CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
|
|
|
- Franklin Mervin Andrews
- 5 years ago
- Views:
Transcription
1 CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1
2 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal (GI) tract: pain nausea vomiting bloating diarrhea constipation Without detectable structural or biochemical abnormalities 2
3 Classification FGIDs ( classified by anatomic region) (A) Esophageal (B) Gastroduodenal (B1: FD) (C) Bowel (C1: IBS) (D) Functional abdominal pain (E) Biliary (F) Anorectal. 3
4 Common Features of FGIDs 1. Pathophysiology 2. Role of psychosocial factors 3. The treatment strategy 4
5 1. Pathophysiology 1) Abnormal motility 2) Visceral hypersensitivity 3) Inflammation 4) Brain-gut interactions 5) Brain-gut peptides: 5-hydroxytryptamine 5- 羟色胺 enkephalins 脑啡肽, substance P, p- 物质 calcitonin gene related polypeptide 降钙素, cholecystokinin 缩胆囊素 5
6 2. Role of psychosocial factors 1)Psychological stress exacerbates GI symptoms. 2)Psychological disturbances modify the experience of illness and illness behaviors such as health care seeking. 3) Psychosocial factors affect health status and clinical outcome. 6
7 FGID biopsychosocial model 7
8 3. Treatment Strategy 1) General treatment approach establish therapeutic relationship education and reassurance dietary and lifestyle modifications 2) Pharmacological therapies symptomatic treatment antidepressant 3) Psychological therapies cognitive-behavioral treatment hypnosis 8
9 Functional dyspepsia (FD) 9
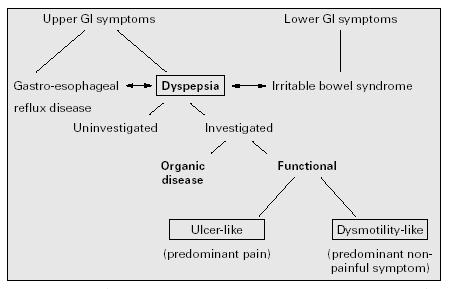
10 Definition Persistent or recurrent pain or discomfort centered in the upper abdomen: including pain, early satiety, nausea, vomiting, abdominal distension, bloating, and anorexia Evidence of organic disease likely to explain the symptoms is absent. 10
11 Pathophysiological mechanisms 1. Gastrointestinal motor abnormalities 2. Altered visceral sensation 3.Psychosocial factors 4. Helicobacter pylori infection? 11








12 Putative Pathogenesis of Stress Dyspepsia Increased Sensitivity Increased Afferent Activity Low Grade Inflammation ± HP Infection ANS Imbalance Sensory Inhibition... Sensitivity Impaired Motor Activity Accommodation Altered Motor & Sensory Function DYSPEPSIA 12
13 1. Alterations in Motility Delayed emptying Impaired accommodation to a meal Antral hypomotility Gastric dysrhythmias Altered duodenojejunal motility 13
14 2. Altered visceral sensation Hypersensitivity to gastric balloon distention: suggesting abnormal afferent function Reflex hyporeactivity: suggesting either abnormal afferent or abnormal efferent function 14
15 3. Psychosocial factors The personality profile impacts on patients with functional dyspepsia. Higher levels of anxiety and depression have been found. A link between childhood abuse and functional gastrointestinal disorders. 15
16 4. Helicobacter pylori infection? Strictly controlled studies have failed to identify any real relationship between Helicobacter pylori infection and FD. 16
17 Clinical Features Dyspepsia: Pain or Discomfort centered in the upper abdomen The symptoms may be intermittent or continuous, and may or may not be related to meals. 17
18 Definitions of the symptom Pain: a subjective, unpleasant sensation Discomfort: a subjective, unpleasant sensation or feeling that is not interpreted as pain according to the patient, including upper abdominal fullness, early satiety, bloating, or nausea centered in the upper abdomen: the pain or discomfort is mainly in or around the midline 18
19 Dyspepsia subgroup classification -based on the predominant single symptom 1. Ulcer-like dyspepsia 2. Dysmotility-like dyspepsia 3. Unspecified (non-specific) dyspepsia 19
20 1. Ulcer-like dyspepsia Pain centered in the upper abdomen is the predominant (most bothersome) symptom. 20
21 2. Dysmotility-like dyspepsia An unpleasant or troublesome non-painful sensation (discomfort) centered in the upper abdomen is the predominant symptom; this sensation may be characterized by or associated with upper abdominal fullness, early satiety, bloating, or nausea. 21
22 3. Non-specific dyspepsia Symptomatic patients whose symptoms do not fulfill the criteria for ulcer-like or dysmotility-like dyspepsia. 22
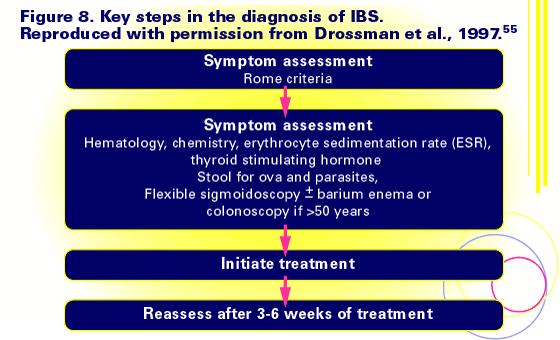
23 Diagnosis Rome II Criteria: At least 12 weeks, which need not be consecutive, within the preceding 12 months of: 1. Persistent or recurrent dyspepsia (pain or discomfort centered in the upper abdomen); 23
24 Diagnosis Rome II Criteria: 2. No evidence of organic disease (including at upper endoscopy) that is likely to explain the symptoms; 24
25 Diagnosis Rome II Criteria: 3. No evidence that dyspepsia is exclusively relieved by defecation or associated with the onset of a change in stool frequency or stool form (i.e., not irritable bowel). 25
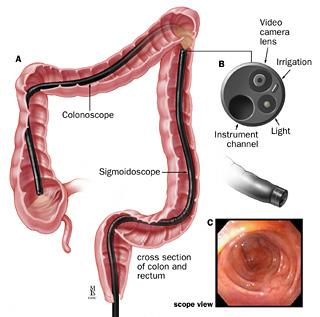
26 Diagnostic process FD remains a diagnosis of exclusion: Careful history and physical examination Upper endoscopy is necessary The others: exclusion of chronic peptic ulcer disease, gastroesophageal reflux disease, esophagitis, pancreatico-biliary disease malignancy 26
27 27



28 Major Causes of Dyspepsia Williams 1988 Stanghellini 1996 Heikkinen 1996 (n=1386) (n=1057) (n=766) 60 % of Patients with Diagnosis Gastric Cancer Peptic Ulcer Esophagitis/ Functional GERD Dyspepsia 28
29 Differential Diagnosis GERD: Heartburn is the predominant symptom Upper endoscopy Prolonged esophageal ph monitoring Twenty-four hour esophageal ph monitoring 29
30 Differential Diagnosis IBS: overlap symptom co-exist with FD 30
31 Treatment The goal is to accept, diminish, and cope with symptoms rather than eliminate them. The most important aspects include explanation that the symptoms are not imaginary, evaluation of relevant psychosocial factors, and dietary advice. 31
32 Pharmacological therapies H. pylori therapy? controversial Acid suppression and prokinetic agents (digestive agents)? may help Gut analgesics? Relaxants of the nervous system of the gut may be beneficial Antidepressant? May help 32


33 Management of Ulcer-like Functional Dyspepsia Ulcer-like Symptoms Dominant Education/lifestyle modification Test Hp + - Eradicate Hp Reassess Trial of acid suppression Success Investigate Failure Trial of prokinetic 33
34 Management of Dysmotility-like Functional Dyspepsia Dysmotility-like Symptoms Dominant Educate/lifestyle modification Success Trial of prokinetic medication Failure Continue with cyclic therapy Investigate Test H. pylori Gastroscopy or UGI + - Success Eradicate Failure Consider H 2 antagonists, tricyclics 34
35 Irritable bowel syndrome (IBS) 35
36 Definition Irritable bowel syndrome (IBS) is a functional GI disorder characterized by abdominal pain or discomfort and altered bowel habits In the absence of demonstrable organic disease. 36
37 Pathophysiological mechanisms 1 Altered gut reactivity (motility, secretion) in response to luminal (e.g., meals, gut distention, inflammation, bacterial factors) or provocative environmental stimuli (psychosocial stress), resulting in symptoms of diarrhea and/or constipation 37
38 Pathophysiological mechanisms 2 A hypersensitive gut with enhanced visceral perception and pain 38
39 Pathophysiological mechanisms 3 Dysregulation of the brain-gut axis, possibly associated with greater stress-reactivity and altered perception and/or modulation of visceral afferent signals 39
40 Pathophysiological mechanisms 4 Inflammation: gut inflammatory and immune factors persisting following infection or inflammation of the bowel 40
41 Pathophysiological mechanisms 5 Autonomic dysfunction: the role of autonomic dysfunction in IBS requires further evaluation 41
42 Role of psychosocial factors 1)Psychological stress exacerbates GI symptoms. 2)Psychological disturbances modify the experience of illness and illness behaviors such as health care seeking. 3) Psychosocial factors affect health status and clinical outcome. 42
43 43

44 Possible causes of IBS 44

45 The biopsychosocial model of IBS 45

46 Nerve cell communication in the wall of the colon. 46
47 Clinical Features Abdominal discomfort or pain is associated with defecation or a change in bowel function and with features of disordered defecation. 47
48 Clinical Features Classifying IBS patients based on their symptomatology: 1. Diarrhea-predominant pattern: IBS associated with abdominal discomfort, fecal urgency, and diarrhea 48
49 Clinical Features 2. Constipation -predominant pattern: IBS associated with abdominal discomfort, bloating, and constipation 49

50 Clinical Features 3. Mixed pattern: IBS alternating between diarrhea and constipation 50

51 Symptoms and signs 51
52 52
53 Diagnosis Rome II Criteria patients must have the following continuous or recurrent symptoms for at least 12 weeks of abdominal pain or discomfort characterized by the following: Relieved by defecation Associated with a change in stool frequency Associated with a change in stool consistency 53
54 54
55 55
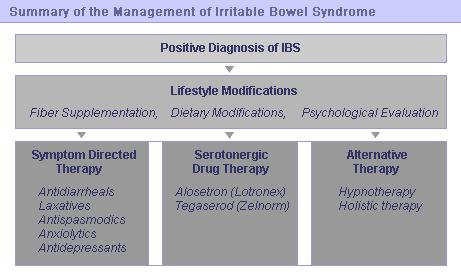
56 Treatmemt General treatment approach 1. Establish therapeutic relationship 2. Education and reassurance 3. Dietary and lifestyle modifications 56
57 Physician-Patient Relationship Reassure the patient that they are not unusual Identify why the patient is currently presenting Obtain a history of referral experiences Examine patient fears or agendas Ascertain patient expectations of physician Determine patient willingness to aid in treatment Uncover the symptom most impacting quality of life and the specific treatment designed to improve management of that symptom 57
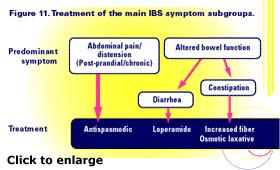
58 Pharmacological therapies Dietary and drug therapy for IBS can be considered in two categories: 1.End organ treatment aimed at relieving abdominal pain (antispasmodic drugs) or disturbed bowel habit (antidiarrhoeal and bulking agents). 2. Central treatment (antidepressants) targeted at patients with associated affective disorder. 58
59 59
60 Psychological therapies Cognitive-behavioral treatment Hypnosis 60
61 61
62 Functional dyspepsia Definition: pain or discomfort without the evidence of organic disease Pathophysiological mechanisms Alterations in Motility and visceral sensation; Psychosocial factors; Hp infection? Clinical Features Ulcer-like dyspepsia; Dysmotility-like dyspepsia; Non-specific dyspepsia. Diagnosis (a diagnosis of exclusion):rome II Criteria: Treatment: Goal; Pharmacological therapies; Psychological therapies 62
63 Irritable bowel syndrome Definition:abdominal pain or discomfort and altered bowel habits without demonstrable organic disease. Pathophysiological mechanisms Clinical Features: 1. Diarrhea-predominant; 2. Constipation-predominant; 3. Mixed Diagnosis: Rome II Criteria Treatment: 1.General treatment approach; 2. Pharmacological therapies 3.Psychological therapies 63
June By: Reza Gholami
 ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
IBS - Definition. Chronic functional disorder of GI generally characterized by:
 IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
IBS - Definition Chronic functional disorder of GI generally characterized by: 3500 3000 No. of Publications 2500 2000 1500 1000 Irritable Bowel syndrome Irritable Bowel Syndrome 500 0 1968-1977 1978-1987
... SELECTED ABSTRACTS...
 ... SELECTED ABSTRACTS... The following abstracts, from medical journals containing literature on irritable bowel syndrome, were selected for their relevance to this supplement. A Technical Review for
... SELECTED ABSTRACTS... The following abstracts, from medical journals containing literature on irritable bowel syndrome, were selected for their relevance to this supplement. A Technical Review for
Non-Ulcer Dyspepsia: what is it? What can we do with these patients? Overview. Dyspepsia Definition. Functional Dyspepsia. Dyspepsia the Basics
 Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Functional Dyspepsia. Norbert Welkovics Heine van der Walt
 Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Irritable Bowel Syndrome
 Irritable Bowel Syndrome Functional gastrointestinal disorders Definition A variable combination of chronic or recurrent gastrointestinal symptoms (attributed to the pharynx, esophagus, stomach, biliary
Irritable Bowel Syndrome Functional gastrointestinal disorders Definition A variable combination of chronic or recurrent gastrointestinal symptoms (attributed to the pharynx, esophagus, stomach, biliary
SUPPLEMENTARY INFORMATION Associated with
 Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Number of studies. Endoscopic finding. Number of subjects. Pooled prevalence 95% CI
 Clinical Approach to the Patient t with Dyspepsia William D. Chey, MD, FACG Professor of Medicine University of Michigan Prevalence of Endoscopic Findings in Individuals with Dyspepsia Systematic Review
Clinical Approach to the Patient t with Dyspepsia William D. Chey, MD, FACG Professor of Medicine University of Michigan Prevalence of Endoscopic Findings in Individuals with Dyspepsia Systematic Review
6/25/ % 20% 50% 19% Functional Dyspepsia Peptic Ulcer GERD Cancer Other
 Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Outline. Definition (s) Epidemiology Pathophysiology Management With an emphasis on recent developments
 Epidemiology Pathophysiology Management With an emphasis on recent developments") Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Functional Dyspepsia
 Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Definition, Pathogenesis, and Management of That Cursed Dyspepsia
 Clinical Gastroenterology and Hepatology 2018;16:467 479 Definition, Pathogenesis, and Management of That Cursed Dyspepsia Pramoda Koduru, Malcolm Irani, and Eamonn M. M. Quigley IM F1 김영기 Dyspepsia Umbrella
Clinical Gastroenterology and Hepatology 2018;16:467 479 Definition, Pathogenesis, and Management of That Cursed Dyspepsia Pramoda Koduru, Malcolm Irani, and Eamonn M. M. Quigley IM F1 김영기 Dyspepsia Umbrella
190 Index Case studies, abdominal pain, 2 Crohn s disease, 2 3, cyclic vomiting syndrome (CVS), 2 fecal incontinence (FI), 2 medical c
, 2 fecal incontinence (FI), 2 medical c") Index Abdominal pain, case study, 2 Achalasia, 75 Acupuncture 108 American Academy of Pediatrics, 49 Anxiety, 8 9, 98 Autism, GI disorders and, 25 27 BASC. See Behavior Assessment System for Children (BASC)
Index Abdominal pain, case study, 2 Achalasia, 75 Acupuncture 108 American Academy of Pediatrics, 49 Anxiety, 8 9, 98 Autism, GI disorders and, 25 27 BASC. See Behavior Assessment System for Children (BASC)
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514
 Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 History of Functional Disorders Douglas A. Drossman, MD Melissa Swantkowski THE PAST HISTORICAL PRECEDENTS Historians
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 History of Functional Disorders Douglas A. Drossman, MD Melissa Swantkowski THE PAST HISTORICAL PRECEDENTS Historians
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
Irritable Bowel Syndrome Now. George M. Logan, MD Friday, May 5, :35 4:05 PM
 Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
Irritable Bowel Syndrome Now George M. Logan, MD Friday, May 5, 2017 3:35 4:05 PM Dr. Logan indicated no potential conflict of interest to this presentation. He does not intend to discuss any unapproved/investigative
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA
 MANAGEMENT OF DYSPEPSIA") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
Functional Dyspepsia
 Linköping University Medical Dissertations No. 792 Functional Dyspepsia Symptoms and Response to Omeprazole in the Short Term by Elisabeth Bolling-Sternevald Department of Biomedicine and Surgery, Faculty
Linköping University Medical Dissertations No. 792 Functional Dyspepsia Symptoms and Response to Omeprazole in the Short Term by Elisabeth Bolling-Sternevald Department of Biomedicine and Surgery, Faculty
Rome III: an ongoing journey for better diagnosis and treatment of functional gastrointestinal disorders
 Mædica - a Journal of Clinical Medicine EDITORIALS Rome III: an ongoing journey for better diagnosis and treatment of functional gastrointestinal disorders Mircea DICULESCU, MD, Tudor ARBANAS, MD Gastroenterology
Mædica - a Journal of Clinical Medicine EDITORIALS Rome III: an ongoing journey for better diagnosis and treatment of functional gastrointestinal disorders Mircea DICULESCU, MD, Tudor ARBANAS, MD Gastroenterology
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders What are functional GI disorders?
 The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
The Use of Antidepressants in the Treatment of Irritable Bowel Syndrome and Other Functional GI Disorders Christine B. Dalton, PA-C Douglas A. Drossman, MD and Kellie Bunn, PA-C What are functional GI
PELVIC PAIN : Gastroenterological Conditions
 PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
PELVIC PAIN : Gastroenterological Conditions Departman Tarih Prof. A. Melih OZEL, MD Department of Gastroenterology Anadolu Medical Center Hospital Gebze Kocaeli - TURKEY Presentation plan 15 min. Introduction
IBS Irritable Bowel syndrome Therapeutics II PHCL 430
 Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
Salman Bin AbdulAziz University College Of Pharmacy IBS Irritable Bowel syndrome Therapeutics II PHCL 430 Email:- ahmedadel.pharmd@gmail.com Ahmed A AlAmer PharmD R.S is 32-year-old woman experiences intermittent
FUNCTIONAL DISORDERS ROME IV CRITERIA AND DIAGNOSTIC QUESTIONNAIRE DDW 2016,REVIEW. Presented by; Marjan Mokhtare Gastroenterologist, IUMS
 FUNCTIONAL DISORDERS ROME IV CRITERIA AND DIAGNOSTIC QUESTIONNAIRE DDW 2016,REVIEW Presented by; Marjan Mokhtare Gastroenterologist, IUMS Functional gastrointestinal disorders (FGIDs), the most common
FUNCTIONAL DISORDERS ROME IV CRITERIA AND DIAGNOSTIC QUESTIONNAIRE DDW 2016,REVIEW Presented by; Marjan Mokhtare Gastroenterologist, IUMS Functional gastrointestinal disorders (FGIDs), the most common
Irritable bowel syndrome (IBS) is a ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome
 is a ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome") ... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome Based on a presentation by Marvin M. Schuster, MD Presentation Summary Approximately 20% of the general population has irritable bowel
... PRESENTATION... Defining and Diagnosing Irritable Bowel Syndrome Based on a presentation by Marvin M. Schuster, MD Presentation Summary Approximately 20% of the general population has irritable bowel
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
The Role of Food in the Functional Gastrointestinal Disorders
 The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
The Role of Food in the Functional Gastrointestinal Disorders H. Vahedi, MD. Gastroentrologist Associate professor of medicine DDRI 92.4.27 vahedi@ams.ac.ir Disorder Sub-category A. Oesophageal disorders
UKLIN1693a, date of preparation: March 2013.
 1 This table shows the ICE model. Defining the patient s ideas, concerns, and expectations is an important part of the consultation that can lead to better outcomes. 2 Patients with IBS may have visceral
1 This table shows the ICE model. Defining the patient s ideas, concerns, and expectations is an important part of the consultation that can lead to better outcomes. 2 Patients with IBS may have visceral
Dyspepsia is a problem commonly seen by primary
 Concise Review for Clinicians Nonulcer Dyspepsia: What It Is and What It Is Not G. RICHARD LOCKE III, MD Nonulcer dyspepsiais a description of persistent or recurrent upper abdominal pain or discomfort
Concise Review for Clinicians Nonulcer Dyspepsia: What It Is and What It Is Not G. RICHARD LOCKE III, MD Nonulcer dyspepsiais a description of persistent or recurrent upper abdominal pain or discomfort
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
What you really need to know about Gastroparesis?
