Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome
|
|
|
- Shawn Ramsey
- 5 years ago
- Views:
Transcription
00022-6 DOI: 10.1016/j.bpg.2016.03.")
1 Accepted Manuscript Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome Matthijs J. Hommel, Bsc, Medical Student, Robertine van Baren, MD, Paediatric Surgeon, Jan Willem Haveman, MD, PhD, Abdominal and Transplant Surgeon PII: S (16) DOI: /j.bpg Reference: YBEGA 1417 To appear in: Best Practice & Research Clinical Gastroenterology Received Date: 15 January 2016 Accepted Date: 5 March 2016 Please cite this article as: Hommel MJ, van Baren R, Haveman JW, Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome, Best Practice & Research Clinical Gastroenterology (2016), doi: /j.bpg This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
2 Surgical Management and Autologous Intestinal Reconstruction in Short Bowel Syndrome Matthijs J Hommel, Bsc, Medical Student m.j.p.hommel@gmail.com Robertine van Baren, MD, Paediatric Surgeon r.van.baren@umcg.nl Corresponding author: Jan Willem Haveman, MD, PhD, Abdominal and Transplant Surgeon j.w.haveman@umcg.nl Department of Surgery University Medical Center Groningen, University of Groningen Hanzeplein 1, 9700 RB Groningen The Netherlands Phone: Fax: Keywords: Intestinal failure, short bowel syndrome, longitudinal intestinal lengthening and tailoring, serial transverse enteroplasty, spiral intestinal lengthening and tailoring, bariatric surgery Total words used: 6861 (including abstract, summary bullet points, tables and figures) 1
3 A. Abstract Short bowel syndrome (SBS) is a serious condition with considerable morbidity and mortality. When treatment with parenteral nutrition fails and life-threatening complications occur, autologous intestinal reconstruction (AIR) should be considered before intestinal transplantation (ITx). Single or combined ITx should be reserved for patients with severe liver disease and as last resort in the treatment of SBS. Longitudinal intestinal lengthening and tailoring (LILT) has proven its value in AIR, but its availability depends on the expertise of the surgeons. Serial transverse enteroplasty (STEP) has similar success rates as LILT and fewer patients progress to ITx. STEP is also applicable at small bowel dilatation in ultra-short bowel syndrome. The scope may be widened when duodenal dilatation can be treated as well. Spiral intestinal lengthening and tailoring (SILT) is a promising alternative. More research is needed to confirm these findings. Therefore we suggest an international data registry for all intestinal lengthening procedures. 2
4 A. Introduction Parenteral nutrition (PN) is the standard treatment in short bowel syndrome (SBS). After its introduction in the late 1960 s (1), several important improvements in the treatment of PN have been introduced. Despite these improvements, PN-dependent patients are still prone to develop severe complications contributing to a high mortality (2 4). Intestinal transplantation is the standard treatment for patients with intestinal failure who develop severe complications from PN or experience a low quality of life (5). The accepted indications nowadays for intestinal transplantation (ITx) are recurrent catheter related infections, thrombosis of the central veins, alteration in growth and development of infants, severe dehydration with refractory electrolyte changes and liver failure and/or liver cirrhosis with portal hypertension (5). The first successful isolated transplantation of the intestine was performed in 1989 (6), 2 years after the first successful multivisceral transplantation in 1987 (7). Improvement in surgical techniques, novel immunosuppressive agents and advances in anaesthesia and critical care led to an overall increase of intestinal transplantations worldwide. However, after the initial enthusiasm it became evident that the long-term results were disappointing with a 5-year graft survival of only 50% for patients transplanted after 2000 (8). As a consequence, the number of intestinal transplantations has decreased from more than 200 procedures in 2008 to only 120 cases in 2012 (8). Given the severe complications and the disappointing survival of ITx and low quality of life of patients on PN, all efforts should be made to prevent a SBS. The ultimate goal of treating SBS is to achieve enteral autonomy through medical and 3
5 surgical intestinal rehabilitation. The aim of this review is to discuss the initial surgical management and autologous intestinal reconstruction (AIR) in patients with SBS. A. Definition and aetiology of short-bowel syndrome B. Definition Short bowel syndrome (SBS) is a condition in which there is a congenital or an acquired shortage of small bowel length and thus a lack of absorptive small bowel surface. This leads to the incapability of retrieving enough nutrients, water and electrolytes to ensure growth in infants and body maintenance in adults and therefore requiring long-term administration of PN. The broader term intestinal failure includes in addition to SBS, mechanical abnormalities and intrinsic bowel diseases. These patients have a normal bowel length, but experience severe bowel obstructions or functional problems caused by motility disorders or mucosal abnormalities (9,10). In this chapter, we will limit ourselves to SBS with an anatomical absence or loss of significant bowel length. The total length of small bowel in a healthy person depends on the gestational age within a natural spread. The younger, the more growth potential there is. Loss of for instance 50 cm is clearly more severe in a premature born child then in a mature neonate (11). From the second year of life, bowel length does not significantly increase further and stays around 340 cm. However, the diameter of the intestinal lumen still increases with age (12). There have been made functional and anatomic classifications, both in 3 types, which enables us to compare treatments of SBS. The classification based on functional outcome 4
6 was introduced by Shaffer in 2002 (13). The latest revision has been made recently by Pironi et al (see Table 1): type I SBS being acute, short-term and usually self-limiting. Type II stands for a prolonged acute condition, often in metabolically unstable patients requiring complex multi-disciplinary care and intravenous supplementation over periods of weeks or months and type III representing chronic intestinal failure in metabolically stable patients, requiring intravenous supplementation over months or years; it may be reversible or irreversible (10,14). In adults the minimal length needed for functional type I or II SBS is at least 115 cm in patients with an endjejunostomy, 60 cm in case of a jejunocolic anastomosis and 35 cm if a jejunoileal anastomosis with an intact colon is present (Table 1 and Fig. 1) (15). Although the exact length is not part of the generally accepted functional classification, we thus know that the remaining bowel length is an important prognostic factor to estimate the amount of enteral autonomy that reasonably can be expected. In addition, a detailed description of the remaining length of the duodenum, jejunum, ileum and colon makes a comparison of the effectiveness of AIR possible. In the anatomical classification, type I represents the potentially severest condition being an end-jejunostomy. In type II there is no ileocaecal valve present, but there is jejunocolic continuity. In type III there is a jejunoileal anastomosis and the ileocaecal valve is preserved (Fig. 1) (16). It is clear from these classifications that small bowel length, presence of an ileocaecal valve and colon length are important prognostic factors in SBS. Other factors that should be taken into account are the age of the patient, diagnosis of an intrinsic bowel disease 5
7 like Crohns disease or a systemic disease, the presence of duodenum and the length of the remnant bowel (see Table 2) (17). B. Aetiology The aetiology of SBS differs between children and adults. In children SBS is most often the result of extensive resections due to necrotizing enterocolitis (NEC), complicated gastroschisis and midgut volvulus resulting from malrotation and severe intestinal atresia (18). The most common causes of SBS in adults are bowel ischemia due to superior mesenteric artery thrombosis, Crohns disease, volvulus and abdominal trauma (19). SBS as a complication of bariatric surgery is relatively upcoming and therefore we consider it worthwhile to include this in our review. A. Initial Surgical Management The initial management of SBS starts immediately after surgery. Abdominal sepsis and organ failure must be treated if present. Enteral nutrition has to be initiated as soon as possible to promote intestinal adaptation (20). Parenteral nutrition, management of bacterial overgrowth and treatment of PN associated liver disease are all essential in treating SBS patients, but are not within the scope of this chapter. All these aspects and possibilities should be discussed in a multidisciplinary team (21). Patients with intestinal failure must preferably be seen in an intestinal failure outpatient clinic by a dedicated gastroenterologist, gastrointestinal surgeon, dietician, stoma or wound nurse, psychologist and other specialists if necessary. A restorative surgical 6
8 procedure has to be discussed with the patient in order to restore the intestinal continuity. It is essential that the patient is in the best possible condition and that the surgical team is fully prepared by reviewing the surgery reports and radiographic imaging. Patients must be in a stable, anabolic state and infections and sepsis settled down. In a non-hostile abdomen it should be considered to restore continuity as early as possible (20). In addition, our own experience is that a relaparotomy performed more than 7-10 days after the initial abdominal exploration has a high change of iatrogenic bowel perforations and intra-operative complications. Most patients would benefit from a delayed intestinal reconstruction procedure performed at least 3 to 6 months after the last surgical procedure. Important principles of these operations are a complete adhesiolysis to get a good overview of the complete intestine and identify all internal fistulas. Also, resections have to be limited to a minimum with tension-free, well perfused anastomoses. All anastomoses have to be covered by peritoneum, omentum if present or at least the abdominal wall. Coverage of the intestine by abdominal wall reconstruction or biomesh interposition when necessary is essential after reconstructive surgery. A. Intestinal Failure after Bariatric Surgery B. Introduction in bariatric surgery Currently, bariatric surgery is the most effective ultimate treatment for severe obesity (22). The dramatic increase in incidence of overweight, severe and morbid obesity worldwide is a well known ongoing trend. Consequently, bariatric surgery has become 7
9 one of the most performed abdominal surgical procedures worldwide. Two different mechanisms contribute to weight loss after bariatric surgery, being restriction and malabsorption, or a combination of both. Two restrictive procedures are commonly used: gastric banding and most often a sleeve gastrectomy. Nowadays, combined restrictive and malabsorptive surgery is most often performed. In this matter, the procedures of choice are the Roux-Y gastric bypass, distal gastric bypass and the biliopancreatic diversion with or without gastric sleeve (23,24). B. Complications can lead to SBS All these operation differ in effectiveness, but also in potential complications. The incidence of severe complications that can potentially lead to SBS is very low. However, due to the dramatic increase in the amount of procedures, complications of bariatric surgery have become an important cause of SBS. There are several mechanisms that can lead to intestinal failure after bariatric surgery. First of all, severe malnutrition from a very short common channel <50 cm can lead to dramatic weight loss that results in severe protein-caloric malnutrition, vitamin deficiencies and liver failure. The malabsorbtive procedure should partially be reversed by increasing the bowel length of the common channel after a period on PN and before irreversible liver failure has occurred. Secondly, catastrophic gut loss is the most severe complication possible and can lead to permanent SBS. This may be the result of internal hernias and volvulus due to the altered anatomy, incarcerated incisional hernias, mesenteric ischemia, obstruction and necrosis due to severe adhesions. Finally, complications like anastomotic breakdown, perforations and fistulas can lead to gut loss (22). 8
10 Internal hernias are of specific concern after bariatric surgery. Internal hernias are difficult to recognize clinically and radiographically and require specific knowledge of the bariatric procedures (Fig. 2). Currently, most surgeons perform an antecolic gastric bypass, as there is evidence of a lower incidence of internal hernia s than with a retrocolic gastric bypass (25). Although ischemia and necrosis from the herniated segment as well as the small bowel bordering the defect can occur. Early recognition, urgent laparoscopic exploration and closure of the defects are important aspects to the success of treatment. Also, mesenteric ischemia due to thrombosis following altered coagulation or a non-recognized clotting disorder can lead to dramatic gut loss (26). B. Patient care Patients should be referred to a centre with expertise in intestinal failure after the initial dramatic event. Obviously, these patients need a thorough and multidisciplinary evaluation. Clinical review of the patient medical history and operative notes are essential. The anatomy and residual length of the intestine should be confirmed with radiological studies and if necessary endoscopic evaluation. Malnutrition, electrolyte disturbances, metabolic and vitamin deficiencies should all be corrected. When indicated, coagulation blood testing, visceral angiograms and full liver function tests with or without a liver biopsy should be performed. As mentioned before, we recommend restorative surgery within 7-10 days or after 3 to 6 months. The aim of this procedure is restoring the nutritional anatomy, reverse stomas and fistulas and avoid the recurrence of severe obesity. In patients with critical bowel length, all efforts should be made to 9
11 minimize additional bowel resection. Reversing bypassed segments and an additional AIR can be offered if needed. A. Antiperistaltic segments, colon interposition and nipple valve reconstruction B. Antiperistaltic segments In a select group of patients, interposition of an antiperistaltic segment might help to wean from PN. The indications for such procedures are rapid transit diarrhoea and/or a persistent high-output stoma despite conservative measures (27). The remaining bowel should be at least 25 cm. An important advantage of this procedure is that there is no need for a dilated bowel. Both the LILT and STEP procedure can only be performed on dilated segments of bowel. There are several options in implementing a reversed segment. The most used option is to reverse, thus not transposition, a cm segment of terminal ileum and to anastomose the distal end to the terminal ileum and the proximal end to the colon (27). Another option is to isolate cm of ileum and reverse transposition this between the proximal jejunum loops. Continuity is then restored with 3 end-to-end anastomoses. The reversed segment decreases transition time, reduces the myoelectric activity and consequently improves the absorption of nutrients. An important disadvantage is the risk for obstruction by isolating a segment that is too long. Also, reversed segments cannot be used in a very short remnant bowel (<15cm). Failure and complications can lead to loss of the reversed small bowel segment. 10
12 There are only a few series that describe the results of antiperistaltic segments in SBS. The largest study is a retrospective analysis of 38 patients from the group of Panis (28). After 5 years of follow-up 45% of their patients were completely weaned from PN. It has to be mentioned that all these procedures were combined with continuity restoration by stoma reversal, consequently inducing a significant gain in bowel length. Despite the encouraging results and acceptable complication rate this method has not gained much popularity (29,30). B. Colon Interposition and nipple valve construction The first publication on isoperistaltic colon interposition in dogs was done by Hutcher et al in 1971 (31). Only very few reports have been published about colon interposition ever since (32,33). Considered as important potential disadvantages are bowel obstruction, bacterial overgrowth and significant loss of bowel in case of complications. The interest in construction of artificial valves lies in the observation that a present ileocaecal valve has a positive influence on achieving enteral autonomy. An artificial valve is constructed at the intussusception of the distal ileum, thereby increasing the transit time and improving the enteral absorption. There are only very few cases known in literature, therefore we do not recommend to use this procedure as a treatment of SBS (34). A. Longitudinal Intestinal Lengthening and Tailoring B. Introduction and technique 11
13 In 1980, Bianchi described the first longitudinal intestinal lengthening and tailoring or LILT procedure in an experimental model using pigs (35). The first clinical application was performed one year after (36). Bianchi isolated a segment of dilated bowel from the rest of the bowel by dividing the proximal and distal end. Then, an avascular plane between the double leaflets of the mesentery is created. After confirmation of this double plane and having successfully separated these parts, the dilated bowel segment is divided using a linear stapling device. Three years later, Bianchi described an alternative for the stapling technique by cutting the bowel instead of stapling and close it afterwards with use of a hand-sewn technique, because of interloop fistulas which occurred frequently when the stapling technique was used (37). After creating an end-to-end anastomosis using a hand-sewn technique, the isolated bowel segment is connected proximally and distally to the small bowel or colon (Fig. 3). The net result is a doubling in length of the isolated bowel segment and a reduction of the diameter by half the size. Anatomical criteria for LILT are an intestinal diameter >3 cm, residual bowel length of > 40 cm and a length of dilated bowel loops >20 cm (38). Significant more complications are described after performing a LILT in shorter bowel segments (39). LILT can lead to less bacterial overgrowth and stasis. Although, evidence on treating bacterial overgrowth with LILT is limited. Bianchi has described a protocol for the management of SBS with an important role for intermittent clamping of the tube jejunostomy to expand the diameter of the small bowel (40). Because the results of LILT are already well reviewed elsewhere, we will only give a brief description of the outcome and complications (40 42). 12
14 B. Enteral autonomy and survival The degree of intestinal lengthening is significant after LILT. Although the isolated segment is doubled in length, the amount of intestinal lengthening of the entire bowel is reported 48-55% (41,42). The most recent series report a success rate of 37-91% for achieving enteral autonomy (40,43 45). B. Complications Initially, the reported complication rate was high with anastomotic stenosis (18%), staple line leakage (13%), interloop abscesses (7%) and fistula formation (7%)(21,42,46 50). Mortality in these series resulting from intra-abdominal sepsis and liver failure were around 30%. However, recent series show that with more surgical experience an acceptable complication rate and no surgical related mortality can be achieved (45). It must be mentioned though that even the most recent series not always clearly describe postoperative morbidity (40,45,51). Survival after LILT is comparable to other AIR procedures between 87-95%. The need for ITx is relatively low between 10-26% after LILT. B. Perspective A disadvantage of LILT is that it cannot be applied when the vessels in one of the mesenteric leaves are compromised. Another limitation is LILT being a one-time surgery that cannot be repeated on the same intestinal segment, as the double leaves of the mesentery can only be separated once. LILT is considered a primary treatment in SBS and is usually performed prior to any other AIR procedure. However, recently it was 13
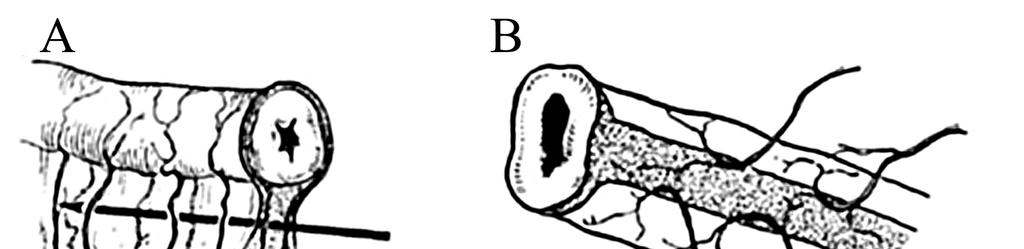
15 successfully applied in a 2-month old infant who experienced redilatation after a prior STEP. Without major complications reported, the patient weaned from PN, however, there is only a short-term follow-up of 7 months (52). Due to the lack of expertise worldwide and upcoming alternative treatments, LILT is nowadays performed only sporadically. Nevertheless, it is the only lengthening procedure with over 30 years of clinical application in the field of SBS and novel treatments should therefore be compared to the results achieved with LILT. A. Serial Transverse Enteroplasty B. Introduction and technique Serial transverse enteroplasty or STEP is a surgical technique to taper and lengthen the dilated small bowel. STEP was first described in 2003 in a porcine model as an alternative to LILT because of its minimal manipulation of the mesenteric vessels (53). That same year the procedure was performed at first in a 2-year old child with SBS (54). Nowadays, STEP is next to LILT one of the two mainly accepted surgical approaches for the treatment of SBS (40,41,55,56) and congenital dilatation and atresia (57). STEP is based on the anatomical principle of the vessels rising from the mesenteric border and enfolding the bowel perpendicularly to the long axis of the bowel. Therefore, there will remain no segments devascularized afterwards. With the use of a linear stapler, a zig-zag pattern is created with staples in opposite directions (Fig. 4), keeping a distance of 2 to 2.5 cm and maintaining a luminal diameter of approximately 2 cm dependent on the age and size of the patient (53). There is no lower limit in bowel length to perform 14
16 STEP, but a minimal luminal diameter of 3.5 to 4 cm is required (53,54). One of the characteristics of the procedure is a minimal manipulation of the mesentery. Also, because there are no anastomoses required, the intestinal lumen remains closed, consequently reducing bacterial contamination. STEP is considered to be a technically less challenging procedure in comparison to LILT and has the possibility to customize the tapering of the bowel (42,58), which is of importance when an asymmetrical dilatation of the bowel is present (53). B. Indications The aim of STEP is similar to that of general AIR procedure. STEP has been used to treat SBS caused by gastroschisis, proximal jejunal atresia, NEC and midgut volvulus (55,59,60). STEP has proven its value as primary therapy in neonates with congenital intestinal dilatation and atresia. It is possibly the only surgical intervention feasible for patients with ultra-short bowel syndrome (USBS) or SBS with a remnant bowel length of <20 cm (61 64). Also, STEP has successfully been performed in adult patients with a 90% survival rate and 47% of all patients who underwent STEP weaned from PN (44). Furthermore, STEP has a clear long-lasting influence on bacterial overgrowth and the associated D-lactic acidosis and therefore being a specific indication (65,66). STEP is preferred in particular as an additive to previous AIR procedures. It is important to realize that it is possible to perform STEP after LILT. Recently, Bueno et al reported a successful attempt to treat the dilated duodenum of 3 patients using a modified STEP procedure (67). To our knowledge, there are only few cases known where STEP was applied to the duodenum (66). Their promising findings may widen the scope of STEP, 15
17 whereas a significant amount of patients who underwent AIR still have to rely on PN (55,56,68,69). Studies in larger populations are needed to confirm these effects on dilatation of the duodenum. B. Enteral autonomy An important predictive factor for achieving enteral autonomy is the post-operative length of the small bowel (41,56,68,69). Multiple studies report the possibility of lengthening the small bowel over a 100% of its pre-operative length (56,60,61,69,70). In a systemic review of 109 patients who underwent STEP, a median percentage of 63% lengthening was reported (42). There is some variety in this finding, whereas other studies report a lengthening of 46-69% of the small bowel (41,55,71). The majority of patients who underwent STEP experience an overall improvement in nutritional status and a decrease in requirement for PN (60,70,72,73). These findings are supported with experimental evidence in animal and human studies. It is known that in patients with SBS, the intestine is able to adapt to enlarge the uptake of nutrients after resection (74). The absorption of xylose, which is a marker for the uptake of carbohydrates and mucosal integrity, generally improves after STEP as also the faecal fat content which is related to absorptive function of the bowel. Besides, motility patterns are preserved after STEP (65,75), with better bowel ratios and stool consistency and frequency improving (55). These improvements in absorption and function continue after both STEP and LILT and takes around 1 2 years (42), but can take years to reach a final plateau (55). If weaning from PN cannot be reached, STEP at least is able to postpone ITx (38). The number of 16
