Attitudes and risk of addiction in Patients Suffering from Chronic Pain and Treated with Long-Term Opioid Therapy
|
|
|
- Oscar Evans
- 5 years ago
- Views:
Transcription


1 Attitudes and risk of addiction in Patients Suffering from Chronic Pain and Treated with Long-Term Opioid Therapy Dr. Grisell Vargas-Schaffer Pain center at CHUM University of Montreal Canada
2 Conflict of interest Astra Zeneca Research funds Conferences Services: travel expenses, accommodation Bayer X x x Medical Advisory Jansen-Ortho x x x Lille x X Merck Frosst x x Pfizer Purdue Pharma x x x x

3 Moral commitment If, in my presentation I suggested off-label for a drug, I agree to inform the audience. I agree to use as far as possible, the pharmacologic terminology instead of brand names.




4 Changes in the Treatment of Chronic Pain Tremendous progress has been made in the study and treatment of pain in the past 2 decades. Efforts have been undertaken to make pain assessment and treatment a priority of medical care and to use all of the weapons in our arsenal to bring relief to the millions of people with chronic pain. However, this progress has been somewhat tempered by the souring of the regulatory climate and the growth of prescription drug abuse.
5 Changes in the Treatment of Chronic Pain Despite these setbacks, the use of long-term opioid therapy to treat chronic non-cancer pain is growing, based in part on evidence from clinical trials and a growing consensus among pain specialists. The appropriate use of these drugs requires skill in the prescription of opioids, knowledge of the issues related to addiction, and a commitment to performing and documenting a comprehensive assessment repeatedly over time.




6 Equipoise We are neither opiophobic nor opiophilic we are supportive of an adequate pain treatment for our patients.
7 3A-CP Study Attitude Addiction Alexithymia In Chronic Pain Patients with long-term opioid therapy.

8 3A-CP Study How many of you believe that patients with chronic pain have a negative attitude towards opioids? How many of you believe that chronic pain patients have a high risk addiction?
9 Original Hypotheses 1. We hypothesized that patients attending the chronic pain center would have high pain scores, a highly negative attitude towards taking opioids 2. We also wished to evaluate the level of risk of addiction in patients with long-term opioid therapy.
10 Study Overview University based chronic pain center. The protocol was approved by the university hospital ethics committee. Patients received an invitation to participate in the mail and completed the questionnaires over the phone. We used French language validated questionnaires. Data analysis was carried out by Montreal Heart Institute Coordinating Center (MHICC).
11 Study exclusion criteria Patients do not take any opioids. Patients with less than 12 month of treatment with opioids. Patients do not speak French. Patients excluded for hospitalisation. Patients who died. Patients-unreachable (tried to reach to at least 3 times with no response)
12 Study inclusion criteria Patients signed the inform consent. Patients with more than one year of treatment with opioids.
13 Study Population 303 patients

14 Study Population (N=303) 63% 36.9% Age Mean age 59.6 years Age range 26 to 91 years Under 65 years 74%
15 Level of Education (N=303) Level of Education N Percent Elementary school High school College University % N/D
16 Job Status (N=303) Job status Workman's compensation or similar Frequency Percent Retired Working (full or partial time) Unemployed Others (housework, N/D) %

17 Types of Pain (N=303)
18 Type of pain (N=303) Type of pain Frequency Percent Spinal pain Musculoskeletal pain Neuropathic pain Fibromyalgia CRPS Abdominal pain Arthritis, arthrosis pain Chest pain Others %
19 Mean Pain Intensity (N= 303) NRS (0-10) 5.5 Level of pain at time of questionnaire 95% CI Average pain in the last 7 days Worst pain in last 7 days
20 Time Course of Suffering, Treatment and Medication (N=303) Mean (years) 10.9 Length of time suffering from chronic pain 95% CI Length of time taking opioids Length of follow-up time in our pain clinic
21
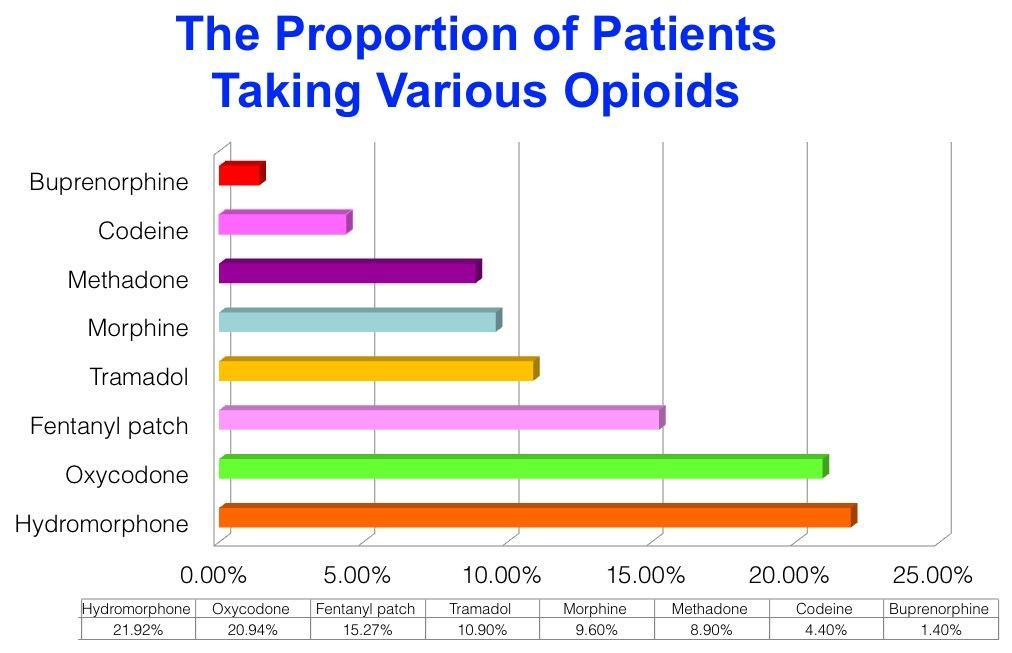
22 Morphine Equivalents (mg per day) (N=303) Opioids used for treatment N Median (mg) Q1 Q2 Codeine Tramadol Buprenorphine Morphine Oxycodone Hydromorphone Fentanyl Methadone
23 Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain Recommendations: Chronic non-cancer pain can be managed effectively in most patients with dosages at or below 200 mg/day of morphine or the equivalent. Consideration of a higher dosage requires careful reassessment of the pain and of the risk for misuse, and frequent monitoring for evidence of improved patient outcomes. Canadian Medical Association Journal (vol. 182, no. 13, pp )
24 Median Number of Morphine Equivalents Per Day for Patients Taking Several Opioids Concurrently (N=291) Number of opioids N Median Q1 Q

25 Cannabis Morphine equivalents not available. 5 patients taking cannabis and another opioid. 7 patients taking only synthetic cannabis.
26 The Drug Attitude Inventory (DAI)
27 Attitudes Towards Medications A multitude of factors play a role in a patient's decision as to whether or not to take medication. Attitudes and beliefs about health and illness have been consistently identified as the major factors in such decisions. A patient s attitudes towards drugs that have a social stigma may play an important role in whether or not they commit to a treatment.
28 The Drug Attitude Inventory (DAI) The aim of this questionnaire is to gain some understanding of what people think about medications and their experiences while taking them. It was designed to identify the subjective responses of patients with schizophrenia taking neuroleptic drugs and their attitude towards disease and treatment. Howan, Awad Psychological Med. 1983


29 Similarities Between the Patients with Chronic Pain and Patients with Schizophrenia The chronic use of medication. The social stigma attached to these medications. The need to take these drugs to be functional.
30 Creating the DAI-M Using this questionnaire for patients in a pain clinic required a few small wording changes. We contacted Dr. Awad (DAI author) who approved the changes. The French validated version was used.
31 The Drug Attitude Inventory DAI-10 Modified with Author's Permission Questions T F 1) For me, the good things about medication outweigh the bad 2) I feel strange, "doped up", on medication 3) I take medications of my own free choice 4) Medications make me feel more relaxed 5) Medication makes me feel tired and sluggish 6) I feel more normal on medication 7) I take medication only when I feel pain* 8) It is unnatural for my mind and body to be controlled by medications 9) My thoughts are clearer on medication 10) Taking medication will prevent me from having crises of pain ** * I take medication only when I feel ill ** Taking medication will prevent me from having a breakdown Howan, Awad Psychological Med. 1983
32 Results of the DAI-M DAI-M N Percent Positive Attitude Negative Attitude Neutral Attitude Incomplete
33 Questions to Assess Feelings of Dependence and Stigma We created five additional questions to assess the following items: Feelings of dependence Sense of stigmatism while taking opioids
34 The Dependence and Stigma Questions (N=303) Questions 1) I feel dependent on painkillers to be functional 2) I'm afraid of the medication, but I take it because it decreases the intensity of pain. 3) I take medication without telling my family that they are opioids 4) I feel dependent on my medication to relieve pain 5) I feel criticized by my family and/or my friends when I take opioids for pain relief. T F
35 The Dependence and Stigma Questions (N=303) Questions 1 and 4 were added to assess feelings of dependence. Questions 3 and 5 were added to assess the potential sense of stigma that patients may experience when taking opioids for chronic pain management. Question 2 is a measure of the presence of fear.
36 Questions Regarding Feelings of Dependence (N=303) Questions I feel dependent on opioids to be functional 67.0* 33.0 I feel dependent on my medication to relieve pain 77.8* 21.4 T % F %
37 Questions Regarding Feelings of Stigma (N=303) Questions I take medication without telling my family that they are opioids 10.8* 88.4 I feel criticized by my family and/or my friends when I take opioids for pain relief. T % F % 23.1* 76.5
38 Question Regarding Fear of Taking Opioids (N=303) Question I'm afraid of the medication, but I take it because it decreases the intensity of pain. T % F % 41.6* 58.4


39 3A-CP Study Attitude Addiction In Chronic Pain Patients with long-term opioid therapy
40 Addiction in Patients with Chronic Pain We used two questionnaires to assess the risk of addiction in patients treated with long-term opioid therapy (LtOT). The Opioid Risk Tool (ORT). The Screening Tool for Addiction Risk (STAR).

41 Opioid Risk Tool (ORT) 5-item questionnaire with yes or no answers. Designed to predict the probability of patients displaying aberrant drug behavior when opioids are prescribed for chronic pain. Recommended tool both nationally and provincially for the safe and effective use of opioids for non-cancer pain. Webster Pain Med 2005 Collège des Médecins du Québec 2009 Canadian Medical Association Journal 2010
42 Opioids Risk Tool (ORT) Webster Pain Med 2005
43 History of Substance Abuse (N=303) Family history Alcohol Illegal drugs 35.3% yes Prescriptions drugs 10.2% yes 11.5% yes 57% 17% 6% Personal history Alcohol Illegal drugs 10.8% yes Prescriptions drugs 5.9% yes 9.2% yes 21% 14% 18%
44 History of other Relevant Risk Factors History of preadolescent sexual abuse 15.1% yes 26% Age % yes 56% ADD Psychological disease OCD Bipolar 6.2% yes 22% Schizophrenia Depression 54.4% yes 65%
45 Opioid Risk Tool (ORT) Low risk: 0-3 Unlikely to abuse opioids Moderate risk: 4-7 As likely will as won t abuse opioids High risk: >=8 Likely to abuse opioids

46 Results of ORT Low risk Addiction 88.0% Moderate risk Addiction 11.2% Low risk: 0-3 Moderate risk: 4-7 High risk: >=8 High risk Addiction 0.6%
47 The Screening Tool for Addiction Risk (STAR) The STAR questionnaire was reported for the first time in item (yes/no) questionnaire. It was developed to identify the cases of substance abuse in patients with chronic pain and long-term opioid treatment. Freidman 2003
48 The Screening Tool for Addiction Risk (STAR) Questions T F 1. Have you felt depressed or anxious over the last 6 months? Have you noticed frequent mood swings over the last 6 months? Are you currently employed? Do you smoke cigarettes? Do you feel that you smoke too much? Do you drink more than three alcohol drinks/day? Have you used recreational drugs during the last year? Have you ever been treated in a drug or alcohol rehabilitation facility? Do you get pain medicine from more than one doctor? Have you been to a pain clinic before? Have you visited an emergency room for pain treatment in the past year? Has anyone in your family (relatives you don t live with) had problems with drug or alcohol abuse? 13. Has anyone in your household (partner, children) had problems with drug or alcohol abuse? Did any family member physically or verbally abuse you when you were a child? Freidman 2003
49 The Screening Tool for Addiction Risk (STAR) Logistic regression showed that history of treatment in a drug or alcohol rehabilitation facility was a significant predictor of addiction with a positive predictive value of 93% and a negative predictive value of 5.9%. Factor analysis revealed that questions relating to tobacco abuse and prior treatment for drug and alcohol abuse distinguished between patients with addiction and pain from patients with chronic pain and long-term opioid therapy. Freidman 2003
50 The Screening Tool for Addiction Risk (STAR) Do you smoke cigarettes? Yes % No % Do you feel that you smoke too much? 4.2% 95.8% Have you ever been treated in a drug or alcohol rehabilitation facility?
51 Level of Addiction in Our Population We had no idea what the risk of addiction would be in our population, The generally held opinion is that risk of addiction in patients with long-term opioid therapy is high, We expected to find high levels such as those sited by Friedman of 27%. We found that the level of risk of addiction in our population is extremely low. ORT: 0.6 % and STAR 4.2%.
52 Conclusion (1) Attitude 38.2 % of patients had a negative attitude towards taking opioids. Patients taking long-term opioid therapy do not feel stigmatized. Addiction ORT: 11.8% with a moderate or high risk of addiction. STAR: 4.2% were found to be at risk for addiction.
53 Conclusion (2) We suggest for the evaluation of risk of addiction: complete the ORT add the 3 relevant questions from STAR This may increase the power to detect patients who are at higher risk for abuse or addiction.

54 Conclusion (3) Because patients do not suffer from the stigma related to long-term opioid therapy, and have a low risk of addiction we can go further in relieving pain by adequately prescribing and adjusting medication.
55 Conclusion (4) Main study limitation: Our results are specific to a tertiary care pain center population therefore may not be easily generalizable to the primary care setting. This study concerns patients with an average of 6 years of LtOT and 5 years of follow-up therefore it is likely that patients with a high risk of addiction have undergone a natural attrition from the pain clinic.
56 Take home message Despite public opinion to the contrary, patients in chronic pain treatment programs are not addicts. We need to listen to our patients, believe their descriptions of their pain and treat them accordingly. We have the opportunity to encourage our patients to be more pro-active in their treatment.
57 Take home message How can we do this? By educating patients and practitioners. By treating patients and not blaming them.


58 Thanks for your attention Questions?...
59 Bibliography Tunks ER, Weir R, Crook J. Epidemiologic perspective on chronic pain treatment. Can.J.Psychiatry 2008; 53: Crook J, Tunks E, Rideout E, Browne G. Epidemiologic comparison of persistent pain sufferers in a specialty pain clinic and in the community. Arch.Phys.Med.Rehabil. 1986; 67: Bell K, Salmon A. Pain, physical dependence and pseudoaddiction: redefining addiction for 'nice' people? Int.J.Drug Policy 2009; 20: Mendelson J, Flower K, Pletcher MJ, Galloway GP. Addiction to prescription opioids: characteristics of the emerging epidemic and treatment with buprenorphine. Exp.Clin.Psychopharmacol. 2008; 16: Peker L, Celebi N, Canbay O et al. Doctors' opinions, knowledge and attitudes towards cancer pain management in a university hospital. Agri. 2008; 20: Ward S, Hughes S, Donovan H, Serlin RC. Patient education in pain control. Support.Care Cancer 2001; 9: Ward SE, Carlson-Dakes K, Hughes SH, Kwekkeboom KL, Donovan HS. The impact on quality of life of patientrelated barriers to pain management. Res.Nurs.Health 1998; 21: Portenoy RK. Opioid therapy for chronic nonmalignant pain: a review of the critical issues. J.Pain Symptom.Manage. 1996; 11: Sutherland G, Edwards G, Taylor C, Phillips G, Gossop M, Brady R. The measurement of opiate dependence. Br.J.Addict. 1986; 81: Canadian Medical Association Journal (vol. 182, no. 13, pp )
60 Bibliography Definitions related to the use of opioids for the treatment of pain. WMJ. 2001; 100: Hogan TP, Awad AG, Eastwood R. A self-report scale predictive of drug compliance in schizophrenics: reliability and discriminative validity. Psychol.Med. 1983; 13: Awad AG, Hogan TP, Voruganti LN, Heslegrave RJ. Patients' subjective experiences on antipsychotic medications: implications for outcome and quality of life. Int.Clin.Psychopharmacol. 1995; 10 Suppl 3: De Las CC, Sanz EJ. Attitudes toward psychiatric drug treatment: the experience of being treated. Eur.J.Clin.Pharmacol. 2007; 63: Friedman R, Li V, Mehrotra D. Treating pain patients at risk: evaluation of a screening tool in opioid-treated pain patients with and without addiction. Pain Med. 2003; 4: Webster LR, Webster RM. Predicting aberrant behaviors in opioid-treated patients: preliminary validation of the Opioid Risk Tool. Pain Med. 2005; 6:
Risk-Assessment Instruments for Pain Populations
 Risk-Assessment Instruments for Pain Populations The Screener and Opioid Assessment for Patients with Pain (SOAPP) The SOAPP is a 14-item, self-report measure that is designed to assess the appropriateness
Risk-Assessment Instruments for Pain Populations The Screener and Opioid Assessment for Patients with Pain (SOAPP) The SOAPP is a 14-item, self-report measure that is designed to assess the appropriateness
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Brief Pain Inventory (Short Form)
") Brief Pain Inventory (Short Form) Study ID# Hospital# Do not write above this line Date: Time: Name: Last First Middle Initial 1) Throughout our lives, most of us have had pain from time to time (such
Brief Pain Inventory (Short Form) Study ID# Hospital# Do not write above this line Date: Time: Name: Last First Middle Initial 1) Throughout our lives, most of us have had pain from time to time (such
Monte H. Moore, MD. Idaho Physical Medicine and Rehabilitation. Meridian, ID
 Monte H. Moore, MD Idaho Physical Medicine and Rehabilitation Meridian, ID Chronic pain brief review Opiates important things to know Factors in determining whether to use an opiate What to watch for if
Monte H. Moore, MD Idaho Physical Medicine and Rehabilitation Meridian, ID Chronic pain brief review Opiates important things to know Factors in determining whether to use an opiate What to watch for if
Universal Precautions in Pain Management A Rational Approach to Management of Chronic Pain
 Universal Precautions in Pain Management A Rational Approach to Management of Chronic Pain Douglas Gourlay, MD, FRCPC, FASAM Wasser Pain Management Centre; Centre for Addiction and Mental Health Toronto,
Universal Precautions in Pain Management A Rational Approach to Management of Chronic Pain Douglas Gourlay, MD, FRCPC, FASAM Wasser Pain Management Centre; Centre for Addiction and Mental Health Toronto,
Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R)
") Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) The Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) is a tool for clinicians to help determine how much
Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) The Screener and Opioid Assessment for Patients with Pain- Revised (SOAPP -R) is a tool for clinicians to help determine how much
Where is your pain located? Please use the diagram below to indicate where most of your pain is located.
 Name: Address: Social Security Number: Email Address: Emergency Contact: Primary Care Physician: Name: Address: Phone Number: Date of Birth: Today's date: Cell Phone Number: Phone #: Referring Physician:
Name: Address: Social Security Number: Email Address: Emergency Contact: Primary Care Physician: Name: Address: Phone Number: Date of Birth: Today's date: Cell Phone Number: Phone #: Referring Physician:
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk
 Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
Chronic Pain, Opioids, & Addiction: Assessing and Managing Risk Randy Brown MD, PhD, FASAM Associate Professor, Dept of Family Medicine Director, Center for Addictive Disorders, UWHC Director, UW Addiction
PATIENT REGISTRATION Form
 318 Richmond Road Ottawa, ON K1Z 6X6 p: 613-695-4923 f: 343-888-2004 e: info@hybridpharm.com PATIENT REGISTRATION Form PATIENT INFORMATION Are you applying for: Myself I am a caregiver First Name(s): Last
318 Richmond Road Ottawa, ON K1Z 6X6 p: 613-695-4923 f: 343-888-2004 e: info@hybridpharm.com PATIENT REGISTRATION Form PATIENT INFORMATION Are you applying for: Myself I am a caregiver First Name(s): Last
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Opioids and Older Adults
 Opioids and Older Adults Kate Lorig, DrPH kate@selfmanagementresource.com Beth Darnall, Ph.D. Twitter: @BethDarnall Heather Zuercher Let me bring you our sponsors SMRC@selfmanagementresource.com
Opioids and Older Adults Kate Lorig, DrPH kate@selfmanagementresource.com Beth Darnall, Ph.D. Twitter: @BethDarnall Heather Zuercher Let me bring you our sponsors SMRC@selfmanagementresource.com
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
MATCP When the Severity of Symptoms Interferes with Progress
 MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
MATCP 2017 When the Severity of Symptoms Interferes with Progress 1 Overview Stages of Change, or Readiness for Change Changing Behavior Medication Adherence Disruptive Behaviors Level of Care Tools including
CBT Intake Form. Patient Name: Preferred Name: Last. First. Best contact phone number: address: Address:
 Patient Information CBT Intake Form Patient Name: Preferred Name: Last Date of Birth: _// Age: _ First MM DD YYYY Gender: Best contact phone number: Email address: _ Address: _ Primary Care Physician:
Patient Information CBT Intake Form Patient Name: Preferred Name: Last Date of Birth: _// Age: _ First MM DD YYYY Gender: Best contact phone number: Email address: _ Address: _ Primary Care Physician:
Removing the Stigma from Substance Use Disorder. Joan Duwve, MD, MPH Associate Dean for Practice Richard M. Fairbanks School of Public Health
 Removing the Stigma from Substance Use Disorder Joan Duwve, MD, MPH Associate Dean for Practice Richard M. Fairbanks School of Public Health Learning Objectives Recognize the impact of Stigma on getting
Removing the Stigma from Substance Use Disorder Joan Duwve, MD, MPH Associate Dean for Practice Richard M. Fairbanks School of Public Health Learning Objectives Recognize the impact of Stigma on getting
Opioids: Use and Misuse/Steven Feinberg, MD; Scott Levy, MD, MPH, FACOEM
 Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
Western Occupational Health Conference September 14, 2012 Opioid - Use & Misuse Scott Levy, MD MPH FACOEM Steven Feinberg, MD, MPH Disclosure Information Western Occupational Health Conference 2012 Steven
San Diego Center for the Treatment of Mood Disorders 1
 San Diego Center for the Treatment of Mood Disorders 1 DATE NAME Last Middle First REFERRAL HISTORY: How did you find us (via a referral, web search, recommendation)? Please provide the name and phone
San Diego Center for the Treatment of Mood Disorders 1 DATE NAME Last Middle First REFERRAL HISTORY: How did you find us (via a referral, web search, recommendation)? Please provide the name and phone
Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 %
 Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Published on OpioidRisk (https://www.opioidrisk.com) Home > Results Test User got 22 of 22 possible points on the Risk Reduction Strategies for ER/LA Opioids Post-Test. Total score: 100 % Question Results
Evidence of Co-occurring Alcohol and Prescription Opioid Abuse in Clinical Populations: Implications for Screening
 November 20-21, 2008 Tufts Health Care Institute Program on Opioid Risk Management Conference on Co-Ingestion of Alcohol with Prescription Opioids Evidence of Co-occurring Alcohol and Prescription Opioid
November 20-21, 2008 Tufts Health Care Institute Program on Opioid Risk Management Conference on Co-Ingestion of Alcohol with Prescription Opioids Evidence of Co-occurring Alcohol and Prescription Opioid
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
Drug Overdoses A Public Health Problem. Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013. Objectives
 Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Prescription for Progress Study conducted by the Siena College Research Institute April 10 - May 4, Stakeholders - MOE +/- 4.
 How serious a public health problem in the State of New York is each of the following: [Q1A-Q1I ROTATED] Q1A. Alcohol abuse Very serious 61% 63% 53% 63% 36% 71% 52% Somewhat serious 35% 35% 38% 33% 52%
How serious a public health problem in the State of New York is each of the following: [Q1A-Q1I ROTATED] Q1A. Alcohol abuse Very serious 61% 63% 53% 63% 36% 71% 52% Somewhat serious 35% 35% 38% 33% 52%
The Biopsychosocial Model of Treating Chronic Pain Opioids Seldom Work. Program Learning Objectives. Key Points
 The Biopsychosocial Model of Treating Chronic Pain Opioids Seldom Work American Board of Vocational Experts April 2016 Dr. Jasen Michael Walker CEC Associates, Incorporated Program Learning Objectives
The Biopsychosocial Model of Treating Chronic Pain Opioids Seldom Work American Board of Vocational Experts April 2016 Dr. Jasen Michael Walker CEC Associates, Incorporated Program Learning Objectives
Opioids: Real People. Real Stories. Real Science.
 Opioids: Real People. Real Stories. Real Science. Virtual Field Trip Companion Activity The use and misuse of opioids in the United States is a problem that is not going away. Although we continue to learn
Opioids: Real People. Real Stories. Real Science. Virtual Field Trip Companion Activity The use and misuse of opioids in the United States is a problem that is not going away. Although we continue to learn
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
BRIEF PAIN INVENTORY LONG FORM
 BRIEF PAIN INVENTORY LONG FORM Date: Name: 1) Marital Status (at present) Single Widowed Married Separated/Divorced 2) Education (Circle only the highest grade or degree completed) Grade 0 1 2 3 4 5 6
BRIEF PAIN INVENTORY LONG FORM Date: Name: 1) Marital Status (at present) Single Widowed Married Separated/Divorced 2) Education (Circle only the highest grade or degree completed) Grade 0 1 2 3 4 5 6
OPIOIDS AND NON-CANCER PAIN
 Ch05.qxd 1/6/04 4:33 PM Page 77 CHAPTER 5 OPIOIDS AND NON-CANCER PAIN Background 78 Side-effects of opioids 78 Tolerance, physical dependence and addiction 79 Opioid-induced pain 79 Practical issues 80
Ch05.qxd 1/6/04 4:33 PM Page 77 CHAPTER 5 OPIOIDS AND NON-CANCER PAIN Background 78 Side-effects of opioids 78 Tolerance, physical dependence and addiction 79 Opioid-induced pain 79 Practical issues 80
Department of Veterans Affairs Network Policy No.: VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA
 Date: September 23, 2014 Long Beach, CA") Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Disclosure. Relationships with commercial interests:
 Disclosure Faculty: Jordi Perez Relationships with commercial interests: Grants/Research Support: None to declare Speakers Bureau/Honoraria: None to declare Consulting Fees: None to declare 1.Epidemiology
Disclosure Faculty: Jordi Perez Relationships with commercial interests: Grants/Research Support: None to declare Speakers Bureau/Honoraria: None to declare Consulting Fees: None to declare 1.Epidemiology
Developing a Public Education Campaign on Prescription Opiates. Samantha Kaan, MPH Multnomah County Health Department April 24, 2015
 Developing a Public Education Campaign on Prescription Opiates Samantha Kaan, MPH Multnomah County Health Department April 24, 2015 Desired Outcomes// What I hope you will get out of this Understand the
Developing a Public Education Campaign on Prescription Opiates Samantha Kaan, MPH Multnomah County Health Department April 24, 2015 Desired Outcomes// What I hope you will get out of this Understand the
Today the overuse of opioids is a problem. Many of
 A PPENDIX B A Word About Opioid Use Today the overuse of opioids is a problem. Many of these opioids are prescribed and thus are legal. Other people steal or buy opioids on the streets. These are illegal.
A PPENDIX B A Word About Opioid Use Today the overuse of opioids is a problem. Many of these opioids are prescribed and thus are legal. Other people steal or buy opioids on the streets. These are illegal.
2017 Opioid Guideline Update
 2017 Opioid Guideline Update The 2017 Canadian Guideline for Opioid Therapy and Chronic Non-Cancer Pain (CNCP) Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine,
2017 Opioid Guideline Update The 2017 Canadian Guideline for Opioid Therapy and Chronic Non-Cancer Pain (CNCP) Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine,
Life, Family and Relationship Questionnaire
 Date of Initial Session: Client Name Date of Birth Address City Zip Phone Number Email Emergency Contact Relationship Emergency Contact Ph. # Client Name: Date: Life, Family and Relationship Questionnaire
Date of Initial Session: Client Name Date of Birth Address City Zip Phone Number Email Emergency Contact Relationship Emergency Contact Ph. # Client Name: Date: Life, Family and Relationship Questionnaire
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Do not write below this line DSM IV Code: Primary Secondary. Clinical Information
 New Client Registration Today s date Name Age Sex Address Social security # Date of birth Home phone May I call you at this number? y / n Leave a message? y / n Other numbers at which I can call you Can
New Client Registration Today s date Name Age Sex Address Social security # Date of birth Home phone May I call you at this number? y / n Leave a message? y / n Other numbers at which I can call you Can
Appendix A. Socio-demographic Characteristics of Survey Respondents Compared to Current Population Survey (2013) Data
 Data") Data Supplement for Kennedy-Hendricks et al. (10.1176/appi.ps.201600056) Appendix A. Socio-demographic Characteristics of Survey Respondents Compared to Current Population Survey (2013) Data Un-weighted
Data Supplement for Kennedy-Hendricks et al. (10.1176/appi.ps.201600056) Appendix A. Socio-demographic Characteristics of Survey Respondents Compared to Current Population Survey (2013) Data Un-weighted
Epidemiology and cost of chronic pain
 Epidemiology and cost of chronic pain Dr Beverly Collett Consultant in Pain Medicine University Hospitals of Leicester Regional Advisor Treasurer of IASP Epidemiology Chronic pain is defined differently,
Epidemiology and cost of chronic pain Dr Beverly Collett Consultant in Pain Medicine University Hospitals of Leicester Regional Advisor Treasurer of IASP Epidemiology Chronic pain is defined differently,
Chronic Disease Management for Pain: It CAN be done in primary care!
 Chronic Disease Management for Pain: It CAN be done in primary care! Sondra Adkinson, PharmD, DAAPM, CPE Thomas B. Gregory, Pharm.D., BCPS, DASPE, CPE Chris Herndon, PharmD, BCPS, CPE Disclosures Adkinson:
Chronic Disease Management for Pain: It CAN be done in primary care! Sondra Adkinson, PharmD, DAAPM, CPE Thomas B. Gregory, Pharm.D., BCPS, DASPE, CPE Chris Herndon, PharmD, BCPS, CPE Disclosures Adkinson:
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Slow Release Opioids. Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain
 Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain") NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
Pocket Card SBIRT Side 1 and 2
 Pocket Card SBIRT Side 1 and 2 Pocket Card SBIRT Health Effects of Substance Abuse Alcohol Use Disorders Identification test (AUDIT) NAME: Date: The following questions concern information about your alcohol
Pocket Card SBIRT Side 1 and 2 Pocket Card SBIRT Health Effects of Substance Abuse Alcohol Use Disorders Identification test (AUDIT) NAME: Date: The following questions concern information about your alcohol
I. Chronic Pain Information Page 2-3. II. The Role of the Primary Care Physician in Chronic Pain Management Page 3-4
 SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
SUTTER MEDICAL FOUNDATION (SMF) 2750 GATEWAY OAKS DRIVE, #150 SACRAMENTO, CA 95833 SPA PCP Treatment & Referral Guidelines PAIN MANAGEMENT Developed June 1, 2003 Revised (Format Revisions) November 13,
The Mid Yorkshire Macmillan Specialist Palliative Care Team
 The Mid Yorkshire Macmillan Specialist Palliative Care Team Morphine and Strong Opioid information leaflet Information for patients/carers The mere mention of Morphine can be enough to conjure up all sorts
The Mid Yorkshire Macmillan Specialist Palliative Care Team Morphine and Strong Opioid information leaflet Information for patients/carers The mere mention of Morphine can be enough to conjure up all sorts
Concurrent Disorders. An Introductory Learning Module for Post Secondary Institutions. Concurrent Disorders Training Strategy Project
 Concurrent Disorders An Introductory Learning Module for Post Secondary Institutions Concurrent Disorders Training Strategy Project 1 Overall Learning Objectives You will: Be able to define a concurrent
Concurrent Disorders An Introductory Learning Module for Post Secondary Institutions Concurrent Disorders Training Strategy Project 1 Overall Learning Objectives You will: Be able to define a concurrent
Abusing drugs can reduce the effectiveness of your treatment, prolong your illness and increase the risk of side effects.
 Depression: This brochure can help you learn more about depression. It does not replace regular medical check-ups or your health care provider s advice. Talk with your health care provider about what you
Depression: This brochure can help you learn more about depression. It does not replace regular medical check-ups or your health care provider s advice. Talk with your health care provider about what you
Top 10 narcotic pain pills
 Top 10 narcotic pain pills Click to go to the item or just scroll down the page. Doctors Respond to FDA Panel Recommendations FDA Considers Banning Popular Prescription Pain Medications and. Top 10 Natural
Top 10 narcotic pain pills Click to go to the item or just scroll down the page. Doctors Respond to FDA Panel Recommendations FDA Considers Banning Popular Prescription Pain Medications and. Top 10 Natural
Patient and Family Agreement on Opioids
 Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
OPIOIDS FOR PERSISTENT PAIN: INFORMATION FOR PATIENTS
 OPIOIDS FOR PERSISTENT PAIN: INFORMATION FOR PATIENTS This leaflet aims to help you understand your pain, so that you can work with your health care team to self-manage your symptoms and improve your quality
OPIOIDS FOR PERSISTENT PAIN: INFORMATION FOR PATIENTS This leaflet aims to help you understand your pain, so that you can work with your health care team to self-manage your symptoms and improve your quality
Pain Control After Surgery. Patient Information
 Pain Control After Surgery Patient Information What is Pain? Pain is an uncomfortable feeling that tells you something may be wrong in your body. Pain is your body s way of sending a warning to your brain.
Pain Control After Surgery Patient Information What is Pain? Pain is an uncomfortable feeling that tells you something may be wrong in your body. Pain is your body s way of sending a warning to your brain.
RADARS System International Pre-Symposium 11 May Global Insights in Prescription Drug Misuse
 RADARS System International Pre-Symposium 11 May 2017 Global Insights in Prescription Drug Misuse WELCOME 2 The Global Mosaic: RADARS System International Program Updates Jody L. Green, PhD, CCRP Director
RADARS System International Pre-Symposium 11 May 2017 Global Insights in Prescription Drug Misuse WELCOME 2 The Global Mosaic: RADARS System International Program Updates Jody L. Green, PhD, CCRP Director
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
Reducing and stopping opioids Information for patients
 Reducing and stopping opioids Information for patients Why stop taking opioids? Opioids like morphine, oxycodone or fentanyl are very good painkillers for short-term pain after surgery or after an accident
Reducing and stopping opioids Information for patients Why stop taking opioids? Opioids like morphine, oxycodone or fentanyl are very good painkillers for short-term pain after surgery or after an accident
Access to pain therapy in the UN resolutions: worldwide perspective
 Access to pain therapy in the UN resolutions: worldwide perspective Elizabeth Mattfeld Drug Prevention and Health Branch The Single Convention recognizes the medical use of narcotic drugs as indispensable
Access to pain therapy in the UN resolutions: worldwide perspective Elizabeth Mattfeld Drug Prevention and Health Branch The Single Convention recognizes the medical use of narcotic drugs as indispensable
OPIOID PRESCRIBING BY ONTARIO DENTISTS
 OPIOID PRESCRIBING BY ONTARIO DENTISTS 2014-2016 2 TABLE OF CONTENTS 1. Executive summary 3 2. Introduction 4 3. Methods 5 4. Provincial data 7 5. Patients and dispense events 10 6. Specific Opioid Dispense
OPIOID PRESCRIBING BY ONTARIO DENTISTS 2014-2016 2 TABLE OF CONTENTS 1. Executive summary 3 2. Introduction 4 3. Methods 5 4. Provincial data 7 5. Patients and dispense events 10 6. Specific Opioid Dispense
Prior Authorization Guideline
 Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Schizophrenia is a serious mental health condition that affects
 Schizophrenia Schizophrenia is a serious mental health condition that affects a person s thoughts, feelings and behaviours. Whilst it is serious, schizophrenia is both treatable and manageable, and we
Schizophrenia Schizophrenia is a serious mental health condition that affects a person s thoughts, feelings and behaviours. Whilst it is serious, schizophrenia is both treatable and manageable, and we
ADULT QUESTIONNAIRE. Date of Birth: Briefly describe the history and development of this issue from onset to present.
 ADULT QUESTIONNAIRE Name: Address: Preferred phone number to reach you: Is it okay to leave a message? Yes No (Please check one) Date of Birth: Reason(s) for seeking treatment at this time? Briefly describe
ADULT QUESTIONNAIRE Name: Address: Preferred phone number to reach you: Is it okay to leave a message? Yes No (Please check one) Date of Birth: Reason(s) for seeking treatment at this time? Briefly describe
Increase in Opioid Related Deaths What the Data Can Tell us. Ontario Methadone Prescriber s Conference November 7, 2014 Tara Gomes
 Increase in Opioid Related Deaths What the Data Can Tell us Ontario Methadone Prescriber s Conference November 7, 2014 Tara Gomes Objectives Prescription Opioid Misuse and Abuse: How did we get here? Opioid
Increase in Opioid Related Deaths What the Data Can Tell us Ontario Methadone Prescriber s Conference November 7, 2014 Tara Gomes Objectives Prescription Opioid Misuse and Abuse: How did we get here? Opioid
Mental Health Referral Form
 Mental Health Referral Form Mailing Address: Niagara Region Mental Health 3550 Schmon Parkway, Second Floor, Unit 2 P.O. Box 1042 Thorold, ON L2V 4T7 905-688-2854 Toll free: 1-888-505-6074 niagararegion.ca/health
Mental Health Referral Form Mailing Address: Niagara Region Mental Health 3550 Schmon Parkway, Second Floor, Unit 2 P.O. Box 1042 Thorold, ON L2V 4T7 905-688-2854 Toll free: 1-888-505-6074 niagararegion.ca/health
Pain CONCERN. Medicines for long-term pain. Opioids
 Pain CONCERN Medicines for long-term pain Opioids Opioids are a group of medicines that come from the extract of poppy seeds or other medicines that work in the same way. Types of opioid The first opioids
Pain CONCERN Medicines for long-term pain Opioids Opioids are a group of medicines that come from the extract of poppy seeds or other medicines that work in the same way. Types of opioid The first opioids
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Opiate Use among Ohio Medicaid Recipients
 Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol
Opiate Use among Ohio Medicaid Recipients July 12, 2012 Ohio Colleges of Medicine Government Resource Center The Ohio State University College of Public Health Sponsored by The Ohio Department of Alcohol
Part I. Demographics. Part II. Presenting Problem. Who referred you to WellStar Psychological Services?
 Part I. Demographics Today s Date Current Time : Patient s Name (Last) (First) (MI) Patient s Date of Birth Patient s Gender Female Male Patient s Address Primary Phone Ok to leave a message? Email Address
Part I. Demographics Today s Date Current Time : Patient s Name (Last) (First) (MI) Patient s Date of Birth Patient s Gender Female Male Patient s Address Primary Phone Ok to leave a message? Email Address
Opioids Are Seniors at Risk? (April 26, 2018)
") Opioids Are Seniors at Risk? (April 26, 2018) Seniors are living longer and, with age, they become vulnerable to health challenges and the pain that may accompany them. Thus, it is perhaps not surprising
Opioids Are Seniors at Risk? (April 26, 2018) Seniors are living longer and, with age, they become vulnerable to health challenges and the pain that may accompany them. Thus, it is perhaps not surprising
Persistent Pain Resources. Educational Slide Set
 Persistent Pain Resources Educational Slide Set October 216 This document has been prepared by a multiprofessional collaborative group, with support from the All Wales Prescribing Advisory Group (AWPAG)
Persistent Pain Resources Educational Slide Set October 216 This document has been prepared by a multiprofessional collaborative group, with support from the All Wales Prescribing Advisory Group (AWPAG)
The Opioid Epidemic and Youth Prescription Drug Abuse. Sandy Chung, MD Chair, Board of Trustees Virginia Foundation for Healthy Youth
 The Opioid Epidemic and Youth Prescription Drug Abuse Sandy Chung, MD Chair, Board of Trustees Virginia Foundation for Healthy Youth Disclosures: I have no relevant financial relationships with the manufacturer(s)
The Opioid Epidemic and Youth Prescription Drug Abuse Sandy Chung, MD Chair, Board of Trustees Virginia Foundation for Healthy Youth Disclosures: I have no relevant financial relationships with the manufacturer(s)
Welcome to NHS Highland Pain Management Service
 Welcome to NHS Highland Pain Management Service Information from this questionnaire helps us to understand your pain problem better. It is important that you read each question carefully and answer as
Welcome to NHS Highland Pain Management Service Information from this questionnaire helps us to understand your pain problem better. It is important that you read each question carefully and answer as
South African guideline for the use of chronic opioid therapy for chronic non-cancer pain. Quick Reference Guide
 South African guideline for the use of chronic opioid therapy for chronic non-cancer pain M Raff, 1 BSc, MB ChB, FCA (SA); J Crosier, 1 MB ChB, ChM, FRCS, FCS (SA); S Eppel, 1 MB ChB, FRCS (Edin), ABU
South African guideline for the use of chronic opioid therapy for chronic non-cancer pain M Raff, 1 BSc, MB ChB, FCA (SA); J Crosier, 1 MB ChB, ChM, FRCS, FCS (SA); S Eppel, 1 MB ChB, FRCS (Edin), ABU
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
teen drug use Percent of 12th-graders Who Used A Substance in the Past Month (Type of Drug & Prevalence): 13% 33% 11% 23%
: 13% 33% 11% 23%") teen drug use As kids get older, they often start to question the life lessons they hear from parents and teachers. They become more heavily influenced by the things they see on TV, the Internet and social
teen drug use As kids get older, they often start to question the life lessons they hear from parents and teachers. They become more heavily influenced by the things they see on TV, the Internet and social
OPIOID CRISIS: A PERSPECTIVE. Karl J. Haake, MD
 OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
WOMEN AND OPIOIDS Media Guide
 Media Guide Canada is in the midst of a serious and growing opioid crisis. Nearly 30% of Canadians report using some form of opioids, such as oxycodone, morphine, codeine, and methadone, in the past five
Media Guide Canada is in the midst of a serious and growing opioid crisis. Nearly 30% of Canadians report using some form of opioids, such as oxycodone, morphine, codeine, and methadone, in the past five
OPIOIDS IN AMERICA. A complex crisis. A comprehensive response.
 OPIOIDS IN AMERICA A complex crisis. A comprehensive response. Prescription opioids play a critical role in helping millions of people effectively manage chronic pain. But for some, opioid use has become
OPIOIDS IN AMERICA A complex crisis. A comprehensive response. Prescription opioids play a critical role in helping millions of people effectively manage chronic pain. But for some, opioid use has become
Mark Asbridge, PhD Donald Langille, MD Jennifer Cartwright, MA. Department of Community Health and Epidemiology Dalhousie University
 Driving under the influence of prescription opioids among senior highschool students in Atlantic Canada: Prevalence, key correlates, and the role of intentions to use Mark Asbridge, PhD Donald Langille,
Driving under the influence of prescription opioids among senior highschool students in Atlantic Canada: Prevalence, key correlates, and the role of intentions to use Mark Asbridge, PhD Donald Langille,
The Bad News and the Good News: Sexual Abuse, Sexual Education, and Positive Sexuality
 The Bad News and the Good News: Sexual Abuse, Sexual Education, and Positive Sexuality Christine White Legal Advocate for People with Developmental Disabilities April 7, 2011 No part of this slideshow
The Bad News and the Good News: Sexual Abuse, Sexual Education, and Positive Sexuality Christine White Legal Advocate for People with Developmental Disabilities April 7, 2011 No part of this slideshow
INTER-AMERICAN DRUG ABUSE CONTROL COMMISSION C I C A D
 INTER-AMERICAN DRUG ABUSE CONTROL COMMISSION C I C A D SIXTY-THIRD REGULAR SESSION April 25-27, 2018 México D.F., México OEA/Ser.L/XIV.2.63 CICAD/doc.2385/18 25 April 2018 Original: English THE OPIOID
INTER-AMERICAN DRUG ABUSE CONTROL COMMISSION C I C A D SIXTY-THIRD REGULAR SESSION April 25-27, 2018 México D.F., México OEA/Ser.L/XIV.2.63 CICAD/doc.2385/18 25 April 2018 Original: English THE OPIOID
F REQUENTLY A SKED Q UESTIONS T REATMENT P ROFESSIONALS
 F REQUENTLY A SKED Q UESTIONS T REATMENT P ROFESSIONALS T hese questions and responses may help a committee when presenting to treatment professionals or when exhibiting at a professional event. Discussing
F REQUENTLY A SKED Q UESTIONS T REATMENT P ROFESSIONALS T hese questions and responses may help a committee when presenting to treatment professionals or when exhibiting at a professional event. Discussing
The Opioid Misuse Crisis and Non- Pharmacological Pain Management. Collaboration with SPTAs, Divisions and Schools
 The Opioid Misuse Crisis and Non- Pharmacological Pain Management Collaboration with SPTAs, Divisions and Schools Learning Objectives Participants will be able to describe the role of non-pharmacological
The Opioid Misuse Crisis and Non- Pharmacological Pain Management Collaboration with SPTAs, Divisions and Schools Learning Objectives Participants will be able to describe the role of non-pharmacological
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain
 Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
Addressing the Opioid Epidemic: Prescribing Opioids for Non-Cancer Pain Ajay D. Wasan, MD, MSc Professor of Anesthesiology and Psychiatry Vice Chair for Pain Medicine, Department of Anesthesiology University
2/7/2017. Avoid compassion traps. Avoid All or Nothing Traps. Some Explanatory Models of Addiction
 Avoid compassion traps Do you want me to lose my job, do you want me to be on the street? I want you to have safe and effective pain control and it is my medical opinion that your current medicine won
Avoid compassion traps Do you want me to lose my job, do you want me to be on the street? I want you to have safe and effective pain control and it is my medical opinion that your current medicine won
Allergic to hydrocodone can i take tramadol
 Allergic to hydrocodone can i take tramadol The Borg System is 100 % Allergic to hydrocodone can i take tramadol Dec 7, 2017. Tramadol and hydrocodone/acetaminophen (Vicodin) are powerful pain relievers
Allergic to hydrocodone can i take tramadol The Borg System is 100 % Allergic to hydrocodone can i take tramadol Dec 7, 2017. Tramadol and hydrocodone/acetaminophen (Vicodin) are powerful pain relievers
LIFE INTEGRATION THERAPIES, PC., INC. KAY WHITEHEAD, MSW., LCSW., FT. 23 E.39 th St. INDIANAPOLIS, IN CLIENT HISTORY FORM
 LIFE INTEGRATION THERAPIES, PC., INC. KAY WHITEHEAD, MSW., LCSW., FT. 23 E.39 th St. INDIANAPOLIS, IN 46205 317-626-3626 CLIENT HISTORY FORM Name Date Address City St Zip Home Phone Work Cell Email (if
LIFE INTEGRATION THERAPIES, PC., INC. KAY WHITEHEAD, MSW., LCSW., FT. 23 E.39 th St. INDIANAPOLIS, IN 46205 317-626-3626 CLIENT HISTORY FORM Name Date Address City St Zip Home Phone Work Cell Email (if
Welcome - we will begin the webinar shortly Please read the participation tips below:
 Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Youth, Opioid Use and Treatment Options. CPSO MMT Providers Conference Dr. Sharon Cirone MD FCFPC November 2016
 Youth, Opioid Use and Treatment Options CPSO MMT Providers Conference Dr. Sharon Cirone MD FCFPC November 2016 Disclosures No propriety involvement in pharmaceutical companies Assessor, CPSO Methadone
Youth, Opioid Use and Treatment Options CPSO MMT Providers Conference Dr. Sharon Cirone MD FCFPC November 2016 Disclosures No propriety involvement in pharmaceutical companies Assessor, CPSO Methadone
University of Pittsburgh
 2017 Family Center Event: Engaging Families Experiencing Opioid Use, Addiction, and Learning Objectives: Identify the impact of opioid use, addiction, and recovery on child development Identify warning
2017 Family Center Event: Engaging Families Experiencing Opioid Use, Addiction, and Learning Objectives: Identify the impact of opioid use, addiction, and recovery on child development Identify warning
Evaluation of Variables in Illicit Drug Use: Does a Controlled Substance Abuse Screening Tool Identify Illicit Drug Use?
 Manchikanti et al Evaluation of Variables in Illicit Drug Use 71 Pain Physician. 2004;7:71-75, ISSN 1533-3159 An Original Contribution Evaluation of Variables in Illicit Drug Use: Does a Controlled Substance
Manchikanti et al Evaluation of Variables in Illicit Drug Use 71 Pain Physician. 2004;7:71-75, ISSN 1533-3159 An Original Contribution Evaluation of Variables in Illicit Drug Use: Does a Controlled Substance
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Introduction to Sensitive Topics and Interviewing for Alcohol Use Practice of Medicine 1 January 7, 2003
 Introduction to Sensitive Topics and Interviewing for Alcohol Use Practice of Medicine 1 January 7, 2003 Objectives At the end of this lecture, you should: Be able to explain to your grandmother or your
Introduction to Sensitive Topics and Interviewing for Alcohol Use Practice of Medicine 1 January 7, 2003 Objectives At the end of this lecture, you should: Be able to explain to your grandmother or your
Principles and language suggestions for talking with patients
 SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team
 Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team Cheryl L Mejta, Ph.D. Nancy H Burley, Ed.D. Serena Wadhwa, Psy. D., LCPC, RYT, CADC Objectives Identify
Responding to the Opioid Epidemic: Behavioral Health Specialists Role on the Interprofessional Team Cheryl L Mejta, Ph.D. Nancy H Burley, Ed.D. Serena Wadhwa, Psy. D., LCPC, RYT, CADC Objectives Identify
Thank you for agreeing to complete the Canadian Mental Health Association (CMHA) of Central Alberta 2017 Speak Up for Mental Health
 of Central Alberta 2017 Speak Up for Mental Health") The 2017 CMHA Speak Up for Mental Health Survey 1. Introduction Thank you for agreeing to complete the Canadian Mental Health Association (CMHA) of Central Alberta 2017 Speak Up for Mental Health survey.
The 2017 CMHA Speak Up for Mental Health Survey 1. Introduction Thank you for agreeing to complete the Canadian Mental Health Association (CMHA) of Central Alberta 2017 Speak Up for Mental Health survey.
National Council on Patient Information and Education
 National Council on Patient Information and Education You are not alone The type of pain that caused your doctor to prescribe a pain medicine for you can make you feel that you are different from everyone
National Council on Patient Information and Education You are not alone The type of pain that caused your doctor to prescribe a pain medicine for you can make you feel that you are different from everyone
William H. Swiggart, MS
 William H. Swiggart, MS Co-Director, Center for Professional Health Vanderbilt University Medical Center 2015 All rights reserved. I have no financial relationships to disclose. The purpose of this session
William H. Swiggart, MS Co-Director, Center for Professional Health Vanderbilt University Medical Center 2015 All rights reserved. I have no financial relationships to disclose. The purpose of this session
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
My Background. State of Behavioral Health. State of Behavioral Health. Tailoring the Messages and the Medicines to Optimize Cessation Interventions
 Tailoring the Messages and the Medicines to Optimize Cessation Interventions Stephen S. Michael, MS Director, ASHLine My Background Master s Degree in Rehabilitation Counseling 20+ years developing and
Tailoring the Messages and the Medicines to Optimize Cessation Interventions Stephen S. Michael, MS Director, ASHLine My Background Master s Degree in Rehabilitation Counseling 20+ years developing and
Opioid Prescribing for Acute Pain
 Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Patient Reference Guide Opioid Prescribing for Acute Pain Care for People 15 Years of Age and Older Quality standards outline what high-quality care looks like. They focus on conditions or topics where
Smoking Cessation Counselling
 Smoking Cessation Counselling Results of a 2005 Survey of Quebec NURSES Michèle Tremblay, Daniel Cournoyer, Daniela Jukic, Jennifer O Loughlin,, Université de Montréal INTRODUCTION More than 13,000 men
Smoking Cessation Counselling Results of a 2005 Survey of Quebec NURSES Michèle Tremblay, Daniel Cournoyer, Daniela Jukic, Jennifer O Loughlin,, Université de Montréal INTRODUCTION More than 13,000 men