Pan Scan Instead of Clinical Exam? David A. Spain, MD
|
|
|
- Jonah Hodge
- 6 years ago
- Views:
Transcription
1 Pan Scan Instead of Clinical Exam? David A. Spain, MD


2

3 Granted, some patients don t t need CT scan
4 Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do

5 LightSpeed The Power to Scan. Finer. Faster. Further.

6 The New ABCs Admit Begin CT T scan Only exam pt if CT doesn t t tell you what s s wrong
7 Everybody loves CT scan Often times, resuscitation seems like a race to CT scan I have seen pts taken to CT without completing primary survey, let alone the secondary portion
8 Death begins in X-ray
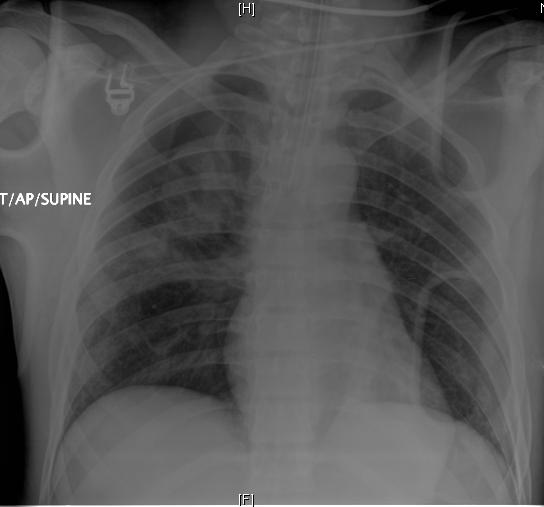
9 Real Case 22 year old man Restrained passenger Side impact on his side Intubated in field (mental status)? Right chest crepitance Being wheeled to CT scan when surgery R4 stopped and insisted on reviewing CXR
10
11 Dilemma What s s the cost of a CT scan Real dollars Versus Cost of missed or delayed injuries Faster thru put (double-edge) edge) Peace of mind Can you accurately predict who needs or doesn t t need a CT scan?
12 Injuries distracting from IAI after blunt trauma Prospective study, GCS 15 and CT of abdomen or DPL Presence of pain and/or tenderness sensitivity 82% specificity 45% positive predictive value 21% negative predictive value 93% Abdominal pain and/or tenderness incidence of IAI, but lack of these findings did not preclude IAI Am J Emerg Med 1998;16:145-9
13 CT for blunt abdominal trauma in the ED: a prospective study. 196 patients were evaluated Abdominal tenderness present in patients had IAI (11%) Abnormal abdomen examination and hematuria sensitivity of 64% specificity of 94% positive predictive value of 56% negative predictive value of 95% Am J Emerg Med 1998;16:338-42


14 Absence of intraabdominal injury predicted with sensitivity of 100% and specificity of 87%

15 Surgery 2002;132, p
16 Abd CT with increased AST in the era of FAST HD stable, FAST negative and an AST > 200 IU/L 42 (63%) had AST level < 360 IU/L and 25 (37%) had an AST > 360 IU/L AST level > 360 IU/L 88% chance any hepatic injury 44% were > grade III AST level < 360 IU/L 14% chance any liver injury no chance of injury > grade III or greater Surgery. 2002;132:642-6

17
18 Admit or obs is not necessary after a negative Abd CT: results of a prospective, multi-institutional institutional trial 22 months at four Level I trauma centers All patients with blunt abdominal trauma suspected by either PE or mechanism were evaluated by protocol PE in the ED Abdominal CT scan Hospitalization for observation Standardized PE was repeated between 4 and 8 hours J Trauma 1998;44:273-80
19 Admit or obs is not necessary after a negative Abd CT 2299 fulfilled the entire study protocol 21% were positive 19% patients with a positive CT scan had no tenderness Negative predictive power of abd CT scan based on prelim reading and need for a laparotomy was 99.63%
20 Can we omit head CT?? Loss of consciousness: when to perform computed tomography? Kids w/ LOC or amnesia and GCS should have a head CT to avoid missing an intracranial injury Minor head trauma: Is computed tomography always necessary? Routine head CT in pts with LOC/amnesia but no Sx/signs of depressed skull fracture has minimal value and not warranted NEXUS
21 Value of repeat cranial CT in patients with minimal head injury MHI and a positive cranial CAT scan 151 had a persistently normal or improved neurological examination none required after the repeat cranial CAT scan? Value repeat CAT scan in this setting J Trauma 2004;56:475-80
22 Do we really need CT in primary evaluation of blunt chest trauma in patients with "normal" CXR? 93 consecutive patients 76% MVC > 10 mph 24% after fall > 5 ft 25 had normal CXR and 13 (52%) CT scan showed multiple injuries 2 (8%)aortic lacerations 3 pleural effusions 1 pericardial effusion J Trauma 2001;51:1173-6
23 Reevaluation of diagnostic procedures for transmediastinal gunshot wounds 22 stable patients CT scans were positive in 7 Directed further diagnostic evaluation 2 operations 68% had negative CT scans and were observed without further evaluation No missed injuries Hospital charges generated with CT-based protocol were significantly less J Trauma 2002;53:635-8
24 Reformatted visceral protocol HCT vs. conventional radiographs of T and L spine in blunt trauma patients prospective evaluation of consecutive patients with thoracic and lumbar spine fractures Screening sensitivity Reformatted HCT: 97% (T) and 95% (L) Conventional Xray:62% (T) and 86% (L) J Trauma 2003;55:665-9


25 It s s always good to exam the patients Restrained rear seat passenger with seatbelt, c/o some abd pain
26

27 Reliability of clinical exam in detecting pelvic fx in blunt trauma 12 studies with 5454 patients 49 false neg cases fx majority had either altered consciousness or minor pelvic fracture only Only 3 clinically relevant pelvic fractures were missed among 441 pts with fracture within a total population > 5000 In stable and alert trauma pts, thorough exam will detect pelvic fractures with nearly 100% sensitivity
28 Selective management of penetrating neck trauma based on level of injury 312 pts over 18 years 75% stab, 25% GSW Zone I=13%, Zone II=67%, Zone III=20% 34% early exploration (16% non- therapeutic) 66% observed (0.5% delayed exploration) Am J Surg 1997;174:
29 Selective Management Unstable Hard signs OR Penetrating Neck Injury Symptoms or Signs Zone I Zone II Zone III study OR angio Zone I study Asymptomatic Zone II/III observe
30 Start with Assessment of Skin Temperature to Identify Hypoperfusion in ICU Trauma or Septic pts w/o obvious low flow Examined distal extremities and measured serum HCO - 3 Either abnormal - check lactate If lactate - resuscitate ± invasive monitor J Trauma 2001;50:620-7
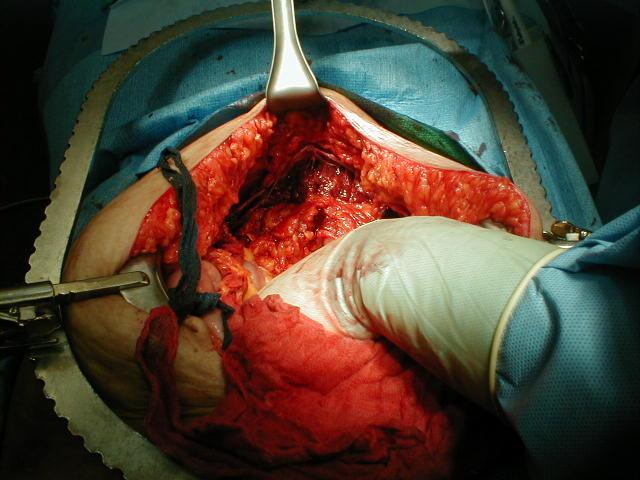
31 You can t t get it back in
32 Not an either/or question CT scan technology will continue to improve Faster More accurate Supplanting other invasive modalities CT is complimentary to good initial assessment and serial examinations

33
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Evaluation of Children with Blunt Abdominal Trauma. James F. Holmes, MD, MPH UC Davis School of Medicine
 Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Evaluation of Children with Blunt Abdominal Trauma James F. Holmes, MD, MPH UC Davis School of Medicine Objectives Epidemiology of intra-abdominal injury (IAI) Physical examination findings with IAI Laboratory
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Selective Spinal Immobilization
 Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
The Secondary Survey
 The Secondary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining
The Secondary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010
 Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
Sasha Dubrovsky, MSc MD FRCPC Pediatric Emergency Medicine Montreal Children s Hospital - MUHC October 2010 Learning objectives 1. Discuss diagnostic goals in pediatric trauma Diagnose All vs. Severe Injuries
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes. Lisa Schwing, RN Trauma Program Manager Dayton Children s
 Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
Little Kids in Big Crashes The Bio-mechanics of Kids in Car Crashes Lisa Schwing, RN Trauma Program Manager Dayton Children s Very Little Research There has been very little research on the forces a crash
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
ESCAMBIA COUNTY TRAUMA TRANSPORT
 TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
TRAUMA ALERT CRITERIA are established state mandated criteria. ADULT TRAUMA ALERT CRITERIA (Physical and anatomical characteristics of a person 16 years of age or older) Any 1 of the following: 1. Airway:
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Cases from the Streets. Kelly Buchanan MD, ATC/L EMS Fellow December, 2011
 Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Cases from the Streets Kelly Buchanan MD, ATC/L EMS Fellow December, 2011 The Scene Car vs Light Pole, 35 mph, front right side damage 10 with no PCI + airbag deployment, starring on windshield Given the
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
17. Imaging and interventional radiology
 17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
17. Imaging and interventional radiology These guidelines have been adapted from the Leeds Major Trauma Centre Imaging in Paediatric Major Trauma guidelines Written by Dr Annmarie Jeanes (Consultant Paediatric
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
Introduction. Objectives C-Spine: Where Are We Now? NAEMSP Medical Director Course 1/9/2013
 NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
UHSM ED Pathway ELDERLY FALL / COLLAPSE
 UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
UHSM ED Pathway ELDERLY FALL / COLLAPSE Patient name / Pathway for patients who require assessment in ED after a fall or collapse Note: - It can be used if the patient has also sustained a minor head injury
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
Pediatric Trauma: Pearls of Management
 Pediatric Trauma: Pearls of Management Judith R. Klein, MD Assistant Professor UCSF-SFGH SFGH Department of Emergency Medicine Pediatric Trauma: The Problem Leading cause of M/M age 1-241 50% of all pediatric
Pediatric Trauma: Pearls of Management Judith R. Klein, MD Assistant Professor UCSF-SFGH SFGH Department of Emergency Medicine Pediatric Trauma: The Problem Leading cause of M/M age 1-241 50% of all pediatric
Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015
![Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015](/thumbs/83/87309292.jpg "Enter modality here Enter modality here, enter none if none. Principal Modality (2): Case Report # [] Date accepted: April 2015") Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Radiological Category: Enter category here Principal Modality (1): Principal Modality (2): Enter modality here Enter modality here, enter none if none Case Report # [] Submitted by: Varun Rachakonda, M.D.
Trauma CT Scanning Protocol
 Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Northern Trauma Network Trauma CT Scanning Protocol Background Whole body CT (WBCT) has assumed a pivotal position in trauma management. UK trauma is typically described as blunt and blind i.e. blunt trauma
Bilateral rib fractures 2 on right and 1 on left In different stages of healing, with left fracture older than right fractures
 More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted
More history: Seen by PCP yesterday because of vomiting and fussinesss. Called by ED today because Mom presents with same complaints. ED found nothing but got an abdominal x ray. ED now wants kid admitted
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Review. 1. Kinetic energy is a calculation of:
 Chapter 22 Review Review 1. Kinetic energy is a calculation of: A. weight and size. B. weight and speed. Caring for victims of traumatic injuries requires the EMT to have a solid understanding of the trauma
Chapter 22 Review Review 1. Kinetic energy is a calculation of: A. weight and size. B. weight and speed. Caring for victims of traumatic injuries requires the EMT to have a solid understanding of the trauma
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
Pediatric CT Protocols (18 years old or less)
") Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
EMS System for Metropolitan Oklahoma City and Tulsa 2019 Medical Control Board Treatment Protocols
 EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 14G PATIENT PRIORITIZATION While each patient will receive the best possible EMS care in a humane and ethical manner, proper patient
EAST MULTICENTER STUDY DATA DICTIONARY
 EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
EAST MULTICENTER STUDY DATA DICTIONARY Does the Addition of Daily Aspirin to Standard Deep Venous Thrombosis Prophylaxis Reduce the Rate of Venous Thromboembolic Events? Data Entry Points and appropriate
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Dose-equivalent equivalent = absorbed
 UCSF General Surgery 2010 Radiation Risks of Diagnostic Radiology in Trauma Robert A. Izenberg, M.D., FACS University of California, San Francisco San Francisco General Hospital Context Increasingly liberal
UCSF General Surgery 2010 Radiation Risks of Diagnostic Radiology in Trauma Robert A. Izenberg, M.D., FACS University of California, San Francisco San Francisco General Hospital Context Increasingly liberal
PEDIATRIC TRAUMA EMERGENCIES
 PEDIATRIC TRAUMA EMERGENCIES Last Revised: January 2015 1 PEDIATRIC COMA SCALE Indicator Eye Opening Spontaneous 4 To verbal stimuli 3 To pain only 2 No response 1 Verbal Response Oriented, appropriate
PEDIATRIC TRAUMA EMERGENCIES Last Revised: January 2015 1 PEDIATRIC COMA SCALE Indicator Eye Opening Spontaneous 4 To verbal stimuli 3 To pain only 2 No response 1 Verbal Response Oriented, appropriate
Identify the risk management issues involved in caring for patient with orthopedic complaints.
 MACEP Risk Management Course Module 4: Emergency Orthopedics Matthew B. Mostofi, D.O., FACEP Course Objectives Identify the risk management issues involved in caring for patient with orthopedic complaints.
MACEP Risk Management Course Module 4: Emergency Orthopedics Matthew B. Mostofi, D.O., FACEP Course Objectives Identify the risk management issues involved in caring for patient with orthopedic complaints.
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
Pediatric Trauma. July 27 th, Suzana Buac, PGY4. Dr. Neil Merritt
 Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pediatric Trauma July 27 th, 2016. Suzana Buac, PGY4 Dr. Neil Merritt Case 5yoM fall from roof Fall from roof of home while father was shingling 5yoM fall from roof Fall from roof of home while father
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL
 Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
Pediatric Aspects of Advanced Trauma Life Support: Transition from EMS to the Trauma Room HALE WILLS, MD PEDIATRIC TRAUMA DIRECTOR, HASBRO CHILDREN S HOSPITAL Objectives 1. Identify the critical components
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Section J: Trauma. Section J: Trauma. Clinical/Diagnostic Problem. (Grade) Head
 Head") J Hea J01. Hea injury (For chilren see Section L) Recommenation (Grae) S Not inicate [B] There is poor correlation between the presence of a skull fracture an a clinically significant hea injury. The only
J Hea J01. Hea injury (For chilren see Section L) Recommenation (Grae) S Not inicate [B] There is poor correlation between the presence of a skull fracture an a clinically significant hea injury. The only
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Clarifying Murky Waters: Head and Cervical Spine Injuries in Children
 Clarifying Murky Waters: Head and Cervical Spine Injuries in Children Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Emergency Services Case #1: Newborn Leo 2 month old
Clarifying Murky Waters: Head and Cervical Spine Injuries in Children Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Emergency Services Case #1: Newborn Leo 2 month old
Management of Penetrating Neck Trauma
 Management of Penetrating Neck Trauma Shashidhar S. Reddy, MD, MPH Faculty Advisor: Shawn D. Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
Management of Penetrating Neck Trauma Shashidhar S. Reddy, MD, MPH Faculty Advisor: Shawn D. Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016
 PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
PEDIATRIC BLUNT TRAUMA WHAT S DIFFERENT? NORDIC TRAUMA COURSE 2016 Ken F. Linnau, MD, MS Emergency Radiology Harborview Medical Center University of Washington Seattle, WA Thanks to Nupur Verma, MD University
North West London Trauma Network Spinal Pathway and Protocols
 North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
North West London Trauma Network Spinal Pathway and Protocols 1. Spinal Clearance in the Trauma Patient Inclusions: All trauma patients who are not alert and orientated, unable to cooperate (including
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
CLINICAL MANUAL. Trauma System Activation Trauma Code Criteria
 CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
CLINICAL MANUAL Policy Number: CM T-28 Approved by: Nursing Congress, Management Forum Issue Date: 09/1999 Applies to: Downtown Value(s): Respect, Integrity, Innovation Page(s): 1 of 4 Trauma System Activation
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Restore adequate respiratory and circulatory conditions. Reduce pain
 Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Pre-hospital management of the trauma patient is best performed by an integrated team focused on minimizing the time from injury to definitive care at an appropriate trauma center. Dispatchers, first responders,
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Registry Documentation December 16, 2014
 Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Trauma Registry Documentation December 16, 2014 The State of Florida now requires ALL Acute Care hospitals to submit data to the statetrauma Registry. Although Baptist Health hospitals are NOT Trauma Centers
Imaging in Trauma. Dr Amir Ashrafi
 + Imaging in Trauma Dr Amir Ashrafi + Portable x-rays n Plain radiographs play an important role in the primary evaluation of the unstable trauma patient. n Prompt imaging of the lateral cervical spine,
+ Imaging in Trauma Dr Amir Ashrafi + Portable x-rays n Plain radiographs play an important role in the primary evaluation of the unstable trauma patient. n Prompt imaging of the lateral cervical spine,
Case Based Review (Whew!)
") Northern California Emergency Ultrasound Course Case Based Review (Whew!) Martine Sargent, MD Ultrasound Director, Assistant Professor UCSF Department of Emergency Medicine San Francisco General Hospital
Northern California Emergency Ultrasound Course Case Based Review (Whew!) Martine Sargent, MD Ultrasound Director, Assistant Professor UCSF Department of Emergency Medicine San Francisco General Hospital
Spine MRI and Spine CT Test Request Tip Sheet
 Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Spine MRI and Spine CT With/Without Contrast CT, MRI Studies should NOT be ordered simultaneously as dual studies (i.e., with and without contrast). Radiation exposure is doubled and both views are rarely
Crash, Bonk, Thud! (Trauma Case Studies) John Beuerle, M.D.
 John Beuerle, M.D.") Crash, Bonk, Thud! (Trauma Case Studies) John Beuerle, M.D. Case 1 (22 y.o. female, wakeboarding injury) Case 1 (22 y.o. female, wakeboarding injury) Arrives via EMS cc: left leg injury HPI: Patient
Crash, Bonk, Thud! (Trauma Case Studies) John Beuerle, M.D. Case 1 (22 y.o. female, wakeboarding injury) Case 1 (22 y.o. female, wakeboarding injury) Arrives via EMS cc: left leg injury HPI: Patient
Extended FAST Exam. Goal of Trauma Care. Golden Hour of Trauma
 Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Chapter 39 Trauma in the Elderly
 Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Chapter 39 Trauma in the Elderly Episode Overview 1) 5 Risk Factors for falls in the elderly? 2) What anatomic and physiologic changes in the elderly patient are important for the management of trauma
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center
 ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
ER-REBOA Patient Selection, the Procedure, and Outcomes Joseph Ibrahim, MD FACS Trauma Medical Director Orlando Regional Medical Center Disclosures Speaking Consultant with Prytime Medical Outline Mechanism
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
10/27/2014. An experience that causes physical, emotional, or psychological distress or harm.
 Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Ann Marie Szoke, DNP, CRNP Supervisor Advanced Practitioners St. Luke s University Hospital To review multiple traumatic events through case presentations Discuss the concept of the Hybrid Operating Room
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
D. Pre-Hospital Trauma Triage and Bypass Algorithm
 D. Pre-Hospital Trauma Triage and Bypass Algorithm Hospital bypass is defined as transporting the patient to the nearest hospital that has the appropriate level of care for the patient s suspected severity
D. Pre-Hospital Trauma Triage and Bypass Algorithm Hospital bypass is defined as transporting the patient to the nearest hospital that has the appropriate level of care for the patient s suspected severity
10O SPLINTING OF INJURIES ADULT & PEDIATRIC. 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric:
 10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
CT PROCEDURE REFERENCE GUIDE 2017
 Head CT PROCEDURE REFERENCE GUIDE 2017 Procedure Contrast Scan Field Preparatio n Base of Skull to Vertex Sinuses Orbits Mastoids/IAC/ Temporal Bones Facial Bones ST Neck Low Dose Lung Screening Routine
Head CT PROCEDURE REFERENCE GUIDE 2017 Procedure Contrast Scan Field Preparatio n Base of Skull to Vertex Sinuses Orbits Mastoids/IAC/ Temporal Bones Facial Bones ST Neck Low Dose Lung Screening Routine
3/14/2014 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION THE PROBLEM OLD THINKING
 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
Table 2 - ATLS 8 th Edition Compendium of Changes (The Evidence for change, Jtrauma, Vol 64, number 6, pages )
") Table 2 - ATLS 8 th Edition Compendium of Changes (The Evidence for change, Jtrauma, Vol 64, number 6, pages 1638-1650) Chapter Subject 7 th Edition 8th Edition 1. Initial Assessment Rectal examination
Table 2 - ATLS 8 th Edition Compendium of Changes (The Evidence for change, Jtrauma, Vol 64, number 6, pages 1638-1650) Chapter Subject 7 th Edition 8th Edition 1. Initial Assessment Rectal examination
Could This Be You? Medical-Legal Case Studies Michael Jay Bresler, M.D., FACEP
 Could This Be You? Medical-Legal Case Studies Michael Jay Bresler, M.D., FACEP Clinical Professor Division of Emergency Medicine Stanford University School of M di i MEDICAL - LEGAL CASE WISDOM We (Should)
Could This Be You? Medical-Legal Case Studies Michael Jay Bresler, M.D., FACEP Clinical Professor Division of Emergency Medicine Stanford University School of M di i MEDICAL - LEGAL CASE WISDOM We (Should)
Yaniv Berliner EMS STABILIZATION
 Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
Yaniv Berliner EMS STABILIZATION Scene survey EMS must first evaluate the safety of the scene. Downed power lines, fire, traffic Is there a need for specialized equipment for extrication. Is there a need
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Dr. Mike Brzozowski Trauma Team Leader and Emergency. Sunnybrook Health Sciences Centre Toronto, Ontario
 Dr. Mike Brzozowski Trauma Team Leader and Emergency Physician i Sunnybrook Health Sciences Centre Toronto, Ontario Learning Objectives To better understand the controversies with respect to the rational
Dr. Mike Brzozowski Trauma Team Leader and Emergency Physician i Sunnybrook Health Sciences Centre Toronto, Ontario Learning Objectives To better understand the controversies with respect to the rational