Sensori-neural deafness and the cochlear implant
|
|
|
- Meredith Alexander
- 6 years ago
- Views:
Transcription
1 Rochester Institute of Technology RIT Scholar Works Theses Thesis/Dissertation Collections Sensori-neural deafness and the cochlear implant Margaret Pence Follow this and additional works at: Recommended Citation Pence, Margaret, "Sensori-neural deafness and the cochlear implant" (1997). Thesis. Rochester Institute of Technology. Accessed from This Thesis is brought to you for free and open access by the Thesis/Dissertation Collections at RIT Scholar Works. It has been accepted for inclusion in Theses by an authorized administrator of RIT Scholar Works. For more information, please contact
2 Approvals Chief Advisor: Glen Hintz Date Associate Advisor: Robert Wabnitz Date :i - /] - q'} Associate Advisor: Catherine Clark Date /~J '/ f? I Associate Advisor: Dr. Paul Dutcher Date /LO/77 Chairperson: Tom Lightfoot Date / 2-/;I/? 7 ~ 1 I I, Margaret Pence, hereby grant permission to the Wallace Memorial Library of RIT to reproduce my thesis in whole or in part. Any reproduction will not be for commercial use or profit. Signature Date
3 Rochester Institute of Technology A Thesis submitted to the Faculty of the College of Imaging Arts and Sciences in candidacy for the degree of Master of Fine Arts. Sensori-neural Deafness and the Cochlear Implant by Margaret Pence 9/30/97
4 Introduction The inner ear is part of an intricate network of fluid filled cavities located in the temporal bone of the skull. Within this bony labyrinth is the cochlea which houses the organ of hearing called the organ of Corti. Any number of factors, including disease, trauma and congenital malformations may interrupt the processing of sound through the inner ear. These conditions may lead to partial or complete hearing loss. This type of hearing loss is called sensori-neural deafness. Since the 1950's medical researchers have sought to restore some sense of hearing in profoundly deaf individuals by way of stimulating cochlear hair cells, and or direct stimulation of the auditory/ cochlear nerve. Their work lead to the development of a device called the cochlear implant. Although not recommended for everyone, this implant has been used with at least partial success in over 13,000 people world wide. The first portion of this thesis presents general information concerning the anatomy and physiology of the hearing process, pathologies that cause deafness, types of hearing aids available, and specific information concerning the development and use of the cochlear implant. Surgical procedures describing the process of implantation are also covered. The second portion of the thesis report focuses on the illustrations that were developed as part of my investigations of the structure and function of the inner ear, particularly the organ of Corti and its involvement in the hearing process. Their purpose is to visually communicate complex structures and processes. Over the last few decades concerns have been voiced both in and out of the deaf community over the use of implants, especially in children. My thesis work is not meant to promote or defend the implants but merely to
5 present information to an interested public. Anatomy and Physiology of Hearing The ear itself is a compound organ that serves a dual purpose as a hearing mechanism for the reception of sound and as an organ of balance. Both functions depend on the movement of fluid through a special labyrinth within the skull and the stimulation of special receptor cells within the complex of the inner ear. The ear is composed of three major areas: outer ear, middle ear and inner ear. The organs of hearing and balance lie within the bony labyrinth of the inner ear. The outer ear is composed of the auricle and the external auditory canal. In humans, the auricle, the visible external portion of the ear, is considered to be vestigial. Ifs function, is to direct sound waves into the external auditory canal for better reception within the ear (transmission of sound waves). This function is still important in many mammals but has become inefficient in humans. The external auditory canal is a short narrow chamber (2.5 cm long by 0.6 cm wide) and extends from the auricle to the tympanic membrane or eardrum. The canal is lined with hairs and sebaceous and modified apocrine sweat glands that secrete cerumen, or ear wax. Both the hairs and wax serve to protect the ear from the invasion of foreign bodies. The tympanic membrane, or eardrum, reverberates with sound waves that travel through the external canal and set the ossicles of the middle ear into motion. The middle ear, or tympanic cavity, is a small air filled cavity that lies within the petrous portion of the temporal bone of the skull. It extends from the tympanic membrane to the auditory (eustachian) tube. The auditory tube
6 provides a link to the nasopharynx and is usually closed but opens to allow an equalization in pressure within the middle ear cavity. This is important for the proper conduction of sound through the tympanic membrane. If pressure within the middle ear cavity is not equal to external pressure, the tympanic membrane may bulge in or out and not allow for proper movement against the ossicles. This distortion of the membrane may cause conductive hearing impairment or other problems. The middle ear contains the three smallest bones in the human body, the ossicles; malleus (hammer), incus (anvil) and stapes (stirrup). They are named for their shape. These tiny bones have the important job of transmitting vibrations of the tympanic membrane to the oval window of the inner ear, which set the fluids of the bony labyrinth in motion and thus excite the receptor cells of hearing. The "handle " of the malleus is connected to the tympanic membrane, or eardrum. The base of the stapes is set against the oval window, the incus serves as the connection between the other two bones. The smallest skeletal muscles are also found within the middle ear. The tensor tympani originates from the wall of the auditory tube and inserts on the handle of the malleus. The stapedius muscle originates from the posterior wall of the middle ear cavity and inserts on the stapes. Both muscles serve to help control the movement of the bones against their respective membranes thus protecting the inner ear from very loud noises. The inner ear is a bony maze-like structure that sits deep within the temporal bone and houses the delicate, sensitive receptor cells of hearing and balance (orientation). Within the bony labyrinth sits a membranous labyrinth, a series of fluid filled channels that can be separated into three
7 distinct areas based on unique structure and function; the vestibule, cochlea and semicircular canals. The membranous labyrinth follows the contours of the hollow bony labyrinth. The bony labyrinth is lined with endosteum and filled with perilymph which is similar in composition to cerebral spinal fluid. Thus the membraneous labyrinth is "floating" within ifs chamber. The membranous labyrinth in turn is filled with endolymph which is similar in composition to intracellular fluid. These two fluids are responsible for conducting the sound vibrations that occur in hearing and detecting changes in body position. This paper will concentrate on the movement of sound vibrations through the middle ear to the cochlea that stimulate the firing of the receptor cells of hearing. The vestibule of the inner ear may be divided into two portions, the saccule and utricle. The utricle is continuous with the semicircular canals while the saccule is continuous with the cochlea. Both these portions contain equilibrium receptors that detect and report changes in head position. Anatomy of the Cochlea The cochlea is a spiral, snail like chamber (cochlea comes from the Greek for "snail) and is about the size of half a split pea. It extends from the vestibule and coils for two and a half turns around a bony pillar called the modiolus. The axial length of the cochlea is 5 mm, the spiral canal extends to mm long. The membranous cochlear duct runs through this chamber ending at the cochlear apex. The cochlear duct and the spiral lamina ( a bony extension of the modiolus) divide the hollow cochlea into three chambers: scala vestibuli (superior), scala media (cochlear duct) and scala tympani (inferior). The scala vestibuli and scala tympani are continuous at the apex, a region called the helicotrema and contain perilymph. The scala media or
8 cochlear duct is filled with endolymph and houses the spiral organ of Corti, the receptor organ of hearing. The membraneous labyrinth is supported by the perilymphatic fluids and a network of tiny blood vessels. The construction of the cochlear duct is important in the understanding of how sound waves are converted to nerve impulses. There are a series of membranes that surround and contain the duct. The roof of the duct which separates the scala media from the scala vestibuli is called the vestibular membrane. The floor of the duct is formed by the spiral lamina (from the bony modiolus) and the basilar membrane which supports the organ of Corti. The spiral ligament serves as a base of attachment for the basilar membrane and Reissner's membrane. The flexible nature of the basilar membrane is important in the stimulation of sensory hair cells. The cochlear nerve, a division of the 8tn cranial or vestibulocochlear nerve, runs from the organ of Corti through the modiolus to the auditory center of the brain. The Organ of Corti The organ of Corti sits atop the basilar membrane and is made up of a series of receptor hair cells and their supporting cells. It is named for Corti who first described its architecture in It consists of the following structure: the pillar cells, Deiter's cells, Hansens cells, inner and outer hair cells and internal and external sulcus cells. All but the hair cells are supporting structures. The hair cells are the receptor cells that cause stimulation of the afferent nerve fibers. There are approximately 3,500 inner hair cells and 12-20,000 outer hair cells. The hairs or stereocilia of the receptor cells are enmeshed in a gelatinous structure, the tectorial membrane that extends from the limbus over the organ of Corti and ends in a border net overlying Hansen's cells.
9 Fluid movement within the cochlear duct causes movement along the tectorial membrane which pull or tweaks the stereocilia of the hair cells. (Fig. 1) At the base of the cells sit afferent nerve fibers that connect to the cochlear nerve. Stimulation of the hair cells causes a release of neurotransmitters which in turn initiate action potential of the nerve fibers and are eventually transmitted to the auditory center of the brain where they are translated into "sounds". The location of the hair cells along the cochlear duct correlates to the type of sound that stimulates them. Cells near the oval window are activated by high-pitched sounds, those near the cochlear apex are activated by the lowest frequencies. Tectorial membrane Stereocilia of hair cells directional movement of stereocila Figure 1. Movement of Basilar Membrane Note the change in direction of stereocilia as the basilar membrane flexes
10 An examination of the close view of up the cochlea shows the different types of cells and orientation to each other. The inner hair cells, located on the modiolar side of the cochlear duct, are flask shaped and contain synaptic structures at their base. They are surrounded by internal pillar cells and border cells. Outer hair cells are located across the tunnel of Corti and run in 2-3 rows. These cells are cylindrical and contain synaptic structures that connect to both afferent and efferent nerve fibers. The outer hair cells have no internal support and maintain their shape by supporting cells. They sit upon Deiter's cells that form a shallow cup. The apical surface of the cell is held in place a reticular membrane by that also anchors the stereocilia. (These cells may be influenced by the central nervous system.) The stereocilia are located on the apical surface of both hair cells and are arranged in rows with the fibers graded at different heights. The rows on inner hair cells are straight, those on outer hair cells form a V or W shape. The hairs are anchored in a dense cuticular plate (reticular membrane) at the apical surface of the cells. These stereocilia are rigid, composed of actin filaments bonded together in a 'paracrystalline array'. There are also sites along the stereocilia fibers that allow them to bond to their neighbor producing a specific spatial arrangement to the fibers. The different bonds between the hairs also affect their movement. The movement of stereocilia against each other and the direction of movement are thought to play a part in opening ion channels leading to changes in membrane potential and thus firing of the cells along the nerve fibers.1 The generally accepted model of hair cell response holds that deflection of the basilar membrane causes deflection of the bundle of stereocilia of each hair cell. The direction of deflection - towards or away from the longest hairs - determines the depolarization or hyperpolarization
11 of the cell and modulates the of activity afferent fibers that synapse at the base of the cells. The majority of nerve fibers make their synaptic contacts with the inner hair cells. It is therefore assumed that it is the job of the inner hair cells to detect movement of the basilar membrane and to transmit that information to the central nervous system.2 The analysis of outer hair cell activity has been more difficult than inner hair cells. Outer hair cells out number inner hair cells roughly 3 to 1. It has also been shown that damage to the outer hair cells affects the mechanical vibrations within the cochlea (efferent nerve fibers run to the cochlea from the Central Nervous System). One hypothesis suggests that the outer hair cells may be able to increase sharpness of mechanical of tuning the basilar membrane. Damaged hair cells maybe unable to control oscillation of the membrane.3 It is the inner hair cells that seem to respond most to sound, 95 percent of afferent nerve fibers (fibers that lead to the brain) innervate the inner hair cells. These nerve fibers respond to sound - specifically to the frequency of sound. The frequency is related to the stimulus threshold of the hair cells and thus the auditory nerve fibers. As sound waves, or mechanical waves pass along the length of the cochlea, different cells are stimulated depending upon the frequency of the waves. This is known as 'place coding of frequency'. Studies that measure the response of different auditory nerve fibers to electrical response have been important in the development of the cochlear implant. Properties of Sound Sound depends on a medium through which to travel - namely air. It is a pressure disturbance originating from a vibrating object. Movement 10
12 compresses air molecules which in turn bump other air molecules and propagate a wave of movement - a new area of compression. These series of compressions are collectively called sound waves. Over time and distance the outward moving molecules give up kinetic energy and the sound eventually dies. Sound can be depicted graphically by use of S-curves which can also describe two properties of sound - frequency and amplitude. (Fig. 2) Wavelength - Crest area ofcompression D. Trough - area of rarefaction Time a. Greater Frequency (more wavelengths over time) Time Figure 2. Frequency and Amplitude The crests of the curves represent areas of compression, the troughs represent areas of rarefaction or low pressure. The distance between two crests is referred to as the wavelength and is constant for a particular tone. Frequency li
13 is defined as the number of waves that pass through a given point in a given time. The shorter the wavelength, the higher the frequency, and vice versa. In humans, we perceive different frequencies as differences in pitch. The higher the frequency, the higher the pitch. The human ear can hear from 20 to 20,000 Hz (or cycles) but is most sensitive to those between Hz. Most sounds are mixtures of several frequencies which lend to their richness, a characteristic called quality. The intensity of sound is dependent on the energy and is related to differences between areas of compression and decompression, or as represented by the sine wave, to the amplitude or height of the sound wave. Sound intensity or loudness is measured in logarithmic units called decibels. The decibel scale as represented on an audiometer begins at zero or barely audible sound. Every fold (logarithmic) increase in sound intensity 10 db increase represents a ten or energy. This correlates to only a twofold increase in loudness. The normal range of hearing for a healthy adult ear is from 0 to over 120 db. Severe and profound hearing loss may occur with overexposure to sound intensities over 90 db. Sound Transmission and The Hearing Pathway Hearing occurs when sound waves transmitted to the inner ear, via air, bone and fluid, reach and stimulate the receptor cells within the organ of Corti. This occurs through a process of transference within the middle ear that amplifies the wave energy. Sound waves are funneled into the ear through the pinna (outer ear) and travel to the middle ear where vibrations against the tympanic membrane set it in motion, vibrating at the same frequency. The motion of the tympanic membrane is transferred, to the oval window of the inner ear, via the ossicles which act much like a hydraulic press. They increase the 12
14 pressure on the oval window which then sets the fluids of the inner ear in motion. The tensor tympani muscle can alter the tension of the tympanic membrane and control the level of vibrations. The stapedius muscle can dampen vibrations, if needed, by pulling the stapes away from the oval window. The ossicles provide a very efficient means of translating sound waves from the air to fluid vibrations within the inner ear. The area of the tympanic membrane is times larger than that of the oval window and thus results in pressure on the smaller window 22 times that of pressure on the tympanic membrane. Because the cochlear fluid is highly resistant to motion, this increase in pressure is necessary to overcome any impedance to movement. Normally only 0.1 percent of sound energy is transferred to fluid, the rest is reflected back at the air-fluid interface. It is the job of the middle ear components to reduce that reflection and increase the transference of energy to the fluids of the inner ear.4 Once set in motion, the cochlear fluid or perilymph within the inner ear swings the basilar membrane up and down causing the cochlear duct to oscillate. Sound waves of different frequencies travel along the cochlea from the oval window to the apex or helicotrema back to the round window. Low frequencies travel along the length of the cochlear duct from the oval to the round window, high frequencies (and therefore shorter wavelengths) fail to travel the entire distance. When pressure waves hit the basilar membrane, they set the entire membrane into motion. Differences in the fibers within the membrane determine how great the effect will be. Fibers near the oval window or base of the cochlea are short and rigid and vibrate in response to high frequencies. As you approach the cochlear apex, the fibers grow long and flexible and 13
