Limb Pain (Tendonitis, Osteoarthritis, Plantar Fasciitis, Piriformis Syndrome)
|
|
|
- Barrie Clarke
- 6 years ago
- Views:
Transcription

1 Limb Pain (Tendonitis, Osteoarthritis, Plantar Fasciitis, Piriformis Syndrome) Martin Taylor, DO, PhD Neurology / OrthoNeuro Clinical Associate Professor, Neurology Ohio University College of Osteopathic Medicine Columbus, OH
2 Disclosures Consultant/independent contractor: Allergen plc, and Ipsen Biopharmaceuticals, Inc. Speaker s Bureau: Allergan plc, Avanir Pharmaceuticals, Inc. Depomed Inc., and Ipsen Biopharmaceuticals, Inc.
3 Questions 1. Which limb pain condition has the strongest literature supporting the use of botulinum toxin? a. Carpal tunnel syndrome b. Reflex sympathetic dystrophy c. Hip pain d. Lateral epicodylitis e. Shoulder pain
4 Questions 2. What is the most common dose range of onabotulinumtoxina used in clinical trials for joint pain? a. 5 to 10 units b. 25 to 50 units c. 50 to 100 units d. 100 to 200 units e. 300 to 500 units
5 Questions 3. True or False. The most common side effect reported in clinical trials after botulinum toxin injections for epicodylitis was grip weakness. True False
6 Botulinum Toxin Therapy for Joint and Limb Pain Shoulder Pain Hip Pain, Piriformis Syndrome Knee Pain Plantar Fasciitis Epicondylitis

7 Shoulder Pain

8

9
10 Long Term Effects of Intra-articular Botulinum Toxin A for Refractory Joint Pain Open label, prospective 9 subjects (osteoarthritis, RA, and psoriatic arthritis) Onabot (Botox) units intra-articular Duration of effect 3 to 12 months No immediate or delayed adverse effects Mohwald ML, et al. Neurotox Res Apr;9(2-3):
11 Long Term Effects of Intra-articular Botulinum Toxin A for Refractory Joint Pain Increased Active Range of Motion 67% 42% Flexion (p <0.01) Abduction Mohwald ML, et al. Neurotox Res Apr;9(2-3):
12 Long Term Effects of Intra-articular Botulinum Toxin A for Refractory Joint Pain Reduction in Shoulder Pain Pretreatment (p <0.001) Posttreatment Mohwald ML, et al. Neurotox Res Apr;9(2-3):
13 Intra-articular Botulinum Toxin Type A: A New Approach to Treat Arthritis Joint Pain Double blind, placebo controlled 36 Subjects with shoulder pain refractory to NSAIDS, intra-articular steroid injection Onabot (Botox) 100 units+lidocaine vs saline+lidocaine (Intra-articular) Response measured at 4 weeks Mahowald ML, et al. Toxicon. 2009; 54(5):
14 Intra-articular Botulinum Toxin Type A: A New Approach to Treat Arthritis Joint Pain Pain Reduction at 4 Weeks Post Treatment 61% 31% Onabot (p <0.002) Saline Mahowald ML, et al. Toxicon. 2009; 54(5):
15 Intra-articular Botulinum Toxin Type A: A New Approach to Treat Arthritis Joint Pain >30% reduction in pain 61% 31% Onabot Saline Mahowald ML, et al. Toxicon. 2009; 54(5):
16 Intra-articular botulinum toxin A for Refractory Shoulder Pain: a Randomized, Double-blinded, Placebo-controlled Trial Double blind, placebo controlled 43 Subjects with moderate-severe arthritis shoulder pain Onabot (Botox) 100 units/lidocaine vs saline/lidocaine Reduction of pain at one month s/p injection Reduction in pain on VAS: Onabot -2.4 vs saline -0.8 (p=0.014) Improvement in SF-36 scores: Onabot (p</=0.035) Clinically meaningful pain relief: Onabot 61% vs saline 36% (p=0.22) Singh JA, et al. Transl Res. 2009;153(5):

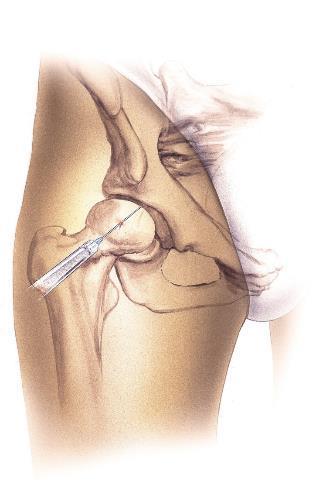
17 Hip Pain
18
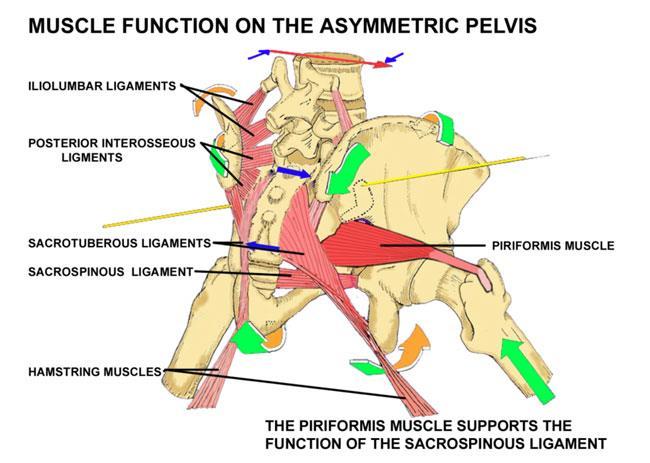
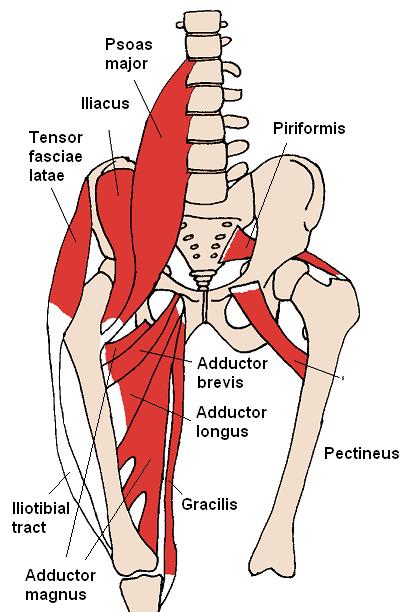
19 Piriformis Muscle

20 Inflamed Sciatic Nerve

21 Piriformis and Sciatic

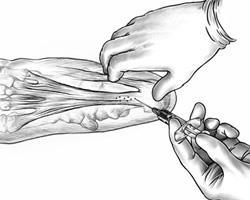
22 Piriformis Injection
23 Efficacy of Botulinum Toxin Type A Treatment of Functional Impairment of Degenerative Hip Joint: Preliminary Results Open label, prospective 39 Subjects (41-82 y/0) with hip pain and osteoarthritis Abobot (Dysport) 400 units injected into the ipsilateral adductor longus/adductor magnus muscles Improvement in Harris Hip Score at 2, 4, and 12 wks (p<0.0001) Decrease in VAS pain scores at 2, 4, and 12 wks (p<0.001) Improved hip mobility noted on exam Marchini C e,t al. J Rehabil Med. 2010: 42(7):
24 Botulinum toxin in Piriformis Syndrome Authors Childers Martin K, et. al. * Fishman Loren M. et. al. * Lang Amy M. Study Botulinum toxin type A use in piriformis muscle syndrome: A pilot study. Am J Phys Med Rehabil Botox and physical therapy in the treatment of piriformis syndrome. Am J Phys Med Rehabil Botulinum Toxin Type B in Piriformis Syndrome. Am J Phys Med Rehabil * RDBPC
25 Botulinum Toxin Use in Piriformis Syndrome: A Pilot Study Study Design Single center, double blind, single group, crossover n=10 Two 10 week treatment arms with 4 weeks washout BoNT-A (Botox) 100 U vs. preservative free normal saline Childers MK et. al. Am. J. Phys. Med. Rehabil (10) 751-9
 Childers Am. MK J. Phys. et. al. Med. Am. Rehabil. J. Phys. Med. 2002. Rehabil. 81(10) 751-9.")
26 Botulinum Toxin Use in Piriformis Syndrome: A Pilot Study Assessment VAS reporting of: Pain Intensity Spasm Interference with Activities Distress H-reflex measurement side-side / pre-post BoNT/A Pain-on-motion analysis (pain perceived during a stepping task) Childers Am. MK J. Phys. et. al. Med. Am. Rehabil. J. Phys. Med Rehabil. 81(10) (10) 751-9
27 Botulinum Toxin Use in Piriformis Syndrome: A Pilot Study Results Functional improvement noted with BoNT/A injections (p<0.05) VAS decreases were detected under every category in BoNT/A treated group (p<0.05) Similarities in H reflex latencies between groups Before injection of study treatments Following injection of study treatments Motion analyses also failed to detect differences between baseline and experimental groups No adverse events were reported Authors Conclusions VAS data suggest that intramuscular piriformis injection with 100 units of botulinum toxin type A (Botox) can reduce pain to a greater extent than similar injections with vehicle alone. Childers MK et. al. Am. J. Phys. Med. Rehabil (10) 751-9
28 BoNT-A and Physical Therapy in the Treatment of Piriformis Syndrome Study Design Double blind, placebo controlled, clinical trial n=87, (n=67 after exclusion of those with <2 follow up visits) BoNT/A (Allergan) 200 U, Lidocaine with steroid, or placebo Standard physical therapy protocol twice weekly X 12 weeks Examinations every 2 weeks 1 o endpoint: VAS Responses at two last visits (10 and 12 weeks) Patient Selection Piriformis syndrome was diagnosed when there were significant discrepancies between anatomic position and FAIR position (per Snow BJ et. al. Neurology 1990;40(suppl 1):382) Fishman et.al. Am J Phys Med Rehabil 2002;81 (12):
29 BoNT-A and Physical Therapy in the Treatment of Piriformis Syndrome Results Injection No. of Patients No. Improved % Improved ** T/L* BoNT/A (Allergan) Placebo *T/L= triamcinolone and lidocaine ** Percent of subjects with 50% or more improvement at each of their last two visits Fishman et.al. Am J Phys Med Rehabil 2002;81 (12):
30 Fishman LM, et. al. Botox and Physical Therapy in the Treatment of Piriformis Syndrome Authors Conclusion: Botox and Physical Therapy were more effective in treating Piriformis Syndrome than either T/L or placebo injections in conjunction with Physical Therapy. No Adverse events were reported in this study. Am Fishman J Phys Med et.al. Rehabil Am J Phys 2002;81 Med (12): Rehabil ;81 (12):
31 BoNT-B in Piriformis Syndrome Study Design Single center, outpatient, open label study n = 20 Follow ups at 2,4,8,12, and 16 weeks 5000 units per piriformis (up to 10,000 units total dose if bilateral injection) infiltrated with EMG guidance Endpoints: Mean VAS for buttock and hip pain and for low back pain. VAS for general and low back pain, pain radiating into lower limbs, and tingling. Lang AM. Am J Phys Med Rehabil. 2004; 83(3):
32 BoNT-B in Piriformis Syndrome Results Significant reductions in VAS Patient rated pain improvement: 95% - fair to excellent 75% - good to excellent Investigator rated efficacy: 90% - fair to excellent 55% - good to excellent Lang AM. Am J Phys Med Rehabil. 2004; 83(3):
33 BoNT-B in Piriformis Syndrome Safety Six patients(30%) experienced mild to severe dry mouth Two patients (10%) experienced mild to moderate flu like symptoms Two patients (10%) reported visual disturbance (10%) One patient (5%) reported dizziness One patient (5%) reported nausea One patient (5%) reported GERD Lang AM. Am J Phys Med Rehabil. 2004; 83(3):

34 Knee Pain
35 Intra-articular Botulinum Toxin Type A: a New Approach to Treat Arthritis Joint Pain Double blind, placebo controlled 42 Subjects with knee pain refractory to NSAIDS, intraarticular steroid injection Onabot (Botox) 100 units+lidocaine vs saline+lidocaine Knee pain reduction on McGill Pain Joint Inventory Scale: Onabot superior to saline: 1 month (p=0.011) 3 months (p=0.002) Mahowald ML, et al. Toxicon. 2009; 54(5):
36 Intraarticular Botulinum Toxin A For Refractory Painful Total Knee Arthroplasty: A Randomized Controlled Trial Randomized, Placebo controlled, triple-blinded 49 subjects with painful total knee arthroplasty, mean duration 4.5 years Onabot (Botox) 100 units vs saline Single intra-articular injection into painful knee Sing JA,et al. J Rheumatol Nov;37(11):
37 Intraarticular Botulinum Toxin A For Refractory Painful Total Knee Arthroplasty: A Randomized Controlled Trial Reduction in VAS rated pain: Onabot 71% vs saline 35% s/p 2 months (p=0.28) s/p 3 and 4 months (p=0.019) Duration of meaningful pain relief : Onabot 39.6 days vs saline 15.7 days (p=0.045) Onabot superior to saline: Western Ontario McMaster Osteoarthritis Index physical function (p=0.026) Reduction in stiffness (p=0.004) and total score (p=0.024) Reduction of pain subscale score on SF-36 (p=0.049) Sing JA, et al. J Rheumatol Nov;37(11):
38 An Open Label Pilot Investigation of the Efficacy Of Botulinum Toxin Type A [Dysport] Injection in the Rehabilitation of Chronic Anterior Knee Pain Open label Pilot Study 8 Subjects with >6 months of anterior knee pain, who had failed conservative therapy Obabot (Dysport) units into distal 2/3 of VL followed by home exercise program to improve recruitment of the VM Subjects reported reduced knee pain and brace dependency Subjects reported increased participation in sporting and daily living activities Singer BJ, et al. Disabil Rehabil Jun 15;28(11):
 500 units vs saline injections the vastus lateralis followed by home exercises focusing on re-training the vastus")
39 Treatment of Refractory Anterior Knee Pain Using Botulinum Toxin Type A (Dysport) Injection to the Distal Vastus Lateralis Muscle: A Randomized Placebo Controlled Crossover Trial Randomized placebo controlled crossover 24 subjects with refractory anterior knee pain Abobot (Dysport) 500 units vs saline injections the vastus lateralis followed by home exercises focusing on re-training the vastus medialis Singer BJ, et al. Br J Sports Med Jun;45(8):
40 Treatment of Refractory Anterior Knee Pain Using Botulinum Toxin Type A (Dysport) Injection to the Distal Vastus Lateralis Muscle: A Randomized Placebo Controlled Crossover Trial 14 subjects received BoNT-A and 10 placebo injection. Improvement at 12 weeks was significantly greater for Abobot compared with placebo-injected subjects for: AKPS (p<0.03) pain on kneeling (p<0.004), squatting (p<0.02) level walking (p<0.04). Singer BJ, et al. Br J Sports Med Jun;45(8):

41 Plantar Fasciitis

42 Plantar Fascia Injection
43 Treatment of Pain Attributed to Plantar Fasciitis with Botulinum Toxin A: A Short Term, Randomized, Placebo Controlled, Double-Blind Study Double blind, placebo controlled 27 Subjects (43 feet) Onabot (Botox) 70 units Babcock MS, et.al. Am J Phys Med Rehabil Sep;84(9):
44 Treatment of Pain Attributed to Plantar Fasciitis with Botulinum Toxin A: A Short Term, Randomized, Placebo Controlled, Double-Blind Study Improvement in all measurements at 3 & 8 weeks At 3 weeks: 39% decrease on the Pain Visual Analog Scale (p<0.005) 34% improvement of the Maryland Foot Score (p< 0.001) 40% increase in pressure algometry response (p<0.003) Maintained at 8 weeks No side effects reported Babcock MS, et al. Am J Phys Med Rehabil Sep;84(9):
45 Ultrasonographic Guided Botulinum Toxin Type A Treatment for Plantar Fasciitis: An Outcome-Based Investigation for Treating Pain and Gait Changes Double blind, placebo controlled 50 subjects with unilateral plantar fasciitis Onabot (Botox) 50 units vs saline Pain reduction on VAS in Onabot group superior to placebo at 3 wks and 3 months (p<0.001) Center of pressure velocity during loading in Onabot group increased compared to placebo (p<0.05) Fat pad thickness remained unchanged Huang YC, et al. J Rehabil Med Feb;42(2):
46 Randomized Controlled Study of the Efficacy of the Injection of Botulinum Toxin Type A versus Corticosteroids in Chronic Plantar Fasciitis: Results at One and Six Months Single blind, placebo controlled 52 subjects Onabot (Botox) vs corticosteroids Outcomes based on Foot Health Square Questionnaire results at 1 and 6 months one month (improvement with botulinum toxin vs. corticosteroid: pain 19.10/-6.84 (P = 0.001) function 16.00/-8.80 (P < 0.001) footwear 13.48/-7.95 (P = 0.004) self-perceived foot health 25.44/-5.41 (P < 0.001).
47 Treatment of Chronic Plantar Fasciitis with Botulinum Toxin A--An Open Pilot Study on 25 Patients with a 14-Week-Follow-Up Open label pilot study 25 subjects refractory to conservative therapy Dose finding: 6 subjects injected with Abobot (Dysport) 100 units and 6 subjects injected with Abobot (Dysport) 200 units. 13 subjects then injected with Abobot (Dysport) 200 units A significant reduction of maximum and continuous pain was seen 2 weeks after injection in the group of 19 patients treated with 200 units BoNT A and persisted until the end of the follow-up No adverse reactions reports Placzek R, et al. Z Orthop Ihre Grenzgeb Jul-Aug; 144(4): Díaz-Llopis IV, et al,.clin Rehabil Jul;26(7):

48 Tennis Elbow

49 Lateral Epicondyle Injection
50 Treatment of Lateral Epicondylitis with Botulinum Toxin: A Randomized, Double-blind, Placebo-controlled Trial Double blind, placebo controlled 60 subjects Onabot (Botox), 60 units vs. saline Decreased pain at weeks 4 & 12 Mean decreased VAS 65 to 25 (p<0.006) at 4 wks No significant difference in grip strength 60% reported some weakness Wong SM, et al. Ann Intern Med Dec 6;143(11):

51 Onabot 60 units vs. Placebo Lateral Epicodylitis Baseline 4 wks 12 wks Onabot Placebo Wong SM, et al, Ann Intern Med Dec 6;143(11):
52 Botulinum Toxin Injection in the Treatment of Tennis Elbow: A Double-blind, Randomized, Controlled, Pilot Study Double blind, placebo controlled 40 subjects (Failed steroid injection) Onabot (Botox) 50 units vs. saline IM injections were performed 5 cm distal to the maximum point of tenderness at the lateral epicondyle Trend toward improvement at 3 months No significant difference in grip strength 60% reported some weakness 12/18 reported extensor weakness Hayton MJ, et al. J Bone Joint Surg Am Mar;87(3):
53 Treatment of Chronic Radial Epicondylitis with Botulinum Toxin A: A Double-blind, Placebo-controlled, Randomized Multicenter Study Double blind, placebo controlled 130 subjects Abobot (Dysport) 60 units vs. saline Decreased pain (VAS) at 2, 6, 12, and 18 weeks (=0.003) Subjective improvement at 6 and 18 weeks (<0.001) Improved grip strength in both groups Extensor weakness at 2 weeks Placzek R, et al. J Bone Joint Surg Am Feb;89(2):
54 Use of Anatomic Measurement to Guide Injection of Botulinum Toxin for the Management of Chronic Lateral Epicondylitis: A Randomized, Controlled Trial Double blind, placebo controlled 60 subjects (refractory lateral epicondylitis) Onabot (Botox), 60 units vs. saline VAS (100 mm scale) at 4, 8, & 16 wks. Espandar R, et al. CMAJ May 18;182(8):
55 Pain score at rest Outcome measure Group; mean (SD) Difference in mean (95% CI) p value (repeated measurement) Baseline 48.8 (23.7) 46.4 (16.2) 2.3 ( 9.5 to 14.2) * Week (15.9) 34.5 (12.2) 14.1 (5.8 to 22.3) Week (18.0) 29.4 (14.5) 11.5 (2.0 to 21.4) Week (6.0) 16.7 (10.5) 12.6 (7.7 to 17.8)
56 Pain score during maximum grip Outcome measure Group; mean (SD) Difference in mean (95% CI) p value (repeated measurement) Baseline 65.8 (22.0) 65.0 (18.3) 0.8 ( 10.9 to 12.6) 0.22 Week (23.3) 57.4 (18.2) 5.3 ( 6.8 to 17.5) Week (23.1) 51.5 (20.1) 7.8 ( 4.8 to 20.4) Week (10.0) 30.6 (15.6) 11.8 (4.2 to 19.4)
57 Pain score during maximum pinch Outcome measure Group; mean (SD) Difference in mean (95% CI) p value (repeated measurement) Baseline 42.6 (26.5) 45.1 (19.0) 2.4 ( 11.0 to 15.9) * Week (16.8) 32.7 (12.6) 15.4 (6.8 to 24.1) Week (14.9) 26.6 (11.3) 14.4 (6.8 to 22.2) Week (9.7) 13.6 (8.3) 8.5 (3.1 to 13.9)
58 Reported Adverse Reactions Adverse reaction; time frame Pain at injection site Botulinum toxin Group; no. of patients Placebo After injection 3 2 Weeks Weeks Weeks Tingling sensation around injection site After injection 0 0 Weeks Weeks Weeks Subjective feeling of muscle spasm around injection site After injection 0 0 Weeks Weeks Weeks Total 23 4
59 Botulinum Toxin Therapy for Joint and Limb Pain Summary Good data for BTX use in lateral epicondylitis and knee pain Evolving data for BTX in plantar fasciitis and shoulder pain Minimal data for BTX in hip pain, Except Piriformis Syndrome
60 Questions 1. Which limb pain condition has the strongest literature supporting the use of botulinum toxin? a. Carpal tunnel syndrome b. Reflex sympathetic dystrophy c. Hip pain d. Lateral epicodylitis e. Shoulder pain
61 Questions 2. What is the most common dose range of onabotulinumtoxina used in clinical trials for joint pain? a. 5 to 10 units b. 25 to 50 units c. 50 to 100 units d. 100 to 200 units e. 300 to 500 units
62 Questions 3. True or False. The most common side effect reported in clinical trials after botulinum toxin injections for epicodylitis was grip weakness. True False
63 Thank You
Botulinum Toxin Therapy Billing & Coding Update 2016
 Botulinum Toxin Therapy Billing & Coding Update 2016 Martin Taylor, DO, PhD Neurology / OrthoNeuro Clinical Associate Professor, Neurology Ohio University College of Osteopathic Medicine Columbus, OH Disclosures
Botulinum Toxin Therapy Billing & Coding Update 2016 Martin Taylor, DO, PhD Neurology / OrthoNeuro Clinical Associate Professor, Neurology Ohio University College of Osteopathic Medicine Columbus, OH Disclosures
Intraarticular platelet-rich plasma injection in the treatment of knee osteoarthritis: review and recommendations.
 Am J Phys Med Rehabil. 2014 Nov;93(11 Suppl 3):S108-21. doi: 10.1097/PHM.0000000000000115. Intraarticular platelet-rich plasma injection in the treatment of knee osteoarthritis: review and recommendations.
Am J Phys Med Rehabil. 2014 Nov;93(11 Suppl 3):S108-21. doi: 10.1097/PHM.0000000000000115. Intraarticular platelet-rich plasma injection in the treatment of knee osteoarthritis: review and recommendations.
Preliminary Report Choosing Wisely Identifying Musculoskeletal Interventions with Limited Levels of Efficacy in the Shoulder & Elbow.
 Preliminary Report Choosing Wisely Identifying Musculoskeletal Interventions with Limited Levels of Efficacy in the Shoulder & Elbow. Prepared for The Canadian Orthopaedic Association Contents Executive
Preliminary Report Choosing Wisely Identifying Musculoskeletal Interventions with Limited Levels of Efficacy in the Shoulder & Elbow. Prepared for The Canadian Orthopaedic Association Contents Executive
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
The Function Effect of Botulimun Toxin A (BtX-A) at the Calf Muscle in Lower Limb Lengthening Dong Hoon Lee, MD, Ph.D, Keun Jung Ryu MD
 at the Calf Muscle in Lower Limb Lengthening Dong Hoon Lee, MD, Ph.D, Keun Jung Ryu MD") The Function Effect of Botulimun Toxin A (BtX-A) at the Calf Muscle in Lower Limb Lengthening Dong Hoon Lee, MD, Ph.D, Keun Jung Ryu MD Limb Lengthening and Deformity Correction Service Department of Orthopaedic
The Function Effect of Botulimun Toxin A (BtX-A) at the Calf Muscle in Lower Limb Lengthening Dong Hoon Lee, MD, Ph.D, Keun Jung Ryu MD Limb Lengthening and Deformity Correction Service Department of Orthopaedic
Treatment of Lateral Elbow Tendinopathy: Medical and Surgical Interventions
 APPENDIX G Treatment of Lateral Elbow Tendinopathy: Medical and Surgical Interventions The purpose of this document is to provide information for physiotherapists of common medical and surgical interventions
APPENDIX G Treatment of Lateral Elbow Tendinopathy: Medical and Surgical Interventions The purpose of this document is to provide information for physiotherapists of common medical and surgical interventions
Collected Scientific Research Relating to the Use of Osteopathy with Knee pain including iliotibial band (ITB) friction syndrome
 friction syndrome") Collected Scientific Research Relating to the Use of Osteopathy with Knee pain including iliotibial band (ITB) friction syndrome Important: 1) Osteopathy involves helping people's own self-healing abilities
Collected Scientific Research Relating to the Use of Osteopathy with Knee pain including iliotibial band (ITB) friction syndrome Important: 1) Osteopathy involves helping people's own self-healing abilities
BOTULINUM TOXIN THERAPY FOR CERVICOGENIC HEADACHE AND NECK PAIN
 BOTULINUM TOXIN THERAPY FOR CERVICOGENIC HEADACHE AND NECK PAIN Dr. Laxman Bahroo Director; Botulinum Toxin Clinic Director; Neurology Residency Program Associate Professor of Neurology Objectives Discuss
BOTULINUM TOXIN THERAPY FOR CERVICOGENIC HEADACHE AND NECK PAIN Dr. Laxman Bahroo Director; Botulinum Toxin Clinic Director; Neurology Residency Program Associate Professor of Neurology Objectives Discuss
Effects of intra-articular botulinum toxin type A (Botox ) in dogs with chronic osteoarthritis A pilot study
 in dogs with chronic osteoarthritis A pilot study") 254 Schattauer 2010 Clinical Communication Effects of intra-articular botulinum toxin type A (Botox ) in dogs with chronic osteoarthritis A pilot study H. S. Hadley 1, 2 ; J. L. Wheeler 1 ; S. W. Petersen
254 Schattauer 2010 Clinical Communication Effects of intra-articular botulinum toxin type A (Botox ) in dogs with chronic osteoarthritis A pilot study H. S. Hadley 1, 2 ; J. L. Wheeler 1 ; S. W. Petersen
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES
 ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
ORTHOPAEDIC INJECTION AND ASPIRATION TECHNIQUES OAAPN October 20, 2016 David H. Sohn, JD MD Chief, Shoulder and Sports Medicine University of Toledo Medical Center When to aspirate? To rule out infection
Is OnabotulinumtoxinA Good for Other Head and Face Pain? Disclosures BoNT/A for non- CM Botulinum neurotoxin (BoNT) in clinical use for headache >20
 in clinical use for headache >20") 1 2 3 4 5 6 Is OnabotulinumtoxinA Good for Other Head and Face Pain? Disclosures BoNT/A for non- CM Botulinum neurotoxin (BoNT) in clinical use for headache >20 years Efficacy of BoNT type A (onabotulinumtoxina,
1 2 3 4 5 6 Is OnabotulinumtoxinA Good for Other Head and Face Pain? Disclosures BoNT/A for non- CM Botulinum neurotoxin (BoNT) in clinical use for headache >20 years Efficacy of BoNT type A (onabotulinumtoxina,
4/1/2016. Total Hip Arthroplasty. DAHR Procedure. Direct Anterior Hip Replacement. DAHR Procedure. DAHR Procedure
 Mercy Orthopedist Types of Approaches Total Hip Arthroplasty Mercy Has a total of 16 Orthopedist that perform all three different approaches Posterior Anterior Lateral Direct Anterior Direct Anterior Hip
Mercy Orthopedist Types of Approaches Total Hip Arthroplasty Mercy Has a total of 16 Orthopedist that perform all three different approaches Posterior Anterior Lateral Direct Anterior Direct Anterior Hip
Management of upper limb in cerebral palsy. Dr Sameer Desai Pediatric Orthopedic Surgeon KEM, Ruby Hall, Sahyadri Hospital, Unique Childrens Hospital
 Management of upper limb in cerebral palsy Dr Sameer Desai Pediatric Orthopedic Surgeon KEM, Ruby Hall, Sahyadri Hospital, Unique Childrens Hospital Importance of upper limb in CP Activities of daily living
Management of upper limb in cerebral palsy Dr Sameer Desai Pediatric Orthopedic Surgeon KEM, Ruby Hall, Sahyadri Hospital, Unique Childrens Hospital Importance of upper limb in CP Activities of daily living
Common Foot and Ankle Conditions: How Can You Find Relief?
 Common Foot and Ankle Conditions: How Can You Find Relief? Your Feet and Ankles are Workhorses They bear a lot of weight They perform various movements Common Conditions That Cause Foot/Ankle Pain Plantar
Common Foot and Ankle Conditions: How Can You Find Relief? Your Feet and Ankles are Workhorses They bear a lot of weight They perform various movements Common Conditions That Cause Foot/Ankle Pain Plantar
Upper limb injuries II. Traumatology RHS 231 Dr. Einas Al-Eisa
 Upper limb injuries II Traumatology RHS 231 Dr. Einas Al-Eisa Capsulitis = inflammatory lesion of the glenohumeral joint capsule leading to: thickening and loss of joint volume painful stiffness of the
Upper limb injuries II Traumatology RHS 231 Dr. Einas Al-Eisa Capsulitis = inflammatory lesion of the glenohumeral joint capsule leading to: thickening and loss of joint volume painful stiffness of the
Common Elbow Problems
 Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
Common Elbow Problems Duncan Ferguson FRACS Knee and Shoulder Specialist Elbow Instability Common 10-25% of elbow injuries Median age 30 yrs Most simple dislocations are stable after reduction recurrence
B ar b ar a J Singer, 1 P e ter L Silb er t, 1,2 S w i t hin S ong, 3 John W Dunne, 1,2 Kev in P Singer 1
 1 Centre for Musculoskeletal Studies, School of Surgery, The University of Western Australia, Perth, Western Australia 2 Department of Neurology, Royal Perth Hospital, Perth, Western Australia 3 Department
1 Centre for Musculoskeletal Studies, School of Surgery, The University of Western Australia, Perth, Western Australia 2 Department of Neurology, Royal Perth Hospital, Perth, Western Australia 3 Department
C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center
 Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
Evaluation and Treatment of the Painful Shoulder in the Primary Care Setting C. Christopher Smith, M.D. Associate Professor of Medicine Harvard Medical School Beth Israel Deaconess Medical Center A 65-year-old
TOP RYDE CHIROPRACTIC
 1. Ankle Pain Conditions Helped by Chiropractic The ankle joint is made up of ligaments, tendons, nerves, and a disc to cushion motion. Distortions of motion of the ankle can strain the ligaments and muscles
1. Ankle Pain Conditions Helped by Chiropractic The ankle joint is made up of ligaments, tendons, nerves, and a disc to cushion motion. Distortions of motion of the ankle can strain the ligaments and muscles
COS SPORTS MEDICINE CONCUSSION ASSESSMENT FORM BASELINE TEST Adapted from SCAT3
 COS SPORTS MEDICINE CONCUSSION ASSESSMENT FORM BASELINE TEST Adapted from SCAT3 Name Sport Examiner Name: Date of BASELINE TEST: Age Gender M / F COGNITIVE ASSESSMENT Orientation (1 pt each) What month
COS SPORTS MEDICINE CONCUSSION ASSESSMENT FORM BASELINE TEST Adapted from SCAT3 Name Sport Examiner Name: Date of BASELINE TEST: Age Gender M / F COGNITIVE ASSESSMENT Orientation (1 pt each) What month
Pain Management. Medicine. without limits
 Pain Management Medicine without limits Minimally invasive therapies for chronic pain relief Thanks to advances in medicine, you don t have to live with the debilitating effects of chronic pain. The physicians
Pain Management Medicine without limits Minimally invasive therapies for chronic pain relief Thanks to advances in medicine, you don t have to live with the debilitating effects of chronic pain. The physicians
Epidural Steroid Injection
 Epidural Steroid Injection Epidural steroid injections (ESI) are performed to place anti-inflammatory medication (steroid) and local anesthetic in the epidural space to target irritated nerves and relieve
Epidural Steroid Injection Epidural steroid injections (ESI) are performed to place anti-inflammatory medication (steroid) and local anesthetic in the epidural space to target irritated nerves and relieve
Tendon Fenestration. Disclosures. Outline: questions. Introduction: Peritendon Steroid Injections. Jon A. Jacobson, MD. Patellar Tendon: tendinosis
 Tendon Fenestration Jon A. Jacobson, MD Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures Consultant: Bioclinica Advisory Board: GE, Philips Book
Tendon Fenestration Jon A. Jacobson, MD Professor of Radiology Director, Division of Musculoskeletal Radiology University of Michigan Disclosures Consultant: Bioclinica Advisory Board: GE, Philips Book
10/1/2009. October 15, 2009 Christina Kuo MD. Anatomy and pathophysiology of Epicondylitis Diagnosis
 October 15, 2009 Christina Kuo MD Anatomy and pathophysiology of Epicondylitis Diagnosis Treatment options Lawn tennis elbow Morris 1882 - described as an injury occurring from the backhand stroke Age
October 15, 2009 Christina Kuo MD Anatomy and pathophysiology of Epicondylitis Diagnosis Treatment options Lawn tennis elbow Morris 1882 - described as an injury occurring from the backhand stroke Age
Outcomes of Surgical Treatment for Insertional Achilles Tendinopathy Using a Central Tendon Splitting Approach
 Outcomes of Surgical Treatment for Insertional Achilles Tendinopathy Using a Central Tendon Splitting Approach Elizabeth Martin, MD; Ruth Chimenti, DPT; Josh Tome, MS; Andrew Hollenbeck, BS; John Ketz,
Outcomes of Surgical Treatment for Insertional Achilles Tendinopathy Using a Central Tendon Splitting Approach Elizabeth Martin, MD; Ruth Chimenti, DPT; Josh Tome, MS; Andrew Hollenbeck, BS; John Ketz,
SPORTS MEDICINE OVERUSE MANAGEMENT PRINCIPLES FOR
 SPORTS MEDICINE OVERUSE INJURIES: DIAGNOSIS AND MANAGEMENT PRINCIPLES FOR THE FAMILY PHYSICIAN DR NG CHUNG SIEN MBBS (SPORE) MSPMED (AUSTRALIA) DFD CAW SENIOR REGISTRAR CHANGI SPORTS MEDICINE CENTRE CHANGI
SPORTS MEDICINE OVERUSE INJURIES: DIAGNOSIS AND MANAGEMENT PRINCIPLES FOR THE FAMILY PHYSICIAN DR NG CHUNG SIEN MBBS (SPORE) MSPMED (AUSTRALIA) DFD CAW SENIOR REGISTRAR CHANGI SPORTS MEDICINE CENTRE CHANGI
Scientific Update Laxman Bahroo, MD
 Scientific Update Laxman Bahroo, MD Associate Professor Director; Botulinum Toxin Clinic Director; Neurology Residency Program Medstar Georgetown University Hospital Washington, D.C. Disclosures Advisory
Scientific Update Laxman Bahroo, MD Associate Professor Director; Botulinum Toxin Clinic Director; Neurology Residency Program Medstar Georgetown University Hospital Washington, D.C. Disclosures Advisory
The Painful Hip. Jennifer R Marks, MD
 The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
The Painful Hip Jennifer R Marks, MD The Painful Hip A 64 yo F presents to clinic complaining of a sore hip What further questions do you have for this patient? What is on your differential diagnosis?
Evaluating concomitant lateral epicondylitis and cervical radiculopathy
 Evaluating concomitant lateral epicondylitis and cervical radiculopathy March 06, 2010 This article describes a study of the prevalence of lateral epicondylitis or tennis elbow among patients with neck
Evaluating concomitant lateral epicondylitis and cervical radiculopathy March 06, 2010 This article describes a study of the prevalence of lateral epicondylitis or tennis elbow among patients with neck
Platelet Rich Plasma (PRP) Dania Segreti, SPT Vanguard In-service - July 31, 2013
 Dania Segreti, SPT Vanguard In-service - July 31, 2013") Platelet Rich Plasma (PRP) Dania Segreti, SPT Vanguard In-service - July 31, 2013 What is PRP? In medicine since 1970s First uses in bone healing began in late 1990s Gained popularity for tissue healing
Platelet Rich Plasma (PRP) Dania Segreti, SPT Vanguard In-service - July 31, 2013 What is PRP? In medicine since 1970s First uses in bone healing began in late 1990s Gained popularity for tissue healing
Prevention Diagnosis Assessment Prescription and /or application of wide range of interventions and PRM program management
 OA PATHOLOGY Characterized by progressive deterioration and ultimate loss of articular cartilage Reactive changes of joint margins and joint thickening of the capsule When OA symptomatic leads to: Pain
OA PATHOLOGY Characterized by progressive deterioration and ultimate loss of articular cartilage Reactive changes of joint margins and joint thickening of the capsule When OA symptomatic leads to: Pain
Physical Exam. Jared Van Der Beek. Basics To Remember. Know the anatomy and how the muscles function.
 Physical Exam Jared Van Der Beek Jared@physio-puncture.com 1 Basics To Remember Know the anatomy and how the muscles function. Know what the special tests are looking for and understand why they are positive.
Physical Exam Jared Van Der Beek Jared@physio-puncture.com 1 Basics To Remember Know the anatomy and how the muscles function. Know what the special tests are looking for and understand why they are positive.
Outline 3D Core Training with Rubber Resistance
 Outline 3D Core Training with Rubber Resistance Mike Bracko, Ed.D. CSCS, FACSM Fitness Educator / Sports Physiologist drbrackofitness@aol.com Introduction Rubber resistance was originally used to train
Outline 3D Core Training with Rubber Resistance Mike Bracko, Ed.D. CSCS, FACSM Fitness Educator / Sports Physiologist drbrackofitness@aol.com Introduction Rubber resistance was originally used to train
Clinical Scenario. Focused Clinical Question. Summary of Search, Best Evidence Appraised, and Key Findings
 Journal of Sport Rehabilitation, 2013, 22, 72-78 2013 Human Kinetics, Inc. Effectiveness of Low-Level Laser Therapy Combined With an Exercise Program to Reduce Pain and Increase Function in Adults With
Journal of Sport Rehabilitation, 2013, 22, 72-78 2013 Human Kinetics, Inc. Effectiveness of Low-Level Laser Therapy Combined With an Exercise Program to Reduce Pain and Increase Function in Adults With
Clinical Policy: Trigger Point Injections for Pain Management
 Clinical Policy: for Pain Management Reference Number: CP.MP.169 Last Review Date: 08/18 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Clinical Policy: for Pain Management Reference Number: CP.MP.169 Last Review Date: 08/18 See Important Reminder at the end of this policy for important regulatory and legal information. Coding Implications
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
IMPORTANT REMINDER DESCRIPTION
 Medical Policy Manual Medicine, Policy No. 40 Prolotherapy Next Review: January 2019 Last Review: February 2018 Effective: March 1, 2018 IMPORTANT REMINDER Medical Policies are developed to provide guidance
Medical Policy Manual Medicine, Policy No. 40 Prolotherapy Next Review: January 2019 Last Review: February 2018 Effective: March 1, 2018 IMPORTANT REMINDER Medical Policies are developed to provide guidance
STAIRS. What s Hip: Top 5 Hip Problems in Primary Care. I have no relevant disclosures. Top 5 (or 6) Pathologies. Big 3- Questions to Ask
 Pathologies. Big 3- Questions to Ask") I have no relevant disclosures. What s Hip: Top 5 Hip Problems in Primary Care Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery December, 2015
I have no relevant disclosures. What s Hip: Top 5 Hip Problems in Primary Care Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery December, 2015
MOTION DIAGNOSTIC IMAGING (CMDI)/ GAIT ANALYSIS
/ GAIT ANALYSIS") Page: 1 of 5 MEDICAL POLICY MEDICAL POLICY DETAILS Medical Policy Title COMPUTERIZED MOTION DIAGNOSTIC IMAGING (CMDI)/ GAIT ANALYSIS Policy Number 2.01.13 Category Technology Assessment Effective Date
Page: 1 of 5 MEDICAL POLICY MEDICAL POLICY DETAILS Medical Policy Title COMPUTERIZED MOTION DIAGNOSTIC IMAGING (CMDI)/ GAIT ANALYSIS Policy Number 2.01.13 Category Technology Assessment Effective Date
Evaluation and Management of Knee Pain. Michael Cassat, MD University of Arkansas for Medical Sciences
 Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Evaluation and Management of Knee Pain Michael Cassat, MD University of Arkansas for Medical Sciences Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
RECIPES FOR RATINGS !!! A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P.
 RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
RECIPES FOR RATINGS 1. THE "0% WPI" RATINGS A. FIBROMYALGIA: 0% WPI P. 569 B. THORACIC OUTLET SYNDROME 0% WPI P. 569 C. MYOFASCIAL PAIN SYNDROME 0% WPI P. 569 D. TENDINITIS OF UPPER EXTREMITY 0% WPI P.
Laser Therapy for Epicondylitis
 Laser Therapy for Epicondylitis BMC Musculoskelet Disord. 2008 May 29;9:75. doi: 10.1186/1471-2474-9-75. A systematic review with procedural assessments and meta-analysis of low level laser therapy in
Laser Therapy for Epicondylitis BMC Musculoskelet Disord. 2008 May 29;9:75. doi: 10.1186/1471-2474-9-75. A systematic review with procedural assessments and meta-analysis of low level laser therapy in
The Lumbopelvic & Hip Region. Contents. Contents. Chapter 5 Assessment & Treatment incorporating corrective exercises/stretching. Chapter 6 Quiz T & F
 The Lumbopelvic & Hip Region Contents Chapter 1 The lumbopelvic & hip region Chapter 2 Muscle firing patterns/endurance Chapter 3 Altered biomechanics to the & hip region lumbopelvic Chapter 4 - Musculoskeletal
The Lumbopelvic & Hip Region Contents Chapter 1 The lumbopelvic & hip region Chapter 2 Muscle firing patterns/endurance Chapter 3 Altered biomechanics to the & hip region lumbopelvic Chapter 4 - Musculoskeletal
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
British Journal of Rheumatology 1991; 30:
 British Journal of Rheumatology 1991; 30:468-470 CASE REPORT CARPAL TUNNEL SYNDROME COMPLICATED BY REFLEX SYMPATHETIC DYSTROPHY SYNDROME BY M.-A. FITZCHARLES AND J.M. ESDAILE Rheumatic Disease Unit, McGill
British Journal of Rheumatology 1991; 30:468-470 CASE REPORT CARPAL TUNNEL SYNDROME COMPLICATED BY REFLEX SYMPATHETIC DYSTROPHY SYNDROME BY M.-A. FITZCHARLES AND J.M. ESDAILE Rheumatic Disease Unit, McGill
Hip Injuries & Arthroscopy in Athletes
 Hip Injuries & Arthroscopy in Athletes John P Salvo, MD Sports Medicine Rothman Institute Philadelphia, PA EATA Annual Meeting January, 2011 Hip Injuries & Arthroscopy in Anatomy History Physical Exam
Hip Injuries & Arthroscopy in Athletes John P Salvo, MD Sports Medicine Rothman Institute Philadelphia, PA EATA Annual Meeting January, 2011 Hip Injuries & Arthroscopy in Anatomy History Physical Exam
VSRF+ Orthopaedics Referral Form. Triage Categories/ Appointment Wait Time Emergency/After Hours:
 Northern Health Orthopaedic Pre referral Management Guidelines Orthopaedic Consultants: Mr A. Bonomo Mr R. Hau Mr A. Chia Mr D. Robin Ms J. Gentle Mr A. Chehata Mr R. Unni Osteoarthritis Hip & Knee Service
Northern Health Orthopaedic Pre referral Management Guidelines Orthopaedic Consultants: Mr A. Bonomo Mr R. Hau Mr A. Chia Mr D. Robin Ms J. Gentle Mr A. Chehata Mr R. Unni Osteoarthritis Hip & Knee Service
Use of anatomic measurement to guide injection of botulinum toxin for the management of chronic lateral epicondylitis: a randomized controlled trial
 CMAJ Use of anatomic measurement to guide injection of botulinum toxin for the management of chronic lateral epicondylitis: a randomized controlled trial Ramin Espandar MD, Pedram Heidari MD, Mohammad
CMAJ Use of anatomic measurement to guide injection of botulinum toxin for the management of chronic lateral epicondylitis: a randomized controlled trial Ramin Espandar MD, Pedram Heidari MD, Mohammad
Anterior knee pain.
 Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Anterior knee pain What are the symptoms? Anterior knee pain is very common amongst active adolescents and athletes participating in contact sports. It is one of the most common problems/injuries seen
Zorvolex Approved by FDA for Treatment of Osteoarthritis Pain
 Zorvolex Approved by FDA for Treatment of Osteoarthritis Pain Am J Orthop. 2014 September;43(9) Authors: Author Affiliation Disclosures Iroko Pharmaceuticals (Philadelphia, Pennsylvania) announced that
Zorvolex Approved by FDA for Treatment of Osteoarthritis Pain Am J Orthop. 2014 September;43(9) Authors: Author Affiliation Disclosures Iroko Pharmaceuticals (Philadelphia, Pennsylvania) announced that
Back and Neck Injuries: Surgical Advances and Treatment
 Back and Neck Injuries: Surgical Advances and Treatment Ara Deukmedjian, MD Board Certified Neurosurgeon June 8, 2017 1 2 Spinal Joints: Anatomy Two types of Spinal Joints: Spinal (intervertebral) disc
Back and Neck Injuries: Surgical Advances and Treatment Ara Deukmedjian, MD Board Certified Neurosurgeon June 8, 2017 1 2 Spinal Joints: Anatomy Two types of Spinal Joints: Spinal (intervertebral) disc
Evaluation of Posterior Hip Pain
 Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
What s Hip: Common Hip Problems and Kids and Adults
 What s Hip: Common Hip Problems and Kids and Adults Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery I have no relevant disclosures. 2 1 Most
What s Hip: Common Hip Problems and Kids and Adults Alan Zhang MD Assistant Professor Sports Medicine and Hip Arthroscopy UCSF Department of Orthopaedic Surgery I have no relevant disclosures. 2 1 Most
Soleus 75 (6 ml) 0 (6 ml) 75 (6 ml. Tibialis posterior 75 (6 ml) 0 (6 ml) 75 (6 ml) Total 300 (24 ml) 0 (24 ml) 300 (24 ml) Dose: U (solution volume)
 0 (6 ml) 75 (6 ml. Tibialis posterior 75 (6 ml) 0 (6 ml) 75 (6 ml) Total 300 (24 ml) 0 (24 ml) 300 (24 ml) Dose: U (solution volume)") Study No.: BTX108512 Title: A Multicenter Study to Evaluate the Efficacy and Safety in Patients with Post-Stroke lower Limb Spasticity Receiving a Double-Blind, -Controlled GSK1358820 Treatment Followed
Study No.: BTX108512 Title: A Multicenter Study to Evaluate the Efficacy and Safety in Patients with Post-Stroke lower Limb Spasticity Receiving a Double-Blind, -Controlled GSK1358820 Treatment Followed
Rance McClain, DO, FACOFP, FAOASM Associate Dean, Clinical Sciences Professor, Clinical Sciences William Carey University College of Osteopathic
 Rance McClain, DO, FACOFP, FAOASM Associate Dean, Clinical Sciences Professor, Clinical Sciences William Carey University College of Osteopathic Medicine Identify common orthopedic conditions presenting
Rance McClain, DO, FACOFP, FAOASM Associate Dean, Clinical Sciences Professor, Clinical Sciences William Carey University College of Osteopathic Medicine Identify common orthopedic conditions presenting
John J Christoforetti, MD Pittsburgh, Pennsylvania
 ARTHROSCOPIC ASSISTED PROXIMAL HAMSTRINGS REPAIR WITH HUMAN ACELLULAR DERMAL ALLOGRAFT PATCH AUGMENTATION FOR REVISION OF FAILED PROXIMAL HAMSTRINGS REPAIR: SHORT TERM CLINICAL AND MRI RESULT John J Christoforetti,
ARTHROSCOPIC ASSISTED PROXIMAL HAMSTRINGS REPAIR WITH HUMAN ACELLULAR DERMAL ALLOGRAFT PATCH AUGMENTATION FOR REVISION OF FAILED PROXIMAL HAMSTRINGS REPAIR: SHORT TERM CLINICAL AND MRI RESULT John J Christoforetti,
Human Anatomy Biology 351
 Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Human Anatomy Biology 351 Lower Limb Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average, between
Module Eight. Application of Health Assessment NUR 225. Physical examination of Musculoskeletal System. King Saud University. Collage of Nursing
 King Saud University Collage of Nursing Medical Surgical Nursing depart Application of Health Assessment NUR 225 Module Eight Physical examination of Musculoskeletal System Obtaining a health history Ask
King Saud University Collage of Nursing Medical Surgical Nursing depart Application of Health Assessment NUR 225 Module Eight Physical examination of Musculoskeletal System Obtaining a health history Ask
Introduction. Introduction. Introduction PREDICTIVE FACTORS FOR FOR RADIAL SHOCK WAVE THERAPY IN THE TREATMENT OF CHRONIC PLANTAR FASCIOPATHY
 PREDICTIVE FACTORS FOR FOR RADIAL SHOCK WAVE THERAPY IN THE TREATMENT OF CHRONIC PLANTAR FASCIOPATHY JAVIER CRUPNIK, PT ALDO BUSTOS, MD Introduction Plantar fasciitis is the most common cause of heel pain.
PREDICTIVE FACTORS FOR FOR RADIAL SHOCK WAVE THERAPY IN THE TREATMENT OF CHRONIC PLANTAR FASCIOPATHY JAVIER CRUPNIK, PT ALDO BUSTOS, MD Introduction Plantar fasciitis is the most common cause of heel pain.
Benefits of Aspiration and Injection JOINT INJECTIONS. Injection Indications. Mechanism of Action 1/11/2016
 Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Benefits of Aspiration and Injection JOINT INJECTIONS Mark Niedfeldt, M.D. Medical College of Wisconsin Decrease or resolution of pain Decrease or resolution of inflammation Decrease or resolution of effusion
Plantar fasciitis: p. 1/6
 Clinical trials published in the international peer-reviewed literature 1 demonstrating efficacy and safety of treatment with the EMS Swiss Dolorclast according to Evidence Based Medicine criteria 2 :
Clinical trials published in the international peer-reviewed literature 1 demonstrating efficacy and safety of treatment with the EMS Swiss Dolorclast according to Evidence Based Medicine criteria 2 :
Timothy S. Ackerman, D.O. Arlington Orthopedics Harrisburg, PA
 Timothy S. Ackerman, D.O. Arlington Orthopedics Harrisburg, PA Introduction We are reminded that the U.S. Population is growing older as the youngest of baby boomers will be turning 50 in 2014. Greatest
Timothy S. Ackerman, D.O. Arlington Orthopedics Harrisburg, PA Introduction We are reminded that the U.S. Population is growing older as the youngest of baby boomers will be turning 50 in 2014. Greatest
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Priorities Forum Statement
 Priorities Forum Statement Number 75 Subject Autologous Blood and Platelet-Rich Plasma Injection in Tendinopathy Date of decision February 2017 Date refreshed February 2017 Date of review February 2020
Priorities Forum Statement Number 75 Subject Autologous Blood and Platelet-Rich Plasma Injection in Tendinopathy Date of decision February 2017 Date refreshed February 2017 Date of review February 2020
An Easy Guide to TENS Pain Relief
 An Easy Guide to TENS Pain Relief 68 ElectroMedical Solutions 1715 E. Bay Dr. Largo, FL 33771 Toll Free 866-243-TENS (8367) Toll Free Fax 866-242-TENS (8367) www.electromedicalsolutions.com A book of indications,
An Easy Guide to TENS Pain Relief 68 ElectroMedical Solutions 1715 E. Bay Dr. Largo, FL 33771 Toll Free 866-243-TENS (8367) Toll Free Fax 866-242-TENS (8367) www.electromedicalsolutions.com A book of indications,
OCCUPATIONAL INJURIES OF THE ELBOW
 PLEASE STAND BY WEBINAR WILL BEGIN AT 12:00 PM PST FOR AUDIO: CALL 866-740-1260 / ACCESS CODE: 764-4915# JAMES VAN DEN BOGAERDE, MD OCCUPATIONAL INJURIES OF THE ELBOW Conflict of Interest Disclosure I,
PLEASE STAND BY WEBINAR WILL BEGIN AT 12:00 PM PST FOR AUDIO: CALL 866-740-1260 / ACCESS CODE: 764-4915# JAMES VAN DEN BOGAERDE, MD OCCUPATIONAL INJURIES OF THE ELBOW Conflict of Interest Disclosure I,
JMSCR Volume 03 Issue 01 Page January 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Management of Chronic Plantar Fasciitis using Hyperosmolar Dextrose Injection Authors Ansarul Haq Lone 1, Omar Khursheed 2, Shakir Rashid
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Management of Chronic Plantar Fasciitis using Hyperosmolar Dextrose Injection Authors Ansarul Haq Lone 1, Omar Khursheed 2, Shakir Rashid
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital
 Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Dr Ng Swee Cheng Senior Consultant Khoo Teck Puat Hospital 1. Soft Tissue Rheumatism 2. Myofascial Pain 3. Neurovascular compression Syndromes 4. Complex Regional Pain Syndromes Tendinitis, tenosynovitis
Workplace Hand Injuries & Disorders: Evaluation and Treatments. Hervey L. Kimball MD, MS Hand Surgical Associates Occupational Medicine Center
 Workplace Hand Injuries & Disorders: Evaluation and Treatments Hervey L. Kimball MD, MS Hand Surgical Associates Occupational Medicine Center Outline Hand Anatomy and Function Workplace injuries & Case
Workplace Hand Injuries & Disorders: Evaluation and Treatments Hervey L. Kimball MD, MS Hand Surgical Associates Occupational Medicine Center Outline Hand Anatomy and Function Workplace injuries & Case
Osteoporosis. World Health Organisation
 Osteoporosis A systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue with subsequent increased risk of fracture. World Health Organisation Epidemiology
Osteoporosis A systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue with subsequent increased risk of fracture. World Health Organisation Epidemiology
Arthritis and Rheumatology Clinics of Kansas Patient Education
 Arthritis and Rheumatology Clinics of Kansas Patient Education Regional Pain Syndromes Introduction: At some time in the course of life, virtually everyone will experience pain in a tendon, muscle, or
Arthritis and Rheumatology Clinics of Kansas Patient Education Regional Pain Syndromes Introduction: At some time in the course of life, virtually everyone will experience pain in a tendon, muscle, or
GP practical procedures Joint and soft tissue injections. Dr Monica Gupta Dr Hilary Wilson Dr John Hunter
 GP practical procedures Joint and soft tissue injections Dr Monica Gupta Dr Hilary Wilson Dr John Hunter Outline of talk Acute mono arthritis Pros & Cons of injections Regional problems Shoulder Knee Soft
GP practical procedures Joint and soft tissue injections Dr Monica Gupta Dr Hilary Wilson Dr John Hunter Outline of talk Acute mono arthritis Pros & Cons of injections Regional problems Shoulder Knee Soft
[ clinical commentary ]
![[ clinical commentary ]](/thumbs/73/68870411.jpg "[ clinical commentary ]") RobRoy L. Martin, PT, PhD, CSCS 1 James J. Irrgang, PT, PhD, ATC 2 A Survey of Self-reported Outcome Instruments for the Foot and Ankle Self-reported outcome instruments, which are used to measure change
RobRoy L. Martin, PT, PhD, CSCS 1 James J. Irrgang, PT, PhD, ATC 2 A Survey of Self-reported Outcome Instruments for the Foot and Ankle Self-reported outcome instruments, which are used to measure change
ICF-based Clinical Practice Guidelines for Common Musculoskeletal Conditions. Board of Directors Meeting. February 2015
 ICF-based Clinical Practice Guidelines for Common Musculoskeletal Conditions Board of Directors Meeting February 2015 Submitted by: Joe Godges DPT* and Christine McDonough PT, PhD** *ICF-based Clinical
ICF-based Clinical Practice Guidelines for Common Musculoskeletal Conditions Board of Directors Meeting February 2015 Submitted by: Joe Godges DPT* and Christine McDonough PT, PhD** *ICF-based Clinical
Human Anatomy and Physiology I Laboratory
 Human Anatomy and Physiology I Laboratory Gross Anatomy of the Muscular System (Two weeks) 1 This lab involves study of the laboratory exercise Gross Anatomy of the Muscular System. Complete the Review
Human Anatomy and Physiology I Laboratory Gross Anatomy of the Muscular System (Two weeks) 1 This lab involves study of the laboratory exercise Gross Anatomy of the Muscular System. Complete the Review
Eastern Bodywork & Neuromuscular Sports Injury and Medicine Massage Therapy Explained
 Eastern Bodywork & Neuromuscular Sports Injury and Medicine Massage Therapy Explained LA#8419 You Can Experience Ease of Movement Once Again! Call Today for your appointment! Higher Purpose Healing 1 (504)
Eastern Bodywork & Neuromuscular Sports Injury and Medicine Massage Therapy Explained LA#8419 You Can Experience Ease of Movement Once Again! Call Today for your appointment! Higher Purpose Healing 1 (504)
ORIGINAL ARTICLE. Department of Orthopedic Surgery, Mashad University of Medical Sciences, Mashad, Iran
 Arch Iranian Med 2003; 6 (3): 196 199 ORIGINAL ARTICLE INJECTION OF METHYLPREDNISOLONE AND LIDOCAINE IN THE TREATMENT OF MEDIAL EPICONDYLITIS: A RANDOMIZED CLINICAL TRIAL Mahmood Bahari MD, Mohammad Gharehdaghi
Arch Iranian Med 2003; 6 (3): 196 199 ORIGINAL ARTICLE INJECTION OF METHYLPREDNISOLONE AND LIDOCAINE IN THE TREATMENT OF MEDIAL EPICONDYLITIS: A RANDOMIZED CLINICAL TRIAL Mahmood Bahari MD, Mohammad Gharehdaghi
Health & Fitness. About Loudoun Sports Therapy
 Health & Fitness The Newsletter About Your Health And Caring For Your Body About Loudoun Sports Therapy The Physical Therapists at Loudoun Sports Therapy Center are medically trained, licensed professionals
Health & Fitness The Newsletter About Your Health And Caring For Your Body About Loudoun Sports Therapy The Physical Therapists at Loudoun Sports Therapy Center are medically trained, licensed professionals
Management of Chronic Elbow Pain
 Mr. Nashat Siddiqui Consultant Upper Limb Orthopaedic Surgeon Management of Chronic Elbow Pain Patients presenting with elbow pain can pose a diagnostic challenge, especially if there is no obvious recent
Mr. Nashat Siddiqui Consultant Upper Limb Orthopaedic Surgeon Management of Chronic Elbow Pain Patients presenting with elbow pain can pose a diagnostic challenge, especially if there is no obvious recent
ACPOMIT Conference 2013 Workshop: Hand and Wrist
 ACPOMIT Conference 2013 Workshop: Hand and Wrist Sarah Turner, MCSP, Clinical Specialist in Hand Therapy Grad Dip Injection Therapy Workshop! Trigger Finger! OA 1 st CMC joint! De Quervain s Tenosynovitis!
ACPOMIT Conference 2013 Workshop: Hand and Wrist Sarah Turner, MCSP, Clinical Specialist in Hand Therapy Grad Dip Injection Therapy Workshop! Trigger Finger! OA 1 st CMC joint! De Quervain s Tenosynovitis!
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy
 The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
The Joints are Painful & Swollen: Do I give Steroids? Dr Tom Kennedy Learning Objectives When to use an acute rheumatology service Appropriate use of steroids by condition Injection or Oral or Intramuscular
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Section: Surgery Effective Date: April 15, 2016 Subsection: Original Policy Date: March 18, 2016 Subject: Page: 1 of 9
 Subject: Radiofrequency Ablation of Peripheral Nerves to Last Review Status/Date: March 2016 Page: 1 of 9 Radiofrequency Ablation of Peripheral Nerves to Summary Radiofrequency ablation of nerves has been
Subject: Radiofrequency Ablation of Peripheral Nerves to Last Review Status/Date: March 2016 Page: 1 of 9 Radiofrequency Ablation of Peripheral Nerves to Summary Radiofrequency ablation of nerves has been
QuickTime and a decompressor are needed to see this picture. QuickTime and a decompressor are needed to see this picture.
 The Hip Andrew Pearse Consultant Trauma and Orthopaedics Worcestershire Acute Hospitals NHS Trust Introduction Brief anatomy and topography History & examination Osteoarthritis Investigations Referral
The Hip Andrew Pearse Consultant Trauma and Orthopaedics Worcestershire Acute Hospitals NHS Trust Introduction Brief anatomy and topography History & examination Osteoarthritis Investigations Referral
Introduction to Ultrasound Guided Shoulder Injections. Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital
 Introduction to Ultrasound Guided Shoulder Injections Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital Safe Robust Aim: to provide a service that is Cost effective To enable patients
Introduction to Ultrasound Guided Shoulder Injections Alison Hall Consultant Sonographer Keele University Cannock Chase Hospital Safe Robust Aim: to provide a service that is Cost effective To enable patients
Prolotherapy. Policy Number: Last Review: 1/2019 Origination: 7/2008 Next Review: 7/2020
 Prolotherapy Policy Number: 2.01.26 Last Review: 1/2019 Origination: 7/2008 Next Review: 7/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for prolotherapy. This
Prolotherapy Policy Number: 2.01.26 Last Review: 1/2019 Origination: 7/2008 Next Review: 7/2020 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage for prolotherapy. This
Botulinum Toxin A (Botox) for Treatment of Proximal Myofascial Pain in Complex Regional Pain Syndrome: Two Cases
 for Treatment of Proximal Myofascial Pain in Complex Regional Pain Syndrome: Two Cases") Botulinum Toxin A (Botox) for Treatment of Proximal Myofascial Pain in Complex Regional Pain Syndrome: Two Cases Delaram Safarpour, MD, Bahman Jabbari, MD Pain Medicine 2010; 11: 1415 1418 Wiley Periodicals,
Botulinum Toxin A (Botox) for Treatment of Proximal Myofascial Pain in Complex Regional Pain Syndrome: Two Cases Delaram Safarpour, MD, Bahman Jabbari, MD Pain Medicine 2010; 11: 1415 1418 Wiley Periodicals,
ClinialTrials.gov Identifier: Sponsor/company: sanofi-aventis
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinialTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinialTrials.gov
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Joint Disorders. Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System
 Module 7 -Chapter 10. Overview Disorders of the Muscular System Disorders of the Skeletal System") Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Musculoskeletal Disorders (Part B-2) Module 7 -Chapter 10 Overview Disorders of the Muscular System Disorders of the Skeletal System Susie Turner, MD 1/9/13 Joint Disorders Arthritis Inflammation of Joint
Hamstring Injury: When to Consider Surgical Treatment
 Hamstring Injury: When to Consider Surgical Treatment Prof. dr. Gino Kerkhoffs Orthopaedic Surgery www.acesamsterdam.nl Gino Kerkhoffs Hans Tol Guus Reurink Mario Maas Pau Golanó Rolf Peters Maarten Moen
Hamstring Injury: When to Consider Surgical Treatment Prof. dr. Gino Kerkhoffs Orthopaedic Surgery www.acesamsterdam.nl Gino Kerkhoffs Hans Tol Guus Reurink Mario Maas Pau Golanó Rolf Peters Maarten Moen
Kineto. Orthopaedics & Rehabilitation Products
 Member of Vincent Medical Holdings Limited Kineto Orthopaedics & Rehabilitation Products Our orthopaedic and rehabilitation products comprise of a variety of adjustable rehabilitation braces for support,
Member of Vincent Medical Holdings Limited Kineto Orthopaedics & Rehabilitation Products Our orthopaedic and rehabilitation products comprise of a variety of adjustable rehabilitation braces for support,
Muscles of the Gluteal Region
 Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
Muscles of the Gluteal Region 1 Some of the most powerful in the body Extend the thigh during forceful extension Stabilize the iliotibial band and thoracolumbar fascia Related to shoulders and arms because
A study of functional outcome after Primary Total Knee Arthroplasty in elderly patients
 Original Research Article A study of functional outcome after Primary Total Knee Arthroplasty in elderly patients Ragesh Chandran 1*, Sanath K Shetty 2, Ashwin Shetty 3, Bijith Balan 1, Lawrence J Mathias
Original Research Article A study of functional outcome after Primary Total Knee Arthroplasty in elderly patients Ragesh Chandran 1*, Sanath K Shetty 2, Ashwin Shetty 3, Bijith Balan 1, Lawrence J Mathias
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Young Adult Hip problems. Aresh Hashemi-Nejad FRCS(Orth)
") Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Young Adult Hip problems Aresh Hashemi-Nejad FRCS(Orth) RNOH founded 1837 by William Little 14 year old presenting with limp Knee pain on and off 4 months Limps Aresh Hashemi-Nejad FRCS(Orth) The Royal
Collected Scientific Research Relating to the Use of Osteopathy with Foot and ankle conditions
 Collected Scientific Research Relating to the Use of Osteopathy with Foot and ankle conditions Important: 1) Osteopathy involves helping people's own self-healing abilities to work better, rather that
Collected Scientific Research Relating to the Use of Osteopathy with Foot and ankle conditions Important: 1) Osteopathy involves helping people's own self-healing abilities to work better, rather that