Update on Osteoporosis 2016
|
|
|
- Mary Flynn
- 5 years ago
- Views:
Transcription
1 WELCOME!
2 Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical Densitometry Unit Joslin Diabetes Center Syracuse NY

3
4

5

6
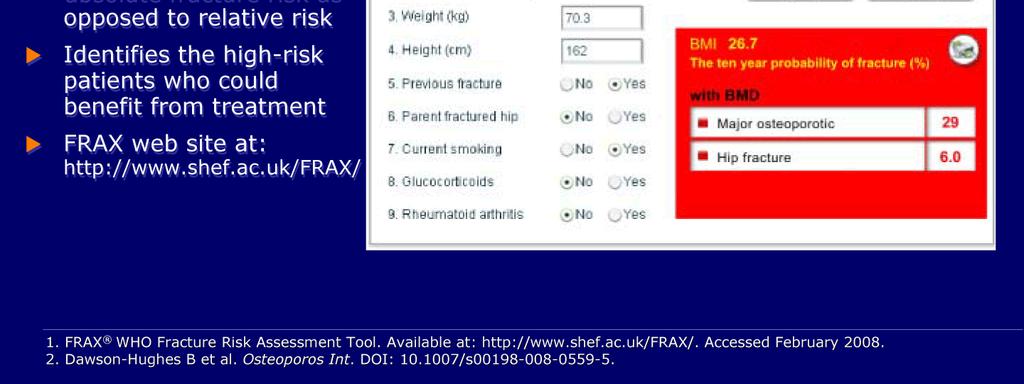
7 Issues with FRAX Only hip BMD in calculations (no spine) FRAX does not take into account other factors (falls) Doses not considered (steroids, # of cigarettes or fractures) Patient treatment decisions should be a judgment FRAX cannot be used for patients already on treatment


8

9 Fewer Than 35% of Hip Fracture Patients Received Pharmacologic Treatment Within 6 Months


10 Vertebral Fracture Assessment

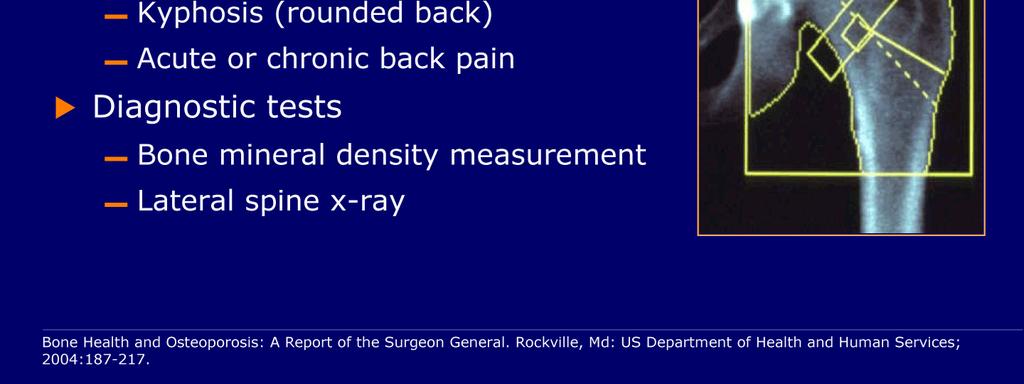
11 Assessment using a DXA System Identify many (~30%) of missed patients based on BMD alone Improve targeting of therapy and patient understanding Improve acceptance and compliance Reduce osteoporotic fractures Steroid use is an ISCD reason for ordering test

12 TBS Trabecular Bone Score
13 Tests to evaluate for secondary causes of Osteoporosis CMP, phosphorus, PTH, 25OH D level. Testosterone in men. 24 hour urine collection for calcium and creatinine. Depending upon the patient, may consider other tests such as screening for Cushings, SPEP. Consider bone turnover markers (P1NP, CTX)
14 Case #1 50 year old woman has a baseline DXA after menopause. No family history of osteoporosis. She is healthy, takes no medications. Her lumbar spine T-score is -2.0, total hip -1.6, femoral neck Should she be treated?
15 Osteopenia, when to treat? Need to assess all risk factors (with FRAX or on own). If a person has had a non-traumatic fracture, they have osteoporosis regardless of their T- score and are at high risk for future fracture. Weigh and discuss with patient risks and benefits of treating vs. not treating.
16 Osteopenia T-score closer to -2.5, may warrant treatment more so than one closer to -1. For instance in a patient with diabetes or RA, may be more likely to treat with osteopenia. Can use osteopenic doses of bisphosphonates.
17 When to treat Osteopenia? In this patient, could emphasize calcium and vitamin D intake, weight bearing exercise, don t smoke, limit alcohol. If she had other risk factors, could consider risks and benefits.
18 New diagnosis of Osteoporosis Case #2 60 year old woman (or man) has a routine DXA. T-score of the lumbar spine -2.6, hip -2.3, femoral neck No other family history, associated meds or risk factors. Should she be treated, and if so with which med?
19 Treatments for Osteoporosis: Bisphosphonates Anti-resorptive medications. Alendronate (Fosamax), risedronate (Actonel) and ibandronate (Boniva). Main concern for side effects related to local GI irritation at the esophagus. Need to take correctly. IV Ibandronate is available every 3 months, IV Zoledronate is available as a once a year infusion (can have acute phase reaction symptoms).
20 Zoledronic Acid (Reclast) Approved to be given yearly for PMO in women, glucocorticoid induced osteoporosis and in men. Given every 2 years for osteopenia. Covered under Medicare part B rather than part D as it is given in an office (does not have an impact on donut hole).
21 Treatments for osteoporosis: SERMs Selective Estrogen Receptor Modulators are approved for use in postmenopausal women. Protects against breast cancer. Raloxifene (Evista) 60 mg oral daily, side effects can include hot flashes and increased risk of DVT. Two other SERMs (basedoxifene and lasofoxifene) are currently under clinical development.
22 Denosumab (Prolia) RANKL inhibitor, anti-resorptive. Given SQ 60 mg every 6 months in office. FDA approved in 2010 but Amgen has 10 years of data. DXAs improve well, generally well tolerated. Can be given at lower GFR (make sure no renal osteodystrophy present first if GFR<30)-may need metabolic bone biopsy. Side effects: skin rashes (seen first 3 yrs of study, not seen in later years), ONJ possible.
23 Treatments for osteoporosis: Calcitonin A 32 amino acid peptide secreted by the C-cells in the thyroid, it inhibits osteoclast resorption. A nasal preparation, salmon calcitonin (Miacalcin) is approved for use in osteoporosis, given 200 IU daily in alternating nostrils. Recently recommended by FDA to no longer be used.
24 Treatments for osteoporosis: Teriparatide The only current FDA approved anabolic agent for osteoporosis, it is a PTH analog. Reserved for patients at high risk of fracture or who could not tolerate or have failed other therapies. Given as a daily SC injection for up to 2 years. Side effects may include dizziness, palpitations, transient hypercalcemia. Black box warning on osteosarcoma in rats. JBMR article in 2013 revealed 10 year safety data.
25 Which med to choose? Most patients do well with oral bisphosphonates, may need to try generic choice first by insurance. If the patient cannot tolerate orals, could try an injectable (or if failed orals previously) If initial T-score quite low (-3), teriparatide may be a good choice. Comes down to patient preference, insurance and any other contraindications, T-score.
26 Questions we ask ourselves before starting an osteoporosis medication? How long do I plan to treat? Do I want to choose something else down the road?
27 Examples: If Teriparatide first, obviously something later. Bisphosphonate may provide chance for a later drug holiday. Denosumab (potent antiresorptive) not amenable to a drug holiday. Can pick Raloxifene in the appropriate pts. Other choices likely in future in pipelines.
28 Treatment Questions? Denosumab works well, how long to give? We really cannot utilize a drug holiday with Denosumab. Future options??

29 Longevity of effect
30 How Long to Treat with Denosumab? This topic was addressed in recent article: How Long to Treat with Denosumab Costa AG, Bilezikian JP Curr Osteoporos Rep Dec 13(6) PMID
31 Use of Denosumab One of the most vexing questions facing a clinician today is how long to treat, which may seem odd for a chronic disease such as osteoporosis, considering most other chronic diseases, including heart disease, diabetes, hypertension and hyperlipidemia, have no limits with regard to duration of therapy.
32 Denosumab Effect Powerful, rapid effect. Good safety profile. Rare ONJ, AFF At discontinuation, rapid increase in BTMs, declines in BMD (5-6%) in 12 months. BTMs and BMDs returned near baseline after 24 months off treatment. Effect reversible, no immediate fracture risk increase, responsiveness demonstrated by retreatment.
33 How long to treat? Rapid reversibility raises concerns. High risk patients might warrant longer-term use. Concern over AFF/ONJ: small increment at nadir of BTM is short and does not persist the whole 6 months. Increase at end, is greater/earlier. At this point, more in favor of continuing long term therapy with Denosumab than bisphosphonates. Need more long term data.
34 Case #3 62 year old woman, on Fosamax for 6 years. She takes it correctly and tolerates it well. Never had a fracture, recent DXA shows T-score of the lumbar spine -2.3, total hip -2.2, femoral neck Could a drug holiday be considered? What if she had a T-score currently of -3 or had previous fractures (or on steroids, etc.) Would that change opinion?
35 Drug Holidays Bisphosphonates have a long retention time in bone. After a bone loading period, it appears the amount of bisphosphonate released back into the circulation can maintain BMD and BTM for a period of time, possibly years. There has been a wider discussion evolving concerning a drug holiday in postmenopausal women after 5-7 years of med use. There is no standard of care on this, but numerous opinions.
36 Drug holidays New Task force paper published in JBMR January 2016 issue. Main data for alendronate up to 10 years (FIT/FLEX study) Main data for zoledronate up to 6 years (HORIZON extension study)

37 Drug holiday? That meant something different in the 1960 s.
38 Drug Holidays Hence, if a drug holiday is considered in low risk person, a minimum duration of 5 years of alendronate use seems reasonable or 3 years of zolendronic acid. Drug holidays not feasible for teriparatide or denosumab as drug effect wears off. T-scores, any previous fractures, high risk medication use, other risk factors should be considered in determining a drug holiday. Could test DXA and/or BTMs one year later to see if stable.
39 Length of treatment There is no expiration date as to when to stop therapy. Need to reassess periodically if still indicated Some patients on therapy over 10 years but if they are high risk for fracture, the benefit outweighs rare risks. Need to individualize.
40 Things people like to ask about Alkaline diet More exercise, other modalities Strontium Other vitamins
41 Strontium Approved for use in many European countries. Ranelate used elsewhere, nutrition shops here have citrate Cannot promise same efficacy/safety CV concerns in Europe with med use.

42 Approved Strontium

43 Strontium ranelate promotes bone formation by osteoblasts, inhibit bone resorption by osteoclast and leads to incorporation of Sr into mineralized matrix formed during treatment
44 Another type of patient Patient on Fosamax 5 years and has decreased T-score (5%) at any site, and/or fracture. Is this a failure? Should a different medication be selected and if so which one?
45 Questionable med failure First assess if they actually were taking the medication and taking it correctly. Look for underlying secondary causes (low Vitamin D, etc) Could consider an injectable (Reclast, Prolia or Forteo) Again need to assess all individual aspects of patient (if concern for oversuppression, an anabolic choice may be better).
46 Long term therapy Experts in the field agree that risk of osteoporotic fracture much higher than rare potential side effects. Can leave patients on long term bisphosphonates if indicated (10 years). Atypical femoral fractures may be another variant of an osteoporotic fracture. ONJ extremely rare, encourage regular dental exams, can hold med if oral surgery to be done. Important to reassess therapy periodically to see if warranted to continue.
47 Combination Therapy Data does not suggest benefit to adding teriparatide to bisphosphonates (perhaps after several months, anabolic window). Some data on small study combining teriparatide to raloxifene Newer data on denosumab and teriparatide shows potential benefit. Concern for decreased bone turnover with 2 anti-resorptives given together (incl. HRT)
48 Take home points Osteoporosis is very common and fractures can be devastating. Most therapies are safe and effective, ask about dental issues, thigh or hip pain at visits. Patients on bisphosphonates over 3-5 years, reassess periodically to see if a drug holiday or change in therapy is appropriate. Treat patients after non traumatic hip fractures. Denosumab (Prolia) good alternative to bisphosphonates, teriparatide (Forteo) to be considered as anabolic therapy. Always ask if patients actually taking meds (correctly) along with calcium and vitamin D.
49 New Medications on the Horizon Sclerostin inhibitor (Romosozumab) monoclonal Ab against Sclerostin (produced by osteocytes & inhibits bone formation). Abaloparatide (is a peptide that selectively binds to the RG conformation of the parathyroid hormone type 1 receptor)

50
51 Crisis in the Treatment of Osteoporosis June 2016 JBMR month in JBMR) We as a physicians who care deeply about the treatment of patients with osteoporosis, find ourselves in a dire situation. Tools to prevent sufferings and mortality, but for osteoporosis we may well be coming back full circle: the downward spiral of vertebral fracture, hip fracture, immobility, loss of independence, and premature death that we thought we had conquered may soon become the accepted norm again.
52 New York Times June 1, 2016 Fearing Drugs Rare Side Effects, Millions Take Their Chances With Osteoporosis


53 It s erroneous to think it s a lady s disease.
54 Conclusion I would like to end with an excerpt from an editorial: Increasing Options for the Treatment of Osteoporosis Sundeep Khosla, MD N Engl J Med 2009; 361:
55 Khosla NEJM 2009 Beyond the science driving new drug development, however, will remain the art of being a physician. Specifically, our success or failure in combating osteoporosis increasingly depends not so much on the drugs available to us but rather on our ability to engage our patients and ensure that they take the medications we prescribe.
56 Thank you!! Questions??
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Osteoporosis - New Guidelines. Michelle Glass B.Sc. (Pharm) June 15, 2011
 June 15, 2011") Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis - New Guidelines Michelle Glass B.Sc. (Pharm) June 15, 2011 Outline What is Osteoporosis? Who is at risk? What treatments are available? Role of the Pharmacy technician Definition of Osteoporosis
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi Watts NB et
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Monitoring Osteoporosis Therapy
 Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Monitoring Osteoporosis Therapy SUZANNE MORIN DEPT OF MEDICINE, DIVISION OF GENERAL INTERNAL MEDICINE, MUHC CENTRE FOR OUTCOMES RESEARCH AND EVALUATION, RI MUHC November 2017 Conflict of Interest Disclosures
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Osteoporosis and Lupus. Andrew Ruthberg, MD University Rheumatologists
 Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Osteoporosis Medications: A Case-Based Discussion. Laila S. Tabatabai, MD August 5, 2017
 Osteoporosis Medications: A Case-Based Discussion Laila S. Tabatabai, MD August 5, 2017 Disclosures Eli Lilly Radius Objectives Determine which patients with low bone density require treatment, along with
Osteoporosis Medications: A Case-Based Discussion Laila S. Tabatabai, MD August 5, 2017 Disclosures Eli Lilly Radius Objectives Determine which patients with low bone density require treatment, along with
SpongeBone Menopants*
 SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
SpongeBone Menopants* Adam Fershko, MD, FACP Kettering Health Network *Postmenopausal Osteoporosis Objectives O Epidemiology O Clinical significance O Pathophysiology O Screening and Diagnosis O Treatment
An Update on Osteoporosis Treatments
 An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
An Update on Osteoporosis Treatments Dr Mike Stone University Hospital Llandough Treatments for osteoporosis Calcium and vitamin D HRT Raloxifene Etidronate Alendronate Risedronate Ibandronate (oral and
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Updates in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
OSTEOPOROSIS MEDICINES
 Bone Basics 2010. NOF. All rights reserved. National Osteoporosis Foundation 1150 17th Street, NW, Suite 850 Washington, DC 20036 (800) 223-9994 www.nof.org OSTEOPOROSIS MEDICINES Although there is no
Bone Basics 2010. NOF. All rights reserved. National Osteoporosis Foundation 1150 17th Street, NW, Suite 850 Washington, DC 20036 (800) 223-9994 www.nof.org OSTEOPOROSIS MEDICINES Although there is no
Osteoporosis for the PCP and consultant COPYRIGHT. Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center
 Osteoporosis for the PCP and consultant Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center Beth Israel Deaconess Medical Center Potential conflicts of interest None GOALS When to screen/treat?
Osteoporosis for the PCP and consultant Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center Beth Israel Deaconess Medical Center Potential conflicts of interest None GOALS When to screen/treat?
Osteoporosis. Treatment of a Silently Developing Disease
 Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis Treatment of a Silently Developing Disease Marc K. Drezner, MD Senior Associate Dean Emeritus Professor of Medicine Emeritus University of Wisconsin-Madison Auditorium The Forest at Duke October
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Osteoporosis Update: Keys to Improving Diagnosis and Preventing Fractures
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/spotlight-on/osteoporosis-update-keys-improving-diagnosis-preventingfractures/9812/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/spotlight-on/osteoporosis-update-keys-improving-diagnosis-preventingfractures/9812/
Guideline for the investigation and management of osteoporosis. for hospitals and General Practice
 Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Guideline for the investigation and management of osteoporosis for hospitals and General Practice Background Low bone density is an important risk factor for fracture. The aim of assessing bone density
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT
 AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Bisphosphonates. Making intelligent drug choices
 Making intelligent drug choices Bisphosphonates are a first choice for treating osteoporosis, according to Kedrin E. Van Steenwyk, DO, an obstetrician/gynecologist at Sycamore Women s Center, Miamisburg,
Making intelligent drug choices Bisphosphonates are a first choice for treating osteoporosis, according to Kedrin E. Van Steenwyk, DO, an obstetrician/gynecologist at Sycamore Women s Center, Miamisburg,
Page 1. Current and Emerging Strategies What s New in Osteoporosis. Osteoporosis. What is Osteoporosis? Traditional Risk Factors for Fracture
 Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis What s New in Osteoporosis Risk stratification Douglas C. Bauer, MD University of California, San Francisco Under recognition and poor compliance New potential
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE. Nelson B. Watts, MD
 TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO Honoraria: Amgen, Radius, Shire Consulting
TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO Honoraria: Amgen, Radius, Shire Consulting
Cortical bone After age 40, gradually decreases % yearly, in both men and women Postmenopausally, loss accelerates to 2-3% yearly
 Osteoporosis POOLE, K.E.S. & COMPSTON, J.E. (2006): Osteoporosis and its management. BMJ 333:1251-6. Physiology Cortical bone After age 40, gradually decreases 0.3-0.5% yearly, in both men and women Postmenopausally,
Osteoporosis POOLE, K.E.S. & COMPSTON, J.E. (2006): Osteoporosis and its management. BMJ 333:1251-6. Physiology Cortical bone After age 40, gradually decreases 0.3-0.5% yearly, in both men and women Postmenopausally,
NEW HORIZONS IN OSTEOPOROSIS THERAPY. Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN
 NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
NEW HORIZONS IN OSTEOPOROSIS THERAPY Sundeep Khosla, M.D. Mayo Clinic, Rochester, MN DISCLOSURES SUNDEEP KHOSLA, M.D. Investigator-initiated grant Merck No non-fda approved recommendations RISK ASSESSMENT
Osteoporosis. Definition
 Osteoporosis Definition Osteoporosis causes bones to become weak and brittle so brittle that a fall or even mild stresses like bending over or coughing can cause a fracture. Osteoporosis-related fractures
Osteoporosis Definition Osteoporosis causes bones to become weak and brittle so brittle that a fall or even mild stresses like bending over or coughing can cause a fracture. Osteoporosis-related fractures
Current and Emerging Approaches for Osteoporosis
 Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Current and Emerging Approaches for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures What s New in Osteoporosis
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Disclosure. Objectives. Osteoporosis. Major Public Health Concern Will I end up like my mother?