15 resonate in response to low frequencies. Thus before ever reaching the receptor hair cells, sounds are mechanically processed based on their frequency and wavelength. The organ of Corti sits atop the basilar membrane within the cochlear duct. It is made up of rows of cochlear hair cells and their supporting cells. Afferent nerve fibers of the cochlear nerve sit at the base of these hair cells. Up and down vibrations of the basilar membrane cause a "tweaking" of the stereocilia of the hair cells that are enmeshed in the overlying tectorial membrane. This "tweaking" stimulates the opening of ion channels in the hair cell membranes which leads to the generation of receptor potentials. Neurotransmitters released by the hair cells stimulate the cochlear nerve fibers at their base initiating action potentials that are sent along the afferent auditory nerves to the brain.5 The afferent nerve fibers originating from the cochlea come together to make up the auditory or vestibulocochlear nerve. The cell bodies of these neurons are found in the spiral ganglion at the center of the cochlea. The auditory nerve travels to the cochlear nuclei located in the pons. Secondary nerve fibers travel to the opposite side of the pons and may project to the superior olivary nucleus or to the inferior colliculus of the midbrain. At the level of the inferior colliculus, impulses from both sides provide information as to the location of sound origination. From the inferior colliculus the nerve fibers travel to the medial geniculate nucleus of the thalamus where all fibers synapse. At this level there is crude discrimination of tone and direction of sound. From the thalamus, impulses travel to the auditory cortex in the superior temporal gyrus and insula where information is further refined and translated (fine tuning occurs). It is at this highest level 14
16 where loudness and a precise discrimination of pitch occurs. There are a progressively larger number of neurons involved from the cochlea to the auditory cortex. Efferent stimuli travel along the same route. Pathologies that cause deafness/types of Deafness Any number of factors, including disease, trauma, ototoxic drugs and genetic malformation, may interrupt the processing of sound through the inner ear. These conditions may lead to partial or complete loss of hearing or deafness. Hearing loss may range from the inability to hear a certain pitch to the complete inability to detect any sound. There is no age limit on hearing loss either, it may occur in young or old depending on the cause. The type of deafness is defined by the cause of the hearing loss - either conductive or sensorineural. Conduction deafness is caused by the interruption of the transmission of sound vibrations to the fluids of the inner ear. Any number of factors may cause this including impacted ear wax, the insertion of foreign objects, and ruptured ear drums. This type of hearing loss generally involves structures of the outer and middle ear. The most common causes of conduction deafness are otitis media (or inflammation of the middle ear) in children, and otosclerosis ("hardening of the ear" or fused ossicles) often a problem related to aging. Otitis Media can lead to a build-up of fluids within the middle ear which may interfere with the vibrations of the tympanic membrane, often causing it to bulge. Normally the auditory or Eustachian tube allows for the drainage of normal and diseased fluids from the middle ear into the nasopharynx. This can also act as a pathway for infection to enter the middle ear from the nasopharynx, especially in children whose auditory tubes run 15
17 more horizontally than in adults. Inflammation of the mucous membrane lining the Eustachian tube may also cause the tube to close preventing drainage and in chronic cases result in a negative pressure within the middle ear. This condition is generally caused by allergies, colds, inflamed tonsils, etc. and can usually be treated with medication or surgery.6 Otosclerosis, or fusion of the ossicles to each other or to the oval window, inhibits vibrations and therefore interferes with the transmission of sound waves. There may be some vibration through the skull, but it is poorly transmitted compared to the usual passage through the ear. Otosclerosis, and other factors inhibiting movement of the ossicles, may be treated surgically. Hearing losses caused by otisis media and otosclerosis are usually treatable and therefore temporary. Sensorineural deafness occurs when there is damage to neural structures and may occur anywhere along the auditory pathway, from the cochlear hair cells to the auditory cortex. Again this type of hearing loss may be partial or complete and has many causes, both congenital and acquired. Partial hearing loss is often the result of aging, the gradual loss of hearing receptor cells (hair cells) throughout life. This type of hearing loss starts with hair cells at the basal turn and progresses gradually toward the apex. It is characterized by high frequency hearing loss. Extremely loud noises, or prolonged exposure to noise can also cause cell damage. Tumors and disease (such as meningitis) can cause irreversible damage to receptor cells and neurons. Ototoxic drugs may actually destroy hair cells, depending on the patient, dosage and length of treatment. Antibiotics of the category aminoglycosides, especially in conjunction with diuretics, may be ototoxic. Some drugs used in the treatment of cancer, and even high doses of aspirin 16
18 may cause temporary damage. Other factors may include head injuries which lead to reduced blood supply to the inner ear, and illnesses that result in high fever for prolonged periods. Hair cells are more susceptible to injury than supporting cells or auditory neurons. And a large percentage of hair cells may be lost with little or no degradation of cochlear neurons. The loss of neurons seems to parallel injury to the supporting cells, especially Deiter's and pillar cells. Total loss of these supporting cells almost always leads to severe loss of cochlear neurons. The nerve endings actually attach to the base of hair cells by desmosomes, the nerve fibers lie in invaginations of the cell membranes of the Deiter and pillar cells. In some cases the auditory pathway to the brain, or the brain itself may be affected. While the outer, middle and inner ear may be intact, those with central hearing disorders may not be able to interpret the sounds they "hear". Complex hearing rehabilitation may bring about some improvement. Depending upon the cause of hearing loss, cochlear implants may be an option for persons with severe or profound sensorineural deafness. These auditory prosthetics act as tiny transmitters converting sound waves to electrical impulses that stimulate the cochlear neurons directly. Implant surgeries aim to preserve as much of the remaining organ of Corti as possible. This includes trying not to disrupt the basilar membrane or Reissner's membrane and to prevent contamination of the perilymph which can lead to secondary nerve degeneration.7 Types of Hearing Aids Hearing thresholds are the levels at which the softest sound is heard for each tone. Those with normal to severe hearing loss, range from less then 17
19 20 to 90 db. Individuals with profound hearing loss not even detect may sound above 90 db. Although some loud noises may be discerned, these individuals cannot rely solely on hearing for communication. Tests conducted by an audiologist will measure the degree of hearing, as well as speech descrimination. The basic function of a hearing aid is to make sounds louder and thus easier to understand, speech. especially There are several types available and are usually used in conjunction with lip reading to improve communication with the hearing community. In general hearing aids all work the same way. A microphone picks up sound waves and converts them to electrical signals. These signals are sent to an amplifier that increases their strength, a battery provides the energy to operate. The receiver then converts the amplified signals back into sound waves and directs them into the ear via a specially fitted ear coupler. This amplification and reshaping of sound waves may help compensate for weaknesses along the neural pathway. Microphone *=& Amplifier t=5> Receiver = ^ Ear Coupler The types of hearing aids currently available are; In the Ear (ITE), Canal Hearing Aids (ITC), Behind the Ear, Eyeglass aids, Body worn aids, and special function aids that include Cochlear Implants. The latter were developed for those with severe hearing impairment that cannot benefit from traditional amplification devices. The development of the Cochlear Implant The idea of electrically stimulating the auditory system is not new. Interest began in the field with experiments by Volta in He inserted metal rods into both ears and attached them to a circuit of his newly 18
20 developed electrolytic cells. Volta experienced a sensation which he described later as "a blow to the head, followed by a sound like the boiling of a viscous fluid. "^ Despite his unpleasant results, interest continued and by the late 19th century the field was referred to as "electro-otiatrics". Many of the discoveries made have influenced the development of the cochlear implant over the last 30 years. During the 1960's Drs William and Howard House began studies of electrical stimulation on patients undergoing middle-ear surgery. In 1961 one deaf patient received a multi electrode device which was subsequently removed due to swelling and redness. Premature publicity and inappropriate insulation materials lead to problems and research was stopped for several years. In the late 60's engineer Jack Urban joined the surgical team and three patients were implanted in By then improved materials had been developed in part due to pacemaker research. Several others in California were also conducting research in the field of electrical stimulation with both animal and human subjects. (Robin Michelson at U of C, San Francisco and Blair Simmons at Stanford)9 Within ten years interest in the implants ranged from enthusiasm to outrage. The 1970's saw much debate over the use and implications of the implants and in general pitted the clinical community against the scientific community. House and Urban reported the first long term implantations and concluded that the device was now ready for widespread testing and development. They cautioned against uncontrolled implantation and use and suggested "careful investigation by teams of surgeons, electronics experts and rehabilitation personnel."10 In 1973, the American Otological Society held a session on the implants and 19
21 many concluded that the implant should not be pursued since it would never be able to restore "normal" hearing. Dr. House and others countered that some sensation of sound was better than none and that studies should continue. "We are entering a new era of otology. For the past thirty years we have been in the conductive hearing loss era... but we are now entering the era of the sensory hearing loss..."11 From that time through the present, researchers have been looking to fully understand the basic principles of hearing that underlie the success of the implants. Today cochlear implants have become accepted auditory prosthetic devices for both children and adults. It has been established through a variety of studies that the implants are effective options in the rehabilitation of the profoundly deaf. Although results vary depending on the medical, social and psychological situation of the individual patients, almost all receive some benefit from the implants.12 The best results have occurred with postlingually deaf adults and according to several studies, pre-lingually deaf children (Miyamoto, et al. 1993, 1997, Clark & Cowen, 1995). Benefits are also shown to improve with continued use. Post -operative rehabilitation and realistic expectations are vital in the success of the implant. Of course continued evaluation of the device is essential. Advancing technology brings about new modifications in their use and therefore new questions in regard to evaluation. Surgical risks and long term evaluations should continue.13 Benefits Just what are the benefits provided by the implants and when should they be considered for use? First it should be understood that implants are usually recommended for the profoundly deaf who have already tried other hearing aids and vibratory devices but did not find these helpful. Cochlear 20
22 implants may help these individuals hear speech at normal conversational levels, be more aware of safety and warning sounds, lipread (speechread) better, have clearer speech, and monitor the rhythm and loudness of their own speech better. They offer greater awareness of environmental noise and therefore, improved safety. Those who became deaf as post-lingual adults may be able to understand speech without speech reading and even use the telephone. The overall objective of the implant is to improve the ability of the deaf to communicate with the hearing world. This generally leads to improved psychological and social benefits as well. 14 Possible Side Effects It must be understood by the recipient that there is no guarantee the implant will work. Any number of factors may interfere with proper functioning. Careful evaluation, both psychological and physical, before the surgery helps to ensure success.15 If there is a mechanical problem with the coil or electrodes, additional surgery may be needed to repair or replace the device. External parts may also be damaged or malfunction but can be corrected without surgery. Another possible side-effect that may occur is infection at the surgical site or around the internal coil. Again, treatment and surgery may be necessary to treat the problem. Muscles in the face may become weak or partially paralyzed due to surgery. The procedures involved are in close proximity to several nerves including the facial nerve which may be damaged or affected in some way.16 Usually this problem is temporary and will resolve itself in time. Lastly, the auditory nerve fibers in the cochlea may not respond to the electrical signal impulse, or there may be some other form of unforeseen interference along the auditory pathway to the brain. It is also 21
23 possible that calcification and new bony growth occur around the may electrode in the cochlea and block the signals. Once again, secondary surgery may be necessary.17 Follow up treatment with patients may be very important in the successful use of the implant. Negative feelings or disappointing results cause some patients to stop using the implant. They may simply stop wearing the external coil and speech processor. How the Implant Works The cochlear implant is an electronic device that is composed of two parts: one that is surgically implanted within the cochlea (inner ear) and one that is worn externally. The external microphone picks up sound and changes it to electrical impulses which are fed into a speech processor, also worn externally. The processor translates the electrical signal into an electrical code which is then sent to an external coil held in place just behind the ear by a magnet or headset. The code is transmitted through the skin to the internal coil which in turn is sent along the electrodes located within the cochlea. The electrodes stimulate the auditory nerve fibers directly and the message is sent along the auditory nerve to the hearing processing centers of the brain. As coding systems improve, so do the signals sent to the brain. The number of electrodes necessary for stimulation has been studied and will continue to be developed and improved. Some of the major differences among commercial cochlear implants include; the location of the external microphone, method of sound processing, the number, type and placement of electrodes, stimulation mode, back telemetry and the programming systems utilized.18 The external components and used are coding strategy designed to 22
24 work with a specific internal device. The coding strategy is carried out by the speech processor and refers to the way sounds are processed. "Coding strategies are designed primarily to optimize speech understanding rather than the enjoyment of sounds such as music and environmental although these other sounds should not be unpleasant.19 A channel is a single line of information about a signal that is transmitted to the inner ear. These lines of communication run parallel to each other. Electrodes refer only to the number of electrical contacts that are inserted into the cochlea (the electrode array). The number of channels and electrodes may or not may be the same. Modern implant devices have 4 or more channels. Studies have determined that four channels are the amount necessary to understand speech, provided optimal conditions.20 Single and two channel users have been able to resolve ambiguities in speech in combination with lip reading. Observations have even been made with 2- channel users who felt they were really "hearing". The illusion was the result of very familiar sound patterns easily recognized in combination with the temporal cues from the reading. lip It was observed that some patterns were so "well learned and robustly stored" could they be understood with only "a minimal amount of spectral detail."21 The number of electrodes needed is still under debate. There may be a point of "diminishing returns" from too electrodes. many Until there is better understanding of speech processing and researchers determine how best to locate the electrodes, it is a matter or quantity over quality. The placement of the array within the scala tympani is also important. Positions close to the medial wall offer closer contact to the ganglion cells within the wall. (Fig.3) The maximum depth of most implant electrode arrays is 24mm 23
25 along the length of the cochlea. The distance between electrodes is also important so that there is minimal overlap between neural stimulation.22 Cochlear duct^ Cochlear nerve Scala tympani Electrode array Figure 3. Position of electrode array within scala tympani Another difference among implants are the processing strategies used, either analog or pulsatile. With a CA (compressed analog) processor, electrical stimuli are carried simultaneously on adjacent channels. There is some danger that signals will interfere with each other, however there is continuous information. With the pulsatile CIS (Continuous Interleaved Sampler) there is a staggered arrangement of pulses along parallel channels that helps alleviate this interference. However, this causes large "following distances" between successive pulses that may lead to gaps in information.23 Brief changes in in acoustic signals may be missed. Different sound information has its own pattern or formant (predictable digital signal). Recognition and simplification of those patterns occurs in the speech processor. There does not appear to be any clear advantage of one coding strategy over the other at this time. Patient Evaluation The implant is not a "cure" for deafness. Recipients must understand that they do not return normal hearing. Wearers describe the "sound" 24
26 produced as being electronic and staticy. Careful evaluation of possible recipients is conducted before surgery to ensure that the patient understands this. CT scans are performed prior to surgery to determine the possible extent of damage and status of the cochlea and surrounding area. The surgeon should know the particular anatomy as well as possible before surgery, for instance, if it will be possible to enter the cochlea through the round window or if it will be necessary to perform a cochleostomy. Co-axial and coronal plane views help to determine the presence of fractures, otosclerosis or malformations.24 It is especially important to visualize the basal turn of the cochlea and any intracochlear calcification. Mastoid air cells of the surrounding area are prone to infection from otitis media and may lead to mastoiditis which needs to be treated with antibiotics. Fibrous bony growth may develop in this area and cause blockages. Meningitis often leads to ossification of the round window, new bone growth up to 6 mm along the scala tympani is possible. Other tests may determine the extent of nerve damage. Promontory stimulation may determine if the cochlear nerve fibers will be able to be stimulated.25 Several factors to be considered in patient selection include; is a hearing aid adequate, has the patient had any ear infections, histology of the cochlea, population and viability of ganglion cells, general medical and psychosocial situation of the person. There is some debate about the use of implants in patients that use hearing aids successfully. Are the implants at all necessary or do they improve hearing? Studies suggest that the implants can offer significant improvements for hearing aid wearers.26 In general, success in the use of implants seems to depend on; the 25
27 population of cochlear neurons remaining, the level of language and speech development present, the ability of auditory associated areas to ascribe meaning to the 8tn cranial (vestibulocochlear) nerve stimulation. As with all hearing aids the level of expectation of the patient is also critical. It takes time and practice to become accustomed to new sounds. Depending on the length of deafness, the absence of sound may have become very familiar - a return to "noise" may be a confusing experience. Success requires motivation, perserverence and patience. New implant users will need to work with their audiology team to make any necessary adjustments. They will need to participate in an aural rehabilitation program. A history of the patient is important to determine the successful candidate. The best results have been seen in post-lingually deaf adults. It is easier for patients to learn to "recode" information if they have heard sounds before. The sounds heard by the implant wearers are "robotic" in nature and if associated with memory may have greater meaning. The shorter the period of deafness, the better, especially under three years. The outcome of success with the device will also be determined by the patient's environment. Those in a positive, well-educated speaking environment will tend to have better use of the device and will continue to use it. The best candidates, according to Simmons (1985), are those living in a hearing world with a strong motivation to continue to do so. The decision to implant and the success after depends very much on the patients support system of friends and family.27 Age also seems to be an important factor. Those implanted as teenagers constitute the biggest group of "non-users". Due to the current trend toward earlier implantation, studies that focus on the benefits to pre-lingually deaf children are becoming more and more 26
28 Cues" important.28 The implant is based on electrical stimulation via a transmitter placed in the scala tympani of the cochlea through the round window. Other possible areas that may be affected or will determine the success of the implant; viable neural elements of the acoustic nerve, higher auditory pathway, receptor areas of the auditory cortex. Implant Research - The Past 30 Years The original implants used prior to 1978, whether single or multi channel devices used broad-band analog electrical waveforms that excited broad regions of auditory neurons synchronously. Unlike the normal cochlea in which different resonances specifically effect the firing of hair cells, this broad range stimulation still allowed descrimination of consonants and "temporal provided by the implant. The prosthetic device was helpful as a supplement to lip reading and the identification of "classes" of sounds. Studies conducted during the 1970's and 80's provided valuable information that enabled vast improvements in the design of the Nucleus cochlear implant speech processor in wide use today. Studies by Tong and colleagues in Australia, provided important information concerning the descrimination of frequency, intensity and patterns of stimulation. Hartman, et al. studied the response of the auditory nerve to electrical stimulation and determined that the spread of neural activity was determined by the location and orientation of electrodes in the cochlea.29 Important studies by Shannon at the University of California, San Francisco ( ) measured hearing thresholds, uncomfortable loudness and the temporal processing of implant patients. It was determined that implant users had a high sensitivity to frequencies below 300 Hz, but that the usable dynamic range with electrical 27
29 stimulation was much smaller than that of normal hearing. Users could descriminate small changes in intensity (less than 1 db) but with smaller dynamic ranges, they could only discern steps in intensity compared to 200+ steps in normal hearing. Frequency descrimination was similar to normal hearing for low frequencies (<300Hz) but absent for high frequencies. The implant has no mechanism to separate different frequencies of electrical stimulation. Temporal processing appeared normal for implant wearers. They can detect gaps in stimulation and have normal recovery time from adaptations from previous stimulus. Overall implant patients had relatively normal ability to follow temporal fluctuations but no ability to descriminate frequencies above 300 Hz (on single channel electrodes). During the 70's and 80's there were continued improvements of commercial devices thanks to information gathered from research. Actual performance in patients often exceeded expectations by researchers. Most recently, developments in cochlear implant signal processing have resulted in dramatic improvements in performance. New processing strategies, such as CIS - continuous interleaved sampler, show improved performance with multichannel speech processors, better than with single channel processes. (Some multichannel users still receive no spectral place cues and function only at the level of single channel users. It is not Jcnown if this is due to poor nerve survival or failure to adjust the device properly.)30 Implant research has also led to a better understanding of the hearing process in individuals without impairment as well. Studies have shown that loudness is actually perceived by two distinct mechanisms in the brain, one for low frequencies, another process for high frequencies. During the early years of development of the implant there were a 28
30 number of safety concerns that could only be answered over time. Would there be long term negative effects on the auditory nervous system from continuous exposure to electrical fields? Would electrical stimulation precipitate bone growth in the cochlea and the area surrounding the auditory nerve, would it cause the death of any remaining neural elements rendering itself ineffective? Would the devices have to be replaced and would this lead to further trauma? Looking back at twenty years of careful monitoring and research, it would seem that the implants can be used successfully and safely with little or no detrimental effects. Implant devices have proven stable and dependable. Even some devices that have been removed and re-implanted still function well. Hermetic sealing, a process developed for pacemakers was key in early technological developments. It prevents leakage of any kind into the implant, from body fluids, that might cause corrosion or shorting of electrical circuits. Once a device has been implanted for a year, the failure rate is less than 1% (von Wallenburg Brinch 1995). Another safety concern, and a debate still in progress is the implantation of pre-lingually deaf children. If a child is congenitally deaf, can they still benefit from use of the implant, or is some auditory experience required? Also will there be detrimental effects to the still developing auditory system? Studies would indicate that there is benefit. The patterns of stimulation provided by the speech processors are rich enough for the developing nervous system to form connections that will allow them to process information in much the same way as a normal hearing child. Some results question the appropriateness of the stimulus - "wrong information" such as that presented in situations with alot of background noise, could cause the brain to adapt in a way that is detrimental to continued successful 29
31 development in later years.31 Surgical Procedures Since the 1970' s there have been a number of implant devices on the market. The major types include the single-channel intracochlear implant and the multichannel device, most often used. The type of device used may depend upon economic and clinical considerations. The single channel implant most widely used has been a model introduced by House and Urban in A number of factors, including safe surgical technique and ease in manufacturing, enabled this implant to be developed early. single- Most channel devices work in the same manner and are similar in design. The surgical procedure involved in placement of the device is virtually the same.32 One possible advantage of the single channel is that it may be placed outside the cochlea, against the round window, although studies have shown that better results occur when the electrode is passed a short distance (6 mm) into the scala tympani. In children and patients that are being implanted for tinnitus suppression, it is still preferable to leave the electrode outside the cochlea. The objective of the multichannel implant is to take advantage of the "spatial representation of frequency in the interpreted in the profoundly and totally cochlea" so that speech may be deaf to improve communication. The best way to take advantage of this spatial stimulation is to place an electrode array along the basilar membrane within the scala tympani, beginning at the basal turn of the cochlea. (Fig. 4) The array is also flexible and tapered to follow the turn of the cochlea and allow for easy placement, and if necessary, replacement.33 Presurgical testing will determine if certain types of pathology and 30
32 High Low anatomical variations exist. Fibrosis or bony growth present in the basal turn can be removed up to 6 mm to allow for insertion of the electrode. Or if completely filled, the electrode may need to be placed around the turn. Alternatively, an extracochlear multichannel device may be necessary. Electrode Array inserted into scala tympani to a depth of 24 mm Base - Frequency Apex - Frequency Fig. 4 Electrode inserted into cochlea The surgical procedures discussed here are well established and general for a variety of implants, based on the techniques for implanting the Melbourne/Cochlear multichannel receiver.34 The surgeon's understanding of the relevant anatomy is vital in the success of the implantation. It is necessary to be completely familiar with the anatomy of the round window and basal turn of the cochlea, since it is possible that a bony overhang may obscure the surgeon's view of the window. More extensive drilling may be required to expose the round window. Experience laboratory.35 may be gained in the temporal bone 31
33 There are several incisions that may be used to expose the implant area. They include the postauricular inverted-u, extended endaural, C- shaped and inverted-l. A generous margin around the site of the proposed implant provides flexibility for the surgeon in case of unforeseen problems. A dummy package is placed in the approximate position of the implant site and marked. Depending on the experience and preference of the surgeon, the skin and subcutaneous fascia may be raised separately from the deep fascia and periosteum.36 Tension sutures may be used to hold the flap/s out of the way. Extra precautions, such as bi-polar coag, are taken to prevent damage to soft tissue. Once the skull is exposed, a limited mastoidectomy is performed to expose the mastoid antrum, the lateral semicircular canal and the short process of the incus. Knowledge of local anatomy is important in avoiding damage to the facial nerve. The short process of the incus provides a guide to the vertical course of the nerve. Removal of bone is carried out with a cutting burr and fine drill. Irrigation is used during drilling to prevent over heating. Landmarks that the surgeon looks for in determining the drilling site are the mastoid air cells and tegmen of the dura (to prevent drilling into the brain cavity). Once the antrum is exposed and the facial nerve located, a posterior tympanotomy is performed to expose the round window via the facial recess. The facial recess is bounded by the short process of the incus, the facial nerve covered by a thin layer of bone and the chorda tympani. The operation proceeds through the facial recess to get to the round window. The stapes and malleus will be visible through the opening made into the middle ear. The ligaments that hold the incus in place may be seen on either side and help in 32
34 locating the course of the facial nerve. The stapes provides a guide to the scala tympani if the round window has been obliterated. (The inferior margin of the scala tympani at the basal turn is 3 mm below the lower margin of the stapes foot plate.) Extended drilling is often necessary to provide adequate exposure of the round window which may increase risk of injury to the facial nerve. The chorda tympani should also be identified and if possible preserved. It is often difficult to locate the round window. This portion, as well as most of the surgery, will be performed under magnification. Once the middle ear and the round window have been located and exposed, the package bed is prepared. A template is used to mark the position at least 1 cm behind the postauricular groove. It is drilled down to a depth that keeps the implant from protruding significantly from the skull. In some cases it may be drilled down to the dura. Upon completion of the package bed a groove is drilled between the bed and the mastoid cavity. This provides a pathway for the lead wire. In order to facilitate placement of the electrode in the cochlea, the membrane of the round window must be exposed. The bony overhang, crista fenestra, may need to be burred down, drilled anterioinferiorly. The membrane of the round window is incised to provide entry to the scala tympani at the basal turn. Or if necessary, due to obstruction of the window, a cochleotomy anterolateral to the round window may be performed. If the window is obliterated due to meningitis, a hole may be drilled higher along the turn to find lumen, or an extracochlear device may be needed. The bone is thinned with a diamond paste burr until a dark blue line (underlying endosteum) is observed. Bone is then picked away to provide an opening adequate for the unimpeded insertion of the electrode. The hole should be 33
35 approximately 1 mm wide (it may be necessary to extend it up to 2 mm wide to provide adequate visibility). Bone growth and fibrous tissue may require further removal to expose the scala tympani.37 An insertion claw is used to direct the electrode tip into the opening of the cochlea. Holding the package in the other hand, the electrode is gently advanced into the cochlea at the basal turn. The "stiffening rings" around the electrode are used to feed it into place. Insertion is halted if any significant resistance is felt to avoid damage to the electrode and the basilar membrane within the cochlear duct. Damage to the spiral lamina and basal membrane leads to loss of ganglion cells (auditory nerves). Since the electrode is thought to stimulate the peripheral process of the auditory nerve and spiral ganglion cells, any damage is undesirable. Withdrawal and rotation of the electrode guides the tip away from the membrane and around the basal turn. Once the electrode insertion is complete, the package is secured in place by suturing it to the skull. If the overlying flap of skin and fascia are too thick (over 6 mm), it may be necessary to excise the deep fascia. If the flap is too thick, the external magnet may not be held in place properly. The skin flap is sutured over the device once everything is in place. Sutures may be removed after 10 days. An x-ray should be taken at the time of surgery or before the patient goes home to ensure that the device is in the proper place. After the surgical wound has healed, the external portion of the device is fitted. Recovery periods vary depending on the type of device and surgical procedures involved, usually 10 days to 6 weeks. The device used also determines the tolerance for distance between the internal receiver and external coil. For instance, the Nucleus device allows for no more than 6 mm between the parts, therefore it is important that postoperative swelling is at a 34
36 minimum before the headset and speech processor can be fitted. Future Improvements At the present time, the perfect device that would enable complete speech descrimination does not exist. The various single and multichannel devices on the market offer the profoundly deaf improved awareness of environmental sounds, improved speech reading and possibly some speech discrimination.38 In the opinion of one researcher, advances in implant performance have resulted from a combination of basic knowledge, research and just plain luck. We are currently approaching the best performance possible from this random search process and the next wave of improvements will need to be based on more systematic studies of basic principles involved in implant function and studies of speech recognition in the brain. With the continued support and interest of speech and auditory specialists, hopefully there will be improvement in the coding schemes necessary to stimulate the impaired auditory system to the point of producing intelligible speech. The basic system will probably not change much, it is the coding schemes that offer the greatest hope of improvement. Techniques for mapping the surviving auditory neurons within the cochlea may also improve the way these neurons are stimulated and therefore offer improved discrimination.39 A number of studies have been conducted to determine the performance differences between different brands and types of implants. Although results vary, all types of implants enhance lip reading abilities. New speech coding strategies offer improvements such as discrimination in noisy situations.40 In some cases implants may not be sufficiently customized to the individual patient. Fitting now is oriented toward the capabilities of 35
37 the device. Improvements may result in looking at the capabilities of the patient. Pre-operative estimation of surviving nerve fibers, with electrical stimulation during auditory brainstem response recording, becomes more essential as multichannel devices are improved. Many questions still need to be answered to determine why there is such variability among patients implanted with the same device.41 Current surgical procedures try to minimize any further damage to the cochlea and the surviving hair cells. However studies have shown that implants may lead to loss of ganglion cells and degeneration of distal processes. Electrode penetration of the scala media may also lead to new bone formation around the electrodes. Flexibility of the electrode and the geometry of the basal turn play a role in the amount of damage done during implantation.42 Again, improvements in presurgical testing may eliminate some of these problems. Radiography and MRI's help to determine the extent of congenital malformations and aplasias of the labyrinth. Damage of the cochlea has also been attributed directly to the length and design of implants.43 Summary During the 1960's when the idea of replacing part of the auditory sensory system with a mechanical device was first proposed, many felt that it was too complex a proposition and would never work. At the time, researchers were only just beginning to fully understand the complex processing of sound through the human ear. Yet, even these early models met with success in restoring some degree of functional hearing to profoundly deaf individuals. Today, many implant users worldwide can understand running speech (even without lip reading) and many can even 36
38 converse on the phone. According to various researchers, advances in implant performance have resulted from a combination of basic knowledge, research and just plain luck.44 The research to explain why implants work lags behind the actual improvements. In the opinion of Shannon, we are currently approaching the best performance possible from this random search process and the next wave of improvements will need to be based on more systematic studies of basic principles involved in implant function and studies of speech recognition in the brain.45 37
39 - - the Artwork My objective for the artwork produced for this thesis was to visually present information pertaining to the overall subject of hearing and the auditory nervous pathway involved. All of the work is appropriate for use in any number of ways, but especially for poster size presentation. The first three major pieces include information of interest to the general public and are meant to educate anyone interested in the hearing pathway. The second set illustrate information specific to the use of cochlear implants including the surgery itself and the position of the implant when in use. To begin with, I reviewed information concerning the auditory system, sensorineural deafness and the use of cochlear implants in the profoundly deaf. My goal was not to promote or condemn the implants but to present necessary and useful information to an interested audience. The illustrations I chose to create help present the data in a visually interesting, yet easily understandable manner. The process of hearing is obviously not a visible one, but the anatomical features are. Understanding the pertinent anatomy hopefully lends itself to a better understanding of the highly complex mechanisms involved. Labels and text that accompany the illustrations help to clarify the information presented. The subject of each informational poster is as follows; The hearing pathway orientation to the middle and inner ear The organ of Corti - a cellular level view of the organ of hearing The auditory pathway route of auditory neurons to the brain Surgical procedures - placement of the cochlear implant Cochlear implants - orientation of the device in place 38
40 - House The artwork for each piece was created individually using traditional illustration techniques. The middle and inner ear, organ of Corti, auditory pathway and orientation of implant device were all painted in watercolor (Winsor & Newton Cottman brand), first with wet wash technique, then refined with dry brush. In order to even out tones in certain areas a layer of pastel dust was applied using a carbon dust technique with sable brushes. Final details were added using pastel and prismacolor pencils. After producing the initial artwork, the pieces were copied and reduced to appropriate sizes using a Cannon color copier. These copies were then scanned into the computer at 300 ppi and brought into Photoshop adjustment. The original pastel palettes were adjusted to slightly for color darker hues with greater contrast. The various illustrations were copied and pasted into layers of the final presentation size of 11x17 in a new document. A color background was added and additional elements such as arrows were created in Photoshop and placed appropriately. When the final background art was complete, the layers were "flattened" and saved as EPS files for importation into Quark Xpress. I chose to add the text and labels in Quark for ease of manipulation and clarity of text. The final computer generated pieces were printed on several color printers to obtain the best results possible. The artwork for the surgical procedures were done using traditional carbon dust techniques on Color-aid brand paper (clay coated). Initial sketches were made from watching a surgical video on cochlear implants. (Discovery channel surgical program Corp., Dec. 1994) Further research was conducted from surgical atlases and illustrations compared to other published works. I was also able to spend some time in the temporal bone lab at the University of Rochester Medical Center which helped in obtaining a better 39
41 perspective of the orientation of the cochlea within the skull and the structures involved in the surgical procedures. The completed illustrations again were scanned into the computer at 300 ppi and brought into Quark for the addition of the accompanying text. I also chose to create two editorial illustrations as an outgrowth of the more traditional pieces. The first is an oil painting of an adolescent girl, profile view. Sound waves float through the background of the figure bombarding the auditory senses. In a semi-transparent view, the location of the internal structures of hearing - namely the cochlea is revealed. The skull and mandible are shown to orient the viewer to the location of this structure. The second illustration was created for a fictional magazine cover for a real journal - Annals of Otology, Rhinology and Laryngology. It was created with an article in mind, "Cochlear Implants: Future Research Directions," confronting the controversy over the implant. The bony and membranous labyrinth are represented. Both are transparent to reveal the pathway taken by the electrode portion of the cochlear implant. The magnified view of these tiny structures sit atop a blue-print type plan for the circuitry involved in creating - the implant a mechanical device being implanted into a morphological form. Supplemental illustrations were created using pen and ink as an outgrowth of writing this thesis paper. They are intended to clarify specific processes referred to in the text. The information presented in all these illustrations serve to create a better understanding of the anatomy and physiology involved in the hearing process, or in some cases, the inability to hear as well. The intended audience is the general public, sixth grade reading level and higher. The information 40
42 is the might be that presented to a deaf individual considering implantation, or their family, as well as anyone else interested in the subject. The Hearing Pathway Illustration Text This illustration depicts the gross anatomy of the middle and inner ear in relationship to each other within the skull. Hearing is a specialized sense that allows us to perceive and interpret sound. During the process of hearing, sound waves from the environment are received by the ear, converted to nerve impulses and transmitted to the auditory centers of the brain where we interpret them as ''sound". The Outer Ear - or pinna, helps funnel sound waves into the external auditory canal. The canal is mm long and ends at the tympanic membrane. The Middle Ear - is a small, irregularly shaped cavity within the petrous portion of the temporal bone of the skull. It extends from the tympanic membrane to the oval window and houses the small bones of the ears - the ossicles. The middle ear is approximately 15 mm high and 2-4 mm wide. The Inner Ear - made up of three cavity systems - semi-circular canals, the vestibule and the cochlea. These systems are encased in a fluid filled membraneous canal within the "bony labyrinth". inner ear is no larger than the diameter of a dime. The entire structure of the The semicircular canals function in maintaining balance. The "snail shell" like cochlea is key in the processing of sound. The auditory nerve arises from within this structure. The Organ of Corti The interior space of the cochlea is divided into 3 separate fluid filled 41
43 chambers - the scala tympani, scala media and scala vestibuli. The organ of Corti is located within the scala media, or cochlear duct. Fluid movement within the chambers of the cochlea cause the basilar membrane to rise and fall in waves depending upon the frequency of the sounds being received. This movement causes the cilia of the hair cells to pull against the tectorial membrane and stimulates them to release neurotransmitters. The neurotransmitters in turn excite the cochlear nerve fibers. This is where the transmission of signals along the auditory pathway begins. The auditory pathway The afferent nerve fibers originating from the cochlea come together to make up the auditory or vestibulocochlear nerve. The cell bodies of these neurons are found in the spiral ganglion at the center of the cochlea. The auditory nerve travels to the cochlear nuclei located in the pons. Secondary nerve fibers travel to the opposite side of the pons and may project to the superior olivary nucleus or to the inferior colliculus of the midbrain. At the level of the inferior colliculus, impulses from both sides provide information as to the location of sound origination. From the inferior colliculus the nerve fibers travel to the medial geniculate nucleus of the thalamus where all fibers synapse. At this level there is crude discrimination of tone and direction of sound. From the thalamus, impulses travel to the auditory cortex in the superior temporal gyrus and insula where information is further refined and translated (fine tuning occurs). It is at this highest level where loudness and a precise discrimination of pitch occurs. 42
44 Surgical Procedures - Multichannel Implant Surgery The steps shown here are a partial representation of the surgical procedure for placing the internal coil and electrode array implant device. Rather than show each step individually, of the cochlear several steps have been combined for efficiency. The orientation illustration shows the location of the surgery behind the ear. Making the initial incision The first step is to mark the location of the incision. Several flap incisions are currently in use. The one shown here is a modified version of the inverted-u incision. The marking of the incision may be expedited by placing a dummy package in the approximate position. The marking device shown here may be used to mark the location of the internal coil on the skull beneath the skin as well. Limited mastoidectomy The next step shows the drilling into the mastoid bone after the flap of skin, fascia and muscle have been pulled back. A limited mastoidectomy will expose the mastoid antrum, the lateral semicircular canal and the short process of the incus. A burring tool is used to chip away the bone. Preparation of the package bed The third step illustrates the preparation of the package bed. It is drilled out after the surgeon has determined and marked the position a using template. It must be placed at least 1 cm behind the postauricular groove. The bed is drilled down to a depth to prevent the package from protruding significantly above the surface of the bone. Note the position of the exposed antrum. Feeding the electrode into the cochlea After the drilling is complete, the electrode is inserted. Exposure of the round window is desirable and may require drilling away of a bony overhang anteroinferiorly. The electrode may 43
45 be inserted through the round window into the scala tympani, or if necessary, at the basal turn of the cochlea. This second option requires a cochleotomy just anterior to the round window. The presence of extensive fibrous tissue or bone may require further drilling into the scala tympani to facilitate placement of the electrode. A special fork like instrument is used to feed the electrode in to the desired depth. The insertion should be stopped if any significant resistance is encountered to prevent injury to the basilar membrane. Securing the inner coil package in place Following placement of the electrode, the package containing the internal coil is secured with dacron ties to the skull. It is further anchored in place by suturing the skin flap over it. Normally the surgery takes 2-3 hours to complete. If there are no further complications the patient may leave the hospital in 1-4 days. Cochlear implant in place Frontal Section showing device in place. (After Ed Zilberts) Following a healing period of 3-6 weeks, the patient will try the implant device for the first time. They are fitted with the external parts: the microphone, speech processor and external coil. The external coil is usually held in place by a magnet or headset just over the location of the internal coil. Electrical codes are sent across the skin from the external to the internal coil and are carried along the electrode to the cochlea. Signals are picked up by sensory neurons leading from the cochlea to the cochlear nerve. Awareness of sound occurs in the auditory cortex of the brain. 44
46 References Berger, Kenneth W. The Hearing Aid - Ifs Operation and Development 3d ed., Livonia, Michigan: The National Hearing Aid Society, Brackman, Derald E., M.D. "Surgical techniques in Cochlear Seminars in Hearing 6 (Feb 1985): Implantation." Burton Koch, Dawn. "Commercial Cochlear Implants." Seminars in Hearing 17 (Nov 1996): Carlson, Neil. Physiology of Behavior.(Boston): Allyn and Bacon, Clark, Graeme M. "Cochlear Implants: Future Research Directions." Annals of Otology, Rhinology and Laryngology 104 (Sept 1995): Clark, Graeme M. and Robert Cowan. eds.annals of Otology. Rhinology and Laryngology International Cochlear Implant, Speech and Hearing Symposium, Melbourne 1994 & Supplement , Clark, Graeme M., Shute, S.A., Sheperd R.K., Carter, T.D. "Cochlear Implantation: Osteogenesis, Electrode - Tissue Impedance and Residual Hearing."Annals of Otology. Rhinology and Laryngology 1995): (Sept Clark, Graeme M., Tong, Yit C, Patrick, James F. Cochlear Prostheses.U.K.: Churchill Livingstone, Medical Division of Longman Group, Cooper, H.U.W., ed. Cochlear Implants A Practical Guide. San Diego, CA: Singular Publishing Group, Inc., Dillier, N., Battmer, R.D., Doring, W.H., Muller-Diele, J."Multicentric Field evaluation of a New Speech Coding Strategy for Cochlear Implants." 45
47 Audiology 34 (May 1995): Dublin, William B. Fundamentals of Sensorineural Auditory Pathology. (Springfield, 111.): Charles C. Thomas, Gray, Robert, ed., Cochlear Implants. San Diego, CA: Chicago-Hill Press, Haskell, George B. and Herbert N. Jordan. "Cochlear Implant Performance as a Function of Electrode Number." Seminars in Hearing 1992): (August Loeb, Gerald E., M.D. "An Information Highway to the Auditory Nerve," Seminars in Hearing 17 (Nov 1996): Marieb, Elaine N. Human Anatomy & Physiology. The Benjamin /Cummings Publishing Company, Inc., Miyamoto, Richard T., M. J. Osberger, A. M. Robbins, W. A. Meyers, K. Kessler, "Speech Intelligibility of Children with Multichannel Cochlear Implants." Annals of Otology. Rhinology & Laryngology. Supplement 168 (May 1997): Miyamoto, Richard T., M. J. Osberger, A. M. Robbins, W. A. Meyers, K. Kessler, "Pre-lingually Deafened Childrens' Performance with the Nucleus Multi-channel Cochlear Implant." American lournal of Otology. 14 (1993): Nadol, J.B. and Harold F. Schunknecht. Surgery Bone. NY, NY: Raven Press, of the Ear and Temporal Ross, Michael H. and Lynn J. Romrell. Histology - A Text and Atlas. Baltimore, MD: Williams and Wilkins,
48 Schultz, Nanci A. Orientation to Deafness. (Boston): Allyn and Bacon, Simon & Schuster, Schuknecht, Harold F. Pathology of the Ear. Cambridge, Massachusetts, London: Harvard University Press, Shallop, Jon K. "Understanding Speech Coding 1994): Strategies." CICI Contact (Fall Shannon, Robert V. "Cochlear Implants: What Have We Learned and Where Are We Going?." Seminars in Hearing 17 (Nov 1996): Simmons, F. Blair, M.D., "Some Medical, Social, and Psychological Considerations in Cochlear Implants." Seminars in Hearing 6 (Feb 1985): 1-6. Sonn, Martin. An Artificial Cochlea for the Sensory Deaf: Presurgical - Development. Portsmouth, RI : Raytheon Company Submarine Signal Division, Spelman, Francis A. and Josef M. Miller. Cochlear Implants - Models of the Electrically Stimulated Ear. NY, NY: Springer-Verlag, Inc., "Cochlear Implants in Adults and Children." National Institute of Health Consensus Development Conference Statement, May 15-17, Treaba, C.G., Xu, J., Clark, G.M. "Pre-curved Electrode and Array Insertion Tool."Annals of Otology. Rhinology and Laryngology (Sept 1995): Tyler, Richard S. "Cochlear Implants and the Deaf Culture." March
49 Wilson, B.S., Lawson, D.T., Zerbi, M., Finley, C.C., Wolford, R.D. "New Processing Otology Implantation." Strategies in Cochlear American lournal of 16 (Sept 1995): Zemlin, Willard R. Speech and Hearing Science - New Jersey: Prentice-Hall, Inc Anatomy and Physiology. 48
50 Anatomy A 1 Robert F. Gray, ed., Cochlear Implants. (San Diego, CA: College-Hill Press. Inc. 1985), Ibid., Ibid., Michael H. Ross and Lynn J. Romrell, Histology - Wilkins, 1985), 757. Text and Atlas (Baltimore, MD: Williams and 3 Elaine N. Marieb, Human Anatomy and Physiology (The Benjamin Cummings Publishing Comp., Inc., 1989), Willard R. Zemlin. Speech and Hearing Science - Inc. 1968), 375. and Physiology (New Jersey: Prentice- Hall, 7 Gray, Cochlear Implants, William M Luxford and Derald E Brachman, "The History of Cochlear Implants" Robert Gray, ed., Cochlear Implants H.U.W. Cooper, ed., Cochlear Implants: A Practical Guide (San Diego, CA: Singular Publishing Group, 1991), Ibid., Ibid. 12 Blair F. Simmons, M.D., "Some Medical, Social and Psychological Considerations in Cochlear Implants," Seminars in Hearing 6 (Feb 1985):3. Learned," 13 Robert V. Shannon,"Cochlear Implants: What Have We Seminars in Hearing (Nov 1996): 14 "Cochlear Implants in Adults and Children," National Institute of Health Consensus Development Conference Statement Mav Cooper, ed., Cochlear Implants: A Practical Guide Dawn Burton Koch, "Commercial Cochlear Implants," Seminars in Hearing 17 (Nov 1996): Clark, G., S.A. Shute, R.K. Sheperd, T.D. Carter, "Cochlear Implantation: Electrode- Osteogenesis, Tissue Impedance and Residual Hearing." Annals of Otology. Rhinology and Laryngology. 104 (Sept 1995): Implants," 18 Dawn Burton Koch, "Commercial Cochlear Seminars in Hearing 17 (Nov 1996): Jon K Shallop. "Understanding Speech Coding Strategies," CICI Contact. (Fall 1994): 32.
