Refinement of a Human Challenge Model for Evaluation of Enterotoxigenic E. coli (ETEC) Vaccines
|
|
|
- Daniel Townsend
- 5 years ago
- Views:
Transcription
1 CVI Accepts, published online ahead of print on 18 August 2011 Clin. Vaccine Immunol. doi: /cvi Copyright 2011, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved. 1 2 Refinement of a Human Challenge Model for Evaluation of Enterotoxigenic E. coli (ETEC) Vaccines Clayton Harro *1, Subhra Chakraborty 1, Andrea Feller 1, Barbara DeNearing 1, Alicia Cage 1, Malathi Ram 1, Anna Lundgren 2, Ann-Mari Svennerholm 2, August L. Bourgeois 3, Richard I. Walker 3, and David A. Sack 1 1 Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 2 Department of Microbiology and Immunology, University of Gothenburg, Gothenburg, Sweden 3 PATH, Washington, DC Running head: Human Challenge Model for Enterotoxigenic E. coli (ETEC) Key words: Escherichia coli; ETEC; challenge model; H10407; vaccine Word count: 5,214 This study was supported by PATH. Correspondence should be directed to: Dr. Clayton Harro, Center for Immunization Research, Johns Hopkins Bloomberg School of Public Health, 624 North Broadway, Hampton House Room 117, Baltimore, MD 21205; e- mail charro@jhsph.edu.
2 ABSTRACT Enterotoxigenic E. coli (ETEC) strain H10407 (serotype O78:H11, LT+, ST+, CFA I) induces reliably high diarrheal attack rates (ARs) in a human challenge model at doses >10 9 CFU. A descending dose challenge study was conducted with changes to standard fasting time and buffer formulation, seeking conditions that permit lower inocula while maintaining reproducibly high ARs. In Cohort 1, 20 subjects were fasted overnight and randomized 1:1:1:1 to receive H10407 at doses of 10 8 CFU w/bicarbonate, 10 8 CFU w/ceravacx, 10 7 CFU w/bicarbonate, or 10 7 CFU w/ CeraVacx. Subsequent cohorts received H10407 (10 7 CFU w/bicarbonate) with similar fasting conditions. Cohort 2 included 15 ETEC-naïve volunteers. Cohort 3 included 10 ETECnaïve volunteers and 10 rechallenged volunteers. In all, 25/35 (71%) ETEC-naïve recipients of 10 7 CFU of H10407 developed moderate-to-severe diarrhea (average maximum stool output/24 hours = 1042gms); and most (97%) shed H10407 (maximum geometric mean titer = 7.5 x 10 7 CFU/gram of stool). Only one of 10 rechallenged volunteers developed diarrhea. These rechallenged subjects had reduced intestinal colonization, reflected by quantitative microbiology of fecal samples. Among the 35 ETEC-naïve subjects, anti-lipopolysaccharide (LPS) O78 serum antibody responses were striking with positive IgA and IgG antibody responses in 33/35 (94%) and 25/35 (71%), respectively. Anti-LTB serum IgA and IgG responses developed in 19/35 (54%) and 14/35 (40%), respectively. Anti-CFA/I serum IgA and IgG responses were detected in 15/35 (43%) and 8/35 (23%). After the second challenge, participants exhibited blunted anti- LPS and LTB responses but a booster response to CFA/I. This ETEC model should prove useful in the future evaluation of ETEC vaccine candidates.
3 48 INTRODUCTION Enterotoxigenic Escherichia coli (ETEC) is a leading bacterial cause of infectious diarrhea in infants and adults living in developing countries and accounts for approximately 30% of traveler s diarrhea in visitors to these regions (1, 7, 22, 24-27, 29, 30). ETEC strains vary in their pathogenicity as a result of differences in expression of heat-labile toxin (LT), heat stable toxin (ST), and several colonization factors (CFAs) that are associated with attachment and colonization in the gut (24, 31). For more than 40 years, human challenge models have been the mainstay for clinical evaluation of ETEC pathogenesis and immunology(8, 16), and for assessment of therapeutic and protective efficacy of antibiotics (3), probiotics (4) and candidate vaccines (19, 20). Recent availability of new resources for ETEC vaccine development has renewed interest in ETEC challenge models. A model with a reliably high attack rate could provide a vehicle for evaluation and screening of vaccine efficacy before conducting expensive, long-term field trials in endemic areas or among at risk travelers. Mixed results from prior ETEC vaccine challenge studies have fueled concerns that ETEC challenge models used in the past required higher inocula than those typically encountered in natural exposure, overwhelming vaccine-induced protective immunity (35). Several wellcharacterized ETEC strains have been used in challenge studies. ETEC strain H10407 has been used most frequently, having been fed to more than 250 subjects most often for preventive ETEC vaccine proof-of-concept studies (3, 12, 13, 15, 19). ETEC H10407 was originally isolated from an adult with severe diarrhea in Dhaka, Bangladesh. It produces both LT and ST, and expresses colonization factor I (CFA/I) (10). ETEC H10407 induces acute, watery diarrhea in otherwise healthy, ETEC-naïve, subjects when they are challenged with >10 8 colony forming units (CFU) 70 of bacteria(19, 21). The majority of ETEC H10407 challenge studies to date have utilized
4 71 72 challenge inocula of 10 9 in order to assure diarrheal attack rates of >70%, which are needed to achieve statistical significance during small volunteer studies Lower ETEC doses have yielded inconsistent attack rates (16, 18), but lower challenge doses have been used effectively for other well established enteric disease challenge models, such as Shigellae (10 2 CFU),(14, 33) Vibrio cholerae (10 5 CFU),(5, 28) and more recently Campylobacter jejuni (10 5 ) (34). Therefore, development of a lower inoculum ETEC H10407 challenge model could be useful when evaluating ETEC vaccines in the future. Typically, ETEC challenge studies have stipulated that on the day of challenge subjects eat breakfast, fast for ninety minutes, drink 120 ml of a sodium bicarbonate buffer solution followed one minute later by ingestion of the challenge inoculum dissolved in 30 ml of bicarbonate buffer, and finally fast again for ninety minutes after challenge. Here, we report on a series of studies designed to refine the ETEC H10407 challenge model for future use with volunteer studies. We elected to examine whether we could achieve a high attack rate (AR) while using a lower inoculum dose if we changed the buffer or if we extended the duration of fasting prior to the challenge. We also wanted to determine if exposure to a first challenge would protect volunteers who were rechallenged using this modified model. Finally, we wanted to measure the serum antibody responses following a first and second challenge. MATERIALS AND METHODS Regulatory approval. The protocol was conducted under BB-IND 12,243 at the Center for Immunization Research (CIR), Johns Hopkins Bloomberg School of Public Health. Approval to conduct the study was provided by the Western Institutional Review Board (Olympia,
5 93 94 Washington) for the Johns Hopkins Bloomberg School of Public Health and PATH and by the Institutional Biosafety Committee of the Johns Hopkins Institutions Study subjects. Healthy, year old, male or female subjects were recruited for the study using print and electronic media advertisement and by word-of-mouth. The study was explained to subjects in detail, time was provided for informed consent review, the consent form was individually reviewed with each subject by a member of the study team, and signed, witnessed consent was obtained. In addition, all subjects were required to pass a written assessment of understanding about the study that reviewed the study rationale, procedures, and risks. The prechallenge health status of subjects was assessed by written and oral medical history, physical examination, complete blood count, urinalysis, urine toxicology, blood chemistries, and tests for liver and kidney function, HIV-1, hepatitis B, and hepatitis C. Subjects were excluded if they had significant medical problems detected by history, physical examination, or screening laboratory tests, or if HIV-1, hepatitis B or hepatitis C tests were positive. Challenge strain. The challenge strain (H10407) is an ETEC serotype O78:H11, that produces both LT and ST and also produces CFA/I. It is sensitive to ampicillin, trimethoprim / sulfamethoxazole and ciprofloxacin which are typically used to treat ETEC H10407 infections. A cgmp-quality production cell bank (PCB) for ETEC H10407 was prepared by the Walter Reed Army Institute of Research (WRAIR) Pilot Bioproduction Facility (Silver Spring, Maryland). The manufacturing information and production records for the PCB of these strains were provided to the FDA under BB-IND-7766 (Batch Production Record: , lot # 0519). The ETEC H10407 challenge strain was stored in 2 ml cryostorage tubes (1 ml per tube) held at
6 o C + 10 o in the Bio-production facility at WRAIR. Cryovials containing organisms from this PCB were transferred on dry ice from WRAIR to the CIR Enterics Research Laboratory, Johns Hopkins Bloomberg School of Public Health, and stored at o C in a locked and temperature monitored freezer. Study design. The study was conducted in three cohorts between February 15, 2009 and August 15, Each cohort was admitted as a group into the 30-bed CIR Isolation Unit. For each cohort, ETEC H10407 was used as the challenge strain, and all subjects received a challenge with the virulent organism; none of the subjects received a placebo challenge. For Cohort 1, 20 subjects were given the challenge, but the cohort participants were randomly divided into four subgroups of five subjects per group in a double-blinded manner. Subgroup A received a dose of 2x10 8 CFU with bicarbonate buffer; subgroup B received a dose of 2x10 8 CFU with CeraVacx buffer; subgroup C received a dose of 2x10 7 CFU with bicarbonate buffer; and subgroup D received a dose of 2x10 7 CFU with CeraVacx buffer. Based on the high attack rates and similar clinical outcomes observed in all subgroups of Cohort 1, the study Steering Committee decided that subsequent cohorts should receive a dose of 2x10 7 CFU with bicarbonate buffer. For Cohort 2, 15 subjects were administered a dose of 2x10 7 CFU with bicarbonate buffer. For Cohort 3, 20 subjects were administered a dose of 2x10 7 CFU with bicarbonate. However, 10 of these subjects in Cohort 3 were new subjects who had not participated in the study previously. The other 10 were subjects who had experienced ETEC-associated diarrhea three months earlier while participating in any subgroup of Cohort 1, or two months earlier while participating in Cohort 2.
7 Inocula and challenge. As in prior ETEC challenge studies, inocula were prepared from fresh, plate-grown organisms, using a study specific procedure (SSP) which validated each step of the process. A dedicated laboratory room and microbiological safety cabinet were used for the inocula preparation. Approximately 66 hours before challenge, a frozen vial of ETEC H10407 was thawed and streaked onto colonization factor antigen agar (CFA agar (9)) and MacConkey agar (Becton, Dickinson and Company, Sparks, MD). The MacConkey agar plate served to further document the purity of the bacteria prior to administration to subjects. After hours of incubation at o C, a sterile cotton swab was used to touch 10 colonies from the CFA agar plate, and then the swab was mixed into a tube with 3 ml of sterile phosphate buffered saline (PBS) (Fisher Scientific, Fair Lawn, NJ). The suspension from the PBS was used to inoculate a lawn onto 6 CFA agar plates for incubation at o C. After hours the CFA agar plates were harvested using sterile PBS and the resulting bacterial suspension further diluted in saline for optical density determination at 600nm. The optical density of the suspension was adjusted to equal that corresponding to the desired concentration of bacterial cells per ml of the inoculum. The number of CFU in the inocula was determined by titrating and plating on Luria agar plates (Becton, Dickinson and Company, Sparks, MD) before and after administration to volunteers. A sample of the final inoculum was also examined by Gram stain for purity and by agglutination in anti-h10407 antiserum before being administered to subjects. The bicarbonate buffer was prepared from USP-grade sodium bicarbonate (Fisher Scientific, Fair Lawn, NJ) by dissolving grams of sodium bicarbonate in 1000 ml of sterile water for irrigation (Hospira, Inc., Lake Forest, IL). Subjects randomized to the sodium bicarbonate group received a total dose of 2 grams of sodium bicarbonate. The CeraVacx was
8 prepared from the commercial product (Cera Products, Inc., Columbia, Maryland) by dissolving 9.5 grams of the powder into 150 ml of sterile water for each dose. Each dose contained 7 grams of rice syrup, 2 grams of sodium bicarbonate, and 0.5 grams of trisodium citrate. Volunteers were admitted to the CIR Isolation Unit the day prior to challenge. All subjects were offered a snack between hours the night prior to challenge and then not allowed any oral intake for the following ~ 9 hours before challenge and ~90 minutes after challenge. At approximately 0900 hours on the day of challenge, subjects drank 120 ml of buffer (sodium bicarbonate or CeraVacx ) to neutralize gastric acidity. Approximately one minute later, subjects drank the ETEC H10407 inoculum dissolved in 30 ml of buffer solution. In Cohort 1, the addition of the bacterial inoculum was done by the research pharmacist in a manner which maintained blinding of the subjects and the investigators. The inocula were given to the subjects using opaque bottles to hide the appearance of the buffers, since they differed slightly in appearance. Clinical evaluation of subjects. Medical interviews and physical examinations were performed daily by the Principal Investigator and additional medical assessments and vital sign measurements were performed by the study team >3 times daily. Active solicitation regarding the following symptoms took place during the medical interview: fever, vomiting, nausea, abdominal pain, abdominal cramping, myalgias, malaise, bloating, flatulence, headache, lightheadedness, chills, constipation and anorexia. Fever was defined as an oral temperature >100.4 F. Fever severity was categorized as mild (>100.4 F and <101.1 F), moderate (>101.1 F and <102.0 F) and severe (>102 F). Vomiting was classified as mild (1 episode within a 24-hour period), moderate (2 episodes within a 24-hour period) or severe (>2 episodes within a 24 hour
9 period). Other constitutional symptoms were graded as follows: mild (discomfort noted, but no disruption of normal daily activities; relieved with or without symptomatic treatment); moderate (discomfort sufficient to reduce or affect normal daily activity; only partially relieved with symptomatic treatment); or severe (discomfort sufficient to reduce or affect normal daily activity considerably; not relieved with symptomatic treatment). Each stool was collected using a stool collection receptacle, weighed, assessed for the presence of blood, and graded as follows: grade 1 (firm, formed); grade 2 (soft, formed); grade 3 (viscous opaque liquid or semi-liquid which assumes the shape of the container); grade 4 (watery, non-viscous, opaque liquid which assumes the shape of the container); grade 5 (clear or translucent, watery or mucoid liquid which assumes the shape of the container). Diarrhea was defined as 1 loose/liquid stool ( Grade 3) of >300 grams or 2 loose/liquid stools totaling 200 grams during any 48-hour period within 120 hours of challenge with ETEC H Diarrhea was classified as mild (1-3 diarrheal stools totaling grams/24 h), moderate (4-5 diarrheal stools or grams/24 h), or severe (6 or more diarrheal stools or >800 grams/24 h). As soon as a subject passed a diarrheal stool, oral rehydration was initiated using oral rehydration solution (Ceralyte, Cera Products, Inc., Columbia, MD) and other fluids, with the aim of replacing the subject s output. If a subject had severe vomiting, passed a large volume stool (>300 grams) at diarrhea onset, or for other reasons was unable to consume adequate amounts of oral replacement fluids to maintain hydration, intravenous fluids were given. Prior to discharge, a 3 day course of antibiotic therapy was initiated to clear the infection. All subjects were administered ciprofloxacin (500 mg twice daily). Trimethoprim-sulfamethoxazole (160mg/800mg twice daily), or amoxicillin (500 mg three times daily) were used as a backup
10 antibiotics if ciprofloxacin could not be used. Early antibiotic treatment was provided to subjects who had severe diarrhea, moderate diarrhea for 2 days, and mild or moderate diarrhea with two or more of the following symptoms: fever (> F), vomiting, and certain severe constitutional symptoms including abdominal pain/cramping, headache, myalgias, or nausea. In addition, the Principal Investigator (PI) could initiate early treatment if it was warranted for other reasons. Subjects who did not meet criteria for early antibiotic therapy were treated with antibiotics approximately 120 hours after challenge. To be eligible for discharge subjects needed to have at least 2 negative stool cultures for ETEC H Subjects were seen as outpatients in the clinic 10 and 28 days after challenge and contacted by telephone about 3 months after challenge. Shedding. After challenge, all stool specimens were collected, graded, and weighed. Up to 2 samples per day were collected for fecal microbiology to detect the challenge strain. Colonization was defined as isolation of ETEC H10407 in two stool specimens collected at least 24 hours after challenge. If a subject was unable to produce at least one stool within the 24 hour period, a rectal swab was obtained. Semi-quantitative cultures were performed on stool samples but not on rectal swabs. Rectal swabs were placed in Cary-Blair media and then streaked onto MacConkey agar for overnight incubation. Up to 5 colonies appearing to be E. coli were tested for agglutination with antiserum to H If at least one of these colonies agglutinated, the sample was considered positive. If none of the 5 colonies agglutinated, the sample was considered negative.
11 For semi-quantitative microbiology, the fecal sample was first diluted ten-fold up to 10 5 dilution in PBS. 0.1 ml aliquots of these dilutions were spread as a lawn onto MacConkey agar. After overnight incubation, the concentration of bacteria which appeared to be E. coli was calculated and the proportion of these colonies (of 5 colonies tested) which agglutinated with anti-h10407 antisera was recorded. The anti-h10407 antiserum was prepared in rabbits at the International Centre for Diarrhoeal Disease Research, Bangladesh using formalinized ETEC H10407 cells as the immunogen. Serology. Blood specimens were collected from volunteers in all cohorts on Study Days 0, 7, 10, and 28 and serum was separated to measure systemic immune responses. For Cohort 3 only, blood specimens were also collected on Study Day 84 to measure serologic immune responses. Immunological responses to purified colonization factor antigen I (CFA/I) (University of Gothenburg), lipopolysaccharide to the O78 antigen (LPS) (University of Gothenburg), and heat labile enterotoxin binding subunit (LTB) (Sigma-Aldrich, St. Louis, MO, USA) were assessed by measuring specific IgA and IgG in serum by ELISA. Secondary antibodies used were goat antihuman IgG or IgA conjugated to HRP (KPL, Gaithersburg, Maryland USA). A >2.5- fold rise in titer from baseline was considered a response. Study Day 0 was the baseline for determining the response to ETEC H Statistical analyses. Chi-square and t-tests were used to determine differences between groups as appropriate for categorical and continuous variables. The sample size for Cohort 1 was selected to provide preliminary information on approximate attack rates. With the addition of subjects in Cohorts 2 and 3, the numbers of subjects receiving the selected challenge dose
12 increased to 35. With this number of subjects, and with an assumed attack rate of 70%, the 95% confidence interval for the attack rate was 55% to 85%. The sample sizes for the third cohort were selected assuming a protective efficacy rate of 90% among the re-challenged subjects and an attack rate of 70% in the naïve group. With these assumptions, there was a 90% power to detect a significant difference in attack rates between naïve and rechallenged subjects. RESULTS Demographics. A total of 45 ETEC H10407 naïve subjects were enrolled in Cohorts 1-3. Seventy-six percent of subjects were African-American, 64% of subjects were male and the mean age was 31 years old (Table 1). Ten subjects from Cohort 1 or 2 who had documented ETEC H10407-induced diarrheal illness after initial challenge were rechallenged in Cohort 3. One subject enrolled in Cohort 1 was challenged, but was treated with antibiotics prior to any illness onset and discharged 76 hours after challenge due to noncompliance with study procedures. Outpatient follow-up of this subject confirmed no clinical illness. Clinical symptoms. Cohort 1: Clinical outcomes for each of the subgroups in Cohort 1 are summarized in Table 2a. Diarrheal attack rates were similar across groups. Nearly all subjects who completed the ETEC challenge and ensuing follow-up developed moderate to severe diarrheal illness, regardless of dose or buffer. In addition, clinical characteristics of illness observed in each group were similar. Though the number of subjects in each group was small, the frequency of fever, early antibiotic treatment and intravenous fluid use did not differ significantly between groups. Some subjects had unique clinical presentations. Subject #101 who received ETEC H x10 7 CFU with
13 bicarbonate (Cohort 1C) had no evident illness. Subject #120 who received ETEC H x10 8 CFU with Ceravacx (Cohort 1B) had two distinct episodes of moderate diarrheal illness that were separated by 46 hours during which time stools were normal. Upon reviewing the clinical records from Cohort 1, the Steering Committee concluded that the volunteers in Cohorts 2 and 3 should receive an inoculum dose of 2x10 7 CFU with bicarbonate buffer. Cohort 2: The clinical outcomes for each subject in Cohort 2 are shown in Table 2b. Ten of fifteen subjects (67%) developed moderate to severe diarrheal illness, confirming clinical trends observed in Cohort 1. One additional subject (#203) developed loose stools and constitutional symptoms consistent with ETEC-induced illness, beginning 30 hours post-challenge. The subject developed severe constitutional symptoms in association with frequent loose stools and met criteria for early antibiotic therapy. However, symptoms rapidly resolved post-treatment and the subject never met the case-definition of diarrhea and was therefore not considered a case. The total volume of diarrheal purge observed in those who were cases varied widely from approximately ⅓ liter to nearly 6 liters. Cohort 3: Attack rates and clinical outcomes observed in ETEC H10407 naïve subjects in Cohort 3 were similar to those seen in the earlier two cohorts. Nine of ten (90%) naïve subjects developed diarrheal illness, the majority of which was classified as moderate-to-severe (Table 2b). In contrast, one of ten subjects rechallenged with ETEC H10407 had diarrhea which was classified as mild. This subject had a single loose stool of approximately 350 grams, but also vomited three times, was given IV fluids, and was started on early antibiotics. The remainder of
14 subjects rechallenged with ETEC H10407 had no diarrheal illness. The difference in attack rates between naïve and rechallenged volunteers was highly significant (Chi square 9.8, p=0.002) Combined Outcomes: A total of 35 naïve subjects received ETEC H10407 at a dose of 2x10 7 (Table 2b). Twenty-eight (80%) of these subjects developed diarrhea, and the majority of this illness was classified as moderate-to-severe diarrhea. The mean incubation period across all groups was 53 hours (range=21-95 hours). Mean stool outputs exceeded one liter in each group. Fever occurred in 6 of 35 subjects (17%), with a maximum recorded temperature of F. Fifteen (43%) subjects vomited and the maximum number of vomiting episodes was 5. Overall, 7 of 35 subjects (20%) were given intravenous fluids during the study. Among all subjects (including those who were challenged twice), 11 of 12 (92%) subjects who were given IVs had vomited, and six of 17 (35%) who vomited were given IVs. Twenty-one subjects (60%) were administered early antibiotic therapy, which likely had the effect of reducing both the quantity of ETEC H10407 shedding and the duration of illness. Post-challenge solicited symptoms reported by subjects rechallenged with ETEC H10407 were remarkably diminished compared to postchallenge symptoms reported by ETEC H10407 naïve subjects, reflecting additional clinical evidence of homologous protection (Table 3). Microbiology. All evaluable subjects in Cohorts 1 and 2 shed ETEC H10407 in their stool postchallenge, with geometric mean maximum concentrations of approximately 2x10 8 CFU per gram in those receiving the 10 8 dose and 8x10 7 CFU per gram in those receiving the 10 7 dose (Table 4). Similarly, 90% of H10407 naïve subjects in Cohort 3 shed the challenge organism. One ETEC H10407 naïve subject who had no diarrheal illness did not shed H All but one
15 rechallenged subject challenged in Cohort 3 shed the challenge organism. Notably, the geometric mean maximum concentration in those who were rechallenged was approximately 3x10 5 CFU per gram, two logs lower than in naïve subjects (p <0.02 versus naïve subjects) challenged with the same dose, portending protection. Serology. In Cohort 1, there were no significant differences in post-challenge serum immune responses between groups receiving sodium bicarbonate and CeraVacx and between groups receiving 10 7 and 10 8 doses. Combined serological results from ETEC-naïve recipients in all cohorts, showed a dramatic increase in serum IgA and IgG immune responses to LPS O78. 94% (33 of 35) and 71% (25 of 35) of subjects demonstrated an elevated IgA and IgG response to H10407 LPS, respectively (p<0.01 for IgA and p<0.01 for IgG). In contrast, only 30% (3 of 10) of rechallenged participants responded to LPS IgA and none responded to LPS IgG (Table 5). In both the naïve and rechallenged groups the highest titers were observed on Study Day 10. The increase in geometric mean titer (GMT) for naive volunteers was 62 fold and 7 fold higher on Study Day 10 for IgA and IgG respectively, compared to baseline. The baseline GMT titer of anti-lps IgG of rechallenged volunteers was almost 2 fold higher than the baseline GMT of naïve volunteers (Figure 1A). Combined serological results from ETEC-naïve recipients in all cohorts showed >2.5 fold rises in anti-ltb serum IgA and IgG responses developed in 54% (19 of 35) and 40% (14 of 35), respectively. In contrast, only 20% (2 of 10) of rechallenged volunteers mounted anti-ltb IgA responses and none of them developed anti-ltb IgG responses (p=0.08 for IgA and p=0.02 for
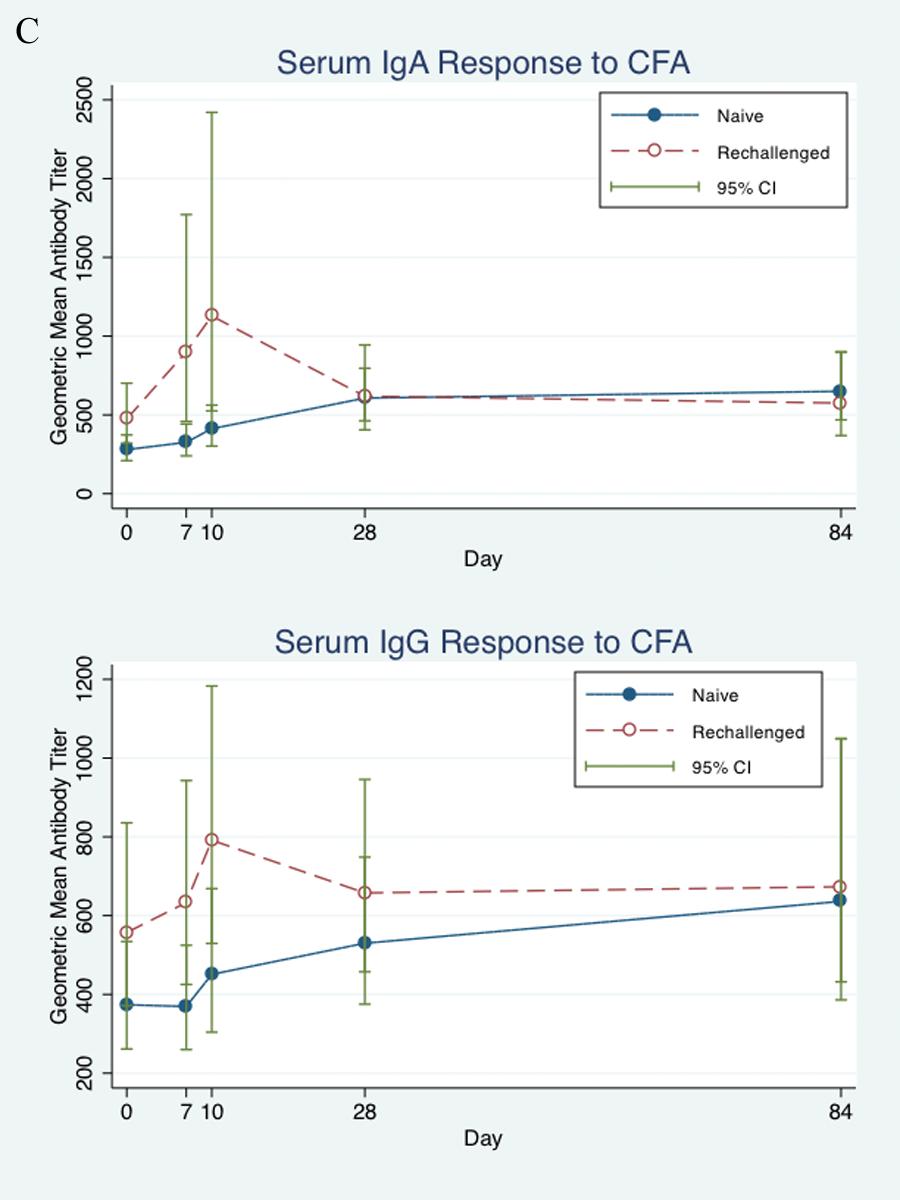
16 IgG). In the ETEC-naïve group the highest post-challenge LTB titers were seen on Study Day 10 for IgA and on Study Day 28 for IgG. As shown in Figure 1B, LTB geometric mean titers (GMT) were 3 fold and 2.6 fold higher than baseline (Study Day 0), respectively The kinetics of the anti CFA/I antibody rises were somewhat different than responses to LPS and LTB. The naïve and the rechallenged groups responded with similar frequencies to CFA/I. 43% (15 of 35) and 23% (8 of 35) of naïve volunteers responded to CFA/I with IgA and IgG responses respectively, while 30% (3/10) and 20% (2/10) of rechallenged volunteers responded to CFA/I with IgA and IgG responses (p=not significant). Notably, in naïve volunteers the highest CFA/I titer was observed on Study Day 28 in Cohorts 1 and 2 and on Study Day 84 in Cohort 3 (Study Day 84 was not done in Cohorts 1 and 2). By contrast, the rechallenged subjects had a more rapid response, with a peak on Study Day 10 (Figure1C). DISCUSSION This study had three primary goals. First, we wanted to determine if a high attack rate could be achieved with a lowered inoculum dose if the challenge was preceded by an overnight fast. Second, we intended to document clinical protection against homologous re-challenge using this lowered inoculum dose. Third, we wanted to measure the serum antibody responses to a single or a repeated challenge with this strain of ETEC. The rationale for attempting to achieve a volunteer model with a lower challenge inoculum relates to the utility of the model for ETEC vaccine evaluation. There has been concern in the field of ETEC vaccines that an excessively high inoculum dose could overwhelm vaccine induced immunity which could otherwise be protective against natural infection. If one
17 were to evaluate a vaccine in volunteers who were then challenged with a high dose of virulent ETEC bacteria, one might falsely conclude that the vaccine was not protective when, in fact, it might have been efficacious if tested against a lower challenge dose. The lower dose might better represent a dose confronted in real life. This study demonstrated that a reproducibly high attack rate can be obtained with a dose of ETEC H10407 which is 2 logs lower than that typically used, if the challenge is preceded by an overnight fast. In previously used challenge models, the bacterial inoculum is given 90 minutes after breakfast, and is followed by withholding food for 90 minutes (20). Since we did not directly compare the longer and shorter fasting periods, we cannot be certain that the longer fast leads to a higher attack rate; however, the use of the longer fast was associated with a reproducibly high attack rate with this lower dose. It may be that the longer fasting period facilitates gastric transit, or that it alters the small bowel milieu in a way that facilitates ETEC colonization. Colonization is largely dependent upon the ability of bacterial adhesins to bind to target cell receptors (11,24). The presence of food particles, particularly simple sugars such as galactose, can inhibit ETEC colonization and their absence could improve colonization. Indeed, previous preclinical studies showed enhanced colonization associated with longer pre-challenge fasting periods (A. Svennerholm, personal communication). In addition, observational data from an earlier LT toxin challenge study suggested enhanced disease severity in subjects who fasted overnight before ingestion (unpublished data, D Sack). The illness observed in this study following ETEC H10407 challenge (2 x 10 7 cfu) was typical of ETEC diarrhea seen in previous ETEC H10407 challenge studies using higher inocula (>10 8 cfu), with symptoms of watery diarrhea, episodic vomiting and occasional mild fever (23
18 ). Though the mean purging was not as severe as is seen with volunteers challenged with V cholerae (28), nevertheless, about 20% were given intravenous fluids and 60% were given early antibiotics. In contrast to previous studies using a higher dose, where the mean incubation periods were typically hours (6, 20) the incubation period observed in this study was somewhat longer, generally exceeding 48 hours. An extended incubation suggests that the lower dose inoculum requires more time to colonize the small intestine and reach the high concentrations of bacteria sufficient to cause symptoms. Even though the time to symptom onset was longer in this study, post-challenge ETEC H10407 shedding by naïve subjects was similar in frequency and magnitude to observations in higher dose challenge studies (4, 18, 19). This study clearly demonstrated that subjects who experienced ETEC diarrhea earlier in the study with ETEC H10407 were protected clinically when they were exposed to a second challenge with the same strain. Homologous protection was expected since this was seen earlier in both animals and previous volunteer studies (2, 17). Nevertheless, demonstration of homologous protection with this lower dose model was important in preparation for future vaccine studies. Protection was also observed microbiologically since the mean of the maximum concentration of H10407 in stools of rechallenged subjects was more than 2 logs lower than volunteers who had not been previously exposed. Though the concentrations were lower, the challenge strain was recovered from all of the volunteers who were clinically protected. This suggests that immune protection was not mediated by sterile immunity. Rather, targeted immunological responses likely limited the ability of the bacteria to colonize and multiply to high concentrations Quantitative microbiology will provide another important outcome when evaluating candidate vaccines in the future. Table four compared the results of the quantitative
19 microbiology for Study Day 2 following challenge to the maximum numbers on any day. In fact these results are quite similar, suggesting that future studies may choose to use results from Study Day 2 without monitoring quantitative microbiology every day. Specimens obtained later may be from subjects who have already been started on antibiotics, and their results would be altered by this intervention. Volunteers challenged with H10407 had marked serological responses to known virulence antigens including LPS, LTB and CFA/I. Most striking was the response to LPS, an antigen which is not commonly measured in challenge studies with ETEC. Interestingly, serum antibody responses to LPS and LTB were muted following the second challenge suggesting that the immune protection from the first challenge interfered with the response to the second. This lesser response may be due to a blocking of the colonization of the challenge strain, resulting in less exposure of the antigen to the antigen sampling cells. The response to LT is similar to studies of a killed oral ETEC vaccine in Egypt in which the most marked response to LT antigen occurred with the first dose, but responses to a second dose were generally not observed among those who responded to the first dose (31). In contrast to the LPS and LT responses in our volunteers, subjects who received a second challenge had an accelerated and accentuated response to CFA/I antigen, suggesting a booster response to this antigen. Since CFA/I is thought to initiate intestinal colonization, this antigen apparently did contact immune cells and the booster response observed with the second challenge suggests that it likely takes more than a single dose to optimize the immune response to this antigen. Consistent with our findings, Evans observed that persons who were previously immune to CFA mounted an anti-cfa response following oral administration of purified CFA, unlike volunteers who were not immune (10). Protective immunity is thought to be related to stimulation of local intestinal immunity, and
20 future studies will be needed to determine the relationship between serum antibody responses and intestinal immune responses to ETEC infection Though the low-dose ETEC H10407 challenge model we describe here is advantageous in many respects, several limitations remain. While we were successful in maintaining a reproducibly high attack rate with a reduced challenge inoculum of 2x10 7 CFU, it is unknown whether the challenge dose could be lowered even further with this strain. In addition, it would have been ideal to directly compare these inoculum dose levels in volunteers who were fasted overnight to those with a 90 minute fast in order to establish clearly the role that a longer fast played in this model. This model used a single challenge strain which expresses LT and ST as well as CFA/I. It is unlikely that volunteer studies can be carried out with all combinations of toxin and CFA profiles. However, to facilitate development of vaccines for ETEC it would seem important to be able to demonstrate protection against ETEC diarrhea due to some additional key toxin/cfa combinations. With the rising prevalence and known pathogenicity of ETEC strains expressing ST only and CS6, the development of a relevant ETEC challenge model based on a wild-type strain containing ST +/- CS6 would be advantageous (27). Currently there are no candidate vaccines which are able to induce immunity to ST, and unless such a vaccine can be developed, vaccines will have to rely on immunity to the colonization factors or other virulence antigens. In summary, our study documents a lower dose volunteer model for ETEC diarrhea using strain H10407, and demonstrates that rechallenge of volunteers who had previously been ill with this strain are protected from subsequent illness. The clinical protection is associated with a lower colonization of the pathogen, but not with sterile immunity. Serum antibody responses were demonstrated to LPS, LTB and CFA/I with maximum responses seen to LPS and LTB with
21 a single dose, but a booster response was seen with CFA/I following the second dose. We anticipate that this lower dose ETEC challenge model will be useful when evaluating ETEC vaccine candidates in the future.
22 ACKNOWLEDGEMENTS The authors thank all the volunteers who participated in this study. The steadfast efforts of Arlene Bloom, Denise Adams, Barbora Hnizda, George Gomes, and Fatuma Mawanda were invaluable. The instructive guidance of Dr. Larry Moulton and Dr. Jorge Flores are gratefully recognized. We also appreciate the contributions to protocol development and study monitoring provided by Amber Cox and Karen Charron. Andrea Feller is supported by the Department of Health and Human Services National Institutes of Health, National Eye Institute Training Grant Number EY07127, Clinical Trials Training Program in Vision Research. Downloaded from on December 9, 2018 by guest
23 469 REFERENCES Future directions for research on enterotoxigenic Escherichia coli vaccines for developing countries. Wkly Epidemiol Rec 81: Ahren, C. M., and A. M. Svennerholm Experimental enterotoxin-induced Escherichia coli diarrhea and protection induced by previous infection with bacteria of the same adhesin or enterotoxin type. Infect Immun 50: Black, R. E., M. M. Levine, M. L. Clements, L. Cisneros, and V. Daya Treatment of experimentally induced enterotoxigenic Escherichia coli diarrhea with trimethoprim, trimethoprim-sulfamethoxazole, or placebo. Rev Infect Dis 4: Clements, M. L., M. M. Levine, R. E. Black, R. M. Robins-Browne, L. A. Cisneros, G. L. Drusano, C. F. Lanata, and A. J. Saah Lactobacillus prophylaxis for diarrhea due to enterotoxigenic Escherichia coli. Antimicrob Agents Chemother 20: Cohen, M. B., R. A. Giannella, J. Bean, D. N. Taylor, S. Parker, A. Hoeper, S. Wowk, J. Hawkins, S. K. Kochi, G. Schiff, and K. P. Killeen Randomized, controlled human challenge study of the safety, immunogenicity, and protective efficacy of a single dose of Peru-15, a live attenuated oral cholera vaccine. Infect Immun 70: Coster, T. S., M. K. Wolf, E. R. Hall, F. J. Cassels, D. N. Taylor, C. T. Liu, F. C. Trespalacios, A. DeLorimier, D. R. Angleberger, and C. E. McQueen Immune response, ciprofloxacin activity, and gender differences after human experimental challenge by two strains of enterotoxigenic Escherichia coli. Infect Immun 75: DuPont, H. L Pathogenesis of traveler's diarrhea. Chemotherapy 41 Suppl 1: DuPont, H. L., S. B. Formal, R. B. Hornick, M. J. Snyder, J. P. Libonati, D. G. Sheahan, E. H. LaBrec, and J. P. Kalas Pathogenesis of Escherichia coli diarrhea. N Engl J Med 285: Evans, D. G., D. J. Evans, Jr., and W. Tjoa Hemagglutination of human group A erythrocytes by enterotoxigenic Escherichia coli isolated from adults with diarrhea: correlation with colonization factor. Infect Immun 18: Evans, D. G., D. Y. Graham, and D. J. Evans, Jr Administration of purified colonization factor antigens (CFA/I, CFA/II) of enterotoxigenic Escherichia coli to volunteers. Response to challenge with virulent enterotoxigenic Escherichia coli. Gastroenterology 87: Evans, D. G., T. K. Satterwhite, D. J. Evans, Jr., and H. L. DuPont Differences in serological responses and excretion patterns of volunteers challenged with enterotoxigenic Escherichia coli with and without the colonization factor antigen. Infect Immun 19: Evans, D. J., Jr., D. G. Evans, A. R. Opekun, and D. Y. Graham Immunoprotective oral whole cell vaccine for enterotoxigenic Escherichia coli diarrhea prepared by in situ destruction of chromosomal and plasmid DNA with colicin E2. FEMS Microbiol Immunol 1:9-18.
24 Graham, D. Y., M. K. Estes, and L. O. Gentry Double-blind comparison of bismuth subsalicylate and placebo in the prevention and treatment of enterotoxigenic Escherichia coli-induced diarrhea in volunteers. Gastroenterology 85: Kotloff, K. L., J. P. Nataro, G. A. Losonsky, S. S. Wasserman, T. L. Hale, D. N. Taylor, J. C. Sadoff, and M. M. Levine A modified Shigella volunteer challenge model in which the inoculum is administered with bicarbonate buffer: clinical experience and implications for Shigella infectivity. Vaccine 13: Levine, M. M., R. E. Black, C. C. Brinton, Jr., M. L. Clements, P. Fusco, T. P. Hughes, S. O'Donnell, R. Robins-Browne, S. Wood, and C. R. Young Reactogenicity, immunogenicity and efficacy studies of Escherichia coli type 1 somatic pili parenteral vaccine in man. Scand J Infect Dis Suppl 33: Levine, M. M., E. S. Caplan, D. Waterman, R. A. Cash, R. B. Hornick, and M. J. Snyder Diarrhea caused by Escherichia coli that produce only heat-stable enterotoxin. Infect Immun 17: Levine, M. M., D. R. Nalin, D. L. Hoover, E. J. Bergquist, R. B. Hornick, and C. R. Young Immunity to enterotoxigenic Escherichia coli. Infect Immun 23: Levine, M. M., M. B. Rennels, L. Cisneros, T. P. Hughes, D. R. Nalin, and C. R. Young Lack of person-to-person transmission of enterotoxigenic Escherichia coli despite close contact. Am J Epidemiol 111: McKenzie, R., A. L. Bourgeois, S. A. Frech, D. C. Flyer, A. Bloom, K. Kazempour, and G. M. Glenn Transcutaneous immunization with the heat-labile toxin (LT) of enterotoxigenic Escherichia coli (ETEC): protective efficacy in a double-blind, placebocontrolled challenge study. Vaccine 25: McKenzie, R., M. Darsley, N. Thomas, R. Randall, C. Carpenter, E. Forbes, M. Finucane, R. B. Sack, E. Hall, and A. L. Bourgeois A double-blind, placebocontrolled trial to evaluate the efficacy of PTL-003, an attenuated enterotoxigenic E. coli (ETEC) vaccine strain, in protecting against challenge with virulent ETEC. Vaccine 26: McKenzie, R., M. M. Venkatesan, M. K. Wolf, D. Islam, S. Grahek, A. M. Jones, A. Bloom, D. N. Taylor, T. L. Hale, and A. L. Bourgeois Safety and immunogenicity of WRSd1, a live attenuated Shigella dysenteriae type 1 vaccine candidate. Vaccine 26: Merson, M. H., G. K. Morris, D. A. Sack, J. G. Wells, J. C. Feeley, R. B. Sack, W. B. Creech, A. Z. Kapikian, and E. J. Gangarosa Travelers' diarrhea in Mexico. A prospective study of physicians and family members attending a congress. N Engl J Med 294: Porter CK., M.S. Riddle, D.R. Tribble, A.L. Bourgeois, R. McKenzie, S.D. Isidean, P. Sebeny, and S.J. Savarino A systematic review of experimental infections with enterotoxigenic Escherichia coli (ETEC). Vaccine (in press).24. Qadri, F., A. M. Svennerholm, A. S. Faruque, and R. B. Sack Enterotoxigenic Escherichia coli in developing countries: epidemiology, microbiology, clinical features, treatment, and prevention. Clin Microbiol Rev 18: Sack, D. A., D. C. Kaminsky, R. B. Sack, J. N. Itotia, R. R. Arthur, A. Z. Kapikian, F. Orskov, and I. Orskov Prophylactic doxycycline for travelers' diarrhea. Results of a prospective double-blind study of Peace Corps volunteers in Kenya. N Engl J Med 298:
25 Sack, D. A., J. C. McLaughlin, R. B. Sack, F. Orskov, and I. Orskov Enterotoxigenic Escherichia coli isolated from patients at a hospital in Dacca. J Infect Dis 135: Sack, D. A., J. Shimko, O. Torres, A. L. Bourgeois, D. S. Francia, B. Gustafsson, A. Karnell, I. Nyquist, and A. M. Svennerholm Randomised, double-blind, safety and efficacy of a killed oral vaccine for enterotoxigenic E. Coli diarrhoea of travellers to Guatemala and Mexico. Vaccine 25: Sack, D. A., C. O. Tacket, M. B. Cohen, R. B. Sack, G. A. Losonsky, J. Shimko, J. P. Nataro, R. Edelman, M. M. Levine, R. A. Giannella, G. Schiff, and D. Lang Validation of a volunteer model of cholera with frozen bacteria as the challenge. Infect Immun 66: Sack, R. B., S. L. Gorbach, J. G. Banwell, B. Jacobs, B. D. Chatterjee, and R. C. Mitra Enterotoxigenic Escherichia coli isolated from patients with severe choleralike disease. J Infect Dis 123: Sack, R. B., N. Hirschhorn, I. Brownlee, R. A. Cash, W. E. Woodward, and D. A. Sack Enterotoxigenic Escherichia-coli-associated diarrheal disease in Apache children. N Engl J Med 292: Savarino, S. J., F. M. Brown, E. Hall, S. Bassily, F. Youssef, T. Wierzba, L. Peruski, N. A. El-Masry, M. Safwat, M. Rao, M. Jertborn, A. M. Svennerholm, Y. J. Lee, and J. D. Clemens Safety and immunogenicity of an oral, killed enterotoxigenic Escherichia coli-cholera toxin B subunit vaccine in Egyptian adults. J Infect Dis 177: Svennerholm, A. M., and J. Tobias Vaccines against enterotoxigenic Escherichia coli. Expert Rev Vaccines 7: Tacket, C. O., S. B. Binion, E. Bostwick, G. Losonsky, M. J. Roy, and R. Edelman Efficacy of bovine milk immunoglobulin concentrate in preventing illness after Shigella flexneri challenge. Am J Trop Med Hyg 47: Tribble, D. R., S. Baqar, M. P. Carmolli, C. Porter, K. K. Pierce, K. Sadigh, P. Guerry, C. J. Larsson, D. Rockabrand, C. H. Ventone, F. Poly, C. E. Lyon, S. Dakdouk, A. Fingar, T. Gilliland, P. Daunais, E. Jones, S. Rymarchyk, C. Huston, M. Darsley, and B. D. Kirkpatrick Campylobacter jejuni strain CG8421: a refined model for the study of Campylobacteriosis and evaluation of Campylobacter vaccines in human subjects. Clin Infect Dis 49: Walker, R. I., D. Steele, and T. Aguado Analysis of strategies to successfully vaccinate infants in developing countries against enterotoxigenic E. coli (ETEC) disease. Vaccine 25:
26 595 Figure Legend Figure 1. Serum antibody geometric mean titers (95% confidence intervals) to LPS (A), LTB (B) and CFA/I (C) following challenge with one or two doses of ETEC H Downloaded from on December 9, 2018 by guest
27 Table 1. Demographics of enrolled subjects (challenged) Cohort 1 Cohort 2 Cohort 3 Group A Group B Group C Group D Naive Rechallenged N Dose given 2 x x x x x x x 10 7 (cfu/dose) Buffer bicarbonate CeraVacx bicarbonate CeraVacx bicarbonate bicarbonate bicarbonate Mean Age (Range) 30.6 (19-45) 28 (19-43) 29.0 (24-41) 33.6 (21-43) 33.5 (19-43) 29.1 (21-41) Females Males Black White Other Mean BMI (Range) 30.0 ( ) 27.5 ( ) 25.6 ( ) 28.9 ( ) 27.4 ( ) 25.2 ( ) 30.3 (19-43) 26.1 ( )
28 Table 2a. Clinical Outcomes for Subjects in Cohort 1 1 Outcome Group A N=5 Group B N=4 Group C N=5 Group D N=5 Number with diarrhea 5 (100%) 4 (100%) 4 (80%) 4 (80%) Number with moderate or severe 4 (80%) 4 (100%) 4 (80%) 4 (80%) diarrhea Mean [median] incubation period in hours (range) 43 [44] (32-51) 42 [43] (35-48) 43 [40] (21-69) 57 [55] (45-71) Mean [median] diarrhea stool output in 24-hour period in grams (range) 966 [669] ( ) 765 [476] ( ) 1032 [1134] ( ) 666 [613] ( ) Mean [median] diarrhea total stool output in grams (range) 1106 [793] ( ) 1359 [1051] ( ) 1707 [1709] ( ) 1021 [932] ( ) Mean [median] duration of diarrhea in hours (range) 36 [37] (12-61) 57 [59] (4-107) 86 [88] (23-143) 52 [55] (28-71) Mean [median] of the maximum number of stools in 24 hours (range) 9 [6] (3-19) 6 [6] (3-9) 6 [6] (4-7) 5 [5] (3-7) Fever (number with fever) Number with vomiting (maximum number of vomiting episodes) 1 (4) 1 (4) 1 (5) 3 (5) 1 Group A=2x10 8 cfu w/bicarbonate; Group B=2x10 8 cfu w/ceravacx ; Group C=2x10 7 cfu w/bicarbonate; Group D=2x10 7 cfu w/ CeraVacx
29 Table 2b. Clinical outcomes for subjects in Cohorts 2 and 3 1 Outcome Cohort 2 N=15 Cohort 3 Naïve N=10 Combined Naïve N=35 Cohort 3 Rechallenged N=10 Number with diarrhea 11 (73%) 9 (90%) 28 (80%) 1 (10%) Number with moderate or severe diarrhea 10 (67%) 7 (70%) 25 (71%) 0 Mean [median] incubation period in hours (range) 52 [47] 56 [54] 53 [49] 71 (30-95) (37-88) (21-95) Mean [median] maximum diarrhea stool output in 1039 [550] 1217 [642] 1042 [636] hour period in grams (range) ( ) ( ) ( ) Mean [median] diarrhea total stool output in grams 1463 [665] 1865 [1021] 1564 [1054] 328 (range) ( ) ( ) ( ) Mean [median] duration of diarrhea in hours 55 [72] 62 [73] 62 [72] 0 (range) (14-95) (14-88) (14-143) Mean [median] of the maximum number of stools 8 [7] 5 [7] 7 [6] 1 in 24 hours (range) (2-18) (2-16) (1-18) Fever (number with fever) Number with vomiting (maximum number of 6 (3) 5 (8) 17 (4) 1 (3) vomiting episodes) 1 Inoculum dose and buffer=2x10 7 cfu w/bicarbonate
30 Table 3. Selected Solicited Adverse Events for Naïve and Rechallenged Subjects (10 7 dose) Adverse Event Combined naïve subjects N=35 Total Number Number with Moderate or Severe AE Total Number Rechallenged N=10 Number with Moderate or Severe AE Nausea Vomiting Myalgia Fever Abdominal Pain Abdominal Cramping Malaise Bloating Flatulence Headache Lightheadedness Chills Anorexia
31 Table 4. Geometric Mean Titer (GMT of the CFU per gram of feces) 1 of H10407 shed on Study Day 2 and maximum shedding for naïve and rechallenged subjects. All Naïve 10 8 dose (n=9) All Naïve 10 7 dose (n=35) Rechallenged 10 7 dose (n=10) GMT day x x x 10 4 GMT Max 1.8 x x x For subjects who did not shed H10407, a value of 1 was used in place of 0 to calculate the GMT. If a subject had a positive qualitative sample, but negative quantitative sample, a value of 500 (corresponding to half of the lowest detectable limit of the quantitative assay) was used for the GMT calculation.
32 Table 5. Serological take rates 1 against ETEC H10407 antigens. Antigens Naïve (n=35) Rechallenged (n=10) IgA IgG IgA IgG LPS 33 (94%) 25 (71%) 3 (30%) 0 CFA/I 15 (43%) 8 (23%) 3 (30%) 2 (20%) LTB 19 (54%) 14 (40%) 2 (20%) 0 1 A 2.5 fold or greater rise in titer from baseline was considered a response.
33
34
35
2008, Johns Hopkins University. All rights reserved.
 Clayton Harro, Barbara DeNearing, Alicia Marcum, Andrea Feller, Subhra Chakraborty, Barbora Hnizda, August Bourgeois, Richard Walker, Anna Lundgren, Ann-Mari Svennerholm, and David Sack. Affiliations:
Clayton Harro, Barbara DeNearing, Alicia Marcum, Andrea Feller, Subhra Chakraborty, Barbora Hnizda, August Bourgeois, Richard Walker, Anna Lundgren, Ann-Mari Svennerholm, and David Sack. Affiliations:
Development, use and refinement of enterotoxigenic Escherichia coli (ETEC) controlled human infections
 controlled human infections") Development, use and refinement of enterotoxigenic Escherichia coli (ETEC) controlled human infections Chad Porter, PhD, MPH Enteric Diseases Department Naval Medical Research Center Disclaimer & Copyright
Development, use and refinement of enterotoxigenic Escherichia coli (ETEC) controlled human infections Chad Porter, PhD, MPH Enteric Diseases Department Naval Medical Research Center Disclaimer & Copyright
Enterotoxigenic Escherichia coli (ETEC) bacteria are the most
 bacteria are the most") crossmark Characterization of Mucosal Immune Responses to Enterotoxigenic Escherichia coli Vaccine Antigens in a Human Challenge Model: Response Profiles after Primary Infection and Homologous Rechallenge
crossmark Characterization of Mucosal Immune Responses to Enterotoxigenic Escherichia coli Vaccine Antigens in a Human Challenge Model: Response Profiles after Primary Infection and Homologous Rechallenge
A systematic review of experimental infections with enterotoxigenic Escherichia coli (ETEC)
") University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Uniformed Services University of the Health Sciences U.S. Department of Defense 2011 A systematic review of experimental
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Uniformed Services University of the Health Sciences U.S. Department of Defense 2011 A systematic review of experimental
Safety and Immunogenicity of a Parenterally Administered Rotavirus VP8 Subunit Vaccine in Healthy Adults
 Safety and Immunogenicity of a Parenterally Administered Rotavirus VP8 Subunit Vaccine in Healthy Adults Stanley Cryz 1, Clayton Harro 2, Monica McNeal 3, Nicole Meyer 3, Barbara DeNearing 2, Alicia Cage
Safety and Immunogenicity of a Parenterally Administered Rotavirus VP8 Subunit Vaccine in Healthy Adults Stanley Cryz 1, Clayton Harro 2, Monica McNeal 3, Nicole Meyer 3, Barbara DeNearing 2, Alicia Cage
Shigella Pathogenesis and Vaccine Development
 Shigella Pathogenesis and Vaccine Development Ryan Ranallo, Ph.D. Department of Enteric Infections Division of Communicable Diseases and Immunology Walter Reed Army Institute of Research Causes of Travelers
Shigella Pathogenesis and Vaccine Development Ryan Ranallo, Ph.D. Department of Enteric Infections Division of Communicable Diseases and Immunology Walter Reed Army Institute of Research Causes of Travelers
From cholera to enterotoxigenic Escherichia coli (ETEC) vaccine development
 vaccine development") Review Article Indian J Med Res 133, February 2011, pp 188-194 From cholera to enterotoxigenic Escherichia coli (ETEC) vaccine development Ann-Mari Svennerholm WHO Collaborating Centre for Research on
Review Article Indian J Med Res 133, February 2011, pp 188-194 From cholera to enterotoxigenic Escherichia coli (ETEC) vaccine development Ann-Mari Svennerholm WHO Collaborating Centre for Research on
Controlled Human Infection Models and Enteric Vaccine Development
 Controlled Human Infection Models and Enteric Vaccine Development 2018 Global Vaccine and Immunization Research Forum March 20, 2018 Beth Kirkpatrick, MD Objectives: What are Controlled Human Infection/Challenge
Controlled Human Infection Models and Enteric Vaccine Development 2018 Global Vaccine and Immunization Research Forum March 20, 2018 Beth Kirkpatrick, MD Objectives: What are Controlled Human Infection/Challenge
X/01/$ DOI: /CDLI Copyright 2001, American Society for Microbiology. All Rights Reserved.
 CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Mar. 2001, p. 424 428 Vol. 8, No. 2 1071-412X/01/$04.00 0 DOI: 10.1128/CDLI.8.2.424 428.2001 Copyright 2001, American Society for Microbiology. All Rights
CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Mar. 2001, p. 424 428 Vol. 8, No. 2 1071-412X/01/$04.00 0 DOI: 10.1128/CDLI.8.2.424 428.2001 Copyright 2001, American Society for Microbiology. All Rights
Received 27 November 2001/Returned for modification 8 January 2002/Accepted 17 January 2002
 INFECTION AND IMMUNITY, Apr. 2002, p. 1965 1970 Vol. 70, No. 4 0019-9567/02/$04.00 0 DOI: 10.1128/IAI.70.4.1965 1970.2002 Copyright 2002, American Society for Microbiology. All Rights Reserved. Randomized,
INFECTION AND IMMUNITY, Apr. 2002, p. 1965 1970 Vol. 70, No. 4 0019-9567/02/$04.00 0 DOI: 10.1128/IAI.70.4.1965 1970.2002 Copyright 2002, American Society for Microbiology. All Rights Reserved. Randomized,
The discovery of cholera - like enterotoxins produced by Escherichia coli causing secretory diarrhoea in humans
 Review Article Indian J Med Res 133, February 2011, pp 171-178 The discovery of cholera - like enterotoxins produced by Escherichia coli causing secretory diarrhoea in humans R. Bradley Sack Johns Hopkins
Review Article Indian J Med Res 133, February 2011, pp 171-178 The discovery of cholera - like enterotoxins produced by Escherichia coli causing secretory diarrhoea in humans R. Bradley Sack Johns Hopkins
GI Bacterial Infections (part-1)
") GI Bacterial Infections (part-1) Mohammed Abdulla Mehdi FIBMS (internal medicine), FIBMS (Gastroenterology & Hepatology) Acute diarrhea and vomiting Acute diarrhea, sometimes with vomiting, is the predominant
GI Bacterial Infections (part-1) Mohammed Abdulla Mehdi FIBMS (internal medicine), FIBMS (Gastroenterology & Hepatology) Acute diarrhea and vomiting Acute diarrhea, sometimes with vomiting, is the predominant
Rifaximin, a Nonabsorbed Oral Antibiotic, Prevents Shigellosis after Experimental Challenge
 MAJOR ARTICLE Rifaximin, a Nonabsorbed Oral Antibiotic, Prevents Shigellosis after Experimental Challenge David N. Taylor, 1,2 Robin McKenzie, 1 Anna Durbin, 1 Colleen Carpenter, 1 Christophe B. Atzinger,
MAJOR ARTICLE Rifaximin, a Nonabsorbed Oral Antibiotic, Prevents Shigellosis after Experimental Challenge David N. Taylor, 1,2 Robin McKenzie, 1 Anna Durbin, 1 Colleen Carpenter, 1 Christophe B. Atzinger,
Enterotoxigenic Escherichia coli
 INFECTION AND IMMUNITY, Aug. 2000, p. 4492 4497 Vol. 68, No. 8 0019-9567/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Safety and Immunogenicity of Two Different Lots
INFECTION AND IMMUNITY, Aug. 2000, p. 4492 4497 Vol. 68, No. 8 0019-9567/00/$04.00 0 Copyright 2000, American Society for Microbiology. All Rights Reserved. Safety and Immunogenicity of Two Different Lots
Intestinal Immune Responses to an Inactivated Oral Enterotoxigenic Escherichia coli Vaccine and Associated Immunoglobulin A Responses in Blood
 INFECTION AND IMMUNITY, July 1998, p. 3311 3316 Vol. 66, No. 7 0019-9567/98/$04.00 0 Copyright 1998, American Society for Microbiology. All Rights Reserved. Intestinal Immune Responses to an Inactivated
INFECTION AND IMMUNITY, July 1998, p. 3311 3316 Vol. 66, No. 7 0019-9567/98/$04.00 0 Copyright 1998, American Society for Microbiology. All Rights Reserved. Intestinal Immune Responses to an Inactivated
Enterotoxigenic Escherichia coli in Developing Countries: Epidemiology, Microbiology, Clinical Features, Treatment, and Prevention
 CLINICAL MICROBIOLOGY REVIEWS, July 2005, p. 465 483 Vol. 18, No. 3 0893-8512/05/$08.00 0 doi:10.1128/cmr.18.3.465 483.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved. Enterotoxigenic
CLINICAL MICROBIOLOGY REVIEWS, July 2005, p. 465 483 Vol. 18, No. 3 0893-8512/05/$08.00 0 doi:10.1128/cmr.18.3.465 483.2005 Copyright 2005, American Society for Microbiology. All Rights Reserved. Enterotoxigenic
Identification of protective immune responses and development of vaccines against ETEC and H. pylori
 Identification of protective immune responses and development of vaccines against ETEC and H. pylori Research group: Ann-Mari Svennerholm, Professor, MD, PhD; Anna Lundgren, PhD; JoshuaTobias, PhD; Marianne
Identification of protective immune responses and development of vaccines against ETEC and H. pylori Research group: Ann-Mari Svennerholm, Professor, MD, PhD; Anna Lundgren, PhD; JoshuaTobias, PhD; Marianne
Lactobacillus Prophylaxis for Diarrhea Due to Enterotoxigenic Escherichia coli
 ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, JUly 1981, p. 104-108 0066-4804/81/070104-05$02.00 Vol. 20, No. 1 Lactobacillus Prophylaxis for Diarrhea Due to Enterotoxigenic Escherichia coli MARY L. CLEMENTS,*
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, JUly 1981, p. 104-108 0066-4804/81/070104-05$02.00 Vol. 20, No. 1 Lactobacillus Prophylaxis for Diarrhea Due to Enterotoxigenic Escherichia coli MARY L. CLEMENTS,*
Serotypes of Enterotoxigenic Escherichia coli in Thailand and
 INFECTION AND IMMUNITY, June 98, p. 8-86 9-967/8/68-6$./ Vol. 36, No. 3 Serotypes of Enterotoxigenic Escherichia coli in Thailand and the Philippines PETER ECHEVERRIA,l* FRITS RSKOV, IDA RSKOV, AND DUANGRATANA
INFECTION AND IMMUNITY, June 98, p. 8-86 9-967/8/68-6$./ Vol. 36, No. 3 Serotypes of Enterotoxigenic Escherichia coli in Thailand and the Philippines PETER ECHEVERRIA,l* FRITS RSKOV, IDA RSKOV, AND DUANGRATANA
Salmonella, Shigella, and Campylobacter
 1 Salmonella, Shigella, and Campylobacter Dr. Hala Al Daghistani Salmonella and enteritis Salmonellae are often pathogenic for humans or animals when acquired by the oral route. They are transmitted from
1 Salmonella, Shigella, and Campylobacter Dr. Hala Al Daghistani Salmonella and enteritis Salmonellae are often pathogenic for humans or animals when acquired by the oral route. They are transmitted from
First steps for managing an outbreak of acute diarrhoea
 GLOBAL HEALTH SECURITY WORLD HEALTH ORGANIZATION E P I D E M I C A L E R T A N D R E S P O N S E First steps for managing an outbreak of acute diarrhoea THIS LEAFLET AIMS AT GUIDING YOU THROUGH THE VERY
GLOBAL HEALTH SECURITY WORLD HEALTH ORGANIZATION E P I D E M I C A L E R T A N D R E S P O N S E First steps for managing an outbreak of acute diarrhoea THIS LEAFLET AIMS AT GUIDING YOU THROUGH THE VERY
Immunity to Enterotoxigenic Escherichia coli
 INFECTION AND IMMUNITY, Mar. 1979, p. 729-736 0019-9567/79/03-0729/08$02.00/0 Vol. 23, No. 3 Immunity to Enterotoxigenic Escherichia coli MYRON M. LEVINE,* DAVID R. NALIN, DAVID L. HOOVER, ERICK J. BERGQUIST,
INFECTION AND IMMUNITY, Mar. 1979, p. 729-736 0019-9567/79/03-0729/08$02.00/0 Vol. 23, No. 3 Immunity to Enterotoxigenic Escherichia coli MYRON M. LEVINE,* DAVID R. NALIN, DAVID L. HOOVER, ERICK J. BERGQUIST,
Uniform Protection Against Heterologous Serotypes of Enterotoxigenic Escherichia coli
 INFECTION AND IMMUNITY, June 1981, p. 1100-1104 0019-956781061100-05$02.000 Vol. 32, No. 3 Immunization of Rats with Heat-Labile Enterotoxin Provides Uniform Protection Against Heterologous Serotypes of
INFECTION AND IMMUNITY, June 1981, p. 1100-1104 0019-956781061100-05$02.000 Vol. 32, No. 3 Immunization of Rats with Heat-Labile Enterotoxin Provides Uniform Protection Against Heterologous Serotypes of
/01/$ DOI: /IAI Copyright 2001, American Society for Microbiology. All Rights Reserved.
 INFECTION AND IMMUNITY, May 2001, p. 2853 2857 Vol. 69, No. 5 0019-9567/01/$04.00 0 DOI: 10.1128/IAI.69.5.2853 2857.2001 Copyright 2001, American Society for Microbiology. All Rights Reserved. Induction
INFECTION AND IMMUNITY, May 2001, p. 2853 2857 Vol. 69, No. 5 0019-9567/01/$04.00 0 DOI: 10.1128/IAI.69.5.2853 2857.2001 Copyright 2001, American Society for Microbiology. All Rights Reserved. Induction
Oral rehydration therapy: efficacy of sodium citrate
 Gut, 1984, 25, 900-904 Clinical trial Oral rehydration therapy: efficacy of sodium citrate equals to sodium bicarbonate for correction of acidosis in diarrhoea M R ISLAM, A R SAMADI, S M AHMED, P K BARDHAN,
Gut, 1984, 25, 900-904 Clinical trial Oral rehydration therapy: efficacy of sodium citrate equals to sodium bicarbonate for correction of acidosis in diarrhoea M R ISLAM, A R SAMADI, S M AHMED, P K BARDHAN,
True Pathogens of the Enterobacteriaceae: Salmonella, Shigella & Yersinia Salmonella
 Lec. 6 Oral Microbiology Dr. Chatin True Pathogens of the Enterobacteriaceae: Salmonella, Shigella & Yersinia Salmonella General Characteristics of Salmonella جامعة تكريت كلية طب االسنان Coliform bacilli
Lec. 6 Oral Microbiology Dr. Chatin True Pathogens of the Enterobacteriaceae: Salmonella, Shigella & Yersinia Salmonella General Characteristics of Salmonella جامعة تكريت كلية طب االسنان Coliform bacilli
Epidemiology of Diarrheal Diseases. Robert Black, MD, MPH Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Correlates of Protection against Enterotoxigenic Escherichia coli
 Correlates of Protection against Enterotoxigenic Escherichia coli Firdausi Qadri Infectious Disease Division Correlates of enteric vaccine induced protection Fondation Merieux, Annecy 22 March, 216 Importance
Correlates of Protection against Enterotoxigenic Escherichia coli Firdausi Qadri Infectious Disease Division Correlates of enteric vaccine induced protection Fondation Merieux, Annecy 22 March, 216 Importance
SEROLOGICAL TYPES OF ESCHERICHIA COLI IN ASSOCIATION WITH
 SEROLOGICAL TYPES OF ESCHERICHIA COLI IN ASSOCIATION WITH INFANTILE GASTROENTERITIS G. S. TAWIL AND S. EL KHOLY Department of Bacteriology, Faculty of Medicine, University of Ein Chams, Cairo, U. A. R.
SEROLOGICAL TYPES OF ESCHERICHIA COLI IN ASSOCIATION WITH INFANTILE GASTROENTERITIS G. S. TAWIL AND S. EL KHOLY Department of Bacteriology, Faculty of Medicine, University of Ein Chams, Cairo, U. A. R.
Acute diarrhoea. What are the mechanisms of acute diarrhoea? What are the causes of acute diarrhoea?
 In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Acute diarrhoea www.corecharity.org.uk What are the mechanisms of acute diarrhoea? What are the causes of acute diarrhoea?
In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Acute diarrhoea www.corecharity.org.uk What are the mechanisms of acute diarrhoea? What are the causes of acute diarrhoea?
SUMMARY OF FOODBORNE AND WATERBORNE DISEASE CHARACTERISTICS
 SUMMARY OF FOODBNE AND WATERBNE DISEASE CHARACTERISTICS BACTERIAL Bacillus cereus Vomiting toxin Diarrheal toxin Brucella species Campylobacter species Clostridium botulinum Clostridium perfringens 1-6
SUMMARY OF FOODBNE AND WATERBNE DISEASE CHARACTERISTICS BACTERIAL Bacillus cereus Vomiting toxin Diarrheal toxin Brucella species Campylobacter species Clostridium botulinum Clostridium perfringens 1-6
Rifaximin for Travellers Diarrhoea
 New Medicines Profile April 2013 Issue No. 13.01 for Travellers Diarrhoea Concise evaluated information to support the managed entry of new medicines in the NHS Summary is a broad spectrum antibiotic licensed
New Medicines Profile April 2013 Issue No. 13.01 for Travellers Diarrhoea Concise evaluated information to support the managed entry of new medicines in the NHS Summary is a broad spectrum antibiotic licensed
Gastroenteritis and viral infections
 Gastroenteritis and viral infections A Large number of viruses are found in the human gut; these include some that are associated with gastroenteritis Rotaviruses Adenoviruses 40/41 Caliciviruses Norwalk-like
Gastroenteritis and viral infections A Large number of viruses are found in the human gut; these include some that are associated with gastroenteritis Rotaviruses Adenoviruses 40/41 Caliciviruses Norwalk-like
ا.م.د.هيفاء الحديثي. Enterobacteriaceae
 ا.م.د.هيفاء الحديثي Bacteriology Genus Salmonella Enterobacteriaceae - Pathogenic for human and animals - They are gram negative rods, motile with peritrichous flagella except Gallinarum-pullorum - Ferment
ا.م.د.هيفاء الحديثي Bacteriology Genus Salmonella Enterobacteriaceae - Pathogenic for human and animals - They are gram negative rods, motile with peritrichous flagella except Gallinarum-pullorum - Ferment
Enteric Illness. Shigellosis
 Section 3 Page 1 of 7 Notification Timeline: From Lab/Practitioner to Public Health: Immediately. From Public Health to Saskatchewan Health: Within 72 hours. Public Health Follow-up Timeline: Initiate
Section 3 Page 1 of 7 Notification Timeline: From Lab/Practitioner to Public Health: Immediately. From Public Health to Saskatchewan Health: Within 72 hours. Public Health Follow-up Timeline: Initiate
Enterotoxigenic Escherichia coli Isolated from Adults with
 INFECrION AND IMMUNITY, Nov. 1977, p. 330-337 Copyright 1977 American Society for Microbiology Vol. 18, No. 2 Printed in U.S.A. Hemagglutination of Human Group A Erythrocytes by Enterotoxigenic Escherichia
INFECrION AND IMMUNITY, Nov. 1977, p. 330-337 Copyright 1977 American Society for Microbiology Vol. 18, No. 2 Printed in U.S.A. Hemagglutination of Human Group A Erythrocytes by Enterotoxigenic Escherichia
Received 10 July 2003/Returned for modification 3 September 2003/Accepted 10 November 2003
 INFECTION AND IMMUNITY, Feb. 2004, p. 923 930 Vol. 72, No. 2 0019-9567/04/$08.00 0 DOI: 10.1128/IAI.72.2.923 930.2004 Copyright 2004, American Society for Microbiology. All Rights Reserved. Two Studies
INFECTION AND IMMUNITY, Feb. 2004, p. 923 930 Vol. 72, No. 2 0019-9567/04/$08.00 0 DOI: 10.1128/IAI.72.2.923 930.2004 Copyright 2004, American Society for Microbiology. All Rights Reserved. Two Studies
Advisory on Gastroenteritis
 10 December 2018 Advisory on Gastroenteritis Background Singapore has seen a spate of four food poisoning outbreaks since November 2018, affecting more than 400 people. The most serious involved a fatality,
10 December 2018 Advisory on Gastroenteritis Background Singapore has seen a spate of four food poisoning outbreaks since November 2018, affecting more than 400 people. The most serious involved a fatality,
Shigella and salmonella
 Sulaimani University College of Pharmacy Microbiology Lec. 9 & 10 Shigella and salmonella Dr. Abdullah Ahmed Hama PhD. Microbiology/Molecular Parasitology abdullah.hama@spu.edu.iq 1 Shigella Shigella species
Sulaimani University College of Pharmacy Microbiology Lec. 9 & 10 Shigella and salmonella Dr. Abdullah Ahmed Hama PhD. Microbiology/Molecular Parasitology abdullah.hama@spu.edu.iq 1 Shigella Shigella species
Received 26 September 2013; Final revision 1 August 2014; Accepted 13 August 2014; first published online 19 September 2014
 Epidemiol. Infect. (2015), 143, 1662 1671. Cambridge University Press 2014 doi:10.1017/s0950268814002295 Toxins and virulence factors of enterotoxigenic Escherichia coli associated with strains isolated
Epidemiol. Infect. (2015), 143, 1662 1671. Cambridge University Press 2014 doi:10.1017/s0950268814002295 Toxins and virulence factors of enterotoxigenic Escherichia coli associated with strains isolated
33. I will recommend this primer to my colleagues. A. Strongly Agree D. Disagree B. Agree E. Strongly Disagree C. Neither agree nor disagree
 27. The primer increased my ability to recognize foodborne illnesses and increased the likelihood that I will consider such illnesses in my patients. 28. The primer increased my knowledge and skills in
27. The primer increased my ability to recognize foodborne illnesses and increased the likelihood that I will consider such illnesses in my patients. 28. The primer increased my knowledge and skills in
Typhoid Fever II. Received for publication 6 May % saline was administered to human volunteers
 INFECTION AND IMMUNITY, Dec. 1975, p. 1290-1294 Copyright( 1975 American Society for Microbiology Vol. 12,, No. 6 Printed in U.S.A. Vi Antigen From Salmonella typhosa And Immunity Against Typhoid Fever
INFECTION AND IMMUNITY, Dec. 1975, p. 1290-1294 Copyright( 1975 American Society for Microbiology Vol. 12,, No. 6 Printed in U.S.A. Vi Antigen From Salmonella typhosa And Immunity Against Typhoid Fever
DUKORAL. Oral inactivated cholera and ETEC vaccine. Consumer Medicine Information. It does not take the place of talking to your doctor or pharmacist.
 What is in this leaflet DUKORAL Oral inactivated cholera and ETEC vaccine Consumer Medicine Information This leaflet answers some common questions about Dukoral. It does not contain all the available information.
What is in this leaflet DUKORAL Oral inactivated cholera and ETEC vaccine Consumer Medicine Information This leaflet answers some common questions about Dukoral. It does not contain all the available information.
Study summaries L. casei 431
 This binder provides you with summaries of selected publications on Lactobacillus paracasei subsp. paracasei L. casei 431. The publications are clinical studies performed in humans documenting the effects
This binder provides you with summaries of selected publications on Lactobacillus paracasei subsp. paracasei L. casei 431. The publications are clinical studies performed in humans documenting the effects
Attachment of Enterotoxigenic Escherichia coli to Human
 INFECTION AND IMMUNITY, Mar. 1983, p. 1102-1106 0019-9567/83/031102-05$02.00/0 Copyright C 1983, American Society for Microbiology Vol. 39, No. 3 Attachment of Enterotoxigenic Escherichia coli to Human
INFECTION AND IMMUNITY, Mar. 1983, p. 1102-1106 0019-9567/83/031102-05$02.00/0 Copyright C 1983, American Society for Microbiology Vol. 39, No. 3 Attachment of Enterotoxigenic Escherichia coli to Human
GENETICALLY ENGINEERED ENTEROPATHOGENIC ESCHERICHIA COLI STRAIN PROTECTS RABBITS AGAINST COLIBACILLOSIS.
 Proceedings - th World Rabbit Congress September -1, Puebla, Mexico GENETICALLY ENGINEERED ENTEROPATHOGENIC ESCHERICHIA COLI STRAIN PROTECTS RABBITS AGAINST COLIBACILLOSIS. BOULLIER S., NOUGAYRÈDE J-P.,
Proceedings - th World Rabbit Congress September -1, Puebla, Mexico GENETICALLY ENGINEERED ENTEROPATHOGENIC ESCHERICHIA COLI STRAIN PROTECTS RABBITS AGAINST COLIBACILLOSIS. BOULLIER S., NOUGAYRÈDE J-P.,
Diarrheal Diseases in Asia: overview and update. G. Balakrish Nair, PhD Ag. Regional Advisor Research Policy and Cooperation WHO, SEARO
 Diarrheal Diseases in Asia: overview and update G. Balakrish Nair, PhD Ag. Regional Advisor Research Policy and Cooperation WHO, SEARO Overview of the talk Global and Regional burden of diarrheal disease
Diarrheal Diseases in Asia: overview and update G. Balakrish Nair, PhD Ag. Regional Advisor Research Policy and Cooperation WHO, SEARO Overview of the talk Global and Regional burden of diarrheal disease
Effect of Vaccine, Route, and Schedule on Antibody
 APPUED MICROBIOLOGY, Mar. 1969, p. 355-359 Copyright 1969 American Society for Microbiology Vol. 17, No. 3 Printed in U.S.A. Effect of Vaccine, Route, and Schedule on Antibody Response of Rabbits to Pasteurella
APPUED MICROBIOLOGY, Mar. 1969, p. 355-359 Copyright 1969 American Society for Microbiology Vol. 17, No. 3 Printed in U.S.A. Effect of Vaccine, Route, and Schedule on Antibody Response of Rabbits to Pasteurella
Evaluation of Peru-15, a New Live Oral Vaccine for Cholera, in Volunteers
 201 Evaluation of Peru-15, a New Live Oral Vaccine for Cholera, in Volunteers David A. Sack, R. Bradley Sack, Janet Shimko, George Gomes, Donna O Sullivan, Karen Metcalfe, and Dale Spriggs Vaccine Testing
201 Evaluation of Peru-15, a New Live Oral Vaccine for Cholera, in Volunteers David A. Sack, R. Bradley Sack, Janet Shimko, George Gomes, Donna O Sullivan, Karen Metcalfe, and Dale Spriggs Vaccine Testing
Gastroenteritis Outbreaks Including Norovirus. Module 7
 Gastroenteritis Outbreaks Including Norovirus Module 7 Learner Outcomes By the end of this module you will be able to: Outline the case definition for a gastroenteritis outbreak. Explain the difference
Gastroenteritis Outbreaks Including Norovirus Module 7 Learner Outcomes By the end of this module you will be able to: Outline the case definition for a gastroenteritis outbreak. Explain the difference
Enterotoxigenic Escherichia coli: Pathogenesis, Natural Infection and the Current State of Vaccine Development
 Enterotoxigenic Escherichia coli: Pathogenesis, Natural Infection and the Current State of Vaccine Development Stephen J. Savarino, MD, MPH U.S. Naval Medical Research Center Silver Spring, MD USA Dealing
Enterotoxigenic Escherichia coli: Pathogenesis, Natural Infection and the Current State of Vaccine Development Stephen J. Savarino, MD, MPH U.S. Naval Medical Research Center Silver Spring, MD USA Dealing
Biological Hazards Module 3
 1 - Objectives - Describe salmonellosis and typhoid fever (salmonella) Recognize symptoms of exposure Describe treatments available Develop a response plan 2 - Salmonellosis Definition - Severe lower GI
1 - Objectives - Describe salmonellosis and typhoid fever (salmonella) Recognize symptoms of exposure Describe treatments available Develop a response plan 2 - Salmonellosis Definition - Severe lower GI
Chapter 1 The Public Health Role of Clinical Laboratories
 Chapter 1 The Public Health Role of Clinical Laboratories A. Epidemic Diarrhea The two most common types of epidemic diarrhea in developing countries are watery diarrhea caused by Vibrio cholerae serogroup
Chapter 1 The Public Health Role of Clinical Laboratories A. Epidemic Diarrhea The two most common types of epidemic diarrhea in developing countries are watery diarrhea caused by Vibrio cholerae serogroup
See external label 96 tests HSV 2 IgA. Cat #
 DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
THE OCCURRENCE OF DIARRHOEAGENIC ESCHERICHIA COLI AMONG CHILDREN UNDER FIVE YEARS OF AGE IN BASRAH, SOUTHERN IRAQ. Hassan J Hasony, MPhil, PhD*
 Bahrain Medical Bulletin, Volume 18, Number 2, June 1996 THE OCCURRENCE OF DIARRHOEAGENIC ESCHERICHIA COLI AMONG CHILDREN UNDER FIVE YEARS OF AGE IN BASRAH, SOUTHERN IRAQ Hassan J Hasony, MPhil, PhD* Objective:
Bahrain Medical Bulletin, Volume 18, Number 2, June 1996 THE OCCURRENCE OF DIARRHOEAGENIC ESCHERICHIA COLI AMONG CHILDREN UNDER FIVE YEARS OF AGE IN BASRAH, SOUTHERN IRAQ Hassan J Hasony, MPhil, PhD* Objective:
more intense treatments are needed to get rid of the infection.
 What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms. The main risk of getting
What Is Clostridium Difficile (C. Diff)? Clostridium difficile, or C. diff for short, is an infection from a bacterium that can grow in your intestines and cause bad GI symptoms. The main risk of getting
CONTROL OF VIRAL GASTROENTERITIS OUTBREAKS IN CALIFORNIA LONG-TERM CARE FACILITIES
 CONTROL OF VIRAL GASTROENTERITIS OUTBREAKS IN CALIFORNIA LONG-TERM CARE FACILITIES California Department of Health Services Division of Communicable Disease Control In Conjunction with Licensing and Certification
CONTROL OF VIRAL GASTROENTERITIS OUTBREAKS IN CALIFORNIA LONG-TERM CARE FACILITIES California Department of Health Services Division of Communicable Disease Control In Conjunction with Licensing and Certification
Gram-Negative rods Introduction to
 Lec 5 Oral Microbiology Dr. Chatin Gram-Negative rods Introduction to Enterobacteriaceae Characteristics: جامعة تكريت كلية طب االسنان Small gram-negative rods (2-5 by 0.5 microns) Most motile with peritrichous
Lec 5 Oral Microbiology Dr. Chatin Gram-Negative rods Introduction to Enterobacteriaceae Characteristics: جامعة تكريت كلية طب االسنان Small gram-negative rods (2-5 by 0.5 microns) Most motile with peritrichous
Peru-15, a live attenuated oral cholera vaccine, is safe and immunogenic in Bangladeshi toddlers and infants
 Vaccine 25 (2007) 231 238 Peru-15, a live attenuated oral cholera vaccine, is safe and immunogenic in Bangladeshi toddlers and infants Firdausi Qadri a,, Mohiul I. Chowdhury a, Shah M. Faruque a, Mohammed
Vaccine 25 (2007) 231 238 Peru-15, a live attenuated oral cholera vaccine, is safe and immunogenic in Bangladeshi toddlers and infants Firdausi Qadri a,, Mohiul I. Chowdhury a, Shah M. Faruque a, Mohammed
Training in Infectious Diseases Modeling. A reflection on vaccination as a disease control measure
 Training in Infectious Diseases Modeling A reflection on vaccination as a disease control measure -Example of Rotavirus disease- Participant s Guide Adapted by Nathalie Elomeiri; Camelia Savulescu; Fernando
Training in Infectious Diseases Modeling A reflection on vaccination as a disease control measure -Example of Rotavirus disease- Participant s Guide Adapted by Nathalie Elomeiri; Camelia Savulescu; Fernando
Herpes Simplex Virus 2 IgM HSV 2 IgM
 DIAGNOSTIC AUTOMATION, INC. 21250 Califa Street, Suite 102 and 116, Woodland Hills, CA 91367 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com
DIAGNOSTIC AUTOMATION, INC. 21250 Califa Street, Suite 102 and 116, Woodland Hills, CA 91367 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com
Analysis of strategies to successfully vaccinate infants in developing countries against enterotoxigenic E. coli (ETEC) disease
 disease") Vaccine 25 (2007) 2545 2566 Review Analysis of strategies to successfully vaccinate infants in developing countries against enterotoxigenic E. coli (ETEC) disease Richard I. Walker a,, Duncan Steele b,
Vaccine 25 (2007) 2545 2566 Review Analysis of strategies to successfully vaccinate infants in developing countries against enterotoxigenic E. coli (ETEC) disease Richard I. Walker a,, Duncan Steele b,
See external label 2 C-8 C 96 tests Chemiluminescence. CMV IgM. Cat # Diluted samples, controls & calibrator 100 µl 30 minutes
 DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
Vibrio parahaemolyticus
 Vibrio parahaemolyticus Frequently Asked Questions What is Vibrio parahaemolyticus? What type of illness is caused by V. parahaemolyticus? How does infection with V. parahaemolyticus occur? How common
Vibrio parahaemolyticus Frequently Asked Questions What is Vibrio parahaemolyticus? What type of illness is caused by V. parahaemolyticus? How does infection with V. parahaemolyticus occur? How common
GRAM-NEGATIVE BACILLI THE ENTERICS: Family Enterobacteriaceae: Genus Escherichia & Genus Klebsiella
 DR. HUDA ABO- ALEES 214-2-15 Obgectives: GRAM-NEGATIVE BACILLI THE ENTERICS: Family Enterobacteriaceae: Genus Escherichia & Genus Klebsiella Describe the morphology & physiology for E.coli & Klebsiella
DR. HUDA ABO- ALEES 214-2-15 Obgectives: GRAM-NEGATIVE BACILLI THE ENTERICS: Family Enterobacteriaceae: Genus Escherichia & Genus Klebsiella Describe the morphology & physiology for E.coli & Klebsiella
Intestinal Immune Responses in Patients Infected with Enterotoxigenic Escherichia coli and in Vaccinees
 INFECTION AND IMMUNITY, Dec. 1999, p. 6234 6241 Vol. 67, No. 12 0019-9567/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Intestinal Immune Responses in Patients Infected
INFECTION AND IMMUNITY, Dec. 1999, p. 6234 6241 Vol. 67, No. 12 0019-9567/99/$04.00 0 Copyright 1999, American Society for Microbiology. All Rights Reserved. Intestinal Immune Responses in Patients Infected
Biological Consulting Services
 Biological Consulting Services of North Florida/ Inc. May 13, 2009 Aphex BioCleanse Systems, Inc. Dear Sirs, We have completed antimicrobial efficacy study on the supplied Multi-Purpose Solution. The testing
Biological Consulting Services of North Florida/ Inc. May 13, 2009 Aphex BioCleanse Systems, Inc. Dear Sirs, We have completed antimicrobial efficacy study on the supplied Multi-Purpose Solution. The testing
Enteric bacteria(pseudomonas+salmonella) Dr.Asem shihabi. Jumanah Nayef Abu Asbeh
 Dr.Asem shihabi. Jumanah Nayef Abu Asbeh") 15 Microbiology sheet #15 1. Gram-negative facultative anaerobic rapidly growing bacteria are divided into 2 major Lactose fermenter group which is represented by the Coliforms. 2. Lactose non-fermenter
15 Microbiology sheet #15 1. Gram-negative facultative anaerobic rapidly growing bacteria are divided into 2 major Lactose fermenter group which is represented by the Coliforms. 2. Lactose non-fermenter
Giardiasis. Table of Contents
 Table of Contents Case Definition... Error! Bookmark not defined. Reporting Requirements... 2 Etiology... Error! Bookmark not defined. Clinical Presentation... Error! Bookmark not defined. Diagnosis...
Table of Contents Case Definition... Error! Bookmark not defined. Reporting Requirements... 2 Etiology... Error! Bookmark not defined. Clinical Presentation... Error! Bookmark not defined. Diagnosis...
DR. HUDA ABO- ALEES GRAM-NEGATIVE BACILLI THE ENTERICS:
 DR. HUDA ABO- ALEES 214-2-15 GRAM-NEGATIVE BACILLI THE ENTERICS: Family Enterobacteriaceae: Genus Escherichia & Genus Klebsiella OBJECTIVES Describe the morphology & physiology for E.coli & Klebsiella
DR. HUDA ABO- ALEES 214-2-15 GRAM-NEGATIVE BACILLI THE ENTERICS: Family Enterobacteriaceae: Genus Escherichia & Genus Klebsiella OBJECTIVES Describe the morphology & physiology for E.coli & Klebsiella
Campylobacter ENTERITIS SURVEILLANCE PROTOCOL
 Campylobacter ENTERITIS SURVEILLANCE PROTOCOL Public Health Action 1. Educate providers and laboratories to report stool cultures positive for Campylobacter jejuni or Campylobacter coli from patients within
Campylobacter ENTERITIS SURVEILLANCE PROTOCOL Public Health Action 1. Educate providers and laboratories to report stool cultures positive for Campylobacter jejuni or Campylobacter coli from patients within
GI Bacterial Infections (part-2)
") GI Bacterial Infections (part-2) Mohammed Abdulla Mehdi FIBMS (internal medicine), FIBMS (G&H) Clostridium difficile infection C. difficile is the most commonly diagnosed cause of antibioticassociated
GI Bacterial Infections (part-2) Mohammed Abdulla Mehdi FIBMS (internal medicine), FIBMS (G&H) Clostridium difficile infection C. difficile is the most commonly diagnosed cause of antibioticassociated
Comparative Evaluation of Efficacy of Antibiotic in Treating Bacterial Enteritis in Children: A Hospital Based Study
 Original article: Comparative Evaluation of Efficacy of Antibiotic in Treating Bacterial Enteritis in Children: A Hospital Based Study Radheshyam Shrotriya, Anju Kochar Principal Specialist (Pediatrics),
Original article: Comparative Evaluation of Efficacy of Antibiotic in Treating Bacterial Enteritis in Children: A Hospital Based Study Radheshyam Shrotriya, Anju Kochar Principal Specialist (Pediatrics),
Measles IgM ELISA Kit
 Measles IgM ELISA Kit Catalog Number KA2257 96 assays Version: 03 Intended for research use only www.abnova.com Table of Contents Introduction... 3 Intended Use... 3 Background... 3 Principle of the Assay...
Measles IgM ELISA Kit Catalog Number KA2257 96 assays Version: 03 Intended for research use only www.abnova.com Table of Contents Introduction... 3 Intended Use... 3 Background... 3 Principle of the Assay...
(From the Biological Department, Chemical Corps, Camp Derrick, Frederick, Maryland)
") OBSERVATIONS ON THE AGGLUTINATION OF POLYSACCHARIDE- TREATED ERYTHROCYTES BY TULAREMIA ANTISERA B~ MARY M. ALEXANDER,* PH.D., GEORGE G. WRIGHT, PH.D., AND AGNES C. BALDWIN" (From the Biological Department,
OBSERVATIONS ON THE AGGLUTINATION OF POLYSACCHARIDE- TREATED ERYTHROCYTES BY TULAREMIA ANTISERA B~ MARY M. ALEXANDER,* PH.D., GEORGE G. WRIGHT, PH.D., AND AGNES C. BALDWIN" (From the Biological Department,
Dear Healthcare Provider, The information contained here may be very important to your practice. Please take a moment to review this document.
 February 2018 Dear Healthcare Provider, The information contained here may be very important to your practice. Please take a moment to review this document. TEST BULLETIN CHLAMYDIA/GONORRHEA SPECIMEN COLLECTION
February 2018 Dear Healthcare Provider, The information contained here may be very important to your practice. Please take a moment to review this document. TEST BULLETIN CHLAMYDIA/GONORRHEA SPECIMEN COLLECTION
Epidemic and Endemic Cholera Trends over a 33-Year Period in Bangladesh
 246 Epidemic and Endemic Cholera Trends over a 33-Year Period in Bangladesh Ira M. Longini, Jr., 1 Mohammed Yunus, 3 K. Zaman, 3 A. K. Siddique, 3 R. Bradley Sack, 2 and Azhar Nizam 1 1 Department of Biostatistics,
246 Epidemic and Endemic Cholera Trends over a 33-Year Period in Bangladesh Ira M. Longini, Jr., 1 Mohammed Yunus, 3 K. Zaman, 3 A. K. Siddique, 3 R. Bradley Sack, 2 and Azhar Nizam 1 1 Department of Biostatistics,
Cholera Clinical Guidelines. OAHPP Rounds January 11, 2011 Vanessa G. Allen MD FRCPC Medical Microbiologist
 Cholera Clinical Guidelines OAHPP Rounds January 11, 2011 Vanessa G. Allen MD FRCPC Medical Microbiologist Overview Cholera clinical guidelines Development and review process Content Reference for diagnosis,
Cholera Clinical Guidelines OAHPP Rounds January 11, 2011 Vanessa G. Allen MD FRCPC Medical Microbiologist Overview Cholera clinical guidelines Development and review process Content Reference for diagnosis,
REFERENCE NUMBER: NH.PMN.47 EFFECTIVE DATE: 11/11
 PAGE: 1 of 5 RETIRED: REVIEWED: 11/11, 12/14, 08/16, 07/17 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough
PAGE: 1 of 5 RETIRED: REVIEWED: 11/11, 12/14, 08/16, 07/17 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough
Astrovirus associated gastroenteritis in a children's ward
 J. clin. Path., 1977, 30, 948-952 Astrovirus associated gastroenteritis in a children's ward J. B. KURTZ, T. W. LEE, AND D. PICKERING From the Virology and Public Health Laboratory, Churchill Hospital,
J. clin. Path., 1977, 30, 948-952 Astrovirus associated gastroenteritis in a children's ward J. B. KURTZ, T. W. LEE, AND D. PICKERING From the Virology and Public Health Laboratory, Churchill Hospital,
Received 18 December 2007/Returned for modification 9 March 2008/Accepted 18 June 2008
 CLINICAL AND VACCINE IMMUNOLOGY, Aug. 2008, p. 1222 1228 Vol. 15, No. 8 1556-6811/08/$08.00 0 doi:10.1128/cvi.00491-07 Randomized Clinical Trial Assessing the Safety and Immunogenicity of Oral Microencapsulated
CLINICAL AND VACCINE IMMUNOLOGY, Aug. 2008, p. 1222 1228 Vol. 15, No. 8 1556-6811/08/$08.00 0 doi:10.1128/cvi.00491-07 Randomized Clinical Trial Assessing the Safety and Immunogenicity of Oral Microencapsulated
Foodborne Disease in the Region of Peel
 Foodborne Disease in the Region of Peel HIGHLIGHTS The incidence of selected foodborne diseases was generally higher in Peel than in Ontario between 1993 and 22. A higher incidence was observed in Peel
Foodborne Disease in the Region of Peel HIGHLIGHTS The incidence of selected foodborne diseases was generally higher in Peel than in Ontario between 1993 and 22. A higher incidence was observed in Peel
Status of Vaccine Research and Development for Shigella Prepared for WHO PD-VAC
 Status of Vaccine Research and Development for Shigella Prepared for WHO PD-VAC I. About the Disease and Pathogen Basic information on pathogen, including transmission, estimated global disease burden
Status of Vaccine Research and Development for Shigella Prepared for WHO PD-VAC I. About the Disease and Pathogen Basic information on pathogen, including transmission, estimated global disease burden
H.pylori IgA Cat #
 DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite D/E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC.
 DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
DIAGNOSTIC AUTOMATION, INC. 23961 Craftsman Road, Suite E/F, Calabasas, CA 91302 Tel: (818) 591-3030 Fax: (818) 591-8383 onestep@rapidtest.com technicalsupport@rapidtest.com www.rapidtest.com See external
Evaluation of a Bivalent (CVD 103-HgR/CVD 111) Live Oral Cholera Vaccine in Adult Volunteers from the United States and Peru
 Live Oral Cholera Vaccine in Adult Volunteers from the United States and Peru") INFECTION AND IMMUNITY, Sept. 1997, p. 3852 3856 Vol. 65, No. 9 0019-9567/97/$04.00 0 Copyright 1997, American Society for Microbiology Evaluation of a Bivalent ( 103-HgR/ 111) Live Oral Cholera Vaccine
INFECTION AND IMMUNITY, Sept. 1997, p. 3852 3856 Vol. 65, No. 9 0019-9567/97/$04.00 0 Copyright 1997, American Society for Microbiology Evaluation of a Bivalent ( 103-HgR/ 111) Live Oral Cholera Vaccine
Bacterial Enteric Pathogens: Clostridium difficile, Salmonella, Shigella, Escherichia coli, and others
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 48 Bacterial Enteric Pathogens: Clostridium difficile, Salmonella, Shigella, Escherichia coli, and others Authors Olivier Vandenberg, MD, PhD Michèle
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 48 Bacterial Enteric Pathogens: Clostridium difficile, Salmonella, Shigella, Escherichia coli, and others Authors Olivier Vandenberg, MD, PhD Michèle
H. pylori Antigen ELISA Kit
 H. pylori Antigen ELISA Kit Catalog Number KA3142 96 assays Version: 04 Intended for research use only www.abnova.com Table of Contents Introduction... 3 Intended Use... 3 Background... 3 Principle of
H. pylori Antigen ELISA Kit Catalog Number KA3142 96 assays Version: 04 Intended for research use only www.abnova.com Table of Contents Introduction... 3 Intended Use... 3 Background... 3 Principle of
Shigellosis. Classification and external resources
 Page 1 of 7 Shigellosis From Wikipedia, the free encyclopedia Shigellosis Classification and external resources Specialty ICD-10 ICD-9-CM infectious disease A03 (http://apps.who.int/classifications/icd10/browse/2016/en#/a03)
Page 1 of 7 Shigellosis From Wikipedia, the free encyclopedia Shigellosis Classification and external resources Specialty ICD-10 ICD-9-CM infectious disease A03 (http://apps.who.int/classifications/icd10/browse/2016/en#/a03)
Infections of the Gastrointestinal Tract. Microbiology, Pathophysiology, and Clinical Features
 Infections of the Gastrointestinal Tract Microbiology, Pathophysiology, and Clinical Features CURRENT TOPICS IN INFECTIOUS DISEASE Series Editors: William B. Greenough III Chief, Infectious Disease Division
Infections of the Gastrointestinal Tract Microbiology, Pathophysiology, and Clinical Features CURRENT TOPICS IN INFECTIOUS DISEASE Series Editors: William B. Greenough III Chief, Infectious Disease Division
Immune Responses in Ileostomy Fluid and Serum after Oral Cholera Vaccination of Patients Colectomized because of Ulcerative Colitis
 INFECTION AND IMMUNITY, Aug. 1998, p. 3995 3999 Vol. 66, No. 8 0019-9567/98/$04.00 0 Copyright 1998, American Society for Microbiology. All Rights Reserved. Immune Responses in Ileostomy Fluid and Serum
INFECTION AND IMMUNITY, Aug. 1998, p. 3995 3999 Vol. 66, No. 8 0019-9567/98/$04.00 0 Copyright 1998, American Society for Microbiology. All Rights Reserved. Immune Responses in Ileostomy Fluid and Serum
Human Obestatin ELISA
 K-ASSAY Human Obestatin ELISA For the quantitative determination of obestatin in human serum and plasma Cat. No. KT-495 For Research Use Only. 1 Rev. 081309 K-ASSAY PRODUCT INFORMATION Human Obestatin
K-ASSAY Human Obestatin ELISA For the quantitative determination of obestatin in human serum and plasma Cat. No. KT-495 For Research Use Only. 1 Rev. 081309 K-ASSAY PRODUCT INFORMATION Human Obestatin
54 MMWR March 17, Appendix B. Guidelines for Confirmation of Foodborne-Disease Outbreaks
 54 MMWR March 17, 2000 Appendix B Guidelines for Confirmation of Foodborne-Disease Outbreaks A foodborne-disease outbreak (FBDO) is defined as an incident in which two or more persons experience a similar
54 MMWR March 17, 2000 Appendix B Guidelines for Confirmation of Foodborne-Disease Outbreaks A foodborne-disease outbreak (FBDO) is defined as an incident in which two or more persons experience a similar
VIRAL AGENTS CAUSING GASTROENTERITIS
 VIRAL AGENTS CAUSING GASTROENTERITIS VIRAL AGENTS CAUSING GASTROENTERITIS Pathogens discussed in our lectures 1. Rotavirus 2. Enteric adenoviruses 3. Caliciviruses 4. Astroviruses 5. Toroviruses Viruses
VIRAL AGENTS CAUSING GASTROENTERITIS VIRAL AGENTS CAUSING GASTROENTERITIS Pathogens discussed in our lectures 1. Rotavirus 2. Enteric adenoviruses 3. Caliciviruses 4. Astroviruses 5. Toroviruses Viruses
Nifuroxazide (Ercefuryl) Plus Oral rehydration solution Versus Oral Rehydration Alone in Hospitalized Pediatric Gastroenteritis
 Plus Oral rehydration solution Versus Oral Rehydration Alone in Hospitalized Pediatric Gastroenteritis") Nifuroxazide (Ercefuryl) Plus Oral rehydration solution Versus Oral Rehydration Alone in Hospitalized Pediatric Gastroenteritis Lourdes T. Santiago, M.D.,* Catherine P. Ranoa, M.D.,** Edmond G. Chan, M.D.***
Nifuroxazide (Ercefuryl) Plus Oral rehydration solution Versus Oral Rehydration Alone in Hospitalized Pediatric Gastroenteritis Lourdes T. Santiago, M.D.,* Catherine P. Ranoa, M.D.,** Edmond G. Chan, M.D.***
however, and the present communication is concerned with some of
 THE AGGLUTINATION OF HUMAN ERYTHROCYTES MODIFIED BY TREATMENT WITH NEWCASTLE DISEASE AND INFLUENZA VIRUS' ALFRED L. FLORMAN' Pediatric Service and Division of Bacteriology, The Mount Sinai Hospital, New
THE AGGLUTINATION OF HUMAN ERYTHROCYTES MODIFIED BY TREATMENT WITH NEWCASTLE DISEASE AND INFLUENZA VIRUS' ALFRED L. FLORMAN' Pediatric Service and Division of Bacteriology, The Mount Sinai Hospital, New
Alberta Health and Wellness Public Health Notifiable Disease Management Guidelines August 2011
 August 2011 Campylobacteriosis Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) August 2011 August 2011 October 2005 Case
August 2011 Campylobacteriosis Revision Dates Case Definition Reporting Requirements Remainder of the Guideline (i.e., Etiology to References sections inclusive) August 2011 August 2011 October 2005 Case
WYANDOT COUNTY 2018 COMMUNICABLE DISEASE REPORT. The communicable disease summary of reportable infectious diseases for January 2018 December 2018.
 WYANDOT COUNTY 2018 COMMUNICABLE DISEASE REPORT The communicable disease summary of reportable infectious diseases for January 2018 December 2018. TABLE OF CONTENTS Annual Communicable Diseases... 3 Communicable
WYANDOT COUNTY 2018 COMMUNICABLE DISEASE REPORT The communicable disease summary of reportable infectious diseases for January 2018 December 2018. TABLE OF CONTENTS Annual Communicable Diseases... 3 Communicable