Nosocomial and healthcare-associated infections
|
|
|
- Paul Gallagher
- 6 years ago
- Views:
Transcription
1 Nosocomial and healthcare-associated infections David Lye FRACP, FAMS Senior consultant, Institute of Infectious Diseases and Epidemiology, Communicable Disease Centre, Tan Tock Seng Hospital Associate professor, Yong Loo Lin School of Medicine, National University of Singapore
2 Definitions Hospital-acquired or healthcare-associated? Centre for Disease Control/National Healthcare Safety Network, January 2014 Healthcare-associated infections (HAI) Localized or systemic condition resulting from an adverse reaction to presence of an infectious agent(s) or its toxin(s) not present on admission to the acute care facility


3 Healthcare risk factors
4 Prevalence of healthcareassociated infections


5 183 hospitals patients 93.2%


6 83%
7 Nosocomial pneumonia
8 Nosocomial pneumonia (VAP HAP HCAP) Increased hospital stay by 7-9 days Excess cost >USD$40,000 25% of ICU infections >50% antibiotic use Attributable mortality 33-50%

9
, Pseudomonas (26%), Non-fermenting GNB (10%), Other")
10 HCAP vs.cap More MRSA (31%), Pseudomonas (26%), Non-fermenting GNB (10%), Other Enterobacteriaceae (9%) Less Pneumococcus, Haemophilus, Legionella
11 Risk factors and prevention General Hand hygiene and contact precaution to prevent crossinfection Mechanical ventilation Non-invasive ventilation, avoid intubation Continuous suction of subglottic secretions Endotrachel tube cuff pressure >20cm H20 Contaminated condensate emptied and prevented from entering ETT Sedation protocol to accelerate weaning Adequate ICU staffing Aspiration, body positioning, enteral feeding Semi-recumbent, degrees Enteral nutrition Colonisation Daily interruption of sedation and avoid paralytic agents Stress bleeding prophylaxis, transfusion and hyperglycaemia H2 antagonist or sucralfate Restricted transfusion trigger policy Insulin to maintain glucose mg/dl

12 Diagnosis CXR new or progressive Fever or leukocytosis Purulent sputum or desaturation CPIS 6 low probability of HAP

13 Culture-guided antibiotic therapy

14 Alternative diagnoses


15
16 Catheter-associated urinary tract infection
17 Catheter-associated UTI (CAUTI) 40% of HAI s 15-25% in general hospitals had urinary catheters for 2-4 days 5-10% nursing home residents had urinary catheters, some for years Bacteraemia 1-4% with mortality ~13% Extended length of stay 2 days Cost CAUTI USD$676, bacteraemia USD$2836

18
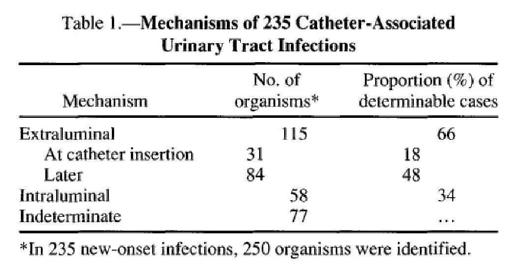

19 Extraluminal 66% GPC 79% GNB 54% Yeast 69%

20 Conditioning film of host urinary components Bacteria attach by hydrophobic and electrostatic interactions, and flagella Cell division, additional planktonic bacteria, extracellular matrix Loosely packed 3-D structure with fluid channels for nutrients and wastes Survival advantage: Resistance to sheer forces and phagocytosis Antimicrobial resistance

21 HICPAC 2009

22 Appropriate indications IDSA 2010

23
24 Silver alloy catheters A Cochrane Review of short-term urethral catheters in hospitalized adults: Silver alloy catheters significantly reduced asymptomatic bacteriuria in catheters inserted for less than (RR:0.54; 95%CI: 0.43 to 0.67) and more than one week (RR:0.64, 95%CI: 0.51 to 0.80) [Cochrane Database Syst Rev. 2008;(2):CD004013] Confounding by comparators as benefit significantly reduced with different comparators In bacterial adherence study, no difference was found between silver alloy hydrogel urinary catheters and hydrogel catheters [Clin Infect Dis. 2010;51:550-60]
25 Antimicrobial-coated catheters Antimicrobial-coated urinary catheters including minocycline and rifampicin (RR:0.36; 95%CI: 0.18 to 0.73) and nitrofurazone (RR:0.52, 95%CI: 0.34 to 0.78) significantly reduced asymptomatic bacteriuria in catheters inserted for less than one week but not in those inserted for more than one week [Cochrane Database Syst Rev. 2008;(2):CD004013]



26
27 Diagnostic criteria Urine culture or urinalysis was found to be nonspecific for CAUTI in 14 patients with long-term urinary catheters [Am J Infect Control. 1985;13: ] A study of 56 patients with spinal cord disorders: Cloudy urine had an accuracy of 83.1%, pyuria Sn 82.8%, and fever Sp 99% but Sn 6.9% for CAUTI [J Spinal Cord Med. 2009;32: ].
28 Urinalysis A study of 106 ICU patients: positive nitrite on urinalysis Sp 91.8% but Sn 29.5% Leukocyte esterase, white cells and presence of yeast or bacteria did not differentiate those with and without CAUTI [Intensive Care Med. 2006;32: ] A study of 144 ICU patients: combining leukocyte esterase and nitrite Sn 87.2%, Sp 61.6%, PPV 30.6% and NPV 96.1% [Intensive Care Med. 2001;27: ]




29

30
31 Evidence base: treatment In a randomised study of 119 women with CAUTI, resolution occurred in 36% without antibiotic, 81% with single dose co-trimoxazole and 79% with 10 days of co-trimoxazole, after removal of urinary catheters [Ann Intern Med. 1991;114:713 9] Another randomised study of 619 patients with pyelonephritis and complicated UTI of whom 68 had urinary catheters, 5 days of levofloxacin versus 10 days of ciprofloxacin resulted in microbiological eradication of 79% versus 53% in the subgroup of catheterised patients [Urology. 2008;71:17 22] In another randomised study of 60 spinal cord patients with predominantly intermittent catheterisation comparing 3 versus 14 days of ciprofloxacin, microbiological cure was lower, and microbiological and clinical relapse higher in the 3-day group; however clinical cure was similar [Clin Infect Dis. 2004;39:658 64]. In a randomised study of 54 patients with LT-UC in nursing home with CAUTI comparing replacement and non-replacement of urinary catheters before antibiotic, 93% in the group with replaced urinary catheters became afebrile by 72 hours [J Urol. 2000;164: ].
32 Central line associated bloodstream infection
33 Central line associated bloodstream infections (CLABSI) CDC HICPAC prevention guideline 2011 Independently increased length of stay and hospital cost, but not mortality
34 Impact: death, length of stay and cost
35 Prevalence
36 Colonisation and bacteraemia


37

38 Treatment Removal of catheter Duration of antibiotic Complicated vs. uncomplicated

39 Treatment Removal of catheter Duration of antibiotic Complicated vs. uncomplicated


40 Catheter salvage and antibiotic lock therapy
41 Clostridium difficile associated diarrhoea

42 Epidemiology Rising incidence since 2001 Severe and fatal CDAD Epidemic strain North American Pulse Field Type 1 (NAP1) or PCR ribotype 027 Increased toxins A and B, fluoroquinolone resistance, binary toxin Deletion tcdc which inhibits toxin production


43 Risk factors
44 Clinical features and epidemiology ICHE 1995; 16: 459 Definition: diarrhoea (6 watery stools 36 hours, 3 unformed stools 24 hours 2 days, 8 unformed stools 48 hours), pseudomembrane endoscopy, toxin A or B stool, +ve stool culture and no other cause +/- antibiotic use <1% ileus without diarrhoea Carriage common in infants, markedly decline by 1 year Adult carriage 2% Sweden to 15% Japan 10% hospital patients colonised Primary cause antibiotic-colitis, 15-25% antibiotic diarrhoea 30% hospital patients diarrhoea CD +ve Rehabilitation 25% Community <1/10000 antibiotic prescriptions
45 Clinical features and epidemiology ICHE 1995; 16: 459 Initial stool negative, test another (increased yield 10% for 3 stools) 20% initial culture-negative adults nosocomially acquire CDAD (high endemicity) 2/3 remain asymptomatic 8% per week 13% 1-2 weeks, 50% >4 weeks (CID 1998; 26: 1027) Median time from admission to CDAD 13 days (NEJM 2005; 353: 2442), 21 days (EID 2003; 9: 730)
 promising, PCR sensitive and")
46 3 or more unformed stools in last 24 hours Testing: Only on unformed stool Not on asymptomatic or test of cure or repeat in same episode of diarrhoea EIA sub-optimal sensitivity, 2-step GDH (with cell cytotoxin assay or culture) promising, PCR sensitive and specific


47

48 Treatment




49 Cure higher with oral vancomycin for severe CDAD only Relapse similar (10%)


50 Fidaxomicin less relapse vs. vancomycin


51 AJG 2002;97:1769



52
53 Surgical site infections
54 Surgical site infections (SSI) ICHE 1999;20:247 Third commonest HAI 14-16% of HAI s Among deaths in surgical patients with SSI, 77% related to SSI, 93% due to organ space SSI Increased length of stay by 10 days Increased cost by USD$2000

55 Diagnosis: SSI

56 ICHE 1999; 20: 247
57 ICHE 1999; 20: 247
58 SSI risk stratification and surveillance ICHE 1999; 20: 247 Within clean wound category, SSI risk % (SENIC) and % (NNIS) SENIC, 4 independent risk factors (abdominal operation, >2 hours, contaminated or dirty wound, >3 discharge diagnoses), each given 1 point if present, score 0-4 NNIS risk index 0-3, 1 point if present for (1) ASA >2 (2) contaminated or dirty wound (3) operating time >T hours [75 th percentile for specific operation] Inpatient, post-discharge and outpatient surveillance Direct and indirect detection 12 84% SSI detected after discharge Most SSI evident within 21 days
59 Risk index and SSI rates Wound category Clean Clean contaminated Contaminated SSI rate, % NNIS risk index SSI rate, % Dirty
60 Surgical site infections ICHE 1999;20:247 Patient factors Preoperative Skin preparation Hand and forearm antisepsis Intraoperative Operating room environment Surgical attire and drapes Asepsis and surgical techniques Postoperative Incision care
61 Pre-operative antibiotic prophylaxis ICHE 1999; 20: principles: Evidence of efficacy or effect of SSI catastrophic Antibiotic: safe, inexpensive, bactericidal, active against probable contaminants Time the infusion so bactericidal drug level in tissue and serum at skin incision Maintain therapeutic level until at most a few hours after incision is closed Indicated for all operations entering hollow viscus and clean operations where prosthetic material inserted or effect of SSI catastrophic Need for second dose depends on: tissue level by standard therapeutic dose, serum half life, MIC 90 of anticipated SSI pathogens Antibiotic given no more than 30 minutes before skin incision Vancomycin needs 1 hour infusion




62 Several good guidelines

63 Evidence: 1=meta-analysis, 2=RCT, 3=well-designed study, 4=opinion


64
65

66 Surgical antibiotic prophylaxis
67 Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomized controlled trials Br J Surg 1998;85:1232 Trials from 1984 to 1995, n=147 Effective for prevention of SSI in colorectal surgery No significant difference between many different regimens Not good: metronidazole OR doxycycline OR piperacillin alone, PO neomycin and erythromycin First-generation cephalosporins as good as newgeneration cephalosporins (OR 1.07, 95% CI )


68

69

70 Visceral, trauma and vascular surgery IV cefuroxime 1.5G +/- metronidazole 500mg
71

72

73
74 Right timing more important With right timing, re-dosing >2 T1/2 of prolonged surgery additional benefit
75 Duration of surgical antibiotic prophylaxis J Thorac Cardiovasc Surg 1977;73:470 Prospective double-blind study, 2 vs. 6 days of cephalothin, prosthetic valve surgery Sternal wound infection 2.1% vs. 2.8% Aust N Z J Surg 1998;68:388 Meta-analysis of prospective, randomised studies, same drug in both arms No advantage of multiple vs. single dose No difference: beta-lactam vs. others, >24 vs. 24 hours BMJ 1979;6165:707 Prospective, 3 doses of cephaloridine vs. 2 weeks flucloxacillin, THJR Overall deep infection 1.3%, no difference between 2 arms Br J Surg 1998;85:1232 Single dose pre-op as effective as long-term post-op (OR 1.17, 95% CI )
76


77
78


79 Control blood sugar for DM


80 Normothermia for all but cardiac surgery
81 Pre-operative hair removal to reduce surgical site infections Cochrane Database Systematic Rev 2006;2:CD Assess RCT of hair removal vs. no hair removal, different methods and times N=11 3 RCT compared depilatory cream/razor vs. no hair removal no difference in SSI 3 RCT compared shaving with clipping more SSI with shaving (OR 2.02, 95% CI ) 7 RCT compared shaving with depilatory cream more SSI with shaving (OR 1.54, 95% CI ) 1 RCT compared each compared shaving OR clipping on day of surgery vs. day before surgery no difference in SSI Use clippers or depilatory cream, or do not shave
82 Questions?
Preventing Surgical Site Infections: The SSI Bundle
 Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Probiotics for Primary Prevention of Clostridium difficile Infection
 Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS
 CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
CATHETER-ASSOCIATED URINARY TRACT INFECTIONS Hamid Emadi M.D Associate professor of Infectious diseases Department Tehran university of medical science The most common nosocomial infection The urinary
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review
 Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Stony Brook Adult Clostridium difficile Management Guidelines. Discontinue all unnecessary antibiotics
 Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI. CPT. Pasri Maharom MD, MPH Dec 15, 2015
 Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
Prevention of Important HAIs: Principle & Case Scenario in VAP/CAUTI CPT. Pasri Maharom MD, MPH Dec 15, 2015 Catheter Associated Urinary Tract Infection CAUTI CAUTI Epidemiology Key Principles of Preventing
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
VAP Prevention bundles
 VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
VAP Prevention bundles Dr. Shafiq A.Alimad MD Head of medical department at USTH YICID workshop, 15-12-2014 Care Bundles What are they & why use them? What are Care Bundles? Types of Care Bundles available
Pneumonia Community-Acquired Healthcare-Associated
 Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Pneumonia Community-Acquired Healthcare-Associated Edwin Yu Clin Infect Dis 2007;44(S2):27-72 Am J Respir Crit Care Med 2005; 171:388-416 IDSA / ATS Guidelines Microbiology Principles and Practice of Infectious
Healthcare-associated infections acquired in intensive care units
 SURVEILLANCE REPORT Annual Epidemiological Report for 2015 Healthcare-associated infections acquired in intensive care units Key facts In 2015, 11 788 (8.3%) of patients staying in an intensive care unit
SURVEILLANCE REPORT Annual Epidemiological Report for 2015 Healthcare-associated infections acquired in intensive care units Key facts In 2015, 11 788 (8.3%) of patients staying in an intensive care unit
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE
 EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
Asyntomatic bacteriuria, Urinary Tract Infection
 Asyntomatic bacteriuria, Urinary Tract Infection C. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asyntomatic Bacteriuria in Adults (2005) Pyuria accompanying asymptomatic
Asyntomatic bacteriuria, Urinary Tract Infection C. Infectious Diseases Society of America Guidelines for the Diagnosis and Treatment of Asyntomatic Bacteriuria in Adults (2005) Pyuria accompanying asymptomatic
EMPIRICAL TREATMENT OF SELECT INFECTIONS ADULT GUIDELINES. Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection
 URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
URINARY TRACT Refer to VIHA Algorithm for the empiric treatment of Urinary Tract Infection and Asymptomatic Bacteriuria on the VIHA Intranet: https://intranet.viha.ca/departments/pharmacy/clinical_pharmacy/pages/infec
The Potential For Microbiome Modification In Critical Illness. Deborah Cook
 The Potential For Microbiome Modification In Critical Illness Deborah Cook To review Objectives The microbiome & concepts about its modification during critical illness Interventions Predisposition to
The Potential For Microbiome Modification In Critical Illness Deborah Cook To review Objectives The microbiome & concepts about its modification during critical illness Interventions Predisposition to
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
NHSN and Public Reporting. Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_
 1 NHSN and Public Reporting Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_ greene@urmc.rochester.edu 2 Objectives Describe challenges and opportunities
1 NHSN and Public Reporting Linda R. Greene, RN,MPS,CIC Manager Infection Prevention Highland Hospital Rochester, NY linda_ greene@urmc.rochester.edu 2 Objectives Describe challenges and opportunities
ABSTRACT PURPOSE METHODS
 ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Potential Conflicts of Interests
 Potential Conflicts of Interests Research Grants Agency for Healthcare Research and Quality Akers Bioscience, Inc. Pfizer, Inc. Scientific Advisory Boards Pfizer, Inc. Cadence Pharmaceuticals Kimberly
Potential Conflicts of Interests Research Grants Agency for Healthcare Research and Quality Akers Bioscience, Inc. Pfizer, Inc. Scientific Advisory Boards Pfizer, Inc. Cadence Pharmaceuticals Kimberly
CAUTI CONFERENCE CAUTI Prevention and Appropriate Use of Indwelling Urinary Catheters in the Hospital Setting
 CAUTI CONFERENCE CAUTI Prevention and Appropriate Use of Indwelling Urinary Catheters in the Hospital Setting James T. Fields, MD Carolinas Center for Medical Excellence Columbia, South Carolina February
CAUTI CONFERENCE CAUTI Prevention and Appropriate Use of Indwelling Urinary Catheters in the Hospital Setting James T. Fields, MD Carolinas Center for Medical Excellence Columbia, South Carolina February
Community Acquired & Nosocomial Pneumonias
 Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
Community Acquired & Nosocomial Pneumonias IDSA/ATS 2007 & 2016 Guidelines José Luis González, MD Clinical Assistant Professor of Medicine Outline Intro - Definitions & Diagnosing CAP treatment VAP & HAP
American College of Surgeons Critical Care Review Course 2012: Infection Control
 American College of Surgeons Critical Care Review Course 2012: Infection Control Overview: I. Central line associated blood stream infection (CLABSI) II. Ventilator associated pneumonia (VAP) I. Central
American College of Surgeons Critical Care Review Course 2012: Infection Control Overview: I. Central line associated blood stream infection (CLABSI) II. Ventilator associated pneumonia (VAP) I. Central
Tied with pneumonia as the second most common type of healthcareassociated
 Tied with pneumonia as the second most common type of healthcareassociated infection. > 15% of HAIs reported to NHSN Estimated > 560,000 nosocomial UTIs annually Increased morbidity & mortality Estimated
Tied with pneumonia as the second most common type of healthcareassociated infection. > 15% of HAIs reported to NHSN Estimated > 560,000 nosocomial UTIs annually Increased morbidity & mortality Estimated
Process audit for SSI. CME on Infection Prevention & Control Breach Candy Hospital Trust
 Process audit for SSI CME on Infection Prevention & Control Breach Candy Hospital Trust Introduction SSIs are the most common healthcare-associated infection, accounting for 31% of all HAIs among hospitalized
Process audit for SSI CME on Infection Prevention & Control Breach Candy Hospital Trust Introduction SSIs are the most common healthcare-associated infection, accounting for 31% of all HAIs among hospitalized
Catheter Associated Urinary Tract Infection
 Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
UTI IN ELDERLY. Zeinab Naderpour
 UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
UTI IN ELDERLY Zeinab Naderpour Urinary tract infection (UTI) is the most frequent bacterial infection in elderly populations. While urinary infection in the elderly person is usually asymptomatic, symptomatic
2018 CNISP HAI Surveillance Case definitions
 2018 CNISP HAI Surveillance Case definitions The following case definitions for the surveillance of healthcare-associated infections (HAIs) are used by all acute-care hospitals that participate in the
2018 CNISP HAI Surveillance Case definitions The following case definitions for the surveillance of healthcare-associated infections (HAIs) are used by all acute-care hospitals that participate in the
9/18/2018. Clostridium Difficile: Updates on Diagnosis and Treatment. Clostridium difficile Infection (CDI) Clostridium difficile Infection (CDI)
 Clostridium difficile Infection (CDI)") Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Ventilator Associated
 Ventilator Associated Pneumonia: Key and Controversial Issues Christopher P. Michetti, MD, FACS Inova Fairfax Hospital, Falls Church, VA Forrest Dell Moore, MD, FACS Banner Healthcare System, Phoenix,
Ventilator Associated Pneumonia: Key and Controversial Issues Christopher P. Michetti, MD, FACS Inova Fairfax Hospital, Falls Church, VA Forrest Dell Moore, MD, FACS Banner Healthcare System, Phoenix,
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018
 Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
INFECTION PREVENTION AND CONTROL
 INFECTION PREVENTION AND CONTROL Health Care-Associated Infection (HAI) Definitions May 28, 2012 The Capital Health Infection Prevention Control (IPAC) department conducts ongoing surveillance reports
INFECTION PREVENTION AND CONTROL Health Care-Associated Infection (HAI) Definitions May 28, 2012 The Capital Health Infection Prevention Control (IPAC) department conducts ongoing surveillance reports
MICHIGAN MEDICINE GUIDELINES FOR TREATMENT OF URINARY TRACT INFECTIONS IN ADULTS
 When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
When to Order a Urine Culture: Asymptomatic bacteriuria is often treated unnecessarily, and accounts for a substantial burden of unnecessary antimicrobial use. National guidelines recommend against testing
HAIs in the USA. March 23, 2017 Department of Public Health Sciences. Infectious Disease Epidemiology BMTRY 713 (Healthcare Associated Infection )
") Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 17 Healthcare-Associated Infections (HAIs) Learning Objectives 1. Describe magnitude and implication of HAIs 2. Identify the main risk
Infectious Disease Epidemiology BMTRY 713 (A. Selassie, DrPH) Lecture 17 Healthcare-Associated Infections (HAIs) Learning Objectives 1. Describe magnitude and implication of HAIs 2. Identify the main risk
URINARY TRACT INFECTIONS 3 rd Y Med Students. Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan
 URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
URINARY TRACT INFECTIONS 3 rd Y Med Students Prof. Dr. Asem Shehabi Faculty of Medicine, University of Jordan Urinary Tract Infections-1 Normal urine is sterile.. It contains fluids, salts, and waste products,
Big five of your hospital
 Big five of your hospital Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Big five of your hospital Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Antisepsis Bath and Oral.. Should We Change Practice? DR AZMIN HUDA ABDUL RAHIM
 Antisepsis Bath and Oral.. Should We Change Practice? DR AZMIN HUDA ABDUL RAHIM Chlorhexidine Exposure in ICU Chlorhexidine gluconate Long acting topical antiseptic In use since 1954 Water soluble Remains
Antisepsis Bath and Oral.. Should We Change Practice? DR AZMIN HUDA ABDUL RAHIM Chlorhexidine Exposure in ICU Chlorhexidine gluconate Long acting topical antiseptic In use since 1954 Water soluble Remains
Advanced Training Program Infection Prevention and Control By Dr. Ahmad Farouk EBFM, MRCGP, CIC
 Advanced Training Program Infection Prevention and Control By Dr. Ahmad Farouk EBFM, MRCGP, CIC Tel: +973 172 80 8 50 Mobile: +973 343 58 323 Fax: +973 a 11446 Address: BMMI Tower, Office 1423, 14 th Floor,
Advanced Training Program Infection Prevention and Control By Dr. Ahmad Farouk EBFM, MRCGP, CIC Tel: +973 172 80 8 50 Mobile: +973 343 58 323 Fax: +973 a 11446 Address: BMMI Tower, Office 1423, 14 th Floor,
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 8-year surveillance (2017) Surgical site infections: prevention and treatment (2008) NICE guideline CG74 Summary of evidence from surveillance... 1 Research
Appendix A: Summary of evidence from surveillance 8-year surveillance (2017) Surgical site infections: prevention and treatment (2008) NICE guideline CG74 Summary of evidence from surveillance... 1 Research
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013
 Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest wit
 Potential for conflicts of interest wit") GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
Updated Clostridium difficile Treatment Guidelines
 Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY
 HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
HEALTHCARE-ASSOCIATED PNEUMONIA: EPIDEMIOLOGY, MICROBIOLOGY & PATHOPHYSIOLOGY David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health
Enpr-EMA PAEDIATRIC ANTIBIOTIC WORKING GROUP
 Enpr-EMA PAEDIATRIC ANTIBIOTIC WORKING GROUP Rationale and outlook Laura Folgori Clinical Research Fellow Paediatric Infectious Diseases Research Group St George s University of London RATIONALE The work
Enpr-EMA PAEDIATRIC ANTIBIOTIC WORKING GROUP Rationale and outlook Laura Folgori Clinical Research Fellow Paediatric Infectious Diseases Research Group St George s University of London RATIONALE The work
MICROBIOLOGICAL TESTING IN PICU
 MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
MICROBIOLOGICAL TESTING IN PICU This is a guideline for the taking of microbiological samples in PICU to diagnose or exclude infection. The diagnosis of infection requires: Ruling out non-infectious causes
Infection Control. Student Orientation
 Infection Control Student Orientation Basic, but important, Principles of Cross Transmission Presence of microorganisms on hands or in environment does not necessarily = cross transmission or infection
Infection Control Student Orientation Basic, but important, Principles of Cross Transmission Presence of microorganisms on hands or in environment does not necessarily = cross transmission or infection
Candiduria in ICU : when and how to treat? Dr. Debashis Dhar Dept of Critical Care and Emergency Medicine Sir Ganga Ram Hospital
 Candiduria in ICU : when and how to treat? Dr. Debashis Dhar Dept of Critical Care and Emergency Medicine Sir Ganga Ram Hospital Introduction Nosocomial bacteriuria or candiduria develops in up to 25%
Candiduria in ICU : when and how to treat? Dr. Debashis Dhar Dept of Critical Care and Emergency Medicine Sir Ganga Ram Hospital Introduction Nosocomial bacteriuria or candiduria develops in up to 25%
Los Angeles County Department of Public Health: Your Partner in CDI Prevention
 Los Angeles County Department of Public Health: Your Partner in CDI Prevention Dawn Terashita, MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health dterashita@ph.lacounty.gov
Los Angeles County Department of Public Health: Your Partner in CDI Prevention Dawn Terashita, MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health dterashita@ph.lacounty.gov
Central Venous Access Devices and Infection
 Central Venous Access Devices and Infection Dr Andrew Daley Microbiology & Infectious Diseases Women s & Children s Health Melbourne Background Types of infection! Local site infection! Blood stream infection!
Central Venous Access Devices and Infection Dr Andrew Daley Microbiology & Infectious Diseases Women s & Children s Health Melbourne Background Types of infection! Local site infection! Blood stream infection!
Treatment Regimens for Bacterial Urinary Tract Infections. Characteristic Pathogen. E. coli, S.saprophyticus P.mirabilis, K.
 HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
HEALTHSPAN URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12, 4-14 Key Stakeholders: IM, Urology, Next Review:
Surveillance report Published: 7 July 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Urinary tract infection in under 16s: diagnosis and management (2007) NICE guideline CG54 Surveillance report Published: 7 July 2016 nice.org.uk NICE 2016. All rights reserved.
Surveillance report 2016 Urinary tract infection in under 16s: diagnosis and management (2007) NICE guideline CG54 Surveillance report Published: 7 July 2016 nice.org.uk NICE 2016. All rights reserved.
CONSIDERATIONS IN UTI DETECTION AND POTENTIAL IMPACT ON ANTIBIOTIC STEWARDSHIP
 CONSIDERATIONS IN UTI DETECTION AND POTENTIAL IMPACT ON ANTIBIOTIC STEWARDSHIP ERIN H. GRAF, PHD, D(ABMM) Director, Infectious Disease Diagnostics Laboratory Assistant Professor, Clinical Pathology and
CONSIDERATIONS IN UTI DETECTION AND POTENTIAL IMPACT ON ANTIBIOTIC STEWARDSHIP ERIN H. GRAF, PHD, D(ABMM) Director, Infectious Disease Diagnostics Laboratory Assistant Professor, Clinical Pathology and
Sustained CAUTI and CLABSI Improvements Using a Bundled Approach
 Sustained CAUTI and CLABSI Improvements Using a Bundled Approach Experiences of a Level 1 Trauma Center Angela Booth-Jones, PHD, MS, CIC Director, Infection Prevention 1 2 3 Miami Valley Hospital MVH has
Sustained CAUTI and CLABSI Improvements Using a Bundled Approach Experiences of a Level 1 Trauma Center Angela Booth-Jones, PHD, MS, CIC Director, Infection Prevention 1 2 3 Miami Valley Hospital MVH has
CLOSTRIDIUM DIFICILE. Negin N Blattman Infectious Diseases Phoenix VA Healthcare System
 CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
Case 1. Which of the following would be next appropriate investigation/s regarding the pts diarrhoea?
 Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017)
 Week 52 (Ending 30/12/2017)") Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017) What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic spore forming bacillus. It is ubiquitous in nature and
Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017) What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic spore forming bacillus. It is ubiquitous in nature and
Methicillin-Resistant Staphylococcus aureus (MRSA) S urveillance Report 2008 Background Methods
 S urveillance Report 2008 Background Methods") Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Methicillin-Resistant Staphylococcus aureus (MRSA) Surveillance Report 2008 Oregon Active Bacterial Core Surveillance (ABCs) Office of Disease Prevention & Epidemiology Oregon Department of Human Services
Catheter-associated Urinary Tract Infection (CAUTI) Toolkit
 Toolkit") Activity C: ELC Prevention Collaboratives Catheter-associated Urinary Tract Infection (CAUTI) Toolkit Carolyn Gould, MD MSCR Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Activity C: ELC Prevention Collaboratives Catheter-associated Urinary Tract Infection (CAUTI) Toolkit Carolyn Gould, MD MSCR Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Infection control in Aged Residential Care Facilities. Dr Sally Roberts Clinical Advisor for IP&C Service, ADHB
 Infection control in Aged Residential Care Facilities Dr Sally Roberts Clinical Advisor for IP&C Service, ADHB Background Endemic infections Epidemic infections Managing outbreaks Administrative measures
Infection control in Aged Residential Care Facilities Dr Sally Roberts Clinical Advisor for IP&C Service, ADHB Background Endemic infections Epidemic infections Managing outbreaks Administrative measures
Catheter-Associated Urinary tract infections: What works in prevention? Anucha Apisarnthanarak, MD
 Catheter-Associated Urinary tract infections: What works in prevention? Anucha Apisarnthanarak, MD Financial disclosure Research Support: Baxter, Interimmune, Lily, Merck Sharpe Dohme, Wyeth Honoraria/Speaker
Catheter-Associated Urinary tract infections: What works in prevention? Anucha Apisarnthanarak, MD Financial disclosure Research Support: Baxter, Interimmune, Lily, Merck Sharpe Dohme, Wyeth Honoraria/Speaker
URINARY TRACT INFECTIONS
 URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
URINARY TRACT INFECTIONS Learning Objectives Identify signs and symptoms that may indicate presence of UTI (both complicated and uncomplicated) List common causative organisms and risk factors for UTIs
! Macrolide antibacterial. Fidaxomicin (Dificid ) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
 package labeling. Optimer Pharmaceuticals, Inc. May 2011.") Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Diagnosis of Ventilator- Associated Pneumonia: Where are we now?
 Diagnosis of Ventilator- Associated Pneumonia: Where are we now? Gary French Guy s & St. Thomas Hospital & King s College, London BSAC Guideline 2008 Masterton R, Galloway A, French G, Street M, Armstrong
Diagnosis of Ventilator- Associated Pneumonia: Where are we now? Gary French Guy s & St. Thomas Hospital & King s College, London BSAC Guideline 2008 Masterton R, Galloway A, French G, Street M, Armstrong
TMP/SMZ DS Ciprofloxacin Norfloxacin Ofloxacin Cefadroxil * 30 Amoxicilin 86* 19 25
 Evidence-Based Evaluation and Treatment of UTI UTI Prevalence Leslee L. Subak, MD Associate Professor Obstetrics, Gynecology & RS Epidemiology & Biostatistics University of California, San Francisco 50%
Evidence-Based Evaluation and Treatment of UTI UTI Prevalence Leslee L. Subak, MD Associate Professor Obstetrics, Gynecology & RS Epidemiology & Biostatistics University of California, San Francisco 50%
Overview of the WHO global guidelines for the prevention of surgical site infection
 Overview of the WHO global guidelines for the prevention of surgical site infection Dr. Mohamed Abbas, MD, MS Semmelweiss CEE Conference Budapest 08.03.2017 Outline of presentation General background Burden
Overview of the WHO global guidelines for the prevention of surgical site infection Dr. Mohamed Abbas, MD, MS Semmelweiss CEE Conference Budapest 08.03.2017 Outline of presentation General background Burden
'Diagnostic Stewardship for Urinary Tract Infections. Surbhi Leekha MBBS, MPH Associate Professor, UMSOM Medical Director, Infection Prevention, UMMC
 'Diagnostic Stewardship for Urinary Tract Infections Surbhi Leekha MBBS, MPH Associate Professor, UMSOM Medical Director, Infection Prevention, UMMC Objectives Describe the difference between asymptomatic
'Diagnostic Stewardship for Urinary Tract Infections Surbhi Leekha MBBS, MPH Associate Professor, UMSOM Medical Director, Infection Prevention, UMMC Objectives Describe the difference between asymptomatic
Urinary Tract Infections
 Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
Urinary Tract Infections Michelle Eslami, M.D., FACP Professor of Medicine Division of Geriatrics David Geffen SOM at UCLA Urinary Tract Infection (UTI) One of most common infections in outpatient and
March 3, To: Hospitals, Long Term Care Facilities, and Local Health Departments
 March 3, 2010 To: Hospitals, Long Term Care Facilities, and Local Health Departments From: NYSDOH Bureau of Healthcare Associated Infections HEALTH ADVISORY: GUIDANCE FOR PREVENTION AND CONTROL OF HEALTHCARE
March 3, 2010 To: Hospitals, Long Term Care Facilities, and Local Health Departments From: NYSDOH Bureau of Healthcare Associated Infections HEALTH ADVISORY: GUIDANCE FOR PREVENTION AND CONTROL OF HEALTHCARE
Prevention of Surgical Site Infections Pola Brenner and Patricio Nercelles
 Chapter 11 Prevention of Surgical Site Infections Pola Brenner and Patricio Nercelles Key points In many countries surgical site infections are the most common healthcare-associated infections accounting
Chapter 11 Prevention of Surgical Site Infections Pola Brenner and Patricio Nercelles Key points In many countries surgical site infections are the most common healthcare-associated infections accounting
DOWNLOAD OR READ : URINARY TRACT INFECTIONS IN CHILDREN PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : URINARY TRACT INFECTIONS IN CHILDREN PDF EBOOK EPUB MOBI Page 1 Page 2 urinary tract infections in children urinary tract infections in pdf urinary tract infections in children MID 11
DOWNLOAD OR READ : URINARY TRACT INFECTIONS IN CHILDREN PDF EBOOK EPUB MOBI Page 1 Page 2 urinary tract infections in children urinary tract infections in pdf urinary tract infections in children MID 11
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES
 MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
MDR AGENTS: RISK FACTORS AND THERAPEUTIC STRATEGIES 1 Marin H. Kollef, MD Professor of Medicine Virginia E. and Sam J. Golman Chair in Respiratory Intensive Care Medicine Washington University School of
Surgical Site Infections: the international guidelines for best practices and effective actions
 Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
Surgical Site Infections: the international guidelines for best practices and effective actions SSIs are the second most common type of adverse event occurring in hospitalised patients. SSIs have been
Diagnosis and Management of UTI s in Care Home Settings. To Dip or Not to Dip?
 Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Diagnosis and Management of UTI s in Care Home Settings To Dip or Not to Dip? 1 Key Summary Points: Treat the patient NOT the urine In people 65 years, asymptomatic bacteriuria is common. Treating does
Clostridium difficile
 Clostridium difficile Care Homes IPC Study Day Sue Barber Infection Prevention & Control Lead AV & Chiltern CCG s Clostridium difficile A spore forming Bacterium. Difficult to grow in the laboratory hence
Clostridium difficile Care Homes IPC Study Day Sue Barber Infection Prevention & Control Lead AV & Chiltern CCG s Clostridium difficile A spore forming Bacterium. Difficult to grow in the laboratory hence
Infection Prevention and Control in Long Term Care Part 2
 Infection Prevention and Control in Long Term Care Part 2 Course ID: 1029 - Credit Hours: 2 Author(s) Bonnie Chustz,RN, BSN WCC Disclosures None Accreditation KLA Education Services LLC is accredited by
Infection Prevention and Control in Long Term Care Part 2 Course ID: 1029 - Credit Hours: 2 Author(s) Bonnie Chustz,RN, BSN WCC Disclosures None Accreditation KLA Education Services LLC is accredited by
Updates to pharmacological management in the prevention of recurrent Clostridium difficile
 Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Infection Control: Surgical Site Infections
 Infection Control: Surgical Site Infections Infectious Disease Epidemiology Section Office of Public Health Louisiana Dept of Health & Hospitals 800-256-2748 www.oph.dhh.louisiana.gov Your taxes at work
Infection Control: Surgical Site Infections Infectious Disease Epidemiology Section Office of Public Health Louisiana Dept of Health & Hospitals 800-256-2748 www.oph.dhh.louisiana.gov Your taxes at work
SSI: Superficial and Deep Space Infections
 Goals of this Presentation SSI: Superficial and Deep Space Infections Discuss the problem of surgical site infection (SSI) in colorectal surgery Review the specific measures that may reduce the rate of
Goals of this Presentation SSI: Superficial and Deep Space Infections Discuss the problem of surgical site infection (SSI) in colorectal surgery Review the specific measures that may reduce the rate of
Infection control in aged care facilities 3 rd February 2019
 Infection control in aged care facilities 3 rd February 2019 A/Prof. Paul Griffin FRACP, FRCPA, FACTM, AFACHSM, FIML, MBBS, BSc(Hons) Infectious Diseases Physician and Clinical Microbiologist Director
Infection control in aged care facilities 3 rd February 2019 A/Prof. Paul Griffin FRACP, FRCPA, FACTM, AFACHSM, FIML, MBBS, BSc(Hons) Infectious Diseases Physician and Clinical Microbiologist Director
Lifting the lid on a difficile problem part 2 (Clinical) Evidence Based Practice. Problem in evolution (1) Problem in evolution (1) Interventions (2)
 Evidence Based Practice. Problem in evolution (1) Problem in evolution (1) Interventions (2)") Lifting the lid on a difficile problem part (Clinical) Dr Philip T Mannion Consultant Microbiologist, Rhyl Evidence Based Practice Antibiotic prescribing guidance Isolation policy Hand hygiene (soap and
Lifting the lid on a difficile problem part (Clinical) Dr Philip T Mannion Consultant Microbiologist, Rhyl Evidence Based Practice Antibiotic prescribing guidance Isolation policy Hand hygiene (soap and
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT
 Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
Care Guideline DRAFT for review cycle 08/02/17 CARE OF THE ADULT PNEUMONIA PATIENT Target Audience: All MHS employed providers within Primary Care, Urgent Care, and In-Hospital Care. The secondary audience
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018
 When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
When should UTIs be treated in the Elderly? Shelby L. Wentworth, MS4 University of Florida College of Medicine 29 AUG 2018 UTIs in Patients >/ 65 yo - Most common infectious illness [1]. - Urinary tract
KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE)
") KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12 Key Stakeholders: IM, Urology, Next
KAISER PERMANENTE OHIO URINARY TRACT INFECTIONS (ADULT FEMALE) Methodology: Evidence-Based Issue Date: 1-98 Champion: Internal Medicine Most Recent Review: 4-10, 4-12 Key Stakeholders: IM, Urology, Next
ASPIRES Urinary Tract Infection Algorithm
 ASPIRES Urinary Tract Infection Algorithm Dr. Jennifer Grant Dr. Tim Lau Donna Leung February 2013 VCH Antimicrobial Stewardship 1 Programme: Innovation, Research, Education & Safety KEY PRINCIPLES 1.
ASPIRES Urinary Tract Infection Algorithm Dr. Jennifer Grant Dr. Tim Lau Donna Leung February 2013 VCH Antimicrobial Stewardship 1 Programme: Innovation, Research, Education & Safety KEY PRINCIPLES 1.
CAP, HCAP, HAP, VAP. 1. In 1898, William Osler described community-acquired pneumonia as:
 1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
1. In 1898, William Osler described community-acquired pneumonia as: Brad Sharpe, M.D. Professor of Clinical Medicine Department of Medicine UCSF sharpeb@medicine.ucsf.edu I have no relevant financial
Update in Hospital Medicine. Update in Hospital Medicine 2009
 2009 Bradley A. Sharpe, MD UCSF Division of Hospital Medicine PE in Acute COPD Exacerbations Question: What is the prevalence of PE in patients with COPD who need hospitalization? Design: Systematic review,
2009 Bradley A. Sharpe, MD UCSF Division of Hospital Medicine PE in Acute COPD Exacerbations Question: What is the prevalence of PE in patients with COPD who need hospitalization? Design: Systematic review,
Infection Prevention & Control Core Skills Level 2
 Infection Prevention & Control Core Skills Level 2 Learning outcomes Risk assessment of patients Critical examination of the situation MRSA, CDT & CPE Ongoing challenges future-proofing infection control
Infection Prevention & Control Core Skills Level 2 Learning outcomes Risk assessment of patients Critical examination of the situation MRSA, CDT & CPE Ongoing challenges future-proofing infection control
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program
 Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Lanny Hsieh, M.D. Infectious Diseases Hospitalist Program Definition of Fever Arbitrary 38.0-38.4 (low grade may be significant in immunocompromised patients) > 38.5 (nurse will call you) Be aware of
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital
 Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Antibiotic Protocols for Paediatrics Steve Biko Academic Hospital Respiratory tract infections in children Uncomplicated URTI A child with a cold should not receive an antibiotic Paracetamol (15 mg/kg/dose
Catheter Associated Urinary Tract Infection
 Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
Catheter Associated Urinary Tract Infection Facts about CAUTI 12% to 16% of adult patients will receive a urinary catheter during hospitalization. 4 th most common HAI Accounts for more than 12% of acute
CASE SCENARIO EXERCISE
 påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
påçííáëü=pìêîéáää~ååé=çñ=eé~äíüå~êé ^ëëçåá~íéç=fåñéåíáçå=mêçöê~ããé CASE SCENARIO EXERCISE CATHETER-ASSOCIATED URINARY TRACT INFECTION SURVEILLANCE SCOTTISH SURVEILLANCE OF HEALTHCARE ASSOCIATED INFECTION
HEALTHCARE-ASSOCIATED PNEUMONIA: DIAGNOSIS, TREATMENT & PREVENTION
 HEALTHCARE-ASSOCIATED PNEUMONIA: DIAGNOSIS, TREATMENT & PREVENTION David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health Care Medical
HEALTHCARE-ASSOCIATED PNEUMONIA: DIAGNOSIS, TREATMENT & PREVENTION David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics, & Epidemiology Associate Chief Medical Officer, UNC Health Care Medical
1/21/2016. Overview. Significance
 Asymptomatic Bacteriuria: Myths, Magic and Management Christopher Ohl MD Professor of Medicine, Section on Infectious Diseases Wake Forest School of Medicine, Winston Salem, NC Slide credits to Katie Wallace,
Asymptomatic Bacteriuria: Myths, Magic and Management Christopher Ohl MD Professor of Medicine, Section on Infectious Diseases Wake Forest School of Medicine, Winston Salem, NC Slide credits to Katie Wallace,
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures
 Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Surgical Care, Pneumonia, Immunizations and Emergency Department Core Measures Audrey Paulman, MD, MMM Principal Clinical Coordinator & Jackie Trojan, RN, BSN Quality Improvement Advisor This material
Nancy Hailpern, Director, Regulatory Affairs K Street, NW, Suite 1000 Washington, DC 20005
 Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Summary of Infection Prevention Issues in the Centers for Medicare & Medicaid Services (CMS) FY 2014 Inpatient Prospective Payment System (IPPS) Final Rule Hospital Readmissions Reduction Program-Fiscal
Current Concepts in VAP: Stress Ulcer Prophylaxis & Probiotics. Deborah Cook
 Current Concepts in VAP: Stress Ulcer Prophylaxis & Probiotics Deborah Cook Objectives VAP The Old: Gastropulmonary route of infection The New: Microbiome modification Role of acid suppression Influence
Current Concepts in VAP: Stress Ulcer Prophylaxis & Probiotics Deborah Cook Objectives VAP The Old: Gastropulmonary route of infection The New: Microbiome modification Role of acid suppression Influence
GUIDELINE FOR THE MANAGEMENT OF ANTIBIOTIC- ASSOCIATED DIARRHOEA IN ADULTS
 GUIDELINE FOR THE MANAGEMENT OF ANTIBIOTIC- ASSOCIATED DIARRHOEA IN ADULTS Version 3.0 Date ratified May 2008 Review date May 2010 Ratified by NUH Antibiotic Guidelines Committee NUH Drugs and Therapeutics
GUIDELINE FOR THE MANAGEMENT OF ANTIBIOTIC- ASSOCIATED DIARRHOEA IN ADULTS Version 3.0 Date ratified May 2008 Review date May 2010 Ratified by NUH Antibiotic Guidelines Committee NUH Drugs and Therapeutics
O3_A2_A_Scientific Evidence
 O3_A2_A_Scientific Evidence PERFORMING URETHROVESICAL CATHETERIZATION (FOLEY PROBE) IN FEMALE PATIENTS Q1 Outcome When is urinary catheterization necessary in patients hospitalized in a palliative settings/facility?
O3_A2_A_Scientific Evidence PERFORMING URETHROVESICAL CATHETERIZATION (FOLEY PROBE) IN FEMALE PATIENTS Q1 Outcome When is urinary catheterization necessary in patients hospitalized in a palliative settings/facility?
LINKS OF INTEREST DISCLOSURE
 LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?
LINKS OF INTEREST DISCLOSURE Name of the speaker: Sarah L. Krein I have no link of interest. www.sf2h.net 7, 8 et 9 juin 2017 And what about getting rid of catheter-associated urinary tract infections?