Clinical Case Conference
|
|
|
- Barbara Boyd
- 5 years ago
- Views:
Transcription

1 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1
2 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation therapy Conventional (RTOG 97-14, TROG 96-05, Norway/Sweden, Spanish) SBRT (Pittsburgh, Henry Ford, RTOG 0613) 2
3 Clinical Case 66 year old male with metastatic prostate cancer, originally diagnosed in 2006 S/p radical prostatectomy in 2006 with Gleason 3+4=7 prostate adenocarcinoma, confined to prostate with negative margins XRT to prostate fossa 70Gy in 35 fractions, completed 2008 Progressed through Lupron, abiraterone, and enzalutamide treatment, with osseous metastases discovered on bone scan in 2012 (C3/4, bilateral ribs) Started docetaxel in , began experiencing right sided leg pain, mostly at night Found to have large right intertrochanteric femur and L3 bony mets on bone scan 3 Case Epi Pathophys Sxs Imaging Surgery XRT
4 Epidemiology Common manifestation of distant relapse for many solid cancers (breast, lung, prostate most common) Up to 80% of patients with solid tumors will develop painful bone metastases to spine, pelvis, and extremities Breast, prostate, lung, thyroid, and kidney cancer account for 80% of all skeletal metastases Bone metastases develop in 50, 44, and 37% of patients with thyroid, lung, and renal cancer 70% of patients who die of cancer have spinal metastases at autopsy <14% are symptomatic 4 Case Epi Pathophys Sxs Imaging Surgery XRT



 Transport")



5 Pathophysiology Primary cancer Angiogenesis Invasion Embolism Response to microenvironment Multicell aggregates (lymphocytes, platelets) Transport Extravasation Adherence Arrest in distant capillary bed in bone Tumor cell proliferation Bone metastases 5 Case Epi Pathophys Sxs Imaging Surgery XRT


6 Osteolytic and osteoblastic metastases Osteolytic Lung Kidney Thyroid Multiple myeloma Osteoblastic Prostate Mixed Breast Testicular Ovarian 6 Case Epi Pathophys Sxs Imaging Surgery XRT
7 Common presentations and symptoms Many metastatic lesions cause little to no symptoms Pain is most common (~90%) presenting symptom Typically constant, present at night Can be poorly characterized, such as referred pain to the ribs Neurologic signs frequently preceded by pain Radiculopathy, myelopathy, cauda equina syndrome 7 Case Epi Pathophys Sxs Imaging Surgery XRT

8 Imaging Bone scan is more sensitive than plain films for sclerotic lesions CT scans are more specific, better for differentiating between Plain films and CT are helpful for detecting pathologic fracture MRI spine series is indicated in setting of suspected neurologic compromise PET/CT similar sensitivity to bone scan, but higher specificity Not effective for more differentiated tumors, i.e. prostate cancer 8 Case Epi Pathophys Sxs Imaging Surgery XRT

9 DG Imaging 9 Case Epi Pathophys Sxs Imaging Surgery XRT
10 Goals of care Goals of palliative treatment of painful bone metastases Pain relief Function preservation Maintenance of skeletal integrity Local XRT to painful sites can provide relief in ~ 60-85% of cases Early intervention may be useful in maintaining quality of life and minimizing side effects of analgesic medications 10 Case Epi Pathophys Sxs Imaging Surgery XRT


11 Surgery Vertebroplasty: Injection of bone cement to support weakened bones Provides immediate and substantial pain relief Kyphoplasty: Balloon inflation of compressed spine bone is performed before cement injection Used for compression fractures 11 Case Epi Pathophys Sxs Imaging Surgery XRT
12 Radiation therapy Conventional RTOG TROG Norway/Sweden Spanish study SBRT Pittsburgh Henry Ford RTOG Case Epi Pathophys Sxs Imaging Surgery XRT
13 Single versus multiple fraction treatment RT0G Phase III prospective randomized trial 898 patients with painful bone metastases (prostate or breast cancer) Excluded spinal cord compression, prior RT to area Life expectancy >3 months, KPS 40 Randomized to 2 arms: 8Gy x 1 fraction versus 3Gy x 10 fractions Primary endpoint: pain relief at 3 months Secondary endpoints Narcotic dose Subsequent pathologic dose Re-treatment dose 13
14 RTOG
15 RTOG
16 RTOG
17 RTOG Outcomes 8 Gy x 1 3 Gy x 10 Significance Complete Pain Relief 15% 18% NS Partial Pain Relief 50% 48% NS Stable Pain 26% 24% NS Progressive Pain 9% 10% NS Acute toxicity 10% 17% SS Retreatment 18% 9% SS Both regimens equivalent for pain control and narcotic relief at 3 months 8 Gy x 1 regimen: less acute toxicity; higher retreatment rate 17
18 Single versus multiple fraction treatment TROG Phase III prospective randomized trial 272 patients with neuropathic pain from bone metastasis No spinal cord compression, cauda equina syndrome, prior RT Life expectancy >3 months, KPS 40 Randomized to 2 arms: 8Gy x 1 fraction versus 4Gy x 5 fractions Primary endpoint: Whether 8Gy x 1 is as effective as 20Gy in 5 fractions in relieving neuropathic bone pain with respect to pain response within 2 months of start of RT and time to treatment failure (TTF) Secondary endpoints Acute side effects Rates of serious complications (pathological fracture and spinal cord/cauda equina compression) at index site 18
19 TROG

20 TROG

21 TROG
22 TROG Outcome 8 Gy x 1 4 Gy x 5 Significance Overall response rate (2 mo) 53% 61% NS Complete response rate (2 mos) 26% 27% NS Time to treatment failure 2.4 mo 3.7 mo NS Median OS: 4.8 months 8Gy x 1 was not shown to be as effective as 20Gy in 5 fractions, nor was it statistically significantly worse No significant differences in the rates of re-treatment, cord compression, or pathological fracture by treatment arm 22
23 Single versus multiple fraction treatment Norway/Sweden Phase III prospective randomized trial 376/1000 patients (trial closed early due to interim analysis findings) Included biopsy- or cytology-proven disease, bone metastasis (any site), KPS >40 Excluded spinal cord compression, previous RT to symptom site, life expectancy <6 weeks, bone surgery needed Randomized to 2 arms: 8Gy x 1 fraction versus 30Gy x 10 fractions Primary endpoint: Degree and duration of pain relief over the first 28 weeks Secondary endpoints Fatigue Quality of life 23
24 Norway/Sweden 24
25 Norway/Sweden 25
26 Norway/Sweden 26
27 Norway/Sweden Study terminated early at interim analysis Conclusions 8Gy x1 versus 30Gy in 10 fractions provides same degree of pain relief and impact on fatigue and overall quality of life is equivalent Recommend 8Gy x1 as standard treatment due to its much lower cost, greater convenience to patients, and being as effective for relief of pain due to bone metastasis as multiple fraction regimens 27

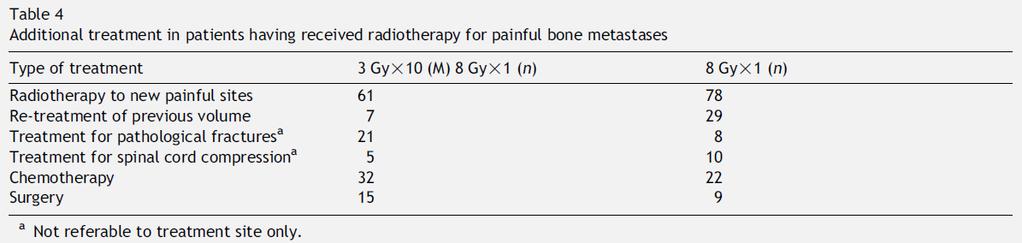
28 Norway/Sweden long-term follow-up 180 pts were included in the analysis Follow-up time until death 32 pts (18%) needed reirradiation Conclusions: Similar efficacy between 8 Gy x 1 and 3 Gy x 10 for treatment of painful bony mets Higher re-irradiation rate for 8 Gy x 1 group Single fraction treatment is considered more convenient as well as more cost-effective 28
29 Single versus multiple fraction treatment Spanish study Phase III prospective randomized trial 160 patients with painful bone metastases Included presence of multiple bone metastases but only one site of pain, life expectancy 4 weeks Excluded pain due to pathological fracture, spinal cord compression, pain at > 1 site, received prior RT at same site Randomized to 2 arms: 8Gy x 1 fraction versus 30Gy x 10 fractions Primary endpoint: Overall, complete, and partial responses Secondary endpoints Acute toxicity Re-treatment 29

30 Spanish study 30

31 Spanish study 31

32 Spanish study 32
33 Spanish study 8 Gy x 1 is as effective as 3 Gy x 10 in terms of complete, partial and overall response rate 8 Gy x 1 group had higher rate of re-irradiation 3 Gy x 10 8 Gy x 1 Significance Overall Response 86% 75% NS Complete Response 13% 15% NS Partial response 73% 60% NS Acute toxicity 18% 12% NS Retreatment 2% 28% SS 33

34 Single versus multiple fraction treatment summary 34
35 Conventional Radiation Symptomatic relief with conventional RT (ie. 30/10, 8/1) provides unsatisfactory results RTOG Arm 1) RT 8/1 vs. Arm 2) 30/10. Primary outcome pain relief at 3 months Outcome: 3-month complete pain relief 8/1 15% vs. 30/10 18% (NS); partial 50% vs. 48% (NS); stable 26% vs 24%; progressive 9% vs 10% TROG Randomized trial of 8 Gy in 1 versus 20 Gy in 5 fractions Response rate: 53% vs. 61% (p=ns) TTF 2.4 mo vs. 3.7 mo 35
36 SBRT UPMC Single institution prospective cohort study 500 cases of spinal metastases (cervical 15%, thoracic 42%, lumbar 22%, sacral 20%), treated with radiosurgery Maximum dose Gy (mean 20 Gy). Prior EBRT 69% (typically 30/10 or 35/14) PTV = GTV Long-term pain control 86%; at least some improvement in neurologic function in 85% 36
37 SBRT Henry Ford Single institution prospective cohort study 49 patients with 61 separate spinal metastases were treated with radiosurgery Dose ranged from Gy, single fraction PTV = involved spinal segment Median time to pain relief 14 days, fastest 24 hrs 1 yr overall pain control rate 84% Strong trend of increasing pain control with dose 14 Gy 37
38 SBRT RTOG 0613 Phase III randomized control trial 352 patients to be recruited Included are localized spine metastasis with up to 3 separate sites Excluded are cord compression/cauda equina, prior RT to site, nonambulatory Randomized to 2 arms (2:1): SBRT 16/18Gy x1 versus 8Gy x1 Primary endpoint: pain control at 3 months Secondary endpoints Rapidity of pain control Duration of pain response Quality of life Adverse events 38
39 SBRT Summary Dose escalation provides potential to improve local control and symptom relief over conventional treatment, especially in the setting of oligometastases and prolonged survival SBRT makes dose escalation possible while limiting dose to the spinal cord Rapid pain control Spares bone marrow especially in patients with multiple segments involved Shorter overall treatment time more convenient and less likely to interfere with systemic therapy 39

40 ASTRO SBRT consensus guidelines 40
41 References Chow et al. Lancet Oncol : Cox et al. IJROBP : Fairchild et al. IJROBP : Foro et al. Radiother Oncol : Gerszten et al. Spine : Hartsell et al. JNCI : Kaasa et al. Radiother Oncol : Konski et al. IJROBP : Lutz et al. IJROBP : Roos et al. Radiother Oncol :54-63 Ryu et al. Journal Pain Sympt Manage : Sande et al. Radiother Oncol :
42 RTOG Evaluated outcome differences by gender and partner status Gender, marital status, KPS and treatments were variables tested when evaluating the time to re-treatment Results: Longer time to retreatment in married men, married women, and single woman receiving 30Gy in 10 fractions No difference in retreatment rate over time in single men receiving either 8 Gy x 1 or 30Gy in 10 fractions Univariate analysis of the entire group with 30Gy in 10 fractions less likely to receive retreatment Conclusions: 8Gy x 1 group had higher retreatment rates Non-disease related variables, such as social support, might influence the results such as retreatment rate 42
43 RT0G No difference in retreatment rates in men without partners receiving either 8Gy x 1 or 30Gy in 10 fractions Patients receiving 8Gy x 1 had significantly higher retreatment rates compared with patients receiving 30Gy in 10 fractions Retreatment rates not influenced by initial pain score 43
44 RTOG 94-17: Economic Analysis RTOG 97-14: Is multiple fraction treatment cost-effective in treating patients with bone metastasis by preventing further re-treatment Markov Model to evaluate the cost-effectiveness Results: Incremental cost-effectiveness ration (ICER): $6973/quality-adjusted life year. Conclusions: Single fraction treatment was less expensive treatment in the treatment of patients with bone metastasis treated on RTOG Gy x 10 8 Gy x 1 Mean cost $ 2316 $ 998 Quality-adjusted survival 9.53 mos 7.26 mos 44
45 International patterns of practice in palliative radiotherapy for painful bone metastases: Evidence-base practice? Surveys showed single fraction schedules remain underused despite multiple randomized control trials demonstrating the equivalence of single fraction radiotherapy compared to multi-fraction radiotherapy Current patterns of practice internationally and factors influencing this practice Internet-based survey of members of ASTRO, CARO, Royal Australian and New Zealand College of Radiologists 5 hypothetical cases describing pts with single or multiple painful bone metastases from breast, lung, prostate cancer XRT dose fractionation recommended? Rating the importance of patient, tumor, institution, and treatment factors. 45
46 International patterns of practice in palliative radiotherapy for painful bone metastases: Evidence-base practice? Results 962 respondents (75% ASTRO members) 101 different dose schedules (3 Gy/1 to 60 Gy/20); overall median dose: 30 Gy/10 Single fractionation used least often by ASTRO members practicing in the US and most often by CARO members Case, membership affiliation, country of training, location of practice and practice type = Independent predictive factors of use of the single fraction radiotherapy Prognosis, risk of spinal cord compression, and performance status: principal factors considered when prescribing 46
47 International patterns of practice in palliative radiotherapy for painful bone metastases: Evidence-base practice? 47

48 International patterns of practice in palliative radiotherapy for painful bone metastases: Evidence-base practice? 48
49 International patterns of practice in palliative radiotherapy for painful bone metastases: Evidence-base practice? Conclusions: Most radiation oncologists continue to prescribe multi-fractionation schedules, despite abundant evidence Delay in the incorporation of evidence into practice for palliative radiotherapy for painful bone metastases 49
50 Re-irradiation : Multicenter, non-blinded, randomized, controlled trial 850 patients with painful bony metastases with prior radiation therapy Arm 1: 8 Gy/1 (425 pts) Arm 2: 20 Gy/8 (425 pts) 8 Gy x Gy x 8 Significance Overall response (intention-to-treat) 28% 32% NS Overal response in per-protocol population 45% 51% NS Lack of appetite 56% 66% SS Diarrhea 23% 31% SS No statistical difference in pathological fractures or cord/cauda equina compression Conclusions 8 Gy x 1 seems to be non-inferior and less toxic than 20 Gy in multiple fractions 50
51 Consortium SBRT contouring guidelines GTV Contour gross tumor using all available imaging Include epidural and paraspinal components of tumor CTV Include abnormal marrow suspicious for microscopic invasion Include bony CTV expansion to account for subclinical spread Should contain GTV Circumferential CTVs encircling the cord should be avoided PTV Uniform expansion around CTV CTV to PTV margin 3mm Never overlaps with cord Should contain entire CTV and GTV 51 Cox et al. IJROBP 2012
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Managing Bone Pain in Metastatic Disease. Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018
 Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Single-Fraction vs Multi-Fraction Radiotherapy in Palliative Bone Metastases Patients
 Single-Fraction vs Multi-Fraction Radiotherapy in Palliative Bone Metastases Patients Acknowledgements GVSU Statistical Consulting Center for help with statistical analysis GVSU Presidential Research Grant
Single-Fraction vs Multi-Fraction Radiotherapy in Palliative Bone Metastases Patients Acknowledgements GVSU Statistical Consulting Center for help with statistical analysis GVSU Presidential Research Grant
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Session 5: Isotope therapies and palliative radiotherapy
 Session 5: Isotope therapies and palliative radiotherapy Jeffrey Tuan, FRCR Radiation Oncology National Cancer Centre Singapore 15 Dec 2016 Bone metastases SREs are clinically important endpoints The burden
Session 5: Isotope therapies and palliative radiotherapy Jeffrey Tuan, FRCR Radiation Oncology National Cancer Centre Singapore 15 Dec 2016 Bone metastases SREs are clinically important endpoints The burden
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Disclosure. Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed to make this presentation possible!
 were harmed to make this presentation possible!") Disclosure The tolerance of the nervous system to SBRT: dogma, data and recommendations Paul Medin, PhD Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed
Disclosure The tolerance of the nervous system to SBRT: dogma, data and recommendations Paul Medin, PhD Paul Medin teaches radiosurgery courses sponsored by BrainLAB Many animals (and humans) were harmed
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
Second Single 4 Gy Reirradiation for Painful Bone Metastasis
 26 Journal of Pain and Symptom Management Vol. 23 No. 1 January 2002 Original Article Second Single 4 Gy Reirradiation for Painful Bone Metastasis Branislav Jeremic, MD, PhD, Yuta Shibamoto, MD, DMSc,
26 Journal of Pain and Symptom Management Vol. 23 No. 1 January 2002 Original Article Second Single 4 Gy Reirradiation for Painful Bone Metastasis Branislav Jeremic, MD, PhD, Yuta Shibamoto, MD, DMSc,
Conflict of interest disclosure
 Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
Stereotactic Body Radiation Therapy (SBRT) I: Radiobiology and Clinical Experience Brian Kavanagh, M.D., MPH University of Colorado Eric Chang, M.D. UT MD Anderson Conflict of interest disclosure I have
The use of surgery in the elderly. for management of metastatic epidural spinal cord compression
 The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
The use of surgery in the elderly Bone Tumor Simulators for management of metastatic epidural spinal cord compression Justin E. Bird, M.D. Assistant Professor Orthopaedic Oncology and Spine Surgery Epidemiology
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
a Phase II Randomised Controlled Trial Matthias Guckenberger
 Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Dose-intensified Image-guided Fractionated Stereotactic Body Radiation Therapy for Painful Spinal Metastases (DOSIS) versus Conventional Radiation Therapy: a Phase II Randomised Controlled Matthias Guckenberger
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Elderly men with prostate cancer + ADT
 Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
JMSCR Vol 06 Issue 12 Page December 2018
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.15 Single Institutional Comparative
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.15 Single Institutional Comparative
Palliative RT. Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University
 Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Palliative RT Jiraporn Setakornnukul, M.D. Radiation Oncology Division Siriraj Hospital, Mahidol University Scope Brain metastasis Metastasis epidural spinal cord compression SVC obstruction Bone pain
Bone metastases of solid tumors Diagnosis and management by
 Bone metastases of solid tumors Diagnosis and management by Dr/RASHA M Abd el Motagaly oncology consultant Nasser institute adult oncology unit 3/27/2010 1 Goals 1- Know the multitude of problem of bone
Bone metastases of solid tumors Diagnosis and management by Dr/RASHA M Abd el Motagaly oncology consultant Nasser institute adult oncology unit 3/27/2010 1 Goals 1- Know the multitude of problem of bone
CLINICAL APPLICATION OF LINEAR-QUADRATIC MODEL IN REIRRADIATION OF SYMPTOMATIC BONE METASTASES
 MEDICAL PHYSICS CLINICAL APPLICATION OF LINEAR-QUADRATIC MODEL IN REIRRADIATION OF SYMPTOMATIC BONE METASTASES L. REBEGEA 1,2, M. DUMITRU 1, D. FIRESCU 2,3 1 Sf. Ap. Andrei Emergency Clinical Hospital,
MEDICAL PHYSICS CLINICAL APPLICATION OF LINEAR-QUADRATIC MODEL IN REIRRADIATION OF SYMPTOMATIC BONE METASTASES L. REBEGEA 1,2, M. DUMITRU 1, D. FIRESCU 2,3 1 Sf. Ap. Andrei Emergency Clinical Hospital,
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Vertebral Body Compression Fracture Following Spine SBRT
 RADIATION ONCOLOGY & MOLECULAR RADIATION SCIENCES Vertebral Body Compression Fracture Following Spine SBRT Kristin J. Redmond, MD, MPH Disclosure & Disclaimer An honorarium is provided by Accuray for this
RADIATION ONCOLOGY & MOLECULAR RADIATION SCIENCES Vertebral Body Compression Fracture Following Spine SBRT Kristin J. Redmond, MD, MPH Disclosure & Disclaimer An honorarium is provided by Accuray for this
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Painful vertebral metastases are a frequent manifestation of malignancies
 2892 COMMUNICATION Palliative Radiation Therapy for Painful Vertebral Metastases A Practice Survey Tejpal Gupta, M.D., D.N.B. Rajiv Sarin, M.D. Department of Radiation Oncology, Tata Memorial Hospital,
2892 COMMUNICATION Palliative Radiation Therapy for Painful Vertebral Metastases A Practice Survey Tejpal Gupta, M.D., D.N.B. Rajiv Sarin, M.D. Department of Radiation Oncology, Tata Memorial Hospital,
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Bone Health in the Cancer Patient. Stavroula Otis, M.D. Primary Care and Oncology: Practical Lessons Conference Brea Community Center May 10, 2018
 Bone Health in the Cancer Patient Stavroula Otis, M.D. Primary Care and Oncology: Practical Lessons Conference Brea Community Center May 10, 2018 Overview Healthy bone is in a constant state of remodelling
Bone Health in the Cancer Patient Stavroula Otis, M.D. Primary Care and Oncology: Practical Lessons Conference Brea Community Center May 10, 2018 Overview Healthy bone is in a constant state of remodelling
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Minesh Mehta, Northwestern University. Chicago, IL
 * Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
* Minesh Mehta, Northwestern University Chicago, IL Consultant: Adnexus, Bayer, Merck, Tomotherapy Stock Options: Colby, Pharmacyclics, Procertus, Stemina, Tomotherapy Board of Directors: Pharmacyclics
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Benefits of Radiation Therapy in the Palliative Cancer Patient
 Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Benefits of Radiation Therapy in the Palliative Cancer Patient Dr Joshua Sappiatzer Radiation Oncologist Page 1 Overview Why we should aim for better palliative radiotherapy treatment Bone metastases Rapid
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
8/3/2017. Spine SBRT: A Clinician's Update On Techniques and Outcomes. Disclosures. Outline
 Spine SBRT: A Clinician's Update On Techniques and Outcomes Chia-Lin (Eric) Tseng, MD FRCPC Radiation Oncologist Sunnybrook Health Sciences Centre University of Toronto August 3, 2017 Disclosures I have
Spine SBRT: A Clinician's Update On Techniques and Outcomes Chia-Lin (Eric) Tseng, MD FRCPC Radiation Oncologist Sunnybrook Health Sciences Centre University of Toronto August 3, 2017 Disclosures I have
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
20. Background. Oligometastases. Oligometastases: bone (including spine) and lymph nodes
 and lymph nodes") 125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
125 20. Oligometastases Background The oligometastatic state can be defined as 1 3 isolated metastatic sites, typically occurring more than six months after successful treatment of primary disease. 1 In
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Palliative treatments for lung cancer: What can the oncologist do?
 Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Palliative treatments for lung cancer: What can the oncologist do? Neil Bayman Consultant Clinical Oncologist GM Cancer Palliative Care and Lung Cancer Education Event Manchester, 31 st January 2017 Most
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Winston Tan MD FACP Associate Professor of Medicine Mayo Clinic Florida
 Winston Tan MD FACP Associate Professor of Medicine Mayo Clinic Florida } none } To develop an understanding of the management of bone metastasis through a multidisciplinary approach } Enable the learner
Winston Tan MD FACP Associate Professor of Medicine Mayo Clinic Florida } none } To develop an understanding of the management of bone metastasis through a multidisciplinary approach } Enable the learner
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Metastatic Spinal Disease
 Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Metastatic Spinal Disease Mr Neil Chiverton Consultant Spinal Surgeon, Sheffield Objectives The scale and nature of the problem NICE recommendations Surgical decision making Case illustrations Incidence
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience. Kevin Yiee MD, MPH Resident Physician
 Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Tecniche Radioterapiche U. Ricardi
 Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Tecniche Radioterapiche U. Ricardi UNIVERSITA DEGLI STUDI DI TORINO Should we always rely on stage? T4N0M0 Stage IIIB T2N3M0 Early stage NSCLC The treatment of choice for early-stage NSCLC is anatomic
Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience.
 Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience. Elisabetta Ponti MD, Gianluca Ingrosso MD, Alessandra Carosi PhD, Luana
Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience. Elisabetta Ponti MD, Gianluca Ingrosso MD, Alessandra Carosi PhD, Luana
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms. Overall Clinical Significance 8/3/13
 Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Stereotactic Radiosurgery for Brain Metastasis: Changing Treatment Paradigms Jason Sheehan, MD, PhD Departments of Neurosurgery and Radiation Oncology University of Virginia, Charlottesville, VA USA Overall
Malignant Spinal cord Compression. Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania
 Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
Malignant Spinal cord Compression Dr. Thiru Thirukkumaran Palliative Care Services - Northwest Tasmania Background Statistics of SCC -1 Incidence of SCC Vertebral body metastases 85 % Para-vertebral (Lymphoma)
The Physics of Oesophageal Cancer Radiotherapy
 The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
The Physics of Oesophageal Cancer Radiotherapy Dr. Philip Wai Radiotherapy Physics Royal Marsden Hospital 1 Contents Brief clinical introduction Imaging and Target definition Dose prescription & patient
Re-irradiation for painful bone metastases: evidence-based approach
 Editor s note: Palliative Radiotherapy Column features articles emphasizing the critical role of radiotherapy in palliative care. Chairs to the columns are Dr. Edward L.W. Chow from Odette Cancer Centre,
Editor s note: Palliative Radiotherapy Column features articles emphasizing the critical role of radiotherapy in palliative care. Chairs to the columns are Dr. Edward L.W. Chow from Odette Cancer Centre,
DRAFT FOR CONSULTATION. Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain
 Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain Information Reader Box (IRB) to be inserted on inside front cover for documents of 6 pages and over, with Publications Gateway
Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain Information Reader Box (IRB) to be inserted on inside front cover for documents of 6 pages and over, with Publications Gateway
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD
 Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
International Spine Radiosurgery Consortium Consensus Guidelines for Target Volume Definition in Spinal Stereotactic Radiosurgery
 CME International Journal of Radiation Oncology biology physics www.redjournal.org Clinical Investigation: Central Nervous System Tumor International Spine Radiosurgery Consortium Consensus Guidelines
CME International Journal of Radiation Oncology biology physics www.redjournal.org Clinical Investigation: Central Nervous System Tumor International Spine Radiosurgery Consortium Consensus Guidelines
ACR Appropriateness Criteria Spinal Bone Metastases EVIDENCE TABLE
 1. Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group.
1. Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group.
Lung Cancer Radiotherapy
 Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors
 Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
Minimally Invasive Radiofrequency Ablation Treatment of Metastatic Spinal Tumors 1 Objectives Demographics of spinal tumors Treatment options and goals Adoption of RF ablation for pain palliation by NCCN
8/2/2018. Acknowlegements: TCP SPINE. Disclosures
 A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
External beam radiotherapy and bone metastases
 Review Article External beam radiotherapy and bone metastases Candice Johnstone 1, Stephen T. Lutz 2 1 Department of Radiation Oncology, Medical College of Wisconsin, Milwaukee, Wisconsin, USA; 2 Department
Review Article External beam radiotherapy and bone metastases Candice Johnstone 1, Stephen T. Lutz 2 1 Department of Radiation Oncology, Medical College of Wisconsin, Milwaukee, Wisconsin, USA; 2 Department
The surgical treatment of metastatic disease of the spine
 The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
The surgical treatment of metastatic disease of the spine Péter Banczerowski National Institute of Neurosurgery, Budapest Spine tumours 15% of the primary tumours of the CNS affect the spine The spine
SBRT in early stage NSCLC
 SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
SBRT in early stage NSCLC Optimal technique and tumor dose Frank Zimmermann Clinic of Radiotherapy and Radiation Oncology University Hospital Basel Petersgraben 4 CH 4031 Basel radioonkologiebasel.ch Techniques
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
4D Radiotherapy in early ca Lung. Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla
 4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
4D Radiotherapy in early ca Lung Prof. Manoj Gupta Dept of Radiotherapy & oncology I.G.Medical College Shimla Presentation focus on ---- Limitation of Conventional RT Why Interest in early lung cancer
Treatment Planning & IGRT Credentialing for NRG SBRT Trials
 Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Treatment Planning & IGRT Credentialing for NRG SBRT Trials Hania Al Hallaq, Ph.D. Department of Radiation & Cellular Oncology The University of Chicago Learning Objectives Explain rationale behind credentialing
Cement augmentation in spinal tumors: a systematic review comparing vertebroplasty and kyphoplasty
 35 35 43 Cement augmentation in spinal tumors: a systematic review comparing vertebroplasty and kyphoplasty Authors Josh E Schroeder¹, Erika Ecker², Andrea C Skelly², Leon Kaplan¹ Institutions ¹ Orthopedic
35 35 43 Cement augmentation in spinal tumors: a systematic review comparing vertebroplasty and kyphoplasty Authors Josh E Schroeder¹, Erika Ecker², Andrea C Skelly², Leon Kaplan¹ Institutions ¹ Orthopedic
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
SBRT in Pancreas Cancer Role of The Radiosurgery Society
 SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
Defining Target Volumes and Organs at Risk: a common language
 Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Defining Target Volumes and Organs at Risk: a common language Eduardo Rosenblatt Section Head Applied Radiation Biology and Radiotherapy (ARBR) Section Division of Human Health IAEA Objective: To introduce
Metastatic Bone Adenocarcinoma with Positive TTF-1 Tumor Stain with a Lung Mass: the Role and Treatment Consideration of RT
 Metastatic Bone Adenocarcinoma with Positive TTF-1 Tumor Stain with a Lung Mass: the Role and Treatment Consideration of RT Case Number: RT2009-74(M) Potential Audiences: Intent Doctor, Oncology Special
Metastatic Bone Adenocarcinoma with Positive TTF-1 Tumor Stain with a Lung Mass: the Role and Treatment Consideration of RT Case Number: RT2009-74(M) Potential Audiences: Intent Doctor, Oncology Special
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
A Subset Analysis of Radiation Therapy Oncology Group Trial 97-14
 Single-Fraction Radiotherapy Versus Multifraction Radiotherapy for Palliation of Painful Vertebral Bone Metastases Equivalent Efficacy, Less Toxicity, More Convenient A Subset Analysis of Radiation Therapy
Single-Fraction Radiotherapy Versus Multifraction Radiotherapy for Palliation of Painful Vertebral Bone Metastases Equivalent Efficacy, Less Toxicity, More Convenient A Subset Analysis of Radiation Therapy
ACR Appropriateness Criteria Metastatic Epidural Spinal Cord Compression and Recurrent Spinal Metastasis EVIDENCE TABLE
 . Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet Neurol. 2008;7(5):59-66. 2. Loblaw DA, Mitera G, Ford M, Laperriere NJ. A 20 updated systematic review and clinical practice
. Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet Neurol. 2008;7(5):59-66. 2. Loblaw DA, Mitera G, Ford M, Laperriere NJ. A 20 updated systematic review and clinical practice
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
PALLIATIVE RADIOTHERAPY FOR BONE METASTASES: AN ASTRO EVIDENCE-BASED GUIDELINE
 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 965 976, 2011 Copyright Ó 2011 American Society for Radiation Oncology and American College of Radiology Printed in the USA. All rights reserved
Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 965 976, 2011 Copyright Ó 2011 American Society for Radiation Oncology and American College of Radiology Printed in the USA. All rights reserved
Current Management of Metastatic Bone Disease
 Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Current Management of Metastatic Bone Disease Evaluation and Medical Management Dr. Sara Rask Head, Medical Oncology Simcoe Muskoka Regional Cancer Centre www.rvh.on.ca Objectives 1. Outline an initial
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
ASTRO econtouring for Lymphoma. Stephanie Terezakis, MD
 ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia
 for Brain Metastasis in Nova Scotia") A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
A Population-Based Study on the Uptake and Utilization of Stereotactic Radiosurgery (SRS) for Brain Metastasis in Nova Scotia Gaurav Bahl, Karl Tennessen, Ashraf Mahmoud-Ahmed, Dorianne Rheaume, Ian Fleetwood,
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
SYNOPSIS PROTOCOL N UC-0107/1602
 SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas
 Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological