Abdominal Pain in Pediatric Patients Image Gently
|
|
|
- Pauline Kennedy
- 6 years ago
- Views:
Transcription
1 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated products and/or services. Challenges of Imaging Infants and Children with Abdominal Pain History and physical findings overlap Diarrhea Bilious vomiting Blood in stool Episodic crying Poorly localized pain Pathologies cluster in specific age groups Newborn Congenital obstructive lesions 1 week 2 months Hypertrophic pyloric stenosis 2-5 months Incarcerated hernia 5 months 2 years Intussusception 3 yrs adolescence Appendicitis 1
2 Learning Objectives Understand varieties of pathology that cause abdominal pain and vomiting in infants and children Plan safe and effective imaging protocols for children with abdominal based on the latest evidence Image Gently Reducing radiation exposure to children during medical imaging Using lower dose CT, DR protocols Implementing dose saving techniques during fluoroscopy Developing guidelines for when imaging is needed Creating imaging algorithms that begin with low dose, effective imaging modalities Most Appropriate Imaging Many factors involved Clear clinical indications Scientific data ACR appropriateness guidelines Patient expectations Referring physician input Sedation requirements Availability of equipment and expertise 2


3 Abdominal Radiographs (Get No Respect) Can be diagnostic When not diagnostic, can provide useful information Bowel obstruction Presence Location Guidance for next exam Small bowel entrapment by magnetic beads Duodenal web XR Non-diagnostic Normal or findings of proximal obstruction Fluoroscopy bilious vomiting Ultrasound most often in children >5 months of age Distal obstruction Fluoroscopy US CT/MRI select circumstances 3

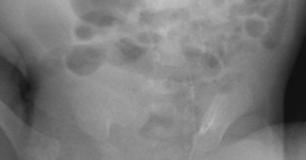




4 3 month old with increasing vomiting Duodenal Web Duodenal Web (missed on initial UGI series 4







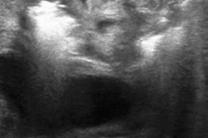
5 9 month and old fever with fever and vomiting Intussusception Most likely cause of small bowel obstruction between 5 months to 2 years or age 1 to 8 Weeks of Age Projectile vomiting Gastroesophageal reflux Gastric outlet obstruction Pyloric muscle Spasm Hypertrophy Hypertrophic pyloric stenosis Most common 3-6 wks of age Not seen in first week of life Very uncommon after 8 weeks of age Normal Pylorus 1-2 mm muscle Length negligible Opens frequently Emptying usually evident D 5







6 Hypertrophic Pyloric Stenosis Transverse 3 mm + muscle 1.5 cm + length Little or no emptying Longitudinal False Positives Contracted, elongated antrum secondary to spasm, inadequate fluid in antrum Incorrect measurements Avoid Gastric Overdistention Stomach Pylorus and duodenum more posteriorly positioned Can make them less easily visible 6








7 Look for other causes of obstruction Gastric antral web Antral masses Adjacent masses/cysts Gastroesophageal Junction The Other Gastric Outlet Often clearly seen with a fluid-distended stomach Gastroesophageal reflux can be identified May obviate the need for an UGI series Often imaged inadvertently Transverse Longitudinal US of the GE Junction 7









8 GE Junction Pylorus L S D GE junction S Duodenal Web Acute Duodenal Obstruction SMV to the Rt of SMA is abnormal, suggests malrotation Midgut volvulus Bilious vomiting Can occur at any age Whirlpool sign 8







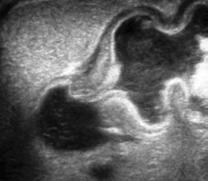
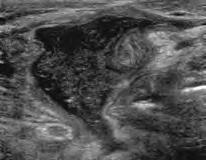
9 Signs of midgut volvulus Abnormal duodenojejunal junction position + swirling Complete obstruction in D3 Midgut Volvulus Intussusception Acute ileocolic obstruction (5months 3 yrs age) Often obstruction not evident on radiographs Symptoms nonspecific Vomiting Intermittent crying Lethargy Early identification of intussusception makes nonsurgical reduction more likely 9
")





10 Ultrasound for Intussusception High frequency (7-12 mhz) transducer Complex mass Target, donut appearance Transverse High sensitivity and specificity If US negative, contrast enema not needed Long Signs of Difficult Enema Reduction Symptoms for more than 48 hours Age under 3 months Small bowel obstruction Target rim > 1 cm in thickness Large amount of trapped fluid Distal migration of intussusceptum 10





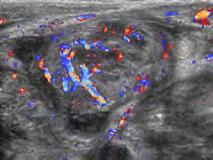
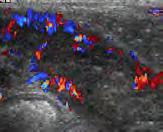
11 Absent Doppler Flow in Intusussceptum Suggests ischemia, but not a contraindication to enema reduction Be prepared to decompress Free Fluid with Intussusception Small amounts are common and do not indicate perforation Complex fluid consult with surgery Transient Intussusception Common in patients with hyperperistalsis Only need surgery if persistent and longer than 3.5 cm in length Munden, AJR 2007;188:







