Rehabilitation of the Paralyzed Face
|
|
|
- Toby Small
- 5 years ago
- Views:
Transcription
1 Rehabilitation of the Paralyzed Face Elizabeth J. Rosen, MD Faculty Advisor: Karen H. Calhoun, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 30, 2002

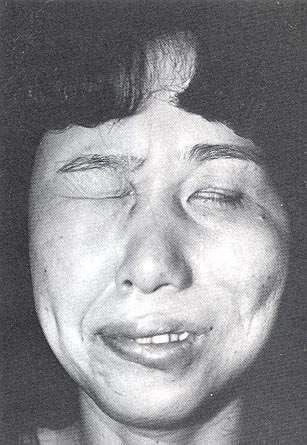
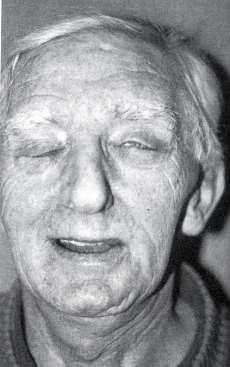
2 Rehabilitation of the Paralyzed Face Personally devastating Cosmetic deformity Psychological distress Functional deficits Lagopthalmos and ectropion Oral incompetence Nasal obstruction Mastication difficulties Articulation difficulties

3 Rehabilitation of the Paralyzed Face Goals Functional EYE PROTECTION Oral competence Cosmetic Symmetry at rest Volitional movement Facial expressions
4 Rehabilitation of the Paralyzed Face Static Slings Gold weight Tarsorrhaphy Lower lid shortening Brow lift Face lift Dynamic Nerve grafting Direct Interposition Crossover Muscle transfer Regional Free flap
5 Rehabilitation of the Facial Nerve Restore neural input Replace nonfunctional facial neuromuscular units Statically resuspend facial tissues Adjunctive procedures to address specific defects
6 Patient Evaluation History Etiology Prognosis Duration Past medical history Neurological disease Physical examination General appearance Complete head and neck exam Donor tissues
7 Rehabilitation of the Facial Nerve Restore neural input Replace nonfunctional facial neuromuscular units Statically resuspend facial tissues Adjunctive procedures to address specific defects
8 Rehabilitation of the Facial Nerve Restore neural input Procedure of Choice Distal facial nerve available Within 3 years of injury Best outcome Options End-to-end anastomosis Interposition graft crossover
9 Rehabilitation of the Facial Nerve Replace nonfunctional facial neuromuscular units 2 nd choice Long standing paralysis Lack of normal neuromuscular units Patient contraindications to nerve crossover Dynamic function Options Regional muscle transfer Free muscle transfer
10 Rehabilitation of the Facial Nerve Statically resuspend facial tissues 3 rd choice Patient factors Temporizing measure Symmetry at rest Options Fascia or synthetic slings
11 Rehabilitation of the Facial Nerve Adjunctive procedures to address specific defects Options Gold weight implants/lid springs Lid shortening procedures Lower lip wedge resection Brow/face lift botox
12 Restoration of Neural Input Primary anastomosis Interposition graft Crossover graft Cross-facial graft


13 Restoration of Neural Input Primary anastomosis Procedure of choice Performed immediately/asap Technique Magnification Epineural/perineural 8-0, 9-0, 10-0 nylon suture Must have no tension Rerouting if necessary


14 Restoration of Neural Input Interposition graft Great auricular nerve Sural nerve


15 Restoration of Neural Input Interposition graft Sural nerve

16 Restoration of Neural Input Interposition graft Sural nerve

17 Restoration of Neural Input Interposition graft Sural nerve
18 Restoration of Neural Input Crossover graft Proximal facial nerve disrupted Donor motor nerve Hypoglossal Accessory Ansa hypoglossus Trigeminal phrenic

19 Restoration of Neural Input Crossover graft - technique

20 Restoration of Neural Input Crossover graft - technique
21 Restoration of Neural Input - Crossover Advantages Reliable Good tone and symmetry Disadvantages Donor site morbidity Synkinesis and hypertonia Unpredictable result for voluntary movements
22 Restoration of Neural Input Crossover graft modifications Splitting hypoglossal nerve Jump interposition graft Branch of accessory to SCM
23 Restoration of Neural Input Crossover graft

24 Restoration of Neural Input Crossover graft

25 Restoration of Neural Input Crossover graft

26 Restoration of Neural Input Cross-facial graft Sural interposition graft From distal branch of normal facial nerve to distal nerve stump Good resting tone and symmetry Theoretically symmetric voluntary movements Disadvantage fewer regenerating axons = weaker muscle contraction
27 Replacement of Nonfunctional Facial Muscles Regional muscle transfer Microneurovascular free muscle transfer Indications Long standing paralysis Abnormal neuromuscular junctions
28 Replacement of Nonfunctional Facial Muscles Regional muscle transfer Temporalis Masseter Preoperative evaluation Lower 1/3 of the face
29 Replacement of Nonfunctional Facial Muscles Temporalis muscle transfer Advantages Technically straightforward Immediate midface symmetry Disadvantages Bulky over zygomatic arch Donor site deformity Chronic TMJ pain
30 Replacement of Nonfunctional Facial Muscles Temporalis muscle transfer

31 Replacement of Nonfunctional Facial Muscles Temporalis muscle transfer

32 Replacement of Nonfunctional Facial Muscles Masseter muscle transfer
33 Replacement of Nonfunctional Facial Muscles Regional muscle transfer

34 Replacement of Nonfunctional Facial Muscles Regional muscle transfer

35 Replacement of Nonfunctional Facial Muscles Regional muscle transfer
36 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer Advantages Native facial nerve anastomosis Cross-facial anastomosis Disadvantages Technically difficult, longer OR time Staged procedure Unpredictable voluntary movements
37 Replacement of Nonfunctional Facial Muscles Donor muscles Vascular pedicle Single Reliable Sufficient length Bulk Excursion Minimal morbidity
38 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer Vessels Nerves Facial (interposition)
39 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer Vessels Nerves Facial (interposition) Crossover (CN XII or XI)
40 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer Vessels Nerves Facial (interposition) Crossover (CN XII or XI) Cross-facial
41 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer Vessels Nerves Facial (interposition) Crossover (CN XII or XI) Cross-facial


42 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer


43 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer


44 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer


45 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer

46 Replacement of Nonfunctional Facial Muscles Microneurovascular free muscle transfer
47 Static Resuspension of Facial Tissue Static elevation of the drooping paralyzed face Cosmetic Functional Indications Patient factors Temporary while awaiting return of nerve function
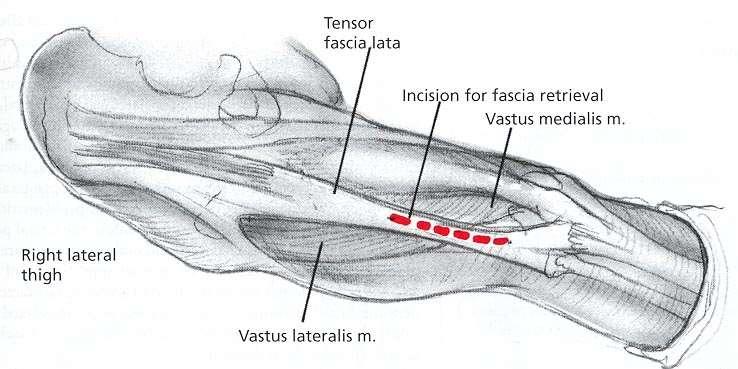
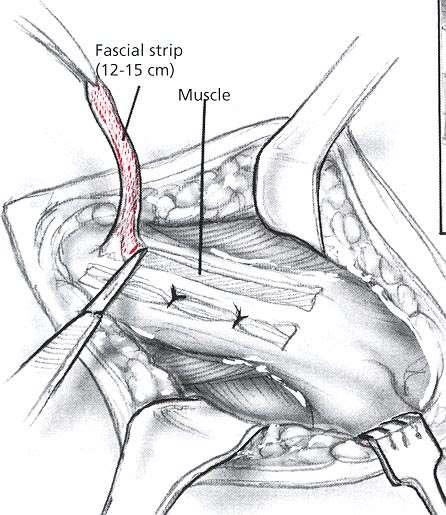
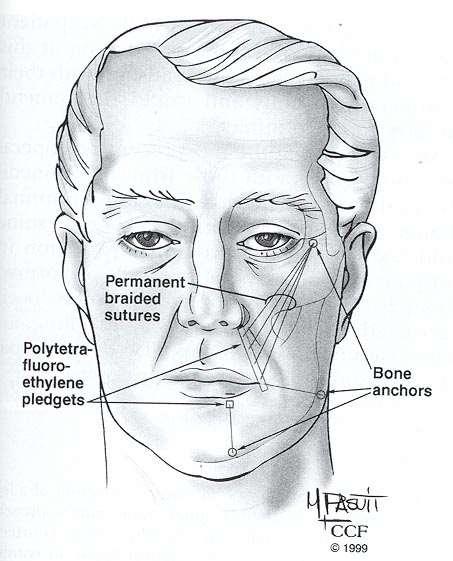
48 Static Resuspension of Facial Tissue Fascia Fascia lata Donor site morbidity Increased OR time Tendency to stretch over time Decreased infection or extrusion Synthetic materials Gore-Tex Alloderm Technically easy No donor site Less stretch over time Increased risk of infection and extrusion
49 Static Resuspension of Facial Tissue

50 Static Resuspension of Facial Tissue
51 Static Resuspension of Facial Tissue

52 Static Resuspension of Facial Tissue
53 Static Resuspension of Facial Tissue

54 Static Resuspension of Facial Tissue
55 Adjunctive Procedures Upper third of the face Gold weight implant Palpebral spring Lower lid shortening Tarsorrhaphy Brow lift Lower third of the face Lower lip wedge resection Rhytidectomy

56 Adjunctive Procedures Gold weight implant Advantages Technically straightforward Consistent Disadvantages Visibility Extrusion
57 Adjunctive Procedures Gold weight implant Advantages Technically straightforward Consistent Disadvantages Visibility Extrusion

58 Adjunctive Procedures Gold weight implant Advantages Technically straightforward Consistent Disadvantages Visibility Extrusion
59 Adjunctive Procedures Palpebral Spring Advantages Less visible Useful in cases with mixed orbicularis and levator dysfunction Disadvantages Technically difficult Higher risk of extrusion
60 Adjunctive Procedures Lower lid shortening Wedge excision with lateral canthopexy
61 Adjunctive Procedures Lower lid shortening Wedge excision with lateral canthopexy Tarsal strip procedure

62 Adjunctive Procedures Tarsorrhaphy Advantages Addresses both upper and lower lid deformity with one procedure Technically easy and effective Disadvantages Visual field defect Lid margin deformity after release

63 Adjunctive Procedures Lower lip wedge resection with transposition of orbicularis oris

64 Adjunctive Procedures Lower lip wedge resection with transposition of orbicularis oris

65 Adjunctive Procedures Lower lip wedge resection with transposition of orbicularis oris
66 Adjunctive Procedures Brow lift Direct Mid-forehead Pretrichial

67 Adjunctive Procedures Endoscopically assisted brow and midface lift


68 Adjunctive Procedures Endoscopically assisted brow and midface lift
69 Adjunctive Procedures Classic rhytidectomy Deep plane rhytidectomy
70 Botulinum Toxin Beneficial for synkinesis and hypertonia Targets specific overactive facial muscles Advantages: easy, temporary, selective Disadvantages: temporary, recurrence of original problem
71 Facial Paralysis < 3 yr >3 yr
72 Healthy pt. Good prognosis Facial Paralysis < 3 yr >3 yr Unhealthy pt. Poor prognosis
73 Healthy pt. Good prognosis Facial Paralysis < 3 yr >3 yr Unhealthy pt. Poor prognosis Facial nerve present and free of disease? Static resuspension
74 Healthy pt. Good prognosis Facial Paralysis < 3 yr >3 yr Unhealthy pt. Poor prognosis Facial nerve present and free of disease? Static resuspension YES NO Regional or free muscle transfer
75 Healthy pt. Good prognosis Facial Paralysis < 3 yr >3 yr Unhealthy pt. Poor prognosis Facial nerve present and free of disease? Static resuspension YES Proximal nerve available? NO Regional or free muscle transfer
76 Healthy pt. Good prognosis Facial Paralysis < 3 yr >3 yr Unhealthy pt. Poor prognosis Facial nerve present and free of disease? Static resuspension YES YES Proximal nerve available? End-to-end anastomosis or interposition graft NO NO Crossover or cross-facial graft Regional or free muscle transfer
77 Healthy pt. Good prognosis Facial nerve present and free of disease? Facial Paralysis < 3 yr >3 yr Unhealthy pt. Poor prognosis Static resuspension Healthy pt. Good prognosis YES YES Proximal nerve available? End-to-end anastomosis or interposition graft NO NO Crossover or cross-facial graft Regional or free muscle transfer


78
Rehabilitation of the Paralyzed Face October 2002
 TITLE: Rehabilitation of the Paralyzed Face SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: October 30, 2002 RESIDENT PHYSICIAN: Elizabeth J. Rosen, MD FACULTY PHYSICIAN: Karen H.
TITLE: Rehabilitation of the Paralyzed Face SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: October 30, 2002 RESIDENT PHYSICIAN: Elizabeth J. Rosen, MD FACULTY PHYSICIAN: Karen H.
REHABILITATION AND REANIMATION. Facial Plastic Surgery. University of Missouri Columbia, Missouri
 FACIAL NERVE PARALYSIS: REHABILITATION AND REANIMATION Matthew A. Kienstra, MD, FACS Facial Plastic Surgery Mercy Health Care Springfield, Missouri University of Missouri Columbia, Missouri Incidence and
FACIAL NERVE PARALYSIS: REHABILITATION AND REANIMATION Matthew A. Kienstra, MD, FACS Facial Plastic Surgery Mercy Health Care Springfield, Missouri University of Missouri Columbia, Missouri Incidence and
The Sublime Beauty of Normal
 Disclosures Basal Cell Carcinoma Surgical Advisory Board, Genentech Corp The Sublime Beauty of Normal P. Daniel Knott, MD FACS Director, Facial Plastic and Reconstructive Surgery UCSF Medical Center The
Disclosures Basal Cell Carcinoma Surgical Advisory Board, Genentech Corp The Sublime Beauty of Normal P. Daniel Knott, MD FACS Director, Facial Plastic and Reconstructive Surgery UCSF Medical Center The
Facial Asymmetry Correction in Facial Palsy Patients with Silhouette Sutures
 International Journal of Clinical Medicine, 2012, 3, 55-59 http://dx.doi.org/10.4236/ijcm.2012.31012 Published Online January 2012 (http://www.scirp.org/journal/ijcm) Facial Asymmetry Correction in Facial
International Journal of Clinical Medicine, 2012, 3, 55-59 http://dx.doi.org/10.4236/ijcm.2012.31012 Published Online January 2012 (http://www.scirp.org/journal/ijcm) Facial Asymmetry Correction in Facial
CHAPTER 11 FACIAL PARALYSIS. Shailesh Agarwal, MD and Arash Momeni, MD
 CHAPTER 11 FACIAL PARALYSIS Shailesh Agarwal, MD and Arash Momeni, MD The facial nerve innervates a total of 23 paired muscles and the orbicularis oris muscle. The majority of muscles innervated by the
CHAPTER 11 FACIAL PARALYSIS Shailesh Agarwal, MD and Arash Momeni, MD The facial nerve innervates a total of 23 paired muscles and the orbicularis oris muscle. The majority of muscles innervated by the
Metadata of the chapter that will be visualized online
 Metadata of the chapter that will be visualized online ChapterTitle Chapter Sub-Title Periorbital Surgical Rehabilitation After Facial Nerve Paralysis Chapter CopyRight - Year Springer Science+Business
Metadata of the chapter that will be visualized online ChapterTitle Chapter Sub-Title Periorbital Surgical Rehabilitation After Facial Nerve Paralysis Chapter CopyRight - Year Springer Science+Business
Static Suspension Technique with Fascia Lata for Facial Reanimation in Facial Palsy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 4 Ver. IV (April. 2017), PP 90-96 www.iosrjournals.org Static Suspension Technique with Fascia
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 4 Ver. IV (April. 2017), PP 90-96 www.iosrjournals.org Static Suspension Technique with Fascia
Face. Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face
 Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Lower Eyelid Malposition
 Oculoplastic Surgeon s DDX for the Red Eye Geeta Belsare Been,MD The Center for Facial Plastic Surgery Barrington, IL Lower Eyelid Malposition Ectropion Involutional Cicatricial Paralytic Entropion Involutional
Oculoplastic Surgeon s DDX for the Red Eye Geeta Belsare Been,MD The Center for Facial Plastic Surgery Barrington, IL Lower Eyelid Malposition Ectropion Involutional Cicatricial Paralytic Entropion Involutional
International Journal of Pharma and Bio Sciences DYNAMIC REANIMATION FOR FACIAL PARALYSIS A REVIEW ABSTRACT
 Review Article Allied Sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 DYNAMIC REANIMATION FOR FACIAL PARALYSIS A REVIEW RATHISHREE 1 AND DR. M.P.SANTHOSH KUMAR *2 1 Intern, saveetha
Review Article Allied Sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 DYNAMIC REANIMATION FOR FACIAL PARALYSIS A REVIEW RATHISHREE 1 AND DR. M.P.SANTHOSH KUMAR *2 1 Intern, saveetha
Facial Paralysis and Contemporary Management
 Facial Paralysis and Contemporary Management Michael Hall, MD Grand Rounds PGY-3 May 13, 2015 Overview Anatomy General Concepts Causes Treatment Options Static Dynamic Management of the Brow Eyelids Mid-Lower
Facial Paralysis and Contemporary Management Michael Hall, MD Grand Rounds PGY-3 May 13, 2015 Overview Anatomy General Concepts Causes Treatment Options Static Dynamic Management of the Brow Eyelids Mid-Lower
VI. Head and Neck and aesthetics.
 UEMS ENT SECTION SUBSPECIALTY LOG BOOK IN HEAD AND NECK SURGERY VI. Head and Neck and aesthetics. A. Diagnostic Procedures and multidisciplinary approach a) CLINICAL EXAMINATION 1 investigation of the
UEMS ENT SECTION SUBSPECIALTY LOG BOOK IN HEAD AND NECK SURGERY VI. Head and Neck and aesthetics. A. Diagnostic Procedures and multidisciplinary approach a) CLINICAL EXAMINATION 1 investigation of the
Grading Facial Nerve Function Following Combined Static and Mimetic Surgical Techniques
 416 Original Article Grading Facial Nerve Function Following Combined Static and Mimetic Surgical Techniques John P. Leonetti 1 Sam J. Marzo 1 Douglas A. Anderson 2 Joshua M. Sappington 1 1 Department
416 Original Article Grading Facial Nerve Function Following Combined Static and Mimetic Surgical Techniques John P. Leonetti 1 Sam J. Marzo 1 Douglas A. Anderson 2 Joshua M. Sappington 1 1 Department
Oral incompetence following composite reconstruction
 IDEAS AND INNOVATIONS Lower Lip Suspension Using Bilateral Temporalis Muscle Flaps and Fascia Lata Grafts Rodney K. Chan, M.D. Branko Bojovic, M.D. Simon G. Talbot, M.D. Denton Weiss, M.D. Julian J. Pribaz,
IDEAS AND INNOVATIONS Lower Lip Suspension Using Bilateral Temporalis Muscle Flaps and Fascia Lata Grafts Rodney K. Chan, M.D. Branko Bojovic, M.D. Simon G. Talbot, M.D. Denton Weiss, M.D. Julian J. Pribaz,
Examination and Diseases of Cranial Nerves
 Cranial nerve evaluation is an important part of a neurologic exam. There are some differences in the assessment of cranial nerves with different species but the general principles are the same. Going
Cranial nerve evaluation is an important part of a neurologic exam. There are some differences in the assessment of cranial nerves with different species but the general principles are the same. Going
jamafacialplasticsurgery.com JAMA Facial Plastic Surgery September/October 2014 Volume 16, Number 5 359
 Research Case Report/Case Series Salvage Procedures fter Failed Facial Reanimation Surgery Using the Masseteric Nerve as the Motor Nerve for Free Functional Gracilis Muscle Transfer Steffen U. Eisenhardt,
Research Case Report/Case Series Salvage Procedures fter Failed Facial Reanimation Surgery Using the Masseteric Nerve as the Motor Nerve for Free Functional Gracilis Muscle Transfer Steffen U. Eisenhardt,
Lower Facial Reanimation Techniques Following Cancer Resection and Free Flap Reconstruction
 The Laryngoscope VC 2016 The American Laryngological, Rhinological and Otological Society, Inc. Lower Facial Reanimation Techniques Following Cancer Resection and Free Flap Reconstruction Alexandra E.
The Laryngoscope VC 2016 The American Laryngological, Rhinological and Otological Society, Inc. Lower Facial Reanimation Techniques Following Cancer Resection and Free Flap Reconstruction Alexandra E.
CHAPTER 17 FACIAL AESTHETIC SURGERY. Christopher C. Surek, DO and Mohammed S. Alghoul, MD. I. BROW LIFT (Figures 1 and 2)
") CHAPTER 17 FACIAL AESTHETIC SURGERY Christopher C. Surek, DO and Mohammed S. Alghoul, MD I. BROW LIFT (Figures 1 and 2) A. Open Coronal Brow Lift Technique 1. Coronal incision is made in the hair-bearing
CHAPTER 17 FACIAL AESTHETIC SURGERY Christopher C. Surek, DO and Mohammed S. Alghoul, MD I. BROW LIFT (Figures 1 and 2) A. Open Coronal Brow Lift Technique 1. Coronal incision is made in the hair-bearing
ASSESSMENT AND TREATMENT OF FACIAL PALSY. Michael J. LaRouere, M.D. Michigan Ear Institute Farmington Hills, Michigan
 ASSESSMENT AND TREATMENT OF FACIAL PALSY Michael J. LaRouere, M.D. Michigan Ear Institute Farmington Hills, Michigan FACIAL PARALYSIS - ETIOLOGY Bells Palsy Ramsay Hunt Syndrome Infection (Acute/Chronic)
ASSESSMENT AND TREATMENT OF FACIAL PALSY Michael J. LaRouere, M.D. Michigan Ear Institute Farmington Hills, Michigan FACIAL PARALYSIS - ETIOLOGY Bells Palsy Ramsay Hunt Syndrome Infection (Acute/Chronic)
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
SOFT TISSUE SUPPORT IS AN
 ORIGINAL ARTICLE Reconstructive Application of the Endotine Suspension Devices James H. Boehmler IV, MD; Benjamin L. Judson, MD; Steven P. Davison, MD, DDS Objective: To illustrate the potential reconstructive
ORIGINAL ARTICLE Reconstructive Application of the Endotine Suspension Devices James H. Boehmler IV, MD; Benjamin L. Judson, MD; Steven P. Davison, MD, DDS Objective: To illustrate the potential reconstructive
Chapter 63: Rehabilitation of Facial Paralysis. Roger L. Crumley, Timothy A. Scott
 Chapter 63: Rehabilitation of Facial Paralysis Roger L. Crumley, Timothy A. Scott Complete unilateral paralysis of the face represents one of the most devastating emotional ordeals an individual can experience.
Chapter 63: Rehabilitation of Facial Paralysis Roger L. Crumley, Timothy A. Scott Complete unilateral paralysis of the face represents one of the most devastating emotional ordeals an individual can experience.
Management of Facial Paralysis
 Section 3: Facial Surgery 6 Management of Facial Paralysis D Bray INTRODUCTION Significant functional, aesthetic and psychosocial sequelae accompany facial paralysis. Dysfunctional lacrimation, palpebral
Section 3: Facial Surgery 6 Management of Facial Paralysis D Bray INTRODUCTION Significant functional, aesthetic and psychosocial sequelae accompany facial paralysis. Dysfunctional lacrimation, palpebral
Head and Face Anatomy
 Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
Excessive skin on the eyelids due to chronic blepharedema, which physically stretches the skin.
 Retired Date: Page 1 of 10 1. POLICY DESCRIPTION: Guideline for Blepharoplasty 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Pharmacy, Claim
Retired Date: Page 1 of 10 1. POLICY DESCRIPTION: Guideline for Blepharoplasty 2. RESPONSIBLE PARTIES: Medical Management Administration, Utilization Management, Integrated Care Management, Pharmacy, Claim
Comparison of one-stage free gracilis muscle flap with two-stage method in chronic facial palsy*
 Original Research Medical Journal of the Islamic Republic of Iran.Vol. 21, No.2, August 2007. pp. 63-70 Comparison of one-stage free gracilis muscle flap with two-stage method in chronic facial palsy*
Original Research Medical Journal of the Islamic Republic of Iran.Vol. 21, No.2, August 2007. pp. 63-70 Comparison of one-stage free gracilis muscle flap with two-stage method in chronic facial palsy*
Blepharoptosis repair is covered as functional/reconstructive surgery to correct: Visual impairment due to droop or displacement of the upper lid.
 Premier Health Insuring Corporation POLICY AND PROCEDURE MANUAL MP.074.PC - Blepharoplasty This policy applies to the following line(s) of business: Premier Health Insuring Corporation MA DSNP Premier
Premier Health Insuring Corporation POLICY AND PROCEDURE MANUAL MP.074.PC - Blepharoplasty This policy applies to the following line(s) of business: Premier Health Insuring Corporation MA DSNP Premier
Facial Nerve Injury: Diagnosis and Repair
 Editor s Note: My thanks to the moderator, Julia K. Terzis, MD, PhD (board-certified plastic surgeon and ASAPS member, Norfolk, VA); and to panelists Ralph Manktelow, MD (board-certified plastic surgeon,
Editor s Note: My thanks to the moderator, Julia K. Terzis, MD, PhD (board-certified plastic surgeon and ASAPS member, Norfolk, VA); and to panelists Ralph Manktelow, MD (board-certified plastic surgeon,
Blepharoplasty. Definitions
 Last Review Date: June 9, 2017 Number: MG.MM.SU.10eC5 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: June 9, 2017 Number: MG.MM.SU.10eC5 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Al Hess MD NERVE REPAIR
 Al Hess MD NERVE REPAIR Historical Aspects 300 BC Hippocrates, description of nervous system 200 AD Galen of Pergamon, nerve injury, questioned possibility of regeneration 600 AD Paul of Arginia, first
Al Hess MD NERVE REPAIR Historical Aspects 300 BC Hippocrates, description of nervous system 200 AD Galen of Pergamon, nerve injury, questioned possibility of regeneration 600 AD Paul of Arginia, first
Kevin T. Kavanagh, MD
 Kevin T. Kavanagh, MD Axial Based upon a named artery. Survival length depends upon the artery not the width of the flap. Random Has random unnamed vessels supplying it. Survival length is directly proportional
Kevin T. Kavanagh, MD Axial Based upon a named artery. Survival length depends upon the artery not the width of the flap. Random Has random unnamed vessels supplying it. Survival length is directly proportional
Endoscopic Approach for Lengthening the Temporalis Muscle
 Ideas and Innovations Endoscopic Approach for Lengthening the Temporalis Muscle Rubén Contreras-García, M.D., Pedro D. Martins, M.D., and Jefferson Braga-Silva, M.D., Ph.D. Porto Alegre, Brazil The temporalis
Ideas and Innovations Endoscopic Approach for Lengthening the Temporalis Muscle Rubén Contreras-García, M.D., Pedro D. Martins, M.D., and Jefferson Braga-Silva, M.D., Ph.D. Porto Alegre, Brazil The temporalis
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
3-Deep fascia: is absent (except over the parotid gland & buccopharngeal fascia covering the buccinator muscle)
") The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
Surgical treatment of bilateral paralytic lagophthalmos using scapha graft in a case of lepromatous leprosy
 Lepr Rev (2009) 80, 448 452 CASE REPORT Surgical treatment of bilateral paralytic lagophthalmos using scapha graft in a case of lepromatous leprosy LAURA LAVILLA, JESÚS CASTILLO, ÁNGEL M. DOMÍNGUEZ, NELSON
Lepr Rev (2009) 80, 448 452 CASE REPORT Surgical treatment of bilateral paralytic lagophthalmos using scapha graft in a case of lepromatous leprosy LAURA LAVILLA, JESÚS CASTILLO, ÁNGEL M. DOMÍNGUEZ, NELSON
be very thin and variable. Facial nerve branches that exit the parotid gland are deep to the SMAS.
 The Superficial musculoaponeurotic system (SMAS) fascia is a fanlike fascia that envelops the face and provides a suspensory sheet which distributes forces of facial expression.. The SMAS is continuous
The Superficial musculoaponeurotic system (SMAS) fascia is a fanlike fascia that envelops the face and provides a suspensory sheet which distributes forces of facial expression.. The SMAS is continuous
The Evaluation and Management of Drooling
 The Evaluation and Management of Drooling Sarah Rodriguez, MD Faculty Advisor: Byron Bailey, MD, FACS The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January
The Evaluation and Management of Drooling Sarah Rodriguez, MD Faculty Advisor: Byron Bailey, MD, FACS The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January
cally, a distinct superior crease of the forehead marks this spot. The hairline and
 4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve
 Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve Muscle weakness or complete paralysis may be secondary to an interruption in the communication between the brain and nerve cells in the
Muscle Weakness Or Paralysis With Compromise Of Peripheral Nerve Muscle weakness or complete paralysis may be secondary to an interruption in the communication between the brain and nerve cells in the
SURGICAL TREATMENT OF SEVENTH NERVE PARALYSIS. By B. GRUNDT, M.D. Oslo, Norway
 SURGICAL TREATMENT OF SEVENTH NERVE PARALYSIS By B. GRUNDT, M.D. Oslo, Norway WE are all familiar with the patient who has paralysis of the facial nerve. The oblique mouth and the corresponding oblique
SURGICAL TREATMENT OF SEVENTH NERVE PARALYSIS By B. GRUNDT, M.D. Oslo, Norway WE are all familiar with the patient who has paralysis of the facial nerve. The oblique mouth and the corresponding oblique
READYTALK. Moderator: Melissa Baumbick June 6, :00 p.m. ET
 Page!1 READYTALK June 6, 2016 2:00 p.m. ET Operator: This is Conference # 39166216. Melissa Baumbick: Welcome to the first Webinar in ANA's 2016 Summer Series. We are honored to welcome Dr. Babak Azizzadeh
Page!1 READYTALK June 6, 2016 2:00 p.m. ET Operator: This is Conference # 39166216. Melissa Baumbick: Welcome to the first Webinar in ANA's 2016 Summer Series. We are honored to welcome Dr. Babak Azizzadeh
INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES
 INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES CRANIAL NERVE I - OLFACTORY I - OLFACTORY NERVE - SMELL TEST: SMELL ODORS (note: not ammonia; pain in nasal cavity CN5 DAMAGE: LOSS OF
INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES CRANIAL NERVE I - OLFACTORY I - OLFACTORY NERVE - SMELL TEST: SMELL ODORS (note: not ammonia; pain in nasal cavity CN5 DAMAGE: LOSS OF
Smile Restoration for Permanent Facial Paralysis
 Continuing Medical Education Smile Restoration for Permanent Facial Paralysis Jonathan Leckenby, Adriaan Grobbelaar Department of Plastic Surgery, The Royal Free Hospital, University of London, London,
Continuing Medical Education Smile Restoration for Permanent Facial Paralysis Jonathan Leckenby, Adriaan Grobbelaar Department of Plastic Surgery, The Royal Free Hospital, University of London, London,
In situations where Reliable Visual Field testing is not possible, see section below, When the Member is Not
 UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (EPO/POS) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas, Inc.
UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (EPO/POS) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas, Inc.
Facial Paralysis Facial Nerve Subcommittee of the American Academy of Otolaryngology-Head & Neck Surgery
 Facial Paralysis Facial Nerve Subcommittee of the American Academy of Otolaryngology-Head & Neck Surgery Editor: Peter S Roland MD Contributors: Peter S Roland MD, Larry Lundy MD, Jacques Herzog MD, Fred
Facial Paralysis Facial Nerve Subcommittee of the American Academy of Otolaryngology-Head & Neck Surgery Editor: Peter S Roland MD Contributors: Peter S Roland MD, Larry Lundy MD, Jacques Herzog MD, Fred
Botulinum Toxin Application
 Botulinum Toxin Application Clostridium botulinum: rod-shaped bacterium producing the neurotoxin botulin Gram-positive anaerobic bacterium Seven serotypes - A, B, C, D, E, F, G http://standeyo.com/news/08_health/081202.biological.weapons.html
Botulinum Toxin Application Clostridium botulinum: rod-shaped bacterium producing the neurotoxin botulin Gram-positive anaerobic bacterium Seven serotypes - A, B, C, D, E, F, G http://standeyo.com/news/08_health/081202.biological.weapons.html
Embouchure Assistive Device
 Embouchure Assistive Device Advisor: John Webster Client: Elon Roti Roti Team Members: Vivian Chen Megan Jones Patrick Cassidy Outline Background Bell s palsy Synkinesis Clarinet embouchure Motivation
Embouchure Assistive Device Advisor: John Webster Client: Elon Roti Roti Team Members: Vivian Chen Megan Jones Patrick Cassidy Outline Background Bell s palsy Synkinesis Clarinet embouchure Motivation
Our Experience with Endoscopic Brow Lifts
 Aesth. Plast. Surg. 24:90 96, 2000 DOI: 10.1007/s002660010017 2000 Springer-Verlag New York Inc. Our Experience with Endoscopic Brow Lifts Ozan Sozer, M.D., and Thomas M. Biggs, M.D. İstanbul, Turkey and
Aesth. Plast. Surg. 24:90 96, 2000 DOI: 10.1007/s002660010017 2000 Springer-Verlag New York Inc. Our Experience with Endoscopic Brow Lifts Ozan Sozer, M.D., and Thomas M. Biggs, M.D. İstanbul, Turkey and
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY NASOLABIAL FLAP FOR ORAL CAVITY RECONSTRUCTION Harry Wright, Scott Stephan, James Netterville Designed as a true myocutaneous flap pedicled
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY NASOLABIAL FLAP FOR ORAL CAVITY RECONSTRUCTION Harry Wright, Scott Stephan, James Netterville Designed as a true myocutaneous flap pedicled
with laser resurfacing, 36, 37 Cryotherapy, lower eyelid cicatricial ectropion after, 151 Cutler-Beard flap. See Fullthickness
 INDEX A Abrasion, from silicone tubing, 230 Acquired immunodeficiency syndrome, eyelid tumor with, 193 AIDS. See Acquired immunodeficiency syndrome Anatomy, eyelid, 155 156 Aneurysm, cerebral, Muller s
INDEX A Abrasion, from silicone tubing, 230 Acquired immunodeficiency syndrome, eyelid tumor with, 193 AIDS. See Acquired immunodeficiency syndrome Anatomy, eyelid, 155 156 Aneurysm, cerebral, Muller s
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: surgical_deactivation_of_migraine_headache_trigger_sites 10/2012 5/2017 5/2018 5/2017 Description of Procedure
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: surgical_deactivation_of_migraine_headache_trigger_sites 10/2012 5/2017 5/2018 5/2017 Description of Procedure
THE pedicled flap, commonly used by the plastic surgeon in the reconstruction
 THE PEDICLE!) SKIN FLAP ROBIN ANDERSON, M.D. Department of Plastic Surgery THE pedicled flap, commonly used by the plastic surgeon in the reconstruction of skin and soft tissue defects, differs from the
THE PEDICLE!) SKIN FLAP ROBIN ANDERSON, M.D. Department of Plastic Surgery THE pedicled flap, commonly used by the plastic surgeon in the reconstruction of skin and soft tissue defects, differs from the
Clinical Policy Bulletin: Bell's Palsy
 Go Clinical Policy Bulletin: Bell's Palsy Number: 0745 Policy *Pleasesee amendment forpennsylvaniamedicaidattheendofthiscpb. I. Aetna considers blink reflex testing medically necessary for the diagnosis
Go Clinical Policy Bulletin: Bell's Palsy Number: 0745 Policy *Pleasesee amendment forpennsylvaniamedicaidattheendofthiscpb. I. Aetna considers blink reflex testing medically necessary for the diagnosis
Sierra Smith Bio 205 Extra Credit Essay. My Face. Growing up I was always told that it takes 43 muscles to frown but only 17
 Sierra Smith Bio 205 Extra Credit Essay My Face Growing up I was always told that it takes 43 muscles to frown but only 17 muscles to smile and I should just smile because it's easier. It wasn't until
Sierra Smith Bio 205 Extra Credit Essay My Face Growing up I was always told that it takes 43 muscles to frown but only 17 muscles to smile and I should just smile because it's easier. It wasn't until
HAND & MICROSURGERY PROCEDURE A ( RM RM 4800 ) PROCEDURE B ( RM RM 4400 ) PROCEDURE C ( RM RM 3600 )
 PROCEDURE B ( RM RM 4400 ) PROCEDURE C ( RM RM 3600 )") HAND & MICROSURGERY PROCEDURE A ( RM 4401 - RM 4800 ) 1 Brachial plexus Exploration with nerve graft 2 Brachial plexus Exploration with neurotisation 3 Brachial plexus Free functioning muscle transfer
HAND & MICROSURGERY PROCEDURE A ( RM 4401 - RM 4800 ) 1 Brachial plexus Exploration with nerve graft 2 Brachial plexus Exploration with neurotisation 3 Brachial plexus Free functioning muscle transfer
SELECTIVE NEURECTOMIES TO ACHIEVE SYMMETRY IN PARTIAL AND COMPLETE FACIAL PARALYSIS
 British Journal of Plastic Surgery (I976), 29, 43-52 SELECTIVE NEURECTOMIES TO ACHIEVE SYMMETRY IN PARTIAL AND COMPLETE FACIAL PARALYSIS By L. CLODIVS, M.D. Plastic Surgery Section, Second Surgical Department,
British Journal of Plastic Surgery (I976), 29, 43-52 SELECTIVE NEURECTOMIES TO ACHIEVE SYMMETRY IN PARTIAL AND COMPLETE FACIAL PARALYSIS By L. CLODIVS, M.D. Plastic Surgery Section, Second Surgical Department,
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Facial palsy is a well-known pathological condition. Masseteric facial nerve neurorrhaphy: results of a case series
 clinical article J Neurosurg 126:312 318, 2017 Masseteric facial nerve neurorrhaphy: results of a case series Federico Biglioli, MD, 1 Valeria Colombo, MD, 1 Dimitri Rabbiosi, MD, 1 Filippo Tarabbia, MD,
clinical article J Neurosurg 126:312 318, 2017 Masseteric facial nerve neurorrhaphy: results of a case series Federico Biglioli, MD, 1 Valeria Colombo, MD, 1 Dimitri Rabbiosi, MD, 1 Filippo Tarabbia, MD,
Regional nerve block of the upper eyelid in oculoplastic surg e r y
 E u ropean Journal of Ophthalmology / Vol. 16 no. 4, 2006 / pp. 5 0 9-5 1 3 Regional nerve block of the upper eyelid in oculoplastic surg e r y A.R. ISMAIL, T. ANTHONY, D.J. MORDANT, H. MacLEAN Portsmouth
E u ropean Journal of Ophthalmology / Vol. 16 no. 4, 2006 / pp. 5 0 9-5 1 3 Regional nerve block of the upper eyelid in oculoplastic surg e r y A.R. ISMAIL, T. ANTHONY, D.J. MORDANT, H. MacLEAN Portsmouth
The Scalp and Face Protocol. Julie Goodwin, BA, LMT
 The Scalp and Face Protocol Julie Goodwin, BA, LMT The Scalp and Face Protocol Julie Goodwin, BA, LMT Julie Goodwin 2014 2 Agenda Pertinent Anatomy and Physiology Treatment Planning Strokes, Techniques
The Scalp and Face Protocol Julie Goodwin, BA, LMT The Scalp and Face Protocol Julie Goodwin, BA, LMT Julie Goodwin 2014 2 Agenda Pertinent Anatomy and Physiology Treatment Planning Strokes, Techniques
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC
 Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
TOTAL Head and Neck Congenital Defects 50
 Operative Minimums Effective July 1, 2014 Review Committee for Plastic Surgery NOTE: The index procedure number for Laser is tracked by Total Laser and not by the subcategories of Aesthetic Laser and Reconstructive
Operative Minimums Effective July 1, 2014 Review Committee for Plastic Surgery NOTE: The index procedure number for Laser is tracked by Total Laser and not by the subcategories of Aesthetic Laser and Reconstructive
Learn Connect Succeed. JCAHPO Regional Meetings 2017
 Learn Connect Succeed JCAHPO Regional Meetings 2017 Aesthetics & The Ophthalmic Patient David A. Kostick, M.D., F.A.C.S. jaxoculoplastics@yahoo.com www.floridaeyespecialists.com Outline Skin Types Skin
Learn Connect Succeed JCAHPO Regional Meetings 2017 Aesthetics & The Ophthalmic Patient David A. Kostick, M.D., F.A.C.S. jaxoculoplastics@yahoo.com www.floridaeyespecialists.com Outline Skin Types Skin
Anatomy and Physiology II. Review Spine and Neck
 Anatomy and Physiology II Review Spine and Neck Spine regions How many cervical vertibrae are there? 7 The curvature is the cervical region posterior? Concave posterior How many thoracic? And curvature?
Anatomy and Physiology II Review Spine and Neck Spine regions How many cervical vertibrae are there? 7 The curvature is the cervical region posterior? Concave posterior How many thoracic? And curvature?
RECONSTRUCTION OF SUBTOTAL DEFECTS OF THE NOSE BY ABDOMINAL TUBE FLAP. By MICHAL KRAUSS. Plastic Surgery Hospital, Polanica-Zdroj, Poland
 RECONSTRUCTION OF SUBTOTAL DEFECTS OF THE NOSE BY ABDOMINAL TUBE FLAP By MICHAL KRAUSS Plastic Surgery Hospital, Polanica-Zdroj, Poland RECONSTRUCTION of the nose is one of the composite procedures in
RECONSTRUCTION OF SUBTOTAL DEFECTS OF THE NOSE BY ABDOMINAL TUBE FLAP By MICHAL KRAUSS Plastic Surgery Hospital, Polanica-Zdroj, Poland RECONSTRUCTION of the nose is one of the composite procedures in
SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY
 MEDICAL UNIVERSITY OF VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AND SID SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY (State examination) ACADEMIC YEAR 2015 2016 1. Asepsis
MEDICAL UNIVERSITY OF VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AND SID SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY (State examination) ACADEMIC YEAR 2015 2016 1. Asepsis
Entropion. Geoffrey J. Gladstone. Examination. Congenital Entropion-Epiblepharon. Etiology
 Entropion 2 Geoffrey J. Gladstone Entropion, or inward rotation of the eyelid margin, is an eyelid malposition commonly seen by general ophthalmologists and oculoplastic surgeons. The severe corneal irritation
Entropion 2 Geoffrey J. Gladstone Entropion, or inward rotation of the eyelid margin, is an eyelid malposition commonly seen by general ophthalmologists and oculoplastic surgeons. The severe corneal irritation
Parotid Gland, Temporomandibular Joint and Infratemporal Fossa
 M1 - Anatomy Parotid Gland, Temporomandibular Joint and Infratemporal Fossa Jeff Dupree Sanger 9-057 jldupree@vcu.edu Parotid gland: wraps around the mandible positioned between the mandible and the sphenoid
M1 - Anatomy Parotid Gland, Temporomandibular Joint and Infratemporal Fossa Jeff Dupree Sanger 9-057 jldupree@vcu.edu Parotid gland: wraps around the mandible positioned between the mandible and the sphenoid
Muscles of the Face, Head, and Neck
 Muscles of the Face, Head, and Neck 1 How Muscles Are Named Many muscles named using such features as Location Function Shape Direction of fibers Number of heads or divisions Points of attachment Size
Muscles of the Face, Head, and Neck 1 How Muscles Are Named Many muscles named using such features as Location Function Shape Direction of fibers Number of heads or divisions Points of attachment Size
ALTERNATIVE TREATMENTS
 Botox Consent INSTRUCTIONS This is an informed- consent document which has been prepared to help your plastic surgeon inform you concerning BOTOX (Botulina Toxin Type A, Allergan) injection, its risks,
Botox Consent INSTRUCTIONS This is an informed- consent document which has been prepared to help your plastic surgeon inform you concerning BOTOX (Botulina Toxin Type A, Allergan) injection, its risks,
Lateral Orbitotomy in the Management of Challenging Exotropia
 Lateral Orbitotomy in the Management of Challenging Exotropia Yahalom C (1, 2), Mc Nab A (3), Ben Simon G (3), Kowal L (1). 1- Centre for Eye Research Australia and Ocular Motility Clinic, Royal Victorian
Lateral Orbitotomy in the Management of Challenging Exotropia Yahalom C (1, 2), Mc Nab A (3), Ben Simon G (3), Kowal L (1). 1- Centre for Eye Research Australia and Ocular Motility Clinic, Royal Victorian
Case Studies in Asian Blepharoplasty
 Aesthetic Surgery Journal XX(X) Takayanagi INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Review Article Case Studies in Asian Blepharoplasty Aesthetic Surgery Journal 31(2) 171 179 2011 The American
Aesthetic Surgery Journal XX(X) Takayanagi INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Review Article Case Studies in Asian Blepharoplasty Aesthetic Surgery Journal 31(2) 171 179 2011 The American
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery FACIAL FRACTURES
 Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
THE MANAGEMENT OF INVOLUTIONAL LOWER LID ECTROPION
 THE MANAGEMENT OF INVOLUTIONAL LOWER LID ECTROPION BYRON C. SMITH, M.D., STEPHEN L. BOSNIAK, M.D., MICHAEL E. SACHS, M.D. New York Eye & Ear Infirmary, Manhattan Eye, Ear & Throat Hospital, New York ABSTRACT
THE MANAGEMENT OF INVOLUTIONAL LOWER LID ECTROPION BYRON C. SMITH, M.D., STEPHEN L. BOSNIAK, M.D., MICHAEL E. SACHS, M.D. New York Eye & Ear Infirmary, Manhattan Eye, Ear & Throat Hospital, New York ABSTRACT
Tarsal fixation of Fascia lata in Frontalis Sling Ptosis Surgery
 Original Article Tarsal fixation of Fascia lata in Frontalis Sling Ptosis Surgery Muhammad Moin Pak J Ophthalmol 2006, Vol. 22 No. 3.......................................................................................
Original Article Tarsal fixation of Fascia lata in Frontalis Sling Ptosis Surgery Muhammad Moin Pak J Ophthalmol 2006, Vol. 22 No. 3.......................................................................................
Clare Gaduzo BSc RMN Registered Aesthetics Practitioner (qualified with Medics Direct)
") Clare Gaduzo BSc RMN Registered Aesthetics Practitioner (qualified with Medics Direct) 07935567067 cjg.aesthetics@yahoo.co.uk www.cjgaesthetics.co.uk http://www.facebook.com/cjgaesthetics @CJGAesthetics
Clare Gaduzo BSc RMN Registered Aesthetics Practitioner (qualified with Medics Direct) 07935567067 cjg.aesthetics@yahoo.co.uk www.cjgaesthetics.co.uk http://www.facebook.com/cjgaesthetics @CJGAesthetics
Facial Paralysis. A Comprehensive Rehabilitative Approach. Mark K. Wax, MD
 Facial Paralysis A Comprehensive Rehabilitative Approach Mark K. Wax, MD Contents Introduction Acknowledgments Contributors vii viii ix 1 Facial Nerve Anatomy and Mastoid Surgery in the Management 1 of
Facial Paralysis A Comprehensive Rehabilitative Approach Mark K. Wax, MD Contents Introduction Acknowledgments Contributors vii viii ix 1 Facial Nerve Anatomy and Mastoid Surgery in the Management 1 of
The SCALP. Prof. Dr. Muhammad Imran Qureshi
 The SCALP By Prof. Dr. Muhammad Imran Qureshi The SCALP includes FIVE layers external to the Calvaria. These are: S: Skin & Superficial Fascia C: Connective Tissue A: Aponeurosis (Epicranial) L: Loose
The SCALP By Prof. Dr. Muhammad Imran Qureshi The SCALP includes FIVE layers external to the Calvaria. These are: S: Skin & Superficial Fascia C: Connective Tissue A: Aponeurosis (Epicranial) L: Loose
Chapter(2):the lid page (1) THE LID
:the lid page (1) THE LID") Chapter(2):the lid page (1) THE LID Anatomy of the lid: * Check movie anatomy of the lid model The eyelids are two movable muco-cutaneous folds which protect the eye on closure. The are joined temporary
Chapter(2):the lid page (1) THE LID Anatomy of the lid: * Check movie anatomy of the lid model The eyelids are two movable muco-cutaneous folds which protect the eye on closure. The are joined temporary
THIEME. Scalp and Superficial Temporal Region
 CHAPTER 2 Scalp and Superficial Temporal Region Scalp Learning Objectives At the end of the dissection of the scalp, you should be able to identify, understand and correlate the clinical aspects: Layers
CHAPTER 2 Scalp and Superficial Temporal Region Scalp Learning Objectives At the end of the dissection of the scalp, you should be able to identify, understand and correlate the clinical aspects: Layers
University of Groningen
 University of Groningen Paralytic ectropion treatment with lateral periosteal flap canthoplasty and introduction of the ectropion severity score Korteweg, Steven F S; Stenekes, Martin W; van Zyl, Fiona
University of Groningen Paralytic ectropion treatment with lateral periosteal flap canthoplasty and introduction of the ectropion severity score Korteweg, Steven F S; Stenekes, Martin W; van Zyl, Fiona
Anatomical Context of Facial Aesthetics Online CME Post-Test
 progressive aesthetic learning essential to technical expertise Anatomical Context of Facial Aesthetics Online CME Post-Test Full Name: Degree: e-mail: May we contact you in approximately three months
progressive aesthetic learning essential to technical expertise Anatomical Context of Facial Aesthetics Online CME Post-Test Full Name: Degree: e-mail: May we contact you in approximately three months
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
BLEPHAROPLASTY, BLEPHAROPTOSIS AND BROW PTOSIS REPAIR
 BLEPHAROPLASTY, BLEPHAROPTOSIS AND BROW PTOSIS REPAIR UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 018.25 T2 Effective Date: June 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE...
BLEPHAROPLASTY, BLEPHAROPTOSIS AND BROW PTOSIS REPAIR UnitedHealthcare Oxford Clinical Policy Policy Number: SURGERY 018.25 T2 Effective Date: June 1, 2017 Table of Contents Page INSTRUCTIONS FOR USE...
Surgical Correction of Crow s Feet Deformity With Radiofrequency Current
 INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Surgical Correction of Crow s Feet Deformity With Radiofrequency Current Min-Hee Ryu, MD; David Kahng, MD; and Yongho Shin, MD, PhD Aesthetic Surgery Journal
INTERNATIONAL CONTRIBUTION Oculoplastic Surgery Surgical Correction of Crow s Feet Deformity With Radiofrequency Current Min-Hee Ryu, MD; David Kahng, MD; and Yongho Shin, MD, PhD Aesthetic Surgery Journal
The Deconstructed Neurological Examination
 The Deconstructed Neurological Examination Marguerite Knipe, DVM, Diplomate ACVIM (Neurology) I. MENTATION: Normal, Quiet, Obtunded (mild, moderate, severe), Stuporous, Comatose Define stuporous and comatose.
The Deconstructed Neurological Examination Marguerite Knipe, DVM, Diplomate ACVIM (Neurology) I. MENTATION: Normal, Quiet, Obtunded (mild, moderate, severe), Stuporous, Comatose Define stuporous and comatose.
Corporate Medical Policy
 Corporate Medical Policy Reconstructive Eyelid Surgery and Brow Lift File Name: Origination: Last CAP Review: Next CAP Review: Last Review: reconstructive_eyelid_surgery_and_brow_lift 1/2000 8/2017 8/2018
Corporate Medical Policy Reconstructive Eyelid Surgery and Brow Lift File Name: Origination: Last CAP Review: Next CAP Review: Last Review: reconstructive_eyelid_surgery_and_brow_lift 1/2000 8/2017 8/2018
Nerve Autografts, Allografts, Conduits, Wraps, and Glue. What Should I Do?
 Nerve Autografts, Allografts, Conduits, Wraps, and Glue. What Should I Do? David Kahan, MD Fellow, Hand & Upper Extremity Surgery Rothman Institute at Thomas Jefferson University Outline Wallerian Degeneration
Nerve Autografts, Allografts, Conduits, Wraps, and Glue. What Should I Do? David Kahan, MD Fellow, Hand & Upper Extremity Surgery Rothman Institute at Thomas Jefferson University Outline Wallerian Degeneration
Surgical correction of unilateral and bilateral facial palsy
 562 REVIEW Surgical correction of unilateral and bilateral facial palsy D H Harrison... Unilateral and bilateral facial palsies are debilitating and depressing conditions for the patient. For the past
562 REVIEW Surgical correction of unilateral and bilateral facial palsy D H Harrison... Unilateral and bilateral facial palsies are debilitating and depressing conditions for the patient. For the past
Facial Palsy Management by the Multidisciplinary Team
 Facial Palsy Management by the Multidisciplinary Team Catriona Neville and Vanessa Venables Extended Scope Practitioner Therapists in Facial Palsy Queen Victoria Hospital East Grinstead 2013 MDT members
Facial Palsy Management by the Multidisciplinary Team Catriona Neville and Vanessa Venables Extended Scope Practitioner Therapists in Facial Palsy Queen Victoria Hospital East Grinstead 2013 MDT members
Eyelid Reconstruction An Oculoplastic Surgical Coding Minicourse. Riva Lee Asbell Philadelphia, PA. Part II
 INTRODUCTION Eyelid Reconstruction An Oculoplastic Surgical Coding Minicourse Riva Lee Asbell Philadelphia, PA Part II In this second part of the Minicourse on Surgical Coding for Eyelid Reconstruction
INTRODUCTION Eyelid Reconstruction An Oculoplastic Surgical Coding Minicourse Riva Lee Asbell Philadelphia, PA Part II In this second part of the Minicourse on Surgical Coding for Eyelid Reconstruction
To successfully perform any facial injection,
 INJECTABLES Newer Understanding of Specific Anatomic Targets in the Aging Face as Applied to Injectables: Facial Muscles Identifying Optimal Targets for Neuromodulators Jonathan M. Sykes, MD Patrick Trevidic,
INJECTABLES Newer Understanding of Specific Anatomic Targets in the Aging Face as Applied to Injectables: Facial Muscles Identifying Optimal Targets for Neuromodulators Jonathan M. Sykes, MD Patrick Trevidic,
INSTRUCTIONS INTRODUCTION RISKS OF BOTULINUM TOXIN / DERMAL FILLER INJECTIONS
 INSTRUCTIONS This is an informed consent document that has been prepared to help inform you concerning botulinum toxin / dermal filler injections and the risks involved. It is important that you read this
INSTRUCTIONS This is an informed consent document that has been prepared to help inform you concerning botulinum toxin / dermal filler injections and the risks involved. It is important that you read this
Clinical Study The Long-Term Results of Frontalis Suspension Using Autogenous Fascia Lata in Children with Congenital Ptosis under 3 Years Old
 Plastic Surgery International Volume 2010, Article ID 609462, 5 pages doi:10.1155/2010/609462 Clinical Study The Long-Term Results of Frontalis Suspension Using Autogenous Fascia Lata in Children with
Plastic Surgery International Volume 2010, Article ID 609462, 5 pages doi:10.1155/2010/609462 Clinical Study The Long-Term Results of Frontalis Suspension Using Autogenous Fascia Lata in Children with
Bone Practical. Labs Muscle Labs. Final Practical. Divisions of the Muscular System. Quiz format
 Bone Practical Labs 17 + 18 Muscles Wed 7/11 @ 8am 40 50 stations About half axial, half appendicular bones Disarticulated bones: Skulls, partial skulls, vertebrae, ribs, skeletons, arm bones, leg bones,
Bone Practical Labs 17 + 18 Muscles Wed 7/11 @ 8am 40 50 stations About half axial, half appendicular bones Disarticulated bones: Skulls, partial skulls, vertebrae, ribs, skeletons, arm bones, leg bones,
Synapse Homework. Back page last question not counted. 4 pts total, each question worth 0.18pts. 26/34 students answered correctly!
 Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Reconstructive and Cosmetic Services
 Reconstructive and Cosmetic Services Policy Number: 10.01.09 Last Review: 4/2018 Origination: 2/2006 Next Review: 4/2019 Policy Determination of whether a proposed therapy would be considered reconstructive
Reconstructive and Cosmetic Services Policy Number: 10.01.09 Last Review: 4/2018 Origination: 2/2006 Next Review: 4/2019 Policy Determination of whether a proposed therapy would be considered reconstructive