Acute Postoperative Pain. David Radvinsky, MD March 24, 2016
|
|
|
- Amanda Gaines
- 6 years ago
- Views:
Transcription
1 Acute Postoperative Pain David Radvinsky, MD March 24, 2016
2 Objectives 1. Discuss the multimodal approach to pain management and discuss the various classes of drugs based on receptor mechanism. 2. Give you applicable examples of pain regimens that you can start using on your patients today. 3. Discuss pain control and sedation in the ICU.
3 Is this painful yet? 55 yo male s/p laparoscopic low anterior resection. What are your postoperative pain orders?
4 Is this painful yet? 55 yo male s/p laparoscopic low anterior resection. What are your postoperative pain orders? Ofirmev 1000 mg IVPB Q6hr
5 Is this painful yet? 55 yo male s/p laparoscopic low anterior resection. What are your postoperative pain orders? Ofirmev 1000 mg IVPB Q6hr Morphine 4mg IM Q4hr prn
6 Is this painful yet? 55 yo male s/p laparoscopic low anterior resection. What are your postoperative pain orders? Ofirmev 1000 mg IVPB Q6hr Morphine 4mg IM Q4hr prn Percocet 5/325 mg PO Q4-6 hr prn
7 Scale of 0-10 Acute postoperative pain is a complex physiological reaction to tissue injury, visceral distention, or disease. It is a manifestation of autonomic, psychological, and behavioral responses that result in patient-specific unpleasant, unwanted sensory and emotional experiences. Wall & Melzack's Textbook of Pain Pain is a personal, subjective experience.
8 Consequences Physiologic Increased stress response Cardiovascular events Pulmonary complications Ventilator dyssynchrony Diaphragmatic dysfunction Stress ulcers Delayed wound healing Immunosuppression Thromboembolic events Chronic pain Psychologic Emotional stress Delirium Depression Anxiety Helplessness PTSD Social/Economic Increased length of stay Increased mortality Increased cost Increased mechanical ventilation duration Decreased quality of care
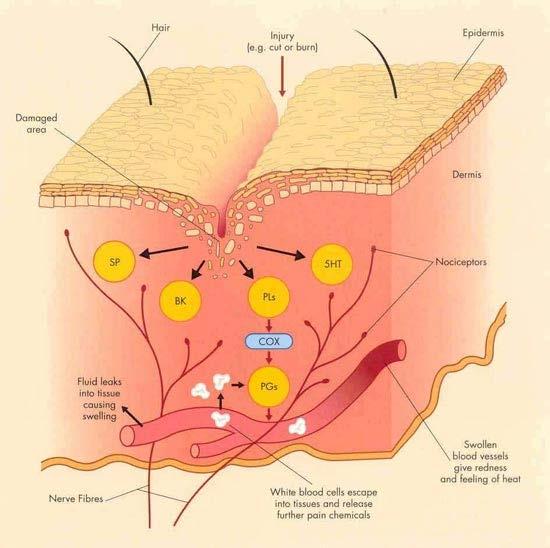
9 Classification of Pain Nociceptive: normal response to noxious insult or injury Neuropathic: pain initiated or caused by a primary lesion or disease in the somatosensory nervous system. Inflammatory: a result of activation and sensitization of the nociceptive pain pathway by a variety of mediators released at a site of tissue inflammation.

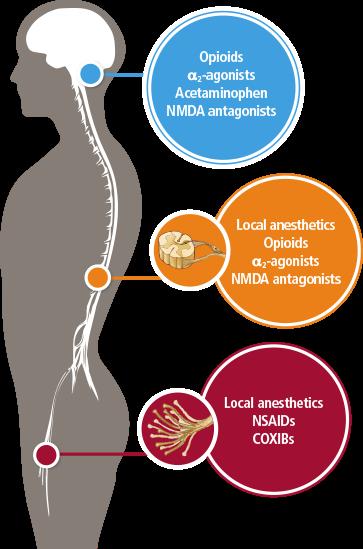
10 Pain pathways
 Administration of 2 or more analgesic agents with different mechanisms of action Synergistic effects Reduced opioid")
11 Multimodal therapy Response to the under treatment of postoperative pain Limitation of opioid monotherapy Introduced in the early 1990 s (Kehlet & Dahl) Administration of 2 or more analgesic agents with different mechanisms of action Synergistic effects Reduced opioid usage

12 Preoperative/Methods of Assessment General Principles Regarding Multimodal therapy Systemic Pharmacologic Therapies Local/Topical Pharmacologic Therapies Peripheral Regional Anesthesia Neuraxial Therapies

13 Perioperative management Guidelines on the Management of Postoperative Pain Preoperative expectations and realistic goals for pain control Decreased opiod use Less preoperative anxiety Fewer requests for sedative medications Reduced length of stay Patient and family-centered, tailored education Assessment & reassessment Pain specialist

14 Opioids Four major subtypes of opioid receptors Side effects: itchiness, sedation, nausea, respiratory depression, constipation, and euphoria. Tolerance and dependence develops with continuous use Withdrawal syndrome upon abrupt discontinuation.