12 18 month old with abdominal pain and fever Perforated Appendicitis Mimics Intussusception Fluid Thickened bowel can resemble intussusceptum Complex free fluid is a clue Pseudomembranous colitis Shiga toxin positive colitis Henoch Schoenlein purpura Regional enteritis 12

: e88.")
13 2 yrs old and greater Inflammatory conditions predominate Appendicitis Mesenteric adenitis Ileocolitis/gastroenteritis Henoch-Schoenlein purpura Hemolytic uremic syndrome Regional enteritis All can be diagnosed with US Pediatric Appendicitis Score Clinical decision rule 8 clinical signs and symptoms Further imaging indicated with scores between 4-7 Imaging with US when scores fall in the intermediate range diagnoses appendicitis with high sensitivity and specificity Samuel M. Pediatric appendicitis score. J Pediatr Surg. 2002;37(6): Saucier A. Prospective evaluation of a clinical pathway for suspected appendicitis. Pediatrics. 2014;133 (1): e88. US for Appendicitis Still accepted as best first screening exam Staged approach using CT for equivocal cases highly accurate Sensitivity 98.6% Specificity 90.6% CT avoided in 53% Krishnamoorthi, Radiol Jan



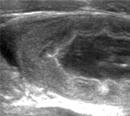
14 Normal Appendix Freely mobile Normal bowel peristalsis Minimal visible periappendiceal fat Appendix Size in Appendicitis 6 mm or > in diameter abnormal PPV 63% NPV 100% More useful for excluding appendicitis Rettenbacher, Radiology 2011; 218: mm or > Similar accuracy Goldin, Pediatr Radiol 2011; 41: 993. Causes of Variable Appendix Size Overlap in diameter between normal and inflamed appendices CT normal can be up to 8.7 mm Benign processes can distend the normal appendix Patient-specific factors influence diameter Grows with age Contents such as stool increase diameter Technical factors and variability in measurement Coronal measurements slightly larger than axial Differences between observers Trout AT, AJR 2014; 202:936. Dietz KR, Pediatr Radiol 2013; 43:232. Trout AT, Pediatr Radiol 2016; 46:



 22:643-649 Acute")




15 Lymphoid Hyperplasia of the Appendix Enlarged lymphoid tissue in the wall of appendix Response to viral infection Can mimic a fluid-filled appendix Look for central mucosal stripe May result in increased size Can cause obstruction of the appendiceal lumen Tip appendicitis Swischuk, et al, Emergency Radiology (2015) 22: Acute suppurative appendicitis Normal appendix Compressibility can be difficult to demonstrate Appendicitis Normal Lack of compressibility one of the most common findings in false positive US Trout AT et. al. A critical evaluation of US for the diagnosis of pediatric acute appendicitis in a real-life setting: how can we improve the diagnostic value of sonography? Pediatr Radiol (2012) 42:






16 Perforated Appendix Dilated small bowel RLQ mass Colon cut-off Flank stripe Perforated appendicitis with abscess Most common cause of SBO over the age of 2 years Secondary findings can be strong indicators of appendicitis Thickened Echogenic Fat = Inflammation Absent peristalsis = ileus Calcifications/fecaliths Localized RLQ tenderness Complex peritoneal fluid Wiersma, Eur Radiol 2009; 19:





17 Standardized Reporting Most valuable for indeterminate exams Ensures that sonographer evaluates for all secondary findings Improves radiologist s accuracy Allows referring physician to understand the radiologist s decision-making process Nielsen JW et.al., Reducing CT scans for appendicitis by introduction of a standardized and validated US report template. J Pediatr Surg 3015; 50: Fallon SC et.al., Development and validation of an US scoring system for children with suspected acute appendicitis. Pediatr Radiol 2015; doi: /s Abdominal/Pelvic CT in Children Often challenging because of lack of abdominal fat Child-size your CT protocols Image Gently website Scan only when necessary Scan only the indicated region Scan only once Ultrafast MRI for Appendicitis Children of age 4-17 years No sedation or contrast Limited exam Axial and coronal SSFSE w/wo fat sat Axial DWI Scan times less than 9 minutes Normal appendix seen 43% of the time Sens/spec 100/99% PPV 98% NPV 100% Johnson, AJR 2012, Jun 198:1424 No difference in time to antibiotics or surgery, negative appendectomy rate, perforation rate, or length of stay. Gudrun A et al, Pediatrics 2014 ;133:








18 MRI for Appendicitis Multiple studies comparing MRI to CT Meta-analysis of accuracy of MRI for appendicitis (Duke E, et al. AJR 2016; ) Sensitivity and specificity 96% Children and pregnant women Personal experience patients CT almost completely eliminated Time from first image to incision (10.7 hours) Negative appendectomy rate (3.7 %) Median imaging costs increased Appendicitis Normal appendix 18

19 Non-GI Causes of Abdominal Pain 5 yr old with abdominal pain, fever, and vomiting Hospital 1 Abdominal US Hospital 2 Abdominal US Abdomen MRI All normal. Right Upper Lobe Pneumonia Imaging Abdominal Emergencies in Children Use age and clinical signs to select best first exam Radiographs can have value US highly reliable with experience and when performed with proper technique Proper fluid distension and positioning Taking time to assess dynamic factors Noting important secondary findings Consider MRI as alternative to CT susan.dsusan.d.john@uth.tmc.edu 19
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success
 Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Vomiting in children: The good coordination between radiologists and pediatricians is the key to success C. Santos Montón 1, M. T. Garzon Guiteria 2, A. Hortal Benito-Sendín 1, K. El Karzazi 1, P. Sanchez
Infantile Hypertrophic Pyloric Stenosis
 A Sonographic walk-through: Infantile Hypertrophic Pyloric Stenosis Tara K. Cielma, RDMS, RDCS, RVT, RT(S) Anjum N. Bandarkar, MD, Adebunmi O. Adeyiga, MD, Diagnostic Imaging and Radiology, Children s
A Sonographic walk-through: Infantile Hypertrophic Pyloric Stenosis Tara K. Cielma, RDMS, RDCS, RVT, RT(S) Anjum N. Bandarkar, MD, Adebunmi O. Adeyiga, MD, Diagnostic Imaging and Radiology, Children s
Emergent Pediatric Ultrasound. Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound
 Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Emergent Pediatric Ultrasound Katharine Dennis, RDMS/RVT Tiffany Schultz, RDMS UNC Health Care Dept of General Ultrasound Introduction Learning Objectives Review common pediatric emergent ultrasound exams
Hirschprung s. Meconium plug R/S >1 R/S <1
 NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR
 Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Imaging Children with Acute Abdominal Pain -- Role/Protocols of US, CT, MR Kimberly E. Applegate, MD, MS Emory University Financial disclosures: AIM (American Imaging Management) radiation protection advisory
Ultrasound of: Appendicitis Intussusception Pyloric Stenosis
 Ultrasound of: Appendicitis Intussusception Pyloric Stenosis Andrew Phelps MD Assistant Professor Pediatric Radiology UCSF Benioff Children s Hospital No Disclosures Take Home Message Appendicitis occurs
Ultrasound of: Appendicitis Intussusception Pyloric Stenosis Andrew Phelps MD Assistant Professor Pediatric Radiology UCSF Benioff Children s Hospital No Disclosures Take Home Message Appendicitis occurs
Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography
 3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
3668 Radiographer Text 1/4/04 2:57 PM Page 11 The Radiographer vol. 51: 11-17 Sonographic Appearances of Common Gut Pathology in Paediatric Patients: Comparison with Plain Abdominal Radiography Lino Piotto
Pediatric Surgical Emergencies Veronica Victorian, PA-C
 Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Pediatric abdominal emergencies In the first year of life
 Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Common Pediatric abdominal emergencies In the first year of life Kristian Stien Thomassen Section of Pediatric Radiology Dept. of Radiology and Nuclear Medicine Oslo University Hospital Understand the
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Summary and conclusions
 Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Pediatric Radiology Update
 Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
Pediatric Radiology Update Douglas Rivard, DO Vice Chairman, Radiology Dept Children s Mercy Hospital Asst Professor of Radiology University of Missouri-Kansas City Objectives Review radiation biology
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: GI SURGICAL EMERGENCIES: VOMITING
 GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
Pelvic Pain in the Pediatric Patient Susan D. John, M.D.
 Pelvic Pain in the Pediatric Patient Susan D. John, M.D. RSNA 2012 Patients First Objectives After attending this presentation, participants will be able to: Understand the common congenital and acquired
Pelvic Pain in the Pediatric Patient Susan D. John, M.D. RSNA 2012 Patients First Objectives After attending this presentation, participants will be able to: Understand the common congenital and acquired
Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy?
 January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
January 2013 Adult Intussusception: A Complication of Metastatic Melanoma or Primary Malignancy? Johanna Sheu, Harvard Medical School Year III 1 Agenda Menu of tests Definition/anatomy/classification Pediatrics
Washington State Hospital Association Safe Table Webcast 100K Children Campaign Safe Imaging September 15, 2014
 Washington State Hospital Association Safe Table Webcast 100K Children Campaign Safe Imaging September 15, 2014 1 Presenters Becky DeMers, RN Director, Quality and Performance Improvement Washington State
Washington State Hospital Association Safe Table Webcast 100K Children Campaign Safe Imaging September 15, 2014 1 Presenters Becky DeMers, RN Director, Quality and Performance Improvement Washington State
Good morning! July 24, 2014
 Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
PEDIATRIC GI EMERGENCIES. AGE-RELATED DIAGNOSIS Early Infancy EXAMINATION TIPS PEDIATRIC ABDOMINAL PAIN. How Common Is It?
 PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
Pitfalls in the CT diagnosis of appendicitis
 The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
Bowel Obstructions in Older Children
 Residents Section Pattern of the Month Hryhorczuk et al. owel Obstructions in Older Children Residents Section Pattern of the Month Residents inradiology nastasia Hryhorczuk 1 Edward Y. Lee 1,2 Ronald
Residents Section Pattern of the Month Hryhorczuk et al. owel Obstructions in Older Children Residents Section Pattern of the Month Residents inradiology nastasia Hryhorczuk 1 Edward Y. Lee 1,2 Ronald
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Pediatric Bowel Obstruction
 Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
Pediatric Bowel Obstruction Matt Zerden, Harvard Medical School III Patient 1 16 year old presents with severe, episodic abdominal pain, nausea and vomiting. Questionable abdominal mass in RLQ Previous
FHS Appendicitis US Protocol
 FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
The Gastrointestinal Tract
 CHAPTER 10 The Gastrointestinal Tract INTRODUCTION Although sonography may not always be the modality of choice for the detection of all gastrointestinal abnormalities, it does provide a noninvasive, nonionizing
CHAPTER 10 The Gastrointestinal Tract INTRODUCTION Although sonography may not always be the modality of choice for the detection of all gastrointestinal abnormalities, it does provide a noninvasive, nonionizing
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. Mnari, M. Zguidi, A. Zrig, M. Maatouk, B. Hmida, R. Salem,
Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015
![Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015](/thumbs/85/92263701.jpg "Flouroscopy CT. Principal Modality (2): Case Report # [] Date accepted: 14 May 2015") Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Radiological Category: Emergency Principal Modality (1): Principal Modality (2): Flouroscopy CT Case Report # [] Submitted by: Haider Virani, M.D. Faculty reviewer: Naga Chinapuvvula, MD Date accepted:
Neonatal intestinal obstruction: how to make etiological diagnosis?
 Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Neonatal intestinal obstruction: how to make etiological diagnosis? Poster No.: C-1414 Congress: ECR 2013 Type: Educational Exhibit Authors: W. MNARI, M. Zguidi, A. Zrig, M. MAATOUK, B. Hmida, R. Salem,
Radiology of GI system diseases
 GI Cycle - Lecture 12 436 Teams Radiology of GI system diseases Objectives 1. 2. 3. To know common GIT Pathologies presentation. To understand step wise approach in requesting GIT Radiology Investigations.
GI Cycle - Lecture 12 436 Teams Radiology of GI system diseases Objectives 1. 2. 3. To know common GIT Pathologies presentation. To understand step wise approach in requesting GIT Radiology Investigations.
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
US in non-traumatic acute abdomen. Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university
 US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
SIMPLE GUIDE FOR SONOLOGICAL EVALUATION OF APPENDICITIS
 SIMPLE GUIDE FOR SONOLOGICAL EVALUATION OF APPENDICITIS A Case Study by Dr. Avni K P Skandhan, India (Consultant Radio Diagnosis, Malabar Institute of Medical Science, Malappuram, Kerala) Email: avniskandhan@gmail.com
SIMPLE GUIDE FOR SONOLOGICAL EVALUATION OF APPENDICITIS A Case Study by Dr. Avni K P Skandhan, India (Consultant Radio Diagnosis, Malabar Institute of Medical Science, Malappuram, Kerala) Email: avniskandhan@gmail.com
Topics for discussion. Pediatric General Surgery. Physiology. Surgical Newborns. Neonatal Intestinal Obstruction
 Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Paediatric surgical emergencies. Mani Thyagarajan BWCH
 Paediatric surgical emergencies Mani Thyagarajan BWCH General points Always discuss Call consultant for help ASAP CT scan is a bad modality in paediatrics Ultrasound? Intussusception? Renal colic? UTI
Paediatric surgical emergencies Mani Thyagarajan BWCH General points Always discuss Call consultant for help ASAP CT scan is a bad modality in paediatrics Ultrasound? Intussusception? Renal colic? UTI
MRI pediatric appendicitis
 Disclosures MRI pediatric appendicitis Brooke Lampl Cleveland Clinic Imaging Institute Section of Pediatric Radiology I have nothing to disclose. Objectives Discuss imaging choices in the evaluation of
Disclosures MRI pediatric appendicitis Brooke Lampl Cleveland Clinic Imaging Institute Section of Pediatric Radiology I have nothing to disclose. Objectives Discuss imaging choices in the evaluation of
APPENDICITIS AND ITS APPEARANCES ON CT
 APPENDICITIS AND ITS APPEARANCES ON CT APPENDICITIS Results from acute inflammation of the appendix. Most common abdominal surgical emergencies. Diagnosis usually clinical based on physical exam and lab
APPENDICITIS AND ITS APPEARANCES ON CT APPENDICITIS Results from acute inflammation of the appendix. Most common abdominal surgical emergencies. Diagnosis usually clinical based on physical exam and lab
Case Whirlpool sign in midgut volvulus
 Case 11454 Whirlpool sign in midgut volvulus Emad El-din Althamer 1, Shagufta Jabeen 2, Nada Al-Assaf 1, Akram Jawad 1, Muhammad Hassan 1, Muhammad Fatani 1, Rumayan Al-Rumyan 1, A Aziz Mosabihi 1, Ahmeduddin
Case 11454 Whirlpool sign in midgut volvulus Emad El-din Althamer 1, Shagufta Jabeen 2, Nada Al-Assaf 1, Akram Jawad 1, Muhammad Hassan 1, Muhammad Fatani 1, Rumayan Al-Rumyan 1, A Aziz Mosabihi 1, Ahmeduddin
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Children's (Pediatric) Ultrasound - Abdomen
 Ultrasound - Abdomen") Scan for mobile link. Children's (Pediatric) Ultrasound - Abdomen Children s (pediatric) ultrasound imaging of the abdomen is a safe, noninvasive test that uses sound waves to produce a clear picture of
Scan for mobile link. Children's (Pediatric) Ultrasound - Abdomen Children s (pediatric) ultrasound imaging of the abdomen is a safe, noninvasive test that uses sound waves to produce a clear picture of
3/30/18. Common Radiology Studies in Pediatric Surgery. Disclosure Information. Objectives
 Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure
Common Radiology Studies in Pediatric Surgery A Scenario Based Approach to Interpretation for the Pediatric Nurse and Provider presented by Elizabeth A. Paton, DNP, RN-BC, PNP-A, PPCNP-BC, CPEN, FAEN Disclosure
Role of radiology and imaging in the daignosis of acute abdominal conditions
 Role of radiology and imaging in the daignosis of acute abdominal conditions Miah MAY Introduction In our day to day practice we have to face many of the acute abdominal conditions. As we know acute abdomen
Role of radiology and imaging in the daignosis of acute abdominal conditions Miah MAY Introduction In our day to day practice we have to face many of the acute abdominal conditions. As we know acute abdomen
Evaluation of the of the sensitivity, accuracy and positive predictive value of ultrasonography in the diagnosis of Appendicitis.
 West African Journal of Ultrasound Vol 17 Number 2 (2016) Evaluation of the of the sensitivity, accuracy and positive predictive value of ultrasonography in the diagnosis of Appendicitis. 1 2 3 Oguntola
West African Journal of Ultrasound Vol 17 Number 2 (2016) Evaluation of the of the sensitivity, accuracy and positive predictive value of ultrasonography in the diagnosis of Appendicitis. 1 2 3 Oguntola
X-ray Corner. Imaging of the Small Bowel. Pantongrag-Brown L. Case 1. A 63-year-old man presented with abdominal pain, nausea and vomiting.
 THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
THAI J 42 Imaging of the Small Bowel GASTROENTEROL 2015 X-ray Corner Imaging of the Small Bowel Pantongrag-Brown L Small bowel is the longest tubular organ in the body, about 18-22 feet. It is anchored
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 09/17/2011 Radiology Quiz of the Week # 38 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
What is Your Diagnosis?
 What is Your Diagnosis? Izabela Ragan, Class of 2014 Signalment Species: Canine Breed: English Bulldog Sex: Male castrated Date of birth: 04/14/11 Presenting Complaint Dog was presented for vomiting and
What is Your Diagnosis? Izabela Ragan, Class of 2014 Signalment Species: Canine Breed: English Bulldog Sex: Male castrated Date of birth: 04/14/11 Presenting Complaint Dog was presented for vomiting and
Emergent Pediatric US: What Every Radiologist Should Know 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. PEDIATRIC IMAGING
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. PEDIATRIC IMAGING
Gastrointestinal Tract Imaging. Objectives. Reference. VMB 960 April 6, Stomach Small Intestine Colon. Radiography & Ultrasound
 Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Gastrointestinal Tract Imaging VMB 960 April 6, 2009 Stomach Small Intestine Colon Objectives Radiography & Ultrasound Contrast Examination of the Small Intestine Reference Chapters 45 47 Pages 750 805
Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies. Author(s): Joseph House (University of Michigan), MD 2012
: Joseph House (University of Michigan), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Increased echogenicity of renal cortex: a transient feature in acutely ill children.
 4 Increased echogenicity of renal cortex: a transient feature in acutely ill children. Fraukje Wiersma Boudewijn R. Toorenvliet Madelon Ruige Herma C. Holscher Published (AJR American Journal of Roentgenology
4 Increased echogenicity of renal cortex: a transient feature in acutely ill children. Fraukje Wiersma Boudewijn R. Toorenvliet Madelon Ruige Herma C. Holscher Published (AJR American Journal of Roentgenology
Appendicitis: When Simple Becomes not so Simple
 Wright State University CORE Scholar Department of Surgery Faculty Publications Surgery 1-26-2010 Appendicitis: When Simple Becomes not so Simple Elizabeth H. Ey Wright State University, elizabeth.ey@wright.edu
Wright State University CORE Scholar Department of Surgery Faculty Publications Surgery 1-26-2010 Appendicitis: When Simple Becomes not so Simple Elizabeth H. Ey Wright State University, elizabeth.ey@wright.edu
US examination of the appendix in children with suspected appendicitis: The additional value of secondary signs.
 3 US examination of the appendix in children with suspected appendicitis: The additional value of secondary signs. Fraukje Wiersma Boudewijn R. Toorenvliet Johan L. Bloem Jan Hein Allema Herma C. Holscher
3 US examination of the appendix in children with suspected appendicitis: The additional value of secondary signs. Fraukje Wiersma Boudewijn R. Toorenvliet Johan L. Bloem Jan Hein Allema Herma C. Holscher
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability
 Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Ventriculoperitoneal Shunt with Communicating Peritoneal & Subcutaneous Pseudocysts Formation
 International Journal of Health Sciences, Qassim University, Vol. 8, No. 1 (January-March 2014) Case Report Ventriculoperitoneal Shunt with Communicating Peritoneal & Subcutaneous Pseudocysts Formation
International Journal of Health Sciences, Qassim University, Vol. 8, No. 1 (January-March 2014) Case Report Ventriculoperitoneal Shunt with Communicating Peritoneal & Subcutaneous Pseudocysts Formation
Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help. Print this Page Add to my Bookmarks Page 3 of 10
 Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Intestinal Malrotation
 Intestinal Malrotation Poster No.: C-1368 Congress: ECR 2015 Type: Educational Exhibit Authors: K. Carpentier, B. De Foer, F. Deckers, P. Leyman, M. 1 1 1 2 1 1 1 2 Pouillon, P. M. Parizel ; Wilrijk/BE,
Intestinal Malrotation Poster No.: C-1368 Congress: ECR 2015 Type: Educational Exhibit Authors: K. Carpentier, B. De Foer, F. Deckers, P. Leyman, M. 1 1 1 2 1 1 1 2 Pouillon, P. M. Parizel ; Wilrijk/BE,
Critically Ill Children in Pediatric Surgery. No disclosures to report.
 Critically Ill Children in Pediatric Surgery Hillary J. Collyer RN, MSN, CPNP, CCRN Pediatric Surgery Nurse Practitioner Hasbro Children s Hospital Disclosure Information Speaker: Hillary Collyer No disclosures
Critically Ill Children in Pediatric Surgery Hillary J. Collyer RN, MSN, CPNP, CCRN Pediatric Surgery Nurse Practitioner Hasbro Children s Hospital Disclosure Information Speaker: Hillary Collyer No disclosures
US diagnosis of acute appendicitis
 US diagnosis of acute appendicitis Poster No.: C-1496 Congress: ECR 2010 Type: Scientific Exhibit Topic: GI Tract Authors: A. Gligorievski; Skopje/MK Keywords: Ultrasound, Acute appendicitis, Diagnosis
US diagnosis of acute appendicitis Poster No.: C-1496 Congress: ECR 2010 Type: Scientific Exhibit Topic: GI Tract Authors: A. Gligorievski; Skopje/MK Keywords: Ultrasound, Acute appendicitis, Diagnosis
MRI of Acute Abdominal Pain in Pregnancy
 MRI of Acute Abdominal Pain in Pregnancy Ivan Pedrosa, M.D. Chief of MRI Jack Reynolds MD Chair in Radiology Associate Professor of Radiology UT Southwestern Medical Center Advanced Imag ing Research Center
MRI of Acute Abdominal Pain in Pregnancy Ivan Pedrosa, M.D. Chief of MRI Jack Reynolds MD Chair in Radiology Associate Professor of Radiology UT Southwestern Medical Center Advanced Imag ing Research Center
I. Intussusception in Children: Diagnostic Imaging and Treatment
 1 I. Intussusception in Children: Diagnostic Imaging and Treatment II. Author Kimberly E. Applegate, MD, MS Indiana University Department of Radiology Riley Hospital for Children 702 Barnhill Rd., Rm 1053b
1 I. Intussusception in Children: Diagnostic Imaging and Treatment II. Author Kimberly E. Applegate, MD, MS Indiana University Department of Radiology Riley Hospital for Children 702 Barnhill Rd., Rm 1053b
Common Pediatric Surgical Emergencies
 Common Pediatric Surgical Emergencies John Doski, Tate Nice San Antonio Pediatric Surgery Associates Division of Pediatric Surgery Departments of Surgery and Pediatrics Disclosure John Doski, MD has no
Common Pediatric Surgical Emergencies John Doski, Tate Nice San Antonio Pediatric Surgery Associates Division of Pediatric Surgery Departments of Surgery and Pediatrics Disclosure John Doski, MD has no
Pictorial review of bowel ultrasound: Common and unsuspected pathologies
 Pictorial review of bowel ultrasound: Common and unsuspected pathologies Poster No.: C-1668 Congress: ECR 2013 Type: Educational Exhibit Authors: A. Law, A. Ali, G. Hutchison; Bolton/UK Keywords: Ultrasound-Colour
Pictorial review of bowel ultrasound: Common and unsuspected pathologies Poster No.: C-1668 Congress: ECR 2013 Type: Educational Exhibit Authors: A. Law, A. Ali, G. Hutchison; Bolton/UK Keywords: Ultrasound-Colour
IV and Oral contrast vs. IV contrast alone computed tomography for the visualization of appendix and diagnosis of appendicitis in adult ED patients
 IV and Oral contrast vs. IV contrast alone computed tomography for the visualization of appendix and diagnosis of appendicitis in adult ED patients Aman Wadhwani, MD/MSc-Candidate Lancia Guo, MD Erik Saude,
IV and Oral contrast vs. IV contrast alone computed tomography for the visualization of appendix and diagnosis of appendicitis in adult ED patients Aman Wadhwani, MD/MSc-Candidate Lancia Guo, MD Erik Saude,
Diagnostic Imaging of Pediatric Gastrointestinal Abnormalities. Learning Objectives
 Diagnostic Imaging of Pediatric Gastrointestinal Abnormalities Tess Chapman, MD Associate Professor of Radiology, University of Washington School of Medicine Staff Radiologist, Seattle Children s Hospital
Diagnostic Imaging of Pediatric Gastrointestinal Abnormalities Tess Chapman, MD Associate Professor of Radiology, University of Washington School of Medicine Staff Radiologist, Seattle Children s Hospital
General Data. 王 X 村 78 y/o 男性
 General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
General Data 王 X 村 78 y/o 男性 Chief Complaint Vomiting twice this early morning Fever up to 38.9ºC was noted Present Illness (1) Old CVA with left side weakness for more than 10 years and with bed ridden
Therapeutic Enema for Intussusception
 Scan for mobile link. Therapeutic Enema for Intussusception Therapeutic enema is used to help identify and diagnose intussusception, a serious disorder in which one part of the intestine slides into another
Scan for mobile link. Therapeutic Enema for Intussusception Therapeutic enema is used to help identify and diagnose intussusception, a serious disorder in which one part of the intestine slides into another
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients).
.") Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Plain abdomen The standard films are supine & erect AP views (alternative to erect, lateral decubitus film is used in ill patients). The stomach can be readily identified by its location, gastric rugae
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging
 Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix.
 The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
Sonographycally guided hydrostatic reduction of childhood intussusception
 Sonographycally guided hydrostatic reduction of childhood intussusception Dubravka Vidmar, Alenka Višnar Perovič Clinical Radiology Institute, University Clinical Centre Ljubljana, Slovenia Background.
Sonographycally guided hydrostatic reduction of childhood intussusception Dubravka Vidmar, Alenka Višnar Perovič Clinical Radiology Institute, University Clinical Centre Ljubljana, Slovenia Background.
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
US examination of the appendix in children with suspected appendicitis: the additional value of secondary signs
 Eur Radiol (2009) 19: 455 461 DOI 10.1007/s00330-008-1176-6 PE DIATRI C Fraukje Wiersma Boudewijn R. Toorenvliet Johan L. Bloem Jan Hein Allema Herma C. Holscher US examination of the appendix in children
Eur Radiol (2009) 19: 455 461 DOI 10.1007/s00330-008-1176-6 PE DIATRI C Fraukje Wiersma Boudewijn R. Toorenvliet Johan L. Bloem Jan Hein Allema Herma C. Holscher US examination of the appendix in children
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
PAEDIATRIC GASTROINTESTINAL RADIOLOGY
 Objective Guide to Radiology of the Paediatric Intestinal Tract Responsibility / Registrar Frequency As required Associated Documents : RADFLPAEPR003 Contrast mixes RADFLPAEPR001 Paediatric Barium swallow
Objective Guide to Radiology of the Paediatric Intestinal Tract Responsibility / Registrar Frequency As required Associated Documents : RADFLPAEPR003 Contrast mixes RADFLPAEPR001 Paediatric Barium swallow
CLINICAL VIGNETTE 2016; 2:1
 CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Sick or not sick? Objectives. Bilious vomiting. Deadly Misdiagnoses: Kids with GI Complaints. Ronald Dieckmann, MD. Problems in assessment
 Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease
 The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Role of Ultrasound in the Assessment of Inflammatory Bowel Disease Dr. Richard A. Beable Consultant Gastrointestinal Radiologist Queen Alexandra Hospital Portsmouth Hospitals NHS Trust Topics for Discussion
The Use of Ultrasound in the Diagnosis of Crohn's Disease
 American Academy of Pediatrics CA2 Ashley Wachsman, MD Namita Singh, MD Newsletter June 2016 Cindy E. Kallman, MD The Use of Ultrasound in the Diagnosis of Crohn's Disease A few years ago, a prominent
American Academy of Pediatrics CA2 Ashley Wachsman, MD Namita Singh, MD Newsletter June 2016 Cindy E. Kallman, MD The Use of Ultrasound in the Diagnosis of Crohn's Disease A few years ago, a prominent
Congenital anomalies of the gastrointestinal tract: A radiological review
 Congenital anomalies of the gastrointestinal tract: A radiological review Poster No.: C-1669 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract Authors: S. P. Ramachandra, M. Bydder, N. Gurjar,
Congenital anomalies of the gastrointestinal tract: A radiological review Poster No.: C-1669 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract Authors: S. P. Ramachandra, M. Bydder, N. Gurjar,
The nontraumatic acute abdomen
 CT features of acute appendicitis: pictorial review Marco ntonio Cura, MD The nontraumatic acute abdomen is one of the most common presentations to the emergency room, with appendicitis being one of the
CT features of acute appendicitis: pictorial review Marco ntonio Cura, MD The nontraumatic acute abdomen is one of the most common presentations to the emergency room, with appendicitis being one of the
Adult bowel obstruction with acute abdomen: spectrum of CT findings
 Adult bowel obstruction with acute abdomen: spectrum of CT findings Poster No.: C-1571 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Turturici, G. Gherarducci, F. Bianchi, R. Pascale, M. Tonerini,
Adult bowel obstruction with acute abdomen: spectrum of CT findings Poster No.: C-1571 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Turturici, G. Gherarducci, F. Bianchi, R. Pascale, M. Tonerini,
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST
 CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
CASE CONFERENCE GASTRIC VOLVULUS PIKOM, MD NONGLUK, MD; RADIOLOGIST IDENTIFICATION DATA ผ ป วยเด กชายไทย อาย 13 ว น เช อชาต ไทย ส ญชาต ไทย ภ ม ล าเนา จ งหว ด อ ท ยธาน เข าร บการร กษาท รพ.มหาว ทยาล ยนเรศวรว
Gastrointestinal Obstruction
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Gastrointestinal Obstruction (Blockage of the Gastrointestinal Tract) Basics OVERVIEW
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Gastrointestinal Obstruction (Blockage of the Gastrointestinal Tract) Basics OVERVIEW
A Comparative Ultrasound and Plain Abdominal X-Ray: Evaluation of Non-Classical Clinical Cases of Appendicitis
 A Comparative Ultrasound and Plain Abdominal X-Ray: Evaluation of Non-Classical Clinical Cases of Appendicitis Dorothy Makanjuola, FRCR; Qasim Al-Qasabi, FRCS; Tajuddin Malabarey, FRCR From the Departments
A Comparative Ultrasound and Plain Abdominal X-Ray: Evaluation of Non-Classical Clinical Cases of Appendicitis Dorothy Makanjuola, FRCR; Qasim Al-Qasabi, FRCS; Tajuddin Malabarey, FRCR From the Departments
elical CT plays an important role
 bdominal Imaging Yu et al. Helical CT of cute RLQ Pain Pictorial Essay Jinxing Yu 1 nn S. Fulcher Mary nn Turner Robert. Halvorsen Yu J, Fulcher S, Turner M, Halvorsen R Helical CT Evaluation of cute Right
bdominal Imaging Yu et al. Helical CT of cute RLQ Pain Pictorial Essay Jinxing Yu 1 nn S. Fulcher Mary nn Turner Robert. Halvorsen Yu J, Fulcher S, Turner M, Halvorsen R Helical CT Evaluation of cute Right
Overview. Imaging Indications. Paediatric Radiation Safety 2015/03/12. Paediatric radiation safety General guidelines Protocols
 Overview Paediatric radiation safety General guidelines Protocols Paediatric Radiation Safety Paediatric patients are unique Children are more susceptible to radiation induced cancer than adults Younger
Overview Paediatric radiation safety General guidelines Protocols Paediatric Radiation Safety Paediatric patients are unique Children are more susceptible to radiation induced cancer than adults Younger
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Chapter 48 Anomalies of Intestinal Rotation
 Chapter 48 Anomalies of Intestinal Rotation François I. Luks Rotational anomalies of the intestinal tract refer to the failure of the primitive midgut to establish its normal anatomical relationships and
Chapter 48 Anomalies of Intestinal Rotation François I. Luks Rotational anomalies of the intestinal tract refer to the failure of the primitive midgut to establish its normal anatomical relationships and
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions