Dyspepsia and upper gastrointestinal bleeding. Dr. Wayne H.C. Hu 胡興正
|
|
|
- Joan Dennis
- 5 years ago
- Views:
Transcription
1 Dyspepsia and upper gastrointestinal bleeding Dr. Wayne H.C. Hu 胡興正
2 25 year old medical student Occasional smoker and drinker. About to take final examinations. 3 week history of epigastric bloating. Worse after meals, early satiety. Appetite fair, lost 0.5 Kg in weight. No night pain. No malaena/ haematemesis. Occasional acid regurgitation.
3 Findings Physical examination normal apart from mild epigastric tenderness on palpation. CBP, liver and renal function tests normal.
4 s None s AXR s Helicobacter testing s Endoscopy s Barium meal s Ultrasound abdomen Investigations?
5 Dyspepsia Very common complaint 19%-30% of population have dyspepsia (Hu( et al 1997) Causes: Peptic ulcer, Erosions, Gastric cancer, Gastroparesis,, Functional dyspepsia, Pancreatic cancer (radiates to back) etc.
6 Causes of upper abdominal discomfort: Non-GI Abdominal wall pain: worse on movement, sitting up, sharp localised pain Angina: pain related to exertion, may be after meals, radiation to the shoulder and throat Myocardial infarction: Constant severe pain, acute onset
7 Causes of upper abdominal discomfort: GI tract Acute pancreatitis: radiation to the back, acute onset Biliary colic: right sided, onset minutes after meal intake (cholecystokinin( release and gallbladder contraction), relation to fatty foods

8 Ductal stone: central pain, spontaneous pain or pain after meals, ultrasound or CT may NOT show small stones Easily confused with stomach pain Ductal stone
9 Causes of upper abdominal discomfort: GI tract Gastric cancer Peptic ulcer Functional dyspepsia Irritable bowel syndrome: better after bowel movement
10 Dyspepsia 26% 23% 31% 19% 34%
11
12 Diagnosis of dyspepsia Make sure the patient has dyspepsia rather than biliary,, large intestinal, cardiac pain etc. Overall,, functional dyspepsia is the commonest cause. Must not miss cancer- fatal if untreated. Duodenal ulcer may respond to empirical treatment with anti-secretive therapy or H. pylori eradication.
13 Alarm symptoms- suggest organic Weight loss Malaena/ haematemesis Vomiting Dysphagia Anaemia Lymphadenopaathy Abdominal mass/ liver Old age disease
14 Approach to dyspepsia Exclude alarm symptoms. Endoscopy + other investigations if present. Empirical treatment: antacids, H2 antagonists if young. Endoscopy if alarm symptoms, age over 45, or poor response to empirical treatment.
15 Approach to dyspepsia?empirical endoscopy: costs similar to empirical treatment in various studies. H. pylori testing and eradication: treats ulcers, functional dyspepsia?benefit. Reflux worsened by H. pylori eradication. Similar benefit to symptoms.
16 Treatment of functional dyspepsia Disease of relapse and remissions. High placebo response rate may be related to the natural remission of the disease. Antacids etc. good and cheap placebo. Useful as first line treatment.
17 Treatment of functional dyspepsia Careful explanation and reassurance. Symptomatic relief and attention to co-morbid factors like anxiety, stress etc. Underlying psychiatric disorders: cognitive therapy to modify beliefs, antidepressant, anxiolytic drugs.
18 Drug treatment: prokinetics Metoclopramide: : not for longterm use. Sedation and extrapyramidal side-effects. effects. Domperidone: : does not cross the blood-brain brain barrier.
19 Drug treatment: acid suppression H2 antagonists not very useful compared to placebo. Proton pump inhibitors better efficacy especially in those with ulcer symptoms. Useful if there is co-existing reflux. Expensive
20 Primary Management of New Onset Uninvestigated Dyspepsia Asia-Pacific Region Exclude by history: biliary pain, irritable bowel, reflux DYSPEPSIA If <2-4 weeks: Dietary advise & observe Review current medication Treatment Trial: Anti-secretory therapy or Prokinetic Duration: <2-4weeks NO Failure or Relapse after early response Locally-validated Hp test ( ulcer test ) Positive Eradication therapy Negative Alarm features? Strong fear of serious disease? Chronic NSAID use in therapeutic doses? **Age > 45 years? FUNCTIONAL DYSPEPSIA Dysmotility-like: Prokinetic Ulcer-like: Anti-secretory drug Non-specific: Prokinetic or Anti-secretory Evaluate after 4 weeks YES Negative Investigate: Endoscopy Positive Structural disease e.g. ulcer, cancer, oesophagitis Treat appropriately SUCCESS FAILURE SUCCESS Change to another class of therapy Final evaluation after 8 weeks FAILURE Specialist referral FOLLOW UP FAILURE ** Age cut-off varies with age-specific incidence of gastric cancer in each country (35-55 Yrs) Reference: N. Talley, SK Lam, KL Goh and KM Fock. Management guidelines for uninvestigated and functional dyspepsia in the Asia-Pacific region: First Asian Pacific working party on functional dyspepsia. Journal of Gastroenterology and Hepatology (1998) 13
21 Primary Management of New Onset Uninvestigated Dyspepsia Asia-Pacific Region DYSPEPSIA Treatment Trial: Anti-secretory therapy or Prokinetic Duration: <2-4weeks NO Alarm features? Strong fear of serious disease? Chronic NSAID use in therapeutic doses? **Age > 45 years? SUCCESS 1
22 Primary Management of New Onset Uninvestigated Dyspepsia Asia-Pacific Region DYSPEPSIA Treatment Trial: Anti-secretory therapy or Prokinetic Duration: <2-4weeks NO Alarm features? Strong fear of serious disease? Chronic NSAID use in therapeutic doses? **Age > 45 years? Failure or Relapse after early response Locally-validated Hp test ( ulcer test ) Negative Positive Eradication therapy FUNCTIONAL DYSPEPSIA Dysmotility-like: Prokinetic Ulcer-like: Anti-secretory drug Non-specific: Prokinetic or Anti-secretory SUCCESS FAILURE 2
23 Primary Management of New Onset Uninvestigated Dyspepsia Asia-Pacific Region DYSPEPSIA Alarm features? Strong fear of serious disease? Chronic NSAID use in therapeutic doses? **Age > 45 years? YES Negative Investigate: Endoscopy FUNCTIONAL DYSPEPSIA Dysmotility-like: Prokinetic Ulcer-like: Anti-secretory drug Non-specific: Prokinetic or Anti-secretory Evaluate after 4 weeks SUCCESS SUCCESS Change to another class of therapy Final evaluation after 8 weeks FAILURE 3
24 Dyspepsia: Pain or discomfort centered in the upper abdomen. Functional dyspepsia: No definite structural or biochemical explanation for the dyspepsia Definitions
25 Symptoms of functional dyspepsia Epigastric pain syndrome: pain or burning, hunger pain, relief with food, not relieved by bowel movement Postprandial distress syndrome: bloating, gaseousness after meals, early satiety A lot of overlap between groups Associated with reflux and irritable bowel syndrome.
26 Dyspepsia subgroups Ulcer-like (epigastric pain) 17% 1% 9% Dysmotility-like (postprandial distress) 3% 18% 9% Talley NJ et al.gastroenterology % Reflux -like Non-specific 27%
27 Dyspeptic symptoms Do not reliably distinguish between functional and organic disease. Severe bloating, nausea and vomiting suggests delayed gastric emptying.
28 Predominant symptom Epigastric pain (ulcer like dyspepsia) Pain most bothersome symptom. Postprandial distress (Dysmotility( like dyspepsia) Unpleasant or troublesome non-painful sensation most bothersome. Associated with fullness, early satiety, bloating, nausea. Unspecified dyspepsia
29 Treatment response Proton-pump inhibitor response in those with predominant pain Losec 20 Losec 10 Placebo 10 Talley Aliment Pharmacol Ther Pain Dysmotility

30 Aetiology of functional dyspepsia?? Motility disorder: delayed gastric emptying, failure of fundus to relax after meal. Sensory disorder: hypersensitivity to intragastric balloon distension.
31 Radiolabelled meal ingestion Dyspeptics Controls 10 0 Proximal Distal Troncon et al Gut 1994
32 Air insufflation (400ml) No Pain Pain 5 0 Dyspeptic Control Lemann et al Dig Dis Sci 1991
33 Aetiology of functional dyspepsia?? Acid secretion??: Probably does not play a role. No difference in basal and stimulated acid output. H. pylori??: Controversial. No difference in prevalence between dyspeptics and non- dyspeptics. However one study showed long- term benefit after eradication; but another multi- centered study showed the opposite.
34 H. pylori in blood donors Hp+ Hp- 5 0 Dyspepsia Nignt pain Pain after meals Reflux Holtmann Dig Dis Sci 1994
35 Aetiology of functional dyspepsia?? Gastritis: Not a cause of dyspepsia! No difference in non-erosive gastritis among dyspeptics and non-dyspeptics. Gastric and duodenal erosions probably belong to the spectrum of ulcer disease.
36 Aetiology of functional dyspepsia?? Psychological??: Psychological morbidity very common in patients in specialist clinics (depression, anxiety etc.) Increased symptoms with stress.
37 Aetiology of functional dyspepsia?? Dyspeptics in the community may not be different psychologically to normals.. Anxiety affects doctor-seeking behaviour.
38 7 Anxiety and Depression 6 5 Mean Score Normal Dyspepsia IBS 1 0 Anxiety score p<0.05 Depression score p<0.05 Hu et al 1997
39 Psychological morbidity determines health seeking Anxiety Deperession Consulter Non-consulter Hu et al 1997

40 Gastrointestinal Bleeding: Why and how Wayne H.C. Hu Hu 胡興正 Specialist in Gastroenterology and Hepatology
41 Outline Clinical considerations Investigations of upper GI bleeding Non-variceal bleeding Variceal bleeding
42 Upper GI bleed: Definition Origin proximal to the ligament of Trietz Present as haematemesis, coffee-ground vomiting, PR bleeding if rapid blood loss
43 Upper GI bleed: Epidemiology 300,000 admissions annually in USA 5x more common than lower GI bleeding Mortality 7-10% 7 Stable mortality rate over the last 30 years
44 Management principals Assessment and stabilisation of haemodynamic state Stop the bleeding Treat the underlying abnormality Prevent recurrent bleeding
45 Assessment History: previous ulcer, aspirin and NSAID intake Examination: haemodynamic state, signs of liver disease
46 Poor prognostic factors Increasing age Comorbid medical condisions Variceal bleed Fresh blood in vomit or stool Shock Active bleeding at endoscopy Large (>2cm) ulcer Onset of bleeding in hospital Emergency surgery
47 Minor bleeding Haemodynamic state Loss <10% intravascular volume No haemodynamic change Moderate bleeding Loss 10-20% intravascular volume Postural hypotension
48 Severe bleed Haemodynamic state Loss>20% intravascular volume Shock and tachycardia
49 Common Gastric ulcer Duodenal ulcer Mallory-Weiss tear Varices Causes of bleeding

50 Causes of bleeding Less common Dieulafoy s lesion Gastric antral vascular ectasia Portal hypertensive gastropathy Neoplasia Oesophagitis Gastric erosions


51 Hereditary haemorrhagic telangiectasia









52 Endoscopy
53

54
55 Endoscopic evaluation Repeat endoscopy may be indicated: 35% of obscure bleeding have definite source on repeat OGD. At enteroscopy,, lesion that should have been identified at OGD in 28%-75% of patients.
")
56 Small bowel investigations Enteroscopy Barium meal and follow-through Small bowel enema (enteroclysis( enteroclysis) Capsule endoscopy

57 Barium studies Ba meal and follow- through less invasive. Small bowel enema require intubation but more sensitive. Difficult to detect small ulcers and bleeding vessels.
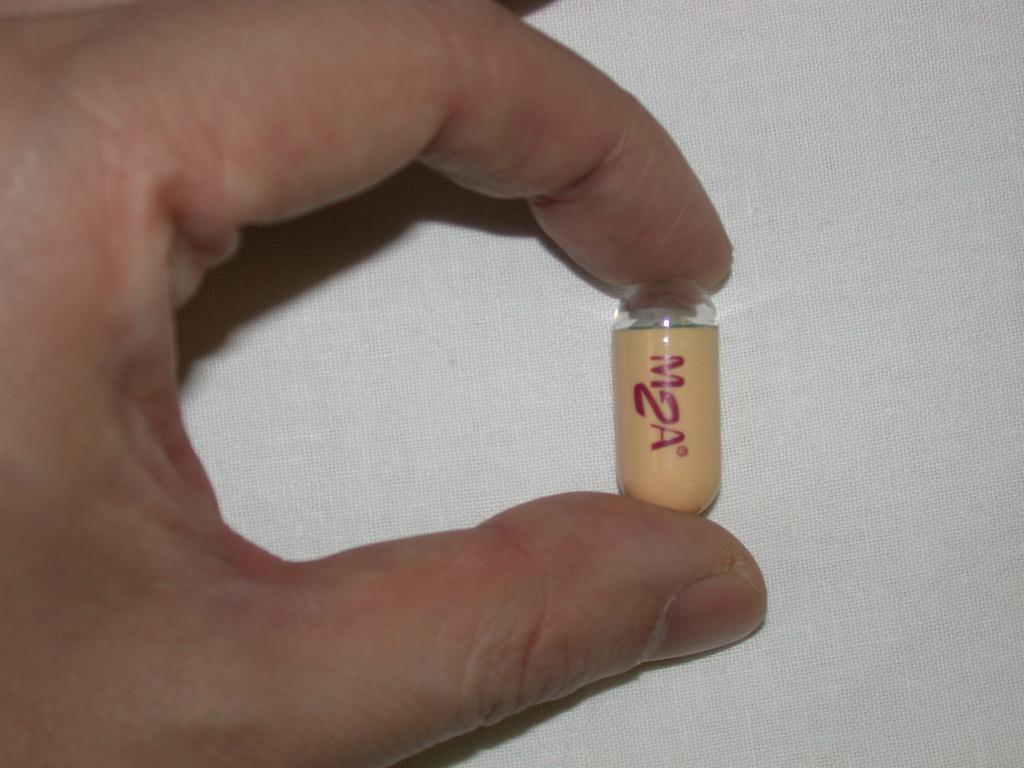
58 Capsule endoscopy 1999: first wireless capsule endoscope used in a human volunteer. Capsule consists of battery, camera, flash and transmitter. 2 pictures/ second transmitted to receiver worn on body.
59


60 1. Capsule Ø11 mm 26 mm Ø11 mm SB ESO 20 min operating time: FPS 10 4 FPS Antenna Gilo-4 Gulp-1 Dome Dome Optics PCB Batteries Spacer Cover Optics

61 Data recorder worn on belt Sensors applied to abdomen with adhesive pads Preparation

62
 Passage Times (Gastric & small bowel) Marker indicating location in study Captured")
63 Main Screen Minimized View Video Control Localization Suspected blood Indications (to show, first mark first duodenal image landmark) Passage Times (Gastric & small bowel) Marker indicating location in study Captured Thumbnails


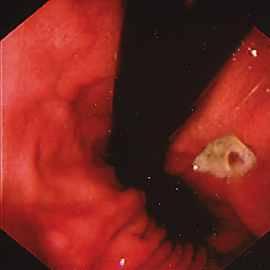
64 Capsule endoscopy findings Angiodysplasia Small bowel ulcer

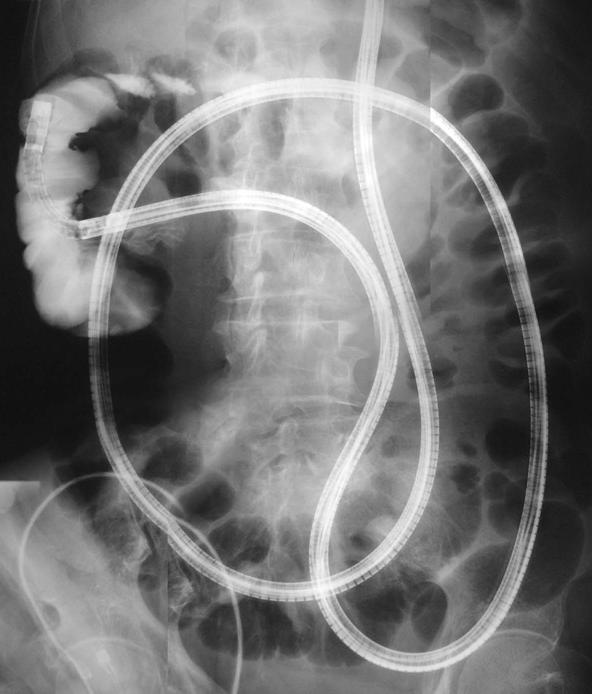
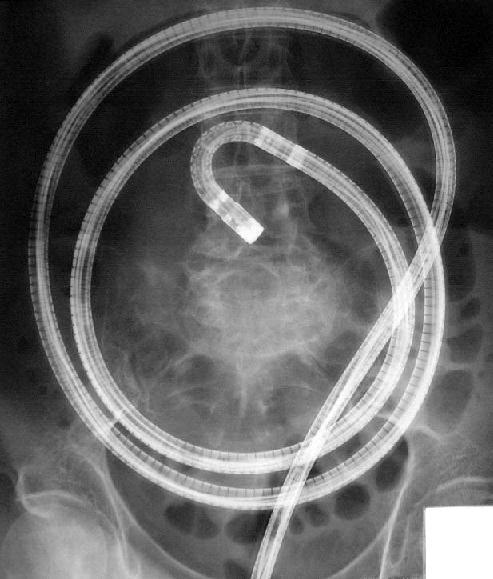
65 Double-balloon balloon enteroscopy Therapy possible. Enteroscope advanced either orally or per rectum. Sequential inflation of balloons to aid intubation.

66 Double-balloon balloon enteroscopy

67
68

69
70

71

72 Technetium red cell scan RBC labelled with 99Tc. Detects bleeding ml/min. Positive in 50% of lower GI bleeding. Alternate test usually needed before intervention.

73 Detects bleeding >0.5ml/min. Positive in 50% of lower GI bleeds overall, 60-70% when actively bleeding. Administration of vasodilators, anticoagulants increase yield. Angiography
74 Therapy during angiography Vasopressin infusion, embolisation. Blue dye injection into bleeding vessel aids identification during surgery.

75 Peptic Ulcer
76 Stigmata Stigmata of bleeding Rebleeding risk Spurting vessel % Visible vessel 50% Adherent clot 30-35% Oozing from ulcer 10-27% Flat spot <8% Clean base <3%

77 Spurting vessel

78 Visible vessel


79 Flat spots

80 Clean base
81 Endoscopic therapy Indicated for active bleeding/ spurting and visible vessel Benefit demonstrated for removing adherent clot and treating underlying lesion Flat spots and slow oozing alone not shown to benefit from treatment
82
83 Injection Adrenaline Sclerosant Thermal Endoscopic treatment Non-contact: laser and argon plasma Contact thermal probe BICAP probe Metallic clips
84 Injection
85 Laser and argon plasma Heating of tissue protein Contraction of arterial wall Laser therapy require direct path and accurate aiming Argon plasma cogulation useful for mucosal bleeding but not ulcer vessel
86

87 Argon plasma coagulator

88
89 Heater probe Seals the vessel Firm tamponade needed Endpoint is footprint at site of vessel

90 Heater probe
91 Metallic clips Difficult to apply tangentially Effective for arterial bleeding
92
93 Second-look endoscopy Repeat endoscopy after initial treatment Repeat treatment if stigmata of bleeding +ve+ Reduction of rebleeding rate
94 Drug treatment Regular dose H2A does not affect bleeding Continuous high dose PPI infusion may lower acid and stabilise the clot, reduce rebleeding H pylori eradication if positive

95 Variceal bleeding
96 Risk of bleeding Larger size (>5mm) Red wale marking Red colour sign Advanced cirrhosis Co-existing gastric varices
97 Injection sclerotherapy First described in 1939 Injection of substances causing thrombosis, inflammation and fibrosis of varix Cyanoacrylate glue superior for gastric variceal bleeding

98
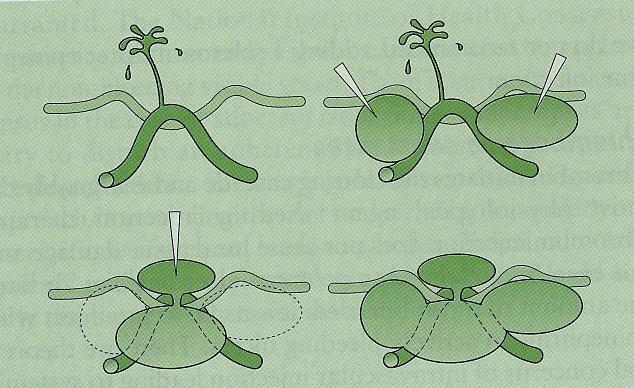
99 Band Ligation Varix approached and sucked into chamber as possible Rubber band released Used for oesophageal varices

100
101 Drug therapy Somatostatin/ octreotide Vasopressin Beta blockers May be used as adjuvant to endoscopic haemostasis
102 Summary GI bleeding sources usually identified by endoscopy Repeat endoscopy may be useful if initially negative Capsule endoscopy and enteroscopy for suspected small bowel lesions Multiple modalities for treatment, comparable efficacy
103 Summary Sclerotherapy or banding for oesophgeal varices Tissue glue for gastric varices

104
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
6/25/ % 20% 50% 19% Functional Dyspepsia Peptic Ulcer GERD Cancer Other
 Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Our evidence. Your expertise. SmartPill : The data you need to evaluate motility disorders.
 Our evidence. Your expertise. SmartPill : The data you need to evaluate motility disorders. SmartPill benefits your practice: Convenient performed right in your office Test standardization Provides direct
Our evidence. Your expertise. SmartPill : The data you need to evaluate motility disorders. SmartPill benefits your practice: Convenient performed right in your office Test standardization Provides direct
Number of studies. Endoscopic finding. Number of subjects. Pooled prevalence 95% CI
 Clinical Approach to the Patient t with Dyspepsia William D. Chey, MD, FACG Professor of Medicine University of Michigan Prevalence of Endoscopic Findings in Individuals with Dyspepsia Systematic Review
Clinical Approach to the Patient t with Dyspepsia William D. Chey, MD, FACG Professor of Medicine University of Michigan Prevalence of Endoscopic Findings in Individuals with Dyspepsia Systematic Review
Non-Ulcer Dyspepsia: what is it? What can we do with these patients? Overview. Dyspepsia Definition. Functional Dyspepsia. Dyspepsia the Basics
 Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
June By: Reza Gholami
 ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA
 MANAGEMENT OF DYSPEPSIA") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
Functional Dyspepsia. Norbert Welkovics Heine van der Walt
 Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Outline. Definition (s) Epidemiology Pathophysiology Management With an emphasis on recent developments
 Epidemiology Pathophysiology Management With an emphasis on recent developments") Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
Dyspepsia is a problem commonly seen by primary
 Concise Review for Clinicians Nonulcer Dyspepsia: What It Is and What It Is Not G. RICHARD LOCKE III, MD Nonulcer dyspepsiais a description of persistent or recurrent upper abdominal pain or discomfort
Concise Review for Clinicians Nonulcer Dyspepsia: What It Is and What It Is Not G. RICHARD LOCKE III, MD Nonulcer dyspepsiais a description of persistent or recurrent upper abdominal pain or discomfort
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Upper GI Bleeds. AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM
 Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
Upper GI Bleeds AMU Nurse Teaching Dr Clare Pollard ST6 AIM & GIM Peptic ulcer disease - GU - DU Talk Plan Important considerations in this group of patients- what you need to know Mallory Weis Tear Other
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Functional Dyspepsia
 Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
Functional Dyspepsia American College of Gastroenterology Boston Massachusetts, June 2015 Brian E. Lacy, PhD, MD, FACG Professor of Medicine Geisel School of Medicine at Dartmouth Chief, Section of Gastroenterology
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Scottish Medicines Consortium
 Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Management of dyspepsia in adults in primary care
 Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
When to Refer for OGD and the Work Up of Upper GI Malignancies
 When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
When to Refer for OGD and the Work Up of Upper GI Malignancies Dr Hong Qiantai Registrar, Department of Surgery GP Forum 27 May 2017 38 year old female, non-smoker, BMI 29 Works as investment banker Presents
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine -
 Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
Dr Simon Smale Before Endoscopy? Indications Thermal Coagulation Injection Therapy Combination Therapy Fibrin Sealant Endoclips Argon Plasma Coagulation Lysine - Haemmostop Variceal Banding Histoacryl
ICU Volume 14 - Issue 2 - Summer Matrix
 ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
ICU Volume 14 - Issue 2 - Summer 2014 - Matrix Upper Gastrointestinal Bleeding Authors David Osman, MD Medical Intensive Care Unit Paris-South University Hospitals Assistance Publique-Hôpitaux de Paris
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Reflux of gastric contents, particularly acid, into the esophagus
 Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Emergency - Upper gastrointestinal haemorrhage
 Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
Emergency - Upper gastrointestinal haemorrhage Definitions in upper gastrointestinal (UGI) haemorrhage UGI haemorrhage: bleeding that arises proximal to the ligament of Treitz i.e. from the oesophagus,
MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia. Disclosures
 The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia Lana Bistritz MD FRCPC Royal Alexandra Hospital GI Update 2016 Disclosures I have no relevant financial disclosures I will be discussing off
The PPI Doesn t Work, Now What? PPI Non-responsive Dyspepsia Lana Bistritz MD FRCPC Royal Alexandra Hospital GI Update 2016 Disclosures I have no relevant financial disclosures I will be discussing off
The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding.
 Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
Original Article ISSN (O):2395-2822; ISSN (P):2395-2814 The Role of Endoscopy in the Diagnosis and Management of Upper Gastrointestinal Bleeding. Faroze A. Khan 1, M. H. Raza 2, Vikrant 1 1 Senior Resident,
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
Blood and guts.. Haemodynamics / resuscitation. Haemodynamics / resuscitation. Blood and guts. Dr Jonathan Hoare
 Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Blood and guts. Dr Jonathan Hoare Consultant St Mary s Hospital Dr Jonathan Hoare Consultant St Mary s Hospital, Paddington Blood and guts.. Presentation Initial assessment and management risk stratification
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
Functional Dyspepsia
 Linköping University Medical Dissertations No. 792 Functional Dyspepsia Symptoms and Response to Omeprazole in the Short Term by Elisabeth Bolling-Sternevald Department of Biomedicine and Surgery, Faculty
Linköping University Medical Dissertations No. 792 Functional Dyspepsia Symptoms and Response to Omeprazole in the Short Term by Elisabeth Bolling-Sternevald Department of Biomedicine and Surgery, Faculty
Definition, Pathogenesis, and Management of That Cursed Dyspepsia
 Clinical Gastroenterology and Hepatology 2018;16:467 479 Definition, Pathogenesis, and Management of That Cursed Dyspepsia Pramoda Koduru, Malcolm Irani, and Eamonn M. M. Quigley IM F1 김영기 Dyspepsia Umbrella
Clinical Gastroenterology and Hepatology 2018;16:467 479 Definition, Pathogenesis, and Management of That Cursed Dyspepsia Pramoda Koduru, Malcolm Irani, and Eamonn M. M. Quigley IM F1 김영기 Dyspepsia Umbrella
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Gastrointestinal bleeding: the management of acute upper gastrointestinal bleeding 1.1 Short title Acute upper GI bleeding
SASKATCHEWAN REGISTERED NURSES ASSOCIATION
 DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
The usual dose is 40 mg daily with amoxycillin 1.5 g (750 mg b.d.) for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.
 for 2 weeks. Up to 2 g/day of amoxycillin has been used in clinical trials.") Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
Name Gasec - 2 Gastrocaps Composition Gasec-20 Gastrocaps Each Gastrocaps contains: Omeprazole 20 mg (in the form of enteric-coated pellets) Properties, effects Proton Pump Inhibitor Omeprazole belongs
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA
 GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
Management of Dyspepsia
 MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
SUPPLEMENTARY INFORMATION Associated with
 Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Endoscopic Management of Vascular Lesions of the GI tract
 Endoscopic Management of Vascular Lesions of the GI tract Lake Louise, June 2014 Sergio Zepeda Gómez MD Assistant Professor Division of Gastroenterology University of Alberta, Edmonton Best Practice &
Endoscopic Management of Vascular Lesions of the GI tract Lake Louise, June 2014 Sergio Zepeda Gómez MD Assistant Professor Division of Gastroenterology University of Alberta, Edmonton Best Practice &
Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication
 Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING
 Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Laboratory Technique ROLE OF CAPSULE ENDOSCOPY IN OBSCURE GASTROINTESTINAL BLEEDING J. JAIN* ABSTRACT Capsule endoscopy (CE) is a safe, non invasive technique for evaluation of small bowel (SB) lesions.
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Picking up their Pieces: Emergency Management of GI Bleeds
 Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
Picking up their Pieces: Emergency Management of GI Bleeds Dr Sean L Preston Consultant Gastroenterologist Stemming the Flow.. Clinical Cases (who s to blame?) Initial assessment and management risk stratification
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap. Simon McPherson, Vascular Interventional Radiologist, Leeds
 Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastro-Intestinal Bleeding- Interventional Radiology turning off the tap Simon McPherson, Vascular Interventional Radiologist, Leeds Scale UK 100,000 /year Commonest Vascular IR on-call 75% UGIB 65% NVUGIB
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Indigestion (dyspepsia)
") Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
A cute upper gastrointestinal haemorrhage is
 399 BEST PRACTICE Management of haematemesis and melaena K Palmer... Acute upper gastrointestinal bleeding is a common medical emergency which carries hospital mortality in excess of 10%. The most important
399 BEST PRACTICE Management of haematemesis and melaena K Palmer... Acute upper gastrointestinal bleeding is a common medical emergency which carries hospital mortality in excess of 10%. The most important
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital ABSTRACT
 Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Original Article Jewsuebpong T THAI J GASTROENTEROL 2008 Vol. 9 No. 2 May - Aug. 2008 67 UGI Bleeding: Impact and Outcome of Early Endoscopy at the Referral Community Hospital Jewsuebpong T ABSTRACT Background:
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY
 GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY DEFINITIONS GERD -Involuntary, effortless passage of gastric contents into the oesophagus +/-ejected from the mouth resulting in troublesome symptoms or complications
GASTRO-OESOPHAGEAL REFLUX DR RONALDA DELACY DEFINITIONS GERD -Involuntary, effortless passage of gastric contents into the oesophagus +/-ejected from the mouth resulting in troublesome symptoms or complications
Disclosures. GI Motility Disorders. Gastrointestinal Motility Disorders & Irritable Bowel Syndrome
 Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
Urea Breath Test for Diagnosis of Helicobactor pylori. Original Policy Date 12:2013
 MP 2.04.04 Urea Breath Test for Diagnosis of Helicobactor pylori Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index
MP 2.04.04 Urea Breath Test for Diagnosis of Helicobactor pylori Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
Note No nausea or vomiting before collapse increases the risk of an arrhythmia. A
 174 40 TACHYCARDIAS SYMPTOMS AND SIGNS Think about cardiac arrhythmias in patients with: palpitations D dyspnoea B chest pain D dizziness or syncope D cardiac arrest. D Ask about: any nausea or vomiting
174 40 TACHYCARDIAS SYMPTOMS AND SIGNS Think about cardiac arrhythmias in patients with: palpitations D dyspnoea B chest pain D dizziness or syncope D cardiac arrest. D Ask about: any nausea or vomiting
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Setting The setting was primary care. The economic study was conducted in Canada.
 Treating Helicobacter pylori infection in primary care patients with uninvestigated dyspepsia: the Canadian adult dyspepsia empiric treatment - Helicobacter pylori positive (CADET-Hp) randomised controlled
Treating Helicobacter pylori infection in primary care patients with uninvestigated dyspepsia: the Canadian adult dyspepsia empiric treatment - Helicobacter pylori positive (CADET-Hp) randomised controlled
QUICK QUERIES. Topical Questions, Sound Answers
 QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
Occult GI Bleed. July 2015
 Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Helicobacter 2008;13:1-6. Am J Gastroent 2007;102: Am J of Med 2004;117:31-35.
 An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
KEYWORDS Dyspepsia, Acid Peptic Disease, Helicobacter Pylori, Urease, Giemsa, Peptic Ulcer, Non-Ulcer Dyspepsia.
 INCIDENCE OF HELICOBACTER PYLORI WITH ACID PEPTIC DISEASE AND MALIGNANT CONDITIONS OF UPPER GASTROINTESTINAL TRACT IN A TERTIARY CENTRE - A PROSPECTIVE STUDY Karunamoorthy Rajachidambaram 1, Dinkaran Kaarthesan
INCIDENCE OF HELICOBACTER PYLORI WITH ACID PEPTIC DISEASE AND MALIGNANT CONDITIONS OF UPPER GASTROINTESTINAL TRACT IN A TERTIARY CENTRE - A PROSPECTIVE STUDY Karunamoorthy Rajachidambaram 1, Dinkaran Kaarthesan
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Original Article. Rattanasupar A Attasaranya S Ovartlarnporn B ABSTRACT
 74 THAI J GASTROENTEROL 2010 Esophagogastroduodenoscopy (EGD) plus Transabdominal Ultrasound (TUS) for Diagnosed Dyspepsia in Elderly Patients Original Article Esophagogastroduodenoscopy (EGD) plus Transabdominal
74 THAI J GASTROENTEROL 2010 Esophagogastroduodenoscopy (EGD) plus Transabdominal Ultrasound (TUS) for Diagnosed Dyspepsia in Elderly Patients Original Article Esophagogastroduodenoscopy (EGD) plus Transabdominal
An approach to dyspepsia for the pharmacist
 An approach to dyspepsia for the pharmacist Ilse Truter, DCom, BPharm, MSc, PhD, Drug Utilization Research Unit (DURU) Department of Pharmacy, Nelson Mandela Metropolitan University Correspondence to:
An approach to dyspepsia for the pharmacist Ilse Truter, DCom, BPharm, MSc, PhD, Drug Utilization Research Unit (DURU) Department of Pharmacy, Nelson Mandela Metropolitan University Correspondence to:
Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Nonvariceal Upper Gastrointestinal Bleeding ABSTRACT
 44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
44 Original Article Upper Gastrointestinal Bleeding Score for Differentiating Variceal and Jaroon Chasawat Varayu Prachayakul Supot Pongprasobchai ABSTRACT Background: Upper gastrointestinal bleeding (UGIB)
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Clinical Evaluation of Himcocid Suspension in Patients with Non-ulcer Dyspepsia
 [The Antiseptic (21): (98), 11, 49-411] Clinical Evaluation of Himcocid Suspension in Patients with Non-ulcer Dyspepsia Upadhyaya, B.N., Reader and Head, and Khagen Basumathy, Junior Resident Department
[The Antiseptic (21): (98), 11, 49-411] Clinical Evaluation of Himcocid Suspension in Patients with Non-ulcer Dyspepsia Upadhyaya, B.N., Reader and Head, and Khagen Basumathy, Junior Resident Department
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Clinical guideline Published: 13 June 2012 nice.org.uk/guidance/cg141
 Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Acute upper gastrointestinal bleeding in over 16s: management Clinical guideline Published: June 2012 nice.org.uk/guidance/cg141 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 2: Abdominal Pain
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 2: Abdominal Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 2: Abdominal Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and
Functional dyspepsia: recent advances in pathophysiology. Citation Hong Kong Practitioner, 1998, v. 20 n. 6, p
 Title Functional dyspepsia: recent advances in pathophysiology Author(s) Hu, HC; Lam, SK Citation Hong Kong Practitioner, 1998, v. 20 n. 6, p. 327-334 Issued Date 1998 URL http://hdl.handle.net/10722/45089
Title Functional dyspepsia: recent advances in pathophysiology Author(s) Hu, HC; Lam, SK Citation Hong Kong Practitioner, 1998, v. 20 n. 6, p. 327-334 Issued Date 1998 URL http://hdl.handle.net/10722/45089
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW
 PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related
PRESCRIBING SUPPORT TEAM AUDIT: PROTON PUMP INHIBITOR PRESCRIBING REVIEW DATE OF AUTHORISATION: AUTHORISING GP: PRESCRIBING SUPPORT TECHNICIAN: SUMMARY Dyspepsia refers to a broad range of symptoms related