Complication of Percutaneous Endoscopic Gastrostomy
|
|
|
- Gillian Lynch
- 6 years ago
- Views:
Transcription
1 Complication of Percutaneous Endoscopic Gastrostomy Tube Ogori N. Kalu MD Morbidity & Mortality Conference General Surgery Service Kings County Hospital Center
2 ACGME Core Competencies 1. Medical knowledge 2. Patient care 3. Interpersonal and communication skills 4. Practice based learning 5. Systems based practice 6. Professionalism
3 Case Presentation 52 AA female on ENT service Medical history: locally invading, non obstructing squamous cell carcinoma of the left side of tongue No prior surgical history History of tobacco and alcohol consumption
4 Case Presentation Tentatively scheduled for primary tumor removal with free flap reconstruction Admitted to KCHC in July 2007 for preprocedure optimization: 1. tracheostomy 2. gastrostomy
5 Case Presentation - Hospital course xx : Tracheostomy done by ENT xx: General surgery consult for PEG xx: PEG placed in operating room Thin woman, all labs wnl Pull (Ponsky-Gauderer) technique endoscope passed into stomach, insufflation with air, puncture site located by transillumination i ti and external pressure 22Fr PEG tube placed with position confirmed endoscopically
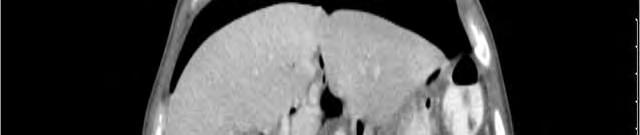
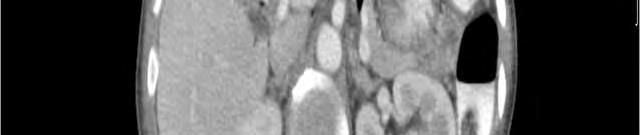
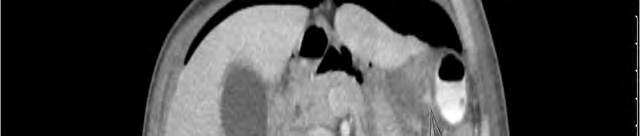
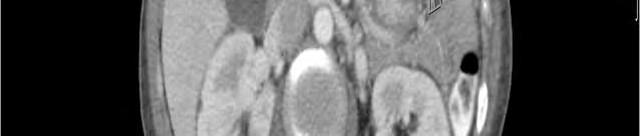
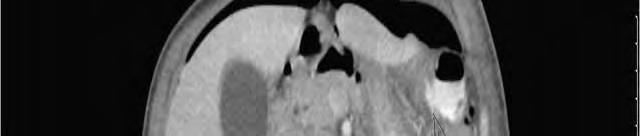
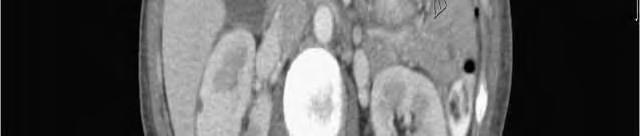
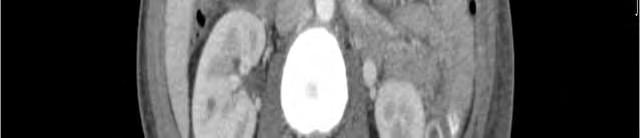
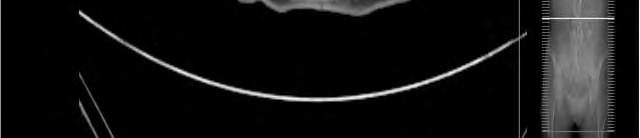
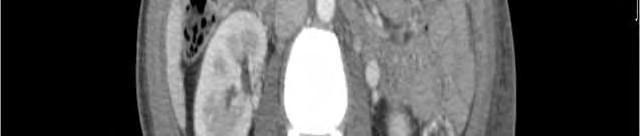
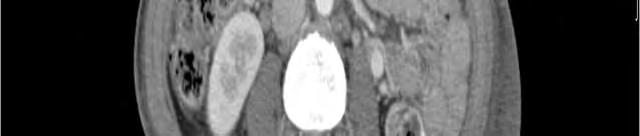
6 Case Presentation - Hospital course 7/15: started t on tube feeds 7/18: called by primary service to reevaluate patient t for drainage around PEG tube. Exam: afebrile, VSS, WBC wnl soft abdomen with moderate distension, i tenderness around PEG site, drainage suspicious for stool CT abdomen/pelvis

7

8

9

10

11
12

13

14
15

16
17 Case Presentation - Hospital course 7/19: exploratory laparotomy via small midline incision Findings: fully dislodged PEG tube, two holes in transverse colon adherent to anterior wall of stomach, with associated defect. Minimal stool spillage 6 cm transverse colon resected with primary anastamosis. Anterior stomach defect repair with new gastrostomy tube (20Fr foley) placed
18 Case presentation Hospital course 7/21 started on tube feeds, well tolerated 7/25 discharged home
19 Prevention and Management of Complications of PEG Tubes
 US Army surgeon, author of")
 Based on the management of traumatic percutaneous")
20 Historical Perspective Dr. William Beaumont ( ) US Army surgeon, author of Experiments and Observations in Gastric Juice and Physiology of Digestion (1833) Based on the management of traumatic percutaneous gastrostomy of finjured dfur catcher Alexis St. Martin
21 Historical Perspective 1837 Norwegian surgeon Christian A. Egeberg initially described a surgical gastrostomy 1876 first successful gastrostomy done by Aristide Verneuil in France









22 Historical Perspective Open gastrostomy modified over time via the Stamm, Witzel, and Janeway techniques Morbidity and mortality rates of gastrostomy by laparotomy vary from 3% to 60%
23 Historical Perspective, cont d Drs. Michael Gauderer and Jeffrey Ponsky at the University Hospital of Cleveland described the first PEG intended for use in children 150 cases, no deaths, 10% minor complications easily treated J Pediatric Surg 1980; 15: Archives of Surgery 1983;118:
24 Historical Prespective, cont d. 1981: Canadian Preshaw described radiological approach of inserting gastrostomy tube via fluoroscopic guidance 1990s: laparoscopic approach


25 Epidemiology Over 200,000 PEG tubes are placed annually Up to 10% of nursing home residents and as many as 1.7% of Medicare patients over 85
26 Methods Comparison Measure Surgical Gastrostomy PEG PRG # of pts # of series Success rate 100% 95.7% 99.2% Procedural Mortality rate 2.5% 0.5% 0.3% Major complication i rate 199% 19.9% 94% 9.4% 59% 5.9% Minor complication rate 9% 5.9% 7.8%
27 Costs Comparison Procedure Surgical $ Endoscopic $ Radiologic$ i Gastrostomy Gastrojejunostomy Barkmeier JM, et al Cardiovasc. Intervent Radiol 1998 Jul-Aug; 21 (4) 324-8
28 Rt Retrospective ti Analysis 82 patients : 14 surgical, 24 PEG, 44 PRG Surgical PEG PRG Mortality Rate 0/14 0/24 1/44 Major complication i 2 (14%) 4 (17%) 5 (11%) Minor complication 6 (43%) 8 (33%) 16 (36%) Function at 1 year 67% 68% 58% Archives of Surgery Vol 133 No.10 October 1998
29 Indications Long term feeding: the American Gastroenterological Association endorses PEG tube placement for prolonged tube feeding (>30days). Replaces nasoenteric tube with decreased risk of aspiration, sinusitis Mechanical dysfunction near esophageal obstruction swallowing disorderd facial fractures
30 Indications Neurologic Impairment: stroke, closed head injury Permit transfer to long term facility Decompressive tube for palliation Gastric volvulus
31 Contraindications Terminal illness (except palliation) Inability to perform upper endoscopy obstructing esophageal tumor, stricture Ascites Inability to appose gastrostomy to anterior abdominal wall: previous subtotal gastrectomy, hepatomegaly
32 Relative Contraindications Coagulopathy Portal hypertension Peritoneal dialysis Large hiatal hernia
33 PEG Techniques The pull (Ponsky-Gauderer) technique vs the push (Sacks-Vine) technique No outcome difference Pull technique used more frequently Push technique used in radiologic and laparoscopic tube placement
34 Pull Technique Guide wire is placed in stomach Guide wire is brought retrograde through the patient s mouth PEG tube is pulled through abdominal wall
35





36
37
38
39
40
41
42





43 Push Technique PEG tube advanced via modified Seldinger approach May involve dilators, peel away introducer
44 Major Complications Complication Frequency enc Aspiration up to 1.0% Hemorrhage 2.5% Peritonitis 1.3% Necrotizing fasciitis rare Death up to 2.1% Tumor implantation rare Gastroenterology 1987:93:48-52 Am. Surg, 2002;68: Practical Gastroenterology November 2004
45 Minor Complications Complication Frequency enc Ileus 1% - 2% Peristomal infection up to 30% Stomal leakage 1% - 2% Buried bumper 2.4% Gastric ulcer 1.2% Fistulous tracts up to 6.7% Inadvertent removal 1.6% - 4.4% Gastroenterology 1987;93;48-52 Gastrointest Endosc, 2002;56: Endoscopy, 2001;33:


46 Perforation of Viscera/Peritonitis Occurs in 0.5%-1.3% 13% of cases Abdominal pain, leukocytosis, ileus, fever Contrast studies Broad spectrum abx and surgical exploration
47
48 Prevention Elevation of the head during placement to displace the colon inferiorly Use of an aspirating syringe filled with saline to identify intervening bowel between the skin and stomach if air bubbles appear in the syringe prior to endoscopic visualization of the needle in the gastric lumen. the safe track technique Fouch PG. Gastrointest Endosc Clin N Am, 1992;2:


49 Peristomal infection Most common complication Up to 30% with <1.6% needing aggressive debridement Increased risk in diabetics, obese, malnourished, steroids If early, oral abx Systemic signs, IV abx and local wound care
50 Buried Bumper Syndrome Partial or complete growth of gastric mucosa over the internal bumper Occurs 0.3% - 2.4% Presents as leakage, infection, immobile catheter, pain, resistance with feeds Risk factors excessive tension between bolsters, malnutrition, weight gain
51 Treatment of BBS Confirm endoscopically or radiographically Gastrograffin study with the patient prone Removal of PEG with any technique that t minimizes trauma to the PEG tract May need surgical removal
52 Practical Gastroenetrology November 2004
Geoffrey Axiak M.Sc. Nursing (Manch.), B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse
, B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse") The Percutaneous Endoscopic Gastrostomy Geoffrey Axiak M.Sc. Nursing (Manch.), B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse What is a P.E.G.? Percutaneous Endoscopic
The Percutaneous Endoscopic Gastrostomy Geoffrey Axiak M.Sc. Nursing (Manch.), B.Sc. Nursing, P.G. Dip. Nutrition & Dietetics Clinical Nutrition Practice Nurse What is a P.E.G.? Percutaneous Endoscopic
Adult Trauma Feeding Access Guideline
 Adult Trauma Feeding Access Guideline Background: Enteral feeding access mode (NGT, NDT, PEG, PEG-J, Jejunostomy tube) dependent upon patient characteristics. Enteral feeding management guidelines aim
Adult Trauma Feeding Access Guideline Background: Enteral feeding access mode (NGT, NDT, PEG, PEG-J, Jejunostomy tube) dependent upon patient characteristics. Enteral feeding management guidelines aim
MIC-KEY * Introducer Kits THE EFFICIENT CLINICAL SOLUTION FOR ENTERAL FEEDING
 MIC-KEY * Introducer Kits THE EFFICIENT CLINICAL SOLUTION FOR ENTERAL FEEDING MIC-KEY * INTRODUCER KIT THE E INTUITIVE TOOLS FOR AN EASE OF USE One convenient kit allows the placement of the broad range
MIC-KEY * Introducer Kits THE EFFICIENT CLINICAL SOLUTION FOR ENTERAL FEEDING MIC-KEY * INTRODUCER KIT THE E INTUITIVE TOOLS FOR AN EASE OF USE One convenient kit allows the placement of the broad range
Ponsky * PEG Safety System - "Pull" Bard * PEG Safety System - "Guidewire" Information for Use