18 patients who receive ultimately an isolated or combined intestinal transplantation varies between 5% and 16% (41,42,73). B. Survival and complications Intestinal lengthening procedures of the last 15 years show a consistently high survivalrate with reports of 89% by the STEP Data Registry and up to 95% in a single-centre retrospective study. The main causes of death were liver failure and sepsis (41,42,58). Recent smaller studies report similar survival rates up to 100% (60,61,70,72,76). It is known that complications are common in STEP procedures, with a chance of intestinal bleeding being up to 26%, which is higher compared to other lengthening procedures (41,77). A recent study also identified a rather high infectious burden of 39% in 14 patients who underwent STEP, which could be of importance considering that sepsis is the second cause of death after STEP (78). Further research is required to identify the relation between infection and STEP. Redilatation is considered a serious complication effecting the nutritional status of the patient causing a lower weaning rate and higher mortality (79). The exact mechanism behind redilatation is still unclear. In literature, rates of redilatation requiring a re-step procedure go from 25% up to 49% (42,58). Re-STEP is not an inevitable problem and has proven its feasibility in both animals (80) and humans (81) with up to 50% of the patients weaned from PN. The possibility of re-step is of specific importance in case of bacterial overgrowth which can occur frequently as a complication of AIR (79). B. Long term outcome and perspective 17
19 Since the introduction in 2003, many studies have shown the positive effect of STEP. Determining the long term outcome has been difficult due to a limited follow-up time of only several years (41,42,55,70,82). More recently, Pakarinen et al reported the longest follow-up time to date with a median follow-up time of 9.7 years ( years) of 8 patients (59). Indications for intestinal lengthening were intestinal failure due to SBS, dilated bowel segments and complications of bacterial overgrowth. Their conclusions support the previous findings with a survival rate of 90% and a promising weaning rate with 8 out of 9 patients remaining off PN at median 6.9 years after AIR. Interestingly, they found the same survival and weaning rate for children with SBS without AIR. These numbers and conclusions have to be interpreted carefully though, considering the sample size and retrospective character of this study. Therefore, larger population studies are needed, preferably including a control group, although due to ethical reasons such a study will probably not be conducted. However, the International STEP Data Registry ( could confirm the promising findings with a next report (71). The scope of STEP can possibly be widened further by using delayed primary STEP in children with USBS, which remains a challenging condition and still has a poor outcome (62). The principle of this approach rests in obstructing the small bowel intermediately and facilitate the dilatation of the bowel with sham feeds to optimize the bowel for STEP. This technique accelerates the growth potential of the bowel, with an observed increase of the small bowel length up to 294%. Controlled bowel expansion is not a novel concept, whereas it has already been applied previously in LILT (21,83 85). Further research is needed to confirm these promising results of delayed primary STEP as treatment for USBS and trace the mechanisms behind it. 18
20 A. Spiral intestinal lengthening and tailoring Spiral intestinal lengthening and tailoring (SILT), was introduced in 2011 by Cersni et al in an experimental animal model as a possible alternative and additive to STEP and LILT (86). With SILT, incisions in the mesentery are made carefully without damaging any vessels. Next, the intestinal wall is cut spirally in an angle to the longitudinal axis. Basically, the total length will increase and its diameter is reduced by stretching the bowel over a tube preserving the adjust luminal diameter (Fig. 5) (87). SILT was then applied in vivo to porcine small bowel in which the jejunum was lengthened with 75% and the luminal diameter reduced by 56% (88) after inducing dilatation with controlled bowel expansion. An advantage of SILT is the mild alteration of the position of the intestinal muscle fibres and therefore should influence peristalsis less. A major disadvantage of SILT is the requirement to open the lumen completely, whereas in a STEP procedure the lumen remains closed, reducing bacterial contamination. Thereto, in an experimental model a modified SILT procedure was developed where the mucosa is remained intact with incisions made only in the muscular and submucosal layer so that the lumen is only opened on the outer ends (89). Recently, the first clinical application of SILT was successfully introduced on a 3-year old patient after initial controlled bowel expansion (90). In this case, the dilated segment was lengthened by 81% (from 11 to 20 cm) leading to an increase in total jejunal length by 41% and a reduction of the diameter by 50% to 2 cm. The patient was weaned from 19
21 PN 4 weeks after surgery and still is at 6 months follow-up. The second successful application on a 10-month old neonate led to a lengthening of 125% (from 4 to 9 cm) without controlled bowel expansion (91). This patient did not fully wean from PN, but did well with a PN requirement of 18% at 12 months after surgery. The indication for AIR in both cases was SBS due to midgut volvulus. In neither case serious complications were reported. These case reports prove that SILT has potential as treatment in SBS. Its remarkable technique is also already studied for other applications (92). A. Patient selection and care Specialized multidisciplinary programs to optimize the management of intestinal failure have irrefutable improved the outcomes in the last decade (93). The chance of weaning from PN and survival rates increased, whereas the cases of central line infections and intestinal failure associated liver disease decreased. Also, patient selection is an important key to successful intestinal lengthening procedures and to prevent unnecessary procedures in patients who could wean from PN without surgery (38). STEP can be performed at any age with cases in literature varying from the first day after delivery until adulthood (41,57). Performing LILT in neonates is not without controversy because of unfavourable outcome and complications (39), although LILT was performed successfully at the age of 6 weeks. For SILT however, no conclusions can be drawn yet due to its recent introduction. Liver failure is an important contraindication to intestinal lengthening procedures (94). Patients with advanced liver disease are facing poor prognoses after AIR and may benefit 20
22 more from an isolated liver transplantation prior to AIR or a combined intestinal/liver transplantation if enteral autonomy is not expected after AIR. (41). Nevertheless, there is a lack of consensus in literature about when intestinal lengthening procedures can be performed in patients developing liver disease (55). A. Discussion and Conclusion SBS has a dramatic impact on the quality of life of a patient and is associated with significant morbidity and mortality. Therefore, it is obvious that every effort should be made to prevent SBS by limiting bowel resections to an absolute minimum and treat the underlying disease. Moreover, patient care for SBS must be optimized in a specialized multidisciplinary intestinal failure program to prevent complications of PN and contain intestinal failure associated liver disease, since this is associated with a higher morbidity and mortality. Therefore, one of the keys to success of AIR in SBS is patient selection. If AIR cannot lead to PN independence, it should be considered as an option to postpone intestinal or combined transplantation, which is currently the last resort for these patients. If AIR is indicated, the first step is restoration of small bowel continuity through relaparotomy in case of unused intestinal segments. In a non-hostile abdomen this can be done relatively early, meaning within 7-10 days, after the initial surgical procedure. The alternative approach is a relaparotomy 3 to 6 months later. AIR can be performed as well during this operation if the bowel is critically short. Important principles of AIR procedures are knowledge of the exact altered gut anatomy and a thoroughly performed adhesiolysis to recognize all fistulas, obstructions or strictures. Any anastomosis has to be 21
23 well perfused, tension free and covered with peritoneum, omentum and at least the abdominal wall. As mentioned, AIR should be considered in every patient with SBS and persistent PN dependence who reached a plateau in their intestinal adaptation. Over the last decades several surgical procedures have been introduced. The least common performed procedures are antiperistaltic segments and colon interposition. Because of complications like obstruction, rapid transit time and disturbance of motility patterns, antiperistaltic segments and colon interposition did not find its way into the clinic, despite initially promising results. Generally, there are serious concerns on the effectiveness and complications of these procedures. Therefore, we cannot recommend this as therapeutic options in the treatment of SBS. Since LILT is surgically a challenging procedure, the type of reconstruction will depend first of all on the experience of the surgeon. If the expertise is not present, STEP should be the first surgical treatment to consider. LILT doubles the length of the isolated segment, whereas in STEP the gained length depends on the extend of the dilated bowel. In clinical setting it is seen that with STEP more length is gained compared to LILT. Both procedures show good survival rates of around 90%. In studies with larger populations included, average rates are reported up to 69% for STEP vs. 55% for LILT. PN independence is achieved in both LILT and STEP in up to 55-60% of the patients, but there is a large spread of these numbers in literature, thus careful interpretation is therefore needed. 22
24 One should consider that after LILT, STEP can be performed relatively easy, but vice versa will be challenging. However, despite what is generally assumed, it is technically possible to perform a LILT procedure after STEP (52). Despite the short follow-up, this is an interesting finding which teaches us that SBS is a dynamic condition that requires a personalized medical and surgical approach. Nevertheless, STEP remains the most performed AIR procedure nowadays, largely due to the technically difficulties of LILT. There are clear advantages of STEP compared to LILT (see Table 2). STEP is the only procedure where the lumen remains closed, potentially reducing the chance of complications. Consequently, (late) interloop fistulas, abscesses, necrosis and leakage are more often seen in LILT. This is of importance when taken into account that these complications could lead to further gut loss. However, the complications are, to our view, not always clearly described. Any postoperative complication or mortality should be clearly described in future publications to get a better view on what short and long term positive or side effects AIR procedures cause. Furthermore, STEP has a wider scope whereas it can be applied to USBS tailored to asymmetrical dilated bowel segments and dilated duodenum. Also, STEP has a clear effect on bacterial overgrowth which is less seen after LILT. Despite this, redilatation is seen more often in STEP, although it is easily reproducible and after a second or third STEP >50% of the patients could still wean from PN after all or at least improve their nutritional status. SILT is novel lengthening procedure with promising clinical results. In unpublished data, a lengthening of 75% is reported in three patients who all weaned from PN (91). 23
