ERAS: Enhanced Recovery After Surgery. Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland
|
|
|
- Eric Preston
- 6 years ago
- Views:
Transcription

1 ERAS: Enhanced Recovery After Surgery Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland
 Multimodal analgesia Regional anesthesia-analgesia ERAS at")
2 Overview History and basic principles of ERAS Review published ERAS data Anesthesiology ERAS topics Goal-directed fluid therapy (GDFT) Multimodal analgesia Regional anesthesia-analgesia ERAS at Hopkins
3 History of ERAS Previously known as fast-track surgery Studies in 1990s (Kehlet Denmark) showed LOS for colon resection from 9-10 d 2 d Also known as enhanced recovery programs (ERP) ERAS : acronym started in 2001 (academic surgeons) Intent: develop optimal evidence-based perioperative care pathway to facilitate patient recovery Changed name from fast-track (implied focus on faster d/c only) to ERAS (focus on overall patient recovery) Br J Surg 1999;86: JPEN 2014;38:559-66
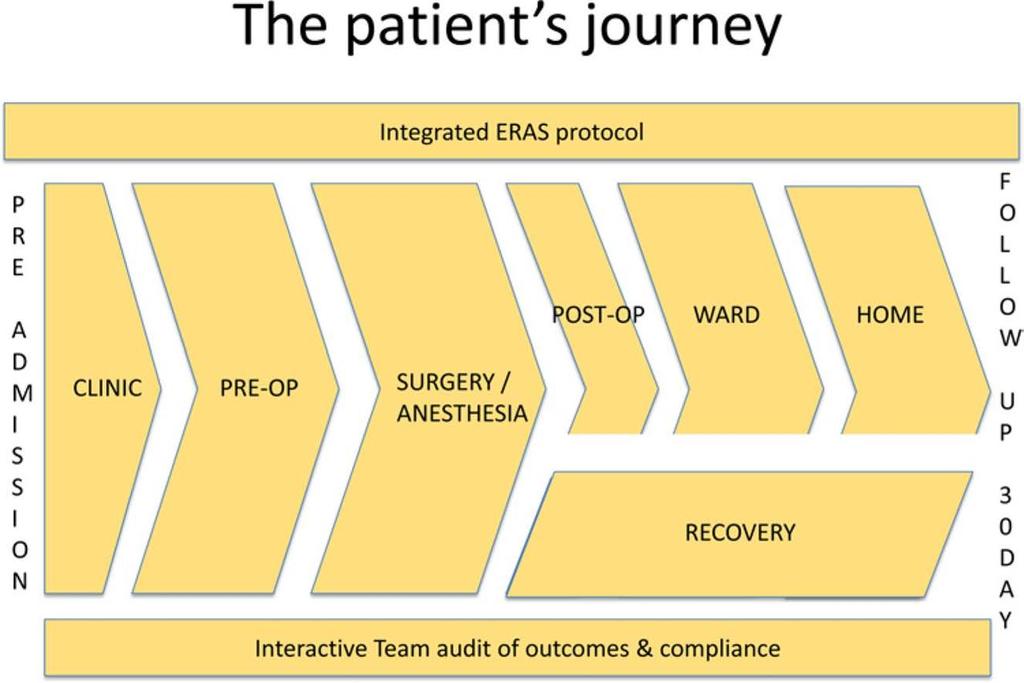
4 Philosophy of ERAS Traditional hospital works in silos need to be removed to optimize patient care One team may have little insight if the treatment they use for their purpose is beneficial hrs or days later Team taking over patient care may have little insight into what occurred before their part of the care process ERAS pathways designed everyone involved in the entire chain of events during patient s care True multidisciplinary effort: improves communication; allows team members to understand each other roles JPEN 2014;38:559-66
5 JPEN 2014;38:559-66
6 ERAS: General Goals Get patient back to normal preoperative function as quickly as possible Normal gastrointestinal function Pain control Mobilization Minimize complications Improve patient experience
7 ERAS: Basic Principles Multidisciplinary and collaborative approach Optimize perioperative nutrition Standardized perioperative anesthestic plan to minimize pain/opioid usage/stress response Early mobilization and oral intake Patient education and participation
8 Clin Nutr 2005;24:466-77
9 Preoperative Information, education and counseling Medical optimization Standardized bowel preparation Preoperative fasting and carbohydrate treatment Preanesthetic medication Prophylaxis against thromboembolism World J Surg 2013;37:259-84
10 Intraoperative Antimicrobial prophylaxis and skin preparation Standardized anesthetic protocol Multimodal approach to PONV prophylaxis Laparoscopy and modifications of surgical access (if applicable) Postoperative nasogastric tubes should not be used routinely (removed at end of surgery) Prevent intraoperative hypothermia Optimize perioperative fluid management World J Surg 2013;37:259-84
11 Postoperative Urinary drainage (limit to 1-2 days) Prevention of postoperative ileus Multimodal analgesia minimize opioids Perioperative nutritional care Postoperative glucose control Early mobilization World J Surg 2013;37:259-84

12
13 Does ERAS Work? Several meta-analyses of existing RCTs to suggest that ERAS (vs. traditional care) implementation will: Length of hospital stay (LOS) Complication rate Urinary tract infection Pneumonia, respiratory complications Cardiovascular complications No difference in mortality or readmission rate Cochrane Data Syst Rev 2011: CD World J Surg 2014;38: Int J Colorectal Dis 2012;27:
14 Decrease in Length of Stay World J Surg 2014;38:
15 Decrease in Respiratory Complications World J Surg 2014;38:
16 Decrease in UTI Yang D, Grant M et al (submitted)
17 Decrease in Cardiovascular Complications World J Surg 2014;38:
18 Decrease in Morbidity World J Surg 2014;38:
19 No Difference in Readmission World J Surg 2014;38:
20 No Difference in Mortality Int J Colorectal Dis 2012;27:

21
22 Anesthesiology ERAS Topics Goal-directed fluid therapy Anesthesiology providers have generally given too much IV fluids intraoperatively Multimodal analgesia Concurrent use of non-opioid analgesic agents will result in additive/synergistic analgesia while providing an opioid-sparing effect Regional anesthesia-analgesia Local anesthetic based technique may provide superior analgesia and physiologic benefits to facilitate patient recovery
23 Goal-directed Fluid Therapy Excessive IV crystalloids cardiac/pulmonary fxn, tissue oxygenation (SSI), paralytic ileus ERAS fluid management continuum through the pre-/intra- /post-operative phases (TE Miller, Duke) Preoperative: to OR in a hydrated and euvolemic state Avoid prolonged fasting; carbohydrate drink 2-3 h before surgery Intraoperative: maintain central euvolemia, avoid excess NaCl Individualized fluid management plan using balanced crystalloid solution (LR) to provide maintenance fluid therapy. Low-risk patients/surgery = "zero-balance" probably sufficient Higher risk patients/major surgery = consider GDFT Br J Anaesth 2002;89: Can J Anaesth 2015;62:158-68
24 Goal-directed Fluid Therapy Meta-analysis of 13 RCT (1399 patients) GDFT = first bowel motion (p=0.02), oral intake (p= 0.03), PONV (p = 0.01) GDFT = more effective outside ERAS, colorectal patients RTC (n = 100): GDFT vs. routine care GDFT = SV/CO, LOS (mean 5 vs 7 days, p=0.03), earlier oral intake of solid food (p=0.01) Meta-analysis (29 RCTs): preemptive hemodynamic intervention 4805 patients with an overall mortality of 7.6% Preemptive HD mortality (OR = 0.48 [ ], p=0.0002), surgical complications (OR = 0.43 [ ], p<0.0001) Br J Surg 2015;102: Anesthesiology 2002;97:820-6 Anesth Analg 2011;112:
25 Br J Surg 2015;102:577-86
26 Multimodal Analgesia Optimal pain control in ERAS is critical to facilitate recovery Multimodal analgesia (improve pain control, opioid-related side effects) is a key component of most ERAS programs Acetaminophen, NSAIDs, NMDA antagonists, local anesthetics, gabapentanoids, alpha-2 agonists, glucocorticoids Opioids sedation, PONV, urinary retention, ileus, RD Combining acetaminophen and NSAID superior analgesia compared with either drug alone Meta-analysis (21 RCTs, 1909 patients) Pain intensity 35% and 38% less for the combination versus acetaminophen alone and NSAID alone, respectively Can J Anaesth 2015;62: Anesth Analg 2010;110:1170-9
27 Single-Dose Analgesics: >50% Relief for Moderate-Severe Postoperative Pain Drug Mean NNT 95% CI Celecoxib PO 400mg Codeine 60mg/Acetam PO 1000mg Oxycodone PO 15mg Ibuprofen PO 400mg Ibuprofen PO 200mg Meperidine IM 100mg Morphine IM 10mg Ketorolac IM 30mg Celecoxib PO 200mg Acetaminophen PO 1000mg Tramadol PO 100mg
28 Regional anesthesia-analgesia Neuraxial (epidural, spinal) or peripheral (TAP, paravertebral, wound infiltration) blocks/catheters TAP block meta (10 RCTs, 633 subjects): TAP vs. control TAP block: pain at rest at 4 and 24 h, postoperative opioid consumption Preoperative (vs. postoperative) TAP block early pain, opioid consumption Analgesic efficacy of wound catheters (infusion of LA via catheters placed in surgical wounds) is uncertain Meta-analysis (32 RCTs): no difference in side effects or analgesia at rest or on activity, except in OB-GYN patients Morphine consumption, wound breakdown, LOS (p=0.04) Anesth Analg 2014;118: Acta Anaesthesiol Scand 2011;55:785-96
29 Anesth Analg 2014;118:454-63
30 Pain at rest-24 h Pain at rest-48 h Acta Anaesthesiol Scand 2011;55:785-96
31 Role of Epidural in ERAS? TEA superior analgesia, some pulmonary/cardiac morbidity, facilitate earlier return of GI function Overall benefits of TEA in laparoscopic procedures uncertain Meta-analysis of 7 RCTs (n=378): epidurals vs. alternative analgesic methods No significant difference in complication rate (OR=1.14 [0.49, 2.64], p=0.76) or LOS; EA faster return of GI fxn, pain scores Meta-analysis (6 RCTs): epidural analgesia on laparoscopic colorectal surgery TEA = first bowel motion (p=0.02) and pain scores (p=0.04) but no difference in LOS hospital, OR time, side effects JAMA Surg 2014;149: Surg Endosc 2013;27:

32
33 ERAS at Hopkins (Anesthesiology) Goal: normal function as soon as possible Superior analgesia to facilitate recovery Minimize analgesic (opioid) side effects Short-term goals: LOS/pain, satisfaction Long-term goal: preservation of perioperative immune function: SSI/cancer recurrence Perioperative period creates a vulnerable period of immunosuppression for our surgical patients
34 Perioperative Period: High Risk Brain Beh Immun 2007;21:881-7
35 ERAS at Hopkins (Anesthesiology) Multiple systematic/literature reviews to examine available evidence for various aspects of care Incorporate appropriate evidence to meet both shortterm and long-term goals Create a preliminary pathway feedback from ERAS anesthesiology members Pathway trial further modifications based on clinical experiences Continued modification of pathway: new evidence or clinical experience warrants discussion/modification
36 ERAS at Hopkins (Anesthesiology) For open procedures = EA + TIVA For lap. procedures = TIVA + IV lidocaine + TAP Preserve immune fxn: avoid opioids, inhalation agents; ketamine, blood transfusions, hypothermia Epidural analgesia: integral part of ERAS pathways Superior analgesia vs. opioids Faster return of gastrointestinal function Attenuation of neuroendocrine stress response Preserve immune function/ opioid use
37 Epidural Anesthesia & Immunosuppression Eur J Canc Prevent 2008;17:269-72
38 Preoperative (Hopkins) Preoperative holding area (day of surgery) Oral celebrex (200 mg) Oral gabapentin (600 mg) Oral acetaminophen (1000 mg) Scopolamine patch (avoid dexamethasone) Insertion of thoracic epidural catheter (open cases)
