Appendicitis: When Simple Becomes not so Simple
|
|
|
- Kristian Jackson
- 6 years ago
- Views:
Transcription

1 Wright State University CORE Scholar Department of Surgery Faculty Publications Surgery Appendicitis: When Simple Becomes not so Simple Elizabeth H. Ey Wright State University, Jeffrey C. Pence Wright State University, Follow this and additional works at: Part of the Surgery Commons Repository Citation Ey, E. H., & Pence, J. C. (2010). Appendicitis: When Simple Becomes not so Simple.. This Presentation is brought to you for free and open access by the Surgery at CORE Scholar. It has been accepted for inclusion in Department of Surgery Faculty Publications by an authorized administrator of CORE Scholar. For more information, please contact


2 Appendicitis: When simple becomes not so simple Appendicitis: When simple becomes not so simple Elizabeth H. Ey, MD Associate Clinical Professor of Pediatrics Department of Medical Imaging Dayton Children s Medical Center Jeffrey C. Pence, MD, FACS, FAAP Associate Professor of Surgery Department of Surgery Dayton Children s Medical Center Learning Objectives To further understand a contemporary approach in the management of acute appendicitis To acknowledge that appendicitis represents a continuum of disease To define simple simple versus complicated complicated appendicitis To understand the importance of diagnostic and therapeutic imaging in appendicitis To explore alternative therapeutic strategies in complicated appendicitis based upon outcomes analyses Historical Perspectives Reginald Fitz (Harvard, 1886) Presented Perforative Inflammation of the Vermiform Appendix with Special Reference to Its Early Diagnosis and Treatment to the Association of American Physicians Conclusively demonstrated that perityphlitis perityphlitis began with inflammation of fth the appendix Suggested immediate surgical intervention (3 days or less) for, or to prevent, spreading peritonitis Fitz RH: Perforating inflammation of the vermiform appendix: With special reference to its early diagnosis and treatment. Trans Assoc Am Physicians 1:107, 1886 Historical Perspectives Charles McBurney (1889) Greatest contributor to the treatment of appendicitis Published the landmark treatise on the surgical treatment of appendicitis before rupture Subsequently published (1894) the exposure of the appendix through an incision which now bears his name McBurney C: Experience with early operative interference in cases of disease of the vermiform appendix. N Y State Med J 50:676, 1889 McBurney C: The incision made in the abdominal wall in cases of appendicitis. Ann Surg 20:38, Historical Perspectives The seat of greatest pain has been very exactly between an inch and a half and two inches from the anterior spinous process of the ilium on a straight line drawn from the process to the umbilicus 1




3 Introduction Introduction Most commonly diagnosed surgical condition of the abdomen Approximately 7% of individuals will develop acute appendicitis in their lifetime 250,000 cases diagnosed annually in United States Accounts for >1 million inpatient hospital days annually Cost of >3 billion US dollars per annum Most commonly misdiagnosed surgical condition of the abdomen Incidence of perforated appendicitis ranges generally from percent in pediatric and elderly populations Continues to cause significant morbidity and rare mortality What s constant Three taeniae coli converge at the junction of the cecum with the appendix Relationship of the appendiceal base to the cecum remains constant Anatomical Considerations LUMINAL OBSTRUCTION Appendicolith (40%) Lymphoid hypertrophy Parasites Foreign bodies Tumors Pathophysiology What s not constant Length of the appendix may vary from <1 cm to >30 cm (typically 6-9 cm) Position of the appendiceal tip is markedly variable INTRALUMINAL HYPERTENSION Ongoing secretion Bacterial proliferation Appendiceal dilation Sympathetic nervous system Vague abdominal pain Pathophysiology A Dichotomous Disease TRANSMURAL INLAMMATION Somatic nervous system Localized abdominal pain Periappendiceal inflammation Simple appendicitis: Early in time course Mild periappendiceal inflammation Nonperforated GANGRENE/MICROPERFORATION GROSS PERFORATION PHLEGMON/ABSCESS Generalized peritonitis Complicated appendicitis: Late in time course Significant periappendiceal inflammation Phlegmon Mass Abscess 2


4 The Surgeon s Dilemma The Surgeon s Dilemma Simple appendicitis Simple Simple appendicitis Operate The Surgeon s Dilemma Complicated appendicitis Not so simple USA Today January 19, 2010 The Surgeon s Dilemma The Surgeon s Dilemma Complicated appendicitis Not so simple Complicated appendicitis Not so simple How do I distinguish complicated appendicitis? Do I operate immediately in complicated appendicitis? If so, what technique? If I don t operate, what should my expectations be? If conservative management is successful, is interval appendectomy necessary? 3
 I")
5 Contemporary The Surgeon s Premise Contemporary The Surgeon s Premise I want to distinguish simple from complicated appendicitis I believe that complicated appendicitis may harbor increased risks with acute appendectomy Higher risk of intraoperative complications Higher risk of open conversion Prolonged operative time Higher risk of postoperative complications (abscess formation) I acknowledge that the total length of hospitalization, antibiotic administration, and cost of treatment will be unchanged if I employ initial nonoperative management Horwitz, JR, et al. Should Laparoscopic Appendectomy Be Avoided for Complicated Appendicitis in Children? J Pediatr Surg 32: , 1997 Retrospective review 2 year period ( ) 1996) 56 children with complicated appendicitis 34 children underwent initial laparoscopic appendectomy 22 children underwent open appendectomy Results No intraoperative complications 7/34 (20%) required laparoscopic to open conversion 15/27 (56%) total complications in laparoscopic group 11/27 (41%) formed postoperative intraabdominal abscess in laparoscopic group 2/11 required laparotomy for drainage Conclusions Laparoscopic appendectomy for complicated appendicitis in children is associated with a notable increase in the incidence of postoperative intraabdominal abscess formation Early open conversion for complicated appendicitis if identified incidentally (intraoperatively) Roach JP, et al. Complicated appendicitis in children: a clear role for drainage and delayed appendectomy. Am J Surg 194: , 773, 2007 Retrospective review 1106 children undergoing either open or laparoscopic appendectomy 5 year study period ( ) 2006) 4
6 Roach JF, et al. Results 360 (32%) radiographic, operative, or pathologic evidence of perforation (complicated appendicitis) 92/360 (26%) abscess or phlegmon on preoperative imaging i 60/92 (65%) immediate appendectomy 32/92 (35%) conservative treatment with delayed (interval) appendectomy Conclusions Optimal treatment of children who present with greater than 5 days of symptoms and preoperative imaging suggestive of complicated appendicitis is delayed appendectomy Initial nonoperative management is safe and effective with no children failing delayed appendectomy and no complications requiring repeat admission Simillis C, et al. A meta-analysis analysis comparing conservative treatment versus acute appendectomy for complicated appendicitis (abscess or phlegmon). Surgery 147:818-29, 2010 Database search using Medline, EMBASE, Ovid, and Cochrane through June 2, total reports identified 17 reports evaluated in final meta-analysis analysis 1/1717 reports was a non-randomized prospective study 7/17 reports were pediatric Outcomes for analysis Duration of hospital stay Mean duration of hospital stay during first hospitalization Overall duration of hospital stay, including IA and complications Duration of antibiotic administration Excluded oral course completed subsequent to discharge Complications Overall Specific, including wound infection and abscess formation Reoperations Postoperative complications after IA or AA Outcome of interest Results Studies Patients OR* P-value Duration of IV antibiotics Duration of initial hospitalization Overall duration of hospital stay Overall complications i 16 1, < Wound infection 10 1, Abdominal/pelvic abscess Ileus/bowel obstruction Reoperation *OR <1.0 favored CT group 5
 CT group had significantly less abdominal/pelvic abscess formation (OR 0.11; P<0.")
7 Pediatric Subset Analysis (n=7) No differences in duration of first hospitalization CT group had fewer overall complications (OR 0.21; P<0.001) CT group had fewer wound infections (OR 0.11; P=0.007) CT group had significantly less abdominal/pelvic abscess formation (OR 0.11; P<0.001) Conclusions Conservative management of complicated appendicitis is associated with: no change in duration of hospital stay no change in duration of intravenous antibiotic administration decreased overall complication rate decreased rate of reoperation Radiology: The importance and impact of imaging Elizabeth H. Ey, M.D. Associate Clinical Professor of Pediatrics, WSUBSOM Department of Medical Imaging Dayton Children s Medical Center Appendicitis: Imaging Evaluation Conventional radiographs 2 views Ultrasound (US) Computerized Tomography (CT) Abdominal Pain Imaging Child presents with abdominal pain Initial evaluation History Physical exam Laboratory evaluations Imaging Conventional Radiographs Advantages Readily available Quick No patient preparation Little radiation (2 views 100 mrad) Low cost 6








8 Useful findings on conventional radiographs for abdominal pain Pneumonia Pneumoperitoneum Pneumonia Fecalith Small bowel obstruction Constipation (?) Pneumonia Pneumoperitoneum Small Bowel Obstruction Fecalith 7
 No intravenous contrast Utility lies in a subgroup of")



9 Fecalith Appendicitis: Imaging Evaluation Ultrasound Ultrasound Appendicitis Advantages No ionizing radiation (0 mrad) No intravenous contrast Utility lies in a subgroup of children Clinical findings are equivocal To establish diagnosis of appendicitis Aid in the diagnosis of other abdominal and pelvic conditions that may mimic appendicitis Ultrasound Appendicitis Disadvantages Examination limited by obesity Limited by bowel gas Operator dependent, site dependent Reported accuracy varies widely Ultrasound Appendicitis Ultrasound Appendicitis Sensitivity Reports range from 44%-94% Specificity Reports range from 47%-95% Sensitivity Reports range from 44%-94% Specificity Reports range from 47%-95% 8
10 Ultrasound Appendicitis Orr RK, Porter D, Hartman D. Ultrasonography to evaluate adults for appendicitis: Decision making based on meta-analysis analysis and probablistic reasoning. Acad Emerg Med 1995: 2: Mt Meta-analysisanalysis US based adult and pediatric studies published 1986 and 1994 Overall sensitivity of 85% Overall specificity of 92% Graded Compression Technique Puylaert JB: Acute appendicitis: US evaluation using graded Compression. Radiology 1986; 158: Using a high resolution, linear array transducer Gentle, gradual pressure applied to anterior abdominal wall to displace and compress normal bowel loops Creating a window to McBurney s point Graded Compression Technique Longitudinal and horizontal imaging is performed Ask the child to point to the site maximal tenderness for reference Localize the ascending colon, move inferiorly Localize normal compressible terminal ileum Cecal tip is 1-2 cm below terminal ileum Ultrasound for Appendicitis Criteria Tubular, blind ending structure Non compressible Diameter (outer wall to outer wall) > 6 mm May also see Fecalith shadowing structure in lumen Hyperemia of wall Enlarged mesenteric lymph nodes Periappendiceal fat inflammation Phlegmon or abscess Ultrasound for Appendicitis False negative diagnosis Failure to visualize the entire appendix Inability to adequately compress the RLQ Aberrant location of appendix retrocecal Appendiceal perforation Early inflammation at the distal tip Ultrasound for Appendicitis False positive diagnosis Identify a normal appendix as abnormal Should be 6 mm or less diameter, compressible, no adjacent inflammatory changes Other causes of RLQ inflammation Crohn disease Inflamed Meckel diverticulum Pelvic inflammatory disease 9





 Loculated, complex")
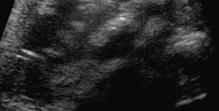
11 Normal Appendix Acute Appendicitis: Simple, non perforated 4 mm Compression Acute Appendicitis: Simple, non perforated Acute Appendicitis: Simple, non perforated Target Appearance: Fluid filled lumen Echogenic mucosa and submucosa Hypoechoic muscularis Echogenic, shadowing fecalith Wall hyperemia Inflamed periappendiceal fat Complicated Appendicitis Spectrum of gangrenous to perforated appendicitis Complicated Appendicitis Loss of echogenic submucosal layer Absent blood flow in thickened wall Lumen may no longer be distended with fluid Periappendiceal or pelvic fluid collection Simple fluid Echogenic, inflammatory mass (phlegmon) Loculated, complex fluid collection (abscess) +/- air bubbles or swirling complex fluid 10
 High anatomic detail More useful than US for complicated")

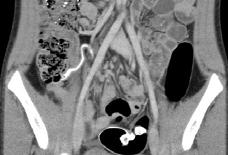
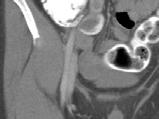
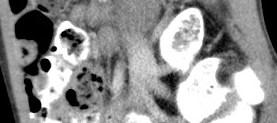
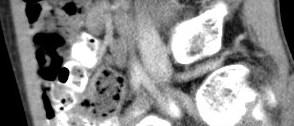
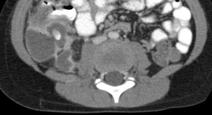
12 Complicated Appendicitis Appendicitis: Imaging Evaluation Computerized Tomography CT Appendicitis Advantages Highly sensitive and specific modality for diagnosis of acute appendicitis Reported sensitivity 87%-100% Reported specificity 89%-98% 98% Reduced operator dependence Superior contrast sensitivity (air, fat, fluid, bone) High anatomic detail More useful than US for complicated appendicitis CT Appendicitis Disadvantages Relatively high radiation dose (1000 mrad) Do it well the first time! Younger, thinner patients t have less intrabdominal i fat to separate the appendix from adjacent bowel Highest diagnostic efficacy found using rectal contrast and IV contrast Callahan MJ, Rodriquez DP, Taylor GA. CT of Appendicitis in Children; Radiology 2002: 224: CT Appendicitis Normal appendix on CT Can be identified in over 75% of children Usually less than 7 mm in diameter Lumen may contain contrast or air CT Appendicitis CT features of appendicitis Distended appendix >7 mm diameter* Appendiceal wall thickening and enhancement Fecalith Circumferential or focal cecal wall thickening* Pericecal fat stranding Adjacent bowel wall thickening Free peritoneal fluid Mesenteric lymphadenopathy Intraperitoneal phlegmon or abscess 11





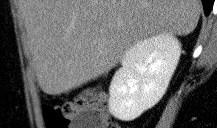


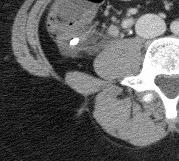
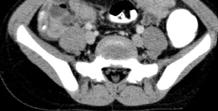

13 CT Normal Appendix CT Normal Appendix CT Normal Retrocecal Appendix CT Simple Appendicitis CT Simple Appendicitis Different patient CT Simple Appendicitis Same patient 12







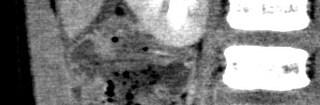
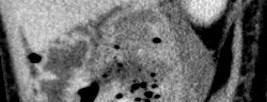


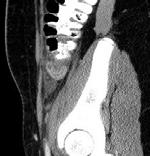
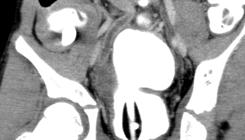
14 Outside CT No Contrast Simple or Complicated? RLQ Ultrasound Same Day CT Complicated Appendicitis After 5 days antibiotics CT Complicated Appendicitis Image Guided Pigtail Drain Placement CT Complicated Appendicitis Phlegmon 13












15 CT Complicated Appendicitis 6 days later Phlegmon now Abscesses CT Complicated Appendicitis Abscesses CT Complicated Appendicitis Percutaneous Abscess Drains Patient 1 Clinical Scenario Patient 2 2 day history of abdominal pain Reported fever Nausea and emesis with anorexia Temperature 38.7 C Right lower quadrant tenderness WBC 16,700 Segmented neutrophils 83% C-reactive protein day history of abdominal pain Reported fever Nausea and emesis with anorexia Temperature 39.0 C Suprapubic tenderness WBC 24,300 Segmented neutrophils 90% C-reactive protein 24.3 Patient 1 Patient 2 14
16 Patient 1 Conservative management PICC Dual antibiotic therapy Oral diet by HD 2 Afebrile by HD 3 WBC 7,500 Segmented neutrophils 60% C-reactive protein 8.2 Total LOS 5 days Interval appendectomy 6-8 weeks Clinical Scenario Patient 2 Operative management PICC Dual antibiotic therapy Oral diet by HD 4 Afebrile by HD 4 WBC 7,000 Segmented neutrophils 69% C-reactive protein 1.6 Total LOS 7 days Treatment Now I ve decided not to operate initially How successful is delayed appendectomy? Bufo AJ, et al. Interval Appendectomy for Perforated Appendicitis in Children. J Laparoendosc Adv Surg Tech A 8(4): ): , 1998 Parameter Results Immediate Appendectomy Interval Appendectomy Retrospective review 87 patients with perforated appendicitis patients underwent immediate appendectomy 41 patients placed on interval appendectomy pathway 34/41 successfully bridged to interval appendectomy Patients 46 34* Hospital days 6.2 +/ /-3.0 Hospital charges (USD) 11,044 +/- 11,321 6,435 +/- 4,447 Total charges (USD) 12,426 +/- 12,002 7,525 +/- 3,250 Percent complications 21 6 *Excludes failures of intent to treat (7 patients = 17%) Conclusions Antibiotic therapy, followed by interval appendectomy, decreases postoperative morbidity in the treatment approach to perforated appendicitis Cost savings are realized in the delayed operative management of perforated appendicitis in children 15
17 Treatment I can successfully perform an interval appendectomy consistently and safely But should I? Recurrent/Interval Appendicitis Hoffmann J, et al. (1984) 20% Eriksson S and Granstrom L (1995) 37% Friedell M and Perez-Izquierdo (2000) 8% Oliak D, et al. (2001) 8% Brown CV, et al. (2003) 6% Ein SH, et al. (2005) 43% + appendicolith 72% - appendicolith 26% Puapong D, et al. Routine interval appendectomy in children is not indicated. J Pediatr Surg 42: , 2007 Retrospective study 12 year period ( ) 2004) 6,439 children 72 (1.1%) initially treated nonoperatively 11/72 (15%) underwent interval appendectomy 61/72 (85%) underwent observation Results Mean observation period of 7.5 years (range 2 months to 12 years) 5/61 (8%) developed recurrent appendicitis All recurrences within 3 years 80% of recurrences within 6 months Cumulative mean LOS without IA 6.6 days Cumulative mean LOS for recurrent appendicitis 9.6 days Cumulative mean LOS for IA 8.5 days Conclusions Recurrent appendicitis is rare in pediatric patients following successful nonoperative management Low recurrence rate of 8%fil fails to justify routine interval appendectomy T R E A T M E N T A L G O R I T H M Simple Appendicitis Surgery Suspected Appendicitis Phlegmon IV Antibiotics Improved? Interval Appendectomy Complicated Appendicitis CT Imaging IV + Rectal Contrast Abscess IV Antibiotics Percutaneous/Transrectal Drainage Improved? Surgery 16
18 Appendicitis: When simple is not so simple Summation Appendicitis happens (relatively frequently) Beat the perforation When in doubt, seek help (adjunct imaging) Distinguish simple from complicated appendicitis Appendicitis: When simple is not so simple Summation Complicated appendicitis can (and probably should) be treated conservatively Interval (laparoscopic) appendectomy remains appropriate in the pediatric population (particularly in the presence of a retained appendicolith) Prospective randomized trial 17
Always keep it in the differential
 Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
Acute Appendicitis Lissa C. Sakata and Lindsey Perea 2 Always keep it in the differential Learning Objectives 1. The learner should be able to describe the etiology of acute appendicitis. 2. The learner
FHS Appendicitis US Protocol
 FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
FHS Appendicitis US Protocol Reviewed By: Shireen Khan, MD; Sarah Farley, MD; Anna Ellermeier, MD Last Reviewed: May 2018 Contact: (866) 761-4200 **NOTE for all examinations: 1. If documenting possible
Pitfalls in the CT diagnosis of appendicitis
 The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
The British Journal of Radiology, 77 (2004), 792 799 DOI: 10.1259/bjr/95663370 E 2004 The British Institute of Radiology Pictorial review Pitfalls in the CT diagnosis of appendicitis 1 C D LEVINE, 2 O
APPENDICITIS AND ITS APPEARANCES ON CT
 APPENDICITIS AND ITS APPEARANCES ON CT APPENDICITIS Results from acute inflammation of the appendix. Most common abdominal surgical emergencies. Diagnosis usually clinical based on physical exam and lab
APPENDICITIS AND ITS APPEARANCES ON CT APPENDICITIS Results from acute inflammation of the appendix. Most common abdominal surgical emergencies. Diagnosis usually clinical based on physical exam and lab
ACUTE ABDOMEN IN OLDER CHILDREN. Carlos J. Sivit M.D.
 ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
ACUTE ABDOMEN IN OLDER CHILDREN Carlos J. Sivit M.D. ACUTE ABDOMEN Clinical condition characterized by severe abdominal pain developing over several hours ACUTE ABDOMINAL PAIN Common childhood complaint
Evaluation of the of the sensitivity, accuracy and positive predictive value of ultrasonography in the diagnosis of Appendicitis.
 West African Journal of Ultrasound Vol 17 Number 2 (2016) Evaluation of the of the sensitivity, accuracy and positive predictive value of ultrasonography in the diagnosis of Appendicitis. 1 2 3 Oguntola
West African Journal of Ultrasound Vol 17 Number 2 (2016) Evaluation of the of the sensitivity, accuracy and positive predictive value of ultrasonography in the diagnosis of Appendicitis. 1 2 3 Oguntola
The nontraumatic acute abdomen
 CT features of acute appendicitis: pictorial review Marco ntonio Cura, MD The nontraumatic acute abdomen is one of the most common presentations to the emergency room, with appendicitis being one of the
CT features of acute appendicitis: pictorial review Marco ntonio Cura, MD The nontraumatic acute abdomen is one of the most common presentations to the emergency room, with appendicitis being one of the
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Summary and conclusions
 Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Summary and conclusions 7 Chapter 7 68 Summary and conclusions Chapter 1 provides a general introduction to this thesis focused on the use of ultrasound (US) in children with abdominal problems. The literature
Interesting Pediatric ultrasound cases. Presented by: Falguni Patel (RDMS, RVT)
") Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Interesting Pediatric ultrasound cases Presented by: Falguni Patel (RDMS, RVT) Role of ultrasound to rule out Appendicitis Overview: Ultrasound is relatively inexpensive, safe and quick solution to rule
Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP
 Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP Texas Children s Hospital Objectives Discuss the surgical and non-operative approaches to the treatment of appendicitis
Medical Management of Appendicitis: Are We There Yet? Monica E. Lopez, MD, FACS, FAAP Texas Children s Hospital Objectives Discuss the surgical and non-operative approaches to the treatment of appendicitis
CLINICAL VIGNETTE 2016; 2:1
 CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
CLINICAL VIGNETTE 2016; 2:1 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. MANAGEMENT OF APPENDICITIS Ibrahim NA, Njokanma
Washington State Hospital Association Safe Table Webcast 100K Children Campaign Safe Imaging September 15, 2014
 Washington State Hospital Association Safe Table Webcast 100K Children Campaign Safe Imaging September 15, 2014 1 Presenters Becky DeMers, RN Director, Quality and Performance Improvement Washington State
Washington State Hospital Association Safe Table Webcast 100K Children Campaign Safe Imaging September 15, 2014 1 Presenters Becky DeMers, RN Director, Quality and Performance Improvement Washington State
SIMPLE GUIDE FOR SONOLOGICAL EVALUATION OF APPENDICITIS
 SIMPLE GUIDE FOR SONOLOGICAL EVALUATION OF APPENDICITIS A Case Study by Dr. Avni K P Skandhan, India (Consultant Radio Diagnosis, Malabar Institute of Medical Science, Malappuram, Kerala) Email: avniskandhan@gmail.com
SIMPLE GUIDE FOR SONOLOGICAL EVALUATION OF APPENDICITIS A Case Study by Dr. Avni K P Skandhan, India (Consultant Radio Diagnosis, Malabar Institute of Medical Science, Malappuram, Kerala) Email: avniskandhan@gmail.com
Abdominal Pain in Pediatric Patients Image Gently
 Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
Abdominal Pain in Pediatric Patients Image Gently Susan D. John, M.D. Baptist Health Emergency Radiology 2017 Disclosure I have no financial relationships with a commercial entity producing healthcarerelated
LAPAROSCOPIC APPENDICECTOMY
 LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
LAPAROSCOPIC APPENDICECTOMY WHAT IS THE APPENDIX? The appendix is a small, fingerlike pouch of the intestinal tract located where the small and large join. It has no known use. It is postulated that the
Value of Contrast Enhanced MDCT in Distinguishing Complicated from Non-Complicated Acute Appendicitis
 Med. J. Cairo Univ., Vol. 84, No. 2, September: 91-98, 2016 www.medicaljournalofcairouniversity.net Value of Contrast Enhanced MDCT in Distinguishing Complicated from Non-Complicated Acute Appendicitis
Med. J. Cairo Univ., Vol. 84, No. 2, September: 91-98, 2016 www.medicaljournalofcairouniversity.net Value of Contrast Enhanced MDCT in Distinguishing Complicated from Non-Complicated Acute Appendicitis
Laparoscopic Appendectomy: Valuable. Joel Baumgartner UCHSC Surgery Grand Rounds Resident Debate November 20, 2006
 Valuable Joel Baumgartner UCHSC Surgery Grand Rounds Resident Debate November 20, 2006 History National Library of Medicine History First open appendectomy in 1889 McBurney C. NY Med J 1889;50:676-84.
Valuable Joel Baumgartner UCHSC Surgery Grand Rounds Resident Debate November 20, 2006 History National Library of Medicine History First open appendectomy in 1889 McBurney C. NY Med J 1889;50:676-84.
US diagnosis of acute appendicitis
 US diagnosis of acute appendicitis Poster No.: C-1496 Congress: ECR 2010 Type: Scientific Exhibit Topic: GI Tract Authors: A. Gligorievski; Skopje/MK Keywords: Ultrasound, Acute appendicitis, Diagnosis
US diagnosis of acute appendicitis Poster No.: C-1496 Congress: ECR 2010 Type: Scientific Exhibit Topic: GI Tract Authors: A. Gligorievski; Skopje/MK Keywords: Ultrasound, Acute appendicitis, Diagnosis
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Appendicitis USG vs CT
 Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
Appendicitis USG vs CT Dr Sateesh Kumar Kailasam MBBS Dip EM (RCGP, UK) MRCEM (UK) Group Head Maxcure Group of Hospitals National Treasurer Society for Emergency Medicine India (SEMI) My Talk includes
POSTER SESSION. Routine Interval Appendectomy Is Not Justified After Initial Nonoperative Treatment of Acute Appendicitis
 POSTER SESSION Routine Interval Appendectomy Is Not Justified After Initial Nonoperative Treatment of Acute Appendicitis Anna Kaminski, MD; In-Lu Amy Liu, MS; Harry Applebaum, MD; Steven L. Lee, MD; Philip
POSTER SESSION Routine Interval Appendectomy Is Not Justified After Initial Nonoperative Treatment of Acute Appendicitis Anna Kaminski, MD; In-Lu Amy Liu, MS; Harry Applebaum, MD; Steven L. Lee, MD; Philip
Appendicitis. Diagnosis and Surgery
 Appendicitis Diagnosis and Surgery What Is Appendicitis? Your side may hurt so much that you called your doctor. Or maybe you went straight to the hospital emergency room. If the symptoms came on quickly,
Appendicitis Diagnosis and Surgery What Is Appendicitis? Your side may hurt so much that you called your doctor. Or maybe you went straight to the hospital emergency room. If the symptoms came on quickly,
Appendiceal diverticular disease
 Formosan Journal of Surgery (2013) 46, 4e9 Available online at www.sciencedirect.com journal homepage: www.e-fjs.com ORIGINAL ARTICLE Appendiceal diverticular disease Yun-Wu Deng a, Hsiao-Bai Yang b,e,
Formosan Journal of Surgery (2013) 46, 4e9 Available online at www.sciencedirect.com journal homepage: www.e-fjs.com ORIGINAL ARTICLE Appendiceal diverticular disease Yun-Wu Deng a, Hsiao-Bai Yang b,e,
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Laparoscopic Appendectomy Overrated. University of Colorado Department of Surgery Grand Rounds November 20, 2006 Carlos Rueda M.D.
 Laparoscopic Appendectomy Overrated University of Colorado Department of Surgery Grand Rounds November 20, 2006 Carlos Rueda M.D. Appendicitis 6-8% of population over lifetime Surgical Treatment 250,000
Laparoscopic Appendectomy Overrated University of Colorado Department of Surgery Grand Rounds November 20, 2006 Carlos Rueda M.D. Appendicitis 6-8% of population over lifetime Surgical Treatment 250,000
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix.
 The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The appendix is located in the lower right portion of the abdomen. It has no known
Small Bowel and Colon Surgery
 Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
Small Bowel and Colon Surgery Why Do I Need a Small Bowel Resection? A variety of conditions can damage your small bowel. In severe cases, your doctor may recommend removing part of your small bowel. Conditions
IV and Oral contrast vs. IV contrast alone computed tomography for the visualization of appendix and diagnosis of appendicitis in adult ED patients
 IV and Oral contrast vs. IV contrast alone computed tomography for the visualization of appendix and diagnosis of appendicitis in adult ED patients Aman Wadhwani, MD/MSc-Candidate Lancia Guo, MD Erik Saude,
IV and Oral contrast vs. IV contrast alone computed tomography for the visualization of appendix and diagnosis of appendicitis in adult ED patients Aman Wadhwani, MD/MSc-Candidate Lancia Guo, MD Erik Saude,
Chapter 93 Appendicitis
 Chapter 93 Appendicitis Episode Overview: 1) List 8 ddx for appendicitis 2) List 5 causes of acute appendiceal obstruction and describe the pathophysiology of appendicitis including pain location 3) List
Chapter 93 Appendicitis Episode Overview: 1) List 8 ddx for appendicitis 2) List 5 causes of acute appendiceal obstruction and describe the pathophysiology of appendicitis including pain location 3) List
Acute appendicitis is the most common surgical emergency in
 FEATURE Is It Safe to Delay Appendectomy in Adults With Acute Appendicitis? Michael F. Ditillo, DO,* James D. Dziura, PhD, and Reuven Rabinovici, MD* Objective: To examine whether delayed surgical intervention
FEATURE Is It Safe to Delay Appendectomy in Adults With Acute Appendicitis? Michael F. Ditillo, DO,* James D. Dziura, PhD, and Reuven Rabinovici, MD* Objective: To examine whether delayed surgical intervention
elical CT plays an important role
 bdominal Imaging Yu et al. Helical CT of cute RLQ Pain Pictorial Essay Jinxing Yu 1 nn S. Fulcher Mary nn Turner Robert. Halvorsen Yu J, Fulcher S, Turner M, Halvorsen R Helical CT Evaluation of cute Right
bdominal Imaging Yu et al. Helical CT of cute RLQ Pain Pictorial Essay Jinxing Yu 1 nn S. Fulcher Mary nn Turner Robert. Halvorsen Yu J, Fulcher S, Turner M, Halvorsen R Helical CT Evaluation of cute Right
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
MRI pediatric appendicitis
 Disclosures MRI pediatric appendicitis Brooke Lampl Cleveland Clinic Imaging Institute Section of Pediatric Radiology I have nothing to disclose. Objectives Discuss imaging choices in the evaluation of
Disclosures MRI pediatric appendicitis Brooke Lampl Cleveland Clinic Imaging Institute Section of Pediatric Radiology I have nothing to disclose. Objectives Discuss imaging choices in the evaluation of
Multislice Computed Tomography Imaging with Clinical Outcome in Inflammatory Appendiceal Masses
 Original Article Multislice Computed Tomography Imaging with Clinical Outcome in Inflammatory Appendiceal Masses ID: IJARS/2016/18502:2116 Radiology Section Varsha Rangankar, Abhijit Pawar, Aditi Dongre,
Original Article Multislice Computed Tomography Imaging with Clinical Outcome in Inflammatory Appendiceal Masses ID: IJARS/2016/18502:2116 Radiology Section Varsha Rangankar, Abhijit Pawar, Aditi Dongre,
Role of Alvarado Score in Diagnosis and Management of Acute Appendicitis
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/510 Role of Alvarado Score in Diagnosis and Management of Acute Appendicitis Chhari Akash Singh 1, Ashish Pratap Singh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2016/510 Role of Alvarado Score in Diagnosis and Management of Acute Appendicitis Chhari Akash Singh 1, Ashish Pratap Singh
Caeco-colic Intussusception Simulating an Appendicular Mass
 Article ID: WMC003206 ISSN 2046-1690 Caeco-colic Intussusception Simulating an Appendicular Mass Corresponding Author: Dr. Matthew O Adelekan, Surgeon, North manchester General Hospital - United Kingdom
Article ID: WMC003206 ISSN 2046-1690 Caeco-colic Intussusception Simulating an Appendicular Mass Corresponding Author: Dr. Matthew O Adelekan, Surgeon, North manchester General Hospital - United Kingdom
Center for Prospective Clinical Trials, The Children's Mercy Hospital, Kansas City, MO
 Journal of Pediatric Surgery (2010) 45, 236 240 www.elsevier.com/locate/jpedsurg Initial laparoscopic appendectomy versus initial nonoperative management and interval appendectomy for perforated appendicitis
Journal of Pediatric Surgery (2010) 45, 236 240 www.elsevier.com/locate/jpedsurg Initial laparoscopic appendectomy versus initial nonoperative management and interval appendectomy for perforated appendicitis
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
12 Blueprints Q&A Step 2 Surgery
 12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
12 Blueprints Q&A Step 2 Surgery 34. A 40-year-old female has been referred to you for a recent ER and hospital admission, from which she was given a diagnosis of acute diverticulitis. Treatment at that
Role of modified Alvarado scoring system and USG abdomen in acute appendicitis: an overview
 International Surgery Journal http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20175404 Role of modified Alvarado scoring
International Surgery Journal http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20175404 Role of modified Alvarado scoring
Emergency MDCT in case of right lower quadrant pain
 Emergency MDCT in case of right lower quadrant pain Poster No.: C-0563 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Lisitskaya, V. Sinitsyn; Moscow/RU Keywords: Abdomen, Emergency, Gastrointestinal
Emergency MDCT in case of right lower quadrant pain Poster No.: C-0563 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Lisitskaya, V. Sinitsyn; Moscow/RU Keywords: Abdomen, Emergency, Gastrointestinal
The role of abdominal X-rays in the investigation of suspected acute appendicitis
 Journal of Medicine and Medical Sciences Vol. 2(11) pp. 1216-1220, November 2011 Available online@ http://www.interesjournals.org/jmms Copyright 2011 International Research Journals Full Length Research
Journal of Medicine and Medical Sciences Vol. 2(11) pp. 1216-1220, November 2011 Available online@ http://www.interesjournals.org/jmms Copyright 2011 International Research Journals Full Length Research
Study of laparoscopic appendectomy: advantages, disadvantages and reasons for conversion of laparoscopic to open appendectomy
 International Surgery Journal Agrawal SN et al. Int Surg J. 2017 Mar;4(3):993-997 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20170849
International Surgery Journal Agrawal SN et al. Int Surg J. 2017 Mar;4(3):993-997 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20170849
Nonoperative Treatment With Antibiotics Versus Surgery for Acute Nonperforated Appendicitis in Children. A Pilot Randomized Controlled Trial
 RANDOMIZED CONTROLLED TRIAL Nonoperative Treatment With Antibiotics Versus Surgery for Acute Nonperforated Appendicitis in Children A Pilot Randomized Controlled Trial Jan F. Svensson, MD, Barbora Patkova,
RANDOMIZED CONTROLLED TRIAL Nonoperative Treatment With Antibiotics Versus Surgery for Acute Nonperforated Appendicitis in Children A Pilot Randomized Controlled Trial Jan F. Svensson, MD, Barbora Patkova,
A Comparative Ultrasound and Plain Abdominal X-Ray: Evaluation of Non-Classical Clinical Cases of Appendicitis
 A Comparative Ultrasound and Plain Abdominal X-Ray: Evaluation of Non-Classical Clinical Cases of Appendicitis Dorothy Makanjuola, FRCR; Qasim Al-Qasabi, FRCS; Tajuddin Malabarey, FRCR From the Departments
A Comparative Ultrasound and Plain Abdominal X-Ray: Evaluation of Non-Classical Clinical Cases of Appendicitis Dorothy Makanjuola, FRCR; Qasim Al-Qasabi, FRCS; Tajuddin Malabarey, FRCR From the Departments
Gallstone ileus:diagnostic and therapeutic dilemma
 Saurabh et al. 1 CASE SERIES OPEN ACCESS Gallstone ileus:diagnostic and therapeutic dilemma Shireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky ABSTRACT Introduction: Gallstone ileus is a rare complication
Saurabh et al. 1 CASE SERIES OPEN ACCESS Gallstone ileus:diagnostic and therapeutic dilemma Shireesh Saurabh, Andrew Camerota, Jeffrey Zavotsky ABSTRACT Introduction: Gallstone ileus is a rare complication
Ultrasound features of secondary appendicitis in pediatric patients
 Ultrasound features of secondary appendicitis in pediatric patients Lyo Min Kwon 1, Kwanseop Lee 1, Soo Kee Min 2, Soo Min Ahn 3, Hong Il Ha 1, Min-Jeong Kim 1 Departments of 1 Radiology, 2 Pathology,
Ultrasound features of secondary appendicitis in pediatric patients Lyo Min Kwon 1, Kwanseop Lee 1, Soo Kee Min 2, Soo Min Ahn 3, Hong Il Ha 1, Min-Jeong Kim 1 Departments of 1 Radiology, 2 Pathology,
The Value of Ultrasound in Diagnosing Acute Appendicitis
 The Value of Ultrasound in Diagnosing Acute Appendicitis *Dr. Baha'a Mushref Abdulsalam Department of Surgery, College of Medicine, University of Anbar, Anbar, Iraq Received 14/2/2012 Accepted 23/5/2012
The Value of Ultrasound in Diagnosing Acute Appendicitis *Dr. Baha'a Mushref Abdulsalam Department of Surgery, College of Medicine, University of Anbar, Anbar, Iraq Received 14/2/2012 Accepted 23/5/2012
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Amyand's Hernia: A Case Report
 Haris N. Shekhani 1*, Saurabh Rohatgi 1, Tarek Hanna 1, Jamlik-Omari Johnson 1 1. Division of Emergency Radiology, Emory University, Atlanta, GA 30308, USA * Correspondence: Haris Naseem Shekhani, Emory
Haris N. Shekhani 1*, Saurabh Rohatgi 1, Tarek Hanna 1, Jamlik-Omari Johnson 1 1. Division of Emergency Radiology, Emory University, Atlanta, GA 30308, USA * Correspondence: Haris Naseem Shekhani, Emory
Surgical Education Series
 Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Surgical Education Series The Acute Abdomen Ahmad kachooei, MD MPH Assistant Professor Division of General Surgery Department of Surgery University of Qom Outline Definitions What causes an acute abdomen
Case Report Urachal Cyst Causing Small Bowel Obstruction in an Adult with a Virgin Abdomen
 Case Reports in Surgery Volume 2016, Article ID 3247087, 4 pages http://dx.doi.org/10.1155/2016/3247087 Case Report Urachal Cyst Causing Small Bowel Obstruction in an Adult with a Virgin Abdomen Michael
Case Reports in Surgery Volume 2016, Article ID 3247087, 4 pages http://dx.doi.org/10.1155/2016/3247087 Case Report Urachal Cyst Causing Small Bowel Obstruction in an Adult with a Virgin Abdomen Michael
Pitfalls in Paediatric Appendicitis: Highlighting Common Clinical Features of Missed Cases
 Original Article Pitfalls in Paediatric Appendicitis: Highlighting Common Clinical Features of Missed Cases Melanie D.W. Seah and Kee-Chong Ng, Department of Emergency Medicine, KK Women s and Children
Original Article Pitfalls in Paediatric Appendicitis: Highlighting Common Clinical Features of Missed Cases Melanie D.W. Seah and Kee-Chong Ng, Department of Emergency Medicine, KK Women s and Children
Ultrasound of: Appendicitis Intussusception Pyloric Stenosis
 Ultrasound of: Appendicitis Intussusception Pyloric Stenosis Andrew Phelps MD Assistant Professor Pediatric Radiology UCSF Benioff Children s Hospital No Disclosures Take Home Message Appendicitis occurs
Ultrasound of: Appendicitis Intussusception Pyloric Stenosis Andrew Phelps MD Assistant Professor Pediatric Radiology UCSF Benioff Children s Hospital No Disclosures Take Home Message Appendicitis occurs
US in non-traumatic acute abdomen. Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university
 US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
US in non-traumatic acute abdomen Lalita, M.D. Radiologist Department of radiology Faculty of Medicine ChiangMai university Sagittal Orientation Transverse (Axial) Orientation Coronal Orientation Intercostal
Evaluation of accuracy of four clinical scores and comparison with ultrasonography for diagnosis of acute appendicitis
 International Surgery Journal Subramaniyan P et al. Int Surg J. 2017 Jun;4(6):1940-1944 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20172108
International Surgery Journal Subramaniyan P et al. Int Surg J. 2017 Jun;4(6):1940-1944 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20172108
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
NON OPERATIVE TREATMENT OF ACUTE APPENDICITIS - IS THIS APPROPRIATE IN SOUTH AFRICA O.D MONTWEDI
 NON OPERATIVE TREATMENT OF ACUTE APPENDICITIS - IS THIS APPROPRIATE IN SOUTH AFRICA O.D MONTWEDI Acute appendicitis is the commonest surgical emergency. About 300000 appendectomies are performed in the
NON OPERATIVE TREATMENT OF ACUTE APPENDICITIS - IS THIS APPROPRIATE IN SOUTH AFRICA O.D MONTWEDI Acute appendicitis is the commonest surgical emergency. About 300000 appendectomies are performed in the
The Use of Ultrasound in the Diagnosis of Crohn's Disease
 American Academy of Pediatrics CA2 Ashley Wachsman, MD Namita Singh, MD Newsletter June 2016 Cindy E. Kallman, MD The Use of Ultrasound in the Diagnosis of Crohn's Disease A few years ago, a prominent
American Academy of Pediatrics CA2 Ashley Wachsman, MD Namita Singh, MD Newsletter June 2016 Cindy E. Kallman, MD The Use of Ultrasound in the Diagnosis of Crohn's Disease A few years ago, a prominent
Contrast-enhanced small bowel ultrasound in the assessment of the small bowel in patients with Crohn s Disease
 Contrast-enhanced small bowel ultrasound in the assessment of the small bowel in patients with Crohn s Disease C.F. Healy 1, D. Ferguson 1, S. Jepson 1, B. Salh 2, F. Donnellan 2, N. Chatur 2, A. C. Harris
Contrast-enhanced small bowel ultrasound in the assessment of the small bowel in patients with Crohn s Disease C.F. Healy 1, D. Ferguson 1, S. Jepson 1, B. Salh 2, F. Donnellan 2, N. Chatur 2, A. C. Harris
Pediatric Surgical Emergencies Veronica Victorian, PA-C
 Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Pediatric Surgical Emergencies Veronica Victorian, PA-C Texas Children s Hospital Division of Pediatric General Surgery Assistant Professor, Baylor College of Medicine Objectives 1. Define Pediatric Surgical
Appendicitis. Controversies and Problems in Surgery December 20, 2013
 Appendicitis Controversies and Problems in Surgery December 20, 2013 Controversies Types and Use of Imaging Modalities Management in Adults, Children, Pregnancy Lap vs Open Management of Appendiceal Mass
Appendicitis Controversies and Problems in Surgery December 20, 2013 Controversies Types and Use of Imaging Modalities Management in Adults, Children, Pregnancy Lap vs Open Management of Appendiceal Mass
Società Medico Chirurgica di Ferrara 12 maggio Malattia diverticolare del colon. La TC in faseacuta
 Società Medico Chirurgica di Ferrara 12 maggio 2012 La TC in faseacuta Pier Marco Cervi U.O. Radiodiagnostica Ospedaliera Direttore Dott. Stefano Bighi Azienda Ospedaliera Universitaria S. Anna di Ferrara
Società Medico Chirurgica di Ferrara 12 maggio 2012 La TC in faseacuta Pier Marco Cervi U.O. Radiodiagnostica Ospedaliera Direttore Dott. Stefano Bighi Azienda Ospedaliera Universitaria S. Anna di Ferrara
Ruptured Acute Appendicitis With Calcified Appendicolith Mimicking Acute Gastroenteritis
 ISPUB.COM The Internet Journal of Health Volume 12 Number 1 Ruptured Acute Appendicitis With Calcified Appendicolith Mimicking Acute Gastroenteritis M Akinkunmi, O Fadiran Citation M Akinkunmi, O Fadiran.
ISPUB.COM The Internet Journal of Health Volume 12 Number 1 Ruptured Acute Appendicitis With Calcified Appendicolith Mimicking Acute Gastroenteritis M Akinkunmi, O Fadiran Citation M Akinkunmi, O Fadiran.
INTRALUMINAL GAS IN NON-PERFORATED ACUTE APPENDICITIS: A predictor of gangrenous appendicitis
 INTRALUMINAL GAS IN NON-PERFORATED ACUTE APPENDICITIS: A predictor of gangrenous appendicitis DM Plata Ariza, MD; E Martínez Chamorro, MD; D Castaño Pardo, MD; M Arroyo López, MD; E Peghini Gavilanes,
INTRALUMINAL GAS IN NON-PERFORATED ACUTE APPENDICITIS: A predictor of gangrenous appendicitis DM Plata Ariza, MD; E Martínez Chamorro, MD; D Castaño Pardo, MD; M Arroyo López, MD; E Peghini Gavilanes,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability
 Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Necrotizing Enterocolitis: the role of ultrasound in the assessment of bowel viability Ricardo Faingold, MD. Department of Medical Imaging The Montreal Children s Hospital McGill University SPR Vancouver
Bushra Arafa Zayed & Hanan Jamal. - Dana AF
 - 10 - Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures
- 10 - Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures
Right Colon, Sigmoid Colon, and Transverse Colon Diverticulitis in the Same Patient: Report of a Case
 Right Colon, Sigmoid Colon, and Transverse Colon Diverticulitis in the Same Patient: Report of a Case Marc Greenwald, M.D., Tzvi Nussbaum, M.D. Department of Surgery, Division of Colon and Rectal Surgery,
Right Colon, Sigmoid Colon, and Transverse Colon Diverticulitis in the Same Patient: Report of a Case Marc Greenwald, M.D., Tzvi Nussbaum, M.D. Department of Surgery, Division of Colon and Rectal Surgery,
Appendicitis. I. Background & Significance: Algorithm Definitions 1. CASE
 I. Background & Significance: Appendicitis Appendicitis is one of the most common acquired surgical conditions of childhood. Diagnosis of appendicitis remains difficult. Much work has been done on validation
I. Background & Significance: Appendicitis Appendicitis is one of the most common acquired surgical conditions of childhood. Diagnosis of appendicitis remains difficult. Much work has been done on validation
Conservative versus surgical management of pediatric appendicitis
 The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Conservative versus surgical management of pediatric appendicitis Kristin Anne Wishnosky Follow this
The University of Toledo The University of Toledo Digital Repository Master s and Doctoral Projects Conservative versus surgical management of pediatric appendicitis Kristin Anne Wishnosky Follow this
Nonoperative Management of Appendiceal Phlegmon or Abscess with an Appendicolith in Children
 J Gastrointest Surg (2013) 17:766 770 DOI 10.1007/s11605-013-2143-3 ORIGINAL ARTICLE Nonoperative Management of Appendiceal Phlegmon or Abscess with an Appendicolith in Children Hai-Lan Zhang & Yu-Zuo
J Gastrointest Surg (2013) 17:766 770 DOI 10.1007/s11605-013-2143-3 ORIGINAL ARTICLE Nonoperative Management of Appendiceal Phlegmon or Abscess with an Appendicolith in Children Hai-Lan Zhang & Yu-Zuo
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX
 Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Specialespecifikt kursus i Patologisk Anatomi 2009: Fordøjelseskanalens patologi APPENDIX Appendix Occurrence of lesions (%) Acute appendicitis 72 Normal 16 Fibrosis 3 (Cyst-)Adenoma 3 Diverticulitis
Pitfalls in CT diagnosis of appendicitis: Pictorial essay
 bs_bs_banner Journal of Medical Imaging and Radiation Oncology 57 (2013) 329 336 RADIOLOGY PICTORIAL ESSAY Pitfalls in CT diagnosis of appendicitis: Pictorial essay Ashkan Shademan and Rafel FR Tappouni
bs_bs_banner Journal of Medical Imaging and Radiation Oncology 57 (2013) 329 336 RADIOLOGY PICTORIAL ESSAY Pitfalls in CT diagnosis of appendicitis: Pictorial essay Ashkan Shademan and Rafel FR Tappouni
Appendicitis Care Map. Go directly to Care Map Flowchart
 Appendicitis Care Map Go directly to Care Map Flowchart How to Use Reference Icons Go directly to Care Map Flowchart When accessing a document, please use the browser return arrow (upper left-hand corner)
Appendicitis Care Map Go directly to Care Map Flowchart How to Use Reference Icons Go directly to Care Map Flowchart When accessing a document, please use the browser return arrow (upper left-hand corner)
Khanal BR, Ansari MA, Pradhan S Department of Radiology and Imaging, Tribhuvan University Teaching Hospital, Maharajgunj, Kathmandu, Nepal.
 Kathmandu University Medical Journal (2008), Vol. 6, No. 1, Issue 21, 70-74 Original Article Accuracy of ultrasonography in the diagnosis of acute appendicitis Khanal BR, Ansari MA, Pradhan S Department
Kathmandu University Medical Journal (2008), Vol. 6, No. 1, Issue 21, 70-74 Original Article Accuracy of ultrasonography in the diagnosis of acute appendicitis Khanal BR, Ansari MA, Pradhan S Department
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
International Journal of Scientific & Engineering Research, Volume 7, Issue 8, August ISSN
 International Journal of Scientific & Engineering Research, Volume 7, Issue 8, August-2016 186 Incidence of Intra-abdominal Collection in Open vs. Laparoscopic Mahdi H. Al-Bandar1, MD, Mansour A. Al-Ramadhan1,
International Journal of Scientific & Engineering Research, Volume 7, Issue 8, August-2016 186 Incidence of Intra-abdominal Collection in Open vs. Laparoscopic Mahdi H. Al-Bandar1, MD, Mansour A. Al-Ramadhan1,
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Intraluminal gas in non-perforated acute appendicitis: a CT sign of gangrenous appendicitis
 Intraluminal gas in non-perforated acute appendicitis: a CT sign of gangrenous appendicitis Poster No.: C-978 Congress: ECR 202 Type: Scientific Exhibit Authors: D. Plata Ariza, E. MARTINEZ CHAMORRO, J.
Intraluminal gas in non-perforated acute appendicitis: a CT sign of gangrenous appendicitis Poster No.: C-978 Congress: ECR 202 Type: Scientific Exhibit Authors: D. Plata Ariza, E. MARTINEZ CHAMORRO, J.
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
ORIGINAL ARTICLE ROLE OF ULTRASONOGRAPHY IN PRE-OPERATIVE EVALUATION OF RIGHT ILIAC FOSSA MASS
 ROLE OF ULTRASONOGRAPHY IN PRE-OPERATIVE EVALUATION OF RIGHT ILIAC FOSSA MASS Madhushankar L 1, Satish Kumar R 2, Sanjay S.C 3, Laxmikanta. L 4, Hemanth V 5 HOW TO CITE THIS ARTICLE: Madhushankar L, Satish
ROLE OF ULTRASONOGRAPHY IN PRE-OPERATIVE EVALUATION OF RIGHT ILIAC FOSSA MASS Madhushankar L 1, Satish Kumar R 2, Sanjay S.C 3, Laxmikanta. L 4, Hemanth V 5 HOW TO CITE THIS ARTICLE: Madhushankar L, Satish
Comparative study between open and laparoscopic appendectomy
 Original article: Comparative study between open and laparoscopic appendectomy 1Dr Mayank Gupta*, 2 Prof Dr Sunil Agarwal, 3 Prof Dr Ashok Gupta 13 rd year P.G. Resident Gen. Surgery, National Institute
Original article: Comparative study between open and laparoscopic appendectomy 1Dr Mayank Gupta*, 2 Prof Dr Sunil Agarwal, 3 Prof Dr Ashok Gupta 13 rd year P.G. Resident Gen. Surgery, National Institute
Critical Review Form Clinical Decision Analysis
 Critical Review Form Clinical Decision Analysis An Interdisciplinary Initiative to Reduce Radiation Exposure: Evaluation of Appendicitis in a Pediatric Emergency Department with Clinical Assessment Supported
Critical Review Form Clinical Decision Analysis An Interdisciplinary Initiative to Reduce Radiation Exposure: Evaluation of Appendicitis in a Pediatric Emergency Department with Clinical Assessment Supported
January 2015 Updates. Dec.4, 2014 SCR Education Call
 January 2015 Updates Dec.4, 2014 SCR Education Call Trauma codes Trauma cases specifically: Any injury with a principal ICD-9 or ICD-10 diagnostic code will be excluded from sampling within the range of:
January 2015 Updates Dec.4, 2014 SCR Education Call Trauma codes Trauma cases specifically: Any injury with a principal ICD-9 or ICD-10 diagnostic code will be excluded from sampling within the range of:
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University.
 Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
Mohamed EL-hemaly Gastro- intestinal surgical center, Mansoura University. Chronic transmural inflammatory process of the bowel & affects any part of the gastro -intestinal tract from the mouth to the
To Evaluate the Efficacy of Alvarado Score and Ultrasonography in Acute Appendicitis
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 15, Issue 9 Ver. XI (September). 16), PP 14-18 www.iosrjournals.org To Evaluate the Efficacy of Alvarado
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 15, Issue 9 Ver. XI (September). 16), PP 14-18 www.iosrjournals.org To Evaluate the Efficacy of Alvarado
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Introduction Diagnosis of acute appendicitis is basically a clinical matter. Many patients present with a typical history and physical examination fin
 Modified Clinical Score of Acute Appendicitis Surgical Department College Of Medicine Karballa University. Abstract B ackground Suspected acute appendicitis is the most common non traumatic admissions
Modified Clinical Score of Acute Appendicitis Surgical Department College Of Medicine Karballa University. Abstract B ackground Suspected acute appendicitis is the most common non traumatic admissions
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
World Journal of Colorectal Surgery Volume 6, Issue 4 2016 Article 3 Laparoscopic Right Colectomy For Appendiceal Mucinous Cystadenoma: A Case Report Dion A. Putra Adianto Nugroho Ibrahim Basir University
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Imaging Patients with Acute Abdominal Pain 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Jaap Stoker, MD Adrienne
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Jaap Stoker, MD Adrienne
Citywide Infectious Disease Conference. March 27 th, 2018
 Citywide Infectious Disease Conference March 27 th, 2018 Citywide Show and Tell Case 1 Summary 60 s year old Puerto Rican born man SCC of Esophagus, treated with radiation and chemotherapy and then esophageal
Citywide Infectious Disease Conference March 27 th, 2018 Citywide Show and Tell Case 1 Summary 60 s year old Puerto Rican born man SCC of Esophagus, treated with radiation and chemotherapy and then esophageal
Post-appendectomy appendicitis: A case report
 www.edoriumjournals.com CASE REPORT PEER REVIEWED OPEN ACCESS Post-appendectomy appendicitis: A case report Ali Safar, Abdulrahman Al-Aqeeli, Ahmad Al-Mass, Bader Al-Shaban ABSTRACT Introduction: Acute
www.edoriumjournals.com CASE REPORT PEER REVIEWED OPEN ACCESS Post-appendectomy appendicitis: A case report Ali Safar, Abdulrahman Al-Aqeeli, Ahmad Al-Mass, Bader Al-Shaban ABSTRACT Introduction: Acute
Postoperative Ultrasound Evaluation of Gastric Distension; A Pilot study
 Postoperative Ultrasound Evaluation of Gastric Distension; A Pilot study M Jaronczyk MD, W Boyan Jr. MD, M Goldfarb MD. FACS. MMC Dept of Surgery Nausea and vomiting are common complaints of postoperative
Postoperative Ultrasound Evaluation of Gastric Distension; A Pilot study M Jaronczyk MD, W Boyan Jr. MD, M Goldfarb MD. FACS. MMC Dept of Surgery Nausea and vomiting are common complaints of postoperative