51 20 Robert V. Shannon,"Cochlear Implants: What Have We Learned," Ibid. 22 Gerald E. Loeb, M.D. "An Information Highway to the Auditory Nerve," Seminars in Hearing 17 (Nov 1996): Ibid., Graeme M. Clark, Yit C. Tong, James F. Patrick, Cochlear Prostheses (UK: Churchill Livingstone, Medical Division of Longman Group, 1990). 2^ Blair F. Simmons, M.D., "Some Medical, Social and Psychological Considerations in Cochlear Implants," Graeme M. Clark, "Cochlear Implants: Future Research Direcuons."Annals of Otology. Rhinology & Laryngology 104 (Sept 1995): Blair F. Simmons, M.D., "Some Medical, Social and Psychological Considerations in Cochlear Implants," Richard T.Miyamoto, M J Osberger, A M Robbins, W A Meyers, K Kessler, "Speech Intelligibility of Children with Multichannel Cochlear Implants," Annals of Otology. Rhinology & Laryngology. Supplement 168 (May 1997): 443. Learned," 29 Robert V. Shannon,"Cochlear Implants: What Have We Ibid Ibid. 32 Cooper.Cochlear Implants C. G. Treaba, J Xu, G.M. Clark, "Pre-curved Electrode Array and Insertion Tool," Annals of Otology. Rhinology & Laryngology 104 (Sept 1995): Clark, et al., Cochlear Prostheses ^ Cooper.Cochlear Implants, Ibid., Ibid., Gray Cochlear Implants Robert V. Shannon/'Cochlear Implants, What Have We Learned", 410.
52 40 N. Dillier, R.D. Battmer, W.H. Doring, J. Muller-Diele, "Multicentric Field evaluation of a New Speech Coding Strategy for Cochlear Implants", Audiologv 34 (May 1995): Robert V. Shannon/'Cochlear Implants: What Have We Learned," C.G. Treaba, et al., "Pre-Curved Electrode Array and Insertion Tool," Gray, Cochlear Implants Learned," Robert V. Shannon,"Cochlear Implants: What Have We Ibid.
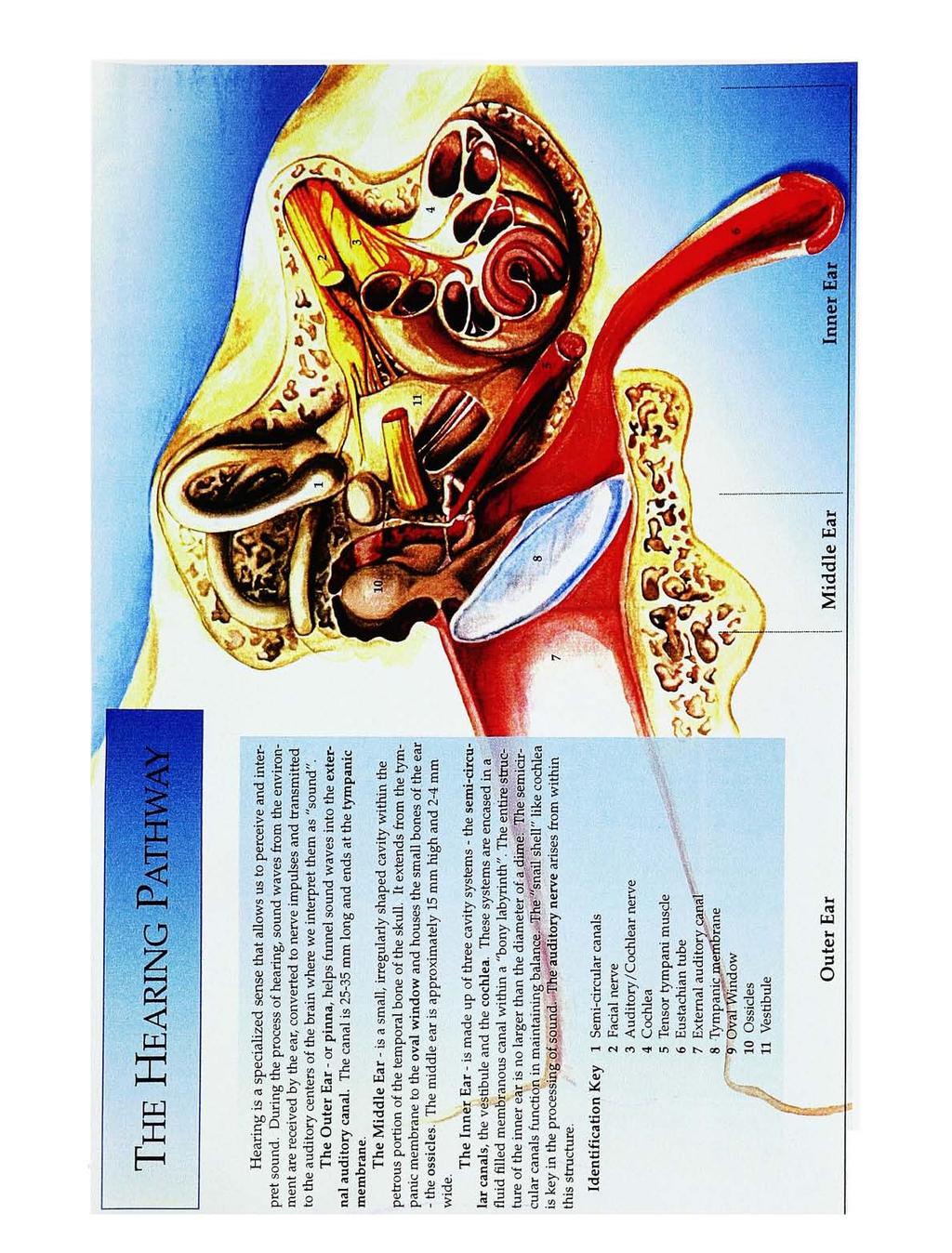
53
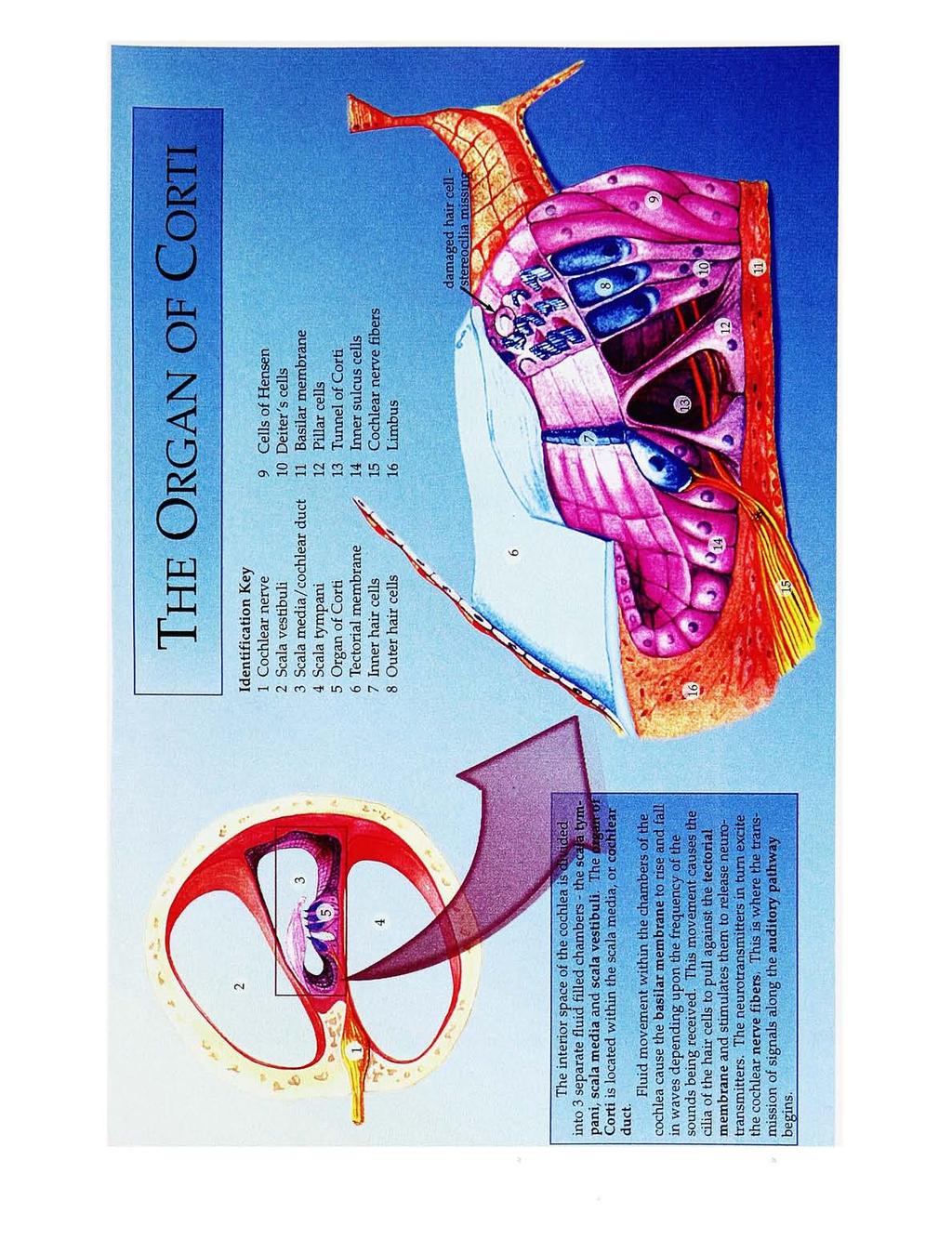
54

55 he Audcbqry- Pathway ^a^cmtoyy-nerve reaches locadon^fcochlear nuclei. e fibers from the cochlea join to form the auditory nerve Sensorineural deafness may ocoar anywhere along the^^ural ptfmw4y to the brain. Damage may^e^caused by genetic abnormalities, disease, drug use, trauma, etc. High Pitch Low Pitch

56 External & Internal Parts 1 Microphone 2 Speech Processor (wire to) 3 External Coil 4 Internal Coil 5 Electrode array (fed into scala tympani) Cochlear implant in place Following a healing period of 3-6 weeks, the patient will try the implant device for the first time. They are fitted with the external parts: the microphone, speech processor and external coil. The external coil is usually held in place by a magnet or headset just over the location of the internal coil. Electrical codes are sent across the skin from the external to the internal coil and are carried along the electrode to from the cochlea to the cochlea. Signals are picked up by sensory neurons leading the cochlear nerve. Awareness of sound occurs in the cortex of auditory the brain.
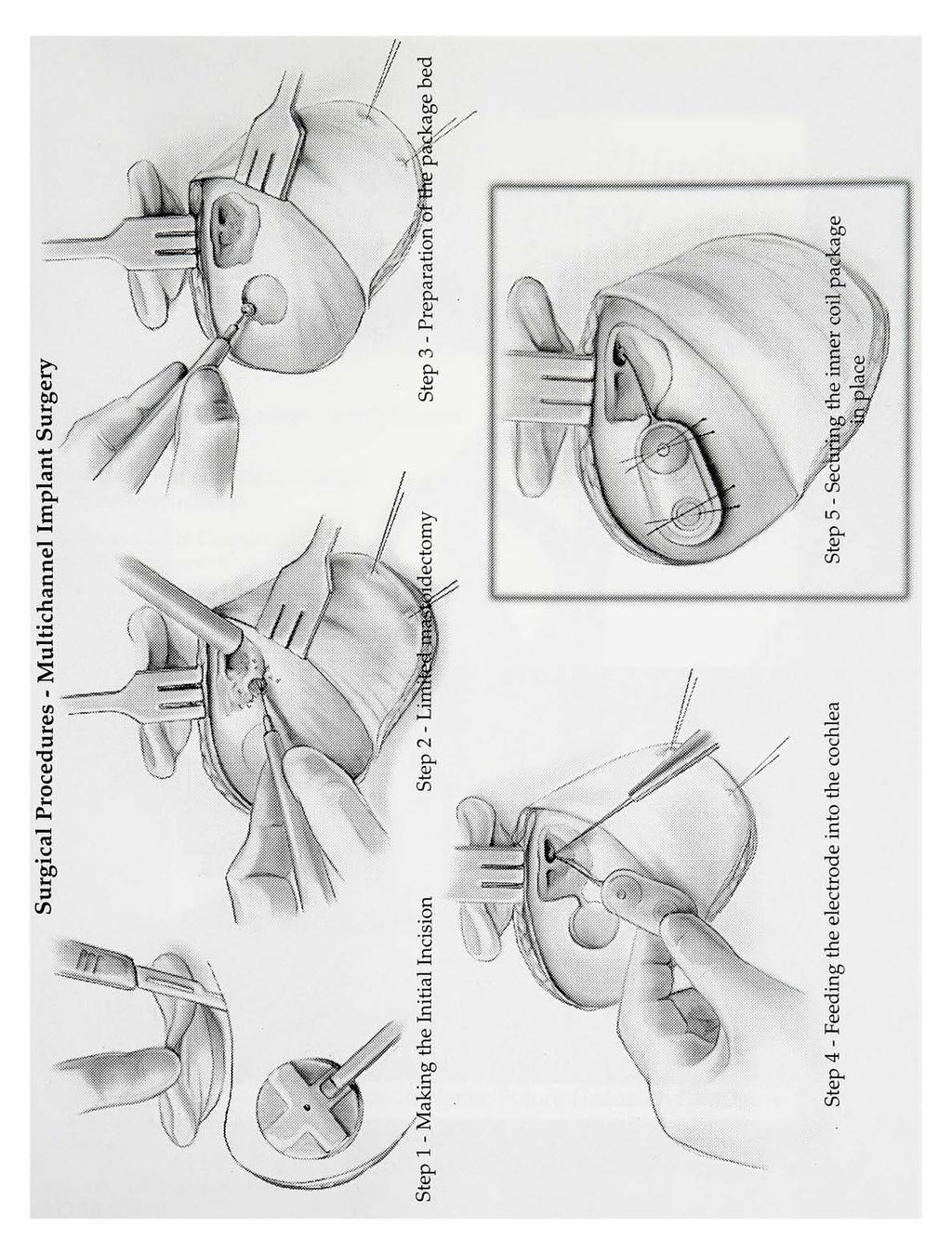
57

58 Cochlear Implants: Future Research Directions - Volume 104 October 1995 NO 10, Part 1
59 f*.
Auditory Physiology Richard M. Costanzo, Ph.D.
 Auditory Physiology Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Describe the morphology and function of the following structures:
Auditory Physiology Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Describe the morphology and function of the following structures:
MECHANISM OF HEARING
 MECHANISM OF HEARING Sound: Sound is a vibration that propagates as an audible wave of pressure, through a transmission medium such as gas, liquid or solid. Sound is produced from alternate compression
MECHANISM OF HEARING Sound: Sound is a vibration that propagates as an audible wave of pressure, through a transmission medium such as gas, liquid or solid. Sound is produced from alternate compression
Auditory System. Barb Rohrer (SEI )
") Auditory System Barb Rohrer (SEI614 2-5086) Sounds arise from mechanical vibration (creating zones of compression and rarefaction; which ripple outwards) Transmitted through gaseous, aqueous or solid medium
Auditory System Barb Rohrer (SEI614 2-5086) Sounds arise from mechanical vibration (creating zones of compression and rarefaction; which ripple outwards) Transmitted through gaseous, aqueous or solid medium
Unit VIII Problem 9 Physiology: Hearing
 Unit VIII Problem 9 Physiology: Hearing - We can hear a limited range of frequency between 20 Hz 20,000 Hz (human hearing acuity is between 1000 Hz 4000 Hz). - The ear is divided into 3 parts. Those are:
Unit VIII Problem 9 Physiology: Hearing - We can hear a limited range of frequency between 20 Hz 20,000 Hz (human hearing acuity is between 1000 Hz 4000 Hz). - The ear is divided into 3 parts. Those are:
ENT 318 Artificial Organs Physiology of Ear
 ENT 318 Artificial Organs Physiology of Ear Lecturer: Ahmad Nasrul Norali The Ear The Ear Components of hearing mechanism - Outer Ear - Middle Ear - Inner Ear - Central Auditory Nervous System Major Divisions
ENT 318 Artificial Organs Physiology of Ear Lecturer: Ahmad Nasrul Norali The Ear The Ear Components of hearing mechanism - Outer Ear - Middle Ear - Inner Ear - Central Auditory Nervous System Major Divisions
Receptors / physiology
 Hearing: physiology Receptors / physiology Energy transduction First goal of a sensory/perceptual system? Transduce environmental energy into neural energy (or energy that can be interpreted by perceptual
Hearing: physiology Receptors / physiology Energy transduction First goal of a sensory/perceptual system? Transduce environmental energy into neural energy (or energy that can be interpreted by perceptual
AUDITORY APPARATUS. Mr. P Mazengenya. Tel 72204
 AUDITORY APPARATUS Mr. P Mazengenya Tel 72204 Describe the anatomical features of the external ear Describe the tympanic membrane (ear drum) Describe the walls of the middle ear Outline the structures
AUDITORY APPARATUS Mr. P Mazengenya Tel 72204 Describe the anatomical features of the external ear Describe the tympanic membrane (ear drum) Describe the walls of the middle ear Outline the structures
Deafness and hearing impairment
 Auditory Physiology Deafness and hearing impairment About one in every 10 Americans has some degree of hearing loss. The great majority develop hearing loss as they age. Hearing impairment in very early
Auditory Physiology Deafness and hearing impairment About one in every 10 Americans has some degree of hearing loss. The great majority develop hearing loss as they age. Hearing impairment in very early
Hearing. By: Jimmy, Dana, and Karissa
 Hearing By: Jimmy, Dana, and Karissa Anatomy - The ear is divided up into three parts - Sound enters in through the outer ear and passes into the middle where the vibrations are received and sent to the
Hearing By: Jimmy, Dana, and Karissa Anatomy - The ear is divided up into three parts - Sound enters in through the outer ear and passes into the middle where the vibrations are received and sent to the
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium!
 Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! Chapter 17 Part 2 Special Senses! The Special Senses! Hearing and Equilibrium!
 Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Required Slide. Session Objectives
 Auditory Physiology Required Slide Session Objectives Auditory System: At the end of this session, students will be able to: 1. Characterize the range of normal human hearing. 2. Understand the components
Auditory Physiology Required Slide Session Objectives Auditory System: At the end of this session, students will be able to: 1. Characterize the range of normal human hearing. 2. Understand the components
Structure, Energy Transmission and Function. Gross Anatomy. Structure, Function & Process. External Auditory Meatus or Canal (EAM, EAC) Outer Ear
 Outer Ear") Gross Anatomy Structure, Energy Transmission and Function IE N O ME 1 Structure, Function & Process 4 External Auditory Meatus or Canal (EAM, EAC) Outer third is cartilaginous Inner 2/3 is osseous Junction
Gross Anatomy Structure, Energy Transmission and Function IE N O ME 1 Structure, Function & Process 4 External Auditory Meatus or Canal (EAM, EAC) Outer third is cartilaginous Inner 2/3 is osseous Junction
Anatomy and Physiology of Hearing
 Anatomy and Physiology of Hearing The Human Ear Temporal Bone Found on each side of the skull and contains the organs for hearing and balance Divided into four major portions: - squamous - mastoid - tympanic
Anatomy and Physiology of Hearing The Human Ear Temporal Bone Found on each side of the skull and contains the organs for hearing and balance Divided into four major portions: - squamous - mastoid - tympanic
Intro to Audition & Hearing
 Intro to Audition & Hearing Lecture 16 Chapter 9, part II Jonathan Pillow Sensation & Perception (PSY 345 / NEU 325) Fall 2017 1 Sine wave: one of the simplest kinds of sounds: sound for which pressure
Intro to Audition & Hearing Lecture 16 Chapter 9, part II Jonathan Pillow Sensation & Perception (PSY 345 / NEU 325) Fall 2017 1 Sine wave: one of the simplest kinds of sounds: sound for which pressure
Hearing: Physiology and Psychoacoustics
 9 Hearing: Physiology and Psychoacoustics Click Chapter to edit 9 Hearing: Master title Physiology style and Psychoacoustics The Function of Hearing What Is Sound? Basic Structure of the Mammalian Auditory
9 Hearing: Physiology and Psychoacoustics Click Chapter to edit 9 Hearing: Master title Physiology style and Psychoacoustics The Function of Hearing What Is Sound? Basic Structure of the Mammalian Auditory
Otoconia: Calcium carbonate crystals Gelatinous mass. Cilia. Hair cells. Vestibular nerve. Vestibular ganglion
 VESTIBULAR SYSTEM (Balance/Equilibrium) The vestibular stimulus is provided by Earth s, and. Located in the of the inner ear, in two components: 1. Vestibular sacs - gravity & head direction 2. Semicircular
VESTIBULAR SYSTEM (Balance/Equilibrium) The vestibular stimulus is provided by Earth s, and. Located in the of the inner ear, in two components: 1. Vestibular sacs - gravity & head direction 2. Semicircular
Anatomy of the Ear Region. External ear Middle ear Internal ear
 Ear Lecture Objectives Make a list of structures making the external, middle, and internal ear. Discuss the features of the external auditory meatus and tympanic membrane. Describe the shape, position,
Ear Lecture Objectives Make a list of structures making the external, middle, and internal ear. Discuss the features of the external auditory meatus and tympanic membrane. Describe the shape, position,
Chapter 11: Sound, The Auditory System, and Pitch Perception
 Chapter 11: Sound, The Auditory System, and Pitch Perception Overview of Questions What is it that makes sounds high pitched or low pitched? How do sound vibrations inside the ear lead to the perception
Chapter 11: Sound, The Auditory System, and Pitch Perception Overview of Questions What is it that makes sounds high pitched or low pitched? How do sound vibrations inside the ear lead to the perception
Chapter 15 Hearing & Equilibrium
 Chapter 15 Hearing & Equilibrium ANATOMY OF THE OUTER EAR EAR PINNA is the outer ear it is thin skin covering elastic cartilage. It directs incoming sound waves to the EXTERNAL AUDITORY CANAL, which is
Chapter 15 Hearing & Equilibrium ANATOMY OF THE OUTER EAR EAR PINNA is the outer ear it is thin skin covering elastic cartilage. It directs incoming sound waves to the EXTERNAL AUDITORY CANAL, which is
Printable version - Hearing - OpenLearn - The Open University
 Skip to content Accessibility Sign in Contact Search the OU The Open University Study at the OU Research at the OU OU Community About the OU Hearing Printable page generated Saturday, 12 November 2011,
Skip to content Accessibility Sign in Contact Search the OU The Open University Study at the OU Research at the OU OU Community About the OU Hearing Printable page generated Saturday, 12 November 2011,
SOLUTIONS Homework #3. Introduction to Engineering in Medicine and Biology ECEN 1001 Due Tues. 9/30/03
 SOLUTIONS Homework #3 Introduction to Engineering in Medicine and Biology ECEN 1001 Due Tues. 9/30/03 Problem 1: a) Where in the cochlea would you say the process of "fourier decomposition" of the incoming
SOLUTIONS Homework #3 Introduction to Engineering in Medicine and Biology ECEN 1001 Due Tues. 9/30/03 Problem 1: a) Where in the cochlea would you say the process of "fourier decomposition" of the incoming
THE EAR AND HEARING Be sure you have read and understand Chapter 16 before beginning this lab. INTRODUCTION: hair cells outer ear tympanic membrane
 BIOLOGY 211: HUMAN ANATOMY & PHYSIOLOGY ****************************************************************************************************** THE EAR AND HEARING ******************************************************************************************************
BIOLOGY 211: HUMAN ANATOMY & PHYSIOLOGY ****************************************************************************************************** THE EAR AND HEARING ******************************************************************************************************
College of Medicine Dept. of Medical physics Physics of ear and hearing /CH
 College of Medicine Dept. of Medical physics Physics of ear and hearing /CH 13 2017-2018 ***************************************************************** o Introduction : The ear is the organ that detects
College of Medicine Dept. of Medical physics Physics of ear and hearing /CH 13 2017-2018 ***************************************************************** o Introduction : The ear is the organ that detects
Ear. Utricle & saccule in the vestibule Connected to each other and to the endolymphatic sac by a utriculosaccular duct
 Rahaf Jreisat *You don t have to go back to the slides. Ear Inner Ear Membranous Labyrinth It is a reflection of bony labyrinth but inside. Membranous labyrinth = set of membranous tubes containing sensory
Rahaf Jreisat *You don t have to go back to the slides. Ear Inner Ear Membranous Labyrinth It is a reflection of bony labyrinth but inside. Membranous labyrinth = set of membranous tubes containing sensory
PSY 215 Lecture 10 Topic: Hearing Chapter 7, pages
 PSY 215 Lecture 10 Topic: Hearing Chapter 7, pages 189-197 Corrections: NTC 09-1, page 3, the Superior Colliculus is in the midbrain (Mesencephalon). Announcements: Movie next Monday: Case of the frozen
PSY 215 Lecture 10 Topic: Hearing Chapter 7, pages 189-197 Corrections: NTC 09-1, page 3, the Superior Colliculus is in the midbrain (Mesencephalon). Announcements: Movie next Monday: Case of the frozen
Auditory System Feedback
 Feedback Auditory System Feedback Using all or a portion of the information from the output of a system to regulate or control the processes or inputs in order to modify the output. Central control of
Feedback Auditory System Feedback Using all or a portion of the information from the output of a system to regulate or control the processes or inputs in order to modify the output. Central control of
Hearing. istockphoto/thinkstock
 Hearing istockphoto/thinkstock Audition The sense or act of hearing The Stimulus Input: Sound Waves Sound waves are composed of changes in air pressure unfolding over time. Acoustical transduction: Conversion
Hearing istockphoto/thinkstock Audition The sense or act of hearing The Stimulus Input: Sound Waves Sound waves are composed of changes in air pressure unfolding over time. Acoustical transduction: Conversion
THE COCHLEA AND AUDITORY PATHWAY
 Dental Neuroanatomy Suzanne S. Stensaas, PhD February 23, 2012 Reading: Waxman, Chapter 16, Review pictures in a Histology book Computer Resources: http://www.cochlea.org/ - Promenade around the Cochlea
Dental Neuroanatomy Suzanne S. Stensaas, PhD February 23, 2012 Reading: Waxman, Chapter 16, Review pictures in a Histology book Computer Resources: http://www.cochlea.org/ - Promenade around the Cochlea
Chapter 13 Physics of the Ear and Hearing
 Hearing 100 times greater dynamic range than vision Wide frequency range (20 ~ 20,000 Hz) Sense of hearing Mechanical system that stimulates the hair cells in the cochlea Sensors that produce action potentials
Hearing 100 times greater dynamic range than vision Wide frequency range (20 ~ 20,000 Hz) Sense of hearing Mechanical system that stimulates the hair cells in the cochlea Sensors that produce action potentials
SENSORY SYSTEM VII THE EAR PART 1
 SENSORY SYSTEM VII THE EAR PART 1 Waves Sound is a compression wave The Ear Ear Outer Ear Pinna Outer ear: - Made up of the pinna and the auditory canal Auditory Canal Outer Ear Pinna (also called the
SENSORY SYSTEM VII THE EAR PART 1 Waves Sound is a compression wave The Ear Ear Outer Ear Pinna Outer ear: - Made up of the pinna and the auditory canal Auditory Canal Outer Ear Pinna (also called the
Systems Neuroscience Oct. 16, Auditory system. http:
 Systems Neuroscience Oct. 16, 2018 Auditory system http: www.ini.unizh.ch/~kiper/system_neurosci.html The physics of sound Measuring sound intensity We are sensitive to an enormous range of intensities,
Systems Neuroscience Oct. 16, 2018 Auditory system http: www.ini.unizh.ch/~kiper/system_neurosci.html The physics of sound Measuring sound intensity We are sensitive to an enormous range of intensities,
Acquired Deafness Loss of hearing that occurs or develops sometime in the course of a lifetime, but is not present at birth.
 Page 1 of 5 URMC» Audiology Glossary of Terms A Acoustic Neuroma A tumor, usually benign, which develops on the hearing and balance nerves and can cause gradual hearing loss, tinnitus, and dizziness. Acquired
Page 1 of 5 URMC» Audiology Glossary of Terms A Acoustic Neuroma A tumor, usually benign, which develops on the hearing and balance nerves and can cause gradual hearing loss, tinnitus, and dizziness. Acquired
Hearing Sound. The Human Auditory System. The Outer Ear. Music 170: The Ear
 Hearing Sound Music 170: The Ear Tamara Smyth, trsmyth@ucsd.edu Department of Music, University of California, San Diego (UCSD) November 17, 2016 Sound interpretation in the auditory system is done by
Hearing Sound Music 170: The Ear Tamara Smyth, trsmyth@ucsd.edu Department of Music, University of California, San Diego (UCSD) November 17, 2016 Sound interpretation in the auditory system is done by
Music 170: The Ear. Tamara Smyth, Department of Music, University of California, San Diego (UCSD) November 17, 2016
 November 17, 2016") Music 170: The Ear Tamara Smyth, trsmyth@ucsd.edu Department of Music, University of California, San Diego (UCSD) November 17, 2016 1 Hearing Sound Sound interpretation in the auditory system is done by
Music 170: The Ear Tamara Smyth, trsmyth@ucsd.edu Department of Music, University of California, San Diego (UCSD) November 17, 2016 1 Hearing Sound Sound interpretation in the auditory system is done by
to vibrate the fluid. The ossicles amplify the pressure. The surface area of the oval window is
 Page 1 of 6 Question 1: How is the conduction of sound to the cochlea facilitated by the ossicles of the middle ear? Answer: Sound waves traveling through air move the tympanic membrane, which, in turn,
Page 1 of 6 Question 1: How is the conduction of sound to the cochlea facilitated by the ossicles of the middle ear? Answer: Sound waves traveling through air move the tympanic membrane, which, in turn,
Presentation On SENSATION. Prof- Mrs.Kuldeep Kaur
 Presentation On SENSATION Prof- Mrs.Kuldeep Kaur INTRODUCTION:- Sensation is a specialty area within Psychology that works at understanding how are senses work and how we perceive stimuli in the environment.
Presentation On SENSATION Prof- Mrs.Kuldeep Kaur INTRODUCTION:- Sensation is a specialty area within Psychology that works at understanding how are senses work and how we perceive stimuli in the environment.
Cochlear Implant The only hope for severely Deaf
 Cochlear Implant The only hope for severely Deaf By: Dr. M. Sohail Awan, FCPS (ENT) Aga Khan University Hospital, Karachi - Pakistan For centuries, people believed that only a miracle could restore hearing
Cochlear Implant The only hope for severely Deaf By: Dr. M. Sohail Awan, FCPS (ENT) Aga Khan University Hospital, Karachi - Pakistan For centuries, people believed that only a miracle could restore hearing
HEARING AND COCHLEAR IMPLANTS
 HEARING AND COCHLEAR IMPLANTS FRANCIS CREIGHTON, MD NEUROTOLOGY & SKULL BASE SURGERY FELLOW JOHNS HOPKINS SCHOOL OF MEDICINE NOV 9 TH, 2017 THANKS TO: CHARLIE DELLA SANTINA, HEIDI NAKAJIMA AND DOUG MATTOX
HEARING AND COCHLEAR IMPLANTS FRANCIS CREIGHTON, MD NEUROTOLOGY & SKULL BASE SURGERY FELLOW JOHNS HOPKINS SCHOOL OF MEDICINE NOV 9 TH, 2017 THANKS TO: CHARLIE DELLA SANTINA, HEIDI NAKAJIMA AND DOUG MATTOX
Hearing. By Jack & Tori
 Hearing By Jack & Tori 3 Main Components of the Human Ear. Outer Ear. Middle Ear. Inner Ear Outer Ear Pinna: >Visible part of ear and ear canal -Acts as a funnel to direct sound Eardrum: >Airtight membrane
Hearing By Jack & Tori 3 Main Components of the Human Ear. Outer Ear. Middle Ear. Inner Ear Outer Ear Pinna: >Visible part of ear and ear canal -Acts as a funnel to direct sound Eardrum: >Airtight membrane
HEARING. Structure and Function
 HEARING Structure and Function Rory Attwood MBChB,FRCS Division of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch Analyse Function of auditory system Discriminate
HEARING Structure and Function Rory Attwood MBChB,FRCS Division of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch Analyse Function of auditory system Discriminate
Perception of Sound. To hear sound, your ear has to do three basic things:
 Perception of Sound Your ears are extraordinary organs. They pick up all the sounds around you and then translate this information into a form your brain can understand. One of the most remarkable things
Perception of Sound Your ears are extraordinary organs. They pick up all the sounds around you and then translate this information into a form your brain can understand. One of the most remarkable things
Assisting in Otolaryngology
 Assisting in Otolaryngology Learning Objectives Identify the structures and explain the functions of the external, middle, and internal ear. Describe the conditions that can lead to hearing loss, including
Assisting in Otolaryngology Learning Objectives Identify the structures and explain the functions of the external, middle, and internal ear. Describe the conditions that can lead to hearing loss, including
THE COCHLEA AND AUDITORY PATHWAY
 Dental Neuroanatomy Suzanne S. Stensaas, PhD April 14, 2010 Reading: Waxman, Chapter 16, Review pictures in a Histology book Computer Resources: http://www.cochlea.org/ - Promenade around the Cochlea HyperBrain
Dental Neuroanatomy Suzanne S. Stensaas, PhD April 14, 2010 Reading: Waxman, Chapter 16, Review pictures in a Histology book Computer Resources: http://www.cochlea.org/ - Promenade around the Cochlea HyperBrain
Learning Targets. Module 20. Hearing Explain how the ear transforms sound energy into neural messages.
 Learning Targets Module 20 Hearing 20-1 Describe the characteristics of air pressure waves that we hear as sound. 20-2 Explain how the ear transforms sound energy into neural messages. 20-3 Discuss how
Learning Targets Module 20 Hearing 20-1 Describe the characteristics of air pressure waves that we hear as sound. 20-2 Explain how the ear transforms sound energy into neural messages. 20-3 Discuss how
Before we talk about the auditory system we will talk about the sound and waves
 The Auditory System PHYSIO: #3 DR.LOAI ZAGOUL 24/3/2014 Refer to the slides for some photos. Before we talk about the auditory system we will talk about the sound and waves All waves have basic characteristics:
The Auditory System PHYSIO: #3 DR.LOAI ZAGOUL 24/3/2014 Refer to the slides for some photos. Before we talk about the auditory system we will talk about the sound and waves All waves have basic characteristics:
The Ear. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 The Ear Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology The Ear The ear consists of the external ear; the middle ear (tympanic cavity); and the internal ear (labyrinth), which contains
The Ear Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology The Ear The ear consists of the external ear; the middle ear (tympanic cavity); and the internal ear (labyrinth), which contains
What is the effect on the hair cell if the stereocilia are bent away from the kinocilium?
 CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
The Sense Organs 10/13/2016. The Human Eye. 1. Sclera 2. Choroid 3. Retina. The eye is made up of three layers:
 The human body gathers information from the outside world by using the five senses of: The Sense Organs 12.3 Sight Hearing Taste Smell Touch This information is essential in helping the body maintain homeostasis.
The human body gathers information from the outside world by using the five senses of: The Sense Organs 12.3 Sight Hearing Taste Smell Touch This information is essential in helping the body maintain homeostasis.
BCS 221: Auditory Perception BCS 521 & PSY 221
 BCS 221: Auditory Perception BCS 521 & PSY 221 Time: MW 10:25 11:40 AM Recitation: F 10:25 11:25 AM Room: Hutchinson 473 Lecturer: Dr. Kevin Davis Office: 303E Meliora Hall Office hours: M 1 3 PM kevin_davis@urmc.rochester.edu
BCS 221: Auditory Perception BCS 521 & PSY 221 Time: MW 10:25 11:40 AM Recitation: F 10:25 11:25 AM Room: Hutchinson 473 Lecturer: Dr. Kevin Davis Office: 303E Meliora Hall Office hours: M 1 3 PM kevin_davis@urmc.rochester.edu
The cochlea: auditory sense. The cochlea: auditory sense
 Inner ear apparatus 1- Vestibule macula and sacculus sensing acceleration of the head and direction of gravity 2- Semicircular canals mainly for sensing direction of rotation of the head 1 3- cochlea in
Inner ear apparatus 1- Vestibule macula and sacculus sensing acceleration of the head and direction of gravity 2- Semicircular canals mainly for sensing direction of rotation of the head 1 3- cochlea in
Taste buds Gustatory cells extend taste hairs through a narrow taste pore
 The Special Senses Objectives Describe the sensory organs of smell, and olfaction. Identify the accessory and internal structures of the eye, and explain their function. Explain how light stimulates the
The Special Senses Objectives Describe the sensory organs of smell, and olfaction. Identify the accessory and internal structures of the eye, and explain their function. Explain how light stimulates the
SPECIAL SENSES: THE AUDITORY SYSTEM
 SPECIAL SENSES: THE AUDITORY SYSTEM REVISION OF PHYSICS: WAVES A wave is an oscillation of power, sound waves have two main characteristics: amplitude, which is the maximum displacement or the power of
SPECIAL SENSES: THE AUDITORY SYSTEM REVISION OF PHYSICS: WAVES A wave is an oscillation of power, sound waves have two main characteristics: amplitude, which is the maximum displacement or the power of
Auditory Physiology PSY 310 Greg Francis. Lecture 29. Hearing
 Auditory Physiology PSY 310 Greg Francis Lecture 29 A dangerous device. Hearing The sound stimulus is changes in pressure The simplest sounds vary in: Frequency: Hertz, cycles per second. How fast the
Auditory Physiology PSY 310 Greg Francis Lecture 29 A dangerous device. Hearing The sound stimulus is changes in pressure The simplest sounds vary in: Frequency: Hertz, cycles per second. How fast the
PSY 310: Sensory and Perceptual Processes 1
 Auditory Physiology PSY 310 Greg Francis Lecture 29 A dangerous device. Hearing The sound stimulus is changes in pressure The simplest sounds vary in: Frequency: Hertz, cycles per second. How fast the
Auditory Physiology PSY 310 Greg Francis Lecture 29 A dangerous device. Hearing The sound stimulus is changes in pressure The simplest sounds vary in: Frequency: Hertz, cycles per second. How fast the
Hearing: the function of the outer, the middle and inner ear. Hearing tests. The auditory pathways
 Hearing: the function of the outer, the middle and inner ear. Hearing tests. The auditory pathways Dr. Gabriella Kékesi 74. Hearing: the function of the outer, the middle and inner ear. Hearing tests.
Hearing: the function of the outer, the middle and inner ear. Hearing tests. The auditory pathways Dr. Gabriella Kékesi 74. Hearing: the function of the outer, the middle and inner ear. Hearing tests.
Chapter Fourteen. The Hearing Mechanism. 1. Introduction.
 Chapter Fourteen The Hearing Mechanism 1. Introduction. 2. Hearing. 3. The Ear. 4. The External Ear. 5. The Inner Ear. 6. Frequency Discrimination. 7. The Organ of Corti. 8. Tests and Exrecises. 9. References.
Chapter Fourteen The Hearing Mechanism 1. Introduction. 2. Hearing. 3. The Ear. 4. The External Ear. 5. The Inner Ear. 6. Frequency Discrimination. 7. The Organ of Corti. 8. Tests and Exrecises. 9. References.
ID# Exam 2 PS 325, Fall 2003
 ID# Exam 2 PS 325, Fall 2003 As always, the Honor Code is in effect and you ll need to write the code and sign it at the end of the exam. Read each question carefully and answer it completely. Although
ID# Exam 2 PS 325, Fall 2003 As always, the Honor Code is in effect and you ll need to write the code and sign it at the end of the exam. Read each question carefully and answer it completely. Although
Sound. Audition. Physics of Sound. Properties of sound. Perception of sound works the same way as light.
 Sound Audition Perception of sound works the same way as light. Have receptors to convert a physical stimulus to action potentials Action potentials are organized in brain structures You apply some meaning
Sound Audition Perception of sound works the same way as light. Have receptors to convert a physical stimulus to action potentials Action potentials are organized in brain structures You apply some meaning
Audition. Sound. Physics of Sound. Perception of sound works the same way as light.
 Audition Sound Perception of sound works the same way as light. Have receptors to convert a physical stimulus to action potentials Action potentials are organized in brain structures You apply some meaning
Audition Sound Perception of sound works the same way as light. Have receptors to convert a physical stimulus to action potentials Action potentials are organized in brain structures You apply some meaning
SPECIAL SENSES PART I: OLFACTION & GUSTATION
 SPECIAL SENSES PART I: OLFACTION & GUSTATION 5 Special Senses Olfaction Gustation Vision Equilibrium Hearing Olfactory Nerves Extend through cribriform plate into nasal cavity on both sides of nasal septum
SPECIAL SENSES PART I: OLFACTION & GUSTATION 5 Special Senses Olfaction Gustation Vision Equilibrium Hearing Olfactory Nerves Extend through cribriform plate into nasal cavity on both sides of nasal septum
Copyright 2009 Pearson Education, Inc.
 Outline Nervous System Sensory Systems I. II. III. IV. V. VI. Biol 105 Lecture 11 Chapter 9 Senses Sensory receptors Touch Vision Hearing and balance Smell Senses Sensory receptor cells Sensory receptors
Outline Nervous System Sensory Systems I. II. III. IV. V. VI. Biol 105 Lecture 11 Chapter 9 Senses Sensory receptors Touch Vision Hearing and balance Smell Senses Sensory receptor cells Sensory receptors
Glossary For Parents. Atresia: closure of the ear canal or absence of an ear opening.
 Glossary For Parents This is not a complete or comprehensive glossary of audiologic and medical terms. It does include many technical and often unfamiliar terms that parents may hear used in connection
Glossary For Parents This is not a complete or comprehensive glossary of audiologic and medical terms. It does include many technical and often unfamiliar terms that parents may hear used in connection
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR.
 The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
A&P 1. Ear, Hearing & Equilibrium Lab. Basic Concepts. These notes follow Carl s Talk at the beginning of lab
 A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts These notes follow Carl s Talk at the beginning of lab In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE:
A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts These notes follow Carl s Talk at the beginning of lab In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE:
The Outer and Middle Ear PERIPHERAL AUDITORY SYSTEM HOW WE HEAR. The Ear in Action AUDITORY NEUROPATHY: A CLOSER LOOK. The 3 parts of the ear
 AUDITORY NEUROPATHY: A CLOSER LOOK HOW WE HEAR The 3 parts of the ear The ear consists of three main parts: 1. The outer ear The part you see, which is called the auricle (ohr-a-kal). 2. The middle ear
AUDITORY NEUROPATHY: A CLOSER LOOK HOW WE HEAR The 3 parts of the ear The ear consists of three main parts: 1. The outer ear The part you see, which is called the auricle (ohr-a-kal). 2. The middle ear
Unit VIII Problem 9 Anatomy of The Ear
 Unit VIII Problem 9 Anatomy of The Ear - The ear is an organ with 2 functions: Hearing. Maintenance of equilibrium/balance. - The ear is divided into 3 parts: External ear. Middle ear (which is also known
Unit VIII Problem 9 Anatomy of The Ear - The ear is an organ with 2 functions: Hearing. Maintenance of equilibrium/balance. - The ear is divided into 3 parts: External ear. Middle ear (which is also known
THE EAR Dr. Lily V. Hughes, Audiologist
 WHY AM I HERE? HEARING & THE BRAIN THE EAR Dr. Lily V. Hughes, Audiologist Fairbanks Hearing & Balance Center at the ENT Clinic 1 out of every 5 adults has hearing loss. That s more than 48 million people
WHY AM I HERE? HEARING & THE BRAIN THE EAR Dr. Lily V. Hughes, Audiologist Fairbanks Hearing & Balance Center at the ENT Clinic 1 out of every 5 adults has hearing loss. That s more than 48 million people
Chapter 3: Anatomy and physiology of the sensory auditory mechanism
 Chapter 3: Anatomy and physiology of the sensory auditory mechanism Objectives (1) Anatomy of the inner ear Functions of the cochlear and vestibular systems Three compartments within the cochlea and membranes
Chapter 3: Anatomy and physiology of the sensory auditory mechanism Objectives (1) Anatomy of the inner ear Functions of the cochlear and vestibular systems Three compartments within the cochlea and membranes
photo courtesy of Oticon Glossary
 photo courtesy of Oticon Glossary 404.591.1884 www.childrensent.com American Sign Language (ASL): a manual language with its own word order and grammar, used primarily by people who are Deaf. Atresia (aural):
photo courtesy of Oticon Glossary 404.591.1884 www.childrensent.com American Sign Language (ASL): a manual language with its own word order and grammar, used primarily by people who are Deaf. Atresia (aural):
Series Preface. Preface. Acknowledgments. Abbreviations
 Contents Series Preface Preface Acknowledgments Abbreviations vii ix xiii xxv Introduction xxxi Definition...xxxi Normal Hearing...xxxi Deafness...xxxi Overall Concept of the Bionic Ear...xxxii Training
Contents Series Preface Preface Acknowledgments Abbreviations vii ix xiii xxv Introduction xxxi Definition...xxxi Normal Hearing...xxxi Deafness...xxxi Overall Concept of the Bionic Ear...xxxii Training
Sound Waves. Sensation and Perception. Sound Waves. Sound Waves. Sound Waves
 Sensation and Perception Part 3 - Hearing Sound comes from pressure waves in a medium (e.g., solid, liquid, gas). Although we usually hear sounds in air, as long as the medium is there to transmit the
Sensation and Perception Part 3 - Hearing Sound comes from pressure waves in a medium (e.g., solid, liquid, gas). Although we usually hear sounds in air, as long as the medium is there to transmit the
Assistive Technology Project. Presented By: Rose Aldan
 Assistive Technology Project Presented By: Rose Aldan Hearing Aid How Your Ear Works An auditory wonder Your ears appear to be relatively simple structures. But they are, in fact, only part of the complex
Assistive Technology Project Presented By: Rose Aldan Hearing Aid How Your Ear Works An auditory wonder Your ears appear to be relatively simple structures. But they are, in fact, only part of the complex
Chapter 7. Audition, the Body Senses, and the Chemical Senses. Copyright Allyn & Bacon 2004
 Chapter 7 Audition, the Body Senses, and the Chemical Senses This multimedia product and its contents are protected under copyright law. The following are prohibited by law: any public performance or display,
Chapter 7 Audition, the Body Senses, and the Chemical Senses This multimedia product and its contents are protected under copyright law. The following are prohibited by law: any public performance or display,
2 Background. 2.1 The Hearing Sense
 2 Background 2.1 The Hearing Sense People hear by detecting sounds vibration. Hearing is one of the five senses (sight, hearing, taste, smell, and touch) that humans possess. The human ear consists of
2 Background 2.1 The Hearing Sense People hear by detecting sounds vibration. Hearing is one of the five senses (sight, hearing, taste, smell, and touch) that humans possess. The human ear consists of
9.01 Introduction to Neuroscience Fall 2007
 MIT OpenCourseWare http://ocw.mit.edu 9.01 Introduction to Neuroscience Fall 2007 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms. 9.01 Recitation (R02)
MIT OpenCourseWare http://ocw.mit.edu 9.01 Introduction to Neuroscience Fall 2007 For information about citing these materials or our Terms of Use, visit: http://ocw.mit.edu/terms. 9.01 Recitation (R02)
Sound and Hearing. Decibels. Frequency Coding & Localization 1. Everything is vibration. The universe is made of waves.
 Frequency Coding & Localization 1 Sound and Hearing Everything is vibration The universe is made of waves db = 2log(P1/Po) P1 = amplitude of the sound wave Po = reference pressure =.2 dynes/cm 2 Decibels
Frequency Coding & Localization 1 Sound and Hearing Everything is vibration The universe is made of waves db = 2log(P1/Po) P1 = amplitude of the sound wave Po = reference pressure =.2 dynes/cm 2 Decibels
Sound and its characteristics. The decibel scale. Structure and function of the ear. Békésy s theory. Molecular basis of hair cell function.
 Hearing Sound and its characteristics. The decibel scale. Structure and function of the ear. Békésy s theory. Molecular basis of hair cell function. 19/11/2014 Sound A type of longitudinal mass wave that
Hearing Sound and its characteristics. The decibel scale. Structure and function of the ear. Békésy s theory. Molecular basis of hair cell function. 19/11/2014 Sound A type of longitudinal mass wave that
Hearing and Balance 1
 Hearing and Balance 1 Slide 3 Sound is produced by vibration of an object which produces alternating waves of pressure and rarefaction, for example this tuning fork. Slide 4 Two characteristics of sound
Hearing and Balance 1 Slide 3 Sound is produced by vibration of an object which produces alternating waves of pressure and rarefaction, for example this tuning fork. Slide 4 Two characteristics of sound
The ear: some applied basic science
 Chapter 1 The ear: some applied basic science The pinna The external ear or pinna is composed of cartilage with closely adherent perichondrium and skin. It is developed from six tubercles of the first
Chapter 1 The ear: some applied basic science The pinna The external ear or pinna is composed of cartilage with closely adherent perichondrium and skin. It is developed from six tubercles of the first
BIOMATERIALS AND COCHLEAR IMPLANTS
 BIOMATERIALS AND COCHLEAR IMPLANTS Attia Qamar & Paolo Sabatini 1 EAR ANATOMY & MECHANICS vestibule Bony Labyrinth Coclear Duct CN VIII Vibration Tympanic Membrane Middle Ear Perilymph From oval window
BIOMATERIALS AND COCHLEAR IMPLANTS Attia Qamar & Paolo Sabatini 1 EAR ANATOMY & MECHANICS vestibule Bony Labyrinth Coclear Duct CN VIII Vibration Tympanic Membrane Middle Ear Perilymph From oval window
Ganglion Cells Blind Spot Cornea Pupil Visual Area of the Bipolar Cells Thalamus Rods and Cones Lens Visual cortex of the occipital lobe
 How We See How We See Cornea Ganglion Cells whose axons form the optic nerve Blind Spot the exit point at the back of the retina Pupil which is controlled by the iris Bipolar Cells Visual Area of the Thalamus
How We See How We See Cornea Ganglion Cells whose axons form the optic nerve Blind Spot the exit point at the back of the retina Pupil which is controlled by the iris Bipolar Cells Visual Area of the Thalamus
ID# Final Exam PS325, Fall 1997
 ID# Final Exam PS325, Fall 1997 Good luck on this exam. Answer each question carefully and completely. Keep your eyes foveated on your own exam, as the Skidmore Honor Code is in effect (as always). Have
ID# Final Exam PS325, Fall 1997 Good luck on this exam. Answer each question carefully and completely. Keep your eyes foveated on your own exam, as the Skidmore Honor Code is in effect (as always). Have
(Thomas Lenarz) Ok, thank you, thank you very much for inviting me to be here and speak to you, on cochlear implant technology.
 Ok, thank you, thank you very much for inviting me to be here and speak to you, on cochlear implant technology.") (Thomas Lenarz) Ok, thank you, thank you very much for inviting me to be here and speak to you, on cochlear implant technology. I want to briefly mention what hearing loss is. And what a cochlear implant
(Thomas Lenarz) Ok, thank you, thank you very much for inviting me to be here and speak to you, on cochlear implant technology. I want to briefly mention what hearing loss is. And what a cochlear implant
Your ear consists of three parts that play a vital role in hearing-the external ear, middle ear, and inner ear.
 What is a Cochlear Implant? A cochlear implant is an electronic device that restores partial hearing to the deaf. It is surgically implanted in the inner ear and activated by a device worn outside the
What is a Cochlear Implant? A cochlear implant is an electronic device that restores partial hearing to the deaf. It is surgically implanted in the inner ear and activated by a device worn outside the
Activity 1: Anatomy of the Eye and Ear Lab
 Activity 1: Anatomy of the Eye and Ear Lab 1. Launch the view! Launch Human Anatomy Atlas. Navigate to Quizzes/Lab Activities, find the Eye and Ear Lab section. Launch Augmented Reality mode and scan the
Activity 1: Anatomy of the Eye and Ear Lab 1. Launch the view! Launch Human Anatomy Atlas. Navigate to Quizzes/Lab Activities, find the Eye and Ear Lab section. Launch Augmented Reality mode and scan the
HEARING GUIDE PREPARED FOR CLINICAL PROFESSIONALS HEARING.HEALTH.MIL. HCE_ClinicalProvider-Flip_FINAL01.indb 1
 HEARING GUIDE PREPARED FOR CLINICAL PROFESSIONALS HCE_ClinicalProvider-Flip_FINAL01.indb 1 TEMPORAL MUSCLE TEMPORAL BONE EXTERNAL AUDITORY CANAL MALLEUS INCUS STAPES SEMICUIRCULAR CANALS COCHLEA VESTIBULAR
HEARING GUIDE PREPARED FOR CLINICAL PROFESSIONALS HCE_ClinicalProvider-Flip_FINAL01.indb 1 TEMPORAL MUSCLE TEMPORAL BONE EXTERNAL AUDITORY CANAL MALLEUS INCUS STAPES SEMICUIRCULAR CANALS COCHLEA VESTIBULAR
Carlson (7e) PowerPoint Lecture Outline Chapter 7: Audition, the Body Senses, and the Chemical Senses
 PowerPoint Lecture Outline Chapter 7: Audition, the Body Senses, and the Chemical Senses") Carlson (7e) PowerPoint Lecture Outline Chapter 7: Audition, the Body Senses, and the Chemical Senses This multimedia product and its contents are protected under copyright law. The following are prohibited
Carlson (7e) PowerPoint Lecture Outline Chapter 7: Audition, the Body Senses, and the Chemical Senses This multimedia product and its contents are protected under copyright law. The following are prohibited
DIAGNOSIS Causes/Etiology of Hearing Loss
 DIAGNOSIS Causes/Etiology of Hearing Loss DIAGNOSIS Causes/Etiology of Hearing Loss VI. How Do We Hear? Sound waves enter our ears and are amplified by the ear drum and middle ear bones (ossicles), allowing
DIAGNOSIS Causes/Etiology of Hearing Loss DIAGNOSIS Causes/Etiology of Hearing Loss VI. How Do We Hear? Sound waves enter our ears and are amplified by the ear drum and middle ear bones (ossicles), allowing
The Ear. The ear can be divided into three major parts: the outer ear, the middle ear and the inner ear.
 The Ear The ear can be divided into three major parts: the outer ear, the middle ear and the inner ear. The Ear There are three components of the outer ear: Pinna: the fleshy outer part of the ear which
The Ear The ear can be divided into three major parts: the outer ear, the middle ear and the inner ear. The Ear There are three components of the outer ear: Pinna: the fleshy outer part of the ear which
INTRODUCTION TO AUDIOLOGY Hearing Balance Tinnitus - Treatment
 INTRODUCTION TO AUDIOLOGY Hearing Balance Tinnitus - Treatment What is Audiology? Audiology refers to the SCIENCE OF HEARING AND THE STUDY OF THE AUDITORY PROCESS (Katz, 1986) Audiology is a health-care
INTRODUCTION TO AUDIOLOGY Hearing Balance Tinnitus - Treatment What is Audiology? Audiology refers to the SCIENCE OF HEARING AND THE STUDY OF THE AUDITORY PROCESS (Katz, 1986) Audiology is a health-care
Senses and Sense Organs
 Senses and Sense Organs SENSORY SYSTEMS Human experience is effected by both internal and external stimuli. Humans are able to distinguish among many different types of stimuli by means of a highly developed
Senses and Sense Organs SENSORY SYSTEMS Human experience is effected by both internal and external stimuli. Humans are able to distinguish among many different types of stimuli by means of a highly developed
Νευροφυσιολογία και Αισθήσεις
 Biomedical Imaging & Applied Optics University of Cyprus Νευροφυσιολογία και Αισθήσεις Διάλεξη 11 Ακουστικό και Αιθουσιαίο Σύστημα (Auditory and Vestibular Systems) Introduction Sensory Systems Sense of
Biomedical Imaging & Applied Optics University of Cyprus Νευροφυσιολογία και Αισθήσεις Διάλεξη 11 Ακουστικό και Αιθουσιαίο Σύστημα (Auditory and Vestibular Systems) Introduction Sensory Systems Sense of
The speed at which it travels is a function of the density of the conducting medium.
 Sound is a compression wave which (unlike light) must have a medium to conduct it. If the medium is uniform in density, the sound will spread at as a uniform ring of circles (actually spheres). The speed
Sound is a compression wave which (unlike light) must have a medium to conduct it. If the medium is uniform in density, the sound will spread at as a uniform ring of circles (actually spheres). The speed
Manchester Adult Cochlear Implant Programme
 Manchester Royal Infirmary Manchester Adult Cochlear Implant Programme Information for Patients and Professionals Contents Introduction 3 The normal ear 4 The cochlear implant 5 The assessment procedure
Manchester Royal Infirmary Manchester Adult Cochlear Implant Programme Information for Patients and Professionals Contents Introduction 3 The normal ear 4 The cochlear implant 5 The assessment procedure
Converting Sound Waves into Neural Signals, Part 1. What happens to initiate neural signals for sound?
 The Ear Outer Ear: Pinna. Collects sounds. Middle Ear: Chamber between eardrum and cochlea containing three tiny bones (hammer, anvil, stirrup) that concentrate the vibrations of the eardrum on the cochlea
The Ear Outer Ear: Pinna. Collects sounds. Middle Ear: Chamber between eardrum and cochlea containing three tiny bones (hammer, anvil, stirrup) that concentrate the vibrations of the eardrum on the cochlea
PSY 214 Lecture 16 (11/09/2011) (Sound, auditory system & pitch perception) Dr. Achtman PSY 214
 (Sound, auditory system & pitch perception) Dr. Achtman PSY 214") PSY 214 Lecture 16 Topic: Sound, auditory system, & pitch perception Chapter 11, pages 268-288 Corrections: None needed Announcements: At the beginning of class, we went over some demos from the virtual
PSY 214 Lecture 16 Topic: Sound, auditory system, & pitch perception Chapter 11, pages 268-288 Corrections: None needed Announcements: At the beginning of class, we went over some demos from the virtual
Hearing. PSYCHOLOGY (8th Edition, in Modules) David Myers. Module 14. Hearing. Hearing
 David Myers. Module 14. Hearing. Hearing") PSYCHOLOGY (8th Edition, in Modules) David Myers PowerPoint Slides Aneeq Ahmad Henderson State University Worth Publishers, 2007 1 Hearing Module 14 2 Hearing Hearing The Stimulus Input: Sound Waves The
PSYCHOLOGY (8th Edition, in Modules) David Myers PowerPoint Slides Aneeq Ahmad Henderson State University Worth Publishers, 2007 1 Hearing Module 14 2 Hearing Hearing The Stimulus Input: Sound Waves The
THE MECHANICS OF HEARING
 CONTENTS The mechanics of hearing Hearing loss and the Noise at Work Regulations Loudness and the A weighting network Octave band analysis Hearing protection calculations Worked examples and self assessed
CONTENTS The mechanics of hearing Hearing loss and the Noise at Work Regulations Loudness and the A weighting network Octave band analysis Hearing protection calculations Worked examples and self assessed
COM3502/4502/6502 SPEECH PROCESSING
 COM3502/4502/6502 SPEECH PROCESSING Lecture 4 Hearing COM3502/4502/6502 Speech Processing: Lecture 4, slide 1 The Speech Chain SPEAKER Ear LISTENER Feedback Link Vocal Muscles Ear Sound Waves Taken from:
COM3502/4502/6502 SPEECH PROCESSING Lecture 4 Hearing COM3502/4502/6502 Speech Processing: Lecture 4, slide 1 The Speech Chain SPEAKER Ear LISTENER Feedback Link Vocal Muscles Ear Sound Waves Taken from: