Development of occlusion:
|
|
|
- Kellie Harris
- 5 years ago
- Views:
Transcription
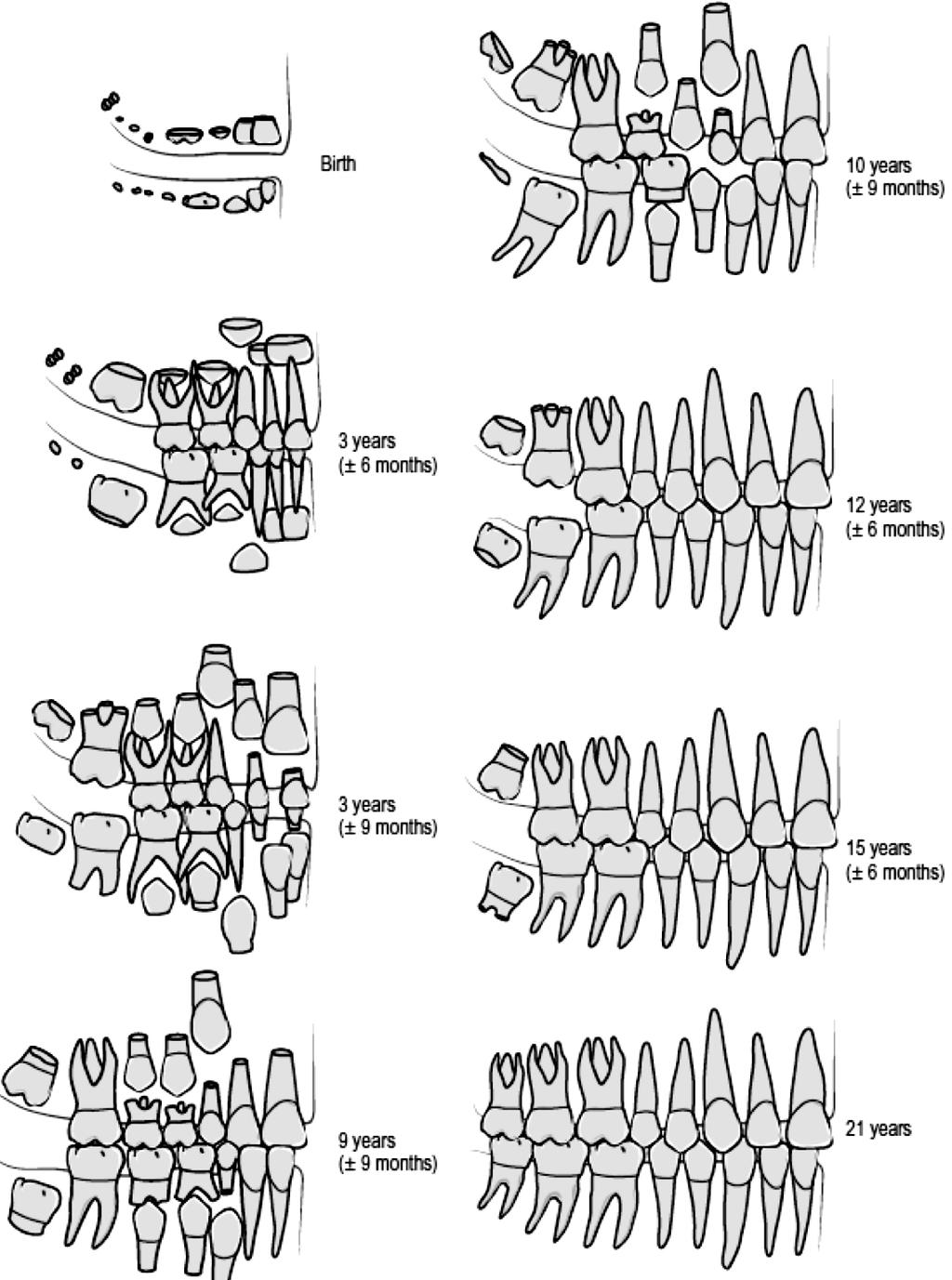
 Postnatal development of the dentition When a child is born, mineralization of all the primary tooth crowns is well underway, with this process also beginning in the first permanent molars.")
1 : Dr.Issam Aljorani (BDS, MSc. Ortho.) Postnatal development of the dentition When a child is born, mineralization of all the primary tooth crowns is well underway, with this process also beginning in the first permanent molars. The primary dentition will start to erupt in the first year of life and will be established by the end of the third. The permanent dentition is heralded by eruption of the first molars at around 6 years of age and is completed in most cases, by the appearance of the third molars in the late teenage years. The jaws at birth At birth, the maxillary dental arch is characteristically horseshoe-shaped whereas the mandibular arch assumes a wider U-shape. The mucous membrane of both the maxilla and mandible is thickened in the newborn infant to produce gum pads, which cover the alveolar processes containing the developing primary teeth. Usually the upper jaw overlaps the lower jaw in antero-posterior and in transverse direction, in other ward: the upper jaw is wider than the lower jaw and at the same time, the lower jaw is in a retrognathic position in relation to the upper. On the upper jaw, we can see the lateral sulcus, which express to the distal margin of the upper deciduous canine 1
2 and the gum pads, which is separated from the masticatory mucosa by a long and continuous groove called gingival groove. The upper lip at this stage is usually short, and the anterior oral seal of the mouth occurs due to the contact between the lower lip and the tongue. At this age the anterior gum pads is averted anteriorly and when the child closes his mouth there is a space between the anterior gum pads and the only part that is in contact are the future growing E(s) (Es region). The maxillary (left) and mandibular (middle) gum pads in isolation and occlusion (right). Note the prominent lateral sulci (LS) present in both arches. A, C, external arch width; B, D, internal arch width; E, F, anterior arch length; G, overjet; H, anteroposterior relationship; I, overbite. The elevations of the Es cannot be seen clearly, until the age of 5 months, the anterior opening of the mouth will facilitate the feeding process without discomfort to the mother, at this age usually the labial frenum is attached to the incisive papillary region and after the eruption of the deciduous it will migrate in upward direction and gives the incisive papillary attachment this is due to alveolar bone formation in association with the development of the deciduous teeth. Occasionally a child is born with teeth already present or that undergo precocious eruption within the oral cavity Natal teeth are present at birth. Neonatal teeth erupt within the first month of life; and Pre-erupted teeth appear within the second and third months of life. 2
3 Natal and neonatal teeth occur in around 1: 3000 children and are usually mandibular primary incisors, although rarely they can be supernumerary teeth. They are often poorly developed, mobile and can cause ulceration of the mouth and nipple during suckling. If these teeth give rise to problems, they should be removed. Deciduous Dentition Usually the deciduous teeth begin to erupt at the sixth months of age until years of age. (All the deciduous teeth will be erupted, completely, at the age of third years), and can be a source of some malaise for the child. Teething is associated with tender swollen gums, irritability, finger sucking, drooling and nocturnal crying. It is generally selflimiting but can be relieved by allowing the child to chew on clean, hard, cool objects and the provision of appropriate analgesia, either in the form of an elixir or lignocaine based teething gel. Occasionally, primary tooth eruption is preceded by the appearance of an eruption cyst, a small bluish-type swelling, which overlies the erupting tooth. These generally disappear, but can be excised if they persist. Eruption sequence of deciduous dentition: This includes: Lower (As) at 6th month, Lower (Bs) at 7th month, Upper (As) at 8th month, Upper (Bs) at 9th moth, Lower (Ds) at 12th month, Upper (Ds) at 14th month, Lower (Cs) at 16th month, upper (Cs) at 18th month, Lower (Es) at 20th month, Then finally, upper (Es) at 24th month. The first sign of the formation of the deciduous teeth is at the age of 4-6 months IUL, and their roots will be completely formed after months after their eruption. When these 3

4 teeth erupt in the mouth, they will erupt in a vertical direction i.e. the upper long axes of the centrals coincide with the long axis of the lower incisors, and usually there is slightly increase in the over-jet. These teeth usually present in their crept in a rotated manner, this is to occupy a less space in the child s mouth; so that, when they erupt, they will erupted in a spaced conditions, and these spaces usually present at the mesial aspect of the upper canine and the distal aspect of the lower canine. These spaces are termed as primary spaces or anthropoid spaces, since it looks like the spaces that are present between the teeth of the higher Apes. Such spaces also present mesial to the Ds, these spaces that are anterior to the Ds, try to close in a way that: the distal surface of the D (upper and lower) will be located on the same terminal plane and usually the lower D is larger in mesiodistal dimension than the upper D. The Es when erupt, they erupt in the same terminal plane (flush terminal). In summery the complete primary dentition is classically associated with a number of characteristic features: The arches are semi-circular in shape; The incisors are spaced, upright and associated with a positive overjet and overbite; Primate or anthropoid spaces are present, mesial to the maxillary primary canines and distal to the mandibular canines; The molar and canine relationship is class I; and The distal edges of the second primary molars are flush in the vertical plane. 4

5 Changes in spaces: The spaces of the deciduous teeth try to increase with age due to the growth of the jaws in: antroposterior, transverse and vertical direction, and due to: attrition; since the shape of the deciduous teeth is triangular and these teeth will be subjected to a great amount of attrition due to wear at the incisal edges; so, the spaces will be increased, especially anteriorly due to the attrition. This attrition will occur at the incisal edges and the proximal surfaces since the deciduous teeth mostly converted into edge to edge relationship at a later stage. At the age of years the permanent teeth begun to erupt, and these teeth contains an eruptive cyst, and this is filled with fluid, this fluid will exert a pressure on the roots of the deciduous teeth causing their resorption with the aid of special enzyme which is produced at this stage of age. The roots resorption of the deciduous teeth means decrease in the root length and since the occlusal forces at the age of 5-6 years are more than those of 3 years; so, these occlusal forces together with the root resorption will increase the mobility of the deciduous teeth and if the deciduous teeth in closed case (without spacing), this will produce attrition of the proximal surfaces due to friction produced by movement during mastication, as the mobility progress the spaces will be increased and this will facilitate the process of normal shedding of the incisors. Usually, the permanent teeth when erupt,they are located at the palatal or lingual aspect of the deciduous incisors, causing their resorption during eruption, but sometimes, the permanent teeth could be deflected from the roots of incisors; therefore, this process will not happen in the normal way, and the permanent erupt,while the deciduous is stay in its space. 5
6 Permanent Teeth: Variations in the eruption sequence of the permanent teeth are common, but as a rule, the mandibular teeth erupt prior to the maxillary. Permanent teeth begin their eruption once crown formation is completed, taking between 2 and 5 years to reach the alveolar crest and a further 1 to 2 years to reach occlusion. Root development is usually completed within 2 years of eruption. Permanent teeth replace the deciduous teeth (A, B, C, D and E) by (1, 2, 3, 4 and 5); while, the molars (6, 7 and 8) are developed in a separate entity. The sequence and timing of emergence of permanent teeth include: 1-First stage for permanent teeth emergence (development). Lower 6 at 6 years Upper 6 at years Lower 1 at 6.5 years Upper 1& lower 2 at 7.5 years Upper 2 at 8.5 years. There is a silent period extend from 8.5 years of age to 10 years of age, this period is called (Lull period). In this stage: there is no teeth emergence (development) or exfoliation, but there is changes in the occlusion including the anteroposterior and vertical dimension. 2-Second stage of permanent teeth emergence: Upper 4& lower 3 at 10 years Lower 4 at 10.5 years Upper & lower 5 at 11 years Upper 3 at 11.5 years Upper & lower 7 at 12 years 6
7 3-Third stage of permanent teeth emergence: It is the stage of emergence of the third molars at the age between 18 to 24 years of age (some time above 25). The sequence of teeth emergence:- For the upper permanent teeth is ( ) 100%. While the sequence of emergence of the lower permanent teeth is either: ( ) in 50% of cases, or: ( ). In the lower arch, the first premolar may erupt after the emergence of the lower canine or before it. Normal emergence at the first stage of permanent teeth The permanent central incisors will replace the deciduous central incisors, and the deciduous lateral incisors also will be replaced by the permanent lateral incisors. Now: the question is that: How the central incisors erupt in a normal condition in spite of their mesiodistal collective width is larger than that of the deciduous teeth? This normal emergence will occur due to these reasons: 1- Utilization of all the spaces that is present between the deciduous teeth. 2- Due to proclination of the incisors during the eruption. 3- Due to the secondary spaces. 4- Transverse increase in the intercanine arch width. About the first reason: usually there is a space mesial to the upper deciduous canine and distal to the lower deciduous canine and this space will be utilized by the incisors during their eruption. However, the space distal to the lower canine can be utilized by the buccal segment teeth during (the early mesial shift). About the second reason: the incisors erupt in a proclined situation and this will increase the available arch length present for the permanent incisors, and this proclination is mainly due to the increase in activity of the tongue at this period (8.5 years) due to the increased amount of the growth stimulation hormone at this period. 7
8 About the third reason: during the eruption of the lower incisor, the lower deciduous canine will be pushed in a distal and buccal direction due to the fact that: the collective mesiodistal width of the permanent incisors is more than the collective mesiodistal width of the deciduous incisors, and since there is a contact between the lower deciduous canine and the upper canine during the lateral extrusion and during the protrusion so, the upper deciduous canine will be pushed in a lateral and distal direction and this will produce an additional spaces named as: secondary spaces, which will be utilized by the permanent incisors. This will permit the permanent incisors of the adult face which is present in a small child face to erupt in a normal way. Variations (changes) exist during the eruption of incisors: The permanent central incisors and the lateral incisors erupt palatal to the deciduous incisors in the upper arch, and lingual to the deciduous incisors in the lower arch, and in their development (eruption), they should be guided into a downward and forward direction to contact the roots of the deciduous incisors causing their resorption. Additionally the permanent incisors located in their crypts in a (zigzag) fashion, and the lateral usually trapped by the central incisors. Anyhow, if the incisors deflected from this path of eruption, they will erupt lingual and/or palatal to the deciduous incisors and this will lead to anterior cross bite, but if 8

9 there is normal path of eruption, they will erupt in a normal way. Since the lateral incisor situated lingual or palatal to the central incisor, therefore they may be influenced by: malocclusion more than the centrals; because they erupt later and if there is no available space in the dental arch the centrals will occupy the available space, and the remnant of the space may be not enough for the eruption of the lateral incisors. Therefore, they will be erupted in a rotated or cross bite condition. In the normal way: the lateral escapes from the central incisors at the time the centrals begun to erupt. A transient anterior open bite can be associated with eruption of the incisors as they approach the occlusal plane and this invariably improves with time. The maxillary central incisors can also be quite distally inclined when they first erupt, which produces a midline diastema between them. This physiological spacing or ugly duckling stage is thought to be due to the combined effect of the maxillary incisor apices being initially quite close together in the anterior maxilla as the incisors erupt and lateral pressure from the erupting maxillary lateral incisors and canines. As these teeth erupt, this pressure is transferred from the apical region of the maxillary incisors more coronally, improving their inclination and usually closing the diastema. Physiological spacing or ugly duckling stage 9
10 The first molars eruption: These teeth erupt as the upper and lower Es are still present. If the Es present with an cusp to cusp relationship (flush terminal plane) the 6s will erupt cusp to cusp relationship and this is the normal situation for eruption of 6s which will developed as a Cl I in 76% of cases, Cl III in 14% and Cl II in 10%. The initial occlusal relationship of the first permanent molars is directly influenced by the primary second molar position. If these teeth are flush in the terminal plane then the first permanent molars assume a cusp-to-cusp relationship when they erupt. In order to establish a class I molar relationship, some mesial movement of the mandibular first permanent molar will be required. This is achieved by two possible mechanisms: Early mesial shift, where the lower primate space (distal to the mandibular canine and therefore adjacent to the primary molar occlusion) is closed by forwards movement of the mandibular molar as the first permanent molar erupts; and Late mesial shift, where the mandibular first molar only moves in a mesial direction after loss of the second primary molar; because the mesiodistal length of the mandibular second primary molar crown is greater than the maxillary, the loss of these teeth results in greater mesial movement of the mandibular first molar. Occasionally, a mesial step occlusion of the primary molars might have been established prior to eruption of the permanent molars; in these cases they will tend to erupt directly into a class III occlusal relationship. Alternatively, there may be a distal step occlusion, in which case the first molars will erupt into a class II relationship. However, it should be remembered that all of these relationships affecting the primary molars and therefore establishment of the molar occlusion will be significantly influenced by the relative amounts of forwards maxillary and mandibular growth that occur during this time. 10
11 11

12 The second stage of development In the second stage of permanent teeth development: the C, D and E are replaced by 3, 4, and 5. In contrast to the incisor dentition, the combined mesiodistal length of the primary canine and molar teeth is greater than that of the permanent canine and premolars, an excess known as the leeway space. In the maxilla, this is approximately 1.5 mm per quadrant, whereas in the mandible it is closer to 2.5 mm, because of the increased size of the lower second primary molar. This difference in space is very important for the development of normal occlusion during late mesial shift. The variation exist in this period includes: Impaction of lower 5(s) due to lack of space for it due to or since it is the latter tooth which is erupted in the lower jaw mesial to the lower seven. While in the upper jaw, the lack of space will influence the canine eruption, since the latter tooth erupts prior to the upper seven in maxilla. For the lower second premolar: it may be erupted in the lingual direction or it may be impacted under the first permanent molar; while, for the upper canine: it could be erupted to the buccal direction or it could be impacted if it is directed palatals. Also in this period the reduction of the arch size lack of space is seen if one of these reasons is/are occur. In Iraq, the malposed canine can be seen in female more than in male and if it is erupted into a buccal direction it takes a mesiobuccal angulation and a buccal inclination. But, if it is directed palatally then, it will be mostly impacted because the masticatory mucosa cannot be pierced by the canine due to the presence of high amount of collagen fibers. The upper canine is influenced by the problem of malocclusion in a great amount in comparison to the other teeth due to its long path of eruption development since its early development occur under the orbit. 12

13 Crowding of the maxillary canine (left panel) and mandibular second premolar (right panel). The UR3 is buccally crowded due to timing of eruption; the LL5 is crowded due to early loss of the LLE. For the canine to developed normally, it should firstly directed mesially until it touches the apical part of the root of the lateral incisors, then it directed into a downward direction, and lateral direction till reaches the occlusal level. If the root of the lateral incisor is abnormal or the lateral is missed, then the canine will loss its guidance plane of eruption and it will be erupted in any direction or in any situation; therefore it will be subjected to more problem of malocclusion due to its tortuous path of eruption and due to the lack of space available for it, and due to its dependence on the presence or absence of the permanent lateral incisors. In this stage, there is a reduction in arch length as a result of; v Premature loss of primary second molars. v Ectopic eruption of the permanent maxillary first molar. v Reduction in arch length as a result of caries. About the eruption of Sevens (upper & lower): They erupt at the age of 12 years old, and they occupy the same position of the 6s and usually the upper seven developed below the maxillary antrum and situated in a high level in the maxillary tuberosity and it takes a long path of eruption, but it is less than the canine. In comparison with canine s path of eruption is twice as long as the second molar s path of eruption. Therefore, it is subjected 7 to a less amount of crowding in comparison with 13
14 the canine. Usually the upper sevens when erupt, they directed distally, occlusally and buccally, but for the lower sevens, they have a short path of eruption in spite of they developed at the anterior border of the ramus, but they are directed mesially and occlusally. Therefore, they are lower 7s subjected to a less amount of crowding in comparison with the upper sevens. The upper 7s in their eruption try to move in a faster rate to compensate for the downward and backward growth of the maxilla at the pterygomaxillary fissure = maxillary tuberosity. For the lower sevens: the ramus will increase in its width by bone resorption at the anterior part, and bone deposition at the posterior part. I.e. posterior border. This will provide a space for the eruption of the lower sevens. The malocclusion of the sevens is very rare and the impaction of the upper sevens is very rare, while the lower sevens may be impacted in some instances. Third stage of development: The eight try to erupt between the ages of years of age. The path of eruption of the 8s is nearly similar to the path of eruption of the 7s. The upper 8s developed at the posteroinferior position of the maxillary tuberosity, so, these teeth are subjected to a high amount of crowding in comparison with the 6s or 7s due to the lack of space available for them. The lower third molar may be subjected to impaction due to lack of space. These teeth may be absent congenitally due to etiological reasons since the human jaws tend to be reduced in size while, the size of teeth are remaining as it is. Occlusal changes in the permanent dentition The dentition does not remain static throughout life. Crowding of the mandibular incisors is one of the most common problems encountered in the permanent dentition and lower incisor alignment is one of the most likely things to relapse after orthodontic treatment. Studies of untreated subjects followed from the mixed dentition into adulthood have shown a tendency for the width and length of the mandibular arch to decrease and for crowding of the anterior teeth to increase. Primary crowding refers to a discrepancy of 14

15 tooth dimension and jaw size, mainly determined genetically. Secondary crowding is caused by environmental factors, including local space conditions in the dental arches and the position and function of the tongue, the lips and the buccal musculature. Tertiary crowding occurs during adolescence and post-adolescence with a predilection for the lower labial segment. Factors contributing to late lower incisor crowding may include: Mandibular growth rotations; Physiologic mesial drift; Soft tissue maturation; Degenerative periodontal changes allowing teeth to drift under light pressures; Change in diet and lack of interproximal wear; Tooth size and shape; Tooth loss and drifting leading to changes in occlusal function; and Mandibular third molars presence and position. In reality, all of these factors may contribute to the development of late lower incisor crowding but the contribution of developing third molars is regarded as being minimal as crowding can develop even in the absence of their development. The prophylactic removal of developing third molars is not recommended to prevent late lower incisor crowding. Late lower incisor crowding in an untreated mandibular arch. 15
16 16
17 References Contemporary orthodontics, Proffit, fifth edition, Development of human dentition, Lindon, second edition, Handbook of orthodontics, Martyn and Andrew, second edition, Textbook of Craniofacial Growth, Sridhar Premkumar, First Edition: Textbook of Orthodontics, Bishara Samir, first edition Dr.Issam M. Abdullah Aljorani BDS, MSc. Ortho
Development of occlusion
 Development of occlusion The development of dentition is an important part of craniofacial growth as the formation, eruption, exfoliation and exchange of teeth take place during this period. Term occlusion
Development of occlusion The development of dentition is an important part of craniofacial growth as the formation, eruption, exfoliation and exchange of teeth take place during this period. Term occlusion
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
Treatment planning of nonskeletal problems. in preadolescent children
 In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Fundamental & Preventive Curvatures of Teeth and Tooth Development. Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L.
 Dr. Margaret L.") Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Dr Robert Drummond. BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015
, FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015") Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
1. What is the highest and sharpest cusp on the lower first deciduous molar? 2. Which of the following is NOT the correct location of an embrasure?
 1 1. What is the highest and sharpest cusp on the lower first deciduous molar? a. mesiobuccal b. distobuccal c. distolingual d.mesiolingual 2. Which of the following is NOT the correct location of an embrasure?
1 1. What is the highest and sharpest cusp on the lower first deciduous molar? a. mesiobuccal b. distobuccal c. distolingual d.mesiolingual 2. Which of the following is NOT the correct location of an embrasure?
Primary Teeth Chapter 18. Dental Anatomy 2016
 Primary Teeth Chapter 18 Dental Anatomy 2016 Primary Teeth - Introduction Synonyms deciduous teeth, baby teeth, temporary teeth, milk teeth. There are 20 primary teeth, designated as A thru T in the Universal
Primary Teeth Chapter 18 Dental Anatomy 2016 Primary Teeth - Introduction Synonyms deciduous teeth, baby teeth, temporary teeth, milk teeth. There are 20 primary teeth, designated as A thru T in the Universal
Dental Morphology and Vocabulary
 Dental Morphology and Vocabulary Palate Palate Palate 1 2 Hard Palate Rugae Hard Palate Palate Palate Soft Palate Palate Palate Soft Palate 4 Palate Hard Palate Soft Palate Maxillary Arch (Maxilla) (Uppers)
Dental Morphology and Vocabulary Palate Palate Palate 1 2 Hard Palate Rugae Hard Palate Palate Palate Soft Palate Palate Palate Soft Palate 4 Palate Hard Palate Soft Palate Maxillary Arch (Maxilla) (Uppers)
#60 Ortho-Tain, Inc TIMING FOR CROWDING CORRECTIONS WITH THE OCCLUS-O-GUIDE AND NITE-GUIDE APPLIANCES
 #60 Ortho-Tain, Inc. 1-800-541-6612 TIMING FOR CROWDING CORRECTIONS WITH THE OCCLUS-O-GUIDE AND NITE-GUIDE APPLIANCES Although timing is not as critical for the Occlus-o-Guide appliance as it is with the
#60 Ortho-Tain, Inc. 1-800-541-6612 TIMING FOR CROWDING CORRECTIONS WITH THE OCCLUS-O-GUIDE AND NITE-GUIDE APPLIANCES Although timing is not as critical for the Occlus-o-Guide appliance as it is with the
#45 Ortho-Tain, Inc PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT
 #45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
#45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
Yasmeen Al-Khatib Pedo Sheet No /03/ /03/201. Dr. Suha Abu ghazaleh. Yasmeen Al-Khatib
 Yasmeen Al-Khatib Pedo Sheet No.7+8 29/03/2015 29/03/201 7+8 Dr. Suha Abu ghazaleh Yasmeen Al-Khatib 1 Yasmeen Al-Khatib Pedo Sheet No.7+8 29/03/2015 Eruption and Arch Development Lecture s Outline (lec.
Yasmeen Al-Khatib Pedo Sheet No.7+8 29/03/2015 29/03/201 7+8 Dr. Suha Abu ghazaleh Yasmeen Al-Khatib 1 Yasmeen Al-Khatib Pedo Sheet No.7+8 29/03/2015 Eruption and Arch Development Lecture s Outline (lec.
6610 NE 181st Street, Suite #1, Kenmore, WA
 660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
Lecture 2 Maxillary central incisor
 Lecture 2 Maxillary central incisor Generally The deciduous tooth appears in the mouth at 3 18 months of age, with 6 months being the average and is replaced by the permanent tooth around 7 8 years of
Lecture 2 Maxillary central incisor Generally The deciduous tooth appears in the mouth at 3 18 months of age, with 6 months being the average and is replaced by the permanent tooth around 7 8 years of
Development of the dentition
 4 Development of the dentition 85 Humans have two dentitions, the deciduous (primary) and permanent (secondary). Each dentition is heterodont, meaning that it consists of teeth with different shapes and
4 Development of the dentition 85 Humans have two dentitions, the deciduous (primary) and permanent (secondary). Each dentition is heterodont, meaning that it consists of teeth with different shapes and
Dental Anatomy and Occlusion
 CHAPTER 53 Dental Anatomy and Occlusion Ma Lou C. Sabino DDS, and Emily G. Smythe, DDS What numerical system is used most commonly in the United States for designating the adult dentition? Pediatric dentition?
CHAPTER 53 Dental Anatomy and Occlusion Ma Lou C. Sabino DDS, and Emily G. Smythe, DDS What numerical system is used most commonly in the United States for designating the adult dentition? Pediatric dentition?
Arrangement of posterior artificial teeth Standardized parameters Curve of Wilson Curve of Spee
 . Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
. Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
APPENDIX A. MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge)
 You will need this scoresheet and a disposable ruler (or a Boley Gauge)") APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
ORTHODONTIC INITIAL ASSESSMENT FORM (OIAF) w/ INSTRUCTIONS
 w/ INSTRUCTIONS") Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
RETENTION AND RELAPSE
 RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
Orthodontics. Anomalies
 Orthodontics Anomalies Anomalies of Teeth Groups of teeth Jaws Intermaxilary relations Anomalies of tooth number Hypodontics (hypodontia) the tooth (or teeth) are missing Third molars (if third molars
Orthodontics Anomalies Anomalies of Teeth Groups of teeth Jaws Intermaxilary relations Anomalies of tooth number Hypodontics (hypodontia) the tooth (or teeth) are missing Third molars (if third molars
Eruption and Shedding of Teeth
 Eruption and Shedding of Teeth Mixed Dentition: Presence of both dentitions Figure from Ten Cate s Oral Histology, Ed., Antonio Nanci, 6 th edition Tooth eruption is the process by which developing teeth
Eruption and Shedding of Teeth Mixed Dentition: Presence of both dentitions Figure from Ten Cate s Oral Histology, Ed., Antonio Nanci, 6 th edition Tooth eruption is the process by which developing teeth
The ASE Example Case Report 2010
 The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
Archived SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS
 SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
Sample Case #1. Disclaimer
 ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
Morphology of an Anatomic Crown. By: Assistant Professor Dr. Baydaa Ali Al - Rawi
 Morphology of an Anatomic Crown By: Assistant Professor Dr. Baydaa Ali Al - Rawi October 4, 2009 Elevated landmarks Depressed landmarks A) Elevated landmarks : 1. Dental lobe : is one of the primary centers
Morphology of an Anatomic Crown By: Assistant Professor Dr. Baydaa Ali Al - Rawi October 4, 2009 Elevated landmarks Depressed landmarks A) Elevated landmarks : 1. Dental lobe : is one of the primary centers
Peninsula Dental Social Enterprise (PDSE)
") Peninsula Dental Social Enterprise (PDSE) Orthodontic Checklist for Clinics Version 3.0 Date approved: November 2017 Approved by: The Board Review due: November 2018 Policy will be updated as required
Peninsula Dental Social Enterprise (PDSE) Orthodontic Checklist for Clinics Version 3.0 Date approved: November 2017 Approved by: The Board Review due: November 2018 Policy will be updated as required
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE
 MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER October 21,1996 October 28,1996 03-96-06 SUBJECT BY Information on New Procedures
MEDICAL ASSISTANCE BULLETIN COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF PUBLIC WELFARE ISSUE DATE EFFECTIVE DATE NUMBER October 21,1996 October 28,1996 03-96-06 SUBJECT BY Information on New Procedures
Class II Correction with Invisalign Molar rotation.
 Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
#27 Ortho-Tain, Inc PREVENTING MALOCCLUSIONS IN THE 5 TO 7 YEAR OLD - CROWDING, ROTATIONS, OVERBITE, AND OVERJET
 #27 Ortho-Tain, Inc. 1-800-541-6612 PREVENTING MALOCCLUSIONS IN THE 5 TO 7 YEAR OLD - CROWDING, ROTATIONS, OVERBITE, AND OVERJET Dr. Earl O. Bergersen A DESCRIPTION OF THE PREVENTIVE TECHNIQUE Preventing
#27 Ortho-Tain, Inc. 1-800-541-6612 PREVENTING MALOCCLUSIONS IN THE 5 TO 7 YEAR OLD - CROWDING, ROTATIONS, OVERBITE, AND OVERJET Dr. Earl O. Bergersen A DESCRIPTION OF THE PREVENTIVE TECHNIQUE Preventing
Treatment of Long face / Open bite
 In the name of GOD Treatment of Long face / Open bite in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 13 William R. Proffit, Henry W.
In the name of GOD Treatment of Long face / Open bite in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 13 William R. Proffit, Henry W.
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
A Clinical and Cephalometric Study of the Influence of Mandibular Third Molars on Mandibular Anterior Teeth
 10.5005/jp-journals-10021-1193 ORIGINAL ARTICLE Tara Ramprakash Kavra, Etika Kabra A Clinical and Cephalometric Study of the Influence of Mandibular Third Molars on Mandibular Anterior Teeth 1 Tara Ramprakash
10.5005/jp-journals-10021-1193 ORIGINAL ARTICLE Tara Ramprakash Kavra, Etika Kabra A Clinical and Cephalometric Study of the Influence of Mandibular Third Molars on Mandibular Anterior Teeth 1 Tara Ramprakash
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: orthodontics_for_pediatric_patients 2/2014 10/2017 10/2018 10/2017 Description of Procedure or Service Children
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: orthodontics_for_pediatric_patients 2/2014 10/2017 10/2018 10/2017 Description of Procedure or Service Children
IMPACTED CANINES. Unfortunately, this important tooth is the second most common tooth to be impacted after third molars
 IMPACTED CANINES After we talked about impacted third molars, today we ll discuss about maxillary impacted canines in upper dental arch, how to manage these cases as a dental surgeon. You will study about
IMPACTED CANINES After we talked about impacted third molars, today we ll discuss about maxillary impacted canines in upper dental arch, how to manage these cases as a dental surgeon. You will study about
Objectives. Discuss the physiology of tooth eruption. Identify the causes of anomalies associated with
 Eruption and eruption disorders Objectives Discuss the physiology of tooth eruption. Identify the causes of anomalies associated with Identify the causes of anomalies associated with tooth eruption. Introduction
Eruption and eruption disorders Objectives Discuss the physiology of tooth eruption. Identify the causes of anomalies associated with Identify the causes of anomalies associated with tooth eruption. Introduction
Early treatment. Interceptive orthodontics
 Early treatment Interceptive orthodontics Early treatment Some malocclusion can be prevented or intercepted. Diphasic treatment is sometimes considered more logical and sensible. During the phase one,
Early treatment Interceptive orthodontics Early treatment Some malocclusion can be prevented or intercepted. Diphasic treatment is sometimes considered more logical and sensible. During the phase one,
Postnatal Growth. The study of growth in growing children is for two reasons : -For health and nutrition assessment
 Growth of The Soft Tissues Postnatal Growth Postnatal growth is defined as the first 20 years of growth after birth krogman 1972 The study of growth in growing children is for two reasons : -For health
Growth of The Soft Tissues Postnatal Growth Postnatal growth is defined as the first 20 years of growth after birth krogman 1972 The study of growth in growing children is for two reasons : -For health
OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC
 Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Mixed Dentition Treatment and Habits Therapy
 Interception Mixed Dentition Treatment and Habits Therapy Anterior Crossbites Posterior Crossbites Interference s with Normal Eruption Habit Therapy Tsung-Ju Hsieh, DDS, MSD 1 2 Anterior Crossbites Anterior
Interception Mixed Dentition Treatment and Habits Therapy Anterior Crossbites Posterior Crossbites Interference s with Normal Eruption Habit Therapy Tsung-Ju Hsieh, DDS, MSD 1 2 Anterior Crossbites Anterior
Treatment of Angle Class III. Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor
 Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor Disorders in Angle Class III The position of the lower jaw is foreward regarding to the upper jaw Mesialocclusion
Department of Paedodontics and Orthodontics Dr. habil. Melinda Madléna associate professor Disorders in Angle Class III The position of the lower jaw is foreward regarding to the upper jaw Mesialocclusion
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD
 REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
Treatment Planning for the Loss of First Permanent Molars D.S. GILL, R.T. LEE AND C.J. TREDWIN
 O R T H O D O N T I C S Treatment Planning for the Loss of First Permanent Molars D.S. GILL, R.T. LEE AND C.J. TREDWIN Abstract: During the mixed-dentition stage of dental development, dentists may encounter
O R T H O D O N T I C S Treatment Planning for the Loss of First Permanent Molars D.S. GILL, R.T. LEE AND C.J. TREDWIN Abstract: During the mixed-dentition stage of dental development, dentists may encounter
AAO / AAPD Scottsdale 2018
 AAO / AAPD Scottsdale 2018 Missing Premolars : What are the Options? David Kennedy Clinical Professor UBC Vancouver Canada drdavidkennedy@yahoo.ca At what age can you know second premolars are absent?
AAO / AAPD Scottsdale 2018 Missing Premolars : What are the Options? David Kennedy Clinical Professor UBC Vancouver Canada drdavidkennedy@yahoo.ca At what age can you know second premolars are absent?
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
The Premolars. Chapter 17 Permanent Posterior Teeth (p )
") The Premolars Chapter 17 Permanent Posterior Teeth (p. 230-244) General Information Function: u Hold and grind food u Work with molars in mastication. u Even without molars one may be able to chew well
The Premolars Chapter 17 Permanent Posterior Teeth (p. 230-244) General Information Function: u Hold and grind food u Work with molars in mastication. u Even without molars one may be able to chew well
Upper arch. 1Prosthodontics. Dr.Bassam Ali Al-Turaihi. Basic anatomy & & landmark of denture & mouth
 1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
Alveolar Growth in Japanese Infants: A Comparison between Now and 40 Years ago
 Bull Tokyo Dent Coll (2017) 58(1): 9 18 Original Article doi:10.2209/tdcpublication.2016-0500 Alveolar Growth in Japanese Infants: A Comparison between Now and 40 Years ago Hiroki Imai 1), Tetsuhide Makiguchi
Bull Tokyo Dent Coll (2017) 58(1): 9 18 Original Article doi:10.2209/tdcpublication.2016-0500 Alveolar Growth in Japanese Infants: A Comparison between Now and 40 Years ago Hiroki Imai 1), Tetsuhide Makiguchi
Tooth eruption and movement
 Tooth eruption and movement Dr. Krisztián Nagy Diphydont dentition Deciduous dentition primary dentition Diphydont dentition Permanent dentition secondary dentition Mixed Dentition: Presence of both dentitions
Tooth eruption and movement Dr. Krisztián Nagy Diphydont dentition Deciduous dentition primary dentition Diphydont dentition Permanent dentition secondary dentition Mixed Dentition: Presence of both dentitions
Orthodontic treatment of midline diastema related to abnormal frenum attachment - A case series.
 Orthodontic treatment of midline diastema related to abnormal frenum attachment - A case series. Running title: Orthodontic treatment of midline diastema. Dr. Amit Dahiya 1, Dr. Minakshi Rana 2, Dr. Arun
Orthodontic treatment of midline diastema related to abnormal frenum attachment - A case series. Running title: Orthodontic treatment of midline diastema. Dr. Amit Dahiya 1, Dr. Minakshi Rana 2, Dr. Arun
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Tooth and Surface Identification (TID and SID)
") Tooth and Surface Identification (TID and SID) Dental treatment documentation and billing require to properly identify teeth and tooth surfaces. Incorrect TID and SID are frequent reasons for claim denial
Tooth and Surface Identification (TID and SID) Dental treatment documentation and billing require to properly identify teeth and tooth surfaces. Incorrect TID and SID are frequent reasons for claim denial
Clinical UM Guideline
 Clinical UM Guideline Subject: Non-Medically Necessary Orthodontia Care Guideline #: #08-002 Current Publish Date: 10/16/2017 Status: Reviewed Last Review Date: 10/11/2017 Description This document addresses
Clinical UM Guideline Subject: Non-Medically Necessary Orthodontia Care Guideline #: #08-002 Current Publish Date: 10/16/2017 Status: Reviewed Last Review Date: 10/11/2017 Description This document addresses
Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results.
 SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion.
 Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Problems of First Permanent Molars - The first group of permanent teeth erupt in the oral cavity. - Deep groove and pit
 Management of the poor first permanent e molar Assoc. Prof. Kadkao Vongsavan * Asst. Prof. Praphasri Rirattanapong* Dr. Pongsakorn Sakkamathya** ** * Department of Pediatric Dentistry Faculty of Dentistry,
Management of the poor first permanent e molar Assoc. Prof. Kadkao Vongsavan * Asst. Prof. Praphasri Rirattanapong* Dr. Pongsakorn Sakkamathya** ** * Department of Pediatric Dentistry Faculty of Dentistry,
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
Early Mixed Dentition Period
 REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
#39 Ortho-Tain, Inc
 1 #39 Ortho-Tain, Inc. 1-800-541-6612 OPTIMUM ORTHODONTICS FOR THE 5 TO 12 YEAR-OLD BY COMBINING REMOVABLE AND FIXED APPLIANCES WITH THE USE OF THE NITE-GUIDE AND OCCLUS-O-GUIDE APPLIANCES INTRODUCTION:
1 #39 Ortho-Tain, Inc. 1-800-541-6612 OPTIMUM ORTHODONTICS FOR THE 5 TO 12 YEAR-OLD BY COMBINING REMOVABLE AND FIXED APPLIANCES WITH THE USE OF THE NITE-GUIDE AND OCCLUS-O-GUIDE APPLIANCES INTRODUCTION:
Case Report n 2. Patient. Age: ANB 8 OJ 4.5 OB 5.5
 Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
You know you would like to stop swearing at the computer after each shot. Troubleshooting oral radiography
 You know you would like to stop swearing at the computer after each shot Troubleshooting oral radiography Goals of oral radiology Achieve diagnostic images of the teeth and surrounding bone. Images should
You know you would like to stop swearing at the computer after each shot Troubleshooting oral radiography Goals of oral radiology Achieve diagnostic images of the teeth and surrounding bone. Images should
NATIONAL EXAMINING BOARD FOR DENTAL NURSES
 NATIONAL EXAMINING BOARD FOR DENTAL NURSES NATIONAL DIPLOMA EXAMINATION DENTAL CHARTING NEBDN is a limited company registered in England & Wales No. 5580200 Registered with the Charity Commisioners No.
NATIONAL EXAMINING BOARD FOR DENTAL NURSES NATIONAL DIPLOMA EXAMINATION DENTAL CHARTING NEBDN is a limited company registered in England & Wales No. 5580200 Registered with the Charity Commisioners No.
Key points for starting off
 Key points for starting off First off, the five questions to ask yourself about a loose tooth before identifying it are: 1. 2. 3. 4. 5. Category (incisor, canine, premolar or molar)? Permanent or deciduous?
Key points for starting off First off, the five questions to ask yourself about a loose tooth before identifying it are: 1. 2. 3. 4. 5. Category (incisor, canine, premolar or molar)? Permanent or deciduous?
ADOLESCENT TREATMENT. Thomas J. Cangialosi. Stella S. Efstratiadis. CHAPTER 18 Pages CLASS II DIVISION 1 WHY NOW?
 ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
Buccally Malposed Mesially Angulated Maxillary Canine Management
 Buccally Malposed Mesially Angulated Maxillary Canine Management Suhad. H. Manhal,* Summery: Maxillary canine is an important tooth in all fields of dentistry. However, malposed upper canine is seemed
Buccally Malposed Mesially Angulated Maxillary Canine Management Suhad. H. Manhal,* Summery: Maxillary canine is an important tooth in all fields of dentistry. However, malposed upper canine is seemed
Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report
 Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Removable appliances
 Removable appliances Melinda Madléna DMD, PhD associate professor Department of Pedodontics and Orthodontics Faculty of Dentistry Semmelweis University Budapest Classification of the orthodontic anomalies
Removable appliances Melinda Madléna DMD, PhD associate professor Department of Pedodontics and Orthodontics Faculty of Dentistry Semmelweis University Budapest Classification of the orthodontic anomalies
ASSESSMENT OF MAXILLARY FIRST MOLAR ROTATION IN SKELETAL CLASS II, AND THEIR COMPARISON WITH CLASS I AND CLASS III SUBJECTS
 ORIGINAL ARTICLE ASSESSMENT OF MAXILLARY FIRST MOLAR ROTATION IN SKELETAL CLASS II, AND THEIR COMPARISON WITH CLASS I AND CLASS III SUBJECTS ABSTRACT FARHAT AMIN, BDS, MCPS, FCPS Mesial rotation of maxillary
ORIGINAL ARTICLE ASSESSMENT OF MAXILLARY FIRST MOLAR ROTATION IN SKELETAL CLASS II, AND THEIR COMPARISON WITH CLASS I AND CLASS III SUBJECTS ABSTRACT FARHAT AMIN, BDS, MCPS, FCPS Mesial rotation of maxillary
A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR
 Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
Short Communication International Journal of Dental and Health Sciences Volume 01,Issue 03 A SIMPLE METHOD FOR CORRECTION OF BUCCAL CROSSBITE OF MAXILLARY SECOND MOLAR Sumit Yadav 1,Davender Kumar 2,Achla
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
Permanent 2 nd Maxillary Molars
 Permanent 2 nd Maxillary Molars In comparison to the first max molar First molars appears in the oral cavity at the age of 6 years old.. While 2 nd molar 3 rd molar Max. 2 nd molar have long roots (sometimes
Permanent 2 nd Maxillary Molars In comparison to the first max molar First molars appears in the oral cavity at the age of 6 years old.. While 2 nd molar 3 rd molar Max. 2 nd molar have long roots (sometimes
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Research methodology University of Turku, Finland
 Research methodology Prospective, controlled cohort study started in 1998 Treatment group: 167 children Treatment with eruption guidance appliance only Control group: 104 children No Keski-Nisula K; Keski-Nisula
Research methodology Prospective, controlled cohort study started in 1998 Treatment group: 167 children Treatment with eruption guidance appliance only Control group: 104 children No Keski-Nisula K; Keski-Nisula
The six keys to normal occlusion
 The six keys to normal occlusion Lawrence F. Andrews, D.D.S. San Diego, Calif. This article will discuss six significant characteristics observed in a study of 120 casts of nonorthodontic patients with
The six keys to normal occlusion Lawrence F. Andrews, D.D.S. San Diego, Calif. This article will discuss six significant characteristics observed in a study of 120 casts of nonorthodontic patients with
Effect of the lower third molars on the lower dental arch crowding Šidlauskas Antanas, Trakinienė Giedrė
 Stomatologija, Baltic Dental and illofacial Journal, 8:80-4, 2006 Effect of the lower third molars on the lower dental arch crowding Šidlauskas Antanas, Trakinienė Giedrė SUMMARY Increasing lower dental
Stomatologija, Baltic Dental and illofacial Journal, 8:80-4, 2006 Effect of the lower third molars on the lower dental arch crowding Šidlauskas Antanas, Trakinienė Giedrė SUMMARY Increasing lower dental
DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA. Dr Muhammad Rizwan Memon FCPS Assistant Professor
 DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor Crest of Residual Ridge Buccal Shelf Shape of supporting structure Mylohyoid Ridge
DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor Crest of Residual Ridge Buccal Shelf Shape of supporting structure Mylohyoid Ridge
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class III malocclusion occurs in less than 5%
 CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique
 Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
ALABAMA DENTAL HYGIENE PROGRAM 50 QUESTIONS PRE ENTRANCE EXAM
 ALABAMA DENTAL HYGIENE PROGRAM 50 QUESTIONS PRE ENTRANCE EXAM NAME DATE RETURN COMPLETED EXAM WITH APPLICATION You may copy for future reference 1. One cause of decay is the Streptococcus mutans bacteria
ALABAMA DENTAL HYGIENE PROGRAM 50 QUESTIONS PRE ENTRANCE EXAM NAME DATE RETURN COMPLETED EXAM WITH APPLICATION You may copy for future reference 1. One cause of decay is the Streptococcus mutans bacteria
Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm.
 Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics
 Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Interdisciplinary management of Impacted teeth in an adult with Orthodontics & Free Gingival graft : A Case Report
 Original article: Interdisciplinary management of Impacted teeth in an adult with Orthodontics & Free Gingival graft : A Case Report Dr Renuka Patel, Dr Falguni Mehta, Dr. Ashish Pandey Assistant Professor,
Original article: Interdisciplinary management of Impacted teeth in an adult with Orthodontics & Free Gingival graft : A Case Report Dr Renuka Patel, Dr Falguni Mehta, Dr. Ashish Pandey Assistant Professor,
ORAL ANATOMY AND PHYSIOLOGY
 CHAPTER 7 ORAL ANATOMY AND PHYSIOLOGY INTRODUCTION This chapter covers the oral anatomy and physiology of the teeth, the histology of the tissues and supporting structures, and concentrates on the external
CHAPTER 7 ORAL ANATOMY AND PHYSIOLOGY INTRODUCTION This chapter covers the oral anatomy and physiology of the teeth, the histology of the tissues and supporting structures, and concentrates on the external
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
6. Timing for orthodontic force
 6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
You. Fix. Could. This? Treatment solutions for typical and atypical adult relapse. 78 SEPTEMBER 2017 // orthotown.com
 by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
Medical NBDE-II. Dental Board Exams Part I.
 Medical NBDE-II Dental Board Exams Part I http://killexams.com/exam-detail/nbde-ii Question: 149 Anatomically, the term "clinical root" can be defined as which of the following: A. The space in the tooth
Medical NBDE-II Dental Board Exams Part I http://killexams.com/exam-detail/nbde-ii Question: 149 Anatomically, the term "clinical root" can be defined as which of the following: A. The space in the tooth
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Advanced Probing Techniques
 Module 21 Advanced Probing Techniques MODULE OVERVIEW The clinical periodontal assessment is one of the most important functions performed by dental hygienists. This module begins with a review of the
Module 21 Advanced Probing Techniques MODULE OVERVIEW The clinical periodontal assessment is one of the most important functions performed by dental hygienists. This module begins with a review of the
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1*
 UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
Oral Embryology and Histology
 Oral Embryology and Histology Chapter 8 Copyright 2018, Elsevier Inc. All Rights Reserved. 1 Learning Objectives Lesson 8.1: Oral Embryology 1. Pronounce, define, and spell the key terms. 2. Define embryology
Oral Embryology and Histology Chapter 8 Copyright 2018, Elsevier Inc. All Rights Reserved. 1 Learning Objectives Lesson 8.1: Oral Embryology 1. Pronounce, define, and spell the key terms. 2. Define embryology
Plaque and Occlusion in Periodontal Disease Wednesday, February 25, :54 AM
 Plaque and Occlusion in Periodontal Disease Wednesday, February 25, 2015 9:54 AM 1. The definition of Trauma From Occlusion: Primary TFO, Secondary TFO, and Combined TFO 2. Clinical and Radiographic signs
Plaque and Occlusion in Periodontal Disease Wednesday, February 25, 2015 9:54 AM 1. The definition of Trauma From Occlusion: Primary TFO, Secondary TFO, and Combined TFO 2. Clinical and Radiographic signs