39 Standardized Anesthetic (Hopkins) GOALS: maintain normothermia; avoid blood tnxs; minimize hypotension/hypoxia; maintain normocarbia Epidural anesthesia + TIVA (propofol) TEA: 2% lidocaine w/ 1:200K epi as bolus ( 10ml) to obtain T4 level + infusion of 2% lidocaine (no epinephrine) at 4-6ml/hr If no epidural, TIVA + IV Lidocaine gtt Adjuvants Acetaminophen 1gm IV x1 (if not given preop) Ketorolac 30 mg IV at end of case ( 15 mg IV for age >75) Ondansetron 8 mg IV 30 min prior to end of case
40 Postoperative (Hopkins) When NPO: PCEA: % bupivacaine only (no fentanyl) Continue 1 day after tolerating oral intake/analgesics Assuming no contraindications Acetaminophen 1 gm IV/PO q8h Ketorolac mg IV q6h or ibuprofen 400 mg PO q6h Breakthrough pain: hydromorphone IV prn
41 Postoperative (Hopkins) When taking PO: Acetaminophen 1000mg PO q8h Gabapentin 100 mg PO tid Ibuprofen 400 mg PO q6h Lidoderm patch Tramadol 50 mg PO q4-6h prn (before opioid) Breakthrough pain: prn opioid of choice

42
43 Hopkins CR ERAS: Results Prior to ERAS: Hopkins (major large and small bowel) mean LOS = 8.6 d (NSQIP: 10th decile) Colorectal ERAS started February 2014 Prelim analysis: colorectal d/c since 1/1/14 = median LOS of 2 days less than last 6 m of CY 2013 Equivalent of freeing up 4 additional beds every day Our own data analysis since 2/1/14 = Mean LOS = 5.3 d; median LOS = 4 d Marburg 2 patient satisfaction survey scores
44 Hopkins CR ERAS: LOS and Cost ERAS Patients Baseline Net Savings Mean Length of Stay 5.3 days 7.2 days (-)1.9 days (26.4%)* *p<0.001 Variable Direct Cost $9,036 $10,933 (-1)$1,897 (17.3%)** **p=0.013 Armstrong Institute for Patient Safety and Quality J Am Coll Surg 2015;221:669-77
45 Early results: ERAS Expansion Liver Resection (Hopkins) Metric Pre ERAS Post ERAS Improvement Patients Case Mix Index (0.1) Length of (2.1) Stay Cost $12,761 $10,450 ($2,311) Complications 9.5% 0.0% (9.5%) Readmissions 21.4% 19.6% (1.8%)

46 Hopkins CR ERAS: SSI Baseline 27% Hospital Target 15% Post-ERAS 6% Colorectal Operating Room CUSP ERAS Armstrong Institute for Patient Safety and Quality
47 Hopkins CR ERAS: Results Data from Johns Hopkins Hospital show a net savings of $400,000 in the first year of implementation Costs of Implementation: $552,783 Reduction in Direct Hospital Costs: $948,500 Net Savings: $395,717

48 NSQIP Report: 2015 Johns Hopkins Armstrong Institute for Patient Safety and Quality
49 Hopkins ERAS: Practical Considerations Attempted to develop an opioid-free ERAS pathway Opioids are ordered as a PRN (as needed) dose 50% pts will still receive opioids during their hospital stay but the overall amounts of opioids given are less With an accepted pathway, we were able to truly administer multimodal analgesia (ERAS ordersets) NSAIDs, acetaminophen, tramadol, gabapentin, epidural analgesia, lidocaine, opioid PRN for breakthrough pain Previously, some were reluctant to accept certain modalities (e.g., NSAIDs, gabapentin, epidural)

50
51 Not a rigid or fixed protocol: Final Thoughts Clinicians should feel free to do whatever they need to do to care for our patients Overall pathway continues to be modified based on updated evidence or clinician input Low volume ventilation, magnesium, acetaminophen Benefits: Focuses care around the patient Collaboration/communication among services true multidisciplinary effort Breaks down silos; staff morale; enhances SSI efforts
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital
 Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Objectives 9/7/2012. Optimizing Analgesia to Enhance the Recovery After Surgery CME FACULTY DISCLOSURE
 Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Current evidence in acute pain management. Jeremy Cashman
 Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
ENHANCED RECOVERY PROTOCOLS FOR KNEE REPLACEMENT
 ENHANCED RECOVERY PROTOCOLS FOR KNEE REPLACEMENT Jeff Gadsden, MD, FRCPC, FANZCA Associate Professor Duke University Department of Anesthesiology Regional Anesthesia and Acute Pain Medicine DISCLOSURES
ENHANCED RECOVERY PROTOCOLS FOR KNEE REPLACEMENT Jeff Gadsden, MD, FRCPC, FANZCA Associate Professor Duke University Department of Anesthesiology Regional Anesthesia and Acute Pain Medicine DISCLOSURES
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons. Karol A Gutowski, MD, FACS
 Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view
 Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view 1st Geneva International SCIENTIFIC DAY February 3 rd 2010 E. Schiffer Dept APSI, HUG 1 Fast-Track in colorectal
Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view 1st Geneva International SCIENTIFIC DAY February 3 rd 2010 E. Schiffer Dept APSI, HUG 1 Fast-Track in colorectal
Laparoscopic Colorectal Surgery
 Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Anesthesia for OutPatient Spine Surgery. Michael A. Kellams, D.O.
 Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
To staple or to sew. Zeng Xuan Hu
 To staple or to sew Zeng Xuan Hu Fast Track Surgery Multimodal Rehabilitation Accelerated recovery Accelerated rehabilitation Enhanced recovery Optimize perioperative care by reducing the expected stress
To staple or to sew Zeng Xuan Hu Fast Track Surgery Multimodal Rehabilitation Accelerated recovery Accelerated rehabilitation Enhanced recovery Optimize perioperative care by reducing the expected stress
ANICOLAU.RO. Enhanced Recovery after Colorectal Surgery. Irina Grecu, Alexandru E. Nicolau, Olle Ljungqvist*
 Enhanced Recovery after Colorectal Surgery Irina Grecu, Alexandru E. Nicolau, Olle Ljungqvist* Clinical Emergency Hospital of Bucharest, Romania *Karolinska Institute, Stockholm, Sweden ERAS - Enhanced
Enhanced Recovery after Colorectal Surgery Irina Grecu, Alexandru E. Nicolau, Olle Ljungqvist* Clinical Emergency Hospital of Bucharest, Romania *Karolinska Institute, Stockholm, Sweden ERAS - Enhanced
ERAS. Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic
 ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic Outline Definition Justification Ileus Pain Outline Specifics Data BMC Data Worldwide Data Implementation What is ERAS? AKA Fast-track
ERAS Presented by Timothy L. Beard MD, FACS, CPI Bend Memorial Clinic Outline Definition Justification Ileus Pain Outline Specifics Data BMC Data Worldwide Data Implementation What is ERAS? AKA Fast-track
Enhanced Recovery After Surgery (ERAS)
") Enhanced Recovery After Surgery (ERAS) Brad White, D.O. Anesthesiology Residency Program Director Oklahoma State University Medical Center Assistant Clinical Professor of Anesthesiology Oklahoma State
Enhanced Recovery After Surgery (ERAS) Brad White, D.O. Anesthesiology Residency Program Director Oklahoma State University Medical Center Assistant Clinical Professor of Anesthesiology Oklahoma State
Click to edit Master subtitle style
 Does Enhanced Recovery Improve Outcomes? Click to edit Master subtitle style Kaare Weber, MD Director of Surgery Associate Medical Director, Surgery A MEMBER OF THE MONTEFIORE HEALTH SYSTEM mes? Click
Does Enhanced Recovery Improve Outcomes? Click to edit Master subtitle style Kaare Weber, MD Director of Surgery Associate Medical Director, Surgery A MEMBER OF THE MONTEFIORE HEALTH SYSTEM mes? Click
Role and safety of epidural analgesia
 Anaesthesia for Liver Resection Surgery The Association of Anaesthetists Seminars 21 Portland Place, London Thursday 15 th December 2005 Role and safety of epidural analgesia Lennart Christiansson MD,
Anaesthesia for Liver Resection Surgery The Association of Anaesthetists Seminars 21 Portland Place, London Thursday 15 th December 2005 Role and safety of epidural analgesia Lennart Christiansson MD,
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Baptist Health Lexington. ERAS Protocols
 Baptist Health Lexington ERAS Protocols Enhanced Recovery After Surgery BHLex Colorectal ERAS Protocol Preoperative Patient/Family Education: PAT and office, ERAS brochure & educational flyer/checklist
Baptist Health Lexington ERAS Protocols Enhanced Recovery After Surgery BHLex Colorectal ERAS Protocol Preoperative Patient/Family Education: PAT and office, ERAS brochure & educational flyer/checklist
If you reduce variability in volume administration, HOW. you can reduce post-surgical complications, LOS and associated costs 1-4
 A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
A large body of clinical evidence* demonstrates If you reduce variability in volume administration, you can reduce post-surgical complications, LOS and associated costs 1-4 Complications Too Dry Too Wet
Enhanced Recovery after Surgery - A Colorectal Perspective. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
Enhanced Recovery after Surgery - A Colorectal Perspective R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus resolves Opioid
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Gastrointestinal and urinary complications in the postoperative period
 The 13 th Annual Perioperative Medicine Summit Fort Lauderdale, Florida Gastrointestinal and urinary complications in the postoperative period Dan Hunt, MD Professor of Medicine Director, Division of Hospital
The 13 th Annual Perioperative Medicine Summit Fort Lauderdale, Florida Gastrointestinal and urinary complications in the postoperative period Dan Hunt, MD Professor of Medicine Director, Division of Hospital
Enhanced Recovery after Surgery
 Enhanced Recovery after Surgery AKA ERAS What is Enhanced Recovery (ER)? Paradigm shift in surgery and surgical care of the patient Philosophy of care Perioperative continuum Multidisciplinary Patient
Enhanced Recovery after Surgery AKA ERAS What is Enhanced Recovery (ER)? Paradigm shift in surgery and surgical care of the patient Philosophy of care Perioperative continuum Multidisciplinary Patient
Acute Postoperative Pain. David Radvinsky, MD March 24, 2016
 Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Acute Postoperative Pain David Radvinsky, MD March 24, 2016 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give
Satisfactory Analgesia Minimal Emesis in Day Surgeries. (SAME-Day study) A Randomized Control Trial Comparing Morphine and Hydromorphone
 A Randomized Control Trial Comparing Morphine and Hydromorphone") Satisfactory Analgesia Minimal Emesis in Day Surgeries (SAME-Day study) A Randomized Control Trial Comparing Morphine and Hydromorphone HARSHA SHANTHANNA ASSISTANT PROFESSOR ANESTHESIOLOGY MCMASTER UNIVERSITY
Satisfactory Analgesia Minimal Emesis in Day Surgeries (SAME-Day study) A Randomized Control Trial Comparing Morphine and Hydromorphone HARSHA SHANTHANNA ASSISTANT PROFESSOR ANESTHESIOLOGY MCMASTER UNIVERSITY
The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting.
 The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting. { Thalia Petropoulou, Clinical Fellow Paul Hainsworth,Colorectal
The effect of laxative use in length of hospital stay and complication rate in patients undergoing elective colorectal surgery within an ERAS setting. { Thalia Petropoulou, Clinical Fellow Paul Hainsworth,Colorectal
Analgesia for ERAS programs. Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital
 Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
ANICOLAU.RO. What is ERAS? Enhanced Recovery After Surgery. A.E.Nicolau*,Irina Grecu** Spitalul Clinic de Urgenta
 Spitalul Clinic de Urgenta ANICOLAU.RO What is ERAS? Enhanced Recovery After Surgery A.E.Nicolau*,Irina Grecu** *Clinica de Chirurgie **Clinica de Anestezie Terapie Intensiva ERAS = Fast-track surgery
Spitalul Clinic de Urgenta ANICOLAU.RO What is ERAS? Enhanced Recovery After Surgery A.E.Nicolau*,Irina Grecu** *Clinica de Chirurgie **Clinica de Anestezie Terapie Intensiva ERAS = Fast-track surgery
Balanced Analgesia With NSAIDS and Coxibs. Raymond S. Sinatra MD, Ph.D
 Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Mr David A McDonald Service Improvement Manager Whole System patient Flow Improvement Programme Scottish Government
 Mr David A McDonald Service Improvement Manager Whole System patient Flow Improvement Programme Scottish Government Introduction Brief update Two main topics Use of Gabapentin Local Infiltration Analgesia
Mr David A McDonald Service Improvement Manager Whole System patient Flow Improvement Programme Scottish Government Introduction Brief update Two main topics Use of Gabapentin Local Infiltration Analgesia
Presentation objectives. Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient
 Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient Ewan McNicol PharmD, MS Presentation objectives Outline principles for management of acute pain, with focus on perioperative
Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient Ewan McNicol PharmD, MS Presentation objectives Outline principles for management of acute pain, with focus on perioperative
Management of Acute Pain in the Chronic Pain Patient. Eric Cannon, MD Mountain West Anesthesia December 1, 2017
 Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Perioperative pathophysiology and the objectives behind Enhanced Recovery Care
 Perioperative pathophysiology and the objectives behind Enhanced Recovery Care Francesco Carli, MD, MPhil McGill University Montreal, Canada franco.carli@mcgill.ca 60 patients (74 yo) Open colon resection
Perioperative pathophysiology and the objectives behind Enhanced Recovery Care Francesco Carli, MD, MPhil McGill University Montreal, Canada franco.carli@mcgill.ca 60 patients (74 yo) Open colon resection
Enhanced Recovery After Surgery: Where Do Pharmacists Come In?
 Enhanced Recovery After Surgery: Where Do Pharmacists Come In? Melinda C. Joyce, Pharm.D., FAPhA, FACHE Vice President, Corporate Support Services Med Center Health Bowling Green, Kentucky Annual Meeting
Enhanced Recovery After Surgery: Where Do Pharmacists Come In? Melinda C. Joyce, Pharm.D., FAPhA, FACHE Vice President, Corporate Support Services Med Center Health Bowling Green, Kentucky Annual Meeting
Does Anesthesia influence Cancer recurrence? Dr Ian McConachie FRCA FRCPC London, ON, Canada
 Does Anesthesia influence Cancer recurrence? Dr Ian McConachie FRCA FRCPC London, ON, Canada Why did my cancer come back? Inadequate resection Micro metastases Lymph spread Tumour biology Immune system
Does Anesthesia influence Cancer recurrence? Dr Ian McConachie FRCA FRCPC London, ON, Canada Why did my cancer come back? Inadequate resection Micro metastases Lymph spread Tumour biology Immune system
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES
 EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Continuous Wound Infusion and Postoperative Pain Current status?
 Continuous Wound Infusion and Postoperative Pain Current status? Pr Patricia Lavand homme Department of Anesthesiology St Luc Hospital University Catholic of Louvain Medical School Brussels, Belgium Severe
Continuous Wound Infusion and Postoperative Pain Current status? Pr Patricia Lavand homme Department of Anesthesiology St Luc Hospital University Catholic of Louvain Medical School Brussels, Belgium Severe
RECENT ADVANCES IN ANALGESIA
 4th ERAS UK Conference RECENT ADVANCES IN ANALGESIA Dr William J Fawcett Royal Surrey County Hospital, Guildford University of Surrey, Guildford November 14th 2014 Conflict of interests Paid honoraria
4th ERAS UK Conference RECENT ADVANCES IN ANALGESIA Dr William J Fawcett Royal Surrey County Hospital, Guildford University of Surrey, Guildford November 14th 2014 Conflict of interests Paid honoraria
Fast-track surgery and anaesthesia
 Andrew J Kitching FRCA Sarah S O Neill FRCA Major surgery induces profound physiological responses; frequent sequelae include pain, nausea, ileus, increased cardiac demands, and impaired pulmonary function.
Andrew J Kitching FRCA Sarah S O Neill FRCA Major surgery induces profound physiological responses; frequent sequelae include pain, nausea, ileus, increased cardiac demands, and impaired pulmonary function.
TAP blocks vs wound infiltration in laparoscopic colectomies Results of a Randomised Controlled Clinical Trial
 TAP blocks vs wound infiltration in laparoscopic colectomies Results of a Randomised Controlled Clinical Trial Kim Gorissen Frederic Ris Martijn Gosselink Ian Lindsey Dept of Colorectal Surgery Dept of
TAP blocks vs wound infiltration in laparoscopic colectomies Results of a Randomised Controlled Clinical Trial Kim Gorissen Frederic Ris Martijn Gosselink Ian Lindsey Dept of Colorectal Surgery Dept of
Colorectal Surgery in the Elderly. Stephen Smith
 Colorectal Surgery in the Elderly Stephen Smith Scope WHO >65 Social definition No COI Age specific incidence of CRC in Australia 2016 (new cases/100,000) My data: elective bowel resections
Colorectal Surgery in the Elderly Stephen Smith Scope WHO >65 Social definition No COI Age specific incidence of CRC in Australia 2016 (new cases/100,000) My data: elective bowel resections
Outpatient Total Knee Arthroplasty: Anesthetic Implications
 Outpatient Total Knee Arthroplasty: Anesthetic Implications Anthony Edelman, MD, MBA Clinical Assistant Professor Director, Division of Orthopedic Anesthesia Disclosures None Objectives Examine current
Outpatient Total Knee Arthroplasty: Anesthetic Implications Anthony Edelman, MD, MBA Clinical Assistant Professor Director, Division of Orthopedic Anesthesia Disclosures None Objectives Examine current
5 th ERAS UK Conference. Advances in Pain Management. Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh
 5 th ERAS UK Conference Advances in Pain Management Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh Pre-op information Optimised organ function No nutritional
5 th ERAS UK Conference Advances in Pain Management Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh Pre-op information Optimised organ function No nutritional
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Assessment. Consults & Referrals
 University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination
 Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination Jason D. Sciarretta, MD, FACS Grand Strand Medical Center, Myrtle Beach, SC University of South Carolina
Creating an Early Recovery Order Set for Colorectal Surgery-It s the Journey as well as the Destination Jason D. Sciarretta, MD, FACS Grand Strand Medical Center, Myrtle Beach, SC University of South Carolina
Measure Abbreviation: PONV 01 (MIPS 430)
") Measure Abbreviation: PONV 01 (MIPS 430) *PONV 01 is built to the specification outlined by the Merit Based Incentive Program (MIPS) 430: Prevention of Post-Operative Nausea and Vomiting (PONV) Combination
Measure Abbreviation: PONV 01 (MIPS 430) *PONV 01 is built to the specification outlined by the Merit Based Incentive Program (MIPS) 430: Prevention of Post-Operative Nausea and Vomiting (PONV) Combination
Opioid reduction strategies in an academic tertiary medical center
 Opioid reduction strategies in an academic tertiary medical center Terry Bosen, PharmD Medication Safety Program Director Vanderbilt University Medical Center Tennessee MME data per capita MME = Morphine
Opioid reduction strategies in an academic tertiary medical center Terry Bosen, PharmD Medication Safety Program Director Vanderbilt University Medical Center Tennessee MME data per capita MME = Morphine
Presentation at ACS NSQIP National Conference in July Surgical Site Infection Reduction Strategies
 Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Presentation at ACS NSQIP National Conference in July 2015 Surgical Site Infection Reduction Strategies PeaceHealth Sacred Heart Medical Center at RiverBend Level II Trauma Center 379 Beds 15,060 cases
Analgesia after c delivery - wound infusions, tap blocks and intrathecal opioids; what more can we offer our patients?
 Analgesia after c delivery - wound infusions, tap blocks and intrathecal opioids; what more can we offer our patients? Ashraf S Habib, MBBCh, MSc, MHSc, FRCA Associate Professor of Anesthesiology Interim
Analgesia after c delivery - wound infusions, tap blocks and intrathecal opioids; what more can we offer our patients? Ashraf S Habib, MBBCh, MSc, MHSc, FRCA Associate Professor of Anesthesiology Interim
Index. Enhanced Recovery in NSQIP (ERIN), 240 Epidural analgesia, 149 Epidural-induced hypotension (EIH) management, ERAS
, 240 Epidural analgesia, 149 Epidural-induced hypotension (EIH) management, ERAS") A Abdominal surgery ERP carbohydrate treatment, 46 comprehensive guide, 258 crystalloid-based perioperative fluid therapy, 120, 122 insulin resistance, 64, 169 laparoscopic order sets, 269, 274 278 laparoscopic
A Abdominal surgery ERP carbohydrate treatment, 46 comprehensive guide, 258 crystalloid-based perioperative fluid therapy, 120, 122 insulin resistance, 64, 169 laparoscopic order sets, 269, 274 278 laparoscopic
Peri operative pain control. Disclosure. Objectives 9/1/2011. No current conflicts of interest
 Peri operative pain control Chris Herndon, PharmD, FASHP Southern Illinois University Edwardsville Disclosure No current conflicts of interest Objectives Discuss studies evaluating the transformation of
Peri operative pain control Chris Herndon, PharmD, FASHP Southern Illinois University Edwardsville Disclosure No current conflicts of interest Objectives Discuss studies evaluating the transformation of
Simone Targa. Impact of an ERAS Colorectal Program on clinical outcomes and costs
 Impact of an ERAS Colorectal Program on clinical outcomes and costs Simone Targa U.O. di Clinica Chirurgica Azienda Ospedaliero-Universitaria di Ferrara Arcispedale S. Anna ERAS Protocol ENHANCED RECOVERY
Impact of an ERAS Colorectal Program on clinical outcomes and costs Simone Targa U.O. di Clinica Chirurgica Azienda Ospedaliero-Universitaria di Ferrara Arcispedale S. Anna ERAS Protocol ENHANCED RECOVERY
Intravenous lidocaine infusions. Dr Ian McConachie FRCA FRCPC
 Intravenous lidocaine infusions Dr Ian McConachie FRCA FRCPC Thank the organisers for inviting me. No conflicts or disclosures Lidocaine 1 st amide local anesthetic Synthesized in 1943 by Lofgren in Sweden.
Intravenous lidocaine infusions Dr Ian McConachie FRCA FRCPC Thank the organisers for inviting me. No conflicts or disclosures Lidocaine 1 st amide local anesthetic Synthesized in 1943 by Lofgren in Sweden.
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings?
 Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Gastrointestinal Feedings Post Op: What s the deal on beginning oral feedings? Kate Willcutts, DCN, RD, CNSC University of Virginia Health System Charlottesville, VA kfw3w@virginia.edu Objectives 1. Discuss
Evaluation of Enhanced Recovery Protocol for Elective Colorectal Surgical Operations in Assiut University Hospital
 Med. J. Cairo Univ., Vol. 85, No. 5, September: 1911-1916, 2017 www.medicaljournalofcairouniversity.net Evaluation of Enhanced Recovery Protocol for Elective Colorectal Surgical Operations in Assiut University
Med. J. Cairo Univ., Vol. 85, No. 5, September: 1911-1916, 2017 www.medicaljournalofcairouniversity.net Evaluation of Enhanced Recovery Protocol for Elective Colorectal Surgical Operations in Assiut University
Basic pathophysiology of recovery: the role of endocrine metabolic response. Franco Carli McGill University Montreal, Canada
 Basic pathophysiology of recovery: the role of endocrine metabolic response Franco Carli McGill University Montreal, Canada ASER, Washington, 2016 postoperative recovery, 1950 Loss of body weight, less
Basic pathophysiology of recovery: the role of endocrine metabolic response Franco Carli McGill University Montreal, Canada ASER, Washington, 2016 postoperative recovery, 1950 Loss of body weight, less
Anesthetic Techniques for Rapid Recovery in Total Knee Arthroplasty
 Anesthetic Techniques for Rapid Recovery in Total Knee Arthroplasty Scott T. Ball, MD Chief, Adult Joint Reconstruction Department of Orthopaedic Surgery University of California, San Diego Disclosures
Anesthetic Techniques for Rapid Recovery in Total Knee Arthroplasty Scott T. Ball, MD Chief, Adult Joint Reconstruction Department of Orthopaedic Surgery University of California, San Diego Disclosures
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Measure Abbreviation: PONV 01 (MIPS 430)
") Measure Abbreviation: PONV 01 (MIPS 430) *PONV 01 is built to the specification outlined by the Merit Based Incentive Program (MIPS) 430: Prevention of Post-Operative Nausea and Vomiting (PONV) Combination
Measure Abbreviation: PONV 01 (MIPS 430) *PONV 01 is built to the specification outlined by the Merit Based Incentive Program (MIPS) 430: Prevention of Post-Operative Nausea and Vomiting (PONV) Combination
Enhanced Recovery After Surgery Getting it Right
 Enhanced Recovery After Surgery Getting it Right Aalok Agarwala, M.D., M.B.A. Division Chief, General Surgery Anesthesia Associate Director, Quality and Safety, MGH DACCPM Assistant Professor, Harvard
Enhanced Recovery After Surgery Getting it Right Aalok Agarwala, M.D., M.B.A. Division Chief, General Surgery Anesthesia Associate Director, Quality and Safety, MGH DACCPM Assistant Professor, Harvard
Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications
 Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications Abstract Authors: Karen Martin, RHIT, CPHQ - Surgical Clinical Reviewer - Quality Management Analyst,
Pain Management Protocol in Adolescent Idiopathic Spinal Fusion Reduces Length of Stay and Complications Abstract Authors: Karen Martin, RHIT, CPHQ - Surgical Clinical Reviewer - Quality Management Analyst,
Operational Efficiency in Colon Surgery Enhanced Recovery Pathways: 23 hour laparoscopic colectomy
 Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Physician Orders ADULT: ANES Enhanced Recovery After Surgery (ERAS) Plan
 Plan") Initiate Orders Phase Non Categorized R Powerplan Open Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Anes (ERAS) Pre-insertion Phase, When to Initiate: Other-See Special Instructions,
Initiate Orders Phase Non Categorized R Powerplan Open Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Anes (ERAS) Pre-insertion Phase, When to Initiate: Other-See Special Instructions,
ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY
 PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY") Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
Department of Surgery Divison of General Surgery ENHANCED RECOVERY AFTER SURGERY (ERAS) PATHWAYS PARESH C. SHAH MD FACS VICE CHAIR OF SURGERY DIRECTOR OF GENERAL SURGERY December 2016 Disclosure Paresh
STARTER PACK: Webinar #1 ADE4 - OPIOIDS
 STARTER PACK: Webinar #1 ADE4 - OPIOIDS Welcome to the Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps
STARTER PACK: Webinar #1 ADE4 - OPIOIDS Welcome to the Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps
What s New in Post-Cesarean Analgesia?
 Anesthesia & Obstetrics What s New in Post-Cesarean Analgesia? October 23rd, 2013 2013 UCSF What Does The Evidence Tell Us? Mark Rollins, MD, PhD UC SF Post-Delivery Pain (Mean pain scores for first 24
Anesthesia & Obstetrics What s New in Post-Cesarean Analgesia? October 23rd, 2013 2013 UCSF What Does The Evidence Tell Us? Mark Rollins, MD, PhD UC SF Post-Delivery Pain (Mean pain scores for first 24
Disclosures. Total knee and Total Hip Replacement, a Fast Track. Outline of my talk. What is Fast Track Arthroplasty? I have nothing to disclose
 Total knee and Total Hip Replacement, a Fast Track Muhammad I Shaikh M.D.,Ph.D. Associate Professor of Anesthesiology, UCSF Outline of my talk Definition of Fast Track Principles of FT as applied to Orthopedics
Total knee and Total Hip Replacement, a Fast Track Muhammad I Shaikh M.D.,Ph.D. Associate Professor of Anesthesiology, UCSF Outline of my talk Definition of Fast Track Principles of FT as applied to Orthopedics
7/31/2015. Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice. Objectives. Enhanced Recovery Society
 Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice Margaret Odhner MS, ANP-BC, COCN Kim Meacham, MSN FNP-C, CWON Objectives 1. Describe the Enhanced Recover After Surgery (ERAS) pathway.
Enhanced Recovery After Surgery: Change Your Mind, Change Your Practice Margaret Odhner MS, ANP-BC, COCN Kim Meacham, MSN FNP-C, CWON Objectives 1. Describe the Enhanced Recover After Surgery (ERAS) pathway.
Enhanced Recovery in Pediatric Surgery
 Enhanced Recovery in Pediatric Surgery Diana L Diesen, M.D., FACS Assistant Professor, Department of Surgery University of Texas Southwestern Medical Center Children s Health Dallas Dallas, Tx Disclosures
Enhanced Recovery in Pediatric Surgery Diana L Diesen, M.D., FACS Assistant Professor, Department of Surgery University of Texas Southwestern Medical Center Children s Health Dallas Dallas, Tx Disclosures
ADE and Harm Collaborative: Reducing ADEs and harm associated with opioids - Safer post-operative pain management. March 21, 2013
 ADE and Harm Collaborative: Reducing ADEs and harm associated with opioids - Safer post-operative pain management March 21, 2013 Agenda, March 21, 2013 Welcome Collaborative education overview Post-operative
ADE and Harm Collaborative: Reducing ADEs and harm associated with opioids - Safer post-operative pain management March 21, 2013 Agenda, March 21, 2013 Welcome Collaborative education overview Post-operative
Professor Narinder Rawal, MD, PhD, FRCA (Hon), EDRA Department of Anaesthesiology and Intensive Care University Hospital Örebro, Sweden
, EDRA Department of Anaesthesiology and Intensive Care University Hospital Örebro, Sweden") Professor Narinder Rawal, MD, PhD, FRCA (Hon), EDRA Department of Anaesthesiology and Intensive Care University Hospital Örebro, Sweden Infiltrative techniques in perioperative pain lecture outline Why
Professor Narinder Rawal, MD, PhD, FRCA (Hon), EDRA Department of Anaesthesiology and Intensive Care University Hospital Örebro, Sweden Infiltrative techniques in perioperative pain lecture outline Why
Fast-Track Colonic Surgery: Status and Perspectives
 Fast-Track Colonic Surgery: Status and Perspectives Henrik Kehlet H. Kehlet ( ) Section for Surgical Pathophysiology, Rigshospitalet, Section 4074, Blegdamsvej 9, 2100 Copenhagen, Denmark e-mail: henrik.kehlet@rh.dk
Fast-Track Colonic Surgery: Status and Perspectives Henrik Kehlet H. Kehlet ( ) Section for Surgical Pathophysiology, Rigshospitalet, Section 4074, Blegdamsvej 9, 2100 Copenhagen, Denmark e-mail: henrik.kehlet@rh.dk
ICU Management of Minimally Invasive Cardiac Surgery
 ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
Postoperative pain management: Analgesics, algorithms and patient activation
 Postoperative pain management: Analgesics, algorithms and patient activation Alfred Deakin Prof. Mari Botti Deakin University/Epworth HealthCare Victorian Perioperative Nurses Group 60 th State Conference,
Postoperative pain management: Analgesics, algorithms and patient activation Alfred Deakin Prof. Mari Botti Deakin University/Epworth HealthCare Victorian Perioperative Nurses Group 60 th State Conference,
Screening - inclusion criteria
 PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
Advancement in the use of multimodal analgesia for acute postoperative pain
 Advancement in the use of multimodal analgesia for acute postoperative pain Ratan K. Banik, M.D., Ph.D. Assistant Professor Department of Anesthesiology University of Minnesota, Minneapolis, USA 4 October
Advancement in the use of multimodal analgesia for acute postoperative pain Ratan K. Banik, M.D., Ph.D. Assistant Professor Department of Anesthesiology University of Minnesota, Minneapolis, USA 4 October
Enthusiasm for enhanced recovery has grown in the
 Evidence Review Conducted for the Agency for Healthcare Research and Quality Safety Program for Improving Surgical Care and Recovery: Focus on Anesthesiology for Colorectal Surgery Kristen A. Ban, MD,*
Evidence Review Conducted for the Agency for Healthcare Research and Quality Safety Program for Improving Surgical Care and Recovery: Focus on Anesthesiology for Colorectal Surgery Kristen A. Ban, MD,*
Nutritional Support in the Perioperative Period
 Nutritional Support in the Perioperative Period Topic 17 Module 17.6 Facilitating Oral or Enteral Nutrition in the Postoperative Period Mattias Soop Learning Objectives To review the causes of postoperative
Nutritional Support in the Perioperative Period Topic 17 Module 17.6 Facilitating Oral or Enteral Nutrition in the Postoperative Period Mattias Soop Learning Objectives To review the causes of postoperative
Screening - inclusion criteria
 A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
Gabapentin Does Not Improve Analgesia Outcomes For Total Joint Replacement. Manyat Nantha-Aree, MD
 Gabapentin Does Not Improve Analgesia Outcomes For Total Joint Replacement Manyat Nantha-Aree, MD Objective n Preliminary results of MOBILE study in total hip and knee arthroplasty Background n Gabapentin=
Gabapentin Does Not Improve Analgesia Outcomes For Total Joint Replacement Manyat Nantha-Aree, MD Objective n Preliminary results of MOBILE study in total hip and knee arthroplasty Background n Gabapentin=
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
Opioid Free Anesthesia
 Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN 1 Why is pain important? Primary contributor to post-operative distress 56% of patients state that
Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN 1 Why is pain important? Primary contributor to post-operative distress 56% of patients state that
Welcome Charles Kennedy
 Welcome Charles Kennedy Comoderators Girish P. Joshi, MBBS, MD, FFARCI Professor of Anesthesiology and Pain Management University of Texas Southwestern Medical Center Dallas, Texas David E. Beck, MD, FACS
Welcome Charles Kennedy Comoderators Girish P. Joshi, MBBS, MD, FFARCI Professor of Anesthesiology and Pain Management University of Texas Southwestern Medical Center Dallas, Texas David E. Beck, MD, FACS
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Acute Peri-Operative Pain Management Strategies
 Slide 1 Acute Peri-Operative Pain Management Strategies Phillip Gallegos, MD USAP Pinnacle Anesthesiologist Director of Anesthesia and Peri-Operative Medicine BOSHA Slide 2 ERAS Enhanced Recovery After
Slide 1 Acute Peri-Operative Pain Management Strategies Phillip Gallegos, MD USAP Pinnacle Anesthesiologist Director of Anesthesia and Peri-Operative Medicine BOSHA Slide 2 ERAS Enhanced Recovery After
Evidenzbasiertes, perioperatives Analgesie- Konzept in der Fast Track Chirurgie. Christoph Konrad Luzern
 Evidenzbasiertes, perioperatives Analgesie- Konzept in der Fast Track Chirurgie Christoph Konrad Luzern Prävalenz Prävalenz 40.0 Hüft TEP Leistenhernie Knie TEP Thorakotomie 30.0 20.0 Br J Anaesth. 2010
Evidenzbasiertes, perioperatives Analgesie- Konzept in der Fast Track Chirurgie Christoph Konrad Luzern Prävalenz Prävalenz 40.0 Hüft TEP Leistenhernie Knie TEP Thorakotomie 30.0 20.0 Br J Anaesth. 2010
Early Recovery after Surgery (ERAS):
:") Early Recovery after Surgery (ERAS): Applying Consistently What We ve Known for 20 Years Dr. Kurt Heiss, MD Objectives Laying Foundation: Who, Why Explore Components: What Start a Program: How and When
Early Recovery after Surgery (ERAS): Applying Consistently What We ve Known for 20 Years Dr. Kurt Heiss, MD Objectives Laying Foundation: Who, Why Explore Components: What Start a Program: How and When
Post-caesarean analgesia. Genevieve Goulding Royal Brisbane & Women's Hospital 1
 Post-caesarean analgesia Genevieve Goulding Royal Brisbane & Women's Hospital 1 Contemporary challenges & barriers to providing optimal post-caesarean analgesia Genevieve Goulding Royal Brisbane & Women's
Post-caesarean analgesia Genevieve Goulding Royal Brisbane & Women's Hospital 1 Contemporary challenges & barriers to providing optimal post-caesarean analgesia Genevieve Goulding Royal Brisbane & Women's
Post Caesarean Analgesia An Update. Kim Ekelund MD, PhD, associate professor Rigshospitalet Copenhagen, Denmark
 Post Caesarean Analgesia An Update Kim Ekelund MD, PhD, associate professor Rigshospitalet Copenhagen, Denmark Post caesarean analgesia No Conflicts of Interests Neuraxial opioids Multimodal therapy Plan
Post Caesarean Analgesia An Update Kim Ekelund MD, PhD, associate professor Rigshospitalet Copenhagen, Denmark Post caesarean analgesia No Conflicts of Interests Neuraxial opioids Multimodal therapy Plan
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
Update Update on Anaesthesia for c-section Dr Kerry Litchfield Consultant Anaesthetist Princess Royal Maternity Glasgow, Scotland
 Update Update on Anaesthesia for c-section Dr Kerry Litchfield Consultant Anaesthetist Princess Royal Maternity Glasgow, Scotland Caesarean section is the most common surgical procedure in the world 1
Update Update on Anaesthesia for c-section Dr Kerry Litchfield Consultant Anaesthetist Princess Royal Maternity Glasgow, Scotland Caesarean section is the most common surgical procedure in the world 1
Reversing the Opioid Epidemic: Pain & Symptom Management Inpatient Considerations and Peri operative Multi Modal Analgesia
 Reversing the Opioid Epidemic: Pain & Symptom Management Inpatient Considerations and Peri operative Multi Modal Analgesia Aaron Wood 25 July 2018 Disclosures No Financial Interests Gratitude Feedback
Reversing the Opioid Epidemic: Pain & Symptom Management Inpatient Considerations and Peri operative Multi Modal Analgesia Aaron Wood 25 July 2018 Disclosures No Financial Interests Gratitude Feedback
Hemodynamic Optimization HOW TO IMPLEMENT?
 Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
Hemodynamic Optimization HOW TO IMPLEMENT? Why Hemodynamic Optimization? Are post-surgical complications exceptions? Patients undergoing surgery may develop post-surgical complications. The morbidity rate,
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Educational Learning Objectives. Evidence into Practice. Audience. Case Presentation. Outline. Multimodal Approach to Colorectal Surgery
 Educational Learning Objectives Multimodal Approach to Colorectal Surgery Value and Impact of Nutrition Interventions May 5, 2011 Dr. Corilee A. Watters, MSc, RD, PhD, CNSC Asst. Prof, Nutrition, University
Educational Learning Objectives Multimodal Approach to Colorectal Surgery Value and Impact of Nutrition Interventions May 5, 2011 Dr. Corilee A. Watters, MSc, RD, PhD, CNSC Asst. Prof, Nutrition, University