Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
|
|
|
- Britton O’Neal’
- 5 years ago
- Views:
Transcription

1
2 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer diptendrasarkar@yahoo.co.in

3 HNC : common inclusives

4 Challenges Anatomical preservation R0 Surgical ablation Functional preservation
5

6 Oral cancer: Lips Wide local excision Cosmesis Function :Good compensation except the angle and commissure Reconstruction with local flap Pedicled flaps in large defects

7 Surgery in the lip
8 Floor of the mouth Approaches : Intraoral Combined Transoral-cervical Mandibular swing Surgery : wide local excision. Mandibular resection if necessary Reconstruction : Small mucosal lesions are managed by local mobilization flaps or skin grafting

9 Floor of the mouth Anterior angle to angle mandibulectomy leads to Andy Gump deformity. Ineffective swallowing/drooling /aspiration Platform of the floor : pectoralis major myocutaneous flap
10 Tongue Approach: Intraoral mandibular swing Principle : wide excision with 1-2 cm margin three dimensionally Types Wedge resection Lateral glossectomy Hemiglossectomy Well tolerated and compensated Anterior glossectomy Total glossectomy Poorly tolerated
11 Challenges in fuctional rahabilitation Mobility of tongue Speech Drooling Aspiration Taste

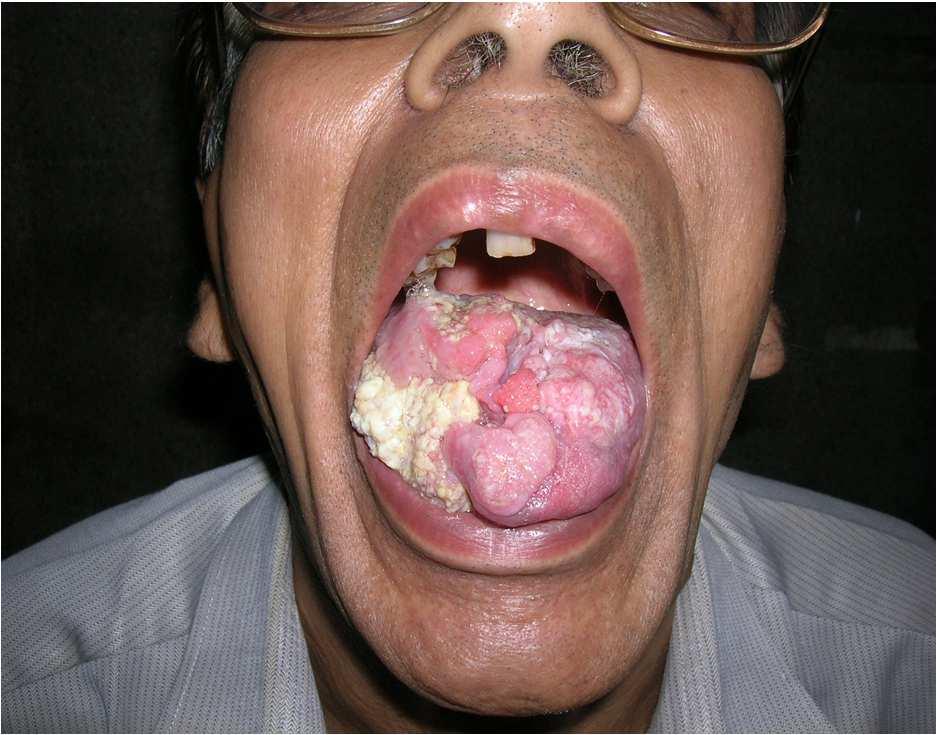
12 Surgery in oral tongue Hemiglossectomy Anterior Glossectomy
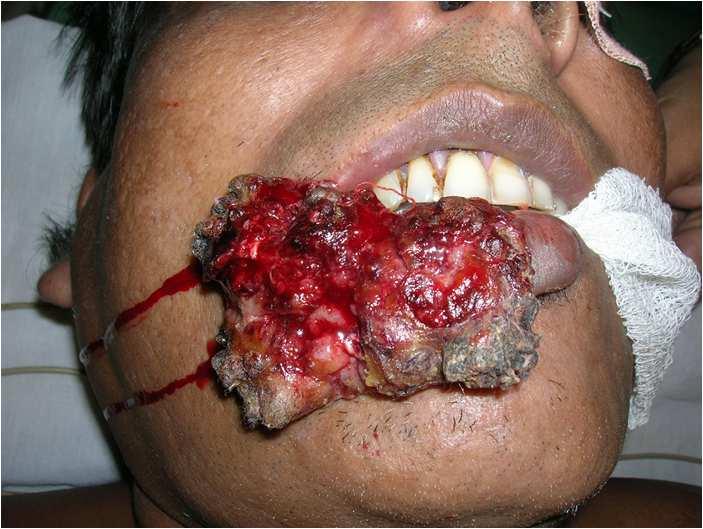
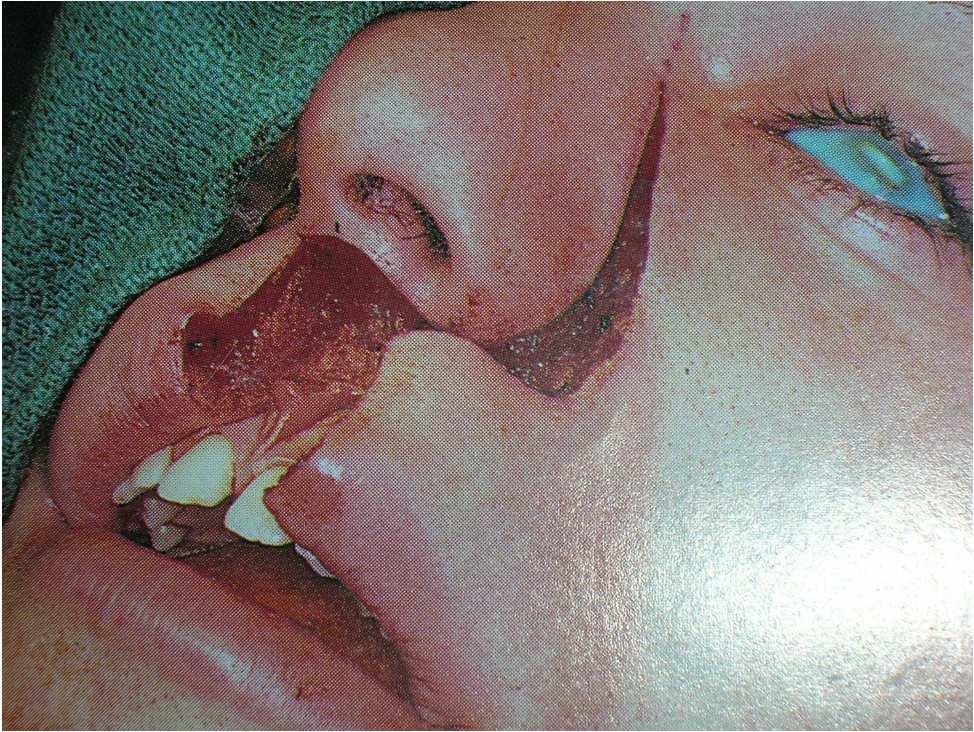
13 Buccal mucosa Mucosal involvement : Peroral excision Mucosa & Muscle : Excision after raising cheek flap Full thickness mucosa to skin involvement : Full thickness excision and reconstruction
14 Challenges in buccal mucosal surgery: Attain R0 resection Contracture avoidance Free flap complex Pedicled flap Skin grafting Better mouth opening and less contracture

15 Buccal mucosa cancer

16 Wide local excision


17 Skin graft


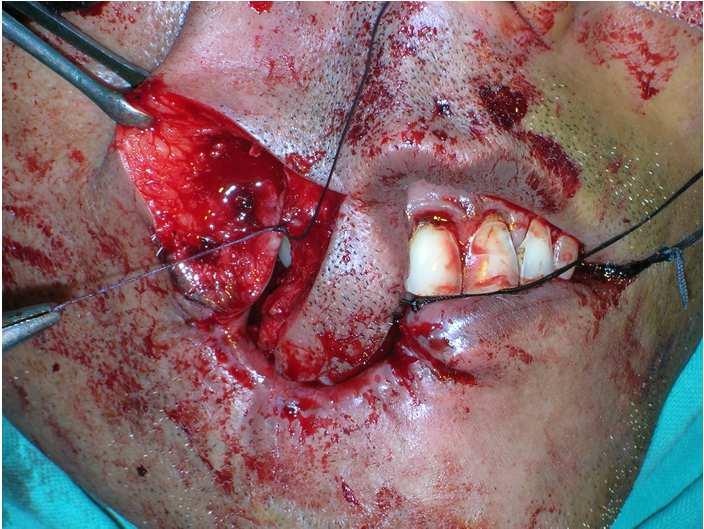
18 Buccal mucosa with overlying skin involvement


19 Wide local excision


20 Forehead flap Superficial temporal vessel base



21


22 Common flaps in head and neck Deltopectoral flap 2 nd /3 rd /4 th perforator of Internal mammary vessels Pectoralis major myocutaneous Flap Acromiothoracic vessel
23 Key words in oral SCC In early oral cancer surgery and radiotherapy gives equal results. Surgery is preferred as RT is associated with xerostomia and dysphagia. Return to normal functioning mucosa is achieved earlier after surgery
24 Algorithm SURGERY Ablative Reconstructive Primary per oral mandubolotomy Lingual release Mandible partial Neck segmental Selective MRND Radical Soft tissue Secondary intention Skin graft Local flap Bone Free flap No reconstruction Soft tissue + Plate Fibular free graft

25 Hard palate :Maxillectomy

26 Oral cancer survivors
27
28 Oropharynx: Tonsil Tonsil: Cryptic location hence diagnosis is delayed Early lesions are managed by radiotherapy Locally advanved but localized : radiotherapy with or without surgical salvage Locally advanced with spread to other subsites : Surgery followed by RT 5yr survival T1:75-85% (S or RT) / T2 :55-80% (S or RT)
29 Oropharynx :Soft palate Surgery is associated with immense functional dysability. Reconstruction does not match the functional results of RT Early cases : RT is the treatment of choice Locally advanced lesions : surgery complex reconstruction followed by RT 5yr survival :T % (S or RT)/ T % (S or RT)
30 Oropharynx :Tongue base Surgery or RT has same local control rates (T1 and T2 cancers 75% to 100%) Early lesions are better managed with RT as functional outcome is better as regards aspiration and speech Locally advanced lesions : Surgery vs RT vs Surgery-RT. Most evidences are in favour of Surgery-RT
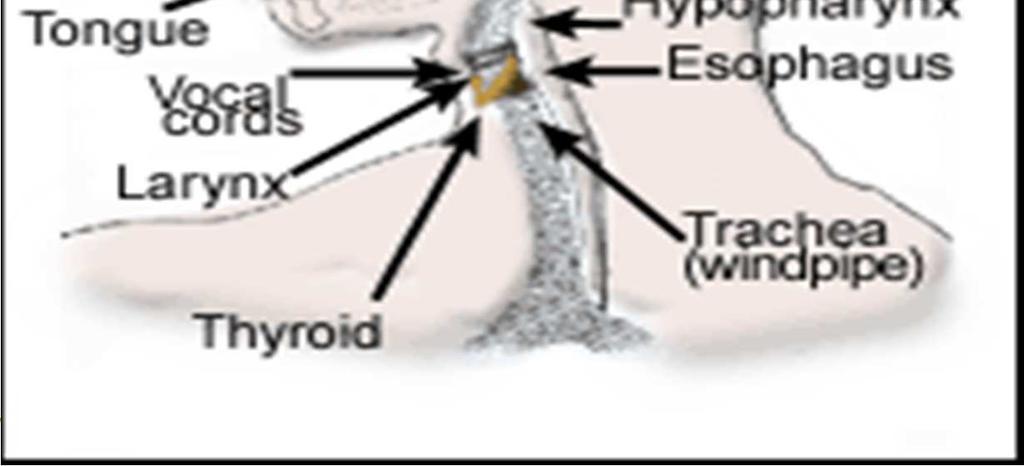
31 Hypopharynx: hyoid to inferior border of cricoid Three subsites : paired pyriform sinus, posterior hypopharyngeal wall, post cricoid Character : submucosal extension & skipping 15 mm 20mm 20mm 30mm
32 Hypopharynx Post pharyngeal wall : wide local excision followed by skin grafting or pedicled flap or free flap ( jejunal free flap). Pyriform sinus : Partial larygopharyngectomy supracricoid partial laryngectomy Reconstruction: Partial wall defect :pedicle flap Circumferential defect : jejunal free flap

