Management of Gallbladder Disease
|
|
|
- Leon Conley
- 6 years ago
- Views:
Transcription
1 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of Medicine - Phoenix Chairman, Department of Surgery Banner University Medicine, Phoenix
2 What are we going to discuss? Cholelithiasis and Choledocholithiasis Acute disease Chronic Disease Acalculus Gallbladder Diseases
3 What are we not going to discuss? Malignant pancreatico-biliary diseases Choledochocal cysts Biliary Ascaris, Cryptosporidium,and Flukes Benign biliary strictures and atresias Chronic pancreatitis
 asymptomatic Annually, 1 4% develop complication Most costly digestive disease in US 1 million hospitalizations, 700,000 operative procedures Annual cost: $5")
4 Gallbladder Disease Spectrum of disease involving the biliary tree, usually related to gallstones Approximately 10 15% general population Increases with age, gender Higher in Arizona, Pima Indian group particularly at risk Most (50%) asymptomatic Annually, 1 4% develop complication Most costly digestive disease in US 1 million hospitalizations, 700,000 operative procedures Annual cost: $5 billion NEJM 330: 403, 1994 J Am Col Surg 210: 668, 2010

5 Gallbladder Disease - Spectrum Asymptomatic cholelithiasis Biliary colic/chronic cholecystitis Biliary dyskinesia Acute cholecystitis Gangrenous cholecystitis Acalculous cholecystitis Asymptomatic choledocholithiasis Choledocholithiasis obstructive jaundice Cholangitis Gallstone pancreatitis
6 Case Presentation 41 yo female with no past medical history presents to the ED following MVC resulting in left femur fracture and no other injuries. She is afebrile, HR 110, BP 140/70, RR 18 Abdominal CT scan demonstrates no acute injuries but
7 Gallstones
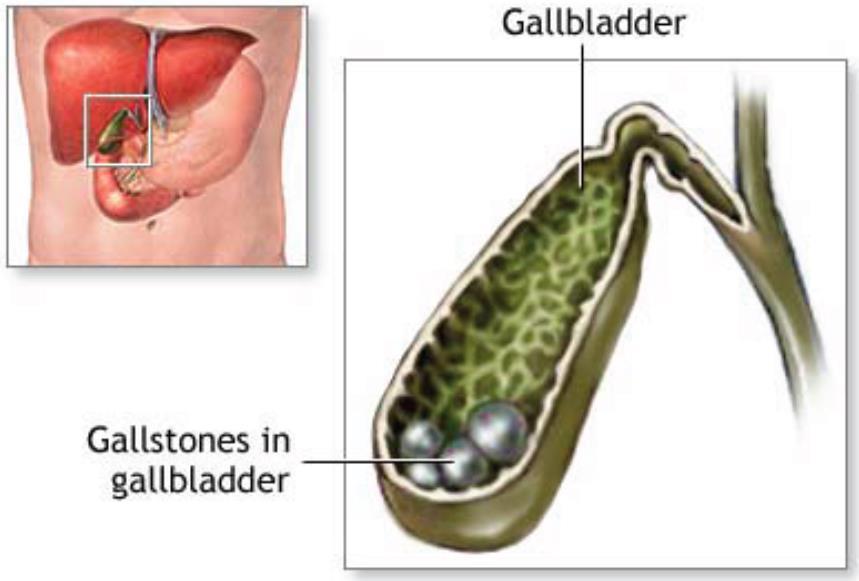
8 Asymptomatic Cholelithiasis

9 Cholelithiasis: Cholesterol and Pigmented Types
10 Risk Factors for Cholelithiasis Cholesterol: Supersaturation, typically too much cholesterol Pigmented: Hemolytic conditions or infections Age increases between years old Female gender Pregnancy/multiple children OCP s/estrogen replacement Estrogen increases biliary cholesterol secretion Progesterone decreases bile acid secretion Family History 2 fold increase, Pima Indians Obesity 35% of gastric bypass patients have stones 5 F s: Fat, Forty, Female, Fertile, Family
11 Asymptomatic Cholelithiasis Her sister had gallstones and had her gallbladder removed. She wants to know if she should get her gallbladder removed Should she?
12 Natural History Asymptomatic Stones 5yrs 10% symptomatic (2%/yr) 10yrs 15% symptomatic 15yrs 18% symptomatic ***90% who become symptomatic initially have just biliary colic Cholecystectomy not needed Symptomatic stones 50% develop recurrent sx 1-2%/yr develop complications of gallstone disease Cholecystectomy indicated Gracie NEJM. 1982

13 Surgery for Asymptomatic Cholelithiasis Gallbladder adenomas > 1 cm Porcelin gallbladder Pre-transplant Bone marrow Cardiac Lung
14 Case Presentation (continued) One year following uneventful recovery from her MVC she develops: Intermittent right upper quadrant/midepigastric abdominal pain Radiates around right side to intrascapular area of back Occurs 6-12 hours after eating, especially Kentucky Fried Chicken (Original Recipe) Associated with nausea and anorexia Antacids don t help but pain spontaneously resolves after several hours

15 Differential Diagnosis of Epigastric Pain Peptic Ulcer Disease Pancreatitis Biliary Colic Hepatitis Gastroenteritis Intestinal Obstruction Mesenteric Ischemia Myocardial Infarction

16 Cholelithiasis: Ultrasound Diagnosis

17
18 Symptomatic Cholelithiasis Biliary Colic Clinical signs and symptoms Ultrasound or other radiographic confirmation No evidence of acute invasive infection or inflammation No evidence of jaundice, pancreatitis, or common bile duct stones or dilatation (>1.0cm) Treatment: Avoid fatty foods Elective cholecystectomy (laparoscopic) at convenience Intraoperative cholangiogram: Hx of CBD involvement
19 Biliary Dyskinesia Classic biliary colic symptoms Absence of cholelithiasis Low (<30%) gallbladder ejection fraction on HIDA scan Symptoms recreated with cholecystokinin injection Due to dysfunctional contraction of gallbladder Treatment: Laparoscopic cholecystectomy without intraoperative cholangiogram Sustained benefit: 70-80% long term pain relief
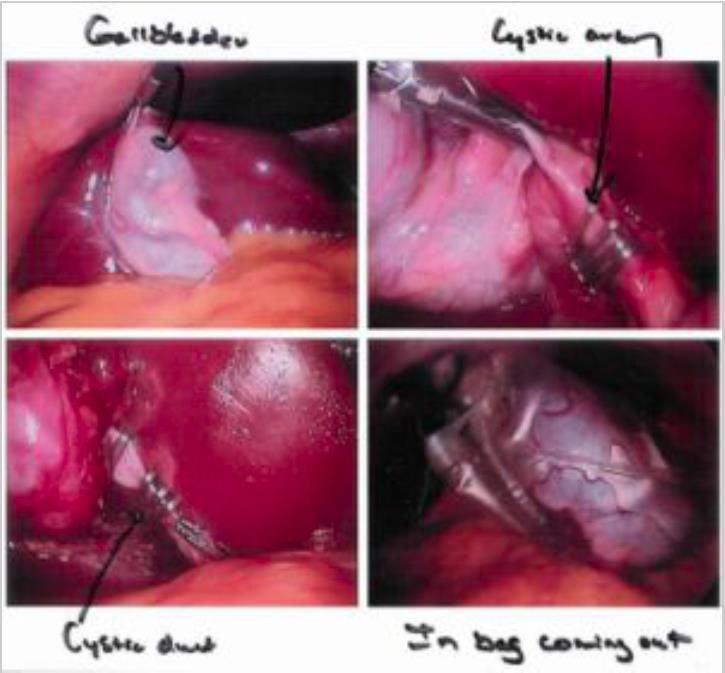
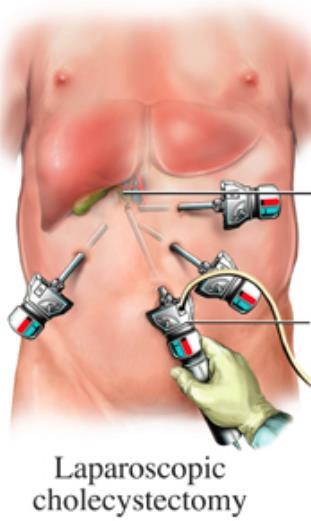
20 Laparoscopic Cholecystectomy
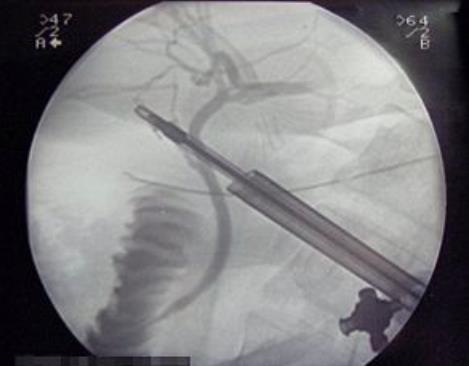
21 Intraoperative Cholangiogram
22 Conversion from Laparoscopy to Open Decision surgeon specific Safety is the most important consideration Factors affecting: Multiple previous operations Extent of pericholecystic inflammation Anatomic variant concerns Bleeding Concern for or recognized CBD injury

23 Conversion to Open Cholecystectomy

24 Conversion to Open Cholecystectomy

25 Conversion to Open Cholecystectomy
26 Case Presentation (continued) Patient scheduled to undergo elective laparoscopic cholecystectomy in 4 weeks One week before surgery presents to ED with 2 days of marked constant RUQ pain associated with fever (102.8F), vomiting, anorexia and (+) Murphy s sign WBC 16.2; HCT 48%; Platelet Count 330 Chem 7 normal ALT 35 AST 26 Alk Phos 150 Bilirubin 1.8 Amylase 30 Lipase 46 Ultrasound consistent with acute cholecystitis

27 Cholecystitis: Acute or Chronic Inflammation

28 Acute Cholecystitis: Ultrasound Findings Gallbladder wall thickening >3mm Pericholecystic fluid Cholelithiasis Sonographic Murphy s sign 90-96% sensitive CBD assessesment Size: < 10 mm Choledocholithiasis
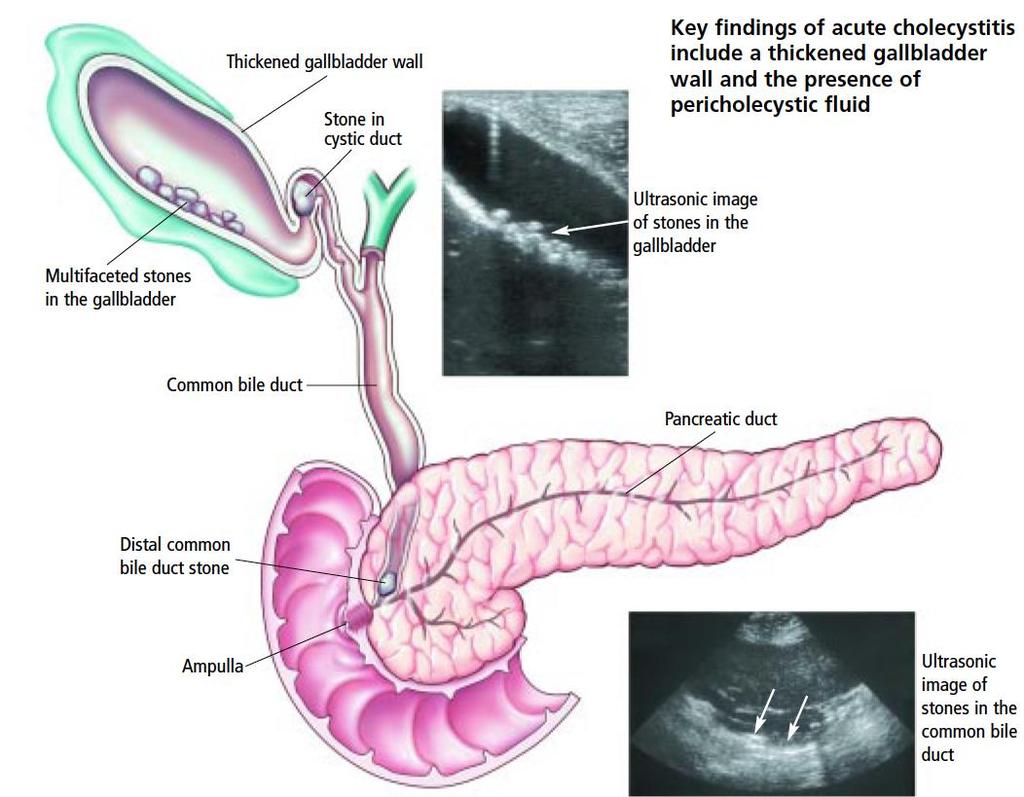
29
30 Acute Cholecystitis Acute inflammation of gallbladder related to stone occluding cystic duct Frequently infected (gram negatives and anaerobes) Assess pain, PO intake, systemic inflammation Admit for IV antibiotics, hydration Consider cholecystectomy during admission Duration of acute symptoms important determinant < 5 days preferable due to decreased fibrous inflammation
31 Acute Cholecystitis: Operate or not J Am Coll Surg 210:668, 2010
32 Acute Cholecystectomy: Timing of Surgery Typically within 5 days of symptoms onset, preferably with 72 hours Acute inflammation progresses to fibrotic changes Higher rate of conversion to open and bile duct injury if delayed High risk patients should be considered for cholecystostomy tube placement ICU patients with other severe co-morbidities (LVAD, ECMO) Advanced liver disease (Child s A:10%, B: 25%, C: 50%)
33 Cholecystostomy vs Cholecystectomy World J Surg 35:826, 2011
34 Acute Acalculous Cholecystitis Acute cholecystitis without cholelithiasis, probably ischemic etiology Disease of acutely ill patients, typically in ICU TPN is a risk factor Diagnosis made by ultrasound and/or HIDA scan Treatment depends on overall condition: Severely ill Percutaneous cholecystotomy tube Mild to moderate - Cholecystectomy
35 Case Presentation (continued) Day after admission labs: TB 4.8, Alk Phos 500, amylase 95, lipase 60, WBC 22 Pain unchanged Fever 102.5, appears jaundiced, decreased mental status, BP 90/40 Intra- and extrahepatic bile duct dilated, CBD 14 mm
36 Acute Cholangitis Obstructive jaundice due to choledocholithiasis, malignancy, or stricture. Jaundice with dark urine (urobilinogen) is surgical Jaundice with clear urine (urobilin) is medical Sepsis related to infected proximal bile in occluded duct, can cause septic shock Cholecystitis increases bilirubin to <2.0 Cholangitis increases bilirubin to >2.0 Treatment: Antibiotics, hydration, and bile duct decompression
37 Acute Cholangitis Charcot s Triad Jaundice RUQ pain Fever, chills Reynold s Pentad Jaundice RUQ pain Fever, chills Mental Status changes Hypotension
38 Choledocholithiasis Risk Factors Jaundice > 2.0 > 4.0 should undergo pre-operative ERCP Alkaline phosphatase > normal Common bile duct > 8 mm (age dependent) U/S or CT evidence of CBD stone Pancreatitis or history of pancreatitis
: PTC or surgical decompression")
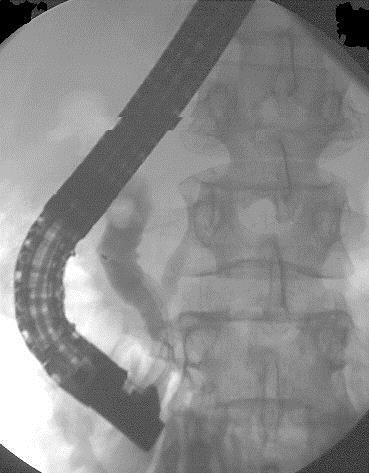
39 Endoscopic Retrograde Cholangiopancreatography ERCP Cannulation of ampulla Diagnostic and therapeutic Determines etiology of obstruction Removal of bile duct stones, placement of biliary stent Unsuccessful (rare): PTC or surgical decompression
40 Common Bile Duct Drains Endoscopically placed biliary stent Percutaneous transhepatic biliary drain Surgically placed bile duct drains T-tube Transhepatic or enteric biliary drain

41
42 Case Presentation (continued) ERCP performed with extraction of impacted CBD stone at level of ampulla Following day: TB 2.8, amylase 3000, lipase 4500 Pain worse, WBC 24, febrile





43 Abdominal Pain and Increased Serum Amylase Cholecystitis Peptic ulcer Cholangitis Pancreatitis Kidney stone Ectopic pregnancy Intestinal obstruction, ischemia or perforation


44 Pancreatic Enzymes in Acute Pancreatitis Fold increase over normal Lipase Amylase Hours after onset
45 fluid gallstones pancreas
46
47 Case Presentation (continued): Our Patient History: She denied alcohol use, she was not taking any medicines, no history of recent trauma Known choledocholithiasis, recent ERCP Labs: Normal calcium and triglycerides * elevated liver enzymes and bilirubin

48 Diagnosis?? Acute Pancreatitis
49 Severity of Acute Pancreatitis Signs and symptoms of pancreatitis range from mild pain to a severe life threatening illness Pancreatitic edema=mild pancreatitis Pancreatic necrosis=severe pancreatitis Cholecystectomy indicated during hospitalization 33-50% recurrance if wait 4-6 weeks Early cholecystectomy indicated when mild inflammation

50 Mild vs Severe Acute Pancreatitis
51 Post-Operative Expectations Pre-operative indication Biliary colic Biliary dyskinesia Systemic manifestations Acute cholecystitis Mild gallstone pancreatitis Cholangitis Co-morbidities Severe pancreatitis Organ dysfunctions
52 Post-Operative Expectations: Elective Outpatient surgery Minimal pain, anorexia Return to usual activities within 7-14 days Fevers, worsening abdominal pain, inability to tolerate PO, or JAUNDICE = potential problem Requires further workup, don t blame other causes Early involvement of surgical service Labs: CBC, amylase/lipase, liver function tests CT or U/S to evaluate for free fluid and CBD size
53 Post-Operative Jaundice Maybe related to pre-operative disease but should immediately be decreasing post-operative if duct cleared Related to bile leak (cystic duct usually), stricture, or obstruction (stone or clip) Risk factors Laparoscopic > open ( % vs %) Acute cholecystitis vs biliary colic Age Pre-operative CBD stones
54 Post-Operative Jaundice Needs further workup Small CBD with fluid: HIDA, MRCP, or ERCP to evaluate for leak Dilated CBD: MRCP or ERCP to evaluate for obstruction ERCP for management of leak or obstruction Cystic duct leak: ERCP stent +/- percutaneous subhepatic drain CBD stricture: ERCP stent, re-evaluate subsequently for surgery CBD obstruction: ERCP +/-stent, most likely surgery AJR 191:94, 2008
55 Summary Gallbladder disease has wide spectrum of presentation, most are asymptomatic Laparoscopic cholecystectomy is preferred management Conversion to open more related to degree of inflammation and safety than skill Cholecystostomy has role in selected critically ill or major co-morbidity patients Post-operative deviation from expected, especially fever, pain or jaundice requires additional workup
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
The campaign on laboratory: focus on Gallstone Disease and ERCP
 The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
EAST MULTICENTER STUDY PROPOSAL
 EAST MULTICENTER STUDY PROPOSAL (Proposal forms must be completed in its entirety, incomplete forms will not be considered) GENERAL INFORMATION Study Title: Prospective Multi-Institutional Evaluation of
EAST MULTICENTER STUDY PROPOSAL (Proposal forms must be completed in its entirety, incomplete forms will not be considered) GENERAL INFORMATION Study Title: Prospective Multi-Institutional Evaluation of
What Are Gallstones? GALLSTONES. Gallstones are pieces of hard, solid matter that form over time in. the gallbladder of some people.
 What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
Biliary Tract Disease. Emmet Andrews Cork University Hospital 6 th September 2010
 Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Hepatobiliary Disease
 Hepatobiliary Disease 大林慈濟綜合醫院 魏昌國 一般外科 Cholelithiasis 膽道結石 Incidence (USA) 10% in adult 85% cholesterol stones 15% pigment stone Risk factors Cholesterol stones Age Female(2x, 25% versus 12% at age 60),
Hepatobiliary Disease 大林慈濟綜合醫院 魏昌國 一般外科 Cholelithiasis 膽道結石 Incidence (USA) 10% in adult 85% cholesterol stones 15% pigment stone Risk factors Cholesterol stones Age Female(2x, 25% versus 12% at age 60),
Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis
 Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Surveillance proposal consultation document
 Surveillance proposal consultation document 2018 surveillance of Gallstone disease: diagnosis and management (NICE guideline CG188) Proposed surveillance decision We propose to not update the NICE guideline
Surveillance proposal consultation document 2018 surveillance of Gallstone disease: diagnosis and management (NICE guideline CG188) Proposed surveillance decision We propose to not update the NICE guideline
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 Appendix B: Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE Post publication note: The title of this guideline changed during development. This scope was published before the guideline
Appendix B: Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE Post publication note: The title of this guideline changed during development. This scope was published before the guideline
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study
 Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
JAUNDICE. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
Rokitansky-Aschoff sinuses are epithelial invaginations in the gallbladder wall that from as a result of increased gallbladder pressures.
 Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Cholangiocarcinoma: Radiologic evaluation and interventions
 November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
CBD stones & strictures (Obstructive jaundice)
") 1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
Study of post cholecystectomy biliary leakage and its management
 Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
ENDOSCOPIC TREATMENT OF A BILE DUCT
 HPB Surgery, 1990, Vol. 3, pp. 67-71 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORT
HPB Surgery, 1990, Vol. 3, pp. 67-71 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORT
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 2018 surveillance of Gallstone disease: diagnosis and management (2014) NICE guideline CG188 Summary of evidence from surveillance Studies identified in
Appendix A: Summary of evidence from surveillance 2018 surveillance of Gallstone disease: diagnosis and management (2014) NICE guideline CG188 Summary of evidence from surveillance Studies identified in
REFERRAL GUIDELINES: GALLSTONES
 REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL AUGUST 2017
 DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
Gallstones. Classification
 Gallstones Nariman Karanjia Tahir Ali Abstract Gallstones are extremely common in the UK and have a major effect on healthcare resources. Presentation depends on whether the stones occlude the cystic duct
Gallstones Nariman Karanjia Tahir Ali Abstract Gallstones are extremely common in the UK and have a major effect on healthcare resources. Presentation depends on whether the stones occlude the cystic duct
Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL
 Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL Differential Diagnosis of RUQ pain Gallstone disease (and its related complications) Gastritis/duodenitis Peptic ulcer
Biliary Tract Disease NIKI TADAYON GENERAL & VASCULAR SURGEON SHOHADA TAJRISH HOSPITAL Differential Diagnosis of RUQ pain Gallstone disease (and its related complications) Gastritis/duodenitis Peptic ulcer
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Imaging of Biliary Tract Emergencies in Jorge A. Soto, MD Professor of Radiology Boston University Medical Center.
 Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Biliary Tract Disease HPB Division, Surgery Department of Ramathibodi. Paramin Muangkaew MD.
 Biliary Tract Disease HPB Division, Surgery Department of Ramathibodi Paramin Muangkaew MD. Anatomy Proximal Intrahepatic bile duct IHD Primary Secondary Extrahepatic bile duct Rt & Lt HD CHD Cystic duct
Biliary Tract Disease HPB Division, Surgery Department of Ramathibodi Paramin Muangkaew MD. Anatomy Proximal Intrahepatic bile duct IHD Primary Secondary Extrahepatic bile duct Rt & Lt HD CHD Cystic duct
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 )
 膽囊切除術 ( 腹腔鏡 / 開放性 )") Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids. Cholestasis
 Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
Noncalculous Biliary Disease Dean Abramson, M.D. Gastroenterologists, P.C. Cedar Rapids Cholestasis Biochemical hallmark Impaired bile flow from liver to small intestine Alkaline phosphatase is primary
From Inflammation to Ischemia May apply to all luminal structures Obstruction Small or large bowel Appendix Gall bladder Ureter Hydrostatic Pressure:
 The Acute Abdomen Surgical Issues for the Family Practitioner Rochelle A. Dicker, MD Assistant Professor of Surgery and Anesthesia UC San Francisco Visceral Pain Vague Deep Associated with nausea/vomiting
The Acute Abdomen Surgical Issues for the Family Practitioner Rochelle A. Dicker, MD Assistant Professor of Surgery and Anesthesia UC San Francisco Visceral Pain Vague Deep Associated with nausea/vomiting
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
LAPAROSCOPIC GALLBLADDER SURGERY
 LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital
 in a District General Hospital") Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Gallstones & Other Biliary Disorders
 Gallstones & Other Biliary Disorders Jason Smith MD DMI FRCS(Gen.Surg) Consultant General & Colorectal Surgeon Introduction Gallstones are found in 12% men and 24% women Prevalence increases with advancing
Gallstones & Other Biliary Disorders Jason Smith MD DMI FRCS(Gen.Surg) Consultant General & Colorectal Surgeon Introduction Gallstones are found in 12% men and 24% women Prevalence increases with advancing
Quality & Safety Committee 17 th August 2017 Agenda item: 6.2
 SUMMARY REPORT ABM University Health Board Quality & Safety Committee 17 th August 2017 Agenda item: 6.2 Subject Improvements in the management of gallstone disease Prepared by Approved & presented by:
SUMMARY REPORT ABM University Health Board Quality & Safety Committee 17 th August 2017 Agenda item: 6.2 Subject Improvements in the management of gallstone disease Prepared by Approved & presented by:
Hepatocellular Dysfunction
 www.nuclearmd.com A Normal HIDA Scan Dynamic or Static images of the abdomen are acquired after the IV administration 6-8 mci of Tc99m disofenin or mebrofenin, for one hour. Patients have to be NPO for
www.nuclearmd.com A Normal HIDA Scan Dynamic or Static images of the abdomen are acquired after the IV administration 6-8 mci of Tc99m disofenin or mebrofenin, for one hour. Patients have to be NPO for
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Comparative Study between Laparoscopic and Open Cholecystectomy for Dr. B. Hemasankararao 1,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Comparative Study between Laparoscopic and Open Cholecystectomy for Dr. B. Hemasankararao 1,
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
MANAGEMENT OF COMPLICATED GALLSTONE DISEASE
 gastrointestinal tract and abdomen MANAGEMENT OF COMPLICATED GALLSTONE DISEASE Carmen L. Mueller, BSc(H), MD, FRCSC, Amy A. Neville, MD, FRCSC, MSc, and Gerald M. Fried, MD, FRCSC, FACS, FCAHS Gallstones
gastrointestinal tract and abdomen MANAGEMENT OF COMPLICATED GALLSTONE DISEASE Carmen L. Mueller, BSc(H), MD, FRCSC, Amy A. Neville, MD, FRCSC, MSc, and Gerald M. Fried, MD, FRCSC, FACS, FCAHS Gallstones
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
SUNY Downstate Medical Center Kings County Hospital
 Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Gallstones. Farhad Zamani Prof. of Gastroenterology and Hepatology IUMS,GILDR Firoozgar Hospital December 2017
 Gallstones Farhad Zamani Prof. of Gastroenterology and Hepatology IUMS,GILDR Firoozgar Hospital December 2017 1 Gallstones Gallstones are composed of a mixture of cholesterol, calcium billirubinate,
Gallstones Farhad Zamani Prof. of Gastroenterology and Hepatology IUMS,GILDR Firoozgar Hospital December 2017 1 Gallstones Gallstones are composed of a mixture of cholesterol, calcium billirubinate,
Greater Manchester EUR Policy Statement on: Asymptomatic Gallstones GM Ref: GM061 Version: 0.2 (21 November 2018)
") Greater Manchester EUR Policy Statement on: Asymptomatic Gallstones GM Ref: GM061 Version: 0.2 (21 November 2018) Commissioning Statement Asymptomatic Gallstones Policy Exclusions (Alternative commissioning
Greater Manchester EUR Policy Statement on: Asymptomatic Gallstones GM Ref: GM061 Version: 0.2 (21 November 2018) Commissioning Statement Asymptomatic Gallstones Policy Exclusions (Alternative commissioning
Bile Duct Injuries. Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India
, MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India") Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
USMLE and COMLEX II. CE / CK Review. General Surgery. 1. Northwestern Medical Review
 USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
USMLE and COMLEX II CE / CK Review General Surgery 1. Northwestern Medical Review Northwestern Medical Review www.northwesternmedicalreview.com Lansing, Michigan 2014-2015 Acute Abdomen 1. Your patient
Case Study: #3: Gallbladder Carcinoma?
 Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Postoperative jaundice
 Postoperative jaundice Principles of Surgery Ehren Eksteen 17/3/2010 Abri Bezuidenhout 28/3/2012 Intro Jaundice is defined as yellow discolouration of the skin,sclera and heavily perfused areas in a patient
Postoperative jaundice Principles of Surgery Ehren Eksteen 17/3/2010 Abri Bezuidenhout 28/3/2012 Intro Jaundice is defined as yellow discolouration of the skin,sclera and heavily perfused areas in a patient
Biliary MRI w Eovist
 Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Percutaneous Cholecystostomy Tube in Acute Cholecystitis: Our Experience in a Tertiary Center in Saudi Arabia
 9 KUWAIT MEDICAL JOURNAL June 0 Original Article Percutaneous Cholecystostomy Tube in Acute Cholecystitis: Our Experience in a Tertiary Center in Saudi Arabia Faisal A Al-Saif, Hamad S AlSubaie, Rafif
9 KUWAIT MEDICAL JOURNAL June 0 Original Article Percutaneous Cholecystostomy Tube in Acute Cholecystitis: Our Experience in a Tertiary Center in Saudi Arabia Faisal A Al-Saif, Hamad S AlSubaie, Rafif
Guidelines for Laparoscopic CBD Exploration
 Guidelines for Laparoscopic CBD Exploration INDICATIONS Since the 1992 National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy the indications
Guidelines for Laparoscopic CBD Exploration INDICATIONS Since the 1992 National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy the indications
In The Name of God. Advanced Concept of Nursing- II UNIT- V Advance Nursing Management of GIT diseases. Cholecystitis.
 In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- V Advance Nursing Management of GIT diseases. Cholecystitis. Shahzad Bashir RN, BScN, DCHN,MScN
In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- V Advance Nursing Management of GIT diseases. Cholecystitis. Shahzad Bashir RN, BScN, DCHN,MScN
Cholelithiasis (Gallstones)
") GALL BLADDER Cholelithiasis (Gallstones) Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates are higher in Latin American countries (20-40%)
GALL BLADDER Cholelithiasis (Gallstones) Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates are higher in Latin American countries (20-40%)
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
Chapter 45 3/2/2017. Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder
 Chapter 45 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights
Chapter 45 Care of the Patient with a Gallbladder, Liver, Biliary Tract, or Exocrine Pancreatic Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights
Evolving Gallstone Ileus. SUNY Downstate Case Conference January 12, 2012
 Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
Evolving Gallstone Ileus SUNY Downstate Case Conference January 12, 2012 Initial Presentation HPI: 90 yo F c 1wk h/o abdominal pain and N/V. Denied F/C. Passing flatus/bm. PMH: DM, HTN, CAD. PSH: C-sections
Endoscopic Retrograde Pancreatography and Laparoscopic Cholecystectomy. TEAM 1 Janix M. De Guzman, MD Presentor
 Endoscopic Retrograde Pancreatography and Laparoscopic Cholecystectomy TEAM 1 Janix M. De Guzman, MD Presentor Premise 40F Jaundice Abdominal pain US finding of gallstones with apparently normal common
Endoscopic Retrograde Pancreatography and Laparoscopic Cholecystectomy TEAM 1 Janix M. De Guzman, MD Presentor Premise 40F Jaundice Abdominal pain US finding of gallstones with apparently normal common