS TO WATCH OUT FOR -Elevation of shoulder -Compensatory techniques throughout the body -Improper use of muscles -Breathing
 Air splint exercises Place arm in splint up until armpit, make sure that fingers are spread to start. Blow up splint until firm. This will stretch out the elbow. So if the elbow is tight, stretch out prior
Air splint exercises Place arm in splint up until armpit, make sure that fingers are spread to start. Blow up splint until firm. This will stretch out the elbow. So if the elbow is tight, stretch out prior
Nerve Injury. 1) Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.
 Upper Lesions of the Brachial Plexus called Erb- Duchene Palsy or syndrome.") Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Nerve Injury - Every nerve goes to muscle or skin so if the nerve is injured this will cause paralysis in the muscle supplied from that nerve (paralysis means loss of function) then other muscles and other
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
Treatment Guidelines - Shoulder
 Treatment Guidelines - Shoulder These guidelines may be applicable to a variety of diagnosis, injuries and dysfunctions. Use you clinical judgment when proceeding on any course of treatment. Description
Treatment Guidelines - Shoulder These guidelines may be applicable to a variety of diagnosis, injuries and dysfunctions. Use you clinical judgment when proceeding on any course of treatment. Description
Brachial Plexopathy in a Division I Football Player
 www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
www.fisiokinesiterapia.biz Brachial Plexopathy in a Division I Football Player Brachial Plexus Injuries in Sport Typically a transient neurapraxia - 70% of injured players said they did not always report
A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy
 An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy") A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy Table of Contents Introduction.. 3 Active Movement Scale 4 AMS Evaluation Form.
A Clinicians Guide To The Active Movement Scale (AMS) An Evaluative Tool For Infants With Obstetrical Brachial Plexus Palsy Table of Contents Introduction.. 3 Active Movement Scale 4 AMS Evaluation Form.
Physical Examination of the Shoulder
 General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
General setup Patient will be examined in both the seated and supine position so exam table needed 360 degree access to patient Expose neck and both shoulders (for comparison); female in gown or sports
The Elbow and Radioulnar Joints Kinesiology. Dr Cüneyt Mirzanli Istanbul Gelisim University
 The Elbow and Radioulnar Joints Kinesiology Dr Cüneyt Mirzanli Istanbul Gelisim University 1 The Elbow & Radioulnar Joints Most upper extremity movements involve the elbow & radioulnar joints. Usually
The Elbow and Radioulnar Joints Kinesiology Dr Cüneyt Mirzanli Istanbul Gelisim University 1 The Elbow & Radioulnar Joints Most upper extremity movements involve the elbow & radioulnar joints. Usually
The Upper Limb III. The Brachial Plexus. Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa
 The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
The Upper Limb III The Brachial Plexus Anatomy RHS 241 Lecture 12 Dr. Einas Al-Eisa Brachial plexus Network of nerves supplying the upper limb Compression of the plexus results in motor & sensory changes
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
WEEKEND 2 Elbow. Elbow Range of Motion Assessment
 Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Virginia Orthopedic Manual Physical Therapy Institute - 2016 Technique Manual WEEKEND 2 Elbow Elbow Range of Motion Assessment - Patient Positioning: Sitting or supine towards the edge of the bed - Indications:
Assessment of the Brachial Plexus EMG Course CNSF Halifax Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University
 Assessment of the Brachial Plexus EMG Course CNSF Halifax 2018 Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University Angela Scott, Association of Electromyography Technologists of
Assessment of the Brachial Plexus EMG Course CNSF Halifax 2018 Fraser Moore, Canadian Society of Clinical Neurophysiology McGill University Angela Scott, Association of Electromyography Technologists of
3/3/2016. International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI)
") International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
International Standards for the Neurologic Classification of Spinal Cord Injury (ISNCSCI) American Spinal Injury Association International Spinal Cord Society Presented by Adam Stein, MD Chairman and Professor
REHABILITATION FOR SHOULDER FRACTURES & SURGERIES. Clavicle fractures Proximal head of humerus fractures
 REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta
REHABILITATION FOR SHOULDER FRACTURES & SURGERIES Clavicle fractures Proximal head of humerus fractures By Dr. Mohamed Behiry Lecturer Department of physical therapy for Orthopaedic and its surgery. Delta
Evaluating Movement Posture Disorganization
 Evaluating Movement Posture Disorganization A Criteria-Based Reference Format for Observing & Analyzing Motor Behavior in Children with Learning Disabilities By W. Michael Magrun, MS, OTR 3 R D E D I T
Evaluating Movement Posture Disorganization A Criteria-Based Reference Format for Observing & Analyzing Motor Behavior in Children with Learning Disabilities By W. Michael Magrun, MS, OTR 3 R D E D I T
The following annexes (I, J, and K) are used to classify athletes for the 2016 DoD Warrior Games. General methodology is below:
 are used to classify athletes for the 2016 DoD Warrior Games. General methodology is below:") The following annexes (I, J, and K) are used to classify athletes for the 2016 DoD Warrior Games. General methodology is below: 1. Review Games Rules and Classification criteria (particularly Appendix
The following annexes (I, J, and K) are used to classify athletes for the 2016 DoD Warrior Games. General methodology is below: 1. Review Games Rules and Classification criteria (particularly Appendix
Therapy Manual DO NOT PRINT
 Therapy Manual Contents 1. Shoulder 2. Shoulder and elbow a. Protraction: 1 DoF 1 b. Flexion: 1 DoF 1-6 c. Extension: 1 DoF 1-2 d. Abduction: 1 DoF 1-4 e. External rotation: 1 DoF 1-14 a. Combined shoulder
Therapy Manual Contents 1. Shoulder 2. Shoulder and elbow a. Protraction: 1 DoF 1 b. Flexion: 1 DoF 1-6 c. Extension: 1 DoF 1-2 d. Abduction: 1 DoF 1-4 e. External rotation: 1 DoF 1-14 a. Combined shoulder
4/28/2015 DR. TRACY W. PRICE, D.C. PPI due to injury or illness AMA GUIDES TO THE EVALUATION OF PERMANENT IMPAIRMENT 5 TH EDITION
 DR. TRACY W. PRICE, D.C CHAPEL HILL CHIROPRACTIC CENTER, INC. 1520 HOME AVE. AKRON, OH 44310 PH.330.630.1500: FAX.330.630.9303 EMAIL: DOCKTRACY@AOL.COM WEB: AKRONCHHIRO.COM AMA GUIDES TO THE EVALUATION
DR. TRACY W. PRICE, D.C CHAPEL HILL CHIROPRACTIC CENTER, INC. 1520 HOME AVE. AKRON, OH 44310 PH.330.630.1500: FAX.330.630.9303 EMAIL: DOCKTRACY@AOL.COM WEB: AKRONCHHIRO.COM AMA GUIDES TO THE EVALUATION
SHOULDER PAIN. A Real Pain in the Neck. Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017
 SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
SHOULDER PAIN A Real Pain in the Neck Michael Wolk, MD Northeastern Rehabilitation Associates October 31, 2017 THE SHOULDER JOINT (S) 1. glenohumeral 2. suprahumeral 3. acromioclavicular 4. scapulocostal
THE SPINE AMA GUIDES CHAPTER 15
 THE SPINE AMA GUIDES CHAPTER 15 Tim Mussack Marlene Phillips Bradford & Barthel, LLP AMA Analysis and Ratings Division HOUSEKEEPING ITEMS To control background noise, all attendees will be muted. Access
THE SPINE AMA GUIDES CHAPTER 15 Tim Mussack Marlene Phillips Bradford & Barthel, LLP AMA Analysis and Ratings Division HOUSEKEEPING ITEMS To control background noise, all attendees will be muted. Access
PNS and ANS Flashcards
 1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
1. Name several SOMATIC SENSES Light touch (being touched by a feather), heat, cold, vibration, pressure, pain are SOMATIC SENSES. 2. What are proprioceptors; and how is proprioception tested? PROPRIOCEPTORS
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
NEWBORN NURSES POLICY AND PROCEDURES. PURPOSE: Varying positions helps to stimulate physiological functioning and provides rest.