 Ponsky * PEG Safety System - "Pull" Bard * PEG Safety System - "Guidewire" Information for Use Rx only Single patient use DEHP-Free This product and package do not contain natural rubber latex STERILE
Ponsky * PEG Safety System - "Pull" Bard * PEG Safety System - "Guidewire" Information for Use Rx only Single patient use DEHP-Free This product and package do not contain natural rubber latex STERILE
BURIED BUMPER SYNDROME: A RARE COMPLICATION OF PERCUTANEOUS ENDOSCOPIC GASTROSTOMY
 BURIED BUMPER SYNDROME: A RARE COMPLICATION OF PERCUTANEOUS ENDOSCOPIC GASTROSTOMY Farhan Khan, Tan Xiao Ping* and Umesh Guragain Department of Gastroenterology, The Affiliated Hospital of Yangtze Medical
BURIED BUMPER SYNDROME: A RARE COMPLICATION OF PERCUTANEOUS ENDOSCOPIC GASTROSTOMY Farhan Khan, Tan Xiao Ping* and Umesh Guragain Department of Gastroenterology, The Affiliated Hospital of Yangtze Medical
Buried bumper syndrome: where did that PEG tube go?!
 Buried bumper syndrome: where did that PEG tube go?! Poster No.: C-3158 Congress: ECR 2018 Type: Educational Exhibit Authors: I. Kavelj, N. BABIC, G. Lovrencic-Prpic, D. Zadravec; Zagreb/HR Keywords: Swallowing
Buried bumper syndrome: where did that PEG tube go?! Poster No.: C-3158 Congress: ECR 2018 Type: Educational Exhibit Authors: I. Kavelj, N. BABIC, G. Lovrencic-Prpic, D. Zadravec; Zagreb/HR Keywords: Swallowing
Enteral Feeding Access: Your BFF or Frenemy?
 Enteral Feeding Access: Your BFF or Frenemy? Elizabeth Hood, APN/CPNP The Ann and Robert H. Lurie Children s Hospital of Chicago Chicago, IL Disclosure Information No disclosures to report Objectives The
Enteral Feeding Access: Your BFF or Frenemy? Elizabeth Hood, APN/CPNP The Ann and Robert H. Lurie Children s Hospital of Chicago Chicago, IL Disclosure Information No disclosures to report Objectives The
Percutaneous Endoscopic Gastrostomies (PEGs)
") Percutaneous Endoscopic Gastrostomies (PEGs) Robin B. Mendelsohn, MD Clinical Director, Gastroenterology, Hepatology and Nutrition Service Memorial Sloan Kettering Cancer Center Goals of today Understand
Percutaneous Endoscopic Gastrostomies (PEGs) Robin B. Mendelsohn, MD Clinical Director, Gastroenterology, Hepatology and Nutrition Service Memorial Sloan Kettering Cancer Center Goals of today Understand
Gastrostomy ( PEG ) tubes and the ED
 tubes and the ED") Gastrostomy ( PEG ) tubes and the ED Percutaneous endoscopic gastrostomy (PEG) and radiology-inserted gastrostomy (RIG) have become the modality of choice for providing enteral access to patients who require
Gastrostomy ( PEG ) tubes and the ED Percutaneous endoscopic gastrostomy (PEG) and radiology-inserted gastrostomy (RIG) have become the modality of choice for providing enteral access to patients who require
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Initial placement 24FR Pull PEG kit REORDER NO:
 Initial placement 24FR Pull PEG kit REORDER NO: 00710805 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 24FR Pull PEG kit is
Initial placement 24FR Pull PEG kit REORDER NO: 00710805 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 24FR Pull PEG kit is
Having a PEG tube inserted
 Having a PEG tube inserted This information leaflet is for patients who are having a PEG (Percutaneous Endoscopic Gastrostomy) tube inserted. It explains what is involved, what to expect and what significant
Having a PEG tube inserted This information leaflet is for patients who are having a PEG (Percutaneous Endoscopic Gastrostomy) tube inserted. It explains what is involved, what to expect and what significant
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Initial placement 20FR Guidewire PEG kit REORDER NO:
 Initial placement 20FR Guidewire PEG kit REORDER NO: 00710802 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 20FR Guidewire
Initial placement 20FR Guidewire PEG kit REORDER NO: 00710802 INSTRUCTIONS FOR USE 1 of 5 These products have been manufactured not to include latex. Intended Use: The Initial placement 20FR Guidewire
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Pediatric ER Half-day Rounds October 12, 2011 Dr. Karen Bailey
 Pediatric ER Half-day Rounds October 12, 2011 Dr. Karen Bailey Objectives to identify various enteral and vascular access lines what do they look like? indications & contraindications proper placement
Pediatric ER Half-day Rounds October 12, 2011 Dr. Karen Bailey Objectives to identify various enteral and vascular access lines what do they look like? indications & contraindications proper placement
Radiologic, Endoscopic or Surgical Gastrostomy: Complementary or Competing techniques?
 Radiologic, Endoscopic or Surgical Gastrostomy: Complementary or Competing techniques? Poster No.: C-0438 Congress: ECR 2013 Type: Educational Exhibit Authors: M. Leyva Vásquez-Caicedo, C. García Villafañe,
Radiologic, Endoscopic or Surgical Gastrostomy: Complementary or Competing techniques? Poster No.: C-0438 Congress: ECR 2013 Type: Educational Exhibit Authors: M. Leyva Vásquez-Caicedo, C. García Villafañe,
Early View Article: Online published version of an accepted article before publication in the final form.
 : Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: Surgical approach
: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title: Surgical approach
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
You ll Need a Tube to Get There!
 You ll Need a Tube to Get There! Ryan T. Hurt, MD,PhD Associate Professor of Medicine Divisions of General Internal Medicine, Gastroenterology, and Endocrinology Director Home Parenteral Enteral Nutrition
You ll Need a Tube to Get There! Ryan T. Hurt, MD,PhD Associate Professor of Medicine Divisions of General Internal Medicine, Gastroenterology, and Endocrinology Director Home Parenteral Enteral Nutrition
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Laparoscopic or Endoscopic Gastrostomy in Children: Comparison of Two Methods. H. STEYAERT, L. CARFAGNA, M.A. LEMBO, E. TREVINO, and J.S.
 Pediatric Endosurgery & Innovative Techniques Volume 7, Number 2, 2003 Mary Ann Liebert, Inc. Laparoscopic or Endoscopic Gastrostomy in Children: Comparison of Two Methods H. STEYAERT, L. CARFAGNA, M.A.
Pediatric Endosurgery & Innovative Techniques Volume 7, Number 2, 2003 Mary Ann Liebert, Inc. Laparoscopic or Endoscopic Gastrostomy in Children: Comparison of Two Methods H. STEYAERT, L. CARFAGNA, M.A.
PEDIATRIC GASTROSTOMY TUBES: The Ins and Outs
 PEDIATRIC GASTROSTOMY TUBES: The Ins and Outs Jenifer Reitsma, MSN, RN, CPNP Pediatric Nurse Practitioner Pediatric Surgery & Trauma Sanford Children s Hospital I have no disclosures Objectives Learner
PEDIATRIC GASTROSTOMY TUBES: The Ins and Outs Jenifer Reitsma, MSN, RN, CPNP Pediatric Nurse Practitioner Pediatric Surgery & Trauma Sanford Children s Hospital I have no disclosures Objectives Learner
DEPARTMENT OF SURGERY DELINEATION OF PRIVILEGES FOR GENERAL SURGERY
 DEPARTMENT OF SURGERY DELINEATION OF PRIVILEGES FOR GENERAL SURGERY NAME: DATE: Please check the box for each privilege requested. Applicants have the burden of producing information deemed adequate by
DEPARTMENT OF SURGERY DELINEATION OF PRIVILEGES FOR GENERAL SURGERY NAME: DATE: Please check the box for each privilege requested. Applicants have the burden of producing information deemed adequate by
The Percutaneous Endoscopic Gastrostomy. Geoffrey Axiak Clinical Nutrition Nurse St. Luke s Hospital
 The Percutaneous Endoscopic Gastrostomy Geoffrey Axiak Clinical Nutrition Nurse St. Luke s Hospital What is a P.E.G.? Percutaneous Endoscopic Gastrostomy Indications for P.E.G. Insertion In cases of long-term
The Percutaneous Endoscopic Gastrostomy Geoffrey Axiak Clinical Nutrition Nurse St. Luke s Hospital What is a P.E.G.? Percutaneous Endoscopic Gastrostomy Indications for P.E.G. Insertion In cases of long-term
Cpt code percutaneous endoscopic gastrostomy tube removal
 РџРѕРёСЃРє... РќР Р С Рё Cpt code percutaneous endoscopic gastrostomy tube removal < Code 43870: Closure of gastrostomy, surgical. Note: There MUST be stitches placed with a surgical closure to use this
РџРѕРёСЃРє... РќР Р С Рё Cpt code percutaneous endoscopic gastrostomy tube removal < Code 43870: Closure of gastrostomy, surgical. Note: There MUST be stitches placed with a surgical closure to use this
CIRSE Standards of Practice Guidelines on Gastrostomy
 Cardiovasc Intervent Radiol (2016) 39:973 987 DOI 10.1007/s00270-016-1344-z CIRSE STANDARDS OF PRACTICE GUIDELINES CIRSE Standards of Practice Guidelines on Gastrostomy James Sutcliffe 1 Andrew Wigham
Cardiovasc Intervent Radiol (2016) 39:973 987 DOI 10.1007/s00270-016-1344-z CIRSE STANDARDS OF PRACTICE GUIDELINES CIRSE Standards of Practice Guidelines on Gastrostomy James Sutcliffe 1 Andrew Wigham
Placing PEG and Jejunostomy Tubes in Dogs and Cats
 Placing PEG and Jejunostomy Tubes in Dogs and Cats I. Gastrostomy tube A. Percutaneous Endoscopic Gastrostomy (PEG) tube placement Supplies for PEG tube placement: Supplies and equipment for general anesthesia
Placing PEG and Jejunostomy Tubes in Dogs and Cats I. Gastrostomy tube A. Percutaneous Endoscopic Gastrostomy (PEG) tube placement Supplies for PEG tube placement: Supplies and equipment for general anesthesia
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
DON T LET OBESITY SPOIL YOUR HEALTH AND YOUR LIFE
 July 2015 Issue No.17 DON T LET OBESITY SPOIL YOUR HEALTH AND YOUR LIFE www.sghgroup.com JEDDAH RIYADH MEDINA ASEER HAIL SANAA DUBAI CAIRO Definitions Over View and General Facts General Key facts! Worldwide
July 2015 Issue No.17 DON T LET OBESITY SPOIL YOUR HEALTH AND YOUR LIFE www.sghgroup.com JEDDAH RIYADH MEDINA ASEER HAIL SANAA DUBAI CAIRO Definitions Over View and General Facts General Key facts! Worldwide
Owen Dickinson. Consultant in Endoscopy & Interventional Radiology. Upper GI Stenting. Rotherham Foundation Trust
 Owen Dickinson Consultant in Endoscopy & Interventional Radiology Upper GI Stenting Rotherham Foundation Trust Owen Dickinson Consultant in Endoscopy & Interventional Radiology Rotherham Foundation Trust
Owen Dickinson Consultant in Endoscopy & Interventional Radiology Upper GI Stenting Rotherham Foundation Trust Owen Dickinson Consultant in Endoscopy & Interventional Radiology Rotherham Foundation Trust
Coding Companion for Emergency Medicine. A comprehensive illustrated guide to coding and reimbursement
 Coding Companion for Emergency Medicine A comprehensive illustrated guide to coding and reimbursement 2009 Contents Getting Started with Coding Companion... i Skin/Incision...1 Debridement...7 Excision...12
Coding Companion for Emergency Medicine A comprehensive illustrated guide to coding and reimbursement 2009 Contents Getting Started with Coding Companion... i Skin/Incision...1 Debridement...7 Excision...12
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
INNOVATIVE PRODUCTS G, J AND GJ-TUBES WITH ENFit TM CONNECTION
 MIC * & MIC-KEY * Enterostomy Tubes INNOVATIVE PRODUCTS G, J AND GJ-TUBES WITH ENFit TM CONNECTION DIGESTIVE HEALTH PRODUCT CATALOGUE INNOVATIVE PRODUCTS - G, J AND GJ-TUBES WITH ENFit TM CONNECTION DIGESTIVE
MIC * & MIC-KEY * Enterostomy Tubes INNOVATIVE PRODUCTS G, J AND GJ-TUBES WITH ENFit TM CONNECTION DIGESTIVE HEALTH PRODUCT CATALOGUE INNOVATIVE PRODUCTS - G, J AND GJ-TUBES WITH ENFit TM CONNECTION DIGESTIVE
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM
 Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM") ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Laparoscopic Witzel gastrostomy a reappraised technique
 Surg Endosc (2007) 21: 793 797 DOI: 10.1007/s00464-006-9018-6 Ó Springer Science+Business Media, Inc. 2006 Laparoscopic Witzel gastrostomy a reappraised technique J.-S. Hsieh, C.-F. Wu, F.-M. Chen, J.-Y.
Surg Endosc (2007) 21: 793 797 DOI: 10.1007/s00464-006-9018-6 Ó Springer Science+Business Media, Inc. 2006 Laparoscopic Witzel gastrostomy a reappraised technique J.-S. Hsieh, C.-F. Wu, F.-M. Chen, J.-Y.
Imaging of gastric bands and their complications: an educational pictorial review
 Imaging of gastric bands and their complications: an educational pictorial review Poster No.: C-1142 Congress: ECR 2014 Type: Educational Exhibit Authors: F. Moloney, M. Twomey, C. Bogue ; Cork/IE, IE,
Imaging of gastric bands and their complications: an educational pictorial review Poster No.: C-1142 Congress: ECR 2014 Type: Educational Exhibit Authors: F. Moloney, M. Twomey, C. Bogue ; Cork/IE, IE,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Home enteral feeding
 Home enteral feeding Item Type Article Authors Corrigan, Grainne Publisher Nursing in General Practice Journal Nursing in General Practice Download date 01/09/2018 00:39:10 Link to Item http://hdl.handle.net/10147/578880
Home enteral feeding Item Type Article Authors Corrigan, Grainne Publisher Nursing in General Practice Journal Nursing in General Practice Download date 01/09/2018 00:39:10 Link to Item http://hdl.handle.net/10147/578880
WallFlex Stents Technique Spotlights
 WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
Case discussion. Anastomotic leakage. intern superviser
 Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Case discussion Anastomotic leakage intern superviser Basic data Name : XX ID: M101881671 Age:51 Y Gender: male Past history: Hospitalized for acute diverticulitis on 2004/7/17, 2005/5/28 controlled by
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Case Presentation: Mr. S
 Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Case Presentation: Mr. S History Seen as inpatient in May, but has significant prior history and is a poor historian 53 y.o. Male no PMH, has been out of contact with medicine for years aside from hernia
Surgical jejunostomy, DEPJ or PEGJ
 Surgical jejunostomy, DEPJ or PEGJ Dr Simon Gabe St Mark s Hospital, London Jejunal feeding NJ PEGJ Surgical jejunostomy Direct PEJ Surgical jejunostomy Different tubes PEGJ Which one? Local expertise
Surgical jejunostomy, DEPJ or PEGJ Dr Simon Gabe St Mark s Hospital, London Jejunal feeding NJ PEGJ Surgical jejunostomy Direct PEJ Surgical jejunostomy Different tubes PEGJ Which one? Local expertise
Jejunostomy after oesophagectomy, how and why I do it
 Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference 2010 2nd & 3rd November Harrogate International
Jejunostomy after oesophagectomy, how and why I do it Graeme Couper. Consultant Oesophago-gastric Surgeon, The Royal Infirmary of Edinburgh BAPEN Conference 2010 2nd & 3rd November Harrogate International
A-Tube Instructions for Use
 a s s i s t A-Tube Instructions for Use Caution: US Federal law restricts this device to sale on or by the order of a physician. IFU-029 Rev. B (06/2016) Rx Only Aspire Bariatrics, Inc. 2016 TABLE OF CONTENTS
a s s i s t A-Tube Instructions for Use Caution: US Federal law restricts this device to sale on or by the order of a physician. IFU-029 Rev. B (06/2016) Rx Only Aspire Bariatrics, Inc. 2016 TABLE OF CONTENTS
Diagnostic imaging and minimally invasive interventions
 Diagnostic imaging and minimally invasive interventions 2018 Old and new Different questions to be answered, new tasks Specific, focused examinationsfókuszált, specifikus vizsgálatok Ionic radiation Cost/benefit
Diagnostic imaging and minimally invasive interventions 2018 Old and new Different questions to be answered, new tasks Specific, focused examinationsfókuszált, specifikus vizsgálatok Ionic radiation Cost/benefit
Types of peritonitis and management. J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016
 Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016 Case Presentation xx year old patient presents to ED with complaints of one day of abdominal pain s ince
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Percutaneous Cecostomy Tube Placement
 Information About Your Child s Procedure Percutaneous Cecostomy Tube Placement Read this form so you understand the procedure and its risks. Please ask questions about anything you do not understand. What
Information About Your Child s Procedure Percutaneous Cecostomy Tube Placement Read this form so you understand the procedure and its risks. Please ask questions about anything you do not understand. What
Itemized Billing and Procedure Description for the AspireAssist
 Itemized Billing and Procedure Description for the AspireAssist The following describes the recommended therapy course for the first year for a patient undergoing AspireAssist therapy. Although providers
Itemized Billing and Procedure Description for the AspireAssist The following describes the recommended therapy course for the first year for a patient undergoing AspireAssist therapy. Although providers
Not over when the surgery is done: surgical complications of obesity
 Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Case Presentation Surgery Grand Round. Amid Keshavarzi, MD UCHSC 4/9/2006
 Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
The following slides are from a. presentation given by. H. Worth Boyce, M.D. on. Specialized Studies on Diseases of the Esophagus.
 The following slides are from a presentation given by H. Worth Boyce, M.D. on Endoscopic Lumen Restoration at the 8 th OESO World Organization for Specialized Studies on Diseases of the Esophagus. Endoscopic
The following slides are from a presentation given by H. Worth Boyce, M.D. on Endoscopic Lumen Restoration at the 8 th OESO World Organization for Specialized Studies on Diseases of the Esophagus. Endoscopic
General Surgery Getting to the Core. Disclaimer
 General Surgery Getting to the Core AAPC Regional Conference Nashville, Tennessee September 2011 1 Disclaimer The information in this presentation was current at the time the presentation was complied
General Surgery Getting to the Core AAPC Regional Conference Nashville, Tennessee September 2011 1 Disclaimer The information in this presentation was current at the time the presentation was complied
Septic Phlebitis and Gas in the Inferior Mesenteric Vein: CT findings in Two Cases and Review of Literature
 ISPUB.COM The Internet Journal of Surgery Volume 16 Number 2 Septic Phlebitis and Gas in the Inferior Mesenteric Vein: CT findings in Two Cases and Review of J McClenathan Citation J McClenathan. Septic
ISPUB.COM The Internet Journal of Surgery Volume 16 Number 2 Septic Phlebitis and Gas in the Inferior Mesenteric Vein: CT findings in Two Cases and Review of J McClenathan Citation J McClenathan. Septic
Single Center Experience with Gastrostomy Insertion in Pediatric Patients: A 10-Year Review
 pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2017.20.1.34 Pediatr Gastroenterol Hepatol Nutr 2017 March 20(1):34-40 Original Article PGHN Single Center Experience with Gastrostomy Insertion
pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2017.20.1.34 Pediatr Gastroenterol Hepatol Nutr 2017 March 20(1):34-40 Original Article PGHN Single Center Experience with Gastrostomy Insertion
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Caustic Esophageal Injury. Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013
 Caustic Esophageal Injury Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013 Case presentation 3F with no PMH presented to outside facility after drinking unmarked bottle containing oven cleaner
Caustic Esophageal Injury Aliu Sanni, MD SUNY Downstate Medical Center March 21, 2013 Case presentation 3F with no PMH presented to outside facility after drinking unmarked bottle containing oven cleaner
Approach to Oral and Enteral Nutrition (PN) in Adults
 in Adults") Approach to Oral and Enteral Nutrition (PN) in Adults Module 8.3 Topic 8 Techniques of Enteral Nutrition Johann Ockenga Learning Objectives To know about the different types of tubes and access routes;
Approach to Oral and Enteral Nutrition (PN) in Adults Module 8.3 Topic 8 Techniques of Enteral Nutrition Johann Ockenga Learning Objectives To know about the different types of tubes and access routes;
Aspira* Peritoneal Drainage Catheter
 Aspira* Peritoneal Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Peritoneal Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid
Aspira* Peritoneal Drainage Catheter Instructions For Use Access Systems Product Description: The Aspira* Peritoneal Drainage Catheter is a tunneled, long-term catheter used to drain accumulated fluid
Gastrostomy Tube Replacement Using Foley s Catheters in Children
 Gastrostomy Tube Replacement Using Foley s Catheters in Children Siriphut Kiatipunsodsai MD* * Pediatric Surgery Unit, Department of Surgery, Faculty of Medicine, Thammasat University, Pathumthani, Thailand
Gastrostomy Tube Replacement Using Foley s Catheters in Children Siriphut Kiatipunsodsai MD* * Pediatric Surgery Unit, Department of Surgery, Faculty of Medicine, Thammasat University, Pathumthani, Thailand
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Swallowing, nutrition and PEG feeding: deciding, doing and managing
 Swallowing, nutrition and PEG feeding: deciding, doing and managing Swallowing in MND Dysphagia disruption in the swallowing process In MND can be variable depending on type Bulbar MND - faster progression
Swallowing, nutrition and PEG feeding: deciding, doing and managing Swallowing in MND Dysphagia disruption in the swallowing process In MND can be variable depending on type Bulbar MND - faster progression
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
University of Maryland Medical Center - Shock Trauma Center Delineation of Clinical Privileges Section of Trauma and Acute Emergency Surgery
 University of Maryland Medical Center - Shock Trauma Center Delineation of Clinical Section of Trauma and Acute Emergency Surgery Type of Request: Initial Renewal Name: /Operative Procedures INTEGUMENTARY/BREAST
University of Maryland Medical Center - Shock Trauma Center Delineation of Clinical Section of Trauma and Acute Emergency Surgery Type of Request: Initial Renewal Name: /Operative Procedures INTEGUMENTARY/BREAST
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus
 Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Emergency Surgery Board Department of General Surgery Rambam Health Care Campus Surgical Complications of Peptic Ulcer Disease Case Presentation and Review of the Literature Case Presentation 40y male
Ventriculoperitoneal Shunt with Communicating Peritoneal & Subcutaneous Pseudocysts Formation
 International Journal of Health Sciences, Qassim University, Vol. 8, No. 1 (January-March 2014) Case Report Ventriculoperitoneal Shunt with Communicating Peritoneal & Subcutaneous Pseudocysts Formation
International Journal of Health Sciences, Qassim University, Vol. 8, No. 1 (January-March 2014) Case Report Ventriculoperitoneal Shunt with Communicating Peritoneal & Subcutaneous Pseudocysts Formation
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Gallstone ileus:diagnostic and therapeutic dilemma
 Saurabh et al. 1 CASE SERIES OPEN ACCESS Gallstone ileus:diagnostic and therapeutic dilemma Shireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky ABSTRACT Introduction: Gallstone ileus is a rare complication
Saurabh et al. 1 CASE SERIES OPEN ACCESS Gallstone ileus:diagnostic and therapeutic dilemma Shireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky ABSTRACT Introduction: Gallstone ileus is a rare complication
Acquired pediatric esophageal diseases Imaging approaches and findings. M. Mearadji International Foundation for Pediatric Imaging Aid
 Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Acquired pediatric esophageal diseases Imaging approaches and findings M. Mearadji International Foundation for Pediatric Imaging Aid Acquired pediatric esophageal diseases The clinical signs of acquired
Initial experience with percutaneous endoscopic gastrostomy with T-fastener fixation in pediatric patients
 Initial experience with percutaneous endoscopic gastrostomy with T-fastener fixation in pediatric patients Authors Morten Kvello 1, 2, Charlotte Kristensen Knatten 3, Gøri Perminow 3,HansSkari 2, Anders
Initial experience with percutaneous endoscopic gastrostomy with T-fastener fixation in pediatric patients Authors Morten Kvello 1, 2, Charlotte Kristensen Knatten 3, Gøri Perminow 3,HansSkari 2, Anders
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title:
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Interventional Radiology for Improved Outcomes in the Neonatal Period
 Interventional Radiology for Improved Outcomes in the Neonatal Period Mark J. Hogan, MD Nationwide Children s Hospital The Ohio State University mark.hogan@nationwidechildrens.org No financial disclosures
Interventional Radiology for Improved Outcomes in the Neonatal Period Mark J. Hogan, MD Nationwide Children s Hospital The Ohio State University mark.hogan@nationwidechildrens.org No financial disclosures
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
E Boldo, G Perez de Lucia, J Aracil, F Martin, D Martinez, J Miralles, A Armelles
 ISPUB.COM The Internet Journal of Gastroenterology Volume 5 Number 1 E Boldo, G Perez de Lucia, J Aracil, F Martin, D Martinez, J Miralles, A Armelles Citation E Boldo, G Perez de Lucia, J Aracil, F Martin,
ISPUB.COM The Internet Journal of Gastroenterology Volume 5 Number 1 E Boldo, G Perez de Lucia, J Aracil, F Martin, D Martinez, J Miralles, A Armelles Citation E Boldo, G Perez de Lucia, J Aracil, F Martin,
Iatrogenic Duodenal Injuries. Downstate Medical Center July 25 th, 2013 David Vivas, MD
 Iatrogenic Duodenal Injuries Downstate Medical Center July 25 th, 2013 David Vivas, MD History Case 71 y/o female who was seen by her PMD c/o 2 h/o RUQ pain radiated to the back. Patient denied fevers,
Iatrogenic Duodenal Injuries Downstate Medical Center July 25 th, 2013 David Vivas, MD History Case 71 y/o female who was seen by her PMD c/o 2 h/o RUQ pain radiated to the back. Patient denied fevers,
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
CASE REPORTS. Giant Esophagus. An Unusual Case of Massive Idiopathic Hypertrophy
 CASE REPORTS An Unusual Case of Massive Idiopathic Hypertrophy and Dilatation of the Esophagus and Proximal Stomach Mark H. Wall, M.D., Epifanio E. Espinas, M.D., Arthur W. Silver, M.D., and Francis X.
CASE REPORTS An Unusual Case of Massive Idiopathic Hypertrophy and Dilatation of the Esophagus and Proximal Stomach Mark H. Wall, M.D., Epifanio E. Espinas, M.D., Arthur W. Silver, M.D., and Francis X.
Primary placement technique of jejunostomy using the entristar skin-level gastrostomy tube in patients with esophageal cancer
 TECHNICAL ADVANCE Open Access Primary placement technique of jejunostomy using the entristar skin-level gastrostomy tube in patients with esophageal cancer Yasushi Rino 1*, Norio Yukawa 1, Hitoshi Murakami
TECHNICAL ADVANCE Open Access Primary placement technique of jejunostomy using the entristar skin-level gastrostomy tube in patients with esophageal cancer Yasushi Rino 1*, Norio Yukawa 1, Hitoshi Murakami
Chapter 29 Gastrointestinal Intubation
 Chapter 29 Gastrointestinal Intubation Intubation Intubation: placement of a tube into a body structure Types of intubation Orogastric: mouth to stomach Nasogastric: nose to stomach Nasointestinal: nose
Chapter 29 Gastrointestinal Intubation Intubation Intubation: placement of a tube into a body structure Types of intubation Orogastric: mouth to stomach Nasogastric: nose to stomach Nasointestinal: nose
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
for the ideal insertion of peritoneal dialysis catheter (patent pending)
") for the ideal insertion of peritoneal dialysis catheter (patent pending) CAUTION: U.S. federal law restricts this device to sale by or on the order of a properly licensed practitioner. DEVICE DESCRIPTION
for the ideal insertion of peritoneal dialysis catheter (patent pending) CAUTION: U.S. federal law restricts this device to sale by or on the order of a properly licensed practitioner. DEVICE DESCRIPTION
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Information Technology Solutions
 2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
Persistence of a Gastrocutaneous Fistula after gastrostomy removal in children: Incidence and predictive factors
 Persistence of a Gastrocutaneous Fistula after gastrostomy removal in children: Incidence and predictive factors by Anne-Sophie MASSY et Olivier REINBERG* Department of Pediatric Surgery, University Hospital
Persistence of a Gastrocutaneous Fistula after gastrostomy removal in children: Incidence and predictive factors by Anne-Sophie MASSY et Olivier REINBERG* Department of Pediatric Surgery, University Hospital
Gastrostomy Tube Placement Outcomes in Children: Comparison of Open and Laparoscopic Methods
 Research Article imedpub Journals http://www.imedpub.com Journal of Universal Surgery DOI: 10.21767/2254-6758.100082 Abstract Gastrostomy Tube Placement Outcomes in Children: Comparison of Open and Laparoscopic
Research Article imedpub Journals http://www.imedpub.com Journal of Universal Surgery DOI: 10.21767/2254-6758.100082 Abstract Gastrostomy Tube Placement Outcomes in Children: Comparison of Open and Laparoscopic