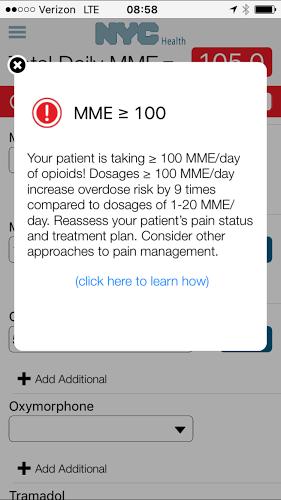
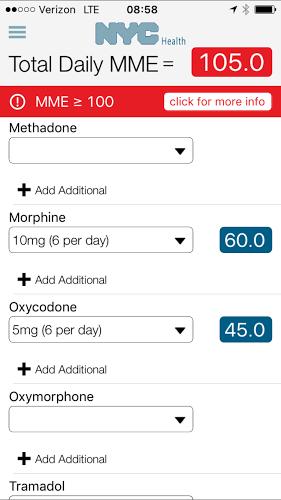
15 Opioids 28,647 deaths from opioid overdose in 2014 No evidence shows a long-term benefit of opioids vs. no opioids for chronic pain Extensive evidence shows the possible harms of opioids. Extensive evidence suggests benefits of non-pharmacologic and non-opioid pharmacologic therapy, with less harm. New York State Electronic prescriptions I-STOP/prescription monitoring
16 Opioids
17 Opioids
18 Opioids Guidelines on the Management of Postoperative Pain Oral over IV opioids Short-acting over long acting No benefit to pre-operative opioids Avoid using IM route for administration PCA for systemic analgesia when parenteral route needed No routine basal infusion of opioids with PCA
19 NSAIDs & Acetaminophen
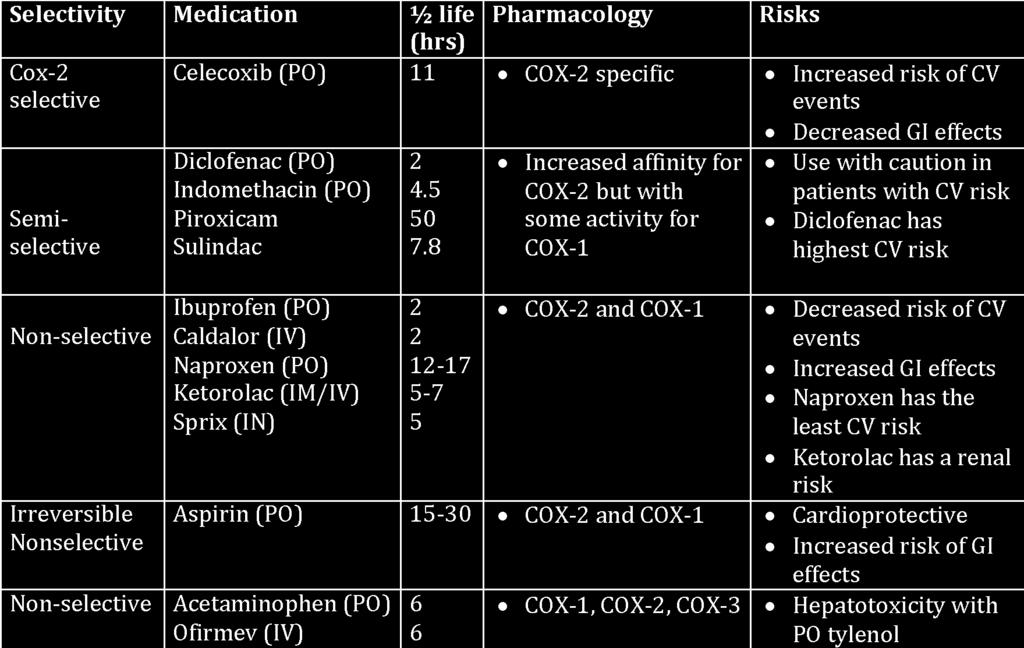
20 NSAIDs & Acetaminophen
21 NSAIDs & Acetaminophen Guidelines on the Management of Postoperative Pain Less postoperative pain or opioid consumption when used in conjunction with opioids than opioids alone. Increased risk of CV events, GI bleeding, and renal dysfunction Celecoxib dose preoperatively (30 minutes to 1 hour) associated with reduced opioid use postoperatively (Not in CABG).
