GASTROINTESTINAL BLEEDING. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
|
|
|
- Elvin Logan
- 5 years ago
- Views:
Transcription
1 GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
2 Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia- bright red blood per rectum indicates a lower GI source of bleeding Blood has a laxative effect so with massive bleeding the stool may be bright red
3 Gastrointestinal Bleeding Blood streaks on the stool indicates anal outlet bleeding Blood mixed with stool indicates bleeding source higher than the rectum Blood with mucus indicates an infectious or inflammatory disease Currant jelly-like material indicates vascular congestion and hyperemia (intussusception or midgut volvulus)
4 Gastrointestinal Bleeding Maroon-colored stools indicate voluminous bleeding proximal to the rectosigmoid area Melena, passage of black, sticky (tarry) stools suggests upper GI tract bleeding, but can be as distal as the right colon Hematemesis suggests a large bleed with possible recurrence, melena alone indicates less voluminous bleeding
5 Causes of Upper GI Bleeding Common Nasopharyngeal bleeding Erosive Esophagitis Peptic ulcer Gastritis (H. pylori) Mallory-Weiss tear Prolapse gastropathy Less Common Bleeding disorders Duplication cyst Foreign body Tube trauma Vascular malformation Esophageal varices
6 Causes of Lower GI Bleeding Common Anal fissure Infectious colitis Salmonella, Shigella, Campylobacter, C.diff Inflammatory bowel disease Intussusception Upper GI source Less Common Meckel s diverticulum Duplication cyst Hirschsprung s enterocolitis Gangrenous intestine Vascular malformation
7 Clinical Findings in Neonatal Period Gastric ulcers are more common than duodenal ulcers in neonates Spontaneous Perforation is a more common presentation than bleeding Frequently associated with: Hypoxia, Sepsis, RDS, CNS disorder
8 Clinical Findings in PUD Infants and Toddlers Presenting symptoms: Vomiting Poor feeding Irritability during and after eating Abdominal distention Hematemesis, melena Commonly associated with underlying disease in this age group
9 Clinical Findings in PUD Pre-Schoolers Periumbilical or generalized abdominal pain Vomiting after eating Nocturnal or early morning pain Gastric ulcers are as common as duodenal ulcers Primary ulcers are as common as secondary ulcers
10 Clinical Findings in School Age Male: Female ratio is 3:1 Burning epigastric pain Nocturnal pain Melena, hematemesis, fecal occult blood Primary ulcers are more common than secondary ulcers
, inflammatory bowel dz Portal hypertension Esophageal varices, hypertensive gastropathy Coagulopathy - Hemophilia, hepatic coagulopathy, CHF")
11 Pathophysiology of GI Bleeding Mucosal lesions Acid-peptic disease, drug-induced (NSAIDs), Infectious (H. pylori), inflammatory bowel dz Portal hypertension Esophageal varices, hypertensive gastropathy Coagulopathy - Hemophilia, hepatic coagulopathy, CHF w/hepatic congestion Vascular lesions - hemangiomas
12 Causes and Effects of H + Ion Backdiffusion Lowflow states Drugs, EtOH Stress H. pylori Bile Reflux Mucosal Barrier Break H + Parietal Cells Release of histamine + Vasodilatation Increased HCl and Pepsin Secretion
13 Peptic Ulcer Disease Diagnostic Evaluation History (medications, family history) Physical exam (include Hemoccult) CBC, type & screen for GI bleeding PT, PTT H. pylori antibody, fasting gastrin level Upper GI Series EGD
14 Indications for EGD Hematemesis, Melena, Heme (+) stool Severe pain, weight loss Unexplained anemia Symptoms persist despite trial of antisecretory therapy Evaluation of abnormal UGI series Evaluation of status of H. pylori
15 Case #1 UGI Bleeding 12 YOWF with S/P splenectomy 2 yr ago for Evan s syndrome Weakness, pallor, melana x 2 days Exam HR- 128, BP-86/54, tachycardic, pale, abdomen nontender, nondistended, no hepatomegaly Lab H/H=6.8/19.1, WBC, 5.7; platelets, 115,000, PT=13.2 sec; AST, 38; ALT, 45; T.bili, 0.5; alk phos, 227
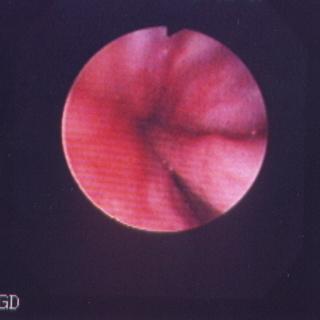
16 Esophageal varices


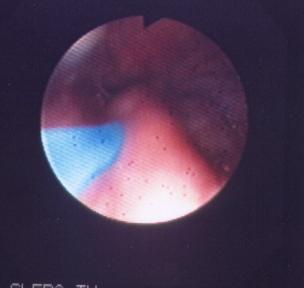
17 Case #2 UGI Bleeding 11 YOWM previously healthy with 1 day h/o fever, vomiting and diarrhea Emesis x 6 over past 24 hr, w/blood last 2 times Exam HR- 84, BP-116/74, abdomen nontender, nondistended, no hepatomegaly Lab H/H=13.8/39.1, WBC, 8.7; platelets, 235,000, PT=12.2 sec

18 Prolapse Gastropathy
19 Meckel s Scan 99m Tc-Pertechnetate Scan - injected IV and accumulates in gastric tissue - RLQ uptake is diagnostic of Meckel s diverticulum False (+) - bleeding lesions such as Crohn s disease, intussusception, hemangioma, PUD False (-) - Barium, bladder overdistention, no gastric mucosa in diverticulum
20 99m Tc- Labeled Red Cell Scan 99m Tc-sulfur colloid is added to a sample of the patient s blood cells and re-infused IVpatient is scanned with gamma camera Half-life is short (2.5 min) so that after 10 minutes only 10% is left in the circulation 99m Tc accumulates at the bleeding site and lights up on scan - can detect 0.1 ml/min
 Transfuse for Hgb < 8 w/active bleeding NG lavage Antacids (1 ml/kg up to 30 ml q 2 hr) PPI 2")
21 GI Bleeding - Treatment ABCs - protect airway with hematemesis in an obtunded patient IV access - two lines (0.9% NS in one line, PRBC s not compatible with dextrose) Transfuse for Hgb < 8 w/active bleeding NG lavage Antacids (1 ml/kg up to 30 ml q 2 hr) PPI 2 mg/kg loading dose, then 1 mg/kg/day IV

22 Drug Efficacy in Healing Ulcers Drug Regimen Ulcers Healed H2RA 4 weeks 8 weeks Cimetidine 40 mg/k/d 80% 90% Ranitidine 4-8 mg/k/d Famotidine 1-2 mg/k/d PPIs Omeprazole mg/k/d 85% 95% Lansoprazole mg/k/d Sucralfate mg/k/d 75% 86%
23 ATLS Classification of Shock Class Blood Loss BP HR Cap refill 1 <15% WNL Up to 10-20% % % % WNL Neuro WNL Decreased >150 > 3 sec Alert Decreased >150 > 3 sec Lethargic Not palpable >150 > 3 sec Obtunded
24 Management Class 1, no anemia, no active bleeding on lavage, may be followed up as outpatient Class 2, mild anemia, active bleeding may be monitored on wards Class 3 or 4 admit to PICU, central line, arterial line IVF boluses, transfusion as needed
25 Management Iced saline? - with cooling, bleeding time increases to 3 x control, clotting time increases up to 60%, and PT can increase to 2 x control, and can cause hypothermia NG tube is useful to monitor bleeding, but not in treatment Therapeutic endoscopy (sclerotherapy) useful in variceal hemorrhage

26 Management - Octreotide Somatostatin analog - octreotide has a longer halflife than somatostatin Decreases splanchnic blood flow and gastrointestinal secretion Make a 1 g/ml drip - begin drip at a rate of 0.1 g/kg/min - increase to 0.5 g/kg/min until bleeding stops, then wean rate Side effects - nausea, gas, hyperglycemia, gallstones, elevated liver enzymes
27 GI Bleeding Summary Remember your abc s IV access if bleeding is significant Plan diagnostic work-up based on presentation Consider non-gi causes of blood in the GI tract (e.g., swallowed blood)
28 Question #1 An 18-month-old boy passed a dark red stool four hours ago and another bloody stool during physical examination. He has no fever, vomiting, diarrhea, or constipation. His growth and development have been normal. On physical examination, his pulse is 140/min, respiratory rate 24/min, and blood pressure is 86/54 mmhg. The abdomen is soft and nontender. Rectal examination reveals maroon-colored stool that is guaiac positive. The remainder of the physical examination is normal. Gastric aspirate is negative for blood. Laboratory evaluation reveals hemoglobin 8 g/dl, hematocrit 26%. Prothrombin time, partial thromboplastin time, and INR were normal. After intravenous fluid administration and erythrocyte transfusion, which of the following is most likely to be diagnostic? A. Barium enema B. Meckel radionuclide scan C. Computerized tomography (CT scan) of the abdomen D. Upper gastrointestinal series with small bowel follow through E. Abdominal angiography
29 Question #2 A 6-week-old infant has done well since birth until blood and mucus appeared in the stool for the past 3 days. He is taking his usual four ounces of cow-milk formula per feeding without vomiting. He is more irritable during defecation. Physical examination reveals that the abdomen is soft and not distended. The hemoglobin is 10 g/dl. Which of the following is the most likely explanation for the findings in this infant? A. Hirschsprung disease B. Meckel diverticulum C. Anal fissure D. Cow-milk protein colitis E. Midgut volvulus
UPPER AND LOWER GASTROINTESTINAL BLEEDING. Prof. G. Zuliani
 UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Objectives: Resources:
 Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
SMALL GROUP DISCUSSION
 MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Gastroduodenal Stress Ulceration. Bryan Woolridge POS Rounds 29 October 2003
 Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Gastroduodenal Stress Ulceration Bryan Woolridge POS Rounds 29 October 2003 Objectives Define entity Etiology Differentiation of UGI ulcers Pathophysiology Identify population at risk/risk factors Clinical
Rectal Bleeding in Infancy
 Rectal Bleeding in Infancy Bittoo Kanwar, MD Assistant Professor of Pediatrics Division of Gastroenterology UCSF Objectives To understand the common and uncommon causes of rectal bleeding in infancy To
Rectal Bleeding in Infancy Bittoo Kanwar, MD Assistant Professor of Pediatrics Division of Gastroenterology UCSF Objectives To understand the common and uncommon causes of rectal bleeding in infancy To
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Good morning! July 24, 2014
 Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
Good morning! July 24, 2014 Prep #1 A 2-year-old boy presents to your office with a 2-day history of swelling of the right eye. He has been otherwise well. There are scattered insect bites on his body,
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Gastroenterology. Chapter 28
 Gastroenterology Chapter 28 Gastroenterology Intestinal Infection Acute gastroenteritis is the most common cause of infant mortality worldwide Viral gastroenteritis is usually associated with small bowel
Gastroenterology Chapter 28 Gastroenterology Intestinal Infection Acute gastroenteritis is the most common cause of infant mortality worldwide Viral gastroenteritis is usually associated with small bowel
Gastro- Intestinal Bleeding in Children
 Gastro- Intestinal Bleeding in Children Upper G1 Bleeding. Lower G1 Bleeding. Upper G1 Bleeding :- Presentation : Hematemesis Causes :- Neonate reflux esophagitis (dark, small amount) PyLoric stenosis
Gastro- Intestinal Bleeding in Children Upper G1 Bleeding. Lower G1 Bleeding. Upper G1 Bleeding :- Presentation : Hematemesis Causes :- Neonate reflux esophagitis (dark, small amount) PyLoric stenosis
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Some slides courtesy of James Markowitz M.D.
 Gastrointestinal Bleeding in Children Clinical Cases Dr. Noam Zevit Schneider Children s Medical Center of Israel Sackler Faculty of Medicine - Tel Aviv University Some slides courtesy of James Markowitz
Gastrointestinal Bleeding in Children Clinical Cases Dr. Noam Zevit Schneider Children s Medical Center of Israel Sackler Faculty of Medicine - Tel Aviv University Some slides courtesy of James Markowitz
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
MHD II Session 3 STUDENT COPY
 MHD II, Session 3, Student Copy - Page 1 MHD II Session 3 January 15, 2016 STUDENT COPY MHD II, Session 3, Student Copy - Page 2 CASE HISTORY 1 Cc: Terrible diarrhea for 1 ½ days A 66 year-old woman presents
MHD II, Session 3, Student Copy - Page 1 MHD II Session 3 January 15, 2016 STUDENT COPY MHD II, Session 3, Student Copy - Page 2 CASE HISTORY 1 Cc: Terrible diarrhea for 1 ½ days A 66 year-old woman presents
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Gastrointestinal Emergencies. Candice M. Quillin BSN CGRN September 27, 2014
 Gastrointestinal Emergencies Candice M. Quillin BSN CGRN September 27, 2014 Objectives List four gastrointestinal emergencies and complications. Identify signs and symptoms of a variety of gastrointestinal
Gastrointestinal Emergencies Candice M. Quillin BSN CGRN September 27, 2014 Objectives List four gastrointestinal emergencies and complications. Identify signs and symptoms of a variety of gastrointestinal
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
The focus of this week s lab will be pathology of the gastrointestinal and hepatobiliary systems.
