Rational Approach to Treating Low Back Pain
|
|
|
- Madlyn Oliver
- 5 years ago
- Views:
Transcription
1 Rational Approach to Treating Low Back Pain Susie Jang, MD Department of Anesthesia, Critical Care & Pain Medicine Beth Israel Deaconess Medical Center Instructor, Harvard Medical School
2 Learning Objectives Overview, impact of low back pain Identification of patients at risk of developing chronic LBP Initial encounter and development of a structured plan for work-up Incorporate a rational and evidence-based approach of available treatments Obtaining timely referral to pain management and surgical specialists
3 OVERVIEW AND EPIDEMIOLOGY

4 Everyone Gets Back Pain Back pain and related symptoms 2 nd most frequent complaints for PCP visits 5 th most common reason for all physician visits Second only to common cold as cause of lost work time In the U.S., lifetime prevalence approximately 80%, one-year prevalence 15% - 20% 90% - non emergent causes 85% - no exact diagnosis Highest prevalence between 45 to 64 age group Most common cause of disability in < 45 years old
5
6 Back Pain is Expensive Total cost of back pain in US $253 billion per year (2011) $150.4 billion - hospital treatment cost (2011) 291 million lost work days per year (2012) Ranked highest for cause of disability worldwide (WHO, Global Burden of Disease Survey 2010) Spinal fusion - 6th most common OR procedure, most expensive in 2011 (Agency for Healthcare Research and Quality 2014) Medical Expenditures Panel Survey (MEPS), Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services, National Health Interview Survey (NHIS)_Adult sample,

7 Back Pain Context 307% 423% 629% 220% Deyo RA, et al. Overtreating Chronic Back Pain: Time to Back Off? Journal of the American Board of Family Medicine. 2009;22(1):62-68.
8 Deyo RA, et al. Overtreating Chronic Back Pain: Time to Back Off? Journal of the American Board of Family Medicine. 2009;22(1):62-68.
9 Most Disability Improves with Time 85% return to work after short episodes of acute LBP
10 But Some People Never Get Better Recovery after 12 weeks slow, uncertain Disabled for 6 month: < 50% return to work Disabled for 1 year: 25% After 2 years absence from work: approaches 0%
11 Chronicity of Low Back Pain Acute: 2-4 weeks Subacute: up to 12 weeks Chronic: > 12 weeks 75-90% of patients with acute LBP in primary care improve within 1 month Exact etiology of acute LBP is identifiable in only 15% of patients
12 Predictors of Pain Chronicity Protective: College education Risk: Unemployed Radiating/wide spread pain, radicular pain Inability to walk for an hour Insomnia, sleep disturbance Catastrophizing Kinesiophobia Tobacco use
13 INITIAL EVALUATION
14 Initial Encounter Thorough history of pain complaint Onset Location, radiation Aggravating factors Alleviating factors Other health or pain problems Cancer history Psych history
15 DIFFERENTIAL DIAGNOSIS & WORKUP
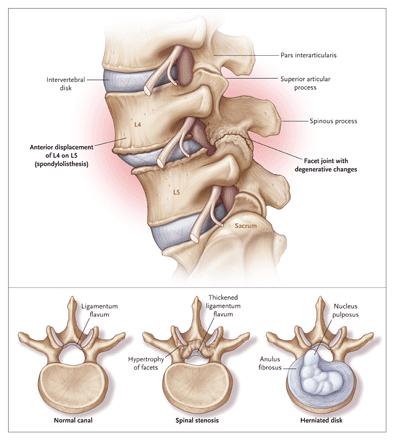
16 Etiologies of Low Back Pain Musculoligamentous injuries Intervertebral disks and facet joints degeneration Herniation of the nucleus pulposus of an intervertebral disk Spinal stenosis Anatomic anomalies of the spine: scoliosis, spondylolisthesis Underlying systemic diseases Primary or metastatic cancer Spinal infections Ankylosing spondylitis Visceral diseases unrelated to the spine Pelvic organs Kidneys Gastrointestinal tract/pancreas Aorta
17 Prevalence of Multiple Etiologies Musculoligamentous injury or degenerative changes - 85% Lumbar spinal stenosis % (incr with age, imaging) Compression fractures - 4% Spondylolisthesis - 3% Spinal malignant neoplasms (primary or metastatic) - 0.7% Ankylosing spondylitis - 0.3% Spinal infections %

18
19
20 Rule Out Cancer Primary or metastatic 80% of patients with cancer as cause > 50 years old Previous history of cancer = cause of pain until proven otherwise Common metastatic: Breast, lung, prostate, lymphoma, renal cell, GI, melanoma Symptomatic due to bone pain, pathologic compression fractures, extension into spinal canal

21
22 Rule out Cancer - continued Symptoms: Unexplained weight loss Pain lasting >1 month Not responsive to conservative therapy Not relieved by rest Physical exam: Spinal tenderness: specific, varied sensitivity Neuromuscular: weakness, atrophy, reflex changes, sensory deficits high specificity Muscle spasm, radiculopathy, Babinski s sign, urinary retention poor sensitivity

23 Spinal Infections While rarely seen, very important to rule out: Blood borne from other sites: UTI, IVDA, skin infections Sx: Fever, diaphoresis, localized spine tenderness


24 . Cauda Equina Syndrome
25 Cauda Equina Syndrome RED FLAGS Severe low back pain (LBP) Radicular pain: often bilateral but sometimes absent, especially at L5/S1 with an inferior sequestration Saddle and/or genital sensory disturbance Bladder, bowel and sexual dysfunction Needs urgent surgical evaluation Eur Spine J May; 20(5):
26 Cauda Equina Syndrome Incomplete: neurogenic urinary difficulties altered urinary sensation loss of desire to void poor urinary stream need to strain in order to micturate saddle and genital sensory deficit often unilateral or partial; trigone sensation should be present. Complete: painless urinary retention and overflow incontinence bladder no longer under executive control. usually extensive or complete saddle and genital sensory deficit with deficient trigone sensation. Eur Spine J May; 20(5):
27 Compression Fractures Although not "systemic" diseases, often with generalized osteoporosis Most patients DO NOT have a history of identifiable trauma Back pain with long-term corticosteroid therapy should prompt consideration of compression fracture African-American and Mexican-American women have only one fourth as many compression fractures as white women Age > 70 years is relatively specific
28
29 TLICS: Thoracolumbar Injury Classification and Severity Score Morphology: immediate stability, XR/CT compression fracture - 1 point burst fracture - 2 points translational rotational injury - 3 points distraction injury - 4 points Posterior ligamentous complex: long term stability, MRI intact - 0 points suspected injury or indeterminate - 2 points injured - 3 points Neurologic involvement: Physical exam intact - 0 points nerve root - 2 points cord/conus medullaris (complete) - 2 points cord/conus medullaris (incomplete) - 3 points cauda equina - 3 points
30 TLICS cont. Based on total points, help determine plan based on co-morbidities and injury 0-3: usually treated non-operatively 4: surgeon's choice, +/- OR >4: usually treated operatively J Orthop Sci Nov; 10(6):

31 Is There Evidence of Neurologic Compromise? Radicular Pain?
32 Radicular Pain Overview Pathology affecting spinal cord, cauda equina, nerve roots Most common cause: herniated intervertebral disk Nerve root entrapment in the root canals due to bony and ligamentous hypertrophy spinal stenosis spinal or paraspinal infections cancer Present as motor, reflex, or sensory dysfunction in the lower extremities, bowel or bladder dysfunction If only low back pain, no radicular pain or neurologic symptoms, prevalence of neurological impairments is so low that extensive neurological evaluation is usually unnecessary.



33 SPINE Volume 26, Number 5, pp E93 E113

34 Lumbar Disc Herniation Radicular pain: high sensitivity - absence makes a clinically important lumbar disk herniation unlikely With significant disc herniation, leg pain > back pain Peak incidence occurs between the ages of 30 and 55 years


35 Lumbar Disc Herniation cont. Symptomatic disk herniation tethers the affected nerve root Most common levels: L4-5, L5-S1 Pain from stretching the nerve = straight leg test Positive straight leg sign = reproduces pain between 30 and 60 of leg elevation Crossed straight leg sign = straight leg raising is performed on contralateral leg, reproducing pain Less sensitive, but highly specific

36 Dermatomes and Myotomes Level Sensory Motor L2-3 Anteromedial thigh Hip flexion L4 Medial Malleolus Dorsiflexion foot L5 Web space b/w 1st and 2nd toes 1 st toe flexion S1 Lateral foot and sole Plantar flexion


37 Spinal Stenosis
38 Spinal Stenosis Characteristic history = neurogenic claudication Pain in the legs and occasionally neurologic deficits after walking Symptomatic while standing, may increase with cough/sneeze Normal arterial pulses compared to vascular claudication Increased pain on spine extension is typical of stenosis vs. flexion is usually most painful with herniated disks Walking uphill is easier than walking down hill Walking with walker or shopping cart easier, forward flexion.
39 Location of pain Neurogenic Thighs, calves, back and rarely buttocks Vascular Buttocks or calves Quality of pain Burning, cramping Cramping Aggravating Relieving Erect position, ambulation Squatting, bending forward, sitting Leg Pulses and BP Usually normal Skin / Trophic changes Usually absent Leg exercises Rest Decreased BP and pulses Often present (pallor, cyanosis, less hair)
40 Axial Low Back Pain Pain limited to the area of the lumbo-sacral junction Facet arthropathy 15% Degenerative disc disease 40% Sacroiliac arthropathy 15% Schwarzer et al 1993
41 Low Back Pain - Multifactorial Spine 65% 7.5% 8% 1.5% SI Joint 5% 0.5% Hip 2.5%

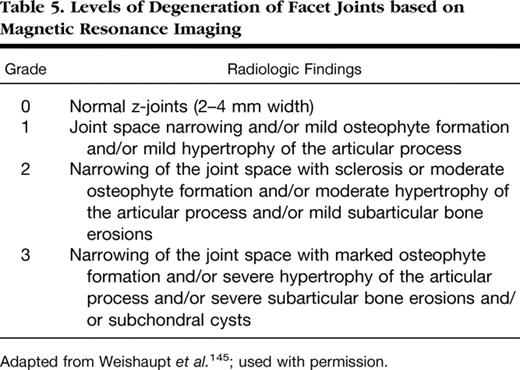
42 Facet Arthropathy Anesthesiology , Vol.106,


43 Facet Arthropathy
44
45 When to order imaging Choosing Wisely initiative ABIM ASA/ACP/AAFP: Avoid in first 6 weeks, unless red flags, concerning history History of cancer AAA Progressive neuro deficit Concern for infection Avoid cost, exposure to radiation Imaging without history/exam does not improve outcome and increases cost

46 Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening Trends in the Management and Treatment of Back Pain. JAMA Intern Med.2013;173(17):
47 TREATMENT
48 Analgesics NSAIDS 1 st line Muscle relaxants Anticonvulsants Antidepressants Opioids Chou R, Qaseem A, Snow V, Casey D, Cross JT, Shekelle P, et al. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:

49
50 LBP and Opioids Retrospective cohort study of WC claims with acute disabling LBP Objective: examine the association between early opioid use for acute LBP and outcomes at 2 years Sample: 8443 claimants from 1/ /2003 Conclusion: Opioids counterproductive to recover Longer length of disability More costs Increased risk of surgery Ongoing opioid use Webster et al. Relationship between early opioid prescribing for acute occupational low back pain and disability duration, medical costs, subsequent surgery and late opioid use. Spine 2007 Sep 1;32(19):
51 Opioids Have Clear Disadvantages A systematic review found aberrant drug-taking behaviors in up to 24% patients prescribed opioids for LBP May be appropriate for short-term use for severe, acute exacerbations; use with caution for long-term treatment of chronic LBP Should restrict to patients not highly vulnerable to drug dependence, abuse, addiction Chou R, et al. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:
52 Characteristics of Initial Prescription Episodes and Likelihood of Long-Term Opioid Use United States, Early opioid prescribing for opioid-naive patients associated with longterm use Chances of chronic use starts to increase after 3rd day supplied, rapid rise thereafter Sharpest increase after 5th and 31st day of therapy 2nd Rx or refill 700 MME cumulative dose Initial 10 or 30 day supply Highest probability of continued use at 1 and 3 years Started on long acting opioid Tramadol Shah A, Hayes CJ, Martin BC. Characteristics of Initial Prescription Episodes and Likelihood of Long-Term Opioid Use United States, MMWR Morb Mortal Wkly Rep 2017;66:
53


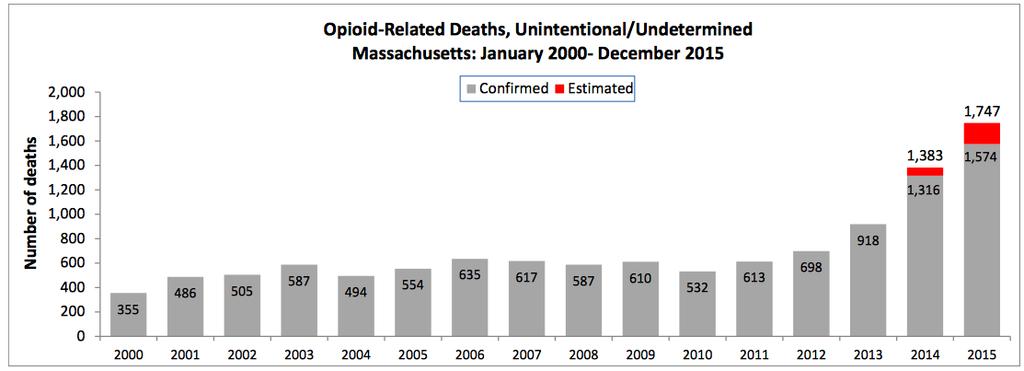
54 National Overdose Deaths Number of Deaths from Prescription Opioid Pain Relievers 20,000 Total Female Male 15,000 10,000 5,000 0 Source: National Center for Health Statistics, CDC Wonder
55
56
57 CDC Guideline - Opioids for Chronic Pain Use non-opioid therapies Exercise Cognitive behavioral therapy Non-opioid pharmacologic therapies, ie. NSAIDS Start low and go slow lowest possible effective dose start with IR vs. ER/long-activing smallest quantity Follow-up regularly monitor determine if benefit > harm; if not, work to taper/discontinue Dowell D, Haegerich TM, Chou R. CDC Guideline for Prescribing Opioids for Chronic Pain United States, MMWR Recomm Rep 2016;65(No. RR-1):1 49
58 NSAIDS and Acetaminophen NSAIDS effective for short-term symptom relief for acute and chronic low back pain Effect size small Exposure to selective COX-2 inhibitors - risk of MI APAP ineffective on both pain and disability outcomes for LBP in immediate and short term Not clinically superior to placebo on both pain and disability outcomes for osteoarthritis Roelofs PD, Deyo RA, et al. Nonsteroidal anti-inflammatory drugs for low back pain: an updated Cochrane review. Spine (Phila Pa 1976) Jul 15;33(16): Machado GC, et al. Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials BMJ 2015; 350 :h1225\
59 Antidepressants No difference between antidepressant and placebo for LBP, no difference between types of antidepressants Associated with higher risk of adverse events vs. placebo drowsiness dry mouth dizziness Because of questionable benefits and known side effects, tricyclic antidepressants, SNRIs are not a first-line option Chou R, et al. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:
60 Muscle Relaxants No difference in short-term muscle spasm between cyclobenzaprine and placebo Skeletal muscle relaxants may be considered as adjunctive therapy to analgesics in patients with acute exacerbations of chronic low back pain Chou R, et al. Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:
61 Benzodiazepines Tetrazepam (not available in US) more effective than placebo for short-term pain intensity after 5 to 7 days and overall improvement Only trial evaluating BZDs used in US, no difference between diazepam and placebo for muscle spasm Limited evidence on efficacy and potential for addiction and abuse - BZDs should not be used for long-term treatment of chronic low back pain Chou et al, Annals of Internal Medicine Volume 147 Number 7
62 Gabapentin Small, statistically significant improvements in pain with movement and leg pain, titrated to 1200 mg/day mg/day more effective than placebo, but lacked a double-blind design. Adverse events Drowsiness (6%) Loss of energy (6%) Dizziness (6%) Chou et al, Annals of Internal Medicine Volume 147 Number 7
63 Gabapentin for Spinal Stenosis N=55, open label trial Pseudoclaudication and spinal stenosis on imaging Titrated to 2400 mg/day, plus supervised exercise therapy, lumbar supports, NSAIDs Moderately improved mean pain scores at four months (2.9 versus 4.7 on a 0 to 10 scale). Chou et al, Annals of Internal Medicine Volume 147 Number 7
64 Gabapentin abuse & misuse At risk: hx of or current substance use d/o, opioid, bzds and other sedatives; psychiatric d/o Abused by up 68% of opioid abusers Self administering excessive amounts to achieve euphoria, MJ like high, helps alleviate withdrawal symptoms Pure gabapentinoid OD safe, but often found on postmortem toxicology screens Bonnet U, Scherbaum N. Eur Neuropsychopharmacol Dec;27(12): Evoy KE, Morrison MD, Saklad SR. Drugs Mar;77(4):
65 Exercise Therapy Systematic review of 43 trials Slightly to moderately superior to no treatment for pain relief, though there were no significant differences in functional outcomes. Surgical decompression similar to PT among patient with lumbar spinal stenosis who were surgical candidates. Early PT reduces cost by >70% in the first year when compared to imaging Delitto A,et al. Ann of Internal Medicine 2015 Fritz JM, et al. Health Serv Res Dec;50(6):
66 Yoga Randomized trial of 101 patients, viniyoga improved functional status and symptoms at 12 weeks compared to a back exercise class, or a self-care book At 26 weeks, yoga equivalent to exercise, remained superior to self-care book. Yoga associated with decreased medication use compared to exercise or the self-care book. Yoga for nonspecific clbp noninferior to PT for function and pain compared to education book.
67 Acupuncture Two systematic reviews found acupuncture moderately more effective than no treatment for short-term pain relief and improvement in function More effective than sham acupuncture for pain relief, but not for improvement in function However, two well-blinded trials found no difference between acupuncture and sham acupuncture for either pain or function
68 Spinal Manipulations Moderately superior to sham manipulation or therapies thought to be ineffective No advantage compared to other interventions: Analgesics physical therapy Other systematic reviews similarly concluded that spinal manipulation has a minimal beneficial effect
69 When to Refer Cauda equina syndrome send to ED Neuromotor deficits Failing to respond to conservative therapies Patients at risk for developing chronic pain
70 Conclusion Everyone gets back pain Most people get better, but need to identify high risk patients for clbp Surgical evaluation for CES, any motor weakness Pain management referral for those at risk for chronic pain, not responding to conservative measures
Rational Approach to Treating Low Back Pain
 Rational Approach to Treating Low Back Pain Susie Jang, MD Faculty, Department of Anesthesia, Critical Care & Pain Medicine Beth Israel Deaconess Medical Center Instructor, Harvard Medical School Learning
Rational Approach to Treating Low Back Pain Susie Jang, MD Faculty, Department of Anesthesia, Critical Care & Pain Medicine Beth Israel Deaconess Medical Center Instructor, Harvard Medical School Learning
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽
 외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
외래에서흔히접하는 요통환자의진단과치료 울산의대서울아산병원가정의학과 R3 전승엽 Index Introduction Etiology & Type Assessment History taking & Physical examination Red flag sign Imaging Common disorder Management Reference Introduction Pain
Hailee Gibson, CCPA Neurosurgery Physician Assistant. Windsor Neurosurgery & Spine Associates. Windsor Regional Hospital Ouellette Campus
 Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Hailee Gibson, CCPA Neurosurgery Physician Assistant Windsor Neurosurgery & Spine Associates Windsor Regional Hospital Ouellette Campus Disclosures I have no disclosures Learning Objectives Provide information
Common Thoraco- Lumbar Problems in the Mature Athlete
 Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
Common Thoraco- Lumbar Problems in the Mature Athlete Diana Heiman, MD Associate Professor, Family Medicine Residency Director East Tennessee State University Objectives Review the pathophysiology of the
LOW BACK PAIN EPIDEMIOLOGY:
 LOW BACK PAIN OBJECTIVES: Discuss epidemiology of low back pain Summarize diagnosis/ special tests Review Red Flags Discuss treatment and referral guidelines Discuss light duty guidelines EPIDEMIOLOGY:
LOW BACK PAIN OBJECTIVES: Discuss epidemiology of low back pain Summarize diagnosis/ special tests Review Red Flags Discuss treatment and referral guidelines Discuss light duty guidelines EPIDEMIOLOGY:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society
 Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society Annals of Internal Medicine October 2007 Volume 147,
Back Pain Update. Steven Andersen, MD Providence Physiatry Clinic 2016
 Back Pain Update Steven Andersen, MD Providence Physiatry Clinic 2016 Back Pain is Very Common Lifetime prevalence 80% 12 month prevalence 40% Point prevalence 20% Centers for Disease Control and Prevention.
Back Pain Update Steven Andersen, MD Providence Physiatry Clinic 2016 Back Pain is Very Common Lifetime prevalence 80% 12 month prevalence 40% Point prevalence 20% Centers for Disease Control and Prevention.
CLINICAL GUIDELINES. Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision
 CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
CLINICAL GUIDELINES Primary Care Guideline Summary Lumbar Spine Thomas J. Gilbert M.D., M.P.P. 3/17/15 revision TRIAGE At the initial visit, a focused history and physical examination is performed to assign
Regional Pain Syndromes: Neck and Low Back
 Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Regional Pain Syndromes: Neck and Low Back Srinivas Nalamachu, MD Disclosures Consultant/Independent Contractor/Honoraria: Ferring 1 Learning Objectives Identify the most common painful conditions in the
Degenerative Disease of the Spine
 Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Degenerative Disease of the Spine Introduction: I. Anatomy Talk Overview II. Overview of Disease Processes: A. Spondylosis B. Intervertebral Disc Disease III. Diagnosis IV. Therapy Introduction: Myelopathy
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Chapter 35 Back Pain. Episode overview: Wisecracks: Crack Cast Show Notes Back Pain July 2016
 Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Chapter 35 Back Pain Episode overview: 1) List 10 historical red flags for back pain 2) List 6 Emergent Diagnosis for back pain Wisecracks: 1) Describe the most common sites of disc protrusion with their
Chiropractic Health Plan - Diagnosis of Low Back Pain
 Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Chiropractic Health Plan - Diagnosis of Low Back Pain 1 Adult Patient with ot for major Trauma Low back pain 2 Intake Evaluation (Inset 1) Recommendation 1 3 Potentially Serious Condition Strongly Suspected
Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center
 Oh My Aching Back! Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center Epidemiology 90% of episodes of LBP resolves
Oh My Aching Back! Francine M. Pulver, MD, Clinical Assistant Professor Department of Physical Medicine & Rehabilitation Ohio State University Medical Center Epidemiology 90% of episodes of LBP resolves
Wendy Field Advanced Physiotherapy Practitioner June 2018
 Wendy Field Advanced Physiotherapy Practitioner June 2018 Radiculopathy???? Lumbar radicular pain is where the clinician suspects the pain is coming from a lumbar nerve root. Essentially we are looking
Wendy Field Advanced Physiotherapy Practitioner June 2018 Radiculopathy???? Lumbar radicular pain is where the clinician suspects the pain is coming from a lumbar nerve root. Essentially we are looking
Disclosure Statement of Financial Interest. Evidence Based Evaluation and. Learning Objectives. What is Low Back Pain?
 Disclosure Statement of Financial Interest Evidence Based Evaluation and Management of Low Back Pain June 28, 2013 St. Charles Medical Center Summer Boslaugh and Alison Little DO NOT have a financial interest/arrangement
Disclosure Statement of Financial Interest Evidence Based Evaluation and Management of Low Back Pain June 28, 2013 St. Charles Medical Center Summer Boslaugh and Alison Little DO NOT have a financial interest/arrangement
Discussion Points 10/17/16. Spine Pain is Ubiquitous. Interventional Pain Management
 Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
Interventional Pain Management Blake Christensen, D.O. Fellowship Trained Interventional Pain Management Board Eligible in Anesthesiology and Interventional Pain Management Oklahoma Interventional Pain
Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia
 Disclosure & Acknowledgment Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia Disclosures - None Acknowledgements Dr. Andrea Furlan Dr. Julia Alleyne Dr. Hamilton Hall
Disclosure & Acknowledgment Getting at the CORE of Low-back pain Treatment Dr. John Flannery Dr. Carlo Ammendolia Disclosures - None Acknowledgements Dr. Andrea Furlan Dr. Julia Alleyne Dr. Hamilton Hall
LUMBAR SPINE CASE 3. Property of VOMPTI, LLC. For Use of Participants Only. No Use or Reproduction Without Consent 1. L4-5, 5-S1 disc, facet (somatic)
") LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE 3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Richmond 2018-2019 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT
 LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
LUMBAR SPINE CASE #3 A.J. Lievre, PT, DPT, OCS, CMPT Aaron Hartstein, PT, DPT, OCS, FAAOMPT Orthopaedic Manual Physical Therapy Series Charlottesville 2017-2018 L4-5, 5-S1 disc, facet (somatic) L5/S1 Radiculopathy
HIGH LEVEL - Science
 Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Learning Outcomes HIGH LEVEL - Science Describe the structure and function of the back and spine (8a) Outline the functional anatomy and physiology of the spinal cord and peripheral nerves (8a) Describe
Paul Allan Regional Clinical Lead - South. Lumbar Spine. Assessment & Differential Diagnosis
 Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Peggers Super Summaries: The Aging Spine
 Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
Aging Spine: AGING PROCESS Osteopenia 10% of 50 year old males and 25% of 50 year females Disc dehydration Facet degeneration Soft tissue hypertrophy 2 0 deformity Leg pain worse than back pain from nerve
Thoracolumbar Spine Conditions: Treatment and Return to Play
 Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
Thoracolumbar Spine Conditions: Treatment and Return to Play C H R I S T O P H E R B U R K S, MD B I E N V I L L E O R T H O P A E D I C S P E C I A L I S T S O C E A N S P R I N G S, MS Thoracolumbar
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery Diagnosis/Imaging/Surgery of Lumbar Spine Disorders Objectives Identify the most common
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R
 The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
The Complex/Challenging Spine Patient Steve Wisniewski, M.D. Department of PM&R 2011 MFMER slide-1 Disclosures None 2011 MFMER slide-2 Learning Objectives Review indications for obtaining imaging studies
An Osteopathic Approach to Low Back Pain. Ryan Seals DO Interim Chair of Family Medicine and OMM
 An Osteopathic Approach to Low Back Pain Ryan Seals DO Interim Chair of Family Medicine and OMM Objectives Review Osteopathic Philosophy and Principles Discuss how somatic dysfunction influences low back
An Osteopathic Approach to Low Back Pain Ryan Seals DO Interim Chair of Family Medicine and OMM Objectives Review Osteopathic Philosophy and Principles Discuss how somatic dysfunction influences low back
Cox Technic Case Report #169 published at (sent 5/9/17) 1
 1") Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
Cox Technic Case Report #169 published at www.coxtechnic.com (sent 5/9/17) 1 Management of Lumbar Radiculopathy Associated with an Extruded L4 L5 disc and concurrent L5 S1 Spondylolytic Spondylolisthesis
YOU ARE THE BEST OPTION FOR LOW BACK PAIN
 YOU ARE THE BEST OPTION FOR LOW BACK PAIN Amy Garrigues PT, DPT Orthopaedic Clinical Specialist Fellow, American Academy of Orthopaedic and Manual Physical Therapists LBP in past 3 months 25% 307% 220%
YOU ARE THE BEST OPTION FOR LOW BACK PAIN Amy Garrigues PT, DPT Orthopaedic Clinical Specialist Fellow, American Academy of Orthopaedic and Manual Physical Therapists LBP in past 3 months 25% 307% 220%
Objectives. Identify and differentiate appropriate surgical cases. Good Surgical Outcomes
 ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
ECHO February 5 th, 2015 Surgical Selection for Low Back Pain Objectives Identify and differentiate appropriate surgical cases Disclosures Medical director for UHN Rehabilitations Solution Back and Neck
Cox Technic Case Report #126 published at (sent December 2013 ) 1
 1") Cox Technic Case Report #126 published at www.coxtechnic.com (sent December 2013 ) 1 Cox Technic Decompression Spinal Manipulation Resolves Symptoms Associated with Disc Protrusion and S1 Radiculopathy,
Cox Technic Case Report #126 published at www.coxtechnic.com (sent December 2013 ) 1 Cox Technic Decompression Spinal Manipulation Resolves Symptoms Associated with Disc Protrusion and S1 Radiculopathy,
University of Jordan. Professor Freih Abuhassan -
 Freih Odeh Abu Hassan F.R.C.S.(Eng.), F.R.C.S.(Tr.& Orth.). Professor of Orthopedics University of Jordan 1 A. Sacroiliitis History Trauma is very common Repetitive LS motion--lumbar rotation or axial
Freih Odeh Abu Hassan F.R.C.S.(Eng.), F.R.C.S.(Tr.& Orth.). Professor of Orthopedics University of Jordan 1 A. Sacroiliitis History Trauma is very common Repetitive LS motion--lumbar rotation or axial
Surgery. Conus medullaris and Cauda Equina Syndromes. Anatomy. See online here
 Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Surgery Conus medullaris and Cauda Equina Syndromes See online here Conus medullaris and cauda equina syndromes are spinal cord injuries that involve injury to the lumbosacral segment of the spinal cord.
Are you getting the best treatment for your low back pain?
 Are you getting the best treatment for your low back pain? Dr.Rahimian Orthopedic surgon Spine fellowship resident Why are we here? To update you on the best evidence for the treatments available To give
Are you getting the best treatment for your low back pain? Dr.Rahimian Orthopedic surgon Spine fellowship resident Why are we here? To update you on the best evidence for the treatments available To give
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Facet Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Facet Injection Please check the indication (reason)
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested is: Please check the indication (reason) for this procedure
Back Pain. John W. Engstrom, MD December 16, Disclosures. A Clinical Approach to the Evaluation of Back Pain and Lumbar Radiculopathy
 Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Disclosures Nothing to declare --- or --- Significant ownership interests Speaker bureaus, honorarium, grants A Clinical Approach to the Evaluation of and Lumbar Radiculopathy John Engstrom, MD Acute Low
Low back pain in a Nutshell Paul Manjaly. Paul Manjaly
 Low back pain in a Nutshell Paul Manjaly Paul Manjaly Pain: An unpleasant sensory and emotional experience which follows actual or potential tissue damage or is described in terms of such damage Unpleasant
Low back pain in a Nutshell Paul Manjaly Paul Manjaly Pain: An unpleasant sensory and emotional experience which follows actual or potential tissue damage or is described in terms of such damage Unpleasant
Alan H Daniels, MD. Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University
 Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
Spinal and Orthopaedic Surgery in the Elderly Alan H Daniels, MD Spine Division, Department of Orthopaedics Warren Alpert School of Medicine of Brown University As the population ages, and patients remain
The Role of the PDMP: Foundational Knowledge and Best Practices
 The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
A Patient s Guide to Treatment Guidelines for Low Back Pain
 A Patient s Guide to Treatment Guidelines for Low Back Pain 15195 Heathcote Blvd Suite 334 Haymarket, VA 20169 Phone: 703-369-9070 Fax: 703-369-9240 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Treatment Guidelines for Low Back Pain 15195 Heathcote Blvd Suite 334 Haymarket, VA 20169 Phone: 703-369-9070 Fax: 703-369-9240 DISCLAIMER: The information in this booklet is compiled
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Patient Selection and Lumbar Operative Interventions
 Patient Selection and Lumbar Operative Interventions John C France MD Professor of Orthopaedic & Neurosurgery West Virginia University Low back pain is a symptom not a diagnosis Epidemiology of LBP General
Patient Selection and Lumbar Operative Interventions John C France MD Professor of Orthopaedic & Neurosurgery West Virginia University Low back pain is a symptom not a diagnosis Epidemiology of LBP General
Which of my patients with chronic back pain doesn t need an MRI? (This could be a short talk) Neil Berrington MMed,FCS,FRCS
 Neil Berrington MMed,FCS,FRCS") Which of my patients with chronic back pain doesn t need an MRI? (This could be a short talk) Neil Berrington MMed,FCS,FRCS Disclosures The Winnipeg Spine Program and the Canadian Spine Society Outcomes
Which of my patients with chronic back pain doesn t need an MRI? (This could be a short talk) Neil Berrington MMed,FCS,FRCS Disclosures The Winnipeg Spine Program and the Canadian Spine Society Outcomes
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center
 Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Gary Rea MD PhD Medical Director OSU Comprehensive Spine Center 1. The less specific the patient is about symptoms and pain, the less likely a specific diagnosis will be made and the less likely the patient
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Injection Please check the indication (reason)
Evaluation and Management of Select Spine Conditions
 Evaluation and Management of Select Spine Conditions Michael E. Zychowicz, DNP, ANP, ONP, FAAN, FAANP Professor & Director, MSN Program Lead Faculty, Orthopedic NP Specialty Director, Duke-Durham VA Nursing
Evaluation and Management of Select Spine Conditions Michael E. Zychowicz, DNP, ANP, ONP, FAAN, FAANP Professor & Director, MSN Program Lead Faculty, Orthopedic NP Specialty Director, Duke-Durham VA Nursing
Treatments for Common Pain Disorders. Matthew R. Kohler, MD Hudson Spine and Pain Medicine 03/01/2017
 Treatments for Common Pain Disorders Matthew R. Kohler, MD Hudson Spine and Pain Medicine 03/01/2017 Acute Disc Herniation Conservative Approach (Four to Six Weeks) Physical Therapy, exercise and gentle
Treatments for Common Pain Disorders Matthew R. Kohler, MD Hudson Spine and Pain Medicine 03/01/2017 Acute Disc Herniation Conservative Approach (Four to Six Weeks) Physical Therapy, exercise and gentle
REVIEW OF LITERATURE BMJ 2007; 334(7607): Diagnosis and treatment of sciatica. Bart W. Koes Maurits W. van Tulder Wilco C.
: Diagnosis and treatment of sciatica. Bart W. Koes Maurits W. van Tulder Wilco C.") 2 REVIEW OF LITERATURE Diagnosis and treatment of sciatica Bart W. Koes Maurits W. van Tulder Wilco C. Peul BMJ 2007; 334(7607):1313-1317 22 CHAPTER 2 DIAGNOSIS AND TREATMENT OF SCIATICA 23 INTRODUCTION
2 REVIEW OF LITERATURE Diagnosis and treatment of sciatica Bart W. Koes Maurits W. van Tulder Wilco C. Peul BMJ 2007; 334(7607):1313-1317 22 CHAPTER 2 DIAGNOSIS AND TREATMENT OF SCIATICA 23 INTRODUCTION
Jessica Jameson MD Post Falls, ID
 Jessica Jameson MD Post Falls, ID Discuss the history of interventiona l pain Discuss previous tools to manage chronic pain Discuss current novel therapies to manage chronic pain and indications HISTORY
Jessica Jameson MD Post Falls, ID Discuss the history of interventiona l pain Discuss previous tools to manage chronic pain Discuss current novel therapies to manage chronic pain and indications HISTORY
The ABC s of LUMBAR SPINE DISEASE
 The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery URMC Neurosurgery APP s Objectives Identify the most common pathology that leads to spine
The ABC s of LUMBAR SPINE DISEASE Susan O. Smith ANP-BC University of Rochester Department of Neurological Surgery URMC Neurosurgery APP s Objectives Identify the most common pathology that leads to spine
Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions:
 Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions: Radiating leg pain Greater leg / buttock pain than back pain Severe pain sets in when walking as
Am I eligible for the TOPS study? Possibly, if you suffer from one or more of the following conditions: Radiating leg pain Greater leg / buttock pain than back pain Severe pain sets in when walking as
Lumbar Disc Prolapse. Dr. Ahmed Salah Eldin Hassan. Professor of Neurosurgery & Consultant spinal surgeon
 Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Lumbar Disc Prolapse By Dr. Ahmed Salah Eldin Hassan Professor of Neurosurgery & Consultant spinal surgeon 1-What are the Functions of the Spine Structural support for upright posture Protection of Spinal
Physical examination of the patient with back pain
 Physical examination of the patient with back pain Mitchell K Freedman DO Clinical Associate Professor at Sidney Kimmel Medical College of Thomas Jefferson University Hospital Goals of Lecture Discuss
Physical examination of the patient with back pain Mitchell K Freedman DO Clinical Associate Professor at Sidney Kimmel Medical College of Thomas Jefferson University Hospital Goals of Lecture Discuss
Patient Chart Quotes. Spine Mythology and Evidence- Based Management of Back Pain. Patient Chart Quotes. Patient Chart Quotes
 Spine Mythology and Evidence- Based Management of Back Pain John Engstrom, MD Professor of Neurology August 11, 2009 Patient Chart Quotes The patient was in his usual state of good health until his airplane
Spine Mythology and Evidence- Based Management of Back Pain John Engstrom, MD Professor of Neurology August 11, 2009 Patient Chart Quotes The patient was in his usual state of good health until his airplane
Spine Pain Management Program
 Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Adhesiolysis Please check the indication (reason)
Spine Pain Management Program Please complete the following information: Patient Name: Patient ID Number: Patient DOB: The procedure being requested: Epidural Adhesiolysis Please check the indication (reason)
LOTHIAN LUMBAR SPINE PATHWAYS
 LOTHIAN LUMBAR SPINE PATHWAYS Patient Completes STarT Back form Assess patient and screen for Red Flags. If present refer to Appendix 1 Establish if Neurogenic. If so refer to Appendix 2 Children under
LOTHIAN LUMBAR SPINE PATHWAYS Patient Completes STarT Back form Assess patient and screen for Red Flags. If present refer to Appendix 1 Establish if Neurogenic. If so refer to Appendix 2 Children under
The NICE revised guidelines for the management of non-specific low back pain and; Implications for Practice
 The NICE revised guidelines for the management of non-specific low back pain and; Implications for Practice David Walsh David.walsh@nottingham.ac.uk National Clinical Guideline Centre Commissioned by NICE
The NICE revised guidelines for the management of non-specific low back pain and; Implications for Practice David Walsh David.walsh@nottingham.ac.uk National Clinical Guideline Centre Commissioned by NICE
Clinical and Contextual Evidence Reviews
 Clinical and Contextual Evidence Reviews Roger Chou, MD Professor of Medicine Oregon Health & Science University Director, Pacific Northwest Evidence-based Practice Center Purpose Summarize methods for
Clinical and Contextual Evidence Reviews Roger Chou, MD Professor of Medicine Oregon Health & Science University Director, Pacific Northwest Evidence-based Practice Center Purpose Summarize methods for
Does patient history and physical examination predict MRI proven cauda equina syndrome?
 27 27 33 Does patient history and physical examination predict MRI proven cauda equina syndrome? Authors Jeremy Fairbank¹, Robin Hashimoto², Andrew Dailey ³, Alpesh A Patel³, Joseph R Dettori² Institutions
27 27 33 Does patient history and physical examination predict MRI proven cauda equina syndrome? Authors Jeremy Fairbank¹, Robin Hashimoto², Andrew Dailey ³, Alpesh A Patel³, Joseph R Dettori² Institutions
Corporate Medical Policy
 Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
Corporate Medical Policy Epidural Steroid Injections for Back Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: epidural_steroid_injections_for_back_pain 2/2016 4/2017 4/2018
DISORDERS OF THE SPINE TREATING PHYSICIAN DATA SHEET
 DISORDERS OF THE SPINE TREATING PHYSICIAN DATA SHEET Short form FOR REPRESENTATIVE USE ONLY REPRESENTATIVE S NAME AND ADDRESS REPRESENTATIVE S TELEPHONE REPRESENTATIVE S EMAIL PHYSICIAN S NAME AND ADDRESS
DISORDERS OF THE SPINE TREATING PHYSICIAN DATA SHEET Short form FOR REPRESENTATIVE USE ONLY REPRESENTATIVE S NAME AND ADDRESS REPRESENTATIVE S TELEPHONE REPRESENTATIVE S EMAIL PHYSICIAN S NAME AND ADDRESS
Painful GP dilemmas Low Back Pain Leg Pain. Dr. Rajiv Chawla Consultant in Pain Medicine The Walton Centre Liverpool
 Painful GP dilemmas Low Back Pain Leg Pain Dr. Rajiv Chawla Consultant in Pain Medicine The Walton Centre Liverpool Low back Pain Up to 80% of all adults will eventually experience back pain, and it is
Painful GP dilemmas Low Back Pain Leg Pain Dr. Rajiv Chawla Consultant in Pain Medicine The Walton Centre Liverpool Low back Pain Up to 80% of all adults will eventually experience back pain, and it is
Suspecting Tumors, or Could it be cancer?
 Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Suspecting Tumors, or Could it be cancer? Donna E. Reece, M.D. Princess Margaret Cancer Centre University Health Network Toronto, ON CANADA 07 February 2018 Background Low back pain is common However,
Discal herniation and spondylosis
 III.8.4.6 Degenerative disorders of the spine Introduction the frequency of locomotor disorders increases with age Low back pain is a very common disorder. According to medical literature, it is the second
III.8.4.6 Degenerative disorders of the spine Introduction the frequency of locomotor disorders increases with age Low back pain is a very common disorder. According to medical literature, it is the second
Lumbar disc prolapse. Done by : Areej Al-Hadidi
 Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Lumbar disc prolapse Done by : Areej Al-Hadidi Anatomy of IVD IVD is composed of two components: 1. anulus fibrosus : it is the outer fibrous layer (fibrocartilage ) **It is comressible &tough 2. nucleus
Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM
 Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM OEMAC Calgary September 23, 2018 OBJECTIVES 1. To name key diagnoses of neuromusculoskeletal conditions
Common neuromusculoskeletal disorders in the workplace W. Shane Journeay, PhD, MD, MPH, FRCPC, BC-OEM OEMAC Calgary September 23, 2018 OBJECTIVES 1. To name key diagnoses of neuromusculoskeletal conditions
What is the role of imaging in acute low back pain?
 Curr Rev Musculoskelet Med (2009) 2:69 73 DOI 10.1007/s12178-008-9037-0 What is the role of imaging in acute low back pain? Humaira Lateef Æ Deepak Patel Published online: 28 April 2009 Ó The Author(s)
Curr Rev Musculoskelet Med (2009) 2:69 73 DOI 10.1007/s12178-008-9037-0 What is the role of imaging in acute low back pain? Humaira Lateef Æ Deepak Patel Published online: 28 April 2009 Ó The Author(s)
Evaluation of Posterior Hip Pain
 Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Evaluation of Posterior Hip Pain Anthony J. Ferretti, D.O., MHSA Hip Pain in the Adult Various etiologies: Traumatic Infectious Neurovascular Degenerative Congenital Pathologic 1 Hip Pain Complex interaction
Lumbar spinal canal stenosis Degenerative diseases F 08
 What is lumbar spinal canal stenosis? This condition involves the narrowing of the spinal canal, and of the lateral recesses (recesssus laterales) and exit openings (foramina intervertebralia) for the
What is lumbar spinal canal stenosis? This condition involves the narrowing of the spinal canal, and of the lateral recesses (recesssus laterales) and exit openings (foramina intervertebralia) for the
10/8/2015. Consultant for Boston Scientific-no conflicts with this presentation
 Consultant for Boston Scientific-no conflicts with this presentation Mehul Sekhadia, DO Medical Director Advocate Lutheran General Hospital Park Ridge, IL Identify when to consider interventional pain
Consultant for Boston Scientific-no conflicts with this presentation Mehul Sekhadia, DO Medical Director Advocate Lutheran General Hospital Park Ridge, IL Identify when to consider interventional pain
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Lumbar Spinal Stenosis
 Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Lumbar Spinal Stenosis This article is also available in Spanish: Estenosis de la columna lumbar (topic.cfm?topic=a00701). A common cause of low back and leg pain is lumbar spinal stenosis. As we age,
Mr. LBP: Case Presentation
 CLINICAL CASES Case: Mr. LBP Mr. LBP: Case Presentation Mr. LBP is a 35-year-old male He fell down while participating in a recreational sports activity He subsequently developed low back pain Upon arrival
CLINICAL CASES Case: Mr. LBP Mr. LBP: Case Presentation Mr. LBP is a 35-year-old male He fell down while participating in a recreational sports activity He subsequently developed low back pain Upon arrival
SpineFAQs. Lumbar Spondylolisthesis
 SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
BACK PAIN. Disclaimer. Integrated web marketing. Multimedia Health Education
 BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
BACK PAIN Disclaimer This movie is an educational resource only and should not be used to make a decision on. All decisions about surgery must be made in conjunction with your surgeon or a licensed healthcare
LUMBAR SPINAL STENOSIS
 LUMBAR SPINAL STENOSIS North American Spine Society Public Education Series WHAT IS LUMBAR SPINAL STENOSIS? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
LUMBAR SPINAL STENOSIS North American Spine Society Public Education Series WHAT IS LUMBAR SPINAL STENOSIS? The vertebrae are the bones that make up the lumbar spine (low back). The spinal canal runs through
Examination of the lumbosacral spine. Dr Lucy Holtzhausen Rotorua GP CME June 2015
 Examination of the lumbosacral spine Dr Lucy Holtzhausen Rotorua GP CME June 2015 Diagnostic Algorithm Presenting symptoms Diagnostic decisions Diagnostic triage LOW BACK PAIN Mechanical NON-SPECIFIC LBP
Examination of the lumbosacral spine Dr Lucy Holtzhausen Rotorua GP CME June 2015 Diagnostic Algorithm Presenting symptoms Diagnostic decisions Diagnostic triage LOW BACK PAIN Mechanical NON-SPECIFIC LBP
Case Studies, Impairment of the Spine in Washington State
 Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Case Studies, Impairment of the Spine in Washington State NAOEM at Skamania, 2015 25 Sep, 2015 Tim Gilmore, MD Several Slides from this Presentation Borrowed with permission from the Washington State Department
Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology
 Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Physical Therapy Diagnostic and Treatment Approach to the Active Patient with Complex Spine Pathology Scott Behjani, DPT, OCS Introduction Prevalence 1-year incidence of first-episode LBP ranges from
Low Back Pain Optimal Management in General Practice
 Low Back Pain Optimal Management in General Practice Dr Neil Hearnden Musculoskeletal Physician M.B. B.S. FRACGP. Grad Dip Musculoskeletal.Med. (Otago) MAFMM Arana Hills Medical Centre Brisbane Outcome
Low Back Pain Optimal Management in General Practice Dr Neil Hearnden Musculoskeletal Physician M.B. B.S. FRACGP. Grad Dip Musculoskeletal.Med. (Otago) MAFMM Arana Hills Medical Centre Brisbane Outcome
Herniated Disk in the Lower Back
 Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Herniated Disk in the Lower Back This article is also available in Spanish: Hernia de disco en la columna lumbar (topic.cfm?topic=a00730). Sometimes called a slipped or ruptured disk, a herniated disk
Outline. Introduction / Epidemiology. Anatomy / Pain generators. Diagnosis. Treatment. Most Important lecture!!
 Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
Acute Low Back Pain Outline Introduction / Epidemiology. Most Important lecture!! Anatomy / Pain generators Diagnosis Treatment Course Objectives Know the RED FLAGS in history taking. Know the Pain Generators
APPROPRIATE USE GUIDELINES
 APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
APPROPRIATE USE GUIDELINES Appropriateness of Advanced Imaging Procedures (MRI, CT, Bone Scan/PET) in Patients with Neck Pain CDI QUALITY INSTITUTE: PROVIDER LED ENTITY (PLE) Updated June, 2017 Contents
Non-Operative Management of Low Back Pain in the Elderly
 www.4-no-pain.com Non-Operative Management of Low Back Pain in the Elderly Brian Kahan, D.O., FAAPMR Low Back Pain Outline Etiologies Initial Assessment Physical examination and Diagnostic work-up Clinical
www.4-no-pain.com Non-Operative Management of Low Back Pain in the Elderly Brian Kahan, D.O., FAAPMR Low Back Pain Outline Etiologies Initial Assessment Physical examination and Diagnostic work-up Clinical
Low Back Pain in the Athlete Steven E. Mayer, MD Northwestern Medicine Physical Medicine and Rehabilitation Sports Medicine
 Low Back Pain in the Athlete Steven E. Mayer, MD Northwestern Medicine Physical Medicine and Rehabilitation Sports Medicine When to Play and When to Sit Controversial Based on clinical/expert opinion Current
Low Back Pain in the Athlete Steven E. Mayer, MD Northwestern Medicine Physical Medicine and Rehabilitation Sports Medicine When to Play and When to Sit Controversial Based on clinical/expert opinion Current
Electrodiagnostics for Back & Neck Pain. Steven Andersen, MD Providence Physiatry Clinic
 Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Move Better, Feel Better: What Can Physical Therapy Do For You
 Back to Basics Move Better, Feel Better: What Can Physical Therapy Do For You Dr. Stephen Baxter, Dr. Dean Yamanuha Department of Physical Therapy and Rehabilitative Sciences 5/16/2017 Dr. Stephen Baxter
Back to Basics Move Better, Feel Better: What Can Physical Therapy Do For You Dr. Stephen Baxter, Dr. Dean Yamanuha Department of Physical Therapy and Rehabilitative Sciences 5/16/2017 Dr. Stephen Baxter
Cervical intervertebral disc disease Degenerative diseases F 04
 Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Cervical intervertebral disc disease Degenerative diseases F 04 How is a herniated cervical intervertebral disc treated? Conservative treatment is generally sufficient for mild symptoms not complicated
Suggests that optimal approach is unsure
 An Important Issue One of the most common reasons for seeking medical attention, second only to respiratory issues 84% of adults will have low back pain at some point Wide variety of approaches for treatment
An Important Issue One of the most common reasons for seeking medical attention, second only to respiratory issues 84% of adults will have low back pain at some point Wide variety of approaches for treatment
A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute
 A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute 26th Annual Southwestern Conference on Medicine AXIAL MUSCULO- SKELETAL PACK PAIN: Common Self-limited
A Surgeon s Perspective for the Primary Care Physician Stephen Curtin M.D. Tucson Orthopeadic Institute 26th Annual Southwestern Conference on Medicine AXIAL MUSCULO- SKELETAL PACK PAIN: Common Self-limited
Cervical Plating BACK PAIN
 BACK PAIN Back Pain Back pain is frequent complaint. It is the commonest cause of work-related absence in the world. Although back pain may be painful and uncomfortable, it is not usually serious. Even
BACK PAIN Back Pain Back pain is frequent complaint. It is the commonest cause of work-related absence in the world. Although back pain may be painful and uncomfortable, it is not usually serious. Even
Medical Affairs Policy
 Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
Medical Affairs Policy Service: Back Pain Procedures-Epidural Injection (Caudal Epidural, Selective Nerve Root Block, Interlaminar, Transforaminal, Translaminar Epidural Injection) PUM 250-0015-1706 Medical
Vertebral Axial Decompression
 Vertebral Axial Decompression Policy Number: 8.03.09 Last Review: 11/2017 Origination: 11/2005 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage
Vertebral Axial Decompression Policy Number: 8.03.09 Last Review: 11/2017 Origination: 11/2005 Next Review: 11/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide coverage
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018
 EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
EVALUATE, TREAT AND WHEN TO REFER RED FLAGS Mid Atlantic Occupational Regional Conference and Environmental Medicine October 6, 2018 Marc J. Levine, MD Rothman Institute Director Spine Surgery Program
IEHP UM Subcommittee Approved Authorization Guidelines Referrals to Pain Management Specialists
 IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
IEHP Policy: Based on a review of the currently available literature and community standards of practice, the IEHP UM Subcommittee will consider referrals to Pain Management Specialists medically necessary
Musculoskeletal Examination of the Pain Patient
 Musculoskeletal Examination of the Pain Patient Joseph F. Audette, M.A., M.D Assistant Clinical Professor, Harvard Medical School Chief, Department of Pain Medicine Harvard Vanguard Medical Associates
Musculoskeletal Examination of the Pain Patient Joseph F. Audette, M.A., M.D Assistant Clinical Professor, Harvard Medical School Chief, Department of Pain Medicine Harvard Vanguard Medical Associates
Numb bum means cauda equina Per rectal examination is indicated to assess anal tone
 SPINE Age and occupation Pain: Where: Low back or leg Which is worse? Where about in the leg? Describe the radiation How long? More than 6 wks need warrant evaluation How the pain is now compared to the
SPINE Age and occupation Pain: Where: Low back or leg Which is worse? Where about in the leg? Describe the radiation How long? More than 6 wks need warrant evaluation How the pain is now compared to the
North American Spine Society Public Education Series
 Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong
Herniated Lumbar Disc North American Spine Society Public Education Series What Is a Herniated Disc? The spine is made up of a series of connected bones called vertebrae. The disc is a combination of strong