22 NMDA antagonists Ketamine (IV) ½ life 2-3 hours Decreased incidence of acute and chronic pain Reduced opiate consumption Significantly lower pain scores Great option for analgesia in children Adverse effects: dissociative analgesia, emergence delirium, hallucinations, increased HR, SV, BP; bronchodilation, increased salivation and secretions, nystagmus, blurred vision ICU Continuous sedation for chronically ventilated patients Severe status asthmaticus unresponsive to standard therapy Memantine (PO) phantom limb pain Magnesium (IV) perioperative reduction of opiates

23 NMDA antagonists Guidelines on the Management of Postoperative Pain Recommends clinicians consider ketamine as a component of multimodal therapy Particularly useful in patients with difficulty titrating opioids because of a high opioid tolerance Recommended dosing Preoperative bolus 0.5 mg/kg Intraoperative drip 10 ug/kg/min
24 Central calcium receptors Gabapentin, Pregabalin Gaba-receptors; Anticonvulsants Gabapentin/Pregabalin Pre and post operative reduction in opiates Major and minor surgeries Higher doses of medication are more effective mg gabapentin mg pregabalin Adverse effects: dizziness, dose reduction in impaired renal function. Limited evidence in children

25 Central calcium receptors Guidelines on the Management of Postoperative Pain Recommends clinicians consider gabapentin or pregabalin as a component of multimodal therapy
26 Alpha-2 central agonists Clonidine and Dexmedetomidine Central and peripheral nervous system Prolongs local anesthetic action Adverse effects: myocardial ischemia, decreased cardiac output, decreased peripheral vascular resistance, bradycardia, orthostatic hypotension, rebound hypertension on withdrawal Clonidine ½ life 8 hours Dexmetomdine ½ life 2 hours No respiratory depression Decreased need of opiates Preserves arousability Neuroprotective Dosing Load 1 mcg/kg over 10 mins, then mcg/kg/hr

27 Alpha-2 central agonists Guidelines on the Management of Postoperative Pain Clinicians should consider the addition of clonidine as an adjuvant for prolongation of analgesia with a single-injection peripheral neural blockade. Might prolong the duration of analgesia and potentially reduce the need for a continuous infusion.
28 Sodium channel antagonist Lidocaine (IV) ½ life min. Stabilizes the open state of the sodium channel - deactivation Analgesic, anti-hyperalgesic, and anti-inflammatory Shorter duration of ileus and better quality of analgesia Decreased need for opioids Adverse effects: drowsiness, headaches, confusion, numb tongue, arrhythmia, seizure, respiratory distress, cardiovascular arrest At low doses no major adverse events recorded Administration as a bolus of 1.5mg/kg then infusion of mg/kg/hr
29 Sodium channel antagonist Guidelines on the Management of Postoperative Pain Clinicians should consider i.v. lidocaine infusions in adults who undergo open and laparoscopic abdominal surgery who do not have contraindications Contraindications: heart block, hypotension, bradycardia
30 Local Anesthesia Lidocaine, bupivacaine, liposomal bupivacaine Subcutaneous or intraarticular infiltration at surgical site Lidocaine 4 mg/kg; 7mg/kg with epi Bupivacaine 2.5 mg/kg Liposomal bupivacaine max dose 266mg Don t use more than 50% if administering with bupivacaine Works for 72 hours No benefit to 50/50 mixture compared to independent use. Topical Lidocaine patches

31 Local Anesthesia Guidelines on the Management of Postoperative Pain Consider surgical site specific local anesthetic infiltration for surgical procedures. Does not recommend intrapleural analgesia with local anesthetics for pain control after thoracic surgery. Recommends that clinicians use topical local anesthetics in combination with nerve blocks before circumcision

32 Regional/Neuraxial Nerve blocks, Epidural, Intrathecal Decreased postoperative pain scores Decreased opioid use Decreased postoperative mortality Decreased VTE, MI, pneumonia, ileus, respiratory depression Epidural continuous or PCA with local anesthetic Optimal for mutliple rib fractures Spinal single dose of opioid Paravertebral block Transversus abdominis plane (TAP) block


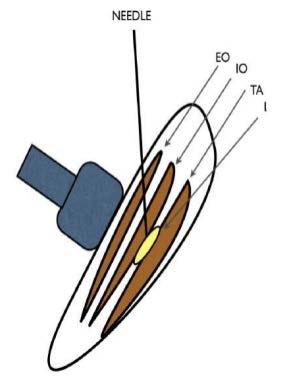
33 Site specific regional blocks
34 Regional/Neuraxial Guidelines on the Management of Postoperative Pain Surgical site specific local anesthetic based peripheral regional Thoracotomy, lower extremity joint surgery, shoulder surgery, cesarean section, hemorrhoid surgery, circumcision Clonidine as an adjuvant for prolongation of analgesia Neuraxial analgesia for major thoracic and abdominal procedures Cardiac complications, pulmonary complications, or prolonged ileus Avoid neuroaxial administration of magnesium, benzos, neostigmine, tramadol, ketamine - no clear benefit
, Robaxin")

35 Muscle relaxants & Benzos? Ativan, klonipin, xanax, valium Flexeril (cyclobenzaprine), Robaxin (Methocarbamol), Baclofen Gaba-receptors No clear evidence to suggest benefit for treatment of acute post-operative pain Still used by many experts as adjuncts to multimodal therapy