33
34
35 Supraglottic cancer: Organ preservation Early supraglottic cancers Exophytic lesions T1/T2 Radoitherapy the gold standard Early lesions with T1/T2 pre epiglottic involvement Impaired VC movement Conservative laryngeal resection T3/T4 lesions : Surgery followed by RT Subtotal supraglottic laryngectomy Three quarter laryngectomy Near total laryngectomy Total laryngectomy
36 Glottic cancer : organ preservation Voice Aspiration(surgery) Dysmotility(RT)


37 Conservative laryngectomy :Glottic cancer Radiotherapy : gold standard in early glottic cancer Surgery : Cordectomy Laser excision Hemilaryngectomy Vertical partial laryngectomy


38 Conservative laryngectomy Vertical partial laryngectomy Supracricoid partial laryngectomy
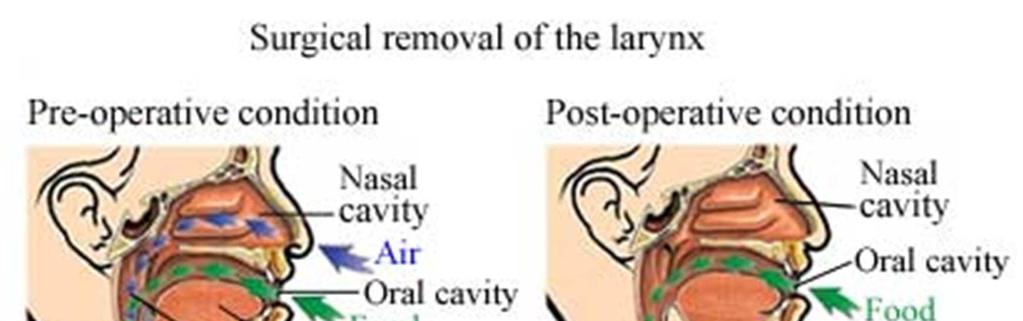
39 Laryngectomy

40 Voice rehabilitation after laryngectomy Esophageal voice
41 Mandibulectomy :indications and options Goal : provide R0 status with 1cm margin Types : Mandible is involved:segmental Hemimadibulectomy(Commando) No clear invasion but within 1cm : marginal mandibulectomy (superior half or lingual cortex shaved off.more than 60% resection required plate stabilization)
42




43 Mandibulectomy-reconstruction
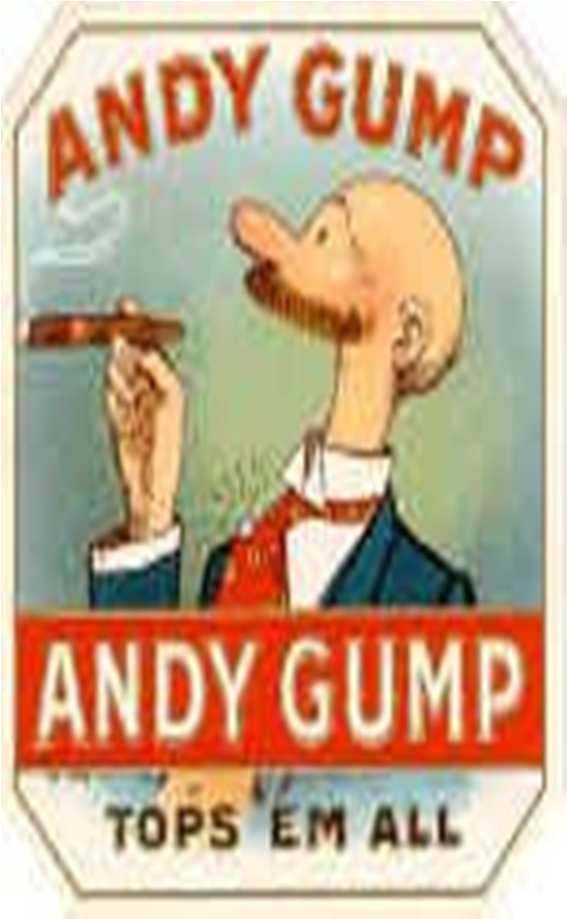
44 Mandibulectomy-Reconstruction Andy Gump deformity
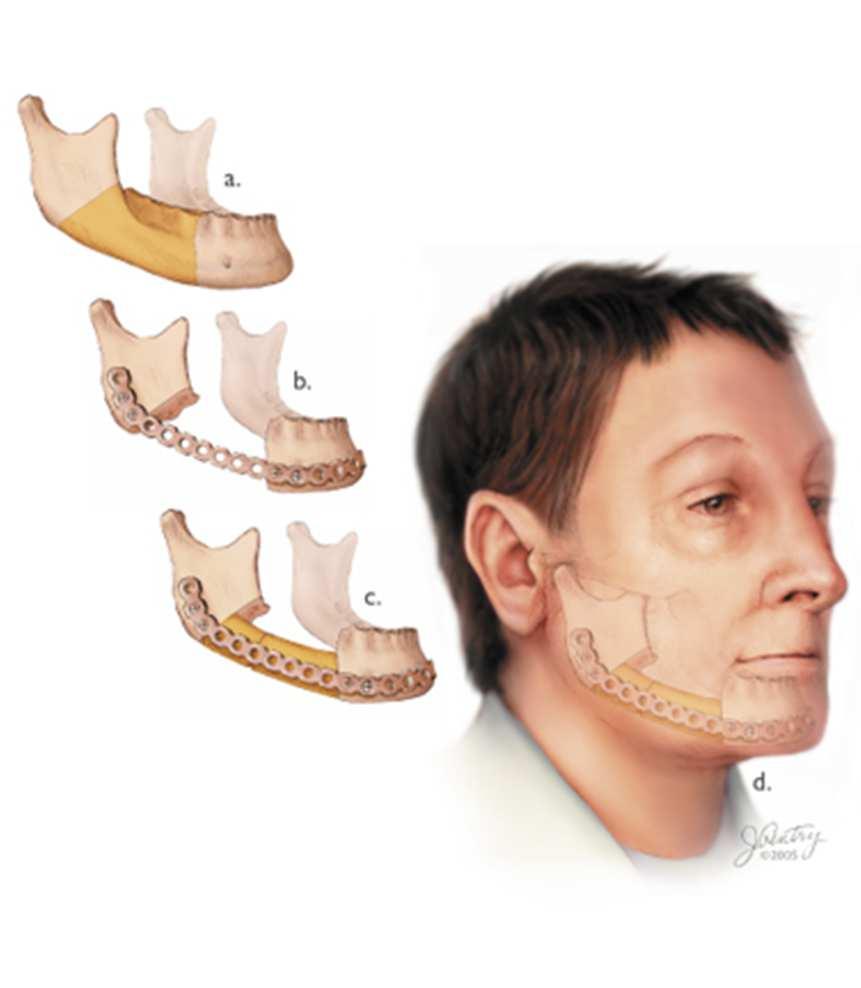
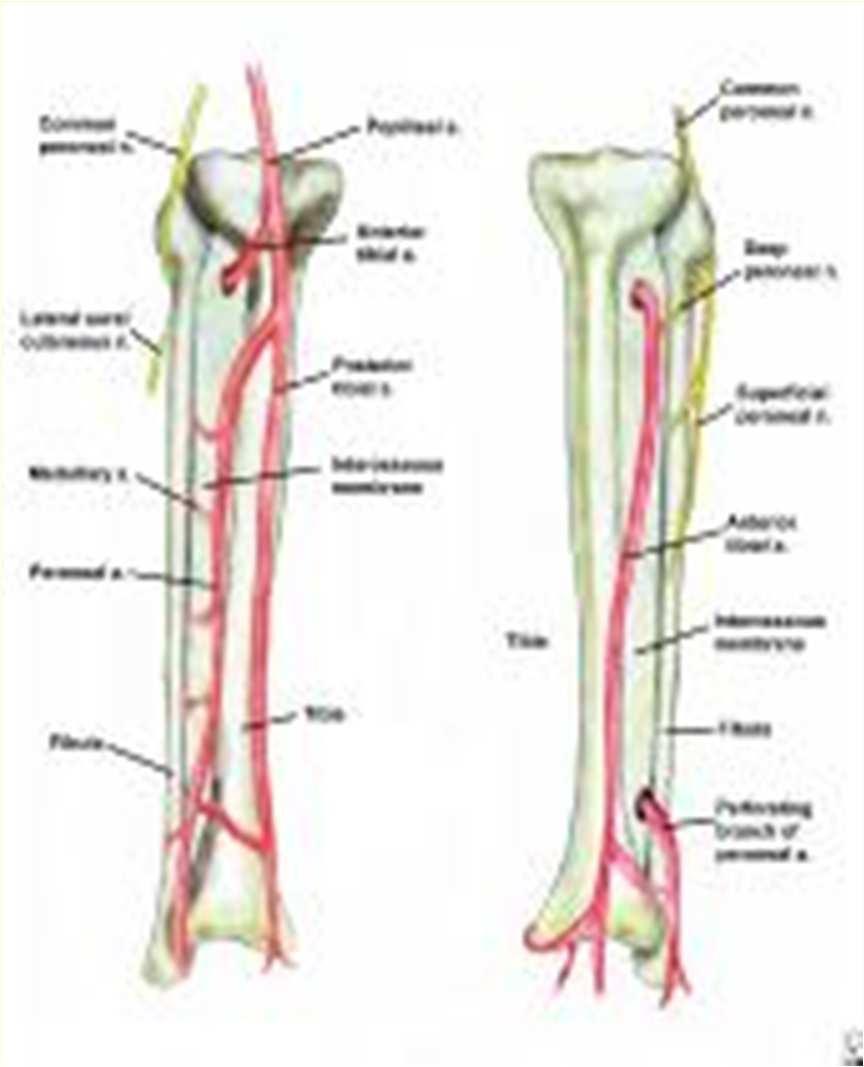
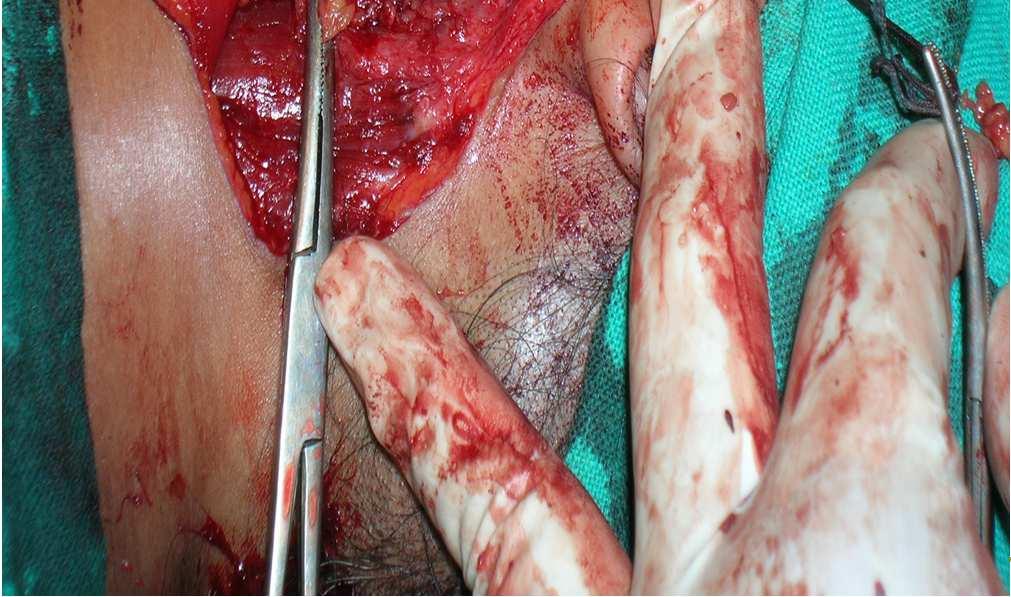
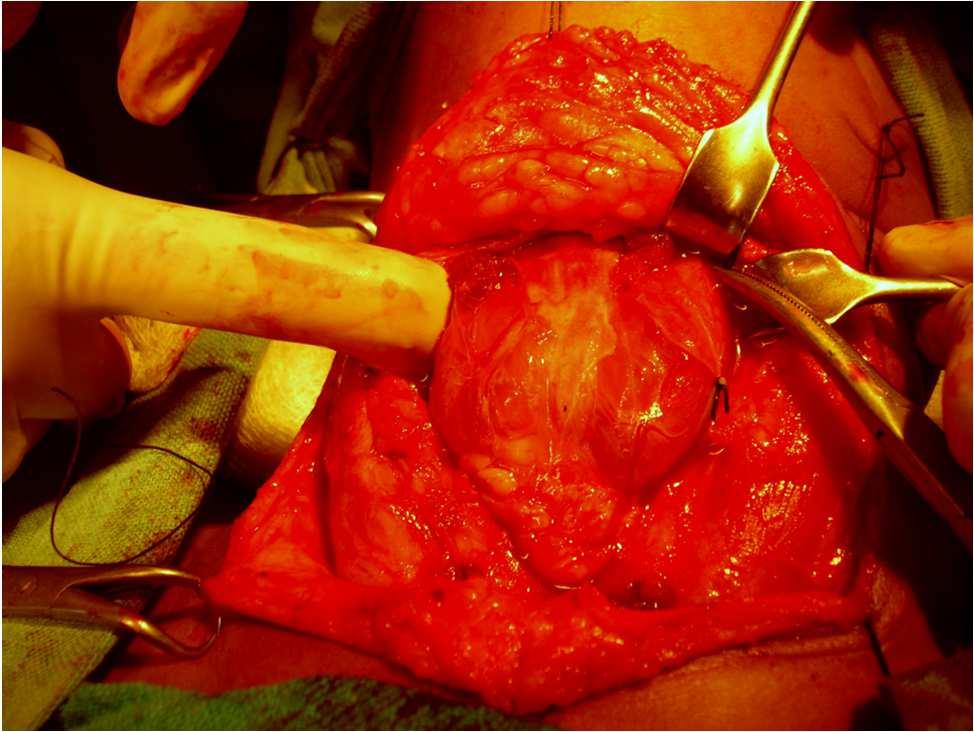
45 Mandibulectomy-reconstruction Soft tissue+plates Fibular free graft (osseomyocutaneous Free graft)


46 HN SCC.. Are we ready to tame the bull?
47



48 Parotid cancers: nerve preservation




49 Parotidectomy :Types Deep Lobe Masseter Superficial lobe Radical parotidectomy +/- Radiotherapy Mandible Facial nerve


50 Malignant Cylindroma of scalp Wide local excision followed by split skin grafting


51 Basal cell cancer


52 Thyroid cancer

53 Parathyroid cancer
54 N0- elective surgery, prophylactic RT,observation N+ (mobile)-surgery N+ (fixed)- Neoadjuvant.. surgery
: Larynx cancers Posterolateral ND(2,3,4,5): SCC, melanoma scalp Anterolateral ND(6) : Thyroid cancers")
55 Management of neck secondaries impalpable neck nodes Supraomohyoid (1,2,3) ND: Oral cavity cancers Lateral ND (2,3,4): Larynx cancers Posterolateral ND(2,3,4,5): SCC, melanoma scalp Anterolateral ND(6) : Thyroid cancers
56 Management of neck secondaries palpable neck nodes Palpable clinically obvious neck metastasis : Modified radical neck dissection (MRND) removal 1to 5 level nodes with preservation of Jugular vein, sternocleidomastoid and spinal accessory nerve Fixed nodes : Radical neck dissection (RND)
57 Management of recurrent HNC Oral cavity :Radical surgery +/- RT CRT and hyperthermia(under evaluation) Oropharynx : Surgery if previous RT fails RT if surgery fails/rt not given CT/hyperthermia (under evaluation) Larynx : Surgery if previously irradiated Reirradiation in small recurrences Hypopharynx : Surgery and/or RT
58 The philosophy The success of HNC treatment only partly lies in improving the 5yrs survival. The true challenge lies in restoring funtion and anatomy. There cannot be any fixed protocol as all cases need tailormade treatment. While planning treatment..
59 The take home message.. Disease extent The anatomy & Function involved Occupation And Social role The Infrastructure available Best and The Optimum outcome



60 Bridging the gap




61
FACULTY OF MEDICINE SIRIRAJ HOSPITAL
 Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
Neck Dissection Pornchai O-charoenrat MD, PhD Division of Head, Neck and Breast Surgery Department of Surgery FACULTY OF MEDICINE SIRIRAJ HOSPITAL Introduction Status of the cervical lymph nodes is the
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City.
 JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
JOSE FRANCISCO GALLEGOS HERNANDEZ Hospital de Oncología, CMN SXXI. IMSS México City. HNSCC with a global incidence of over 500,000 cases and 200,000 deaths annually is the leading cause of mortality and
(loco-regional disease)
") (loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
(loco-regional disease) (oral cavity) (circumvillae papillae) (subsite) A (upper & lower lips) B (buccal membrane) C (mouth floor) D (upper & lower gingiva) E (hard palate) F (tongue -- anterior 2/3 rds
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
A220: Larynx cancer tissues. (formalin fixed)
") A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A220: Larynx cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Larynx cancer tissues No. of spots: 2 spots from each cancer case (90 spots) 4 non-neoplastic
A Pathologist s Guide to Neck Dissection. Neck Dissections. Lymphatics of head and neck. Neck Dissections
 A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
A Pathologist s Guide to Neck Dissection North American Society for Head and Neck Pathology Companion Meeting 2006 Sigrid Wayne, M.D. Department of Pathology University of Iowa The presence of cervical
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
2. Guidelines for Reporting Head and Neck Tumours
 39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
39 40 2. Guidelines for Reporting Head and Neck Tumours Compilation and editing of this volume: Dr. Modini Jayawickrama (Consultant Histopathologist) List of contributors Consultant Histopathologists Dr.
Cancer of the Oral Cavity
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology Cancer of the Oral Cavity Ashok Shaha Principals of Management of Oral Cancer A)
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Principles of Management of Head & Neck Cancer. Jinka Sathya Associate professor of Oncology
 Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Lecture 07. Lymphatic's of Head & Neck. By: Dr Farooq Amanullah Khan PMC
 Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Oral cancer: Prognosis & Treatment. Dr. Hani Al Sheikh Radhi
 Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
Oral cancer: Prognosis & Treatment Dr. Hani Al Sheikh Radhi Prognostic factors in Oral caner TNM staging T stage N stage M stage Site Histological Factors Vascular & Perineural Invasion Surgical Margins
THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION
 THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION Emre Vural, MD, James Y. Suen, MD Department of Otolaryngology-Head and Neck Surgery, University of Arkansas for Medical Sciences, 4301 West Markham,
THE SUBMENTAL ISLAND FLAP IN HEAD AND NECK RECONSTRUCTION Emre Vural, MD, James Y. Suen, MD Department of Otolaryngology-Head and Neck Surgery, University of Arkansas for Medical Sciences, 4301 West Markham,
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
A novel classification system for the evaluation and reconstruction of oral defects following oncological surgery
 ONCOLOGY LETTERS 14: 7049-7054, 2017 A novel classification system for the evaluation and reconstruction of oral defects following oncological surgery WEI WEI LIU, CHU YI ZHANG, JIAN YIN LI, MING FANG
ONCOLOGY LETTERS 14: 7049-7054, 2017 A novel classification system for the evaluation and reconstruction of oral defects following oncological surgery WEI WEI LIU, CHU YI ZHANG, JIAN YIN LI, MING FANG
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Volumi di trattamento del cavo orale
 SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
Management of Salivary Gland Malignancies. No Disclosures or Conflicts of Interest. Anatomy 10/4/2013
 Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
Management of Salivary Gland Malignancies Daniel G. Deschler, MD Director: Division of Head and Neck Surgery Massachusetts Eye & Ear Infirmary Massachusetts General Hospital Professor Harvard Medical School
CERVICAL LYMPH NODES
 CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
(formalin fixed) 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm
 6 non-neoplastic spots (6 spots) Corresponding normal tissues with cancers: Yes Diameter: 1. 0 mm") CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
CBA729-Test slide, Head and neck cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 6 Tissue type: Test slide, Head and neck cancer tissues No. of spots: 6 spots from each
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Surgery. Head and Neck Cancers III: Treatment and Survival. Lip. Surgery might be the only treatment
 Head and Neck Cancers III: Treatment and Survival 2004 A.D.A.M., Inc. Division of Cancer Prevention and Control NCCDPHP, CoCHP Centers for Disease Control and Prevention Atlanta, Georgia Surgery 2 Lip
Head and Neck Cancers III: Treatment and Survival 2004 A.D.A.M., Inc. Division of Cancer Prevention and Control NCCDPHP, CoCHP Centers for Disease Control and Prevention Atlanta, Georgia Surgery 2 Lip
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
Long Term Toxicities of Head & Neck Cancer Therapies. Faith Mutale Abramson Cancer Center University of Pennsylvania
 Long Term Toxicities of Head & Neck Cancer Therapies Faith Mutale Abramson Cancer Center University of Pennsylvania Head & Neck Cancer 2-3% of all cancers 1-2% of all cancer deaths Incidence includes:
Long Term Toxicities of Head & Neck Cancer Therapies Faith Mutale Abramson Cancer Center University of Pennsylvania Head & Neck Cancer 2-3% of all cancers 1-2% of all cancer deaths Incidence includes:
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Report of Head and Neck Cancer Registry of Japan. Clinical Statistics of Registered Patients, 2002
 Report of Head and Neck Cancer Registry of Japan Clinical Statistics of Registered Patients, Japan Society for Head and Neck Cancer Cancer Registry Committee Preface The Head and Neck Cancer Registry of
Report of Head and Neck Cancer Registry of Japan Clinical Statistics of Registered Patients, Japan Society for Head and Neck Cancer Cancer Registry Committee Preface The Head and Neck Cancer Registry of
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic space
 Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Stroboscopy Rounds February 8, 2008 C. Matt Stewart, M.D.,Ph.D. Compartmentalization of the larynx Sites and subsites Supraglottis Glottis subglottis Spaces Pre-epiglottic epiglottic space Para-glottic
Delineation Of Privileges Otolaryngology Privileges
 OTOLARYNGOLOGY PRIVILEGES Criteria - New Applicants: Board Certification or qualified for certification by the American Board of Otolaryngology. Criteria - Current Staff Members Only: Successful completion
OTOLARYNGOLOGY PRIVILEGES Criteria - New Applicants: Board Certification or qualified for certification by the American Board of Otolaryngology. Criteria - Current Staff Members Only: Successful completion
Delineation Of Privileges Otolaryngology Privileges
 Delineation Of s Otolaryngology s OTOLARYNGOLOGY PRIVILEGES Criteria - New Applicants: Board Certification or qualified for certification by the American Board of Otolaryngology. Criteria - Current Staff
Delineation Of s Otolaryngology s OTOLARYNGOLOGY PRIVILEGES Criteria - New Applicants: Board Certification or qualified for certification by the American Board of Otolaryngology. Criteria - Current Staff
Reconstruction of Hypopharynx and Cervical Oesophagus for Treatment of Advanced Hypopharyngeal Carcinoma and Recurrent Laryngeal Carcinoma
 Original Article Reconstruction of Hypopharynx and Cervical Oesophagus for Treatment of Advanced Hypopharyngeal Carcinoma and Recurrent Laryngeal Carcinoma Guo-Hua Hu, Shi-Xun Zhong, Qing Xiao, 1 Yi Qian,
Original Article Reconstruction of Hypopharynx and Cervical Oesophagus for Treatment of Advanced Hypopharyngeal Carcinoma and Recurrent Laryngeal Carcinoma Guo-Hua Hu, Shi-Xun Zhong, Qing Xiao, 1 Yi Qian,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Oral cavity : consist of two parts: the oral vestibule and the oral cavity proper. Oral vestibule : is slit like space between.
 Oral cavity Oral cavity : consist of two parts: the oral vestibule and the oral cavity proper Oral vestibule : is slit like space between the teeth, buccal gingiva, lips, and cheeks 1 Oral cavity Oral
Oral cavity Oral cavity : consist of two parts: the oral vestibule and the oral cavity proper Oral vestibule : is slit like space between the teeth, buccal gingiva, lips, and cheeks 1 Oral cavity Oral
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Prevertebral Region, Pharynx and Soft Palate
 Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
Unit 20: Prevertebral Region, Pharynx and Soft Palate Dissection Instructions: Step1 Step 2 Step 1: Insert your fingers posterior to the sternocleidomastoid muscle, vagus nerve, internal jugular vein,
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto
 Wharton Head and Neck Centre The Toronto General Hospital Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto Controversies
Wharton Head and Neck Centre The Toronto General Hospital Dr. P. Gullane Wharton Chair Head & Neck Surgery Professor Department of Otolaryngology -Head & Neck Surgery University of Toronto Controversies
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
9.1 Local Address 9.2 Name & Address of Referring / Family Doctor......
 8. Duration of Stay (at the permanent place of residence (in years)) 9.1 Local Address 9.2 Name & Address of Referring / Family Doctor............ Name of City/Town/District... Pin Code Name of City/Town/District...
8. Duration of Stay (at the permanent place of residence (in years)) 9.1 Local Address 9.2 Name & Address of Referring / Family Doctor............ Name of City/Town/District... Pin Code Name of City/Town/District...
Anatomy of Head of Neck Cancer
 Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Anatomy of Head of Neck Cancer J. Robert Newman, MD The ENT Center of Central GA H&N Cancer Overview Most categories of cancer are represented in the H&N Squamous cell carcinoma most common mucosal cancer
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
ORIGINAL ARTICLE. Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx
 ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
ORIGINAL ARTICLE Salvage Surgery After Failure of Nonsurgical Therapy for Carcinoma of the Larynx and Hypopharynx Sandro J. Stoeckli, MD; Andreas B. Pawlik, MD; Margareta Lipp, MD; Alexander Huber, MD;
Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :
![Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :](/thumbs/88/115294566.jpg "Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :") Lec [5] / Temporal fossa : Borders of the Temporal Fossa: Superior: Superior temporal line. Inferior: gap between zygomatic arch and infratemporal crest of sphenoid bone. Anterior: Frontal process of the
Lec [5] / Temporal fossa : Borders of the Temporal Fossa: Superior: Superior temporal line. Inferior: gap between zygomatic arch and infratemporal crest of sphenoid bone. Anterior: Frontal process of the
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Tympanic Bulla Temporal Bone. Digastric Muscle. Masseter Muscle
 Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Superior view Hyoid Bone The hyoid bone does not articulate with any other bones. It is held in place by ligaments to the styloid process of the temporal bone and the thyroid cartilage of the larynx. It
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Anatomy of Oral Cavity DR. MAAN AL-ABBASI
 Anatomy of Oral Cavity DR. MAAN AL-ABBASI By the end of this lecture you should be able to: 1. Differentiate different parts of the oral cavity 2. Describe the blood and nerve supply of mucosa and muscles
Anatomy of Oral Cavity DR. MAAN AL-ABBASI By the end of this lecture you should be able to: 1. Differentiate different parts of the oral cavity 2. Describe the blood and nerve supply of mucosa and muscles
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide
 The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
Polymorphous Low-Grade. December 5 th, 2008
 Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Learning Objectives. Head and Neck Cancer: Post-Treatment Changes. Neck Dissection Classification * Radical neck dissection. Radical Neck Dissection
 Head and Neck Cancer: Post-Treatment Changes Daniel W. Williams III, MD Learning Objectives In patients treated for H/N Cancer: Describe the various types of neck dissections Explain reconstruction techniques
Head and Neck Cancer: Post-Treatment Changes Daniel W. Williams III, MD Learning Objectives In patients treated for H/N Cancer: Describe the various types of neck dissections Explain reconstruction techniques
Basic Anatomy and Physiology of the Lips and Oral Cavity. Dr. Faghih
 Basic Anatomy and Physiology of the Lips and Oral Cavity Dr. Faghih It is divided into seven specific subsites : 1. Lips 2. dentoalveolar ridges 3. oral tongue 4. retromolar trigone 5. floor of mouth 6.
Basic Anatomy and Physiology of the Lips and Oral Cavity Dr. Faghih It is divided into seven specific subsites : 1. Lips 2. dentoalveolar ridges 3. oral tongue 4. retromolar trigone 5. floor of mouth 6.
Information and support
 13 11 20 Information and support Surgery for head and neck cancer Last reviewed June 2012 Contents Types of surgeries Surgery for oral cancer Surgery for salivary gland cancer Surgery for pharyngeal cancer
13 11 20 Information and support Surgery for head and neck cancer Last reviewed June 2012 Contents Types of surgeries Surgery for oral cancer Surgery for salivary gland cancer Surgery for pharyngeal cancer
Neck Dissection. Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)
, BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL)") Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
Neck Dissection Asst Professor Jeeve Kanagalingam MA (Cambridge), BM BCh (Oxford), MRCS (Eng), DLO, DOHNS, FRCS ORL-HNS (Eng), FAMS (ORL) History radical neck Henry Butlin proposed enbloc removal of upper
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Q&A. Fabulous Prizes. Collecting Cancer Data: Pharynx 12/6/12. NAACCR Webinar Series Collecting Cancer Data Pharynx
 Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Pharynx NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
NAACCR Hospital Registry Webinar Series
 NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
NAACCR Hospital Registry Webinar Series Shannon Vann, CTR Jim Hofferkamp, CTR Webinar Series 1 Abstracting Larynx Cancer Incidence & Treatment Data Estimated new cases and deaths from laryngeal cancer
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Neck-2. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Neck-2 ` Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Triangles of the neck Side of the neck Midline Lower border of mandible Line between angle of mandible and mastoid Superior nuchal
Temporal region. temporal & infratemporal fossae. Zhou Hong Ying Dept. of Anatomy
 Temporal region temporal & infratemporal fossae Zhou Hong Ying Dept. of Anatomy Temporal region is divided by zygomatic arch into temporal & infratemporal fossae. Temporal Fossa Infratemporal fossa Temporal
Temporal region temporal & infratemporal fossae Zhou Hong Ying Dept. of Anatomy Temporal region is divided by zygomatic arch into temporal & infratemporal fossae. Temporal Fossa Infratemporal fossa Temporal
SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR
 HPV CS SITE SPECIFIC FACTOR") SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR Anus: Anal Canal; Anus, NOS; Other Parts of Rectum C21.0-C21.2, C21.8 C21.0 Anus, NOS (excludes skin of anus and perianal skin C44.5) C21.1 Anal canal C21.2
SITES (ALPHABETICAL) HPV CS SITE SPECIFIC FACTOR Anus: Anal Canal; Anus, NOS; Other Parts of Rectum C21.0-C21.2, C21.8 C21.0 Anus, NOS (excludes skin of anus and perianal skin C44.5) C21.1 Anal canal C21.2
Hiroyuki Hanakawa, Nobuya Monden, Kaori Hashimoto, Aiko Oka, Isao Nozaki, Norihiro Teramoto, Susumu Kawamura
 Accepted Manuscript Radiation-induced laryngeal angiosarcoma: Case report Hiroyuki Hanakawa, Nobuya Monden, Kaori Hashimoto, Aiko Oka, Isao Nozaki, Norihiro Teramoto, Susumu Kawamura PII: S2468-5488(18)30005-5
Accepted Manuscript Radiation-induced laryngeal angiosarcoma: Case report Hiroyuki Hanakawa, Nobuya Monden, Kaori Hashimoto, Aiko Oka, Isao Nozaki, Norihiro Teramoto, Susumu Kawamura PII: S2468-5488(18)30005-5
Department of Otolaryngology, Kurume University School of Medicine, Kurume, Japan
 THE KURUME MEDICAL JOURNAL Vol. 16, No. 3, 1969 PATHOLOGICAL STUDIES RELATING TO NEOPLASMS OF THE HYPOPHARYNX AND THE CERVICAL ESOPHAGUS IKUICHIRO HIROTO, YASUSHI NOMURA, KUSUO SUEYOSHI, SHIGENOBU MITSUHASHI,
THE KURUME MEDICAL JOURNAL Vol. 16, No. 3, 1969 PATHOLOGICAL STUDIES RELATING TO NEOPLASMS OF THE HYPOPHARYNX AND THE CERVICAL ESOPHAGUS IKUICHIRO HIROTO, YASUSHI NOMURA, KUSUO SUEYOSHI, SHIGENOBU MITSUHASHI,
Reconstruction of large mandibular defects
 Immediate Reconstruction of a Large Mandibular Defect of Locally Invasive Benign Lesions (A New Method) Gholamreza Shirani, OMFS, DDS, MS,* Mahnaz Arshad, DDS, 1 Farnoush Mohammadi, OMFS, DDS, MS* Tehran,
Immediate Reconstruction of a Large Mandibular Defect of Locally Invasive Benign Lesions (A New Method) Gholamreza Shirani, OMFS, DDS, MS,* Mahnaz Arshad, DDS, 1 Farnoush Mohammadi, OMFS, DDS, MS* Tehran,
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
CASE REPORT Reconstruction and Characterization of Composite Mandibular Defects Requiring Double Skin Paddle Fibular Free Flaps
 CASE REPORT Reconstruction and Characterization of Composite Mandibular Defects Requiring Double Skin Paddle Fibular Free Flaps Austin M. Badeau, BA, a and Frederic W.-B. Deleyiannis, MD, MPhil, MPH b
CASE REPORT Reconstruction and Characterization of Composite Mandibular Defects Requiring Double Skin Paddle Fibular Free Flaps Austin M. Badeau, BA, a and Frederic W.-B. Deleyiannis, MD, MPhil, MPH b
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY VERTICAL PARTIAL LARYNGECTOMY Management of small tumours involving the true vocal folds can be contentious. Tumour control is achieved
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
Piero Nicolai SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART. Department of Otorhinolaryngology University of Brescia
 Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
Biology and technology contribution to clinical advancement: the case of oropharyngeal cancer Brescia May 8 th, 2009 SURGERY FOR THE TREATMENT OF OROPHARYNGEAL CARCINOMA: STATE OF ART Piero Nicolai Department
Materials and Methods:
 Summary: Bipolar Vessel Sealing with the marclamp /marcut Bipolar Instruments and the maxium High-Frequency Generator in Thyroid Operations, Tumor Operations, Flap Plasties, and Neck Soft Tissue Interventions
Summary: Bipolar Vessel Sealing with the marclamp /marcut Bipolar Instruments and the maxium High-Frequency Generator in Thyroid Operations, Tumor Operations, Flap Plasties, and Neck Soft Tissue Interventions
Anterior triangle of neck
 Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Anterior triangle of neck Dept. of Anatomy Zhou Hong Ying Outline boundary and subdivisions of ant. triangle contents of the triangle Muscles: suprahyoid muscles, infrahyoid muscles Nerves: CNⅩ, CNⅪ, CNⅫ,
Infratemporal fossa: Tikrit University college of Dentistry Dr.Ban I.S. head & neck Anatomy 2 nd y.
 Infratemporal fossa: This is a space lying beneath the base of the skull between the lateral wall of the pharynx and the ramus of the mandible. It is also referred to as the parapharyngeal or lateral pharyngeal
Infratemporal fossa: This is a space lying beneath the base of the skull between the lateral wall of the pharynx and the ramus of the mandible. It is also referred to as the parapharyngeal or lateral pharyngeal
CLINICAL MEDICATION POLICY
 CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY TOTAL GLOSSECTOMY FOR TONGUE CANCER Johan Fagan Total glossectomy has significant morbidity in terms of intelligible speech, mastication,
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY TOTAL GLOSSECTOMY FOR TONGUE CANCER Johan Fagan Total glossectomy has significant morbidity in terms of intelligible speech, mastication,
L ARYNX S TAGING F ORM
 CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
CLI N I CA L Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX T0 Tis a b L ARYNX S TAGING F ORM LATERALITY: TUMOR SIZE: left
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Surgical Effects on Swallowing DYSPHAGIA AFTER TREATMENT FOR HNC: WHAT CAUSES IT? WHAT TREATMENT WORKS? Surgical Effects on Swallowing
 Susan Langmore, PhD, CCC-SLP, BRS-S Professor, BUMC, BU September 27, 2010 DYSPHAGIA AFTER TREATMENT FOR HNC: WHAT CAUSES IT? WHAT TREATMENT WORKS? Incidence of dysphagia after XRT VA study (Wolf; Terrell
Susan Langmore, PhD, CCC-SLP, BRS-S Professor, BUMC, BU September 27, 2010 DYSPHAGIA AFTER TREATMENT FOR HNC: WHAT CAUSES IT? WHAT TREATMENT WORKS? Incidence of dysphagia after XRT VA study (Wolf; Terrell
Indications and techniques of surgery for the primary treatment of HNSCC
 Prof. Christian Simon Chef-de-service Service d ORL et chirurgie cervico-faciale Centre Hospitalier Universitaire Vaudois (CHUV) Université de Lausanne Lausanne, Suisse Indications and techniques of surgery
Prof. Christian Simon Chef-de-service Service d ORL et chirurgie cervico-faciale Centre Hospitalier Universitaire Vaudois (CHUV) Université de Lausanne Lausanne, Suisse Indications and techniques of surgery
Since the first description of the radical neck dissection by George Crile almost a century
 ORIGINAL ARTICLE Neck Dissection Classification Update Revisions Proposed by the American Head and Neck Society and the American Academy of Otolaryngology Head and Neck Surgery K. Thomas Robbins, MD; Garry
ORIGINAL ARTICLE Neck Dissection Classification Update Revisions Proposed by the American Head and Neck Society and the American Academy of Otolaryngology Head and Neck Surgery K. Thomas Robbins, MD; Garry
Head & Neck Case # 1
 DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge
DISCHARGE SUMMARY Head & Neck Case # 1 Date of Admission: 10/30/2010 Date of Discharge: 11/02/2010 Present Medical History: The patient is a 33-year-old lady with a history of right superior alveolar ridge