25 SILT has similar advantages as STEP compared to LILT, being a technically less challenging procedure with a minimal handling of the mesentery without compromising the blood supply. However, STEP is considered a technically less challenging and quicker procedure than SILT. With both SILT and STEP it is possible to reduce the luminal diameter more than 50%, (91) whereas in LILT the luminal diameter can only be reduced by half. Cserni et al state that in STEP the physiology of the muscle fibres is dramatically altered and reverses the role of longitudinal fibres to circular and vice versa, possibly compromising peristalsis (86,88,91). However, one could argue that experimental evidence showed that motility in STEP is preserved (65,75), therefore the relation between altered muscle fibres direction and peristalsis remains unclear and needs to be studied further. Finally, whereas STEP has the potential of treating duodenal dilatation (67), SILT could probably not be applied to the duodenum due to its relation with the pancreas. Nevertheless, SILT has an undeniably potential in the treatment of SBS. Promising results are encouraging further studies in a larger population to confirm the effects of SILT and determine the long-term outcome. Also, SILT needs to be compared to other AIR techniques like LILT and STEP. We are curious to see more data and maybe a prospective randomized controlled trial could be conducted between STEP and SILT in the future. Based on the current literature, most patients who received AIR are treated with LILT or STEP. The results are relatively good, but the considerable morbidity remains a point of concern. Comparison between frequently used AIR procedures has been difficult due to discrepancy in follow-up times, methods and lack of control groups. Only recently, long- 24
26 term outcome of STEP has started to become clearer, but only in case reports or retrospective studies. Currently, a randomized controlled trial between LILT and STEP is in our opinion almost impossible to conduct due to the low patient numbers and limited surgical expertise in both AIR procedures. In our opinion it might be worthwhile to initiate a combined online data registry for all intestinal lengthening procedures, including LILT, STEP and possibly SILT. This will give us more insights in all aspects of the lengthening procedures. 25
27 Summary In general, AIR should be considered in SBS patients who are dependent on long-term PN. Since there is no lengthening procedure without the risk of complications, all efforts should be made to limit bowel resection wherever possible and prevent complications of PN. If AIR is needed after all, restoration of bowel continuity should be the first step. Currently, in clinical practice two mainly applied surgical interventions are available; being LILT and STEP. We think LILT, however being a technically difficult procedure demanding specific expertise, should be performed if possible. If not, STEP can be performed as both primary treatment and after prior AIR procedures. Of specific importance is the right assessment of the indication. STEP is superior to LILT in treating bacterial overgrowth and seems the only feasible option in treating USBS and duodenal dilatation. Also, complications leading to gut loss are seldom seen after STEP. If PN independence is not within reach, AIR can be considered as a bridge to intestinal transplantation. Novel techniques like SILT need to be further investigated before widespread clinical implication. Since there are no randomized controlled studies that confirm these conclusions and it is unlike there is going to be one, it will be difficult to determine an evidence based golden standard because of the spread in results in the currently available literature of the last decade. To create the best possible evidence based clinical guidelines, we suggest that an international online data registry for LILT, STEP and SILT should be founded. 26
28 Bullet points: Research agenda SILT Found online data registry and compare outcomes. Treatment of duodenal dilatation with STEP. Combination of controlled bowel expansion and STEP. Determine an international accepted golden standard for the surgical management of short and ultra-short bowel syndrome. Practice point If expertise is available, perform LILT as initial intestinal lengthening procedure. A second or third STEP can still lead to independence of PN for >50% of patients. STEP is the treatment of choice in bacterial overgrowth when medical management fails. STEP should be considered in persistent PN dependence ultra-short bowel syndrome without improvement. When PN independence is not to be expected, intestinal lengthening procedures should be considered a bridge to intestinal transplantation. Conflict of interest statement 27
29 No conflict of interest has been declared by the authors. 28
30 Bibliography 1. Wilmore DW, Dudrick SJ. Growth and development of an infant receiving all nutrients exclusively by vein. JAMA. 1968;203(10): Lyn H, Marvin A, Fleming CR, Shine M, Steiger E. Current Use and Clinical Outcome of Home Parenteral and Enteral Nutrition Therapies in the United States. Gastroenterology. 1995;109: Pironi L, Joly F, Forbes A, Colomb V, Lyszkowska M, Baxter J, et al. Long-term follow-up of patients on home parenteral nutrition in Europe: implications for intestinal transplantation. Gut. 2011;60: Squires RH, Duggan C, Teitelbaum DH, Wales PW, Balint J, Venick R, et al. Natural History of Pediatric Intestinal Failure: Initial Report from the Pediatric Intestinal Failure Consortium. J Pediatr. Mosby, Inc.; 2012;161(4): Sudan D. The Current State of Intestine Transplantation: Indications, Techniques, Outcomes and Challenges. Am J Transplant. 2014;14: Goulet O, Revillon Y, Canioni D, Jan D, Brousse N, Sadoun E, et al. Two and one-half-year follow-up after isolated cadaveric small bowel transplantation in an infant. Transplant Proc. 1992;24(3): Starzl TE, Rowe MI, Todo S, Jaffe R, Tzakis A, Hoffman AL, et al. Transplantation of Multiple Abdominal Viscera. JAMA. 1989;261(10): Grant D, Abu-elmagd K, Mazariegos G, Vianna R, Lagnas A, Mangus R, et al. Intestinal Transplant Registry Report : Global Activity and Trends. Am J Transplant. 2015;15: Soden JS. Clinical assessment of the child with intestinal failure. Semin Pediatr 29
31 Surg. Elsevier Inc.; 2010;19: Pironi L, Arends J, Baxter J, Bozzetti F, Burgos R, Cuerda C, et al. ESPEN endorsed recommendations. Definition and classification of intestinal failure in adults. Clin Nutr. 2015;34: Touloukian RJ, Smith GJ. Normal intestinal length in preterm infants. J Pediatr Surg. 1983;18(6): Gondolesi G, Ramisch D, Padin J, Almau H, Sandi M, Schelotto B, et al. What Is the Normal Small Bowel Length in Humans? First Donor-Based Cohort Analysis. Am J Transplant. 2012;12: Shaffer J. Intestinal failure: definition and service development. Clin Nutr. Elsevier Science Ltd.; 2002;21: Shaffer J. Intestinal failure: definition and service development. Clin Nutr. 2002;21(Suppl. 1): Nightingale J, Woodward JM. Guidelines for management of patients with a short bowel. Gut. 2006;55(suppl_4):iv Feldman M, Friedman LS, Sleisenger MH. Sleisenger & Fordtran s Gastrointestinal and Liver Disease: Pathofysiologym Diagnosis, Management. In: 7th ed. Elsevier; p Infantino BJ, Mercer DF, Hobson BD, Fischer RT, Gerhardt BK, Grant WJ, et al. Successful rehabilitation in pediatric ultrashort small bowel syndrome. J Pediatr. 2013;163(5): Wales PW, Christison-lagay ER. Short bowel syndrome: epidemiology and etiology. Semin Pediatr Surg. Elsevier Inc.; 2010;19:
32 19. Grant D, Abu-Elmagd K, Mazariegos G, Vianna R, Langnas a., Mangus R, et al. Intestinal Transplant Registry Report: Global Activity and Trends. Am J Transplant. 2015;15(1): Andorsky DJ, Lund DP, Lillehei CW, Jaksic T, Dicanzio J, Richardson DS, et al. Nutritional and other postoperative management of neonates with short bowel syndrome correlates with clinical outcomes. J Pediatr. 2001;139(1): Bianchi A. From the cradle to enteral autonomy: The role of autologous gastrointestinal reconstruction. Gastroenterology. 2006;130(2): Abu-Elmagd K, Costa G, McMichael D, Khanna A, Cruz RJ, Parekh NR, et al. Autologous Reconstruction and Visceral Transplantation for Management of Patients With Gut Failure After Bariatric Surgery: 20 Years of Experience. Ann Surg. 2015;262(4): The International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) [Internet]. Available from: American Society for Metabolic and Bariatric Surgery [Internet]. Available from: Rondelli F, Bugiantella W, Desio M, Vedovati MC, Boni M, Avenia N, et al. Antecolic or Retrocolic Alimentary Limb in Laparoscopic Roux-en-Y Gastric Bypass? A Meta-Analysis. Obes Surg. 2016;26(1): Eriksson S, Backman L, Ljungström KG. The incidence of clinical postoperative thrombosis after gastric surgery for obesity during 16 years. Obes Surg. 1997;7(4):332 5; discussion Panis Y, Messing B, Rivet P, Coffin B, Hautefeuille P, Matuchansky C, et al. 31
33 Segmental reversal of the small bowel as an alternative to intestinal transplantation in patients with short bowel syndrome. Ann Surg. 1997;225(4): Beyer-Berjot L, Joly F, Maggiori L, Corcos O, Bouhnik Y, Bretagnol F, et al. Segmental Reversal of the Small Bowel Can End Permanent Parenteral Nutrition Dependency. Ann Surg. 2012;256(5): Pigot F, Messing B, Chaussade S, Pfeiffer A, Pouliquen X, Jian R. Severe Short Bowel Syndrome with a Surgically Reversed Small Bowel Segment. Dig Dis Sci. 1990;35(1): Layec S, Beyer L, Corcos O, Alves A, Dray X, Amiot A, et al. Increased intestinal absorption by segmental reversal of the small bowel in adult patients with shortbowel syndrome: a case-control study. Am J Clin Nutr. 2013;97: Hutcher, NE SA. Pre-ileal transposition of colon to prevent the development of short bowel syndrome in puppies with 90% small intestinal resection. Surgery. 1971;70(2): Garcia VF, Templeton JM, Eichelberger MR, Koop CE, Vinograd I. Colon Interposition for the Short Bowel Syndrome. J Pediatr Surg. 1981;16(6): Glick BPL, Lorimier AA De, Adzick NS, Harrison MR. Colon Interposition: An Adjuvant Operation for Short-Gut Syndrome. J Pediatr Surg. 1984;19(6): Georgeson K, Halpin D, Figueroa R, Vincente Y, Hardin WJ. Sequential intestinal lengthening procedures for refractory short bowel syndrome. J Pediatr Surg. 1994;29(2): Bianchi A. Intestinal loop lengthening A technique for increasing small intestinal length. J Pediatr Surg. 1980;15(2):
34 36. Boeckman CR, Traylor R. Bowel lengthening for short gut syndrome. J Pediatr Surg. 1981;16(6): Bianchi A. Intestinal lengthening: An experimental and clinical review. J R Soc Med. 1984;77(SUPPL. 3): Rege A. The Surgical Approach to Short Bowel Syndrome - Autologous Reconstruction versus Transplantation. Viszeralmedizin. 2014;30(3): Bianchi A. Longitudinal intestinal lengthening and tailoring: results. J R Soc Med. 1997;90(Ic): Walker SR, Nucci A, Yaworski JA, Barksdale EM. The Bianchi procedure: A 20- year single institution experience. J Pediatr Surg. 2006;41: Sudan D, Thompson J, Botha J, Grant W, Antonson D, Raynor S, et al. Comparison of Intestinal Lengthening Procedures for Patients With Short Bowel Syndrome. Ann Surg. 2007;246(4): Frongia G, Kessler M, Weih S, Nickkholgh A, Mehrabi A, Holland-Cunz S. Comparison of LILT and STEP procedures in children with short bowel syndrome A systematic review of the literature. J Pediatr Surg. Elsevier Inc.; 2013;48(8): Bonnard A, Staub G, Segura J-F, Malbezin S, Dorgeret S, Aigrain Y, et al. Evaluation of intestinal absorption after longitudinal intestinal lengthening for short bowel syndrome. J Pediatr Surg. 2005;40(10): Yannam GR, Sudan DL, Grant W, Botha J, Langnas A, Thompson JS. Intestinal lengthening in adult patients with short bowel syndrome. J Gastrointest Surg. 2010;14:
35 45. Khalil BA, Ba ath ME, Aziz A, Forsythe L, Gozzini S, Murphy F, et al. Intestinal rehabilitation and bowel reconstructive surgery: improved outcomes in children with short bowel syndrome. J Pediatr Gastroenterol Nutr. 2012;54(4): Weber TR. Isoperistaltic Bowel Lengthening for Short Bowel Syndrome in Children. Am J Surg. 1999;178: Figueroa-Colon R, Harris PR, Birdsong E, Franklin FA, Georgeson KE. Impact of Intestinal Lengthening on the Nutritional Outcome for Children With Short Bowel Syndrome. J Pediatr Surg. 1996;31(7): Weber R, Powell MA. Early Improvement in Intestinal Function After Isoperistaltic Bowel Lengthening. J Pediatr Surg. 1996;31(1): Bueno BJ, Guiterrez J, Mazariegos G V, Abu-elmagd K, Madariaga J, Ohwada S, et al. Analysis of Patients With Longitudinal Intestinal Lengthening Procedure Referred for Intestinal Transplantation. J Pediatr Surg. 2001;36(1): Weber TR, Powell MA. Early improvement in intestinal function after isoperistaltic bowel lengthening. J Pediatr Surg. 1996;31(1):61 3; discussion Bonnard A, Staub G, Segura S, Malbezin S, Dorgeret S, Aigrain Y, et al. Evaluation of intestinal absorption after longitudinal intestinal lengthening for short bowel syndrome. J Pediatr Surg. 2005;40: Fusaro F, Hermans D, Wanty C, Veyckemans F, Pirenne J, Reding R. Post-serial transverse enteroplasty bowel redilatation treated by longitudinal intestinal lengthening and tailoring procedure. J Pediatr Surg. Elsevier Inc.; 2012;47(10):e Kim HB, Fauza D, Garza J, Oh JT, Nurko S, Jaksic T. Serial transverse 34
