A cross-sectional study to assess the long-term health status of patients with lower respiratory tract infections, including Q fever
|
|
|
- Kelly Daniel
- 6 years ago
- Views:
Transcription
1 Postprint Version Journal website &fileId=S Pubmed link DOI /S A cross-sectional study to assess the long-term health status of patients with lower respiratory tract infections, including Q fever A. S. G. VAN DAM A1A2 C1, J. A. F. VAN LOENHOUT A2, J. B. PETERS A3, A. RIETVELD A1A2, W. J. PAGET A2, R. P. AKKERMANS A2, A. OLDE LOOHUIS A2, J. L. A. HAUTVAST A2 AND J. VAN DER VELDEN A2 a1 Department of Infectious Disease Control, Municipal Health Service Hart voor Brabant, s- Hertogenbosch, The Netherlands a2 Academic Collaborative Centre AMPHI, Department of Primary and Community Care, Radboud University Medical Centre, The Netherlands a3 Department of Medical Psychology and Department of Lung Diseases, Radboud University Medical Centre, The Netherlands SUMMARY Patients with a lower respiratory tract infection (LRTI) might be at risk for longterm impaired health status. We assessed whether LRTI patients without Q fever are equally at risk for developing long-term symptoms compared to LRTI patients with Q fever. The study was a cross-sectional cohort design. Long-term health status information of 50 Q fever-positive and 32 Q fever-negative LRTI patients was obtained. Health status was measured by the Nijmegen Clinical Screening Instrument. The most severely affected subdomains of the Q feverpositive group were general quality of life (40%) and fatigue (40%). The most severely affected subdomains of the Q fever-negative group were fatigue (64%) and subjective pulmonary symptoms (35%). Health status did not differ significantly between Q fever-positive LRTI patients and Q fever-negative LRTI patients for all subdomains, except for subjective pulmonary symptoms (P = 0 048). INTRODUCTION Each year, around 25% of the Dutch population visit their General Practitioner (GP) with respiratory symptoms [1]. Part of this group presents with a lower respiratory tract infection (LRTI), which is generally more serious than an upper respiratory infection. A Dutch study showed that patients with community-acquired pneumonia still have an impaired health status 18 months after onset of illness compared to a
2 control population, although these results were attributed more to the effects of age and/or comorbidity than the pneumonia [2]. Furthermore, several studies have shown that Q fever, an infectious illness which presents with high rates of pneumonia in patients in some countries [3] (61 5% in The Netherlands [4]), may have a long-term impact on patients health [5 10]. We found limited information on long-term health status of LRTI patients in general [2]. We assessed the health status of patients who experienced a LRTI the previous year by using a standard questionnaire. Special attention was paid to Q fever in this study, because of the large outbreak that affected The Netherlands during that period [11]. Since patients with Q fever as well as patients with other causes of LRTI appear to be at risk for long-term impaired health status, including fatigue, we investigated whether a LRTI caused by Q fever is a more severe infection in terms of health status at 15 months after onset of illness than other LRTIs. METHODS Design In a cross-sectional cohort study, patients presenting with a LRTI to their GP in 2009 were included, and subsequently their health status was assessed at 15 months after onset of illness. Study site GP practices (n = 14) in the provinces of Northern Brabant and Gelderland, located in or around the epicentre of the Q fever outbreak in The Netherlands, registered patients with a LRTI. Study population Patients with a LRTI, as diagnosed by their GP, were included in the study. Diagnosis was based on clinical symptoms. Patients were categorized into one of the following International Classification of Primary Care (ICPC) groups: R78 acute bronchitis, R80 influenza, R81 pneumonia and R83 other lower respiratory tract infections. Patients aged <18 and >75 years were excluded since the proportion of Q fever infections compared to other infections is limited for these age groups. The inclusion period was from 1 May to 30 September 2009, to exclude a high proportion of pathogens specific for the winter period. All included patients were serologically tested for Q fever in one out of two hospital laboratories as part of regular care. Diagnostic tests were polymerase chain reaction (PCR), immunofluorescence assay (IFA) and complement fixation assay (CFA). Patients were diagnosed as either Q fever positive or Q fever negative. Regular care for Q fever-positive patients also included serological follow-up to diagnose potential cases of chronic Q fever, but these results were not included in our study. Of the 194 registered LRTI patients who were tested for Q fever in 2009, 19 patients could not be contacted, two patients died and six patients moved to a GP practice not included in the study area. This left a total of 167 patients that were invited to participate.
3 Data collection Information on hospitalization of patients during the acute phase of the disease was obtained through their GPs. Between July and September 2010, patients received a health status questionnaire with a consent form from their GP. If the patient did not return the questionnaire within 4 weeks, a reminder was sent by the GP. Health status questionnaire Health status was assessed using the Nijmegen Clinical Screening Instrument (NCSI). The NCSI is a validated instrument and measures health status on eight subdomains of three domains: Symptoms, Functional impairment and Quality of life. The NCSI consists of a battery of instruments (Table 1) and provides a valid and detailed picture of a patients health status [12]. It allows a description of health status at the individual level (as a normal, mild or severe score is available for each subdomain). In addition, the questionnaire contained questions on personal characteristics (gender, age, smoking behaviour) and comorbidity. [TABLE 1.] Statistical analysis SPSS for Windows v. 20 (IBM SPSS Statistics, USA) was used for data entry and analyses of the data. A value of P < 0 05 was considered as statistically significant. All identifiers were removed and data were analysed anonymously. The baseline data of 2009 (from the GP registration of LRTI patients) enabled us to compare responders and non-responders with regard to gender, age, ICPC, hospitalization and Q fever status. χ 2 tests and an unpaired t test were used for comparison of characteristics between patients who tested positive for Q fever vs. patients who tested negative for Q fever. Scores of all eight subdomains of the NCSI were calculated and the proportion of patients with normal, mild and severe scores on the different subdomains were determined, as described in a study by Peters et al. [12]. Differences in NCSI subdomain scores between the group of Q fever-positive and Q fever-negative LRTI patients were analysed using a multivariate model for each subdomain, with correction for relevant confounding characteristics, i.e. gender, age, smoking behaviour, ICPC and comorbidity. ICPC was dichotomized into two items; pneumonia (R81) and other LRTI (an aggregation of R78, R80 and R83). Comorbidity was also dichotomized into two items due to small numbers: no comorbidity vs. one or more underlying diseases (e.g. heart or vascular disease, chronic disease, cancer, immune disorder, diabetes, lung disease, depression).
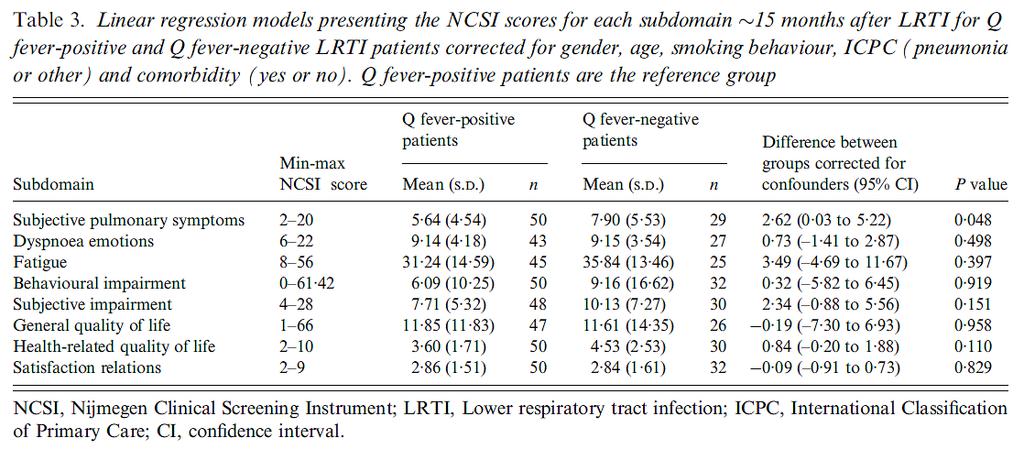
4 RESULTS Eighty-two patients returned the questionnaire, resulting in a response rate of 49%. Patients completed the questionnaire months after initial infection in 2009, with a mean response time of 15 months. There was no significant difference in gender, age and hospitalization between responders and non-responders (data not shown). Responders more often had pneumonia as an ICPC classification (65% vs. 42%, P = 0 004) and more often tested positive for Q fever in 2009 (61% vs. 45%, P = 0 035) compared to non-responders. Characteristics of the study population Of the responders, 50 (61%) patients tested positive for a Q fever infection (Table 2). Significantly more Q fever-positive patients were diagnosed with pneumonia compared to Q fever-negative patients (76% vs. 47%, P = 0 004). Q fever-positive patients were younger (mean age 48 1 years) than Q fever-negative patients (mean age 57 2 years), although the difference was not significant. There were no significant differences between the two groups for hospitalization at baseline, gender, smoking behaviour and comorbidity. Health status Health status of a large proportion of the patients within each group was severely affected at 15 months after onset of illness as measured by the NCSI, ranging from 12% on the subdomains satisfaction relations and behavioural impairment to 64% on the subdomain fatigue (Fig. 1). Within the Q fever-positive LRTI group, general quality of life (40%) and fatigue (40%) were the most severely affected subdomains, while most severely affected subdomains of the Q fever-negative LRTI group were fatigue (64%) and subjective pulmonary symptoms (35%). The proportions of patients who were severely affected on more than one subdomain 15 months after onset of illness were 40% and 56% for the Q fever-positive and Q fever-negative LRTI patients, respectively. [TABLE 2][FIGURE 1] Health status scores between Q fever-positive and Q fever-negative LRTI patients were compared at 15 months after initial illness. Q fever-negative patients scored significantly worse for the subdomain subjective pulmonary symptoms after correcting for the confounders gender, age, smoking behaviour, pneumonia and comorbidity (2 62, P = 0 048) (Table 3). DISCUSSION This study demonstrates that a large group of GP-registered LRTI patients was affected on one or more aspects of health status 15 months after LRTI, especially on fatigue, general quality of life and subjective pulmonary symptoms. These long-term symptoms have also been described in a study by El Moussaoui et al. in
5 community-acquired pneumonia patients with an impaired health status 18 months after their initial illness, especially in patients with a comorbidity [2]. Long-term symptoms and an impaired health status were also seen in patients with Legionnaires disease, for which most patients experience pneumonia during the acute phase of the disease [13]. There was no significant difference in health status scores at 15 months between LRTI patients who were diagnosed with Q fever compared to patients who did not have Q fever, except for the subdomain subjective pulmonary symptoms. The Q fever-negative group experienced significantly more subjective symptoms (overall burden of pulmonary symptoms) than the Q fever-positive group, although we cannot explain why this group had more symptoms. A previous study in The Netherlands identified having Q fever as well as pneumonia as risk factors for a long-term impaired health status [5], which is why one would expect a larger impact on health in the Q fever-positive group of LRTI patients. The main outcome of our study is, however, that long-term health status of Q fever-positive and Q fevernegative LRTI patients was very similar. Results concerning Q fever patients within this study are comparable to previous Dutch Q fever studies, even though this study only considers Q fever patients with a LRTI (in contrast to other studies, where all Q fever patients are considered). Fatigue and general quality of life were the subdomains with the highest proportions of severe scores; these results were also found in the other Dutch studies [5, 6]. Forty per cent of the Q fever patients showed severe fatigue at 15 months after their initial illness, which is similar to the 44% and 52% from the other studies as well. Studies outside The Netherlands also showed fatigue as one of the main long-term health problems for Q fever patients [7 9]. However, it has been shown that over 30% of the general population suffer from chronic fatigue [14, 15], which raises uncertainty about the proportion of fatigue in patients that can be attributed to Q fever. Strengths and limitations of the study Despite the fact that reminders were sent and that patients received the questionnaire from their own GP, the response rate was relatively low (49%). The fact that responders were more often Q fever positive may have been due to the fact that Q fever and its burden of disease received a great deal of media attention during the outbreak. Q fever patients may therefore have deemed it more important to complete a questionnaire on their health status, despite the fact that the letter and questionnaire that were sent to patients did not contain the word Q fever. The low response rate may have resulted in a relatively high proportion of study participants with an impaired health status, especially in the Q fever-negative group (patients with symptoms are considered more eager to participate in studies), indicating that our results might show an overrepresentation of their health impact. Patients were tested for Q fever by two different laboratories, using different diagnostic methods. The most frequently used laboratory tests in Q fever-positive
6 patients were the IFA (50%) and PCR (43%). However, all tests used are considered suitable serodiagnostic assays to diagnose acute Q fever [16, 17]. A potential limitation of our study was that we did not further diagnose the microbiological cause of illness of the Q fever-negative LRTI patients. A study conducted in The Netherlands showed that a wide variety of pathogens is present in patients with acute respiratory tract infections [18], which indicates that it is often difficult to establish the source of an infection in this population. Moreover, Marrie et al. were unable to find any difference in disease recovery at 30 days after onset of illness in patients with atypical pneumonia with unknown microbiological cause and patients with atypical pneumonia due to a pathogen from a series of underlying agents [19]. We do not therefore feel this disproves the overall findings and conclusions. More generally, studies on the health impact of infectious diseases have demonstrated that long-term recovery in patients with varying microbiological diseases, such as Epstein Barr virus, enteroviruses and Coxiella burnetii, all experience long-term fatigue [10, 20], and that post-infective fatigue syndrome is largely predicted by severity of the acute illness rather than by microbiological factors [10]. The observation in our study that Q fever-positive as well as Q fevernegative LRTI patients showed a long-term impaired health status is in line with these studies. CONCLUSIONS This study showed that a large group of LRTI patients was affected on more than one aspect of health status at 15 months after LRTI. We have demonstrated that there is little difference in long-term health status between Q fever-positive and Q fevernegative LRTI patients. GPs should be aware of long-term health problems in LRTI patients, not only those that are Q fever positive but also those that are Q fever negative. ACKNOWLEDGEMENTS We thank all the GPs from the NUHP (Network of GP practices affiliated to Radboud University Medical Centre) who participated in the study, and Clementine Wijkmans from the GGD Hart voor Brabant for the initial idea and preparations of the study. The study was funded by Robuust, a regional supporting organization for primary care in the South of The Netherlands and the Provinciale Raad Gezondheid (county council of health) in the province of Northern Brabant. REFERENCES 1. National Information Network for General Practitioners. Facts and figures about care of General Practitioners in the Netherlands, 2011 ( Accessed June El, Moussaoui R, et al. Long-term symptom recovery and health-related quality of life in patients with mild-to-moderate-severe community-acquired pneumonia. Chest 2006; 130:
7 3. Raoult, D, Marrie, T, Mege, J. Natural history and pathophysiology of Q fever. Lancet Infect Diseases 2005; 5: Dijkstra, F, et al. The Q fever epidemic in The Netherlands: characteristics of notified acute Q fever patients and the association with dairy goat farming. FEMS Immunology and Medical Microbiology 2012; 64: Morroy, G, et al. The health status of Q-fever patients after long-term follow-up. BMC Infectious Diseases 2011; 11: Limonard, GJ, et al. Detailed analysis of health status of Q fever patients 1 year after the first Dutch outbreak: a case-control study. QJM 2010; 103: Ayres, JG, et al. Post-infection fatigue syndrome following Q fever. QJM 1998; 91: Wildman, MJ, et al. Chronic fatigue following infection by Coxiella burnetii (Q fever): tenyear follow-up of the 1989 UK outbreak cohort. QJM 2002; 95: Hatchette, TF, et al. The effect of C. burnetii infection on the quality of life of patients following an outbreak of Q fever. Epidemiology and Infection 2003; 130: Hickie, I, et al. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort study. British Medical Journal 2006; 333: RIVM. National Institute for Public Health and the Environment: diseases and infections ( 12. Peters, JB, et al. Development of a battery of instruments for detailed measurement of health status in patients with COPD in routine care: the Nijmegen Clinical Screening Instrument. Quality of Life Research 2009; 18: Lettinga, KD, et al. Health-related quality of life and posttraumatic stress disorder among survivors of an outbreak of Legionnaires disease. Clinical Infectious Diseases 2002; 35: van't Leven, M, et al. Fatigue and chronic fatigue syndrome-like complaints in the general population. European Journal of Public Health 2010; 20: Kocalevent, RD, et al. Determinants of fatigue and stress. BMC research notes 2011; 4: Schneeberger, PM, et al. Real-time PCR with serum samples is indispensable for early diagnosis of acute Q fever. Clinical and Vaccine Immunology 2010; 17: Herremans, T, et al. Comparison of the performance of IFA, CFA, and ELISA assays for the serodiagnosis of acute Q fever by quality assessment. Diagnostic Microbiology and Infectious Disease 2013; 75: van Gageldonk-Lafeber, AB, et al. A case-control study of acute respiratory tract infection in general practice patients in The Netherlands. Clinical Infectious Diseases 2005; 41: Marrie, TJ, et al. Ambulatory patients with community-acquired pneumonia: the frequency of atypical agents and clinical course. American Journal of Medicine 1996; 101: Devanur, LD, Kerr, JR. Chronic fatigue syndrome. Journal of Clinical Virology 2006; 37:
8 TABLES AND FIGURES

9 Fig. 1. Proportion of patients with normal/mild/severe scores on the different subdomains of the Nijmegen Clinical Screening Instrument at _15 months after lower respiratory tract infection, presented for Q fever-positive (Q+) and Q fevernegative (Q ) patients. QoL, Quality of life; HrQoL, health-related quality of life.
10
Detailed analysis of health status of Q fever patients 1 year after the first Dutch outbreak: a case control study
 Q J Med 2010; 103:953 958 doi:10.1093/qjmed/hcq144 Advance Access Publication 27 August 2010 Detailed analysis of health status of Q fever patients 1 year after the first Dutch outbreak: a case control
Q J Med 2010; 103:953 958 doi:10.1093/qjmed/hcq144 Advance Access Publication 27 August 2010 Detailed analysis of health status of Q fever patients 1 year after the first Dutch outbreak: a case control
Joris AF van Loenhout 1*, W John Paget 1,2, Jan H Vercoulen 3, Clementine J Wijkmans 1,4, Jeannine LA Hautvast 1 and Koos van der Velden 1
 van Loenhout et al. BMC Infectious Diseases 2012, 12:280 STUDY PROTOCOL Open Access Assessing the long-term health impact of Q-fever in the Netherlands: a prospective cohort study started in 2007 on the
van Loenhout et al. BMC Infectious Diseases 2012, 12:280 STUDY PROTOCOL Open Access Assessing the long-term health impact of Q-fever in the Netherlands: a prospective cohort study started in 2007 on the
Risk Factors for Q Fever in the Netherlands
 Article ID: WMC002006 ISSN 2046-1690 Risk Factors for Q Fever in the Netherlands Corresponding Author: Mr. Thijs Veenstra, Epidemiologist, Centre for Infectious Disease Control, National Institute for
Article ID: WMC002006 ISSN 2046-1690 Risk Factors for Q Fever in the Netherlands Corresponding Author: Mr. Thijs Veenstra, Epidemiologist, Centre for Infectious Disease Control, National Institute for
The health status of Q-fever patients after longterm
 RESEARCH ARTICLE Open Access The health status of Q-fever patients after longterm follow-up Gabriëlla Morroy 1,2*, Jeannette B Peters 3,4, Malou van Nieuwenhof 1, Hans HJ Bor 2, Jeannine LA Hautvast 2,
RESEARCH ARTICLE Open Access The health status of Q-fever patients after longterm follow-up Gabriëlla Morroy 1,2*, Jeannette B Peters 3,4, Malou van Nieuwenhof 1, Hans HJ Bor 2, Jeannine LA Hautvast 2,
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/109522
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/109522
Meteorology and infectious diseases: a risk for public health?
 Meteorology and infectious diseases: a risk for public health? Jeroen van Leuken Ph.D. RIVM National Institute for Public Health and the Environment Centre for Infectious Disease Control jeroen.van.leuken@rivm.nl
Meteorology and infectious diseases: a risk for public health? Jeroen van Leuken Ph.D. RIVM National Institute for Public Health and the Environment Centre for Infectious Disease Control jeroen.van.leuken@rivm.nl
Alberta Health. Seasonal Influenza in Alberta. 2012/2013 Season. Surveillance and Assessment Branch. November Government of Alberta 1
 Alberta Health Seasonal Influenza in Alberta 2012/2013 Season Surveillance and Assessment Branch November 2013 2013 Government of Alberta 1 For more information contact: Surveillance and Assessment Branch
Alberta Health Seasonal Influenza in Alberta 2012/2013 Season Surveillance and Assessment Branch November 2013 2013 Government of Alberta 1 For more information contact: Surveillance and Assessment Branch
Fatigue in COPD. Dr. Jan Vercoulen, Clinical Psychologist. Dpt. Medical Psychology Radboud University Nijmegen Medical Center
 Fatigue in COPD Dr. Jan Vercoulen, Clinical Psychologist Dpt. Medical Psychology Radboud University Nijmegen Medical Center Definition COPD GOLD, 2016 Chronic Obstructive Pulmonary Disease = common preventable
Fatigue in COPD Dr. Jan Vercoulen, Clinical Psychologist Dpt. Medical Psychology Radboud University Nijmegen Medical Center Definition COPD GOLD, 2016 Chronic Obstructive Pulmonary Disease = common preventable
Chest radiography in patients suspected of pneumonia in primary care: diagnostic yield, and consequences for patient management
 Chest radiography in patients suspected of pneumonia in primary care: diagnostic yield, and consequences for patient management 4 Speets AM, Hoes AW, Van der Graaf Y, Kalmijn S, Sachs APE, Mali WPThM.
Chest radiography in patients suspected of pneumonia in primary care: diagnostic yield, and consequences for patient management 4 Speets AM, Hoes AW, Van der Graaf Y, Kalmijn S, Sachs APE, Mali WPThM.
The Dubbo Infection Outcomes Study
 The Dubbo Infection Outcomes Study Determinants of protracted illness after acute infection Dubbo Infection Outcomes Study Three parallel cohorts Epstein-Barr virus: - infectious mononucleosis - established
The Dubbo Infection Outcomes Study Determinants of protracted illness after acute infection Dubbo Infection Outcomes Study Three parallel cohorts Epstein-Barr virus: - infectious mononucleosis - established
Australian National Influenza Centres Activity
 Australian National Influenza Centres Activity 2011-12 Professor Dominic Dwyer Medical Virologist Director ICPMR and WHO NIC Westmead Hospital Sydney, NSW 2145, Australia dominic.dwyer@sydney.edu.au WHO
Australian National Influenza Centres Activity 2011-12 Professor Dominic Dwyer Medical Virologist Director ICPMR and WHO NIC Westmead Hospital Sydney, NSW 2145, Australia dominic.dwyer@sydney.edu.au WHO
Weekly Influenza & Respiratory Activity: Statistics Summary
 Weekly Influenza & Respiratory Activity: Statistics Summary 2011-12 updated 7/12/12 Influenza Activity in Minnesota Summary of the 2011-12 Season Since the start of the influenza season, 552 people were
Weekly Influenza & Respiratory Activity: Statistics Summary 2011-12 updated 7/12/12 Influenza Activity in Minnesota Summary of the 2011-12 Season Since the start of the influenza season, 552 people were
Weekly Influenza Activity: Statistics Summary
 Weekly Influenza Activity: Statistics Summary 2010-11 updated 9/9/11 Summary of the 2010-11 Influenza Season Since the start of the influenza season, 215 schools reported outbreaks of ILI. Influenza Activity
Weekly Influenza Activity: Statistics Summary 2010-11 updated 9/9/11 Summary of the 2010-11 Influenza Season Since the start of the influenza season, 215 schools reported outbreaks of ILI. Influenza Activity
Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians
 MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
MEMORANDUM DATE: October 1, 2009 TO: FROM: SUBJECT: Microbiology Laboratory Directors, Infection Preventionists, Primary Care Providers, Emergency Department Directors, Infectious Disease Physicians Michael
Q fever in the Netherlands: public perceptions and behavioral responses in three different epidemiological regions: a follow-up study
 Bults et al. BMC Public Health 2014, 14:263 RESEARCH ARTICLE Open Access Q fever in the Netherlands: public perceptions and behavioral responses in three different epidemiological regions: a follow-up
Bults et al. BMC Public Health 2014, 14:263 RESEARCH ARTICLE Open Access Q fever in the Netherlands: public perceptions and behavioral responses in three different epidemiological regions: a follow-up
2014/2015 Ottawa County Influenza Surveillance Summary
 214/215 Ottawa County Influenza Surveillance Summary Time Period: October 1, 211 to March 31, 215 Michigan Disease Surveillance System (MDSS) MDSS data in Table 1 indicates that there were no new laboratory
214/215 Ottawa County Influenza Surveillance Summary Time Period: October 1, 211 to March 31, 215 Michigan Disease Surveillance System (MDSS) MDSS data in Table 1 indicates that there were no new laboratory
NCCID RAPID REVIEW. 1. What are the case definitions and guidelines for surveillance and reporting purposes?
 NCCID RAPID REVIEW 1. What are the case definitions and guidelines for surveillance and reporting purposes? Middle East Respiratory Syndrome Coronavirus: Ten Questions and Answers for Canadian Public Health
NCCID RAPID REVIEW 1. What are the case definitions and guidelines for surveillance and reporting purposes? Middle East Respiratory Syndrome Coronavirus: Ten Questions and Answers for Canadian Public Health
Burden of acute respiratory infections across Western Australian emergency departments
 Burden of acute respiratory infections across Western Australian emergency departments Rosanne Barnes, Chris C. Blyth, Nick de Klerk, Peter Richmond, Meredith Borland, Parveen Fathima, Faye J. Lim & Hannah
Burden of acute respiratory infections across Western Australian emergency departments Rosanne Barnes, Chris C. Blyth, Nick de Klerk, Peter Richmond, Meredith Borland, Parveen Fathima, Faye J. Lim & Hannah
Surveillance of Hospitalisations for 2009 Pandemic Influenza A(H1N1) in the Netherlands, 5 June 31 December 2009
 in the Netherlands, 5 June 31 December 2009") Surveillance and outbreak reports Surveillance of Hospitalisations for 2009 Pandemic Influenza A(H1N1) in the Netherlands, 5 June 31 December 2009 T M van t Klooster (tessa.van.t.klooster@rivm.nl) 1, C
Surveillance and outbreak reports Surveillance of Hospitalisations for 2009 Pandemic Influenza A(H1N1) in the Netherlands, 5 June 31 December 2009 T M van t Klooster (tessa.van.t.klooster@rivm.nl) 1, C
Coxiella burnetii in bulk tank milk samples from dairy goat and dairy sheep farms in The Netherlands in 2008
 Coxiella burnetii in bulk tank milk samples from dairy goat and dairy sheep farms in The Netherlands in 28 R. van den Brom, E. van Engelen, S. Luttikholt, L. Moll, K. van Maanen, P. Vellema In 27, a human
Coxiella burnetii in bulk tank milk samples from dairy goat and dairy sheep farms in The Netherlands in 28 R. van den Brom, E. van Engelen, S. Luttikholt, L. Moll, K. van Maanen, P. Vellema In 27, a human
Q Fever What men and women on the land need to know
 Q Fever What men and women on the land need to know Dr. Stephen Graves Director, Australian Rickettsial Reference Laboratory Director, Division of Microbiology, Pathology North (Hunter) NSW Health Pathology,
Q Fever What men and women on the land need to know Dr. Stephen Graves Director, Australian Rickettsial Reference Laboratory Director, Division of Microbiology, Pathology North (Hunter) NSW Health Pathology,
Antimicrobial Stewardship in Community Acquired Pneumonia
 Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
Antimicrobial Stewardship in Community Acquired Pneumonia Medicine Review Course 2018 Dr Lee Tau Hong Consultant Department of Infectious Diseases National Centre for Infectious Diseases Scope 1. Diagnosis
2009 (Pandemic) H1N1 Influenza Virus
 H1N1 Influenza Virus") 2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
2009 (Pandemic) H1N1 Influenza Virus September 15, 2009 Olympia, Washington Anthony A Marfin Washington State Department of Health Goals Understand current situation & pattern of transmission of 2009 H1N1
Downloaded from:
 Muller-Pebody, B; Crowcroft, NS; Zambon, MC; Edmunds, WJ (2006) Modelling hospital admissions for lower respiratory tract infections in the elderly in England. Epidemiology and infection, 134 (6). pp.
Muller-Pebody, B; Crowcroft, NS; Zambon, MC; Edmunds, WJ (2006) Modelling hospital admissions for lower respiratory tract infections in the elderly in England. Epidemiology and infection, 134 (6). pp.
STARK COUNTY INFLUENZA SNAPSHOT, WEEK 06 Week ending February 11, 2012, with updates through 02/20/2012.
 STARK COUNTY INFLUENZA SNAPSHOT, WEEK 06 Week ending February 11, 2012, with updates through 02/20/2012. All data are preliminary and may change as additional information is received. NOTE: Compilation
STARK COUNTY INFLUENZA SNAPSHOT, WEEK 06 Week ending February 11, 2012, with updates through 02/20/2012. All data are preliminary and may change as additional information is received. NOTE: Compilation
Acute Q fever related in-hospital mortality in the Netherlands
 O r i g i n a l a r t i c l e Acute Q fever related in-hospital mortality in the Netherlands L.M. Kampschreur 1*, M.C.A. Wegdam-Blans 2, S.F.T. Thijsen 3, C.A.R. Groot 4, P.M. Schneeberger 5, A.A.M.J.
O r i g i n a l a r t i c l e Acute Q fever related in-hospital mortality in the Netherlands L.M. Kampschreur 1*, M.C.A. Wegdam-Blans 2, S.F.T. Thijsen 3, C.A.R. Groot 4, P.M. Schneeberger 5, A.A.M.J.
Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories
 8 Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories Willeke P.J. Franken 1, Steven Thijsen 2, Ron Wolterbeek 3, John J.M. Bouwman 2, Hanane el Bannoudi
8 Variation in T-SPOT.TB spot interpretation between independent observers of different laboratories Willeke P.J. Franken 1, Steven Thijsen 2, Ron Wolterbeek 3, John J.M. Bouwman 2, Hanane el Bannoudi
For questions, or to receive this report weekly by , send requests to either or
 STARK COUNTY INFLUENZA SNAPSHOT, WEEK 47 Week ending November 24, 2012, with updates through 12/1/2012. All data are preliminary and may change as additional information is received. NOTE: Compilation
STARK COUNTY INFLUENZA SNAPSHOT, WEEK 47 Week ending November 24, 2012, with updates through 12/1/2012. All data are preliminary and may change as additional information is received. NOTE: Compilation
Q FEVER Australian and global perspectives including the recent Netherlands outbreak
 Q FEVER Australian and global perspectives including the recent Netherlands outbreak Coxiella burnetii, the causative bacterium for Q Fever is ubiquitous. Thought to be present in every land mass with
Q FEVER Australian and global perspectives including the recent Netherlands outbreak Coxiella burnetii, the causative bacterium for Q Fever is ubiquitous. Thought to be present in every land mass with
THE EPIDEMIOLOGY OF RESPIRATORY SYNCYTIAL VIRUS INFECTIONS IN NSW CHILDREN,
 THE EPIDEMIOLOGY OF RESPIRATORY SYNCYTIAL VIRUS INFECTIONS IN NSW CHILDREN, 1992 1997 Susan Lister * and Peter McIntyre National Centre for Immunisation Research and Surveillance of Vaccine Preventable
THE EPIDEMIOLOGY OF RESPIRATORY SYNCYTIAL VIRUS INFECTIONS IN NSW CHILDREN, 1992 1997 Susan Lister * and Peter McIntyre National Centre for Immunisation Research and Surveillance of Vaccine Preventable
INFLUENZA VIRUS. INFLUENZA VIRUS CDC WEBSITE
 INFLUENZA VIRUS INFLUENZA VIRUS CDC WEBSITE http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm 1 THE IMPACT OF INFLUENZA Deaths: PANDEMICS 1918-19 S p a n is h flu 5 0 0,0 0 0 U S 2 0,0 0 0,0 0 0 w o rld
INFLUENZA VIRUS INFLUENZA VIRUS CDC WEBSITE http://www.cdc.gov/ncidod/diseases/flu/fluinfo.htm 1 THE IMPACT OF INFLUENZA Deaths: PANDEMICS 1918-19 S p a n is h flu 5 0 0,0 0 0 U S 2 0,0 0 0,0 0 0 w o rld
Weekly Influenza Surveillance Report. Week 11
 Weekly Influenza Surveillance Report Week 11 Report produced: 22/03/2001 Influenza activity in Ireland For the week ending the 18/03/01, week 11, influenza activity has increased. Sentinel general practices
Weekly Influenza Surveillance Report Week 11 Report produced: 22/03/2001 Influenza activity in Ireland For the week ending the 18/03/01, week 11, influenza activity has increased. Sentinel general practices
NVRL. Summary Report of Influenza Season 2003/2004. Report produced: 28 th September 2004
 Summary Report of Influenza Season 23/24 NVRL Report produced: 28 th September 24 This report is produced in collaboration with the Departments of Public Health Summary Report of Influenza Season 23/24
Summary Report of Influenza Season 23/24 NVRL Report produced: 28 th September 24 This report is produced in collaboration with the Departments of Public Health Summary Report of Influenza Season 23/24
STARK COUNTY INFLUENZA SNAPSHOT, WEEK 10 Week ending March 10, 2012, with updates through 03/19/2012.
 STARK COUNTY INFLUENZA SNAPSHOT, WEEK 10 Week ending March 10, 2012, with updates through 03/19/2012. All data are preliminary and may change as additional information is received. NOTE: Compilation of
STARK COUNTY INFLUENZA SNAPSHOT, WEEK 10 Week ending March 10, 2012, with updates through 03/19/2012. All data are preliminary and may change as additional information is received. NOTE: Compilation of
Duration of antibiotic treatment and symptom recovery in community-acquired pneumonia El Moussaoui, R.
 UvA-DARE (Digital Academic Repository) Duration of antibiotic treatment and symptom recovery in community-acquired pneumonia El Moussaoui, R. Link to publication Citation for published version (APA): El
UvA-DARE (Digital Academic Repository) Duration of antibiotic treatment and symptom recovery in community-acquired pneumonia El Moussaoui, R. Link to publication Citation for published version (APA): El
Surveillance of Influenza in Northern Ireland
 Surveillance of Influenza in Northern Ireland 2016 2017 Contents Summary... 1 Introduction... 3 Enhanced influenza surveillance systems... 3 In-hours Sentinel GP Practice surveillance... 3 GP Out-of-Hours
Surveillance of Influenza in Northern Ireland 2016 2017 Contents Summary... 1 Introduction... 3 Enhanced influenza surveillance systems... 3 In-hours Sentinel GP Practice surveillance... 3 GP Out-of-Hours
Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic. Webinar Agenda
 in Older Adults: A Hidden Annual Epidemic. Webinar Agenda") Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic Wednesday, November 2, 2016 12:00 PM ET Webinar Agenda Agenda Welcome and Introductions William Schaffner, MD, NFID Medical Director
Respiratory Syncytial Virus (RSV) in Older Adults: A Hidden Annual Epidemic Wednesday, November 2, 2016 12:00 PM ET Webinar Agenda Agenda Welcome and Introductions William Schaffner, MD, NFID Medical Director
University of Bristol - Explore Bristol Research. Peer reviewed version. Link to published version (if available): /
: /") Katz, B., Collin, S., Murphy, G., Moss-Morris, R., Bruun Wyller, V., Wensaas, K-A.,... Lloyd, A. (2018). The international collaborative on fatigue following infection (COFFI). Fatigue: Biomedicine, Health
Katz, B., Collin, S., Murphy, G., Moss-Morris, R., Bruun Wyller, V., Wensaas, K-A.,... Lloyd, A. (2018). The international collaborative on fatigue following infection (COFFI). Fatigue: Biomedicine, Health
Laboratory Evidence of Human Viral and Selected Non-viral Infections in Canada
 Canada Communicable Disease Report ISSN 1188-4169 Date of publication: October 1998 Volume 24S7 Supplement Laboratory Evidence of Human Viral and Selected Non-viral Infections in Canada 1989 to 1996 Our
Canada Communicable Disease Report ISSN 1188-4169 Date of publication: October 1998 Volume 24S7 Supplement Laboratory Evidence of Human Viral and Selected Non-viral Infections in Canada 1989 to 1996 Our
Guideline for the Surveillance of Pandemic Influenza (From Phase 4 Onwards)
") Guideline for the Surveillance of Pandemic Influenza (From Phase 4 Onwards) March 26, 2007 Pandemic Influenza Experts Advisory Committee 31 Guidelines for the Surveillance of Pandemic Influenza From Phase
Guideline for the Surveillance of Pandemic Influenza (From Phase 4 Onwards) March 26, 2007 Pandemic Influenza Experts Advisory Committee 31 Guidelines for the Surveillance of Pandemic Influenza From Phase
Late diagnosis of influenza in adult patients during a seasonal outbreak
 ORIGINAL ARTICLE Korean J Intern Med 2018;33:391-396 Late diagnosis of influenza in adult patients during a seasonal outbreak Seong-Ho Choi 1, Jin-Won Chung 1, Tark Kim 2, Ki-Ho Park 3, Mi Suk Lee 3, and
ORIGINAL ARTICLE Korean J Intern Med 2018;33:391-396 Late diagnosis of influenza in adult patients during a seasonal outbreak Seong-Ho Choi 1, Jin-Won Chung 1, Tark Kim 2, Ki-Ho Park 3, Mi Suk Lee 3, and
RESPIRATORY DISEASES AND ITS TREATMENT THROUGH AYURVEDIC AND HEBAL MEDICINES
 RESPIRATORY DISEASES AND ITS TREATMENT THROUGH AYURVEDIC AND HEBAL MEDICINES page 1 / 5 page 2 / 5 respiratory diseases and its pdf The Global Alliance against Chronic Respiratory Diseases (GARD) contributes
RESPIRATORY DISEASES AND ITS TREATMENT THROUGH AYURVEDIC AND HEBAL MEDICINES page 1 / 5 page 2 / 5 respiratory diseases and its pdf The Global Alliance against Chronic Respiratory Diseases (GARD) contributes
Information collected from influenza surveillance allows public health authorities to:
 OVERVIEW OF INFLUENZA SURVEILLANCE IN NEW JERSEY Influenza Surveillance Overview Surveillance for influenza requires monitoring for both influenza viruses and disease activity at the local, state, national,
OVERVIEW OF INFLUENZA SURVEILLANCE IN NEW JERSEY Influenza Surveillance Overview Surveillance for influenza requires monitoring for both influenza viruses and disease activity at the local, state, national,
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
New viruses causing respiratory tract infections. Eric C.J. Claas
 New viruses causing respiratory tract infections Eric C.J. Claas (Re) emerging infectious diseases: what is new? Morens et al. Nature 2004 Virus discovery New molecular methods result in frequent detection
New viruses causing respiratory tract infections Eric C.J. Claas (Re) emerging infectious diseases: what is new? Morens et al. Nature 2004 Virus discovery New molecular methods result in frequent detection
Evaluation of the Oxoid Xpect Legionella test kit for Detection of Legionella
 JCM Accepts, published online ahead of print on 6 May 2009 J. Clin. Microbiol. doi:10.1128/jcm.00397-09 Copyright 2009, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
JCM Accepts, published online ahead of print on 6 May 2009 J. Clin. Microbiol. doi:10.1128/jcm.00397-09 Copyright 2009, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights
Whooping cough Topic owner: Dr. H. de Melker, (RIVM) ( )
 ( )") Whooping cough Topic owner: Dr. H. de Melker, (RIVM) (1998-2013) Introduction Whooping cough is an acute, very infectious disease of the upper airways that is caused by the bacteria Bordetella pertussis
Whooping cough Topic owner: Dr. H. de Melker, (RIVM) (1998-2013) Introduction Whooping cough is an acute, very infectious disease of the upper airways that is caused by the bacteria Bordetella pertussis
Influenza Weekly Surveillance Bulletin
 Influenza Weekly Surveillance Bulletin Northern Ireland, Week 15 (9 th April 15 th April 2018) Summary In week 15, the surveillance data indicates influenza activity continues to decrease. Rates remain
Influenza Weekly Surveillance Bulletin Northern Ireland, Week 15 (9 th April 15 th April 2018) Summary In week 15, the surveillance data indicates influenza activity continues to decrease. Rates remain
Linking Environment and Health Data
 Linking Environment and Health Data Experiences from the Netherlands Oscar Breugelmans Brigit Staatsen Contents 1. Developments in Environmental Public Health policy and research 2. Examples of recent
Linking Environment and Health Data Experiences from the Netherlands Oscar Breugelmans Brigit Staatsen Contents 1. Developments in Environmental Public Health policy and research 2. Examples of recent
Ageing and the burden of diseases in the elderly. Karl-Heinz Krause Geneva University Hospitals and Medical Faculty
 Ageing and the burden of diseases in the elderly Karl-Heinz Krause Geneva University Hospitals and Medical Faculty - Norwegian Surveillance System for Communicable Diseases (MSIS) - Clinicians and laboratories
Ageing and the burden of diseases in the elderly Karl-Heinz Krause Geneva University Hospitals and Medical Faculty - Norwegian Surveillance System for Communicable Diseases (MSIS) - Clinicians and laboratories
Influenza-Associated Pediatric Mortality rev Jan 2018
 rev Jan 2018 Infectious Agent Influenza A, B or C virus BASIC EPIDEMIOLOGY Transmission Transmission occurs via droplet spread. After a person infected with influenza coughs, sneezes, or talks, influenza
rev Jan 2018 Infectious Agent Influenza A, B or C virus BASIC EPIDEMIOLOGY Transmission Transmission occurs via droplet spread. After a person infected with influenza coughs, sneezes, or talks, influenza
Reporting of Severe and Fatal Pediatric Influenza New Jersey Department of Health Influenza Season
 Reporting of Severe and Fatal Pediatric Influenza New Jersey Department of Health 2016-2017 Influenza Season Patients meeting the below criteria should be entered into the Communicable Disease Reporting
Reporting of Severe and Fatal Pediatric Influenza New Jersey Department of Health 2016-2017 Influenza Season Patients meeting the below criteria should be entered into the Communicable Disease Reporting
Respiratory Viruses Policy
 Respiratory Viruses Policy Page 1 of 8 Document Control Sheet Name of document: Version: 3 Status: Owner: File location / Filename: Respiratory viruses policy Date of this version: February 2013 Infection
Respiratory Viruses Policy Page 1 of 8 Document Control Sheet Name of document: Version: 3 Status: Owner: File location / Filename: Respiratory viruses policy Date of this version: February 2013 Infection
Reference Guide for Group Education
 A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
A p l a n o f a c t i o n f o r l i f e Reference Guide for Group Education Session 5 Plan of Action: Part I Overview of the Plan of Action and Management of Respiratory Infections Plan of Action: Objectives
Surveillance of influenza in Northern Ireland
 Surveillance of influenza in Northern Ireland 2012 2013 Contents Summary... 1 Introduction... 2 Sources of data... 2 Sentinel GP surveillance... 2 Out-of-Hours Centres... 2 Virological surveillance...
Surveillance of influenza in Northern Ireland 2012 2013 Contents Summary... 1 Introduction... 2 Sources of data... 2 Sentinel GP surveillance... 2 Out-of-Hours Centres... 2 Virological surveillance...
Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance
 2009 virus: updated interim WHO guidance on global surveillance") Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance 10 July 2009 Background This document updates the interim WHO guidance on global surveillance of pandemic
Human infection with pandemic (H1N1) 2009 virus: updated interim WHO guidance on global surveillance 10 July 2009 Background This document updates the interim WHO guidance on global surveillance of pandemic
Austin Public Health Epidemiology and Disease Surveillance Unit. Travis County Influenza Surveillance
 Travis County Influenza Surveillance Summary Season 2016-2017 (Data through the week ending March 18, 2017). Travis County influenza and influenza-like illness (ILI) activity: Since March 18 th, influenza
Travis County Influenza Surveillance Summary Season 2016-2017 (Data through the week ending March 18, 2017). Travis County influenza and influenza-like illness (ILI) activity: Since March 18 th, influenza
SUMMARY OF THE DISCUSSION AND RECOMMENDATIONS OF THE SARS LABORATORY WORKSHOP, 22 OCTOBER 2003
 SUMMARY OF THE DISCUSSION AND RECOMMENDATIONS OF THE SARS LABORATORY WORKSHOP, 22 OCTOBER 2003 An informal SARS Laboratory Workshop was held at WHO, Geneva, on Wednesday, 22 October 2003, to discuss aspects
SUMMARY OF THE DISCUSSION AND RECOMMENDATIONS OF THE SARS LABORATORY WORKSHOP, 22 OCTOBER 2003 An informal SARS Laboratory Workshop was held at WHO, Geneva, on Wednesday, 22 October 2003, to discuss aspects
The causes and diagnosis of influenza-like illness
 Cough THEME The causes and diagnosis of influenza-like illness BACKGROUND Influenza and other respiratory viruses circulate between spring and autumn in temperate climates and all year in tropical climates.
Cough THEME The causes and diagnosis of influenza-like illness BACKGROUND Influenza and other respiratory viruses circulate between spring and autumn in temperate climates and all year in tropical climates.
TABLE OF CONTENTS. Peterborough County-City Health Unit Pandemic Influenza Plan Section 1: Introduction
 TABLE OF CONTENTS 1. Introduction...1-2 1.1 Background...1-2 1.2 Why Does Peterborough County and City Need a Plan for Influenza Pandemic?...1-2 1.3 About Influenza...1-3 1.4 When Does Influenza Become
TABLE OF CONTENTS 1. Introduction...1-2 1.1 Background...1-2 1.2 Why Does Peterborough County and City Need a Plan for Influenza Pandemic?...1-2 1.3 About Influenza...1-3 1.4 When Does Influenza Become
Estimating RSV Disease Burden in the United States
 Estimating RSV Disease Burden in the United States Brian Rha, MD, MSPH Medical Epidemiologist, Division of Viral Diseases Centers for Disease Control and Prevention Severe Acute Respiratory Infection Surveillance
Estimating RSV Disease Burden in the United States Brian Rha, MD, MSPH Medical Epidemiologist, Division of Viral Diseases Centers for Disease Control and Prevention Severe Acute Respiratory Infection Surveillance
The Importance of Appropriate Treatment of Chronic Bronchitis
 ...CLINICIAN INTERVIEW... The Importance of Appropriate Treatment of Chronic Bronchitis An interview with Antonio Anzueto, MD, Associate Professor of Medicine, University of Texas Health Science Center,
...CLINICIAN INTERVIEW... The Importance of Appropriate Treatment of Chronic Bronchitis An interview with Antonio Anzueto, MD, Associate Professor of Medicine, University of Texas Health Science Center,
Surveillance for encephalitis in Bangladesh: preliminary results
 Surveillance for encephalitis in Bangladesh: preliminary results In Asia, the epidemiology and aetiology of encephalitis remain largely unknown, particularly in Bangladesh. A prospective, hospital-based
Surveillance for encephalitis in Bangladesh: preliminary results In Asia, the epidemiology and aetiology of encephalitis remain largely unknown, particularly in Bangladesh. A prospective, hospital-based
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/89560
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/89560
Defining the patient population: one of the problems for palliative care research
 Postprint 1.0 Version Journal website http://pmj.sagepub.com/cgi/content/abstract/20/2/63 Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/16613401 DOI 10.1191/0269216306pm1112oa Defining the patient population:
Postprint 1.0 Version Journal website http://pmj.sagepub.com/cgi/content/abstract/20/2/63 Pubmed link http://www.ncbi.nlm.nih.gov/pubmed/16613401 DOI 10.1191/0269216306pm1112oa Defining the patient population:
3. Rapidly recognize influenza seasons in which the impact of influenza appears to be unusually severe among children.
 07-ID-14 Committee: Title: Infectious Disease Influenza-Associated Pediatric Mortality Statement of the Problem: In 2004, CSTE adopted influenza-associated pediatric mortality reporting with a provision
07-ID-14 Committee: Title: Infectious Disease Influenza-Associated Pediatric Mortality Statement of the Problem: In 2004, CSTE adopted influenza-associated pediatric mortality reporting with a provision
Interim WHO guidance for the surveillance of human infection with swine influenza A(H1N1) virus
 virus") Interim WHO guidance for the surveillance of human infection with swine influenza A(H1N1) virus 29 April 2009 Introduction The audiences for this guidance document are the National Focal Points for the
Interim WHO guidance for the surveillance of human infection with swine influenza A(H1N1) virus 29 April 2009 Introduction The audiences for this guidance document are the National Focal Points for the
Ottawa Public Health Respiratory and Enteric Surveillance Report March 23, 2018 (Week 12)
") Ottawa Public Health Respiratory and Enteric Surveillance Report March 23, 2018 (Week 12) This report summarizes information on influenza in the community and acute care in Ottawa and the rest of the province.
Ottawa Public Health Respiratory and Enteric Surveillance Report March 23, 2018 (Week 12) This report summarizes information on influenza in the community and acute care in Ottawa and the rest of the province.
IT S A LIFESAVER EVERY YEAR FLU CAUSES SEVERE ILLNESS AND DEATH. GET YOUR FLU VACCINE NOW. IF YOU ARE: worker
 FLU VACCINE Information FOR Health care workers EVERY YEAR FLU CAUSES SEVERE ILLNESS AND DEATH. IF YOU ARE: A health care worker Over 65 Have a longterm illness Pregnant GET YOUR FLU VACCINE NOW. IT S
FLU VACCINE Information FOR Health care workers EVERY YEAR FLU CAUSES SEVERE ILLNESS AND DEATH. IF YOU ARE: A health care worker Over 65 Have a longterm illness Pregnant GET YOUR FLU VACCINE NOW. IT S
Epidemiology and Etiology of Community-Acquired Pneumonia 761 Lionel A. Mandell
 LOWER RESPIRATORY TRACT INFECTIONS Preface Thomas M. File, Jr xiii Community-Acquired Pneumonia: Pathophysiology and Host Factors with Focus on Possible New Approaches to Management of Lower Respiratory
LOWER RESPIRATORY TRACT INFECTIONS Preface Thomas M. File, Jr xiii Community-Acquired Pneumonia: Pathophysiology and Host Factors with Focus on Possible New Approaches to Management of Lower Respiratory
Texas Influenza Summary Report, Season (September 28, 2008 April 11, 2009)
") Texas Influenza Summary Report, 2008 2009 Season (September 28, 2008 April 11, 2009) Background Influenza and influenza-like illnesses (ILI) were last reportable by law in any county in Texas in 1993 (1).
Texas Influenza Summary Report, 2008 2009 Season (September 28, 2008 April 11, 2009) Background Influenza and influenza-like illnesses (ILI) were last reportable by law in any county in Texas in 1993 (1).
Influenza Weekly Surveillance Bulletin
 Influenza ly Surveillance Bulletin Northern Ireland, (11-17 December ) Summary All indicators of influenza virus activity have increased. GP consultation rates for combined flu/ FLI increased from 28.1/,
Influenza ly Surveillance Bulletin Northern Ireland, (11-17 December ) Summary All indicators of influenza virus activity have increased. GP consultation rates for combined flu/ FLI increased from 28.1/,
Suggestions to prevent / control Respiratory Disease Complex in poultry
 Suggestions to prevent / control Respiratory Disease Complex in poultry Dr. J. L. Vegad Adviser Phoenix Group 201/15, Gorakhpur, Jabalpur - 482001 Introduction Today, respiratory disease complex has emerged
Suggestions to prevent / control Respiratory Disease Complex in poultry Dr. J. L. Vegad Adviser Phoenix Group 201/15, Gorakhpur, Jabalpur - 482001 Introduction Today, respiratory disease complex has emerged
Minors Access to Tobacco
 Minors Access to Tobacco Background The purpose of this health indicator report is to provide information about the general awareness of legal age limits on retailer tobacco sales, and the opinion and
Minors Access to Tobacco Background The purpose of this health indicator report is to provide information about the general awareness of legal age limits on retailer tobacco sales, and the opinion and
Influenza Division, National Center for Immunization and Respiratory Diseases (NCIRD/CDC), at
, at") Overview Information Issuing Organization Council of State and Territorial Epidemiologists (CSTE) at www.cste.org/ Participating Organizations Centers for Disease Control and Prevention (CDC), at http://www.cdc.gov/
Overview Information Issuing Organization Council of State and Territorial Epidemiologists (CSTE) at www.cste.org/ Participating Organizations Centers for Disease Control and Prevention (CDC), at http://www.cdc.gov/
IgM. (Polioviruses) 71 (EV71) B (Coxsackievirus B) (Virus isolation/ifa, VI-IFA) 7~14 [1,2] (Centers for Disease Control and Prevention, CDC) 1.
![IgM. (Polioviruses) 71 (EV71) B (Coxsackievirus B) (Virus isolation/ifa, VI-IFA) 7~14 [1,2] (Centers for Disease Control and Prevention, CDC) 1.](/thumbs/93/111050187.jpg "IgM. (Polioviruses) 71 (EV71) B (Coxsackievirus B) (Virus isolation/ifa, VI-IFA) 7~14 [1,2] (Centers for Disease Control and Prevention, CDC) 1.") 267 DOI: 10.6526/ICJ.2017.603 (Polioviruses) 71 (EV71) B (Coxsackievirus B) [1,2] 1998 EV71 (Centers for Disease Control and Prevention, CDC) 1. (Hand, foot and mouth disease, HFMD) (herpangina) [3,4]
267 DOI: 10.6526/ICJ.2017.603 (Polioviruses) 71 (EV71) B (Coxsackievirus B) [1,2] 1998 EV71 (Centers for Disease Control and Prevention, CDC) 1. (Hand, foot and mouth disease, HFMD) (herpangina) [3,4]
Breaking the chain of transmission: Immunisation and outbreak investigation Whelan, Jane
 UvA-DARE (Digital Academic Repository) Breaking the chain of transmission: Immunisation and outbreak investigation Whelan, Jane Link to publication Citation for published version (APA): Whelan, E. J. (2013).
UvA-DARE (Digital Academic Repository) Breaking the chain of transmission: Immunisation and outbreak investigation Whelan, Jane Link to publication Citation for published version (APA): Whelan, E. J. (2013).
Influenza-Associated Hospitalization and Death Surveillance: Dallas County
 Influenza-Associated Hospitalization and Death Surveillance: Dallas County 2009 2015 Sonya Hughes, MPH, CPH Epidemiology Surveillance Coordinator July 22, 2015 Dallas County Health and Human Services Overview:
Influenza-Associated Hospitalization and Death Surveillance: Dallas County 2009 2015 Sonya Hughes, MPH, CPH Epidemiology Surveillance Coordinator July 22, 2015 Dallas County Health and Human Services Overview:
Enhanced service specification Childhood seasonal influenza vaccination programme NHS England gateway reference: 01641
 Enhanced service specification Childhood seasonal influenza vaccination programme NHS England gateway reference: 01641 Introduction 1. All GMS practices are expected to provide essential and those additional
Enhanced service specification Childhood seasonal influenza vaccination programme NHS England gateway reference: 01641 Introduction 1. All GMS practices are expected to provide essential and those additional
Appendix B: Provincial Case Definitions for Reportable Diseases
 Infectious Diseases Protocol Appendix B: Provincial Case Definitions for Reportable Diseases Disease: Influenza Revised December 2014 Influenza 1.0 Provincial Reporting Confirmed cases of disease 2.0 Type
Infectious Diseases Protocol Appendix B: Provincial Case Definitions for Reportable Diseases Disease: Influenza Revised December 2014 Influenza 1.0 Provincial Reporting Confirmed cases of disease 2.0 Type
2,434 cases of Q fever From the French National reference center Dr Cléa Melenotte Marseille IHU Méditerranée Infection
 2,434 cases of Q fever From the French National reference center 1991-2016 Dr Cléa Melenotte Marseille IHU Méditerranée Infection Q fever Coxiella burnetii, gram negative intracellular bacteria Worldwide
2,434 cases of Q fever From the French National reference center 1991-2016 Dr Cléa Melenotte Marseille IHU Méditerranée Infection Q fever Coxiella burnetii, gram negative intracellular bacteria Worldwide
HPS Monthly National Seasonal Respiratory Report
 HPS Monthly National Seasonal Respiratory Report Week ending 18 March 218 week 11 1 Overall assessment In week 11, the overall assessment remains green (below baseline activity). GP consultation rate for
HPS Monthly National Seasonal Respiratory Report Week ending 18 March 218 week 11 1 Overall assessment In week 11, the overall assessment remains green (below baseline activity). GP consultation rate for
Downloaded from:
 Granerod, J; Davison, KL; Ramsay, ME; Crowcroft, NS (26) Investigating the aetiology of and evaluating the impact of the Men C vaccination programme on probable meningococcal disease in England and Wales.
Granerod, J; Davison, KL; Ramsay, ME; Crowcroft, NS (26) Investigating the aetiology of and evaluating the impact of the Men C vaccination programme on probable meningococcal disease in England and Wales.
HIV AND LUNG HEALTH. Stephen Aston Infectious Diseases SpR Royal Liverpool University Hospital
 HIV AND LUNG HEALTH Stephen Aston Infectious Diseases SpR Royal Liverpool University Hospital Introduction HIV infection exerts multiple effects on pulmonary immune responses: Generalised state of immune
HIV AND LUNG HEALTH Stephen Aston Infectious Diseases SpR Royal Liverpool University Hospital Introduction HIV infection exerts multiple effects on pulmonary immune responses: Generalised state of immune
Prof Marion Eckert Rosemary Bryant AO Research Centre
 Willingness of cancer survivors to complete patient reported outcomes (PRO) surveys: a pilot study at Flinders Centre for Innovation in Cancer (FCIC), South Australia Prof Marion Eckert Rosemary Bryant
Willingness of cancer survivors to complete patient reported outcomes (PRO) surveys: a pilot study at Flinders Centre for Innovation in Cancer (FCIC), South Australia Prof Marion Eckert Rosemary Bryant
How you can help support the Beat Flu campaign
 How you can help support the Beat Flu campaign Toolkit www.beatflu.org f T Beat Flu 1 How can you help Beat Flu? Template news story You may wish to use the following news story as a template, which can
How you can help support the Beat Flu campaign Toolkit www.beatflu.org f T Beat Flu 1 How can you help Beat Flu? Template news story You may wish to use the following news story as a template, which can
Influenza Activity in Indiana
 Objectives of Influenza Surveillance Influenza Activity in Indiana 2014-2015 Reema Patel, MPH Respiratory Epidemiologist Epidemiology Resource Center Indiana State Department of Health Monitor influenza-like
Objectives of Influenza Surveillance Influenza Activity in Indiana 2014-2015 Reema Patel, MPH Respiratory Epidemiologist Epidemiology Resource Center Indiana State Department of Health Monitor influenza-like
THE PHARMA INNOVATION - JOURNAL Acute exacerbation of chronic obstructive pulmonary disease, caused by viruses: the need of combined antiinfective
 Received: 19-11-2013 Accepted: 28-12-2013 ISSN: 2277-7695 CODEN Code: PIHNBQ ZDB-Number: 2663038-2 IC Journal No: 7725 Vol. 2 No. 11. 2014 Online Available at www.thepharmajournal.com THE PHARMA INNOVATION
Received: 19-11-2013 Accepted: 28-12-2013 ISSN: 2277-7695 CODEN Code: PIHNBQ ZDB-Number: 2663038-2 IC Journal No: 7725 Vol. 2 No. 11. 2014 Online Available at www.thepharmajournal.com THE PHARMA INNOVATION
COHORT STUDY OF HIV POSITIVE AND HIV NEGATIVE TUBERCULOSIS in PENANG HOSPITAL: COMPARISON OF CLINICAL MANIFESTATIONS
 COHORT STUDY OF HIV POSITIVE AND HIV NEGATIVE TUBERCULOSIS in PENANG HOSPITAL: COMPARISON OF CLINICAL MANIFESTATIONS Ong CK 1, Tan WC 2, Leong KN 2, Abdul Razak M 1, Chow TS 2 1 Respiratory Unit, Penang
COHORT STUDY OF HIV POSITIVE AND HIV NEGATIVE TUBERCULOSIS in PENANG HOSPITAL: COMPARISON OF CLINICAL MANIFESTATIONS Ong CK 1, Tan WC 2, Leong KN 2, Abdul Razak M 1, Chow TS 2 1 Respiratory Unit, Penang
University of Groningen. Exercise induced bronchoconstriction in childhood asthma van Leeuwen, Janneke
 University of Groningen Exercise induced bronchoconstriction in childhood asthma van Leeuwen, Janneke IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to
University of Groningen Exercise induced bronchoconstriction in childhood asthma van Leeuwen, Janneke IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to
Western Pacific Regional Office of the World Health Organization.
 Western Pacific Regional Office of the World Health Organization WPRO Influenza Situation Update, 19 November 2013 http://www.wpro.who.int/emerging_diseases/influenza/en/index.html SUMMARY Northern Hemisphere
Western Pacific Regional Office of the World Health Organization WPRO Influenza Situation Update, 19 November 2013 http://www.wpro.who.int/emerging_diseases/influenza/en/index.html SUMMARY Northern Hemisphere
Influenza Weekly Surveillance Report
 Influenza Weekly Surveillance Report A REPORT BY THE HEALTH PROTECTION SURVEILLANCE CENTRE IN COLLABORATION WITH THE IRISH COLLEGE OF GENERAL PRACTITIONERS, THE NATIONAL VIRUS REFERENCE LABORATORY & THE
Influenza Weekly Surveillance Report A REPORT BY THE HEALTH PROTECTION SURVEILLANCE CENTRE IN COLLABORATION WITH THE IRISH COLLEGE OF GENERAL PRACTITIONERS, THE NATIONAL VIRUS REFERENCE LABORATORY & THE
Received 3 August 2005/Returned for modification 13 September 2005/Accepted 13 January 2006
 CLINICAL AND VACCINE IMMUNOLOGY, Mar. 2006, p. 361 364 Vol. 13, No. 3 1556-6811/06/$08.00 0 doi:10.1128/cvi.13.3.361 364.2006 Copyright 2006, American Society for Microbiology. All Rights Reserved. Evaluation
CLINICAL AND VACCINE IMMUNOLOGY, Mar. 2006, p. 361 364 Vol. 13, No. 3 1556-6811/06/$08.00 0 doi:10.1128/cvi.13.3.361 364.2006 Copyright 2006, American Society for Microbiology. All Rights Reserved. Evaluation
Health Board Logo. Post SARS Outbreak Surveillance. Report of possible or probable cases (Form version 1) February 11 th 2004
 February 11 th 2004") Post SARS Outbreak Surveillance Report of possible or probable cases (Form version 1) February 11 th 2004 This form is to be used for persons who fit the surveillance case definition of possible or probable
Post SARS Outbreak Surveillance Report of possible or probable cases (Form version 1) February 11 th 2004 This form is to be used for persons who fit the surveillance case definition of possible or probable
Pediatric influenza-associated deaths in Arizona,
 Pediatric influenza-associated deaths in Arizona, 2004-2012 (Poster is shared here as an 8.5 x11 document for easier viewing. All content is identical, though graphs and tables are formatted differently.)
Pediatric influenza-associated deaths in Arizona, 2004-2012 (Poster is shared here as an 8.5 x11 document for easier viewing. All content is identical, though graphs and tables are formatted differently.)
Design - Multicentre prospective cohort study. Setting UK Community Pharmacies within one CCG area within the UK
 Enabling Patient Health Improvements through COPD (EPIC) Medicines Optimisation within Community Pharmacy: a prospective cohort study Abstract Objectives To improve patients ability to manage their own
Enabling Patient Health Improvements through COPD (EPIC) Medicines Optimisation within Community Pharmacy: a prospective cohort study Abstract Objectives To improve patients ability to manage their own
Surveillance of influenza in Northern Ireland
 Surveillance of influenza in Northern Ireland 2011-2012 Summary: The influenza season started later than normal, clinical indices began to increase marginally in mid-february, much later than previous
Surveillance of influenza in Northern Ireland 2011-2012 Summary: The influenza season started later than normal, clinical indices began to increase marginally in mid-february, much later than previous
Guidance for Influenza in Long-Term Care Facilities
 Guidance for Influenza in Long-Term Care Facilities DSHS Region 2/3 Epidemiology Team January 2018 1. Introduction Every year, the flu affects people around the world, regardless of age. However, residents
Guidance for Influenza in Long-Term Care Facilities DSHS Region 2/3 Epidemiology Team January 2018 1. Introduction Every year, the flu affects people around the world, regardless of age. However, residents
Research in Real Life
 Research in Real Life Study 1: Exploratory study - identifying the benefits of pmdi versus Diskus for delivering fluticasone/salmeterol combination therapy in patients with chronic obstructive pulmonary
Research in Real Life Study 1: Exploratory study - identifying the benefits of pmdi versus Diskus for delivering fluticasone/salmeterol combination therapy in patients with chronic obstructive pulmonary
REPLICATION DATA SET FOR:
 REPLICATION DATA SET FOR: Cohen, S., Janicki-Deverts, D., Turner, R.B., & Doyle, W.J. (in press). Does hugging provide stress-buffering social support? A study of susceptibility to upper respiratory infection
REPLICATION DATA SET FOR: Cohen, S., Janicki-Deverts, D., Turner, R.B., & Doyle, W.J. (in press). Does hugging provide stress-buffering social support? A study of susceptibility to upper respiratory infection