Jeff Gould, LAc, DiplAc, DiplCH. Johns Hopkins Integrative Medicine and Digestive Center. Blending Traditional Healing with Modern Biomedicine
|
|
|
- Jessica Booker
- 6 years ago
- Views:
Transcription


1 Jeff Gould, LAc, DiplAc, DiplCH Johns Hopkins Integrative Medicine and Digestive Center Blending Traditional Healing with Modern Biomedicine
2 Fire = inflammation, heat, burning sensations, bloody stools, rapid bowel transit Dampness = borborygmus, tenesmus, gas, bloating, diarrhea, mucus, yeast infections Wind = migraines, tremors, itching and dermatological conditions, external infections


3 Chinese Dietary Therapy Looks at the energetics of food vs. essential vitamins, minerals and other nutrients. Uses food to promote health but ALSO to treat illness. Designs meals using the 5 flavors: sweet, sour, acrid, bitter, and salty, to build and circulate energy.
4
5 How some foods and other substances can exacerbate your symptoms: Foods that may increase fire and exacerbate inflammation, e.g., coffee, soda, overly spicy foods, alcohol, smoking cigarettes, and marijuana Foods that may increase cold and decrease your ability to digest efficiently, like ice cold beverages Foods that may increase dampness and produce excess gas or to which you may have a sensitivity, e.g., gluten, dairy, cruciferous vegetables, and legumes

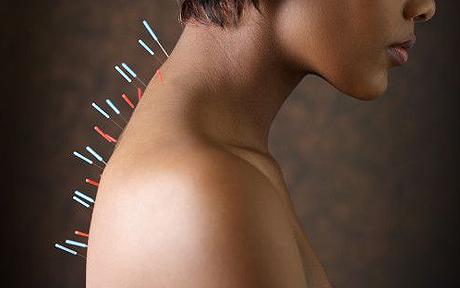
6 Acupuncture The insertion of tiny, filiform needles at specific points on the body to promote health and treat specific illnesses. The treatment may include electroacupuncture.
7 Goals of Acupuncture in Trea=ng IBD Cool heat and drain fire: reduce inflammation, slow bowel transit time to improve absorption of nutrients, decrease GERD if present Warm the physiological fire and expel cold: improve normal digestion Consolidate the stool: reduce diarrhea Drain dampness: reduce gas, bloating, distention, tenesmus

8 Powering Up! Where the mind goes, the Qi follows
9 Acupuncture Demonstra=on

10 Chinese Herbal Medicine Herbs may often be safely used in conjunction with drugs. The whole herb is used, not a concentrated or isolated active ingredient, leading to fewer side- effects. Formulas can be tailor- made to address a patient s unique constellation of symptoms and modified each day or week as symptoms change.
11 Examples of Individual Herbs with a Diges=ve Func=on Ginger and pinellia to treat nausea and vomiting Tangerine peel and cardamom for gas and bloating Rhubarb root and hemp seed for constipation Coptis and gardenia seed for reflux White peony for abdominal and other muscle cramping Turmeric for abdominal pain and inflammation Coix and white atractylodis for diarrhea
12 Diagnosing IBD: Differen=a=on of Syndromes Identify the full constellation of signs and symptoms This includes digestive s/s as well as those not generally considered to be digestive in nature
13 A Pa=ent Presents with a Diagnosis of IBD Dietary history, both from the Western perspective of micronutrients and the Chinese perspective of the energetics of food Digestion: appetite, taste of foods, presence of gas, bloating or distention, presence of reflux, nausea, or vomiting, cravings, any unusual tastes in the mouth Bowel Movements: diarrhea, constipation, frequency, urgency, presence of mucus, undigested food, or blood in the stools, sludginess of the stool, do you feel better or worse after a bowel movement?
14 A Pa=ent Presents with a Diagnosis of IBD cont. PLUS The Ten Questions : Presence of headaches or dizziness Visual issues, e.g., redness, dryness, floaters, etc. Cognitive symptoms, such as decreased mental clarity Lung issues, such as excess production of mucus, shortness of breath, and seasonal allergies, skin conditions Sleep patterns Presence of different types of fever or unusual sweating patterns
15 A Pa=ent Presents with a Diagnosis of IBD cont. Overall energy, better or worse with activity Abnormal menstrual patterns Abnormal bleeding or bruising patterns Predominant emotions Effects on libido and sexual health issues The tongue The pulse




16
17 Based on the differen=a=on of syndromes as determined by all these gathered data, we generate a treatment protocol, which may include dietary changes, acupuncture, an herbal formula, and nutri=onal supplements.
18 Ex. Biomedical Diagnosis of Moderate Ulcera=ve Coli=s Involvement of more than the distal colon Inflammation process extending to at least the splenic flexure Frequent, loose, bloody stools (up to 10 per day) Mild anemia not requiring blood transfusions Abdominal pain that is not severe Low grade fever Adequate nutrition is usually maintained
19 Chinese Medicine Differen=a=on Damp Accumula=on with Spleen Deficiency All the digestive information provided by the biomedical diagnosis, including: Incessant diarrhea with stool that is watery or sticky with pus, mucus, and or blood. Dull pain and distention in the abdomen. Malabsorption and malnutrition are common. Epigastric fullness and discomfort after eating. Decreased sense of taste, poor appetite, and lack of thirst
20 Chinese Medicine Differen=a=on Damp Accumula=on with Spleen Deficiency cont. PLUS Fatigue and lack of vitality Lower than normal libido, possible ED in men and orgasmic problems in women Shortness of breath, excess mucus production Disturbed sleep, unusual dreams Sallow complexion Short term memory problems and lack of clarity of thought
21 Chinese Medicine Differen=a=on Damp Accumula=on with Spleen Deficiency cont. Irregular menstrual cycle Possible presence of skin conditions, including weepy rashes Unusual sweating patterns, e.g., head, chest, groin Flat or suppressed affect Flabby or large tongue with teeth marks and thin or thick white coat Weak and thready pulses
22 Treatment Protocol Dietary 1. Decrease consumption of heat- producing products, e.g., coffee, soda, alcohol, marijuana, and spicy foods 2. Decrease consumption of damp- producing foods, e.g., fewer grains, dairy, sugar, and candy 3. Consider possibility of food sensitivities Acupuncture 1. Select points that clear heat, reduce dampness, strengthen digestive function, and consolidate the stool, e.g., SP- 9, LV- 2, GB- 34, ST- 36, SP- 8, ST- 25
