Wound and Skin Care. What every nurse needs to know! Ruhama Bond, RN. Updated 14 February 2013/ Updated 6/17/13 Updated 10/28/13
|
|
|
- Hester Terry
- 6 years ago
- Views:
Transcription
1 Wound and Skin Care What every nurse needs to know! Ruhama Bond, RN Updated 14 February 2013/ Updated 6/17/13 Updated 10/28/13
2 Objectives Demonstrate the use of the Braden Scale Pressure Ulcer Risk Assessment Tool in simulated patient situations Discuss interventions to reduce patient's risk of skin breakdown Identify pressure ulcers according to NPUAP staging system Discuss essential factors for a comprehensive wound assessment
3 Wounds - CMS and Joint Commission CMS and TJC endorsed the concept that pressure ulcers are directly linked to hospital quality The national treatment cost is estimated at $5-8 billion annually Experts agree that costs to treat pressure ulcers is much greater than costs of prevention In 2008, CMS classified pressure ulcers as a PREVENTABLE hospital acquired condition and is no longer reimbursable.
4 Expectations at CFV Skin and wound assessments are completed on admission Skin assessment is completed every shift If patient has a wound, the wound assessment is done with dressing changes or as noted with the skin assessments Braden Risk Assessment is completed on admission and whenever there is a change in the patient s condition or change in care plan interventions for prevention of a pressure ulcer
5 Expectations at CFV.cont Perform head to toe, front to back skin assessment: Include HOT SPOTS (bony prominences) Occiput, ears, knees, toes, scapula, thoracic spine, sacrum, posterior buttocks, heels Remove non-surgical dressings and assess the wound (surgical dressings typically have specific physician orders ) Initiate the Skin /Wound Protocol if indicated or follow physician wound orders (obtain wound VAC orders) If pressure ulcers are not documented within 24 hrs of admission it is considered to be hospital acquired
6 Expectations at CFV-..cont Orders should be initiated immediately when they are written including specialty beds, wound care consults Don t forget critical referrals such as Nutrition Good nutrition is critical for healing monitor intake Ask MD to order supplements The primary nurse should attend to the patient when the wound care nurse assesses the wound/pressure ulcer
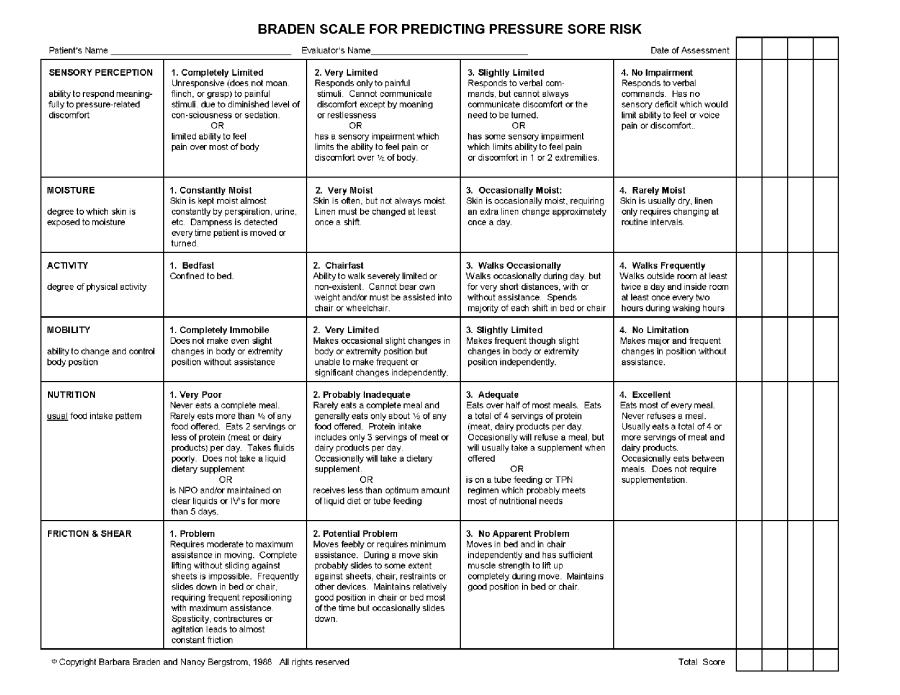
7 Braden Scale A Pressure Ulcer Risk Assessment Tool
8 What is the Braden Scale? Tool to assess risk of Pressure Ulcer Category scores added to indicate risk Lower score = higher risk Clinically validated Reliable
9 Key Benefits Short Good reminder Consistency for nurses with varied experience Focuses prevention in 6 key areas It only takes about 30 seconds to complete an accurate Braden score.
10 Key Benefits Proven track record: Nosocomial pressure ulcers 40-60% Severity of nosocomial pressure ulcers Cost of care by inappropriate use of specialty beds Cost of treating ulcers

11
12 6 Categories of Braden Scale Sensory Perception Moisture Activity Mobility Nutrition Friction & shear
13 Sensory Perception Ability to respond meaningfully to pressurerelated discomfort. 1. Completely Limited Unresponsive (does not moan, flinch, or grasp) to painful stimuli, due to diminished level of consciousness or sedation. OR Limited ability to feel pain over most of the body. This is the quadriplegic patient or the patient in a vegetative state.
14 Sensory Perception 2. Very Limited Responds only to painful stimuli. Cannot communicate discomfort except by moaning or restlessness. OR Has a sensory impairment which limits the ability to feel pain or discomfort over ½ of body. This is the paraplegic patient or the patient who is weak.
15 Sensory Perception 3. Slightly Limited Responds to verbal commands, but cannot always communicate discomfort or the need to be turned. OR Has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities. This is the patient that is weak, has had a stroke and affects extremities, or diabetic patient with neuropathy.
16 Sensory Perception 4. No Impairment Responds to verbal commands. Has no sensory deficit which would limit ability to feel or voice pain or discomfort.
17 Moisture Degree to which skin is exposed to moisture. This is based on linen change. 1. Constantly Moist Skin is kept moist almost constantly by perspiration, urine, etc. Dampness is detected every time patient is moved or turned. This is the patient that is febrile, post menopausal, obese, and third spacing. The sheets could be changed each time the patient is moved or turned.
18 Moisture 2. Very Moist Skin is often, but not always moist. Linen must be changed at least once a shift. Despite patient or family members objections, linen may need to be changed more often than only during bath time. Please provide patient education as to the rationale for maintaining dry linen.
19 Moisture 3. Occasionally Moist Skin is occasionally moist, requiring an extra linen change approximately once a day. This extra linen may be done on either shift. This is part of communication SBARR and Nurse to Nursing assistant collaboration. If extra linen changes are not communicated, the Braden scale will be scored incorrectly.
20 Moisture 4. Rarely Moist Skin is usually dry, linen only requires changing at routine intervals. Look on the communication board in your patients room to see when the patient prefers to have their linen changed. When linens changed, update white board.
21 Activity Degree of physical activity 1. Bedfast - Confined to bed Immobility is what leads to pressure that deprives an area of it's blood supply and that this is the underlying cause of a pressure ulcer. This patient might be comatose, in traction, and contracted.
22 Activity 2. Chairfast Ability to walk severely limited or non-existent. Cannot bear weight and/or must be assisted into the chair or wheelchair. This patient is total care or one that you sit on the side of the bed have the chair next to the bed pivot and place in the chair.
23 Activity 3. Walks Occasionally Walks occasionally during the day, but for very short distances, with or without assistance. Spends majority of each shift in bed or chair. This patient might only walk in the room or to the bathroom.
24 Activity 4. Walks Frequently Walks outside room at least twice a day and inside room at least once every two (2) hours during waking hours. The patient is walking without assistance. Please take note of the frequency and where the patient is walking.
25 Mobility Ability to change and control body position. 1. Completely Immobile Does not make even slight changes in body or extremity position without assistance. This is the quadriplegic patient or the patient in a vegetative state.
26 Mobility 2. Very Limited Makes occasional slight changes in body or extremity position but unable to make frequent or significant changes independently. This is the paraplegic patient, the patient who is weak, or the patient that has just had a stroke and has not learned the use of the non affected extremity to pull the affected extremity and turn.
27 Mobility 3. Slightly Limited Makes frequent though slight changes in body or extremity position independently. 4. No Limitation Makes major and frequent changes in position without assistance.
28 Nutrition Usual food intake pattern. 1. Very Poor Never eats a complete meal. Rarely eats more than 1/3 of any food offered. Eats 2 servings or less of protein (meat or dairy products) per day. Takes fluids poorly. Does not take a liquid dietary supplement. OR Is NPO and/or maintained on clear liquids or IV s for more than 5 days
29 Nutrition 2. Probably Inadequate Rarely eats a complete meal and generally eats only about ½ of any food offered. Protein intake includes only 3 servings of meat or dairy products per day. Occasionally will take a dietary supplement. OR Receives less than optimum amount of liquid diet or tube feeding.
30 Nutrition 3. Adequate Eats over half of most meals. Eats a total of 4 servings of protein (meat, dairy products) per day. Occasionally will refuse a meal, but will usually take a supplement when offered. OR Is on a tube feeding or TPN regimen which probably meets most nutritional needs.
31 Nutrition 4. Excellent Eats most of every meal. Never refuses a meal. Usually eats a total of 4 or more servings of meat and dairy products. Occasionally eats between meals. Does not require supplementation.
32 Friction and Shear 1. Problem Requires moderate to maximum assistance in moving. Complete lifting without sliding against sheets is impossible. Frequently slides down in the bed or chair, requiring frequent repositioning with maximum assistance. Spasticity, contractures or agitation leads to almost constant friction.
33 Friction and Shear 2. Potential Problem Moves feebly or requires minimum assistance. During move skin probably slides to some extent against sheets, chair, restraints or other devices. Maintains relatively good position in chair or bed most of the time but occasionally slides down.
34 Friction and Shear 3. No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move. Maintains good position in bed or chair.
35 Score Interpretation At Risk Moderate Risk High Risk 9 or below Very High Risk Score of 16 or below: initiate the skin breakdown prevention orders
36 Daily skin inspection is vital Note red areas Initiate interventions Head to toe skin inspection takes roughly 4 minutes Are your patients worth it?
37 Interventions Objective: Discuss interventions to reduce patient's risk of skin breakdown
38 Mobility/Activity/Sensory Establish Turning Schedule Avoid positioning on trochanter HOB elevated no more than 30 o Elevate knee gatch Float heels off of bed If pillows used, place under calves do not use towel or blanket rolls, this puts extra pressure on the back of the calf and Achilles tendon
39 Moisture (Incontinence) Clean with approved perineal cleanser after each episode of incontinence Apply protective ointment after each episode of bowel/bladder incontinence Use only 1 polymer pads On Clinitron & Envision beds only 1 draw sheet and 1 blue care pad, extra linen defeats the purpose of the bed, no air flow Do not use diapers! Use external urine collection device (if needed/applicable)

40 Moisture (Incontinence) Guidelines for Use of Patient Under pads Blue Procedure Pad Use to protect surfaces during procedures such as dressing changes, blood draws, clean-up, labor & delivery or draining wounds covered with a dressing. Updated 6/17/13

41 Moisture (Incontinence) Green Underpad Use to protect surfaces from drainage/body fluids if patient is not at risk for skin breakdown. Place one pad only under patient. Do not stack pads. Updated 6/17/13

42 Moisture (Incontinence) Ultrasorbs AP White Under pad Use to protect patient s skin from drainage/body fluids if patient is at risk for skin breakdown and needs assistance to move. Pad draws moisture away from the skin and feels dry to the touch in minutes. Use with low air loss mattress therapy- protects the bedding and permits air flow (clinitron,p500) Place one pad under the patient. Do not stack pads under the patient. Updated 6/17/13
43 Fecal Incontinence Collector Use fecal incontinence appliance (if applicable) REMEMBER the Fecal Incontinence Collector Does Not require a MD/DO/PA/NP order.
44 Flexi Seal Flexi Seal is a fecal management system. Use of this device REQUIRES a MD/DO/PA/NP Order. This is not optional one cannot place this device at anytime without the order. So one cannot place this during the night with the intent of getting the order in the morning.
45 Friction The rubbing of the skin on the surface due to the slide down, or repetitive movements (like restless legs), or incomplete lifting of the body when being pulled up in the bed dragging instead of lifting.
46 Shear Great definition: A mechanical force that acts parallel rather than perpendicular. The skin is moist, sticks to the sheets, while the skeleton slides down inside the skin. The blood vessels can then be stretched or torn causing ischemia to the tissue.
47 What causes a patient to slide down in the bed??? Head of the bed > 30 degrees!!
48 Friction and Shear Protective ointment daily on all bony prominences Transparent dressing, hydrocolloid or silicone foam on bony prominences Moisturize skin after bathing Turning sheet Heel and elbow protectors as needed Remove every shift to assess When patient is OOB: Use a chair pad Elevate legs 90 o to hip
49 On a side note: Partial-thickness tissue loss is skin only. No granulation tissue formation; heals by resurfacing, so NO SCAR FORMATION. Full-thickness tissue loss is tissue damage past the skin; sub-q, fascia, muscle, tendon, or bone involved. Heals by remodeling / granulation, so SCAR IS FORMED.
50 Nutrition Dietary consult Increase protein intake Increase calorie intake Vitamin supplements Assist at mealtimes
51 To Find the Wound Nurse Consult Note: In Valley Link, look under patient record. On left side of screen use drop down box; go to Wound Nurse evaluation. Click on Comments and assessment.
52 Pressure Ulcers Objective Identify pressure ulcers according to NPUAP staging system
53 Staging Pressure ulcers Pressure ulcers are staged according to the level of tissue destruction / damage. There are 6 stages: Stage I-IV, Unstageable and Suspected Deep Tissue Injury. Only pressure ulcers are staged!!!

54 Incontinence Associated Dermatitis: Red, broken skin from moisture, heat (diapers)
55 Pressure Ulcer A pressure ulcer is a localized injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure or pressure in combination with shear and/or friction.
56 Stage I Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching: its color may differ from the surrounding area.
57 Stage 1 Description Stage 1 may be difficult to detect in individuals with dark skin tones. May be painful, firm, soft, warmer, or cooler than adjacent tissue. May indicate at risk persons.

58 Stage 1 pressure Ulcer Copyright Medline, 2007 used with permission

59 Stage 1 pressure Ulcer

60 What Do You See? Stage I: intact nonblanchable red skin Location-bilat heels, ankles Drainage none( color and amount) ( no drainage) Odor- none Surrounding tissue- WDL
61 Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure and/or shear.
62 Deep Tissue Injury- DTI DTI may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler than adjacent tissue. May be difficult to detect in individuals with dark skin tones. May begin as thin blister over dark wound bed. May rapidly expose additional layers of tissue even with optimal treatment.

63 Deep Tissue Injury
64 Deep Tissue Injury
65 What Do You See? Wound bed- purple/red blood filled blister Drainage- none Odor- None Surrounding tissueintact but red Location Top of left foot Wound bed Intact, nonblanchable purple tissue Drainage none Odor none Surrounding tissue WDL
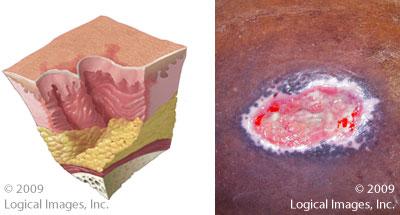
66 Stage 2 Pressure Ulcer Partial thickness loss of dermis presenting as a shallow open ulcer with a red or pink wound bed, without slough. May also present as an intact or open/ruptured serum filled blister. NO SCAR FORMATION!!
67 Stage 2 DO NOT use to describe: Skin tears Tape burns Perineal dermatitis Maceration or denudation

68 Stage 2

69 Stage 2
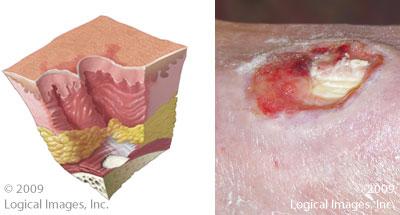
70 Stage 3
71 Stage 3 Pressure Ulcers Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present, but does not obscure the depth of tissue loss. Full thickness tissue loss.
72 Stage 3 Pressure Ulcers The depth of a Stage 3 pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have (adipose) subcutaneous tissue and stage 3 ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep stage 3 pressure ulcers. Bone/tendon is not visible or directly palpable.

73 Stage 3

74 What do You See? Location left heel Wound bed color Beefy red, minimal tan slough Drainage serosanguinous Odor None Surrounding tissue Scarring from larger wound, thick wound edges, thick skin
75 Stage 4
76 Stage 4 Full thickness tissue loss with exposed bone, tendon, joint or muscle. Slough or eschar may be present on some parts of the wound bed, often include undermining and tunneling.
77 Stage 4 The depth of a Stage 4 pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have adipose tissue and these ulcers can be shallow. Do not mistake them for Stage 2 or 3 pressure ulcers. Stage 4 ulcers can extend into muscle and/or supporting structures i.e., fascia, tendon or joint capsule making osteomyelitis likely to occur. Exposed bone/tendon is visible or directly palpable.

78 Stage 4

79 Stage 4

80 What Do You See? Location Sacrum Wound bed 90% red, 10% yellow / tan / grey Full thickness tissue loss with palpable bone Drainage Moderate amount of serosanguinous Odor Musty Surrounding tissue Intact, dry
81 Unstageable Full thickness tissue loss in which the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black). Unable to view wound bed (Not enough wound tissue is exposed to reveal the actual depth of tissue damage).
82 Unstageable Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and therefore stage, cannot be determined. Stable (dry, adherent, intact without erythema or fluctuance) eschar on the heels serves as "the body's natural (biological) cover" and should not be removed.

83 Unstageable

84 Unstageable
85 Unstagable
86 What Do You See? Location Right heel Wound bed Dry, black eschar ( unstageable pressure ulcer) Drainage None Odor? Surrounding tissue Pink/red
87 Wounds Unlocking the Secrets Objective: Discuss essential factors for a comprehensive wound assessment
88 Why do YOU Need to Know? Every nurse will encounter some kind of wound Chronic, trauma, surgical Nurses must know how to accurately assess a wound.
89 Why do YOU Need to Know? Systemic factors affect wound healing Comprehensive assessment on all patients: Age Body type Chronic disease Nutritional status Vascular insufficiencies Immunosuppression Radiation therapy
90 Wound Assessment - Etiology Understanding cause 1 st step in treatment Venous stasis ulcer Pressure ulcer Other causes
91 Wound Assessment - Infection Signs and symptoms of infection redness purulent drainage increased edema foul odor only after wound has been cleaned increased pain systemic temperature < 96.8 or> 100.4
92 Wound Assessment - Location Use anatomical terminology Be as precise as possible Identify by underlying bony prominence Ex: buttock wound = ischial wound Other terminology - Medial, lateral, proximal, superior, inferior
93 Wound Assessment Wound Bed Accurate assessment imperative for dressing/treatment selection. Color and type of wound tissue. Granulation tissue- living tissue presents as beefy red (granular). Non-granular tissue- living tissue presents as pale red or pink (slick).
94 Wound Assessment Wound Bed Non-viable or necrotic (dead) tissue Slough yellow, tan or grey often slimy or moist May be firm or loose and stringy Eschar Hard, leathery may be dark brown or black Do not mistake for a scab

95 Granular Tissue

96 Red / Pink non-granular tissue

97 Slough
98 What do you see? Location L buttock Wound bed- 30% yellow, nonviable tissue, 70 % pink Drainagemoderate amount serosanguinous drainage Odor- none Surrounding tissue-red, denuded skin from wet 4x4 gauze dsg

99 Eschar
100 Wound Bed Documentation Type of tissue within the wound bed in percentages totaling 100%. Example: 80% granulation tissue in the center of the wound bed with 20% yellow stringy slough on outer edges.
101 Wound Assessment Odor Various dressings may create foul odor as they absorb drainage Clean wound BEFORE assessing odor Foul odor may indicate infection - report to MD/DO
102 Wound Assessment Drainage Made up of dead cells liquefied necrotic tissue white blood cells natural growth factors Assess amount, type, color, odor and consistency
103 Wound Assessment Drainage Amount - small, moderate or heavy Note how long dressing was in place saturated after 12 hours vs. saturated after 2 days. drainage may indicate bioburden/ infection- report to MD/DO/PA/NP
104 Wound Assessment -Periwound Skin condition around wound is good indicator of wound healing. Use clock method to describe position Maceration- skin too moist. Can cause further breakdown Redness 3-5cm beyond wound edges may indicate cellulitis.

105 Possible Cellulitis Copyright Medline, 2007 used with permission
106 Wound Assessment -Periwound Assess color sensation induration edema Hyperkeratosis- hard, white/grey tissue Epithelialization- flat, pale white, pink/lavender, dry, shiny skin

107 Epithelialization

108 Epithelialization
109 Wound Undermining & Tunneling Undermining- Tissue destruction underlying intact skin along the margins of a wound. Undermining can travel in more that one direction. (think of swishing your tongue over your teeth under your lip) Tunneling/Sinus Tract- A canal or passage under the wound surface that travels in one direction. (think of sticking your finger up your nose)
110 Wound Assessment- Pain Assess for & relieve causes/contributors to pain: Pain medication is needed with wounds. Edema Swelling Inflammation Infection Dressing changes Adhesives Dry wound beds Debridement Always give pain medication prior to dressing changes.
111 Wound Assessment- Documentation Essential to: Paint a picture - The next provider will know what the wound looks like before removing the dressing by your documentation. Communication - Among the health care team - SBARR
112 Wound Assessment- Documentation Plan care plan of care includes interventions. Change these interventions as necessary Remember this is a legal record; if the assessment or interventions are not documented, they were not done. Completed in a timely, concise, and accurate manner
113 References National Pressure Ulcer Advisory Panel Update Hess, Cathy Thomas. Clinical Guide to Wound Care, 6 th ed. Wolters-Kluwer, www. Braden scale.com.
114 References Bryant, Ruth. Acute and Chronic Wounds, 3 rd ed. St. Louis: Mosby, Medline Industries Inc. The Wound Care Handbook. Mundelin, IL: Medline Industries, Handout from presentation by Lori McNicole RN, BSN, CWOCN, 2005.
Advanced Clinical Solutions. Pressure Ulcer. Carilex Medical Group 1
 Advanced Clinical Solutions Pressure Ulcer Carilex Medical Group 1 Advanced Clinical Solutions Contents About Pressure Ulcer! 2 Stages of Pressure Ulcer! 5 Reference! 7 Carilex Medical Group 1 About Pressure
Advanced Clinical Solutions Pressure Ulcer Carilex Medical Group 1 Advanced Clinical Solutions Contents About Pressure Ulcer! 2 Stages of Pressure Ulcer! 5 Reference! 7 Carilex Medical Group 1 About Pressure
Pressure Ulcer Staging. Staging of Wounds are based on the deepest level of tissue damage
 Pressure Ulcer Staging Staging of Wounds are based on the deepest level of tissue damage Pressure Ulcer Staging New Pressure Ulcer Staging Stage I Stage II Stage III Stage IV Unstageable Suspected Deep
Pressure Ulcer Staging Staging of Wounds are based on the deepest level of tissue damage Pressure Ulcer Staging New Pressure Ulcer Staging Stage I Stage II Stage III Stage IV Unstageable Suspected Deep
Pressure Ulcer Staging and Documentation. Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center
 Pressure Ulcer Staging and Documentation Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center Overview of the Pressure Ulcer Problem Scope Over 1 million cases each year, 1 in 4 patients Cost In acute
Pressure Ulcer Staging and Documentation Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center Overview of the Pressure Ulcer Problem Scope Over 1 million cases each year, 1 in 4 patients Cost In acute
The Importance of Skin Examination. following Spinal Cord Injury
 The Importance of Skin Examination following Spinal Cord Injury An individual who sustains a spinal cord injury (SCI) has a lifetime of increased susceptibility to skin problems, including pressure ulcers
The Importance of Skin Examination following Spinal Cord Injury An individual who sustains a spinal cord injury (SCI) has a lifetime of increased susceptibility to skin problems, including pressure ulcers
Pressure Ulcer. Patient information leaflet. Category I. Category II. Category III. Category IV. Unstageable. Deep Tissue Injury
 Pressure Ulcers Patient information leaflet Pressure Ulcer Category I Category II Category III Category IV Unstageable Deep Tissue Injury Introduction This leaflet is about pressure ulcers and includes
Pressure Ulcers Patient information leaflet Pressure Ulcer Category I Category II Category III Category IV Unstageable Deep Tissue Injury Introduction This leaflet is about pressure ulcers and includes
Wound Jeopardy: Name That Wound Session 142 Saturday, September 10 th 2011
 Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology. Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP
 Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP Objectives Understand updated definitions as well as staging and classification
Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP Objectives Understand updated definitions as well as staging and classification
Acute and Chronic WOUND ASSESSMENT. Wound Assessment OBJECTIVES ITEMS TO CONSIDER
 WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
Pressure Injury Definition and Stages
 Program Objective Pressure Injury Definition and Stages Identify the changes to the 2016 NPUAP staging system Changes to the Staging System in 2016 2 Anatomy of the Skin Anatomy of the Skin Largest organ
Program Objective Pressure Injury Definition and Stages Identify the changes to the 2016 NPUAP staging system Changes to the Staging System in 2016 2 Anatomy of the Skin Anatomy of the Skin Largest organ
Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell
 Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell Objectives Identify the stages of pressure ulcer according to the depth of tissue destruction. Discuss the differences
Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell Objectives Identify the stages of pressure ulcer according to the depth of tissue destruction. Discuss the differences
Recognizing Pressure Injury
 Recognizing Pressure Injury Karen Zulkowski, DNS, RN Hawaii Recorded on March 8, 2017 1 A Little About Myself Executive editor of the Journal of the World Council of Enterostomal Therapists (JWCET) and
Recognizing Pressure Injury Karen Zulkowski, DNS, RN Hawaii Recorded on March 8, 2017 1 A Little About Myself Executive editor of the Journal of the World Council of Enterostomal Therapists (JWCET) and
Pressure Injury Staging Update 2016
 Pressure Injury Staging Update 2016 A Review of the New Changes for Pressure Injury Documentation and Staging Jeanne Terefenko, BSN, RN, CWOCN Ext. 5855 Pressure Ulcer Staging Updates: In April, 2016,
Pressure Injury Staging Update 2016 A Review of the New Changes for Pressure Injury Documentation and Staging Jeanne Terefenko, BSN, RN, CWOCN Ext. 5855 Pressure Ulcer Staging Updates: In April, 2016,
SECTION M: SKIN CONDITIONS. M0210: Unhealed Pressure Ulcer(s) Item Rationale
 Item Rationale") SECTION M: SKIN CONDITIONS Intent: The items in this section of the April 1, 2014 release of the LTCH CARE Data Set Version 2.01 document the presence, appearance, and change of pressure ulcers. If warranted
SECTION M: SKIN CONDITIONS Intent: The items in this section of the April 1, 2014 release of the LTCH CARE Data Set Version 2.01 document the presence, appearance, and change of pressure ulcers. If warranted
Objectives. Major Changes to Section M. MDS 3.0 Section M Pressure Ulcers. Risk assessment Introduction of NPUAP guidelines
 MDS 3.0 Section M Pressure Ulcers Moderator: Barbara Baylis Sr. VP of Clinical and Residential Services, Kindred Healthcare Presenter: Glenda Mack, Sr. Director of Clinical Operations, Peoplefirst Rehabilitation
MDS 3.0 Section M Pressure Ulcers Moderator: Barbara Baylis Sr. VP of Clinical and Residential Services, Kindred Healthcare Presenter: Glenda Mack, Sr. Director of Clinical Operations, Peoplefirst Rehabilitation
Wound Care Program for Nursing Assistants-
 Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
2 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?)
") Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Ann Rambusch, MSN, HCS D, HCS O, RN June 28, 2016 1 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Understanding NPUAP
Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Ann Rambusch, MSN, HCS D, HCS O, RN June 28, 2016 1 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Understanding NPUAP
Objectives are included in the participant handout and include the detail for the last objective: Describe a pressure ulcer prevention program for a
 1 Objectives are included in the participant handout and include the detail for the last objective: Describe a pressure ulcer prevention program for a nursing home, including: Education of residents, staff
1 Objectives are included in the participant handout and include the detail for the last objective: Describe a pressure ulcer prevention program for a nursing home, including: Education of residents, staff
Treat the whole patient, not just the hole in the patient! 3/21/2017 CAN YOU CONNECT THE DOTS?? PHILOSOPHY OBJECTIVES
 CAN YOU CONNECT THE DOTS?? Boone Hospital Wound Healing Center Kimberly Jamison, MD, FACP, FAPWCA, PCWC Kim Mitchell, RN, BSN OBJECTIVES Describe the basic concepts of chronic wound care to ensure an optimal
CAN YOU CONNECT THE DOTS?? Boone Hospital Wound Healing Center Kimberly Jamison, MD, FACP, FAPWCA, PCWC Kim Mitchell, RN, BSN OBJECTIVES Describe the basic concepts of chronic wound care to ensure an optimal
Negative Pressure Wound Therapy
 Origination: 6/29/04 Revised: 8/24/16 Annual Review: 11/10/16 Purpose: To provide Negative Pressure Wound Therapy (wound care treatment) guidelines for the Medical Department staff to reference when making
Origination: 6/29/04 Revised: 8/24/16 Annual Review: 11/10/16 Purpose: To provide Negative Pressure Wound Therapy (wound care treatment) guidelines for the Medical Department staff to reference when making
Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification
: NPUAP Terminology and Staging Clarification") Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification We encourage you to share this information with your staff and colleagues by facilitating clinician
Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification We encourage you to share this information with your staff and colleagues by facilitating clinician
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Knowledge Checkup Module 2 Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup Module
Pressure Ulcers ecourse Knowledge Checkup Module 2 Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup Module
Stop The Pressure: Patient Safety and Tissue Viability
 Portsmouth Hospitals NHS Trust Stop The Pressure: Patient Safety and Tissue Viability Alison Cole Claire Brett Karen Oakley Presentation Focus Etiology and cause of a pressure ulcer The impact of pressure
Portsmouth Hospitals NHS Trust Stop The Pressure: Patient Safety and Tissue Viability Alison Cole Claire Brett Karen Oakley Presentation Focus Etiology and cause of a pressure ulcer The impact of pressure
Pressure Ulcers Memory Aid
 Pressure Ulcers Memory Aid Pocket Guide This pocket guide is intended as a memory aid at the bedside. For more complete information on pressure ulcers, please refer to the Ferris-sponsored Pressure Ulcer
Pressure Ulcers Memory Aid Pocket Guide This pocket guide is intended as a memory aid at the bedside. For more complete information on pressure ulcers, please refer to the Ferris-sponsored Pressure Ulcer
If both a standardized, validated screening tool and an evaluation of clinical factors are utilized, select Response 2.
 (M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers? 0 - No assessment conducted [Go to M1306 ] 1 - Yes, based on an evaluation of clinical factors (for
(M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers? 0 - No assessment conducted [Go to M1306 ] 1 - Yes, based on an evaluation of clinical factors (for
E-learning module: Stages of pressure injuries. Disclaimer
 E-learning module: Stages of pressure injuries 1 Disclaimer Classification of pressure injuries The International Pressure Injury Category System (2009) was developed by:! the National Pressure Ulcer Advisory
E-learning module: Stages of pressure injuries 1 Disclaimer Classification of pressure injuries The International Pressure Injury Category System (2009) was developed by:! the National Pressure Ulcer Advisory
New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries
 New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries Janet Cuddigan, PhD, RN, CWCN, FAAN Professor, UNMC College of Nursing Omaha, NE Focus of this Presentation New developments
New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries Janet Cuddigan, PhD, RN, CWCN, FAAN Professor, UNMC College of Nursing Omaha, NE Focus of this Presentation New developments
(Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.)
") (Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.) (Fades to next slide titled Pressure Ulcer Staging. *Video contains Graphic Imagery is noted
(Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.) (Fades to next slide titled Pressure Ulcer Staging. *Video contains Graphic Imagery is noted
Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre.
 Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre. What does skin do? 1. It protects you. 2. It provides sensory information. 3. It helps
Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre. What does skin do? 1. It protects you. 2. It provides sensory information. 3. It helps
OASIS NP August 2011: Special Training. OASIS-C Integument Assessment. Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute
 OASIS NP August 211: Special Training OASIS-C Integument Assessment Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute 243 King Street, Suite 246 Northampton, MA 16 413-584-53
OASIS NP August 211: Special Training OASIS-C Integument Assessment Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute 243 King Street, Suite 246 Northampton, MA 16 413-584-53
PRESSURE ULCERS SIMPLIFIED
 10 PRESSURE ULCERS SIMPLIFIED This leaflet is intended to give you information and answers to some question you may have around pressure ulcers PRESSURE ULCERS SIMPLIFIED Pressure ulcer development has
10 PRESSURE ULCERS SIMPLIFIED This leaflet is intended to give you information and answers to some question you may have around pressure ulcers PRESSURE ULCERS SIMPLIFIED Pressure ulcer development has
Skin Integrity and Wound Care
 Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Beyond the Basics ImprovingYour Wound Care Knowledge. Berna Goldentyer RN, BSN, CWOCN Kathy Hugen RN, BSN, CWOCN
 Beyond the Basics ImprovingYour Wound Care Knowledge Berna Goldentyer RN, BSN, CWOCN Kathy Hugen RN, BSN, CWOCN Projects and Posters These resources were developed by creative VA nurses who had no special
Beyond the Basics ImprovingYour Wound Care Knowledge Berna Goldentyer RN, BSN, CWOCN Kathy Hugen RN, BSN, CWOCN Projects and Posters These resources were developed by creative VA nurses who had no special
C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME?
 M D S A N D P R E S S U R E U L C E R S C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME? 1777: decubitus is the oldest term used 1942
M D S A N D P R E S S U R E U L C E R S C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME? 1777: decubitus is the oldest term used 1942
ד"ר בוריס פונצ' קי PRESSURE ULCERS
 ד"ר בוריס פונצ' קי 25.12.2013 PRESSURE ULCERS International EPUAP-NPUAP Pressure Ulcer Definition: (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2010).. is localized
ד"ר בוריס פונצ' קי 25.12.2013 PRESSURE ULCERS International EPUAP-NPUAP Pressure Ulcer Definition: (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2010).. is localized
Wound Care Assessment in the Home Care Setting
 Wound Care Assessment in the Home Care Setting Lynn Peterson, RN, BSN, CWOCN Technical Service Specialist 3M Health Care Wednesday, May 14, 2008 Objectives Describe essential elements of a wound assessment
Wound Care Assessment in the Home Care Setting Lynn Peterson, RN, BSN, CWOCN Technical Service Specialist 3M Health Care Wednesday, May 14, 2008 Objectives Describe essential elements of a wound assessment
Assisted Living Resident Assessment (To be used when yes is indicated for skin issues under Section 5 of Assisted Living Resident Assessment)
") Skin Assessment Current open skin areas: Yes No Current pressure ulcer: Yes No A. Stage 1 Ulcers Report based on highest stage of existing ulcers at its worst; do not reverse stage. Number of existing
Skin Assessment Current open skin areas: Yes No Current pressure ulcer: Yes No A. Stage 1 Ulcers Report based on highest stage of existing ulcers at its worst; do not reverse stage. Number of existing
Critically Assessing Pressure Injuries
 Critically Assessing Injuries Copyright 2016 Gordian Medical, Inc. dba American Medical Technologies. LeadingAge Indiana presents FACULTY PAMELA SCARBOROUGH PT, DPT, CDE, CWS DIRECTOR OF PUBLIC POLICY
Critically Assessing Injuries Copyright 2016 Gordian Medical, Inc. dba American Medical Technologies. LeadingAge Indiana presents FACULTY PAMELA SCARBOROUGH PT, DPT, CDE, CWS DIRECTOR OF PUBLIC POLICY
Differentiating Incontinence Associated Dermatitis from Category/Stage II Pressure Ulcers
 Differentiating Incontinence Associated Dermatitis from Category/Stage II Pressure Ulcers Suzanne Collins, MS BSN RN CWOCN Mid Atlantic Region Clinical Specialist Mölnlycke Health Care 1 Pre-Test: 1. What
Differentiating Incontinence Associated Dermatitis from Category/Stage II Pressure Ulcers Suzanne Collins, MS BSN RN CWOCN Mid Atlantic Region Clinical Specialist Mölnlycke Health Care 1 Pre-Test: 1. What
Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again
 Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again October 4 th, 2017 Ryan P. Dirks PA-C Founder and CEO Road to success Detailed Wound Assessment/Risk Assessment External Support Individualized
Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again October 4 th, 2017 Ryan P. Dirks PA-C Founder and CEO Road to success Detailed Wound Assessment/Risk Assessment External Support Individualized
Pressure Ulcers in the Developmentally Disabled Arizona Department of Economic Security Division of Developmental Disabilities
 Pressure Ulcers in the Developmentally Disabled Arizona Department of Economic Security Division of Developmental Disabilities Compiled by Nancy Braden MD, Medical Director, Mercy Care Plan 1 PRESSURE
Pressure Ulcers in the Developmentally Disabled Arizona Department of Economic Security Division of Developmental Disabilities Compiled by Nancy Braden MD, Medical Director, Mercy Care Plan 1 PRESSURE
Pressure Ulcer Prevention for OR. Jeanne Knecht RN, CWON Wound/Ostomy Specialist
 Pressure Ulcer Prevention for OR Jeanne Knecht RN, CWON Wound/Ostomy Specialist Benefis Hospital Stats 2009 12 month incident rate 1.90 Benefis Benchmark 3 National Benchmark 5-8 How did we achieve Education
Pressure Ulcer Prevention for OR Jeanne Knecht RN, CWON Wound/Ostomy Specialist Benefis Hospital Stats 2009 12 month incident rate 1.90 Benefis Benchmark 3 National Benchmark 5-8 How did we achieve Education
Braden Scale For Predicting Pressure Sore Risk
 Braden Scale For Predicting Pressure Sore Risk How to use the Braden scale Each patient is assessed for the following risk factors: Sensory Perception Moisture Activity Mobility Nutrition Friction and
Braden Scale For Predicting Pressure Sore Risk How to use the Braden scale Each patient is assessed for the following risk factors: Sensory Perception Moisture Activity Mobility Nutrition Friction and
Consider the possibility of pressure ulcer development
 Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Durable Medical Equipment Providers
 August 2009 Provider Bulletin Number 974 Durable Medical Equipment Providers Vacuum Assisted Wound Closure Therapy Negative pressure wound therapy (NPWT) must be requested and supplied by an enrolled durable
August 2009 Provider Bulletin Number 974 Durable Medical Equipment Providers Vacuum Assisted Wound Closure Therapy Negative pressure wound therapy (NPWT) must be requested and supplied by an enrolled durable
Pathway to excellence. A comprehensive clinical education platform from Smith & Nephew
 Pathway to excellence A comprehensive clinical education platform from Smith & Nephew Pathway to Excellence Support Each year, we train more than 150,000 healthcare professional around the globe. In addition
Pathway to excellence A comprehensive clinical education platform from Smith & Nephew Pathway to Excellence Support Each year, we train more than 150,000 healthcare professional around the globe. In addition
Ann Leland, APRN, CNP, DNP Instructor, college of surgery
 Ann Leland, APRN, CNP, DNP Instructor, college of surgery leland.ann@mayo.edu 2015 MFMER 3543652-1 Pressure ulcers Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for NPs
Ann Leland, APRN, CNP, DNP Instructor, college of surgery leland.ann@mayo.edu 2015 MFMER 3543652-1 Pressure ulcers Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for NPs
Successful Wound Management Strategies : An Introduction. Alex Khan, APRN ACNS-BC. Organization of Wound Care Nurses
 Successful Wound Management Strategies : An Introduction Alex Khan, APRN ACNS-BC Organization of Wound Care Nurses www.woundcarenurses.org Goals & Objectives The role and importance of wound care management
Successful Wound Management Strategies : An Introduction Alex Khan, APRN ACNS-BC Organization of Wound Care Nurses www.woundcarenurses.org Goals & Objectives The role and importance of wound care management
WOUND CARE. By Laural Aiesi, RN, BSN Alina Kisiel RN, BSN Summit ElderCare
 WOUND CARE By Laural Aiesi, RN, BSN Alina Kisiel RN, BSN Summit ElderCare PRESSURE ULCER DIABETIC FOOT ULCER VENOUS ULCER ARTERIAL WOUND NEW OR WORSENING INCONTINENCE CHANGE IN MENTAL STATUS DECLINE IN
WOUND CARE By Laural Aiesi, RN, BSN Alina Kisiel RN, BSN Summit ElderCare PRESSURE ULCER DIABETIC FOOT ULCER VENOUS ULCER ARTERIAL WOUND NEW OR WORSENING INCONTINENCE CHANGE IN MENTAL STATUS DECLINE IN
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Module 4.1: Prevention of Pressure Ulcers Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module
Pressure Ulcers ecourse Module 4.1: Prevention of Pressure Ulcers Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Module
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa
 CENTRAL IOWA HEALTHCARE Marshalltown, Iowa ASSESSMENT OF PATIENTS POLICY & PROCEDURE Policy Number: 3.2 Subject: Purpose: Policy: Assessment And Treatment Of Skin Integrity Identification and treatment
CENTRAL IOWA HEALTHCARE Marshalltown, Iowa ASSESSMENT OF PATIENTS POLICY & PROCEDURE Policy Number: 3.2 Subject: Purpose: Policy: Assessment And Treatment Of Skin Integrity Identification and treatment
INSIDE. Stage II pressure ulcers are now
 Spring 2007, Volume 21 National Pressure Ulcer Advisory Panel the NPUAP In this issue President s Message NPUAP Award Honors CAC Member Profile: Healthpoint, Ltd. NPUAP Conferences Milestones Corporate
Spring 2007, Volume 21 National Pressure Ulcer Advisory Panel the NPUAP In this issue President s Message NPUAP Award Honors CAC Member Profile: Healthpoint, Ltd. NPUAP Conferences Milestones Corporate
Appropriate Dressing Selection For Treating Wounds
 Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
Pressure injury Prevention. Pressure injury staging and prevention. Etiology of a Pressure Injury
 Pressure injury staging and prevention Pressure injury Prevention Etiology of a Pressure Injury Pressure Shear Friction Moisture Etiology of a Pressure Injury Pressure Localized injury from ischemia that
Pressure injury staging and prevention Pressure injury Prevention Etiology of a Pressure Injury Pressure Shear Friction Moisture Etiology of a Pressure Injury Pressure Localized injury from ischemia that
Pressure Ulcer Management in Older Adults
 Pressure Ulcer Management in Older Adults Pressure Ulcer Caring for Seniors HIGHMARK.COM Objectives Identify Medicare Advantage members who are at risk for developing pressure ulcers Provide appropriate
Pressure Ulcer Management in Older Adults Pressure Ulcer Caring for Seniors HIGHMARK.COM Objectives Identify Medicare Advantage members who are at risk for developing pressure ulcers Provide appropriate
Wound Care per HHVNA Wound Product Formulary
 Venous Ulcers ABI of 0.9-1.2 = normal blood flow An ABI MUST be obtained prior to inititiation of compression therapy. Compression is the Gold Standard of care to promote wound of venous ulcers. Elevation
Venous Ulcers ABI of 0.9-1.2 = normal blood flow An ABI MUST be obtained prior to inititiation of compression therapy. Compression is the Gold Standard of care to promote wound of venous ulcers. Elevation
CARE GUIDE for Pressure Ulcers
 Prevention (1,3) Risk assessment should be performed in both the inpatient and outpatient setting Evaluate for susceptibility for pressure ulcer using a standardized tool such as the Braden Scale The Braden
Prevention (1,3) Risk assessment should be performed in both the inpatient and outpatient setting Evaluate for susceptibility for pressure ulcer using a standardized tool such as the Braden Scale The Braden
CLPNA Pressure Ulcers ecourse: Module 4 Quiz II page 1
 CLPNA Pressure Ulcers ecourse: Module 4 Quiz II 1. When are good times to do a skin inspection of a patient or resident? a. Bathing b. Meal times c. Dressing d. Assisting e. Sleeping 2. For patients who
CLPNA Pressure Ulcers ecourse: Module 4 Quiz II 1. When are good times to do a skin inspection of a patient or resident? a. Bathing b. Meal times c. Dressing d. Assisting e. Sleeping 2. For patients who
Prepared and Presented by: Ms. Sohad Noorsaeed, RN. MSN
 Prepared and Presented by: Ms. Sohad Noorsaeed, RN. MSN Learning Outcomes Upon the completion of Skin integrity lecture, the learners will be able to: 1. Describe factors affecting skin integrity. 2. Identify
Prepared and Presented by: Ms. Sohad Noorsaeed, RN. MSN Learning Outcomes Upon the completion of Skin integrity lecture, the learners will be able to: 1. Describe factors affecting skin integrity. 2. Identify
QUICK GUIDE PRESSURE ULCER PREVENTION FOR HEALTHCARE PROFESSIONALS
 QUICK GUIDE PRESSURE ULCER PREVENTION FOR HEALTHCARE PROFESSIONALS This booklet has been produced by Invacare for healthcare professionals working with individuals at risk of developing pressure ulcers.
QUICK GUIDE PRESSURE ULCER PREVENTION FOR HEALTHCARE PROFESSIONALS This booklet has been produced by Invacare for healthcare professionals working with individuals at risk of developing pressure ulcers.
Oregon Health Care Association Presents. F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care
 Oregon Health Care Association Presents F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care FACULTY: PAMELA SCARBOROUGH PT, DPT, MS, CWS, CEEAA DIRECTOR OF PUBLIC POLICY & EDUCATION
Oregon Health Care Association Presents F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care FACULTY: PAMELA SCARBOROUGH PT, DPT, MS, CWS, CEEAA DIRECTOR OF PUBLIC POLICY & EDUCATION
Pressure Ulcer Prevention and Management. Glenn Smith Clinical Nurse Specialist Nutrition and Tissue Viability
 Pressure Ulcer Prevention and Management Glenn Smith Clinical Nurse Specialist Nutrition and Tissue Viability Objectives An understanding of how pressure ulcers develop and what can be done to prevent
Pressure Ulcer Prevention and Management Glenn Smith Clinical Nurse Specialist Nutrition and Tissue Viability Objectives An understanding of how pressure ulcers develop and what can be done to prevent
Chapter 36 & 37. Types of wounds. Skin Tear
 Chapter 36 & 37 Wound Care and Pressure Ulcers Types of wounds A wound is a break in the skin d/t trauma, surgical incision, pressure sore, circulatory ulcers Abrasion, Contusion, Incision, Laceration,
Chapter 36 & 37 Wound Care and Pressure Ulcers Types of wounds A wound is a break in the skin d/t trauma, surgical incision, pressure sore, circulatory ulcers Abrasion, Contusion, Incision, Laceration,
Determining Wound Diagnosis and Documentation Tips Job Aid
 Determining Wound Diagnosis and Job Aid 1 Coding Is this a traumatic injury from an accident? 800 Codes - Injury Section of the Coding Manual Code by specific site of injury. Only use for accidents or
Determining Wound Diagnosis and Job Aid 1 Coding Is this a traumatic injury from an accident? 800 Codes - Injury Section of the Coding Manual Code by specific site of injury. Only use for accidents or
Promoting Skin Integrity in End of Life Care. Part 1. Tracey McKenzie Head of Tissue Viability Services TSDFT
 Promoting Skin Integrity in End of Life Care Part 1 Tracey McKenzie Head of Tissue Viability Services TSDFT To Understand the Extrinsic Factors of Pressure Ulcer (PU) development To understand the Intrinsic
Promoting Skin Integrity in End of Life Care Part 1 Tracey McKenzie Head of Tissue Viability Services TSDFT To Understand the Extrinsic Factors of Pressure Ulcer (PU) development To understand the Intrinsic
Pressure Ulcers Patient Information Leaflet
 Pressure Ulcers Patient Information Leaflet Shining a light on the future Introduction This leaflet is about pressure ulcers and includes information about what they are what can cause them and how they
Pressure Ulcers Patient Information Leaflet Shining a light on the future Introduction This leaflet is about pressure ulcers and includes information about what they are what can cause them and how they
Pressure Ulcers Patient Information Leaflet
 Further information about the content, reference sources or production of this leaflet can be obtained from the Patient Information Centre. Pressure Ulcers Patient Information Leaflet This information
Further information about the content, reference sources or production of this leaflet can be obtained from the Patient Information Centre. Pressure Ulcers Patient Information Leaflet This information
PATIENT CARE MANUAL POLICY
 PATIENT CARE MANUAL POLICY NUMBER #VII-F-20 PAGE 1 OF 2 APPROVED BY: CATEGORY: Senior Vice President, Medicine and Chief of Staff; Vice President and Senior Operating Officer, Covenant Health, Rural Health
PATIENT CARE MANUAL POLICY NUMBER #VII-F-20 PAGE 1 OF 2 APPROVED BY: CATEGORY: Senior Vice President, Medicine and Chief of Staff; Vice President and Senior Operating Officer, Covenant Health, Rural Health
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE
 CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE JOIE WHITNEY, PHD, RN, CWCN, FAAN PROFESSOR BIOBEHAVIORAL NURSING AND HEALTH SYSTEMS UNIVERSITY OF WASHINGTON HARBORVIEW ENDOWED PROFESSOR IN CRITICAL
CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE JOIE WHITNEY, PHD, RN, CWCN, FAAN PROFESSOR BIOBEHAVIORAL NURSING AND HEALTH SYSTEMS UNIVERSITY OF WASHINGTON HARBORVIEW ENDOWED PROFESSOR IN CRITICAL
Wound Care Evaluation by Kris Dalseg MS PT CWS CLT
 Wound Care Evaluation by Kris Dalseg MS PT CWS CLT This document is intended to describe a standard wound care evaluation for healthcare practitioners. In healthcare, all aspects of our treatment have
Wound Care Evaluation by Kris Dalseg MS PT CWS CLT This document is intended to describe a standard wound care evaluation for healthcare practitioners. In healthcare, all aspects of our treatment have
CRRN Review Course 2017 Skin and Wound Management. Presented by: Jenifer Stevenson BSN, CRRN, CNML
 CRRN Review Course 2017 Skin and Wound Management Presented by: Jenifer Stevenson BSN, CRRN, CNML Disclosure The presenter for this presentation has disclosed no conflict of interest related to this topic.
CRRN Review Course 2017 Skin and Wound Management Presented by: Jenifer Stevenson BSN, CRRN, CNML Disclosure The presenter for this presentation has disclosed no conflict of interest related to this topic.
COMPLETION PROJECT POSITIONING THE PATIENT IN THE OR Source- Alexander s Care of the Patient in Surgery
 COMPLETION PROJECT POSITIONING THE PATIENT IN THE OR Source- Alexander s Care of the Patient in Surgery Name Date 1. The systems involved with anesthesia, positioning and operative procedures are: a. b.
COMPLETION PROJECT POSITIONING THE PATIENT IN THE OR Source- Alexander s Care of the Patient in Surgery Name Date 1. The systems involved with anesthesia, positioning and operative procedures are: a. b.
Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians
 Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians Table of Contents Table of Contents... 2 Acknowledgments... 3 Introduction... 4 Purpose...
Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians Table of Contents Table of Contents... 2 Acknowledgments... 3 Introduction... 4 Purpose...
Skin matters Preventing Pressure Ulcers: a Guide for Patients and Carers
 Skin matters Preventing Pressure Ulcers: a Guide for Patients and Carers We recommend that you follow the advice within this leaflet and provided by your healthcare provider. However if anything changes
Skin matters Preventing Pressure Ulcers: a Guide for Patients and Carers We recommend that you follow the advice within this leaflet and provided by your healthcare provider. However if anything changes
Pressure Ulcer Prevention Guidelines
 EUROPEAN PRESSURE ULCER ADVISORY PANEL Pressure Ulcer Prevention Guidelines INTRODUCTION Pressure damage is common in many healthcare settings across Europe, affecting all age groups, and is costly both
EUROPEAN PRESSURE ULCER ADVISORY PANEL Pressure Ulcer Prevention Guidelines INTRODUCTION Pressure damage is common in many healthcare settings across Europe, affecting all age groups, and is costly both
SKIN INTEGRITY & WOUND CARE
 SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
Pressure ulcer recognition and prevention. Mark Collier Tissue Viability Nurse Consultant United Lincoln Hospitals NHS Trust
 Pressure ulcer recognition and prevention Mark Collier Tissue Viability Nurse Consultant United Lincoln Hospitals NHS Trust PRESSURE ULCER RECOGNITION AND PREVENTION.. United Lincolnshire Hospitals NHS
Pressure ulcer recognition and prevention Mark Collier Tissue Viability Nurse Consultant United Lincoln Hospitals NHS Trust PRESSURE ULCER RECOGNITION AND PREVENTION.. United Lincolnshire Hospitals NHS
Preventing Pressure Ulcers or Bed Sores
 Preventing Pressure Ulcers or Bed Sores Keeping Your Skin Healthy In the Hospital As partners in your care, this brochure will help you, your care givers and care helpers learn how to prevent pressure
Preventing Pressure Ulcers or Bed Sores Keeping Your Skin Healthy In the Hospital As partners in your care, this brochure will help you, your care givers and care helpers learn how to prevent pressure
Preventing Pressure Ulcers or Bed Sores
 Preventing Pressure Ulcers or Bed Sores Keeping Your Skin Healthy In the Hospital As partners in your care, this brochure will help you, your care givers and care helpers learn how to prevent pressure
Preventing Pressure Ulcers or Bed Sores Keeping Your Skin Healthy In the Hospital As partners in your care, this brochure will help you, your care givers and care helpers learn how to prevent pressure
CARE OF THE NEONATE: ITS ALL ABOUT THE SKIN. Katherine Kunkel, MSN, RNC-NIC, WCC
 CARE OF THE NEONATE: ITS ALL ABOUT THE SKIN Katherine Kunkel, MSN, RNC-NIC, WCC Learning Objectives Recognize what are risk factors for the neonate within the intensive care unit. Understand the physiology
CARE OF THE NEONATE: ITS ALL ABOUT THE SKIN Katherine Kunkel, MSN, RNC-NIC, WCC Learning Objectives Recognize what are risk factors for the neonate within the intensive care unit. Understand the physiology
Lower Extremity Venous Disease (LEVD)
") Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Welcome to NuMed! Our Commitment: Quality Products, Cost Savings, Exceptional Service
 It s a New Day in Wound Care Welcome to NuMed! Our Commitment: Quality Products, Cost Savings, Exceptional Service NuMed Industries is a manufacturing company that specializes in Advanced Wound Care products.
It s a New Day in Wound Care Welcome to NuMed! Our Commitment: Quality Products, Cost Savings, Exceptional Service NuMed Industries is a manufacturing company that specializes in Advanced Wound Care products.
Slide 1. Slide 2 Disclosures. Slide 3 Objectives. Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician
 Slide 1 Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician Slide 2 Disclosures Wound and Ostomy RN at St. Vincent Healthcare and Billings Clinic, Billings, MT Former employee of KCI, a division
Slide 1 Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician Slide 2 Disclosures Wound and Ostomy RN at St. Vincent Healthcare and Billings Clinic, Billings, MT Former employee of KCI, a division
See Policy CPT/HCPCS CODE section below for any prior authorization requirements
 Effective Date: 7/1/2018 Section: DME Policy No: 377 Medical Officer 7/1/18 Date Technology Assessment Committee Approved Date: 10/10; 10/13; 9/14: 9/15; 4/16 Medical Policy Committee Approved Date: 3/03;
Effective Date: 7/1/2018 Section: DME Policy No: 377 Medical Officer 7/1/18 Date Technology Assessment Committee Approved Date: 10/10; 10/13; 9/14: 9/15; 4/16 Medical Policy Committee Approved Date: 3/03;
WOUND MANAGEMENT. A Clinical Perspective. Furqan Alex Khan, APRN ACNS-BC MSN
 WOUND MANAGEMENT A Clinical Perspective Furqan Alex Khan, APRN ACNS-BC MSN alexkhan@prohealthcare.us Ket Harris Davis, APRN FNP-C DNP keturahnp@keturah-hms.com. Objectives Understand types of wounds Discuss
WOUND MANAGEMENT A Clinical Perspective Furqan Alex Khan, APRN ACNS-BC MSN alexkhan@prohealthcare.us Ket Harris Davis, APRN FNP-C DNP keturahnp@keturah-hms.com. Objectives Understand types of wounds Discuss
Palliative Care. EPUAP/NPUAP Publish New Pressure Ulcer Guidelines for. Treatment. Improving Quality of Care Based on CMS Guidelines 39
 Treatment EPUAP/NPUAP Publish New Pressure Ulcer Guidelines for Palliative Care Dealing with the end of a loved one s life is difficult enough, but when wound and skin care issues are involved, the decisions
Treatment EPUAP/NPUAP Publish New Pressure Ulcer Guidelines for Palliative Care Dealing with the end of a loved one s life is difficult enough, but when wound and skin care issues are involved, the decisions
Excellence in OASIS-C COS-C Prep & OASIS Training
 Excellence in OASIS-C COS-C Prep & OASIS Training Webinar Series - Session 5 April 2, 2014 2:00 3:00PM EST PRESENTER: JOAN L. USHER, BS, RHIA, COS-C, ACE JLU HEALTH RECORD SYSTEMS TEL: (781) 829-9632 FAX:
Excellence in OASIS-C COS-C Prep & OASIS Training Webinar Series - Session 5 April 2, 2014 2:00 3:00PM EST PRESENTER: JOAN L. USHER, BS, RHIA, COS-C, ACE JLU HEALTH RECORD SYSTEMS TEL: (781) 829-9632 FAX:
Pressure ulcers can develop in a relatively short time, therefore it is important to prevent them or notice and recognise early signs of damage.
 Preventing Pressure Damage A Guide for Patients and Carers What is pressure damage? A pressure ulcer, (previously often referred to as a bed sore or pressure sore ) is a localised area of damage to the
Preventing Pressure Damage A Guide for Patients and Carers What is pressure damage? A pressure ulcer, (previously often referred to as a bed sore or pressure sore ) is a localised area of damage to the
Prevention and management of Pressure ulcers
 Prevention and management of Pressure ulcers A guide for patients, carers and relatives What is a pressure ulcer? Pressure ulcers are an injury to the skin and/or underlying tissues. They are also known
Prevention and management of Pressure ulcers A guide for patients, carers and relatives What is a pressure ulcer? Pressure ulcers are an injury to the skin and/or underlying tissues. They are also known
Heel Pressure Ulcers: A to Z. Event ID:
 Heel Pressure Ulcers: A to Z Event ID: 192526 Q & A Dr. Diane Langemo: Thank you for tuning into the webinar and we will now address the questions that were submitted. We have many excellent questions.
Heel Pressure Ulcers: A to Z Event ID: 192526 Q & A Dr. Diane Langemo: Thank you for tuning into the webinar and we will now address the questions that were submitted. We have many excellent questions.
Wound Care for Hospice Patients
 Wound Care for Hospice Patients Kristen Lyn Brodrick, RN, BSN, CHPN,CWCN No financial disclosures. Unique Population Patients needing hospice/palliative care are often at risk for developing multiple skin
Wound Care for Hospice Patients Kristen Lyn Brodrick, RN, BSN, CHPN,CWCN No financial disclosures. Unique Population Patients needing hospice/palliative care are often at risk for developing multiple skin
Essential Elements of Pressure Ulcer Prevention & Management
 All Wales Tissue Viability Nurse Forum Fforwm Nyrsys Hyfywedd Meinwe Cymru Gyfan Essential Elements of Pressure Ulcer Prevention & Management All Wales Guidance for the Prevention & Management of Pressure
All Wales Tissue Viability Nurse Forum Fforwm Nyrsys Hyfywedd Meinwe Cymru Gyfan Essential Elements of Pressure Ulcer Prevention & Management All Wales Guidance for the Prevention & Management of Pressure
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Knowledge Checkup All Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup All Page
Pressure Ulcers ecourse Knowledge Checkup All Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup All Page
Update on Pressure Ulcers: Utilizing an Interdisciplinary Approach to Pressure Ulcer Prevention. Charlene A. Demers GNP-BC, CWOCN
 Update on Pressure Ulcers: Utilizing an Interdisciplinary Approach to Pressure Ulcer Prevention Charlene A. Demers GNP-BC, CWOCN Scope of the Issue Cost $9 billion to $11 billion $20,000-$150,000 per ulcer
Update on Pressure Ulcers: Utilizing an Interdisciplinary Approach to Pressure Ulcer Prevention Charlene A. Demers GNP-BC, CWOCN Scope of the Issue Cost $9 billion to $11 billion $20,000-$150,000 per ulcer
DMEPOS: hospital beds, bed accessories, and pressurereducing
 ACTION: Final DATE: 07/02/2018 10:03 AM 5160-10-18 DMEPOS: hospital beds, bed accessories, and pressurereducing support surfaces. (A) Definitions and explanations. (1) "Group 1," "group 2," and "group
ACTION: Final DATE: 07/02/2018 10:03 AM 5160-10-18 DMEPOS: hospital beds, bed accessories, and pressurereducing support surfaces. (A) Definitions and explanations. (1) "Group 1," "group 2," and "group
How to prevent pressure ulcers
 How to prevent pressure ulcers Information for patients Find out more at 01522 511566 StBarnabasHospice.co.uk @StBarnabasLinc StBarnabasLinc Prevention is better than cure You have been given this information
How to prevent pressure ulcers Information for patients Find out more at 01522 511566 StBarnabasHospice.co.uk @StBarnabasLinc StBarnabasLinc Prevention is better than cure You have been given this information
Frequently Asked Questions about Pressure Injury Staging. February 20, 2018, 1 to 2 pm ET
 Frequently Asked Questions about Pressure February 20, 2018, 1 to 2 pm ET Scott Bolhack, MD, MBA, CMD, CWSP, FACP, FAAP Janet Cuddigan. PhD, RN, CWCN, FAAN Joyce A. Pittman, PhD, ANP-BC, FNP-BC, CWOCN
Frequently Asked Questions about Pressure February 20, 2018, 1 to 2 pm ET Scott Bolhack, MD, MBA, CMD, CWSP, FACP, FAAP Janet Cuddigan. PhD, RN, CWCN, FAAN Joyce A. Pittman, PhD, ANP-BC, FNP-BC, CWOCN
WHY WOUNDS FAIL TO HEAL SIMPLIFIED
 WHY WOUNDS FAIL TO HEAL SIMPLIFIED 10 Some of the common signs of failure to heal with possible causes and some interventions WHY WOUNDS FAIL TO HEAL There must be adequate supplies of nutrients and oxygen
WHY WOUNDS FAIL TO HEAL SIMPLIFIED 10 Some of the common signs of failure to heal with possible causes and some interventions WHY WOUNDS FAIL TO HEAL There must be adequate supplies of nutrients and oxygen
2/11/2016. Palliative Wound Management Workshop. Carolyn Brown BS, MEd, RN, ARM, CWS, FACCWS Carolyn Brown Consulting
 Palliative Wound Management Workshop Be the best that you can be! Carolyn Brown BS, MEd, RN, ARM, CWS, FACCWS Carolyn Brown Consulting 727-348-5856 cbjackwill@gmail.com Learner Objectives After attending
Palliative Wound Management Workshop Be the best that you can be! Carolyn Brown BS, MEd, RN, ARM, CWS, FACCWS Carolyn Brown Consulting 727-348-5856 cbjackwill@gmail.com Learner Objectives After attending