Summer Communicable Disease Forum. July 30, 2015
|
|
|
- Angela Murphy
- 5 years ago
- Views:
Transcription



1 Summer Communicable Disease Forum July 30, 2015
2 Overview Communicable Disease Forum format Continuing education credits group signin sheet needed for persons not logged in to webinar Questions Recording Slides posted on NJLMN under Practice Exchange



3 CDS Training Resources Website

4

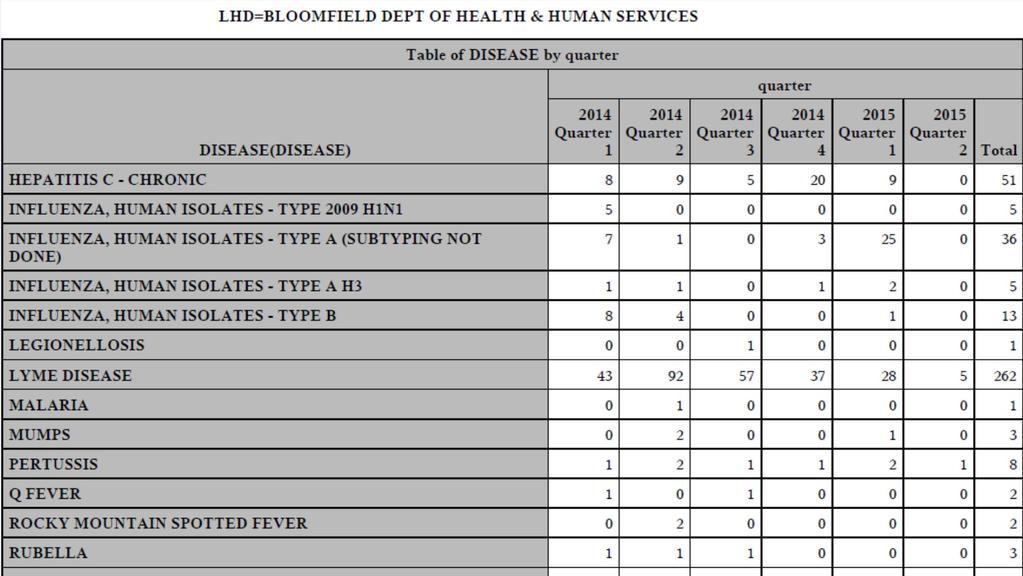
5 Quarterly Reports Quarterly regional highlight report feedback CD reports by LHD Discuss other data needs with regional epi


6
7 Nurses Participants must attend the entire session in order to earn contact hour credits Attendees must participate in all learning activities Verification of participation will be noted by webinar attendance reports or group sign-in sheet and completion of online evaluation Participants cannot miss more than 5 minutes from a 30 minute session; 10 minutes from a 60 minute session Participants must complete the online program evaluation and include your name and address to receive nursing certificate
8 Nurses No commercial support has influenced the planning of the educational objectives and content of this event No influential relationships have been disclosed by planners or presenters which would influence the planning of this activity. If any arise, an announcement will be made at the beginning of the session There is no endorsement of any product by the NJSNA or the ANCC associated with this session
9 STEPS TO INVESTIGATING LEGIONELLA ASSOCIATED WITH A HOSPITAL/LONG- TERM CARE FACILITY Rebecca Greeley, MPH, Infectious Disease Team Coordinator Eric Weren, MSIH, Research Scientist, Environmental & Occupational Health Assessment

10 Legionella Organisms Legionella are ubiquitous in natural and artificial fresh water environments Hot tubs Cooling towers Hot water tanks Large plumbing systems Decorative fountains Grows best in warm temperatures, F Dormant under 77 F and killed above 124 F Legionella pneumonophila serogroup 1 causes majority of human illness, but other serogroups do cause disease

11 Amplification Aerosolization Asolization Protozoa Biofilms Pathogen Proliferation Aerosol Exposure Droplet Size Size Distance Risk of Contracting Legionnaires Disease Susceptible Population Immunosuppressed Elderly
12 Legionellosis Legionnaires' Disease Low attack rate: 5% High mortality: 15% Incubation: 2-14 days Fever: F Breathing difficulty Cough (dry/phlegm) Chills Chest pain Pontiac Fever High attack rate: 90% No mortality Incubation: 1-3 days Muscle aches Flu-like symptoms Self-limiting
13 Who is at risk for legionellosis? Most healthy individuals do not become infected with Legionella bacteria after exposure. People at higher risk of getting sick are: Older people (usually 50 years of age or older) Current or former smokers Those with a chronic lung disease (like COPD or emphysema) Those with a weak immune system from diseases like cancer, diabetes, or kidney failure People who take drugs that suppress (weaken) the immune system (like after a transplant operation or chemotherapy) Aspiration risk or swallowing problems
14 Who to test for legionellosis? Patients who have failed outpatient antibiotic therapy Patients with severe pneumonia, in particular those requiring intensive care Immunocompromised host with pneumonia Patients with pneumonia in the setting of a legionellosis outbreak Patients with a travel history (Patients that have traveled away from their home within two weeks before the onset of illness.) Patients suspected of healthcare-associated pneumonia NO Person-to-Person Spread!
15 Public Health Investigations Surveillance Rationale Monitor and describe incidence and trends of cases Rapidly recognize cases that occur in similar locations or with similar exposures Identify opportunities for control and prevention
16 Reporting of Cases Cases are reported into NJ s Communicable Disease Reporting and Surveillance System (CDRSS) Local Health Departments are responsible for performing a disease investigation into each case reported for their residents Information needed includes illness onset, incubation period, potential exposures that include water, LTC resident, over-night travel, decorative fountains
17 Perfect Partnership Public Health LHD NJDOH Healthcare Stakeholders Acute care Patients being seen who may be cases IPs obtaining pertinent info Long-term care Residents with pneumonia Building investigations
18 Initial Steps in Long-Term Care Investigations One-confirmed case of legionellosis in LTC resident = OUTBREAK LHD to verify the person meets confirmed case definition LHD to establish illness onset date and incubation period LHD needs to confirm patient was only in LTC (or healthcare facility) during incubation period
19 Investigation Continues Once case is linked to the building, NJDOH generates an Outbreak Number (E-number) LHD and NJDOH to set up conference call with facility Facility Administrators Director of Nursing Infection Preventionist Facility Manager and Maintenance Information needed on initial conference call: Clinical information on the case (nebulizer, oxygen, aspiration risk?) Possible water exposures of the case Building information (age, size, number of water outlets)
20 Immediate Actions for Facility Immediate prevention actions: shower filters, bottled water, removing aerators from sinks Hiring water consultant with experience in Legionella control Schedule building walk-through with consultant, LHD and NJDOH represented On-going surveillance for clinical pneumonias Water sampling for Legionella culture Remediation Follow-up testing
21 BUILDING INVESTIGATION
22 Building Investigation Hire experienced water consultant Schedule building walk-through Facility management Consultant LHD and NJDOH Water sampling for Legionella culture and speciation Plan Remediation & Follow-up
23 Conditions for Legionella amplification Water from supplier is not sterile Temperatures: optimum F Grow F Water stagnation Scale and sediment Symbiotic with amoeba, protozoa & algae Rubber, some plastics support growth
24 Building information Age, size & construction, room configurations Renovation History Plumbing system Design Number & type of water outlets Preventive Maintenance Connection to fire sprinkler system Heating/Cooling System Occupancy
25 Building Assessment: Water condition as supplied (Cl & Temp) Whirlpool spas and hot tubs Decorative fountains Cooling towers and evaporative condensers AC drip pan drainage Recent or ongoing construction/renovation Repair or construction of public water system
26 Sources of Exposure Breath mist Cooling tower mist Showers & aerators Nebulizer Spa/whirlpool Decorative fountain Aspiration of water Ice machines Drinking tap water Eating food made with tap water
27 Plumbing System Risk Factors Tanks sediment & temp stratification Biofilm in plumbing Deadlegs stagnant water Pipes inappropriately capped off Unused rooms (sections closed off, rooms unoccupied) Rubber gaskets & expansion tank lining Water temperature & Cl at outlets
28 Pre-Remediation Sampling Recommendations Use a CDC certified ELITE Laboratory ( Sample & process entire1 liter Approximately 10% of outlets Rooms associated with case Rooms distal to the case room Unused & underused outlets All tank(s) Hot water return(s) Supply water
29 Safe Limits in Potable Water No known safe amount Shoot for ALARA OSHA Technical Manual limits do NOT apply Assess preventive maintenance if detected in <30% of samples Remediate if detect in >30% of samples Local remediation at locations with >1 cfu/ml
30 Emergency Remediation Superheat or Hyperchlorination hours Minimum contact level at outlets Heat >160F Chlorine >50 ppm Hourly sampling to assure contact level Significant Patient Safety Issues to address
31 Post-Remediation Sampling Recommendations Same analysis and locations as the preremediation sampling Every 2 weeks for 3 months Monthly for 3 months Quarterly for 1.5 years Review all results to reassess situation Can relocate for repeat negative results LHD to get updates from facility progress
32 Secondary Disinfection Systems Chlorination Chlorine Dioxide Monochloramine Copper-Silver Ion Heat Ozone UV
33 LHD Follow-up Plan? Maintain communication with facility Assure sampling results are distributed LHD NJDOH Schedule conference calls as needed Frequent and regular contact with facility
34 Questions? Rebecca Greeley Eric Weren

35 UPDATE ON VIRAL RESPIRATORY PATHOGENS AVIAN INFLUENZA & MERS Lisa McHugh, Influenza Surveillance Coordinator / Manager, Regional Epidemiology Program
 Wild birds are the natural reservoir Greatest risk for")

36 Influenza Viruses Three types Type A Can infect humans and a variety of animals (birds, pigs, horses) Wild birds are the natural reservoir Greatest risk for epidemic/pandemic Type B Humans only known reservoir Can cause epidemics but not pandemics Type C Humans and swine known reservoirs Mild illness in humans without seasonality
37 Antigenic Shift and Drift Shift (Type A only) Major changes new subtype Exchange of gene segments May cause pandemic Example: H3N2 replaced H2N2 in 1968 Drift (Types A and B) Minor change, within subtype Gradual accumulation of amino acid changes in HA and/or NA May cause epidemic Example: drifted A/H3N2/Fujian circulated A/H3N2/Panama (vaccine strain 2003/4) Occurs infrequently Occurs continuously Cox NJ, Subbarao K. Lancet 1999;354:
38 Novel Influenza A Virus Human infections with influenza A virus subtypes that are different from the currently circulating human subtypes (A/H1 and A/H3) Human infections with novel influenza A viruses which are transmissible person to person may signal the beginning of an influenza pandemic
39 Pandemics Factors that can favor a pandemic Ability to replicate in humans and cause serious disease with high mortality Have immunologically naïve human population Efficient human-to-human transmission
40 Novel Influenza A In June 2007, Novel Influenza A was added to the nationally notifiable disease list Novel influenza A viruses under surveillance H5N1 Avian Influenza 2009 H1N1 Swine Influenza H3N2 Swine Influenza H7N9 Avian Influenza H10N8 Avian Influenza H1N1 Swine Influenza H5Nx Avian Influenza
41 Avian Influenza (AI) Viruses Type A viruses Natural reservoir is wild waterfowl Birds carry virus in respiratory tract and intestines Does not usually cause illness in wild birds May cause severe disease in domesticated birds Can survive at low temperatures and low humidity for days to weeks Can survive in water
 Low Pathogenic Avian Influenza (LPAI) Does not usually cause illness in wild birds May cause mild disease in poultry Cause poultry outbreaks worldwide Can")
42 LPAI vs. HPAI (Birds) Low Pathogenic Avian Influenza (LPAI) Does not usually cause illness in wild birds May cause mild disease in poultry Cause poultry outbreaks worldwide Can evolve into HPAI Highly Pathogenic Avian Influenza (HPAI) Usually does not cause illness in wild birds Usually causes high mortality in domestic poultry Examples: H5,H7
43 HPAI H5Nx US Detections began December 2014 H5N2, H5N8, H5N1 Detected in 21 states Pacific, Central, and Mississippi Flyways 15 states with outbreak in domestic poultry/captive birds 6 states with detections in wild birds only NJ has not been impacted No human illness to date

44
45 Response Animals USDA/NJDA lead agency illness in animals Ongoing AI surveillance Outbreaks in animals Quarantine restrict movement Eradicate - depopulation Monitor region Disinfect affected locations Test to confirm virus-free

46 Response Animals Outbreak identified/confirmed Zones created around area Depopulation of inner rings Foam or CO Gas Surveillance and prevention of outer rings Establishment of control zones to prevent spread On-site composting and burial
47 Public Health Response CDC/NJDOH lead for human illness Reporting and testing of ill individuals Monitoring of exposed individuals 10 days from last exposure Type of monitoring TBD Administration of antiviral post exposure prophylaxis
48 Public Health Guidance Risk to general public LOW Highest risk to impacted farm and outbreak response workers Same reporting and testing as other novel influenza A viruses ILI plus exposure Antivirals are being recommended for workers
49 Middle East Respiratory Syndrome Coronavirus (MERS CoV)
50 Coronavirus (CoV) Common virus Mild to moderate upper-respiratory tract illnesses (common cold) Can be associated with GI illness CoV was the cause of SARS (severe acute respiratory syndrome) Incubation periods longer than common cold Usually circulate in the winter and spring
51 CoV Prevalent in humans and domestic animals (cats, dogs, birds) SARS was a novel coronavirus believed to originate from civet cats Current novel coronavirus is believed to have originated in bats
52 Middle Eastern Respiratory Syndrome (MERS- CoV) Identified in human in April 2012 Initial circulation Arabian peninsula (Jordan, Saudi Arabia, and Qatar) Case count as of 7/17/15 1,368 cases; 490 deaths Travel related cases in other countries Clusters with person to person spread have been documented (not sustained)


53
 Most with chronic co-morbidities Case fatality")
54 MERS CoV Epidemiology Asymptomatic to severe Fever, chills, headache, cough, dyspnea, myalgia are common Mostly adults (median age 50 years) Most with chronic co-morbidities Case fatality ~35%
55 MERS CoV Epidemiology Incubation period 5 days (range 2-14) Infectious period at least while symptomatic may be as long as 3 weeks No shedding prior to symptoms Asymptomatic cases have been identified HCW s and children who had contact with confirmed cases
56 Surveillance Criteria Need to meet both clinical and epidemiologic criteria Fever and pneumonia or acute respiratory distress Travel history to affected country Close contact with confirmed/suspect case History of working in health care facility in impacted country Less symptoms requirement
57 Surveillance Criteria A patient with fever (>100.4 F) AND pneumonia or acute respiratory distress syndrome (based on clinical or radiologic evidence) AND one of more of the following: History of travel from countries in or near the Arabian Peninsula within 14 days before symptom onset OR Close contact with a symptomatic traveler who developed fever and acute respiratory illness (not necessarily pneumonia) within 14 days after traveling from countries in or near the Arabian Peninsula OR History of being in a healthcare facility (as a patient, worker, or visitor) in the Republic of Korea within 14 days before symptom onset, OR A member of a cluster of patients with severe acute respiratory illness (e.g., feve and pneumonia requiring hospitalization) of unknown etiology in which MERSCoV is being evaluated by state of local health officials
58 Surveillance Criteria A patient with fever (>100.4 F) AND pneumonia or acute respiratory distress syndrome (based on clinical or radiologic evidence) AND one of more of the following: History of travel from countries in or near the Arabian Peninsula within 14 days before symptom onset OR Close contact with a symptomatic traveler who developed fever and acute respiratory illness (not necessarily pneumonia) within 14 days after traveling from countries in or near the Arabian Peninsula OR History of being in a healthcare facility (as a patient, worker, or visitor) in the Republic of Korea within 14 days before symptom onset, OR A member of a cluster of patients with severe acute respiratory illness (e.g., feve and pneumonia requiring hospitalization) of unknown etiology in which MERSCoV is being evaluated by state of local health officials
59 Surveillance Criteria (con t) A patient with fever (>100.4 F) AND symptoms of respiratory illness (not necessarily pneumonia; e.g., cough, shortness of breath) AND history of being in a healthcare facility (as a patient, worker, or visitor) within 14 days before symptom onset in countries in or near the Arabian Peninsula in which recent healthcare associate cases of MERS have been identified, OR Fever OR symptoms of respiratory illness (not necessarily pneumonia; e.g. cough, shortness of breath) AND close contact with a confirmed MERS case while the case was ill.
60 Republic of Korea May 2015 first case Symptomatic traveler from Middle East Seen at 2 clinics and 2 hospitals Extensive contact tracing/monitoring 186 laboratory confirmed cases and 35 deaths (7/21/15) To date, all cases (excluding the index case) have been linked to a single chain of transmission and are associated with health care facilities.

61 Last onset July 2

62

63
64 MERS COMMON ISSUES/CONCERNS
65 MERS CoV Lab Testing PHEL can conduct testing NP/OP, Sputum, Serum Others Priority of testing on a case by case basis Results with 6-8 hours after receipt at PHEL Transportation of specimens can be challenging
66 Clinical Management Mostly supportive care Standard, contact, and airborne precautions should be implemented upon suspicion Hospitalization is not required e-care.html
67 Facility Response/Implications Implement measures to quickly identify suspect cases and prevent additional transmission Monitor staff, patients and visitors that came in contact with case Will be asked to monitor staff for signs/symptoms Asymptomatic workers with unprotected exposures will be excluded from work for 14 days
68 Local Health Department Gather case information Complete or assist with PUI form Assist facility in specimen transport At home patient management Monitoring of exposed contacts
69 Questions? Lisa McHugh, MPH New Jersey Department of Health Communicable Disease Service Phone:
70 COMMUNICABLE DISEASE BRIEFS Kristin Innes, Zoonotic Disease Epidemiologist Shereen Semple, Vectorborne Disease Coordinator Diana Theriault, Regional Epidemiologist
71 Kristin Innes, MPH, CHES RABIES UPDATE
72 Rabies Exposure A bite (penetration of the skin by teeth) from a potentially rabid animal Non-bite - Scratches, abrasions, open wounds (bleeding within 24 hrs.), or mucous membranes (eyes) contaminated with saliva or other potentially infectious material (brain or spinal cord) from a potentially rabid animal
73 Bat Exposures Known bite or non bite exposure Any direct contact with a bat when a bite or other exposure cannot be excluded Rabies prophylaxis should be considered when a bat is in the same room as a person/domestic animal who might be unaware, or cannot communicate that a bite or direct contact occurred Deeply sleeping person who awakens to find a bat in the room An adult witnessing a bat in the room with a previously unattended small child or mentally disabled or intoxicated person or domestic animal
74 Rabies Submission State couriers can transport low risk specimens to Rabies Lab Know where your nearest location is and its scheduled pick up time Test results are generally available the next working day, if received by 2:00pm Submit specimens Monday Wednesday, if possible, for timely results. High risk samples should be delivered directly to the Rabies Lab to prevent delay in prophylaxis
75 Notification of Test Result All test results will be faxed to the Health Officer from the Rabies Lab NJDOH will call the LHD to confirm that results were received and to assist in identification of exposed persons or domestic animals The LHD should notify all parties involved This may include investigating and identifying other exposed individuals and domestic animals Note: The NJ Dept. of Agriculture will handle exposed livestock species.
76 Constituent Outreach Provide after hours contact information to ACOs, vets, EDs, and physicians If you notice an increase in calls from a certain provider or on a specific topic, provide education to the facility
77 Resources NJDOH Rabies website: Bat Guidance: Specimen submission: Guide to Post-exposure Prophylaxis: pdf
78 Shereen Semple, MS, Vectorborne Disease and Ebola Team Lead VIRAL HEMORRHAGIC FEVERS: EBOLA UPDATES AND LASSA CASE INVESTIGATION
79 Diana Theriault, MPH, Regional Epidemiologist IDENTIFYING & MONITORING COMMUNITY CONTACTS IN RESPONSE TO LASSA FEVER CASE
80 Community contact tracing and monitoring Newark HD established a local response team Key responsibilities Identify close community contacts Survey administration Risk assessment Daily symptom monitoring and response Data management Identify community leaders and educators to assist in messaging REP collaborated onsite with Newark HD and was liaison to NJDOH response team
81 Contact Identification Case patient had a close-knit extended family 37 potential contacts identified Standard questionnaire was developed and used to interview contacts and determine risk
82 High Risk Classification & Response Exposure: Direct, unprotected contact (skin/mucosal) with potentially infectious material (vomitus, excreta, blood or body fluids) Including mouth-to-mouth kissing or sexual contact Response: Direct active monitoring for 21 days 2x daily temperature readings, 1 directly observed Exclusions Young children excluded from daycare; no other work/school restrictions No airline travel, no commercial conveyances Out of state travel case-by-case basis
83 Low Risk Classification & Response Exposure: Casual contact (skin to skin, sharing room/vehicle) or protected close contact (healthcare, cleaning/laundry, lab) with PPE (no contact with blood/body fluids) Response: Active monitoring for 21 days 2x daily self-monitored temperature readings, reported 1x daily to LHD with any symptoms Exclusions Young children excluded from daycare; no other work/school restrictions International travel case-by-case basis
84 Risk Classifications Risk assessment questionnaires reviewed by regional epidemiologists and Newark HD and assigned risk category 37 total community contacts 14high risk 13low risk 9no known risk 1refused interview PEP was offered for high risk contacts; all declined
85 Daily Monitoring All contacts monitored temperatures twice daily Low risk contacts were contacted by phone once daily (same as EVD active monitoring) High risk contacts were observed taking temperatures at the family s home or via FaceTime/Skype once daily The LHD made a site visit at the home for any non-complaint community members
86 Data Management All exposed community contacts entered and managed in CDRSS Temperature readings entered by Newark HD; compliance issues documented in case Regional epidemiologists monitored CDRSS data daily and brought compliance issues/ symptoms to DOH lassa response team REP notified LHDs where persons resided if outside Newark, but Newark monitored all community contacts At end of monitoring period, cases closed as not a case
87 When Exposed Persons Become Symptomatic #1: One high risk community contact became symptomatic with a low grade temperature (99ºF), back pain, heavy eyes and swelling. Admitted to Hospital C on day 7 of DAM. Tested negative for lassa and was released home #2: The same contact also became ill on day 20 of DAM with increasingly severe symptoms of fever, headache, and tonsilitis while at work in Morris County. Contact visited Occupational Health and consulted NJDOH NJDOH and CDC decided to have contact evaluated. Morris County EMS transported her to Hospital C Contact was again tested for lassa fever, result negative
88 Challenges Difficult to quickly identify and interview large number of contacts Some contacts hesitant to provide information Cultural practices regarding mourning and burial Direct active monitoring logistics, sensitivity to family concerns
89 Importance of Messaging Community meetings held to educate contacts and build rapport with the community Meetings held with a religious leader to address concerns with the family while respecting customs Discussing the stigma faced with community members helped to address concerns and foster good communication Establishing a point of contact within the extended family for communications addressed both logistics and sensitivity to family concerns
90 Lessons Learned Previously established relationships with community and religious partners provided assistance in communication and education Stigma associated with on going EVD outbreak in Liberia may have contributed to delayed diagnosis and hesitancy with contact interviews Previously established EVD monitoring protocols facilitated implementation for lassa fever response Collaboration between NJDOH and LHD was essential to a coordinated response
91 Acknowledgements Newark Department of Health and Human Services Essex Regional Health Commission Morris County Office of Health Management Livingston Health Department All Local Health Departments involved Community leaders throughout Newark NJDOH Lassa Team CDC CERT Team THANK YOU!!!

92


93 Fifth Disease New Education Materials FAQ Exposure Notice for Childcare
94 Upcoming training / meetings 2015 Northeast Epidemiology Conference ($): September 30 October 2, 2015; New Brunswick: e.html Fall 2015 Communicable Disease Forums (in-person) October/November dates TBD
95 Evaluations and Credits Attendees will receive an evaluation link If you are registered with gotowebinar, you have attended If you watched webinar in a group: Send sign-in sheet containing Summer 2015 CD Forum, today s date (July 30, 2015), participant s name/signature, organization, and NJLMN address to Kim Cervantes, at fax or kim.cervantes@doh.state.nj.us Evaluation will be active for 1 week Public health CEs will appear on NJLMN transcript Nursing certificates will be ed following completion of evaluation include name/ *Credits may take up to 2 weeks

96 Questions / Suggestions: Kim Cervantes, kim.cervantes@doh.state.nj.us
INFLUENZA SURVEILLANCE
 Cough, Cough, Sneeze, Wheeze: Update on Respiratory Disease Lisa McHugh, MPH Infectious and Zoonotic Disease Program Communicable Disease Service New Jersey Department of Health INFLUENZA SURVEILLANCE
Cough, Cough, Sneeze, Wheeze: Update on Respiratory Disease Lisa McHugh, MPH Infectious and Zoonotic Disease Program Communicable Disease Service New Jersey Department of Health INFLUENZA SURVEILLANCE
Cough, Cough, Sneeze, Wheeze: Update on Respiratory Disease
 Cough, Cough, Sneeze, Wheeze: Update on Respiratory Disease Lisa McHugh, MPH Infectious and Zoonotic Disease Program Communicable Disease Service New Jersey Department of Health INFLUENZA SURVEILLANCE
Cough, Cough, Sneeze, Wheeze: Update on Respiratory Disease Lisa McHugh, MPH Infectious and Zoonotic Disease Program Communicable Disease Service New Jersey Department of Health INFLUENZA SURVEILLANCE
CMS REQUIREMENTS TO REDUCE LEGIONELLA: RISK IN HEALTHCARE FACILITY WATER SYSTEMS. May 21, 2018
 CMS REQUIREMENTS TO REDUCE LEGIONELLA: RISK IN HEALTHCARE FACILITY WATER SYSTEMS May 21, 2018 LEGIONELLOSIS AND PUBLIC HEALTH Rebecca Greeley, MPH Infectious Disease Team Lead Communicable Disease Service
CMS REQUIREMENTS TO REDUCE LEGIONELLA: RISK IN HEALTHCARE FACILITY WATER SYSTEMS May 21, 2018 LEGIONELLOSIS AND PUBLIC HEALTH Rebecca Greeley, MPH Infectious Disease Team Lead Communicable Disease Service
EPIDEMIOLOGY SURVEILLANCE REPORT Northeast Region. Namitha Reddy Regional Coordinator North/Central West Region
 EPIDEMIOLOGY SURVEILLANCE REPORT Northeast Region Namitha Reddy Regional Coordinator North/Central West Region 1 This report is for use by Public Health Officials only and not for public distribution.
EPIDEMIOLOGY SURVEILLANCE REPORT Northeast Region Namitha Reddy Regional Coordinator North/Central West Region 1 This report is for use by Public Health Officials only and not for public distribution.
Lassa Fever /1/17. Reporting Requirements. Timeline. Timeline Continued NICOLE L. MAZUR, MPH EPIDEMIOLOGIST NEW JERSEY DEPARTMENT OF HEALTH
 Reporting Requirements Cases should be reported by phone to the local health department where the patient resides. Lassa Fever 2015 NICOLE L. MAZUR, MPH EPIDEMIOLOGIST NEW JERSEY DEPARTMENT OF HEALTH Call
Reporting Requirements Cases should be reported by phone to the local health department where the patient resides. Lassa Fever 2015 NICOLE L. MAZUR, MPH EPIDEMIOLOGIST NEW JERSEY DEPARTMENT OF HEALTH Call
What is Legionnaires' disease?
 Understanding Legionnaires disease: A Fact Sheet For Workers Organization(s): New York Committee for Occupational Safety and Health Other languages: Spanish Summary Statement: This NYCOSH fact sheet is
Understanding Legionnaires disease: A Fact Sheet For Workers Organization(s): New York Committee for Occupational Safety and Health Other languages: Spanish Summary Statement: This NYCOSH fact sheet is
Legionellosis Water Management and Investigation Case Study
 Legionellosis Water Management and Investigation Case Study Michigan Department of Health and Human Services Bryce Spiker, MPH Legionellosis Epidemiologist Mike Wesenberg Environmental Health Specialist
Legionellosis Water Management and Investigation Case Study Michigan Department of Health and Human Services Bryce Spiker, MPH Legionellosis Epidemiologist Mike Wesenberg Environmental Health Specialist
WINTER COMMUNICABLE DISEASE FORUM
 WINTER COMMUNICABLE DISEASE FORUM FEBRUARY 01, 2017 Overview Continuing education credits group sign-in sheet needed for persons not logged in to webinar Questions Recording Slides posted on NJLMN under
WINTER COMMUNICABLE DISEASE FORUM FEBRUARY 01, 2017 Overview Continuing education credits group sign-in sheet needed for persons not logged in to webinar Questions Recording Slides posted on NJLMN under
ANSI/ASHRAE Standard Legionellosis: Risk Management for Building Water Systems
 ANSI/ASHRAE Standard 188-2015 Legionellosis: Risk Management for Building Water Systems Published June 26, 2015 Patricia T. Graef, P.E. Member SSPC-188 January, 2018 PURPOSE: Establish minimum legionellosis
ANSI/ASHRAE Standard 188-2015 Legionellosis: Risk Management for Building Water Systems Published June 26, 2015 Patricia T. Graef, P.E. Member SSPC-188 January, 2018 PURPOSE: Establish minimum legionellosis
THIS IS AN OFFICIAL NH DHHS HEALTH ALERT
 THIS IS AN OFFICIAL NH DHHS HEALTH ALERT Distributed by the NH Health Alert Network Health.Alert@nh.gov August 25, 2018 0800 EDT NH-HAN 20180825 Cluster of Legionella pneumophila Pneumonia (Legionnaire
THIS IS AN OFFICIAL NH DHHS HEALTH ALERT Distributed by the NH Health Alert Network Health.Alert@nh.gov August 25, 2018 0800 EDT NH-HAN 20180825 Cluster of Legionella pneumophila Pneumonia (Legionnaire
Legionnaires Disease Q&A (General) (Source: OSHA) (4/29/10)
 (Source: OSHA) (4/29/10)") Legionnaires Disease Q&A (General) (Source: OSHA) (4/29/10) Q. What is Legionnaires Disease? A. Legionnaires disease is a common name for one of the several illnesses caused by Legionella bacteria. Legionnaires
Legionnaires Disease Q&A (General) (Source: OSHA) (4/29/10) Q. What is Legionnaires Disease? A. Legionnaires disease is a common name for one of the several illnesses caused by Legionella bacteria. Legionnaires
National Legionnaires Disease Surveillance, Outbreak Detection, and Response
 National Center for Immunization & Respiratory Diseases National Legionnaires Disease Surveillance, Outbreak Detection, and Response Ally Binder, MS Surveillance Epidemiologist Respiratory Diseases Branch
National Center for Immunization & Respiratory Diseases National Legionnaires Disease Surveillance, Outbreak Detection, and Response Ally Binder, MS Surveillance Epidemiologist Respiratory Diseases Branch
Pandemic Preparedness
 Pandemic Preparedness Disclosure Dr. Michael Braida is a full-time International SOS / MedAire employee Regional Medical Director Northern Seas based in Aberdeen MedAire Medical Director for Europe Medical
Pandemic Preparedness Disclosure Dr. Michael Braida is a full-time International SOS / MedAire employee Regional Medical Director Northern Seas based in Aberdeen MedAire Medical Director for Europe Medical
Legionella Bacteria and Microorganisms in Data Center HVAC Systems
 Legionella Bacteria and Microorganisms in Data Center HVAC Systems Rob Rottersman, MS, CIH Principal Ramboll #DATACENTERWORLD #CPEXPO CHANNELPARTNERSCONFERENCE.COM DATACENTERWORLD.COM Data Center World
Legionella Bacteria and Microorganisms in Data Center HVAC Systems Rob Rottersman, MS, CIH Principal Ramboll #DATACENTERWORLD #CPEXPO CHANNELPARTNERSCONFERENCE.COM DATACENTERWORLD.COM Data Center World
Information collected from influenza surveillance allows public health authorities to:
 OVERVIEW OF INFLUENZA SURVEILLANCE IN NEW JERSEY Influenza Surveillance Overview Surveillance for influenza requires monitoring for both influenza viruses and disease activity at the local, state, national,
OVERVIEW OF INFLUENZA SURVEILLANCE IN NEW JERSEY Influenza Surveillance Overview Surveillance for influenza requires monitoring for both influenza viruses and disease activity at the local, state, national,
PUBLIC HEALTH SIGNIFICANCE SEASONAL INFLUENZA AVIAN INFLUENZA SWINE INFLUENZA
 INFLUENZA DEFINITION Influenza is an acute highly infectious viral disease characterized by fever, general and respiratory tract catarrhal manifestations. Influenza has 3 Types Seasonal Influenza Avian
INFLUENZA DEFINITION Influenza is an acute highly infectious viral disease characterized by fever, general and respiratory tract catarrhal manifestations. Influenza has 3 Types Seasonal Influenza Avian
Preventing Legionella Transmission An Environmental Health View
 Preventing Legionella Transmission An Environmental Health View April 25, 2013 Erin Reinsborough Environmental Health Specialist Mission Statement Together with the Halton community, the Health Department
Preventing Legionella Transmission An Environmental Health View April 25, 2013 Erin Reinsborough Environmental Health Specialist Mission Statement Together with the Halton community, the Health Department
AVIAN FLU BACKGROUND ABOUT THE CAUSE. 2. Is this a form of SARS? No. SARS is caused by a Coronavirus, not an influenza virus.
 AVIAN FLU BACKGROUND 1. What is Avian Influenza? Is there only one type of avian flu? Avian influenza, or "bird flu", is a contagious disease of animals caused by Type A flu viruses that normally infect
AVIAN FLU BACKGROUND 1. What is Avian Influenza? Is there only one type of avian flu? Avian influenza, or "bird flu", is a contagious disease of animals caused by Type A flu viruses that normally infect
Outbreak of travel-associated Legionnaires' disease Palmanova, Mallorca (Spain), September October Main conclusions and options for response
, September October Main conclusions and options for response") RAPID RISK ASSESSMENT Outbreak of travel-associated Legionnaires' disease Palmanova, Mallorca (Spain), September October 2017 23 October 2017 Main conclusions and options for response An increase in Legionnaires
RAPID RISK ASSESSMENT Outbreak of travel-associated Legionnaires' disease Palmanova, Mallorca (Spain), September October 2017 23 October 2017 Main conclusions and options for response An increase in Legionnaires
Running head: INFLUENZA VIRUS SEASON PREPAREDNESS AND RESPONSE 1
 Running head: INFLUENZA VIRUS SEASON PREPAREDNESS AND RESPONSE 1 Electron micrograph of H1N1 Virus (CDC, 2009) Influenza Virus Season Preparedness and Response Patricia Bolivar Walden University Epidemiology
Running head: INFLUENZA VIRUS SEASON PREPAREDNESS AND RESPONSE 1 Electron micrograph of H1N1 Virus (CDC, 2009) Influenza Virus Season Preparedness and Response Patricia Bolivar Walden University Epidemiology
Richmond, Virginia. Assignment Description
 Infectious Diseases, Environmental Health Virginia Department of Health, Division of Environmental Epidemiology/Division of Surveillance and Investigation Richmond, Virginia Assignment Description The
Infectious Diseases, Environmental Health Virginia Department of Health, Division of Environmental Epidemiology/Division of Surveillance and Investigation Richmond, Virginia Assignment Description The
Ralph KY Lee Honorary Secretary HKIOEH
 HKIOEH Round Table: Updates on Human Swine Influenza Facts and Strategies on Disease Control & Prevention in Occupational Hygiene Perspectives 9 July 2009 Ralph KY Lee Honorary Secretary HKIOEH 1 Influenza
HKIOEH Round Table: Updates on Human Swine Influenza Facts and Strategies on Disease Control & Prevention in Occupational Hygiene Perspectives 9 July 2009 Ralph KY Lee Honorary Secretary HKIOEH 1 Influenza
1918 Influenza; Influenza A, H1N1. Basic agent information. Section I- Infectious Agent. Section II- Dissemination
 1918 Influenza; Influenza A, H1N1 Basic agent information Section I- Infectious Agent Risk Group: - RG3 Synonym or Cross reference: - Spanish Flu - 1918 Flu - El Grippe Characteristics: - SELECT AGENT
1918 Influenza; Influenza A, H1N1 Basic agent information Section I- Infectious Agent Risk Group: - RG3 Synonym or Cross reference: - Spanish Flu - 1918 Flu - El Grippe Characteristics: - SELECT AGENT
Influenza: The Threat of a Pandemic
 April, 2009 Definitions Epidemic: An increase in disease above what you what would normally expect. Pandemic: A worldwide epidemic 2 What is Influenza? Also called Flu, it is a contagious respiratory illness
April, 2009 Definitions Epidemic: An increase in disease above what you what would normally expect. Pandemic: A worldwide epidemic 2 What is Influenza? Also called Flu, it is a contagious respiratory illness
Influenza B viruses are not divided into subtypes, but can be further broken down into different strains.
 Influenza General Information Influenza (the flu) is a highly transmissible respiratory illness caused by influenza viruses. It can cause mild to severe illness, and may lead to death. Older people, young
Influenza General Information Influenza (the flu) is a highly transmissible respiratory illness caused by influenza viruses. It can cause mild to severe illness, and may lead to death. Older people, young
Middle East respiratory syndrome coronavirus (MERS-CoV) and Avian Influenza A (H7N9) update
 and Avian Influenza A (H7N9) update") 30 August 2013 Middle East respiratory syndrome coronavirus (MERS-CoV) and Avian Influenza A (H7N9) update Alert and Response Operations International Health Regulations, Alert and Response and Epidemic
30 August 2013 Middle East respiratory syndrome coronavirus (MERS-CoV) and Avian Influenza A (H7N9) update Alert and Response Operations International Health Regulations, Alert and Response and Epidemic
NCCID RAPID REVIEW. 1. What are the case definitions and guidelines for surveillance and reporting purposes?
 NCCID RAPID REVIEW 1. What are the case definitions and guidelines for surveillance and reporting purposes? Middle East Respiratory Syndrome Coronavirus: Ten Questions and Answers for Canadian Public Health
NCCID RAPID REVIEW 1. What are the case definitions and guidelines for surveillance and reporting purposes? Middle East Respiratory Syndrome Coronavirus: Ten Questions and Answers for Canadian Public Health
Current and Emerging Legionella Diagnostics
 Current and Emerging Legionella Diagnostics Nicole Wolter Centre for Respiratory Diseases and Meningitis (CRDM) National Institute for Communicable Diseases nicolew@nicd.ac.za 7 th FIDSSA Conference, Cape
Current and Emerging Legionella Diagnostics Nicole Wolter Centre for Respiratory Diseases and Meningitis (CRDM) National Institute for Communicable Diseases nicolew@nicd.ac.za 7 th FIDSSA Conference, Cape
Legionnella. You can t t see it but you can catch it. Dr Charmaine Gauci MD, MSc, PhD Head of Disease Surveillance Unit
 Legionnella You can t t see it but you can catch it Dr Charmaine Gauci MD, MSc, PhD Head of Disease Surveillance Unit Legionella infections First documented outbreak name from 221 cases of pneumonia occurred
Legionnella You can t t see it but you can catch it Dr Charmaine Gauci MD, MSc, PhD Head of Disease Surveillance Unit Legionella infections First documented outbreak name from 221 cases of pneumonia occurred
SAFETY BULLETIN #3-05 November 11, 2005 Key Facts About Avian Influenza
 Pacific Maritime Association Accident Prevention Department 550 California Street, P. O. Box 7861 San Francisco, California 94120-7861 SAFETY BULLETIN #3-05 November 11, 2005 Key Facts About Avian Influenza
Pacific Maritime Association Accident Prevention Department 550 California Street, P. O. Box 7861 San Francisco, California 94120-7861 SAFETY BULLETIN #3-05 November 11, 2005 Key Facts About Avian Influenza
RESEARCH WITH MIDDLE EAST RESPIRATORY SYNDROME CORONAVIRUS (MERS-CoV)
") Page 1 of 5 RESEARCH WITH SYNDROME CORONAVIRUS (MERS-CoV) The University of Pittsburgh has developed guidelines to establish a system of education and safeguards to ensure that all Federal, State, and
Page 1 of 5 RESEARCH WITH SYNDROME CORONAVIRUS (MERS-CoV) The University of Pittsburgh has developed guidelines to establish a system of education and safeguards to ensure that all Federal, State, and
Outbreak Basics. Alice Shumate, PhD Jason Mehr, MPH
 Outbreak Basics Alice Shumate, PhD Jason Mehr, MPH Local Health Department (LHD) Roles and Responsibilities LHD Preparation LHDs are required to respond to public health emergencies LHD must provide health
Outbreak Basics Alice Shumate, PhD Jason Mehr, MPH Local Health Department (LHD) Roles and Responsibilities LHD Preparation LHDs are required to respond to public health emergencies LHD must provide health
Legionellosis Outbreak-Genesee County, June, 2014 March, Summary Analysis
 Legionellosis Outbreak-Genesee County, June, 2014 March, 2015 Summary Analysis Michigan Department of Health and Human Services Genesee County Health Department (This report was edited on January 15, 2016
Legionellosis Outbreak-Genesee County, June, 2014 March, 2015 Summary Analysis Michigan Department of Health and Human Services Genesee County Health Department (This report was edited on January 15, 2016
RESEARCH WITH HIGHLY PATHOGENIC AVIAN INFLUENZA H5N1
 Page 1 of 8 RESEARCH WITH HIGHLY PATHOGENIC AVIAN INFLUENZA H5N1 The University of Pittsburgh has developed guidelines to establish a system of education and safeguards to ensure compliance with both the
Page 1 of 8 RESEARCH WITH HIGHLY PATHOGENIC AVIAN INFLUENZA H5N1 The University of Pittsburgh has developed guidelines to establish a system of education and safeguards to ensure compliance with both the
Avian influenza Avian influenza ("bird flu") and the significance of its transmission to humans
 and the significance of its transmission to humans") 15 January 2004 Avian influenza Avian influenza ("bird flu") and the significance of its transmission to humans The disease in birds: impact and control measures Avian influenza is an infectious disease
15 January 2004 Avian influenza Avian influenza ("bird flu") and the significance of its transmission to humans The disease in birds: impact and control measures Avian influenza is an infectious disease
Legionnaire s disease
 Legionnaire s disease Connecticut Environmental Health Association Meeting April 9, 2019 Paul Gacek MPH, CPH Legionellosis Surveillance Coordinator & Waterborne Disease Coordinator Epidemiology and Emerging
Legionnaire s disease Connecticut Environmental Health Association Meeting April 9, 2019 Paul Gacek MPH, CPH Legionellosis Surveillance Coordinator & Waterborne Disease Coordinator Epidemiology and Emerging
Acute respiratory illness This is a disease that typically affects the airways in the nose and throat (the upper respiratory tract).
.") Influenza glossary Adapted from the Centers for Disease Control and Prevention, US https://www.cdc.gov/flu/glossary/index.htm and the World Health Organization http://www.wpro.who.int/emerging_diseases/glossary_rev_sept28.pdf?ua=1
Influenza glossary Adapted from the Centers for Disease Control and Prevention, US https://www.cdc.gov/flu/glossary/index.htm and the World Health Organization http://www.wpro.who.int/emerging_diseases/glossary_rev_sept28.pdf?ua=1
Influenza Infection In Human. Dr. Zuhaida A. Jalil Surveillance Sector Disease Control Division, MOH Malaysia 3 May 2018
 Influenza Infection In Human Dr. Zuhaida A. Jalil Surveillance Sector Disease Control Division, MOH Malaysia 3 May 2018 Objective of the session: After completing this session, you will be able to: Understand
Influenza Infection In Human Dr. Zuhaida A. Jalil Surveillance Sector Disease Control Division, MOH Malaysia 3 May 2018 Objective of the session: After completing this session, you will be able to: Understand
Influenza-Associated Pediatric Mortality rev Jan 2018
 rev Jan 2018 Infectious Agent Influenza A, B or C virus BASIC EPIDEMIOLOGY Transmission Transmission occurs via droplet spread. After a person infected with influenza coughs, sneezes, or talks, influenza
rev Jan 2018 Infectious Agent Influenza A, B or C virus BASIC EPIDEMIOLOGY Transmission Transmission occurs via droplet spread. After a person infected with influenza coughs, sneezes, or talks, influenza
WHAT S INFECTIOUS and HOT: 2014
 WHAT S INFECTIOUS and HOT: 2014 Gary Garber MD FRCPC FACP FIDSA CCPE Medical Director-Infection Prevention and Control Professor-Division of Infectious Diseases Ottawa Hospital/U Ottawa OUTBREAK ALERT:
WHAT S INFECTIOUS and HOT: 2014 Gary Garber MD FRCPC FACP FIDSA CCPE Medical Director-Infection Prevention and Control Professor-Division of Infectious Diseases Ottawa Hospital/U Ottawa OUTBREAK ALERT:
Middle East Respiratory Syndrome Coronavirus
 GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 54 Middle East Respiratory Syndrome Coronavirus Author Ziad.A. Memish, MD, FRCPC, FACP Chapter Editor Michael Stevens, MD, MPH Topic Outline Topic outline
GUIDE TO INFECTION CONTROL IN THE HOSPITAL CHAPTER 54 Middle East Respiratory Syndrome Coronavirus Author Ziad.A. Memish, MD, FRCPC, FACP Chapter Editor Michael Stevens, MD, MPH Topic Outline Topic outline
MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers, Secretary
 MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers, Secretary COMMUNITY HEALTH ADMINISTRATION Peter A. Sybinsky, Ph.D., Director Richard W. Stringer, Deputy Director April 29, 2009 Swine
MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers, Secretary COMMUNITY HEALTH ADMINISTRATION Peter A. Sybinsky, Ph.D., Director Richard W. Stringer, Deputy Director April 29, 2009 Swine
Influenza and Novel Respiratory Infections
 Influenza and Novel Respiratory Infections Implementing Effective Surveillance on the College Campus Craig Roberts, PA-C, MS Epidemiologist University Health Services University of Wisconsin-Madison Objectives
Influenza and Novel Respiratory Infections Implementing Effective Surveillance on the College Campus Craig Roberts, PA-C, MS Epidemiologist University Health Services University of Wisconsin-Madison Objectives
INFLUENZA-2 Avian Influenza
 INFLUENZA-2 Avian Influenza VL 7 Dec. 9 th 2013 Mohammed El-Khateeb Overview 1. Background Information 2. Origin/History 3. Brief overview of genome structure 4. Geographical Distribution 5. Pandemic Nature
INFLUENZA-2 Avian Influenza VL 7 Dec. 9 th 2013 Mohammed El-Khateeb Overview 1. Background Information 2. Origin/History 3. Brief overview of genome structure 4. Geographical Distribution 5. Pandemic Nature
Avian Influenza: Worker Health and Safety
 Avian Influenza: Worker Health and Safety Lisa J. Delaney, M.S., C.I.H. National Institute for Occupational Safety and Health (NIOSH) The findings and conclusions in this presentation are those of the
Avian Influenza: Worker Health and Safety Lisa J. Delaney, M.S., C.I.H. National Institute for Occupational Safety and Health (NIOSH) The findings and conclusions in this presentation are those of the
Influenza: The past, the present, the (future) pandemic
 pandemic") Influenza: The past, the present, the (future) pandemic Kristin Butler, MLS (ASCP) cm Department of Clinical Laboratory Sciences Louisiana Health Sciences Center - Shreveport Fall 2017 Objectives 1) Detail
Influenza: The past, the present, the (future) pandemic Kristin Butler, MLS (ASCP) cm Department of Clinical Laboratory Sciences Louisiana Health Sciences Center - Shreveport Fall 2017 Objectives 1) Detail
Swine Influenza A: Information for Child Care Providers INTERIM DAYCARE ADVISORY General Information: do not
 Swine Influenza A: Information for Child Care Providers INTERIM DAYCARE ADVISORY 4-29-2009 The State of Connecticut Department of Public Health (DPH) would like to provide information to childcare providers
Swine Influenza A: Information for Child Care Providers INTERIM DAYCARE ADVISORY 4-29-2009 The State of Connecticut Department of Public Health (DPH) would like to provide information to childcare providers
Pandemic Influenza. Bradford H. Lee, MD Nevada State Health Officer. Public Health: Working for a Safer and Healthier Nevada
 Pandemic Influenza Bradford H. Lee, MD Nevada State Health Officer EXHIBIT C Legislative Committee on Health Care Document consists of 29 slides. Entire document provided. Due to size limitations, pages
Pandemic Influenza Bradford H. Lee, MD Nevada State Health Officer EXHIBIT C Legislative Committee on Health Care Document consists of 29 slides. Entire document provided. Due to size limitations, pages
Health care workers (HCWs) caring for suspected (clinically diagnosed) or confirmed cases of. Influenza A(H1N1)v FREQUENTLY ASKED QUESTIONS
 caring for suspected (clinically diagnosed) or confirmed cases of. Influenza A(H1N1)v FREQUENTLY ASKED QUESTIONS") Health care workers (HCWs) caring for suspected (clinically diagnosed) or confirmed cases of Questions found here: FREQUENTLY ASKED QUESTIONS What is pandemic flu? What is the difference between seasonal
Health care workers (HCWs) caring for suspected (clinically diagnosed) or confirmed cases of Questions found here: FREQUENTLY ASKED QUESTIONS What is pandemic flu? What is the difference between seasonal
Novel Coronavirus 2012
 Novel Coronavirus 2012 Susan I. Gerber, MD Respiratory Virus Program Division of Viral Diseases National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention Jan.
Novel Coronavirus 2012 Susan I. Gerber, MD Respiratory Virus Program Division of Viral Diseases National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention Jan.
Viruses: Select Agents and Emerging Pathogens. Patricia Bolívar MS., CLS, PHM
 Viruses: Select Agents and Emerging Pathogens Patricia Bolívar MS., CLS, PHM Objectives Review Select Agent Viruses. Key features to recognize Smallpox virus Update on emerging Viruses of possible pandemic
Viruses: Select Agents and Emerging Pathogens Patricia Bolívar MS., CLS, PHM Objectives Review Select Agent Viruses. Key features to recognize Smallpox virus Update on emerging Viruses of possible pandemic
University of Colorado Denver. Pandemic Preparedness and Response Plan. April 30, 2009
 University of Colorado Denver Pandemic Preparedness and Response Plan April 30, 2009 UCD Pandemic Preparedness and Response Plan Executive Summary The World Health Organization (WHO) and the Centers for
University of Colorado Denver Pandemic Preparedness and Response Plan April 30, 2009 UCD Pandemic Preparedness and Response Plan Executive Summary The World Health Organization (WHO) and the Centers for
Preparing for a Pandemic: What Parents Need to Know About Seasonal and Pandemic Flu
 Preparing for a Pandemic: What Parents Need to Know About Seasonal and Pandemic Flu A Message from the Health Officer An influenza, or flu, pandemic happens when a new flu virus appears that easily spreads
Preparing for a Pandemic: What Parents Need to Know About Seasonal and Pandemic Flu A Message from the Health Officer An influenza, or flu, pandemic happens when a new flu virus appears that easily spreads
Influenza: Wrap- Up and Preview of the Upcoming Season. October 6, 2016 Anita Valiani, MPH
 Influenza: 2015-2016 Wrap- Up and Preview of the Upcoming Season October 6, 2016 Anita Valiani, MPH Anita.valiani@dhhs.nc.gov NC SHARPPS Surveillance for Healthcare-Associated Infections and Resistant
Influenza: 2015-2016 Wrap- Up and Preview of the Upcoming Season October 6, 2016 Anita Valiani, MPH Anita.valiani@dhhs.nc.gov NC SHARPPS Surveillance for Healthcare-Associated Infections and Resistant
2009 H1N1 (Pandemic) virus IPMA September 30, 2009 Anthony A Marfin
 virus IPMA September 30, 2009 Anthony A Marfin") 2009 H1N1 (Pandemic) virus IPMA September 30, 2009 Anthony A Marfin Introduction to Influenza What is influenza? What is pandemic influenza? What is 2009 H1N1 influenza? Current situation & predictions
2009 H1N1 (Pandemic) virus IPMA September 30, 2009 Anthony A Marfin Introduction to Influenza What is influenza? What is pandemic influenza? What is 2009 H1N1 influenza? Current situation & predictions
VIROLOGY OF INFLUENZA. Subtypes: A - Causes outbreak B - Causes outbreaks C - Does not cause outbreaks
 INFLUENZA VIROLOGY OF INFLUENZA Subtypes: A - Causes outbreak B - Causes outbreaks C - Does not cause outbreaks PATHOGENICITY High pathogenicity avian influenza (HPAI) Causes severe disease in poultry
INFLUENZA VIROLOGY OF INFLUENZA Subtypes: A - Causes outbreak B - Causes outbreaks C - Does not cause outbreaks PATHOGENICITY High pathogenicity avian influenza (HPAI) Causes severe disease in poultry
Pandemic H1N1 2009: The Public Health Perspective. Massachusetts Department of Public Health November, 2009
 Pandemic H1N1 2009: The Public Health Perspective Massachusetts Department of Public Health November, 2009 Training Objectives Describe and distinguish between seasonal and pandemic influenza. Provide
Pandemic H1N1 2009: The Public Health Perspective Massachusetts Department of Public Health November, 2009 Training Objectives Describe and distinguish between seasonal and pandemic influenza. Provide
FACT SHEET FOR ADDITIONAL INFORMATION CONTACT
 FACT SHEET FOR ADDITIONAL INFORMATION CONTACT Caroline Calderone Baisley, MPH, RS Michael S. Long, MS Director of Health Director of Environmental Services Tel. 203-622-7836 Tel: 203-622-7838 FREQUENTLY
FACT SHEET FOR ADDITIONAL INFORMATION CONTACT Caroline Calderone Baisley, MPH, RS Michael S. Long, MS Director of Health Director of Environmental Services Tel. 203-622-7836 Tel: 203-622-7838 FREQUENTLY
Influenza. Dr Bhakti Vasant Public Health Physician Metro South Public Health Unit. Metro South Public Health Unit
 Metro South Public Health Unit Influenza Dr Bhakti Vasant Public Health Physician Metro South Public Health Unit Source of image: CDC. Influenza images. Available from URL: https://www.cdc.gov/flu/images/h1
Metro South Public Health Unit Influenza Dr Bhakti Vasant Public Health Physician Metro South Public Health Unit Source of image: CDC. Influenza images. Available from URL: https://www.cdc.gov/flu/images/h1
2009 (Pandemic) H1N1 Influenza Virus
 H1N1 Influenza Virus") 2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
Public Health Responds to Avian Influenza Outbreaks in Commercial Poultry: Lessons from Nigeria
 Public Health Responds to Avian Influenza Outbreaks in Commercial Poultry: Lessons from Nigeria Lora Baker Davis, DVM, MPH Washington State Dept of Agriculture Avian Influenza Surveillance Activity Learning
Public Health Responds to Avian Influenza Outbreaks in Commercial Poultry: Lessons from Nigeria Lora Baker Davis, DVM, MPH Washington State Dept of Agriculture Avian Influenza Surveillance Activity Learning
Complete the Distinguished Lecturer Event Summary Critique
 This ASHRAE Distinguished Lecturer is brought to you by the Society Chapter Technology Transfer Committee Complete the Distinguished Lecturer Event Summary Critique CTTC needs your feedback to continue
This ASHRAE Distinguished Lecturer is brought to you by the Society Chapter Technology Transfer Committee Complete the Distinguished Lecturer Event Summary Critique CTTC needs your feedback to continue
INFLUENZA (Outbreaks; hospitalized or fatal pediatric cases)
") INFLUENZA (Outbreaks; hospitalized or fatal pediatric cases) 1. Agent: Influenza viruses A, B, and C. Only influenza A and B are of public health concern since they are responsible for epidemics. 2. Identification:
INFLUENZA (Outbreaks; hospitalized or fatal pediatric cases) 1. Agent: Influenza viruses A, B, and C. Only influenza A and B are of public health concern since they are responsible for epidemics. 2. Identification:
Influenza A H1N1 Swine Flu Update:
 Influenza A H1N1 Swine Flu Update: Pandemic Influenza Planning for the Workplace Current as of August 2009 Georgia Tech OSHA Consultation Program This course does not necessarily reflect the views or policies
Influenza A H1N1 Swine Flu Update: Pandemic Influenza Planning for the Workplace Current as of August 2009 Georgia Tech OSHA Consultation Program This course does not necessarily reflect the views or policies
Mahoning County Public Health. Epidemiology Response Annex
 Mahoning County Public Health Epidemiology Response Annex Created: May 2006 Updated: February 2015 Mahoning County Public Health Epidemiology Response Annex Table of Contents Epidemiology Response Document
Mahoning County Public Health Epidemiology Response Annex Created: May 2006 Updated: February 2015 Mahoning County Public Health Epidemiology Response Annex Table of Contents Epidemiology Response Document
BC MHOs, PHNLs, ICPs, ERDOCs, IDSPEC, MEDMICRO, AMBULANCE, BCCDC Internal Groups, National Surveillance Network Partners
 To: Subject: Purpose: Action required: Recommendations: BC MHOs, PHNLs, ICPs, ERDOCs, IDSPEC, MEDMICRO, AMBULANCE, BCCDC Internal Groups, National Surveillance Network Partners November 1, 2013 Emerging
To: Subject: Purpose: Action required: Recommendations: BC MHOs, PHNLs, ICPs, ERDOCs, IDSPEC, MEDMICRO, AMBULANCE, BCCDC Internal Groups, National Surveillance Network Partners November 1, 2013 Emerging
Supplemental Resources
 Supplemental Resources Key Chain Questions 15 Key Questions Activity Key Questions: 1. What are the core community mitigation measures? 2. How can community mitigation measures reduce the effects of
Supplemental Resources Key Chain Questions 15 Key Questions Activity Key Questions: 1. What are the core community mitigation measures? 2. How can community mitigation measures reduce the effects of
Module 1 : Influenza - what is it and how do you get it?
 Module 1 : Influenza - what is it and how do you get it? Responsible/facilitators General Objective Specific Objectives Methodology Agency medical coordinator Understand the mechanism how influenza is
Module 1 : Influenza - what is it and how do you get it? Responsible/facilitators General Objective Specific Objectives Methodology Agency medical coordinator Understand the mechanism how influenza is
Conflict of Interest and Disclosures. Research funding from GSK, Biofire
 Pandemic Influenza Suchitra Rao, MBBS, Assistant Professor, Pediatric Infectious Diseases, Hospital Medicine and Epidemiology Global Health and Disasters Course, 2018 Conflict of Interest and Disclosures
Pandemic Influenza Suchitra Rao, MBBS, Assistant Professor, Pediatric Infectious Diseases, Hospital Medicine and Epidemiology Global Health and Disasters Course, 2018 Conflict of Interest and Disclosures
A. No. There are no current reports of avian influenza (bird flu) in birds in the U.S.
 in birds in the U.S.") Bird Flu FAQ 2 Frequently Asked Avian Influenza Questions Avian influenza in birds Q. What is avian influenza? A. Avian influenza is an infectious disease of birds caused by type A strains of the influenza
Bird Flu FAQ 2 Frequently Asked Avian Influenza Questions Avian influenza in birds Q. What is avian influenza? A. Avian influenza is an infectious disease of birds caused by type A strains of the influenza
What is Influenza? Patricia Daly MD, FRCPC Medical Health Officer and Medical Director of Communicable Disease Control
 Vancouver Coastal Health & The Vancouver Coastal Health Research Institute presents: On Call with VGH Experts Lecture Series The Flu and You What is Influenza? Patricia Daly MD, FRCPC Medical Health Officer
Vancouver Coastal Health & The Vancouver Coastal Health Research Institute presents: On Call with VGH Experts Lecture Series The Flu and You What is Influenza? Patricia Daly MD, FRCPC Medical Health Officer
Surveillance, Reporting and Control of Influenza and Pertussis. Steve Fleming, EdM Hillary Johnson, MHS Epidemiologists Immunization Program, MDPH
 Surveillance, Reporting and Control of Influenza and Pertussis Steve Fleming, EdM Hillary Johnson, MHS Epidemiologists Immunization Program, MDPH Disclosures The speaker has no financial interest or conflict
Surveillance, Reporting and Control of Influenza and Pertussis Steve Fleming, EdM Hillary Johnson, MHS Epidemiologists Immunization Program, MDPH Disclosures The speaker has no financial interest or conflict
UTSW/BioTel EMS TRAINING BULLETIN October EMS TB Ebola Virus Disease (EVD)
") UTSW/BioTel EMS TRAINING BULLETIN October 2014 EMS TB 14-006 Ebola Virus Disease (EVD) Purpose: 1. To inform & provide management recommendations to UTSW/BioTel EMS System EMS Providers about Ebola Virus
UTSW/BioTel EMS TRAINING BULLETIN October 2014 EMS TB 14-006 Ebola Virus Disease (EVD) Purpose: 1. To inform & provide management recommendations to UTSW/BioTel EMS System EMS Providers about Ebola Virus
H1N1 Influenza. Influenza-A Basics. Influenza Basics. April 1, History of Influenza Pandemics. April 1 September 25, 2009
 April 1, 2009 H1N1 Influenza Jeff Goad, Pharm.D., MPH Associate Professor of Clinical Pharmacy USC School of Pharmacy April 1 September 25, 2009 History of Influenza Pandemics 400 B.C. 1889 Russian Flu
April 1, 2009 H1N1 Influenza Jeff Goad, Pharm.D., MPH Associate Professor of Clinical Pharmacy USC School of Pharmacy April 1 September 25, 2009 History of Influenza Pandemics 400 B.C. 1889 Russian Flu
Influenza Update for Iowa Long-Term Care Facilities. Iowa Department of Public Health Center for Acute Disease Epidemiology
 Influenza Update for Iowa Long-Term Care Facilities Iowa Department of Public Health Center for Acute Disease Epidemiology Webinar Information All participants will be muted during the presentation. Questions
Influenza Update for Iowa Long-Term Care Facilities Iowa Department of Public Health Center for Acute Disease Epidemiology Webinar Information All participants will be muted during the presentation. Questions
CDC Health Advisory 04/29/2009
 H1N1 (Swine Flu) is a sub-type of Influenza A. Wexford Labs disinfectants are effective against Influenza A. Current CDC Recommendations for Environmental Control in the Healthcare Setting: CDC Health
H1N1 (Swine Flu) is a sub-type of Influenza A. Wexford Labs disinfectants are effective against Influenza A. Current CDC Recommendations for Environmental Control in the Healthcare Setting: CDC Health
County-Wide Pandemic Influenza Preparedness & Response Plan
 County-Wide Pandemic Influenza Preparedness & Response Plan Presented by the Santa Clara County Public Health Department to the Emergency Managers Association April 27, 2006 Why the Concern About Pandemic
County-Wide Pandemic Influenza Preparedness & Response Plan Presented by the Santa Clara County Public Health Department to the Emergency Managers Association April 27, 2006 Why the Concern About Pandemic
Novel H1N1 Influenza A: Protecting the Public
 Novel H1N1 Influenza A: Protecting the Public Humayun J. Chaudhry, DO, MS, SM, FACOI, FACP, FAODME President, American College of Osteopathic Internists; Clinical Associate Professor of Preventive Medicine,
Novel H1N1 Influenza A: Protecting the Public Humayun J. Chaudhry, DO, MS, SM, FACOI, FACP, FAODME President, American College of Osteopathic Internists; Clinical Associate Professor of Preventive Medicine,
EBOLA 101. Update for EMS System Stakeholders. Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Nor Cal EMS Version 10/25/2014
 EBOLA 101 Update for EMS System Stakeholders Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Nor Cal EMS Version 10/25/2014 Conference 1 Version #1 Date 10/25/14 Content good for current situation 10/25/14
EBOLA 101 Update for EMS System Stakeholders Eric M. Rudnick, MD, FACEP, FAAEM Medical Director Nor Cal EMS Version 10/25/2014 Conference 1 Version #1 Date 10/25/14 Content good for current situation 10/25/14
Preparing for a Pandemic What Business and Organization Leaders Need to Know
 Preparing for a Pandemic What Business and Organization Leaders Need to Know Information provided by. Introduction An influenza, or flu, pandemic happens when a new flu virus appears that easily spreads
Preparing for a Pandemic What Business and Organization Leaders Need to Know Information provided by. Introduction An influenza, or flu, pandemic happens when a new flu virus appears that easily spreads
Frequently Asked Questions on Avian Influenza
 Frequently Asked Questions on Avian Influenza What is bird flu (avian influenza) and how does it differ from seasonal flu and pandemic influenza? Avian influenza or bird flu is a disease of birds caused
Frequently Asked Questions on Avian Influenza What is bird flu (avian influenza) and how does it differ from seasonal flu and pandemic influenza? Avian influenza or bird flu is a disease of birds caused
SEA/CD/154 Distribution : General. Avian Influenza in South-East Asia Region: Priority Areas for Research
 SEA/CD/154 Distribution : General Avian Influenza in South-East Asia Region: Priority Areas for Research World Health Organization Publications of the World Health Organization enjoy copyright protection
SEA/CD/154 Distribution : General Avian Influenza in South-East Asia Region: Priority Areas for Research World Health Organization Publications of the World Health Organization enjoy copyright protection
Influenza : What is going on? How can Community Health Centers help their patients?
 Influenza 2008-2009: What is going on? How can Community Health Centers help their patients? Beth Nivin Bureau of Communicable Diseases New York City Dept. of Health and Mental Hygiene By the end of this
Influenza 2008-2009: What is going on? How can Community Health Centers help their patients? Beth Nivin Bureau of Communicable Diseases New York City Dept. of Health and Mental Hygiene By the end of this
Legionellosis Surveillance System Evaluation
 Environmental Health Waterborne Diseases, Infectious Diseases Wisconsin Department of Health Services, Division of Public Health, Bureau of Environmental & Occupational Health and Bureau of Communicable
Environmental Health Waterborne Diseases, Infectious Diseases Wisconsin Department of Health Services, Division of Public Health, Bureau of Environmental & Occupational Health and Bureau of Communicable
Current Swine Influenza Situation Updated frequently on CDC website 109 cases in US with 1 death 57 confirmed cases aroun
 Swine Flu Olga Emgushov, MD, MPH Director Epidemiology/Public Health Preparedness Brevard County Health Department April 30, 2009 Current Swine Influenza Situation Updated frequently on CDC website http://www.cdc.gov/swineflu/
Swine Flu Olga Emgushov, MD, MPH Director Epidemiology/Public Health Preparedness Brevard County Health Department April 30, 2009 Current Swine Influenza Situation Updated frequently on CDC website http://www.cdc.gov/swineflu/
(and what you can do about them)
") (and what you can do about them) What s an outbreak? In general, more cases than expected (baseline) More cases clustered in a specific unit or facility than you d expect at a particular time of year Some
(and what you can do about them) What s an outbreak? In general, more cases than expected (baseline) More cases clustered in a specific unit or facility than you d expect at a particular time of year Some
County of Los Angeles Department of Health Services Public Health
 Biological Incident Plan PANDEMIC INFLUENZA GUIDELINES County of Los Angeles Department of Health Services Public Health January 2006 Executive Summary Page 1 The Los Angeles County (LAC) Department of
Biological Incident Plan PANDEMIC INFLUENZA GUIDELINES County of Los Angeles Department of Health Services Public Health January 2006 Executive Summary Page 1 The Los Angeles County (LAC) Department of
Fact Sheet: Legionellosis March 2017
 Fact Sheet Fact Sheet: Legionellosis March 2017 Brought to you by the APSP Recreational Water Quality Committee (RWQC) I. INTRODUCTION Legionellosis is an infection caused by the bacterium Legionella.
Fact Sheet Fact Sheet: Legionellosis March 2017 Brought to you by the APSP Recreational Water Quality Committee (RWQC) I. INTRODUCTION Legionellosis is an infection caused by the bacterium Legionella.
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE
 THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. PREVENTION AND CONTROL OF INFLUENZA Lisa McHugh, MPH Influenza can be a serious
THIS ACTIVITY HAS EXPIRED. CME CREDIT IS NO LONGER AVAILABLE The following content is provided for informational purposes only. PREVENTION AND CONTROL OF INFLUENZA Lisa McHugh, MPH Influenza can be a serious
Influenza & Other Respiratory Viruses Update
 Influenza & Other Respiratory Viruses Update 2013-2014 Pete Shult, PhD. Director, Communicable Disease Division and Emergency Response Erik Reisdorf, MPH M (ASCP) CM Team Lead, Virology Laboratory WCLN
Influenza & Other Respiratory Viruses Update 2013-2014 Pete Shult, PhD. Director, Communicable Disease Division and Emergency Response Erik Reisdorf, MPH M (ASCP) CM Team Lead, Virology Laboratory WCLN
Outbreak Investigation Guidance for Vectorborne Diseases
 COMMUNICABLE DISEASE OUTBREAK MANUAL New Jersey s Public Health Response APPENDIX T3: EXTENDED GUIDANCE Outbreak Investigation Guidance for Vectorborne Diseases As per N.J.A.C. 8:57, viruses that are transmitted
COMMUNICABLE DISEASE OUTBREAK MANUAL New Jersey s Public Health Response APPENDIX T3: EXTENDED GUIDANCE Outbreak Investigation Guidance for Vectorborne Diseases As per N.J.A.C. 8:57, viruses that are transmitted
Epidemiology and Control. Amy D. Sullivan, PhD, MPH Multnomah County Health Department Communicable Disease Services
 Epidemiology and Control Amy D. Sullivan, PhD, MPH Multnomah County Health Department Communicable Disease Services Recognize norovirus clusters in Long Term Care Facilities Partner with your local health
Epidemiology and Control Amy D. Sullivan, PhD, MPH Multnomah County Health Department Communicable Disease Services Recognize norovirus clusters in Long Term Care Facilities Partner with your local health
Incidence of Seasonal Influenza
 What Is All the Fuss? A Just-in in-time Primer on H1N1 Influenza A and Pandemic Influenza provided by the National Association of State EMS Officials May 1, 2009 Disclaimer This self-learning learning
What Is All the Fuss? A Just-in in-time Primer on H1N1 Influenza A and Pandemic Influenza provided by the National Association of State EMS Officials May 1, 2009 Disclaimer This self-learning learning
Something in the Water
 Something in the Water Brian G. Shelton, MPH President & CEO, PathCon Laboratories Ben Kollmeyer, MPH, CIH Chief Technical Officer, Forensic Analytical Consulting Services Presenters Brian G. Shelton,
Something in the Water Brian G. Shelton, MPH President & CEO, PathCon Laboratories Ben Kollmeyer, MPH, CIH Chief Technical Officer, Forensic Analytical Consulting Services Presenters Brian G. Shelton,
Human Cases of Swine Influenza in California, Kansas, New York City, Ohio, Texas, and Mexico Key Points April 26, 2009
 1 Today, CDC confirmed additional human cases of swine influenza A (H1N1) virus infection in the United States, bringing the total number of U.S. confirmed cases to 21. This includes cases in California,
1 Today, CDC confirmed additional human cases of swine influenza A (H1N1) virus infection in the United States, bringing the total number of U.S. confirmed cases to 21. This includes cases in California,
ISPUB.COM. Bird flu: A Throbbing Stone In An Infectious Era. T Wadhwa, P Kumar Thirupathi EPIDEMIOLOGY TRANSMISSION FROM AVIAN TO HUMAN
 ISPUB.COM The Internet Journal of Infectious Diseases Volume 7 Number 1 T Wadhwa, P Kumar Thirupathi Citation T Wadhwa, P Kumar Thirupathi.. The Internet Journal of Infectious Diseases. 2008 Volume 7 Number
ISPUB.COM The Internet Journal of Infectious Diseases Volume 7 Number 1 T Wadhwa, P Kumar Thirupathi Citation T Wadhwa, P Kumar Thirupathi.. The Internet Journal of Infectious Diseases. 2008 Volume 7 Number
with a state park - New Jersey 2012 Rebecca Greeley, MPH Antimicrobial Resistance & Waterborne Disease Coordinator, NJDOH
 Waterborne outbreak of Shigella sonnei associated with a state park - New Jersey 20 Rebecca Greeley, MPH Antimicrobial Resistance & Waterborne Disease Coordinator, NJDOH - 2013 Steps of an Outbreak Investigation
Waterborne outbreak of Shigella sonnei associated with a state park - New Jersey 20 Rebecca Greeley, MPH Antimicrobial Resistance & Waterborne Disease Coordinator, NJDOH - 2013 Steps of an Outbreak Investigation
Severe Acute Respiratory Infection (SARI) Guidelines. Chief Public Health Office Department of Health & Wellness
 Guidelines. Chief Public Health Office Department of Health & Wellness") Severe Acute Respiratory Infection (SARI) Guidelines Chief Public Health Office Department of Health & Wellness 2013 The following document was prepared by the SARI Working Group. Maureen Anderson, Public
Severe Acute Respiratory Infection (SARI) Guidelines Chief Public Health Office Department of Health & Wellness 2013 The following document was prepared by the SARI Working Group. Maureen Anderson, Public
Infection Prevention & Control Resources for York Region Long-Term Care Homes
 Infection Prevention & Control Resources for York Region Long-Term Care Homes September 2017 CONTENTS INTRODUCTION 1 PUBLIC HEALTH INSPECTIONS 1 POLICY REVIEW 1 OUTBREAK MANAGEMENT 2 EDUCATION AND TRAINING
Infection Prevention & Control Resources for York Region Long-Term Care Homes September 2017 CONTENTS INTRODUCTION 1 PUBLIC HEALTH INSPECTIONS 1 POLICY REVIEW 1 OUTBREAK MANAGEMENT 2 EDUCATION AND TRAINING
H5N1 / Avian Influenza Essentials. Quick Reference for Providers and Public Health Officials
 H5N1 / Avian Influenza Essentials Quick Reference for Providers and Public Health Officials December 2005 INFLUENZA Family: Orthomyxoviridae Genus: influenza virus Subtypes: A, B, and C Influenza A INFLUENZA
H5N1 / Avian Influenza Essentials Quick Reference for Providers and Public Health Officials December 2005 INFLUENZA Family: Orthomyxoviridae Genus: influenza virus Subtypes: A, B, and C Influenza A INFLUENZA