 NEWBORN NURSES POLICY AND PROCEDURES SUBJECT: POSITIONING EFFECTIVE DATE: 6/91 PURPOSE: Varying positions helps to stimulate physiological functioning and provides rest. POLICY: 1. The nurse will vary
NEWBORN NURSES POLICY AND PROCEDURES SUBJECT: POSITIONING EFFECTIVE DATE: 6/91 PURPOSE: Varying positions helps to stimulate physiological functioning and provides rest. POLICY: 1. The nurse will vary
[7] 5-214F - 5 = 06%
![[7] 5-214F - 5 = 06%](/thumbs/86/93472785.jpg "[7] 5-214F - 5 = 06%") Craig Andrew Lange craig@pdratings.com Our Document # 1201Taffy (PTP Rating) Impairment & Disability Rating Specialists http://www.pdratings.com/ Voice: (415) 861-4040 / Fax: (415) 276-3741 Luis Pérez-Cordero
Craig Andrew Lange craig@pdratings.com Our Document # 1201Taffy (PTP Rating) Impairment & Disability Rating Specialists http://www.pdratings.com/ Voice: (415) 861-4040 / Fax: (415) 276-3741 Luis Pérez-Cordero
ELBOW - 1 FLEXION: ROM (Supine / Sitting)
") ELBOW - 1 FLEXION: ROM (Supine / Sitting) Position (A) Patient: Place arm against side of trunk. Helper: Hold elbow to stabilize. (B) - Lift hand toward shoulder, palm up. - Keep wrist straight. Do sessions
ELBOW - 1 FLEXION: ROM (Supine / Sitting) Position (A) Patient: Place arm against side of trunk. Helper: Hold elbow to stabilize. (B) - Lift hand toward shoulder, palm up. - Keep wrist straight. Do sessions
"INDUSTRIAL ERGONOMICS"
 PRESENTER'S GUIDE "INDUSTRIAL ERGONOMICS" Part of the General Safety Series Quality Safety and Health Products, for Today... and Tomorrow OUTLINE OF MAJOR PROGRAM POINTS OUTLINE OF MAJOR PROGRAM POINTS
PRESENTER'S GUIDE "INDUSTRIAL ERGONOMICS" Part of the General Safety Series Quality Safety and Health Products, for Today... and Tomorrow OUTLINE OF MAJOR PROGRAM POINTS OUTLINE OF MAJOR PROGRAM POINTS
This presentation is the intellectual property of the author. Contact them for permission to reprint and/or distribute.
 The Stiff Hand: Manual Therapy Sylvia Dávila, PT, CHT San Antonio, Texas Orthopedic Manual Therapy Common Applications Passive stretch Tensile force to tissue to increase extensibility of length & ROM
The Stiff Hand: Manual Therapy Sylvia Dávila, PT, CHT San Antonio, Texas Orthopedic Manual Therapy Common Applications Passive stretch Tensile force to tissue to increase extensibility of length & ROM
An Illustrated Guide For Peripheral Nerve Examination. Bedside Teaching for 2 nd year medical Students
 An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
An Illustrated Guide For Peripheral Nerve Examination Bedside Teaching for 2 nd year medical Students Prepared by: Dr. Farid Ghalli Clinical Teacher (Hon) November 2016 Before Examination : Wash hands
Steven Feinberg MD Andrew Sew Hoy MD
 Steven Feinberg MD Andrew Sew Hoy MD COA Conference April 17 th 2010 September 3 rd 2009 PD Rating rebuttable may use any method within the Guides of the Evaluation of Permanent Impairment 5 th Edition
Steven Feinberg MD Andrew Sew Hoy MD COA Conference April 17 th 2010 September 3 rd 2009 PD Rating rebuttable may use any method within the Guides of the Evaluation of Permanent Impairment 5 th Edition
General Procedure and Rules
 General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
General Procedure and Rules PROCEDURE Description: This assessment is a measure of upper extremity (UE) and lower extremity (LE) motor and sensory impairment. Equipment: A chair, bedside table, reflex
Humerus. Ulna. Radius. Carpals
 Posture Analysis Exercise T. Armstrong M. Ebersole 1.0 Objectives: 1. Improve skill for rating over all job and identifying specific force and posture problems 2. Learn how to characterize posture 3. Learn
Posture Analysis Exercise T. Armstrong M. Ebersole 1.0 Objectives: 1. Improve skill for rating over all job and identifying specific force and posture problems 2. Learn how to characterize posture 3. Learn
Gross Anatomy Questions That Should be Answerable After October 27, 2017
 Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Gross Anatomy Questions That Should be Answerable After October 27, 2017 1. The inferior angle of the scapula of a woman who was recently in an automobile accident seems to protrude making a ridge beneath
Clinical examination of the wrist, thumb and hand
 Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
Clinical examination of the wrist, thumb and hand 20 CHAPTER CONTENTS Referred pain 319 History 319 Inspection 320 Functional examination 320 The distal radioulnar joint.............. 320 The wrist.......................
GLOSSARY. Active assisted movement: movement where the actions are assisted by an outside force.
 GLOSSARY The technical words used in this guide are listed here in alphabetic order. The first time one of these words is used in the guide, it is written in italics. Sometimes there is reference to a
GLOSSARY The technical words used in this guide are listed here in alphabetic order. The first time one of these words is used in the guide, it is written in italics. Sometimes there is reference to a
Assessment Form Post Polio Syndrome and Late Effects of Polio
 FULL NAME: DATE OF BIRTH: PHONE NUMBER: CURRENT HOME ADDRESS: EMAIL ADDRESS: THERAPIST: REFERRAL SOURCE: CURRENT GP: NEXT OF KIN: ACC/NHI NUMBER: PATIENT GOALS OF TODAY S ASSESSMENT: MAIN PROBLEMS PATIENT
FULL NAME: DATE OF BIRTH: PHONE NUMBER: CURRENT HOME ADDRESS: EMAIL ADDRESS: THERAPIST: REFERRAL SOURCE: CURRENT GP: NEXT OF KIN: ACC/NHI NUMBER: PATIENT GOALS OF TODAY S ASSESSMENT: MAIN PROBLEMS PATIENT
What is Kinesiology? Basic Biomechanics. Mechanics
 What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
D: Doorway Stretch E: Towel Stretch for Pectoralis Minor Blackburn Exercises: 6 Positions A: Prone Horizontal Abduction (Neutral)
") D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
D: Doorway Stretch Bring your shoulder into a horizontal position out to your side (abduction) and flex your elbow 90û Place your elbow against the edge of a doorway Lead forward and downwards with your
ORTHOSCAN MOBILE DI POSITIONING GUIDE
 ORTHOSCAN MOBILE DI POSITIONING GUIDE Table of Contents SHOULDER A/P of Shoulder... 4 Tangential (Y-View) of Shoulder... 5 Lateral of Proximal Humerus... 6 ELBOW A/P of Elbow... 7 Extended Elbow... 8 Lateral
ORTHOSCAN MOBILE DI POSITIONING GUIDE Table of Contents SHOULDER A/P of Shoulder... 4 Tangential (Y-View) of Shoulder... 5 Lateral of Proximal Humerus... 6 ELBOW A/P of Elbow... 7 Extended Elbow... 8 Lateral
Lowe Plastic Surgery (LPS)
") Lowe Plastic Surgery (LPS) PATIENT EDUCATION FOR: CUMULATIVE TRAUMA DISORDER THE PROBLEM: There has been a remarkable increase in what is termed cumulative trauma disorder (CTD) in the last 20 years. Other
Lowe Plastic Surgery (LPS) PATIENT EDUCATION FOR: CUMULATIVE TRAUMA DISORDER THE PROBLEM: There has been a remarkable increase in what is termed cumulative trauma disorder (CTD) in the last 20 years. Other
Pain Assessment Patient Interview (location/nature of symptoms), Body Diagram. Observation and Examination: Tests and Measures
, Body Diagram. Observation and Examination: Tests and Measures") Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
Examination of Upper Quarter Neurogenic Pain Jane Fedorczyk, PT, PhD, CHT Thomas Jefferson University, Philadelphia, PA Center of Excellence for Hand and Upper Limb Rehabilitation I. History Mechanism
region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla.
 1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
Peripheral Nerve Injuries of the Upper Limb.
 Peripheral Nerve Injuries of the Upper Limb www.fisiokinesiterapia.biz Definitions Radiculopathy Process affecting the nerve root, most commonly by a herniated disc Weakness in muscles supplied by the
Peripheral Nerve Injuries of the Upper Limb www.fisiokinesiterapia.biz Definitions Radiculopathy Process affecting the nerve root, most commonly by a herniated disc Weakness in muscles supplied by the
Clinical examination of the dog with thoracic limb lameness
 Clinical examination of the dog with thoracic limb lameness Examination of the patient Examination of the patient with musculoskeletal disease should start with a general physical examination. Particular
Clinical examination of the dog with thoracic limb lameness Examination of the patient Examination of the patient with musculoskeletal disease should start with a general physical examination. Particular
Types of Body Movements
 Types of Body Movements Bởi: OpenStaxCollege Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles
Types of Body Movements Bởi: OpenStaxCollege Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles
Chapter 8 8/23/2016. Body Mechanics and Patient Mobility. Introduction to Body Mechanics and Patient Mobility
 Chapter 8 Body Mechanics and Patient Mobility All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Introduction to Body Mechanics and Patient Mobility
Chapter 8 Body Mechanics and Patient Mobility All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Introduction to Body Mechanics and Patient Mobility
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age - Certain conditions are more prevalent in particular age groups (i.e. Full rotator cuff tears are more common over the age of 45, traumatic injuries
*Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus.
 *Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus. *Vertebral column is formed by the union of 33 sequential vertebrae
*Our main subject is the brachial plexus but it's important to understand the spinal cord first in order to understand the brachial plexus. *Vertebral column is formed by the union of 33 sequential vertebrae
Basics of Soft- Tissue Examination
 Basics of Soft- Tissue Examination Basics of Soft Tissue Exam For practitioners who primarily use their hands to treat the human structure: Examination must include functional tests to determine the type
Basics of Soft- Tissue Examination Basics of Soft Tissue Exam For practitioners who primarily use their hands to treat the human structure: Examination must include functional tests to determine the type
Presidency General Hospital, Calcutta
 CONGENITAL ANOMALY OF HAND: " MIRROR HAND " By M. MUKERJI, F.R.C.S. Presidency General Hospital, Calcutta Case Report.--S. B., aged 4 months, was born with eight fingers and no thumb on the left hand and
CONGENITAL ANOMALY OF HAND: " MIRROR HAND " By M. MUKERJI, F.R.C.S. Presidency General Hospital, Calcutta Case Report.--S. B., aged 4 months, was born with eight fingers and no thumb on the left hand and
Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual
 Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual 2nd Edition Isabelle M. Bohman, M.S., P.T., NDT Coordinator Instructor TM Published by Clinician s View Albuquerque, NM 505-880-0058
Handling Skills Used in the Management of Adult Hemiplegia: A Lab Manual 2nd Edition Isabelle M. Bohman, M.S., P.T., NDT Coordinator Instructor TM Published by Clinician s View Albuquerque, NM 505-880-0058
GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017
 GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only
GENERAL EXERCISES THUMB, WRIST, HAND BMW MANUFACTURING CO. PZ-AM-G-US I July 2017 Disclosure: The exercises, stretches, and mobilizations provided in this presentation are for educational purposes only
1-Apley scratch test.
 1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
1-Apley scratch test. The patient attempts to touch the opposite scapula to test range of motion of the shoulder. 1-Testing abduction and external rotation( +ve sign touch the opposite scapula, -ve sign
Evidence-Based Examination of the Elbow, Wrist, and Hand
 Evidence-Based Examination of the Elbow, Wrist, and Hand Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check-offs Chapter Five: Movement Examination of the Elbow, Wrist, and Hand
Evidence-Based Examination of the Elbow, Wrist, and Hand Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check-offs Chapter Five: Movement Examination of the Elbow, Wrist, and Hand
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone
, to the elbow joint (distal) - it has one bone ; the humerus which is a long bone") *the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
MOTOR EVALUATION SCALE FOR UPPER EXTREMITY IN STROKE PATIENTS (MESUPES-arm and MESUPES-hand)
") MOTOR EVALUATION SCALE FOR UPPER EXTREMITY IN STROKE PATIENTS (MESUPES-arm and MESUPES-hand) Name patient: Test date - hour: Name examiner: Duration of the test: min Handedness: right/left Support sitting
MOTOR EVALUATION SCALE FOR UPPER EXTREMITY IN STROKE PATIENTS (MESUPES-arm and MESUPES-hand) Name patient: Test date - hour: Name examiner: Duration of the test: min Handedness: right/left Support sitting
WTC II Term 3 Notes & Assessments
 Term 3 Notes & Assessments Planes of Motion/Axes The body moves in a number of various ways and directions. In the past you have learned about the terminology for movements at specific joints, for example,
Term 3 Notes & Assessments Planes of Motion/Axes The body moves in a number of various ways and directions. In the past you have learned about the terminology for movements at specific joints, for example,
Inhibition Associated with somatic dysfunctions, no matter which components are impaired Implies consideration of all components in treatment planning
 Somatic Dysfunction Impaired or altered function of related components of the somatic system including the skeletal, arthrodial, myofascial structures and their related vascular, lymphatic and neural elements.
Somatic Dysfunction Impaired or altered function of related components of the somatic system including the skeletal, arthrodial, myofascial structures and their related vascular, lymphatic and neural elements.
Nerve Conduction Studies and EMG
 Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Nerve Conduction Studies and EMG Limitations of other methods of investigations of the neuromuscular system - Dr Rob Henderson, Neurologist Assessment of Weakness Thanks Peter Silburn PERIPHERAL NEUROPATHY
Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects
 Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects Test protocol Muscle test procedures. Prior to each test participants
Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body weight, height, and sex in 178 healthy subjects Test protocol Muscle test procedures. Prior to each test participants
CKSS 2012 Exercise Science Section 1: The Anatomical Position An Introduction to Health and Physical Education
 CKSS 2012 Exercise Science Section 1: The Anatomical Position An Introduction to Health and Physical Education Ted Temertzoglou Paul Challen ISBN 1-55077-132-9 Text Books, Work Book and Reading List Introductions
CKSS 2012 Exercise Science Section 1: The Anatomical Position An Introduction to Health and Physical Education Ted Temertzoglou Paul Challen ISBN 1-55077-132-9 Text Books, Work Book and Reading List Introductions
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Location Terms. Anterior and posterior. Proximal and Distal The term proximal (Latin proximus; nearest) describes where the appendage joins the body.
 describes where the appendage joins the body.") HUMAN ANAT OMY Location Terms Anterior and posterior In human anatomical usage, anterior refers to the front of the individual. Similarly, posterior refers to the back of the subject. In standard anatomical
HUMAN ANAT OMY Location Terms Anterior and posterior In human anatomical usage, anterior refers to the front of the individual. Similarly, posterior refers to the back of the subject. In standard anatomical
G24: Shoulder and Axilla
 G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson
 Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson Abstract Title: Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Background:
Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Courtney Convey and Dr. Erickson Abstract Title: Dynamic Neuromobilization for the Treatment of Thoracic Outlet Syndrome Background:
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.
 Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow.") MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
MLT Muscle(s) Patient Position Therapist position Stabilization Limb Position Picture Put biceps on slack by bending elbow. Pectoralis Minor Supine, arm at side, elbows extended, supinated Head of Table
Evaluation of Tingling and Numbness in the Upper Extremities
 Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
Evaluation of Tingling and Numbness in the Upper Extremities DR. W. ANTHONY FRISELLA M.D. ADVANCED BONE & JOINT, ST CHARLES MO MONA 2018 Overview Polyneuropathy Compressive nerve lesions Carpal tunnel
THE EXTREMITY SCREEN MANUAL: A Guide to the Subjective and Objective Outcomes Assessment of the Upper and Lower Extremity
 THE EXTREMITY SCREEN MANUAL: A Guide to the Subjective and Objective Outcomes Assessment of the Upper and Lower Extremity Steven G. Yeomans, DC, FACO INTRODUCTION: Objective screen for the extremities
THE EXTREMITY SCREEN MANUAL: A Guide to the Subjective and Objective Outcomes Assessment of the Upper and Lower Extremity Steven G. Yeomans, DC, FACO INTRODUCTION: Objective screen for the extremities
18 The Independent Orthopaedic Medical Examination
 18 The Independent Orthopaedic Medical Examination Noubar Didizian, M.D. and Samuel D. Hodge, Jr., Esq. INTRODUCTION Orthopaedic surgery is that discipline of medicine that deals with the musculoskeletal
18 The Independent Orthopaedic Medical Examination Noubar Didizian, M.D. and Samuel D. Hodge, Jr., Esq. INTRODUCTION Orthopaedic surgery is that discipline of medicine that deals with the musculoskeletal
Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Evidence- Based Examination of the Shoulder Practice Session & Skills Check- offs Evidence- Based Examination of the Shoulder Presented by Eric Hegedus, PT, DPT, MHSC, OCS, CSCS Practice Sessions/Skill
Shoulder Joint Examination. Shoulder Joint Examination. Inspection. Inspection Palpation Movement. Look Feel Move
 Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Shoulder Joint Examination History Cuff Examination Instability Examination AC Joint Examination Biceps Tendon Examination Superior Labrum Examination Shoulder Joint Examination Inspection Palpation Movement
Essential intervention No. 3 Oedema control KEY OBJECTIVES. Danger
 Essential intervention No. 3 Oedema control KEY OBJECTIVES To know what causes oedema. To know which kind of oedema needs to be referred for emergency surgery and why. To know the effects of oedema on
Essential intervention No. 3 Oedema control KEY OBJECTIVES To know what causes oedema. To know which kind of oedema needs to be referred for emergency surgery and why. To know the effects of oedema on
Key Points for Success:
 SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
SELF WRIST & HAND 1 2 All of the stretches described in this chapter are detailed to stretch the right side. Key Points for Success: Sit comfortably in a position where you can straighten or fully extend
Importance of Developmental Kinesiology for Manual Medicine
 Importance of Developmental Kinesiology for Manual Medicine Pavel Kolá!, 1996 Dpt. of Rehabilitation, University Hospital Motol, Prague, Czech Republic (Czech Journal of Rehabilitation and Physical Therapy)
Importance of Developmental Kinesiology for Manual Medicine Pavel Kolá!, 1996 Dpt. of Rehabilitation, University Hospital Motol, Prague, Czech Republic (Czech Journal of Rehabilitation and Physical Therapy)
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi. E. mail:
 Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Nerves of the upper limb Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Brachial plexus Median nerve After originating from the brachial plexus in the axilla,
Hands PA; Obl. Lat.; Norgaard s Thumb AP; Lat. PA. PA; Lat.: Obls.; Elongated PA with ulnar deviation
 Projections Region Basic projections Additional / Modified projections Upper Limbs Hands PA; Obl. Lat.; Norgaard s Thumb ; Lat. PA Fingers PA; Lat. Wrist PA; Lat. Obls. Scaphoid Lunate Trapezium Triquetral
Projections Region Basic projections Additional / Modified projections Upper Limbs Hands PA; Obl. Lat.; Norgaard s Thumb ; Lat. PA Fingers PA; Lat. Wrist PA; Lat. Obls. Scaphoid Lunate Trapezium Triquetral
Treatment of the Child with Cerebral Palsy Post Surgical Rehabilitation
 Treatment of the Child with Cerebral Palsy Post Surgical Rehabilitation Sheelah Cochran OTR/L, CPAM, CKTP Objectives Perform an initial evaluation of post-surgical conditions Identify appropriate splinting
Treatment of the Child with Cerebral Palsy Post Surgical Rehabilitation Sheelah Cochran OTR/L, CPAM, CKTP Objectives Perform an initial evaluation of post-surgical conditions Identify appropriate splinting
Biceps Brachii. Muscles of the Arm and Hand 4/4/2017 MR. S. KELLY
 Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Muscles of the Arm and Hand PSK 4U MR. S. KELLY NORTH GRENVILLE DHS Biceps Brachii Origin: scapula Insertion: radius, fascia of forearm (bicipital aponeurosis) Action: supination and elbow flexion Innervation:
Considerations in the selection of patients for Selective Dorsal Rhizotomy
 Considerations in the selection of patients for Selective Dorsal Rhizotomy The best and the worst surgery I have ever been associated with. A therapist's perspective Dean Morgan, PT Disclosure Statement
Considerations in the selection of patients for Selective Dorsal Rhizotomy The best and the worst surgery I have ever been associated with. A therapist's perspective Dean Morgan, PT Disclosure Statement
Adult Brachial Plexus Injuries: Introduction and the Role of Surgery
 Adult Brachial Plexus Injuries: Introduction and the Role of Surgery Tim Hems Scottish National Brachial Plexus Injury Service Department of Orthopaedic Surgery, Queen Elizabeth University Hospital, GLASGOW.
Adult Brachial Plexus Injuries: Introduction and the Role of Surgery Tim Hems Scottish National Brachial Plexus Injury Service Department of Orthopaedic Surgery, Queen Elizabeth University Hospital, GLASGOW.
Spinal Hygiene Exercise
 Spinal Hygiene Exercise Incorporate your Spinal Hygiene exercises (AHC, Y/W/T/L, and R.O.M.) into your daily routine (during breaks at the office, whenever you get up to go to the washroom, in the morning
Spinal Hygiene Exercise Incorporate your Spinal Hygiene exercises (AHC, Y/W/T/L, and R.O.M.) into your daily routine (during breaks at the office, whenever you get up to go to the washroom, in the morning
Supplemental Information Packet for Classifiers: 2016 DOD WARRIOR GAMES
 FOR TEAM STAFF TRACK and FIELD - Please complete the table below if the athlete has an amputation AMPUTATION TRACK FIELD Below Knee TR4.5 SE6.0 / ST4.5 Above Knee TR4.0 SE5.0 / ST4.0 Double BK or BK &
FOR TEAM STAFF TRACK and FIELD - Please complete the table below if the athlete has an amputation AMPUTATION TRACK FIELD Below Knee TR4.5 SE6.0 / ST4.5 Above Knee TR4.0 SE5.0 / ST4.0 Double BK or BK &
Human Anatomy Biology 351
 1 Human Anatomy Biology 351 Upper Limb Exam Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
1 Human Anatomy Biology 351 Upper Limb Exam Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
OMT Without An OMT Table Workshop. Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP
 OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint
 / Shoulder Joint") INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
INSTRUCTION MANUAL FOR THE FLEXTEND AC Exercise System for The Acromioclavicular (AC) / Shoulder Joint FLEXTEND -AC: Congratulations! You have chosen to use the FLEXTEND -AC Upper Extremity Training System,
Chapter 6 The Elbow and Radioulnar Joints
 The Elbow & Radioulnar Chapter 6 The Elbow and Radioulnar Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Most upper extremity movements involve the elbow & radioulnar joints Usually grouped
The Elbow & Radioulnar Chapter 6 The Elbow and Radioulnar Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Most upper extremity movements involve the elbow & radioulnar joints Usually grouped
Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs Chapter Five: Movement Examination of the Lumbar Spine Time) (45 minutes
Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs Chapter Five: Movement Examination of the Lumbar Spine Time) (45 minutes
PREPARED FOR. Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016. REFERRING DOCTOR : Dr.
 Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
Motion of Left Upper Extremity During A Right- Handed Golf Swing
 Motion of Left Upper Extremity During A Right- Handed Golf Swing Description of Movement While the movement required for a golf swing requires many muscles, joints, & ligaments throughout the body, the
Motion of Left Upper Extremity During A Right- Handed Golf Swing Description of Movement While the movement required for a golf swing requires many muscles, joints, & ligaments throughout the body, the
THE LOWER EXTREMITIES AMA GUIDES CHAPTER 17
 THE LOWER EXTREMITIES AMA GUIDES CHAPTER 17 Tim Mussack Marlene Phillips Bradford & Barthel, LLP AMA Analysis and Ratings Division Bradford & Barthel AMA Analysis and Ratings Division Tim Mussack (916)
THE LOWER EXTREMITIES AMA GUIDES CHAPTER 17 Tim Mussack Marlene Phillips Bradford & Barthel, LLP AMA Analysis and Ratings Division Bradford & Barthel AMA Analysis and Ratings Division Tim Mussack (916)
The arm: *For images refer back to the slides
 The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
PHYSIOTHERAPY PROTOCOLS FOR THE MANAGEMENT OF DIFFERENT TYPES OF BRACHIAL PLEXUS INJURIES
 PHYSIOTHERAPY PROTOCOLS FOR THE MANAGEMENT OF DIFFERENT TYPES OF BRACHIAL PLEXUS INJURIES Introduction As such, protocols in the management of brachial plexus injuries (BPI) are a bit of a misnomer. This
PHYSIOTHERAPY PROTOCOLS FOR THE MANAGEMENT OF DIFFERENT TYPES OF BRACHIAL PLEXUS INJURIES Introduction As such, protocols in the management of brachial plexus injuries (BPI) are a bit of a misnomer. This