THE NORTH, SOUTH, EAST AND WEST OF OCCLUSION. Dr Tom Bereznicki BDS (Edin)
|
|
|
- Jerome Goodman
- 5 years ago
- Views:
Transcription
1 THE NORTH, SOUTH, EAST AND WEST OF OCCLUSION Dr Tom Bereznicki BDS (Edin)
2 At one end of the spectrum are dentists who believe that they can go through their working lives with scant regard for their patient s occlusion. They seem to believe that essentially they can conduct their practice ignoring the occlusal consequences of the treatment that they perform daily. This is bizarre given the fact that very few dental treatments do not involve the occlusal surfaces of teeth Conversely there is a body of opinion that considers occlusion to be such a central pillar in our working lives and to be of such systemic import to the well-being of our patients, that occlusion takes on an almost mystic importance and attracts cult-like devotion. This can lead some dentists to advocate occlusion as being the key to resolving or preventing a range of disorders far removed from the masticating re-system, for example prolapsed lumbar discs. The danger is that both of these approaches lead to inappropriate levels patient care; patients suffer through either over or under treatment. S Davies et al
3 It is a common criticism of dentists that our dental schools ignore the third part of the masticatory system, the articulatory system, in their teaching. It appears that dentists feel that their time at university did not prepare them adequately in this area The inescapable fact that almost all dental treatment has an occlusal consequence, it is wrong to consider the study of the articulatory system to be less important than either of the teeth of the periodontal tissues No practising dentist can care well for their patients without having regard for good occlusal practice S Davies et al

4





5

6



7

8



9 NON-WORKING SIDE INTERFERENCE

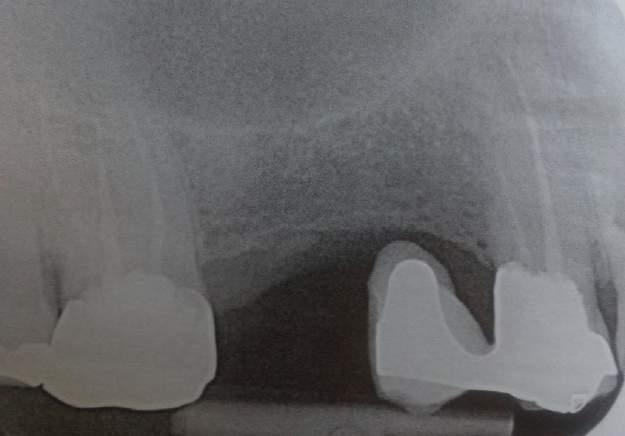
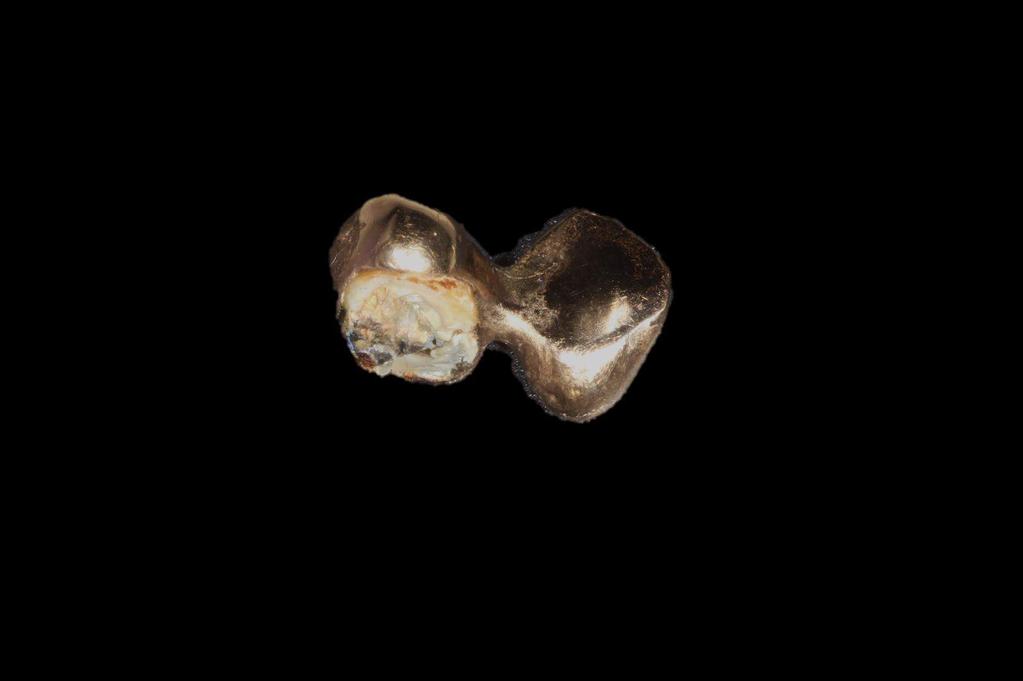
10 EXTRACTION ALLOWS THE DEVELOPMENT OF PROPER GROUP FUNCTION TO PROTECT THE CANINE WHICH IS ROOT TREATED AND HAS A METL POST



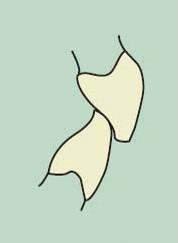
11 OCCLUSAL DETERIORATION STAGE 1 THE INITIAL LOSS OF OCCLUSAL HARMONY RESULTS IN THE LOWER DISTO-BUCCAL CUSP OF THE LAST STANDING LOWER MOLAR DRIVING INTO THE CONTACT POINT BETWEEN THE TWO UPPER MOLARS AND ACTING LIKE A WEDGE. THE UPPER LAST MOLAR IS SLOWLY PUSHED DISTALLY, MOBILITY INCREASES AND EVENTUALLY IT IS LOST SPONTANEOUSLY



12 OCCLUSAL DETERIORATION STAGE 2 THE SAME PROCESS NOW BEGINS WITH THE UPPER MOLAR PALATAL CUSP DRIVING INTO THE INTERPROXIMAL CONTACT BETWEEN THE TWO LOWER MOLARS. EVENTUALLY, THE LAST LOWER MOLAR BECOMES SO LOOSE IT HAS TO BE EXTRACTED
13 BASIC PRINCIPLES In normal occlusions Centric Relation (CR) should be coincident with maximum Intercuspation (ICP) -??? In lateral jaw excursions there should ideally be Canine Guidance or Group Function with or without Canine Guidance With the lower jaw in Working Side (WS) there should be no contacts on the Non- Working Side (NWS) In protrusive jaw movements all the contacts should be on the anterior teeth with no contacts on the posterior teeth Any undesirable contacts are known as premature contacts or prematurities in centric and interferences if in lateral and protrusive excursions Ideally there should be Anterior Guidance also known as a Anterior Protected Occlusion
14 Most responses to occlusal disharmony are adaptive in nature The possibility of converting a patient with a symptom free adapting occlusion to one which is uncomfortable because of high fillings increases with the number and complexity of the restorations - moreover the response varies between individuals M Wise
15 CENTRIC
16 WHERE SHOULD THE CONDYLES BE? Courtesy of Michael Wise

17 CENTRIC PREMATURITIES A centric occlusal interference often occurs during mandibular closure between maxillary mesial-facing cusp inclines and mandibular distal-facing cusp inclines. As a result the mandible is deflected anteriorly and possibly also laterally Fundamentals of Fixed Prosthodontics Shillingborg/Hobo/Whitsett
18 Centric occlusion can be described as the occlusion the patient makes when they fit their teeth together in maximum intercuspation. Common synonyms for this are Intercuspation Position (ICP) or Habitual Bite Centric Relation is not an occlusion at all. CR is nothing to do with teeth because it is the only centric that is reproducible with or without teeth present. It can be paraphrased as being the uppermost and foremost position of the mandible relative to the maxilla, with the articular disc in place, when the muscles that support the mandible are their most relaxed and least constrained position. The head of the condyle is thus in its terminal hinge position. It is a reproducible position if registered correctly it would be the same even if different dentists were involved in the recordings S Davies et al
19 WHERE SHOULD THE CONDYLE BE IN CENTRIC? THE IMPORTANT THING ABOUT CENTRIC IS THAT IT IS REPRODUCABLE BY ANYONE IN RCP THE CONDYLE IS POSITIONED SUPERIORLY WITH THIS ANTERIOR SURFACE SEATED BY WAY OF THE DISC AGAINST THE POSTERIOR FACING SLOPE OF THE EMINENCE M Wise THERE ARE MANY TECHNIQUES TO FIND THIS HINGE AXIS SEE ARTICLES ICP - THE RELATIONSHIP OF THE MANDIBLE TO THE MAXILLA WHEN THE TEETH ARE MESHED MAXIMALLY TOGETHER M Wise RCP - THE POINT OF INITIAL OCCLUSAL CONTACT THAT HAS OCCURED FOLLOWING CLOSURE IN RETRUDED ARC OF CLOSURE M Wise IN 80%+ OF PATIENTS ICP WILL BE APPROXIMATELY 1 MM ANTERIOR TO RCP M Wise
20 DO WE NEED TEETH TO FIND CENTRIC?
21 SHOULD RCP = ICP?

22 THE PERFECT BITE? ICP MAY BE UP TO 1mm ANTERIOR TO RCP
23 THE CONCEPT KNOWN AS LONG CENTRIC DOES IT MATTER IF CR AND ICP ARE NOT COINCIDENT? NO! BUT ONLY IF THERE ARE NUMEROUS EVEN CONTACTS BETWEEN THE UPPER AND LOWER TEETH The concept of allowing some freedom of movement in an anterior and posterior direction is known as long centric. Long centric is mm of free space between CR position and maximum intercuspation without a change in the vertical dimension of occlusion. In some advanced cases where the upper anterior teeth are being restored, if the centric contacts provided on the palatal surfaces of the crowns are in CR the patient will feel locked and uncomfortable. The long centric needs to be re-established by extending the centric stops on the palatal surfaces of the restored anterior teeth to allow the freedom of movement the patient requires to feel comfortable.

24 Figs (a) SHOW NORMAL OCCLUSAL CONTACTS, Figs (b) SHOW THE FREEDOM PATIENTS REQUIRE IN LONG CENTRIC
25 PARTICULARLY IF RESTORING UPPER ANTERIOR TEETH WITH CROWNS OR DENTURES, IT IS EASY TO LOCK THE PATIENT INTO RCP AND DENY THEM THE FREEDOM THAT THEY WERE USED TO PREVIOUSLY WHEN THEY HAD LONG-CENTRIC. THE PATIENT WILL FEEL INCREDIBLY UNCOMFORTABLE AND FEEL LOCKED. THE NEWLY PLACED ANTERIOR RESTORATIONS WILL REQUIRE ADJUSTMENT TO RE-INTRODUCE THE FREEDOM OF MOVEMENT THAT THE PATIENT WAS USED TO. THIS IS EASIEST TO ACHIEVE BY GETTING THE PATIENT TO SIT UP AND TAP ON ARTICULATING PAPER
26 CENTRIC/INTERCUSPAL CONFORMATIVE V REORGANISED


27 ARE ICP AND RCP COINCIDENT HERE?


28 A DIFFICULT PHOTO TO TAKE BUT THE FIRST CONTACT POINT IS ON THE PALATAL EDGE OF UL3 AND THEN ON SQUEEZING THE TEETH TOGETHER THERE IS A SLIDE LATERALLY LEFT TO ICP WITHIN THE FOSSA


29 THE CLINICAL OCCLUSAL PICTURE IS CONFIRMED BY FACEBOW MOUNTING STUDY MODELS ON A SEMI-ADJUSTABLE ARTICULATOR. RESTORATIONS HAVE TO BE PROVIDED IN THIS CENTRIC OCCLUSAL RELATIONSHIP NOT IN INTERCUSPAL ie THE TREATMENT IS CARRIED OUT AS A RE-ORGANISED CASE AND CANNOT BE RESTORED IN CONFORMATORY FASHION



30 AND HERE?
31 THE PATIENT COMING INTO RCP IN THE HING AXIS ARC OF CLOSURE


32 THE INITIAL POINT OF CONTACT IN THE CENTRIC ARC OF CLOSURE IS SHOWN ON THE ARTICULATED STUDY MODELS. BY REORGANISING THE OCCLUSION AND WORKING TO SUFFICIENT VERTICAL HEIGHT IS ACHIEVED TO ALLOW ROOM FOR THE RESTORATIVE MATERIAL


33 THE PATIENT CANNOT POSSIBLY BE RESTORED PREDICTABLY UNLESS THE TREATMENT IS CARRIED OUT AND REORGANISED IN RCP

34 OVERERUPTED WISDOME TEETH ARE A COMMON CAUSE OF CENTRIC PREMATURITIES


35 WHEN YOU SEE TILTED MOLARS IN THE POSTERIOR QUADRANT, THERE ARE OFTEN CENTIC PREMATURITIES IN THE AREA
36 WHEN THERE IS FOOD PACKING BETWEEN THE LAST TWO STANDING MOLARS, BUT THERE IS A TIGHT CONTACT WHEN FLOSS IS PASSED THROUGH THE CONTACT AREA, IT MEANS THERE MAY BE A CENTRIC PREMATURITY - THIS OPENS THE GAP BETWEEN THE TWO LAST TEETH AS THE PATIENT CLOSES HIS TEETH TOGETHER ALLOWING FOOD TO PACK. THE GAP CLOSES AS SOON AS THE PATIENT OPENS HIS MOUTH
37 TOOTH POSITION IS DICTATED BY THE NEUTRAL ZONE

38 IN THE PRESENCE OF PERIODONTAL DISEASE, OCCLUSAL FORCES, DUE TO LOSS OF VERTICAL DIMENSION IN THE POSTERIOR SEGMENTS, CAN RESULT IN THE FRONT TEETH MIGRATING AS WELL AS SUFFER ACCELERATING BONE LOSS SPLAYING. A LARGE CENTRIC PREMATURITY WILL CAUSE THE SAME PROBLEM



39 A DIASTEMA THAT APPEARED IN A MATTER OF WEEKS SHOWING SPONTANEOUS CLOSURE IN ONE WEEK FOLLOWING OCCLUSAL ADJUSTMENT. ONLY THE PREMATURE CONTACT BETWEEN THE LOWER MOLAR AND THE OVERERUPTED UPPER SECOND MOLAR WAS REMOVED.

40 THIS DIASTEMA APPEARED OVER A PERIOD OF SEVERAL MONTHS. THE UNDERLYING BONE LOSS WAS LONGSTANDING AND PERIODONTAL CONDITION STABLE. A LOSS OF VERTICAL DIMENSION FOLLOWING OCCLUSAL WEAR/ EROSION WAS DIAGNOSED

41 SPONTANEOUS SPACE CLOSURE IN 2 MONTHS FOLLOWING OCCLUSAL ADJUSTMENT OF PREMATURITIES IN CENTRIC AND RELEIVING THE HIGH OCCLUSAL FORCES ON THE UPPER ANTERIOR TEETH BY RE-SHAPING THE PALATAL SURFACES AND/OR THE INCISAL EDGES OF LOWER INCISORS


42 2008 NEW VENEERS



43 2016 PATIENT PRESENTS WITH TWO DIASTEMAS THAT HAD RECENTLY APPEARED




44 2 WEEKS POST OCCLUSAL ADJUSTMENT OF CENTRIC PREMATURIES IN THE POSTERIOR QUADRANTS

45 STABILITY AND TOTAL CLOSURE 6 MONTHS LATER


46 SIMPLY RE-ARRANGING THE OCCLUSION CAN LEAD TO SPONTANEOUS RESOLUTION OF TOOTH MAL-ALIGNMENT THE PATIENT S IMMEDIATE UPPER DENTURE WAS FABRICATED WITH AN INCREASED VERTICAL DIMENSION TO ALLOW THE ESTABLISHMENT OF A NORMAL CLASS 1 ANTERIOR RELATIONSHIP THE LOWER ANTERIOR TEETH RE-ALIGNED SPONTANEOUSLY WITHIN 2 MONTHS. THE FINAL RESTORATION IS AN ACRYLIC/TITANIUM SCREW-RETAINED FULL ARCH BRIDGE
47 Working Side Interference Infers a heavy or early occlusal contact towards the back of the mouth during an excursive movement S Davies et al


48 THE MECHANICS OF OCCLUSION CAN BE COMPARED TO A NUTCRACKER


49 FORCES IN BRUXING CAN BE 10X THAT DURING NORMAL FUNCTION AND GO UP TO BETEWEEN 300 AND 900 psi 8X 5X 1X


50 CANINE RISE


51 IDEALLY THERE SHOULD BE A PROGRESSIVE SMOOTH TRANSLATION FROM THE CANINE TO THE LATERAL TO THE CENTRAL INCISOR

52 GROUP FUNCTION IF CANINE GUIDANCE IS NOT POSSIBLE, GROUP FUNCTION SHOULD BE PRESENT, IDEALLY INCLUDING SOME CANINE GUIDANCE. THE TOOTH CONTACTS SHOULD BE AS ANTERIORLY PLACED AS POSSIBLE OR EVENLY DISTRIBUTED BETWEEN ALL THE TEETH AS SHOWN BELOW
53 AS SOON AS THERE ARE ANY LATERAL EXCURSIONS OF THE LOWER JAW, OCCLUSAL CONTACTS SHOULD PASS TO THE FRONT TEETH, IDEALLY IN CANINE GUIDANCE OR IN GROUP FUNCTION IN ORDER TO PROTECT THE POSTERIOR TEETH FROM LATERAL FORCES

54 WHAT WOULD ONE EXPECT HERE?

55 IS THIS GROUP FUNCTION? WOULD YOU REGARD IT AS BEING POSSIBLE CAUSE OF FUTURE PATHOLOGY?
56 CROSS-OVER IN WORKING SIDE Dawson Academy 2009 Why Porcelain Breaks and Chips CORRECT CROSSOVER DISCLUSION IT IS NOT BY CHANCE THAT THE MOST COMMON ANTERIOR AESTHETIC FRACTURE IS TO THE MAXILLARY LATERAL INCISOR. PROPER OCCLUSAL DESIGN DICTATES A SMOOTH TRANSITION TO THE INCISAL EDGE OF THE MAXILLARY CENTRALS AS THE PATIENT MOVES BEYOND THE CANINE IN LATERAL EXCURSION. WHEN THIS POSITIONING IS OVERLOOKED, EXCESSIVE LOADS CAN BE PLACED ON THE DISTAL OF THE LATERAL INCISORS LEADING TO FRACTURE.

57 BE AWARE OF WORKING SIDE LINGUAL CUSP INTERFERENCE THE EXCURSION SHOULD TRAVEL SMOOTHLY FROM THE CANINE TO THE INCISORS AND NOT CATCH IN THE MOLAR AREAS IN EXTREME MOVEMENT BEYOND THE CANINE A working side interference occurs between maxillary palatal facing cusp inclines and mandibular buccal facing cusp inclines of the lingual on the working side Fundamentals of Fixed Prosthodontics Shillingborg/Hobo/Whitsett
58 CORRECT LATERAL GUIDANCE When the mandible moves laterally, the goal is to have immediate disclusion of the posterior teeth on the working and balancing side. When posterior teeth are allowed to contact in excursive movements, increased muscle activity, combined with the increased mechanical stress contributes to the increased chance of fracture. Creating the correct contour and the lingual of the maxillary canines is one of the most important decisions a clinician makes during the restorative process. If the cusp is too steep for the patient s functional pattern fracture, mobility and migration is likely. Dawson Academy 2009 Why Porcelain Breaks and Chips
59 NORMAL ANTERIOR CROSS-OVER THE PROGRESSION OF THE EXCURSION SHOULD PASS SMOOTHLY FROM CANINE TO LATERAL TO CENTRAL INCISOR AND STAY ON THE ANTERIOR TEETH UNTIL THE PATIENT CANNOT GO FURTHER LATERALLY

60 FITTED CROWN IS COMFORTABLE IN ICP


61 THE BUCCAL CUSPS ARE TOO LONG AND PRODUCE INTERFERENCES IN BOTH WORKINGSIDE AND PROTRUSIVE MANDIBULAR EXCURSIONS THE PROBABLE REASON FOR FRACTURE OF THE BUCCAL CUSPS AND NEED FOR A CROWN LOOK AT THE FRACTURE LINES ON THE LOWER OPPOSING TOOTH Working-side Protrusive

62 IF THE CUSPS ARE NOT ADJUSTED TO ELIMINATE THE INTERFERENCE, THE RESULTANT HEAVY PRESSURES FREQUENTLY LEAD TO PORCELAIN FRACTURE



63 OR PAIN AND ASSOCIATED TMJ PROBLEMS
64 CROSS-OVER IN WORKING SIDE Dawson Academy 2009 Why Porcelain Breaks and Chips CORRECT CROSSOVER DISCLUSION IT IS NOT BY CHANCE THAT THE MOST COMMON ANTERIOR AESTHETIC FRACTURE IS TO THE MAXILLARY LATERAL INCISOR. PROPER OCCLUSAL DESIGN DICTATES A SMOOTH TRANSITION TO THE INCISAL EDGE OF THE MAXILLARY CENTRALS AS THE PATIENT MOVES BEYOND THE CANINE IN LATERAL EXCURSION. WHEN THIS POSITIONING IS OVERLOOKED, EXCESSIVE LOADS CAN BE PLACED ON THE DISTAL OF THE LATERAL INCISORS LEADING TO FRACTURE.

65 THE PONTIC FRACTURED AS THERE WAS AN ABSENCE OF SMOOTH PROGRESSION FROM THE CANINE TO THE LATERAL TO THE CENTRAL INCISOR MOST OF THE PRESSURE WAS ON THE DISTAL CORNER OF THE LATERAL INCISOR LEADING TO PORCELAIN FRACTURE

66 ANTERIOR CROSS-OVER THE PROGRESSION OF THE EXCURSION SHOULD PASS SMOOTHLY FROM CANINE TO LATERAL TO CENTRAL INCISOR

67 WORKING-SIDE CROSSOVER SHOWN IN A SERIES OF SLIDES UNTIL THE INTERFERENCES APPEAR ON THE LINGUAL CUPS OF THE PREMOLARS AND ANTERIOR GUIDANCE LOST

68

69

70
71

72

73

74 LINGUAL CUSP HEIGHT OF BOTH PREMOLARS ADJUSTED TO BRING THE ANTERIOR GUIDANCE INTO CONTACT ON THE CENTRAL INCISORS

75 ANTERIOR GUIDANCE RE-ESTABLISHED

76 BEFORE AND AFTER OCCLUSAL ADJUSTMENT BY REDUCTION OF THE LINGUAL CUSPS ANTERIOR DISCLUSION RE-INTRODUCED


77 PLEASE DON T SAY YOU CANNOT IMAGINE ANYONE PUTTING THEIR JAW INTO THIS EXTREME POSITION IN REAL LIFE!!

78


79 ANTERIOR CROSS-OVER AS THE PATIENT MOVES INTO WORKING SIDE ANTERIOR DISCLUSION APPEARS BECAUSE THE LL6 LINGUAL CUSP GIVES A WORKING SIDE INTERFERENCE THIS IS THE COMMON CAUSE OF FRACTURED LINGUAL CUSPS IN THE MOLAR AREA HIGH LINGUAL CUSP ANTERIOR DISCLUSION


80 LOWER LINGUAL CUSPS WHICH BECOME WORKING SIDE INTERFERENCES CAN BE CONFIDENTLY RE-SHAPED AS LONG AS THE TEETH ARE NOT IN A CROSS-BITE. IN A CROSS- BITE THE UPPER BUCCAL AND LOWER LINGUAL CUSPS BECOME THE CENTRIC HOLDING CUSPS AND MUST NEVER BE ADJUSTED
81 Non-Working Side Interference Is an anterior guidance on the back teeth of the non-working side during lateral excursions S Davies et al

82 NON-WORKING SIDE INTERFERENCES ARE MOST OFTEN ASSOCIATED CLINICALLY WITH CUSPAL FRACTURE AND TMJ PROBLEMS, AS WELL AS CONTRIBUTING TO INCREASING TOOTH MOBILITY AND BONE LOSS IN PERIODONTAL CASES A non-working side interference results when there is contact between maxillary buccal-facing cusp inclines and mandibular lingual-facing cusp inclines on the non-working side Fundamentals of Fixed Prosthodontics Shillingborg/Hobo/Whitsett
83

84


85 IN A CROSS BITE THE HOLDING CUSPS ARE THE BUCCAL UPPERS AND LOWER LINGUALS
86 PROTRUSIVE There are three forms of protrusive: Edge to edge Protrusive with anterior disclusion and posterior contacts Protrusive with crossover

87 PROTRUSIVE INTERFERENCES A protrusive interference occurs when distal-facing inclines of maxillary posterior teeth contact the mesial-facing inclines of mandibular posterior teeth during a protrusive movement Fundamentals of Fixed Prosthodontics Shillingborg/Hobo/Whitsett
88 Edge to edge with posterior disclusion

89 USUALLY ONLY RESULTS IN ANTERIOR WEAR

90 AVOID INTRODUCING PROTRUSIVE CONTACTS WITH INCORRECTLY SHAPED RESTORATIONS





91 PROTRUSIVE WITH ANTERIOR DISCLUSION AND ONLY CONTACTS IN THE POSTERIOR QUADRANTS IDEALLY THESE SHOULD BE BILATERAL VERY DIFFICULT CASES WHEN PROVIDING CROWNS IN THESE EXTREME PROTRUSIVE CASES


92 IN THE PRESENCE OF PERIODONTAL DISEASE THIS TYPE OF HEAVY PROTRUSIVE CONTACT PROSTERIORLY LEADS TO RAPIDLY PROGRESSING BONE LOSS. IN A NORMAL HEALTHY MOUTH, IN ALL PROBABILITY, MULTIPLE CUSP FRACTURES WILL BE SEEN RATHER THAN BONE LOSS

93 TYPICAL ADVANCED BONE LOSS PATTERNS IN THE POSTERIOR SEGMENTS WHERE THERE IS A LOSS OF ANTERIOR GUIDANCE BY CONTACTS AT THE BACK OF THE MOUTH


94 TOOTH FRACTURE SEEN IN CASES WHERE THE ANTERIOR GUIDANCE IS LOST



95 TYPICAL RADIOGRAPHIC APPEARANCE OF OCCLUSIONS WHICH ARE LIKELY TO HAVE PROTRUSIVE INTERFERENCES

96 PROTRUSIVE WITH ANTERIOR CROSSOVER
97 IS ANTERIOR CROSSOVER THE CAUSE OF LOWER FIXED RETAINERS DE-BONDING?



98

99 PLACED 1986 AND STILL SUCCESSFUL

100




101 IN PROTRUSIVE CROSS-OVER AS MANY TEETH AS POSSIBLE SHOULD CONTACT TO REDUCE THE PRESSURE ON ANY ONE SPOT. IF THE PATIENT CAN ADVANCE WELL BEYOND THE CROSOVER, CONTACTS SHOULD STILL BE AS FAR FORWARD AS POSSIBLE IDEALLY NO FURTHER THAN THE CANINES

102 TYPICAL PORCELAIN FRACTURE CAUSED BY ANTERIOR CROSSOVER
103


104 COSMETIC BONDING THE PATIENT PRESENTS WITH FAILED COSMETIC BONDING OF THE CANINE TEETH WHICH ARE IN THE POSITON OF THE CONGENITALLY ABSENT LATERAL INCISORS centric


105 Working-side anterior disclusion Protrusive with crossover


106 COSMETICALLY BONDING THE LATERALS IS DOOMED TO FAILURE WITH THIS OCCLUSION


107 IF COSMETIC COMPOSITE BONDING IS TO GO AHEAD, THE LOWER CANINE TIPS NEED TO BE SHORTENED, WITH THE PATIENTS PERMISSION, IF A PREDICATABLE LASTING RESULT IS TO BE ACHIEVED
108 WHAT ARE THE IMPLICATIONS OF OCCLUSION IN THE PROVISION OF TREATMENT?
109 DIAGNOSIS

110



111


112


113 FORCES ON POSTERIOR TEETH IN NORMAL FUNCTION VARY FROM 5 TO 44 psi WHEREAS IN PARAFUNCTION THEY RANGE FROM 300 TO 900 psi FRACTURE LINE EXTENT OF FRACTURE LINGUAL CUSP WEAR FACET

114 LEARN TO LOOK AND ANALYSE THE FRACTURE THROUGH THE MESIAL RIDGE IS EASY TO SPOT. DO YOU SEE ANYTHING ELSE? LINGUAL BUCCAL
115 THERE IS A WEAR FACET PRESENT ON THE MESIO- LINGUAL CUSP WHICH HAS MORE THAN LIKELY CONTRIBUTED TO THE CAUSE OF THE FRACTURE. MERELY RE-FILLING THE TOOTH WITHOUT ELIMINATING THE OCCLUSAL INTERFERENCE WILL NOT PREVENT PROPAGATION OF A DEEPER PULPAL FLOOR OR CUSPAL FRACTURE WEAR FACET



116 RESTORED TEETH ARE PARTICULARLY SUSCEPTIBLE TO FRACTURE DUE TO OCCLUSAL FORCES FILLINGS WEAKEN TEETH, THEY DO NOT STRENGTHEN THEM - AMALGAM NOT AT ALL, BONDED COMPOSITES ONLY TO A CERTAIN EXTENT


117 A TYPICAL PICTURE IN BRUXERS WITH LITTLE ANTERIOR GUIDANCE. APART FROM THE OBVIOUS FRACTURES, THERE IS ALSO A WORN AMALGAM. IF THE OPPOSING PLUNGER CUSP IS NOT RE- SHAPED, THE OCCLUSAL FLOOR OF THE TOOTH BEING FILLED WILL NEED TO BE DEEPENED (ie HEALTHY TOOTH TISSUE REMOVED) TO GIVE AN ADEQUATE THICKNESS OF RESTORATIVE MATERIAL. THIS DEEPENING OF THE CAVITY WILL FURTHER WEAKEN THE TOOTH AND THE WEDGING EFFECT OF THE NEW CUSP/FOSSA RELATIONSHIP WILL ADD FURTHER STRESS TO THE LOWER TOOTH
118


119 LEARN TO LOOK AT ABNORMAL OCCLUSAL LINES ESPECIALLY WHERE TEETH HAVE OVER-ERUPTED LARGE PROTRUSIVE INTERFERENCE WITH RESULTANT ANTERIOR DISCLUSION

120 Diagram copied from Mike Wise article series IN PFM S OR ANY OTHER PORCELAIN CROWN, PANCAKE OCCLUSAL REDUCTIONS AND FAILURE TO REDUCE THE BUCCAL ASPECT, AS SHOWN, LEADS TO EITHER VERY THIN PORCELAIN WHICH FRACTURES, OR POOR AESTHETICS AS THERE IS INSUFFICIENT DEPTH OF PORCELAIN FOR THE TECHNICIAN TO COVER THE OPAQUER. ALTERNATIVELY, THE CROWN IS OVERCONTOURED REDUCTION TO ACCOMMODATE THE OCCLUSION RUNS THE RISK OF EXPOSING THE METAL SUBSTRUCTURE AND IF CEMENTED HIGH OCCLUSAL TRAUMA TO THE TOOTH, PAIN USUALLY WITH COLD AND PRESSURE, INCREASED MOBILITY. IF THE PORCELAIN FRACTURES WHO PAYS FOR THE REMAKE??

121 THIS PATIENT PRESENTED WITH PAIN IN RELATION TO LR6 HOT COLD AND PRESSURE. IN ADDITION SHE HAD DEVELOPED EARACHE ON THE RIGHT AND WAS FINDING IF DIFFICULT TO OPEN HER MOUTH

122 THE BUCCAL CUSPS LR6 HAVE BEEN OVERBUILT BY THE TECHNICIAN AND A WORKING SIDE INTERFERENCE CREATED WITH LOSS OF ANTERIOR DISCLUSION. THE ONLY VIABLE TREATMENT WAS?

123 THE ONLY VIABLE TREATMENT WAS ADJUSTMENT OF THE CROWN. THE UPPER BUCCAL CUSP COULD NOT BE REDUCED AS IT WAS THE HOLDING CUSP IN A CROSSBITE. THE PATIENT WAS WARNED THAT PERFORATION AND/OR PORCELAIN FRACTURE OF THE CROWN WAS A POSSIBILITY DURING ADJUSTMENT OF THE LOWER BUCCAL CUSP IN WHICH CASE IT WOULD REQUIRE REPLACEMENT

124 FORTUNATELY DESPITE BEING UNDER-PREPARED, THE CROWN WAS NOT PERFORATED DURING RE-SHAPING. BEING A NON-WORKING CUSP THE REDUCTION DID NOT NEED TO BE TOO SCIENTIFIC IN ORDER TO RE-ESTABLISH ANTERIOR GUIDANCE. THE PATIENTS SYMPTOMS ALL DISAPPEARED WITHIN A WEEK
125 ENDODONTICS


126 TEETH UNDERGOING ROOT CANAL THERAPY SHOULD ROUTINELY BE RELEIVED OF THE BITE TO PREVENT INADVERTANT CUSPAL FRACTURE DURING TREATMENT AND PROVIDED WITH CUSPAL COVERAGE RESTORATIONS AFTER



127 BEWARE OF CANTILEVERING PONTICS OFF ROOT TREATED TEETH


128
129 Some patients become exquisitely sensitive about the way their teeth meet to the extent that they are better at detecting interferences than many dentists. These patients appear to have an amplified level of sensation which can be troublesome when perceived as pain. There is often a heavy occlusal contact present - you just need to know how to look for it and adjust it. A pitfall of not recognising such a patient is unnecessary root canal treatment R Wassell - Occlusal pitfalls and how to avoid them BDJ Vol 212 No 6 24th March 2102

130 THE PATIENT HAD UR7 RCT d BUT DESPITE THE BEAUTIFUL RCT HAD ONGOING DISCOMFORT AND WAS RELUCTANT TO PROCEED WITH CROWN PLACEMENT UNTIL SYMPTOMS DISAPPEARED.


131 MODELS WERE NOT TAKEN AT THE TIME THAT THE PATIENT PRESENTED FOR A SECOND OPINION BUT FROM THE ARTICULATED MODELS TAKEN FOLLOWING CROWN PREPARATION, THE MASSIVE INTERFERENCE IS VISIBLE IN PROTRUSIVE IN THE NEXT TWO SLIDES EVEN AFTER SUBSTANTIAL OCCLUSAL REDUCTION.



132 AT THE TIME OF THE SECOND OPINION THE PATIENT WAS INFORMED THAT THE OVERERUPTED THIRD MOLAR WOULD IN ALL LIKELYHOOD REQUIRE OCCLUSAL RESHAPING TO ELIMINATE THE INTERFERENCE AND ASSOCIATED PAIN. 2 DAYS AFTER ADJUSTMENT ALL THE SYMPTOMS DISAPPEARED AND THE PATIENT WAS HAPPY TO PROCEED WITH THE DEFINTIVE CROWN.



133 THE TOOTH PRIOR TO ADJUSTMENT AND RESHAPING OVERERUPTION AND MALPOSITIONING CLEARLY VISIBLE

134 THE RADIOGRAPHS CLEARLY SHOW THAT THE ADJUSTMENT WAS WITHIN ENAMEL
135 AVOIDING FAILING RESTORATIONS

136 ABFRACTION


137 VENEERS IN BRUXERS MORE COMMONLY DEBOND AT THE GINGIVAL THIRD RATHER THAN INCISALLY DUE TO TOOTH FLEXION SIMILAR TO THE ABFRACTION THEORY

138 MINIMAL PREP DOES NOT MEAN NO PREP
139 Always consider, particularly if working on the last standing molar, whether there a premature contact in RCP- if there is, as soon as you carry out an occlusal adjustment there will be distal movement of the mandible and it is likely that you will require further adjustment of the occlusal surface as the vertical dimension in that area will be diminished Michael Wise

140 TAKE CARE WHEN CROWNING LAST STANDING MOLARS
141 Most responses to occlusal disharmony are adaptive in nature The possibility of converting a patient with a symptom free adapting occlusion to one which is uncomfortable because of high fillings increases with the number and complexity of the restorations - moreover the response varies between individuals M Wise
142 SHOULD CROWNS BE CEMENTED HIGH?


143 DIFFERENTIAL WEAR COMMONLY RESULTS IN THE CREATION OF INTERFERENCES AROUND THE MOUTH


144 ALWAYS POLISH MEATAL OR PORCELAIN AFTER CROWN ADJUSTMENT WITH THE APPROPRIATE POLISHING KIT TO AVOID WEAR OF THE OPPOSING DENTITION Glazed porcelain Surface texture following adjustment with a diamond bur


145 Surface texture following adjustment with a diamond bur Porcelain surface after polishing with the Meisinger porcelain polishing kit
146 IMPLANTS
147 Occlusal loading of a fully integrated implant can be the point of success or failure long term. Implant stability can be quickly lost if not introduced into a healthy occlusal environment an environment where stress is minimised by good anterior guidance, posterior disclusion and good centric stops. Light occlusal stops on implant teeth need routine adjustment to maintain proper occlusal timing with the natural dentition. Occlusal overload and lateral interferences will quickly show signs of bone loss around the implants 7 Deadly Sins of Implants Dawson Academy, Nov 15


148 FULL ARCH IMPLANT CASES SHOULD ALSO IDEALLY FOLLOW CONVENTIONAL OCCLUSAL PRINCIPLES. REPLICATING THIS MALOCCLUSION WOULD NOT BE REGARDED AS BEING IDEAL



149 THE IMMEDIATE DENTURE HAS BEEN DESIGNED TO ELIMINATE BOTH THE CROSS-BITE AND THE ANTERIOR OPEN BITE

150 TRIAL RUNNING THE FULL DENTURE PRIOR TO IMPLANT PLACEMENT ENSURES THAT THE PATIENT IS BOTH COMFORTABLE WITH THE OCCLUSAL AND VERTICAL DIMENSION CHANGES, AND PLEASED WITH THE NEW APPERANCE


151 THE RE-DESIGNED OCCLUSION

152 IMPLANT PLACEMENT AND TEETH IN A DAY
153 Ortho cases All clinicians involved in a multidisciplinary treatment need to be mindful of the overall duty of care to the patient particularly the referring dentist. An assumption that the other clinician was dealing with the problem will be viewed as a very poor defence Dental Protection - Annual Review 2015.


154 BEFORE AND AFTER ORTHODONTIC CASE WHICH WAY SHOULD LATERALS POINT IN BEAUTY? - TOWARDS THE TUMMY BUTTON. RECESSION LL1 UNNOTICED ANDUNTREATED DURING ORTHO TREATMENT
155 WHAT WAS THE PROBLEM ON COMPLETION OF TREATMENT: THE PATIENT KNEW SHE HAD A RECESSION PROBLEM LOWER FRONT WHY HAD NOTHING BEEN DONE? THE PATIENT HAD EXPERIENCED TMJ PROBLEMS ON THE RIGHT SIDE SINCE TREATMENT BEGAN THE PATIENT HAD PERSISTENT PAIN ON UL5 PRESSURE AND HOT/COLD THE PATIENT HAD ONGOING PROBLEMS WITH DISCOMFORT/MILD PAIN UR2 WHY HAD SHE NOT BEEN FORE-WARNED THAT, AFTER 2+ YEARS OF FIXED LINGUAL APPLIANCES, SHE WOULD REQUIRE FURTHER TREATMENT WITH CONVENTIONAL ORTHODONTIC TREATMENT FOR FINAL ALIGNMENT AND THAT HER TEETH WOULD NOT NECESSARILY MEET CORRECTLY WHAT EXACTLY IS SHE TO DO IF THE TEETH DO NOT DRIFT BACK INTO OCCLUSION DAHL STYLE


156 IN THE FINISHED CASE, THERE IS A PARTIAL LOSS OF CANINE GUIDANCE IN LATERAL EXCURSION WITH VERY HEAVY CONTACT ON THE LATERAL INCISOR AND NONE ON THE CENTRAL INCISOR ie THE CANINE SHOULD HAVE BEEN EXTRUDED FURTHER TO PROVIDE EFFECTIVE GUIDANCE. THE PATIENT FEELS THAT THE LATERAL INCISOR SEEMS BRUISED AND UNCOMFORTABLE ALL THE TIME. INTERESTINGLY, THE PATIENT REPORTED THAT DURING LINGUAL APPLIANCE THERAPY A GAP WOULD APPEAR IN THIS AREA DURING TREATMENT, CLOSE WHEN THE APPLIANCES WERE TIGHTENED AND THEN RE-OPEN BEFORE THE NEXT REVIEW APPOINTMENT
157 CROSS-OVER IN WORKING SIDE Dawson Academy 2009 Why Porcelain Breaks and Chips CORRECT CROSSOVER DISCLUSION IT IS NOT BY CHANCE THAT THE MOST COMMON ANTERIOR AESTHETIC FRACTURE IS TO THE MAXILLARY LATERAL INCISOR. PROPER OCCLUSAL DESIGN DICTATES A SMOOTH TRANSITION TO THE INCISAL EDGE OF THE MAXILLARY CENTRALS AS THE PATIENT MOVES BEYOND THE CANINE IN LATERAL EXCURSION. WHEN THIS POSITIONING IS OVERLOOKED, EXCESSIVE LOADS CAN BE PLACED ON THE DISTAL OF THE LATERAL INCISORS LEADING TO FRACTURE.



158 OCCUSAL ANALYSIS SHOWED THAT THE ONLY CONTACT IN CENTRIC IS ON THE UPPER AND LOWER LEFT PREMOLARS


159 WITH THE PATIENT IN THE INITIAL POINT OF CONTACT IN THE RETRUDED ARC OF CLOSURE, THE ANTERIOR AND POSTERIOR TEETH ARE A LONG WAY AWAY FROM MEETING ON THE RIGHT SIDE, CLOSER ANTERIORLY ON THE LEFT. THE ENTIRE OCCLUSION WAS SUPPORTED BY THE PREMOLARS ON THE LEFT SIDE. THERE WAS A SLIDE INTO INTERCUSPAL WHERE A FEW MORE, BUT NOT ALL, TEETH MET


160 THIS IS THE BEST THAT COULD BE ACHIEVED WITH OCCLUSAL ADJUSTMENT MORE CONTACTS LEFT SIDE, BUT ONLY ONE ON THE RIGHTSIDE Before After
161 PATIENT 1 MONTH AFTER OCCLUSAL EQUILIBRATION I wanted to write to thank you for the adjustments you made to my teeth and the night plate the other week. A vast improvement. My bite is much more comfortable now and I am not getting the pain on the left premolars now that the pressure has been reduced. The pain in the right TMJ is also much less frequent. I was able to enjoy my holiday as a result!


162 1 YEAR LATER MOST OF THE TEETH HAVE FINALLY DRIFTED INTO OCCLUSION DAHL STYLE ALBEIT UNPLANNED


163 WHEN TO SAY NO

164 THERE IS NO SPACE TO PLACE A RESTORATIVE MATERIAL
165 MISCELLANEOUS
166
167

168
169
170
171

172
173
174
175
176
177 HOW DOES OCCLUSION DIFFER WITH IMPLANTS
178 ACKNOWLEDGEMENTS IMPLANT PLACEMENT DR ANDREW DAWOOD ALL CLINICAL SLIDES USED ARE MY OWN IF NOT THEN ATTRIBUTED TO LAST YEAR S STUDENTS REFERENCES ATTRIBUTED AS MUCH AS POSSIBLE BIBLIOGRAPHY Occlusion and Restorative Dentistry for the General Practitioner Michael Wise 10 Part BDJ series - Feb 1982 onwards What is Occlusion S Davies,RMJ Gray et al 7 Part series BDJ - Sept 2001 onwards Dawson Academy various short articles Please respect that this is my intellectual property and for personal usage not dissemination
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Dr Mohammed Alfarsi Page 1 9 December Principles of Occlusion
 Dr Mohammed Alfarsi Page 1 9 December 2013 Principles of Occlusion Overview: The occlusion is a very large, yet easy to manage once properly understood, topic. Thus, no one handout is enough to fully understand
Dr Mohammed Alfarsi Page 1 9 December 2013 Principles of Occlusion Overview: The occlusion is a very large, yet easy to manage once properly understood, topic. Thus, no one handout is enough to fully understand
Occlusion & Prosthodontics
 Occlusion & Prosthodontics Occlusion and Prosthodontic Treatments Babak Shokati DDS, MSc. MSc. Candidate (Prosthodontics) Occlusion: A Controversial Issue Occlusion related issues and contradictory debates:
Occlusion & Prosthodontics Occlusion and Prosthodontic Treatments Babak Shokati DDS, MSc. MSc. Candidate (Prosthodontics) Occlusion: A Controversial Issue Occlusion related issues and contradictory debates:
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
THE ROYAL COLLEGE OF SURGEONS OF ENGLAND FACULTY OF GENERAL DENTAL PRACTICE (UK) DIPLOMA IN RESTORATIVE DENTISTRY. Case 3 Mrs JG
 DIPLOMA IN RESTORATIVE DENTISTRY. Case 3 Mrs JG") THE ROYAL COLLEGE OF SURGEONS OF ENGLAND FACULTY OF GENERAL DENTAL PRACTICE (UK) DIPLOMA IN RESTORATIVE DENTISTRY Case 3 Mrs JG Andrew Shelley October 2007 Table of Contents 1 One Page Case summary...1
THE ROYAL COLLEGE OF SURGEONS OF ENGLAND FACULTY OF GENERAL DENTAL PRACTICE (UK) DIPLOMA IN RESTORATIVE DENTISTRY Case 3 Mrs JG Andrew Shelley October 2007 Table of Contents 1 One Page Case summary...1
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Managing the failing dentition
 C L I N I C A L Managing the failing dentition Kamal Suri 1 Increasingly, the numbers of patients walking through the doors of our practices are those whose dentition is slowly in decline. I am presented
C L I N I C A L Managing the failing dentition Kamal Suri 1 Increasingly, the numbers of patients walking through the doors of our practices are those whose dentition is slowly in decline. I am presented
ALTERNATE OCCLUSAL SCHEMES
 ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
Splint Appliance. Selection Guide. Great Lakes. See inside...
 Great Lakes Splint Appliance Selection Guide This guide includes helpful tips on how to choose the right splint for your patient and information on standard function and specifications for Great Lakes
Great Lakes Splint Appliance Selection Guide This guide includes helpful tips on how to choose the right splint for your patient and information on standard function and specifications for Great Lakes
Dzakovich Conclusions
 Definitions Attrition Tooth wear resulting from contact between opposing teeth. Erosion A gradual tooth-surface loss process caused by an electrolytic or chemical mechanism without bacteria being involved.
Definitions Attrition Tooth wear resulting from contact between opposing teeth. Erosion A gradual tooth-surface loss process caused by an electrolytic or chemical mechanism without bacteria being involved.
Principle of Occlusion
 Principle of Occlusion Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Overview Principle of Occlusion Overview Principle of Occlusion Point centric Long centric Freedom
Principle of Occlusion Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Overview Principle of Occlusion Overview Principle of Occlusion Point centric Long centric Freedom
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
OCCLUSION IN NEWLY FABRICATED BRIDGE*
 15 OCCLUSION IN NEWLY FABRICATED BRIDGE* (OKLUSI PADA GIGI TIRUAN JEMBATAN YANG BARU DIBUAT) Natasya Ahmad Tarib, Marlynda Ahmad Department of Prosthodontics, Faculty of Dentistry, University Kebangsaan
15 OCCLUSION IN NEWLY FABRICATED BRIDGE* (OKLUSI PADA GIGI TIRUAN JEMBATAN YANG BARU DIBUAT) Natasya Ahmad Tarib, Marlynda Ahmad Department of Prosthodontics, Faculty of Dentistry, University Kebangsaan
Restoring Severe Anterior Wear Cases; A Step by step Process
 0 Restoring Severe Anterior Wear Cases; Solving the Most Difficult Cases: A Step by Step Process" A Step by step Process Friday, February 6, 2015 Glenn E. DuPont, D.D.S. 1 The presence of worn dentition,
0 Restoring Severe Anterior Wear Cases; Solving the Most Difficult Cases: A Step by Step Process" A Step by step Process Friday, February 6, 2015 Glenn E. DuPont, D.D.S. 1 The presence of worn dentition,
Horizontal Jaw Relation
 Horizontal Jaw Relation Horizontal Jaw Relation It is the relationship of the mandible to the maxilla in a horizontal plane. It can also be described as the relationship of the mandible to the maxilla
Horizontal Jaw Relation Horizontal Jaw Relation It is the relationship of the mandible to the maxilla in a horizontal plane. It can also be described as the relationship of the mandible to the maxilla
Horizontal jaw relations: The relationship of mandible to maxilla in a
 Horizontal relations Horizontal jaw relations: The relationship of mandible to maxilla in a horizontal plane (in anteroposterior and side to side direction). a- Protruded or forward relation. b-lateral
Horizontal relations Horizontal jaw relations: The relationship of mandible to maxilla in a horizontal plane (in anteroposterior and side to side direction). a- Protruded or forward relation. b-lateral
Jaw relation registration in RPD
 Jaw relation registration in RPD Why to Record the Jaw Relations? To establish and maintain a harmonious relationship with all oral structures and to provide a masticatory apparatus that is efficient and
Jaw relation registration in RPD Why to Record the Jaw Relations? To establish and maintain a harmonious relationship with all oral structures and to provide a masticatory apparatus that is efficient and
#45 Ortho-Tain, Inc PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT
 #45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
#45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
A conservative restorative smile makeover
 C L I N I C A L A conservative restorative smile makeover Aneta Grzesinska 1 Introduction The patient was a 37-year-old female who presented to the practice requesting six porcelain veneers for her upper
C L I N I C A L A conservative restorative smile makeover Aneta Grzesinska 1 Introduction The patient was a 37-year-old female who presented to the practice requesting six porcelain veneers for her upper
INSIGHT & INNOVATION. Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been
 Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been employed in regard to treatment planning and correct restorative sequence. Assuming that the patient has healthy
Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been employed in regard to treatment planning and correct restorative sequence. Assuming that the patient has healthy
Deprogrammers made. Deprogrammers can be used for... How do deprogrammers work?
 Deprogrammers made asy Easy Deprogrammers made Deprogrammers can be used for... Headache sufferers Bruxers and/or clenchers Muscle relaxation Determining proper joint position Protection against wear Diagnosis
Deprogrammers made asy Easy Deprogrammers made Deprogrammers can be used for... Headache sufferers Bruxers and/or clenchers Muscle relaxation Determining proper joint position Protection against wear Diagnosis
Selection and arrangement of teeth in rpd
 Selection and arrangement of teeth in rpd upon completion of the articulator mounting and a thorough assessment of the occlusal requirements, the practitioner should be able to perform the proper arrangement
Selection and arrangement of teeth in rpd upon completion of the articulator mounting and a thorough assessment of the occlusal requirements, the practitioner should be able to perform the proper arrangement
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1.
 Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1. A longitudinal root fracture was suspected and confirmed when the
Patient s Presenting Complaint V.C. presented with discomfort and mobility from the crowned maxillary left central incisor tooth. Fig 1. A longitudinal root fracture was suspected and confirmed when the
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
TURN CLASS II INTO SIMPLE CLASS I PATIENTS.
 TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration
 Reality or Resin; Free Hand Artistry with Anterior Bonding Dennis B. Hartlieb, DDS CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration Wish List: 1. Reversible (no prep/ minimal
Reality or Resin; Free Hand Artistry with Anterior Bonding Dennis B. Hartlieb, DDS CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration Wish List: 1. Reversible (no prep/ minimal
Occlusion in complete denture
 Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
Shadeguides Finding the Centric Relation The Kois Deprogrammer
 Maciej Zarow Shadeguides Finding the Centric Relation The Kois Deprogrammer 21 Jun 2018 Finding the centric relation might sometimes seem hard, but with appropriate devices, such as the Kois Deprogrammer
Maciej Zarow Shadeguides Finding the Centric Relation The Kois Deprogrammer 21 Jun 2018 Finding the centric relation might sometimes seem hard, but with appropriate devices, such as the Kois Deprogrammer
Occlusion and removable prosthodontics
 12 Occlusion and removable prosthodontics R. Jagger Synopsis Occlusal considerations for removable prostheses are essentially the same as for fixed restorations. The approach to establishing occlusion
12 Occlusion and removable prosthodontics R. Jagger Synopsis Occlusal considerations for removable prostheses are essentially the same as for fixed restorations. The approach to establishing occlusion
Complex Occlusal Rehabilitation: A Case Report
 Complex Occlusal Rehabilitation: A Case Report DR. ALI TUNKIWALA INTRODUCTION The most difficult problems in clinical practice are those where there is interaction of various pathogenic factors with consequent
Complex Occlusal Rehabilitation: A Case Report DR. ALI TUNKIWALA INTRODUCTION The most difficult problems in clinical practice are those where there is interaction of various pathogenic factors with consequent
Nine Steps To Occlusal Harmony
 Nine Steps To Occlusal Harmony Dr. Ali Tunkiwala has graduated from Nair Hospital Dental College in 1996 & completed his Masters Degree in Prosthetic Dentistry from Mumbai University (GDC, Mumbai) in 1998.
Nine Steps To Occlusal Harmony Dr. Ali Tunkiwala has graduated from Nair Hospital Dental College in 1996 & completed his Masters Degree in Prosthetic Dentistry from Mumbai University (GDC, Mumbai) in 1998.
NATIONAL EXAMINING BOARD FOR DENTAL NURSES
 NATIONAL EXAMINING BOARD FOR DENTAL NURSES NATIONAL DIPLOMA EXAMINATION DENTAL CHARTING NEBDN is a limited company registered in England & Wales No. 5580200 Registered with the Charity Commisioners No.
NATIONAL EXAMINING BOARD FOR DENTAL NURSES NATIONAL DIPLOMA EXAMINATION DENTAL CHARTING NEBDN is a limited company registered in England & Wales No. 5580200 Registered with the Charity Commisioners No.
Hands-on Posterior Tooth Preparation. Practical Skills Courses, SWL, 25/11/2016
 Hands-on Posterior Tooth Preparation Practical Skills Courses, SWL, 25/11/2016 Hands-On Didactic Teaching A Tooth-Friendly-Approach - Hands-on Tooth Preparation Course - Dental Simulation to include: Posterior
Hands-on Posterior Tooth Preparation Practical Skills Courses, SWL, 25/11/2016 Hands-On Didactic Teaching A Tooth-Friendly-Approach - Hands-on Tooth Preparation Course - Dental Simulation to include: Posterior
Class II. Bilateral Cleft Lip and Palate. Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Cleft Lip and Palate.
 Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
What is occlusion? S. Davies, 1 and R. M. J. Gray, 2. Dentists need a balanced view on occlusion
 1 What is? S. Davies, 1 and R. M. J. Gray, 2 PRACTICE The aim of this series of papers is to explore the role of in dental practice. The range of opinion in the dental profession as to the importance of
1 What is? S. Davies, 1 and R. M. J. Gray, 2 PRACTICE The aim of this series of papers is to explore the role of in dental practice. The range of opinion in the dental profession as to the importance of
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Question #2: What range of options would you present to this patient?
 Question #2: What range of options would you present to this patient? Some highlights of different treatment planning perspectives 1 Tidy up orthodontic treatment before proceeding with any type of treatment,...implant/
Question #2: What range of options would you present to this patient? Some highlights of different treatment planning perspectives 1 Tidy up orthodontic treatment before proceeding with any type of treatment,...implant/
Replacing Missing or Debonded Brackets
 CFAST Help Sheet Replacing Missing or Debonded Brackets Brackets becoming deboned are not uncommon you will almost certainly experience this. The important thing to remember is - DON T PANIC! And tell
CFAST Help Sheet Replacing Missing or Debonded Brackets Brackets becoming deboned are not uncommon you will almost certainly experience this. The important thing to remember is - DON T PANIC! And tell
TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE
 TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics( prosthodontics), Adelaide, FRACDS
TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics( prosthodontics), Adelaide, FRACDS
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL
 MANUAL") AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique
 10.5005/JP-Journals-10012-1099 Koshika Tandon et al CASE REPORT Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique Koshika Tandon, Ajay Singh, Himanshu Gupta, Rajdeep
10.5005/JP-Journals-10012-1099 Koshika Tandon et al CASE REPORT Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique Koshika Tandon, Ajay Singh, Himanshu Gupta, Rajdeep
Fixed Twin Blocks. Guidelines for case selection are similar to those for removable Twin Block appliances.
 Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Fixed Twin Blocks Development of Fixed Twin Blocks Dr Clark has enjoyed the cooperation of Dynaflex in developing the Fixed Twin Block. Six years of clinical testing has confirmed that this technique produces
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion.
 Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
See the end from the beginning
 Staub Cranial See the end from the beginning with Staub Cranial Recently a new technology was introduced to the United States that will revolutionize the way our industry restores teeth. The Staub Cranial
Staub Cranial See the end from the beginning with Staub Cranial Recently a new technology was introduced to the United States that will revolutionize the way our industry restores teeth. The Staub Cranial
How to provide intraoral scans to SomnoMed for the production of SomnoDent device.
 How to provide intraoral scans to SomnoMed for the production of SomnoDent device. KEY QUESTIONS: 1. Where do I send my Case? Send intra-oral scan files (maxilla and mandible in protrusive bite) and an
How to provide intraoral scans to SomnoMed for the production of SomnoDent device. KEY QUESTIONS: 1. Where do I send my Case? Send intra-oral scan files (maxilla and mandible in protrusive bite) and an
A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture
 Rita Zarina et al Mini Review 10.5005/jp-journals-10052-0097 A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture 1 Rita Zarina, 2 JL Jaini, 3 Rajan S Raj ABSTRACT Long-term success
Rita Zarina et al Mini Review 10.5005/jp-journals-10052-0097 A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture 1 Rita Zarina, 2 JL Jaini, 3 Rajan S Raj ABSTRACT Long-term success
Contouring vs. Orthodontics. Contouring to Eliminate Fractures and Enhance Proportions
 Contouring vs. Orthodontics Photo 1 Maxillary central incisors are overlapped. Patient chose rapid tooth movement instead of contouring. Photo 2 Maxillary central incisors after six months of orthodontic
Contouring vs. Orthodontics Photo 1 Maxillary central incisors are overlapped. Patient chose rapid tooth movement instead of contouring. Photo 2 Maxillary central incisors after six months of orthodontic
Class II Correction with Invisalign Molar rotation.
 Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Tips from your peers to help you treat with confidence. Class II Correction with Invisalign Molar rotation. Dr. Mazyar Moshiri. Class II Correction with Invisalign Molar Rotation. Dr. Mazyar Moshiri. Orthodontic
Archived SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS
 SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
Restoration of the worn dentition
 Clin Dent Rev (2017) 1:4 https://doi.org/10.1007/s41894-017-0003-3 TREATMENT Restoration of the worn dentition Paul King 1 Received: 16 March 2017 / Accepted: 31 May 2017 / Published online: 30 June 2017
Clin Dent Rev (2017) 1:4 https://doi.org/10.1007/s41894-017-0003-3 TREATMENT Restoration of the worn dentition Paul King 1 Received: 16 March 2017 / Accepted: 31 May 2017 / Published online: 30 June 2017
#60 Ortho-Tain, Inc TIMING FOR CROWDING CORRECTIONS WITH THE OCCLUS-O-GUIDE AND NITE-GUIDE APPLIANCES
 #60 Ortho-Tain, Inc. 1-800-541-6612 TIMING FOR CROWDING CORRECTIONS WITH THE OCCLUS-O-GUIDE AND NITE-GUIDE APPLIANCES Although timing is not as critical for the Occlus-o-Guide appliance as it is with the
#60 Ortho-Tain, Inc. 1-800-541-6612 TIMING FOR CROWDING CORRECTIONS WITH THE OCCLUS-O-GUIDE AND NITE-GUIDE APPLIANCES Although timing is not as critical for the Occlus-o-Guide appliance as it is with the
أ.م. هدى عباس عبد اهلل CROWN AND BRIDGE جامعة تكريت كلية. Lec. (2) طب االسنان
 طب االسنان") Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Lec. (2) CROWN AND BRIDGE أ.م. هدى عباس عبد اهلل Patient selection and examination A thorough diagnosis must first be made of the patient's dental condition, considering both hard and soft tissues. this
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
Using the Lucia Jig to take an accurate & reliable centric relation bite registration
 Trimming Instructions Trimming the silicone bite records is an important step to ensure an accurate fit on the model. Trimming eliminates all the interferences so there is no movement once the models are
Trimming Instructions Trimming the silicone bite records is an important step to ensure an accurate fit on the model. Trimming eliminates all the interferences so there is no movement once the models are
Treatment planning of nonskeletal problems. in preadolescent children
 In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Aesthetic and functional restoration of the severely worn dentition
 A SYSTEMATIC APPROACH TO FULL-MOUTH RECONSTRUCTION OF THE SEVERELY WORN DENTITION JAY LERNER Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge.
A SYSTEMATIC APPROACH TO FULL-MOUTH RECONSTRUCTION OF THE SEVERELY WORN DENTITION JAY LERNER Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge.
Avoiding Restorative Failure
 Avoiding Restorative Failure Lee Ann Brady, DMD Dr. Brady has no relevant financial relationships to disclose. Presentation partially sponsored by DMG and GC America Friday, June 15, 2018 1:30pm 4:30pm
Avoiding Restorative Failure Lee Ann Brady, DMD Dr. Brady has no relevant financial relationships to disclose. Presentation partially sponsored by DMG and GC America Friday, June 15, 2018 1:30pm 4:30pm
DENT Advanced Topics in Removable Prosthodontics, Winter 2008
 University of Michigan Deep Blue deepblue.lib.umich.edu 2008-01 DENT 718 - Advanced Topics in Removable Prosthodontics, Winter 2008 Shotwell, Jeffrey Shotwell, J. (2008, April 23) Advanced Topics in Removable
University of Michigan Deep Blue deepblue.lib.umich.edu 2008-01 DENT 718 - Advanced Topics in Removable Prosthodontics, Winter 2008 Shotwell, Jeffrey Shotwell, J. (2008, April 23) Advanced Topics in Removable
You. Fix. Could. This? Treatment solutions for typical and atypical adult relapse. 78 SEPTEMBER 2017 // orthotown.com
 by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
by Dan Grob, DDS, MS, editorial director, Orthotown magazine You Could Fix This? Treatment solutions for typical and atypical adult relapse 78 SEPTEMBER 2017 // orthotown.com OT0917_Mechanics_AG.indd 78
DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION
 DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION WHO IS PETER DAWSON? WHO IS PETER DAWSON? Peter Dawson is a dentist that specializes in the treatment of the exposed exterior surfaces of the teeth.
DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION WHO IS PETER DAWSON? WHO IS PETER DAWSON? Peter Dawson is a dentist that specializes in the treatment of the exposed exterior surfaces of the teeth.
Arrangement of posterior artificial teeth Standardized parameters Curve of Wilson Curve of Spee
 . Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
. Arrangement of posterior artificial teeth Posterior teeth are set up in tight centric occlusion. The mandibular teeth are set in the wax occlusion rim over the residual ridge in their ideal buccolingual
Types of prostetic appliances Dr. Barbara Kispélyi
 Semmelweis University Faculty of Dentistry Department of Prosthodontics Types of prostetic appliances Dr. Barbara Kispélyi Types of prostetic appliances Types of the fixed prostetic appliances According
Semmelweis University Faculty of Dentistry Department of Prosthodontics Types of prostetic appliances Dr. Barbara Kispélyi Types of prostetic appliances Types of the fixed prostetic appliances According
529-A Treatment and Management of the Edentulous Patient. Upon completion of this course the student should be able to:
 Course & Title: Session & Topic: 529-A Treatment and Management of the Edentulous Patient Jaw Relations General Goal: To understand the principles of orientational, horizontal and vertical jaw relations
Course & Title: Session & Topic: 529-A Treatment and Management of the Edentulous Patient Jaw Relations General Goal: To understand the principles of orientational, horizontal and vertical jaw relations
1. What is the highest and sharpest cusp on the lower first deciduous molar? 2. Which of the following is NOT the correct location of an embrasure?
 1 1. What is the highest and sharpest cusp on the lower first deciduous molar? a. mesiobuccal b. distobuccal c. distolingual d.mesiolingual 2. Which of the following is NOT the correct location of an embrasure?
1 1. What is the highest and sharpest cusp on the lower first deciduous molar? a. mesiobuccal b. distobuccal c. distolingual d.mesiolingual 2. Which of the following is NOT the correct location of an embrasure?
TURN CLASS II INTO SIMPLE CLASS I PATIENTS.
 TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
TURN CLASS II INTO SIMPLE CLASS I PATIENTS. THE CARRIERE MOTION TM APPLIANCE fast gentle natural The Carriere Philosophy. Fast. Shortens overall treatment time by up to four months as it treats Class II
Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure
 Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure Saurav Banerjee, Nabarun Chakraborty, Rajwinder Singh, Tapas Gupta Abstract Excessive occlusal wear can
Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure Saurav Banerjee, Nabarun Chakraborty, Rajwinder Singh, Tapas Gupta Abstract Excessive occlusal wear can
Fundamental & Preventive Curvatures of Teeth and Tooth Development. Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L.
 Dr. Margaret L.") Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Fundamental & Preventive Curvatures of Teeth and Tooth Development Lecture Three Chapter 15 Continued; Chapter 6 (parts) Dr. Margaret L. Dennis Proximal contact areas Contact areas are on the mesial and
Full mouth occlusal rehabilitation; by Pankey Mann Schuyler philosophy
 Case Report DOI: 10.18231/2455-8486.2017.0006 Jinsa P. Devassy 1, Ankitha Sivadas 2, Shabas Muhammed 3 1 Consultant Prosthodontist, Ernakulam, Kerala, 2 Assistant Professor, 3 PG Student, Dept. of Prosthodontics,
Case Report DOI: 10.18231/2455-8486.2017.0006 Jinsa P. Devassy 1, Ankitha Sivadas 2, Shabas Muhammed 3 1 Consultant Prosthodontist, Ernakulam, Kerala, 2 Assistant Professor, 3 PG Student, Dept. of Prosthodontics,
Complete denture copy technique A practical application
 Singapore Dental Journal 35 (2014) 65 70 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/sdj Case report Complete denture copy technique A practical application Steven
Singapore Dental Journal 35 (2014) 65 70 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/sdj Case report Complete denture copy technique A practical application Steven
SCD Case Study. Background
 SCD Case Study Background A female aged over 70 presented with an unremarkable medical history seeking a comprehensive examination as the last dental examination was over four years ago. The patient is
SCD Case Study Background A female aged over 70 presented with an unremarkable medical history seeking a comprehensive examination as the last dental examination was over four years ago. The patient is
Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results.
 SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
Invisalign Finishing. Treatment Monitoring & Tips & Techniques Guide to Help Doctors Achieve Ideal Patient Outcomes
 Invisalign Finishing Treatment Monitoring & Tips & Techniques Guide to Help Doctors Achieve Ideal Patient Outcomes Introduction This Guide is intended to help the Invisalign practitioner address monitoring
Invisalign Finishing Treatment Monitoring & Tips & Techniques Guide to Help Doctors Achieve Ideal Patient Outcomes Introduction This Guide is intended to help the Invisalign practitioner address monitoring
OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC
 Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Interdisciplinary Treatment Planning in Transitioning Periodontally Hopeless Dentition
 Interdisciplinary Treatment Planning in Transitioning Periodontally Hopeless Dentition A clinical case review I NTRODUCTION Decreasing risk in an advanced periodontally diseased dentition presents a great
Interdisciplinary Treatment Planning in Transitioning Periodontally Hopeless Dentition A clinical case review I NTRODUCTION Decreasing risk in an advanced periodontally diseased dentition presents a great
MemRx Orthodontic Appliances
 MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
MemRx Orthodontic Appliances Uses and Instructions The MemRx Fundamentals As the need for faster, more efficient treatment of non-compliant patients increases, orthodontic!technology and materials has
PG Dip (Level II), Advanced Course in Restorative & Aesthetic Dentistry
, Advanced Course in Restorative & Aesthetic Dentistry") Syllabus and Specific & GDC Development Outcomes PG Dip (Level II), Advanced Course in Restorative & Aesthetic Dentistry www.dominic-hassall-training.co.uk 1 Day 1 Course Introduction Dominic Hassall Tutorial
Syllabus and Specific & GDC Development Outcomes PG Dip (Level II), Advanced Course in Restorative & Aesthetic Dentistry www.dominic-hassall-training.co.uk 1 Day 1 Course Introduction Dominic Hassall Tutorial
If we listen to our patients, our treatment acceptance can approach 100%
 Module 2 ADVANCED TREATMENT PLANNING: CONCEPTS Treatment Planning: Edentulism Dentures: Standard or Turbyfill. Dentures: Mini-Implant Retained: Soft tissue supported denture. Dentures: Standard Implant
Module 2 ADVANCED TREATMENT PLANNING: CONCEPTS Treatment Planning: Edentulism Dentures: Standard or Turbyfill. Dentures: Mini-Implant Retained: Soft tissue supported denture. Dentures: Standard Implant
Parafunction poses a risk for any. Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion
 Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion BRIAN S. VENCE, DDS* ABSTRACT The goal of this clinical report is to describe and illustrate the principles for achieving
Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion BRIAN S. VENCE, DDS* ABSTRACT The goal of this clinical report is to describe and illustrate the principles for achieving
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations The outline form
 Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Lec. 3-4 Dr. Saif Alarab Clinical Technique for Class I Amalgam Restorations Class I refers to -Restorations on the occlusal surfaces of posterior teeth, - The occlusal two thirds of facial and lingual
Managing. Not on course. Unplanned reaction 9/15/2011. Possible Reactions. Probable Root causes. invisalign Aligner Tracking Issues
 Managing invisalign Aligner Tracking Issues Tips and Techniques for keeping treatment on course Dr. Karol Miranda DDS Universidad Latino Americana de Ciencia y Tecnología, (ULACIT), Costa Rica. Private
Managing invisalign Aligner Tracking Issues Tips and Techniques for keeping treatment on course Dr. Karol Miranda DDS Universidad Latino Americana de Ciencia y Tecnología, (ULACIT), Costa Rica. Private
Dr Robert Drummond. BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015
, FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015") Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
The patient gave a history of hypertension and gastritis for which was taking Lacidipine 4mg, Omeprazole 20mg and Simvastatin 40mg.
 A.S. was referred by her general dental practitioner for assessment for possible implant placement to restore the space where her bridge replacing her maxillary central incisors had recently failed. Fig
A.S. was referred by her general dental practitioner for assessment for possible implant placement to restore the space where her bridge replacing her maxillary central incisors had recently failed. Fig
PG Cert Contemporary Restorative and Aesthetic Dentistry (Level I)
") PG Cert Contemporary Restorative and Aesthetic Dentistry (Level I) www.dominic-hassall-training.co.uk DAY 1 Periodontology Module Contemporary Periodontics Course introduction and philosophy o Cosmetic,
PG Cert Contemporary Restorative and Aesthetic Dentistry (Level I) www.dominic-hassall-training.co.uk DAY 1 Periodontology Module Contemporary Periodontics Course introduction and philosophy o Cosmetic,
Primary Teeth Chapter 18. Dental Anatomy 2016
 Primary Teeth Chapter 18 Dental Anatomy 2016 Primary Teeth - Introduction Synonyms deciduous teeth, baby teeth, temporary teeth, milk teeth. There are 20 primary teeth, designated as A thru T in the Universal
Primary Teeth Chapter 18 Dental Anatomy 2016 Primary Teeth - Introduction Synonyms deciduous teeth, baby teeth, temporary teeth, milk teeth. There are 20 primary teeth, designated as A thru T in the Universal
6610 NE 181st Street, Suite #1, Kenmore, WA
 660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
RETENTION AND RELAPSE
 RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
RETENTION AND RELAPSE DEFINITION Maintaining newly moved teeth long enough to aid in stabilizing their correction MOYERS loss of any correction achieved by any orthodontic treatment RELAPSE CAUSES OF RELAPSE
Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report
 J. Adv Oral Research Case Report All Rights Res Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report Hemal S. Agrawal
J. Adv Oral Research Case Report All Rights Res Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report Hemal S. Agrawal
Introduction to Occlusion and Mechanics of Mandibular Movement
 Introduction to Occlusion and Mechanics of Mandibular Movement Dr. Pauline Hayes Garrett Department of Endodontics, Prosthodontics, and Operative Dentistry University of Maryland, Baltimore Assigned reading
Introduction to Occlusion and Mechanics of Mandibular Movement Dr. Pauline Hayes Garrett Department of Endodontics, Prosthodontics, and Operative Dentistry University of Maryland, Baltimore Assigned reading
Chapter 12. Prosthodontics
 Chapter 12 Prosthodontics Golbarg Kolahi 1 Prosthesis [prahs-thee-sis] A replacement for a missing body part Golbarg Kolahi 2 Prosthesis In the dental field, it is a fixed or removable appliance replacing
Chapter 12 Prosthodontics Golbarg Kolahi 1 Prosthesis [prahs-thee-sis] A replacement for a missing body part Golbarg Kolahi 2 Prosthesis In the dental field, it is a fixed or removable appliance replacing
AAO Meeting Mutilated Dentition in Aging Population
 AAO Meeting 2018 Mutilated Dentition in Aging Population 1. Introduction & Presentation 2. Anterior Missing Teeth 3. Posterior Missing Teeth 4. Analyze, Visualize and Optimize 5. Case Presentation 6. Challenge
AAO Meeting 2018 Mutilated Dentition in Aging Population 1. Introduction & Presentation 2. Anterior Missing Teeth 3. Posterior Missing Teeth 4. Analyze, Visualize and Optimize 5. Case Presentation 6. Challenge
30/01/2012. Aim. Learning Objectives. Learning Objectives. We know that. Learning Objectives. Diagnosing. Treatment planning.
 Aim Advanced Partial Dentures A contradiction or a true advance? Looking to the Partial denture option Learning Objectives Diagnosing Treatment planning Learning Objectives Expectations have greatly overtaken
Aim Advanced Partial Dentures A contradiction or a true advance? Looking to the Partial denture option Learning Objectives Diagnosing Treatment planning Learning Objectives Expectations have greatly overtaken
Occlusal rehabilitation of posterior fixed prostheses: A clinical report
 J Korean Acad Prosthodont : Volume 39, Number 3, 2001 Occlusal rehabilitation of posterior fixed prostheses: A clinical report In-Sung Yeo, DDS a, and Jae-Ho Yang, DDS, MSD, PhD b College of Dentistry,
J Korean Acad Prosthodont : Volume 39, Number 3, 2001 Occlusal rehabilitation of posterior fixed prostheses: A clinical report In-Sung Yeo, DDS a, and Jae-Ho Yang, DDS, MSD, PhD b College of Dentistry,
Upper and Lower RPD. Increasing VDO? Please Help. Photos in Thread.
 Upper and Lower RPD. Increasing VDO? Please Help. Photos in Thread. A Townie shares a challenging removable case with good feedback Post: 1 of 40 Hello, all Inexperienced dentist (two years since graduation
Upper and Lower RPD. Increasing VDO? Please Help. Photos in Thread. A Townie shares a challenging removable case with good feedback Post: 1 of 40 Hello, all Inexperienced dentist (two years since graduation
Digital Smile Design using the M Proportions and GPS 2D to 3D Digital Facebow: Clinical Case 1
 Digital Smile Design using the M Proportions and GPS 2D to 3D Digital Facebow: Clinical Case 1 Dr Alain Méthot Dr Marco Delcorso A young female patient previously suffering from gastric reflux came to
Digital Smile Design using the M Proportions and GPS 2D to 3D Digital Facebow: Clinical Case 1 Dr Alain Méthot Dr Marco Delcorso A young female patient previously suffering from gastric reflux came to
Tooth preparation for posterior fi xed partial denture (FPD) Tooth preparation for anterior fi xed partial denture (FPD)
 Tooth preparation for anterior fi xed partial denture (FPD)") CHAPTER 17 Tooth preparation for posterior fi xed partial denture (FPD) 1 Defi nition and feature of FPD 2 Actual sequence of tooth preparation for posterior FPD Verify abutment teeth Occlusal guide groove
CHAPTER 17 Tooth preparation for posterior fi xed partial denture (FPD) 1 Defi nition and feature of FPD 2 Actual sequence of tooth preparation for posterior FPD Verify abutment teeth Occlusal guide groove
م.م. طارق جاسم حممد REMOVABLE PARTIAL DENTURE INTRODUCTION
 Lec.1 م.م. طارق جاسم حممد REMOVABLE PARTIAL DENTURE INTRODUCTION االسنان طب Prosthodontics is the branch of dentistry pertaining to the restoration and maintenance of oral function, comfort, appearance,
Lec.1 م.م. طارق جاسم حممد REMOVABLE PARTIAL DENTURE INTRODUCTION االسنان طب Prosthodontics is the branch of dentistry pertaining to the restoration and maintenance of oral function, comfort, appearance,
Occlusion and Attachments
 THE VOICE OF TECHNO-CLINICAL DENTISTRY Occlusion and Attachments The Underlying Scheme for Successful Overdentures Dennis Urban, CDT Vol. 9 No. 4 - April 2010 - Reprint 2 Spectrum dialogue Vol. 9 No. 4
THE VOICE OF TECHNO-CLINICAL DENTISTRY Occlusion and Attachments The Underlying Scheme for Successful Overdentures Dennis Urban, CDT Vol. 9 No. 4 - April 2010 - Reprint 2 Spectrum dialogue Vol. 9 No. 4