Article in press. Distraction Osteogenesis: Role and Clinical Application in the Maxillofacial Region. Case Report
|
|
|
- Brianna Wilson
- 5 years ago
- Views:
Transcription
1 Case Report Distraction Osteogenesis: Role and Clinical Application in the Maxillofacial Region Thongchai Nuntanaranont 1, Wipapan Ritthagol 2 and Butsakorn Akarawatcharangura 1 1 Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Prince of Songkla University, Songkhla, Thailand 2 Department of Preventive Dentistry, Faculty of Dentistry, Prince of Songkla University, Songkhla, Thailand Correspondence to: Butsakorn Akarawatcharangura. Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Prince of Songkla University, Hat Yai, Songkhla Thailand Tel: Fax: butsakorn.a@psu.ac.th Abstract Distraction osteogenesis or callostasis is a technique for new bone formation by gradual separation of bony fragments. The method was first developed for limb lengthening but recently this process has been widely applied in the cranio-maxillofacial bone. The application of this technique included bone lengthening and reconstruction of segmental defects. Several designs of extraoral and intraoral distraction devices were invented to suit different areas of the craniofacial bone. Nevertheless, intraoral distractors have several advantages including minimal scarring and being less cumbersome. Clinical cases using intraoral distraction osteogenesis technique as the alternative treatment for conventional surgical procedures for maxillo-mandibular lengthening and reconstruction of the alveolar segmental defect after tumor resection and before implant installation are presented and discussed in this study. Key words: Distraction application; Distraction osteogenesis; Maxillofacial region Received Date: Dec 11, 2015, Accepted Date: May 19, 2015 doi: /jdat Nuntanaranont et al.,
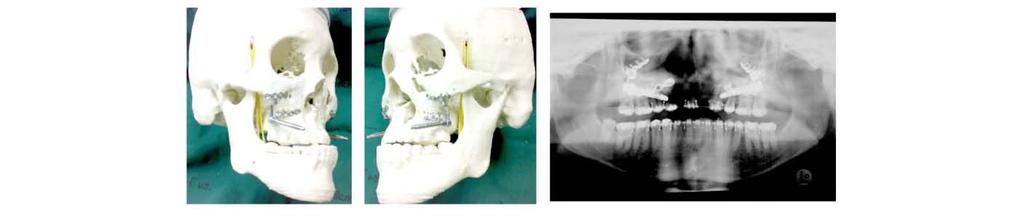
2 Introduction Distraction osteogenesis is a method of producing living bone directly from a special osteotomy by controlled mechanical distraction. The regenerated fibrovascular tissues in the distraction gap align themselves parallel to the distraction vector. Then the osteoid tissue is lay down and fill with the mineralize tissue. The new bone spontaneously bridges the gap and rapidly remodels to a normal macrostructure local bone. 1-3 Distraction osteogenesis is also called Callostasis (generating new bone by stretching the callus, as in a fracture). This concept of bone lengthening was first described by Codivilla in , who used it to elongate a femur by repeated pulling forces. Other investigators also applied this technique but it remained undeveloped because of associated complications such as nonunion, nerve damage, local edema, skin necrosis, and pin track infection. 5,6 However, the technique of bone lengthening by gradual distraction was further developed and refined by Russian orthopeadic surgeon G.A. Ilizarov in Since distraction osteogenesis used local host tissue to regenerate new bone, it offers many potential advantages over bone grafting. Sources for autografts are limited and may leave local morbidity at the donor site. Allografts may transmit unknown antigens, bacteria or even viruses. As dead foreign bodies, allografts may not be desirable in infected wound. The use of distraction osteogenesis in the craniofacial skeleton was first reported by Snyder et al. 7 who used monofocal distraction to lengthen the canine mandible. Successful clinical bone lengthening in craniofacial surgery was first described by McCarthy et al. in Using extraoral distraction devices; McCarthy lengthened the congenital hypoplastic mandible in four children with Nager s syndrome. The result was satisfied with new bone formation without any relapse being found. Since then several clinical reports with a variety of devices and techniques are available to lengthen segments or entire maxillary or mandibular arches Although the application of the Ilizarov technique to the maxillofacial skeleton showed promising outcome, its use has not been widespread. Extraoral appliances have been effective in clinical cases, but their use has been hampered by many complications. 8,13 These included skin or bone necrosis, pin track infection, scarring, facial nerve and inferior alveolar nerve injury, and poor predictability. 8,14 Michieli and Miotti addressed these concerns by the use of a specially fabricated intraoral tooth-borne appliance to provide the necessary distraction. The development of intraoral appliances occurred in several centers and authorities as reported by Guerrero 15, McCarthy et al 16, Chin and Toth 9 and Diner et al Potential benefits of internal devices included 1) elimination of skin scars caused by translation of transcutaneous fixation pins, 2) improved patient compliance during the fixation or consolidation phase because there is no external component, and 3) improved stability of the attachment of the device to the bone. The following cases report demonstrated the use of intraoral distraction devices to correct a variety of maxillofacial skeletal deformities in four patients. These included mandibular lengthening in hemifacial microsomia and severe mandibular deficiency patients, maxillary distraction for hypoplastic maxilla in cleft lip and palate patient and interdental distraction of posterior maxilla in patients with benign odontogenic tumor after tumor resection. Cases illustration Case I An 11-year-old female presented with the diagnosis of left hemifacial microsomia type II b. Hypoplastic face and ear deformities were noticed on the left side of the face (Fig. 1: A1, A2). The radiographic examination revealed hypo-development of the right ramus and condyle with chin deviation to the affected side (Fig. 1: B1, B2). Severe malocclusion and canting of the occlusal plane to the right side were demonstrated (Fig. 1: C1 - C4). Mandibular ramus distraction osteogenesis was done using an intraoral partially submerged mandibular distraction device. The osteotomy was performed and the distraction device was installed in the planed 156 J DENT ASSOC THAI VOL. 65 NO. 3 JULY - SEPTEMBER 2015


.")

.")
.")
, left sagittal split ramus osteotomy")
.")
3 position leaving the activation rod outside the mucosal cuff (Fig. 1: D1 - D3). After the 3-day latency period the bone stumps were gradually separated by 0.5 mm twice a day to obtain a total bone lengthening of 14 mm (Fig. 1: E1). After a consolidation period of 8 weeks the device was removed without any complication. The facial asymmetry of the patient dramatically improved (Fig. 1: F1, F2). The radiographic study demonstrated a normal cortico-medullary pattern of the distraction gap indistinguishable from the adjacent native bone. The chin deviation was significantly improved by ramus lengthening (Fig. 1: G1, G2). The satisfied occlusion and less canting of the occlusal plane were obtained following the post-distraction orthodontic treatment (Fig. 1: H1 - H4). One year later, Phase II surgical correction was performed including right intraoral vertical ramus osteotomy (IVRO), left sagittal split ramus osteotomy (Lt SSRO) and advancement genioplasty to correct the residual deformities and obtain the optimum facial profile balance (Fig. 1: I1 I3; J1, J2). The stable occlusion and canting of the occlusal plane was corrected (Fig. 1: K1 K3; L1) PRE-OP A1 A2 B1 B2 C1 C2 C3 C4 INTRA-OP D1 D2 D3 E1 POST-OP1 F1 F2 G1 G3 2 H1 H2 H3 H4 Nuntanaranont et al.,



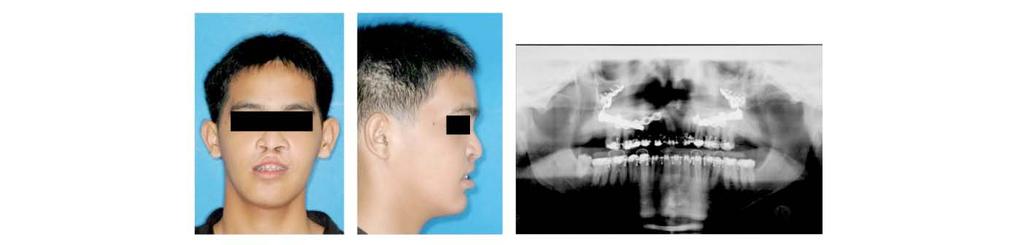
4 I1 I2 I3 J1 J2 K1 K2 K3 L1 Figure 1 Clinical case of an 11-year-old girl with hemifacial microsomia who underwent right mandibular ramus distraction osteogensis. A1 - A2 B1 - B2 C1 - C4 D1 - D3 E1 F1 - F2 G1 - G2 H1 - H4 I1 - I3 J1 - J2 K1 - K3, L1 Pre-operative view showed left hypoplastic face and ear deformities. Hypo-development of right ramus and condyle with chin deviation. Severe malocclusion and canting of the occlusal plane to the right side. A distraction device was fixed to the osteotomized bone and the surgical wound was closed leaving the activation rod exposed to the oral cavity. A 14-mm-distraction gap was achieved. Improvement of the hypodevelopment on the right side of the face. A distraction gap filled with radiographically normal bone and the lengthening mandible resulted in improvement of the deviated chin. Satisfactory occlusion and less canting of the occlusal plane. Clinical appearance of the patient after Phase II surgical correction including Rt IVRO, Lt SSRO and advancement genioplasty. The bone gap was completely healed and the facial profile was improved. Stable occlusion and canting of the occlusal plane was corrected. Case II An 11-year-old male presented with a marked retrusive chin caused by a non-syndromic severe mandibular deficiency (Fig. 2: A1 - A7). The functional orthodontic treatment to enhance mandibular growth was not successful after two years of treatment. Bilateral mandibular distraction osteogenesis was planned using 2 intraoral partially submerged mandibular distraction devices. The osteotomy line was cut just anterior to the mandibular angle. After complete bone separation, the distractor was placed in position guided by prediction tracing. A similar procedure was duplicated on the other side. The activation rods were left uncovered in both buccal vestibular areas (Fig. 2: B1 - B3). Gradual distraction of 0.5 mm twice a day was performed after a 3 days latency period. The vector of the distraction movement was controlled by the preformed occlusal splint with a total distance gain in both sides of approximately 14 mm (Fig. 2: B4, B5). After the consolidation 158 J DENT ASSOC THAI VOL. 65 NO. 3 JULY - SEPTEMBER 2015




 after postoperative orthodontic treatment.")
.")
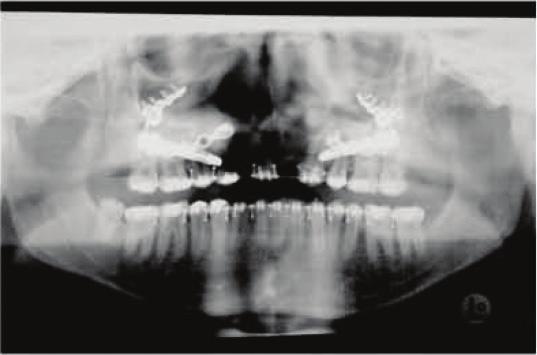
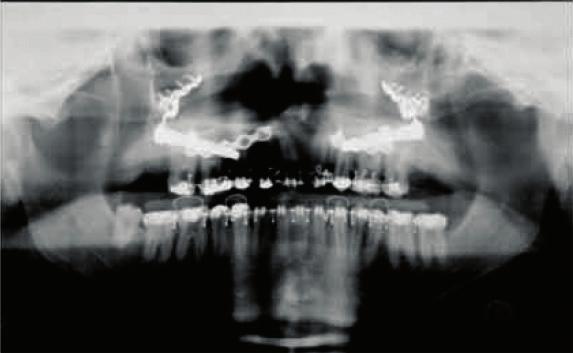
5 period of 8 weeks, the distraction devices were removed without any complication. The clinical facial profile was significantly improved with a straight profile and better chin prominence (Fig. 2: C1 - C3). The radiographs showed a 14 mm gain with normal cortico-medullary pattern of new bone in the previous distraction gap similar to the adjacent normal bone (Fig. 2: C4, C5). The final class I occlusion was achieved (Fig. 2: C6 - C8) after postoperative orthodontic treatment. The occlusion was stable without relapse after 3 years follow up (Fig. 2: D1 - D7). PRE-OP A1 A2 A3 A4 INTRA-OP A5 A6 A7 B1 B2 B3 B4 B5 C1 C2 C3 C4 C5 POST-OP C6 C7 C8 D1 D2 D3 D4 Nuntanaranont et al.,


6 POST-OP 3 YR D5 D6 D7 Figure 2 Clinical case of an 11-year-old male with a severe retrusive chin receiving mandibular lengthening by bilateral distraction osteogenesis of mandibular body. A1 - A7 B1 - B3 B4 - B5 C1 - C3 C4 - C5 C6 - C8 D1 - D7 Clinical appearance of the patient showed marked retrusive chin and malocclusion from severe mandibular deficiency. The distractor were placed after mandibular osteotomy on both sides and the mucosa was closed leaving the activation rod exposed in both buccal vestibules. 14-mm-distraction gap was created on both sides of the mandibular body. A dramatically improved of the facial profile with normal chin projection postoperatively. A normal radiographic pattern of mature bone filled in the distraction gap. Class I occlusion was achieved after post-distraction orthodontic treatment. Final stable occlusion was stable without any relapse was detected after 3 years follow up. Case III An 18-year-old male born with a bilateral complete cleft lip and palate had undergone surgery for lip repair in infancy, and his cleft palate was repaired in early childhood. Alveolar bone grafting had been performed two years prior the operation with satisfactory results. The residual problem was severe hypoplasia of the maxilla resulting in a concaved facial profile with large negative anterior overjet (Fig. 3: A1 - A7). Maxillary distraction osteogenesis was planned using an intraoral bone borne maxillary distractor. Le Fort I level osteotomy was performed, and the maxilla was partially mobilized to facilitate the distraction movement. The distraction devices were placed according to the planned direction according to the lateral cephalometric film prediction tracing on both sides of the maxilla and fixed on the zygomatic buttress and subapical areas with titanium screws (Fig. 3: B1 - B7). The activation was done intraoperatively to confirm the possibility of the maxillary bone movement vector and stability. The surgical wound was closed leaving the activation rod uncovered in the anterior vestibular area. After a latency of 3 days, activation of both maxillary distracters commenced at 1 mm per day in 2 rhythms. An advance of the maxilla by 12 mm was achieved. Eventually the dramatically improvement of the facial profile and stable class I occlusal relationship were obtained (Fig. 3: C1 - C3). Quality of life was achieved from both significantly improved in facial profile and good occlusion after the postoperative orthodontic treatment without any relapse (Fig. 3: D1 - D7). PRE-OP A1 A2 A3 A4 160 J DENT ASSOC THAI VOL. 65 NO. 3 JULY - SEPTEMBER 2015


7 PRE-OP A5 A6 A7 B1 B2 B3 B4 INTRA-OP B5 B6 B7 IMM.POST-DO C1 C2 C3 POST-OP D1 D2 D3 D4 D5 D6 D7 Nuntanaranont et al.,
8 Figure 3 Clinical courses of an 18-year-old male born with bilateral cleft lip and palate who underwent maxillary distraction osteogenesis for correcting cleft maxillary hypoplasia. A1 - A7 B1 - B4 B5 - B7 C1 - C3 D1 - D4 D5 - D7 A clinical examination and radiographic study revealed a concaved facial profile from severe maxillary deficiency and marked negative overjet. Le Fort I level osteotomy was performed and minimum mobilized. The distraction devices were fixed on both sides. The exposed activation rods were located at the anterior vestibule. Excellent position of the devices were achieved by pre-bending of the distractor in the individual fabricated stereo-model. Clinical appearance of the patient after 12 mm gradual maxillary advancement, the improved facial profile and stable class I occlusion were achieved. Significant improvement of the facial profile and normal radiographic pattern of bone remodeling with normal relationship of both jaw bones. Class I occlusion was achieved after postoperative orthodontic treatment with stable occlusion without any relapse. Case IV A 51-year-old female patient presented with a painless slow growing mass at the right posterior maxilla with pathological diagnosis of cementoblastoma (Fig. 4: A1 - A5). The tumor with the adjacent bone including the molar teeth and maxillary tuberosity were surgically removed by partial maxillectomy (Fig. 4: B1 - B3). A vertical interdental osteotomy line between the maxillary canine and first premolar teeth for a subapical bone osteotomy was performed. The transported dentoosseous segment comprised of two premolar teeth and its alveolar process was completely mobilized leaving only the palatal pedicle as the source of blood supply. The mandibular ramus distraction device was modified and placed on the buccal surface and fixed to the transported segment and apical bone above the canine area (Fig. 4: B4 - B7). The vector of the distraction was adjusted to accord with the posterior maxillary arch form and lower dentition. Following a 3 days latency period, the distractor was activated, 0.5 mm per time, twice daily for 13 consecutive days. A distraction gap of approximately 13 mm was achieved between the right maxillary canine and the first premolar (Fig. 4: C1 - C3). The distraction device had good stability during the distraction procedure and throughout the 6 weeks consolidation period. The transported segment was moved posteriorly along the planned direction until the maxillary second premolar occluded on the mandibular second molar without any occlusal interference. The regenerated tissue in the distraction gap eventually healed with normal contour and covered with soft tissue similar to the adjacent mucosa (Fig. 4: D1, D2). The radiographic and histological study obtained from the tissue in the distraction area demonstrated newly formed bone in the distraction gap with normal gingival tissue coverage (Fig. 4: D3 - D5). Six months after the consolidation period, the distracted gap was reentry and dental implant was inserted into the normal appearance regenerated bone. Eventually the final dental prosthesis was successfully constructed with fully function. 162 J DENT ASSOC THAI VOL. 65 NO. 3 JULY - SEPTEMBER 2015






9 PRE-OP A1 A2 A3 A4 A5 B1 B2 B3 B4 INTRA-OP B5 B6 B7 IMM.POST-DO POST-OP C1 C2 C3 D1 D2 D3 D4 D5 Figure 4 A clinical case of a 51-year-old female patient with diagnosis of cementoblastoma underwent interdental transport distraction osteogenesis. A1 - A5 A painless slow growing mass at the right posterior maxilla with diagnosis of cementoblastoma. B1 - B3 A right posterior partial maxillectomy was performed. B4 - B7 An interdental osteotomy line between the maxillary canine and the first premolar teeth was created to mobilize the transported segment then the distraction device was fixed to secure the segments. C1 - C3 Following gradual distraction, a distraction gap of approximately 13 mm was achieved. D1- D2 Regenerated tissue in the distraction gap eventually healed with normal contour and covered with intact mucosa. D3 - D5 Radiographic and histological study showed new bone formation in the distraction gap with normal gingival tissue coverage. Nuntanaranont et al.,
10 Discussion The technique of distraction osteogenesis involves creation of new bone by gradual movement of two or more bony fragments following their surgical division. This technique can provide required amounts of regenerated bone in the skeleton that still has the potential of fracture healing. Distraction osteogenesis was first developed in the field of orthopaedic surgery and was principally utilized in limb lengthening. Knowledge from long bone lengthening provided the major basis for development of the distraction osteogenesis in the membranous bone of the craniofacial skeleton. Nevertheless, application of extraoral distraction devices in the maxillofacial region does not seem to be popular with the majority of the patients because of the cumbersome appearance, scar tissue formation and social adjustment. The innovation of the intraoral distraction devices provided treatment that is more acceptable in the mainstream practice of maxillofacial surgery. The intraoral approach for device placement can avoid skin incision that resulted in reducing the risk of injury to the nerves such as marginal mandibular branch of facial nerve. The other potential benefits include no skin scars caused by translation of transcutaneous fixation pins, improved compliance during the long consolidation phase, and no maintenance is required because the submerged placement. Nevertheless the drawbacks of this technique are the expensive sophisticated device and multiple operation including device installation and removal. In addition, in some cases the adjunction surgical procedure must be performed to obtain the optimum result. In the present study demonstrated four clinical cases with different deformities using an intraoral distraction device to correct the skeletal deficiencies with satisfactory outcomes. Mandibular lengthening in the present report was performed in an early stage of life in hemifacial microsomia patient. This deformity should be treated as early as possible since mandibular asymmetry becomes worse over time in comparison to the normal growth of the non-affected, contralateral side. This then leads to secondary malformation of the maxilla, nose and orbit. A progression of facial deformity and psychological problems may occur with time. 19 Therefore, the mandible should be operated upon early in order to support the growth of the adjacent structures and to avoid or minimize secondary deformities. In addition, in hemifacial microsomia, lengthening of the hypoplastic mandible will create an ipsilateral posterior open bite. The provided space will allow occlusal canting correction by orthodontic means over a short period by gradual selective grinding on the occlusal splint since there still has vertical growth of the maxilla in children when it is released from the constriction effect of the mandible and soft tissue. 20 By this protocol of treatment, the maxillary surgery can be avoided when comparing to the delay treatment in the adult stage with the conventional surgical operation. Major advancement of the maxilla is one of the unstable procedures since the movement of the large skeletal fragment of maxilla typically requires overcoming significant resistance from the soft tissue envelopes. This situation seems worse when the advancement of maxilla is performed in the cicatrized tissue from a previous operation in cleft palate patients. Incremental movement using distraction mechanics allows displacement of fragments over large distances because the soft tissue is allowed to accommodate slowly. The elongation of muscles, ligaments, vessels, nerves, subcutaneous fat, and skin that can not be achieved by other more radical procedures is one of the main advantages of this method. 21 By combining the conventional Le Fort I osteotomy with postoperative gradual distraction, a correction of severe overjet of approximately 12 mm was achieved in case III. Eventually a soft tissue facial profile and stable positive overjet occlusion was obtained without any detected relapse during the follow up period. In addition to the application of distraction osteogenesis to craniomaxillofacial defects, this modality of treatment could be modified to use in the dentoalveolar region. Interdental transport distraction osteogenesis 164 J DENT ASSOC THAI VOL. 65 NO. 3 JULY - SEPTEMBER 2015
11 was demonstrated in case IV. The transported dento-osseo segment comprised of two premolars, and their adjacent subapical bone was gradually moved posteriorly to close the distal defect created by the partial maxillectomy for tumor resection. The vector of movement was planned and controlled by distraction device to conform to the posterior maxillary arch, and lower dentition resulted in acceptable post-distraction occlusion. The regenerated tissue in the distraction gap eventually healed without any complications. The newly formed bone in the distraction alveolar segment and normal mucosal coverage could be demonstrated by both radiographic and histological studies. The transported segment retained good stability after distractor removal without detectable relapse and provided sufficient bone volume for implant placement. According to the satisfactory outcome, interdental transport distraction osteogenesis offers an alternative treatment for segmental defect reconstruction. The procedure could be performed in a single operation where the tumor was resected without additional donor site morbidity. Distraction ostegenesis demonstrates a significant role and provides a variety of applications in the maxillofacial region with acceptable results. The development of an intraoral distractor holds the promise of allowing the patient to enjoy a more normal life during the course of treatment. 22,23 Further development including design, miniaturization of the intraoral devices and multidirectional vectors are essential to reconstruct various parts for complex cranio-maxillofacial malformation. Long-term follow up is necessary to monitor the post-distraction growth potential and possible relapse References Ilizarov GA. The tension-stress effect on the genesis and growth of tissue: Part I. The influence of stability of fixation and soft-tissue preservation. Clin Orthop Relat Res 1989;238: Ilizarov GA. The tension-stress effect on the genesis and growth of tissues: Part II. The influence of the rate and frequency of distraction. Clin Orthop Relat Res 1989;239: Ilizarov GA. Clinical application of the tension-stress effect for limb lengthening. Clin Orthop Relat Res.1990;250: Codivilla A. On the means of lengthening in the lower limbs, the muscles and tissues which are shortened through deformity. Am J Orthop Surg 1905;2: Abbott LC. The operative lengthening of the tibia and fibula. J Bone Joint Surg (Br) 1927;9: Abbott LC, Saunders JB. The operative lengthening of the Tibia and Fibula: a preliminary report on the furhter development of the principles and technic. Ann Surg 1939; 110: Snyder CC, Levine GA, Swanson HM, Browne EZ Jr. Mandibular lengthening by gradual distraction. Plast Reconstr Surg 1973;51: McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg 1992;89: Chin M, Toth BA. Distraction osteogenesis in maxillofacial surgery using internal devices: review of five cases. J Oral Maxillofac Surg 1996;54: Block MS, Chang A, Crawford C. Mandibular alveolar ridge augmentation in the dog using distraction osteogenesis. J Oral Maxillofac Surg 1996;54: Altuna G, Walker DA, Freeman E. Rapid orthopedic lengthening of the mandible in primates by sagittal split osteotomy and distraction osteogenesis: a pilot study. Int J Adult Orthodon Orthognath Surg 1995;10: Rachmiel A, Levy M, Laufer D. Lengthening of the mandible by distraction osteogenesis: report of cases. J Oral Maxillofac Surg 1995;53: Molina F, Ortiz Monasterio F. Mandibular elongation and remodeling by distraction: a farewell to major osteotomies. Plast Reconstr Surg 1995;96: Aronson J. Experimental and clinical experience with distraction osteogenesis. Cleft Palate Craniofac J 1994;31: Guerrero CA, Bell WH, Contasti GI, Rodríguez AM. Intraoral mandibular distraction osteogenesis. Semin Orthod 1999;5: McCarthy JG, Staffenberg DA, Wood RJ, Cutting CB, Grayson BH, Nuntanaranont et al.,
12 Thorne CH. Introduction of an intraoral bone-lengthening device. Plast Reconstr Surg 1995;96: Diner PA, Kollar E, Martinez H, Vazquez MP. Submerged intraoral device for mandibular lengthening J Craniomaxillofac Surg 1997;25: Diner PA, Kollar EM, Martinez H, Vazquez MP.Intraoral distraction for mandibular lengthening: a technical innovation. J Craniomaxillofac Surg 1996;24:92-5. Murray JE, Kaban LB, Mulliken JB. Analysis and treatment of hemifacial microsomia. Plast Reconstr Surg 1984;74: Ortiz Monasterio F, Molina F, Andrade L, Rodriguez C, Sainz Arregui J. Simultaneous mandibular and maxillary distraction in hemifacial microsomia in adults: avoiding occlusal disasters. Plast Reconstr Surg 1997;100: Sawaki Y, Ohkubo H, Hibi H, Ueda M. Mandibular lengthening by distraction osteogenesis using osseointegrated implants and an intraoral device: a preliminary report. J Oral Maxillofac Surg 1996;54: Sawaki Y, Ohkubo H, Yamamoto H, Ueda M. Mandibular lengthening by intraoral distraction using osseointegrated implants. Int J Oral Maxiilofac Implants 1996;11: J DENT ASSOC THAI VOL. 65 NO. 3 JULY - SEPTEMBER 2015
Intraoral mandibular distraction osteogenesis in facial asymmetry patients with unilateral temporomandibular joint bony ankylosis
 Int. J. Oral Maxillofac. Surg. 2002; 31: 544 548 doi:10.1054/ijom.2002.0297, available online at http://www.idealibrary.com on Intraoral mandibular distraction osteogenesis in facial asymmetry patients
Int. J. Oral Maxillofac. Surg. 2002; 31: 544 548 doi:10.1054/ijom.2002.0297, available online at http://www.idealibrary.com on Intraoral mandibular distraction osteogenesis in facial asymmetry patients
Correction of Dentofacial Deformities (Orthognathic Surgery)
") Correction of Dentofacial Deformities (Orthognathic Surgery) BDS, MSc, German board of Oral and Maxillofacial Surgery ( Berlin-Germany), Doctoral degree by LBMS Definition Orthognathic surgery is a combination
Correction of Dentofacial Deformities (Orthognathic Surgery) BDS, MSc, German board of Oral and Maxillofacial Surgery ( Berlin-Germany), Doctoral degree by LBMS Definition Orthognathic surgery is a combination
Treatment of Mandibular Asymmetry by Distraction Osteogenesis and Orthodontics: A Report of Four Cases
 Case Report Treatment of Mandibular Asymmetry by Distraction Osteogenesis and Orthodontics: A Report of Four Cases Azita Tehranchi, DMD a ; Hossein Behnia, DMD b Abstract: Distraction osteogenesis devices
Case Report Treatment of Mandibular Asymmetry by Distraction Osteogenesis and Orthodontics: A Report of Four Cases Azita Tehranchi, DMD a ; Hossein Behnia, DMD b Abstract: Distraction osteogenesis devices
The America Association of Oral and Maxillofacial Surgeons classify occlusion/malocclusion in to the following three categories:
 Subject: Orthognathic Surgery Policy Effective Date: 04/2016 Revision Date: 07/2018 DESCRIPTION Orthognathic surgery is an open surgical procedure that corrects anomalies or malformations of the lower
Subject: Orthognathic Surgery Policy Effective Date: 04/2016 Revision Date: 07/2018 DESCRIPTION Orthognathic surgery is an open surgical procedure that corrects anomalies or malformations of the lower
Closure of an Oronasal Fistula in an Irradiated Palate by Tissue and Bone Distraction Osteogenesis CASE REPORT
 Closure of an Oronasal Fistula in an Irradiated Palate by Tissue and Bone Distraction Osteogenesis Peter J. Taub, MD* James P. Bradley, MD* Henry K. Kawamoto, MD, DDS* Los Angeles, California Pittsburgh,
Closure of an Oronasal Fistula in an Irradiated Palate by Tissue and Bone Distraction Osteogenesis Peter J. Taub, MD* James P. Bradley, MD* Henry K. Kawamoto, MD, DDS* Los Angeles, California Pittsburgh,
Case Report. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System.
 Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
Case Report Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System and MatrixORTHOGNATHIC Plating System. Orthognathic Correction of Class II Open Bite. Using the Piezoelectric System
What is Hemifacial Microsomia? By Pravin K. Patel, MD and Bruce S. Bauer, MD Children s Memorial Hospital, Chicago, IL
 What is Hemifacial Microsomia? By Pravin K. Patel, MD and Bruce S. Bauer, MD Children s Memorial Hospital, Chicago, IL 773-880-4094 Early in the child s embryonic development the structures destined to
What is Hemifacial Microsomia? By Pravin K. Patel, MD and Bruce S. Bauer, MD Children s Memorial Hospital, Chicago, IL 773-880-4094 Early in the child s embryonic development the structures destined to
GENERAL DISCUSSION & SUMMARY
 GENERAL 9 DISCUSSION & SUMMARY 139 140 Chapter 9 The aim of this thesis was to investigate problems, obstacles, and complications arising from treatment using mandibular DO. Further specification for various
GENERAL 9 DISCUSSION & SUMMARY 139 140 Chapter 9 The aim of this thesis was to investigate problems, obstacles, and complications arising from treatment using mandibular DO. Further specification for various
Dental Implants: A Predictable Solution for Tooth Loss. Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor
 Oral & Maxillofacial Surgeon Associate Clinical Professor") Dental Implants: A Predictable Solution for Tooth Loss Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor What are Dental Implants? Titanium posts used to replace missing
Dental Implants: A Predictable Solution for Tooth Loss Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor What are Dental Implants? Titanium posts used to replace missing
Case Report. Eduardo Yugo Suzuki a ; Masayo Watanabe b ; Boonsiva Buranastidporn c ; Yoshiyuki Baba d ; Kimie Ohyama e ; Masatoshi Ishii f
 Case Report Simultaneous Maxillary Distraction Osteogenesis Using a Twin-Track Distraction Device Combined with Alveolar Bone Grafting in Cleft Patients: Preliminary Report of a Technique Eduardo Yugo
Case Report Simultaneous Maxillary Distraction Osteogenesis Using a Twin-Track Distraction Device Combined with Alveolar Bone Grafting in Cleft Patients: Preliminary Report of a Technique Eduardo Yugo
Distraction osteogenesis therapy in patients affected by Goldenhar syndrome: a case series
 JOURNAL of OSSEOINTEGRATION FRANCESCO GRECCHI 1, GIOVANNI EVANGELISTA MANCINI 2, RAFFAELLA BIANCO 1, ILARIA ZOLLINO 3, FRANCESCO CARINCI 3 1 2 3 Consultant, Maxillofacial Surgery, Galeazzi Hospital, Milan,
JOURNAL of OSSEOINTEGRATION FRANCESCO GRECCHI 1, GIOVANNI EVANGELISTA MANCINI 2, RAFFAELLA BIANCO 1, ILARIA ZOLLINO 3, FRANCESCO CARINCI 3 1 2 3 Consultant, Maxillofacial Surgery, Galeazzi Hospital, Milan,
ORTHOGNATHIC SURGERY
 Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-16 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-16 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Intraoral mandibular distraction osteogenesis: special attention to treatment planning
 Journal of Cranio-Maxillofacial Surgery (2001) 29, 254 262 # 2001 European Association for Cranio-Maxillofacial Surgery doi:10.1054/jcms.2001.0235, available online at http://www.idealibrary.com on Intraoral
Journal of Cranio-Maxillofacial Surgery (2001) 29, 254 262 # 2001 European Association for Cranio-Maxillofacial Surgery doi:10.1054/jcms.2001.0235, available online at http://www.idealibrary.com on Intraoral
INTERNATIONAL MEDICAL COLLEGE
 INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Specialized Modules: List of individual modules Specialized Module 1 Basic principles of implantology
INTERNATIONAL MEDICAL COLLEGE Joint Degree Master Program: Implantology and Dental Surgery (M.Sc.) Specialized Modules: List of individual modules Specialized Module 1 Basic principles of implantology
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Treatment of Hemifacial Microsomia: A Case Report
 Iran J Ortho. 2015 June; 10(1):e4931. Published online 2015 June 13. doi: 10.17795/ijo-4931 Case Report Treatment of Hemifacial Microsomia: A Case Report Mohsen Shirazi, 1 Elahe Soltanmohamadi Borujeni,
Iran J Ortho. 2015 June; 10(1):e4931. Published online 2015 June 13. doi: 10.17795/ijo-4931 Case Report Treatment of Hemifacial Microsomia: A Case Report Mohsen Shirazi, 1 Elahe Soltanmohamadi Borujeni,
Case Reports Pediatric Mandibular Distraction Osteogenesis: The Present and the Future
 Case Reports Pediatric Mandibular Distraction Osteogenesis: The Present and the Future Samuel T. Rhee, MD, and Steven R. Buchman, MD Ann Arbor, Michigan Pediatric mandibular distraction osteogenesis (MDO)
Case Reports Pediatric Mandibular Distraction Osteogenesis: The Present and the Future Samuel T. Rhee, MD, and Steven R. Buchman, MD Ann Arbor, Michigan Pediatric mandibular distraction osteogenesis (MDO)
DISTRACTION PRODUCT OVERVIEW. For a wide variety of facial applications
 DISTRACTION PRODUCT OVERVIEW For a wide variety of facial applications DISTRACTION PRODUCT OVERVIEW. STRONG, MODULAR, VERSATILE CRANIOFACIAL DISTRACTION External Midface Distractor Distraction of the maxilla,
DISTRACTION PRODUCT OVERVIEW For a wide variety of facial applications DISTRACTION PRODUCT OVERVIEW. STRONG, MODULAR, VERSATILE CRANIOFACIAL DISTRACTION External Midface Distractor Distraction of the maxilla,
International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 01, October 2014, Pages
 Original article: Distraction osteogenesis following gap arthroplasty to correct facial asymmetry - a defined protocol in treatment of patients with temporomandibular joint ankylosis. 1Dr. Babu S. Parmar,
Original article: Distraction osteogenesis following gap arthroplasty to correct facial asymmetry - a defined protocol in treatment of patients with temporomandibular joint ankylosis. 1Dr. Babu S. Parmar,
Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery
 European Journal of Orthodontics 24 (2002) 471 476 2002 European Orthodontic Society Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery Kiyoshi
European Journal of Orthodontics 24 (2002) 471 476 2002 European Orthodontic Society Post-operative stability of the maxilla treated with Le Fort I and horseshoe osteotomies in bimaxillary surgery Kiyoshi
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/31632 holds various files of this Leiden University dissertation. Author: Mensink, Gertjan Title: Bilateral sagittal split osteotomy by the splitter-separator
Cover Page The handle http://hdl.handle.net/1887/31632 holds various files of this Leiden University dissertation. Author: Mensink, Gertjan Title: Bilateral sagittal split osteotomy by the splitter-separator
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S.
 THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S. Skeletal anchorage, the concept of using the facial skeleton to control tooth
THE USE OF TEMPORARY ANCHORAGE DEVICES FOR MOLAR INTRUSION & TREATMENT OF ANTERIOR OPEN BITE By Eduardo Nicolaievsky D.D.S. Skeletal anchorage, the concept of using the facial skeleton to control tooth
MORPHOFUNCTIONAL APPROACH TO TREAT TMJ ANKYLOSIS RESECTION OF TMJ ANKYLOSIS. FACIAL ASYMMETRY CORRECTION Prof. Dr. Dr. Srinivas Gosla Reddy
 MORPHOFUNCTIONAL APPROACH TO TREAT TMJ ANKYLOSIS RESECTION OF TMJ ANKYLOSIS FACIAL ASYMMETRY CORRECTION Prof. Dr. Dr. Srinivas Gosla Reddy MBBS MDS FDSRCS (Edin) FDSRCS (Eng) PhD Dr. Dr. Rajgopal Reddy
MORPHOFUNCTIONAL APPROACH TO TREAT TMJ ANKYLOSIS RESECTION OF TMJ ANKYLOSIS FACIAL ASYMMETRY CORRECTION Prof. Dr. Dr. Srinivas Gosla Reddy MBBS MDS FDSRCS (Edin) FDSRCS (Eng) PhD Dr. Dr. Rajgopal Reddy
LOGIC SURGICAL TECHNIQUE GUIDE. In d i c at i o n s. Co n t r a i n d i c at i o n s. Mandibular Distraction System
 TM SURGICAL TECHNIQUE GUIDE In d i c at i o n s The OSTEOMED Mandibular Distractor system is indicated for use as a mandibular bone lengthener for patients diagnosed with conditions where treatment includes
TM SURGICAL TECHNIQUE GUIDE In d i c at i o n s The OSTEOMED Mandibular Distractor system is indicated for use as a mandibular bone lengthener for patients diagnosed with conditions where treatment includes
Topic: Orthognathic Surgery Date of Origin: October 5, Section: Surgery Last Reviewed Date: December 2013
 Medical Policy Manual Topic: Orthognathic Surgery Date of Origin: October 5, 2004 Section: Surgery Last Reviewed Date: December 2013 Policy No: 137 Effective Date: March 1, 2014 IMPORTANT REMINDER Medical
Medical Policy Manual Topic: Orthognathic Surgery Date of Origin: October 5, 2004 Section: Surgery Last Reviewed Date: December 2013 Policy No: 137 Effective Date: March 1, 2014 IMPORTANT REMINDER Medical
MAHP Orthognathic Surgery Guidelines. Medical Policy Statement. Criteria
 Introduction The word orthognathic comes from the Greek words for straighten and jaw. Orthognathic surgery is the surgical correction of abnormalities of the mandible and/or maxilla. 1 It involves the
Introduction The word orthognathic comes from the Greek words for straighten and jaw. Orthognathic surgery is the surgical correction of abnormalities of the mandible and/or maxilla. 1 It involves the
Postoperative Evaluation on SSRO performed by Short Lingual Osteotomy and IVRO
 140 J Meikai Dent Med 43 2, 140 147, 2014 Short Lingual Osteotomy SSRO IVRO 1 1 1 1 1 1 2 2 1 2 1 1 2 SSRO SSRO IVRO SSRO short lingual osteotomy SL SL IVRO SL 4 6 IVRO SL IVRO SL 1 IVRO SL short lingual
140 J Meikai Dent Med 43 2, 140 147, 2014 Short Lingual Osteotomy SSRO IVRO 1 1 1 1 1 1 2 2 1 2 1 1 2 SSRO SSRO IVRO SSRO short lingual osteotomy SL SL IVRO SL 4 6 IVRO SL IVRO SL 1 IVRO SL short lingual
Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document.
 ORTHOGNATHIC SURGERY Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
ORTHOGNATHIC SURGERY Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
ORTHOGNATHIC SURGERY
 ORTHOGNATHIC SURGERY MEDICAL POLICY Effective Date: February 1, 2017 Review Dates: 1/93, 7/95, 10/97, 4/99, 10/00, 8/01, 12/01, 4/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11,
ORTHOGNATHIC SURGERY MEDICAL POLICY Effective Date: February 1, 2017 Review Dates: 1/93, 7/95, 10/97, 4/99, 10/00, 8/01, 12/01, 4/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11,
Developing Facial Symmetry Using an Intraoral Device: A Case Report
 Developing Facial Symmetry Using an Intraoral Device: A Case Report by Theodore R. Belfor, D.D.S.; and G. Dave Singh, D.D.Sc., Ph.D., B.D.S. Dr. Theodore Belfor graduated from New York University College
Developing Facial Symmetry Using an Intraoral Device: A Case Report by Theodore R. Belfor, D.D.S.; and G. Dave Singh, D.D.Sc., Ph.D., B.D.S. Dr. Theodore Belfor graduated from New York University College
Case Study. Case # 1 Author: Dr. Suheil Boutros (USA) 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.
 2013 Zimmer Dental, Inc. All rights reserved. 6557, Rev. 03/13.") Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
Placement of a Zimmer Trabecular Metal Dental Implant with Simultaneous Ridge Augmentation and Immediate Non-Functional Loading Following Tooth Extraction and Orthodontic Treatment for Implant Site Development
CHAPTER 8 SECTION 1.4 ORAL SURGERY TRICARE/CHAMPUS POLICY MANUAL M DEC 1998 SPECIAL BENEFIT INFORMATION
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report
 Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Assessment of Relapse Following Intraoral Vertical Ramus Osteotomy Mandibular Setback and Short-term Immobilization
 Assessment of Relapse Following Intraoral Vertical Ramus Osteotomy Mandibular Setback and Short-term Immobilization Koroush Taheri Talesh, DDS, a Mohammad Hosein Kalantar Motamedi, DDS, b Mahdi Sazavar,
Assessment of Relapse Following Intraoral Vertical Ramus Osteotomy Mandibular Setback and Short-term Immobilization Koroush Taheri Talesh, DDS, a Mohammad Hosein Kalantar Motamedi, DDS, b Mahdi Sazavar,
Christoph Kunz, MD, DMD,* Lorenz Brauchli, MD, Torsten Moehle, Berton Rahn, MD, DMD, and Beat Hammer, MD, DMD
 J Oral Maxillofac Surg 61:364-368, 2003 Theoretical Considerations for the Surgical Correction of Mandibular Deformity in Hemifacial Microsomia Patients Using Multifocal Distraction Osteogenesis Christoph
J Oral Maxillofac Surg 61:364-368, 2003 Theoretical Considerations for the Surgical Correction of Mandibular Deformity in Hemifacial Microsomia Patients Using Multifocal Distraction Osteogenesis Christoph
Educational Training Document
 Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Educational Training Document Table of Contents Part 1: Resource Document Disclaimer Page: 2 Part 2: Line Item Grade Sheets Page: 3 Release: 11/2016 Page 1 of 6 Part 1: Resource Document Disclaimer The
Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report
 Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
2018 Dental Code Set For dates of service from 1/1/ /31/2018
 D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT D0140 LIMITED ORAL EVALUATION - PROBLEM FOCUSED D0150 COMPREHENSIVE ORAL EVALUATION - NEW OR ESTABLISHED PATIENT D0160 DETAILED AND EXTENSIVE ORAL EVALUATION
D0120 PERIODIC ORAL EVALUATION - ESTABLISHED PATIENT D0140 LIMITED ORAL EVALUATION - PROBLEM FOCUSED D0150 COMPREHENSIVE ORAL EVALUATION - NEW OR ESTABLISHED PATIENT D0160 DETAILED AND EXTENSIVE ORAL EVALUATION
2018 Dental Code Set
 D0120 D0140 D0150 D0160 D0180 D0210 D0220 D0230 D0240 D0250 D0251 D0270 D0272 D0273 D0274 D0277 D0290 D0310 D0330 D0340 D0350 D0393 D0470 D0502 PERIODIC ORAL EVALUATION ESTABLISHED PATIENT LIMITED ORAL
D0120 D0140 D0150 D0160 D0180 D0210 D0220 D0230 D0240 D0250 D0251 D0270 D0272 D0273 D0274 D0277 D0290 D0310 D0330 D0340 D0350 D0393 D0470 D0502 PERIODIC ORAL EVALUATION ESTABLISHED PATIENT LIMITED ORAL
06/12/18. [Note: When orthognathic surgery is not a covered benefit, it is non-covered for any diagnosis, including sleep apnea.]
![06/12/18. [Note: When orthognathic surgery is not a covered benefit, it is non-covered for any diagnosis, including sleep apnea.]](/thumbs/84/91182117.jpg "06/12/18. [Note: When orthognathic surgery is not a covered benefit, it is non-covered for any diagnosis, including sleep apnea.]") Reference #: MC/B002 Page: 1 of 5 PRODUCT APPLICATION: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne Administrative Services, Inc. (PAS)
Reference #: MC/B002 Page: 1 of 5 PRODUCT APPLICATION: PreferredOne Community Health Plan (PCHP) PreferredOne Administrative Services, Inc. (PAS) ERISA PreferredOne Administrative Services, Inc. (PAS)
Stress Distribution in Mandible and. A 3-Dimensional Finite-element Anal. Katada, H; Arakawa, T; Ichimura, K; Author(s) Sameshima, GT
 Sameshima, GT") Stress Distribution in Mandible and TitleTemporomandibular Joint by Mandibul A 3-Dimensional Finite-element Anal Katada, H; Arakawa, T; Ichimura, K; Author(s) Sameshima, GT Journal Bulletin of Tokyo Dental
Stress Distribution in Mandible and TitleTemporomandibular Joint by Mandibul A 3-Dimensional Finite-element Anal Katada, H; Arakawa, T; Ichimura, K; Author(s) Sameshima, GT Journal Bulletin of Tokyo Dental
Oral Health and Dentistry
 Page 107 to 118 Volume 1 Issue 2 2017 Case Report Oral Health and Dentistry ISSN: 2573-4989 Full Mouth Implants Rehabilitation of a Patient with Ectodermal Dysplasia After 3-Ds Ridge Augmentation and Bilateral
Page 107 to 118 Volume 1 Issue 2 2017 Case Report Oral Health and Dentistry ISSN: 2573-4989 Full Mouth Implants Rehabilitation of a Patient with Ectodermal Dysplasia After 3-Ds Ridge Augmentation and Bilateral
The treatment of dentofacial deformities is
 CASE REPORT Orthodontic and surgical treatment of a patient with hemifacial microsomia Gustavo Zanardi, a Eduardo Varela Parente, b Lucas Senhorinho Esteves, b Rafael Seabra Louro, c and Jonas Capelli
CASE REPORT Orthodontic and surgical treatment of a patient with hemifacial microsomia Gustavo Zanardi, a Eduardo Varela Parente, b Lucas Senhorinho Esteves, b Rafael Seabra Louro, c and Jonas Capelli
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
LATERAL CEPHALOMETRIC EVALUATION IN CLEFT PALATE PATIENTS
 POLSKI PRZEGLĄD CHIRURGICZNY 2009, 81, 1, 23 27 10.2478/v10035-009-0004-2 LATERAL CEPHALOMETRIC EVALUATION IN CLEFT PALATE PATIENTS PRADEEP JAIN, ANAND AGARWAL, ARVIND SRIVASTAVA Department of Plastic
POLSKI PRZEGLĄD CHIRURGICZNY 2009, 81, 1, 23 27 10.2478/v10035-009-0004-2 LATERAL CEPHALOMETRIC EVALUATION IN CLEFT PALATE PATIENTS PRADEEP JAIN, ANAND AGARWAL, ARVIND SRIVASTAVA Department of Plastic
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults
 Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
ORTHOGNATHIC (JAW) SURGERY
 SURGERY") UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (IEX EPO, IEX PPO) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas,
UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (IEX EPO, IEX PPO) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas,
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: orthodontics_for_pediatric_patients 2/2014 10/2017 10/2018 10/2017 Description of Procedure or Service Children
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: orthodontics_for_pediatric_patients 2/2014 10/2017 10/2018 10/2017 Description of Procedure or Service Children
Professor, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital,
 Dr. Ellen Wen-Ching Ko, DDS, MS Professor, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taipei, Taiwan Professor, Graduate Institute of Craniofacial and Dental Science, Chang
Dr. Ellen Wen-Ching Ko, DDS, MS Professor, Department of Craniofacial Orthodontics, Chang Gung Memorial Hospital, Taipei, Taiwan Professor, Graduate Institute of Craniofacial and Dental Science, Chang
 Evaluation of the maxillary morphological changes following distraction in CLP patients decrease in the Ul to NF except for Case 6. me [35] instance,血e small maxillary advancement of 2.4 mm and maxillary
Evaluation of the maxillary morphological changes following distraction in CLP patients decrease in the Ul to NF except for Case 6. me [35] instance,血e small maxillary advancement of 2.4 mm and maxillary
Longitudinal dento-skeletal changes in UCLP patients following maxillary distraction osteogenesis using RED system
 J Med Dent Sci 2004; 51: 27 33 Original Article Longitudinal dento-skeletal changes in UCLP patients following maxillary distraction osteogenesis using RED system Eduardo Yugo Suzuki, Nobuyoshi Motohashi
J Med Dent Sci 2004; 51: 27 33 Original Article Longitudinal dento-skeletal changes in UCLP patients following maxillary distraction osteogenesis using RED system Eduardo Yugo Suzuki, Nobuyoshi Motohashi
ORTHOGNATHIC (JAW) SURGERY
 SURGERY") ORTHOGNATHIC (JAW) SURGERY UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 069.12 T2 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
ORTHOGNATHIC (JAW) SURGERY UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 069.12 T2 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF COVERAGE...
ORTHOGNATHIC (JAW) SURGERY
 SURGERY") Oxford ORTHOGNATHIC (JAW) SURGERY UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 069.14 T2 Effective Date: October 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF
Oxford ORTHOGNATHIC (JAW) SURGERY UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 069.14 T2 Effective Date: October 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 CONDITIONS OF
Mixed-reality simulation for orthognathic surgery
 Fushima and Kobayashi Maxillofacial Plastic and Reconstructive Surgery (2016) 38:13 DOI 10.1186/s40902-016-0059-z METHODOLOGY Mixed-reality simulation for orthognathic surgery Kenji Fushima 1* and Masaru
Fushima and Kobayashi Maxillofacial Plastic and Reconstructive Surgery (2016) 38:13 DOI 10.1186/s40902-016-0059-z METHODOLOGY Mixed-reality simulation for orthognathic surgery Kenji Fushima 1* and Masaru
PAIN PERCEPTION DURING MINIPLATE-ASSISTED ORTHODONTIC THERAPY
 PAIN PERCEPTION DURING MINIPLATE-ASSISTED ORTHODONTIC THERAPY Yu-Chuan Tseng, 1 Chun-Ming Chen, 2 Huang-Chi Wang, 3 Chau-Hsiang Wang, 4 Huey-Er Lee, 4 and Kun-Tsung Lee 5 Departments of 1 Orthodontics,
PAIN PERCEPTION DURING MINIPLATE-ASSISTED ORTHODONTIC THERAPY Yu-Chuan Tseng, 1 Chun-Ming Chen, 2 Huang-Chi Wang, 3 Chau-Hsiang Wang, 4 Huey-Er Lee, 4 and Kun-Tsung Lee 5 Departments of 1 Orthodontics,
Intraoral Distraction Osteogenesis of the Mandible in Hemifacial Microsomia
 J Oral Maxillofac Surg 59:728-733, 2001 Intraoral Distraction Osteogenesis of the Mandible in Hemifacial Microsomia Adi Rachmiel, DMD, PhD,* Ronen Manor, DMD, Micha Peled, DMD, MD, and Dov Laufer, DMD
J Oral Maxillofac Surg 59:728-733, 2001 Intraoral Distraction Osteogenesis of the Mandible in Hemifacial Microsomia Adi Rachmiel, DMD, PhD,* Ronen Manor, DMD, Micha Peled, DMD, MD, and Dov Laufer, DMD
BUILDING A. Achieving total reconstruction in a single operation. 70 OCTOBER 2016 // dentaltown.com
 BUILDING A MANDI Achieving total reconstruction in a single operation by Dr. Fayette C. Williams Fayette C. Williams, DDS, MD, FACS, is clinical faculty at John Peter Smith Hospital in Fort Worth, Texas,
BUILDING A MANDI Achieving total reconstruction in a single operation by Dr. Fayette C. Williams Fayette C. Williams, DDS, MD, FACS, is clinical faculty at John Peter Smith Hospital in Fort Worth, Texas,
Sample Case #1. Disclaimer
 ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
Cephalometric Analysis
 Cephalometric Analysis of Maxillary and Mandibular Growth and Dento-Alveolar Change Part III In two previous articles in the PCSO Bulletin s Faculty Files, we discussed the benefits and limitations of
Cephalometric Analysis of Maxillary and Mandibular Growth and Dento-Alveolar Change Part III In two previous articles in the PCSO Bulletin s Faculty Files, we discussed the benefits and limitations of
Alveolar Bone Remodeling and Development after Immediate Orthodontic Root Movement
 Journal of Dental Health, Oral Disorders & Therapy Alveolar Bone Remodeling and Development after Immediate Orthodontic Root Abstract Introduction: Adult orthodontics is rapidly expanding primarily due
Journal of Dental Health, Oral Disorders & Therapy Alveolar Bone Remodeling and Development after Immediate Orthodontic Root Abstract Introduction: Adult orthodontics is rapidly expanding primarily due
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note
 Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Interesting Case Series. Virtual Surgical Planning in Orthognathic Surgery
 Interesting Case Series Virtual Surgical Planning in Orthognathic Surgery Suraj Jaisinghani, MS, a Nicholas S. Adams, MD, b,c Robert J. Mann, MD, b,c,d John W. Polley, MD, b,c,d, and John A. Girotto, MD,
Interesting Case Series Virtual Surgical Planning in Orthognathic Surgery Suraj Jaisinghani, MS, a Nicholas S. Adams, MD, b,c Robert J. Mann, MD, b,c,d John W. Polley, MD, b,c,d, and John A. Girotto, MD,
King's College Hospital Dental School, London, S.E. 5.
 OSTECTOMY AT THE MANDIBULAR SYMPHYSIS J. H. SOWRAY, B.D.S., F.D.S.R.C.S. (Eng.), L.R.C.P., M.R.C.S. and R. HASKELL, M.B., B.S., F.D.S.R.C.S. (Eng.). King's College Hospital Dental School, London, S.E.
OSTECTOMY AT THE MANDIBULAR SYMPHYSIS J. H. SOWRAY, B.D.S., F.D.S.R.C.S. (Eng.), L.R.C.P., M.R.C.S. and R. HASKELL, M.B., B.S., F.D.S.R.C.S. (Eng.). King's College Hospital Dental School, London, S.E.
Reconstruction of a Maxillary Oncologic Defect with a Fibula Osteocutaneous Flap. Using Synthes ProPlan CMF and the MatrixMIDFACE Plating System.
 Case Report Reconstruction of a Maxillary Oncologic Defect with a Fibula Osteocutaneous Flap. Using Synthes ProPlan CMF and the MatrixMIDFACE Plating System. Reconstruction of a Maxillary Oncologic Defect
Case Report Reconstruction of a Maxillary Oncologic Defect with a Fibula Osteocutaneous Flap. Using Synthes ProPlan CMF and the MatrixMIDFACE Plating System. Reconstruction of a Maxillary Oncologic Defect
Research report for MSc Dent. University of Witwatersrand. Faculty of health science. Dr J Beukes. Student number: h
 Research report for MSc Dent University of Witwatersrand Faculty of health science Dr J Beukes Student number: 9507510h Supervisor: Prof JP Reyneke October 2011 1 1. Title 2. Aim 3. Introduction 4. Objectives
Research report for MSc Dent University of Witwatersrand Faculty of health science Dr J Beukes Student number: 9507510h Supervisor: Prof JP Reyneke October 2011 1 1. Title 2. Aim 3. Introduction 4. Objectives
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Surgically assisted rapid palatal expansion (SARPE) prior to combined Le Fort I and sagittal osteotomies: A case report
 prior to combined Le Fort I and sagittal osteotomies: A case report") 200 Carlos Alberto E. Tavares, DDS, MS, DOrth Professor Department of Orthodontics Associação Brasileira de Odontologia - RS Porto Alegre, Brazil Miguel Scheffer, DDS, MS Chairman Department of Oral and
200 Carlos Alberto E. Tavares, DDS, MS, DOrth Professor Department of Orthodontics Associação Brasileira de Odontologia - RS Porto Alegre, Brazil Miguel Scheffer, DDS, MS Chairman Department of Oral and
NC Medicaid Dental Reimbursement Rates General Dentist, Oral Surgeon, Pediatric Dentist, Periodontist, & Orthodontist Effective Date: January 1, 2017
 NC Dental Reimbursement s Refer to the NC and Health Choice Clinical Coverage Policies on the DMA website. D0120 Periodic oral evaluation 24.51 D0140 Limited oral evaluation - problem focused 34.94 D0145
NC Dental Reimbursement s Refer to the NC and Health Choice Clinical Coverage Policies on the DMA website. D0120 Periodic oral evaluation 24.51 D0140 Limited oral evaluation - problem focused 34.94 D0145
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Oral and Maxillofacial Surgery Privileges REAPPOINTMENT Effective from July 1, 2015 to June 30, 2016
 Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the Health Authority or Hospital, effective: 11/Dec/2014.
Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the Health Authority or Hospital, effective: 11/Dec/2014.
Non-surgical management of skeletal malocclusions: An assessment of 100 cases
 Non-surgical management of skeletal malocclusions: An assessment of 100 cases In early 1970 s reduced risks associated with surgical procedures allowed the treatment planning process for skeletal malocclusions
Non-surgical management of skeletal malocclusions: An assessment of 100 cases In early 1970 s reduced risks associated with surgical procedures allowed the treatment planning process for skeletal malocclusions
Management of Severe Mandibular Retrognathia in the Adult Patient Using Distraction Osteogenesis
 CLINICAL CONTROVERSIES IN ORAL AND MAXILLOFACIAL SURGERY: PART TWO J Oral Maxillofac Surg 60:1341-1346, 2002 Management of Severe Mandibular Retrognathia in the Adult Patient Using Distraction Osteogenesis
CLINICAL CONTROVERSIES IN ORAL AND MAXILLOFACIAL SURGERY: PART TWO J Oral Maxillofac Surg 60:1341-1346, 2002 Management of Severe Mandibular Retrognathia in the Adult Patient Using Distraction Osteogenesis
Revisions for CDT 2016
 Revisions for CDT 2016 This document was developed from preliminary actions of the Code Maintenance Committee (CMC). This document has been compared to the CMC meeting notes and the ASCII file. This document
Revisions for CDT 2016 This document was developed from preliminary actions of the Code Maintenance Committee (CMC). This document has been compared to the CMC meeting notes and the ASCII file. This document
Medical Policy Oral and Maxillofacial Surgery and Procedures
 Medical Policy Oral and Maxillofacial Surgery and Procedures Document Number: 003 Commercial and Qualified Health Plans MassHealth Authorization required X X No Prior Authorization *Cleft lip and palate
Medical Policy Oral and Maxillofacial Surgery and Procedures Document Number: 003 Commercial and Qualified Health Plans MassHealth Authorization required X X No Prior Authorization *Cleft lip and palate
2016 Dental Code Set For dates of service from 1/1/16-12/31/16
 HCPCS DESCRIPTIONS D0120 D0140 D0150 D0160 D0180 D0210 D0220 D0230 D0240 D0250 D0260 D0270 D0272 D0273 D0274 D0277 D0290 D0310 D0330 D0340 D0350 D0470 D0502 D1110 D1206 D1208 D1352 D2140 D2150 D2160 D2161
HCPCS DESCRIPTIONS D0120 D0140 D0150 D0160 D0180 D0210 D0220 D0230 D0240 D0250 D0260 D0270 D0272 D0273 D0274 D0277 D0290 D0310 D0330 D0340 D0350 D0470 D0502 D1110 D1206 D1208 D1352 D2140 D2150 D2160 D2161
By JOHN MARQUIS CONVERSE, M.D., and DAUBERT TELSEY, D.D.S.
 THE TRIPARTITE OSTEOTOMY OF THE MID-FACE FOR ORBITAL EXPANSION AND CORRECTION OF THE DEFORMITY IN CRANIOSTENOSIS By JOHN MARQUIS CONVERSE, M.D., and DAUBERT TELSEY, D.D.S. Center for Craniofacial Anomalies
THE TRIPARTITE OSTEOTOMY OF THE MID-FACE FOR ORBITAL EXPANSION AND CORRECTION OF THE DEFORMITY IN CRANIOSTENOSIS By JOHN MARQUIS CONVERSE, M.D., and DAUBERT TELSEY, D.D.S. Center for Craniofacial Anomalies
Restoration of Congenitally Missing Lateral Incisors with Single Stage Implants: An Interdisciplinary Approach
 10.5005/jp-journals-10012-1045 CASE REPORT Restoration of Congenitally Missing Lateral Incisors with Single Stage Implants: An Interdisciplinary Approach 1 Mitha M Shetty, 2 Akshai KR Shetty, 3 N Kalavathy,
10.5005/jp-journals-10012-1045 CASE REPORT Restoration of Congenitally Missing Lateral Incisors with Single Stage Implants: An Interdisciplinary Approach 1 Mitha M Shetty, 2 Akshai KR Shetty, 3 N Kalavathy,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Author(s) Fujimura, Kazuma; Bessho, Kazuhisa.
 Fujimura, Kazuma; Bessho, Kazuhisa.") Title Rigid fixation of intraoral mandibular prognathism. vertico Author(s) Fujimura, Kazuma; Bessho, Kazuhisa Citation Journal of oral and maxillofacial s 1173 Issue Date 2012-05 URL http://hdl.handle.net/2433/155855
Title Rigid fixation of intraoral mandibular prognathism. vertico Author(s) Fujimura, Kazuma; Bessho, Kazuhisa Citation Journal of oral and maxillofacial s 1173 Issue Date 2012-05 URL http://hdl.handle.net/2433/155855
Surgical Orthodontic Treatment Of Skeletal Class Iii Facial Asymmetry
 ISPUB.COM The Internet Journal of Bioengineering Volume 5 Number 1 Surgical Orthodontic Treatment Of Skeletal Class Iii Facial Asymmetry S Yadav, V Dhupar, F Akkara Citation S Yadav, V Dhupar, F Akkara.
ISPUB.COM The Internet Journal of Bioengineering Volume 5 Number 1 Surgical Orthodontic Treatment Of Skeletal Class Iii Facial Asymmetry S Yadav, V Dhupar, F Akkara Citation S Yadav, V Dhupar, F Akkara.
Contemporary Implant Dentistry
 Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Severe Malocclusion: Appropriately Timed Treatment. This article discusses challenging issues clinicians face when treating
 Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
Maxillary Growth Control with High Pull Headgear- A Case Report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. X January. (2018), PP 09-13 www.iosrjournals.org Maxillary Growth Control with High
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. X January. (2018), PP 09-13 www.iosrjournals.org Maxillary Growth Control with High
Simultaneous gap arthroplasty and intraoral distraction and secondary contouring surgery for unilateral temporomandibular joint ankylosis
 Sharma et al. Maxillofacial Plastic and Reconstructive Surgery (2016) 38:12 DOI 10.1186/s40902-016-0058-0 CASE REPORT Open Access Simultaneous gap arthroplasty and intraoral distraction and secondary contouring
Sharma et al. Maxillofacial Plastic and Reconstructive Surgery (2016) 38:12 DOI 10.1186/s40902-016-0058-0 CASE REPORT Open Access Simultaneous gap arthroplasty and intraoral distraction and secondary contouring
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Surgical Treatment of the Nasal-Maxillary Complex in Adolescents With Cleft Lip and Palate
 Surgical Treatment of the Nasal-Maxillary Complex in Adolescents With Cleft Lip and Palate Fernando D. Burstein MD, FACS, FAAP Atlanta, Georgia, USA Rather than treating nasal, maxillary, and soft tissue
Surgical Treatment of the Nasal-Maxillary Complex in Adolescents With Cleft Lip and Palate Fernando D. Burstein MD, FACS, FAAP Atlanta, Georgia, USA Rather than treating nasal, maxillary, and soft tissue
Orthognathic treatment of facial asymmetry due to temporomandibular joint ankylosis
 Orthognathic treatment of facial asymmetry due to temporomandibular joint ankylosis Ayse Gulsen 1, Serhat Sibar 2, Selahattin Ozmen 3 1 Department of Plastic, Reconstructive, and Aesthetic Surgery, Gazi
Orthognathic treatment of facial asymmetry due to temporomandibular joint ankylosis Ayse Gulsen 1, Serhat Sibar 2, Selahattin Ozmen 3 1 Department of Plastic, Reconstructive, and Aesthetic Surgery, Gazi
DOWNLOAD OR READ : RIGID FIXATION FOR MAXILLOFACIAL SURGERY PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : RIGID FIXATION FOR MAXILLOFACIAL SURGERY PDF EBOOK EPUB MOBI Page 1 Page 2 rigid fixation for maxillofacial surgery rigid fixation for maxillofacial pdf rigid fixation for maxillofacial
DOWNLOAD OR READ : RIGID FIXATION FOR MAXILLOFACIAL SURGERY PDF EBOOK EPUB MOBI Page 1 Page 2 rigid fixation for maxillofacial surgery rigid fixation for maxillofacial pdf rigid fixation for maxillofacial
Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis
 CASE REPORT Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis Dr Ashish Yadav 1, Dr Aratee Gupta 2, Dr Archana Singh 3, 1,3-
CASE REPORT Rehabilitation of atrophic partially edentulous mandible using ridge split technique and implant supported removable prosthesis Dr Ashish Yadav 1, Dr Aratee Gupta 2, Dr Archana Singh 3, 1,3-
Virtual model surgery and wafer fabrication for orthognathic surgery
 Int. J. Oral Maxillofac. Surg. 2009; 38: 1306 1323 available online at http://www.sciencedirect.com Technical Note Orthognathic Surgery Virtual model surgery and wafer fabrication for orthognathic surgery
Int. J. Oral Maxillofac. Surg. 2009; 38: 1306 1323 available online at http://www.sciencedirect.com Technical Note Orthognathic Surgery Virtual model surgery and wafer fabrication for orthognathic surgery
The Application of Cone Beam CT Image Analysis for the Mandibular Ramus Bone Harvesting
 44 The Application of Cone Beam CT Image Analysis for the Mandibular Ramus Bone Harvesting LivingWell Institute of Dental Research Lee, Jang-yeol, Youn, Pil-sang, Kim, Hyoun-chull, Lee Sang-chull Ⅰ. Introduction
44 The Application of Cone Beam CT Image Analysis for the Mandibular Ramus Bone Harvesting LivingWell Institute of Dental Research Lee, Jang-yeol, Youn, Pil-sang, Kim, Hyoun-chull, Lee Sang-chull Ⅰ. Introduction
Treatment of Condylar Hypoplasia with Distraction Osteogenesis: A Case Report
 Case Report Treatment of Condylar Hypoplasia with Distraction Osteogenesis: A Case Report Tülin Arun, DDS, PhD a ; Fulya Kayhan, DDS, PhD b ; Meral Kiziltan, MD, PhD c Abstract: This report describes the
Case Report Treatment of Condylar Hypoplasia with Distraction Osteogenesis: A Case Report Tülin Arun, DDS, PhD a ; Fulya Kayhan, DDS, PhD b ; Meral Kiziltan, MD, PhD c Abstract: This report describes the
Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy
 1 Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy J. Beukes 1,, J. P. Reyneke 1,2,3,4, P. J. Becker 5,6
1 Variations in the anatomical dimensions of the mandibular ramus and the presence of third molars: its effect on the sagittal split ramus osteotomy J. Beukes 1,, J. P. Reyneke 1,2,3,4, P. J. Becker 5,6
Class II. Bilateral Cleft Lip and Palate. Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Cleft Lip and Palate.
 Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
A lingual orthodontic case with 3M Incognito Appliance System combined with orthognathic surgery.
 SM 3M Health Care Academy A lingual orthodontic case with 3M Incognito Appliance System combined with orthognathic surgery. Dr. B. Iglesias-Sánchez Dr. F. Hernandez-Alfaro Dr. J.C. Pérez-Varela DDS, MS.
SM 3M Health Care Academy A lingual orthodontic case with 3M Incognito Appliance System combined with orthognathic surgery. Dr. B. Iglesias-Sánchez Dr. F. Hernandez-Alfaro Dr. J.C. Pérez-Varela DDS, MS.
Unilateral intraoral vertical ramus osteotomy based on preoperative three-dimensional simulation surgery in a patient with facial asymmetry
 CASE REPORT http://dx.doi.org/10.5125/jkaoms.2014.40.1.32 pissn 2234-7550 eissn 2234-5930 Unilateral intraoral vertical ramus osteotomy based on preoperative three-dimensional simulation surgery in a patient
CASE REPORT http://dx.doi.org/10.5125/jkaoms.2014.40.1.32 pissn 2234-7550 eissn 2234-5930 Unilateral intraoral vertical ramus osteotomy based on preoperative three-dimensional simulation surgery in a patient