The Monster Back : Non-Opioid Pain Management 16 February 2017
|
|
|
- Clemence Perry
- 5 years ago
- Views:
Transcription

1 The Monster Back : Non-Opioid Pain Management 16 February 2017 Paul F. Pasquina, M.D. Professor and Chair, Physical Medicine & Rehabilitation Director, Center for Rehabilitation Sciences Research Uniformed Services University of the Health Sciences Chief, Department of Rehabilitation Walter Reed National Military Medical Center
2 Disclaimer No conflicts of interest to report. Medical Research Consultant for American Orthotic and Prosthetic Association (AOPA) Research support: MRMC, USUHS, DARPA, CNRM, CRSR The views expressed in this presentation are those of the author and do not reflect the official policy of the Department of Army, Department of Defense, or U.S. Government
3
4 Epidemiology Lifetime incidence ~ 85% Chronic (>3mo) 15-45% of population 90% improve within 3 months, 50% recur Second only to common cold as cause of lost work time Most common disability in those under 45 Most expensive health care issue for patients between 20 and 50 10% of patients responsible for 80-90% of costs

5 Epidemiology Neuropathic (stenosis, HNP): 37-54% Discogenic : 35%-50% SI joint pain: 15%-35% Facetogenic: 10%-25% Myofascial: 20%
6 Differential Diagnosis (Determine the pain generator) Pain Generators: Bone Soft Tissue Nerve Referred Lumbosacral Strain/Sprain Radiculopathy (sciatica) Spondylosis, Spondylolysis, Spondylolisthesis Visceral referred pain Cauda Equina Syndrome Cancer Infection Seronegative spondyloarthropathies Compression fractures

7 Normal Vertebral Anatomy

8 Most common site of back pain Normally comprises ~ 25% of length of spine Consists of a central nucleus pulposus Composed of ~ 88% water Annulus fibrosus Consists of concentric lamellae of fibrocartilage fibers arranged obliquely With each layer, they are arranged in opposite directions Intervertebral Disc

9


10


11 Kinetic Chain
12 History Intensity Location Radiation Duration Trauma Modifiers Sleep Anxiety Red Flags Age <20 or >50 Systemic Illness Fevers Chills Night sweats Weight Loss Bowel or Bladder Changes Numbness/Weakness History of Cancer Rest pain Drug use
13 Physical Exam Vitals Inspection Palpation Range of motion Special Tests Motor Sensory Reflexes

14 Inspection General appearance Cutaneous inspection Infection Trauma Developmental Abnormalities Other deformities
15 Palpation Percussion of vertebral bodies Fracture Infection Spasms Trigger points

16 Range of Motion Flexion Extension Lateral bending Facet loading
17 Special Tests Tests to stretch spinal cord, cauda equina, or sciatic nerve Tests to assess the sacroiliac joint Spondylolysis - Stork Test Limb Length Tests Core stability testing Flexibility Tests Tests to assess for non-organic signs

18 Tests to Stretch the Spinal Cord or Sciatic Nerve Straight Leg Raise Lasegue s Sign Cross Leg SLR Hoover Test Kernig Test Valsalva Maneuver

19 Hoover Test

20 Tests to Stretch the Spinal Cord or Sciatic Nerve Straight Leg Raise Lasegue s Sign Well Leg SLR Hoover Test Kernig Test Valsalva Maneuver

21 Test to Assess the Sacroiliac Joint Pelvic Rock Test Gaenslen s Sign Patrick or FABER Test

22 Posterior Element Facet Pain vs. Spondylolysis Stork Test


23 True vs. Functional Leg Length Discrepancy Leg length assessment Pelvic obliquity Supine leg lengths

24 Thomas test Popliteal angle Ober test Piriformis test Flexibility Tests
 Ober test Piriformis test Flexibility")
25 Thomas test Popliteal angle Knee Flexion (measure heel from buttocks) Ober test Piriformis test Flexibility Tests
26 Thomas test Popliteal angle Ober Test Piriformis test Flexibility Tests


27 Flexibility Tests Thomas test Popliteal angle Shober test Piriformis test
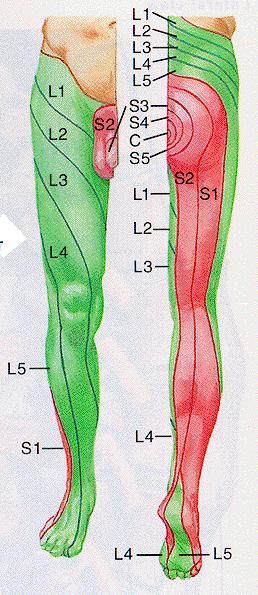
 Great Toe / toe extension (L5) Foot eversion - peroneus (S1) DTRS Knee jerk reflex (L4) Ankle jerk reflex (S1) Sensation: L4: medial side of foot, medial leg L5: dorsum of foot,")
28 Neuromuscular Screening Heel Walk - anterior tibialis (L4, 5) Toe Walk - tibial nerve (S1, 2) Strength testing Quadriceps extension (L2,3,4) Foot inversion - ant. tib (L4) Great Toe / toe extension (L5) Foot eversion - peroneus (S1) DTRS Knee jerk reflex (L4) Ankle jerk reflex (S1) Sensation: L4: medial side of foot, medial leg L5: dorsum of foot, lateral leg S1: lateral side of foot
29

30

31 Motor/Strength Exam

32
33 Accuracy of History & Exam Tests for Lumbosacral Radiculopathy Herniated Disc (sens, spec) Sciatica (95%, 88%) Ipsilateral SLR (83%, 40%) Crossed SLR (25%, 90%) Ankle dorsilflexion weakness (35%, 70%) Great toe extensor weakness (50%, 70%) Impaired Achille s reflex (50%, 60%) Ankle plantar flexion weakness (6%, 95%) Spinal Stenosis (sens, spec) Age > 65 (77%, 69%) Severe LE pain (65%, 67%) No pain when seated (46%, 93%) Symptoms worse with walking (71%, 30%) Numbness (63%, 59%) Wide-based gait (43%, 97%) Pinprick deficit (47%, 81%) Weakness (47%, 78%) Vibration deficit (53%, 81%) Absent Achille s reflex (46%, 78%)

34 Motor/Strength Exam

35 Tests for Core Stability Trendelenberg Test Pelvic Bridging
36 Tests for Core Stability Trendelenberg Test Pelvic Bridging
37 WADDELL S SIGNS Simulation (Axial Loading, Rotation) Tenderness (Superficial) Distraction Overreaction - Exaggerated painful response to a stimulus Regional weakness / sensory changes


38 Metastatic Disease BLT KP Myeloma, Lymphoma, Sarcoma 96% of spinal metastases, back pain is the initial symptom

39 Discitis

40 Spondylosis

41 Spondylolysis

42 Spondylolysis

43 Spondylolisthesis

44 Nerve Root Impingement (Radiculopathy) Only represent 1% of all patients with LBP Causes: Herniated nucleus pulposus Foraminal stenosis Mass occupying lesion Disc Spinal Nerve


45

46

47 Facet Joint Pathology True synovial joints Innervation by 2 medial branches Protect against axial rotation, shearing forces, and assist disc in resisting compressive forces in lordotic postures Prevalence varies between 5-15% in L-spine, 35-50% in C- spine, and 35-45% in T-spine Load borne by l-z-joints varies between 3-25% of axial load
48 Diagnosis No single historical or PE exam sign can reliably identify facet block responders Paraspinal tenderness weakly associated with facet block and RF treatment outcomes Imaging has low specificity for identifying a painful z-joint Medial branch blocks and IA injections often touted as equivalent, but this is unproven. MBB may be more predictive of RF treatment outcome, and IA may be more specific for identifying a painful joint Face Validity Comparison of clinical trials evaluating RF denervation


49 Underestimated by surgeons & PCPs Heterogeneous condition Represents 15%-30% of cases of axial LBP below L5 Bi-modal peaks in prevalence rates Intra- and extra-articular etiologies 40%-50% 2 o to trauma Sacroiliac Joint Pain Prevalence Rates

50 Predisposing Factors Rotation and axial loading Leg length discrepancy Pelvic & scapular obliquity Scoliosis Previous back surgery Lumbar pathology/ Transitional anatomy Pregnancy
 47 described buttock pain (94%) 36 described lower lumbar pain (72%) 25 had lower extremity pain (50%) 14 had leg pain distal to the knee (28%) 7 described")
51 SI Joint Pain Referral Zones Retrospective analysis in 50 pts diagnosed with SIJ pain based on diagnostic blocks (Slipman et al. 2000) 47 described buttock pain (94%) 36 described lower lumbar pain (72%) 25 had lower extremity pain (50%) 14 had leg pain distal to the knee (28%) 7 described groin pain (14%) 6 reported foot pain (12%)

52 Ankylosing Spondylitis

53

54

55

56 Evidence Based Treatments Acute Low Back Pain Chronic Low Back Pain
57 Negative Outcome Predictors for Back Pain Previous LBP episode Low education High physical job stress Physically demanding job Poor job satisfaction Obesity Somatization Low levels of physical activity Older age Poor coping skills High anxiety levels Depression Negative attitude Smoking Fear-avoidance Catastrophization Ongoing litigation Higher baseline pain & disability Not having opportunity for reduced work load after RTD Adapted from Cohen et al. BMJ 2009

58

59

60 Manipulation

61
 Disrupts the pain cycle Stops hyper-responsive")
62 Myofascial Pain Syndrome Trigger Points: Treatments Spray and stretch Ultrasound Massage Manipulation Trigger point injection Injection material 1cc lidocaine +/- Corticosteroid Dry needle (more post injection soreness) Disrupts the pain cycle Stops hyper-responsive signals

63


64 Epidural Steroid Injections


65 Sacroiliac Joint Injections


66 Intra-articular Facet Injection
 SPECT scans suggests they may provide intermediate-term relief in a subset of patients with acute inflammation")
 pts (n=28) fared better than in SPECT (-) pts (n=5) @ 1-month Intra-Articular &")
67 IA injections shown to be ineffective in 3 RCTs Anecdotal evidence & results of a small (n=46) RCT comparing it to MBB in those with (+) SPECT scans suggests they may provide intermediate-term relief in a subset of patients with acute inflammation MBB blocks: Very weak evidence in the form of clinical trials by one group showing > 1-year benefit, and a very small uncontrolled study showing MBB in SPECT (+) pts (n=28) fared better than in SPECT (-) pts 1-month Intra-Articular & MBB as Treatments

68 Exercises Should Target Physical Exam Findings

69

70 Aerobic Conditioning/ Activity Specific Exercise
71 Questions?
72 Take-Home Points Almost all procedural interventions have conflicting evidence behind them, but are likely provide short to intermediate-term benefit to a well-selected population More effective for subacute pain in an anatomical distribution Factors predicting success for interventional procedures mirror predictive factors for back pain in general Moderate-strong evidence for intermediate-term relief with facet & SI joint radiofrequency denervation Moderate evidence for very short-term benefit with SI joint injections Moderate evidence for short benefit for ESI in a carefully selected population with clear-cut radicular pain Conflicting evidence for TPI s Moderate evidence for very short-term benefit with SI joint injections Procedures as adjunct for physical therapy interventions
73 RCT s Involving Muscle Injections for LBP Trigger Point Injections Garvey et al. 1989: DB study comparing lidocaine, lidocaine/steroid, acupuncture and vapocoolant spray with acupressure: No difference between groups No difference between injectates c/w other studies Di Cesare et al. 2011: DB clinical trial that found acupuncture mesotherapy injections > TPI mesotherapy Botulinum Toxin Botox vs. Saline for nonspecific LBP: 1 of 2 positive Botox vs. steroid/la for piriformis syndrome: 1 of 1 positive Botox vs. acupuncture for LBP: 1 of 1 positive
Thoracolumbar Spine Conditions: Treatment and Return to Play
 Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
LOW BACK PAIN EPIDEMIOLOGY:
 LOW BACK PAIN OBJECTIVES: Discuss epidemiology of low back pain Summarize diagnosis/ special tests Review Red Flags Discuss treatment and referral guidelines Discuss light duty guidelines EPIDEMIOLOGY:
LOW BACK PAIN OBJECTIVES: Discuss epidemiology of low back pain Summarize diagnosis/ special tests Review Red Flags Discuss treatment and referral guidelines Discuss light duty guidelines EPIDEMIOLOGY:
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽
 외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Examination of the lumbosacral spine. Dr Lucy Holtzhausen Rotorua GP CME June 2015
 Examination of the lumbosacral spine Dr Lucy Holtzhausen Rotorua GP CME June 2015 Diagnostic Algorithm Presenting symptoms Diagnostic decisions Diagnostic triage LOW BACK PAIN Mechanical NON-SPECIFIC LBP
Examination of the lumbosacral spine Dr Lucy Holtzhausen Rotorua GP CME June 2015 Diagnostic Algorithm Presenting symptoms Diagnostic decisions Diagnostic triage LOW BACK PAIN Mechanical NON-SPECIFIC LBP
Outline. Introduction / Epidemiology. Anatomy / Pain generators. Diagnosis. Treatment. Most Important lecture!!
 Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Chiropractic Health Plan - Diagnosis of Low Back Pain
 Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center
 Oh My Aching Back! Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center Epidemiology 90% of episodes of LBP resolves
Oh My Aching Back! Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center Epidemiology 90% of episodes of LBP resolves
Numb bum means cauda equina Per rectal examination is indicated to assess anal tone
 SPINE Age and occupation Pain: Where: Low back or leg Which is worse? Where about in the leg? Describe the radiation How long? More than 6 wks need warrant evaluation How the pain is now compared to the
SPINE Age and occupation Pain: Where: Low back or leg Which is worse? Where about in the leg? Describe the radiation How long? More than 6 wks need warrant evaluation How the pain is now compared to the
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society
 Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Back and Neck Injuries: Surgical Advances and Treatment
 Back and Neck Injuries: Surgical Advances and Treatment Ara Deukmedjian, MD Board Certified Neurosurgeon June 8, 2017 1 2 Spinal Joints: Anatomy Two types of Spinal Joints: Spinal (intervertebral) disc
Back and Neck Injuries: Surgical Advances and Treatment Ara Deukmedjian, MD Board Certified Neurosurgeon June 8, 2017 1 2 Spinal Joints: Anatomy Two types of Spinal Joints: Spinal (intervertebral) disc
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
5/5/2010. Session 1. Session 2
 A PHYSIATRIST S VIEW ON LOW BACK PAIN: PART I 41 st Annual Family Medicine Review Lexington, KY November 2009 NINAD KARANDIKAR, MD ASSISTANT PROFESSOR DEPT. OF PHYSICAL MEDICINE AND REHABILITATION UNIVERSITY
A PHYSIATRIST S VIEW ON LOW BACK PAIN: PART I 41 st Annual Family Medicine Review Lexington, KY November 2009 NINAD KARANDIKAR, MD ASSISTANT PROFESSOR DEPT. OF PHYSICAL MEDICINE AND REHABILITATION UNIVERSITY
The NICE revised guidelines for the management of non-specific low back pain and; Implications for Practice
 The NICE revised guidelines for the management of non-specific low back pain and; Implications for Practice David Walsh David.walsh@nottingham.ac.uk National Clinical Guideline Centre Commissioned by NICE
The NICE revised guidelines for the management of non-specific low back pain and; Implications for Practice David Walsh David.walsh@nottingham.ac.uk National Clinical Guideline Centre Commissioned by NICE
SPINAL PAIN. Mr. Yagnesh Vellore FRACS Neurosurgeon and Spine Surgeon
 SPINAL PAIN Mr. Yagnesh Vellore FRACS Neurosurgeon and Spine Surgeon PAIN GENERATORS IN THE SPINE Ligaments: ALL,PLL Muscle Periosteum bone Outer 1/3 annulus disc Facet joints Sacro-iliac joint sinuvertebral
SPINAL PAIN Mr. Yagnesh Vellore FRACS Neurosurgeon and Spine Surgeon PAIN GENERATORS IN THE SPINE Ligaments: ALL,PLL Muscle Periosteum bone Outer 1/3 annulus disc Facet joints Sacro-iliac joint sinuvertebral
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Back Pain. John W. Engstrom, MD December 16, Disclosures. A Clinical Approach to the Evaluation of Back Pain and Lumbar Radiculopathy
 Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
405 Firemans Ave LaVale, Maryland 21502
 Dec 19, 2016 CHIEF COMPLAINT: Iris presents with a chief complaint involving her lower lumbar and sacral region, left sacroiliac region and left anterior hip and groin. ONSET OF SYMPTOMS Iris states this
Dec 19, 2016 CHIEF COMPLAINT: Iris presents with a chief complaint involving her lower lumbar and sacral region, left sacroiliac region and left anterior hip and groin. ONSET OF SYMPTOMS Iris states this
Physical examination of the patient with back pain
 Physical examination of the patient with back pain Mitchell K Freedman DO Clinical Associate Professor at Sidney Kimmel Medical College of Thomas Jefferson University Hospital Goals of Lecture Discuss
Physical examination of the patient with back pain Mitchell K Freedman DO Clinical Associate Professor at Sidney Kimmel Medical College of Thomas Jefferson University Hospital Goals of Lecture Discuss
Musculoskeletal Examination of the Pain Patient
 Musculoskeletal Examination of the Pain Patient Joseph F. Audette, M.A., M.D Assistant Clinical Professor, Harvard Medical School Chief, Department of Pain Medicine Harvard Vanguard Medical Associates
Musculoskeletal Examination of the Pain Patient Joseph F. Audette, M.A., M.D Assistant Clinical Professor, Harvard Medical School Chief, Department of Pain Medicine Harvard Vanguard Medical Associates
Discussion Points 10/17/16. Spine Pain is Ubiquitous. Interventional Pain Management
 Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
Lumbar disc prolapse. Done by : Areej Al-Hadidi
 Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Herniated Disk in the Lower Back
 Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Sacroiliitis. Devin Peck, M.D. Associate Program Director Tri-Institute Pain Fellowship Weill Cornell Medical Center
 Sacroiliitis Devin Peck, M.D. Associate Program Director Tri-Institute Pain Fellowship Weill Cornell Medical Center Epidemiology First described as a source of pain by Goldthwaite and Osgood in 1905 Accounts
Sacroiliitis Devin Peck, M.D. Associate Program Director Tri-Institute Pain Fellowship Weill Cornell Medical Center Epidemiology First described as a source of pain by Goldthwaite and Osgood in 1905 Accounts
Painful GP dilemmas Low Back Pain Leg Pain. Dr. Rajiv Chawla Consultant in Pain Medicine The Walton Centre Liverpool
 Painful GP dilemmas Low Back Pain Leg Pain Dr. Rajiv Chawla Consultant in Pain Medicine The Walton Centre Liverpool Low back Pain Up to 80% of all adults will eventually experience back pain, and it is
Painful GP dilemmas Low Back Pain Leg Pain Dr. Rajiv Chawla Consultant in Pain Medicine The Walton Centre Liverpool Low back Pain Up to 80% of all adults will eventually experience back pain, and it is
Clinical Reference Guide
 Clinical Reference Guide Table of Clinical References PREVALENCE Bernard, 1987 Cohen, 2005 Weksler, 2007 Sembrano, 2009 POST LUMBAR FUSION Maigne, 2005 Ha, 2008 Ivanov, 2009 Liliang, 2011 DePalma, 2011
Clinical Reference Guide Table of Clinical References PREVALENCE Bernard, 1987 Cohen, 2005 Weksler, 2007 Sembrano, 2009 POST LUMBAR FUSION Maigne, 2005 Ha, 2008 Ivanov, 2009 Liliang, 2011 DePalma, 2011
Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia
 Disclosure & Acknowledgment Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia Disclosures - None Acknowledgements Dr. Andrea Furlan Dr. Julia Alleyne Dr. Hamilton Hall
Disclosure & Acknowledgment Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia Disclosures - None Acknowledgements Dr. Andrea Furlan Dr. Julia Alleyne Dr. Hamilton Hall
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Cervical intervertebral disc disease Degenerative diseases F 04
 Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Common Orthopedic Conditions of the Spine
 Common Orthopedic Conditions of the Spine Learning Objective Given a scenario describing a patient with symptoms suggestive of an orthopedic or musculoskeletal condition, formulate a treatment plan after
Common Orthopedic Conditions of the Spine Learning Objective Given a scenario describing a patient with symptoms suggestive of an orthopedic or musculoskeletal condition, formulate a treatment plan after
10/8/2015. Consultant for Boston Scientific-no conflicts with this presentation
 Consultant for Boston Scientific-no conflicts with this presentation Mehul Sekhadia, DO Medical Director Advocate Lutheran General Hospital Park Ridge, IL Identify when to consider interventional pain
Consultant for Boston Scientific-no conflicts with this presentation Mehul Sekhadia, DO Medical Director Advocate Lutheran General Hospital Park Ridge, IL Identify when to consider interventional pain
Patient Chart Quotes. Spine Mythology and Evidence- Based Management of Back Pain. Patient Chart Quotes. Patient Chart Quotes
 Spine Mythology and Evidence- Based Management of Back Pain John Engstrom, MD Professor of Neurology August 11, 2009 Patient Chart Quotes The patient was in his usual state of good health until his airplane
Spine Mythology and Evidence- Based Management of Back Pain John Engstrom, MD Professor of Neurology August 11, 2009 Patient Chart Quotes The patient was in his usual state of good health until his airplane
Hailee Gibson, CCPA Neurosurgery Physician Assistant. Windsor Neurosurgery & Spine Associates. Windsor Regional Hospital Ouellette Campus
 Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Common Thoraco- Lumbar Problems in the Mature Athlete
 Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
Chapter 35 Back Pain. Episode overview: Wisecracks: Crack Cast Show Notes Back Pain July 2016
 Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Cox Technic Case Report #169 published at (sent 5/9/17) 1
 1") Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Functional Anatomy and Exam of the Lumbar Spine. Thomas Hunkele MPT, ATC, NASM-PES,CES Coordinator of Rehabilitation
 Functional Anatomy and Exam of the Lumbar Spine Thomas Hunkele MPT, ATC, NASM-PES,CES Coordinator of Rehabilitation Disclosure Anatomical Review Quick Review of Bony and Ligamentous structures Discal anatomy
Functional Anatomy and Exam of the Lumbar Spine Thomas Hunkele MPT, ATC, NASM-PES,CES Coordinator of Rehabilitation Disclosure Anatomical Review Quick Review of Bony and Ligamentous structures Discal anatomy
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery URMC Neurosurgery APP s Objectives Identify the most common pathology that leads to spine
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery URMC Neurosurgery APP s Objectives Identify the most common pathology that leads to spine
Diagnosis. Lumpers vs splitters. Non specific Low back pain Biopsychosocial model good GPs already incorporate this into daily practice
 Spinal Pain COL Tony Delaney RFD MB BS FACSP Sports Physician Narrabeen Sports Medicine Centre Sydney Academy of Sport Chair ADF Musculoskeletal, Sports, Rehabilitation Consultative Group 1999-2012 Background
Spinal Pain COL Tony Delaney RFD MB BS FACSP Sports Physician Narrabeen Sports Medicine Centre Sydney Academy of Sport Chair ADF Musculoskeletal, Sports, Rehabilitation Consultative Group 1999-2012 Background
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
Interventional Pain Management
 Spinal Injections Can be beneficial for both chronic and acute pain depending on pathology Contraindications: Patient refusal Active infection Platelets less than 75 or inability to stop anticoagulation
Spinal Injections Can be beneficial for both chronic and acute pain depending on pathology Contraindications: Patient refusal Active infection Platelets less than 75 or inability to stop anticoagulation
Evaluation of Posterior Hip Pain
 Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Corporate Medical Policy
 Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
An Osteopathic Approach to Low Back Pain. Ryan Seals DO Interim Chair of Family Medicine and OMM
 An Osteopathic Approach to Low Back Pain Ryan Seals DO Interim Chair of Family Medicine and OMM Objectives Review Osteopathic Philosophy and Principles Discuss how somatic dysfunction influences low back
An Osteopathic Approach to Low Back Pain Ryan Seals DO Interim Chair of Family Medicine and OMM Objectives Review Osteopathic Philosophy and Principles Discuss how somatic dysfunction influences low back
Evaluation of Patient with Spine Symptoms. Kenneth Nguyen, DO Providence Physiatry
 Evaluation of Patient with Spine Symptoms Kenneth Nguyen, DO Providence Physiatry Epidemiology of Low Back Pain (LBP) Lifetime prevalence of 84% Chronic symptoms in 10-15% 80-90% of economic resources
Evaluation of Patient with Spine Symptoms Kenneth Nguyen, DO Providence Physiatry Epidemiology of Low Back Pain (LBP) Lifetime prevalence of 84% Chronic symptoms in 10-15% 80-90% of economic resources
Interlaminar Decompression & Stabilization. Reginald Davis, M.D., FAANS, FACS Director of Clinical Research
 Interlaminar Decompression & Stabilization Reginald Davis, M.D., FAANS, FACS Director of Clinical Research Disclosures Background Device meant to stabilize the spine without fusion following decompression
Interlaminar Decompression & Stabilization Reginald Davis, M.D., FAANS, FACS Director of Clinical Research Disclosures Background Device meant to stabilize the spine without fusion following decompression
Low Back Pain in the Athlete Steven E. Mayer, MD Northwestern Medicine Physical Medicine and Rehabilitation Sports Medicine
 Low Back Pain in the Athlete Steven E. Mayer, MD Northwestern Medicine Physical Medicine and Rehabilitation Sports Medicine When to Play and When to Sit Controversial Based on clinical/expert opinion Current
Low Back Pain in the Athlete Steven E. Mayer, MD Northwestern Medicine Physical Medicine and Rehabilitation Sports Medicine When to Play and When to Sit Controversial Based on clinical/expert opinion Current
Paul Allan Regional Clinical Lead - South. Lumbar Spine. Assessment & Differential Diagnosis
 Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
LUMBAR SPINE CASE 3. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1. L4-5, 5-S1 disc, facet (somatic)
") LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT
 LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management.
 River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
Therapeutic Exercise And Manual Therapy For Persons With Lumbar Spinal Stenosis
 Therapeutic Exercise And Manual Therapy For Persons With Lumbar Spinal Stenosis The program consisted of manual therapy twice per week (eg, soft tissue and neural The components of the Boot Camp Program
Therapeutic Exercise And Manual Therapy For Persons With Lumbar Spinal Stenosis The program consisted of manual therapy twice per week (eg, soft tissue and neural The components of the Boot Camp Program
Medical Affairs Policy
 Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
A. DESCENDING MODULATORY INFLUENCES HISTORY
 Chronic Low Back +/- Leg Pain in Older Adults: Essential Clinical Contributors Screen NOTE: The following should be performed on all older adults with chronic low back pain in whom red flags of serious
Chronic Low Back +/- Leg Pain in Older Adults: Essential Clinical Contributors Screen NOTE: The following should be performed on all older adults with chronic low back pain in whom red flags of serious
RADICULOPATHY AN INTRODUCTION TO
 AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
AN INTRODUCTION TO RADICULOPATHY This booklet provides general information on radiculopathy. It is not meant to replace any personal conversations that you might wish to have with your physician or other
EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS
 CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
CERVICAL SPINE EVALUATION AND MANAGEMENT OF CERVICAL SPINE DISORDERS Gregory M Yoshida MD Supports the skull Allows movement of the head Houses the spinal cord CERVICAL SPINE Unique anatomy Upper C spine
Wendy Field Advanced Physiotherapy Practitioner June 2018
 Wendy Field Advanced Physiotherapy Practitioner June 2018 Radiculopathy???? Lumbar radicular pain is where the clinician suspects the pain is coming from a lumbar nerve root. Essentially we are looking
Wendy Field Advanced Physiotherapy Practitioner June 2018 Radiculopathy???? Lumbar radicular pain is where the clinician suspects the pain is coming from a lumbar nerve root. Essentially we are looking
Case Studies, Impairment of the Spine in Washington State
 Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Spinal and Trigger Point Injections
 Spinal and Trigger Point Injections I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain when determined to be medically
Spinal and Trigger Point Injections I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain when determined to be medically
BACK PAIN. Disclaimer. Integrated web marketing. Multimedia Health Education
 BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
North American Spine Society Public Education Series
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Nonsurgical Interventional Treatments for Spinal Pain Management
 Nonsurgical Interventional Treatments for Spinal Pain Management I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain
Nonsurgical Interventional Treatments for Spinal Pain Management I. Policy University Health Alliance (UHA) will reimburse for nonsurgical interventional treatment for subacute and chronic spinal pain
Placename CCG. Policies for the Commissioning of Healthcare. Policy for Managing Back Pain- Spinal Injections
 Placename CCG Policies for the Commissioning of Healthcare Policy for Managing Back Pain- Spinal Injections 1 Introduction 1.1 This document is part of a suite of policies that the CCG uses to drive its
Placename CCG Policies for the Commissioning of Healthcare Policy for Managing Back Pain- Spinal Injections 1 Introduction 1.1 This document is part of a suite of policies that the CCG uses to drive its
Move Better, Feel Better: What Can Physical Therapy Do For You
 Back to Basics Move Better, Feel Better: What Can Physical Therapy Do For You Dr. Stephen Baxter, Dr. Dean Yamanuha Department of Physical Therapy and Rehabilitative Sciences 5/16/2017 Dr. Stephen Baxter
Back to Basics Move Better, Feel Better: What Can Physical Therapy Do For You Dr. Stephen Baxter, Dr. Dean Yamanuha Department of Physical Therapy and Rehabilitative Sciences 5/16/2017 Dr. Stephen Baxter
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Medical Affairs Policy
 Medical Affairs Policy Service: Back Pain: Sacroiliac and Coccydynia Treatments PUM 250-0024-1706 Medical Policy Committee Approval 06/15/18 Effective Date 10/01/18 Prior Authorization Needed Yes Disclaimer:
Medical Affairs Policy Service: Back Pain: Sacroiliac and Coccydynia Treatments PUM 250-0024-1706 Medical Policy Committee Approval 06/15/18 Effective Date 10/01/18 Prior Authorization Needed Yes Disclaimer:
Lumbar spinal canal stenosis Degenerative diseases F 08
 What is lumbar spinal canal stenosis? This condition involves the narrowing of the spinal canal, and of the lateral recesses (recesssus laterales) and exit openings (foramina intervertebralia) for the
What is lumbar spinal canal stenosis? This condition involves the narrowing of the spinal canal, and of the lateral recesses (recesssus laterales) and exit openings (foramina intervertebralia) for the
Kevin S. Ladin, M.D. Board Certified in Physical Medicine & Rehabilitation ABMS Subspecialty Board Certified in Pain Medicine
 Kevin S. Ladin, M.D. Board Certified in Physical Medicine & Rehabilitation ABMS Subspecialty Board Certified in Pain Medicine kslmd@cox.net EBM in Pain Medicine Evidence-based medicine (EBM) is a form
Kevin S. Ladin, M.D. Board Certified in Physical Medicine & Rehabilitation ABMS Subspecialty Board Certified in Pain Medicine kslmd@cox.net EBM in Pain Medicine Evidence-based medicine (EBM) is a form
Common Low Back Injuries in Dancers
 Common Low Back Injuries in Dancers Bones Anatomy of the Spine Ligaments & Discs Muscles Quadratus Lumborum (QL) Muscle Strain or Trigger Point The QL originates from the posterior iliac crest and inserts
Common Low Back Injuries in Dancers Bones Anatomy of the Spine Ligaments & Discs Muscles Quadratus Lumborum (QL) Muscle Strain or Trigger Point The QL originates from the posterior iliac crest and inserts
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
NASS Diagnosis and Treatment of Low-Back Pain Guideline Draft Clinical Question Protocol
 NASS Diagnosis and Treatment of Low-Back Pain Draft Clinical Questions Public Comment period: June 16-July 14, 2015 Comments should be sent to guidelines@spine.org Background The North American Spine Society
NASS Diagnosis and Treatment of Low-Back Pain Draft Clinical Questions Public Comment period: June 16-July 14, 2015 Comments should be sent to guidelines@spine.org Background The North American Spine Society
LUMBAR SPINE EXAMINATION AND ASSESSMENT. Dermot More O Ferrall, M.D. President, Advanced Pain Management
 LUMBAR SPINE EXAMINATION AND ASSESSMENT Dermot More O Ferrall, M.D. President, Advanced Pain Management Objectives Importance of good history Systematic approach to P/E Understand limitations Problem Focused
LUMBAR SPINE EXAMINATION AND ASSESSMENT Dermot More O Ferrall, M.D. President, Advanced Pain Management Objectives Importance of good history Systematic approach to P/E Understand limitations Problem Focused
All About? What is Sciatica. Disclaimer. Integrated web marketing. Multimedia Health Education
 What is Sciatica All About? Disclaimer This movie is an educational resource only and should not be used to manage sciatica. All decisions about the management of sciatica must be made in conjunction with
What is Sciatica All About? Disclaimer This movie is an educational resource only and should not be used to manage sciatica. All decisions about the management of sciatica must be made in conjunction with
Understanding your spine and how it works can help you better understand low back pain.
 Low Back Pain Almost everyone will experience low back pain at some point in their lives. This pain can vary from mild to severe. It can be short-lived or long-lasting. However it happens, low back pain
Low Back Pain Almost everyone will experience low back pain at some point in their lives. This pain can vary from mild to severe. It can be short-lived or long-lasting. However it happens, low back pain
Objectives. Identify and differentiate appropriate surgical cases. Good Surgical Outcomes
 ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
Discal herniation and spondylosis
 III.8.4.6 Degenerative disorders of the spine Introduction the frequency of locomotor disorders increases with age Low back pain is a very common disorder. According to medical literature, it is the second
III.8.4.6 Degenerative disorders of the spine Introduction the frequency of locomotor disorders increases with age Low back pain is a very common disorder. According to medical literature, it is the second
The Athlete s Lumbar Spine: Current Concepts
 The Athlete s Lumbar Spine: Current Concepts Content / Objectives Anatomy Common injuries Treatment and prevention Pablo Vazquez Seoane, M.D. 44 th Annual Sports Medicine Symposium January 19 21, 2017
The Athlete s Lumbar Spine: Current Concepts Content / Objectives Anatomy Common injuries Treatment and prevention Pablo Vazquez Seoane, M.D. 44 th Annual Sports Medicine Symposium January 19 21, 2017
Back Pain Update. Steven Andersen, MD Providence Physiatry Clinic 2016
 Back Pain Update Steven Andersen, MD Providence Physiatry Clinic 2016 Back Pain is Very Common Lifetime prevalence 80% 12 month prevalence 40% Point prevalence 20% Centers for Disease Control and Prevention.
Back Pain Update Steven Andersen, MD Providence Physiatry Clinic 2016 Back Pain is Very Common Lifetime prevalence 80% 12 month prevalence 40% Point prevalence 20% Centers for Disease Control and Prevention.
7) True/False: Rigid motor strategies are the most effective way to handle high forces
 True/False: Rigid motor strategies are the most effective way to handle high forces") The Sacro-Iliac Joint 1) Which of the following make up part of the SIJ provocative physical examination? A. Gaenslen s, FABERS, stork, joint distraction B. Fortin finger test, joint compression, thigh
The Sacro-Iliac Joint 1) Which of the following make up part of the SIJ provocative physical examination? A. Gaenslen s, FABERS, stork, joint distraction B. Fortin finger test, joint compression, thigh
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
CLINICAL GUIDELINES. Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision
 CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
Treatments for Common Pain Disorders. Matthew R. Kohler, MD Hudson Spine and Pain Medicine 03/01/2017
 Treatments for Common Pain Disorders Matthew R. Kohler, MD Hudson Spine and Pain Medicine 03/01/2017 Acute Disc Herniation Conservative Approach (Four to Six Weeks) Physical Therapy, exercise and gentle
Treatments for Common Pain Disorders Matthew R. Kohler, MD Hudson Spine and Pain Medicine 03/01/2017 Acute Disc Herniation Conservative Approach (Four to Six Weeks) Physical Therapy, exercise and gentle
12. Acromioclavicular (AC) Joint Compression Test (Shear)
 Joint Compression Test (Shear)") List of Some Common Orthopedic tests: Shoulder 1. Empty Can (Supraspinatus) Test 2. Yergason Test 3. Speed's Test 4. Ludington's Sign 5. Drop Arm Test 6. Apley's Scratch Test 7. Cross-Over Impingement
List of Some Common Orthopedic tests: Shoulder 1. Empty Can (Supraspinatus) Test 2. Yergason Test 3. Speed's Test 4. Ludington's Sign 5. Drop Arm Test 6. Apley's Scratch Test 7. Cross-Over Impingement
7 cervical (neck) vertebrae. 12 thoracic (middle back) vertebrae. 5 lumbar (low back) vertebrae. Sacrum (fused vertebrae) Coccyx (tailbone)
 vertebrae. 12 thoracic (middle back) vertebrae. 5 lumbar (low back) vertebrae. Sacrum (fused vertebrae) Coccyx (tailbone)") 7 cervical (neck) vertebrae 12 thoracic (middle back) vertebrae 5 lumbar (low back) vertebrae Sacrum (fused vertebrae) Coccyx (tailbone) The human spinal column is the center of postural control. It is
7 cervical (neck) vertebrae 12 thoracic (middle back) vertebrae 5 lumbar (low back) vertebrae Sacrum (fused vertebrae) Coccyx (tailbone) The human spinal column is the center of postural control. It is
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Cox Technic Case Report #126 published at (sent December 2013 ) 1
 1") Cox Technic Case Report #126 published at www.coxtechnic.com (sent December 2013 ) 1 Cox Technic Decompression Spinal Manipulation Resolves Symptoms Associated with Disc Protrusion and S1 Radiculopathy,
Cox Technic Case Report #126 published at www.coxtechnic.com (sent December 2013 ) 1 Cox Technic Decompression Spinal Manipulation Resolves Symptoms Associated with Disc Protrusion and S1 Radiculopathy,
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Coventry Pain Clinic - Spianl Pain - Sciatica and Brachalgia
 Coventry Pain Clinic - Spianl Pain - Sciatica and Brachalgia Copyright 2002-2005 Dr. Richard S. Walker Introduction Spinal Nerve Root Pain (Radiculopathy) can arise from the problems affecting the:- C4
Coventry Pain Clinic - Spianl Pain - Sciatica and Brachalgia Copyright 2002-2005 Dr. Richard S. Walker Introduction Spinal Nerve Root Pain (Radiculopathy) can arise from the problems affecting the:- C4
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
Case Studies: Low Back Pain in the Athlete. Jim Messerly DO
 Case Studies: Low Back Pain in the Athlete Jim Messerly DO Nothing to disclose Case #1 History 15 y/o male presents for evaluation of his low back pain. His pain has been present for several months. The
Case Studies: Low Back Pain in the Athlete Jim Messerly DO Nothing to disclose Case #1 History 15 y/o male presents for evaluation of his low back pain. His pain has been present for several months. The
University of Jordan. Professor Freih Abuhassan -
 Freih Odeh Abu Hassan F.R.C.S.(Eng.), F.R.C.S.(Tr.& Orth.). Professor of Orthopedics University of Jordan 1 A. Sacroiliitis History Trauma is very common Repetitive LS motion--lumbar rotation or axial
Freih Odeh Abu Hassan F.R.C.S.(Eng.), F.R.C.S.(Tr.& Orth.). Professor of Orthopedics University of Jordan 1 A. Sacroiliitis History Trauma is very common Repetitive LS motion--lumbar rotation or axial
Cervical and Thoracic Spinal Conditions Chapter 11
 Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION
 THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION William Micheo, MD Professor and Chairman Physical Medicine, Rehabilitation, and Sports Medicine Department University of Puerto Rico
THE OLDER TENNIS AND GOLF ATHLETE: INJURY MANAGEMENT AND PREVENTION William Micheo, MD Professor and Chairman Physical Medicine, Rehabilitation, and Sports Medicine Department University of Puerto Rico