Assessment and Treatment of Chronic, Non-malignant Pain. Jill Chaplin, MD
|
|
|
- Quentin Sherman Payne
- 6 years ago
- Views:
Transcription
1 Assessment and Treatment of Chronic, Non-malignant Pain Jill Chaplin, MD
2 I have nothing to disclose I work for Peace Health Medical Group, and will share some of our processes, but have no commercial interest
3 Goals of this presentation Brief overview of chronic pain as a clinical problem Review standard of care for evaluation and treatment of chronic pain Review examples of tools and processes that make this care easier and safer To increase the safety of our patients and communities, the standardization to best practice and the professional satisfaction of our provider colleagues
4 Chronic Pain: Definition Pain: An unpleasant sensory and emotional experience associated with actual, or potential, tissue damage. Acute = 6 weeks; Subacute = 6-12 weeks Chronic = beyond normal tissue healing- about 3 months
5 Chronic Pain: How bad is it?
6 Chronic Pain: incidence and impact U.S. population: 37% with chronic pain - Comparison: Diabetes = 8% - American adults: 20% report pain disrupting sleep - Cost: $560 billion to $635 billion/ year, US (care + disability + lost wages & productivity) Those with chronic pain: 59% - reduced enjoyment of life. 77% - depressed
7 Chronic Pain Treatment Challenges Biggest dis-satisfier of clinicians and staff Providers reluctant to accept pain patients, reducing access for the underserved Majority of Americans feel, pain should be a high, or top, medical priority Prescription drugs= second-most abused in the US, after marijuana. Nearly half of all drug deaths are from prescription pain relievers
8 Chronic pain: What causes it?
9 . What we know:
10 Chronic Pain: Top Diagnoses National Health and Nutrition Examination Survey,(NHANES) 1999 to 2002 : Low back pain: 10%- Leading cause of disability, Americans < age 45 Chronic Regional Pain 11.1% Leg/foot pain 7.1% Arm/hand pain 4.1% Severe headache or migraine: 3.5% - most common pain causing lost productive time
11 . Fibromyalgia: 2% of US population Majority of patients with chronic pain have more than one type of pain
12 Types of pain: Neuropathic pain peripheral, eg post-herpetic neuralgia, diabetic neuropathy; vs central, eg post-stroke pain or multiple sclerosis Musculoskeletal pain eg, back pain, myofascial pain syndrome, ankle pain
13 Types of pain: Inflammatory pain eg, inflammatory arthropathies, infection Mechanical/compressive pain eg, renal calculi, visceral pain from expanding tumor masses Note: these are not mutually exclusive eg back pain might be both musculoskeletal and mechanical/compressive, (nerve root compression)
14 Chronic Pain- What we suspect: Neuroplasticity
15 Neuroplasticity and chronic pain..increased sensibility of the spinal cord upon severe, long lasting pain perception, a mechanism called windup. Hyperalgesia is accompanied by persisting genetic changes of spinal cord cells, which may contribute to the chronification of pain. The severity and duration of acute pain apparently contributes to the possibility of chronic pain development. Klinik für Anästhesie, Intensivmedizin und Schmerztherapie Klinikum Kemperhof, Koblenz. Anasthesiologie, Intensivmedizin, Notfallmedizin, Schmerztherapie : AINS [2000, 35(5): ] 2000/06 Type: Journal Article, Review, English Abstract (lang: ger) DOI: /s
16 Contribution of central neuroplasticity to pathological pain: review of clinical and experimental evidence: changes in central neural function may play a significant role. noxious stimuli may sensitize central neural structures involved in pain perception.. in addition to a contribution of neuronal hyperactivity to pathological pain, there are specific cellular and molecular changes that affect membrane excitability and induce new gene expression. Terence J. Coderre a,b,c, Joel Katz d,e, Anthony L. Vaccarino c,* and Ronald Melzack
17 Mental vs Physical Pain- A broken Heart and a Broken Leg- Much the Same to our Brains the neural circuits important for emotional distress feelings of social isolation, grief, jealousy, and shame have much in common with those responsible for pain following physical injury. The overlap is strongest in those parts of the brain thought to be important in the suffering or avoidance aspect of physical pain Mary Heinricher, Ph.D. Professor, departments of Neurological Surgery and Behavioral Neuroscience OHSU Brain Institute
18 Mental and Physical Pain may be Different After All Physical pain and social rejection do activate similar regions of the brain. But by using a new analysis tool, we were able to look more closely and see that they are actually quite different. University of Colorado, Choong-Wan Woo, John M. Grohol, Psy.D. November 19, 2014
19 Opioids may cause chronic pain After adjustment for pain, function, injury severity, and other baseline covariates, receipt of opioids for more than 7 days (odds ratio = 2.2; 95% confidence interval, ) and receipt of more than 1 opioid prescription were associated significantly with work disability at 1 year Spine, 2008
20 Relationship Between Early Opioid Prescribing for Acute Occupational Low Back Pain and Disability Duration, Medical Costs, Subsequent Surgery and Late Opioid Use After controlling for the covariates, mean disability duration, mean medical costs, and risk of surgery and late opioid use increased monotonically with increasing MEA. Those who received more than 450 mg MEA were, on average, disabled 69 days longer than those who received no early opioids. Spine: 1 September Volume 32 - Issue 19 - pp doi: /BRS.0b013e318145a731 Health Services Research
21 Opioid Tolerance and Hyperalgesia in Chronic Pain Patients After One Month of Oral Morphine Therapy: A Preliminary Prospective Study There is accumulating evidence that opioid therapy might not only be associated with the development of tolerance but also with an increased sensitivity to pain. The Journal of Pain Volume 7, Issue 1, January 2006, Pages 43 48
22 Chronic pain: How Do We Treat It?.
23 Sources for Standard of Care Private and government group guidelines Pain specialist guidelines and practices State and Federal Laws Published standards, guidelines, and resources eg ICSI Federated State Medical Board Guidelines Oregon Medical Board published statements Interagency Guideline on Opioid Dosing for Chronic Non-Cancer Pain- Washington State Agency Medical Directors Group
24 Treatment of Chronic Non-cancer Pain 1. Evaluation
25 Standard of Care for Evaluation: History History for evaluation of chronic pain includes: 1. History of the Pain: onset, duration, diagnosis, past treatments and their efficacy, past providers 2. General Medical History 3. Current Symptoms: location, quality, severity, timing of the pain; modifying factors, related symptoms 4. Function 5. Psychiatric Comorbidities 6. Narcotic Use Risk
26 Standard of Care for Evaluation: History Record Review Treatment prior to record review may be unsafe. At PHMG, decision to treat prior to record review is per provider judgment, not system policy. This may change
27 Standard of Care for Evaluation: History Drug use history: State prescription drug monitoring programs Should check at first visit; may any time thereafter Requires provider to establish an account and password Review may be delegated to staff Oregon Washington Alaska
28 Standard of Care for Evaluation: History General Medical History: Be cautious when using opioids with conditions that may potentiate opioid adverse effects (COPD, CHF, sleep apnea, Alcohol or substance abuse, elderly, renal or hepatic dysfunction.) Do not combine opioids with sedative-hypnotics, benzodiazepines, or barbiturates unless there is a specific medical or psychiatric indication for the combination.
29 Standard of Care for Evaluation: History Current Symptoms: location, quality, severity, timing, modifying factors, related symptoms -Check every visit -Most groups use patient handouts to assess current symptoms -PHMG uses Brief Pain Inventory. Others are available.
30 Standard of Care: Evaluation: Function Evaluation of Function: Current function Effect of pain on function Confirmed improvement in function with treatment
31 Standard of Care: Evaluation: Function Treatment must be aimed towards improving function, not just reducing pain. -Function may improve without improvement in pain, if pain control increases activity. Improved function alone may demonstrate adequate treatment. -Improved pain with reduction in function may represent drug side effect, and may be an indication to reduce or stop opioids.
32 Standard of Care: Evaluation: Function Most groups use a standardized screening tool for evaluation of function Evaluate at each visit PHMG uses the FAQ5, and questions about activity Discussion of patient activities, and observation of function are also valid assessment
33 Standard of Care: Evaluation: Psychiatric Comorbidity Assessment of Psychiatric Comorbidity includes: Psychiatric Diagnoses Current psychiatric symptoms Many psychiatric diagnoses are risks for chronic pain, and also risks for misuse of narcotic medication. Treatment of psychiatric symptoms often reduces pain
34 Standard of Care: Evaluation: Psychiatric Comorbidity Many groups use a standardized screening tool for evaluation of current psychiatric symptoms PHMG screens for depression; used by PHQ9 GAD 7 measures anxiety, another risk
35 Standard of Care: Evaluation: Narcotic Use Risk Evaluation of risk of use of narcotics includes: Medical conditions potentially impacted, and Risk for drug misuse: Standardized screening tools: ORT, SOAPP-R, COMM Past aberrant behaviors- The best predictor of future behavior is past behavior Urine Drug Screens- at least yearly; more if higher risk Random pill counts- sometimes helpful
36 Standard of Care: Evaluation: Narcotic Use Risk Screening Tools for Drug Misuse Risk: ORT: includes history of alcohol and substance abuse and sexual abuse, predicts baseline risk of misuse of medications. -use only once COMM: asks about current misuse, current mood and cognitive symptoms (must be licensed) SOAPP-R asks a combination of past and current status questions -use sometimes, or every time
37 Make it Easy: Use a Questionnaire PHMG Chronic Pain Questionnaire Combines 4 standardized, validated screening tools: Brief Pain Questionnaire FAQ5 Epworth Sleepiness Scale PHQ9 (may also include COMM or SOAPP-R) One, 3 page handout for patients to complete For use at each visit
38
39
40 Assess 4 A s at every visit: Analgesia Activity Adverse effects Aberrancy PHMG handout eg screens for all of these. May use with every pain visit for patients on chronic opioids
41 Pain Questionnaires: process for use Identify chronic pain patients during scrub and huddle MOA give labeled questionnaire to front desk to give to patient to complete; check that it is done before provider visit. Provider reviews questionnaire during visit. Key is included with the form (don t give to patient) May be scanned to patient chart. Managers can get forms printed for clinic supply.
42 Standard of Care: Evaluation: Physical Exam Pain related physical exam Don t forget to do it
43 Treatment: 1. Establish diagnosis 2. Establish treatment goals 3. Comprehensive treatment plan

44 Medical indications for opioids:
45 Standard of Care: Treatment Goals of treatment should be specific, related to function, and established and documented at outset. The Peace Health Pain Questionnaire asks, what is your goal in treatment? Patients often say no pain. This expectation is not realistic, and should be corrected. Realistic, functional goals should be negotiated instead.
46 Example of Functional Goals: What do you want to be able to do? Clean my house and take care of my kids Sleep without pain waking me Work Exercise
47 Standard of Care: Treatment Effective pain treatment is comprehensive and holistic Narcotics are rarely needed for chronic pain. Narcotics are appropriate only if benefit exceeds risk, only in patients with moderate or severe pain that can t be controlled otherwise Narcotics give on average 30% pain reduction Narcotics may not be effective with long term use
48 Example: ICSI guidelines: Level 1 Pain Management: (find this on Crossroads, Physician Web Portal) Mechanical/ Compressive Pain: (back pain, visceral pain, musculoskeletal pain) Or: Inflammatory Pain: (inflammatory arthritis, post-surgical pain, infection) RX: Physical rehab, behavioral management, NSAIDs, antidepressants Neuropathic Pain: (Neuropathy, HIV, CVA, MS, fibromyalgia, migraine) RX: Local or systemic neural modulators
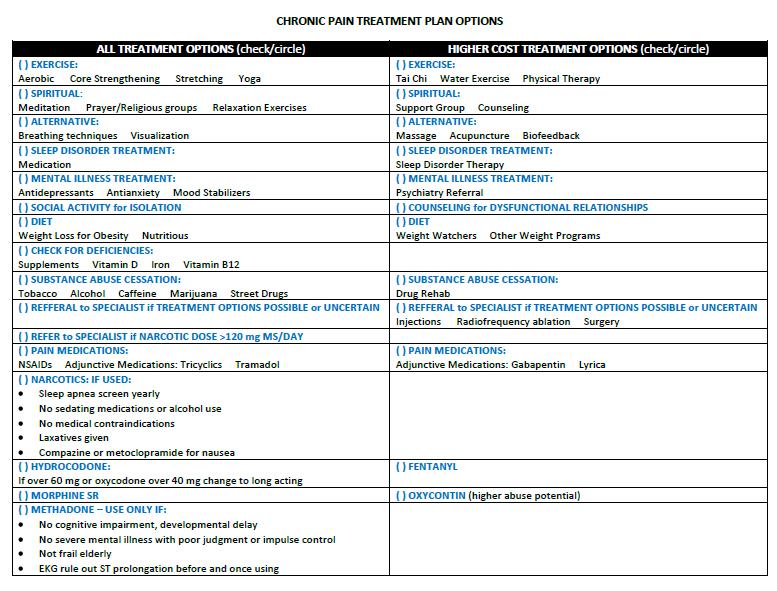
49 Treatment plan should/may include: Lifestyle modifications, exercise Non-opioid medications Treatment for nutritional or endocrine deficiencies Physical and behavioral therapies Spirituality and social support. Not just opioids!
50
51 Standard of Care: Treatment When to use Opioids: Not treating pain at all is not the standard of care. Nor is refusal to treat patients with chronic pain. In considering use of opioids, consider the patient s individual circumstance. General rules about non-use of opioids are not appropriate, but must be considered in the context of the individual patient.
52 Example: VA policy: 1. A trial of opioid therapy is indicated for a patient with chronic pain who meets all of the following criteria: a. Moderate to severe pain that has failed to adequately respond to indicated non-opioid and non-drug therapeutic interventions b. The potential benefits of opioid therapy are likely to outweigh the risks ( i.e., no absolute contraindications) c. The patient is fully informed and consents to the therapy d.. Clear and measurable treatment goals are established 2. The ethical imperative is to provide the pain treatment with the best benefit-to-harm profile for the individual patient.
53 Example: Washington State Policy: Use opioids for acute or chronic pain only after determining that alternative therapies do not deliver adequate pain relief. Use the lowest effective dose.
54 Dosing opioids Doses >120 mg morphine equivalent show increased frequency of morbidity and mortality Washington State guidelines require specialist consultation if using >120 mg MED without pain relief American College of Occupational and Environmental Medicine, March 26, 2014, MED doses should be limited to 50 mg in most cases, particularly in the acute setting; although, sub-acute and chronic pain patients may require higher doses.
55 American College of Occupational and Environmental Medicine: Short-acting, breakthrough pain opioid analgesics are generally not recommended in chronic pain. Long-acting, baseline pain agents should be utilized in this patient population, if necessary.
56 For safe opioid use: Use the lowest effective dose Convert to long acting opioid if possible to reduce dependency potential. When converting from one opioid to another, reduce morphine equivalency initially and taper back up, to avoid increasing effect from differences in metabolism Give laxatives to prevent constipation.
57 For safe opioid use: Dose methadone very carefully, increase very slowly! It shows non-linear pharmacokinetics Consider pain specialist referral for any patient needing more than 120 mg morphine equivalent per day.
58 Prescribing Opioids- mechanics Write all prescriptions in 4 week increments (rather than monthly) so patients don t run out on weekends. Write the name of the pharmacy on the prescription. If writing scripts to fill ahead of time, write the date of fill on the script, as well as the date of the script. Make appointment for patient to get refills when due, rather than allowing them to call for refills.
59 Assessing for Side Effects Brief Pain questionnaire includes list of side effects Epworth Sleepiness Scale assesses sedation Methadone: check EKG yearly for QT prolongation and consider checking also prior to start, and for dose changes,. Get sleep study in patients with significant STOPBANG scores (3-4+) Beware: accidents, mood symptoms, and bowel dysfunction may all be opioid related- don t ignore if occurring.
60 Standard of Care: Treatment Treatment plan must include: -Informed consent- review risks and benefits- all patients -Medication agreement Consider in high risk patients High risk is defined by patient status, and by dose.


61 PHMG chronic opioid policy:
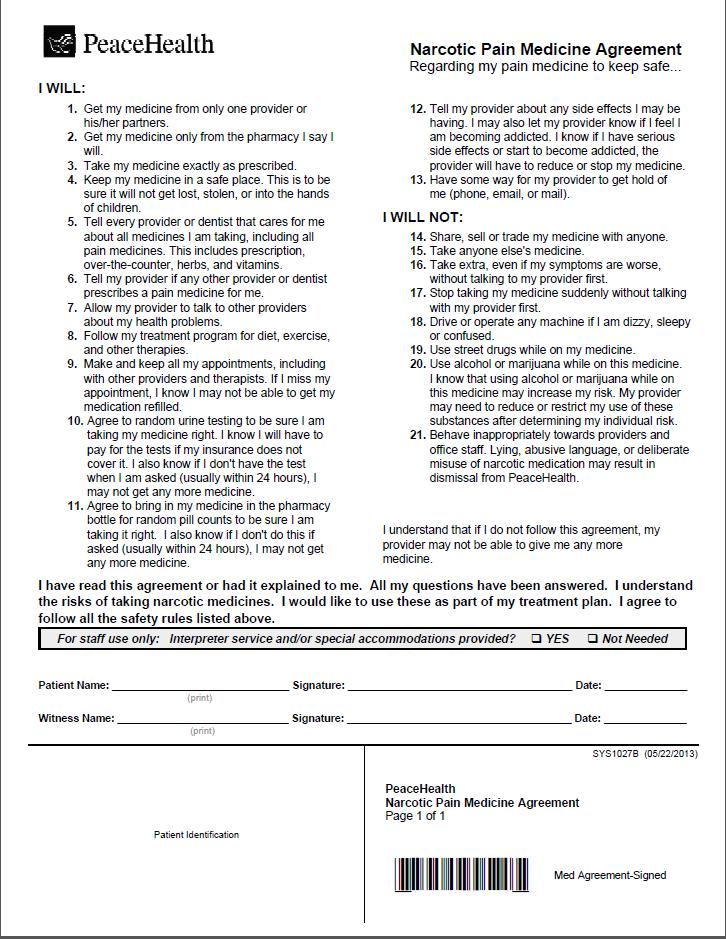
62 Medication agreement
63 Standard of Care: Evaluation: Periodic Review when using opioids FSMB Guidelines: evaluation should be periodic. Most groups, Q3 months is baseline, with frequency varied per risk Suggested process: Recheck Q12 weeks, to correspond with need for refills Increase frequency (to monthly) for patients with high baseline risk or high risk behaviors Decrease frequency (every 6 months) only for patients with very low risk (very low doses, infrequent use, end stage cancer, etc.)
64 Document: If you didn t write it down, it didn t happen
65 Standard of Care: Treatment Opioids should be discontinued if: There is no improvement in function or pain with treatment There are significant adverse effects There are serious contraindications There is evidence of misuse, addiction, or diversion.
66 Washington State Policy: If a patient s dosage has increased to 120 mg/day MS equivalent without substantial improvement in function and pain, seek a consult from a pain specialist.
67 Washington State Policy: If substantial risk is identified through screening, extreme caution should be used and a specialty consultation is strongly encouraged.
68 Refer to Specialist when: Diagnosis or treatment options are unclear Treatments must be performed by specialist Need confirmation on the right treatment Poor response to treatment High doses of opioids High risk patients Complicating medical issues: sleep apnea, addiction, unresponsive psychiatric issues, etc.
69 Specialists for referrals: Consider: Pain Sleep Neurosurgery Orthopedics Neurology Addiction treatment Keep a list of your local and regional resources
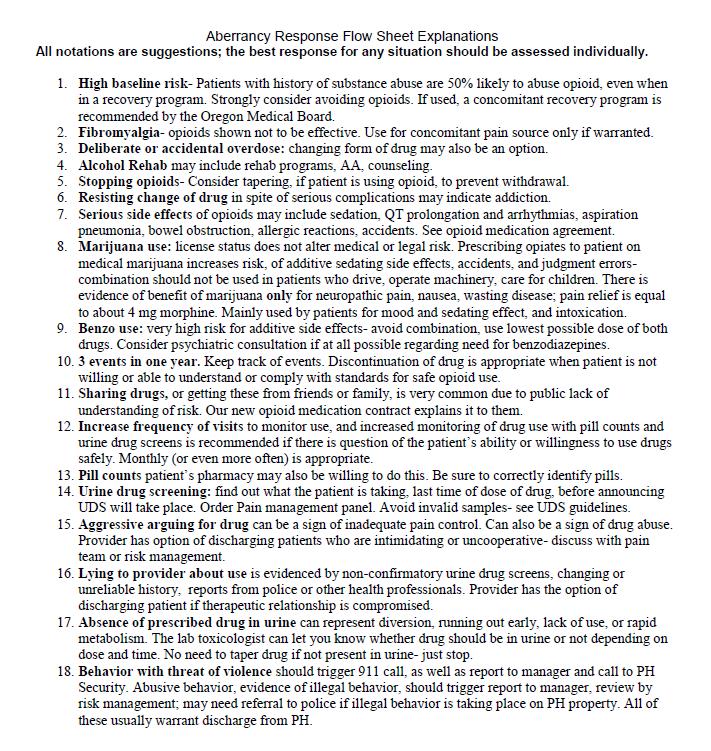
70 Addressing Aberrancy:
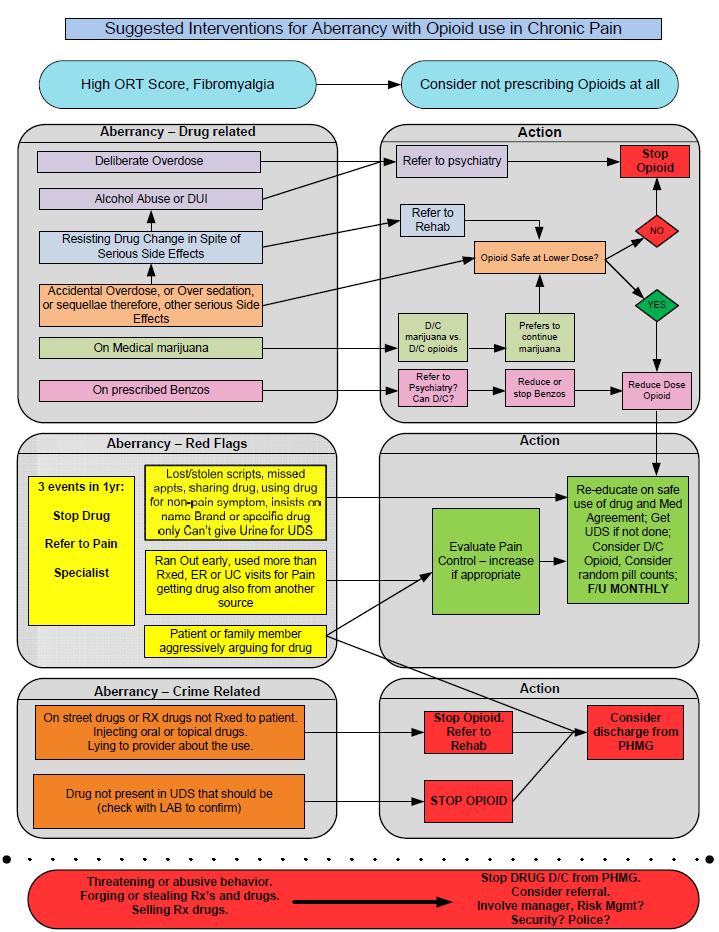
71 Aberrancy: Don t ignore it! Some aberrancies are red flags: Some are absolute contraindications! Examples: street drugs in urine, selling or diverting drugs, absence on UDS, lying about use, overdosing (usually), life threatening side effects, DUI, alcohol abuse, reports by family or friends of drug abuse.
72 Addressing Aberrancy Use Language of Caring Don t make it about your comfort; this is about the patient s safety Best practice for addiction is treatment, not dismissal
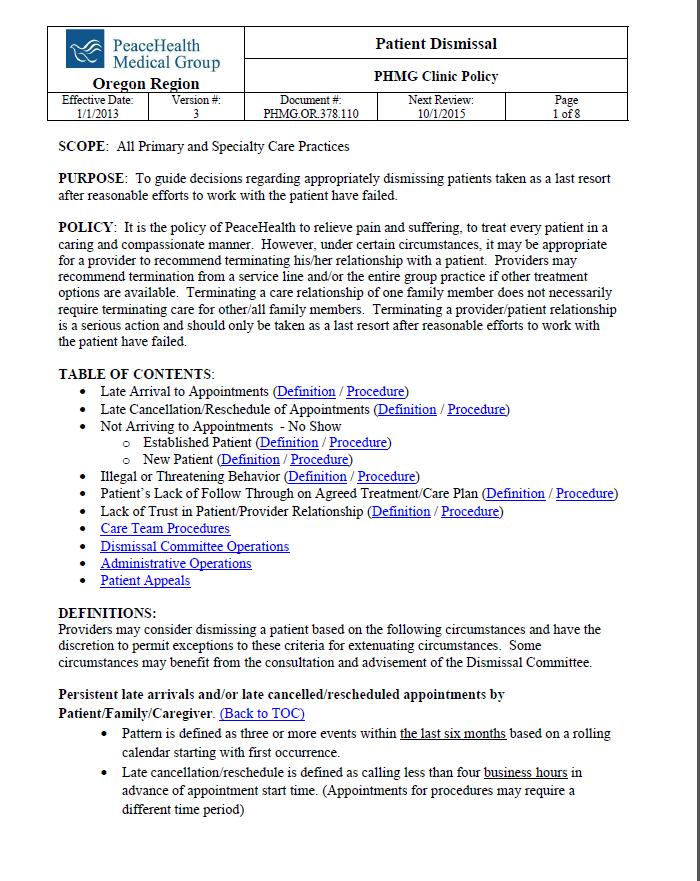
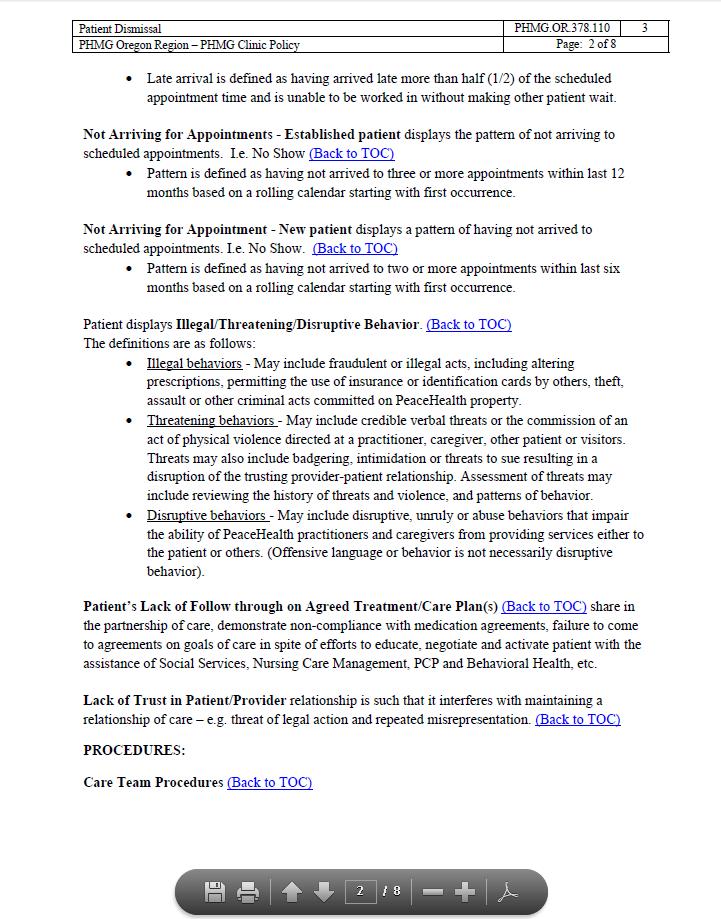
73 Dismissing patients
74 Questions?
75 References Review article: 2009 Clinical Guidelines from the American Pain Society and the American Academy of Pain Medicine on the use of chronic opioid therapy in chronic noncancer pain, Roger Chou, Department of Medicine and Department of Medical Informatics and Clinical Epidemiology, Oregon Health & Science University, Portland, OR, United States The American Academy Of Pain Medicine, Model Policy for the Use of Controlled Substances for the Treatment of Pain: Federation of State Medical Boards of the United States, Inc. Responsible Opioid Prescribing: A Physician s Guide; Scott M. Fishman, MD
76 References, cont. Institute for Clinical Systems Improvement: Health Care Guideline: Assessment and Management of Chronic Pain Veteran s Administration guidelines on opioid therapy for chronic pain Coalition of Community Health Clinics/ Multnoma County Health Clinics Opioid Prescription policies Agency Medical Director s Group- Interagency Guideline on Opioid Dosing for Chronic Non-cancer Pain: An educational aid to improve care and safety with opioid therapy, 2010 Update
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Use of Opioids for Chronic Non Malignant Pain (CNMP)
") I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
Opioids in the Management of Chronic Pain: An Overview
 Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Opioids in the Management of Chronic Pain: An Overview Appropriate treatment of chronic pain may include both pharmacologic and non-pharmacologic modalities. The Board realizes that controlled substances,
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Approaches to Responsible Opioid Prescribing. The Opioid Naïve Patient
 Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approaches to Responsible Opioid Prescribing The Opioid Naïve Patient Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Chronic Pain Management in the Primary Care Setting
 Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Universal Precautions and Opioid Risk. Assessment. Questions: How often do you screen your patients for risk of misuse when prescribing opioids?
 Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Learning objectives 1. Identify the contribution of psychosocial and spiritual factors to pain 2. Incorporate strategies for identifying and mitigating opioid misuse 3. Incorporate non-pharmaceutical modalities
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain
 Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Assessment and Management of Chronic Pain Guideline Summary
 I CSI I NSTITUTE FOR CLINICAL S YSTEMS IMPROVEMENT Implementation Tool: Assessment and Management of Chronic Pain Guideline Summary Assessment Algorithm A = Annotation 1 Patient has pain 2 Critical first
I CSI I NSTITUTE FOR CLINICAL S YSTEMS IMPROVEMENT Implementation Tool: Assessment and Management of Chronic Pain Guideline Summary Assessment Algorithm A = Annotation 1 Patient has pain 2 Critical first
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
IEHP UM Subcommittee Approved Authorization Guidelines Referrals to Pain Management Specialists
 IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
I. Chronic Pain Information Page 2-3. II. The Role of the Primary Care Physician in Chronic Pain Management Page 3-4
 SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
Acupuncture. Opioid Prescribing: Pitfalls for Occupational Medicine Physicians
 Opioid Prescribing: Pitfalls for Occupational Medicine Physicians Presented by Scott Levy M.D. M.P.H. FACOEM Assistant Regional Medical Director, Occupational Health Services The Permanente Medical Group
Opioid Prescribing: Pitfalls for Occupational Medicine Physicians Presented by Scott Levy M.D. M.P.H. FACOEM Assistant Regional Medical Director, Occupational Health Services The Permanente Medical Group
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Managed Care Pushes for Safer Opioid Oversight
 Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
IEHP UM Subcommittee Approved Authorization Guidelines Referrals to Pain Management Specialists
 IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
Vermont. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Oklahoma. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine
 D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
Tennessee. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Ahsan U. Rashid, M.D., F.A.C.P.
 Ahsan U. Rashid, M.D., F.A.C.P. OPIOID MAINTENANCE AND CONSENT Instructions: Review this document before signing. This document will help both the patient and caregivers in establishing a medical program
Ahsan U. Rashid, M.D., F.A.C.P. OPIOID MAINTENANCE AND CONSENT Instructions: Review this document before signing. This document will help both the patient and caregivers in establishing a medical program
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
Rhode Island. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Rhode Island Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Rhode Island Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Monte H. Moore, MD. Idaho Physical Medicine and Rehabilitation. Meridian, ID
 Monte H. Moore, MD Idaho Physical Medicine and Rehabilitation Meridian, ID Chronic pain brief review Opiates important things to know Factors in determining whether to use an opiate What to watch for if
Monte H. Moore, MD Idaho Physical Medicine and Rehabilitation Meridian, ID Chronic pain brief review Opiates important things to know Factors in determining whether to use an opiate What to watch for if
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Missouri Guidelines for the Use of Controlled Substances for the Treatment of Pain
 Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 %
 Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Patient Agreement for the use of Opioid Medications
 today s date Patient Name date of birth Patient Agreement for the use of Opioid Medications The purpose of this agreement is to give you information about the medications that may be part of your treatment
today s date Patient Name date of birth Patient Agreement for the use of Opioid Medications The purpose of this agreement is to give you information about the medications that may be part of your treatment
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain
 Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Taking Opioids Responsibly for Your Safety and the Safety of Others: Patient Information Guide on Long-term Opioid Therapy for Chronic Pain Department of Veterans Affairs (VA) and Department of Defense
Striking a Balance: a provider perspective.
 Striking a Balance: a provider perspective kpfeifer@chcf.org Beth s story 38 years old, erratically employed Counseling doesn t help Chronic low back pain after car accident 8 Vicodin/day grew to 180 mg
Striking a Balance: a provider perspective kpfeifer@chcf.org Beth s story 38 years old, erratically employed Counseling doesn t help Chronic low back pain after car accident 8 Vicodin/day grew to 180 mg
Syllabus. Questions may appear on any of the topics below: I. Multidimensional Nature of Pain
 Questions may appear on any of the topics below: I. Multidimensional Nature of Pain Syllabus A. Epidemiology 1. Pain as a public health problem with social, ethical, legal and economic consequences 2.
Questions may appear on any of the topics below: I. Multidimensional Nature of Pain Syllabus A. Epidemiology 1. Pain as a public health problem with social, ethical, legal and economic consequences 2.
No disclosures for any of the speakers!
 Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist Gabriel Paulian M.D Christopher Ong, M.D Yuliet Sanchez, M.D Uma Suryadevara, M.D No disclosures for any of the speakers!
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
OPIOIDS FOR PERSISTENT PAIN: INFORMATION FOR PATIENTS
 OPIOIDS FOR PERSISTENT PAIN: INFORMATION FOR PATIENTS This leaflet aims to help you understand your pain, so that you can work with your health care team to self-manage your symptoms and improve your quality
OPIOIDS FOR PERSISTENT PAIN: INFORMATION FOR PATIENTS This leaflet aims to help you understand your pain, so that you can work with your health care team to self-manage your symptoms and improve your quality
WHAT YOU NEED TO KNOW TO ABOUT AB 474
 WHAT YOU NEED TO KNOW TO ABOUT AB 474 PRESENTED BY: NEVADA STATE BOARD OF OSTEOPATHIC MEDICINE 2275 Corporate Circle, Suite 210 Henderson, NV 89074 702-732-2147 Fax 702-732-2079 Web Site: www.bom.nv.gov
WHAT YOU NEED TO KNOW TO ABOUT AB 474 PRESENTED BY: NEVADA STATE BOARD OF OSTEOPATHIC MEDICINE 2275 Corporate Circle, Suite 210 Henderson, NV 89074 702-732-2147 Fax 702-732-2079 Web Site: www.bom.nv.gov
Pharmacist s Role In Pain Management. Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017
 Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Pharmacist s Role In Pain Management Katrina Lynn, Pharm D PSHP Annual Assembly: October 12, 2017 1 Presentation Objectives Briefly discuss Geisinger Health System and the use of Pain Management Pharmacists
Department of Veterans Affairs Network Policy No.: VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA
 Date: September 23, 2014 Long Beach, CA") Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2099-5 Program Prior Authorization/Medical Necessity Buprenorphine Products (Pain Indications) Medication Belbuca (buprenorphine
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2099-5 Program Prior Authorization/Medical Necessity Buprenorphine Products (Pain Indications) Medication Belbuca (buprenorphine
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk
 Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
The Difficult Patient: Risk Mitigation Strategies
 The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction
The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction
MEDICATION MANAGEMENT AGREEMENT
 MEDICATION MANAGEMENT AGREEMENT The goal of this agreement is to ensure that you and your physician comply with all state and federal regulations concerning the prescribing of controlled substances. The
MEDICATION MANAGEMENT AGREEMENT The goal of this agreement is to ensure that you and your physician comply with all state and federal regulations concerning the prescribing of controlled substances. The
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Prescription Opioid Overdose in Oregon: A public health perspective
 Prescription Opioid Overdose in Oregon: A public health perspective Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Health Authority All-Cause Mortality,
Prescription Opioid Overdose in Oregon: A public health perspective Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Health Authority All-Cause Mortality,
Pain, Opioids and the EMR. Dr. Gordon Schacter April 12, 2018
 Pain, Opioids and the EMR Dr. Gordon Schacter April 12, 2018 Faculty/Presenter Disclosure Faculty: Gordon Schacter Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
Pain, Opioids and the EMR Dr. Gordon Schacter April 12, 2018 Faculty/Presenter Disclosure Faculty: Gordon Schacter Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
Colorado State Board of Medical Examiners Policy
 POLICY NUMBER: 10-14 Title: Guidelines for the Use of Controlled Substances for the Treatment of Pain Date Issued: May 16, 1996 Date(s) Revised: November 18, 2004 Reference: 12-36-117, C.R.S. Purpose:
POLICY NUMBER: 10-14 Title: Guidelines for the Use of Controlled Substances for the Treatment of Pain Date Issued: May 16, 1996 Date(s) Revised: November 18, 2004 Reference: 12-36-117, C.R.S. Purpose:
Six Building Blocks Self-Assessment Questionnaire Workshop Version July 2017
 July 2017 Background The Six Building Blocks were developed as part of a research project on Team Based Opioid Management in rural clinics. The three year research study is a collaboration between 20 rural
July 2017 Background The Six Building Blocks were developed as part of a research project on Team Based Opioid Management in rural clinics. The three year research study is a collaboration between 20 rural
KANSAS Kansas State Board of Healing Arts. Source: Kansas State Board of Healing Arts. Approved: October 17, 1998
 KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
Opioids: What You Should Know About Opioid Prescribing. Denis G. Patterson, DO Nevada State Medical Association October 19, 2016
 Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
West Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile West Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile West Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Alberta WCB Policies & Information
 1. What are the objectives of WCB regarding the authorization of prescribed opioid analgesics As part of an overall approach to effective, appropriate claims management, including the provision of and
1. What are the objectives of WCB regarding the authorization of prescribed opioid analgesics As part of an overall approach to effective, appropriate claims management, including the provision of and
OPIOID CRISIS: A PERSPECTIVE. Karl J. Haake, MD
 OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina
 Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Approved Procedures for Prescribing and Monitoring Controlled Substances in South Carolina Robert B. Hanlin, M.D., FAAFP Vice Chair, Medical Staff Affairs Greenville Health System Greenville, SC Disclosures
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Understanding pain and mental illness Impact on management principles
 Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
About Your Pain Management
 UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions This handout outlines the goals of pain management treatment. It also reviews the guidelines that you are expected to
UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions This handout outlines the goals of pain management treatment. It also reviews the guidelines that you are expected to
MQAC Rules for the Management of Chronic Non-Cancer Pain For Allopathic Physicians Effective January 2, 2012
 MQAC Rules for the Management of Chronic Non-Cancer Pain For Allopathic Physicians Effective January 2, 2012 WAC 246-919-850 Pain management Intent. These rules govern the use of opioids in the treatment
MQAC Rules for the Management of Chronic Non-Cancer Pain For Allopathic Physicians Effective January 2, 2012 WAC 246-919-850 Pain management Intent. These rules govern the use of opioids in the treatment
Location of initiative York Region Chronic Kidney Disease Program, Mackenzie Richmond Hill Hospital, Richmond Hill, ON
 Story # CSHP 015 objective Objective.1 - In 70% of ambulatory and specialized care clinics providing clinic care, pharmacists will manage medication therapy for clinic patients with complex and high-risk
Story # CSHP 015 objective Objective.1 - In 70% of ambulatory and specialized care clinics providing clinic care, pharmacists will manage medication therapy for clinic patients with complex and high-risk
Pain and its Treatments. Our Goals: Understand: What is pain and what causes it? 2. What are different types of pain? 3. How do opioid drugs work?
 Pain and its Treatments Cheryl Stucky, Ph.D. Medical College of Wisconsin Our Goals: Understand: 1. What is pain and what causes it? 2. What are different types of pain? 3. How do opioid drugs work? What
Pain and its Treatments Cheryl Stucky, Ph.D. Medical College of Wisconsin Our Goals: Understand: 1. What is pain and what causes it? 2. What are different types of pain? 3. How do opioid drugs work? What
OPIOID PAIN MEDICATION Agreement and Informed Consent
 OPIOID PAIN MEDICATION Agreement and Informed Consent I. Introduction Research and clinical experience show that opioid (narcotic) pain medications are helpful for some patients with chronic pain. The
OPIOID PAIN MEDICATION Agreement and Informed Consent I. Introduction Research and clinical experience show that opioid (narcotic) pain medications are helpful for some patients with chronic pain. The
Opioid Prescribing Improvement Program
 Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine
 INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
Louisiana. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Louisiana Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Louisiana Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescription Monitoring Program (PMP)
") 06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
Effective Date: May 19, Revised Date: August 18, Policy Number: MED Policy 313. Pain Management Long Term Opioid Use
 Effective Date: May 19, 2008 Revised Date: August 18, 2015 Approved by: Thomas M Tocher, MD, MPH, Chief Clinical Officer Policy Number: MED Policy 313 Title: Pain Management Long Term Opioid Use POLICY
Effective Date: May 19, 2008 Revised Date: August 18, 2015 Approved by: Thomas M Tocher, MD, MPH, Chief Clinical Officer Policy Number: MED Policy 313 Title: Pain Management Long Term Opioid Use POLICY
Prescription Review Program and College Expectations
 Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP ABAM Consultant, Prescription Review Program Prescribers Course May 13, 2016 Disclosure Never had any commercial
Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP ABAM Consultant, Prescription Review Program Prescribers Course May 13, 2016 Disclosure Never had any commercial
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Disclosures. Management of Chronic Pain for Cancer Survivors. University of Kentucky HealthCare, Lexington, KY
 Management of Chronic Pain for Cancer Survivors Paul A. Sloan, M.D. Professor and Vice Chair for Research Associate Program Director, Pain Medicine Fellowship Department of Anesthesiology University of
Management of Chronic Pain for Cancer Survivors Paul A. Sloan, M.D. Professor and Vice Chair for Research Associate Program Director, Pain Medicine Fellowship Department of Anesthesiology University of
New Mexico. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile New Mexico Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile New Mexico Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Pain Management: Overview of A Practical Approach
 Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Chronic Pain: Advances in Psychotherapy
 Questions from chapter 1 Chronic Pain: Advances in Psychotherapy 1) Pain is a subjective experience. 2) Pain resulting from a stimulus that would normally not produce pain such as a breeze is a) analgesia
Questions from chapter 1 Chronic Pain: Advances in Psychotherapy 1) Pain is a subjective experience. 2) Pain resulting from a stimulus that would normally not produce pain such as a breeze is a) analgesia
About Your Pain Management
 UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions about opioids This handout explains the goals of managing pain with opioids, which are a type of prescription pain medicine.
UW MEDICINE PATIENT EDUCATION About Your Pain Management Answers to common questions about opioids This handout explains the goals of managing pain with opioids, which are a type of prescription pain medicine.
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
An unpleasant sensory and emotional experience associated with actual or potential tissue damage.
 An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Acute Pain results from disease, inflammation or injury to tissues; generally comes on suddenly and may
An unpleasant sensory and emotional experience associated with actual or potential tissue damage. Acute Pain results from disease, inflammation or injury to tissues; generally comes on suddenly and may
Pain and Addiction. Edward Jouney, DO Department of Psychiatry
 Pain and Addiction Edward Jouney, DO Department of Psychiatry Case 43 year-old female with a history chronic lower back pain presents to your clinic ongoing care. She has experienced pain difficulties
Pain and Addiction Edward Jouney, DO Department of Psychiatry Case 43 year-old female with a history chronic lower back pain presents to your clinic ongoing care. She has experienced pain difficulties
Pain Management and Addiction: Clinical Challenges
 Pain Management and Addiction: Clinical Challenges MMS Pain Management Forum March 12, 2010 Associate Professor of Medicine Boston University School of Medicine Boston Medical Center Conflicts of Interest
Pain Management and Addiction: Clinical Challenges MMS Pain Management Forum March 12, 2010 Associate Professor of Medicine Boston University School of Medicine Boston Medical Center Conflicts of Interest
Nancy Elder, MD, MSPH Cincinnati, Ohio
 Nancy Elder, MD, MSPH Cincinnati, Ohio My neck has hurt ever since my motorcycle crash in 2001. You got to help me, Doc! Great. Another drug seeking patient wanting narcotics. When I was working and had
Nancy Elder, MD, MSPH Cincinnati, Ohio My neck has hurt ever since my motorcycle crash in 2001. You got to help me, Doc! Great. Another drug seeking patient wanting narcotics. When I was working and had
Mandatory PDMP Use PDMP Use STATE Prescriber Dispenser Conditions, if applicable
 Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Arizona Amends worker s compensation statute to require physicians to request PMP information within two (2) business days of writing or dispensing prescriptions for at least a 30 day supply of an opioid
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand