Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
|
|
|
- Susan Williamson
- 5 years ago
- Views:
Transcription
1 Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
2 Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement Methods of treating postoperative pain (various routes) Patient-controlled analgesia (PCA) Non-opioids Weak opioids Strong opioids Regional analgesia

3 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage


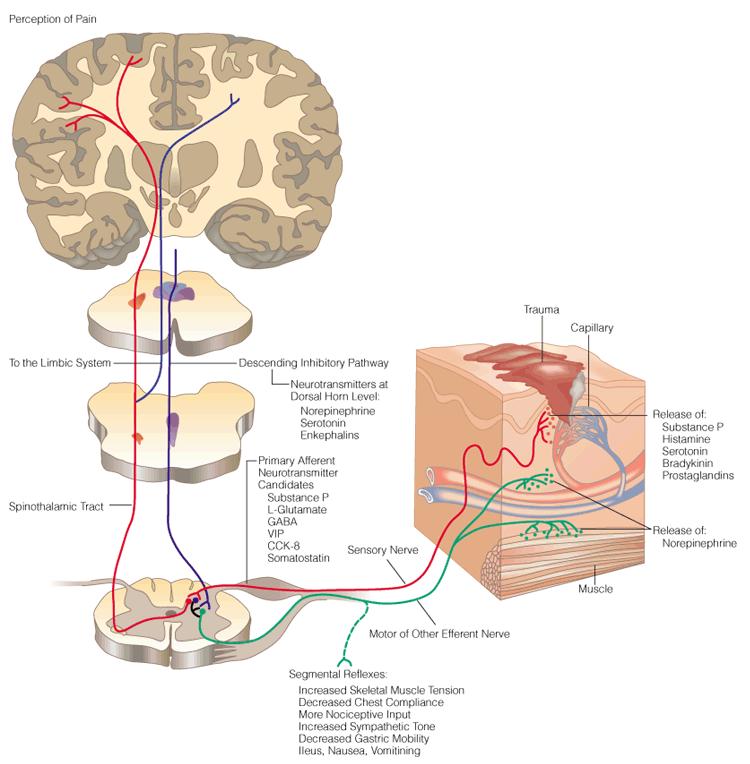
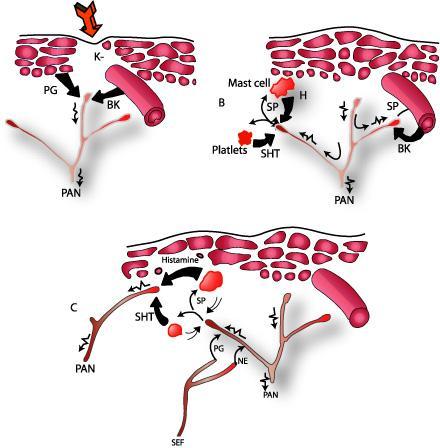
4 Neurobiology of Pain
 s")
5 Descartes (Cartesian) s Model of Pain
6
7
8
9
10 Classification of Pain Duration Acute Chronic Pathophysiology Nociceptive Neuropathic
11 Insult The Continuum of Pain Time to resolution Acute Chronic <1 month 3-6 months Usually obvious tissue damage Increased nervous system activity Pain resolves upon healing Serves a protective function Pain for 3-6 months or more Pain beyond expected period of healing Usually has no protective function Degrades health and function

12 Progression from Acute to Chronic Pain
13 Incidence of Chronic Pain after Surgery Amputation Thoracotomy Mastectomy Cholecystectomy Inguinal hernia Vasectomy Dental surgery % 5-67 % % 3-56 % 0-63 % 0-37 % 5-13 %
14 Risk Factors for Chronic Postsurgical Pain Preop factors Pain, moderate to severe, > 1/12 Repeat surgery Psychologic vulnerability Workers compensation Intraop factors Surgical approach with risk of nerve damage Postop factors Pain (acute, moderate to severe) Radiation to area Neurotoxic chemotherapy Depression Psychologic vulnerability Neuroticism Anxiety

15 Adverse Consequences of Uncontrolled Postoperative Pain Physiological effects Psychological effects
16 Physiological Adverse Effects Increase sympathetic activity Increase risk of MI Decrease GI motility (ileus) Increase incidence of pulmonary complications (atelectasis, hypoxia) Suppress immunity

17 Psychological Adverse Effects Receive less attention than those asso. w chronic pain But not less important Failure to control postop. Pain Anxiety Insomnia Inability to think and interact w others etc.
18 Postoperative Pain Management Multimodal analgesia Preventive analgesia Step down approach
19 Multimodal Analgesia
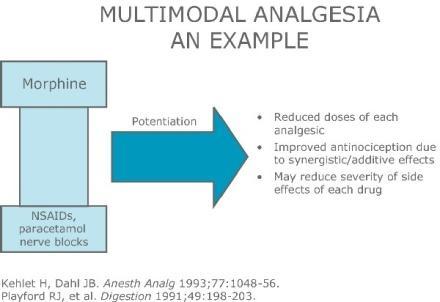
20
21 Clinically Meaningful Adverse Events CMEs The incidence of clinically meaningful adverse events is dose-related (level II)
22 Preventive Analgesia

23 Step Down Approach
24 Measurement of Pain

25 Pain Measurement Pain is a subjective, personal experience The logical and true assessment of pt s pain must therefore be pt s own report Self report is gold standard Unidimension Multidimensions
 Visual analog scales (VAS) Picture scales / pain drawings")
26 Unidimensional Tools Categorical scales Numerical rating scales (NRS) Visual analog scales (VAS) Picture scales / pain drawings

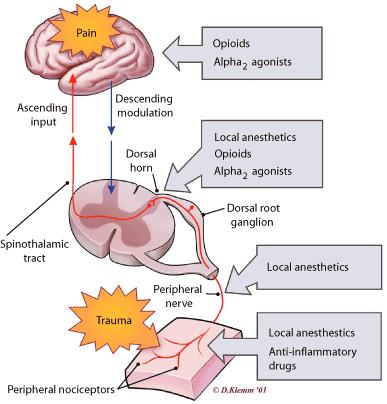
27 Methods of Treating Postoperative Pain
28 Methods of Treating Postoperative Pain Traditional administration of opioids Parenteral administration of opioids Non-parenteral administration of opioids Local anesthetic techniques Non-opioid analgesics Non-pharmacological methods
29 Parenteral Administration of Opioids Bolus IV administration Continuous IV infusion Patient-controlled analgesia (PCA) Bolus IV Bolus + infusion Subcutaneous
30 Non-parenteral Administration of Opioids Sublingual Oral Transmucosal Rectal Transdermal Nasal Inhalation Intra-articular opioids
 Paracetamol NMDA antagonists Central α 2 -adrenergic")
31 Non-opioid Analgesics Non-steroidal anti-inflammatory drugs (NSAIDs) Selective COX-2 inhibitors (COXIBs) Paracetamol NMDA antagonists Central α 2 -adrenergic agonists

32 Patient-controlled Analgesia (PCA)




33 Patient-controlled Analgesia (PCA)
34 Patient-controlled Analgesia (PCA)
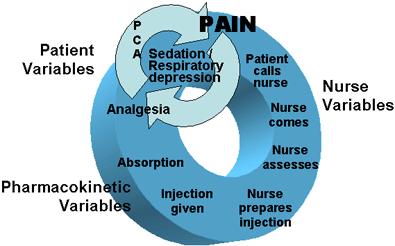
35 Advantages of PCA

36 Non-parenteral Opioid Administration

37 Non-parenteral Administration of Opioids Sublingual Oral Transmucosal Rectal Transdermal Nasal Inhalation Intra-articular opioids

38 Sublingual Opioids Cooperation required No need for painful injections Popular for pts Convenient for nurses Buprenorphine Partial agonist / ceiling effect
 Immediate postop.")
39 Oral Route All opioids undergo extensive first-pass metabolism Low oral bioavailability (20-30%) Immediate postop. period : invariably reduction of gastric emptying

40 Oral Route Absorption may be delayed, with poor analgesia If given on regular basis : a danger of a large dose being propelled into upper GI tract when gastric motility returns to normal Over dosage Ventilatory depression

41 Transmucosal Route Premedication in children Onset of pain relief : 9/60

42 Rectal Route Bioavailability varies according to site of suppository Venous blood from lower part of rectum drains directly into systemic circulation But upper part drains into portal circulation

43 Inhaled / Intranasal Route Intranasal spray devices for fentanyl Metered inhalers with improved pulmonary drug delivery systems and lockout times Future : may allow noninvasive PCA administration

44 Pharmacological Approach
45 Classification of Pain Medications Non-opioid analgesics Opioid analgesics Adjuvants
46 Paracetamol
47 Paracetamol (Acetaminophen) Effective analgesic with antipyretic activity Does not inhibit COX in peripheral tissues -> lack of anti-inflammatory activity Mechanism of analgesic action remains unclear

48 Paracetamol Generally well tolerated Most serious adverse effect of acute overdosage is a dose-dependent (150 mg/kg), potentially fetal, hepatic necrosis Insufficient glutathione (liver disease, alcohol consumption> 3 units/day, malnutrition etc.)
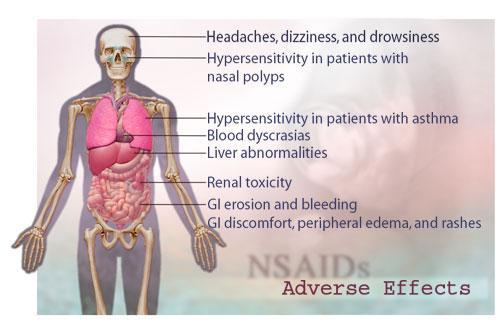
49 NSAIDs
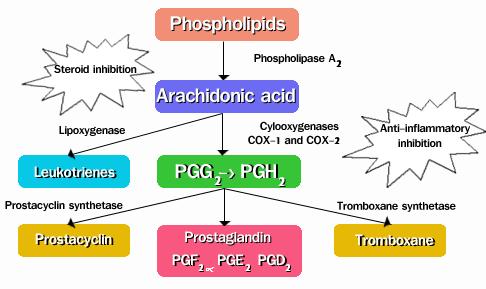
50 Mechanisms of Action
51
52 Selective COX-2 Inhibitors (COXIBs)
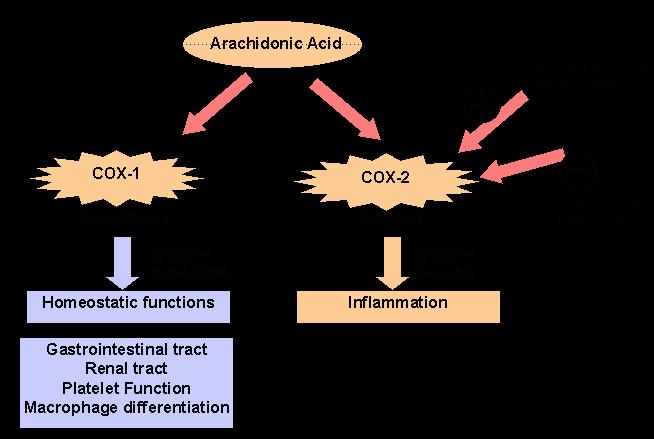
53

54 COXIBS COX-2 is constitutively expressed in kidney Maintenance of renal blood flow Mediation of renin release Regulation of Na + excretion COXIBs & NSAIDs have similar renal adverse effects ed risk in pre-existing renal impairment, hypovolumia, hypotension, use of nephrotoxic agents & ACEIs
55 COXIBs The pharmacological class of COXIBs appears to be associated with an increased risk of CV adverse events The CV risks may increase with dose & duration of exposure The shortest duration possible & the lowest effective daily dose should be used
56 COXIBs Must not be used in pts with established Ischemic heart disease Cerebrovascular disease Peripheral arterial disease To exercise caution in pts with risk factors of heart disease Hypertension Hyperlipidemia DM Smoking
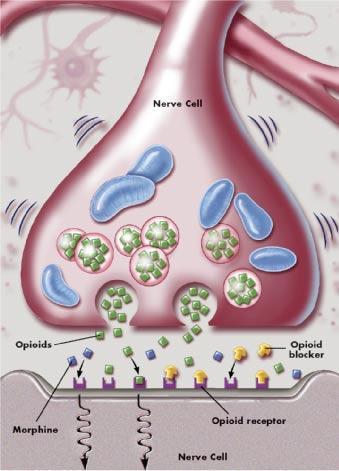
57 Opioids
58 Classification of Opioids Weak opioids (mild - moderate pain) Strong opioids (moderate - severe pain)
59 Weak Opioids Codeine Tramadol
60 Codeine Classic weak opioid Potency 1/10 of MO (CYP2D6, MO) mg q 4/24 Dose limiting side effects (constipation, N/V, confusion) Fixed combination

61 Paracetamol vs Paracetamol plus Codeine

62 Tramadol Dual-acting analgesic Tramadol & M1 (CYP2D6) have affinity at μ-opioid receptors Also inhibits reuptake of serotonin & noradrenaline Potency 1/20 1/5 of MO
63 Tramadol Max 400 mg/day Max 200 mg/day in pts with hepatic / renal impairment Tramadol Retard (12/24) Less sedation & constipation Unfortunately, N/V frequently reported
64 Strong Opioids Morphine Pethidine Fentanyl
65 Strong Opioids Mainstay for the Rx of moderate to severe pain Interpatient requirements vary greatly Doses need to be titrated to suit each pt In adults, age rather than weight is the predictor of requirement
66 Strong Opioids All full agonists given in equianalgesic doses produce the same analgesic effects & side effects One opioid is not superior over others but some are better in some pts (level II) The incidence of clinically meaningful adverse effects is dose related (level II) Pethidine should be discouraged

67 Opioids Assessment of sedation level is a more reliable way of detecting early opioidinduced respiratory depression
68 Morphine M3G & M6G are main metabolites, excreted via kidney M6G Opioid agonist May potent than morphine M3G No analgesic activity May antagonise analgesic effect May cause hyperalgesia, allodynia & muoclonus
69 Pethidine Widely used even though it has multiple disadvantages Despite common belief that it is the most effective opioid in treatment of renal colic, it is no better than morphine Pethidine & morphine have similar effects on sphincter of Oddi & biliary tract No evidence that pethidine is better in the treatment of biliary colic
70 Norpethidine Metabolized in liver to several inactive compounds and norpethidine Accumulation leads to neuroexcitatory Nervousness Tremors Twitches Multifocal myoclonus Seizures
71 Pethidine / Norpethidine Impaired renal function half-life of norpethidine Patients in renal failure are at ed risk of norpethidine toxicity Naloxone not reverses & may norpethidine toxicity Overall, the use of pethidine should be discouraged in favor of other opioids
72 Fentanyl High lipid solubility Potency 100X of morphine Lack of active metabolite Fast onset Short duration of action

73 Guideline for Postoperative Pain Management (Example)
74
75 Regional Analgesia

76 Epidural Analgesia

77 Peripheral Nerve Block

78 Ultrasound-guided Peripheral Nerve Block supraclavicular brachial plexus block


79 Peripheral Nerve Block Single shot Continuous infusion

80
OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4
![OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4](/thumbs/90/104143670.jpg "OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4") Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Opioid MCQ OP01 [Mar96] With regards to pethidine s physical properties: A. It has an octanol coefficient of 10 B. It has a pka of 8.4 OP02 [Mar96] Which factor does NOT predispose to bradycardia with
Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone
 Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
Opioid Definition All drugs, natural or synthetic, that bind to opiate receptors Agonists: morphine, fentanyl Agonists-Antagonists: nalbuphine Antagonists: naloxone Opioid agonists increase pain threshold
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Multi Modal Analgesia
 Analgesic Drugs and Pharmacology Richard Craig R.N. B.N. M. Sci. Med (Pain Mgmt) Nurse Consultant Acute Pain Management Service Christchurch Hospital Multi Modal Analgesia Patients benefit from multi modal
Analgesic Drugs and Pharmacology Richard Craig R.N. B.N. M. Sci. Med (Pain Mgmt) Nurse Consultant Acute Pain Management Service Christchurch Hospital Multi Modal Analgesia Patients benefit from multi modal
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
GUIDELINEs ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINEs ON PAIN MANAGEMENT IN UROLOGY (Text update March 2009) P. ader (chair), D. Echtle, V. Fonteyne, G. De Meerleer, E.G. Papaioannou, J.H. Vranken General principles of cancer pain management The
GUIDELINEs ON PAIN MANAGEMENT IN UROLOGY (Text update March 2009) P. ader (chair), D. Echtle, V. Fonteyne, G. De Meerleer, E.G. Papaioannou, J.H. Vranken General principles of cancer pain management The
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Pharmacogenetics of Codeine. Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA
 Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Clinical Guideline. Guidelines for the use of opioid analgesics in the management of acute pain in adults
 Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Clinical Guideline Guidelines for the use of opioid analgesics in the management of acute pain in adults Document detail Document location West Kent and MTW Formulary Version 1.0 Effective from July 2017
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Pharmaceutics I صيدالنيات 1. Unit 2 Route of Drug Administration
 Pharmaceutics I صيدالنيات 1 Unit 2 Route of Drug Administration 1 Routs of Drug administration The possible routes of drug entry into the body may be divided into two classes: Parenteral Rout Enteral Rout
Pharmaceutics I صيدالنيات 1 Unit 2 Route of Drug Administration 1 Routs of Drug administration The possible routes of drug entry into the body may be divided into two classes: Parenteral Rout Enteral Rout
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
PAIN PODCAST SHOW NOTES:
 PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
PAIN PODCAST SHOW NOTES: Dallas Holladay, DO Ultrasound Fellow Cook County Hospital Rush University Medical Center Jonathan D. Alterie, DO PGY-2, Emergency Medicine Midwestern University An overview of
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
Prescription Pain Management. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D
 Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Advanced Pain Management LYRA SIHRA MD
 Advanced Pain Management LYRA SIHRA MD Objectives Describe the importance of pain management Define the types of pain Discuss opioid pharmacology Identify barriers to pain management Discuss ethical responsibilities
Advanced Pain Management LYRA SIHRA MD Objectives Describe the importance of pain management Define the types of pain Discuss opioid pharmacology Identify barriers to pain management Discuss ethical responsibilities
CHAMP: Bedside Teaching TREATING PAIN. Stacie Levine MD. What is the approach to treating pain in the aging adult patient?
 CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
CHAMP: Bedside Teaching TREATING PAIN Stacie Levine MD Teaching Trigger: An older adult patient is identified as having pain. Clinical Question: What is the approach to treating pain in the aging adult
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
The Fifth Vital Sign.
 Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
Effective pain management begins with OFIRMEV (acetaminophen) injection FIRST Proven efficacy with rapid reduction in pain 1
 injection FIRST Proven efficacy with rapid reduction in pain 1") Effective pain management begins with OFIRMEV (acetaminophen) injection FIRST Proven efficacy with rapid reduction in pain 1 Fast onset of pain relief with 7% reduction in visual analog scale (VAS) scores
Effective pain management begins with OFIRMEV (acetaminophen) injection FIRST Proven efficacy with rapid reduction in pain 1 Fast onset of pain relief with 7% reduction in visual analog scale (VAS) scores
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Drugs Used In Management Of Pain. Dr. Aliah Alshanwani
 Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
CHRONIC PAIN MANAGEMENT
 CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT
 CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT Alicia Z Karas DVM, DACVA Cummings School of Veterinary Medicine, Tufts University, North Grafton, MA There are a number of factors that make cats different
CHALLENGES OF PERIOPERATIVE FELINE PAIN MANAGEMENT Alicia Z Karas DVM, DACVA Cummings School of Veterinary Medicine, Tufts University, North Grafton, MA There are a number of factors that make cats different
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
Pain control in Cancer patients. Dr Ali Shoeibi, Assistant Professor of Neurology
 Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
Analgesia in patients with impaired renal function Formulary Guidance
 Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Screening - inclusion criteria
 PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
PAIN OUT Community research EU ROP EAN COMMISSION A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Room number: Screening
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT
 NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, CVA, CCRT, DAAPM Past-President, IVAPM Animal Pain Management Center Executive Director www.vasg.org 06-11 Chronic pain management is one
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, CVA, CCRT, DAAPM Past-President, IVAPM Animal Pain Management Center Executive Director www.vasg.org 06-11 Chronic pain management is one
Opioid Pharmacology. Dr Ian Paterson, MA (Pharmacology), MB BS, FRCA, MAcadMEd. Consultant Anaesthetist Sheffield Teaching Hospitals
, MB BS, FRCA, MAcadMEd. Consultant Anaesthetist Sheffield Teaching Hospitals") Opioid Pharmacology Dr Ian Paterson, MA (Pharmacology), MB BS, FRCA, MAcadMEd Consultant Anaesthetist Sheffield Teaching Hospitals Introduction The available opioids and routes of administration - oral
Opioid Pharmacology Dr Ian Paterson, MA (Pharmacology), MB BS, FRCA, MAcadMEd Consultant Anaesthetist Sheffield Teaching Hospitals Introduction The available opioids and routes of administration - oral
Analgesics OPIOID ANALGESICS
 Analgesics Opioid (Narcotic analgesics) Non-opioid (Nonsteroidal antiinflammatory drugs) OPIOID ANALGESICS Morphine is the most important alkaloid of opium the dried juice obtained from the capsules of
Analgesics Opioid (Narcotic analgesics) Non-opioid (Nonsteroidal antiinflammatory drugs) OPIOID ANALGESICS Morphine is the most important alkaloid of opium the dried juice obtained from the capsules of
6/6/2018. Nalbuphine: Analgesic with a Niche. Mellar P Davis MD FCCP FAAHPM. Summary of Advantages. Summary of Advantages
 Nalbuphine: Analgesic with a Niche Mellar P Davis MD FCCP FAAHPM 1 Summary of Advantages Safe in renal failure- fecal excretion Analgesia equal to morphine with fewer side effects Reduced constipation
Nalbuphine: Analgesic with a Niche Mellar P Davis MD FCCP FAAHPM 1 Summary of Advantages Safe in renal failure- fecal excretion Analgesia equal to morphine with fewer side effects Reduced constipation
Screening - inclusion criteria
 A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
A Date of data collection: B Time of data collection: C Ward where data is collected: 2 0 1 Y M M D D H H M M D Research assistant Code: Patient code (local): Room number: Screening - inclusion criteria
Balanced Analgesia With NSAIDS and Coxibs. Raymond S. Sinatra MD, Ph.D
 Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Balanced Analgesia With NSAIDS and Coxibs Raymond S. Sinatra MD, Ph.D Prostaglandins and Pain The primary noxious mediator released from damaged tissue is prostaglandin (PG) PG is responsible for nociceptor
Pain Management in the Surgical Patient. Peter Vogel, VMD, DACVS
 Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone
Pain Management in the Surgical Patient Peter Vogel, VMD, DACVS Pain Pathways u Specialized neurons that travel through the spinal cord u Free nerve endings in skin, connective tissue, muscle and bone
Drug CHAPTER 2. Pharmacologic Principles. NDEG 26A Eliza Rivera-Mitu, RN, MSN. Pharmacology. Drug Names. Pharmacologic Principles. Drug Names (cont'd)
") CHAPTER 2 Pharmacologic Principles NDEG 26A Eliza Rivera-Mitu, RN, MSN Drug Any chemical that affects the physiologic processes of a living organism Pharmacology The study or science of drugs Drug Names
CHAPTER 2 Pharmacologic Principles NDEG 26A Eliza Rivera-Mitu, RN, MSN Drug Any chemical that affects the physiologic processes of a living organism Pharmacology The study or science of drugs Drug Names
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Advanced Medical Care: Improving Veterinary Anesthesia. Advanced Medical Care: Improving Veterinary Anesthesia
 Advanced Medical Care: Improving Thursday, April 23, 2009 By Tamara Grubb, DVM, MS, DACVA AAHA gratefully acknowledges the following for their sponsorship of this Web Conference: Advanced Medical Care:
Advanced Medical Care: Improving Thursday, April 23, 2009 By Tamara Grubb, DVM, MS, DACVA AAHA gratefully acknowledges the following for their sponsorship of this Web Conference: Advanced Medical Care:
THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT
 1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT
 NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, DAAPM President, IVAPM Animal Pain Management Center Founder/Webmaster www.vasg.org VIN Anesthesia/Analgesia Consultant Editor Chronic pain
NEWER OPTIONS FOR CHRONIC PAIN MANAGEMENT Robert M. Stein, DVM, DAAPM President, IVAPM Animal Pain Management Center Founder/Webmaster www.vasg.org VIN Anesthesia/Analgesia Consultant Editor Chronic pain
5 MUSCULOSKELETAL SYSTEM
 5 MUSCULOSKELETAL SYSTEM 5.01 NON-STEROIDAL ANTIILAMMATORY DRUGS (NSAIDS) *Acetylsalicylic Acid (Aspirin) Tab Soluble 300mg Diclofenac Sodium Tab 25mg, Supp 25mg, 50mg & 100mg (Voltaren) 300-900mg every
5 MUSCULOSKELETAL SYSTEM 5.01 NON-STEROIDAL ANTIILAMMATORY DRUGS (NSAIDS) *Acetylsalicylic Acid (Aspirin) Tab Soluble 300mg Diclofenac Sodium Tab 25mg, Supp 25mg, 50mg & 100mg (Voltaren) 300-900mg every
A. Correct! Nociceptors are pain receptors stimulated by harmful stimuli, resulting in the sensation of pain.
 Pharmacology - Problem Drill 19: Anti-Inflammatory and Analgesic Drugs No. 1 of 10 1. are pain receptors stimulated by harmful stimuli, resulting in the sensation of pain. #01 (A) Nociceptors (B) Histamines
Pharmacology - Problem Drill 19: Anti-Inflammatory and Analgesic Drugs No. 1 of 10 1. are pain receptors stimulated by harmful stimuli, resulting in the sensation of pain. #01 (A) Nociceptors (B) Histamines
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Source of pain relievers for nonmedical use among users 12 years or older:
 ACUTE PAIN MANAGEMENT OF THE OPIOID TOLERANT TRAUMA PATIENT James D. Colson, MS, MD Department of Anesthesiology WVU Hospitals Learning Objectives Identify criteria pertaining to the opioid-tolerant patient;
ACUTE PAIN MANAGEMENT OF THE OPIOID TOLERANT TRAUMA PATIENT James D. Colson, MS, MD Department of Anesthesiology WVU Hospitals Learning Objectives Identify criteria pertaining to the opioid-tolerant patient;
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Analgesia is a labeled indication for all of the approved drugs I will be discussing.
 Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Choose a category. You will be given the answer. You must give the correct question. Click to begin.
 Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
Acute Pain Management
 Acute Pain Management Dr Zamil Karim MBBS, FANZCA,FFPMANZCA, FIPP The journey to Acute pain management begins in the perioperative period. The evaluation and assessment occurs in the perioperative period
Acute Pain Management Dr Zamil Karim MBBS, FANZCA,FFPMANZCA, FIPP The journey to Acute pain management begins in the perioperative period. The evaluation and assessment occurs in the perioperative period
Inpatient Management of Trauma Related Pain
 Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
If Not Opioids then LEAH EDMONDS CSHP OCTOBER 26, 2017
 If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
disease or in clients who consume alcohol on a regular basis. bilirubin
 NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
NON-OPIOID Acetaminophen(Tylenol) Therapeutic class: Analgesic, antipyretic Aspirin (ASA, Acetylsalicylic Acid) Analgesic, NSAID, antipyretic Non-Opioid Analgesics COMMON USES WHAT I NEED TO KNOW AS A
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
NOVIDADES NO TRATAMENTO COM OPIOIDES. Novelties in therapeutic with opioids. V Congresso National de Cuidados Palliativos Marco 2010, Lisboa
 NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Using methadone alongside other opioids. Dr. Jo Murrell BVSc. (hons), PhD, DiplECVAA, MRCVS
, PhD, DiplECVAA, MRCVS") Using methadone alongside other opioids Dr. Jo Murrell BVSc. (hons), PhD, DiplECVAA, MRCVS Why might we want to use methadone alongside other opioids? 1. Multi-modal analgesia strategies e.g. using methadone
Using methadone alongside other opioids Dr. Jo Murrell BVSc. (hons), PhD, DiplECVAA, MRCVS Why might we want to use methadone alongside other opioids? 1. Multi-modal analgesia strategies e.g. using methadone
POSTOPERATIVE PAIN RELIEF
 POSTOPERATIVE PAIN RELIEF Caesarean sections are equal to laparotomies in many aspects, pain relief not an exception. The widespread use of spinal anaesthesia often lends to the mistaken belief that these
POSTOPERATIVE PAIN RELIEF Caesarean sections are equal to laparotomies in many aspects, pain relief not an exception. The widespread use of spinal anaesthesia often lends to the mistaken belief that these
PARACOD Tablets (Paracetamol + Codeine phosphate)
") Published on: 22 Sep 2014 PARACOD Tablets (Paracetamol + Codeine phosphate) Composition PARACOD Tablets Each effervescent tablet contains: Paracetamol IP...650 mg Codeine Phosphate IP... 30 mg Dosage Form/s
Published on: 22 Sep 2014 PARACOD Tablets (Paracetamol + Codeine phosphate) Composition PARACOD Tablets Each effervescent tablet contains: Paracetamol IP...650 mg Codeine Phosphate IP... 30 mg Dosage Form/s
12/14/2018. Disclosures. Buprenorphine. Drug-Receptor Interactions. Affinity
 ECHO Ontario Chronic Pain Bootcamp OPIOID CHALLENGE Buprenorphine/Naloxone: What and How? Friday, December 7, 2018 Disclosures Presenters: John Flannery & Andrew Smith Conflicts of Interest: None John
ECHO Ontario Chronic Pain Bootcamp OPIOID CHALLENGE Buprenorphine/Naloxone: What and How? Friday, December 7, 2018 Disclosures Presenters: John Flannery & Andrew Smith Conflicts of Interest: None John
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Victoria L. Thornton, MD, MBA Consulting Associate Duke University School of Nursing. Sickle Cell Disease: Breaking Down the Myths and Barriers
 Victoria L. Thornton, MD, MBA Consulting Associate Duke University School of Nursing Sickle Cell Disease: Breaking Down the Myths and Barriers Disclosure Statement I, nor my spouse/partner, have no relevant
Victoria L. Thornton, MD, MBA Consulting Associate Duke University School of Nursing Sickle Cell Disease: Breaking Down the Myths and Barriers Disclosure Statement I, nor my spouse/partner, have no relevant
Slide 1. Slide 2. Slide 3. Drug Action and Handling. Lesson 2.1. Lesson 2.1. Drug Action and Handling. Drug Action and Handling.
 Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
POST-OP MULTIMODAL PAIN MANAGEMENT. Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management
 POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
POST-OP MULTIMODAL PAIN MANAGEMENT Maripat Welz-Bosna Reading Hospital Medical Center Department of Medicine Hospitalist Services/Pain Management Objectives Understand the basic neurobiology of the pain
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Trust Guideline for the Management of Patient Controlled Analgesia (PCA) in Adults
 in Adults") Patient Controlled Analgesia (PCA) in Adults A clinical guideline recommended for use For Use in: In all Clinical Areas By: Anaesthetists, Ward Nurses, Recovery Staff Acute Pain Service Staff For: Adult
Patient Controlled Analgesia (PCA) in Adults A clinical guideline recommended for use For Use in: In all Clinical Areas By: Anaesthetists, Ward Nurses, Recovery Staff Acute Pain Service Staff For: Adult
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Overview of Pain Types and Prevalence
 Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
Management of Pain. Agenda: Definitions Pathophysiology Analgesics
 C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
What do we want for pain medications?
 New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
New Trends in Pain Pharmacotherapy Dr. Chi Wai Cheung MBBS(HK), FHKCA, FHKAM(Anaesthesiology), Dip Pain Mgt(HKCA) Clinical Assistant Professor Department of Anaesthesiology The University of Hong Kong
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Appendix D: Drug Tables
 Appendix D: Drug Tables A. Short-acting, Orally Administered Opioids Table D-1: Use of Short-acting, Orally Administered Opioids in Adults [198] Additional Maximum APAP dose: 4000 mg/d (2000 mg/d in chronic
Appendix D: Drug Tables A. Short-acting, Orally Administered Opioids Table D-1: Use of Short-acting, Orally Administered Opioids in Adults [198] Additional Maximum APAP dose: 4000 mg/d (2000 mg/d in chronic
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
The WHY and HOW of Acute Pain Control
 The WHY and HOW of Acute Pain Control James S. Gaynor, DVM, MS, DACVAA, DAAPM Frisco, CO USA jgaynor@nopetpain.com www.peakvets.com Principles of Pain Management Pain control is good medicine Pre-emptive,
The WHY and HOW of Acute Pain Control James S. Gaynor, DVM, MS, DACVAA, DAAPM Frisco, CO USA jgaynor@nopetpain.com www.peakvets.com Principles of Pain Management Pain control is good medicine Pre-emptive,
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital
 Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
5 th ERAS UK Conference. Advances in Pain Management. Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh
 5 th ERAS UK Conference Advances in Pain Management Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh Pre-op information Optimised organ function No nutritional
5 th ERAS UK Conference Advances in Pain Management Jayne Balson Advanced Nurse Specialist Pain Management Western General Hospital Edinburgh Pre-op information Optimised organ function No nutritional
Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine
 Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine ACUTE PAIN MANAGEMENT: SCIENTIFIC EVIDENCE 2 ND EDITION UPDATES Last update: DECEMBER 2007 Acute Pain Management: Scientific
Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine ACUTE PAIN MANAGEMENT: SCIENTIFIC EVIDENCE 2 ND EDITION UPDATES Last update: DECEMBER 2007 Acute Pain Management: Scientific