23 Herbal - Shen ling bai zhu san Ginseng, Poria, and Atractylodes Macrocephala Powder Radix Ginseng/ren shen Rhizoma Atractylodis Macrocephalae/bai zhu Sclerotium Poriae Cocos/fu ling Honey- fried Radix Glycyrrhizae Uralensis/zhi gan cao Radix Dioscoreae Oppositae/shan yao Semen Dolichoris Lablab/bai bian dou Semen Nelumbinis Nuciferae/lian zi Semen Coicis Lachryma- jobi/yi yi ren Fructus Amomi/sha ren Radix Platycodi Grandiflori/jie geng

24 Joos, S, Brinkhaus, B, Maluche, C, Maupai, N, Kohnen, R, et al. Digestion, 2004; 69:
25 Methods: Prospective, randomized, controlled, single- blind clinical trial Primary outcome measure: changes in the CD activity index (CDAI) after treatment and assessment of entering remission (CDAI score 150 points) Secondary outcome measures: Changes in quality of life (IBDQ) and general well- being (VAS) Changes in serum markers of inflammation (α₁- acid glycoprotein and C- reactive protein) 51 patients with mild to moderately active CD (true acupuncture n =27, sham acupuncture control n= 24) received 10 treatments over 4 weeks with a 12 week followup
26 Results: True acupuncture CDAI decreased significantly from 250 ± 51 to 163 ± 56 points, which remained stable in the 12 week followup. Remission occurred in 11 patients, near remission in 4 (CDAI between ) Sham acupuncture group CDAI decreased from 220 ± 42 to 181 ± 46 points, considerable, but less superior. Remission occurred in 8 patients Both groups reported improvements in quality of life and general well- being, no significant difference between groups α₁- acid glycoprotein concentration fell significantly only in the true acupuncture group after 4 weeks No significant changes in C- reactive protein
27 Conclusions: Apart from a marked placebo effect, traditional acupuncture offers an additional therapeutic benefit in patients with mild to moderately active CD
28 Acupuncture and Moxibus=on in the Treatment of Ac=ve Crohn s Disease: A Randomized Controlled Study Strengths of the Study Randomized, controlled, single- blind Both objective and validated subjective measures utilized Diagnosis confirmed by endoscopic biopsy within 2 years of participation Clear inclusion/exclusion criteria 12 week followup Weaknesses of the Study Comparison problems with sham acupuncture not inert All true acupuncture patients received the same core points, but each also received additional points based on differentiation Some patients received an additional therapy, moxa Not replicable as performed
Patient Intake Form for Acupuncture Treatment at Infinite Healing
 Section A: Your Information Patient Intake Form for Acupuncture Treatment at Infinite Healing Last Name: First Name: Middle Initial: Mailing Address: _ City: Postal Code: E-mail: Birth date: M D YR Age:
Section A: Your Information Patient Intake Form for Acupuncture Treatment at Infinite Healing Last Name: First Name: Middle Initial: Mailing Address: _ City: Postal Code: E-mail: Birth date: M D YR Age:
!!!! Traditional & Contemporary Acupuncture! 19 Golden Ave, Toronto ON! ! Gregory Cockerill, R.
 Traditional & Contemporary Acupuncture 19 Golden Ave, Toronto ON info@livehandacupuncture.com 416-899-3364 Gregory Cockerill, R.Ac First Name: Last Name: Birthdate: Gender: Female Male Address: Email:
Traditional & Contemporary Acupuncture 19 Golden Ave, Toronto ON info@livehandacupuncture.com 416-899-3364 Gregory Cockerill, R.Ac First Name: Last Name: Birthdate: Gender: Female Male Address: Email:
Course: Diagnostics II Date: Class #: 2
 Course: Diagnostics II Date: 10-03-07 Class #: 2 Eight principles cont d Know: what is true/what is false (true cold/false heat for example) Know yin deficiency symptoms Know exterior/interior dx. Note:
Course: Diagnostics II Date: 10-03-07 Class #: 2 Eight principles cont d Know: what is true/what is false (true cold/false heat for example) Know yin deficiency symptoms Know exterior/interior dx. Note:
Chinese Medicine Adult Intake Form. Name (Last, First): Home address: Phone: Emergency contact name & phone number: Relationship Status:
: Home address: Phone: Emergency contact name & phone number: Relationship Status:") Chinese Medicine Adult Intake Form Name (Last, First): Date of Birth: Occupation: Hours per week: Home address: Phone: Email: Preferred contact method (circle one): Phone / Email Emergency contact name
Chinese Medicine Adult Intake Form Name (Last, First): Date of Birth: Occupation: Hours per week: Home address: Phone: Email: Preferred contact method (circle one): Phone / Email Emergency contact name
Dang Gui Si Ni Tang Tangkuei Decoction for Frigid Extremities
 Dang Gui Si Ni Tang Tangkuei Decoction for Frigid Extremities D F E G ctions: Warms the channels, disperses cold, nourishes the xue, and unblocks the xue vessels. hief Deputy (a) Dang Gui (b) Gui Zhi (c)
Dang Gui Si Ni Tang Tangkuei Decoction for Frigid Extremities D F E G ctions: Warms the channels, disperses cold, nourishes the xue, and unblocks the xue vessels. hief Deputy (a) Dang Gui (b) Gui Zhi (c)
205 W Giaconda Way, Suite 135 Tucson, AZ, (520) Name: Birth date: Age: Today s Date:
 Name: Birth date: Age: Today s Date:") 205 W Giaconda Way, Suite 135 Tucson, AZ, 85704 (520) 219-2400 www.forever-able.com info@forever-able.com Name: Birth date: Age: Today s Date: Address: Email: Home phone: Mobile phone: May we add you to
205 W Giaconda Way, Suite 135 Tucson, AZ, 85704 (520) 219-2400 www.forever-able.com info@forever-able.com Name: Birth date: Age: Today s Date: Address: Email: Home phone: Mobile phone: May we add you to
ALIGN ACUPUNCTURE AND HERBS LLC Rebekah V. Michaels MAOM, Diplomate OM, Lic Ac
 ALIGN ACUPUNCTURE AND HERBS LLC Rebekah V. Michaels MAOM, Diplomate OM, Lic Ac. 617-835-2512 Patient Information and Health History Date: Name: Date of Birth: Street: City: State: Zip: Phone: (H) (W) )
ALIGN ACUPUNCTURE AND HERBS LLC Rebekah V. Michaels MAOM, Diplomate OM, Lic Ac. 617-835-2512 Patient Information and Health History Date: Name: Date of Birth: Street: City: State: Zip: Phone: (H) (W) )
Symptom Questionnaire
 Symptom Questionnaire The following questionnaire is a general assessment of your health developed by Dr Royal Lee D.D.S. Each grouping represents a particular area of your body that may be causing you
Symptom Questionnaire The following questionnaire is a general assessment of your health developed by Dr Royal Lee D.D.S. Each grouping represents a particular area of your body that may be causing you
ACUPUNCTURE SPECIFIC INTAKE FORM
 ACUPUNCTURE SPECIFIC INTAKE FORM A naturopathic approach to medicine is holistic and seeks to understand all factors that may be affecting your health. Please answer the following questions to the best
ACUPUNCTURE SPECIFIC INTAKE FORM A naturopathic approach to medicine is holistic and seeks to understand all factors that may be affecting your health. Please answer the following questions to the best
Emotional Relationships Social Life Sexually Recreation
 Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
Name Date Address City State Zip Married Single Partner Divorced Widowed Date of Birth SS# Email Work Phone Home Phone Cell Phone Occupation Referred by Emergency Contact Family Physician Contact May we
4-1 Dyspnea (Chuan, 喘 )
") 4-1 Dyspnea (Chuan, 喘 ) Concept Breathing with difficulty (open wide mouth, raise shoulders) Etiology and pathogenesis Climatic factors Phlegm fluid Emotion Chronic diseases Exertion Over sex Diagnosis
4-1 Dyspnea (Chuan, 喘 ) Concept Breathing with difficulty (open wide mouth, raise shoulders) Etiology and pathogenesis Climatic factors Phlegm fluid Emotion Chronic diseases Exertion Over sex Diagnosis
Qi & Blood Deficiency Signs. Qi & Blood Deficiency Signs. Weak voice and lack of desire to speak. Chinese Pathology of 10
 Qi & Blood Deficiency Signs Qi Deficiency Blood Deficiency Qi & Blood Deficiency Signs Qi Deficiency Pale bright complexion Shortness of breath Weakness/Exhaustion (Lassitude of spirit) Weak voice and
Qi & Blood Deficiency Signs Qi Deficiency Blood Deficiency Qi & Blood Deficiency Signs Qi Deficiency Pale bright complexion Shortness of breath Weakness/Exhaustion (Lassitude of spirit) Weak voice and
Traditional Chinese Medicine (TCM) Assessment Instructions
 Assessment Instructions") Traditional Chinese Medicine (TCM) Assessment Instructions This assessment form is designed to determine your current health condition according to Traditional Chinese Medicine (TCM). Each patient must
Traditional Chinese Medicine (TCM) Assessment Instructions This assessment form is designed to determine your current health condition according to Traditional Chinese Medicine (TCM). Each patient must
Medicated diet. Tonify the Qi
 Medicated diet Tonify the Qi 1. Ren shen ginseng root Properties: sweet, slightly bitter, slightly warm Channels entered: LU, SP a. Strongly tonifies the basal qi, Tonifies the lung and spleen qi. a. Benefits
Medicated diet Tonify the Qi 1. Ren shen ginseng root Properties: sweet, slightly bitter, slightly warm Channels entered: LU, SP a. Strongly tonifies the basal qi, Tonifies the lung and spleen qi. a. Benefits
Bridges Family Wellness PC. New Patient Intake. Bridges Family Wellness Intake Form SE Lake Rd, Suite 102 Milwaukie, OR
 New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
New Patient Intake Bridges Family Wellness Intake Form Full Name: * What is your birthdate? MM/DD/YYYY * What is your gender identity? * Home address: * Cell Phone * Other Phone number(s): Emergency Contact
Symptom Review (page 1) Name Date
 Name Date") v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
v2.4, 2/13 JonathanTreasure.com Botanical Medicine & Cancer Herb Drug Interactions Herbalism 3.0 Symptom Review (page 1) Name Date INSTRUCTIONS Please read each section below carefully and, after each
CONSULTATION & CONSENT FORMS p. 1 of 5
 CONSULTATION & CONSENT FORMS p. 1 of 5 ******************************************************************************** List your full name, age, sex, and today's date List your complete address List your
CONSULTATION & CONSENT FORMS p. 1 of 5 ******************************************************************************** List your full name, age, sex, and today's date List your complete address List your
ACUPUNCTURE FOR HEALTH WENDY STALKER R.Ac. Dip.Ac. B.Sc. Name: Date of Birth: Date:
 Name: Date of Birth: Date: Address: Postal Code: Occupation: Telephone: Day: Cell Phone: E-mail address: Emergency Contact: Evening: Telephone: Male Female Where did you hear about Acupuncture for Health?
Name: Date of Birth: Date: Address: Postal Code: Occupation: Telephone: Day: Cell Phone: E-mail address: Emergency Contact: Evening: Telephone: Male Female Where did you hear about Acupuncture for Health?
New Patient Medical History Intake Form
 New Patient Medical History Intake Form Name: Todays Date: / / Date of Birth: / / Age: Gender: M / F Marital Status: S M D W Address: City: State: Zip Code Primary Ph.# (cell, hm, wk) Email Address 2nd
New Patient Medical History Intake Form Name: Todays Date: / / Date of Birth: / / Age: Gender: M / F Marital Status: S M D W Address: City: State: Zip Code Primary Ph.# (cell, hm, wk) Email Address 2nd
PHYSIOTHERAPIST. Date of last visit MASSAGE THERAPIST. Date of last visit SPECIALISTS. Date of last visit WHAT ARE YOUR PRIMARY HEALTH CONCERNS?
 2 PHYSIOTHERAPIST Date of last visit MASSAGE THERAPIST Date of last visit SPECIALISTS Date of last visit WHAT ARE YOUR PRIMARY HEALTH CONCERNS? WHAT IS THE PRIMARY REASON YOU ARE SEEKING CONSULTATION/TREATMENT?
2 PHYSIOTHERAPIST Date of last visit MASSAGE THERAPIST Date of last visit SPECIALISTS Date of last visit WHAT ARE YOUR PRIMARY HEALTH CONCERNS? WHAT IS THE PRIMARY REASON YOU ARE SEEKING CONSULTATION/TREATMENT?
Shiatsu Intake Form PURCHASED PRODUCT/SERVICE. Date of Birth Age Height Weight. Home Address City State ZIP
 Shiatsu Intake Form DATE PURCHASED PRODUCT/SERVICE FIRST NAME LAST NAME Date of Birth Age Height Weight Home Address City State ZIP Home Phone Cell Phone Email Name of Emergency Contact Would you like
Shiatsu Intake Form DATE PURCHASED PRODUCT/SERVICE FIRST NAME LAST NAME Date of Birth Age Height Weight Home Address City State ZIP Home Phone Cell Phone Email Name of Emergency Contact Would you like
Digestion Assessment Scorecard
 Name Digestion Assessment Age Height Weight Based upon your health profile for the past 30 days, please select the appropriate number, from '0-3' on all questions (0 as least/never/no and 3 as most/always/yes).
Name Digestion Assessment Age Height Weight Based upon your health profile for the past 30 days, please select the appropriate number, from '0-3' on all questions (0 as least/never/no and 3 as most/always/yes).
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ Patient General Information
 Patient General Information Name: (first) (middle) (last) Date of Birth: / / (mo) (day) (year) 中 文名字 : Gender: Occupation: Address: (street, apt) Phone #: (city, state, zip code) Email: Emergency Contact:
Patient General Information Name: (first) (middle) (last) Date of Birth: / / (mo) (day) (year) 中 文名字 : Gender: Occupation: Address: (street, apt) Phone #: (city, state, zip code) Email: Emergency Contact:
Upper Jiao problem Pallor of face Qi/Yang/Blood Xu or Cold Can be excess, or Blood Deficiency
 Course: Diagnostics II Date: Dec 8, 2007 Combination Symptoms Combination Syndrome Symptom Caused by Qi Deficiency of Heart and Lung Palpitation Indicative of heart problem Cough with difficult inhalation,
Course: Diagnostics II Date: Dec 8, 2007 Combination Symptoms Combination Syndrome Symptom Caused by Qi Deficiency of Heart and Lung Palpitation Indicative of heart problem Cough with difficult inhalation,
(city) (State) (zip)
 (State) (zip)") ACUPUNCTURE PATIENT INTAKE FORM DATE: / / NAME: DATE OF BIRTH: / / AGE SEX: M F HEIGHT: WEIGHT: ADDRESS: (street) (city) (State) (zip) PHONE: / / (Home) (Work) (Cell) E-MAIL: EMERGENCY CONTACT: Name: Address:
ACUPUNCTURE PATIENT INTAKE FORM DATE: / / NAME: DATE OF BIRTH: / / AGE SEX: M F HEIGHT: WEIGHT: ADDRESS: (street) (city) (State) (zip) PHONE: / / (Home) (Work) (Cell) E-MAIL: EMERGENCY CONTACT: Name: Address:
METABOLIC ASSESSMENT FORM
 METABOLIC ASSESSMENT FORM Name: Age: Sex: Date: PART 1 Please list the 5 major health concerns in your order of importance: 1. 2. 3. 4. 5. PART 2 Please circle the appropriate number 0-3 on all questions
METABOLIC ASSESSMENT FORM Name: Age: Sex: Date: PART 1 Please list the 5 major health concerns in your order of importance: 1. 2. 3. 4. 5. PART 2 Please circle the appropriate number 0-3 on all questions
Caspian Acupuncture -- Health History Form Anita Tayyebi EAMP, LAc. 652 SW 150 th St Burien WA 98166
 Frist Name Last: Date Phone (H) (C) (W) E-mail Address City State Zip Age DOB Place of Birth _ Marital/Partnership Status Preferred Gender Pronoun _ Profession Family Physician Telephone # Referred By
Frist Name Last: Date Phone (H) (C) (W) E-mail Address City State Zip Age DOB Place of Birth _ Marital/Partnership Status Preferred Gender Pronoun _ Profession Family Physician Telephone # Referred By
NEW PATIENT HEALTH HISTORY
 NEW PATIENT HEALTH HISTORY Debra Joan Wood, Lic Ac, MAcOM Acupuncture and Herbs Please help me provide you with a complete evaluation by taking the time to fill out this questionnaire carefully. If there
NEW PATIENT HEALTH HISTORY Debra Joan Wood, Lic Ac, MAcOM Acupuncture and Herbs Please help me provide you with a complete evaluation by taking the time to fill out this questionnaire carefully. If there
Male Fertility Questionnaire
 Male Fertility Questionnaire Name (Last, First) Age Date Birth Date / / Address: City: State: Zip: Phone(cell) E-mail address: How did you hear about Presidio Acupuncture? Friend (who?) Internet MD/Midwife
Male Fertility Questionnaire Name (Last, First) Age Date Birth Date / / Address: City: State: Zip: Phone(cell) E-mail address: How did you hear about Presidio Acupuncture? Friend (who?) Internet MD/Midwife
Natalie Kilheeney L.Ac., Dipl. OM Licensed Acupuncturist & Herbalist
 *All information is important to your intake and valuable to your personal treatment plan. Please answer as thorough as possible. Patient Information: Name: Date: / / (First Middle Last) Address: City:
*All information is important to your intake and valuable to your personal treatment plan. Please answer as thorough as possible. Patient Information: Name: Date: / / (First Middle Last) Address: City:
CMHB221 Chinese Herbal Formulae
 CMHB221 Chinese Herbal Formulae Session Three Tonifying Chinese herbal formulae: Qi: o o o o o English name; Pin yin name and Chinese name Composition; dosage and administration Functions and indications
CMHB221 Chinese Herbal Formulae Session Three Tonifying Chinese herbal formulae: Qi: o o o o o English name; Pin yin name and Chinese name Composition; dosage and administration Functions and indications
Oriental Medicine Questionnaire
 Oriental Medicine Questionnaire Date: Name: DOB Sex: M F SS# Address: City State Zip Cell Phone: Home Phone: Business Phone Occupation: Height: Weight: Who referred you to this office? 1.What brought you
Oriental Medicine Questionnaire Date: Name: DOB Sex: M F SS# Address: City State Zip Cell Phone: Home Phone: Business Phone Occupation: Height: Weight: Who referred you to this office? 1.What brought you
CMCS121. Session 4. Interview Workshop/ Abdominal Pain. Chinese Medicine Department.
 CMCS121 Session 4 Interview Workshop/ Abdominal Pain Chinese Medicine Department www.endeavour.edu.au Abdominal Pain o Maciocia, p 145-147, o Pain, p 255-259, 735-745 o Digestive symptoms p 262, o Asking
CMCS121 Session 4 Interview Workshop/ Abdominal Pain Chinese Medicine Department www.endeavour.edu.au Abdominal Pain o Maciocia, p 145-147, o Pain, p 255-259, 735-745 o Digestive symptoms p 262, o Asking
HOW DID YOU HEAR ABOUT US?
 427 Bloomfield Ave. Ste. 306 Montclair, NJ 07042 Phone: 973-746- 2848 Fax: 973-746- 2088 HOW DID YOU HEAR ABOUT US? Eastern School of Acupuncture and Traditional Medicine Student Clinic Intake Form Intake
427 Bloomfield Ave. Ste. 306 Montclair, NJ 07042 Phone: 973-746- 2848 Fax: 973-746- 2088 HOW DID YOU HEAR ABOUT US? Eastern School of Acupuncture and Traditional Medicine Student Clinic Intake Form Intake
HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON
 HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON Indigestion is a condition that is often a symptom of another, underlying condition and is associated with various forms of discomfort in the stomach including
HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON Indigestion is a condition that is often a symptom of another, underlying condition and is associated with various forms of discomfort in the stomach including
Initial Questions Form
 Initial Questions Form 422 Broadway Denver CO 80203 (303)921-2993 Please answer as thoroughly as possible. This is detailed so that I can better understand what is going on with you as a whole person.
Initial Questions Form 422 Broadway Denver CO 80203 (303)921-2993 Please answer as thoroughly as possible. This is detailed so that I can better understand what is going on with you as a whole person.
DIFFERENTIAL QUESTIONS
 4 IMBALANCES AND 5 ORGANS A New System for Diagnosis and Treatment DIFFERENTIAL QUESTIONS Jeremy Ross www.jeremyross.com DIFFERENTIAL QUESTIONS A New System for Diagnosis 90 Organ syndromes In Chinese
4 IMBALANCES AND 5 ORGANS A New System for Diagnosis and Treatment DIFFERENTIAL QUESTIONS Jeremy Ross www.jeremyross.com DIFFERENTIAL QUESTIONS A New System for Diagnosis 90 Organ syndromes In Chinese
Lucas D. Brown, L.Ac. (312)
") Today s date: Mr. Miss Mrs. Ms. Dr. Birth date: (mm/dd/yy) Social Security Number: First name: Last name: Age: Email: Marital status: Single Divorced Married Separated Partner Widowed Street address: Apt:
Today s date: Mr. Miss Mrs. Ms. Dr. Birth date: (mm/dd/yy) Social Security Number: First name: Last name: Age: Email: Marital status: Single Divorced Married Separated Partner Widowed Street address: Apt:
What do you feel are your child s strengths at this time?
 PEDIATRIC MEDICAL QUESTIONNAIRE Our ability to draw effective conclusions about your present state of health and how to improve it depends, to a significant extent, on your ability to respond thoughtfully
PEDIATRIC MEDICAL QUESTIONNAIRE Our ability to draw effective conclusions about your present state of health and how to improve it depends, to a significant extent, on your ability to respond thoughtfully
Nivolumab. Other Names: Opdivo. About this Drug. Possible Side Effects (More Common) Warnings and Precautions
 Warnings and Precautions") Nivolumab Other Names: Opdivo About this Drug Nivolumab is used to treat cancer. It is given in the vein (IV). Possible Side Effects (More Common) Bone marrow depression. This is a decrease in the number
Nivolumab Other Names: Opdivo About this Drug Nivolumab is used to treat cancer. It is given in the vein (IV). Possible Side Effects (More Common) Bone marrow depression. This is a decrease in the number
1. Have you ever had or now have: 2. Have you ever had or now have:
 1. Have you ever had or now have: 2. Have you ever had or now have: Yes No Please Check each item no blanks CARDIOVASCULAR Yes No Often Seldom 1. Chronic or frequent colds 1. Shortness of breath with normal
1. Have you ever had or now have: 2. Have you ever had or now have: Yes No Please Check each item no blanks CARDIOVASCULAR Yes No Often Seldom 1. Chronic or frequent colds 1. Shortness of breath with normal
Inner Balance Acupuncture
 Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Patient Information Inner Balance Acupuncture 274 Southland Drive, Suite 101, Lexington, KY 40503 859-595-2164 www.acupunctureky.com Name: Today s date: Age: Male Female Marital status: Date of Birth:
Used for exterior conditions such as common colds, fevers, and flu s. Many of these formulas induce sweating. This category can be subdivided into
 Section 1 Used for exterior conditions such as common colds, fevers, and flu s. Many of these formulas induce sweating. This category can be subdivided into formulas the release cold or heat. Traditionally
Section 1 Used for exterior conditions such as common colds, fevers, and flu s. Many of these formulas induce sweating. This category can be subdivided into formulas the release cold or heat. Traditionally
Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA
 Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA 98136 206.200.3595 Today s date Name Legal name (if different) Phone (primary) (secondary) Address City State Zip Email
Sound View Acupuncture and Chinese Herbs 5410 California Ave SW, #202, Seattle, WA 98136 206.200.3595 Today s date Name Legal name (if different) Phone (primary) (secondary) Address City State Zip Email
The Herbalist s Corner
 Acupuncture Today, July 2008 The Herbalist s Corner Jake Paul Fratkin, OMD. L.Ac. MANAGING A PATIENT WITH MULTIPLE COMPLAINTS A situation common to American herbalist/acupuncturists is the arrival of a
Acupuncture Today, July 2008 The Herbalist s Corner Jake Paul Fratkin, OMD. L.Ac. MANAGING A PATIENT WITH MULTIPLE COMPLAINTS A situation common to American herbalist/acupuncturists is the arrival of a
Patient Health History Questionnaire
 Patient Health History Questionnaire Manitou Springs Acupuncture Randall Johnson, L.Ac., LLC Certified Seitai Shinpo Acupuncturist License Number: Acu-0002072 Phone: (719) 237-4547 Email: 719acupuncture@gmail.com
Patient Health History Questionnaire Manitou Springs Acupuncture Randall Johnson, L.Ac., LLC Certified Seitai Shinpo Acupuncturist License Number: Acu-0002072 Phone: (719) 237-4547 Email: 719acupuncture@gmail.com
Personal Information
 Personal Information 1. Date: / / mm dd yy 2. Name: 3. Gender: M F 4. Date of Birth: / / mm dd yy 5. Marital Status: Single Married Divorce Widow 6. Do you have insurance? Y N 7. Patient's address: Address:
Personal Information 1. Date: / / mm dd yy 2. Name: 3. Gender: M F 4. Date of Birth: / / mm dd yy 5. Marital Status: Single Married Divorce Widow 6. Do you have insurance? Y N 7. Patient's address: Address:
Patient Intake Form. Relationship. Contact information
 Acupuncture & Massage Therapy 895 rue St. Francois, Florissant 314 921-3366 Mary S. Wallis, L.Ac, L.M.T. National Board Certified in Acupuncture (NCCAOM) MO License No. 2007002923 Patient Intake Form Today
Acupuncture & Massage Therapy 895 rue St. Francois, Florissant 314 921-3366 Mary S. Wallis, L.Ac, L.M.T. National Board Certified in Acupuncture (NCCAOM) MO License No. 2007002923 Patient Intake Form Today
Rebecca Shatles M.Ac, L.Ac Dipl.Ac, LMT
 Rebecca Shatles M.Ac, L.Ac Dipl.Ac, LMT 801 623 8253 1291 South 1100 East #202 Salt Lake City, UT 84105 www.peakacupunctureclinic.com info@peakacupunctureclinic.com CLIENT INFORMATION Client Name: If Patient
Rebecca Shatles M.Ac, L.Ac Dipl.Ac, LMT 801 623 8253 1291 South 1100 East #202 Salt Lake City, UT 84105 www.peakacupunctureclinic.com info@peakacupunctureclinic.com CLIENT INFORMATION Client Name: If Patient
Patient Contact Information
 Patient Contact Information Name: Date: Address: City, State & Zip: Primary Phone: Home Cell Work Alternative Phone: Home Cell Work E-mail Address: Preferred Method of Contact: Phone E-mail Would you like
Patient Contact Information Name: Date: Address: City, State & Zip: Primary Phone: Home Cell Work Alternative Phone: Home Cell Work E-mail Address: Preferred Method of Contact: Phone E-mail Would you like
American Health Acupuncture LLC Healing the Body, Mind, & Spirit 7130 N Omar Dr Tucson AZ (520)
") American Health Acupuncture LLC Healing the Body, Mind, & Spirit 7130 N Omar Dr Tucson AZ 85741 (520) 544-6603 Notes for new Patients: Your first session * Can you imagine not having to wait at a doctor's
American Health Acupuncture LLC Healing the Body, Mind, & Spirit 7130 N Omar Dr Tucson AZ 85741 (520) 544-6603 Notes for new Patients: Your first session * Can you imagine not having to wait at a doctor's
Methotrexate. About This Drug. Possible Side Effects. Warnings and Precautions
 Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Health History Questionnaire
 CLINICAL ACUPUNCTURE SERVICES Cathy D. Adelman, RN, LAc PO Box 91451 Tucson, AZ 85752-1451 (520) 822-6844 cdarnlac@hughes.net www.clinicalacupunctureservices.com Health History Questionnaire I. GENERAL
CLINICAL ACUPUNCTURE SERVICES Cathy D. Adelman, RN, LAc PO Box 91451 Tucson, AZ 85752-1451 (520) 822-6844 cdarnlac@hughes.net www.clinicalacupunctureservices.com Health History Questionnaire I. GENERAL
Trastuzumab (Herceptin )
") Trastuzumab (Herceptin ) About This Drug Trastuzumab is used to treat cancer. It is given in the vein (IV) Possible Side Effects Bone marrow depression. This is a decrease in the number of white blood
Trastuzumab (Herceptin ) About This Drug Trastuzumab is used to treat cancer. It is given in the vein (IV) Possible Side Effects Bone marrow depression. This is a decrease in the number of white blood
Course: Diagnostics I Date: August 14, 2007 Class #: 7. Drinking (pt of Q5)
") Course: Diagnostics I Date: August 14, 2007 Class #: 7 For quiz review the 10 trad questions, 16 questions. And more. 10 Traditional q s (cont d) Thirsty? Ask this first. Most important question. Drinking
Course: Diagnostics I Date: August 14, 2007 Class #: 7 For quiz review the 10 trad questions, 16 questions. And more. 10 Traditional q s (cont d) Thirsty? Ask this first. Most important question. Drinking
Essential Wellness Of Illinois, LLC Health History Questionnaire Christine A. Renz L.Ac., Dipl OM, MSTOM
 Name Date Address City State Zip Home Phone Cell Fax Email Emergency Contact Emergency Number Date of Birth Age Sex Height Weight Lbs Marital Status Occupation Who referred you to this office? Name of
Name Date Address City State Zip Home Phone Cell Fax Email Emergency Contact Emergency Number Date of Birth Age Sex Height Weight Lbs Marital Status Occupation Who referred you to this office? Name of
Headache Follow-up Visit Form
 !1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
!1 Headache Follow-up Visit Form We will be unable to see you unless this form is completely filled out. We appreciate your thoroughness. Name DOB Age Today s Date Referring doctor: Primary doctor: Neurologist:
Patient Health History for Fertility
 Patient Health History for Fertility Name: Date: Address: City, State, Zip code Phones: Home Work: Cell: Email address: Date of Birth: Age: Occupation: Emergency contact: Ob/Gyn: Current Medications: What
Patient Health History for Fertility Name: Date: Address: City, State, Zip code Phones: Home Work: Cell: Email address: Date of Birth: Age: Occupation: Emergency contact: Ob/Gyn: Current Medications: What
For the Patient: USMAVNIV
 For the Patient: USMAVNIV Other Names: Treatment of Unresectable or Metastatic Melanoma Using Nivolumab U = Undesignated (requires special approval) SM = Skin and Melanoma AV = AdVanced NIV = NIVolumab
For the Patient: USMAVNIV Other Names: Treatment of Unresectable or Metastatic Melanoma Using Nivolumab U = Undesignated (requires special approval) SM = Skin and Melanoma AV = AdVanced NIV = NIVolumab
POST GRADUATE DIPLOMA IN ACUPUNCTURE (PGDACP) Term-End Examination December, 2010 PGDACP-01 : BASIC THEORIES OF ACUPUNCTURE/TCM DIAGNOSIS
 Term-End Examination December, 2010 PGDACP-01 : BASIC THEORIES OF ACUPUNCTURE/TCM DIAGNOSIS") No. of Printed Pages : 11 PGDACP - 01 l POST GRADUATE DIPLOMA IN ACUPUNCTURE (PGDACP) 00061 Term-End Examination December, 2010 PGDACP-01 : BASIC THEORIES OF ACUPUNCTURE/TCM DIAGNOSIS Time : 2 Hours Maximum
No. of Printed Pages : 11 PGDACP - 01 l POST GRADUATE DIPLOMA IN ACUPUNCTURE (PGDACP) 00061 Term-End Examination December, 2010 PGDACP-01 : BASIC THEORIES OF ACUPUNCTURE/TCM DIAGNOSIS Time : 2 Hours Maximum
DIAGNOSIS YES NO. KIDNEY YIN DEFICIENTY (Ki Yi- -) Do you have lower back weakness, soreness, or pain, or knee problems?
 Do you have lower back weakness, soreness, or pain, or knee problems?") Answer yes or no to each of the following questions. Don t worry about what the symptoms mean; just note whether you experience them. If you have more than one--fourth to one--third yes re- sponses in
Answer yes or no to each of the following questions. Don t worry about what the symptoms mean; just note whether you experience them. If you have more than one--fourth to one--third yes re- sponses in
New Patient Intake. How did you hear about Presidio Acupuncture? Friend (who?) Emergency Contact: Relation: Phone #:
 Emergency Contact: Relation: Phone #:") New Patient Intake Name Age Date Birth Date / / Address: City: State: Zip: Phone(cell) E-mail address: How did you hear about Presidio Acupuncture? Friend (who?) Internet MD/Midwife Other Emergency Contact:
New Patient Intake Name Age Date Birth Date / / Address: City: State: Zip: Phone(cell) E-mail address: How did you hear about Presidio Acupuncture? Friend (who?) Internet MD/Midwife Other Emergency Contact:
Written by Laurence B. Palevsky, MD Friday, 01 December :00 - Last Updated Thursday, 26 February :42
 Infants and children are not simply small adults, especially when it comes to feeding and nourishing their little bodies. They are less able than adults to receive, transform and assimilate the nutrients
Infants and children are not simply small adults, especially when it comes to feeding and nourishing their little bodies. They are less able than adults to receive, transform and assimilate the nutrients
For the Patient: ULUAVPMB
 For the Patient: ULUAVPMB Other Names: Treatment of Advanced Non-Small Cell Lung Cancer Using Pembrolizumab U = Undesignated (requires special approval) LU = LUng AV = AdVanced PMB = PeMBrolizumab ABOUT
For the Patient: ULUAVPMB Other Names: Treatment of Advanced Non-Small Cell Lung Cancer Using Pembrolizumab U = Undesignated (requires special approval) LU = LUng AV = AdVanced PMB = PeMBrolizumab ABOUT
Patient Information. Marital Status (Single, Married, Life Partner, Divorced, Widowed) CHIEF COMPLAINT
 CHIEF COMPLAINT") Patient Information Name Date Home Address City State Zip Phone E-mail Address Cell Phone: Business Address City State Zip Phone Occupation Place of Birth Date of Birth Age Height Weight Soc. Sec. # Sex
Patient Information Name Date Home Address City State Zip Phone E-mail Address Cell Phone: Business Address City State Zip Phone Occupation Place of Birth Date of Birth Age Height Weight Soc. Sec. # Sex
At the outset, we want to clear up some terminology issues. IBS is COPYRIGHTED MATERIAL. What Is IBS?
 1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
1.0 Presenting complaint: Onset 1.1 When it started? 1.2 How did it start? Progress 1.3 Has the problem increased /decreased so far?
 Case history Sr. No. Name Sex M / F Age Marital Status B / S / M / W Occupation Date 1.0 Presenting complaint: Onset 1.1 When it started? 1.2 How did it start? Progress 1.3 Has the problem increased /decreased
Case history Sr. No. Name Sex M / F Age Marital Status B / S / M / W Occupation Date 1.0 Presenting complaint: Onset 1.1 When it started? 1.2 How did it start? Progress 1.3 Has the problem increased /decreased
Patient Information. Vibrant Health Acupuncture & Wellness Center, LLC 260 Gateway Drive, Suite 7B Bel Air, Maryland
 Patient Information Vibrant Health Acupuncture & Wellness Center, LLC 260 Gateway Drive, Suite 7B Bel Air, Maryland 21014 410-913-8322 Patient Name: Date of Birth: Age: Male: Female: Single: Married: Separated:
Patient Information Vibrant Health Acupuncture & Wellness Center, LLC 260 Gateway Drive, Suite 7B Bel Air, Maryland 21014 410-913-8322 Patient Name: Date of Birth: Age: Male: Female: Single: Married: Separated:
City State Zip Code. Ethnic Background: Caucasian African-American Asian Hispanic Native American. Previous. Hobbies/Leisure activities:,,,
 History # UPIN # (Please leave blank) Name: First M.I. Last Address: Street (Apt #) City State Zip Code Phone number: ( ) ( ) Home Business Birth Date: / / Day-Month-Year Gender: M F Marital status: (Maiden
History # UPIN # (Please leave blank) Name: First M.I. Last Address: Street (Apt #) City State Zip Code Phone number: ( ) ( ) Home Business Birth Date: / / Day-Month-Year Gender: M F Marital status: (Maiden
Copyright The Food Intolerance Testing Group. All rights reserved. No part of this publication may be
 Copyright 2018 The Food Intolerance Testing Group All rights reserved. No part of this publication may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording,
Copyright 2018 The Food Intolerance Testing Group All rights reserved. No part of this publication may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording,
Metabolic Assessment Form
 Metabolic Assessment Form Approach Wellness and Aesthetics 200 Forsythe Street Fayetteville, NC 28303 Office: (910) 322-7368 Fax: (910) 483-5796 www.tawellness.net Name: Age: Sex: Date: Part 1: Please
Metabolic Assessment Form Approach Wellness and Aesthetics 200 Forsythe Street Fayetteville, NC 28303 Office: (910) 322-7368 Fax: (910) 483-5796 www.tawellness.net Name: Age: Sex: Date: Part 1: Please
725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA (770) (770) (facsimile)
 (770) (facsimile)") Charles Nash, III, M.D., F.A.C.P. Richard J. LoCicero, M.D. Anup K. Lahiry, M.D. Timothy M. Carey, M.D. Andrew Johnson, M.D. 725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA 30501 (770) 297-5700 (770)
Charles Nash, III, M.D., F.A.C.P. Richard J. LoCicero, M.D. Anup K. Lahiry, M.D. Timothy M. Carey, M.D. Andrew Johnson, M.D. 725 Jesse Jewell Pkwy, Suite 390 Gainesville, GA 30501 (770) 297-5700 (770)
Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop.
, by mouth, or as an eye drop.") Dexamethasone Other Names: Decadron About This Drug Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop. Possible Side Effects (More Common) Increased
Dexamethasone Other Names: Decadron About This Drug Dexamethasone is used to treat cancer. This drug can be given in the vein (IV), by mouth, or as an eye drop. Possible Side Effects (More Common) Increased
Metabolic Assessment Form Please list your five major health concerns in your order of importance.
 Metabolic Assessment Form Please list your five major health concerns in your order of importance. 1. 2. 3. 4. 5. Please check the appropriate number on all questions below, using zero as least/never to
Metabolic Assessment Form Please list your five major health concerns in your order of importance. 1. 2. 3. 4. 5. Please check the appropriate number on all questions below, using zero as least/never to
Course: Formulas 1 Date: December 2, 2009 Class #: 10. Function in Formula. Disperse stagnation
 Course: Formulas 1 Date: December 2, 2009 Class #: 10 Xi Jiao Di Huang Tang : o Clear Heat toxins o o Disperse stagnation : o Heat in the blood Xi jiao Sheng di Shao yao Mu dan pi Clear Heart heat Nourish
Course: Formulas 1 Date: December 2, 2009 Class #: 10 Xi Jiao Di Huang Tang : o Clear Heat toxins o o Disperse stagnation : o Heat in the blood Xi jiao Sheng di Shao yao Mu dan pi Clear Heart heat Nourish
Patient Health History
 Patient Health History Name: Date: Address: City, State, Zip code Phones: Home Work: Cell: Email address: Date of Birth: Age: Occupation: Emergency contact: Referred by: Current Medications: Are you/might
Patient Health History Name: Date: Address: City, State, Zip code Phones: Home Work: Cell: Email address: Date of Birth: Age: Occupation: Emergency contact: Referred by: Current Medications: Are you/might
Northeast Ohio Urogynecology Patient History Intake Form. Last Name First Name Age. Date of Birth Race Referring Physician.
 Northeast Ohio Urogynecology Patient History Intake Form Last Name _First Name Age_ Date of Birth Race Referring Physician Reason for Visit: _ Allergies: Preferred Lab (circle): QUEST LABCARE PLUS LABCORP
Northeast Ohio Urogynecology Patient History Intake Form Last Name _First Name Age_ Date of Birth Race Referring Physician Reason for Visit: _ Allergies: Preferred Lab (circle): QUEST LABCARE PLUS LABCORP
CECILIA P MARGRET MD PhD MPH Child, Adolescent and Adult Psychiatry NE 24th ST Suite 104, Bellevue WA 98007, Phone / Fax: +1 (425)
") IDENTIFYING INFORMATION PATIENT INFORMATION FORM Patient's Name: DOB: Ethnicity/race: Gender: Primary language if other than English: Address: Phone: Home/ Mobile/ Work Email: Occupation: Marital Status:
IDENTIFYING INFORMATION PATIENT INFORMATION FORM Patient's Name: DOB: Ethnicity/race: Gender: Primary language if other than English: Address: Phone: Home/ Mobile/ Work Email: Occupation: Marital Status:
Diet, Nutrition and Inflammatory
 Diet, Nutrition and Inflammatory Bowel Disease Sumner Brooks, MPH, RDN, LD March 11, 2017 Objectives Identify factors that may alter nutritional status in IBD Understand the role of diet and nutrition
Diet, Nutrition and Inflammatory Bowel Disease Sumner Brooks, MPH, RDN, LD March 11, 2017 Objectives Identify factors that may alter nutritional status in IBD Understand the role of diet and nutrition
Avery Acupuncture & Natural Medicine New Patient Registration
 Welcome to Avery Acupuncture & Natural Medicine. Our goal is to make your experience here as comfortable as possible. If you have any questions, comments, concerns or suggestions, please let Veronica or
Welcome to Avery Acupuncture & Natural Medicine. Our goal is to make your experience here as comfortable as possible. If you have any questions, comments, concerns or suggestions, please let Veronica or
Clear Heat and Cool Blood Herbs
 Course: Chinese Herbology 1 Date: October 28, 2008 Class #: 6 Clear Heat/Cool Blood Herbs Clear Heat and Cool Blood Herbs Introduction Used for Ying and Xue stages, the 2 deepest of the four levels of
Course: Chinese Herbology 1 Date: October 28, 2008 Class #: 6 Clear Heat/Cool Blood Herbs Clear Heat and Cool Blood Herbs Introduction Used for Ying and Xue stages, the 2 deepest of the four levels of
Have you had all childhood diseases i.e.? chickenpox. Y N. Have you ever suffered from an infectious illness? i.e. glandular fever.
 Acupuncture case history card Name: Date: Address: Ph No: (H) (W) (M) E-mail: Fax: D.O.B Sex: M F Marital Status: Occupation: Dr: Suburb: Referred by: Health fund Medical history For the following questions,
Acupuncture case history card Name: Date: Address: Ph No: (H) (W) (M) E-mail: Fax: D.O.B Sex: M F Marital Status: Occupation: Dr: Suburb: Referred by: Health fund Medical history For the following questions,
What do you believe is causing your most important health concern?
 Intake form Name Today s Date Date of Birth Address City Phone Postal Code Email Primary Health Care Provider Emergency Contact Phone Note: By providing your email address you are giving us consent to
Intake form Name Today s Date Date of Birth Address City Phone Postal Code Email Primary Health Care Provider Emergency Contact Phone Note: By providing your email address you are giving us consent to
ACUPUNCTURE INTAKE FORM
 ACUPUNCTURE INTAKE FORM This questionnaire is CONFIDENTAL and used to gather information to give you the most effective treatment possible. Name Address City State Zip Phone Home Work Cell Email Birth
ACUPUNCTURE INTAKE FORM This questionnaire is CONFIDENTAL and used to gather information to give you the most effective treatment possible. Name Address City State Zip Phone Home Work Cell Email Birth
NEW PATIENT INTAKE FORM
 NEW PATIENT INTAKE FORM Acupuncture * Herbs * Nutrition Located inside of Yoga 360 91 Bankview Drive Frankfort, IL 60423 815-806-0360/www.yoga-360.com lkacupuncture.com lizkelchak@gmail.com How To Prepare
NEW PATIENT INTAKE FORM Acupuncture * Herbs * Nutrition Located inside of Yoga 360 91 Bankview Drive Frankfort, IL 60423 815-806-0360/www.yoga-360.com lkacupuncture.com lizkelchak@gmail.com How To Prepare
TONICS TO TONIFY OR TO EXPEL: THAT IS THE QUESTION
 TONICS "The three months of Autumn are the time of harvest. The energy of Heaven begins to blow swiftly and the energy of Earth begins to change colour. One should go to bed early and rise early: maintain
TONICS "The three months of Autumn are the time of harvest. The energy of Heaven begins to blow swiftly and the energy of Earth begins to change colour. One should go to bed early and rise early: maintain
Patient Information & Health History
 Patient Information & Health History Name Date Date of Birth (mm/dd/yy) Age Male Female Address City Postal Code Occupation Phone (H) E-mail Phone (C) Married Single Divorced Widowed Phone (W) Spouse s
Patient Information & Health History Name Date Date of Birth (mm/dd/yy) Age Male Female Address City Postal Code Occupation Phone (H) E-mail Phone (C) Married Single Divorced Widowed Phone (W) Spouse s
Traditional Chinese Medicine Diagnostic 10 Questions Please answer each question.
 1 Traditional Chinese Medicine Diagnostic 10 Questions Please answer each question. 1. Thinking about your internal thermostat and where you feel your body temperature is most of the day, do you think
1 Traditional Chinese Medicine Diagnostic 10 Questions Please answer each question. 1. Thinking about your internal thermostat and where you feel your body temperature is most of the day, do you think
PATIENT HISTORY FORM
 PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
LAST NAME FIRST NAME MI SEX BIRTH DATE AGE ADDRESS CITY STATE ZIP ( ) - ( ) - PHONE CELL PHONE ADDRESS DRIVER S LICENSE NO.
 - ( ) - PHONE CELL PHONE ADDRESS DRIVER S LICENSE NO.") Cathryn Aiken, L.Ac. 530 Traffic Way Arroyo Grande, CA 93420 T: 805.489.8592 F: 805.489.9509 www.arroyograndehealthandwellness.com aghealthandwellness@gmail.com PLEASE PRINT LEGIBLY TODAY S DATE: M / F
Cathryn Aiken, L.Ac. 530 Traffic Way Arroyo Grande, CA 93420 T: 805.489.8592 F: 805.489.9509 www.arroyograndehealthandwellness.com aghealthandwellness@gmail.com PLEASE PRINT LEGIBLY TODAY S DATE: M / F
All nutrition appointments NOT given 24 hours notice of cancellation will incur a $50 charge.
 Nutritional Counseling Food Sensitivity Testing Neurotransmitter Testing Hormone Testing Wellness & Prevention 111 O Fallon Commons Drive O Fallon, MO 63368 Phone: 636-978-0970 Fax: 636-978-7570 Dr. Olivia
Nutritional Counseling Food Sensitivity Testing Neurotransmitter Testing Hormone Testing Wellness & Prevention 111 O Fallon Commons Drive O Fallon, MO 63368 Phone: 636-978-0970 Fax: 636-978-7570 Dr. Olivia
Health Intake Form. List your top five concerns or reasons for requesting your appointment with Dr. Weiss
 List your top five concerns or reasons for requesting your appointment with Dr. Weiss 1. 2. 3. 4. 5. Please give any information you think is important regarding these top concerns: Health Intake Form
List your top five concerns or reasons for requesting your appointment with Dr. Weiss 1. 2. 3. 4. 5. Please give any information you think is important regarding these top concerns: Health Intake Form
Healthy Living. with Arbonne
 Healthy Living with Arbonne Did You Know? The #1 killer of men and women in the U.S. is heart disease 2 out of 3 U.S. adults are overweight or obese U.S. adults consume approx. 2-3 lbs. of sugar each week!
Healthy Living with Arbonne Did You Know? The #1 killer of men and women in the U.S. is heart disease 2 out of 3 U.S. adults are overweight or obese U.S. adults consume approx. 2-3 lbs. of sugar each week!
For the Patient: USMAVPEM
 For the Patient: USMAVPEM Other Names: Treatment of Unresectable or Metastatic Melanoma Using Pembrolizumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced PEM = Pembrolizumab
For the Patient: USMAVPEM Other Names: Treatment of Unresectable or Metastatic Melanoma Using Pembrolizumab U = Undesignated (requires special request) SM = Skin and Melanoma AV = Advanced PEM = Pembrolizumab
New Client Health & Wellness Paper Work
 Nutritionally Yours Health Solutions 604 Macy Drive, Roswell GA 30076 678-372-2913 / alanepnd@gmail.com New Client Health & Wellness Paper Work Today's Date Patient Name: _ Parents Name (if patient is
Nutritionally Yours Health Solutions 604 Macy Drive, Roswell GA 30076 678-372-2913 / alanepnd@gmail.com New Client Health & Wellness Paper Work Today's Date Patient Name: _ Parents Name (if patient is
New Client Intake Form
 New Client Intake Form Name DOB Age Gender Address City State Zip Preferred phone # Alternate phone # Email address Occupation Referred by Have you had acupuncture before: When Emergency, contact: Phone
New Client Intake Form Name DOB Age Gender Address City State Zip Preferred phone # Alternate phone # Email address Occupation Referred by Have you had acupuncture before: When Emergency, contact: Phone
Carlette Zottola Lac, MSTOM Acupuncture New Patient Intake Form. Patient Information. Emergency Contact Information.
 Carlette Zottola Lac, MSTOM Acupuncture New Patient Intake Form Patient Information Name: Date of Birth: Age: Gender(please circle) M or F Occupation: Address: City, State, Zip: Email: Home Phone: Cell
Carlette Zottola Lac, MSTOM Acupuncture New Patient Intake Form Patient Information Name: Date of Birth: Age: Gender(please circle) M or F Occupation: Address: City, State, Zip: Email: Home Phone: Cell
Course: Formulas 1 Date: September 30, 2009 Class #: 2 Prof: Dr. Ma
 Course: Formulas 1 Date: September 30, 2009 Class #: 2 Prof: Dr. Ma WEEK TWO: Class 2 Goals: Students will learn traditional treatment methods - sweating, vomiting, draining downward, harmonizing, warming,
Course: Formulas 1 Date: September 30, 2009 Class #: 2 Prof: Dr. Ma WEEK TWO: Class 2 Goals: Students will learn traditional treatment methods - sweating, vomiting, draining downward, harmonizing, warming,
SYSTEMS SURVEY FORM. Doctor
 Patient Birth Date / / Approx Weight SYSTEMS SURVEY FORM Doctor INSTRUCTIONS: Fill in only the circles which apply to you. Leave blank if you don't have the problem. Fill in the circle marked 1 for MILD
Patient Birth Date / / Approx Weight SYSTEMS SURVEY FORM Doctor INSTRUCTIONS: Fill in only the circles which apply to you. Leave blank if you don't have the problem. Fill in the circle marked 1 for MILD