36 Regimens Neuraxial anesthetic treatment Epidural with local anesthetic (+/- opioids) or intrathecal opioids Nonpharmacologic Cognitive modalities, TENS
37 Regimens
38 Step up approach Recognizing pain Removing or modifying the cause Non-pharmacologic therapies (reassurance, position change, ice packs) Pharmacologic therapies NSAIDS, acetaminophen Opiates (weak to strong) Adjuncts (gabapentin, pregabalin, flexeril, baclofen) Regional/Neuroaxial blocks Pain experts
39 The addicted patient Tolerance -> Dependence -> Addiction May require increased doses of analgesia Look for signs of withdrawal of opiates Nausea, vomiting, diaphoresis, abdominal cramps, convulsions Opiate withdrawal symptoms can be suppressed with clonidine and dexmetomidine Methadone should be restarted as soon as possible Alternatives to opiates in former drug addicts - relapse

40 ICU pain management Assess pain 4 times per shift Treat and assess within 30 mins Validated scores not vitals Pain meds before procedure wait for effect! Daily sedation breaks Early mobilization
41 ICU pain/sedation Benzos increase LOS and duration on mechanical ventilation Independent risk factor for delirium Dexmetomadine/Propofol less delirium Remifentanil shorted duration to extubation, better neurologic evaluation Ketamine minimal hemodynamic effects; decreased volume resuscitation in TBI patients Regional/Neuroaxial blocks


42 Questions?
43 Question The maximum safe dose of local anesthetic administered subcutaneously in a 70 kg man A ml of 1% bupivacaine B ml of 1% lidocaine C ml of 1% lidocaine without epinephrine D ml of 1% lidocaine with epinephrine E ml of 2% lidocaine with epinephrine
44 Question The maximum safe dose of local anesthetic administered subcutaneously in a 70 kg man A ml of 1% bupivacaine B ml of 1% lidocaine C ml of 1% lidocaine without epinephrine D ml of 1% lidocaine with epinephrine E ml of 2% lidocaine with epinephrine
45 Question Which of the following is true concerning PCA? A. satisfactory pain relief is provided with administration of low dose narcotics B. Technique cannot be used in the semiconscious or uncooperative patient C. PCA is as safe as IM administration D. Excessive administration of narcotics can be limited with a lockout duration E. All of the above
46 Question Which of the following is true concerning PCA? A. satisfactory pain relief is provided with administration of low dose narcotics B. Technique cannot be used in the semiconscious or uncooperative patient C. PCA is as safe as IM administration D. Excessive administration of narcotics can be limited with a lockout duration E. All of the above
47 Question 63 yo male undergoes elective colon resection for adenocarcinoma found in a polyp. His home meds include NSAIDs and H2 blockers. A continuous infusion epidural supplemented by general anesthesia are used during the case. Two days later he has headache, stiff neck, and fever to Which of the following is true A. Hydration and bed rest are curative B. Vasodilators are needed to relieve spasm of the anterior spinal artery C. Exam of the CSF fluid is warranted D NSAIDs are probably contributing to the complication E. Injection of a blood patch into the epidural space will alleviate the symptoms
48 Question 63 yo male undergoes elective colon resection for adenocarcinoma found in a polyp. His home meds include NSAIDs and H2 blockers. A continuous infusion epidural supplemented by general anesthesia are used during the case. Two days later he has headache, stiff neck, and fever to Which of the following is true A. Hydration and bed rest are curative B. Vasodilators are needed to relieve spasm of the anterior spinal artery C. Exam of the CSF fluid is warranted D NSAIDs are probably contributing to the complication E. Injection of a blood patch into the epidural space will alleviate the symptoms
Current evidence in acute pain management. Jeremy Cashman
 Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Current evidence in acute pain management Jeremy Cashman Optimal analgesia Best possible pain relief Lowest incidence of side effects Optimal analgesia Best possible pain relief Lowest incidence of side
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Objectives 9/7/2012. Optimizing Analgesia to Enhance the Recovery After Surgery CME FACULTY DISCLOSURE
 Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Optimizing Analgesia to Enhance the Recovery After Surgery Francesco Carli, M.D.. McGill University, Montreal, QC, Canada. ASPMN, Baltimore, 2012 CME FACULTY DISCLOSURE Francesco Carli has no affiliation
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons. Karol A Gutowski, MD, FACS
 Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Nerve Blocks & Long Acting Analgesia for Plastic Surgeons Karol A Gutowski, MD, FACS Disclosures None related to this topic Why is Non-Opioid Analgesia Important Opioid epidemic Less opioid use Less PONV
Anesthesia for OutPatient Spine Surgery. Michael A. Kellams, D.O.
 Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Anesthesia for OutPatient Spine Surgery Michael A. Kellams, D.O. DISCLOSURE None! Hot Topics 2017 -Multimodal Analgesia/ERAS -TAP block -Inpatient procedures outpatient (Fusions) Multimodal Analgesia -Using
Perioperative Pain Management
 Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Perioperative Pain Management Overview and Update As defined by the Anesthesiologist's Task Force on Acute Pain Management are from the practice guidelines from the American Society of Anesthesiologists
Innovative Pain Management Practices in Spine Surgery Patients
 Disclosures Innovative Pain Management Practices in Spine Surgery Patients There are no conflicts of interest or relevant financial interests in making this presentation. Matt Kresl PharmD, BCPS Pharmacist
Disclosures Innovative Pain Management Practices in Spine Surgery Patients There are no conflicts of interest or relevant financial interests in making this presentation. Matt Kresl PharmD, BCPS Pharmacist
Presentation objectives. Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient
 Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient Ewan McNicol PharmD, MS Presentation objectives Outline principles for management of acute pain, with focus on perioperative
Overcoming Acute Pain Management Hurdles in the Tertiary Setting The High Risk Patient Ewan McNicol PharmD, MS Presentation objectives Outline principles for management of acute pain, with focus on perioperative
ERAS: Enhanced Recovery After Surgery. Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland
 ERAS: Enhanced Recovery After Surgery Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland Overview History and basic principles of ERAS Review published
ERAS: Enhanced Recovery After Surgery Christopher L. Wu, M.D. Professor of Anesthesiology The Johns Hopkins University; Baltimore, Maryland Overview History and basic principles of ERAS Review published
Acute Pain Management in the Opioid Tolerant Patient. Objectives. Opioids. The participant will be able to define opioid tolerance
 Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Analgesia for ERAS programs. Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital
 Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
Analgesia for ERAS programs Dr Igor Lemech VMO Anaesthetist Wagga Wagga Base Hospital Disclosure I have received honoraria from Mundipharma and MSD The new Wagga Wagga Rural Referral Centre Scope Analgesic
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
5 th ERAS UK Conference. Advances in Pain Management. Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh
 5 th ERAS UK Conference Advances in Pain Management Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh Pre-op information Optimised organ function No nutritional
5 th ERAS UK Conference Advances in Pain Management Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh Pre-op information Optimised organ function No nutritional
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
Balanced Analgesia With NSAIDS and Coxibs. Raymond S. Sinatra MD, Ph.D
 Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital
 Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Management of Acute Pain in the Chronic Pain Patient. Eric Cannon, MD Mountain West Anesthesia December 1, 2017
 Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Management of Acute Pain in the Chronic Pain Patient Eric Cannon, MD Mountain West Anesthesia December 1, 2017 Objectives 1. Describe the unique challenges of managing acute pain episodes in patients being
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
The Pain of Pain: or Patience for Patients
 The pain of pain or: Patience for Patients Alan Bielsky Objectives Discuss mechanisms of acute on chronic pain Explain the practical use of multimodal analgesia Detail different regimens that may benefit
The pain of pain or: Patience for Patients Alan Bielsky Objectives Discuss mechanisms of acute on chronic pain Explain the practical use of multimodal analgesia Detail different regimens that may benefit
SEEING KETAMINE IN A NEW LIGHT
 SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
SEEING KETAMINE IN A NEW LIGHT BobbieJean Sweitzer, M.D., FACP Professor of Anesthesiology Director of Perioperative Medicine Northwestern University Bobbie.Sweitzer@northwestern.edu LEARNING OBJECTIVES
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
POST-OP MULTIMODAL PAIN MANAGEMENT. Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management
 POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Intravenous lidocaine infusions. Dr Ian McConachie FRCA FRCPC
 Intravenous lidocaine infusions Dr Ian McConachie FRCA FRCPC Thank the organisers for inviting me. No conflicts or disclosures Lidocaine 1 st amide local anesthetic Synthesized in 1943 by Lofgren in Sweden.
Intravenous lidocaine infusions Dr Ian McConachie FRCA FRCPC Thank the organisers for inviting me. No conflicts or disclosures Lidocaine 1 st amide local anesthetic Synthesized in 1943 by Lofgren in Sweden.
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
INTRAVENOUS LIDOCAINE INFUSIONS AND INTRALIPID RESCUE
 INTRAVENOUS LIDOCAINE INFUSIONS AND INTRALIPID RESCUE Acute Pain Service-LHSC VH and UH sites HISTORY Lidocaine and procaine used by IV infusion in the 1950s and 1960s for general analgesia Often continued
INTRAVENOUS LIDOCAINE INFUSIONS AND INTRALIPID RESCUE Acute Pain Service-LHSC VH and UH sites HISTORY Lidocaine and procaine used by IV infusion in the 1950s and 1960s for general analgesia Often continued
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
ICU Management of Minimally Invasive Cardiac Surgery
 ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
ICU Management of Minimally Invasive Cardiac Surgery Benjamin A. Kohl, MD, FCCM Chief of Critical Care, Aria-Jefferson Health Professor of Anesthesiology Thomas Jefferson University Sidney Kimmel Medical
MD (Anaesthesiology) Title (Plan of Thesis) (Session )
 Title (Plan of Thesis) (Session )") S.No. 1. COMPARATIVE STUDY OF CENTRAL VENOUS CANNULATION USING ULTRASOUND GUIDANCE VERSUS LANDMARK TECHNIQUE IN PAEDIATRIC CARDIAC PATIENT. 2. TO EVALUATE THE ABILITY OF SVV OBTAINED BY VIGILEO-FLO TRAC
S.No. 1. COMPARATIVE STUDY OF CENTRAL VENOUS CANNULATION USING ULTRASOUND GUIDANCE VERSUS LANDMARK TECHNIQUE IN PAEDIATRIC CARDIAC PATIENT. 2. TO EVALUATE THE ABILITY OF SVV OBTAINED BY VIGILEO-FLO TRAC
Drugs Used In Management Of Pain. Dr. Aliah Alshanwani
 Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
The Fifth Vital Sign.
 Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT
 CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT Alicia Z Karas DVM, DACVA Cummings School of Veterinary Medicine, Tufts University, North Grafton, MA There are a number of factors that make cats different
CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT Alicia Z Karas DVM, DACVA Cummings School of Veterinary Medicine, Tufts University, North Grafton, MA There are a number of factors that make cats different
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006.
 Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Frederic J., Gerges MD. Ghassan E. Kanazi MD., Sama, I. Jabbour-Khoury MD. Review article from Journal of clinical anesthesia 2006 Introduction Laparoscopic surgery started in the mid 1950s. In recent
Inpatient Management of Trauma Related Pain
 Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Complex Acute Surgical Pain Management. Thomas Baribeault MSN, CRNA
 Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient Introduction
Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient Introduction
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline
 Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Opioid Free Anesthesia
 Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN 1 Why is pain important? Primary contributor to post-operative distress 56% of patients state that
Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN Opioid Free Anesthesia Michael H Wilhelm, CRNA, APRN 1 Why is pain important? Primary contributor to post-operative distress 56% of patients state that
Appendix A: Pharmacologic approaches to pain management during MVA
 Pain medication Though the medications shown below are commonly used for pain management during uterine evacuation, many other options exist. This table does not cover general anesthetic agents. Both anxiolytics
Pain medication Though the medications shown below are commonly used for pain management during uterine evacuation, many other options exist. This table does not cover general anesthetic agents. Both anxiolytics
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Baclofen is a GABA-agonist, although its exact mechanism of action remains uncertain. It is known to reduce release of excitatory neurotransmitters.
 Muscle relaxants may be needed, including benzodiazepines such as diazepam (Valium). For increased muscle tone (spasticity) Baclofen (Lioresal?) is a useful drug. Baclofen is a GABA-agonist, although its
Muscle relaxants may be needed, including benzodiazepines such as diazepam (Valium). For increased muscle tone (spasticity) Baclofen (Lioresal?) is a useful drug. Baclofen is a GABA-agonist, although its
Opioid reduction strategies in an academic tertiary medical center
 Opioid reduction strategies in an academic tertiary medical center Terry Bosen, PharmD Medication Safety Program Director Vanderbilt University Medical Center Tennessee MME data per capita MME = Morphine
Opioid reduction strategies in an academic tertiary medical center Terry Bosen, PharmD Medication Safety Program Director Vanderbilt University Medical Center Tennessee MME data per capita MME = Morphine
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Navigating the Waters of Acute Postoperative Pain
 Navigating the Waters of Acute Postoperative Pain ASPMN 28 th Annual Conference Susan Pendergrass MSN, MEd, FNP-BC Conflict of Interest Disclosure Author/Speaker: Susan Pendergrass, no conflict of interest
Navigating the Waters of Acute Postoperative Pain ASPMN 28 th Annual Conference Susan Pendergrass MSN, MEd, FNP-BC Conflict of Interest Disclosure Author/Speaker: Susan Pendergrass, no conflict of interest
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Labor Epidural: Local Anesthetics and Beyond
 Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
Goals: Labor Epidural: Local Anesthetics and Beyond Pedram Aleshi MD The Changing Practice of Anesthesia September 2012 Review Concept of MLAC Local anesthetic efficacy Local anesthetic sparing effects:
EXPAREL. An Innovative Non-Opioid Option for the Management of Postsurgical Pain. Presenter s Name Affiliation Date
 EXPAREL An Innovative Non-Opioid Option for the Management of Postsurgical Pain Presenter s Name Affiliation Date Disclosures The speaker has a consulting relationship with Pacira Pharmaceuticals, Inc.
EXPAREL An Innovative Non-Opioid Option for the Management of Postsurgical Pain Presenter s Name Affiliation Date Disclosures The speaker has a consulting relationship with Pacira Pharmaceuticals, Inc.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for geriatric surgical patients, 569 570 Acute kidney injury, critical care issues in geriatric patients with, 555 556
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
PAIN. Physiology of pain relating to pain management
 PAIN Physiology of pain relating to pain management What is pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. (Melzac and Wall) The generation of pain
PAIN Physiology of pain relating to pain management What is pain? An unpleasant sensory and emotional experience associated with actual or potential tissue damage. (Melzac and Wall) The generation of pain
Multimodal perioperative pain management protocols
 Multimodal perioperative pain management protocols Nader M. Hebela, MD كليفالند كلينك أبوظبي Dhabi Cleveland Clinic Abu معهد األعصاب Institute Neurological slide count: 30 January 2016 title slide explained
Multimodal perioperative pain management protocols Nader M. Hebela, MD كليفالند كلينك أبوظبي Dhabi Cleveland Clinic Abu معهد األعصاب Institute Neurological slide count: 30 January 2016 title slide explained
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Fast Track Surgery and Surgical Carepath in Optimising Colorectal Surgery R Sim Centre for Advanced Laparoscopic Surgery, TTSH Conventional Surgery Postop care Nasogastric tube Enteral feeds when ileus
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4
![OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4](/thumbs/90/104143670.jpg "OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4") Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Effective Postoperative Pain Management for Children. Nancy L. Glass, MD, MBA,
 Effective Postoperative Pain Management for Children Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Effective Postoperative Pain Management for Children Nancy L. Glass, MD, MBA, FAAP nglass@bcm.edu @DrNancyGlass1 None Disclosures Learning Objectives At the end of this presentation, participants will
Sedation For Cardiac Procedures A Review of
 Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Sedation For Cardiac Procedures A Review of Sedative Agents Dr Simon Chan Consultant Anaesthesiologist Department of Anaesthesia and Intensive Care Prince of Wales Hospital Hong Kong 21 February 2009 Aims
Pharmacology. Definitions. Pharmacology Definitions 8/20/2013. Drug:
 Pharmacology Medications and their potential implications in physical therapy Definitions Drug: Any substance that alters physiologic function in the organism, regardless of whether the effect is beneficial
Pharmacology Medications and their potential implications in physical therapy Definitions Drug: Any substance that alters physiologic function in the organism, regardless of whether the effect is beneficial
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
GUIDELINEs ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINEs ON PAIN MANAGEMENT IN UROLOGY (Text update March 2009) P. ader (chair), D. Echtle, V. Fonteyne, G. De Meerleer, E.G. Papaioannou, J.H. Vranken General principles of cancer pain management The
GUIDELINEs ON PAIN MANAGEMENT IN UROLOGY (Text update March 2009) P. ader (chair), D. Echtle, V. Fonteyne, G. De Meerleer, E.G. Papaioannou, J.H. Vranken General principles of cancer pain management The
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
STARTER PACK: Webinar #1 ADE4 - OPIOIDS
 STARTER PACK: Webinar #1 ADE4 - OPIOIDS Welcome to the Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps
STARTER PACK: Webinar #1 ADE4 - OPIOIDS Welcome to the Starter Pack Webinar #1 Why this is important Establishing a Team Best practices Understanding the Measures Completing a gap analysis First Steps
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Use of PCA devices in Difficult Populations
 Use of PCA devices in Difficult Populations Diane M. Santangelo MS RN ANP-C Stony Brook University Medical Center Acute Pain Service September 10, 2011 1 PCA technology? Why Bother? Costly Nurses complain:
Use of PCA devices in Difficult Populations Diane M. Santangelo MS RN ANP-C Stony Brook University Medical Center Acute Pain Service September 10, 2011 1 PCA technology? Why Bother? Costly Nurses complain:
What do we want for pain medications?
 New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
R Sim, D Cheong, KS Wong, B Lee, QY Liew Tan Tock Seng Hospital Singapore
 Prospective randomized, double-blind, placebo-controlled study of pre- and postoperative administration of a COX-2- specific inhibitor as opioid-sparing analgesia in major colorectal resections R Sim,
Prospective randomized, double-blind, placebo-controlled study of pre- and postoperative administration of a COX-2- specific inhibitor as opioid-sparing analgesia in major colorectal resections R Sim,
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014
 Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Source of pain relievers for nonmedical use among users 12 years or older:
 ACUTE PAIN MANAGEMENT OF THE OPIOID TOLERANT TRAUMA PATIENT James D. Colson, MS, MD Department of Anesthesiology WVU Hospitals Learning Objectives Identify criteria pertaining to the opioid-tolerant patient;
ACUTE PAIN MANAGEMENT OF THE OPIOID TOLERANT TRAUMA PATIENT James D. Colson, MS, MD Department of Anesthesiology WVU Hospitals Learning Objectives Identify criteria pertaining to the opioid-tolerant patient;
As laparoscopic surgeries are gaining popularity, Original Article. Maharjan SK 1, Shrestha S 2 1. Introduction
 , Vol. 1, No. 1, Issue 1, Jul.-Sep., 2012 Original Article Maharjan SK 1, Shrestha S 2 1 Associate Professor, 2 Assistant Professor, Department of Anaesthesiology and Intensive Care Kathmandu Medical College,
, Vol. 1, No. 1, Issue 1, Jul.-Sep., 2012 Original Article Maharjan SK 1, Shrestha S 2 1 Associate Professor, 2 Assistant Professor, Department of Anaesthesiology and Intensive Care Kathmandu Medical College,
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pain Management in the Surgical Patient. Peter Vogel, VMD, DACVS
 Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone
Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone
Prevention and Treatment Patrick Levelle, MD
 Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Prevention and Treatment Patrick Levelle, MD LOCAL ANESTHETIC TOXICITY 1. PERIPHERAL NERVE BLOCKS 2. ROLE OF THE PERIANESTHESIA RN 3. LOCAL ANESTHETIC TOXICITY Use of Lipid Emulsion Regional and Peripheral
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Clinical Staff Executive Committee MEDICAL CENTER POLICY NO A. SUBJECT: Pediatric Pain Assessment and Management
 Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0318 A. SUBJECT: Pediatric Pain Assessment and Management B. EFFECTIVE DATE: April 1, 2014 This policy applies to all neonatal and pediatric
Clinical Staff Executive Committee MEDICAL CENTER POLICY NO. 0318 A. SUBJECT: Pediatric Pain Assessment and Management B. EFFECTIVE DATE: April 1, 2014 This policy applies to all neonatal and pediatric
RECENT ADVANCES IN ANALGESIA
 4th ERAS UK Conference RECENT ADVANCES IN ANALGESIA Dr William J Fawcett Royal Surrey County Hospital, Guildford University of Surrey, Guildford November 14th 2014 Conflict of interests Paid honoraria
4th ERAS UK Conference RECENT ADVANCES IN ANALGESIA Dr William J Fawcett Royal Surrey County Hospital, Guildford University of Surrey, Guildford November 14th 2014 Conflict of interests Paid honoraria
The Role of Ketamine in the Management of Complex Acute Pain
 The Role of Ketamine in the Management of Complex Acute Pain Dr James Bennett Consultant Anaesthetist Consultant Lead for Inpatient Pain Service East Sussex Healthcare NHS Trust STAPG Committee Member
The Role of Ketamine in the Management of Complex Acute Pain Dr James Bennett Consultant Anaesthetist Consultant Lead for Inpatient Pain Service East Sussex Healthcare NHS Trust STAPG Committee Member