Sepsis Review. Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center
|
|
|
- Barnard Ross
- 5 years ago
- Views:
Transcription
1 Sepsis Review Angela Craig APN,MS,CCNS Clinical Nurse Specialist Intensive Care Unit Cookeville Regional Medical Center
2 Discuss the Updated International Guidelines Discuss how you can make a difference Review the ED pilot project Objectives

3 Cookeville Regional Medical Center 247 Bed Community Hospital (Non-Teaching) Regional referral center in the heart of the Upper Cumberland in middle Tennessee

4 CRMC Sepsis Initiative Go live ICU/CVICU ED and Rapid Response September 2009 Go live Hospital Wide October 2010 Cost Savings per patient Mortality Decrease = Lives Saved!!!

5 Sepsis Disease Specific Certification CRMC March 2015 (First in State of TN)
6 Severe Sepsis: A Significant Healthcare Challenge Major cause of morbidity and mortality worldwide Leading cause of death in noncoronary ICU (US) 1 10th leading cause of death overall (US) 2 * In the US, more than 700 patients die of severe sepsis daily (1.6 million new cases per year) * Based on data for septicemia Reflects hospital-wide cases of severe sepsis as defined by infection in the presence of organ dysfunction 1 Sands KE, et al. JAMA 1997;278: National Vital Statistics Reports Angus DC, et al. Crit Care Med 2001;29: **AHRQ Healthcare cost & Utilization Project October 2011

7 Sepsis: CDC Vital Sign % of sepsis begins outside the hospital 7 out of 10 patients with sepsis had recently used health services or had chronic dx requiring frequent care 4 types of infections most connected to sepsis; lung, urinary tract, skin and gut HCP: think sepsis & act fast
8 Sepsis Definitions
9 Sepsis (Severe Sepsis) and septic shock are medical emergencies, and we recommend that treatment and resuscitation begin immediately 2017 Surviving Sepsis Guidelines Best Practice Statement
10 2016 New Definitions
11 2016 Guideline Definitions Sepsis: life-threatening organ dysfunction caused by a dysregulated host response to infection Septic Shock: a subset of sepsis with circulatory and cellular/metabolic dysfunction associated with a higher risk of mortality

12 Sepsis-3 Workflow Singer et al, JAMA PMID: Keep doing what you are doing and consider measuring q-sofa and SOFA scores in addition to current practice to assess high risk of death until CMS changes or large prospective studies are performed Simpson SQ, et al. Chest, 2016; doi: /j.chest
13 The SOFA score is an illness-severity score which may be used to predict the mortality of any critically ill patient. qsofa was also designed to predict mortality < badness > within the context of a cohort of patients with suspected infection. Thus, qsofa and SOFA are predictors of mortality; they are not tests of early sepsis at risk to progress to organ failure. qsofa will inevitably be misunderstood to be a sepsis screen.
14 The definitions are mortality predictors, not screening definitions for early identification CMS definitions and core measures have NOT changed ICD-10 has NOT changed No pathway to implement at our current institutions how would a transition happen? Incompatibility with Current Proven QI Efforts
15 Core Measure Sepsis Definitions
16 Definitions Sepsis: infection plus 2 or more SIRS Severe Sepsis: infection plus 2 or more SIRS plus new organ dysfunction Septic Shock: severe sepsis with a lactic acid greater than or equal to 4mmol/L OR continued hypotension (systolic BP<90 or 40mmHg decrease from their baseline) after initial fluid bolus (30ml/kg)
17 International Guidelines for Management of Sepsis and Septic Shock & CMS Core Measure

18 Discuss the latest guidelines for severe sepsis and septic shock published March 2017 SCCM

19 Guidelines GRADE System SCCM March 2017, Vol 45, Number 3

20 Guidelines GRADE System SCCM March 2017, Vol 45, Number 3

21 Dellinger, etal, Critical Care Medicine, Feb 2013, Vol 41 Number 2
22
23 CMS Bundle summary: 3- hour bundle: 6-hour bundle: Severe Sepsis 1. Initial lactate level (NP) 2. Blood culture prior to antibiotics (NP) 3. Broad spectrum antibiotic 4. 30ml/kg crystalloid fluid NP = Nursing Protocol Severe Sepsis 1. Repeat lactate level (NP) If initial LA>2.0 Septic Shock 1. Vasopressor if hypotension persist 2. Volume status and tissue perfusion reassessment if hypotension persist 23
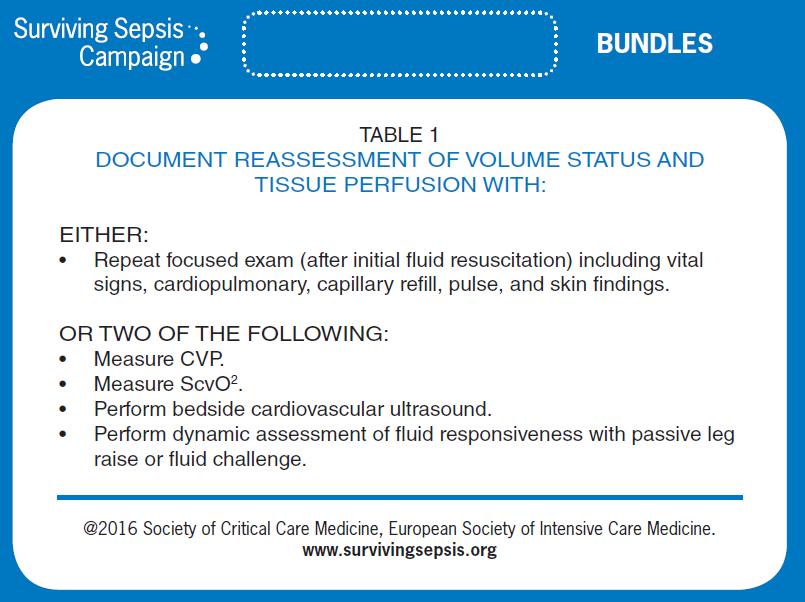
24 Repeat volume status and tissue Assessment (one of two ways): A. Focused exam documented by Provider (Midlevels included) and which includes ALL the following: Vital signs(includes all: BP, Pulse, Resp., Temp) Cardiopulmonary exam (heart and lung) Capillary refill evaluation Peripheral pulse evaluation Skin examination OR 24
25 Volume Status/Tissue Assessment Continued: B. Any two of the following: Central venous pressure measurement Can see in Nursing Notes Central venous oxygen measurement Can see in Nursing Notes Bedside Cardiovascular Ultrasound Time and Date of Bedside Cardiovascular Ultrasound Does NOT have to be always done at the bedside Echo, TEE, Doppler echocardiogram etc. Passive Leg Raise (PLR) or Fluid Challenge Time and Date of PLR Time and Date of Fluid challenge 25
26 Sample Progress Note 26
27
28 SSC Guidelines A: Initial Resuscitation 1. Sepsis and septic shock are medical emergencies, and we recommend that treatment and resuscitation begin immediately (BPS) 2. We recommend that, in the resuscitation from sepsis-induced hypoperfusion, at least 30mL/kg of IV crystalloid fluid be given within the first 3 hours (strong recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3
29 SSC Guidelines A: Initial Resuscitation 3. We recommend that, following initial fluid resuscitation, additional fluids be guided by frequent reassessment of hemodynamic status (BPS) 4. We recommend further hemodynamic assessment (such as assessing cardiac function) to determine the type of shock if the clinical examination does not lead to a clear diagnosis (BPS) SCCM March 2017, Vol 45, Number 3
30 SSC Guidelines A: Initial Resuscitation 5. We suggest that dynamic over static variables be used to predict fluid responsiveness, where available (weak recommendation, low quality of evidence) 6. We recommend an initial target mean arterial pressure (MAP) of 65mmHg in patients with septic shock requiring vasopressors (strong recommendation, moderate quality of evidence) SCCM March 2017, Vol 45, Number 3
31 NICE Protocol
32 SSC Guidelines A: Initial Resuscitation 7. We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion (weak recommendation, low quality of evidence) Other Items: *Use of CVP alone to guide fluid resuscitation can no longer be justified because the ability to predict a response to a fluid challenge when the CVP is within a relatively normal range is limited SCCM March 2017, Vol 45, Number 3
33 SSC Guidelines A: Initial Resuscitation Other Items: * Serum lactate is not a direct measure of tissue perfusion. Increases in the serum lactate level may represent tissue hypoxia, accelerated aerobic glycolysis driven by excess beta adrenergic stimulation, or other causes (liver failure) SCCM March 2017, Vol 45, Number 3

34 Application of Fluid Resuscitation in Adult Septic Shock User s Guide to the 2016 Surviving Sepsis Guidelines Dellinger, CCM published ahead of print

35 Can Lactate Clearance Be Used As a Resuscitation Endpoint? Rivers EP, et al. Chest. 2011;140:
36 SSC Guidelines B. Screening We recommend that hospitals and hospital systems have a performance improvement program for sepsis, including sepsis screening for acutely ill, high-risk patients (BPS) SCCM March 2017, Vol 45, Number 3
37 Why Do You Need to Have a Screening Process? TIME IS TISSUE!! Similar to polytrauma, AMI, or stroke, the speed and appropriateness of therapy administered in the initial hours after severe sepsis develops are likely to influence outcomes. 1 To screen effectively, it must be part of the nurses daily routines i.e., part of admission and shift assessment Must define a process for what to do with the results of the screen If you don t screen you will miss patients that may have benefited from the interventions. 1. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: Crit Care Med. 2008;36:

38 Floor Screening Tool
39 ED Screening Tool
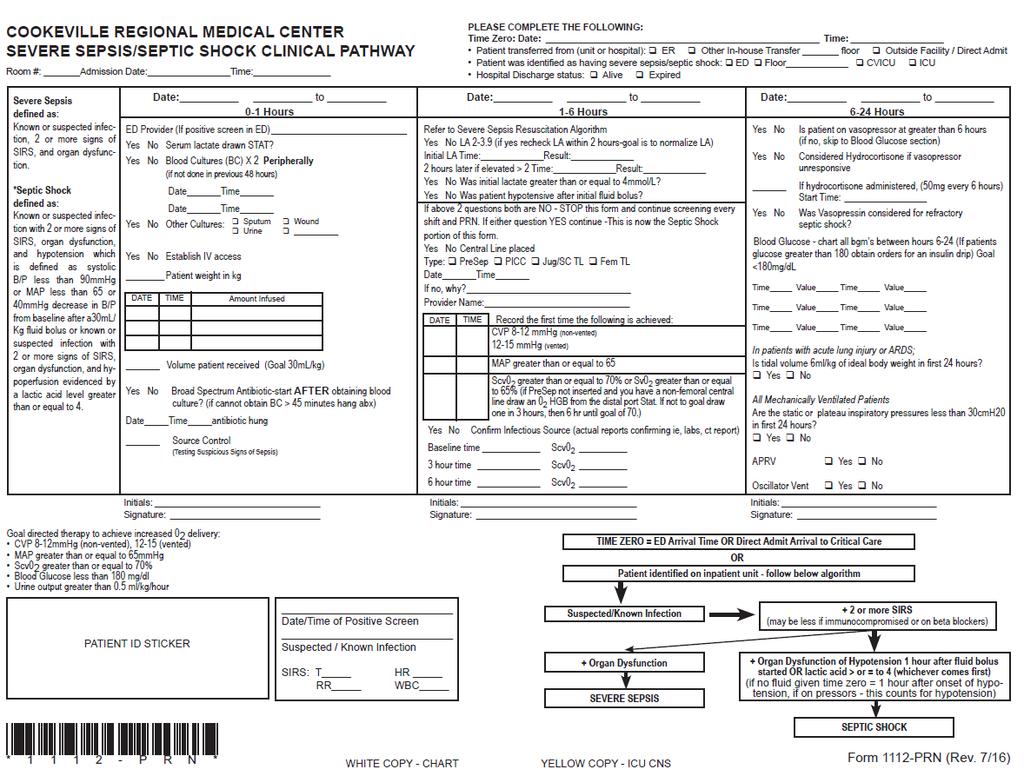
40 Pathway
41 SSC Guidelines C: Diagnosis We recommend that appropriate routine microbiologic cultures (including blood) be obtained before starting antimicrobial therapy in patients with suspected sepsis or septic shock if doing so results in no substantial delay in the start of antimicrobials (BPS) Remarks: Appropriate routine microbiologic cultures always include at least two sets of blood cultures (aerobic and anaerobic) SCCM March 2017, Vol 45, Number 3
42 SSC Guidelines D. Antimicrobial Therapy 1. We recommend that administration of IV antimicrobials be initiated as soon as possible after recognition and within one hour for both sepsis and septic shock (strong recommendation, moderate quality of evidence; grade applies to both conditions) 2. We recommend empiric broad-spectrum therapy with one or more antimicrobials for patients presenting with sepsis or septic shock to cover all likely pathogens (including bacterial and potentially fungal or viral coverage) (strong recommendation, moderate quality of evidence) SCCM March 2017, Vol 45, Number 3
43 SSC Guidelines D. Antimicrobial Therapy 3. We recommend that empiric antimicrobial therapy be narrowed once pathogen identification and sensitivities are established and/or adequate clinical improvement is noted (BPS) 4. We recommend against sustained antimicrobial prophylaxis in patients with severe inflammatory states of noninfectious origin (e.g., severe pancreatitis, burn injury) (BPS) SCCM March 2017, Vol 45, Number 3
44 SSC Guidelines D. Antimicrobial Therapy 5. We recommend that dosing strategies of antimicrobials be optimized based on accepted pharmacokinetic/pharmacodynamic principles and specific drug properties in patients with sepsis or septic shock (BPS) 6. We suggest empiric combination therapy (using at least two antibiotics of different antimicrobial classes) aimed at the most likely bacterial pathogen(s) for the initial management of septic shock (weak recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3

45 SCCM March 2017, Vol 45, Number 3
46 SSC Guidelines D. Antimicrobial Therapy 7. We suggest that combination therapy not be routinely used for ongoing treatment of most other serious infections, including bacteremia and sepsis without shock (weak recommendation, low quality of evidence) Remarks: This does not preclude the use of multidrug therapy to broaden antimicrobial activity 8. We recommend against combination therapy for the routine treatment of neutropenic sepsis/bacteremia (strong recommendation, moderate quality of evidence) SCCM March 2017, Vol 45, Number 3
47 SSC Guidelines D. Antimicrobial Therapy 9. If combination therapy is initially used for septic shock we recommend de-escalation with discontinuation of combination therapy within the first few days in response to clinical improvement and/or evidence of infection resolution. This applies to both targeted (for culture positive infections) and empiric (for culture-negative infections) combination therapy (BPS) SCCM March 2017, Vol 45, Number 3
48 SSC Guidelines D. Antimicrobial Therapy 10. We suggest that an antimicrobial treatment duration of 7 to 10 days is adequate for most serious infections associated with sepsis and septic shock (weak recommendation, low quality of evidence) 11. We suggest that longer courses are appropriate in patients who have a slow clinical response, undrainable foci of infection, bacteremia with S aureus, some fungal and viral infections or immunologic deficiencies, including neutropenia. (weak recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3
49 SSC Guidelines D. Antimicrobial Therapy 12. We suggest that shorter courses are appropriate in some patients, particularly those with rapid clinical resolution following effective source control of intra-abdominal or urinary sepsis and those with anatomically uncomplicated pyelonephritis (weak recommendation, low quality of evidence) 13. We recommend daily assessment for deescalation of antimicrobial therapy in patients with sepsis and septic shock (BPS) SCCM March 2017, Vol 45, Number 3
50 SSC Guidelines D. Antimicrobial Therapy 14. We suggest that measurement of procalcitonin levels can be used to support shortening the duration of antimicrobial therapy in sepsis patients (weak recommendation, low quality of evidence) 15. We suggest that procalcitonin levels can be used to support the discontinuation of empiric antibiotics in patients who initially appeared to have sepsis, but subsequently have limited clinical evidence of infection (weak recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3
51 SSC Guidelines E. Source Control 1. We recommend that a specific anatomical diagnosis of infection requiring emergent source control be identified or excluded as rapidly as possible in patients with sepsis or septic shock, and that any required source control intervention be implemented as soon as medically and logistically practical after the diagnosis is made (BPS) 2. We recommend prompt removal of intravascular access devices that are a possible source of sepsis or septic shock after other vascular access has been established (BPS) SCCM March 2017, Vol 45, Number 3
52 SSC Guidelines F. Fluid Therapy 1. We recommend that a fluid challenge technique be applied where fluid administration is continued as long as hemodynamic factors continue to improve (BPS) 2. We recommend crystalloids as the fluid of choice for initial resuscitation and subsequent intravascular volume replacement in patients with sepsis and septic shock (strong recommendation, moderate quality of evidence) SCCM March 2017, Vol 45, Number 3
53 SSC Guidelines F. Fluid Therapy 3. We suggest using either balanced crystalloids or saline for fluid resuscitation of patients with sepsis or septic shock (weak evidence, low quality of evidence) 4. We suggest using albumin in addition to crystalloids for initial resuscitation and subsequent intravascular volume replacement in patients with sepsis and septic shock when patients require substantial amounts of crystalloids (weak recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3
54 SSC Guidelines F. Fluid Therapy 5. We recommend against using hydroxyethyl starches with sepsis or septic shock (strong recommendation, high quality of evidence) 6. We suggest using crystalloids over gelatins (synthetic colloids) when resuscitating patients with sepsis or septic shock (weak recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3
55 SSC Guidelines G. Vasoactive Medications 1. We recommend norepinephrine as the first choice vasopressor (strong recommendation, moderate quality of evidence) 2. We suggest adding either vasopressin (up to 0.03 U/min) (weak recommendation, moderate quality of evidence) or epinephrine (weak recommendation, low quality of evidence) to norepinephrine with the intent of raising MAP to target, or adding vasopressin (up to 0.03 U/min) (weak recommendation, moderate quality of evidence) to decrease norepinephrine dosage SCCM March 2017, Vol 45, Number 3
56 SSC Guidelines G. Vasoactive Medications 3. We suggest using dopamine as an alternative vasopressor agent to norepinephrine only in highly selected patients (e.g., patients with low risk of tachyarrhythmias and absolute or relative bradycardia) (weak recommendation, low quality of evidence) 4. We recommend against using low-dose dopamine for renal protection (strong recommendation, high quality of evidence) SCCM March 2017, Vol 45, Number 3
57 SSC Guidelines G. Vasoactive Medications 5. We suggest using dobutamine in patients who show evidence of persistent hypoperfusion despite adequate fluid loading and the use of vasopressor agents (weak recommendation, low quality of evidence) Remarks: If initiated, vasopressors dosing should be titrated to an end point reflecting perfusion, and the agent reduced or discontinued in the face of worsening hypotension or arrhythmias SCCM March 2017, Vol 45, Number 3
58 SSC Guidelines G. Vasoactive Medications 6. We suggest that all patients requiring vasopressors have an arterial catheter placed as soon as practical if resources are available (weak recommendation, very low quality of evidence) SCCM March 2017, Vol 45, Number 3
59 SSC Guidelines H. Corticosteroids 6. We suggest against using IV hydrocortisone to treat septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore hemodynamic stability. If this is not achievable, we suggest IV hydrocortisone at a dose of 200mg per day (weak recommendation, low quality of evidence) SCCM March 2017, Vol 45, Number 3
60 SSC Guidelines I. Blood Products 1. We recommend that RBC transfusion occur only when hemoglobin concentration decreases to <7.0g/dL in adults in the absence of extenuating circumstances, such as myocardial ischemia, severe hypoxemia, or acute hemorrhage (strong recommendation, high quality of evidence) 2. We recommend against the use of erythropoietin for treatment of anemia associated with sepsis (strong recommendation, moderate quality of evidence) SCCM March 2017, Vol 45, Number 3
61 SSC Guidelines I. Blood Products 3. We suggest against the use of fresh frozen plasma to correct clotting abnormalities in the absence of bleeding or planned invasive procedures (weak recommendation, very low quality of evidence) 4. We suggest prophylactic platelet transfusion when counts are <10,000/mm 3 in the absence of apparent bleeding and when counts are <20,000/mm 3 if the patient has a significant risk of bleeding. Higher platelet counts 50,000/mm 3 are advised for active bleeding surgery, or invasive procedures (weak recommendation, very low quality of evidence) SCCM March 2017, Vol 45, Number 3
62 SSC Guidelines J. Immunoglobulins K. Blood Purification L. Anticoagulants M. Mechanical Ventilation N. Sedation and Analgesia O. Glucose Control P. Renal Replacement Therapy Q. Bicarbonate Therapy R. Venous Thromboembolism Prophylaxis SCCM March 2017, Vol 45, Number 3
63 SSC Guidelines S. Stress Ulcer Prophylaxis T. Nutrition U. Setting Goals of Care SCCM March 2017, Vol 45, Number 3
64 References: Rhodes et al, Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: Critical Care Medicine. 2017; 45:1-67. Guidelines are available Go to the Surviving Sepsis Campaign Website and look under the tab Guidelines. There will be a link there.
65 Emergency Room Opportunities
66 Have you even considered monitoring hemodynamics as early as in the Emergency Dept. or on a Rapid Response Call?
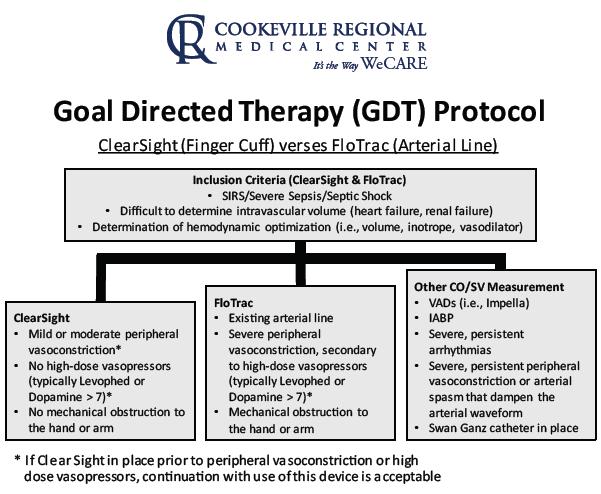
67 Hyperdynamic phase produces increased CO and decreased peripheral resistance (SVR) Hypotension Tachycardia Tachypnea Bounding pulse Warm, well perfused extremities Skin flushed, moist Hypodynamic phase characterized by decreased CO & increased peripheral resistance (SVR) Hypotensive Tachycardia Narrow, thread pulse Cold, poorly perfused extremities Skin pale, dry Non-Invasive Finger Cuff Effective in monitoring patients in the hyperdynamic phase of sepsis 3/18/2016) Am J Emerg Med an;2(1):74-7. Pathophysiology and treatment of septic shock. Schumer W accessed 4/5/16 67
68
69
70

71 EMS radio report: 54 year old Db with c/o SOB. Left below the knee amputation with ulcer. Suspected respiratory infection + possible infection to ulcer on stump Subtle rise in SV with PLR and Fluid bolus <10% ClearSight applied PLR performed raising 1 ½ legs. SV has a subtle rise but <10% IV initiated at 999. Monitoring for rise in SV with fluid bolus Again SV has a subtle rise but not >10% Interpretation: Respiratory infection is localized not systemic. No intravascular volume shift noted with PLR or fluid bolus. Nickle size abrasion to stump 2 nd to ill fitting prosthesis. No infection to stump noted. 71

 increasing >10% to (102-105) with 3 rd liter.")
72 61 year old male with C/O SOB. Tachypnea with suspected source respiratory. Screening positive for Sepsis initiating Sepsis 3 Hour Bundle. Increase in SV with volume administration Volume administration restarted Return from BR, drop in SV Interpretation: Need for 3 rd liter 2 nd to rise in SV >10%. Drop in SV upon return from BR signifying need for additional volume. Rise in SV upon restarting volume administration. Upon my arrival bundle in progress with 2L infused, continuing with 3rd liter.+ antibiotics LA 2.4 +WBC 21,000 SV (82-86) increasing >10% to ( ) with 3 rd liter. Post 3 rd liter walking to bathroom. IV infusion + ClearSight stopped. Upon return from bathroom drop in SV. Volume administration restarted. 72
73 Data Sample from CRMC Severe Sepsis/Septic Shock Summary Jan'16 Feb'16 Mar'16 April'16 May'16 June'16 July'16 Aug' 16 Sept'16 Oct'16 Nov'16 Early Mgt Bundle Compliance Rate: 59% 72% 64% 67% 60% 69% 72% 66% 70% 71% 65% Severe Sepsis Bundle: # of patients that met criteria Initial Lactate w/in 3 hrs 96% 95% 97% 95% 100% 98% 98% 97% 99% 100% 100% Bld C/S prior to ATB and w/in 3 hrs 88% 95% 96% 91% 94% 92% 94% 94% 99% 100% 95% ATB w/in 3 hrs 96% 90% 93% 97% 92% 95% 96% 92% 94% 94% 91% Repeat lactate w/in 6 hrs (if initial >2) 83% 90% 74% 87% 88% 91% 95% 90% 98% 93% 93% Septic Shock Bundle: # of patients that met criteria Resuscitation W/cystalloid fluid w/in 3 hrs for pt w/initial hypot 88% 86% Resuscitation w/cystalloid fluid w/in 3hrs for pt w/septic shock 83% 93% 83% 84% 80% 60% 73% 84% 76% 93% 94% Vasopressors for persist. Hypotension w/in 6 hrs 100% 100% 100% 83% 50% 100% 50% 100% 89% 100% 86% Repeat volume status/ tissue perfusion assessment w/in 6 hrs 75% 75% 90% 74% 80% 87% 73% 79% 84% 57% 77% Other: Central line inserted for septic shock patients 39% 41% 67% 63% 53% 73% 64% 42% 53% 50% 55% Survival rate for severe sepsis and septic shock patients 88% 88% 83% 88% 82% 80% 94% 95% 94% 88% 91% Readmission Rate 0% 2% 1% 3% 8% 5% 4% 9% 4% 6% 6%

74 Questions
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of
 Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Jawad Nazir, MD, FACP Medical Director, Infection Prevention and Control Avera Health and Avera McKennan Hospital Clinical Associate Professor of Medicine Sanford School of Medicine, Univ of South Dakota
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Sepsis Update: Early Identification and Management
 Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Update: Early Identification and Management Q&A From the Live Webinar Presenter: Tom Ahrens, RN, PhD, FAAN Live webinar: Thursday, May 09, 2013 The AACN Critical Care Webinar Series is not only
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
6-horas 24 horas Coleta de lactato Hemoculturas. Corticosteróides. Controle glicêmico. Fluidos/vasopressores. Otimização de SvO 2
 Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Novas diretrizes da Surviving Sepsis Campaign 2012 o que foi atualizado? Os pacotes da sepse 6-horas 24 horas Coleta de lactato Hemoculturas Corticosteróides Antibióticos Proteína C ativdada Fluidos/vasopressores
Pediatric Sepsis Treatment:
 Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
Disclosures Pediatric Sepsis Treatment: (treat) Early & (reevaluate) Often None June 11, 2018 Leslie Dervan, MD MS Pacific Northwest Sepsis Conference 1 Agenda Sepsis: pathophysiology at-a-glance Pediatric
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018
 Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018") Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
Sepsis Bundle Project (SEP) Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: April 2015 Most recent Revision: December 2018 Objectives 1. To identify the symptom of severe sepsis and septic shock syndrome.
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP
 Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP Objectives Review the changes to the 2012 sepsis guidelines and the 2016 Sepsis Guidelines Discuss the literature impacting the sepsis
Sepsis Guideline Updates LEANNE CURRENT MOORE, PHARMD, BCPS, BCCCP Objectives Review the changes to the 2012 sepsis guidelines and the 2016 Sepsis Guidelines Discuss the literature impacting the sepsis
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
SEPSIS 2015 DISCLOSURES FINANCIAL DISCLOSURES 9/1/2015. William M. Johnson, MD Nebraska Pulmonary Specialties. William Johnson
 SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
SEPSIS 2015 William M. Johnson, MD Nebraska Pulmonary Specialties 1 DISCLOSURES William Johnson No financial interests related to this presentation 2 FINANCIAL DISCLOSURES I do however have 3 children
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center
 UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
UPDATES IN SEPSIS MANAGEMENT Shannon Fry, Pharm.D. Critical Care Pharmacy Specialist St. Joseph Medical Center ShannonFry@fhshealth.org DISCLOSURE I have no financial relationships to disclose OBJECTIVES
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients. November/December 2017
 McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
McHenry Western Lake County EMS System CE for Paramedics, EMT-B and PHRN s Sepsis Patients November/December 2017 This month we are going to take a look at the patient with Sepsis. Webster s defines septic
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part II Questions and Answers Moderator: Candace Jackson, RN Inpatient Quality Reporting (IQR) Program Lead Hospital Inpatient Value, Incentives,
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
SEPSIS MANAGEMENT. Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah
 Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah") SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
SEPSIS MANAGEMENT Abdulhadi Tashkandi, MD, FRCP(c) Assistant Prof. Of Medicine Head of E.D. PMBAH-National Guard hospital Al-Madinah Al-Munawarah goals Treatment of pts. with septic shock consists of
Sepsis - A Year in Transition
 Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
Sepsis - A Year in Transition Todd L. Allen, MD, FACEP Chair, Emergency Department Development Team; Assistant Quality Officer, Institute for Healthcare Leadership Russell R. Miller, III, MD, MPH, FCCM
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Surviving Sepsis Campaign Updates
 Surviving Sepsis Campaign Updates Emily Kauffman, DO, MPH OSU Wexner Medical Center DISCLOSURE STATEMENT It is the policy of the American Osteopathic Association (AOA) and Ohio University Heritage College
Surviving Sepsis Campaign Updates Emily Kauffman, DO, MPH OSU Wexner Medical Center DISCLOSURE STATEMENT It is the policy of the American Osteopathic Association (AOA) and Ohio University Heritage College
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
TERMINOLOGY SIRS 10/30/2014 SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU
 Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Lisa Johnson DrNP, CRNP, ACNP BC Director, AG ACNP Program, DeSales University ACNP with Eastern Pennsylvania Infectious Disease Associates SURVIVING SEPSIS: FROM THE OFFICE TO THE ICU TERMINOLOGY Infection
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
SEPSIS AND SEPTICEMIA St. Charles Bend / Dec. 18, 2015
 SEPSIS AND SEPTICEMIA St. Charles Bend / Dec. 18, 2015 DEFINITIONS SYSTEMIC INFLAMMATORY RESPONSE SYNDROME SEPSIS SEVERE SEPSIS SEPTIC SHOCK MULTIPLE ORGAN FAILURE BACTEREMIA SEPTICEMIA THOMAS C CESARIO
SEPSIS AND SEPTICEMIA St. Charles Bend / Dec. 18, 2015 DEFINITIONS SYSTEMIC INFLAMMATORY RESPONSE SYNDROME SEPSIS SEVERE SEPSIS SEPTIC SHOCK MULTIPLE ORGAN FAILURE BACTEREMIA SEPTICEMIA THOMAS C CESARIO
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
Diagnosis and Management of Sepsis. Disclosures
 Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Diagnosis and Management of Sepsis David Shimabukuro, MDCM Medical Director, 13 ICU Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction I have no disclosures Disclosures 1 The following
Prehospital treatment of sepsis Christopher W. Seymour, MD MSc
 Prehospital treatment of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
Prehospital treatment of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
12/12/2017. Notice. Sepsis is defined as life-threatening organ dysfunction due to a dysregulated host response to infection.
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami