Early Hearing Detection and Intervention How You Matter! Laura Davis-Keppen, MD SD AAP EHDI Champion Professor of Pediatrics, USD
|
|
|
- Scot Garrison
- 6 years ago
- Views:
Transcription
1 Early Hearing Detection and Intervention How You Matter! Laura Davis-Keppen, MD SD AAP EHDI Champion Professor of Pediatrics, USD Jessica J Messersmith, PhD, CCC-A, FAAA Associate Professor of Audiology, USD Pediatric and Cochlear Implant Audiologist
2 Why is early identification of hearing loss important? Hearing loss is the most common birth condition Previous methods for detecting hearing loss have been ineffective Undetected hearing loss can delay speech, language, social & academic development
3 Hearing in Children Hearing loss is the most common birth abnormality About 2 or 3 out of every 1000 children in the United States are born deaf or hard-of-hearing (NIDCD, 2013) ~ 12,000 per year ~ Another 4,000 to 6,000 infants and children are identified with hearing loss by age 3 years (NIDCD, 2013) Incidence per 10,000 of Congenital Defects/Diseases
4 Identification is crucial Hearing is necessary to grow neural connections throughout the brain Crucial for development of spoken language, reading, and auditory learning [Gordon, Papsin, and Harrison, 2004] Even those with profound HL can achieve auditory brain access through use of current technology Allows developmental model of intervention rather than re/habilitative
5 Early identification is critical Children identified before 6 months of age have better developmental outcomes than those identified later (Yoshinaga-Itano et al., 1998) Expressive and receptive language skills Regardless of degree of hearing loss Higher vocabulary and verbal reasoning skills at age 5 for those children with hearing loss who began intervention by 11 months of age compared to children who began intervention later (Moeller, 2000)

6 Neural projections are impacted Gilley, Sharma, & Dorman, 2008 Left image: NH children: bilateral activation of the auditory cortical areas (superior temporal sulcus and inferior temporal gyrus) Middle image: early treatment: activation of the auditory cortical areas contralateral to their CI Right image: late treatment: activation outside the auditory cortical areas (in the visual, insula, and parietotemporal areas)
7 Newborn Hearing Screening Considerations for implementing universal screening (World Health Organization) Is the problem significant? To the individual To society Yes! Is there good evidence on an effective treatment once the problem is detected? Has the screening test been properly evaluated and shown to be appropriate in the setting where the screening is to be performed? Is there evidence that a screening program that leads to treatment is of greater benefit than waiting until symptoms develop? Have cost issues been considered and developed? Are there plausible strategies and sufficient resources to ensure implementation? Yes! Yes! Yes! Yes! Yes!
8 Previous methods for detecting hearing loss have been ineffective High risk screening failed to identify ~ 50% of the infants with hearing loss Large retrospective cohort study5, 6: mean age of diagnosis 21.6 months Similar findings reported in US7,8,9
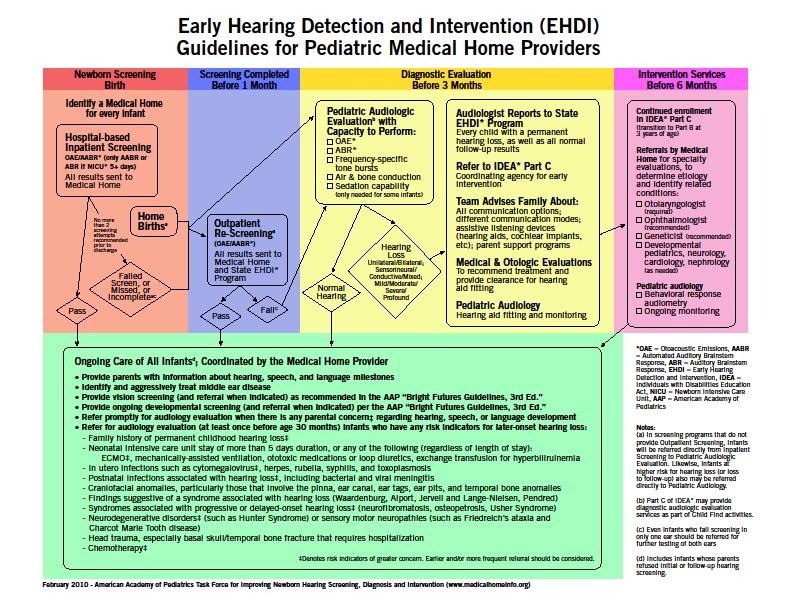
9 EHDI: EARLY HEARING LOSS DETECTION AND INTERVENTION The process
10 Early Identification of Hearing Loss- Method Screening No later than 1 month of age Diagnostic testing with Pediatric Audiologist No later than 3 months of age Early Intervention No later than 6 months of age 1:3:6


11 Screening method AABR More $$$ than OAE Sensitive to more types of HL Needed if baby in NICU >5 days OAE Less $$$ than AABR Faster than AABR Not sensitive to all types of HL Can obtain invalid results from both if obstruction in middle or outer ear (e.g. fluid or vernix)
12 2007 JCIH Position on Screening2 NICU >5 days in NICU ABR should be included to screen for neural loss Rescreen BOTH ears, even if only one ear fails Non pass refer to Audiologist Readmission rescreen before discharge Well baby nursery Screen with OAE or ABR Repeat screen when necessary before discharge When using 2 step protocol test order should be OAE then ABR Rescreen BOTH ears, even if only one ear doesn t pass
13 Does UNHS Improve the Age of Identification and Intervention? Prior to UNHS (Harrison and Roush, 1996) Median age of identification without risk factors was 13 months for severe-to-profound SNHL Median age of identification with risk factors was 12 months for severe-to-profound SNHL After UNHS (NY State, 2000) Median age of identification was 3 months EHDI 10 years later- (Holte et al., 2012) only 32% children included in NIH OCHL study met all of the benchmarks
14 What is the role of the provider and nurse? Initial hospital Pass No pass Discuss results Facilitate visit for rescreen Like any newborn screen, the initial screen is not diagnostic
15 What is the role of the provider and nurse? Initial hospital Pass No pass Ensure that family understands that a pass does not mean that a HL will not be dx later on Children who pass UNHS but have risk factor should have at least one dx audiology assessment by months of age (JCIH, 2007)
16 What is the role of the provider and nurse? Initial hospital Pass No pass Rescreen Pass No Pass Connect infants to audiologic follow-up

17 Who is an audiologist? Audiologist are the primary health care professional who diagnose, treat, and manage hearing loss, tinnitus, and/or balance disorders. Doctoral level education Licensure requirements Certification

18 Only refer infants to a pediatric audiologist

19 A pediatric audiologist is best equipped to diagnose hearing loss in infants/children Detailed history Diagnostic evaluation using a test battery No one single test can identify the type, degree, and configuration of HL Otoscopy Immitance Physiologic Behavioral Counsel parents
20 Treatment plan Mode of communication is parent(s) choice If spoken- pursue amplification ASAP (pediatric audiologist) No age limit on fitting amplification Cochlear Implant Center should be involved in those case of severe or greater HL, bacterial meningitis, ANSD, those demonstrating limited benefit from amplification If sign- connect family with sign support
21 What is the role of the provider and nurse? No Dx HL Audiologist Dx HL Talk with family about results Review family history and examine child for craniofacial abnormalities or syndromes associated with hearing loss Refer to ENT Refer to ophthalmology Refer for genetic testing/consultation
22 National EHDI Data Universal Newborn Hearing Screening Percent of Infants Receiving Hearing Screening: Percent of Infants
23 2005 (n=44) 2006 (n=47) 2007 (n=44) 2008 (n=48) 2009 (n=49) 2010 (n=52) 2011 (n=50) 2012 (n=55) Infants Identified as Permanently Deaf or Hard Of Hearing, Total = 34,416 7,000 6,000 5,718 National EHDI Data Incidence of Children who are Deaf or Hard of Hearing 5,000 4,000 3,000 2,000 1, ,054 3,430 3,261 2,634 5,103 5,046 5,170 Year
24 2012 National CDC EHDI Data % Screened: 96.6% (n=3,820,624) Prevalence of children who are deaf/hh: 1.6 per 1,000 screened (Range per 1,000) % of those identified receiving Early Intervention: 61.7% (n=3,527) % Screened before 1 month of age: 86.0% (n=3,287,614) % Diagnosed before 3 months of age: 69.1% (n=20,102) % Receiving Intervention before 6 months of age: 67.1% (n=2,367) % Loss to Follow-up or Documentation: 35.9% (n=19,006)
25 2012 South Dakota EHDI Data % Screened: 97% (n=12,722), 96.4% by 1 month Rescreened 65% Audiologist by 3 months 77.7% Birth to 3 only 18.75% 33.4% of South Dakota s newborns who should have been rescreened did not have hearing evaluated. Based on national data 68.6% of SD infants who were deaf/hh did not receive early diagnosis and intervention. Early intervention should be considered a developmental emergency. Children identified as deaf/hh who begin services before 6 months develop language (spoken or signed) on a par with their hearing peers. 86.8% loss to follow-up/loss of documentation

26 The Role of Medical Home Early Hearing Detection and Intervention The medical home plays a key role in the success of EHDI programs. A medical home can help families understand the EHDI process. The medical home ensures that appropriate and timely steps are taken to identify children who are deaf/hh and get them into an early intervention program. The medical home serves as the primary coordinating entity which can help significantly reduce loss to followup/documentation.
27 Medical Home: Strategies to Promote Follow Up At prenatal visit, encourage families to identify you as follow-up care location Inform hospital to facilitate communication of results Provide checkbox on newborn well child form/patient chart for hearing screening results & risk factors AAP: The primary care provider must assume responsibility to ensure that audiological assessment is conducted on infants who do not pass screening and must initiate referral for medical specialty evaluations necessary to determine the etiology of the hearing loss. Set up tracking system for infants who do not pass hearing screening.
28 Counseling Parents Effective communication of results to families has an influence on follow up behaviors Balance between reassurance and importance of follow up testing Your infant may or may not have a hearing loss but let s be sure about it. If further testing shows hearing loss, the earlier we get started helping the child, the better.
29 Optimal Surveillance in the Medical Home (JCIH, 2007) 2 If hearing loss is diagnosed, refer siblings of infant for audiological evaluation Refer infants with any RISK indicators for audiological assessment by months of age Carefully assess middle ear status at all well child visits; refer for otologic evaluation if persistent middle ear effusion lasts for > 3 months
30 Risk Indicators of Delayed Onset or Progressive Hearing Loss Caregiver concerns* about hearing, speech, language, development Family history* of permanent childhood hearing loss NICU stay > 5 days or any of following (regardless of length of stay): ECMO assisted ventilation* Ototoxic medications (gentamycin, tobramycin) Loop diuretics (furosemide, Lasix) Hyperbilirubinemia requiring exchange transfusion JCIH, 2007
31 Risk Indicators for permanent congenital, delayed onset or progressive hearing loss 2 In Utero infections CMV*, herpes, rubella, syphilis, toxoplasmosis Craniofacial anomalies Physical findings (e.g. white forelock) Syndromes* involving hearing loss Neurofibromatosis, osteopetrosis, Usher, Waardenburg, Alport, Pendred, Jervell & Lange- Nielson * = greater risk for delayed onset HL
32 Risk Indicators for permanent congenital, delayed onset or progressive hearing loss2 Neurodegenerative disorders Sensory motor neuropathies (Frieidrich ataxia, Charcot-Marie-Tooth) Culture positive postnatal infections associated with HL* Herpes, varicella, meningitis Head trauma (basal skull, temporal bone)* Chemotherapy* * = greater risk for delayed onset HL
33 Medical Workup Complete prenatal & perinatal history Family Hx of onset of HL < age 30 Physical exam: unusual facial appearance with attention to asymmetry, ear anomalies, neurologic, balance, skeletal, other unusual physical findings Test for CMV as soon as possible, before age 6 weeks. Refer to ENT Refer to Genetics and Ophthalmology As needed: developmental pediatrics, cardiology, neurology

34 Causes of Prelingual Hearing Loss > 40dB



35 Waardenburg Syndrome Abnormal pigmentation of skin and hair Lateral displacement of medial canthi-type I Heterochromia iridis Deafness in some-not always present
36 Branchio-Oto-Renal (BOR) Syndrome Pre-auricular pits 82% Branchial fistulae 49% Cupped or mildly altered auricle 36% Renal abnormalities 67% Hearing loss 93% Mixed 52% Conductive 33% Sensorineural 29% Autosomal Dominant: EYA1 gene (8q13.3) or SIX5 gene (19q13.32)



37

38 Treacher Collins Syndrome Malar hypoplasia Downslanting palpebral fissures Defects of lower lid Malformations of external ear
39 Usher syndrome 3-6% of Children Who Are Deaf or Hard of Hearing Develop retinitis pigmentosa-deterioration of vision Left: Usher syndrome-optic nerve-pale, Vessels (stars) very thin, Characteristic pigment (double arrows)
40 Usher Syndrome Usher Syndrome Type I (70%) Congenital, profound SNHL Childhood onset of retinitis pigmentosa Clumsiness & developmental delay Absent vestibular function Type II (26%) Congenital SNHL, high frequency > low frequency, stable Later onset of retinitis pigmentosa Normal vestibular function Type III (4%) Normal hearing and vision at birth Deterioration of hearing and vision over the years
41 Jervell and Lange-Neilsen Syndrome Prolongation of QT interval on EKG. May develop arrhythmias leading to sudden death Profound sensorineural hearing loss Autosomal recessive inheritance. Due to mutations in the KVLQT1 gene on chromosome 11p15 and KCNE1 gene on chromosome 21q22 potassium channel genes
42 70% of Genetic Hearing Loss is Nonsyndromic DFNB1 locus which includes the GJB2 gene encoding the gap junction protein connexin 26 and GJB6 gene encoding the gap junction protein connexin 30 is the most common cause of AR nonsyndromic HL Next-generation sequencing technologies are replacing single gene-sequencing tests for hearing loss. Advantage: ability to address genetic heterogeneity since many different genes results in phenotypes that cannot be distinguished clinically. Disadvantage: Large deletions and duplications and copy-number and structural variations not as efficiently detected so alternative genetic testing strategies may be necessary
43 Comprehensive Genetic Testing for Hereditary HL Using Massively Parallel Sequencing The most common cause of prelingual-onset SNHL is genetic in developed countries Panels may test for all genes known to cause NSHL, Usher syndrome, and Pendred syndrome using custom-targeted sequence capture for DNA enrichment followed by massively parallel DNA sequencing. All genes sequenced at the same time. The panel we use currently tests for 109 genes known to cause NSHL and some syndromic HL. Total of genes currently tested 116 genes. Cost effective-$1500. Familial mutation testing $200.
44 Targeted Next-Generation Sequencing of Deafness Genes When 30 individuals with nonsyndromic hearing loss were tested using targeted next-gen sequencing, 52% of the probands were diagnosed with monogenic nonsyndromic HL Determining the etiology of HL provides answers: recurrence risk, prognosis (will HL worsen over time), best treatment (cochlear implants or hearing aids), and whether vision will also be later affected.
45 Other Tests/Recommendations CMV recommended as an initial test if the NB hearing screen is not passed. Congenital CMV is a leading cause of hearing lossfound in 30%. CMV testing most diagnostic when done before 3-6 weeks. With increasing age there is a greater likelihood that a +CMV test is due to postnatal exposure. Consider testing for mitochondrial mutations associated with aminoglycoside ototoxicity for individuals with a history of aminoglycoside antibiotics Every infant with confirmed HL should have an evaluation by an ophthalmologist. Temporal bone imagining should be considered if indicated.
46 CMV CMV is the leading cause of nongenetic hearing loss 1/3 of NSHL in young children At birth infant may be asymptomatic or have microcephaly, IUGR, petechiae, hepatosplenomegaly Hearing loss may be fluctuating and progressive Stabilization or improvement of hearing with antiviral tx Test for CMV if initial hearing screen not passed. This testing is mandated in some states.
47 Hearing Screening Myths Misconception vs Clinical Fact Parents can tell if their child has a hearing loss by age 2-3 months Parents/physicians can test for hearing loss by clapping hands or banging pots near the baby Hearing loss risk factor assessments will identify all children with hearing loss Hearing loss if rare, so newborn hearing screening is not necessary There is no rush to identify hearing loss Before NB hearing screening hearing loss not recognized until 2-3 years of age; age 4 if milder Babies who are deaf/hh can still startle to loud noises but may not be able to hear all the sounds important for speech 50% of infants who are deaf/hh have no known risk factors Hearing loss affects 1-3 per 1000 births-the most common condition Identification before 6 mo. can avoid speech and language delays through evidence-based early intervention
48 Hearing Screening Myths Misconception vs Clinical Fact Children younger than 12 months cannot be fitted with hearing aids Newborns can be fit with amplification Babies need to be sedated to complete ABR testing Fluid prevents completion of diagnostic ABR Abnormal OAEs along with a flat tympanogram (normal volume) confirms a conductive hearing loss Babies younger than 3 months can typically be tested without need for sedation Underlying sensory loss can and should be ruled out as soon as possible through use of bone conduction ABR stimuli Diagnostic ABR including bone conduction testing is needed in combinations with OAE and tympanograms for a complete diagnosis of type and degree of hearing loss in each ear.
 system to include results of auditory screening Flag all patient charts for children that require follow-up for hearing screens Flag all")
49 Do listen to parents concerns The Role of Medical Home Encourage prompt follow-up with rescreens and diagnostic evaluations Make sure diagnostic evaluations are done by an audiologist who has experience with infants Set up electronic medical record (EMR) system to include results of auditory screening Flag all patient charts for children that require follow-up for hearing screens Flag all patient charts for children that are at risk for late onset hearing loss

50 Infants identified as deaf or hard of hearing Address the family s concerns Ensure the family is seeing an experienced pediatric audiologist Refer the family to appropriate specialists Otolaryngology, Genetics, Ophthalmology Help the family obtain early intervention services Monitor developmental milestones and ear infections
51 Resources: Early Intervention SDSD (South Dakota School for the Deaf) Birth to 3 Program Parent Physician hi.htm
52
53 1. Identify the correct guidelines for hearing detection and intervention a. Screen hearing no later than 1 month of age, repeat hearing screen by 3 months of age, referral to ENT no later than 6 months of age b. Screen hearing no later than 1 month of age, referral to ENT no later than 3 months of age, enrollment in early intervention if speech delayed c. Screen hearing before hospital discharge, rescreen in the office since middle ear fluid likely, refer to ENT if infant doesn't pass 3 screens d. Screen hearing no later than 1 month of age, diagnostic evaluation for hearing loss no later than 3 months of age, enrollment in early intervention no later than 6 months of age
54 Correct Answer: D. Screen hearing no later than 1 month of age, diagnosis of hearing loss no later than 3 months of age, enrollment in early intervention no later than 6 months of age
55 2. Which of the following statements is incorrect: a. Infants admitted to the NICU for more than 5 days should have an ABR for the hearing screen b. It is not necessary to rescreen hearing if only 1 ear did not pass the initial screening c. At least 1 ABR test is recommended as part of a complete audiology evaluation to confirm hearing loss d. Early intervention services should begin as soon as possible after diagnosis of hearing loss but at no later than 6 months of age.
56 Answer: B. It is not necessary to rescreen hearing if only 1 ear did not pass the initial screening
57 3. If an infant receives a refer on their newborn hearing screening and does not pass an outpatient rescreen what is the next step: a. Refer to ENT b. Repeat the hearing screen again c. Refer to a pediatric audiologist for a full audiologic evaluation d. Check to see if the infant startles to loud noises or clapping.
58 Correct Answer: C. Refer to a pediatric audiologist for a full audiologic evaluation
59 4. What is/are additional recommended evaluations for infants identified with a hearing loss? a. CMV testing in the first month b. Ophthalmology c. Refer to genetics-complete family history, evaluate for syndrome, genetic testing d. All of the above
60 Correct Answer: D. All of the above.
61 5. Which statement is NOT correct: a. If the family is concerned about hearing or communication a repeat hearing test is recommended b. Regular audiologic monitoring is recommended when there has been an NICU stay > 5 days or there is a history of a congenital infection, ECHMO, chemotherapy, or a family history of childhood hearing loss c. Children younger than 12 months cannot be fitted with hearing aids d. It is the primary physician's responsibility to ensure that infants who do not pass the hearing screen receive a diagnostic evaluation by an audiologist, are referred for intervention, and report this to the state EHDI program
62 Answer: C. Children younger than 12 months cannot be fitted with hearing aids
JCIH Recommendations for Following Children At Risk for Hearing Loss
 JCIH Recommendations for Following Children At Risk for Hearing Loss With newborn hearing screening, the Joint Commission on Infant Hearing (JCIH) has recommendations for following children who may be
JCIH Recommendations for Following Children At Risk for Hearing Loss With newborn hearing screening, the Joint Commission on Infant Hearing (JCIH) has recommendations for following children who may be
Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014)
") Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014) Being deaf is a worse handicap than being blind because deafness separates people from people. -Helen Keller Goals of the Newborn
Hearing Loss, Deaf Culture and ASL Interpreters By Laura Jacobsen (4/2014) Being deaf is a worse handicap than being blind because deafness separates people from people. -Helen Keller Goals of the Newborn
Early Hearing Detection and Intervention (EHDI): The Role of the Medical Home
: The Role of the Medical Home") Early Hearing Detection and Intervention (EHDI): The Role of the Medical Home A PRESENTATION FROM THE AMERICAN ACADEMY OF PEDIATRICS Hearing Facts Early identification and intervention of a child who is
Early Hearing Detection and Intervention (EHDI): The Role of the Medical Home A PRESENTATION FROM THE AMERICAN ACADEMY OF PEDIATRICS Hearing Facts Early identification and intervention of a child who is
Disclosures. Objectives 2/29/2016. Bradley Golner M.D. FAAP. AzEHDI chapter champion AAP EHDI leadership team
 Bradley Golner M.D. FAAP AzEHDI chapter champion AAP EHDI leadership team Disclosures HRSA/EHDI Grant compensation as Arizona EHDI program chapter champion and Newborn Screening Partner member Objectives
Bradley Golner M.D. FAAP AzEHDI chapter champion AAP EHDI leadership team Disclosures HRSA/EHDI Grant compensation as Arizona EHDI program chapter champion and Newborn Screening Partner member Objectives
Congenital permanent hearing loss occurs in about 3
 Online Exclusive Problem with baby s hearing? An intervention checklist It s time to make sure infants with positive screens for hearing loss get the follow-up treatment they need and deserve. This tool
Online Exclusive Problem with baby s hearing? An intervention checklist It s time to make sure infants with positive screens for hearing loss get the follow-up treatment they need and deserve. This tool
Guidelines for Primary Care and Medical Home Providers
 EARLY HEARING DETECTION AND INTERVENTION Guidelines for Primary Care and Medical Home Providers Original Publication: April 2009 Last Revision Approved: February 2017 INTRODUCTION This document is intended
EARLY HEARING DETECTION AND INTERVENTION Guidelines for Primary Care and Medical Home Providers Original Publication: April 2009 Last Revision Approved: February 2017 INTRODUCTION This document is intended
3/20/2017. D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital
 D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital Pediatric providers have a reasonable chance to see a child with hearing loss in your
D. Richard Kang, MD, FACS, FAAP Pediatric Otolaryngology Director, ENT Institute Boys Town National Research Hospital Pediatric providers have a reasonable chance to see a child with hearing loss in your
Historical Perspective. JCIH 1973 Position Statement. JCIH Goals. JCIH 1982 Position Statement
 Historical Perspective Effects of Policy Changes on Universal Newborn Hearing Screening Follow up Lata A. Krishnan, PhD, CCC A Shannon Van Hyfte, AuD, CCC A Purdue University The Joint Committee on Infant
Historical Perspective Effects of Policy Changes on Universal Newborn Hearing Screening Follow up Lata A. Krishnan, PhD, CCC A Shannon Van Hyfte, AuD, CCC A Purdue University The Joint Committee on Infant
KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT
 KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT SoundBeginnings Early Hearing Detection and Intervention Program Kansas Department of Health & Environment 1000 SW Jackson Ste. 220 Topeka, Kansas 66612-1274
KANSAS GUIDELINES FOR INFANT AUDIOLOGIC ASSESSMENT SoundBeginnings Early Hearing Detection and Intervention Program Kansas Department of Health & Environment 1000 SW Jackson Ste. 220 Topeka, Kansas 66612-1274
Christine Yoshinaga-Itano, Ph.D. Professor University of Colorado, Boulder Department of Speech, Language & Hearing Sciences Allison Sedey, Ph.D.
 Christine Yoshinaga-Itano, Ph.D. Professor University of Colorado, Boulder Department of Speech, Language & Hearing Sciences Allison Sedey, Ph.D. Rosalinda Baca, Ph.D. Molly Dalpes, AuD Kristin Uhler,
Christine Yoshinaga-Itano, Ph.D. Professor University of Colorado, Boulder Department of Speech, Language & Hearing Sciences Allison Sedey, Ph.D. Rosalinda Baca, Ph.D. Molly Dalpes, AuD Kristin Uhler,
Ototoxicity monitoring as part of risk monitoring in the EHDI system
 Ototoxicity monitoring as part of risk monitoring in the EHDI system Jessica Stich-Hennen, Au.D., PASC Doctor of Audiology Specialty Certification in Pediatric Audiology October 7, 2015 JCIH Position Statements
Ototoxicity monitoring as part of risk monitoring in the EHDI system Jessica Stich-Hennen, Au.D., PASC Doctor of Audiology Specialty Certification in Pediatric Audiology October 7, 2015 JCIH Position Statements
Usher Syndrome: Why a definite diagnosis matters
 Usher Syndrome: Why a definite diagnosis matters Margaret Kenna, MD, MPH Katherine Lafferty, MS, CGC Heidi Rehm, PhD Anne Fulton, MD Boston Children s Hospital Harvard Medical School Harvard Medical School
Usher Syndrome: Why a definite diagnosis matters Margaret Kenna, MD, MPH Katherine Lafferty, MS, CGC Heidi Rehm, PhD Anne Fulton, MD Boston Children s Hospital Harvard Medical School Harvard Medical School
What the Health Care Professional Should Know FROM ALD TO ZIKA: NEWBORN SCREENING AND SURVEILLANCE IN NJ
 Hearing Loss What the Health Care Professional Should Know MI C HAEL GRAFF, MD DI REC TOR, DI VI SI ON OF NEONATOLOGY K. HOVNANI AN C HI LDREN S HOSPI TAL JERSEY SHORE U NI VERSI TY MEDI C AL C ENTER HAC
Hearing Loss What the Health Care Professional Should Know MI C HAEL GRAFF, MD DI REC TOR, DI VI SI ON OF NEONATOLOGY K. HOVNANI AN C HI LDREN S HOSPI TAL JERSEY SHORE U NI VERSI TY MEDI C AL C ENTER HAC
Executive Summary. JCIH Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs
 Executive Summary JCIH Year 2007 : Principles and Guidelines for Early Hearing Detection and Intervention Programs Joint Committee on Infant Hearing Reference this material as: American Speech-Language-Hearing
Executive Summary JCIH Year 2007 : Principles and Guidelines for Early Hearing Detection and Intervention Programs Joint Committee on Infant Hearing Reference this material as: American Speech-Language-Hearing
Childhood Hearing Clinic causes of congenital hearing loss Audit of results of investigations
 Childhood Hearing Clinic causes of congenital hearing loss Audit of results of investigations Dr Karen Liddle - 20th May 2017 9th Australasian Newborn Screening Conference Childhood Hearing Clinic Multidisciplinary
Childhood Hearing Clinic causes of congenital hearing loss Audit of results of investigations Dr Karen Liddle - 20th May 2017 9th Australasian Newborn Screening Conference Childhood Hearing Clinic Multidisciplinary
Effective factors on Auditory Brainstem Response test in Newborns
 BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2557-2561 Effective factors on Auditory Brainstem Response test in Newborns Mozafar Sarafraz 1, Maryam Kardooni 1 and Somayeh Araghi
BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2557-2561 Effective factors on Auditory Brainstem Response test in Newborns Mozafar Sarafraz 1, Maryam Kardooni 1 and Somayeh Araghi
Usher Syndrome: When to Suspect it and How to Find It
 Usher Syndrome: When to Suspect it and How to Find It Margaret Kenna, MD, MPH Katherine Lafferty, MS, CGC Heidi Rehm, PhD Anne Fulton, MD Harvard Medical School Harvard Medical School Center for Hereditary
Usher Syndrome: When to Suspect it and How to Find It Margaret Kenna, MD, MPH Katherine Lafferty, MS, CGC Heidi Rehm, PhD Anne Fulton, MD Harvard Medical School Harvard Medical School Center for Hereditary
Update on Pediatric Hearing Loss & Cochlear Implantation
 Update on Pediatric Hearing Loss & Cochlear Implantation Anna K. Meyer, MD, FAAP Assistant Professor Division of Pediatric Otolarynoglogy University of California, San Francisco February 16, 2013 No disclosures
Update on Pediatric Hearing Loss & Cochlear Implantation Anna K. Meyer, MD, FAAP Assistant Professor Division of Pediatric Otolarynoglogy University of California, San Francisco February 16, 2013 No disclosures
Why Pediatric Hearing Clinic
 Why Pediatric Hearing Clinic RICHARD KANG, M.D., ASHLEY KAUFMAN, AU.D. AND MALLORY AUCH, RN Our Staff: Mallory Auch, RN Nurse Coordinator Kristen Janky, PhD, AuD, CCC-A Vestibular Audiologist Richard Kang,
Why Pediatric Hearing Clinic RICHARD KANG, M.D., ASHLEY KAUFMAN, AU.D. AND MALLORY AUCH, RN Our Staff: Mallory Auch, RN Nurse Coordinator Kristen Janky, PhD, AuD, CCC-A Vestibular Audiologist Richard Kang,
Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module. Inside this issue:
 Volume 3, Issue 11 Jul-Sept 2010 Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module NORTH DAKOTA EARLY HEARING DETECTION & INTERVENTION Even the best program to identify
Volume 3, Issue 11 Jul-Sept 2010 Hear Now! ND EHDI Announces the release of North Dakota s Early Intervention Module NORTH DAKOTA EARLY HEARING DETECTION & INTERVENTION Even the best program to identify
Outline ANATOMY OF EAR. All about Cochlear implants/why does this child not have a Cochlear Implant?
 All about Cochlear implants/why does this child not have a Cochlear Implant? Dr.S.Rangan Consultant Audiovestibular Physician (Paediatrics) St Catherine s Health Centre WUTH/BAPA Outline How does the ear
All about Cochlear implants/why does this child not have a Cochlear Implant? Dr.S.Rangan Consultant Audiovestibular Physician (Paediatrics) St Catherine s Health Centre WUTH/BAPA Outline How does the ear
Developmental Hearing and Auditory Milestones. Presented by : Amy Packer & Marilyn Nelson
 Developmental Hearing and Auditory Milestones Presented by : Amy Packer & Marilyn Nelson Today s Objectives: 1. The EAR and the Development of Hearing 2. The Developmental Urgency of Hearing 3. The Impact
Developmental Hearing and Auditory Milestones Presented by : Amy Packer & Marilyn Nelson Today s Objectives: 1. The EAR and the Development of Hearing 2. The Developmental Urgency of Hearing 3. The Impact
CHILDREN WITH CMV: DON T FORGET THE IMPORTANCE OF EARLY INTERVENTION. Paula Pittman, PhD Director, Utah Parent Infant Program for the Deaf
 CHILDREN WITH CMV: DON T FORGET THE IMPORTANCE OF EARLY INTERVENTION Paula Pittman, PhD Director, Utah Parent Infant Program for the Deaf STRAW POLL ON CMV 100 people surveyed regarding CMV How many knew
CHILDREN WITH CMV: DON T FORGET THE IMPORTANCE OF EARLY INTERVENTION Paula Pittman, PhD Director, Utah Parent Infant Program for the Deaf STRAW POLL ON CMV 100 people surveyed regarding CMV How many knew
The Whole Child: Hearing Screening and Identification in Children who are Deaf/Hard of Hearing. Rachel St. John, MD, NCC, NIC-A
 The Whole Child: Hearing Screening and Identification in Children who are Deaf/Hard of Hearing Rachel St. John, MD, NCC, NIC-A Disclosure I will not be discussing off-label uses of any medications, and
The Whole Child: Hearing Screening and Identification in Children who are Deaf/Hard of Hearing Rachel St. John, MD, NCC, NIC-A Disclosure I will not be discussing off-label uses of any medications, and
Cochlear Implants: The Role of the Early Intervention Specialist. Carissa Moeggenberg, MA, CCC-A February 25, 2008
 Cochlear Implants: The Role of the Early Intervention Specialist Carissa Moeggenberg, MA, CCC-A February 25, 2008 Case Scenario 3 month old baby with a confirmed severe to profound HL 2 Counseling the
Cochlear Implants: The Role of the Early Intervention Specialist Carissa Moeggenberg, MA, CCC-A February 25, 2008 Case Scenario 3 month old baby with a confirmed severe to profound HL 2 Counseling the
A SUPPLEMENT TO AUDIOLOGY TODAY NOVEMBER/DECEMBER 2007
 A SUPPLEMENT TO AUDIOLOGY TODAY NOVEMBER/DECEMBER 2007 REPRODUCED WITH PERMISSION FROM PEDIATRICS, VOL. 120, PAGES 898-921, COPYRIGHT 2007 BY THE AAP. COPIES MADE AVAILABLE THROUGH FINANCIAL SUPPORT FROM
A SUPPLEMENT TO AUDIOLOGY TODAY NOVEMBER/DECEMBER 2007 REPRODUCED WITH PERMISSION FROM PEDIATRICS, VOL. 120, PAGES 898-921, COPYRIGHT 2007 BY THE AAP. COPIES MADE AVAILABLE THROUGH FINANCIAL SUPPORT FROM
Risk Factors for Late-Onset Hearing Loss in Children
 Risk Factors for Late-Onset Hearing Loss in Children Richard Folsom University of Washington Susan Norton Esther Ehrmann Children s Hospital & Regional Medical Center In collaboration with Washington State
Risk Factors for Late-Onset Hearing Loss in Children Richard Folsom University of Washington Susan Norton Esther Ehrmann Children s Hospital & Regional Medical Center In collaboration with Washington State
10/26/2016. CMV and Connexin 26 Frontiers of Research and Therapy for Congenital Hearing Loss. CMV and Cx26 Hearing Loss. CMV and Cx26 Hearing Loss
 CMV and Connexin 26 Frontiers of Research and Therapy for Congenital Hearing Loss Dylan K. Chan, MD, PhD, FAAP Assistant Professor Pediatric Otolaryngology-Head and Neck Surgery Director, Children s Communication
CMV and Connexin 26 Frontiers of Research and Therapy for Congenital Hearing Loss Dylan K. Chan, MD, PhD, FAAP Assistant Professor Pediatric Otolaryngology-Head and Neck Surgery Director, Children s Communication
DIAGNOSIS Causes/Etiology of Hearing Loss
 DIAGNOSIS Causes/Etiology of Hearing Loss DIAGNOSIS Causes/Etiology of Hearing Loss VI. How Do We Hear? Sound waves enter our ears and are amplified by the ear drum and middle ear bones (ossicles), allowing
DIAGNOSIS Causes/Etiology of Hearing Loss DIAGNOSIS Causes/Etiology of Hearing Loss VI. How Do We Hear? Sound waves enter our ears and are amplified by the ear drum and middle ear bones (ossicles), allowing
Management of Hearing Loss in Children
 Management of Hearing Loss in Children Margaret Kenna, MD, MPH Dept. of Otolaryngology and Communication Enhancement Children s Hospital Boston Dept. of Otology and Laryngology Harvard Medical School Harvard
Management of Hearing Loss in Children Margaret Kenna, MD, MPH Dept. of Otolaryngology and Communication Enhancement Children s Hospital Boston Dept. of Otology and Laryngology Harvard Medical School Harvard
NEWBORN HEARING SCREENING
 NEWBORN HEARING SCREENING UPDATED GUIDELINES FOR SURVEILLANCE AND AUDIOLOGY REFERRAL OF INFANTS AND CHILDREN FOLLOWING NEWBORN HEARING SCREENING (JULY 2012) 1 Document Control Document Control Version
NEWBORN HEARING SCREENING UPDATED GUIDELINES FOR SURVEILLANCE AND AUDIOLOGY REFERRAL OF INFANTS AND CHILDREN FOLLOWING NEWBORN HEARING SCREENING (JULY 2012) 1 Document Control Document Control Version
Deaf Children and Young People
 Deaf Children and Young People Professor Barry Wright Clinical Lead - National Deaf Children Young People and Family Service, York National Deaf Child and Adolescent Mental Health Service (NDCAMHS) Definitions
Deaf Children and Young People Professor Barry Wright Clinical Lead - National Deaf Children Young People and Family Service, York National Deaf Child and Adolescent Mental Health Service (NDCAMHS) Definitions
Genetics of Hearing Loss
 Genetics of Hearing Loss Daryl A. Scott MD/PhD Molecular & Human Genetics 1/20/2015 Why do we care? 1 100% 75% Hearing Loss 500:1000 50% 314:1000 25% 1:1000 17:1000 Newborn 18 yrs 65 yrs 75 yrs 60% Members
Genetics of Hearing Loss Daryl A. Scott MD/PhD Molecular & Human Genetics 1/20/2015 Why do we care? 1 100% 75% Hearing Loss 500:1000 50% 314:1000 25% 1:1000 17:1000 Newborn 18 yrs 65 yrs 75 yrs 60% Members
Screening Training Manual. Section 4: The Auditory System
 Screening Training Manual Section 4: The Auditory System 4.1 Anatomy and Physiology of the Ear 4.2 Types, Degrees and Implications of Hearing Loss 4.3 Risk Factors for Late onset Hearing Loss Page 1 of
Screening Training Manual Section 4: The Auditory System 4.1 Anatomy and Physiology of the Ear 4.2 Types, Degrees and Implications of Hearing Loss 4.3 Risk Factors for Late onset Hearing Loss Page 1 of
Hearing Screening, Diagnostics and Intervention
 JCIH Newborn Hearing Screening Guidelines 1-3-6 Model By 1 month Screenhearing Hearing Screening, Diagnostics and Intervention By 3 months: Evaluate hearing and complete diagnosticaudiology and otolaryngology
JCIH Newborn Hearing Screening Guidelines 1-3-6 Model By 1 month Screenhearing Hearing Screening, Diagnostics and Intervention By 3 months: Evaluate hearing and complete diagnosticaudiology and otolaryngology
The hearing-impaired child. D J H Wagenfeld. (CME, Nov/Dec 2003, Vol 21, No 11.)
") The hearing-impaired child D J H Wagenfeld (CME, Nov/Dec 2003, Vol 21, No 11.) It has become universally accepted that early identification and intervention in children with hearing loss is the key to
The hearing-impaired child D J H Wagenfeld (CME, Nov/Dec 2003, Vol 21, No 11.) It has become universally accepted that early identification and intervention in children with hearing loss is the key to
School Nurses Guide to Otoacoustic Emissions (OAEs)
") School Nurses Guide to Otoacoustic Emissions (OAEs) www.maico-diagnostics.com Rationale for hearing screening with OAEs Hearing loss is not uncommon in children. Approximately 6 out of every thousand children
School Nurses Guide to Otoacoustic Emissions (OAEs) www.maico-diagnostics.com Rationale for hearing screening with OAEs Hearing loss is not uncommon in children. Approximately 6 out of every thousand children
3. If the presence of middle ear pathology is suspected based on immittance test results, case history, or otoscopic exam, perform Wave V threshold se
 GUIDELINES FOR DIAGNOSTIC AUDIOLOGIC EVALUATION Audiologic evaluation of infants should be completed as soon as possible after a referral from the newborn hearing screening. The assessment should be completed
GUIDELINES FOR DIAGNOSTIC AUDIOLOGIC EVALUATION Audiologic evaluation of infants should be completed as soon as possible after a referral from the newborn hearing screening. The assessment should be completed
The Evaluation & Treatment of Hearing Loss in Children & Adults 2018
 The Evaluation & Treatment of Hearing Loss in Children & Adults 2018 Overview Types of hearing loss and common causes of hearing loss Dangers of noise exposure When to refer to an audiologist and how to
The Evaluation & Treatment of Hearing Loss in Children & Adults 2018 Overview Types of hearing loss and common causes of hearing loss Dangers of noise exposure When to refer to an audiologist and how to
Audiology 101 SOFT HIGH PITCH LOUD. How do we hear? Ear to the Brain. Main parts of the Ear
 Audiology 1 How do we hear? Main parts of the Ear Hear We Go! 6 Lori A. Van Riper, MS CCC-A University of Michigan Health System Sound Support Outer -pinna, ear canal eardrum Middle -air filled, ossicles
Audiology 1 How do we hear? Main parts of the Ear Hear We Go! 6 Lori A. Van Riper, MS CCC-A University of Michigan Health System Sound Support Outer -pinna, ear canal eardrum Middle -air filled, ossicles
Jackson Roush, PhD University of North Carolina Chapel Hill
 HEARING SCREENING IN THE NEONATAL INTENSIVE CARE UNIT: CURRENT STATUS AND FUTURE NEEDS Shana Jacobs, AuD University of North Carolina Chapel Hill Jackson Roush, PhD University of North Carolina Chapel
HEARING SCREENING IN THE NEONATAL INTENSIVE CARE UNIT: CURRENT STATUS AND FUTURE NEEDS Shana Jacobs, AuD University of North Carolina Chapel Hill Jackson Roush, PhD University of North Carolina Chapel
4/24/18 CAPD AND ANSD: A BASIC OVERVIEW. Presenters: Objectives for Today. IECC Session B16 May 3, 2018
 CAPD AND ANSD: A BASIC OVERVIEW IECC Session B16 May 3, 2018 Presenters: Nancy Hatfield, Ph.D. Early Childhood Consultant, WSDS/Deaf-Blind Project Emma Packard, M.Ed./M.A. TVI, O&M Specialist Consultant,
CAPD AND ANSD: A BASIC OVERVIEW IECC Session B16 May 3, 2018 Presenters: Nancy Hatfield, Ph.D. Early Childhood Consultant, WSDS/Deaf-Blind Project Emma Packard, M.Ed./M.A. TVI, O&M Specialist Consultant,
Emissions are low-intensity sounds that may be detected in the external ear canal by a microphone
 OAEs Emissions are low-intensity sounds that may be detected in the external ear canal by a microphone OAE is a pre-neural phenomenon They can be measured even when the 8 th cranial nerve is severely damaged
OAEs Emissions are low-intensity sounds that may be detected in the external ear canal by a microphone OAE is a pre-neural phenomenon They can be measured even when the 8 th cranial nerve is severely damaged
FUNCTIONAL HEARING SCREENING WHO WE ARE: YOU TELL ME OBJECTIVES: SLIGHT HIGH FREQUENCY HEARING LOSS OUTLINE: A PASS IS NOT A PASS FOR LIFE!
 FUNCTIONAL HEARING SCREENING A PASS IS NOT A PASS FOR LIFE! KRISTEN TINA SCHRAML CHILDRES, M.S. S, M.A., SPECIAL CCC-A ED. ILLINOIS SCHOOL FOR FOR THE THE DEAF DEAF OUTREA C HC H CONSULT A NA NT/ RT AI
FUNCTIONAL HEARING SCREENING A PASS IS NOT A PASS FOR LIFE! KRISTEN TINA SCHRAML CHILDRES, M.S. S, M.A., SPECIAL CCC-A ED. ILLINOIS SCHOOL FOR FOR THE THE DEAF DEAF OUTREA C HC H CONSULT A NA NT/ RT AI
A Little Audiology 101 Normal Auditory Development Two Paths: Diagnosed & Undiagnosed Syndromes, High Risk Factors and Red Flags
 A Little Audiology 101 Normal Auditory Development Two Paths: Diagnosed & Undiagnosed Syndromes, High Risk Factors and Red Flags 1 The Ear Video of how the ear works (http://www.entnet.org/content/how-ear-works)
A Little Audiology 101 Normal Auditory Development Two Paths: Diagnosed & Undiagnosed Syndromes, High Risk Factors and Red Flags 1 The Ear Video of how the ear works (http://www.entnet.org/content/how-ear-works)
Impact of the Early Hearing Detection and Intervention Program on the Detection of Hearing Loss at Birth Michigan,
 Journal of Educational Audiology 12 (2005) Impact of the Early Hearing Detection and Intervention Program on the Detection of Hearing Loss at Birth Michigan, 1998-2002 Darline K. El Reda, DrPH, MPH, CHES
Journal of Educational Audiology 12 (2005) Impact of the Early Hearing Detection and Intervention Program on the Detection of Hearing Loss at Birth Michigan, 1998-2002 Darline K. El Reda, DrPH, MPH, CHES
Early Hearing Detection & Intervention Programs, Pediatricians, Audiologists & School Nurses use AuDX Screeners
 Early Hearing Detection & Intervention Programs, Pediatricians, Audiologists & School Nurses use AuDX Screeners The Portable OAE Hearing Screener of Choice... Ear canal Middle ear Eardrum The AuDX device
Early Hearing Detection & Intervention Programs, Pediatricians, Audiologists & School Nurses use AuDX Screeners The Portable OAE Hearing Screener of Choice... Ear canal Middle ear Eardrum The AuDX device
Newborn hearing screening - well baby protocol Paediatrics > Screening > Newborn hearing screening
 Map of Medicine National Library for Health Newborn hearing screening well baby protocol Automated oto-acoustic emission (AOAE) screening test Missed or incomplete AOAE screening test AOAE no clear response
Map of Medicine National Library for Health Newborn hearing screening well baby protocol Automated oto-acoustic emission (AOAE) screening test Missed or incomplete AOAE screening test AOAE no clear response
Newborn hearing screening - NICU or SCBU protocol Paediatrics > Screening > Newborn hearing screening
 Map of Medicine National Library for Health Newborn hearing screening NICU/SCBU protocol Automated oto-acoustic emission (AOAE) screening test Automated auditory brainstem response (AABR) screening test
Map of Medicine National Library for Health Newborn hearing screening NICU/SCBU protocol Automated oto-acoustic emission (AOAE) screening test Automated auditory brainstem response (AABR) screening test
EHDI Conference 2009 Addison, TX
 Update on the Joint Committee on Infant Hearing Activities EHDI Conference 2009 Addison, TX Judith Widen - University of Kansas Medical Center - Kansas City, KS Judith Harrison, AG Bell Association Washington,
Update on the Joint Committee on Infant Hearing Activities EHDI Conference 2009 Addison, TX Judith Widen - University of Kansas Medical Center - Kansas City, KS Judith Harrison, AG Bell Association Washington,
Article Rating (internal/ external validity; study design) Sample (N with postnatal HL/N with HL; selection period )
 Sample (N with postnatal HL/N with HL; selection period )") Table A1. Studies on children with a hearing loss that included postnatally developed hearing loss (Trend 1 publications) [where 35delG = 35 deleted Guanine; ABR = Auditory Brainstem Response; ASSR = Auditory
Table A1. Studies on children with a hearing loss that included postnatally developed hearing loss (Trend 1 publications) [where 35delG = 35 deleted Guanine; ABR = Auditory Brainstem Response; ASSR = Auditory
Section: Division of Nursing ************** Index: b * PROTOCOL * Page: 1 of 8 Approval: ************** Issue Date: January, 2010
 Section: Division of Nursing ************** Index: 6170.073b * PROTOCOL * Page: 1 of 8 Approval: ************** HACKETTSTOWN REGIONAL MEDICAL CENTER Originator: Revised by: D. Vanderwiele, RN, MSN, MPA
Section: Division of Nursing ************** Index: 6170.073b * PROTOCOL * Page: 1 of 8 Approval: ************** HACKETTSTOWN REGIONAL MEDICAL CENTER Originator: Revised by: D. Vanderwiele, RN, MSN, MPA
City: Person Completing this Form (if not patient): Relation to patient: Reason for Appointment:
: Relation to patient: Reason for Appointment:") Ball State University Speech and Audiology Clinic Family Medical History Form : Date: Birthdate: Sex: Address: City: State: ZIP: Home Phone: ( ) Other Phone: ( ) Email: Primary Care Physician: Maternal
Ball State University Speech and Audiology Clinic Family Medical History Form : Date: Birthdate: Sex: Address: City: State: ZIP: Home Phone: ( ) Other Phone: ( ) Email: Primary Care Physician: Maternal
2. stereocilia make contact with membrane, feel vibration. Tiplink is deflected, allows ions to go inside cell body and chemical signal is generated.
 Hearing Loss 1. Most common sensory deficit in human 2. 3 in ten people over age 60 have hearing loss 3. At least 1.4 million children have hearing problems 4. Estimated that 3 in 1,000 infants are born
Hearing Loss 1. Most common sensory deficit in human 2. 3 in ten people over age 60 have hearing loss 3. At least 1.4 million children have hearing problems 4. Estimated that 3 in 1,000 infants are born
Improving Loss to Follow-up Rates Diagnostic Center Guidelines for 2011
 Improving Loss to Follow-up Rates Diagnostic Center Guidelines for 2011 2011 National Early Hearing Detection and Intervention Conference Atlanta, Georgia Janet Farrell, Sarah Stone, Rashmi Dayalu MA DPH
Improving Loss to Follow-up Rates Diagnostic Center Guidelines for 2011 2011 National Early Hearing Detection and Intervention Conference Atlanta, Georgia Janet Farrell, Sarah Stone, Rashmi Dayalu MA DPH
Neonatal Hearing Screening Program in Wallonia and Brussels
 EUSUHM 2017 Mind the gap! Building bridges to better health for all young people Session: Early detection of hearing impairment Neonatal Hearing Screening Program in Wallonia and Brussels Bénédicte VOS
EUSUHM 2017 Mind the gap! Building bridges to better health for all young people Session: Early detection of hearing impairment Neonatal Hearing Screening Program in Wallonia and Brussels Bénédicte VOS
Avg. age of diagnosis 3 mo. majority range.5-5 mo range 1-7 mo range 6-12 mo
 Team Approach to Determining Cochlear Implant Candidacy in Early Infancy Jean Thomas, M.S., CCC-A Kristin Lutes, M.S., CCC-SLP Mary Willis, M.S., CCC-SLP Carle Foundation Hospital, Urbana, Illinois Early
Team Approach to Determining Cochlear Implant Candidacy in Early Infancy Jean Thomas, M.S., CCC-A Kristin Lutes, M.S., CCC-SLP Mary Willis, M.S., CCC-SLP Carle Foundation Hospital, Urbana, Illinois Early
Just What Do Your Pediatric Audiologists Know?
 Just What Do Your Pediatric Audiologists Know? Lisa Satterfield, M.S., CCC/A Jennifer Sherwood, M.A., F/AAA California Department of Health Care Services EHDI Conference, March 2, 2010 California Infant
Just What Do Your Pediatric Audiologists Know? Lisa Satterfield, M.S., CCC/A Jennifer Sherwood, M.A., F/AAA California Department of Health Care Services EHDI Conference, March 2, 2010 California Infant
Recommendations for monitoring hearing in children using a risk factor registry
 Recommendations for monitoring hearing in children using a risk factor registry Rachael Beswick Carlie Driscoll Joseph Kei Shirley Glennon 7th Australasian Newborn Hearing Screening Conference 2012 Background
Recommendations for monitoring hearing in children using a risk factor registry Rachael Beswick Carlie Driscoll Joseph Kei Shirley Glennon 7th Australasian Newborn Hearing Screening Conference 2012 Background
OUTCOMES OF CHILDREN WHO ARE HARD OF HEARING
 OUTCOMES OF CHILDREN WHO ARE HARD OF HEARING A N E W C H AP T E R M A R Y P A T M O E L L E R, P H. D. N A T I O N A L E H D I C O N F E R E N C E, J A C K S O N V I L L E, F L A, A P R I L 1 4, 2 0 1
OUTCOMES OF CHILDREN WHO ARE HARD OF HEARING A N E W C H AP T E R M A R Y P A T M O E L L E R, P H. D. N A T I O N A L E H D I C O N F E R E N C E, J A C K S O N V I L L E, F L A, A P R I L 1 4, 2 0 1
REFERRAL AND DIAGNOSTIC EVALUATION OF HEARING ACUITY. Better Hearing Philippines Inc.
 REFERRAL AND DIAGNOSTIC EVALUATION OF HEARING ACUITY Better Hearing Philippines Inc. How To Get Started? 1. Testing must be done in an acoustically treated environment far from all the environmental noises
REFERRAL AND DIAGNOSTIC EVALUATION OF HEARING ACUITY Better Hearing Philippines Inc. How To Get Started? 1. Testing must be done in an acoustically treated environment far from all the environmental noises
PURPOSE OF THIS PRESENTATION GUIDELINES DEVELOPMENT CONFERENCE GUIDELINES DEVELOPMENT CONFERENCE: FACULTY GUIDELINES DEVELOPMENT CONFERENCE: OUTCOMES
 PURPOSE OF THIS PRESENTATION GUIDELINES DEVELOPMENT CONFERENCE: COMO ITALY 2008 Deborah Hayes, Ph.D. Co-Chair Bill Daniels Center for Children s Hearing The Children s Hospital - Colorado Explain the concept
PURPOSE OF THIS PRESENTATION GUIDELINES DEVELOPMENT CONFERENCE: COMO ITALY 2008 Deborah Hayes, Ph.D. Co-Chair Bill Daniels Center for Children s Hearing The Children s Hospital - Colorado Explain the concept
to the child and the family, based on the child's and family's abilities and needs. The IFSP needs to address the communication needs of the child and
 GUIDELINES FOR EARLY INTERVENTION The goals of newborn hearing screening are to provide a hearing screen to all newborns before one month of age, to ensure that all newborns who do not pass the birth admission
GUIDELINES FOR EARLY INTERVENTION The goals of newborn hearing screening are to provide a hearing screen to all newborns before one month of age, to ensure that all newborns who do not pass the birth admission
thorough physical and laboratory investigations fail to define the etiology of hearing loss. (2000, p. 16). In a report produced for the Maternal and
. In a report produced for the Maternal and") GUIDELINES FOR GENETIC EVALUATON REFERRAL The prevalence of permanent hearing loss in infants is estimated to be 2-3/1000 in the United States (Finitzo et al., 1998; Prieve et al., 2000). One or both ears
GUIDELINES FOR GENETIC EVALUATON REFERRAL The prevalence of permanent hearing loss in infants is estimated to be 2-3/1000 in the United States (Finitzo et al., 1998; Prieve et al., 2000). One or both ears
NEWBORN HEARING SCREENING AND WHY IT S IMPORTANT
 NEWBORN HEARING SCREENING AND WHY IT S IMPORTANT -Department of ENT and Audiology HOSPITAL MANKHOOL ASTERHOSPITAL.COM 04-4400500 RELIABLE EASY FAST SAFE (WHO) states that 0.5-5 newborns in every 1000 births
NEWBORN HEARING SCREENING AND WHY IT S IMPORTANT -Department of ENT and Audiology HOSPITAL MANKHOOL ASTERHOSPITAL.COM 04-4400500 RELIABLE EASY FAST SAFE (WHO) states that 0.5-5 newborns in every 1000 births
The Two I s in EHDI: Intervention and Impact. Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK
 The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK Hearing Loss Facts: Brief Overview The most common birth anomaly: 2 to
The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK Hearing Loss Facts: Brief Overview The most common birth anomaly: 2 to
Childhood Hearing Impairment
 Childhood Hearing Impairment N. Wendell Todd MD MPH Adrienne M. Laury MD Emory University Disclaimer: The opinions I am about to express are my own. They do not necessarily represent the opinions of Emory
Childhood Hearing Impairment N. Wendell Todd MD MPH Adrienne M. Laury MD Emory University Disclaimer: The opinions I am about to express are my own. They do not necessarily represent the opinions of Emory
Newborn Screening and Middle Ear Problems
 Lisa L. Hunter 1, Douglas H. Keefe 2, M. Patrick Feeney 3;4, David K. Brown 1, Jareen Meinzen-Derr and Denis F. Fitzpatrick 2 1 Cincinnati Children's Hospital Medical Center, 2 Boys Town National Research
Lisa L. Hunter 1, Douglas H. Keefe 2, M. Patrick Feeney 3;4, David K. Brown 1, Jareen Meinzen-Derr and Denis F. Fitzpatrick 2 1 Cincinnati Children's Hospital Medical Center, 2 Boys Town National Research
Diagnosis and Management of ANSD: Outcomes of Cochlear Implants versus Hearing Aids
 Diagnosis and Management of ANSD: Outcomes of Cochlear Implants versus Hearing Aids Gary Rance PhD The University of Melbourne International Paediatric Conference, Shanghai, April 214 Auditory Neuropathy
Diagnosis and Management of ANSD: Outcomes of Cochlear Implants versus Hearing Aids Gary Rance PhD The University of Melbourne International Paediatric Conference, Shanghai, April 214 Auditory Neuropathy
An Update on Auditory Neuropathy Spectrum Disorder in Children
 An Update on Auditory Neuropathy Spectrum Disorder in Children Gary Rance PhD The University of Melbourne Sound Foundations Through Early Amplification Meeting, Chicago, Dec 2013 Overview Auditory neuropathy
An Update on Auditory Neuropathy Spectrum Disorder in Children Gary Rance PhD The University of Melbourne Sound Foundations Through Early Amplification Meeting, Chicago, Dec 2013 Overview Auditory neuropathy
AUDIOLOGY INFORMATION SERIES ASHA S CONSUMER NEWSLETTER. Hearing Loss and Its Implications for Learning and Communication
 AUDIOLOGY INFORMATION SERIES ASHA S CONSUMER NEWSLETTER Vol. 1 No. 2 2000 Hearing Loss and Its Implications for Learning and Communication Hearing Loss and Children: The Facts and Why They Are Important!
AUDIOLOGY INFORMATION SERIES ASHA S CONSUMER NEWSLETTER Vol. 1 No. 2 2000 Hearing Loss and Its Implications for Learning and Communication Hearing Loss and Children: The Facts and Why They Are Important!
Map of Medicine National Library for Health
 Map of Medicine National Library for Health Newborn hearing screening Check eligibility Eligible for screening Not eligible for screening Consider risk factors for hearing loss Provide information and
Map of Medicine National Library for Health Newborn hearing screening Check eligibility Eligible for screening Not eligible for screening Consider risk factors for hearing loss Provide information and
Hearing Evaluation: Diagnostic Approach
 Hearing Evaluation: Diagnostic Approach Hearing Assessment Purpose - to quantify and qualify in terms of the degree of hearing loss, the type of hearing loss and configuration of the hearing loss - carried
Hearing Evaluation: Diagnostic Approach Hearing Assessment Purpose - to quantify and qualify in terms of the degree of hearing loss, the type of hearing loss and configuration of the hearing loss - carried
Early Hearing Detection and Intervention
 Early Hearing Detection and Intervention ACTION REQUESTED Please co-sponsor and support passage of the Early Hearing Detection and Intervention (EHDI) Act of 2009 (H.R. 1246) that would reauthorize the
Early Hearing Detection and Intervention ACTION REQUESTED Please co-sponsor and support passage of the Early Hearing Detection and Intervention (EHDI) Act of 2009 (H.R. 1246) that would reauthorize the
Rory Attwood MBChB,FRCS
 Hearing loss Overview Rory Attwood MBChB,FRCS Division of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch Not deafness Deaf is a total lack of hearing Deafness
Hearing loss Overview Rory Attwood MBChB,FRCS Division of Otorhinolaryngology Faculty of Health Sciences Tygerberg Campus, University of Stellenbosch Not deafness Deaf is a total lack of hearing Deafness
Auditory Neuropathy Spectrum Disorder (ANSD)
") Auditory Neuropathy Spectrum Disorder (ANSD) Information for BC Families This booklet was created by the BC Early Hearing Program to help provide you and your family with accurate information. Thank you
Auditory Neuropathy Spectrum Disorder (ANSD) Information for BC Families This booklet was created by the BC Early Hearing Program to help provide you and your family with accurate information. Thank you
MINNESOTA EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM. EHDI Goals, Indicators and Benchmarks
 PROGRAM. EHDI Goals, Indicators and Benchmarks") Protecting, maintaining and improving the health of all Minnesotans MINNESOTA EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM EHDI Goals, Indicators and Benchmarks The measures described in this
Protecting, maintaining and improving the health of all Minnesotans MINNESOTA EARLY HEARING DETECTION AND INTERVENTION (EHDI) PROGRAM EHDI Goals, Indicators and Benchmarks The measures described in this
Hearing Loss in Infants and Children: Could it be Usher Syndrome?
 Hearing Loss in Infants and Children: Could it be Usher Syndrome? Margaret A. Kenna, MD, MPH Dept. of Otolaryngology and Communication Enhancement Boston Children s Hospital Dept. of Otology and Laryngology
Hearing Loss in Infants and Children: Could it be Usher Syndrome? Margaret A. Kenna, MD, MPH Dept. of Otolaryngology and Communication Enhancement Boston Children s Hospital Dept. of Otology and Laryngology
The Two I s in EHDI: Intervention and Impact. Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK
 The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK As the CEO of EI Services Hearing Loss Facts: Brief Overview The most
The Two I s in EHDI: Intervention and Impact Teresa H. Caraway, Ph.D., CCC-SLP, LSLS Cert. AVT Hearts for Hearing Oklahoma City, OK As the CEO of EI Services Hearing Loss Facts: Brief Overview The most
Corporate Medical Policy
 Corporate Medical Policy Genetic Testing for Hereditary Hearing Loss File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_hereditary_hearing_loss 10/2013 7/2018 7/2019
Corporate Medical Policy Genetic Testing for Hereditary Hearing Loss File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_hereditary_hearing_loss 10/2013 7/2018 7/2019
Trends across the country. Indiana Early Hearing Detection 4/13/2015
 Trends across the country Indiana Early Hearing Detection and Intervention (EHDI) Shortage of pediatric audiologists Shortage of educators and SLPs skilled in working with deaf and hard of hearing children
Trends across the country Indiana Early Hearing Detection and Intervention (EHDI) Shortage of pediatric audiologists Shortage of educators and SLPs skilled in working with deaf and hard of hearing children
ROADMAP TO SPOKEN LANGUAGE C H R I S T I N E Y O S H I N A G A - I T A N O, P H. D. U N I V E R S I T Y O F C O L O R A D O, B O U L D E R
 ROADMAP TO SPOKEN LANGUAGE C H R I S T I N E Y O S H I N A G A - I T A N O, P H. D. U N I V E R S I T Y O F C O L O R A D O, B O U L D E R THE JOURNEY BEGINS WITH AN OPPORTUNITY 2011 NATIONAL CDC EHDI
ROADMAP TO SPOKEN LANGUAGE C H R I S T I N E Y O S H I N A G A - I T A N O, P H. D. U N I V E R S I T Y O F C O L O R A D O, B O U L D E R THE JOURNEY BEGINS WITH AN OPPORTUNITY 2011 NATIONAL CDC EHDI
Dizziness/Balance Questionnaire
 Dizziness/Balance Questionnaire Name: Date: 1. Which of these best describes your dizziness? Please mark only one. A sensation of movement of yourself or the room (spinning, tilting, or wave-like movement)
Dizziness/Balance Questionnaire Name: Date: 1. Which of these best describes your dizziness? Please mark only one. A sensation of movement of yourself or the room (spinning, tilting, or wave-like movement)
Prevalence of Hearing Impairment
 Prevalence of Hearing Impairment 28 million Americans 2 million profoundly deaf 1/1000 congenitally deaf 1/3 impaired by age 65 1/2 impaired by age 80 NIDCD National Strategic Research Plan, 1989 Genetic
Prevalence of Hearing Impairment 28 million Americans 2 million profoundly deaf 1/1000 congenitally deaf 1/3 impaired by age 65 1/2 impaired by age 80 NIDCD National Strategic Research Plan, 1989 Genetic
Melissa Wake Director, Research & Public Health Centre for Community Child Health
 Melissa Wake Director, Research & Public Health Centre for Community Child Health The Team Why screen for hearing loss in newborns? Importance of Early Identification Deafness is currently detected late
Melissa Wake Director, Research & Public Health Centre for Community Child Health The Team Why screen for hearing loss in newborns? Importance of Early Identification Deafness is currently detected late
ABC s of Pediatric Audiology
 ABC s of Pediatric Audiology Marnie Pomeroy, AuD, CCC A Pediatric Audiologist Little Ears Hearing Center at Open Arms Children s Health a service of Home of the Innocents Home of the Innocents Home of
ABC s of Pediatric Audiology Marnie Pomeroy, AuD, CCC A Pediatric Audiologist Little Ears Hearing Center at Open Arms Children s Health a service of Home of the Innocents Home of the Innocents Home of
FEASIBILITY ASSESSMENT OF A UNIVERSAL NEWBORN HEARING SCREENING PROGRAMME AT RAHIMA MOOSA MOTHER AND CHILD HOSPITAL
 FEASIBILITY ASSESSMENT OF A UNIVERSAL NEWBORN HEARING SCREENING PROGRAMME AT RAHIMA MOOSA MOTHER AND CHILD HOSPITAL Jacqueline Kim Bezuidenhout A research report submitted to the Faculty of Health Sciences,
FEASIBILITY ASSESSMENT OF A UNIVERSAL NEWBORN HEARING SCREENING PROGRAMME AT RAHIMA MOOSA MOTHER AND CHILD HOSPITAL Jacqueline Kim Bezuidenhout A research report submitted to the Faculty of Health Sciences,
Early Detection of Deafness & Neonatal Hearing Screening Dr. Abdul Monem Alshaikh
 Early Detection of Deafness & Neonatal Hearing Screening Dr. Abdul Monem Alshaikh Consultant of Otorhinolaryngology Otology & Cochlear implant Jeddah - KSA Screening It is the process of applying to a
Early Detection of Deafness & Neonatal Hearing Screening Dr. Abdul Monem Alshaikh Consultant of Otorhinolaryngology Otology & Cochlear implant Jeddah - KSA Screening It is the process of applying to a
A New Era for the Identification and Treatment of Children with Auditory Disorders
 1 A New Era for the Identification and Treatment of Children with Auditory Disorders ROSS J. ROESER AND MARION P. DOWNS Nothing great was ever achieved without enthusiasm. Ralph Waldo Emerson It is a new
1 A New Era for the Identification and Treatment of Children with Auditory Disorders ROSS J. ROESER AND MARION P. DOWNS Nothing great was ever achieved without enthusiasm. Ralph Waldo Emerson It is a new
Surgical and Non-Surgical Causes of Progressive Hearing Loss in Children: What can be done about it?
 Surgical and Non-Surgical Causes of Progressive Hearing Loss in Children: What can be done about it? Daniela Carvalho, MD, MMM, FAAP Professor, Surgery Department UCSD Pediatric Otolaryngology Rady Children
Surgical and Non-Surgical Causes of Progressive Hearing Loss in Children: What can be done about it? Daniela Carvalho, MD, MMM, FAAP Professor, Surgery Department UCSD Pediatric Otolaryngology Rady Children
A PARENT S GUIDE TO DEAF AND HARD OF HEARING EARLY INTERVENTION RECOMMENDATIONS
 A PARENT S GUIDE TO DEAF AND HARD OF HEARING EARLY INTERVENTION RECOMMENDATIONS 2017 Developed by the Early Hearing Detection & Intervention Parent to Parent Committee A PARENT S GUIDE TO DEAF AND HARD
A PARENT S GUIDE TO DEAF AND HARD OF HEARING EARLY INTERVENTION RECOMMENDATIONS 2017 Developed by the Early Hearing Detection & Intervention Parent to Parent Committee A PARENT S GUIDE TO DEAF AND HARD
EHDI in Michigan. Introduction. EHDI Goals and Communication Options. Review of EHDI Goals. Effects of Universal Newborn Hearing Screening (UNHS)
") EHDI Goals and Communication Options Anita Vereb,, MS, CCC-A University of Michigan Division of Audiology Introduction Hearing loss is the most frequently occurring birth defect 2 out of every 1000 babies
EHDI Goals and Communication Options Anita Vereb,, MS, CCC-A University of Michigan Division of Audiology Introduction Hearing loss is the most frequently occurring birth defect 2 out of every 1000 babies
ORIGINAL ARTICLE. The Distribution of Risk Factors among High Risk Infants who Failed at Hearing Screening
 ORIGINAL ARTICLE The Distribution of Risk Factors among High Risk Infants who Failed at Hearing Screening Figen Baflar, Ayfle Gül Güven Ondokuz May s University Medical Faculty ENT Dept, Audiology Unit.
ORIGINAL ARTICLE The Distribution of Risk Factors among High Risk Infants who Failed at Hearing Screening Figen Baflar, Ayfle Gül Güven Ondokuz May s University Medical Faculty ENT Dept, Audiology Unit.
Iowa EHDI A Work in Progress. Coordinating Council for Hearing Services November 24, 2008
 Iowa EHDI A Work in Progress Coordinating Council for Hearing Services November 24, 2008 Presenter Lenore Holte, PhD University of Iowa Hospitals and Clinics Center for Disabilities and Development 100
Iowa EHDI A Work in Progress Coordinating Council for Hearing Services November 24, 2008 Presenter Lenore Holte, PhD University of Iowa Hospitals and Clinics Center for Disabilities and Development 100
HEALTH VISITOR INFORMATION PACK
 HEALTH VISITOR INFORMATION PACK NEWBORN HEARING SCREENING WALES Health Visitor Information Pack Contents: 1. Overview - Background Information - The Newborn Hearing Screening Programme for Wales - Methods
HEALTH VISITOR INFORMATION PACK NEWBORN HEARING SCREENING WALES Health Visitor Information Pack Contents: 1. Overview - Background Information - The Newborn Hearing Screening Programme for Wales - Methods
EHDI: An Amazing Journey
 EHDI: An Amazing Journey Jackson Roush, PhD Professor & Director Division of Speech and Hearing Sciences Director, North Carolina LEND Program Carolina Institute for Developmental Disabilities UNC School
EHDI: An Amazing Journey Jackson Roush, PhD Professor & Director Division of Speech and Hearing Sciences Director, North Carolina LEND Program Carolina Institute for Developmental Disabilities UNC School
Syndromic Deafness Variant of Waardenburg syndrome
 International Journal of Pharmaceutical Science Invention ISSN (Online): 2319 6718, ISSN (Print): 2319 670X Volume 3 Issue 4 April 2014 PP.18-22 Syndromic Deafness Variant of Waardenburg syndrome 1, Dr.
International Journal of Pharmaceutical Science Invention ISSN (Online): 2319 6718, ISSN (Print): 2319 670X Volume 3 Issue 4 April 2014 PP.18-22 Syndromic Deafness Variant of Waardenburg syndrome 1, Dr.
(OAEs) for. Steven D. Smith, Au.D.
 for. Steven D. Smith, Au.D.") A Guide to Otoacoustic Emissions (OAEs) for School Nurses Steven D. Smith, Au.D. Director of Audiology, Director of Physicians Hearing & Balance Center Drs. Kitchens, Chapman, & Anderson, PA, Montgomery,
A Guide to Otoacoustic Emissions (OAEs) for School Nurses Steven D. Smith, Au.D. Director of Audiology, Director of Physicians Hearing & Balance Center Drs. Kitchens, Chapman, & Anderson, PA, Montgomery,
Online Courses for Parents and Professionals Who Want to Know More About Children who are Deaf or Hard of Hearing
 fl pennsylvania OFRCE OF CHILD DEVELOPMENT AND EAR Y LEARNING New Online Co u r s e s! Online Courses for Parents and Professionals Who Want to Know More About Children who are Deaf or Hard of Hearing
fl pennsylvania OFRCE OF CHILD DEVELOPMENT AND EAR Y LEARNING New Online Co u r s e s! Online Courses for Parents and Professionals Who Want to Know More About Children who are Deaf or Hard of Hearing