 What you really need to know about Gastroparesis? John M. Wo, MD Division of Gastroenterology/Hepatology Director of GI Motility and Neurogastroenterology 8/3/2016 1/4/2017 1 What you really need to know
What you really need to know about Gastroparesis? John M. Wo, MD Division of Gastroenterology/Hepatology Director of GI Motility and Neurogastroenterology 8/3/2016 1/4/2017 1 What you really need to know
Chronic Abdominal Pain. Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016
 Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Chronic Abdominal Pain Dr. Robert B. Smith Tupelo Digestive Health Specialists August 26, 2016 Disclosures Speaker Bureau for Allergan Pharmaceuticals Abdominal Pain - Definitions Acute occurring for several
Gut involvement in PoTS an overview
 Gut involvement in PoTS an overview Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology Case Hx * 28 year old lady presents with a long hx of constipation
Gut involvement in PoTS an overview Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology Case Hx * 28 year old lady presents with a long hx of constipation
Disclosures. GI Motility Disorders. Gastrointestinal Motility Disorders & Irritable Bowel Syndrome
 Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514
 Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 Normal Gastrointestinal Motility and Function "Motility" is an unfamiliar word to many people; it is used primarily
Drossman Gastroenterology 55 Vilcom Center Drive Boyd Hall, Suite 110 Chapel Hill, NC 27514 Normal Gastrointestinal Motility and Function "Motility" is an unfamiliar word to many people; it is used primarily
A Guide to Gastrointestinal Motility Disorders
 A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord André Smout Jan Tack A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord Gastroenterology and Hepatology Academic Medical
A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord André Smout Jan Tack A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord Gastroenterology and Hepatology Academic Medical
Functionele Maagdarmklachten als Stoornissen van Gut-Brain Interacties Leiden alle wegen naar Rome IV?
 Functionele Maagdarmklachten als Stoornissen van Gut-Brain Interacties Leiden alle wegen naar Rome IV? Lukas Van Oudenhove, MD, PhD Assistant Professor (KU Leuven Special Research Fund) Laboratory for
Functionele Maagdarmklachten als Stoornissen van Gut-Brain Interacties Leiden alle wegen naar Rome IV? Lukas Van Oudenhove, MD, PhD Assistant Professor (KU Leuven Special Research Fund) Laboratory for
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Presenter. Irritable Bowel Syndrome. Objectives. Introduction. Rome Criteria. Irritable Bowel Syndrome 2/28/2018
 Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
Presenter Irritable Bowel Syndrome Current evidence for diagnosis & management Julie Daniels DNP, CNM Assistant Professor Course Coordinator of Primary Care of Women Faculty at Frontier Nursing University
MANAGEMENT OF VISCERAL PAIN
 MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
IBS: overview and assessment of pain outcomes and implications for inclusion criteria
 IBS: overview and assessment of pain outcomes and implications for inclusion criteria William D. Chey, MD Professor of Medicine University of Michigan What is the Irritable Bowel Syndrome Symptom based
IBS: overview and assessment of pain outcomes and implications for inclusion criteria William D. Chey, MD Professor of Medicine University of Michigan What is the Irritable Bowel Syndrome Symptom based
Why does my stomach hurt? Exploring irritable bowel syndrome
 Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
Why does my stomach hurt? Exploring irritable bowel syndrome By Flavio M. Habal, MD, PhD, FRCPC Case In this article: 1. What is IBS? A 45-year-old female is referred to your office with recurrent 2. How
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
IRRITABLE BOWEL SYNDROME
 c IRRITABLE BOWEL SYNDROME Success is no accident. It is hard work, perseverance, learning, studying, sacrifice and most of all, love of what you are doing or learning to do. Color code Important doctor
c IRRITABLE BOWEL SYNDROME Success is no accident. It is hard work, perseverance, learning, studying, sacrifice and most of all, love of what you are doing or learning to do. Color code Important doctor
ABDOMINAL PAIN, CHRONIC
 Introduction Incidence Aetiology Clinical Assessment Formulation Investigations Management Prognosis Conclusion References Introduction The generally accepted definition of this condition is three or more
Introduction Incidence Aetiology Clinical Assessment Formulation Investigations Management Prognosis Conclusion References Introduction The generally accepted definition of this condition is three or more
Digestion. Text. What You Don t Know Can Hurt You!
 Digestion Text What You Don t Know Can Hurt You! Digestive Problems Approximately 36.5 million visits annually to ambulatory care facilities due to the diseases of the digestive system Over 4 million ulcers
Digestion Text What You Don t Know Can Hurt You! Digestive Problems Approximately 36.5 million visits annually to ambulatory care facilities due to the diseases of the digestive system Over 4 million ulcers
Is one of the most common chronic disorders. causing patients to seek medical treatment.
 ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
ILOs After this lecture you should be able to : Define IBS Identify causes and risk factors of IBS Determine the appropriate therapeutic options for IBS Is one of the most common chronic disorders causing
At the outset, we want to clear up some terminology issues. IBS is COPYRIGHTED MATERIAL. What Is IBS?
 1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
1 What Is IBS? At the outset, we want to clear up some terminology issues. IBS is the abbreviation that doctors use for irritable bowel syndrome, often when they are talking about people with IBS. We will
IBS. Patient INFO. A Guide to Irritable Bowel Syndrome
 Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
Patient INFO IBS A Guide to Irritable Bowel Syndrome The information provided by the AGA Institute is not medical advice and should not be considered a replacement for seeing a medical professional. About
Entrustable Professional Activity
 Entrustable Professional Activity 1. Title: Care for infants, children, and adolescents with common outpatient GI, liver/biliary, pancreatic and nutritional issues 2. Description of Activity Pediatric
Entrustable Professional Activity 1. Title: Care for infants, children, and adolescents with common outpatient GI, liver/biliary, pancreatic and nutritional issues 2. Description of Activity Pediatric
The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia. Disclosures
 The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia Lana Bistritz MD FRCPC Royal Alexandra Hospital GI Update 2016 Disclosures I have no relevant financial disclosures I will be discussing off
The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia Lana Bistritz MD FRCPC Royal Alexandra Hospital GI Update 2016 Disclosures I have no relevant financial disclosures I will be discussing off
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders. TERRAGASTRO - Good health starts in the gut
 Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
Clinically proven to quickly relieve symptoms of common gastrointestinal disorders GASTROINTESTINAL DISEASE Referred to as gastrointestinal diseases, they are common disorders which affect the esophagus,
An approach to dyspepsia for the pharmacist
 An approach to dyspepsia for the pharmacist Ilse Truter, DCom, BPharm, MSc, PhD, Drug Utilization Research Unit (DURU) Department of Pharmacy, Nelson Mandela Metropolitan University Correspondence to:
An approach to dyspepsia for the pharmacist Ilse Truter, DCom, BPharm, MSc, PhD, Drug Utilization Research Unit (DURU) Department of Pharmacy, Nelson Mandela Metropolitan University Correspondence to:
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Objectives. Identify age-related changes in the gastrointestinal tract
 The Primary Care Physician s Approach to Gastrointestinal Complaints in the Elderly Brian Viviano, D.O. Medical Associates of Erie Objectives Identify age-related changes in the gastrointestinal tract
The Primary Care Physician s Approach to Gastrointestinal Complaints in the Elderly Brian Viviano, D.O. Medical Associates of Erie Objectives Identify age-related changes in the gastrointestinal tract
Zelmac Learning System: Module 2
 Learning Objectives Zelmac Learning System: Module 2 Overview of Gastrointestinal Disorders 2-1 Learning Objectives Recognize that a variety of GI conditions can cause symptoms similar to those present
Learning Objectives Zelmac Learning System: Module 2 Overview of Gastrointestinal Disorders 2-1 Learning Objectives Recognize that a variety of GI conditions can cause symptoms similar to those present
There are clues to help to decide if the bellyache is a medical problem:
 Bellyaches in Children Pediatric and Adolescent Gastrointestinal Motility & Pain Program Department of Pediatrics, Louisiana State University Health Sciences Center, New Orleans, Louisiana By: Paul Hyman,
Bellyaches in Children Pediatric and Adolescent Gastrointestinal Motility & Pain Program Department of Pediatrics, Louisiana State University Health Sciences Center, New Orleans, Louisiana By: Paul Hyman,
Management of Functional Dyspepsia (FD)
") Management of Functional Dyspepsia (FD) Amy S. Oxentenko, MD, FACG Program Director and Associate Chair, IM Associate Professor of Medicine Mayo Clinic, Rochester Outline Define functional dyspepsia (FD)
Management of Functional Dyspepsia (FD) Amy S. Oxentenko, MD, FACG Program Director and Associate Chair, IM Associate Professor of Medicine Mayo Clinic, Rochester Outline Define functional dyspepsia (FD)
Our evidence. Your expertise. SmartPill : The data you need to evaluate motility disorders.
 Our evidence. Your expertise. SmartPill : The data you need to evaluate motility disorders. SmartPill benefits your practice: Convenient performed right in your office Test standardization Provides direct
Our evidence. Your expertise. SmartPill : The data you need to evaluate motility disorders. SmartPill benefits your practice: Convenient performed right in your office Test standardization Provides direct
Gastrointestinal Society 2016 SURVEY RESULTS
 Gastrointestinal Society 2016 SURVEY RESULTS Irritable Bowel Syndrome (IBS) The GI (Gastrointestinal) Society represents Canadians living with gastrointestinal diseases and disorders including those who
Gastrointestinal Society 2016 SURVEY RESULTS Irritable Bowel Syndrome (IBS) The GI (Gastrointestinal) Society represents Canadians living with gastrointestinal diseases and disorders including those who
The Risk Factors and Quality of Life in Patients with Overlapping Functional Dyspepsia or Peptic Ulcer Disease with Gastroesophageal Reflux Disease
 Gut and Liver, Vol. 8, No. 2, March 2014, pp. 160-164 ORiginal Article The Risk Factors and Quality of Life in Patients with Overlapping Functional Dyspepsia or Peptic Ulcer Disease with Gastroesophageal
Gut and Liver, Vol. 8, No. 2, March 2014, pp. 160-164 ORiginal Article The Risk Factors and Quality of Life in Patients with Overlapping Functional Dyspepsia or Peptic Ulcer Disease with Gastroesophageal
HELICOBACTER PYLORI; PATIENTS WITH FUNCTIONAL DYSPEPSIA
 The Professional Medical Journal www.theprofesional.com ORIGINAL PROF-2404 1. Associate Professor and Health Sciences, (LUMHS) 2. MD, Consultant Physician,, Medical-III, Ward 06 Liaquat University Hospital,
The Professional Medical Journal www.theprofesional.com ORIGINAL PROF-2404 1. Associate Professor and Health Sciences, (LUMHS) 2. MD, Consultant Physician,, Medical-III, Ward 06 Liaquat University Hospital,
Throughout recorded history, and alongside structural
 GASTROENTEROLOGY 2006;130:1377 1390 INTRODUCTION The Functional Gastrointestinal Disorders and the Rome III Process DOUGLAS A. DROSSMAN, Guest Editor Division of Gastroenterology and Hepatology, UNC Center
GASTROENTEROLOGY 2006;130:1377 1390 INTRODUCTION The Functional Gastrointestinal Disorders and the Rome III Process DOUGLAS A. DROSSMAN, Guest Editor Division of Gastroenterology and Hepatology, UNC Center
F unctional gastrointestinal disorders (FGID) are clinical
 are clinical") 1445 IRRITABLE BOWEL SYNDROME Symptom patterns in functional dyspepsia and irritable bowel syndrome: relationship to disturbances in gastric emptying and response to a nutrient challenge in consulters
1445 IRRITABLE BOWEL SYNDROME Symptom patterns in functional dyspepsia and irritable bowel syndrome: relationship to disturbances in gastric emptying and response to a nutrient challenge in consulters
J Neurogastroenterol Motil, Vol. 17 No. 3 July, 2011 DOI: /jnm Journal of Neurogastroenterology and Motility
 ㅋ JNM J Neurogastroenterol Motil, Vol. 17 No. 3 July, 2011 DOI: 10.5056/jnm.2011.17.3.279 Journal of Neurogastroenterology and Motility Original Article Functional Gastrointestinal Disorders Diagnosed
ㅋ JNM J Neurogastroenterol Motil, Vol. 17 No. 3 July, 2011 DOI: 10.5056/jnm.2011.17.3.279 Journal of Neurogastroenterology and Motility Original Article Functional Gastrointestinal Disorders Diagnosed
Amyloidosis & the GI Tract
 Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
Treat primary. symptoms. Offer general lifestyle advice. Manage IBS according to the dominant symptom. Follow up. Symptoms do not improve
 Treat primary symptoms Background information for clinicians Offer general lifestyle advice Background information for patients Manage IBS according to the dominant symptom Provenance Psychological symptoms
Treat primary symptoms Background information for clinicians Offer general lifestyle advice Background information for patients Manage IBS according to the dominant symptom Provenance Psychological symptoms
Weekly Prevalence of Symptoms USA vs. Colombia
 THE OVERLAP BETWEEN INFLAMMATORY BOWEL DISEASE AND FUNCTIONAL GASTROINTESTINAL DISORDERS: CHALLENGES AND TREATMENT IMPLICATIONS Miguel Saps, MD Professor of Pediatrics, Ohio State University Director of
THE OVERLAP BETWEEN INFLAMMATORY BOWEL DISEASE AND FUNCTIONAL GASTROINTESTINAL DISORDERS: CHALLENGES AND TREATMENT IMPLICATIONS Miguel Saps, MD Professor of Pediatrics, Ohio State University Director of
FUNCTIONAL GASTROINTESTINAL DISORDERS: RELATIONS BETWEEN PSYCHOSOCIAL FACTORS, SYMPTOMS AND SENSORIMOTOR DISTURBANCE
 FUNCTIONAL GASTROINTESTINAL DISORDERS: RELATIONS BETWEEN PSYCHOSOCIAL FACTORS, SYMPTOMS AND SENSORIMOTOR DISTURBANCE ETHELLE JEANETTE BENNETT BA (HONS) A thesis submitted in fulfilment of the requirements
FUNCTIONAL GASTROINTESTINAL DISORDERS: RELATIONS BETWEEN PSYCHOSOCIAL FACTORS, SYMPTOMS AND SENSORIMOTOR DISTURBANCE ETHELLE JEANETTE BENNETT BA (HONS) A thesis submitted in fulfilment of the requirements
Constipation An Overview. Definition Physiology of GI tract Etiology Assessment Treatment
 CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
CONSTIPATION Constipation An Overview Definition Physiology of GI tract Etiology Assessment Treatment Definition Constipation = the infrequent passage of hard feces Definition of Infrequent The meaning
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Chapter 34. Nursing Care of Patients with Lower Gastrointestinal Disorders
 Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
Chapter 34 Nursing Care of Patients with Lower Gastrointestinal Disorders Lower Gastrointestinal System Small Intestines Large Intestines Rectum Anus Constipation Fecal Mass Held In Rectum Feces Become
GI Complications in heds and HSD
 GI Complications in heds and HSD Qasim Aziz PhD, FRCP Professor in Neurogastroenterology Neurogastroenterology Group GUT = Gastrointestinal (GI) tract Oesophagus / gullet Gastro-oesophageal junction Stomach
GI Complications in heds and HSD Qasim Aziz PhD, FRCP Professor in Neurogastroenterology Neurogastroenterology Group GUT = Gastrointestinal (GI) tract Oesophagus / gullet Gastro-oesophageal junction Stomach
Functional dyspepsia: recent advances in pathophysiology. Citation Hong Kong Practitioner, 1998, v. 20 n. 6, p
 Title Functional dyspepsia: recent advances in pathophysiology Author(s) Hu, HC; Lam, SK Citation Hong Kong Practitioner, 1998, v. 20 n. 6, p. 327-334 Issued Date 1998 URL http://hdl.handle.net/10722/45089
Title Functional dyspepsia: recent advances in pathophysiology Author(s) Hu, HC; Lam, SK Citation Hong Kong Practitioner, 1998, v. 20 n. 6, p. 327-334 Issued Date 1998 URL http://hdl.handle.net/10722/45089
OPERATIVE TREATMENT OF ULCER DISEASE
 Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Low FODMAP Dietary Approach For FGD/IBS. Our Experience. Charlotte McCamphill 19 th February 2015
 Low FODMAP Dietary Approach For FGD/IBS Our Experience Charlotte McCamphill 19 th February 2015 CONTENTS What Is IBS What are FODMAPs Service Provision Audit Results Future Work WHAT IS IBS The Rome III
Low FODMAP Dietary Approach For FGD/IBS Our Experience Charlotte McCamphill 19 th February 2015 CONTENTS What Is IBS What are FODMAPs Service Provision Audit Results Future Work WHAT IS IBS The Rome III
Human Anatomy rectum
 rectum The colon is also called the large intestine. The ileum (last part of the small intestine) connects to the cecum (first part of the colon) in the lower right abdomen. The rest of the colon is divided
rectum The colon is also called the large intestine. The ileum (last part of the small intestine) connects to the cecum (first part of the colon) in the lower right abdomen. The rest of the colon is divided
University Medical Center at Brackenridge. Gastroenterology Clinic Worksheet
 Gastroenterology Clinic Worksheet 1. GI Bleeding (occult or symptomatic) a. CBC b. Iron, Ferritin b. Medication history 2. Iron Deficiency Anemia and no evident source (if no iron deficiency consider hematological
Gastroenterology Clinic Worksheet 1. GI Bleeding (occult or symptomatic) a. CBC b. Iron, Ferritin b. Medication history 2. Iron Deficiency Anemia and no evident source (if no iron deficiency consider hematological
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider
 For the Primary Care Provider") Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Diagnosis and Management of Irritable Bowel Syndrome (IBS) For the Primary Care Provider Elizabeth Coss, MD General Gastroenterologist Audie Murphy Veterans Hospital UT Health This presentation does not
Bowel cancer risk in the under 50s. Greg Rubin Professor of General Practice and Primary Care
 Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Bowel cancer risk in the under 50s Greg Rubin Professor of General Practice and Primary Care Prevalence of GI problems in the consulting population Thompson et al, Gut 2000 Number of patients % of patients
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP
 Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology GI involvement in autonomic dysfunction Conditions Diabetes
Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology GI involvement in autonomic dysfunction Conditions Diabetes
IBS. Dan Carter, M.D. Institute of Gastroenterology Sheba medical center
 IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort
IBS Dan Carter, M.D. Institute of Gastroenterology Sheba medical center Epidemiology Irritable bowel syndrome is a common functional gastrointestinal disorder that manifests as abdominal pain or discomfort
GASTROPARESIS. C. Prakash Gyawali, MD Professor of Medicine Washington University in St. Louis
 GASTROPARESIS C. Prakash Gyawali, MD Professor of Medicine Washington University in St. Louis Symptom Definitions Nausea: a subjective feeling of wanting to vomit Vomiting: forceful expulsion of gastroduodenal
GASTROPARESIS C. Prakash Gyawali, MD Professor of Medicine Washington University in St. Louis Symptom Definitions Nausea: a subjective feeling of wanting to vomit Vomiting: forceful expulsion of gastroduodenal
Microbiome GI Disorders
 Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
Microbiome GI Disorders Prof. Ram Dickman Neurogastroenterology Unit Rabin Medical Center Israel 1 Key Points Our gut microbiota Were to find them? Symbiosis or Why do we need them? Dysbiosis or when things
HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON
 HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON Indigestion is a condition that is often a symptom of another, underlying condition and is associated with various forms of discomfort in the stomach including
HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON Indigestion is a condition that is often a symptom of another, underlying condition and is associated with various forms of discomfort in the stomach including
Chapter 1. General introduction and outline
 Chapter 1 General introduction and outline General introduction The function of the stomach comprises storage of ingested food, production of gastric secretion and mixing food with gastric secretion,
Chapter 1 General introduction and outline General introduction The function of the stomach comprises storage of ingested food, production of gastric secretion and mixing food with gastric secretion,
2.08 Understand the functions and disorders of the digestive system Essential questions
 2.08 Understand the functions and disorders of the digestive system Essential questions What are the functions of the digestive system? How do the functions of chemical and physical digestion interrelate?
2.08 Understand the functions and disorders of the digestive system Essential questions What are the functions of the digestive system? How do the functions of chemical and physical digestion interrelate?
What is Irritable Bowel Syndrome (IBS)?
?") What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
What is Irritable Bowel Syndrome (IBS)? Irritable bowel syndrome (IBS) is a health issue found in your intestines (gut). IBS can cause symptoms such as: Belly pain. Cramping. Gas. Bloating (or swelling)
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics. Dr. Alia Shatanawi
 GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
GI Pharmacology -4 Irritable Bowel Syndrome and Antiemetics Dr. Alia Shatanawi 11-04-2018 Drugs used in Irritable Bowel Syndrome Idiopathic, chronic, relapsing disorder characterized by abdominal discomfort
Irritable Bowel Syndrome. Mustafa Giaffer March 2017
 Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Irritable Bowel Syndrome Mustafa Giaffer March 2017 Introduction First described in 1771. 50% of patients present
Primary Management of Irritable Bowel Syndrome
 Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
Primary Management of Irritable Bowel Syndrome Jasmine Zia, MD Acting Instructor, Division of Gastroenterology Current Concepts in Drug Therapy CME Course April 23, 2015 Irritable Bowel Syndrome (IBS)
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome. Dr Miranda Lomer RD.
 The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
The long-term impact of the low-fodmap diet for management of irritable bowel syndrome Dr Miranda Lomer RD Email: miranda.lomer@kcl.ac.uk What is IBS - ROME IV Criteria A functional bowel disorder in which
Peripheral and central factors in the pathophysiology of irritable bowel syndrome
 Section of Gastroenterology and Hepatology Department of Internal Medicine Sahlgrenska University Hospital Göteborg University Göteborg, Sweden Peripheral and central factors in the pathophysiology of
Section of Gastroenterology and Hepatology Department of Internal Medicine Sahlgrenska University Hospital Göteborg University Göteborg, Sweden Peripheral and central factors in the pathophysiology of
IBS and Functional GI Disorders (FGIDs)
") Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/ibs-and-functional-gi-disorders-fgids/7424/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/gi-insights/ibs-and-functional-gi-disorders-fgids/7424/