 GASTROINTESTINAL AND HEPATOBILIARY SYSTEMS The focus of this week s lab will be pathology of the gastrointestinal and hepatobiliary systems. GASTROINTESTINAL SYSTEM AND HEPATOBILIARY SYSTEM We will examine
GASTROINTESTINAL AND HEPATOBILIARY SYSTEMS The focus of this week s lab will be pathology of the gastrointestinal and hepatobiliary systems. GASTROINTESTINAL SYSTEM AND HEPATOBILIARY SYSTEM We will examine
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
But.. Capsule Endoscopy. Guidelines (OMED ECCO) Why is Enteroscopy so Important? 4/19/2017
 Why is Enteroscopy so Important? 4/19/2017") Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Pediatric Gastroenterology Referral Guidelines
 Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Suggested Pre-Referral Workup This is a general suggestion of possible testing to confirm a suspected diagnosis. Although referrals will be accepted without the suggested work up being complete, to ensure
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
UPPER GI DISEASES 11/15/2014. Lesson Objectives. GI Tract Review. NUTR 2050 Nutrition for Nursing Professionals. Mrs. Deborah A. Hutcheon, MS, RD, LD
 UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
Second term/
 Second term/ 2015-2016 L. 1 Dr Mohammed AL-Zobaidy Learning objectives GIT pharmacology After completing this chapter the student will be able to: Recognise pathophysiological factors implicated in acid-peptic
Second term/ 2015-2016 L. 1 Dr Mohammed AL-Zobaidy Learning objectives GIT pharmacology After completing this chapter the student will be able to: Recognise pathophysiological factors implicated in acid-peptic
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Gastrointestinal bleeding definitions (I)
") definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
definitions (I) Acute bleeding: vomiting blood or profuse rectal bleeding within 3 days, leading to hemodynamically unstable condition of the patient. Problems arising from blood loss must be treated often
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
CHAPTER 72. GASTROINTESTINAL BLEEDING
 Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Pediatric Emergency Medicine > Section X: Gastrointestinal Emergencies > CHAPTER 72. GASTROINTESTINAL
Print Close Window Note: Large images and tables on this page may necessitate printing in landscape mode. Pediatric Emergency Medicine > Section X: Gastrointestinal Emergencies > CHAPTER 72. GASTROINTESTINAL
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
GASTROINTESTINAL HEMORRHAGE
 Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Gastrointestinal Hemorrhage, Lower
 Gastrointestinal Hemorrhage, Lower What is a lower gastrointestinal hemorrhage? A lower gastrointestinal (GI) hemorrhage, also called lower GI bleeding or rectal bleeding, is abnormal blood loss from the
Gastrointestinal Hemorrhage, Lower What is a lower gastrointestinal hemorrhage? A lower gastrointestinal (GI) hemorrhage, also called lower GI bleeding or rectal bleeding, is abnormal blood loss from the
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Gastroduodenal Ulcer Disease
 Gastroduodenal Ulcer Disease (Ulcers in the Stomach and Upper Small Intestine [Duodenum]) Basics OVERVIEW Gastro- refers to the stomach; duodenal refers to the upper small intestine or duodenum Ulcers
Gastroduodenal Ulcer Disease (Ulcers in the Stomach and Upper Small Intestine [Duodenum]) Basics OVERVIEW Gastro- refers to the stomach; duodenal refers to the upper small intestine or duodenum Ulcers
Reflux of gastric contents, particularly acid, into the esophagus
 Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
HCPCS Codes (Alphanumeric, CPT AMA) ICD-9-CM Codes Covered by Medicare Program
 ICD-9-CM Codes Covered by Medicare Program") HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
HASPI Medical Biology Lab 03
 Patient 1001 is a 42-year-old female that is experiencing severe heartburn, abdominal pain, bloating, nausea, and vomiting. Ulcers Bleeding sores in the stomach or intestine Gallbladder Disease Gallstones
Patient 1001 is a 42-year-old female that is experiencing severe heartburn, abdominal pain, bloating, nausea, and vomiting. Ulcers Bleeding sores in the stomach or intestine Gallbladder Disease Gallstones
PEDIATRIC GI EMERGENCIES. AGE-RELATED DIAGNOSIS Early Infancy EXAMINATION TIPS PEDIATRIC ABDOMINAL PAIN. How Common Is It?
 PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
PEDIATRIC ABDOMINAL PAIN How Common Is It? PEDIATRIC GI EMERGENCIES Ghazala Q. Sharieff, MD 5% of unscheduled visits 2% of patients are admitted 1% need operative intervention EXAMINATION TIPS Palpate
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Abdominal Pain. Luke Donnelly, MD Emergency Medicine
 Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Abdominal Pain Luke Donnelly, MD Emergency Medicine Objectives Approach to abdominal pain Evaluation Critical diagnoses and treatments Abdominal Pain Most Common ER Complaint Broad Differential Can often
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
RECTAL PROLAPSE objectives
 RECTAL PROLAPSE objectives 1.Classify rectal prolapse 2. Enumerate the causes of rectal prolapse 3. Differentiate between complete rectal prolapse and intussusception 4. List the modalities of treatment
RECTAL PROLAPSE objectives 1.Classify rectal prolapse 2. Enumerate the causes of rectal prolapse 3. Differentiate between complete rectal prolapse and intussusception 4. List the modalities of treatment
Objectives. Pain Types Brief Review. Referred Pain. Chronic/Recurrent Abdominal Pain 1/12/2017. I have no conflicts of interest to disclose
 Joshua D Noe, MD Associate Professor of Pediatric Gastroenterology Hepatology and Nutrition Medical College of Wisconsin I have no conflicts of interest to disclose Objectives Differentiate functional
Joshua D Noe, MD Associate Professor of Pediatric Gastroenterology Hepatology and Nutrition Medical College of Wisconsin I have no conflicts of interest to disclose Objectives Differentiate functional
The Usefulness of Capsule Endoscopy
 The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Peptic Ulcer Disease Update
 Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CHAPTER 30 Gastrointestinal Bleeding
 CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
CHAPTER 30 Gastrointestinal Bleeding Eric Goralnick and David A. Meguerdichian PERSPECTIVE Epidemiology Gastrointestinal bleeding (GIB) accounts for more than 1 million hospitalizations annually in the
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
What Is an Endoscopic Ultrasound (EUS)?
?") ENDOSCOPIC ULTRASOUND (EUS) What Is an Endoscopic Ultrasound (EUS)? An endoscopic ultrasound (EUS) is a specialized procedure that blends: Endoscopy use of a scope to look at the inside lining of the gastrointestinal
ENDOSCOPIC ULTRASOUND (EUS) What Is an Endoscopic Ultrasound (EUS)? An endoscopic ultrasound (EUS) is a specialized procedure that blends: Endoscopy use of a scope to look at the inside lining of the gastrointestinal
Chapter 44 10/17/2015. Care of the Patient with a Gastrointestinal Disorder. The Digestive System. Organs of the Digestive System
 Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
Chapter 44 Care of the Patient with a Gastrointestinal Disorder All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. The Digestive System Consists
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Sick or not sick? Objectives. Bilious vomiting. Deadly Misdiagnoses: Kids with GI Complaints. Ronald Dieckmann, MD. Problems in assessment
 Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
Deadly Misdiagnoses: Kids with GI Complaints Objectives Understand key assessment techniques for recognition of serious illness in children. Ronald Dieckmann, MD Professor of Clinical Pediatrics and Emergency
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2
 Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Original Article Clinical Endoscopic Parameters of Upper Gastrointestinal Bleeding Hemal Shah, 1 T. P. Manohar 2 1 Junior Resident 2 Associate Professor,Department of Medicine, N.K.P. Salve Institute Of
Objectives. Pediatric Mortality. Another belly pain. Gastroenteritis. Spewing & Pooing Child 4/18/16
 Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
Gastro-tastrophies A Review of Pediatric GI Emergencies Objectives Discuss common presentations of Pediatric Abdominal Pain complaints Discuss work up and physical exam findings Discuss care, management
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse What is gastritis? Gastritis is a condition in which the stomach lining known as the mucosa is inflamed, or swollen. The stomach lining contains
Gastritis National Digestive Diseases Information Clearinghouse What is gastritis? Gastritis is a condition in which the stomach lining known as the mucosa is inflamed, or swollen. The stomach lining contains
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS
 DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
DR JAIKISHOR JOTHIRAJ MD POST GRADUATE DEPT OF RADIODIAGNOSIS YASHODAMMAL 70 YRS OD LADY had C/o diffuse lower abdominal pain 20 days h/o blood in stools 4 days h/o vomiting 2 days h/o burning micturation
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
OBJECTIVES VISCERAL PAIN RECEPTORS LOCATION & NATURE OF THE PAIN LOCATION OF VISCERAL PAIN RECEPTORS 4/12/2018. Nancy Brown, APRN, CPNP April 18, 2018
 Nancy Brown, APRN, CPNP April 18, 2018 OBJECTIVES 1. Understand the principle causes of acute abdominal pain in children. 2. Make symptom based diagnoses of functional abdominal pain in children. 3. Recognize
Nancy Brown, APRN, CPNP April 18, 2018 OBJECTIVES 1. Understand the principle causes of acute abdominal pain in children. 2. Make symptom based diagnoses of functional abdominal pain in children. 3. Recognize
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
PEDIATRIC EMERGENCY DEPARTMENT CLINICAL GUIDELINE: GI SURGICAL EMERGENCIES: VOMITING
 GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
GI SURGICAL EMERGENCIES: VOMITING PYLORIC STENOSIS Population: Infants: onset between 2-5 weeks of age 1 in 250 births Male: female ratio 4:1 Familial incidence History: No vomiting in the first few weeks
Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies. Author(s): Joseph House (University of Michigan), MD 2012
: Joseph House (University of Michigan), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
Project: Ghana Emergency Medicine Collaborative Document Title: Non-Traumatic Abdominal Pain/Abdominal Emergencies Author(s): Joseph House (University of Michigan), MD 2012 License: Unless otherwise noted,
CT Angiography g of Lower Intestinal Bleeding
 CT Angiography g of Lower Intestinal Bleeding Jorge A. Soto, MD General concepts: Learning Objectives Clinical Importance Presentation, Location Etiologies CT Ttchniques: CT Angiography CT Enterography
CT Angiography g of Lower Intestinal Bleeding Jorge A. Soto, MD General concepts: Learning Objectives Clinical Importance Presentation, Location Etiologies CT Ttchniques: CT Angiography CT Enterography
pthaigastro.org Caustic injury The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management
 The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management Caustic injury Phisek Yimyaem Pediatric Department, Khon Kaen Regional Hospital 18 July 2013 Outlines Introduction
The 5 th Pediatric GI Days Pediatric GI & Liver Emergency : Current Practical Management Caustic injury Phisek Yimyaem Pediatric Department, Khon Kaen Regional Hospital 18 July 2013 Outlines Introduction
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Occult GI Bleed. July 2015
 Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Abdominal Pain in a Young Aviator
 Abdominal Pain in a Young Aviator Calen N. Wherry, MD, MPH Maj, USAF, MC, FS Peter A. Baldwin, MD, MBA, MPH Capt, USAF, MC, FS USAF School of Aerospace Medicine WPAFB, OH RAM 2013 Distribution A: Approved
Abdominal Pain in a Young Aviator Calen N. Wherry, MD, MPH Maj, USAF, MC, FS Peter A. Baldwin, MD, MBA, MPH Capt, USAF, MC, FS USAF School of Aerospace Medicine WPAFB, OH RAM 2013 Distribution A: Approved
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding
 ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division
ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding Lauren B. Gerson, MD, MSc, FACG 1, Jeff L. Fidler 2, MD, David R. Cave, MD, PhD, FACG 3, Jonathan A. Leighton, MD, FACG 4 1 Division