 Everything a Pharmacist Needs to Know About Osteoporosis New Mexico Pharmacists Association Mid-Winter Meeting January 27-28, 2018 Albuquerque, NM Consulting Amgen, Radius Speaking Radius Disclosure E.
Everything a Pharmacist Needs to Know About Osteoporosis New Mexico Pharmacists Association Mid-Winter Meeting January 27-28, 2018 Albuquerque, NM Consulting Amgen, Radius Speaking Radius Disclosure E.
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
Osteoporosis in Men Wendy Rosenthal PharmD. This program has been brought to you by PharmCon
 Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Assessment and Treatment of Osteoporosis Professor T.Masud
 Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Assessment and Treatment of Osteoporosis Professor T.Masud Nottingham University Hospitals NHS Trust University of Nottingham University of Derby University of Southern Denmark What is Osteoporosis? Osteoporosis
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Therapeutic Updates in the Prevention and Treatment of Osteoporosis
 Therapeutic Updates in the Prevention and Treatment of Osteoporosis 2013 Fall Managed Care Forum Las Vegas November 15, 2013 Steven T Harris MD FACP Clinical Professor of Medicine University of California,
Therapeutic Updates in the Prevention and Treatment of Osteoporosis 2013 Fall Managed Care Forum Las Vegas November 15, 2013 Steven T Harris MD FACP Clinical Professor of Medicine University of California,
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
How to treat osteoporosis With what and for how long?
 How to treat osteoporosis With what and for how long? Professor Neil Gittoes Consultant Endocrinologist & Honorary Professor Where will we be going? Drug therapies Current Indications Contraindications/unmet
How to treat osteoporosis With what and for how long? Professor Neil Gittoes Consultant Endocrinologist & Honorary Professor Where will we be going? Drug therapies Current Indications Contraindications/unmet
Focusing on the Patient: Diagnosis and Management of Osteoporosis
 Focusing on the Patient: Diagnosis and Management of Osteoporosis Learning Objectives After participating in this educational activity, participants should be able to: 1. Apply updated guidelines to assess
Focusing on the Patient: Diagnosis and Management of Osteoporosis Learning Objectives After participating in this educational activity, participants should be able to: 1. Apply updated guidelines to assess
Steven W. Ing, M.D., MSCE Assistant Professor of Internal Medicine
 Osteoporosis Steven W. Ing, M.D., MSCE Assistant Professor of Internal Medicine Department of Internal Medicine Division of Endocrinology, Diabetes, & Metabolism Ohio State University Medical Center Case
Osteoporosis Steven W. Ing, M.D., MSCE Assistant Professor of Internal Medicine Department of Internal Medicine Division of Endocrinology, Diabetes, & Metabolism Ohio State University Medical Center Case
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Osteoporosis: A Review of Treatment Options
 Kristie N. Tu, PharmD, BCPS, CGP; Janette D. Lie, PharmD, BCACP; Chew King Victoria Wan, PharmD Candidate; Madison Cameron, PharmD Candidate; Alaina G. Austel, PharmD Candidate; Jenny K. Nguyen, PharmD
Kristie N. Tu, PharmD, BCPS, CGP; Janette D. Lie, PharmD, BCACP; Chew King Victoria Wan, PharmD Candidate; Madison Cameron, PharmD Candidate; Alaina G. Austel, PharmD Candidate; Jenny K. Nguyen, PharmD
Osteoporosis: current treatment and future prospects. Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus
 Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Osteoporosis: current treatment and future prospects Juliet Compston Professor Emeritus of Bone Medicine Cambridge Biomedical Campus Disclosures Consultancy and speaking fees for Gilead, related to development
Hot Topics in Osteoporosis and Fracture Prevention
 Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Bone Health for Women: Current Research, Initiatives and Recommendations
 Page 1 BONE HEALTH FOR WOMEN: CURRENT RESEARCH, INITIATIVES AND RECOMMENDATIONS Dr. Melissa Kagarise This program has been brought to you by PharmCon PharmCon is accredited by the Accreditation Council
Page 1 BONE HEALTH FOR WOMEN: CURRENT RESEARCH, INITIATIVES AND RECOMMENDATIONS Dr. Melissa Kagarise This program has been brought to you by PharmCon PharmCon is accredited by the Accreditation Council
Rheumatology. keeping Joints in Motion. Treating and Preventing Fractures
 Rheumatology keeping Joints in Motion Treating and Preventing Fractures Robin K. Dore, MD Clinical Professor of Medicine David Geffen School of Medicine at UCLA, Los Angeles CA Private practice, Tustin
Rheumatology keeping Joints in Motion Treating and Preventing Fractures Robin K. Dore, MD Clinical Professor of Medicine David Geffen School of Medicine at UCLA, Los Angeles CA Private practice, Tustin
Page 1
 Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only.
 This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
Emerging Challenges in Primary Care: Osteoporosis and Fracture Prevention Strategies
 Emerging Challenges in Primary Care: 2017 Osteoporosis and Fracture Prevention Strategies Faculty Nancy R. Berman, MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner Certified Menopause Practitioner Millennium
Emerging Challenges in Primary Care: 2017 Osteoporosis and Fracture Prevention Strategies Faculty Nancy R. Berman, MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner Certified Menopause Practitioner Millennium
Emerging Challenges in Primary Care: Osteoporosis and Fracture Prevention Strategies. Faculty. Disclosures. [Insert Lecture Name Here]
![Emerging Challenges in Primary Care: Osteoporosis and Fracture Prevention Strategies. Faculty. Disclosures. [Insert Lecture Name Here]](/thumbs/76/74138758.jpg "Emerging Challenges in Primary Care: Osteoporosis and Fracture Prevention Strategies. Faculty. Disclosures. [Insert Lecture Name Here]") Emerging Challenges in Primary Care: 2017 Osteoporosis and Fracture Prevention Strategies Faculty Nancy R. Berman, MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner Certified Menopause Practitioner Millennium
Emerging Challenges in Primary Care: 2017 Osteoporosis and Fracture Prevention Strategies Faculty Nancy R. Berman, MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner Certified Menopause Practitioner Millennium
Talking to patients with osteoporosis about initiating therapy
 Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Talking to patients with osteoporosis about initiating therapy Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for
Disclosures. Osteoporosis and Fracture Prevention. Objectives. Objectives. Osteoporosis Overview. Advisory Board: Hologic Advisory Board: LabCorp
 Disclosures Osteoporosis and Fracture Prevention Advisory Board: Hologic Advisory Board: LabCorp Nancy R. Berman MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner/Colposcopist Certified Menopause Practitioner
Disclosures Osteoporosis and Fracture Prevention Advisory Board: Hologic Advisory Board: LabCorp Nancy R. Berman MSN, ANP-BC, NCMP, FAANP Adult Nurse Practitioner/Colposcopist Certified Menopause Practitioner
Osteoporosis in Men Professor Peter R Ebeling
 Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
Page 1. Current and Emerging Strategies for Osteoporosis. Osteoporosis Warm-Up: Which of the Following is True?
 Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
HRT and Risedronate Combined Anabolic and Antiresorptive Therapy
 Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Optimizing Combined and Sequential Osteoanabolic and Antiresorptive Therapy Benjamin Leder, M.D. Endocrine Unit Massachusetts General Hospital Boston, MA Antiresorptive and Osteoanabolic Therapies Increase
Osteoporosis Diagnosis, Treatment and Controversies. Feb, 2018
 Osteoporosis Diagnosis, Treatment and Controversies Feb, 2018 Shawn Baca, M.D., F.A.C.R. Rheumatology Associates of South Florida RASF RASF Clinical Research Osteoporosis Diagnosis and Treatment Center
Osteoporosis Diagnosis, Treatment and Controversies Feb, 2018 Shawn Baca, M.D., F.A.C.R. Rheumatology Associates of South Florida RASF RASF Clinical Research Osteoporosis Diagnosis and Treatment Center
Outline. Osteoporosis Definition DXA* Osteoporosis is Common. Brittle bones: Pitfalls in the evaluation and management of osteoporosis
 Brittle bones: Pitfalls in the evaluation and management of osteoporosis Sri Harsha Tella, MD CCD Department of Internal Medicine Division of Endocrinology, Diabetes and Metabolism University of South
Brittle bones: Pitfalls in the evaluation and management of osteoporosis Sri Harsha Tella, MD CCD Department of Internal Medicine Division of Endocrinology, Diabetes and Metabolism University of South
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Musculoskeletal Clinical Correlates: Osseous Conditions in Dental Patients
 Musculoskeletal Clinical Correlates: Osseous Conditions in Dental Patients Learning Objectives Define osteoporosis and explain how it is diagnosed. Describe the main risk factors for developing osteoporosis.
Musculoskeletal Clinical Correlates: Osseous Conditions in Dental Patients Learning Objectives Define osteoporosis and explain how it is diagnosed. Describe the main risk factors for developing osteoporosis.
Dumfries and Galloway. Treatment Protocol for Osteoporosis
 Dumfries and Galloway Treatment Protocol for Osteoporosis DIAGNOSIS OF OSTEOPOROSIS 2 Diagnostic Criteria 2 Multiple low trauma vertebral fractures in the absence of myeloma or metastatic disease. 2 T-score
Dumfries and Galloway Treatment Protocol for Osteoporosis DIAGNOSIS OF OSTEOPOROSIS 2 Diagnostic Criteria 2 Multiple low trauma vertebral fractures in the absence of myeloma or metastatic disease. 2 T-score
Bone Health in Celiac Disease. Partha S. Sinha MD, PhD October 29 th, 2017
 Bone Health in Celiac Disease Partha S. Sinha MD, PhD October 29 th, 2017 No Disclosures Objectives Recognize the mechanisms by which celiac disease can affect bone health Review what diagnostic tests
Bone Health in Celiac Disease Partha S. Sinha MD, PhD October 29 th, 2017 No Disclosures Objectives Recognize the mechanisms by which celiac disease can affect bone health Review what diagnostic tests
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents
 AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
Bone Health Update Susan L. Greenspan, MD Professor of Medicine University of Pittsburgh
 Bone Health Update 2018 Susan L. Greenspan, MD Professor of Medicine University of Pittsburgh The Problem 50% women and 20% of men have an osteoporotic fracture after age 50 2 million fractures annually
Bone Health Update 2018 Susan L. Greenspan, MD Professor of Medicine University of Pittsburgh The Problem 50% women and 20% of men have an osteoporotic fracture after age 50 2 million fractures annually
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Biochemical Markers of Bone Turnover: Definitions and Recommendations for Monitoring Therapy Learning Objectives for Biochemical
Annual Rheumatology & Therapeutics Review for Organizations & Societies Biochemical Markers of Bone Turnover: Definitions and Recommendations for Monitoring Therapy Learning Objectives for Biochemical