Facial Trauma. Rural Emergency Services and Trauma Symposium 2008
|
|
|
- Garey Perkins
- 6 years ago
- Views:
Transcription
1 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Mitchell Stotland, MD Associate Professor of Surgery and Pediatrics Dartmouth-Hitchcock Medical Center Children s Hospital of Dartmouth
2 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Outline of presentation: 5 W s and How: What kinds of injuries? Who should treat these injuries? Where are the injuries best treated? When are they best treated - timeframe? Why is there an indication for referral? How are the injuries best managed on your end?
3 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma What kinds of injuries?: Mechanisms: sports, falls, bites, occupational, altercations, self-inflicted, MVC Tissue or structures involved: skin, fat, sensory/motor nerves, salivary glands, sinuses, eye and lids, lacrimal system, scalp/brow, nose, ears, muscle, bone, teeth Potential effects of trauma: scars, facial deformity, facial numbness or palsy, diplopia, globe malposition, lacrimal obstruction, salivary gland fistula, salivary incontinence, sinus obstruction, compromised nasal and/or oropharygeal airway, speech, dental malocclusion, TMJ ankylosis
4 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Who should treat facial trauma?: ED providers from local/regional/tertiary care hospitals with appropriate experience and expertise Ophthalmology Otolaryngology Oral-Maxillofacial Surgery Plastic Surgery
5 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Where are the injuries best treated?: Emergency department: assuming stable, cooperative patient adequate local anesthetic and/or sedation proper setting (sterility, lighting, pulse-lavage, assistance, etc.) Lacerations, abrasions Skin, scalp, hairline, galea, brow, eyelid, tarsal plate, auricle (including cartilage), nose, lip; traumatic tattoo Fractures Nasal

6 Traumatic tattoo
7 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Where are the injuries best treated?: Operating Room: unstable, uncooperative patient inadequate local anesthetic and/or sedation poor setting (sterility, lighting, pulse-lavage, assistance, etc.) Extensive lacerations, avulsions e.g., scalp avulsion, chain-saw, MVC, gunshot blast, etc. Fractures nasal, frontal, nasoethmoidal, zygomaticomaxillary, Lefort patterns, mandibular
8 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Where are the injuries best treated?: Operating Room: unstable, uncooperative patient inadequate local anesthetic and/or sedation poor setting (sterility, lighting, pulse-lavage, assistance, etc.) Nerve injuries sensory, motor Specialized structures Parotid duct, lacrimal canalicular injuries
9 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma When are the injuries best treated?: Lacerations earlier is better, 8-12 hours or more, depending on circumstances Fractures within first few hours or after 5-7 days (up to 14 days!) Nerve injury sensory: rarely repair early, if at all motor: early is better if high level of suspicion tag! Parotid duct, lacrimal duct earlier is better; explore wound at time of laceration and tag!
10 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Why is there an indication for referral?: Lacerations, Abrasions, Avulsions: within epidermis: steristrip or glue wounds gape only when dermis lacerated traumatic tattoo: pulse-lavage, remove particles what to do with the following? galea, eyebrow, ear and nasal cartilage, eyelid and tarsal plate, lacrimal system, parotid duct, scalp and nasal avulsion
11 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Why is there an indication for referral?: Fractures: Nasal rule out septal hematoma with speculum exam (drain if necessary) many show no evidence of lateral deviation or collapse no surgery antibiotics not required imaging may not be necessary? closed reduction in ED is reasonable option to consider Orbital Floor document visual acuity CT required including thin-cut axial and coronal images diplopia often is transient globe displacement = indication for surgery


12 Orbital floor fracture and diplopia EOM entrapment


13 Orbital floor fracture and enopthalmos pseudoptosis globe positioned caudad and posterior



14 Orbital floor fracture and enopthalmos pseudoptosis enophthalmos

15 Zygomaticomaxillary fracture aka quadripod fracture true fracture path
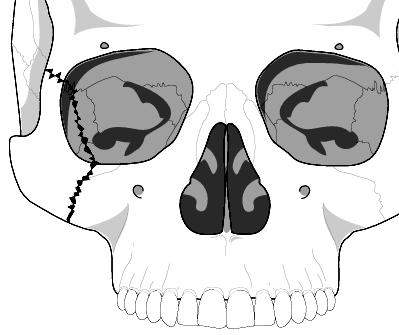
16 Zygomaticomaxillary fracture aka quadripod fracture
17 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Why is there an indication for referral?: Fractures: Zygomaticomaxillary (aka tripod, quadripod, malar ) CT imaging required, fine-cut axial and coronal V2 numbness is characteristic, resolves spontaneously involves orbital floor and lateral wall by definition involves maxillary sinus fracture, by definition not associated with dental malocclusion lower lid may drop laterally antibiotics not required indication for surgery generally is deformity = shared-decision making

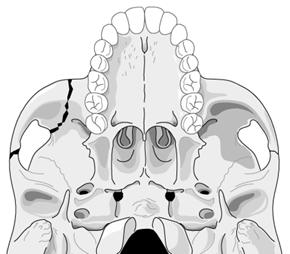
18 Lefort fractures
19 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Why is there an indication for referral?: Fractures: Lefort fractures CT imaging required, fine-cut axial and coronal differentiating I, II, and III clinically document loose and missing teeth blenderized diet antibiotics indicated surgery is required;usually repaired at 5-14 days post-injury

20 Mandible fractures
21 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma Why is there an indication for referral?: Fractures: Mandible CT imaging preferable, fine-cut axial and coronal V3 numbness is characteristic, usu. resolves spontaneously document loose and missing teeth requires analgesia! requires mouthwash (peridex) blenderized diet antibiotics indicated indication for surgery is dental malocclusion (usual) usually repaired at 5-14 days post-injury
22 Rural Emergency Services and Trauma Symposium 2008 Facial Trauma One request regarding facial fractures referrals: Please, no NSAIDs prior to referral!
23 Rural Emergency Services and Trauma Symposium 2008 Common concerns galea is violated eyelid is lacerated +/- some full-thickness lid missing tarsal plate is lacerated eyebrow laceration ear or nasal cartilage involved concern about facial nerve injury open mandible fracture lip laceration parotid duct; lacrimal apparatus how to preserve avulsed tissue? how to preserve avulsed teeth? patient/family wants a plastic surgeon
24 Rural Emergency Services and Trauma Symposium 2008 Common concerns galea is violated no special significance other than very vascular and good layer for a sturdy repair cauterize galea liberally; but be careful cauterizing around hair follicles irrigate and repair with 2-0 or 3-0 PDS/vicryl
25 Rural Emergency Services and Trauma Symposium 2008 Common concerns tarsal plate is injured should be primarily repaired 6-0 or 7-0 vicryl or silk conjunctiva does not need to be repaired since it is firmly adherent to the tarsal plate make sure tarsal sutures do not go thru conj. use silk suture on lid margin and leave ends long and taped to cheek skin to avoid corneal irritation

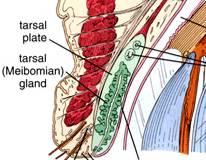
26 Tarsal plate repair
27 Rural Emergency Services and Trauma Symposium 2008 Common concerns eyelid is lacerated, full-thickness is missing <25% of lid missing: repair primarily 25-35%: release lateral canthal ligament and local advancement flap >35-50% more complex flap repair

28 Eyelid defect (70% full-thickness)


29 Eyelid defect (70% full-thickness) tarsoconjunctival flap


30 Eyelid defect (full-thickness) tarsoconjunctival flap
31 Rural Emergency Services and Trauma Symposium 2008 Common concerns eyebrow laceration repair in layers with care to align and orient properly avoid cauterizing follicles avoid turned-in hairs
32 Rural Emergency Services and Trauma Symposium 2008 Common concerns ear or nasal cartilage injury repair cartilage primarily use tapered needle - avoid cheese-wiring cartilage use un-dyed suture: e.g., 4-0 vicryl if cartilage is exposed consider sulfamylon
33 Rural Emergency Services and Trauma Symposium 2008 Common concerns facial nerve injury? if palsy, consider exploring wound if found, tag nerve ends prior to referral frontal and marginal mandib. branches key repair: loupe magnification with 8-0 or 9-0 nylon
34 Facial nerve injury to the frontal branch and marginal mandibular branch most concerning division of the branches of the facial nerve anterior to this line = minimal risk

35 Sensory nerve repair V2 injury
36 Rural Emergency Services and Trauma Symposium 2008 Common concerns open mandible fracture same rules apply oral antibiotics mouthwash analgesia surgery within 5-14 days
37 Rural Emergency Services and Trauma Symposium 2008 Common concerns lip laceration key is to align landmarks philtral columns white roll vermiliocutaneous junction wet-dry line

38 Lip landmarks philtrum column white-roll VC junction wet-dry line
39 Dogbite

40 Dogbite lip switch procedure


41 Dogbite
42 Rural Emergency Services and Trauma Symposium 2008 Common concerns parotid duct injury can lead to salivary fistula know where the location of the duct is if wound is suspicious can consider intubating duct opening intraoral with methylene blue dye
43 Parotid duct The parotid duct lies under the middle third of a line between the tragus and the oral commissure

44 Dogbite (think: parotid duct?)

45 Parotid duct Parotid Duct
46 Cannulating the parotid duct fine catheter passed through parotid duct opening Cut ends of parotid duct
47 Rural Emergency Services and Trauma Symposium 2008 Common concerns lacrimal canalicular injury injury occuring near medial canthus exploring the wound is low-yield if wound is suspicious consider intubating canaliculus with methylene blue dye and 22G angiocath
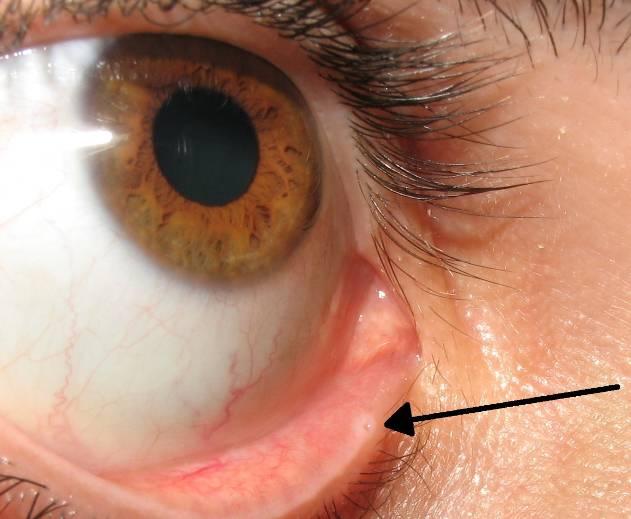
48 Lacrimal canaliculus

49 Lacrimal system
50 Rural Emergency Services and Trauma Symposium 2008 Common concerns how to preserve avulsed teeth? Handle tooth by crown only Attempt reimplantation in the field (if < 1 hour) If unable to reimplant, use carrier media and consult dentist e.g, Hanks solution, milk, saline, saliva, water
51 Rural Emergency Services and Trauma Symposium 2008 Common concerns how to preserve avulsed tissue? sterile, moist, chilled (not frozen)


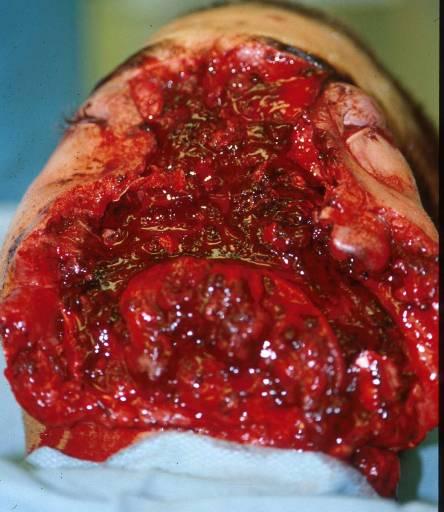
52 Chainsaw accident


53 Chainsaw accident



54 Motor vehicle collision facial avulsion, scalp, lid, nose

55 Motor vehicle collision facial avulsion, scalp, lid, nose




56 Motor vehicle collision facial avulsion, scalp, lid, nose

57 Scalp avulsion


58 Scalp avulsion rule out neck injury first!

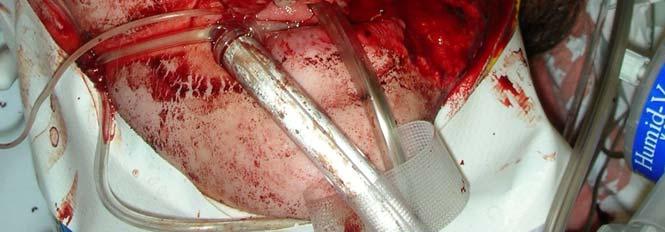
59 Self-inflicted gunshot blast

60 Self-inflicted gunshot blast
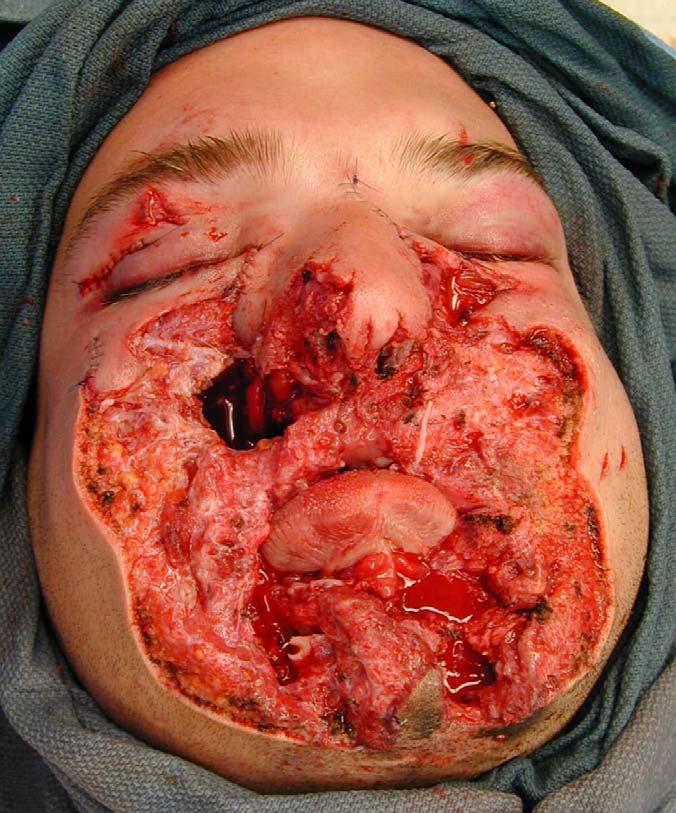
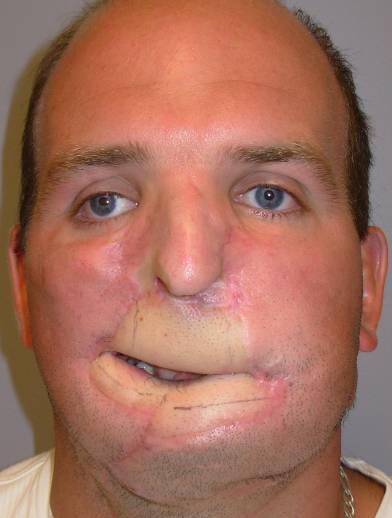
61 Self-inflicted gunshot blast
62 Rural Emergency Services and Trauma Symposium 2008 Common concerns patient/family wants a plastic surgeon!


63 Nasoorbital-ethmoidal fracture
64 Pre/Post Test Questions FACIAL TRAUMA: 1. ideally, within what time frame should a facial fracture be repaired? a 24 hours b 72 hours c 1 week d 2 weeks correct answer is d 2. what are the indications for surgical intervention for a zygomatic fracture? a. diplopia b. facial deformity c. trigeminal (V2) numbness d. dental malocclusion correct answer is b
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery FACIAL FRACTURES
 Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Core Curriculum Syllabus Emergencies in Otolaryngology-Head and Neck Surgery A. General Considerations FACIAL FRACTURES Look for other fractures like skull and/or cervical spine fractures Test function
Maxillofacial and Ocular Injuries
 Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Maxillofacial and Ocular Injuries Objectives At the conclusion of this presentation the participant will be able to: Identify the key anatomical structures of the face and eye and the impact of force on
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line.
 Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
Lesson Plans and Objectives: Review material for article Prep work for article Picture recovery Review for placement on-line. After reading the article, the staff will be able to: Define facial trauma
15. Facial and dental injuries
 15. Facial and dental injuries Priorities in management Best practice is based on current APLS / ATLS guidelines. Maxillofacial injuries will often take a lower priority than other potentially life or
15. Facial and dental injuries Priorities in management Best practice is based on current APLS / ATLS guidelines. Maxillofacial injuries will often take a lower priority than other potentially life or
Maxillofacial Injuries Practical Tips
 Saturday, October 29, 2016 Maxillofacial Injuries Practical Tips Suyash Mohan MD, PDCC THE ROOTS OF PENN RADIOLOGY RADIOLOGICAL Assistant Professor of Radiology Assistant Professor of Neurosurgery Neuroradiology
Saturday, October 29, 2016 Maxillofacial Injuries Practical Tips Suyash Mohan MD, PDCC THE ROOTS OF PENN RADIOLOGY RADIOLOGICAL Assistant Professor of Radiology Assistant Professor of Neurosurgery Neuroradiology
CT of Maxillofacial Fracture Patterns. CT of Maxillofacial Fracture Patterns
 CT of Maxillofacial Fracture Patterns CT of Maxillofacial Fracture Patterns Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology
CT of Maxillofacial Fracture Patterns CT of Maxillofacial Fracture Patterns Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology
Oral and Maxillofacial Surgeons and the seriously injured patient. Barts and The London NHS Trust
 Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
Oral and Maxillofacial Surgeons and the seriously injured patient Barts and The London NHS Trust How do you assess this? Primary Survey A B C D E Airway & Cervical Spine Breathing & Ventilation Circulation
Assessment and Management of Ocular Trauma. Disclosure I have no direct financial interests in today s subject matter. 3/25/2019. Normal Eye Anatomy
 Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Assessment and Management of Ocular Trauma Samiksha Fouzdar Jain, MD,FRCS Department of Ophthalmology & Visual Sciences Truhlsen Eye Institute Disclosure I have no direct financial interests in today s
Face. Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face
 Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Ears. Mouth. Jowls 6 Major Bones of the Face Nasal bone Two
 1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
1 2 3 4 5 Chapter 25 Injuries to the Face, Neck, and Eyes Injuries to the Face and Neck Face and neck are to injury Relatively unprotected positions on body Some injuries are life-threatening. trauma to
CT of Maxillofacial Injuries
 CT of Maxillofacial Injuries Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology changes the diagnosis Technologic Evolution
CT of Maxillofacial Injuries Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Viking 1 1976 MGS 2001 Technology changes the diagnosis Technologic Evolution
Chapter 16. Cosmetic Concerns. Better Blood Supply and Circulation
 Chapter 16 FACIAL LACERATIONS KEY FIGURES: Tissue flap Suture bites: face vs. rest of body Lip anatomy Soft tissue loss The face has several unique properties that dictate the choice of treatment after
Chapter 16 FACIAL LACERATIONS KEY FIGURES: Tissue flap Suture bites: face vs. rest of body Lip anatomy Soft tissue loss The face has several unique properties that dictate the choice of treatment after
Ocular Urgencies and Emergencies
 Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Head and Face Anatomy
 Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
Head and Face Anatomy Epicranial region The Scalp The soft tissue that covers the vault of skull. Extends from supraorbital margin to superior nuchal line. Layers of the scalp S C A L P = skin = connective
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma The face is vital to human appearance and function. Facial injuries can impair a patient
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #1 Facial Trauma The face is vital to human appearance and function. Facial injuries can impair a patient
Principles of Facial Reconstruction After Mohs Surgery
 Objectives Principles of Facial Reconstruction After Mohs Surgery Identify important functional anatomy and aesthetic units of the face. Describe techniques used in facial reconstruction. Discuss postoperative
Objectives Principles of Facial Reconstruction After Mohs Surgery Identify important functional anatomy and aesthetic units of the face. Describe techniques used in facial reconstruction. Discuss postoperative
Ocular and periocular trauma
 Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
TRAUMA TO THE FACE AND MOUTH
 Dr.Yahya A. Ali 3/10/2012 F.I.C.M.S TRAUMA TO THE FACE AND MOUTH Bailey & Love s 25 th edition Injuries to the orofacial region are common, but the majority are relatively minor in nature. A few are major
Dr.Yahya A. Ali 3/10/2012 F.I.C.M.S TRAUMA TO THE FACE AND MOUTH Bailey & Love s 25 th edition Injuries to the orofacial region are common, but the majority are relatively minor in nature. A few are major
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
THIEME. Scalp and Superficial Temporal Region
 CHAPTER 2 Scalp and Superficial Temporal Region Scalp Learning Objectives At the end of the dissection of the scalp, you should be able to identify, understand and correlate the clinical aspects: Layers
CHAPTER 2 Scalp and Superficial Temporal Region Scalp Learning Objectives At the end of the dissection of the scalp, you should be able to identify, understand and correlate the clinical aspects: Layers
MAXILLOFACIAL TRAUMA. The on-call maxillofacial surgeons can be contacted through the switchboard at the Southern General Hospital
 MAXILLOFACIAL TRAUMA The on-call maxillofacial surgeons can be contacted through the switchboard at the Southern General Hospital Mandibular Injuries Mechanism of injury Assault, falls, RTA-Direct trauma
MAXILLOFACIAL TRAUMA The on-call maxillofacial surgeons can be contacted through the switchboard at the Southern General Hospital Mandibular Injuries Mechanism of injury Assault, falls, RTA-Direct trauma
3-Deep fascia: is absent (except over the parotid gland & buccopharngeal fascia covering the buccinator muscle)
") The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Facial Sports Injuries
 Facial Sports Injuries Playing catch, shooting hoops, bicycling on a scenic path or just kicking around a soccer ball have more in common than you may think. On the up side, these activities are good exercise
Facial Sports Injuries Playing catch, shooting hoops, bicycling on a scenic path or just kicking around a soccer ball have more in common than you may think. On the up side, these activities are good exercise
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. Railway accidents injured pedal cyclist
 Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Supplementary Table 1. ICD-9/-10 codes used to identify cycling injury hospitalizations. ICD Code ICD-9 E800-E807(.3) E810-E816, E818-E819(.6) E820-E825(.6) E826-E829(.1) ICD-10-CA V10-V19 (including all
Ocular and Periocular Trauma. Tina Rutar, MD. Assistant Professor of Ophthalmology and Pediatrics. Director, Visual Center for the Child
 Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Ocular and Periocular Trauma Tina Rutar, MD Assistant Professor of Ophthalmology and Pediatrics Director, Visual Center for the Child University of California, San Francisco Phone: 415-353-2560 Fax: 415-353-2468
Imaging Orbit/Periorbital Injury
 Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Imaging Orbit/Periorbital Injury 9 th Nordic Trauma Radiology Course 2016 Stuart E. Mirvis, M.D., FACR Department of Radiology University of Maryland School of Medicine Fireworks Topics to Cover Struts
Facial Trauma. Facial Trauma. Facial Trauma
 Facial Trauma Facial Trauma Brian Bast DMD, MD Department of Oral and Maxillofacial Surgery University of California, San Francisco School of Dentistry Brian Bast DMD, MD Department of Oral and Maxillofacial
Facial Trauma Facial Trauma Brian Bast DMD, MD Department of Oral and Maxillofacial Surgery University of California, San Francisco School of Dentistry Brian Bast DMD, MD Department of Oral and Maxillofacial
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY BUCCINATOR MYOMUCOSAL FLAP The Buccinator Myomucosal Flap is an axial flap, based on the facial and/or buccal arteries. It is a flexible
SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY
 MEDICAL UNIVERSITY OF VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AND SID SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY (State examination) ACADEMIC YEAR 2015 2016 1. Asepsis
MEDICAL UNIVERSITY OF VARNA FACULTY OF DENTAL MEDICINE DEPARTMENT OF ORAL AND MAXILLOFACIAL SURGERY AND SID SYLLABUS OF ORAL AND MAXILLOFACIAL SURGERY (State examination) ACADEMIC YEAR 2015 2016 1. Asepsis
Older age, MVC and TBI higher incidence. Facial fractures a distracting injury? Carotid artery injury. Blindness may occur with facial fractures
 Dr Donald C. DeLisi Jr Oral & Maxillofacial Surgeon Multisystem injury 20 50% Nasal and mandibular fractures most common in community ED s Midface and zygomatic injuries most common in Trauma centers 25%
Dr Donald C. DeLisi Jr Oral & Maxillofacial Surgeon Multisystem injury 20 50% Nasal and mandibular fractures most common in community ED s Midface and zygomatic injuries most common in Trauma centers 25%
ZYGOMATIC (MALAR) FRACTURES
 FRACTURES") b854_chapter-12.qxd 1/31/2011 9:40 AM Page 129 ZYGOMATIC (MALAR) FRACTURES CHAPTER 12 Anatomical articulations FZ Fronto-zygomatic ZT Zygomaticotemporal ZMB Zygomatico - maxillary buttress IO Infraorbital
b854_chapter-12.qxd 1/31/2011 9:40 AM Page 129 ZYGOMATIC (MALAR) FRACTURES CHAPTER 12 Anatomical articulations FZ Fronto-zygomatic ZT Zygomaticotemporal ZMB Zygomatico - maxillary buttress IO Infraorbital
Facial and Temporal Bone Trauma Diagnostic imaging and therapeutic challenges in emergency
 Facial and Temporal Bone Trauma Diagnostic imaging and therapeutic challenges in emergency ATTYE A, KRAINIK A Department of Neuroradiology and MRI University Hospital Grenoble / University Grenoble Alpes
Facial and Temporal Bone Trauma Diagnostic imaging and therapeutic challenges in emergency ATTYE A, KRAINIK A Department of Neuroradiology and MRI University Hospital Grenoble / University Grenoble Alpes
Both the major and minor glands have ducts, which are the channels down which the saliva travels on its way to the mouth.
 What and where are salivary glands? make the saliva in your mouth, which is very important for the health of your mouth and teeth (eg it stops your mouth drying out) - and also for the first stages of
What and where are salivary glands? make the saliva in your mouth, which is very important for the health of your mouth and teeth (eg it stops your mouth drying out) - and also for the first stages of
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Oral and Maxillofacial Surgery Privileges REAPPOINTMENT Effective from July 1, 2015 to June 30, 2016
 Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the Health Authority or Hospital, effective: 11/Dec/2014.
Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the Health Authority or Hospital, effective: 11/Dec/2014.
Remember from the first year embryology Trilaminar disc has 3 layers: ectoderm, mesoderm, and endoderm
 Development of face Remember from the first year embryology Trilaminar disc has 3 layers: ectoderm, mesoderm, and endoderm The ectoderm forms the neural groove, then tube The neural tube lies in the mesoderm
Development of face Remember from the first year embryology Trilaminar disc has 3 layers: ectoderm, mesoderm, and endoderm The ectoderm forms the neural groove, then tube The neural tube lies in the mesoderm
Management of Lid Lacerations
 Ocular Ocular Trauma Management of Lid Lacerations Nitin Vichare MS, DNB, FAICO Nitin Vichare MS, DNB,FAICO Dept. of Ophthalmology, Command Hospital, (Southern Command), Pune, Maharashtra Eyelids are not
Ocular Ocular Trauma Management of Lid Lacerations Nitin Vichare MS, DNB, FAICO Nitin Vichare MS, DNB,FAICO Dept. of Ophthalmology, Command Hospital, (Southern Command), Pune, Maharashtra Eyelids are not
UC SF. g h. Eye Trauma. Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California
 UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
Management of Extensive Maxillofacial Trauma With Bony Foreign Body Within the Orbit From a Chainsaw Injury
 Management of Extensive Maxillofacial Trauma With Bony Foreign Body Within the Orbit From a Chainsaw Injury Randall O. Craft, MD, a Kyle R. Eberlin, MD, a Michael H. Stella, MD, b and Edward J. Caterson,
Management of Extensive Maxillofacial Trauma With Bony Foreign Body Within the Orbit From a Chainsaw Injury Randall O. Craft, MD, a Kyle R. Eberlin, MD, a Michael H. Stella, MD, b and Edward J. Caterson,
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Facial Trauma ASHNR. Disclosures: Acknowledgments: None. Edward P. Quigley, III, MD PhD University of Utah
 Disclosures: Facial Trauma ASHNR Edward P. Quigley, III, MD PhD University of Utah None Acknowledgments: Dr. Rebecca Cornelius Dr. Ilona M. Schmalfuss Dr. Richard Wiggins III Dr. Yoshimi Anzai Dr. Lindell
Disclosures: Facial Trauma ASHNR Edward P. Quigley, III, MD PhD University of Utah None Acknowledgments: Dr. Rebecca Cornelius Dr. Ilona M. Schmalfuss Dr. Richard Wiggins III Dr. Yoshimi Anzai Dr. Lindell
Eye Trauma. Lid Laceration. Orbital Fracture
 Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
Eye Trauma Lid Laceration The presence of a lid laceration, however insignificant, mandates careful exploration of the wound and examination of the globe. 1. Superficial lacerations parallel to the lid
MAXILLOFACIAL TRAUMATOLOGY Department of Maxillofacial Surgery Semmelweis University, Budapest. Dr. Huszár Tamás
 MAXILLOFACIAL TRAUMATOLOGY Department of Maxillofacial Surgery Semmelweis University, Budapest Dr. Huszár Tamás Maxillofacial injuries isolated maxillofacial injury multiple injuries polytrauma (injury
MAXILLOFACIAL TRAUMATOLOGY Department of Maxillofacial Surgery Semmelweis University, Budapest Dr. Huszár Tamás Maxillofacial injuries isolated maxillofacial injury multiple injuries polytrauma (injury
Face and Throat Injuries. Chapter 26
 Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Face and Throat Injuries Chapter 26 Anatomy of the Head Landmarks of the Neck Injuries to the Face Injuries around the face can lead to upper airway obstructions. Bleeding from the face can be profuse.
Property Latmedical, LLC.
 Dr. Goed provides a complete and innovate product portfolio solution to the growing healthcare need within the field of non-invasive orthopedics, sports medicine, bandaging, wound care and compression
Dr. Goed provides a complete and innovate product portfolio solution to the growing healthcare need within the field of non-invasive orthopedics, sports medicine, bandaging, wound care and compression
1 Eyelids. Lacrimal Apparatus. Orbital Region. 3 The Orbit. The Eye
 1 1 Eyelids Orbital Region 2 Lacrimal Apparatus 3 The Orbit 4 The Eye 2 Eyelids The eyelids protect the eye from injury and excessive light by their closure. The upper eyelid is larger and more mobile
1 1 Eyelids Orbital Region 2 Lacrimal Apparatus 3 The Orbit 4 The Eye 2 Eyelids The eyelids protect the eye from injury and excessive light by their closure. The upper eyelid is larger and more mobile
Epidemiology 3002). Epidemiology and Pathophysiology
. Epidemiology and Pathophysiology") Epidemiology Maxillofacial trauma or injuries are commonly encountered in the practice of emergency medicine and are presenting one of the most challenging problems to the attending surgeons or physicians
Epidemiology Maxillofacial trauma or injuries are commonly encountered in the practice of emergency medicine and are presenting one of the most challenging problems to the attending surgeons or physicians
PTERYGOPALATINE FOSSA
 PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
The diagnostic value of Computed Tomography in evaluation of maxillofacial Trauma
 The diagnostic value of Computed Tomography in evaluation of maxillofacial Trauma Qais H. Muassa FICMS College of Dentistry, Babylon University Ibrahim S. Gataa, BDS, FICMS College of Dentistry, Sulaimania
The diagnostic value of Computed Tomography in evaluation of maxillofacial Trauma Qais H. Muassa FICMS College of Dentistry, Babylon University Ibrahim S. Gataa, BDS, FICMS College of Dentistry, Sulaimania
Chapter 7: Head & Neck
 Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
NASOLACRIMAL DUCT OBSTRUCTION (BLOCKED TEAR DUCT) AND TEARY EYE - PATIENT INFORMATION
 AND TEARY EYE - PATIENT INFORMATION") NASOLACRIMAL DUCT OBSTRUCTION (BLOCKED TEAR DUCT) AND TEARY EYE - PATIENT INFORMATION What is lacrimal sac and nasolacrimal duct? The lacrimal apparatus is composed of a lacrimal gland (tear producing
NASOLACRIMAL DUCT OBSTRUCTION (BLOCKED TEAR DUCT) AND TEARY EYE - PATIENT INFORMATION What is lacrimal sac and nasolacrimal duct? The lacrimal apparatus is composed of a lacrimal gland (tear producing
Technique Guide. Titanium Wire with Barb and Needle. Surgical Technique Guide for Canthal Tendon Prodecures.
 Technique Guide Titanium Wire with Barb and Needle. Surgical Technique Guide for Canthal Tendon Prodecures. Indications/Features Indications The Synthes Titanium Wire with Barb and straight Needle is
Technique Guide Titanium Wire with Barb and Needle. Surgical Technique Guide for Canthal Tendon Prodecures. Indications/Features Indications The Synthes Titanium Wire with Barb and straight Needle is
Repair of Eyelid Trauma
 Repair of Eyelid Trauma Yunia Irawati, MD Plastic Reconstruction Division, Department of Ophthalmology FKUI / RSCM Introduction Eyelid trauma defined as a trauma to external surface of the lids with or
Repair of Eyelid Trauma Yunia Irawati, MD Plastic Reconstruction Division, Department of Ophthalmology FKUI / RSCM Introduction Eyelid trauma defined as a trauma to external surface of the lids with or
Consumer summary. Endoscopic modified Lothrop procedure for the. treatment of chronic frontal sinusitis
 ASERNIP S Australian Safety and Efficacy Register of New Interventional Procedures Surgical Consumer summary Endoscopic modified Lothrop procedure for the treatment of chronic frontal sinusitis (The report
ASERNIP S Australian Safety and Efficacy Register of New Interventional Procedures Surgical Consumer summary Endoscopic modified Lothrop procedure for the treatment of chronic frontal sinusitis (The report
Anatomy and Physiology. Bones, Sutures, Teeth, Processes and Foramina of the Human Skull
 Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
Titanium Wire with Barb and Needle. Surgical Technique Guide for Canthal Tendon Procedures.
 Titanium Wire with Barb and Needle. Surgical Technique Guide for Canthal Tendon Procedures. Technique Guide This publication is not intended for distribution in the USA. Instruments and implants approved
Titanium Wire with Barb and Needle. Surgical Technique Guide for Canthal Tendon Procedures. Technique Guide This publication is not intended for distribution in the USA. Instruments and implants approved
Tikrit University College of Dentistry Dr.Ban I.S. head & neck anatomy 2 nd y.
 Lec [3]/The scalp The scalp extends from the supraorbital margins anteriorly to the nuchal lines at the back of the skull and down to the temporal lines at the sides. The forehead, from eyebrows to hairline,
Lec [3]/The scalp The scalp extends from the supraorbital margins anteriorly to the nuchal lines at the back of the skull and down to the temporal lines at the sides. The forehead, from eyebrows to hairline,
Head and Neck Examination
 Head and Neck Examination Statement of Goals Understand and perform an examination of the head and neck. Learning Objectives Head Ears Nose Sinus A. Describe the anatomy of the head, including regions
Head and Neck Examination Statement of Goals Understand and perform an examination of the head and neck. Learning Objectives Head Ears Nose Sinus A. Describe the anatomy of the head, including regions
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI. Monitor the vital signs. Monitor the vital signs. Complications of Facial Traumas.
 Complications of Facial Traumas 1) Immediate Complications 2) Late Complications Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI Assistant Professor Oral & Maxillofacial Surgeon Taibah University Monitor
Complications of Facial Traumas 1) Immediate Complications 2) Late Complications Dr. Esam Ahmad Z. Omar BDS, MSc-OMFS, FFDRCSI Assistant Professor Oral & Maxillofacial Surgeon Taibah University Monitor
CHAPTER 8 SECTION 1.4 ORAL SURGERY TRICARE/CHAMPUS POLICY MANUAL M DEC 1998 SPECIAL BENEFIT INFORMATION
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
Wound Repair. Epidemiology. History. Location of Injuries Face/Scalp Extremities. Legal Risk Missed FB and Fx Infection
 Wound Repair Edwin W. Schaefer, DNP, R.N. - FNP Emergency Nurse Practitioner Epidemiology Location of Injuries Face/Scalp Extremities Legal Risk Missed FB and Fx Infection History Mechanism of Injury Associated
Wound Repair Edwin W. Schaefer, DNP, R.N. - FNP Emergency Nurse Practitioner Epidemiology Location of Injuries Face/Scalp Extremities Legal Risk Missed FB and Fx Infection History Mechanism of Injury Associated
EYE INJURIES OBJECTIVES COMMON EYE EMERGENCIES 7/19/2017 IMPROVE ASSESSMENT OF EYE INJURIES
 EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Dr. Sami Zaqout Faculty of Medicine IUG
 The Nose External Nose Nasal Cavity External Nose Blood and Nerve Supplies of the External Nose Blood Supply of the External Nose The skin of the external nose Branches of the ophthalmic and the maxillary
The Nose External Nose Nasal Cavity External Nose Blood and Nerve Supplies of the External Nose Blood Supply of the External Nose The skin of the external nose Branches of the ophthalmic and the maxillary
Maxilla, ORBIT and infratemporal fossa. Neophytos C Demetriades MD, DDS, MSc Associate professor European University of Cyprus School of Medicine
 Maxilla, ORBIT and infratemporal fossa Neophytos C Demetriades MD, DDS, MSc Associate professor European University of Cyprus School of Medicine MAXILLA Superior, middle, and inferior meatus Frontal sinus
Maxilla, ORBIT and infratemporal fossa Neophytos C Demetriades MD, DDS, MSc Associate professor European University of Cyprus School of Medicine MAXILLA Superior, middle, and inferior meatus Frontal sinus
This is the largest of the three major glands. It lies partly in the front of the lower half of the ear and partly below the earlobe.
 Parotid Gland Lumps The lining of the mouth contains many small saliva glands. In addition there are three major glands on each side of the face, the parotid, submandibular and sublingual glands. The Parotid
Parotid Gland Lumps The lining of the mouth contains many small saliva glands. In addition there are three major glands on each side of the face, the parotid, submandibular and sublingual glands. The Parotid
DENTAL TRAUMA IN DECIDUOUS TEETH
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Dental Trauma in Deciduous Teeth must be made in conjunction with
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of Dental Trauma in Deciduous Teeth must be made in conjunction with
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL MP.138.MH Oral Maxillofacial Prosthesis This policy applies to the following lines of business: MedStar Employee (Select) MedStar MA DSNP CSNP MedStar CareFirst
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL MP.138.MH Oral Maxillofacial Prosthesis This policy applies to the following lines of business: MedStar Employee (Select) MedStar MA DSNP CSNP MedStar CareFirst
CHAPTER 17 FACIAL AESTHETIC SURGERY. Christopher C. Surek, DO and Mohammed S. Alghoul, MD. I. BROW LIFT (Figures 1 and 2)
") CHAPTER 17 FACIAL AESTHETIC SURGERY Christopher C. Surek, DO and Mohammed S. Alghoul, MD I. BROW LIFT (Figures 1 and 2) A. Open Coronal Brow Lift Technique 1. Coronal incision is made in the hair-bearing
CHAPTER 17 FACIAL AESTHETIC SURGERY Christopher C. Surek, DO and Mohammed S. Alghoul, MD I. BROW LIFT (Figures 1 and 2) A. Open Coronal Brow Lift Technique 1. Coronal incision is made in the hair-bearing
Clues of a Ruptured Globe
 Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Definition any eye that has sustained a full thickness traumatic disruption of the cornea or sclera Overwhelmingly, rupture accidents occur in young men, small children and the elderly Corneal laceration
Diagnosis of Midface Fractures with CT: What the Surgeon Needs to Know 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. EDUCATION EXHIBIT
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. EDUCATION EXHIBIT
cally, a distinct superior crease of the forehead marks this spot. The hairline and
 4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
4 Forehead The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The
Case Report Reconstruction of Total Lower Eyelid Defects with the Temporoparietal Fascial Flap
 Volume 2012, Article ID 927260, 4 pages doi:10.1155/2012/927260 Case Report Reconstruction of Total Lower Eyelid Defects with the Temporoparietal Fascial Flap Simon R. Bababeygy, 1 Anne R. Kao, 1 Niels
Volume 2012, Article ID 927260, 4 pages doi:10.1155/2012/927260 Case Report Reconstruction of Total Lower Eyelid Defects with the Temporoparietal Fascial Flap Simon R. Bababeygy, 1 Anne R. Kao, 1 Niels
Trauma Series: FACIAL INJURIES
 Trauma Series: FACIAL INJURIES Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and
Trauma Series: FACIAL INJURIES Jassin M. Jouria, MD Dr. Jassin M. Jouria is a medical doctor, professor of academic medicine, and medical author. He graduated from Ross University School of Medicine and
Eyes, ears, teeth and everything in between
 Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Chapter 7 Part A The Skeleton
 Chapter 7 Part A The Skeleton Why This Matters Understanding the anatomy of the skeleton enables you to anticipate problems such as pelvic dimensions that may affect labor and delivery The Skeleton The
Chapter 7 Part A The Skeleton Why This Matters Understanding the anatomy of the skeleton enables you to anticipate problems such as pelvic dimensions that may affect labor and delivery The Skeleton The
Management of Craniofacial injuries
 Management of Craniofacial injuries Plastic and Reconstructive Surgery Cirujanos PlástiKos Mundi Cranio-Facial Trauma 1. Introduction Cranio-facial trauma is as old as the human race. What has changed
Management of Craniofacial injuries Plastic and Reconstructive Surgery Cirujanos PlástiKos Mundi Cranio-Facial Trauma 1. Introduction Cranio-facial trauma is as old as the human race. What has changed
The sebaceous glands (glands of Zeis) open directly into the eyelash follicles, ciliary glands (glands of Moll) are modified sweat glands that open
 open directly into the eyelash follicles, ciliary glands (glands of Moll) are modified sweat glands that open") The Orbital Region The orbits are a pair of bony cavities that contain the eyeballs; their associated muscles, nerves, vessels, and fat; and most of the lacrimal apparatus upper eyelid is larger and more
The Orbital Region The orbits are a pair of bony cavities that contain the eyeballs; their associated muscles, nerves, vessels, and fat; and most of the lacrimal apparatus upper eyelid is larger and more
CONSENT FOR RHINOPLASTY, SEPTOPLASTY AND TURBINATES
 CONSENT FOR RHINOPLASTY, SEPTOPLASTY AND TURBINATES Surgery of the nose (rhinoplasty) is an operation frequently performed by plastic surgeons. This surgical procedure can produce changes in the appearance,
CONSENT FOR RHINOPLASTY, SEPTOPLASTY AND TURBINATES Surgery of the nose (rhinoplasty) is an operation frequently performed by plastic surgeons. This surgical procedure can produce changes in the appearance,
be very thin and variable. Facial nerve branches that exit the parotid gland are deep to the SMAS.
 The Superficial musculoaponeurotic system (SMAS) fascia is a fanlike fascia that envelops the face and provides a suspensory sheet which distributes forces of facial expression.. The SMAS is continuous
The Superficial musculoaponeurotic system (SMAS) fascia is a fanlike fascia that envelops the face and provides a suspensory sheet which distributes forces of facial expression.. The SMAS is continuous
DELINEATION OF PRIVILEGES - ORAL AND MAXILLOFACIAL SURGERY
 KALEIDA HEALTH Name Date DELINEATION OF PRIVILEGES - ORAL AND MAXILLOFACIAL SURGERY PLEASE NOTE: Please check the box for each privilege requested. Do not use an arrow or line to make selections. We will
KALEIDA HEALTH Name Date DELINEATION OF PRIVILEGES - ORAL AND MAXILLOFACIAL SURGERY PLEASE NOTE: Please check the box for each privilege requested. Do not use an arrow or line to make selections. We will
PRE-OP and POST-OP SURGICAL CONSIDERATIONS
 PRE-OP and POST-OP SURGICAL CONSIDERATIONS Darlene Sorrell, DMD, is not an oral surgeon. AIDC is an out-patient facility. 29 years of experience in IHS. Advanced General Practice Residency. No access
PRE-OP and POST-OP SURGICAL CONSIDERATIONS Darlene Sorrell, DMD, is not an oral surgeon. AIDC is an out-patient facility. 29 years of experience in IHS. Advanced General Practice Residency. No access
with laser resurfacing, 36, 37 Cryotherapy, lower eyelid cicatricial ectropion after, 151 Cutler-Beard flap. See Fullthickness
 INDEX A Abrasion, from silicone tubing, 230 Acquired immunodeficiency syndrome, eyelid tumor with, 193 AIDS. See Acquired immunodeficiency syndrome Anatomy, eyelid, 155 156 Aneurysm, cerebral, Muller s
INDEX A Abrasion, from silicone tubing, 230 Acquired immunodeficiency syndrome, eyelid tumor with, 193 AIDS. See Acquired immunodeficiency syndrome Anatomy, eyelid, 155 156 Aneurysm, cerebral, Muller s
The Orbit. The Orbit OCULAR ANATOMY AND DISSECTION 9/25/2014. The eye is a 23 mm organ...how difficult can this be? Openings in the orbit
 The eye is a 23 mm organ...how difficult can this be? OCULAR ANATOMY AND DISSECTION JEFFREY M. GAMBLE, OD COLUMBIA EYE CONSULTANTS OPTOMETRY & UNIVERSITY OF MISSOURI DEPARTMENT OF OPHTHALMOLOGY CLINICAL
The eye is a 23 mm organ...how difficult can this be? OCULAR ANATOMY AND DISSECTION JEFFREY M. GAMBLE, OD COLUMBIA EYE CONSULTANTS OPTOMETRY & UNIVERSITY OF MISSOURI DEPARTMENT OF OPHTHALMOLOGY CLINICAL
ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section. REVIEW SHEET Exercise 10 Axial Skeleton
 ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section REVIEW SHEET Exercise 10 Axial Skeleton 1 POINT EACH. THE SKULL MULTIPLE CHOICE 1. The major components of the axial skeleton include the 7. The
ANATOMY & PHYSIOLOGY I Laboratory Version B Name Section REVIEW SHEET Exercise 10 Axial Skeleton 1 POINT EACH. THE SKULL MULTIPLE CHOICE 1. The major components of the axial skeleton include the 7. The
Bundeswehrkrankenhaus Ulm Abteilung HNO Kopf-Halschirurgie
 Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
Kai Johannes Lorenz and Klaus Effinger Department of Otorhinolaryngology, Head and Neck Surgery Department of Radiology and interventional Radiology German Armed Forces Hospital Incidence of hemorrhage
70480 CT Orbit, et al without contrast CAT 9023
 70480 CT Orbit, et al without contrast CAT 9023 190.0 MALIG NEO EYEBALL 190.1 MALIG NEO ORBIT 190.2 MALIG NEO LACRIMALIG GLAND 190.9 MALIG NEO EYE UNSPEC 224.1 BENIGN NEO ORBIT 360.51 FB MAGNET ANT CHAMB
70480 CT Orbit, et al without contrast CAT 9023 190.0 MALIG NEO EYEBALL 190.1 MALIG NEO ORBIT 190.2 MALIG NEO LACRIMALIG GLAND 190.9 MALIG NEO EYE UNSPEC 224.1 BENIGN NEO ORBIT 360.51 FB MAGNET ANT CHAMB
Maxillary and Periorbital Fractures January 2004
 TITLE: Maxillary and Periorbital Fractures SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 7, 2004 RESIDENT PHYSICIAN: Gordon Shields, MD FACULTY ADVISOR: Francis B. Quinn,
TITLE: Maxillary and Periorbital Fractures SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 7, 2004 RESIDENT PHYSICIAN: Gordon Shields, MD FACULTY ADVISOR: Francis B. Quinn,
LOCAL ANESTHESIA IN PEDIATRIC DENTISTRY
 Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of local anesthesia in pediatric dentistry must be made in conjunction
Disclaimer This movie is an educational resource only and should not be used to manage your health. All decisions about the management of local anesthesia in pediatric dentistry must be made in conjunction
COMPLICATIONS IN ENDOSCOPIC SINUS SURGERY
 COMPLICATIONS IN ENDOSCOPIC SINUS SURGERY John M. DelGaudio, MD Professor and Vice Chair Chief of Rhinology and Sinus Surgery Department of Otolaryngology-Head and Neck Surgery Emory University School
COMPLICATIONS IN ENDOSCOPIC SINUS SURGERY John M. DelGaudio, MD Professor and Vice Chair Chief of Rhinology and Sinus Surgery Department of Otolaryngology-Head and Neck Surgery Emory University School
INFORMATION REGARDING YOUR NASAL SURGERY
 INFORMATION REGARDING YOUR NASAL SURGERY This document contains information about the following aspects of nasal surgery: Pre-op information: How to prepare for surgery. Procedure: Wat is done during surgery.
INFORMATION REGARDING YOUR NASAL SURGERY This document contains information about the following aspects of nasal surgery: Pre-op information: How to prepare for surgery. Procedure: Wat is done during surgery.
Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus
 Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
The Scalp and Face Protocol. Julie Goodwin, BA, LMT
 The Scalp and Face Protocol Julie Goodwin, BA, LMT The Scalp and Face Protocol Julie Goodwin, BA, LMT Julie Goodwin 2014 2 Agenda Pertinent Anatomy and Physiology Treatment Planning Strokes, Techniques
The Scalp and Face Protocol Julie Goodwin, BA, LMT The Scalp and Face Protocol Julie Goodwin, BA, LMT Julie Goodwin 2014 2 Agenda Pertinent Anatomy and Physiology Treatment Planning Strokes, Techniques