36 enteroplasty (STEP): A novel bowel lengthening procedure. J Pediatr Surg. 2003;38(3): Kim HB, Lee PW, Garza J, Duggan C, Fauza D, Jaksic T. Serial Transverse Enteroplasty for Short Bowel Syndrome: A Case Report. J Pediatr Surg. 2003;38(6): Oliveira C, Silva N De, Wales PW. Five-year outcomes after serial transverse enteroplasty in children with short bowel syndrome. J Pediatr Surg. Elsevier B.V.; 2012;47: Jones BA, Hull MA, Potanos KM, Zurakowski D, Fitzgibbons SC, Ching YA, et al. Report of 111 Consecutive Patients Enrolled in the International Serial Transverse Enteroplasty ( STEP ) Data Registry : A Retrospective Observational Study. J Am Coll Surg. 2013;216(3): Cowles RA, Lobritto SJ, Stylianos S, Brodlie S, Smith LJ, Jan D. Case Report Serial Transverse Enteroplasty in a Newborn Patient. J Pediatr Gastroenterol Nutr. 2007;45: Pakarinen MP. Autologous intestinal reconstruction surgery as part of comprehensive management of intestinal failure. Pediatr Surg Int. 2015;31: Pakarinen MP, Kurvinen A, Koivusalo AI, Iber T, Rintala RJ. Long-term controlled outcomes after autologous intestinal reconstruction surgery in treatment of severe short bowel syndrome. J Pediatr Surg. Elsevier Inc.; 2013;48: Oh PS, Fingeret AL, Shah MY, Ventura K a, Brodlie S, Ovchinsky N, et al. Improved tolerance for enteral nutrition after serial transverse enteroplasty (STEP) 35
37 in infants and children with short bowel syndrome--a seven-year single-center experience. J Pediatr Surg. Elsevier Inc.; 2014;49(11): Garnett GM, Kang KH, Jaksic T, Woo RK, Puapong DP, Kim HB, et al. First STEPs: serial transverse enteroplasty as a primary procedure in neonates with congenital short bowel. J Pediatr Surg. Elsevier Inc.; 2014;49(1):104 7; discussion Wales PW, Jancelewicz T, Romao RL, Piper HG, Silva NT De, Avitzur Y. Delayed primary serial transverse enteroplasty as a novel management strategy for infants with congenital ultra-short bowel syndrome. J Pediatr Surg. Elsevier Inc.; 2013;48(5): Coletta R, Khalil BA, Morabito A. Short bowel syndrome in children: Surgical and medical perspectives. Semin Pediatr Surg. Elsevier; 2014;23(5): Khalil BA, Ba ath ME, Aziz A, Forsythe L, Gozzini S, Murphy F, et al. Intestinal rehabilitation and bowel reconstructive surgery: improved outcomes in children with short bowel syndrome. J Pediatr Gastroenterol Nutr. 2012;54(4): Chang RW, Javid PJ, Oh J-T, Andreoli S, Kim HB, Fauza D, et al. Serial Transverse Enteroplasty Enhances Intestinal Function in a Model of Short Bowel Syndrome. Ann Surg. 2006;243(2): Modi BP, Langer M, Duggan C, Kim HB, Jaksic T. Case Report Serial Transverse Enteroplasty for Management of Refractory D -Lactic Acidosis in Short-bowel Syndrome. J Pediatr Gastroenterol Nutr. 2006;43: Bueno J, Redecillas S, GarcÍa L, Lara A, Giné C, Molino JA, et al. Duodenal lengthening in short bowel with dilated duodenum. J Pediatr Surg. Elsevier Inc.; 36
38 2015;50(3): Reinshagen K, Kabs C, Wirth H, Hable N, Brade J, Zahn K, et al. Long-term outcome in patients with short bowel syndrome after longitudinal intestinal lengthening and tailoring. J Pediatr Gastroenterol Nutr. 2008;47(5): Javid PJ, Sanchez SE, Horslen SP, Healey PJ. Intestinal lengthening and nutritional outcomes in children with short bowel syndrome. Am J Surg. Elsevier Inc; 2013;205(5): Mercer DF, Hobson BD, Gerhardt BK, Grant WJ, Vargas LM, Langnas AN, et al. Serial Transverse Enteroplasty Allows Children with Short Bowel to Wean from Parenteral Nutrition. J Pediatr. Elsevier Ltd; 2014;164(1): Modi BP, Javid PJ, Jaksic T, Piper H, Langer M, Duggan C, et al. First Report of the International Serial Transverse Enteroplasty Data Registry: Indications, Efficacy, and Complications. J Am Coll Surg. 2007;204(3): Wester T, Borg H, Naji H, Stenström P, Westbacke G, Lilja HE. Serial transverse enteroplasty to facilitate enteral autonomy in selected children with short bowel syndrome. Br J Surg. 2014;101(10): King B, Carlson G, Khalil BA, Morabito A. Intestinal Bowel Lengthening in Children with Short Bowel Syndrome : Systematic Review of the Bianchi and STEP Procedures. World J Surg. 2013;37: Tappenden KA. Intestinal Adaptation Following Resection. J Parenter Enter Nutr. 2014;38(Supplement 1):23S 31S. 75. Modi BP, Ching YA, Langer M, Donovan K, Fauza DO, Kim HB, et al. Preservation of intestinal motility after the serial transverse enteroplasty procedure 37
39 in a large animal model of short bowel syndrome. J Pediatr Surg. Elsevier Inc.; 2009;44: Wang J, Du L, Cai W, Pan W, Yan W. Prolonged feeding difficulties after surgical correction of intestinal atresia: a 13-year experience. J Pediatr Surg. Elsevier Inc.; 2014;49(11): Fisher JG, Stamm DA, Modi BP, Duggan C, Jaksic T. Gastrointestinal bleeding as a complication of serial transverse enteroplasty. J Pediatr Surg. Elsevier Inc.; 2014;49(5): Fujioka WK, Cowles RA. Infectious complications following serial transverse enteroplasty in infants and children with short bowel syndrome. J Pediatr Surg. Elsevier Inc.; 2015;50(3): Miyasaka EA, Brown PI, Teitelbaum DH. Redilation of bowel after intestinal lengthening procedures--an indicator for poor outcome. J Pediatr Surg. Elsevier; 2011 Jan 1;46: Piper H, Modi BP, Kim HB, Fauza D, Glickman J, Jaksic T. The second STEP: the feasibility of repeat serial transverse enteroplasty. J Pediatr Surg. 2006;41(12): Andres AM, Thompson J, Grant W, Botha J, Sunderman B, Antonson D, et al. Repeat Surgical Bowel Lengthening With the STEP Procedure. Transplantation. 2008;85(9): Lourenço L, Campos M, Monteiro J. Serial transverse enteroplasty ( STEP ): intermediate outcomes in children with short bowel syndrome. Eur J Pediatr. 2012;171:
40 83. Murphy F, Khalil B a, Gozzini S, King B, Bianchi a, Morabito a. Controlled tissue expansion in the initial management of the short bowel state. World J Surg. 2011;35(5): Bianchi A, Morabito A. The dilated bowel: a liability and an asset. Semin Pediatr Surg. Elsevier Inc.; 2009;18(4): J. CIII, Y. V, K. G, D. K. Partial intestinal obstruction induces substantial mucosal proliferation in the pig. J Pediatr Surg. 1996;31(3): Cserni T, Takayasu H, Muzsnay Z, Varga G, Murphy F, Folaranmi SE, et al. New idea of intestinal lengthening and tailoring. Pediatr Surg Int. 2011;27(9): Cserni T. Spiral Intestinal Lengthening and Tailoring [Internet]. Available from: Cserni T, Varga G, Erces D, Kaszaki J, Boros M, Laszlo A, et al. Spiral intestinal lengthening and tailoring - First in vivo study. J Pediatr Surg. Elsevier Inc.; 2013;48(9): Mehrabi V, Mehrabi A, Jamshidi SH, Pedram MS, Sabagh MS, Jaberansari N, et al. Modified Spiral Intestinal Lengthening and Tailoring for Short Bowel Syndrome. Surg Innov. 2015; 90. Cserni T, Biszku B, Guthy I, Dicso F, Szaloki L, Folaranmi S, et al. The first clinical application of the spiral intestinal lengthening and tailoring (silt) in extreme short bowel syndrome. J Gastrointest Surg. 2014;18(10): Alberti D, Boroni G, Giannotti G, Parolini F, Armellini A, Morabito A, et al. Spiral intestinal lenghtening and tailoring (SILT) for a child with severely short bowel. Pediatr Surg Int. 2014;30(11):
41 92. Cervellione RM, Hajnal D, Varga G, Rakoczy G, Kubiak R, Kaszaki J, et al. New alternative Mitrofanoff channel based on spiral intestinal lengthening and tailoring. J Pediatr Urol. Elsevier Ltd; 2015;11(3):131.e1 131.e Stanger JD, Oliveira C, Blackmore C, Avitzur Y, Wales PW. The impact of multidisciplinary intestinal rehabilitation programs on the outcome of pediatric patients with intestinal failure: A systematic review and meta-analysis. J Pediatr Surg. Elsevier Inc.; 2013;48(5): Ba ath ME, Almond S, King B, Bianchi A, Khalil B a., Morabito A. Short bowel syndrome: A practical pathway leading to successful enteral autonomy. World J Surg. 2012;36: Bakker, de JK, Namen, van YWB, Bruin SC, Brauw, de LM. Gastric Bypass and Abdominal Pain: Think of Petersen Hernia. JSLS, J Soc Laparoendosc Surg. 2012;16(2):
42 Table 1. Anatomical and functional classification of short bowel syndrome Anatomical Functional Type I End-jejunostomy Acute, short-term, usually self limiting Type II Type III Jejunocolonic continuitiy, ileocaecal valve not present Jejunoileal anastomosis, ileocaecal valve present Prolonged acute condition Often metabolically unstable patients Complex multidisciplinairy care Intravenous supplementation for weeks/months Chronic condition Metabolically stable patients Intravenous supplementation for months/years Reversible or irreversable The anatomical classification was derived from Feldman et al (16), the functional classification was derived from Pironi et al (10). 41
43 Table 2 Prognostic Factors for Short Bowel Syndrome. Factor Favourable Unfavourable Age Young Extremely young or old Systemic disease Not present Present Intrinsic Bowel Disease Not present Present Duodenum Complete Bypassed or (partially) resected Length small bowel > 150 cm < 150 cm Part resected Jejunum Ileum Ileocaecal valve Present Not present Colon Present Not present 42
44 Table 3 Comparison of technique and outcome of SILT, STEP and SILT. LILT STEP SILT Mesenteric handling Significant Minimum Minimum Apply to duodenum No Yes No Bowel length limitation cm Any length Any length Anatomical criteria Double leaflet present, Dilated bowel, also Dilated bowel dilated bowel asymmetrical Surgical complexity Complex Not complex Less complex World wide experience Low High Nihil Risk of necrosis Considerable Low Unknown Lumen Opened Closed Opened Repeatable No Yes Unknown Complications Bleeding, obstruction, leakage, intestinal necrosis, perforation, Bleeding, obstruction, leakage Obstruction, leakage, bleeding, possibly fistula, abscess. fistula, abscess Average lengthening* 48 55% 43 69% - PN independence* 55 71% 48 60% - Estimated survival* 87-95% 77-89% - ITx needed* 10 26% 5-8% - *average rates mentioned are based on recent systematic reviews (41,42,56,58,73). 43
45 Fig. 1. Classification of short bowel syndrome. (Type I) endjejunostomy. (Type II) jejunocolic continuity, no ileocecal valve present. (Type III) jejunoileal anastomosis, ileocecal valve present. (Freely adapted after Feldman, Friedman & Sleisenger (16)) 44
46 Fig. 2. Internal hernia s after Roux-Y gastric bypass. (1) Herniation of the small bowel through the opening in the mesentery of the jejunojejunostomy. (2) Herniation of the small bowel through the opening between the alimentary loop and the mesocolon (Petersen Hernia). (Obtained from Bakker et al. (95)) 45
47 Fig. 3. Bianchi procedure or LILT. (A) separating the two leaves of the mesentery of the isolated small bowel segment. (B) Creating a funnel on the mesenteric site for dividing the small bowel. (C), (D) Separating the small bowel by introducing a surgical stapler. This can also be done by cutting the bowel half. (E) The two bowel loops are then anastomosed together in a isoperistaltic manner. (Obtained from Bianchi A. (35)) 46
48 Fig. 4. Schematic view of STEP. Perpendicular to the longitudinal axis, a stapler line is made preserving a 2 cm luminal diameter. After multiple staples, the bowel is lengthened. (Adapted to Kim et al. (53)) 47
49 Fig. 5. A model of the SILT technique. (A) The bowel is cut spirally in an angle to the longitudinal axis. (B) maintaining orientation by using a silicon catheter, the bowel is stretched. (C) When adjusted to the right length and diameter, the lumen is closed by suturing. (D) The bowel in a longer and narrower shape. (Adapted to Cserni et al. (90)) 48

50




51 AC C EP TE D M AN U SC RI PT

52



53




54
Morabito A UK. -Royal Manchester Children s Hospital (PABRRU) -Intestinal Failure Unit Salford Royal Hospital
 -Intestinal Failure Unit Salford Royal Hospital") NON-TRANSPLANT SURGERY IMPROVES OUTCOME IN SHORT BOWEL PATIENTS Morabito A UK -Royal Manchester Children s Hospital (PABRRU) -Intestinal Failure Unit Salford Royal Hospital antonino.morabito@cmft.nhs.uk
NON-TRANSPLANT SURGERY IMPROVES OUTCOME IN SHORT BOWEL PATIENTS Morabito A UK -Royal Manchester Children s Hospital (PABRRU) -Intestinal Failure Unit Salford Royal Hospital antonino.morabito@cmft.nhs.uk
Gastroschisis Sequelae and Management
 Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
BOWEL LENGTHENING procedures may be beneficial
 Serial Transverse Enteroplasty (STEP): A Novel Bowel Lengthening Procedure By Heung Bae Kim, Dario Fauza, Jennifer Garza, Jung-Tak Oh, Samuel Nurko, and Tom Jaksic Boston, Massachusetts Background/Purpose:
Serial Transverse Enteroplasty (STEP): A Novel Bowel Lengthening Procedure By Heung Bae Kim, Dario Fauza, Jennifer Garza, Jung-Tak Oh, Samuel Nurko, and Tom Jaksic Boston, Massachusetts Background/Purpose:
Commonly Performed Bariatric Procedures in Singapore. Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital
 Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE!
 : A MANAGEMENT CHALLENGE!") SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
Complications after laparoscopic gastric bypass for morbid obesity. Background LGBP. Eirik Hornes Halvorsen, MD, PhD Oslo
 Complications after laparoscopic gastric bypass for morbid obesity Eirik Hornes Halvorsen, MD, PhD Oslo 20.05.2015 Background Ca 3000 patients are surgically treated for morbid obesity in Norway each year.
Complications after laparoscopic gastric bypass for morbid obesity Eirik Hornes Halvorsen, MD, PhD Oslo 20.05.2015 Background Ca 3000 patients are surgically treated for morbid obesity in Norway each year.
Postgastrectomy Syndromes
 Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Intestinal Rehabilitation and Transplantation
 Intestinal Rehabilitation and Transplantation Joel Lim, MD Associate Professor of Pediatrics Children s Mercy Hospital University of Missouri in Kansas City Objective: Intestinal Failure/Short Bowel Syndrome
Intestinal Rehabilitation and Transplantation Joel Lim, MD Associate Professor of Pediatrics Children s Mercy Hospital University of Missouri in Kansas City Objective: Intestinal Failure/Short Bowel Syndrome
Definition and Types of Intestinal Failure
 Definition and Types of Intestinal Failure Jeremy Nightingale Consultant Gastroenterologist St Mark s Hospital Intestinal Failure - Definitions Reduction in functioning gut mass below the minimum amount
Definition and Types of Intestinal Failure Jeremy Nightingale Consultant Gastroenterologist St Mark s Hospital Intestinal Failure - Definitions Reduction in functioning gut mass below the minimum amount
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Long term home parenteral nutrition or small bowel transplantation? Florence LACAILLE Necker-enfants malades, Paris
 Long term home parenteral nutrition or small bowel transplantation? Florence LACAILLE Necker-enfants malades, Paris Intestinal failure : definitive Ultra-short bowel : ± < 30 cm - valve ± < 20 cm + valve
Long term home parenteral nutrition or small bowel transplantation? Florence LACAILLE Necker-enfants malades, Paris Intestinal failure : definitive Ultra-short bowel : ± < 30 cm - valve ± < 20 cm + valve
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS
 Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Improved survival in a multidisciplinary short bowel syndrome program
 Journal of Pediatric Surgery (2008) 43, 20 24 www.elsevier.com/locate/jpedsurg Improved survival in a multidisciplinary short bowel syndrome program Biren P. Modi a,b, Monica Langer a,b, Y. Avery Ching
Journal of Pediatric Surgery (2008) 43, 20 24 www.elsevier.com/locate/jpedsurg Improved survival in a multidisciplinary short bowel syndrome program Biren P. Modi a,b, Monica Langer a,b, Y. Avery Ching
Different Surgical Techniques in Management of Small Intestinal Atresia in High Risk Neonates
 Annals of Pediatric Surgery Vol 5, No 1, January 2009, PP 31-35 Original Article Different Surgical Techniques in Management of Small Intestinal Atresia in High Risk Neonates Almoutaz A. Eltayeb Pediatric
Annals of Pediatric Surgery Vol 5, No 1, January 2009, PP 31-35 Original Article Different Surgical Techniques in Management of Small Intestinal Atresia in High Risk Neonates Almoutaz A. Eltayeb Pediatric
Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help. Print this Page Add to my Bookmarks Page 3 of 10
 Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Imaging findings in complications of bariatric surgery.
 Imaging findings in complications of bariatric surgery. Poster No.: C-1791 Congress: ECR 2012 Type: Educational Exhibit Authors: A. Fernandez Alfonso, G. Anguita Martinez, D. C. Olivares Morello, C. García
Imaging findings in complications of bariatric surgery. Poster No.: C-1791 Congress: ECR 2012 Type: Educational Exhibit Authors: A. Fernandez Alfonso, G. Anguita Martinez, D. C. Olivares Morello, C. García
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications
 A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
LA CHIRURGIA RIABILITATIVA
 LA CHIRURGIA RIABILITATIVA SINDROME DA INTESTINO CORTO: GLI ASPETTI ETICI, L APPROCCIO MEDICO E LE ESIGENZE IN CAMPO NORMATIVO VII CONGRESSO NAZIONALE ASSOCIAZIONE A.N.A.D.P. UN FILO PER LA VITA ONLUS
LA CHIRURGIA RIABILITATIVA SINDROME DA INTESTINO CORTO: GLI ASPETTI ETICI, L APPROCCIO MEDICO E LE ESIGENZE IN CAMPO NORMATIVO VII CONGRESSO NAZIONALE ASSOCIAZIONE A.N.A.D.P. UN FILO PER LA VITA ONLUS
Surgery for Intestinal Failure
 Surgery for Intestinal Failure Kishore Iyer, MBBS, FRCS (Eng), FACS Director, Adult & Pediatric Intestinal Transplantation Associate Professor of Surgery & Pediatrics Mount Sinai School of Medicine New
Surgery for Intestinal Failure Kishore Iyer, MBBS, FRCS (Eng), FACS Director, Adult & Pediatric Intestinal Transplantation Associate Professor of Surgery & Pediatrics Mount Sinai School of Medicine New
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
ESPEN Congress Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION. Loris Pironi
 ESPEN Congress Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi 27 th ESPEN - Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi Chronic Intestinal Failure Centre
ESPEN Congress Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi 27 th ESPEN - Brussels 2005 INDICATIONS FOR INTESTINAL TRANSPLANTATION Loris Pironi Chronic Intestinal Failure Centre
Management of Short Bowel Syndrome in the Era of Teduglutide. Charlene Compher, PhD, RD University of Pennsylvania
 Management of Short Bowel Syndrome in the Era of Teduglutide Charlene Compher, PhD, RD University of Pennsylvania compherc@nursing.upenn.edu Disclosures Research funding for clinical trials by NPS Pharmaceuticals
Management of Short Bowel Syndrome in the Era of Teduglutide Charlene Compher, PhD, RD University of Pennsylvania compherc@nursing.upenn.edu Disclosures Research funding for clinical trials by NPS Pharmaceuticals
ESPEN Congress Geneva 2014 NUTRITION IN PAEDIATRIC PATIENTS 2. Nutrition treatment in children with intestinal failure S.
 ESPEN Congress Geneva 2014 NUTRITION IN PAEDIATRIC PATIENTS 2 Nutrition treatment in children with intestinal failure S. Kolaček (HR) Nutrition treatment in children with intestinal failure - IF special
ESPEN Congress Geneva 2014 NUTRITION IN PAEDIATRIC PATIENTS 2 Nutrition treatment in children with intestinal failure S. Kolaček (HR) Nutrition treatment in children with intestinal failure - IF special
Case Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery.
 Case 14127 Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery. Peters B 1, 2, Waked K 3, Vanhoenacker FM 1, 2, 4, Ceulemans J 5, Mespreuve M 2, 4 University Hospital Antwerp,
Case 14127 Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery. Peters B 1, 2, Waked K 3, Vanhoenacker FM 1, 2, 4, Ceulemans J 5, Mespreuve M 2, 4 University Hospital Antwerp,
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Surgical Management of Short Bowel Syndrome
 529446PENXXX10.1177/0148607114529446Journal of Parenteral and Enteral NutritionIyer research-article2014 Invited Review Surgical Management of Short Bowel Syndrome Kishore R. Iyer, MBBS, FRCS, FACS 1 Journal
529446PENXXX10.1177/0148607114529446Journal of Parenteral and Enteral NutritionIyer research-article2014 Invited Review Surgical Management of Short Bowel Syndrome Kishore R. Iyer, MBBS, FRCS, FACS 1 Journal
Isolated Liver Transplantation in Infants with End-Stage Liver Disease Due to Short Bowel Syndrome
 LIVER TRANSPLANTATION 12:1062-1066, 2006 ORIGINAL ARTICLE Isolated Liver Transplantation in Infants with End-Stage Liver Disease Due to Short Bowel Syndrome Jean F. Botha, Wendy J. Grant, Clarivet Torres,
LIVER TRANSPLANTATION 12:1062-1066, 2006 ORIGINAL ARTICLE Isolated Liver Transplantation in Infants with End-Stage Liver Disease Due to Short Bowel Syndrome Jean F. Botha, Wendy J. Grant, Clarivet Torres,
Nutritional Requirements in Intestinal Failure
 Nutritional Requirements in Intestinal Failure Christopher Duggan, MD, MPH Center for Nutrition Center for Advanced Intestinal Rehabilitation (CAIR) Division of Gastroenterology, Hepatology and Nutrition
Nutritional Requirements in Intestinal Failure Christopher Duggan, MD, MPH Center for Nutrition Center for Advanced Intestinal Rehabilitation (CAIR) Division of Gastroenterology, Hepatology and Nutrition
Overview. Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco
 GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
GASTROINTESTINAL COMPLICATIONS AFTER BARIATRIC SURGERY Stanley J. Rogers, MD, FACS Associate Clinical Professor of Surgery University of California San Francisco UCSF DEPARTMENT OF SURGERY Original Article
Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor
 Sleeve Plus Options Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor Mederi - Speaker Novadaq - Advisory
Sleeve Plus Options Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor Mederi - Speaker Novadaq - Advisory
Reoperation Bariatric Surgery:
 Reoperative Bariatric Surgery, Achieving Insurance Authorization Achieving insurance authorization for reoperative bariatric procedures is not difficult provided that prior insurance company authorization
Reoperative Bariatric Surgery, Achieving Insurance Authorization Achieving insurance authorization for reoperative bariatric procedures is not difficult provided that prior insurance company authorization
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SMALL BOWEL 7-Nov-2016 DEVELOPED BY: Graham Cullingford,
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: SMALL BOWEL 7-Nov-2016 DEVELOPED BY: Graham Cullingford,
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
Here are some types of gastric bypass surgery:
 Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Corporate Medical Policy
 Corporate Medical Policy Small Bowel, Small Bowel with Liver, or Multivisceral Transplant File Name: Origination: Last CAP Review: Next CAP Last Review: small_bowel_liver_and_multivisceral_transplant 2/1996
Corporate Medical Policy Small Bowel, Small Bowel with Liver, or Multivisceral Transplant File Name: Origination: Last CAP Review: Next CAP Last Review: small_bowel_liver_and_multivisceral_transplant 2/1996
COLLECTIVE REVIEW. Current Surgical Options in Short Bowel Syndrome. PattamapondLimpanopas MD. Assoc.Prof.Dr. SurasakSangkhathat(Supervisor)
") COLLECTIVE REVIEW Current Surgical Options in Short Bowel Syndrome PattamapondLimpanopas MD. Assoc.Prof.Dr. SurasakSangkhathat(Supervisor) Current surgical options in Short Bowel Syndrome Definition Intestinal
COLLECTIVE REVIEW Current Surgical Options in Short Bowel Syndrome PattamapondLimpanopas MD. Assoc.Prof.Dr. SurasakSangkhathat(Supervisor) Current surgical options in Short Bowel Syndrome Definition Intestinal
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
ESPEN Congress Florence 2008
 ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in gastroenterology A. van Gossum (Belgium) ESPEN-Parenteral Guidelines in Gastroenterology André Van Gossum, Eduard Cabre, Xavier
ESPEN Congress Florence 2008 PN Guidelines presentation PN Guidelines in gastroenterology A. van Gossum (Belgium) ESPEN-Parenteral Guidelines in Gastroenterology André Van Gossum, Eduard Cabre, Xavier
Not over when the surgery is done: surgical complications of obesity
 Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
Not over when the surgery is done: surgical complications of obesity Gianluca Bonanomi, MD, FRCS Consultant Surgeon and Honorary Senior Lecturer Chelsea and Westminster Hospital London The Society for
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA)
") STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
STRATEGIES TO IMPROVE ENTERAL FEEDING TOLERANCE. IS IT WORTH IT? ENGELA FRANCIS RD(SA) DEFINITION OF ENTERAL FEEDING INTOLERANCE Gastrointestinal feeding intolerance are usually defined as: High gastric
Adipocytes, Obesity, Bariatric Surgery and its Complications
 Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
RECTAL PROLAPSE objectives
 RECTAL PROLAPSE objectives 1.Classify rectal prolapse 2. Enumerate the causes of rectal prolapse 3. Differentiate between complete rectal prolapse and intussusception 4. List the modalities of treatment
RECTAL PROLAPSE objectives 1.Classify rectal prolapse 2. Enumerate the causes of rectal prolapse 3. Differentiate between complete rectal prolapse and intussusception 4. List the modalities of treatment
ADVANCE AT YOUR OWN PACE
 ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
Serial Transverse Enteroplasty Enhances Intestinal Function in a Model of Short Bowel Syndrome
 ORIGINAL ARTICLES Serial Transverse Enteroplasty Enhances Intestinal Function in a Model of Short Bowel Syndrome Robert W. Chang, MD, Patrick J. Javid, MD, Jung-Tak Oh, MD, Steven Andreoli, BA, Heung Bae
ORIGINAL ARTICLES Serial Transverse Enteroplasty Enhances Intestinal Function in a Model of Short Bowel Syndrome Robert W. Chang, MD, Patrick J. Javid, MD, Jung-Tak Oh, MD, Steven Andreoli, BA, Heung Bae
Antecolic versus retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass: a comparative study
 Surgery for Obesity and Related Diseases 3 (2007) 423 427 Original article Antecolic versus retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass: a comparative study Alex Escalona, M.D.
Surgery for Obesity and Related Diseases 3 (2007) 423 427 Original article Antecolic versus retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass: a comparative study Alex Escalona, M.D.
7th International Congress of the Spanish Society of Obesity Surgery. Valladolid Spain May, 2004.
 7th International Congress of the Spanish Society of Obesity Surgery. Valladolid Spain May, 2004. DIMINISHING POSTOPERATIVE RISKS OF GASTRIC BYPASS Stenosis Stenosis Leak Leak Bleeding Bleeding Stenosis
7th International Congress of the Spanish Society of Obesity Surgery. Valladolid Spain May, 2004. DIMINISHING POSTOPERATIVE RISKS OF GASTRIC BYPASS Stenosis Stenosis Leak Leak Bleeding Bleeding Stenosis
The Physician as Medical Illustrator
 The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19
 in Adult Patients Topic 19") Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and Outcome Learning Objectives André Van Gossum Head of the Clinic of Intestinal
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and Outcome Learning Objectives André Van Gossum Head of the Clinic of Intestinal
Policy Specific Section: April 14, 1970 June 28, 2013
 Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
Gastric bypass vs. Sleeve gastrectomy
 Gastric bypass vs. Sleeve gastrectomy SLEEVEPASS-study Sleeve gastrectomy Paulina Salminen, M.D., PhD Turku University Hospital Department of Surgery Stockholms Obesitasdagar 19.4.2012 Swedish Obese Subjects
Gastric bypass vs. Sleeve gastrectomy SLEEVEPASS-study Sleeve gastrectomy Paulina Salminen, M.D., PhD Turku University Hospital Department of Surgery Stockholms Obesitasdagar 19.4.2012 Swedish Obese Subjects
Internal hernias after laparoscopic Roux-en-Y gastric bypass
 The American Journal of Surgery 188 (2004) 796 800 Scientific paper Internal hernias after laparoscopic Roux-en-Y gastric bypass Ernesto Garza, Jr., M.D., Joseph Kuhn, M.D., David Arnold, M.D., William
The American Journal of Surgery 188 (2004) 796 800 Scientific paper Internal hernias after laparoscopic Roux-en-Y gastric bypass Ernesto Garza, Jr., M.D., Joseph Kuhn, M.D., David Arnold, M.D., William
RADIATION INDUCED SMALL BOWEL DISEASE. Dr Mnguni Supervisor: Dr Lohlun Radiation Oncology
 RADIATION INDUCED SMALL BOWEL DISEASE Dr Mnguni Supervisor: Dr Lohlun Radiation Oncology INTRODUCTION Radiation therapy is not regularly indicated in the treatment of small bowel disease. Reasons are complex
RADIATION INDUCED SMALL BOWEL DISEASE Dr Mnguni Supervisor: Dr Lohlun Radiation Oncology INTRODUCTION Radiation therapy is not regularly indicated in the treatment of small bowel disease. Reasons are complex
SWISS SOCIETY OF NEONATOLOGY. Spontaneous intestinal perforation or necrotizing enterocolitis?
 SWISS SOCIETY OF NEONATOLOGY Spontaneous intestinal perforation or necrotizing enterocolitis? June 2004 2 Stocker M, Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital of Lucerne,
SWISS SOCIETY OF NEONATOLOGY Spontaneous intestinal perforation or necrotizing enterocolitis? June 2004 2 Stocker M, Berger TM, Neonatal and Pediatric Intensive Care Unit, Children s Hospital of Lucerne,
The Surgical Management of Obesity
 The Surgical Management of Obesity Omar al noubani MD,MRCS وك ل وا و اش ز ب وا و ال ت س رف وا األعراف ما مأل ابن آدم وعاء شر ا من بطنه Persons who are naturally fat are apt to die earlier than those who
The Surgical Management of Obesity Omar al noubani MD,MRCS وك ل وا و اش ز ب وا و ال ت س رف وا األعراف ما مأل ابن آدم وعاء شر ا من بطنه Persons who are naturally fat are apt to die earlier than those who
SOUTHERN WEST MIDLANDS NEWBORN NETWORK
 SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Title : Person Responsible for Review : Management of Gastro-Intestinal Stomata In Neonates R. Wragg & G.Jawaheer
SOUTHERN WEST MIDLANDS NEWBORN NETWORK Hereford, Worcester, Birmingham, Sandwell & Solihull Title : Person Responsible for Review : Management of Gastro-Intestinal Stomata In Neonates R. Wragg & G.Jawaheer
Case Whirlpool sign in midgut volvulus
 Case 11454 Whirlpool sign in midgut volvulus Emad El-din Althamer 1, Shagufta Jabeen 2, Nada Al-Assaf 1, Akram Jawad 1, Muhammad Hassan 1, Muhammad Fatani 1, Rumayan Al-Rumyan 1, A Aziz Mosabihi 1, Ahmeduddin
Case 11454 Whirlpool sign in midgut volvulus Emad El-din Althamer 1, Shagufta Jabeen 2, Nada Al-Assaf 1, Akram Jawad 1, Muhammad Hassan 1, Muhammad Fatani 1, Rumayan Al-Rumyan 1, A Aziz Mosabihi 1, Ahmeduddin
University of Groningen. Colorectal Anastomoses Bakker, Ilsalien
 University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
ANZMOSS 2018 Melbourne Bariatric Surgery Masterclass
 ANZMOSS 2018 Melbourne Bariatric Surgery Masterclass WHICH OPERATION TO CHOOSE ANTHONY CLOUGH The options SURGICAL OPTIONS? - A MINEFIELD An explosion of operative variants Local technical variations Local
ANZMOSS 2018 Melbourne Bariatric Surgery Masterclass WHICH OPERATION TO CHOOSE ANTHONY CLOUGH The options SURGICAL OPTIONS? - A MINEFIELD An explosion of operative variants Local technical variations Local
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Topics for discussion. Pediatric General Surgery. Physiology. Surgical Newborns. Neonatal Intestinal Obstruction
 Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Topics for discussion Pediatric General Surgery Professor General & Thoracic Surgery What makes Pediatric Surgery unique? Neonatal intestinal obstruction Abdominal wall defects Inguinal hernias Appendicitis
Isolated Small Bowel Transplant. Populations Interventions Comparators Outcomes Individuals: With intestinal failure
 Protocol Isolated Small Bowel Transplant (70304) Medical Benefit Effective Date: 01/01/15 Next Review Date: 03/19 Preauthorization Yes Review Dates: 01/10, 01/11, 01/12, 01/13, 01/14, 11/14, 11/15, 11/16,
Protocol Isolated Small Bowel Transplant (70304) Medical Benefit Effective Date: 01/01/15 Next Review Date: 03/19 Preauthorization Yes Review Dates: 01/10, 01/11, 01/12, 01/13, 01/14, 11/14, 11/15, 11/16,
Fistuloclysis (distal limb feeding) Dr Alison Culkin Research Dietitian AuSPEN 2015
 Dr Alison Culkin Research Dietitian AuSPEN 2015") Fistuloclysis (distal limb feeding) Dr Alison Culkin Research Dietitian AuSPEN 2015 Overview Consider the evidence Describe the practicalities Present some cases Fistuloclysis/distal limb feeding Infusion
Fistuloclysis (distal limb feeding) Dr Alison Culkin Research Dietitian AuSPEN 2015 Overview Consider the evidence Describe the practicalities Present some cases Fistuloclysis/distal limb feeding Infusion
SURGICAL MANAGEMENT OF MORBID OBESITY
 Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
AN EXPERIMENTAL TUBE PEDICLE LINED WITH SMALL BOWEL. By J. H. GOLDIN, F.R.C.S.(Edin.) Plastic Surgery Unit, St Thomas' Hospital, London
 Plastic Surgery Unit, St Thomas' Hospital, London") British Journal of Plastic Surgery (I972), 25, 388-39z AN EXPERIMENTAL TUBE PEDICLE LINED WITH SMALL BOWEL By J. H. GOLDIN, F.R.C.S.(Edin.) Plastic Surgery Unit, St Thomas' Hospital, London ONE of the
British Journal of Plastic Surgery (I972), 25, 388-39z AN EXPERIMENTAL TUBE PEDICLE LINED WITH SMALL BOWEL By J. H. GOLDIN, F.R.C.S.(Edin.) Plastic Surgery Unit, St Thomas' Hospital, London ONE of the
Endoscopic management of sleeve leaks
 Endoscopic management of sleeve leaks Mr Damien Loh Oesophagogastric and Bariatric Surgeon The Alfred The clinical problem Incidence 0.1-7% Inpatient mortality 2-5% High morbidity Prolonged ICU and in-hospital
Endoscopic management of sleeve leaks Mr Damien Loh Oesophagogastric and Bariatric Surgeon The Alfred The clinical problem Incidence 0.1-7% Inpatient mortality 2-5% High morbidity Prolonged ICU and in-hospital
Hirschprung s. Meconium plug R/S >1 R/S <1
 NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
NEONATAL ABDOMINAL EMERGENCIES LOW OBSTRUCTION HIGH OBSTRUCTION INTESTINAL OBSTRUCTION High obstruction - proximal to mid-ileumileum Few dilated, air filled bowel loops Complete obstruction diagnosed by
The Bariatric and Heartburn Center of Northeast Ohio
 The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
Information for patients (and their families) waiting for liver transplantation
 waiting for liver transplantation") Information for patients (and their families) waiting for liver transplantation Waiting list? What is liver transplant? Postoperative conditions? Ver.: 5/2017 1 What is a liver transplant? Liver transplantation
Information for patients (and their families) waiting for liver transplantation Waiting list? What is liver transplant? Postoperative conditions? Ver.: 5/2017 1 What is a liver transplant? Liver transplantation
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Small bowel atresia. Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families
 Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Benefits of Bariatric Surgery
 Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Benefits of Bariatric Surgery Dr Tan Bo Chuan Registrar, Department of Surgery GP Forum 27 May 2017 Improvements of Co-morbidities Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint
Managing obesity and the gastric bypass: understanding anatomy and major postoperative complications
 Managing obesity and the gastric bypass: understanding anatomy and major postoperative complications Poster No.: C-1323 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Tincey, A. N. Tavare, A.
Managing obesity and the gastric bypass: understanding anatomy and major postoperative complications Poster No.: C-1323 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Tincey, A. N. Tavare, A.
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Title: Aerophagia due to abdomino-phrenic dyssynergia in a 2-year-old child. Authors: Pablo Ercoli, Belinda García, Enrique del Campo, Sergio Pinillos
 Title: Aerophagia due to abdomino-phrenic dyssynergia in a 2-year-old child Authors: Pablo Ercoli, Belinda García, Enrique del Campo, Sergio Pinillos DOI: 10.17235/reed.2018.5444/2017 Link: PubMed (Epub
Title: Aerophagia due to abdomino-phrenic dyssynergia in a 2-year-old child Authors: Pablo Ercoli, Belinda García, Enrique del Campo, Sergio Pinillos DOI: 10.17235/reed.2018.5444/2017 Link: PubMed (Epub
Case Report The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in a Newborn
 Case Reports in Pediatrics Volume 2015, Article ID 129098, 4 pages http://dx.doi.org/10.1155/2015/129098 Case Report The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in a Newborn
Case Reports in Pediatrics Volume 2015, Article ID 129098, 4 pages http://dx.doi.org/10.1155/2015/129098 Case Report The Combination of Gastroschisis, Jejunal Atresia, and Colonic Atresia in a Newborn
Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant
 Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant 2 Indication for intravenous nutrition/pn: Intestinal Failure Inability to maintain weight and growth despite adequate enteral
Advances in intestinal Rehabilitation Susan Hill Gastroenterology Consultant 2 Indication for intravenous nutrition/pn: Intestinal Failure Inability to maintain weight and growth despite adequate enteral
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
JAWDA Bariatric Quality Performance Indicators. JAWDA Quarterly Guidelines for Bariatric Surgery (BS)
") JAWDA Guidelines for Bariatric Surgery (BS) January 2019 1 Table of Contents Executive Summary... 3 About this Guidance... 4 Bariatric Surgery Indicators... 5 Appendix A: Glossary... 19 Appendix B: Approved
JAWDA Guidelines for Bariatric Surgery (BS) January 2019 1 Table of Contents Executive Summary... 3 About this Guidance... 4 Bariatric Surgery Indicators... 5 Appendix A: Glossary... 19 Appendix B: Approved
Obesity Management Workshop for Health Professionals
 Obesity Management Workshop for Health Professionals 17 th November 2017 Dr Graeme Rich Gastroenterologist Director of Bariatrics Australia Is a procedure the magic bullet? Energy in >> Energy out Accepted
Obesity Management Workshop for Health Professionals 17 th November 2017 Dr Graeme Rich Gastroenterologist Director of Bariatrics Australia Is a procedure the magic bullet? Energy in >> Energy out Accepted
Accepted Manuscript. External iliac artery injury secondary to indirect pressure wave effect from gun shot wound. Eugene Ng, Andrew MTL.
 Accepted Manuscript External iliac artery injury secondary to indirect pressure wave effect from gun shot wound Eugene Ng, Andrew MTL. Choong PII: S1008-1275(16)00034-1 DOI: 10.1016/j.cjtee.2016.01.013
Accepted Manuscript External iliac artery injury secondary to indirect pressure wave effect from gun shot wound Eugene Ng, Andrew MTL. Choong PII: S1008-1275(16)00034-1 DOI: 10.1016/j.cjtee.2016.01.013
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers
 WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
WHEN To Initiate Parenteral Nutrition A Frequent Question With New Answers Ainsley Malone, MS, RD, LD, CNSC, FAND, FASPEN Dubai International Nutrition Conference 2018 Disclosures No commercial relationship
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Single Stage Transanal Pull-Through for Hirschsprung s Disease in Neonates: Our Early Experience
 Journal of Neonatal Surgery 2013;2(4):39 ORIGINAL ARTICLE Single Stage Transanal Pull-Through for Hirschsprung s Disease in Neonates: Our Early Experience Pradeep Bhatia,* Rakesh S Joshi, Jaishri Ramji,
Journal of Neonatal Surgery 2013;2(4):39 ORIGINAL ARTICLE Single Stage Transanal Pull-Through for Hirschsprung s Disease in Neonates: Our Early Experience Pradeep Bhatia,* Rakesh S Joshi, Jaishri Ramji,
Isolated Small Bowel Transplant
 Medical Policy Manual Transplant, Policy No. 09 Isolated Small Bowel Transplant Next Review: January 2019 Last Review: January 2018 Effective: March 1, 2018 IMPORTANT REMINDER Medical Policies are developed
Medical Policy Manual Transplant, Policy No. 09 Isolated Small Bowel Transplant Next Review: January 2019 Last Review: January 2018 Effective: March 1, 2018 IMPORTANT REMINDER Medical Policies are developed
Short Bowel Syndrome: Medical management
 Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: January 15, 2018 Related Policies: 7.03.05 Small Bowel/Liver and Multivisceral Transplant Isolated Small Bowel Transplant Description A small bowel transplant
FEP Medical Policy Manual Effective Date: January 15, 2018 Related Policies: 7.03.05 Small Bowel/Liver and Multivisceral Transplant Isolated Small Bowel Transplant Description A small bowel transplant
Nutrition Management in GI Diseases
 Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19
 in Adult Patients Topic 19") Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and outcome André Van Gossum Learning objectives: Learning about indications
Nutritional Support outside the Hospital: Home Parenteral Nutrition (HPN) in Adult Patients Topic 19 Module 19.1 Indications and outcome André Van Gossum Learning objectives: Learning about indications
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Managing Complications of Bariatric Surgery. Objectives
 Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
Managing Complications of Bariatric Surgery John J. Vargo, II, MD, MPH, FACG Chair, Department of Gastroenterology and Hepatology Digestive Disease and Surgery Institute Cleveland Clinic Cleveland, OH
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Bariatric Surgery MM /11/2001. HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient; Inpatient
 of Service: Outpatient; Inpatient") Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Effect of changing lipid formulation in Parenteral Nutrition in the Newborn Experimental Pathology BSc
 Effect of changing lipid formulation in Parenteral Nutrition in the Newborn Experimental Pathology BSc Word count: 6939 0 CONTENTS Abstract...2 Acknowledgements...3 Introduction...4 Materials and Methods...11
Effect of changing lipid formulation in Parenteral Nutrition in the Newborn Experimental Pathology BSc Word count: 6939 0 CONTENTS Abstract...2 Acknowledgements...3 Introduction...4 Materials and Methods...11
The jury is still out: changes in gastroschisis management over the last decade are associated with both benefits and shortcomings
 Journal of Pediatric Surgery (2012) 47, 119 124 www.elsevier.com/locate/jpedsurg The jury is still out: changes in gastroschisis management over the last decade are associated with both benefits and shortcomings
Journal of Pediatric Surgery (2012) 47, 119 124 www.elsevier.com/locate/jpedsurg The jury is still out: changes in gastroschisis management over the last decade are associated with both benefits and shortcomings
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Surgery Type of Article: Case Report Title:
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Removal of a lap band and revision to an alternative bariatric procedure in one procedure.
 How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization