Treating Cervical Dystonia. Atul T. Patel, MD, MHSA Vice President, Kansas City Bone & Joint Clinic Overland Park, KS
|
|
|
- Veronica Carroll
- 6 years ago
- Views:
Transcription

1 Treating Cervical Dystonia Atul T. Patel, MD, MHSA Vice President, Kansas City Bone & Joint Clinic Overland Park, KS
2 Disclosures Grant/Research support and Speaker s Bureau for Allegan plc, Merz Pharmaceuticals, LLC, and Ipsen Biopharmaceuticals, Inc.
3 Goals and Objectives To describe clinical aspects relevant to the diagnosis of cervical dystonia To provide the clinician with available options for treatment in patients with cervical dystonia To allow clinicians to determine the process of determining candidates for treatment of chemodenervation To provide clinicians with an introduction to techniques of botulinum toxin injections for cervical dystonia
4 Recognizing Dystonia A motor disorder characterized by inappropriate muscle contraction Sustained ( tonic ) contractions usually result in abnormal postures Irregular, unsustained ( clonic ) contractions often result in jerky movements may occur frequently enough to resemble tremor Both contraction types occur in consistent patterns characteristic of each individual Both are often present simultaneously
5 Recognizing Dystonia Multichannel electrophysiological characteristics Co-contraction: simultaneous activation of antagonistic muscles Overflow: recruitment of muscles not normally involved in specific actions Electrophysiological analysis not used in routine clinical practice No definitive diagnostic laboratory tests Other than DNA analysis of genetic forms
6 Recognizing Cervical Dystonia Cervical dystonia (CD) a.k.a. spasmodic torticollis A focal form of dystonia involving the neck the most common area of the body affected by dystonia Featuring head postures and movements produced by dystonic cervical muscles Direction(s) of movement determined by specific muscles involved
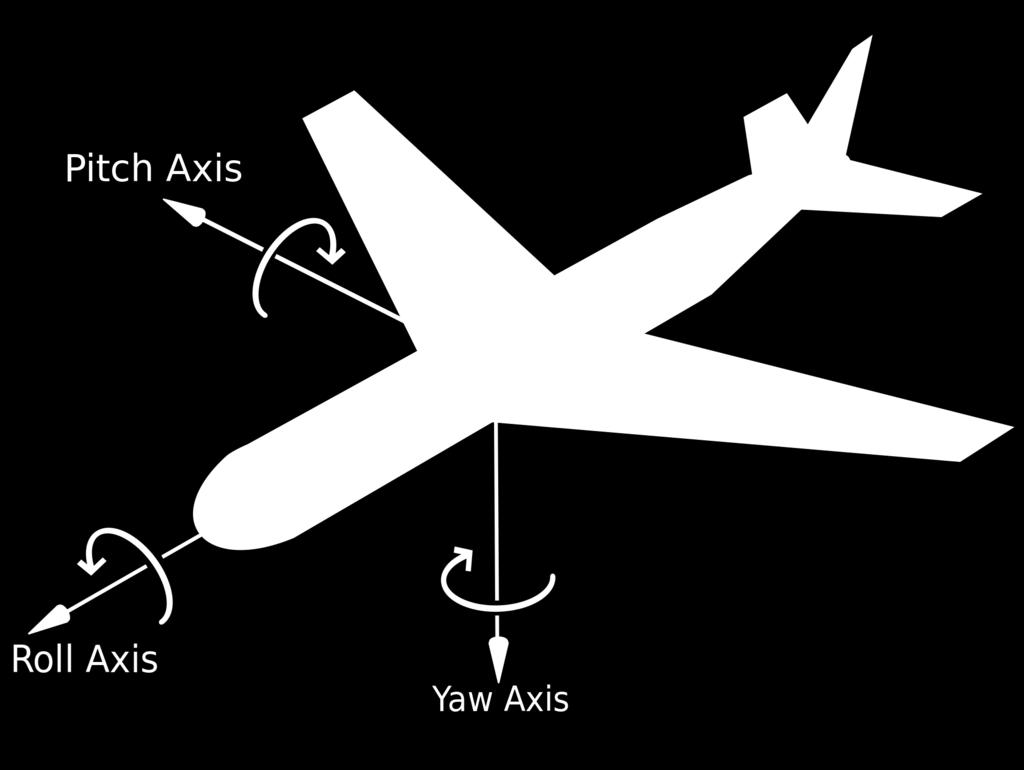
7 Recognizing Cervical Dystonia Head movement may involve any combination of 3 directional planes, plus horizontal shifts : Flexion/extension ( pitch ) Right/left rotation ( yaw ) Right/left tilt ( roll ) Horizontal shifts anterior/posterior (A-P) lateral right/left Cartoon of aircraft illustrating 3 vectors of movement


8 Internet images of vectors of movement

9 Head Postures in CD Torticollis 82% 97% Laterocollis 42% 63% Retrocollis 29% 32% Anterocollis 14% 25% Most pa(ents exhibit a combina(on of these postures
10 Head Postures in CD
11 Cervical Dystonia - Clinical Features Sensory tricks Physical maneuvers or gestures that ameliorate dystonia in a way that cannot be explained by simple opposition to the dystonic movement Approximately 75% of cervical dystonia patients report sensory tricks Although called sensory, the mechanism by which they work is unknown Llaneza Ramos V, et al. J Neurol Neurosurg Psychiatry. 2014: 85:
12 Cervical Dystonia - Clinical Features Pain CD and limb dystonia are the only focal dystonias that commonly cause pain About 2/3 of CD patients experience significant pain For many CD patients, pain is their most bothersome symptom
13 Examination for Cervical Dystonia Observe spontaneous head movements during history-taking Ask the patient not to oppose the dystonia Observe head and shoulder posture Rotation/tilt/lateral shift from front view Flexion/extension/anteroposterior shift from side view Observe symmetry of muscle mass Examine range of neck motion in 3 planes Observe any directional limitation Observe any rotation or tilt on neck extension Examine postures and movements while walking Observe shoulder posture from posterior view Examine for dystonia in other body regions
14 Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) 85-point maximum standard rating scale for severity of CD used in clinical studies Multiple scores assigned for 3 different aspects of CD 1. Objective head movements/postures 2. Subjective disability 3. Pain Time-consuming; not often used in routine clinical practice
15 Differential Diagnosis of CD Consists of disorders that cause: Neck pain Numerous musculoskeletal causes Cervical arthritis often coexists with CD Abnormal head postures/movements Also may have musculoskeletal origins The most common movement disorder mimicking CD is essential tremor (ET) 50% of ET patients have head tremor
16 Differential Diagnosis Essential Tremor Cervical dystonia Tonic and/or irregular clonic movement Directional head posture Usually directional range of motion restriction Pain often prominent Upper limb tremor absent or not prominent Essential tremor Regular, rhythmic oscillation Neutral head position No restriction of range of motion No pain Prominent postural and kinetic upper limb tremor
17 Cervical Dystonia Delayed Diagnosis Despite the fact that: CD appears to be a distinctive syndrome CD is the most common form of dystonia Many patients encounter a delay in diagnosis in recently diagnosed ( ) CD cases: mean time to diagnosis was 14.8 months after seeing a mean of 3.0 providers Tiderington E, et al. J Neurol Sci. 2013; 335: Timely identification of cervical dystonia requires clinical knowledge and vigilance
18 Epidemiology & Disease Course Mean age of onset ~ 42 years Women : men = 2:1 Typical disease course 1. Insidious onset 2. Progression over 5-10 years 3. Stabilization
19 Etiology Heredity ~ 10% of CD patients have a positive family history 3 known genetic forms: DYT23, DYT24, DYT25 other genetic forms of dystonia may present with CD Identifiable non-hereditary causes include: Acute dystonia secondary to anti-dopaminergic drugs Tardive dystonia Trauma Congenital But most cases are sporadic and idiopathic
20 Management Education regarding limits of knowledge Unknown: what causes CD or how to cure it Unknown: what is wrong in the CNS or how to fix it Symptomatic nature of treatment Treatment is aimed at reducing abnormal muscle contractions Non-curative, need for ongoing therapy Discuss realistic goals of treatment Establish patient priorities re symptoms Discuss success rates and risks associated with each treatment modality
21 Potential Goals of CD Treatment Normalization of head posture Reduce reliance on sensory tricks Reduction of clonic movements Relief of pain Successful pain relief may produce patient satisfaction, regardless of effects on head posture Reduction of disability Record scope and severity prior to initiation of treatment
22 CD Treatment Options Oral medications Botulinum toxin injections Surgery Other
23 Oral Medications for CD Drugs reported to be useful in CD: Anticholinergic drugs trihexyphenidyl, diphenhydramine, benztropine, others Benzodiazepines clonazepam, others Baclofen Levodopa, dopamine agonists Tetrabenazine (presynaptic dopamine depletor) Dopamine antagonists Others All drugs are designed and approved for other indications None are FDA-approved for dystonia Utility in dystonia discovered by trial and error, or happenstance The sheer variety underlines our lack of understanding of the pathopysiology of CD Antagonistic drugs suggest different pathophysiologies in different individuals
24 Oral Medications for CD No oral medication provides adequate monotherapy for a majority of individuals with CD Oral drug therapy consists of sequential trials of medications, hoping to find one that benefits Benefit is usually only partial, with significant residual symptoms and disability Side effects are common Bottom line: Few patients are content with oral medication therapy alone But patients often find them useful as adjuncts
25 Botulinum Toxin for CD Botulinum toxin (BT) is the treatment of choice for CD Efficacy and safety established in multiple DBPC trials More effective than any other option Fewer side effects than oral medications Much less risky than brain surgery Limitations: More costly than most oral medications Benefits wear off after several months; thus repeated injections are necessary for ongoing symptom control
26 Botulinum Toxin for CD Four available BT preparations Botox (onabotulinumtoxin A) Dysport (abobotulinumtoxin A) Myobloc (rimabotulinumtoxin B) Xeomin (incobotulinumtoxin A) CD is the only indication for which all 4 toxins have been FDA-approved No accepted dose equivalence or conversion ratio between different toxin preparations Few head-to-head studies Clinical experience suggests they are equally effective for CD
27 Botulinum Toxin for CD BT works by preventing acetylcholine release at the neuromuscular junction A process known as chemodenervation BT action depends on incorporation into motor neuron terminals in target muscles Thus successful treatment with BT depends on: 1. Proper identification of muscles involved in CD 2. Selecting an appropriate dose of toxin 3. Delivering the toxin where it can reach the neuromuscular junction
28 Identification of Muscles Involved in CD Based on: Patient reporting of: Direction of involuntary movement/pulling sensation Spontaneous pain Observation of: Head/shoulder posture and spontaneous movement Muscle mass Range of motion Palpation for hypertrophy, clonic contractions, and tenderness Knowledge of: Cervical muscle anatomy Mechanical action of major muscles contributing to head deviation(s)
29 Muscles Most Often Injected for CD CD PROBE: observational study of 1,041 CD patients undergoing BT therapy Charles D, et al. 2014; pdf/poster_00061.pdf Muscles most often injected: Splenius capitis (86.1%) Sternocleidomastoid (76.9%) Levator scapulae (67.3%) Trapezius (63.6%) all others under 33%
30 Selecting an Appropriate Dose of BT Must be tailored to the individual patient based on: Severity of head and neck deviation Localization of pain Muscle bulk Age Response to prior injections Initial dosing in a naive patient should begin conservatively
31 Selecting an Appropriate Dose of BT Manufacturers' recommended dose ranges for cervical dystonia: Muscle Botox Dysport Myobloc Levator scapulae U U 1,000-2,500 U Splenius capitis U U 1,000-2,500 U Sternocleidomastoid U U 1,000-2,500 U Trapezius U U 1,000-2,500 U Scalene complex U U 500-1,000 U Semispinalis capitis U U 1,000-2,500 U The manufacturers of Xeomin state only "The recommended initial total dose of XEOMIN for cervical dystonia is 120 Units" without individual muscle recommendations
32 Delivering the Toxin Motor nerve terminals are mainly located near the midpoint between the origin and insertion Thus toxin delivery should be concentrated around the central region of the muscle In many CD patients, specific musculature can be identified by surface inspection or by palpation

33 Cervical Muscles Surface Anatomy Splenius capitis Trapezius Sternocleidomastoid Levator scapulae
34 Delivering the Toxin In other patients, particularly with considerable adipose tissue or for less frequently injected muscles, muscle detection may require assistance Electromyography Detects muscular tissue and active contraction Does not distinguish between muscles Ultrasound Allows visual confirmation of muscle injection Especially useful to distinguish layered muscles Both techniques require thorough knowledge of neck muscle anatomy
35 Botulinum Toxin for CD A key aspect of BT treatment is an informed patient Discussions should include: Time course of benefit Onset mean (7 days) and range (1-14 days) Time to maximum benefit (up to 3 weeks) Duration of benefit (ideally 3 months or more) Specific expected benefits Allows patients to make/report pertinent observations about type, magnitude and duration of effects Potential side effects Costs and insurance coverage
36 Botulinum Toxin for CD Additional topics for discussion with patients: Trial and error approach to BT therapy Determining the appropriate muscles and doses may require multiple sets of injections to fine-tune First injections based on what is known generally about BT Subsequent injections guided by the individual s prior responses Options available to improve results include: Increasing doses, changing muscles to increase benefit Decreasing doses, changing muscles to minimize side effects Adding muscle localization technology (EMG, ultrasound) Changing toxins
37 Side Effects of Botulinum Toxin for CD Excess weakness of targeted muscles Patients may report head heaviness, or difficulty raising head when bending or lying down Diffusion of toxin leading to weakness in nontargeted muscles Dysphagia is common with injection of anterior cervical muscles Atrophy, similar to anatomic denervation Most visible in sternocleidomastoid Development of immune resistance Occurs after repeated injections Associated with short interinjection intervals, high doses
38 Surgical Options for CD Surgery is the riskiest and costliest option Reserved for CD patients who fail to respond adequately to BT or oral medications Success rates fall between those for BT and those for oral medications Two procedures: Deep brain stimulation (DBS) Selective denervation (SD)
39 Surgical Options for CD Deep brain stimulation (DBS) Pulsatile electrical stimulation of bilateral globus pallidus internus via implanted electrodes Prospective study 10 patients refractory to BT followed for 5 years Mean total TWSTRS improvement: 54.5 ± 27.4% but only 3/9 had > 50% improvement in pain scores Blinded video mean improvement: 47.6 ± 15.4% 2 patients required lead replacement for infection: Improvement mostly sustained by unilateral stimulation for 3 and 2 years respectively 3 patients developed micrographia, 2 dysarthria Walsh R, et al. Brain. 2013; 136:
40 Surgical Options for CD Selective denervation (SD) Surgical destruction of peripheral innervation of muscles deemed to be involved in CD Prospective study 68% of 37 patients who failed BT obtained meaningful benefit from SD Mean magnitude of benefit was 20-40% on the three TWSTRS subscores 37.5% developed dysphagia, mostly transient Reinnervation was detected within 6-12 months in 45% of sternocleidomastoids and 20% of splenii Münchau A, et al. Brain. 2001; 124:
41 Other Treatments for CD Physical therapy (PT) Stretching exercises may improve range of motion But PT has a limited role in dystonia Essentially, dystonic muscles already get too much exercise; what they need is something to relax them
42 Other Treatments for CD Anecdotal reports of benefit for: Acupuncture Massage Mindfulness/meditation Hypnosis Yoga Numerous disciplines described online But formal clinical studies are lacking
43 Conclusions Cervical dystonia is a clinical diagnosis Awareness by physicians leads to prompt diagnosis Management is symptomatic Engaged interaction with patients is key to success Botulinum toxin injections are the treatment of choice Proper application requires knowledge of anatomy, toxin dosages, and technical proficiency Other treatments are potentially useful
Hubert H. Fernandez, MD
 Hubert H. Fernandez, MD Associate Professor Co-Director, Movement Disorders Center Director, Clinical Trials for Movement Disorders Program Director, Neurology Residency and Movement Disorders Fellowship
Hubert H. Fernandez, MD Associate Professor Co-Director, Movement Disorders Center Director, Clinical Trials for Movement Disorders Program Director, Neurology Residency and Movement Disorders Fellowship
Dystonia: Title. A real pain in the neck. in All the Wrong Places
 Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Quantitative Assessment of Botulinum Toxin Treatment in 43 Patients with Head Tremor
 ~~~~~ ~ ~ Movement Disorder& Vol. 12, NO. 5, 1997, pp 122-126 0 1997 Movemcnt Disorder Society Quantitative Assessment of Botulinum Toxin Treatment in 43 Patients with Head Tremor "tjorg Wissel, "Florian
~~~~~ ~ ~ Movement Disorder& Vol. 12, NO. 5, 1997, pp 122-126 0 1997 Movemcnt Disorder Society Quantitative Assessment of Botulinum Toxin Treatment in 43 Patients with Head Tremor "tjorg Wissel, "Florian
Cervical dystonia is a form of abnormal movement characterized by abnormal head and neck posi8on caused by involuntary contrac8on of neck muscles.
 1 Cervical dystonia is a form of abnormal movement characterized by abnormal head and neck posi8on caused by involuntary contrac8on of neck muscles. This may result in sustained abnormal posi8on or jerky
1 Cervical dystonia is a form of abnormal movement characterized by abnormal head and neck posi8on caused by involuntary contrac8on of neck muscles. This may result in sustained abnormal posi8on or jerky
Scottish Medicines Consortium
 Scottish Medicines Consortium clostridium botulinum neurotoxin type A, 100 unit powder for solution for injection (Xeomin ) No. (464/08) Merz Pharma UK Ltd 09 May 2008 The Scottish Medicines Consortium
Scottish Medicines Consortium clostridium botulinum neurotoxin type A, 100 unit powder for solution for injection (Xeomin ) No. (464/08) Merz Pharma UK Ltd 09 May 2008 The Scottish Medicines Consortium
Journal of Anesthesia & Pain Medicine
 Case Report To spasm, or Not to Spasm, That is the Question Journal of Anesthesia & Pain Medicine John C McDonald BA 1 and Terence K Gray DO 1,2* 1 Mercy Pain Center, Mercy Hospital, Portland, Maine, USA
Case Report To spasm, or Not to Spasm, That is the Question Journal of Anesthesia & Pain Medicine John C McDonald BA 1 and Terence K Gray DO 1,2* 1 Mercy Pain Center, Mercy Hospital, Portland, Maine, USA
THE CLINICAL USE OF BOTULINUM TOXIN IN THE TREATMENT OF MOVEMENT DISORDERS, SPASTICITY, AND SOFT TISSUE PAIN
 THE CLINICAL USE OF BOTULINUM TOXIN IN THE TREATMENT OF MOVEMENT DISORDERS, SPASTICITY, AND SOFT TISSUE PAIN Spasmodic torticollis (cervical dystonia), blepharospasm, and writer s cramp are specific types
THE CLINICAL USE OF BOTULINUM TOXIN IN THE TREATMENT OF MOVEMENT DISORDERS, SPASTICITY, AND SOFT TISSUE PAIN Spasmodic torticollis (cervical dystonia), blepharospasm, and writer s cramp are specific types
Deep Brain Stimulation: Patient selection
 Deep Brain Stimulation: Patient selection Halim Fadil, MD Movement Disorders Neurologist Kane Hall Barry Neurology Bedford/Keller, TX 1991: Thalamic (Vim) DBS for tremor Benabid AL, et al. Lancet. 1991;337(8738):403-406.
Deep Brain Stimulation: Patient selection Halim Fadil, MD Movement Disorders Neurologist Kane Hall Barry Neurology Bedford/Keller, TX 1991: Thalamic (Vim) DBS for tremor Benabid AL, et al. Lancet. 1991;337(8738):403-406.
Botulinum Toxin Therapy Billing & Coding Update 2016
 Botulinum Toxin Therapy Billing & Coding Update 2016 Martin Taylor, DO, PhD Neurology / OrthoNeuro Clinical Associate Professor, Neurology Ohio University College of Osteopathic Medicine Columbus, OH Disclosures
Botulinum Toxin Therapy Billing & Coding Update 2016 Martin Taylor, DO, PhD Neurology / OrthoNeuro Clinical Associate Professor, Neurology Ohio University College of Osteopathic Medicine Columbus, OH Disclosures
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Xeomin) Reference Number: CP.PHAR.231 Effective Date: 07.01.16 Last Review Date 05.18 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Xeomin) Reference Number: CP.PHAR.231 Effective Date: 07.01.16 Last Review Date 05.18 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
Understanding Dystonia
 Understanding Dystonia Sand Sharks Anthony Richardsen, Lindsey Rathbun, Evan Harrington, Chris Erzen The Essentials What, Why, How What is Dystonia? Dystonias are movement disorders often characterized
Understanding Dystonia Sand Sharks Anthony Richardsen, Lindsey Rathbun, Evan Harrington, Chris Erzen The Essentials What, Why, How What is Dystonia? Dystonias are movement disorders often characterized
This guide describes some of the important facts about Neurobloc that you need to be aware of, however, it does not replace the advice given to you
 This guide describes some of the important facts about Neurobloc that you need to be aware of, however, it does not replace the advice given to you by a healthcare professional. Further very important
This guide describes some of the important facts about Neurobloc that you need to be aware of, however, it does not replace the advice given to you by a healthcare professional. Further very important
Ms Anne Recordon. Physiotherapist Neuro Rehab Results Queenstown
 Ms Anne Recordon Physiotherapist Neuro Rehab Results Queenstown 14:00-14:55 WS #106: Managing Dystonia in Children and Adults 15:05-16:00 WS #117: Managing Dystonia in Children and Adults (Repeated) Dystonia
Ms Anne Recordon Physiotherapist Neuro Rehab Results Queenstown 14:00-14:55 WS #106: Managing Dystonia in Children and Adults 15:05-16:00 WS #117: Managing Dystonia in Children and Adults (Repeated) Dystonia
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Dysport) Reference Number: CP.PHAR.230 Effective Date: 07.01.16 Last Review Date: 05.18 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Dysport) Reference Number: CP.PHAR.230 Effective Date: 07.01.16 Last Review Date: 05.18 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: IncobotulinumtoxinA (Xeomin) Reference Number: ERX.SPA.194 Effective Date:
 Reference Number: ERX.SPA.194 Effective Date:") Clinical Policy: (Xeomin) Reference Number: ERX.SPA.194 Effective Date: 01.11.17 Last Review Date: 11.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Xeomin) Reference Number: ERX.SPA.194 Effective Date: 01.11.17 Last Review Date: 11.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Source: *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD
 Source: http://www.medicinenet.com/script/main/art.asp?articlekey=349 Dystonia facts* *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD Dystonia is a disorder of muscle control; it can
Source: http://www.medicinenet.com/script/main/art.asp?articlekey=349 Dystonia facts* *Dystonia facts medically edited by: Charles Patrick Davis, MD, PhD Dystonia is a disorder of muscle control; it can
Pallidal Deep Brain Stimulation
 Pallidal Deep Brain Stimulation Treatment for Dystonia Dystonia Dystonia is a neurological disorder characterized by involuntary muscle contractions resulting in abnormal postures. These movements may
Pallidal Deep Brain Stimulation Treatment for Dystonia Dystonia Dystonia is a neurological disorder characterized by involuntary muscle contractions resulting in abnormal postures. These movements may
Deep Brain Stimulation: Indications and Ethical Applications
 Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
MYOBLOC and Cervical Dystonia A Patient s Guide
 MYOBLOC and Cervical Dystonia A Patient s Guide MYOBLOC (rimabotulinumtoxinb) Injection is indicated for the treatment of adults with cervical dystonia to reduce the severity of abnormal head position
MYOBLOC and Cervical Dystonia A Patient s Guide MYOBLOC (rimabotulinumtoxinb) Injection is indicated for the treatment of adults with cervical dystonia to reduce the severity of abnormal head position
THE MEDICAL AND SURGICAL TREATMENT OF DYSTONIA
 THE MEDICAL AND SURGICAL TREATMENT OF DYSTONIA Samuel Frank, MD Beth Israel Deaconess Medical Center Boston, MA Dystonia may present as an isolated disorder or as part of another disease process. The clinical
THE MEDICAL AND SURGICAL TREATMENT OF DYSTONIA Samuel Frank, MD Beth Israel Deaconess Medical Center Boston, MA Dystonia may present as an isolated disorder or as part of another disease process. The clinical
Clinical Policy: IncobotulinumtoxinA (Xeomin) Reference Number: CP.PHAR.231
 Reference Number: CP.PHAR.231") Clinical Policy: (Xeomin) Reference Number: CP.PHAR.231 Effective Date: 07/16 Last Review Date: 07/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Xeomin) Reference Number: CP.PHAR.231 Effective Date: 07/16 Last Review Date: 07/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Myobloc) Reference Number: CP.PHAR.233 Effective Date: 07.01.16 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Myobloc) Reference Number: CP.PHAR.233 Effective Date: 07.01.16 Last Review Date: 05.18 Line of Business: Commercial, Medicaid Coding Implications Revision Log See Important Reminder
Neurological disorders. Dystonia Search date September 2013 Ailsa Snaith and Derick Wade ...
 Search date September 213 Ailsa Snaith and Derick Wade.................................................. ABSTRACT INTRODUCTION: is usually a lifelong condition with persistent pain and disability. Focal
Search date September 213 Ailsa Snaith and Derick Wade.................................................. ABSTRACT INTRODUCTION: is usually a lifelong condition with persistent pain and disability. Focal
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Pearce, Catharine. Downloaded 22-Oct :14:
 Is using a patient s estimated lean body mass a suitable method of predicting their eventual therapeutic units of botulinum toxin for the treatment of cervical dystonia? Item type Authors Other Pearce,
Is using a patient s estimated lean body mass a suitable method of predicting their eventual therapeutic units of botulinum toxin for the treatment of cervical dystonia? Item type Authors Other Pearce,
Cervical Dystonia. One type of dystonia Julie Rope
 Cervical Dystonia One type of dystonia Julie Rope Cervical Dystonia Patterned, repetitive, and spasmodic or sustained muscle contractions resulting in abnormal movements and postures of the head and neck
Cervical Dystonia One type of dystonia Julie Rope Cervical Dystonia Patterned, repetitive, and spasmodic or sustained muscle contractions resulting in abnormal movements and postures of the head and neck
Dystonias Peter McAllister, MD
 Dystonias Peter McAllister, MD Medical Director, New England Institute for Neurology and Headache Chief Medical Officer, New England Institute for Clinical Research Clinical Assistant Professor, Neurology,
Dystonias Peter McAllister, MD Medical Director, New England Institute for Neurology and Headache Chief Medical Officer, New England Institute for Clinical Research Clinical Assistant Professor, Neurology,
Parkinson's Disease Center and Movement Disorders Clinic
 Parkinson's Disease Center and Movement Disorders Clinic 7200 Cambridge Street, 9th Floor, Suite 9A Houston, Texas 77030 713-798-2273 phone www.jankovic.org Dystonia Diagnosis Dystonia is a neurologic
Parkinson's Disease Center and Movement Disorders Clinic 7200 Cambridge Street, 9th Floor, Suite 9A Houston, Texas 77030 713-798-2273 phone www.jankovic.org Dystonia Diagnosis Dystonia is a neurologic
Management of Spasticity
 Management of Spasticity Stephen P. Moran, M.D. Department of Physical Medicine and Rehabilitation Ochsner Medical Center Outline Review pathophysiology of spasticity Discuss epidemiology of spasticity
Management of Spasticity Stephen P. Moran, M.D. Department of Physical Medicine and Rehabilitation Ochsner Medical Center Outline Review pathophysiology of spasticity Discuss epidemiology of spasticity
GENETICS AND TREATMENT OF DYSTONIA
 GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
GENETICS AND TREATMENT OF DYSTONIA Oksana Suchowersky, M.D., FRCPC, FCCMG Professor of Medicine, Medical Genetics, and Psychiatry Toupin Research Chair in Neurology DYSTONIA Definition: abnormal sustained
Dystonia. The condition can vary from very mild to severe. Dystonia may get worse over time or it may stay the same or get better.
 Dystonia What are movement disorders? Movement disorders are conditions that cause involuntary body movements. With all movement disorders, abnormal signals from the brain cause patients to have trouble
Dystonia What are movement disorders? Movement disorders are conditions that cause involuntary body movements. With all movement disorders, abnormal signals from the brain cause patients to have trouble
Original Article. Annals of Rehabilitation Medicine INTRODUCTION
 Original Article Ann Rehabil Med 2013;37(6):777-784 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2013.37.6.777 Annals of Rehabilitation Medicine Threshold of Clinical Severity of Cervical
Original Article Ann Rehabil Med 2013;37(6):777-784 pissn: 2234-0645 eissn: 2234-0653 http://dx.doi.org/10.5535/arm.2013.37.6.777 Annals of Rehabilitation Medicine Threshold of Clinical Severity of Cervical
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Botulinum toxin type A in the treatment of patients with cervical dystonia
 REVIEW Botulinum toxin type A in the treatment of patients with cervical dystonia Allison Brashear Dept of Neurology, Wake Forest University Baptist, Medical Center, Winston Salem, NC, USA Correspondence:
REVIEW Botulinum toxin type A in the treatment of patients with cervical dystonia Allison Brashear Dept of Neurology, Wake Forest University Baptist, Medical Center, Winston Salem, NC, USA Correspondence:
TREATMENT OF CHRONIC MECHANICAL NECK PAIN IN AN OUTPATIENT ORTHOPEDIC SETTING
 TREATMENT OF CHRONIC MECHANICAL NECK PAIN IN AN OUTPATIENT ORTHOPEDIC SETTING Clinical Problem Solving II Allison Walsh PATIENT OVERVIEW Age: 22 years Gender: Female Chief Complaint: Cervical pain, cervicogenic
TREATMENT OF CHRONIC MECHANICAL NECK PAIN IN AN OUTPATIENT ORTHOPEDIC SETTING Clinical Problem Solving II Allison Walsh PATIENT OVERVIEW Age: 22 years Gender: Female Chief Complaint: Cervical pain, cervicogenic
Tremor 101. Objectives 9/30/2015. Importance of tremors
 Tremor 101 Umer Akbar, MD Assistant Professor, Brown University Movement Disorders Program, Rhode Island Hospital & Butler Hospital Objectives Recognize and describe the qualities of common types of tremor
Tremor 101 Umer Akbar, MD Assistant Professor, Brown University Movement Disorders Program, Rhode Island Hospital & Butler Hospital Objectives Recognize and describe the qualities of common types of tremor
CEDAC FINAL RECOMMENDATION
 CEDAC FINAL RECOMMENDATION CLOSTRIDIUM BOTULINUM NEUROTOXIN TYPE A, FREE FROM COMPLEXING PROTEINS (Xeomin Merz Pharma Canada Ltd.) Indication: Blepharospasm Recommendation: The Canadian Expert Drug Advisory
CEDAC FINAL RECOMMENDATION CLOSTRIDIUM BOTULINUM NEUROTOXIN TYPE A, FREE FROM COMPLEXING PROTEINS (Xeomin Merz Pharma Canada Ltd.) Indication: Blepharospasm Recommendation: The Canadian Expert Drug Advisory
82a Orthopedic Massage! Introduction - Thoracic Outlet"
 82a Orthopedic Massage! Introduction - Thoracic Outlet" 82a Orthopedic Massage! Introduction - Thoracic Outlet! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
82a Orthopedic Massage! Introduction - Thoracic Outlet" 82a Orthopedic Massage! Introduction - Thoracic Outlet! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders " 10 minutes "Lecture:"
DEEP BRAIN STIMULATION
 DEEP BRAIN STIMULATION Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
DEEP BRAIN STIMULATION Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
R AT I N G S C A L E S. CODING/BILLING.
 Paieška Paieška Paieška Cpt code for botox injection into the splenius capitis Cpt code for botox injection into the splenius capitis > > Correct coding using current procedural terminology (CPT) and International.
Paieška Paieška Paieška Cpt code for botox injection into the splenius capitis Cpt code for botox injection into the splenius capitis > > Correct coding using current procedural terminology (CPT) and International.
Neuromuscular Blocking Agents
 Neuromuscular Blocking Agents DRUG POLICY This Prior Authorization request will be reviewed for medical necessity only. Benefits are subject to the terms and conditions of the patient s contract. Please
Neuromuscular Blocking Agents DRUG POLICY This Prior Authorization request will be reviewed for medical necessity only. Benefits are subject to the terms and conditions of the patient s contract. Please
Patient selection for surgery: Hyperkinetic movement disorders
 Patient selection for surgery: Hyperkinetic movement disorders Alfons Schnitzler, MD, PhD Dept. of Neurology, Movement Disorder and Neuromodulation, Heinrich-Heine-University Düsseldorf, Germany Hyperkinetic
Patient selection for surgery: Hyperkinetic movement disorders Alfons Schnitzler, MD, PhD Dept. of Neurology, Movement Disorder and Neuromodulation, Heinrich-Heine-University Düsseldorf, Germany Hyperkinetic
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Botuli focal d THERAPEUTIC INTERVENTION
 30 PRACTICAL NEUROLOGY THERAPEUTIC INTERVENTION The Little Milkmaid by Amedeo Modigliani (1884 1920). Does this represent artistic licence or cervical dystonia? Nigel Hyman Department of Neurology, Radcliffe
30 PRACTICAL NEUROLOGY THERAPEUTIC INTERVENTION The Little Milkmaid by Amedeo Modigliani (1884 1920). Does this represent artistic licence or cervical dystonia? Nigel Hyman Department of Neurology, Radcliffe
Deep brain s,mula,on refers to implan,ng electrodes into specific areas of the brain and hooking the electrodes up to pacemaker- like devices in
 1 Deep brain s,mula,on refers to implan,ng electrodes into specific areas of the brain and hooking the electrodes up to pacemaker- like devices in order to send signals into the brain to jam the abnormal
1 Deep brain s,mula,on refers to implan,ng electrodes into specific areas of the brain and hooking the electrodes up to pacemaker- like devices in order to send signals into the brain to jam the abnormal
85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain
 85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain 85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain! Class Outline 5 minutes Attendance, Breath of Arrival, and Reminders 10
85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain 85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain! Class Outline 5 minutes Attendance, Breath of Arrival, and Reminders 10
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
86b Orthopedic Massage:! Technique Review and Practice - Neck Pain
 86b Orthopedic Massage:! Technique Review and Practice - Neck Pain 86b Orthopedic Massage:! Technique Review and Practice - Neck Pain! Class Outline 5 minutes Attendance, Breath of Arrival, and Reminders
86b Orthopedic Massage:! Technique Review and Practice - Neck Pain 86b Orthopedic Massage:! Technique Review and Practice - Neck Pain! Class Outline 5 minutes Attendance, Breath of Arrival, and Reminders
85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain"
 85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain" 85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain" 85b Orthopedic Massage:! Technique Demo and Practice - Neck Pain! Class Outline" 5 minutes" "Attendance, Breath of Arrival, and Reminders
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Medication Prior Authorization Form
 (OnabotulinumtoxinA) Dysport (abobotulinumtoxina) Myobloc (rimabotulinumtoxinb) Xeomin (incobotulinumtoxina) Policy Number: 1042 Policy History Approve Date: 12/11/2015 Revise Dates: 7/7/2016 Next Review:
(OnabotulinumtoxinA) Dysport (abobotulinumtoxina) Myobloc (rimabotulinumtoxinb) Xeomin (incobotulinumtoxina) Policy Number: 1042 Policy History Approve Date: 12/11/2015 Revise Dates: 7/7/2016 Next Review:
Surgical Treatment for Movement Disorders
 Surgical Treatment for Movement Disorders Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence St Vincent
Surgical Treatment for Movement Disorders Seth F Oliveria, MD PhD The Oregon Clinic Neurosurgery Director of Functional Neurosurgery: Providence Brain and Spine Institute Portland, OR Providence St Vincent
PACEMAKERS ARE NOT JUST FOR THE HEART! Ab Siadati MD
 PACEMAKERS ARE NOT JUST FOR THE HEART! Ab Siadati MD WHAT IS DEEP BRAIN STIMULATION? WHY SHOULD YOU CONSIDER DBS SURGERY FOR YOUR PATIENTS? HOW DOES DBS WORK? DBS electrical stimulation overrides abnormal
PACEMAKERS ARE NOT JUST FOR THE HEART! Ab Siadati MD WHAT IS DEEP BRAIN STIMULATION? WHY SHOULD YOU CONSIDER DBS SURGERY FOR YOUR PATIENTS? HOW DOES DBS WORK? DBS electrical stimulation overrides abnormal
Table of Contents. 1.0 Description of the Procedure, Product, or Service Safety and Provider Compliance... 1
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Safety and Provider Compliance... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1 General... 1 2.1.2 Specific...
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Safety and Provider Compliance... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1 General... 1 2.1.2 Specific...
BOTULINUM TOXIN: RESEARCH ISSUES ARISING FROM PRACTICE
 % of baseline CMAP Botulinum toxin: mechanism of action BOTULINUM TOXIN: RESEARCH ISSUES ARISING FROM PRACTICE Clinical benefits of botulinum toxin (BT) injections depend primarily on the toxin's peripheral
% of baseline CMAP Botulinum toxin: mechanism of action BOTULINUM TOXIN: RESEARCH ISSUES ARISING FROM PRACTICE Clinical benefits of botulinum toxin (BT) injections depend primarily on the toxin's peripheral
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Treating Adults with Cervical Dystonia
 Treating Adults with Cervical Dystonia Learn more about Dysport Talk to your doctor about Dysport and find out if it is right for you. What is Dysport? Dysport is a prescription medicine that is injected
Treating Adults with Cervical Dystonia Learn more about Dysport Talk to your doctor about Dysport and find out if it is right for you. What is Dysport? Dysport is a prescription medicine that is injected
For Our Loved Ones. First Aid Massage
 For Our Loved Ones First Aid Massage First Aid Massage Introduction Communication Anatomy Basics Care: First Aid Massage Communication Where Ask where the pain is. Determine the anatomical location. What
For Our Loved Ones First Aid Massage First Aid Massage Introduction Communication Anatomy Basics Care: First Aid Massage Communication Where Ask where the pain is. Determine the anatomical location. What
Outcome of selective ramisectomy for botulinum toxin resistant torticollis
 472 Center for Dystonia, Neurological Institute, Columbia-Presbyterian Medical Center B Ford E D Louis P Greene S Fahn Sergievsky Center, Columbia University, New York, USA E D Louis Correspondence to:
472 Center for Dystonia, Neurological Institute, Columbia-Presbyterian Medical Center B Ford E D Louis P Greene S Fahn Sergievsky Center, Columbia University, New York, USA E D Louis Correspondence to:
Botox. Botox (onabotulinum toxin A) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.01 Subject: Botox Page: 1 of 8 Last Review Date: September 15, 2017 Botox Description Botox (onabotulinum
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.75.01 Subject: Botox Page: 1 of 8 Last Review Date: September 15, 2017 Botox Description Botox (onabotulinum
Changes in Cortical and Pallidal Oscillatory Activity during the Execution of a Sensory Trick in Patients with Cervical Dystonia
 Changes in Cortical and Pallidal Oscillatory Activity during the Execution of a Sensory Trick in Patients with Cervical Dystonia Joyce KH Tang 1 Neil Mahant 2 Danny Cunic 2 Robert Chen 2 Elena Moro 2 Anthony
Changes in Cortical and Pallidal Oscillatory Activity during the Execution of a Sensory Trick in Patients with Cervical Dystonia Joyce KH Tang 1 Neil Mahant 2 Danny Cunic 2 Robert Chen 2 Elena Moro 2 Anthony
Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014
 Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014 Dr. Ngai Ho Yin Allen Family Medicine Specialist PGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK),
Upper Cross Syndrome: Assessment & Management in Family Practice HKDU Symposium Dec 2014 Dr. Ngai Ho Yin Allen Family Medicine Specialist PGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK),
National Institute for Health and Clinical Excellence
 National Institute for Health and Clinical Excellence 319 Deep brain stimulation for tremor and dystonia (excluding Parkinson s disease) nts table IPAC date: 16 June 2006 Consultee name nts The Dystonia
National Institute for Health and Clinical Excellence 319 Deep brain stimulation for tremor and dystonia (excluding Parkinson s disease) nts table IPAC date: 16 June 2006 Consultee name nts The Dystonia
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor
 Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Xeomin) Reference Number: CP.PHAR.231 Effective Date: 07.01.16 Last Review Date: 02.19 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
Clinical Policy: (Xeomin) Reference Number: CP.PHAR.231 Effective Date: 07.01.16 Last Review Date: 02.19 Line of Business: Commercial, HIM, Medicaid Coding Implications Revision Log See Important Reminder
This policy addresses only the type B formulation rimabotulinumtoxinb marketed as Myobloc.
 RimabotulinumtoxinB NDC CODE(S) 10454-0710-XX Myobloc 2500 UNIT/0.5ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0711-XX Myobloc 5000 UNIT/ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0712-XX Myobloc 10000 UNIT/2ML
RimabotulinumtoxinB NDC CODE(S) 10454-0710-XX Myobloc 2500 UNIT/0.5ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0711-XX Myobloc 5000 UNIT/ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0712-XX Myobloc 10000 UNIT/2ML
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Is OnabotulinumtoxinA Good for Other Head and Face Pain? Disclosures BoNT/A for non- CM Botulinum neurotoxin (BoNT) in clinical use for headache >20
 in clinical use for headache >20") 1 2 3 4 5 6 Is OnabotulinumtoxinA Good for Other Head and Face Pain? Disclosures BoNT/A for non- CM Botulinum neurotoxin (BoNT) in clinical use for headache >20 years Efficacy of BoNT type A (onabotulinumtoxina,
1 2 3 4 5 6 Is OnabotulinumtoxinA Good for Other Head and Face Pain? Disclosures BoNT/A for non- CM Botulinum neurotoxin (BoNT) in clinical use for headache >20 years Efficacy of BoNT type A (onabotulinumtoxina,
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 Generic Brand HICL GCN Exception/Other ONABOTULINUMTOXINA BOTOX 04867 BRAND BOTOX COSMETIC ABOBOTULINUMTOXINA DYSPORT 36477 RIMABOTULINUMTOXINB MYOBLOC 21869 INCOBOTULINUMTOXINA XEOMIN 36687 Please use
Generic Brand HICL GCN Exception/Other ONABOTULINUMTOXINA BOTOX 04867 BRAND BOTOX COSMETIC ABOBOTULINUMTOXINA DYSPORT 36477 RIMABOTULINUMTOXINB MYOBLOC 21869 INCOBOTULINUMTOXINA XEOMIN 36687 Please use
85a Orthopedic Massage: Introduction - Neck Pain!
 85a Orthopedic Massage: Introduction - Neck Pain! 85a Orthopedic Massage: Introduction - Neck Pain " Class Outline! 5 minutes!!attendance, Breath of Arrival, and Reminders! 10 minutes!lecture:! 25 minutes!lecture:!
85a Orthopedic Massage: Introduction - Neck Pain! 85a Orthopedic Massage: Introduction - Neck Pain " Class Outline! 5 minutes!!attendance, Breath of Arrival, and Reminders! 10 minutes!lecture:! 25 minutes!lecture:!
Medication Prior Authorization Form
 (OnabotulinumtoxinA) Dysport (abobotulinumtoxina) Myobloc (rimabotulinumtoxinb) Xeomin (incobotulinumtoxina) Policy Number: 1042 Policy History Approve Date: 12/11/2015 Revise Dates: 07/07/2017 Next Review:
(OnabotulinumtoxinA) Dysport (abobotulinumtoxina) Myobloc (rimabotulinumtoxinb) Xeomin (incobotulinumtoxina) Policy Number: 1042 Policy History Approve Date: 12/11/2015 Revise Dates: 07/07/2017 Next Review:
BOTULINUM TOXIN THERAPY FOR CERVICOGENIC HEADACHE AND NECK PAIN
 BOTULINUM TOXIN THERAPY FOR CERVICOGENIC HEADACHE AND NECK PAIN Dr. Laxman Bahroo Director; Botulinum Toxin Clinic Director; Neurology Residency Program Associate Professor of Neurology Objectives Discuss
BOTULINUM TOXIN THERAPY FOR CERVICOGENIC HEADACHE AND NECK PAIN Dr. Laxman Bahroo Director; Botulinum Toxin Clinic Director; Neurology Residency Program Associate Professor of Neurology Objectives Discuss
Overview. Spasticity. Spasticity. Oral Medications. Spasticity 3/10/2012. Medication Management of Spasticity in the Traumatic Brain Injured Patient
 Medication Management of in the Traumatic Brain Injured Patient 6 th Annual Northern Kentucky TBI Conference March 23, 2012 www.bridgesnky.org Chad Walters, D.O. Medical Director Radical Rehab Solutions
Medication Management of in the Traumatic Brain Injured Patient 6 th Annual Northern Kentucky TBI Conference March 23, 2012 www.bridgesnky.org Chad Walters, D.O. Medical Director Radical Rehab Solutions
EMERGING TREATMENTS FOR PARKINSON S DISEASE
 EMERGING TREATMENTS FOR PARKINSON S DISEASE Katerina Markopoulou, MD, PhD Director Neurodegenerative Diseases Program Department of Neurology NorthShore University HealthSystem Clinical Assistant Professor
EMERGING TREATMENTS FOR PARKINSON S DISEASE Katerina Markopoulou, MD, PhD Director Neurodegenerative Diseases Program Department of Neurology NorthShore University HealthSystem Clinical Assistant Professor
Botox (onabotulinumtoxina) Dysport (abobotulinumtoxina) Xeomin (incobotulinumtoxina) Myobloc (rimabotulinumtoxinb)
 Dysport (abobotulinumtoxina) Xeomin (incobotulinumtoxina) Myobloc (rimabotulinumtoxinb)") Botox (onabotulinumtoxina) Dysport (abobotulinumtoxina) Xeomin (incobotulinumtoxina) Myobloc (rimabotulinumtoxinb) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date:
Botox (onabotulinumtoxina) Dysport (abobotulinumtoxina) Xeomin (incobotulinumtoxina) Myobloc (rimabotulinumtoxinb) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date:
Giving your clients self-care tips they can perform at home and work will help ensure the relief that your work provides won t be so quickly undone.
 by joe muscolino body mechanics Giving your clients self-care tips they can perform at home and work will help ensure the relief that your work provides won t be so quickly undone. seven keys to healthy
by joe muscolino body mechanics Giving your clients self-care tips they can perform at home and work will help ensure the relief that your work provides won t be so quickly undone. seven keys to healthy
Treatment of dystonia
 Review Treatment of dystonia Roongroj Bhidayasiri and Daniel Tarsy CONTENTS Pharmacological therapy Anticholinergic drugs Antidopaminergic drugs Other pharmacological agents Botulinum toxin therapy Surgical
Review Treatment of dystonia Roongroj Bhidayasiri and Daniel Tarsy CONTENTS Pharmacological therapy Anticholinergic drugs Antidopaminergic drugs Other pharmacological agents Botulinum toxin therapy Surgical
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Palladotomy and Pallidal Deep Brain Stimulation
 Palladotomy and Pallidal Deep Brain Stimulation Parkinson s disease Parkinson s Disease is a common neurodegenerative disorder that affects about 1:100 individuals over the age of 60. In a small percentage
Palladotomy and Pallidal Deep Brain Stimulation Parkinson s disease Parkinson s Disease is a common neurodegenerative disorder that affects about 1:100 individuals over the age of 60. In a small percentage
9/4/10. James J. Lehman, DC, MBA, DABCO. Why is posture important to you, the chiropractic physician?
 James J. Lehman, DC, MBA, DABCO The posture of homo sapiens is a complex biomechanical continuum, which involves the function of muscles, ligaments, fascia, nerves, osseous structures, neuromuscular control,
James J. Lehman, DC, MBA, DABCO The posture of homo sapiens is a complex biomechanical continuum, which involves the function of muscles, ligaments, fascia, nerves, osseous structures, neuromuscular control,
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
For adults with spasticity or cervical dystonia How long does your patients symptom * relief last?
 For adults with spasticity or cervical dystonia How long does your patients symptom * relief last? Consider Dysport because a long duration of response should matter 1 In clinical trials, retreatment was
For adults with spasticity or cervical dystonia How long does your patients symptom * relief last? Consider Dysport because a long duration of response should matter 1 In clinical trials, retreatment was
How do we record the activity of the deep cervical flexor muscles?
 Management of Cervicogenic Headache: Assessment and Retraining of the Deep Cervical Flexors Deep Cervical Flexors Longus colli and longus capitis Segmental support Counter bending of the cervical lordosis
Management of Cervicogenic Headache: Assessment and Retraining of the Deep Cervical Flexors Deep Cervical Flexors Longus colli and longus capitis Segmental support Counter bending of the cervical lordosis
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
NEEDLE EMG GUIDANCE FOR IMPROVED OUTCOMES
 T H E M Y O G U I D E S Y S T E M Needle EMG Guided Injection System NEEDLE EMG GUIDANCE FOR IMPROVED OUTCOMES INTRONIX TECHNOLOGIES CORPORATION VALUE - INNOVATION - PERFORMANCE Dr. Evan Friedman, June
T H E M Y O G U I D E S Y S T E M Needle EMG Guided Injection System NEEDLE EMG GUIDANCE FOR IMPROVED OUTCOMES INTRONIX TECHNOLOGIES CORPORATION VALUE - INNOVATION - PERFORMANCE Dr. Evan Friedman, June
HISTORY AND CHIEF COMPLAINT:
 submitted by Keith M. Bartley, D.C. Jasper, IN 07/21/11 presented at Cox Seminar in Nashville, TN, on October 8 9, 2011 HISTORY AND CHIEF COMPLAINT: 01/21/11 55 year old male press operator for Jasper
submitted by Keith M. Bartley, D.C. Jasper, IN 07/21/11 presented at Cox Seminar in Nashville, TN, on October 8 9, 2011 HISTORY AND CHIEF COMPLAINT: 01/21/11 55 year old male press operator for Jasper
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019
 WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
WHAT DEFINES YOPD? HANDLING UNIQUE CONCERNS REBECCA GILBERT, MD, PHD VICE PRESIDENT, CHIEF SCIENTIFIC OFFICER, APDA MARCH 14, 2019 YOUNG ONSET PARKINSON S DISEASE Definition: Parkinson s disease diagnosed
Tremor What is tremor? What causes tremor? What are the characteristics of tremor? What are the different categories of tremor?
 Tremor What is tremor? Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary
Tremor What is tremor? Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary
Policy. Medical Policy Manual Approved Revised: Do Not Implement Until 4/2/19. IncobotulinumtoxinA
 IncobotulinumtoxinA NDC CODE(S) 00259-1605-XX Xeomin 50 UNIT SOLR (MERZ PHARMACEUTICAL) 00259-1610-XX Xeomin 100 UNIT SOLR (MERZ PHARMACEUTICAL) 00259-1620-XX Xeomin 200 UNIT SOLR (MERZ PHARMACEUTICAL)
IncobotulinumtoxinA NDC CODE(S) 00259-1605-XX Xeomin 50 UNIT SOLR (MERZ PHARMACEUTICAL) 00259-1610-XX Xeomin 100 UNIT SOLR (MERZ PHARMACEUTICAL) 00259-1620-XX Xeomin 200 UNIT SOLR (MERZ PHARMACEUTICAL)
10/5/2017. Cervical Manual Evaluation and Mobilizations. Upper Cervical Stability Testing Alar Ligament
 Cervical Manual Evaluation and Mobilizations Upper Cervical Stability Testing Alar Ligament Upper Cervical Stability Testing Transverse Ligament 1 Upper Cervical Stability Testing Transverse Plane Positive
Cervical Manual Evaluation and Mobilizations Upper Cervical Stability Testing Alar Ligament Upper Cervical Stability Testing Transverse Ligament 1 Upper Cervical Stability Testing Transverse Plane Positive
The Use of Musculoskeletal Modelling to Assess Head- Worn Mass Properties
 The Use of Musculoskeletal Modelling to Assess Head- Worn Mass Properties SAFE Europe 2017 Dr Ross D Pollock 4/5 th April 2017 1 Neck Pain Prevalence and Contributory Factors Neck pain is a common complaint
The Use of Musculoskeletal Modelling to Assess Head- Worn Mass Properties SAFE Europe 2017 Dr Ross D Pollock 4/5 th April 2017 1 Neck Pain Prevalence and Contributory Factors Neck pain is a common complaint
Understanding Tremor Diagnosis, Cause, Treatment. Monique Giroux, MD Englewood and Fort Collins, CO
 Understanding Tremor Diagnosis, Cause, Treatment Monique Giroux, MD Englewood and Fort Collins, CO What is Tremor? Involuntary Rhythmic and Oscillatory Produced by contraction of alternating muscles Types
Understanding Tremor Diagnosis, Cause, Treatment Monique Giroux, MD Englewood and Fort Collins, CO What is Tremor? Involuntary Rhythmic and Oscillatory Produced by contraction of alternating muscles Types
No Financial Disclosures
 Deep Brain Stimulation: A Physician and Patient Perspective Jessica McClure Warren Marks, MD Cook Children s Medical Center Cook Children s Health Foundation Endowed Chair in Neurosciences Department of
Deep Brain Stimulation: A Physician and Patient Perspective Jessica McClure Warren Marks, MD Cook Children s Medical Center Cook Children s Health Foundation Endowed Chair in Neurosciences Department of
INDIANA HEALTH COVERAGE PROGRAMS
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Injections, Vaccines, and Other Physician-Administered Drugs Codes Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER CODE TABLES Injections, Vaccines, and Other Physician-Administered Drugs Codes Note: Due to possible changes in Indiana Health Coverage Programs (IHCP) policy
Botulinum toxin type A with or without needle electromyographic guidance in patients with cervical dystonia
 DOI 10.1186/s40064-016-2967-x RESEARCH Open Access Botulinum toxin type A with or without needle electromyographic guidance in patients with cervical dystonia Chuanjie Wu 1, Fang Xue 2, Wansheng Chang
DOI 10.1186/s40064-016-2967-x RESEARCH Open Access Botulinum toxin type A with or without needle electromyographic guidance in patients with cervical dystonia Chuanjie Wu 1, Fang Xue 2, Wansheng Chang
Treatment of cervical dystonia with botulinum toxins
 European Journal of Neurology 2006, 13 (Suppl. 1): 16 20 Treatment of cervical dystonia with botulinum toxins C. L. Comella a and P. D. Thompson b a Department of Neurological Sciences, Rush University
European Journal of Neurology 2006, 13 (Suppl. 1): 16 20 Treatment of cervical dystonia with botulinum toxins C. L. Comella a and P. D. Thompson b a Department of Neurological Sciences, Rush University
Myofascial Pain Syndrome and Trigger Points. Paul S. Sullivan, Do Trinity Health Care New England - Family Medicine
 Myofascial Pain Syndrome and Trigger Points Paul S. Sullivan, Do Trinity Health Care New England - Family Medicine Objectives Discuss why this topic is pertinent to our practices Review diagnostic criteria
Myofascial Pain Syndrome and Trigger Points Paul S. Sullivan, Do Trinity Health Care New England - Family Medicine Objectives Discuss why this topic is pertinent to our practices Review diagnostic criteria
The symptoms of the Parkinson s disease may vary from person to person. The symptoms might include the following:
 1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
1 PARKINSON S DISEASE Parkinson's disease is a long term disease related to the central nervous system that mainly affects the motor system, resulting in the loss of dopamine, which helps in producing
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,