Στοματική κοιλότητα και IBD
|
|
|
- Harry Nichols
- 6 years ago
- Views:
Transcription
1 Στοματική κοιλότητα και IBD Κωνσταντίνος Χ. Κατσάνος Ιωάννινα, Ιούνιος 2016
2 Στοματική κοιλότητα και IBD ΚΑΛΟΗΘΕΙΣ ΕΚΔΗΛΩΣΕΙΣ ΠΡΟ-ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ
3 ΚΑΛΟΗΘΕΙΣ ΕΚΔΗΛΩΣΕΙΣ
4 ΙBD & ΣΤΟΜΑΤΚΗ ΚΟΙΛΟΤΗΤΑ A significant proportion of patients may have one or more manifestations in the oral cavity and in the perioral skin area. The prevalence of oral lesions in IBD has been reported to range from 5-50%. oral lesions are more common in CD as compared to UC more prevalent in children as compared to adults.
5 ΙBD & ΣΤΟΜΑΤΚΗ ΚΟΙΛΟΤΗΤΑ Oral manifestations may be associated with the disease itself with nutritional deficiencies with complications from therapy. may precede IBD diagnosis may or not be associated with active disease may involve any part of the oral cavity They may cause significant symptoms and disability
6 ΙBD & ΣΤΟΜΑΤΚΗ ΚΟΙΛΟΤΗΤΑ two common clinical scenarios: 1) oral lesions associated with altered bowel habits 2) established IBD but complaining of new oral lesions.
7 Oral lesions in CD Oral lesions have a prevalence rate between 20-50%. higher in proximal gastrointestinal tract and/or perianal involvement. Aphthous ulcers, the most common preceding GI symptoms in 5%-10% of patients.
8 Oral lesions in children with CD The highest reported rate almost 50% 30% may continue to manifest oral lesions despite intestinal disease control. Paediatric doctors and dentists play a critical role
9 Oral manifestations in UC Aphthous ulcers in 10% of UC. in pediatric patients with UC in up one third and are usually non-specific.
10 DIAGNOSIS OF ORAL LESIONS IN IBD Oral lesions in IBD can be specific non-specific
11 Table Specific and non-specific oral changes in patients with IBD. 1.Specific oral changes or lesions Description Orofacial Crohn s disease Granular cheilitis Pyostomatitis vegetans 2. Non-specific oral changes or lesions -Oral cavity changes -Lip changes -Malabsorption-related oral changes or lesions Folic acid deficiency Iron deficiency Zinc deficiency Vitamin A deficiency Vitamin B complex deficiency Vitamin C deficiency Vitamin K deficiency -Medication-related oral changes or lesions Adalimumab Azathioprine Budesonide Certolizumab pegol Cholestyramine Cyclosporin Ciprofloxacin Infliximab Loperamide Mesalazine Methotrexate Metronidazole (Methyl)prednisolone Mycophenolate mofetil Sulphasalazine Mostly young patients with Crohn s Mostly in Crohn s disease In ulcerative colitis and in Crohn s Ulcers, cobblestonning, swelling, abscesses, tags, tongue changes, gingival changes etc. cheilitis, swelling, redness, scaling, fissures, ulcers Glossitis and/or cheilitis Glossitis and/or cheilitis Oral candidiasis, glossitis Oral white patches/keratinization Stomatitis, glossitis, angular cheilitis, burning mouth syndrome, reduced or altered taste Scurvy Gum and/or oral cavity bleeding Infections, angioedema, paradoxical reactions Sicca syndrome Glossitis, dry mouth Angioedema, Stevens-Jonhson syndrome/toxic epidermal necrolyis, paradoxical reactions Glossitis, altered taste,dental changes, gum bleeding Gingivitis, gum hyperplasia Angioedema,Stevens-Jonhson syndrome/ Toxic epidermal necrolyis, oral candidiasis, loss of taste Infections, angioedema, paradoxical reactions Angioedema, Stevens-Jonhson syndrome/ toxic epidermal necrolyis, dry mouth Stomatitis, dry mouth, altered taste Stomatitis, gingivitis Metallic taste, glossitis, stomatitis, candidiasis, dry mouth Oral candidiasis Sicca syndrome Angioedema, stomatitis, Stevens-Jonhson syndrome/toxic epidermal necrolyis, altered taste
12 Table Clinical signs of oral involvement in IBD by oral anatomic location. Oral involvement in IBD Orofacial Crohn disease Oral mucosa [masticatory or lining (labial / buccal)] Lip(s) Gingiva Hard palate Teeth Tongue Tonsills Salivary glands Clinical Signs One or more clinical signs of spectrum: perioral erythema, metastatic Crohn s of skin of the face with ulcers, facial swelling, mucosal tags, deep linear ulcers, cobblestoning, lip swelling or fissuring, granulomatous cheilitis, mucogingivitis, papules, nodules, plaques or persistent swelling. abscesses (mostly in buccal space) aphthous lesions (minor or major) aphthous stomatitis circumferential ulcers cobblestoning, cobblestone plaques diffuse oral edema fissures IgA pustulosis, leukoplakia, hairy leukoplakia linear ulcers,lumps mucosal tags,permanent maloformartions / scarring pseudopolyps polypoid lesions,pyostomatitis vegetans swelling and induration angular cheilitis fissuring, induration granulomatous cheilitis,macrocheilia with or without fissuring neoformations of the genian mucosa (papilloma,fibroma),swelling non specific gingivitis hyperplastic granular gingivitis palatal ulcer(s) parodontal lesions paraodontosis reduction of the alveolar bony tissue erosions glossitis ulcers granulomatous tonsillitis tonsillar granulomas Fistula,granulomatous inflammation, minor salivary gland enlargement reduced salivation sicca syndrome
13 Table Oral symptoms in patients with inflammatory bowel disease. Dental symptoms Oral symptoms Discomfort, pain, infections, dental caries, decay, periodontal involvement dry mouth (sicca syndrome), reduced salivation,difficulty in speaking and/or swallowing, halitosis Gingiva Lip changes Oral mucosa changes Perioral skin changes Lymphadenopathy Tongue changes gingival hypertrophy, swelling, pain, bleeding swelling, macrocheilia, redness, scaling, fissures ulcer(s), cobblestoning, polypoid tags, buccal swelling, leukoplakia, mucosal discoloration perioral erythema with scaling, erythema migrans, swelling, malformations, scarring persistent submandibular lymphadenopathy painful tongue, glossitis in top or lateral or whole tongue, hairy tongue, metallic dysgeusia
14 Table Differential diagnosis of oral aphthous and oral granulomatous lesions in patients with inflammatory bowel disease. Oral aphthous or ulcerous or edematous lesions Recurrent aphthous stomatitis (RAS) Autoimmune rheumatic diseases (Reiter's syndrome, systemic lupus erythematosus, Adamandiadis-Behcet's syndrome) Autoimmune bullous diseases, cicatricial pemphigoid, pemphigus vulgaris, epidermolysis bullosa acquisita Infections (mucobacterial, systemic fungal infections, parasites, sexually transmitted infections, herpetic gingivostomatitis, CMV, Coxsackie, oral histoplasmosis) Oral staphylococcal (S. aureus) mucositis Lymphatic edema, lymphangioma, vascular edema, Neutropenias Desquamative gingivitis Precancerous lesions (lichen planus) Cancer (mouth T-cell lymphoma) Oral granulomatous lesions Orofacial granulomatosis (OFG) Melkersson-Rosenthal syndrome Cheilitis granulomatosa (Miescher cheilitis) Foreign body reaction-sarcoid-like (Polishing-paste-induced silica granuloma, delayed hypersensitivity to cobalt, oral cavity piercing) Sarcoidosis Sjögren syndrome Wegener s granulomatosis Tuberculosis Tuberculoid leprosy Traumas and Allergies
15 Spectrum of oral manifestations and lesions in inflammatory bowel disease Crohn s disease Ulcerative colitis Highly specific - Metastatic -Orofacial -Granulomatous cheilitis Highly suspicious -Tag-like lesions -Cobblestoning -Mucogingivitis -Lip swelling & vertical fissuring -Deep linear oral ulcers (buccal sulci) Non-specific oral lesions In IBD and non-ibd patients -Malabsorption related -Medication related -Other Highly specific -pyostomatitis vegetans
16 a. Highly specific oral lesions Highly specific oral lesions are almost pathognomonic for IBD diagnosis orofacial and granulomatous cheilitis in CD pyostomatitis vegetans in UC and CD
17 Orofacial Crohn s disease oral ulcers and cobblestoning appearance in the mouth of patients with CD CD of the mouth. Orofacial CD is a specific manifestation of CD (5-15% ) relapsing aphthous ulceration with coexisting edema of the oral cavity and of the lips Usually the bowel disease develops within a few months of the orofacial condition, but delays of up to nine years have also been reported.

18

19

20
21 Orofacial Crohn s disease Orofacial CD is clinically and histologically indistinguishable from orofacial granulomatosis (OFG), which occurs in the absence of any bowel disease. OFG encompasses two conditions: Granulomatous cheilitis (or Miescher cheilitis or cheilitis granulomatosa) Melkersson-Rosenthal syndrome

22

23
24 Orofacial granulomatosis Granulomatous cheilitis Melkerson-Rosenthal syndrome Other causes (i.e sarcoidosis, allergy) Orofacial Crohn s (preceeding bowel symptoms) Orofacial Crohn s (extraintestinal manifestation) Absence of bowel disease Bowel disease
25 Granulomatous cheilitis Granulomatous cheilitis (or cheilitis granulomatosa or Miescher cheilitis) Changes are restricted to the lip, mostly focal granulomatous inflammation of the lower lip.

26
27 Pyostomatitis vegetans Pyostomatitis vegetans (PV) is a rare condition characterized by erythematous and thickened oral mucosa with multiple pustules and superficial erosions. PV is associated with IBD in 75% of cases Other differential diagnoses include autoimmune pemphigoid diseases and sometimes infections.

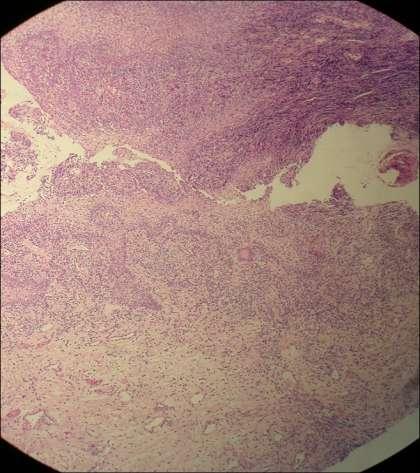
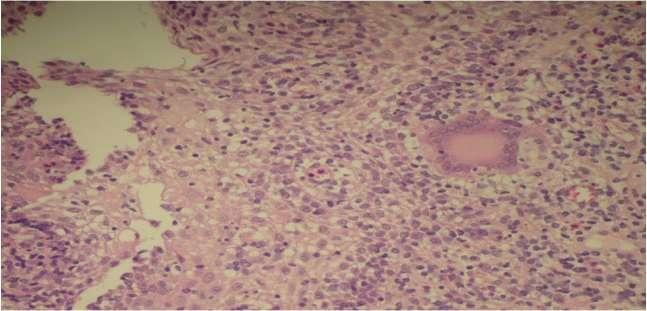
28
29 b. Highly suspicious oral lesions for IBD are highly suggestive of underlying IBD, especially CD The most common affected portions are the buccal mucosa, gingiva, lips

30
31 c. Non-specific lesions in IBD
32 Recurrent aphthous stomatitis Any patient with recurring or insisting oral ulcers should be evaluated medically for the possible presence of a more serious systemic disease. Aphthous-like lesions may be seen in 4-5% of patients with IBD. Colonic, rather than small intestinal, CD is more often associated with oral The list of differential diagnosis is long
33 Salivary duct and saliva in IBD Patients with IBD may complain of dry mouth, similar to the sicca syndrome observed in transplanted patients under immunosuppressive therapy. Granulomatous inflammation of minor salivary gland ducts has been suggested as another oral manifestation of active intestinal CD.
34 Tongue involvement in IBD Rare cases of non-neoplastic tongue involvement in IBD have been described Alterations of taste (metallic dysgeusia) may be related with disease activity, nutritional habits therapy with metronidazole.
35 Dental and gingival manifestations in IBD dental infections and dental alterations related to malabsorption and to disease activity of IBD. Gingival involvement in CD is infrequent. Gingival biopsy may be helpful for early diagnosis of an underlying CD.
36 Oral lesions secondary to nutritional deficiencies Nutritional deficiencies may cause oral lesions, the most common being angular cheilitis associated with iron deficiency. deficiencies in iron, folic acid, vitamin B12, potassium, calcium, magnesium, vitamin A, vitamin C, vitamin D, zinc and selenium.
37 Therapy-related oral lesions All medications may cause oral lesions or symptoms Oral paradoxical reactions to biologicals include oral lichenoid reaction to infliximab and new onset of oral lichen planus during certolizumab pegol use.
38 MEDICAL TREATMENT OF ORAL MANIFESTATIONS IN IBD topical and/or systemic therapies combined with dietary instructions In refractory or intractable cases the algorithms of management may also include surgical treatment
39 Table Treatment of the oral manifestations in inflammatory bowel diseases. Medical treatment of oral IBD Effective treatment of intestinal IBD Standard treatment (reported) -Corticosteroids (methlyprednisolone) -Azathioprine -Infliximab -Thalidomide (refractory cases) -isotretinoin, dapsone (pyostomatitis) -Long-term p.os antibiotics (tetracycline, erythromycin, penicillin, metronidazole) Other possible options (unreported) -Methotrexate -Adalimumab -Certolizumab Nutrition -Total enteral nutrition (selected cases) -Elemental diet (selected cases) -Elimination diets (special dietary restrictions i.e cinnamate- and benzoatefree diet) -Supplementation formulas, vitamins (A,B,C) and trace elements (zinc) Topical treatement Local intralesional injections -corticosteroids - triamcinolone 0.1% -Infliximab -analgesics -lidocaine 2%, Local ointments -corticosteroids(1% hydrocortisone) -tacrolimus -non-steroidal anti-inflammatory pastes Mouthwash -5-aminosalicylic,-corticosteroids,-antiseptic,Elixirs (dexamethasone) Surgical treatment of oral IBD Major surgery Oral and oropharyngeal surgery -Oral surgery -Orthognathic surgery -Maxillofacial surgery Plastic facial and lip surgery -Reconstructive -Elimination Colectomy in intractable oral IBD Minimal or Elective surgery -small lesion removal -small fistula repair -abcess drainage - oral biopsies (multiple) Local dental surgery (functional repair and cosmetic) -Dental surgery -Biopsy of small oral lesion -Laser for gingival Crohn's disease
40 Treatments of oral IBD Type of oral IBD Author/Year Number of all patients Type of trial (controlled/c Uncontrolled/U) Response rates Oral Crohn s Plauth et al, Topical steroids/ U 7 of 12 (58%) patients Oral Crohn s Casson et al, Orofacial Mignogna et al, 139 franulomatosis/ora 2004 l Crohn s 3 Topical tacrolimus ointment /U Marked improvement in 1-6 months 7 Triamcinolone injections Response (2 or 3 injection / U sessions over 14 or 21 days) Oral Crohn s Plauth et al, Azathioprine and/or systemic 13 of 26 (50%) patients steroids / U Oral Crohn s Williams J et al, Systemic steroids / U Improvement in all, steroid-dependent Oral Crohn s Litsas 140, 1 Systemic prednisone / U Response after 6 months 2011 Resistant oral Hegarty et al, Thalidomide/ U Response Crohn s 2003 Oral Crohn s Campbell et al, Phenolic acid exclusion diet 7 responded 2013 with micronutrient supplementation/ U Oral Crohn s White et al, Elimination diets cinnamon- and benzoate-free diet (CB-free diet) / U Response after 8 weeks Oral Crohn s Cameron et al, Elemental diet/ U Response but 2 relapses 2003 Granulomatous Kano et al, Metronidazole / U Response cheilitis Oral Crohn s Sánchez et al, Adalimumab+dapsone/ U Response after 5 months 2005 Oral Crohn s Cardoso et al, Infliximab/ U Successful treatment Fistulizing oral Staines et al, Infliximab/ U Successful treatment Crohn s 2007
41 Figure. Algorithm for management for oral aphthous ulcers in IBD. Management of oral aphthous ulcers in IBD (Target in parallel bowel disease remission) Topical treatment Antibiotics, tacrolimus ointment, corticosteroids (elixirs, ointments, mouthwashes, intralesional injections), analgesics (lidocaine 2%), antiseptic mouthwashes, NSAID pastes Elimination diets (Cinnamon, benzoate, glutaminate, cocoa) Vitamin and trace element supplementation Systemic treatment Corticosteroids, azathioprine, methotrexate, tacrolimus Systemic treatment for refractory cases Biological therapy, thalidomide, long-term antibiotics
42 Figure. Algorithm for recommended management for oral Crohn s disease. Management of oral Crohn s disease (Target in parallel bowel disease remission) Topical treatment Antibiotics, tacrolimus ointment, corticosteroids (elixirs, ointments, mouthwashes, intralesional injections), analgesics (lidocaine 2%), antiseptic mouthwashes, NSAID pastes Elimination diets (Cinnamon, benzoate, glutaminate, cocoa) Vitamin and trace element supplementation Systemic treatment Corticosteroids, azathioprine, methotrexate, tacrolimus, biological therapies Food restriction, Enteral / Parenteral nutrition Systemic treatment for refractory cases Switch to a 2nd biological therapy, thalidomide, long-term antibiotics, dapsone, Cyclosporin A (for pyostomatitis) Surgical treatment Head-neck surgery, oral surgery (for local repair and cosmesis) Dental surgery
43 SURGICAL TREATMENT OF ORAL MANIFESTATIONS IN IBD for severe complications refractory to medical therapy. Minimal or elective surgery Local dental surgery Major surgical interventions include oral and oropharyngeal surgery, (orthognathic and/or maxillofacial surgery) plastic surgery (reconstructive, elimination i.e for hyperplastic gingiva). Colectomy is reserved as an ultimate option for patients with UC and intractable or highly resistant oral lesions that significantly affect oral feeding and overall quality of life.
44
45 ΠΡΟ-ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ
46 Figure. The puzzle of mechanisms and conditions leading to the development of oral precancerous lesions and oral cancer in inflammatory bowel diseases. Environmental factors Sun exposure (UV light), passive smoking(?) Demographics (age>40, males, African-American (oral cavity cancer), fair skin (lip cancer) Life style (smoking, smokeless tobacco use, pipe smoking, marijuana use, heavy alcohol use, access to medical care or dental care, low consumption of fruits and vegetables) Chronic irritation in oral cavity (traumatic ulcers, poor fitting denture, broken or sharp-edged teeth or fillings) Infections (HPV E6 and E7 oncogenes, HIV, syphilis DNA detected from CMV and EBV in oral cancerous lesions, chronic candidiasis) Drugs (immunosuppressants, anti-tnfa?, others?) Education level (Absence of oral screening, no annual oral exam, poor oral hygiene) Nutrition deficiencies (low vitamin A, B12, folic acid levels, iron deficiency) Underlying conditions (immunodeficiency, transplantation, Plummer-Vinson) Alterations in oral homeostasis (xerostomia, reduced salivary flow, candida colonization) Precancerous oral lesions unrecognized and untreated (leukoplakia, erythroplakia, leukoerythroplakia, chronic candidiasis (?) p53 gene alterations-dysplasia-cancer in situ-invasive cancer
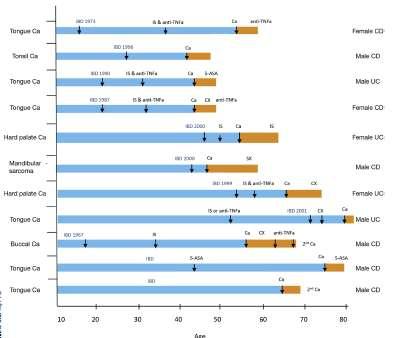
47 Table. Oral precancerous lesions reported in the form of case reports in patients with inflammatory bowel disease. Author Drug Patient Disease Type of oral lesion Mocciaro et al. 54 Certolizumab 1 Crohn s Oral lichen pegol planus Fluckiger et al. 55 Azathioprine 1 Ulcerative Oral hairy colitis leukoplakia Worsnop et al. 52 Infliximab 1 Crohn s Oral lichen planus (probable) Moss et al. 53 Infliximab 1 Crohn s Oral lichenoid reaction to IFX Outcome Non evolution to Ca Non evolution to Ca, HIV(-) Non evolution to Ca (Paradoxical reaction to IFX) Non evolution to Ca (Paradoxical reaction to IFX)
48
 c. Cheek s OL erosive and planus. (AB & ED) d. Tongue s atrophic OLP after a long time evolution.")
49 a. Typical oral lichen planus (OLP) of the tongue s right side. (AB) b. Diffuse OLP, plaque form, of the entire oral mucosa. Note the leukokeratotic aspect to be distinguished from a leukokeratosis. (AB) c. Cheek s OL erosive and planus. (AB & ED) d. Tongue s atrophic OLP after a long time evolution. Note the typical network of overlapping white striae of the point. (AB)
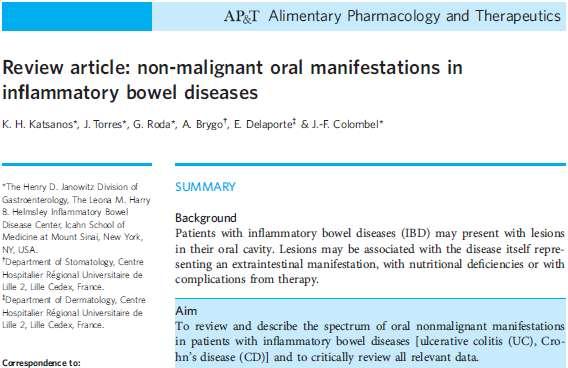
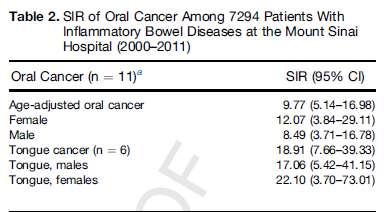
50 ΝΕΟΠΛΑΣΜΑΤΙΚΕΣ ΕΚΔΗΛΩΣΕΙΣ The incidence and prevalence of oral cancerous and pre-cancerous lesions in IBD is currently unknown. No routine oral screening is performed or is advised so far. HPV infection!
 c.typical SCC of the lower lip in a smoker patient arising on a leukokeratosis. (ED) d.")
51 a.squamous cell carcinoma (SCC) of the tongue s point arising on an atrophic oral lichen planus. (ED) b.scc of the tongue in a 19-year-old smoker female. The question of the responsability of HPV as cofactors is raised in such a case. (AB & ED) c.typical SCC of the lower lip in a smoker patient arising on a leukokeratosis. (ED) d.scc of the lower lip in a young male, rapidly appeared after a kidney transplantation. (ED)

52 Melanoma of the soft palate in non-ibd non-hiv patient

53 Kaposi sarcoma of the hard palate in non-ibd non-hiv patient
54 Table. Oral cancers reported in patients with inflammatory bowel disease. Author Drug Patient(s) with oral Ca Vilas-Boas et al. 61 (case report) Li et al. 60 (case report) Dulai et al. 39 (case report) Biancone et al. 26 (multicenter study) Lichtenstein et al. 42 (TREAT cohort registry n=6,773) Cottone et al. 43 (cohort study) Pasternak et al. 62 (Danish IBD cohort database n=45,986) Nyboe- Andersen et al. 50 (Danish IBD cohort database) Colombel et al. 44 (Adalimumab cohort trials) Sandborn et al. 45 (ULTRA cohort study) Beaugerie et al. 57 (CESAME cohort n=17,047) Fidder et al. 46 cohort n=734 ) Katsanos et al. 47 cohort n=681) (Leuven IFX (EC-IBD Katsanos et al. 48 (Leuven cohort n=1815) Fraser et al. 49 n=2204) (Oxford cohort AZA (9 years) Disease Location / Type of oral cancer 1 CD Right superior retromollar trigone, SCC / HPV (-) AZA (3 years) 1 CD Tongue SCC (ulcerous in situ) IFX+AZA 1 IBD Parotid Non-Hodgkin lymphoma non-biological therapies 1 CD Oropharyngeal (larynx) IFX 6 CD Oral cavity or (3 patients on IFX) Any other therapy Details Surgery Surgery Unknown Death SIR (95%(CI) IFX-treated 1.77 (0.37, 5.17) Any other therapy 1.78 (0.37, 5.21) IFX=2,475 ADA= CD Pharyngeal 18 months after IFX (died) AZA= 5, IBD Lip/oral cavity/pharynx non-aza=60 RR 95%(CI) former AZA=4 Non-users (referrent) current AZA=5 Former users 1.70 ( ) Users 1.69 ( ) antitnf=4,553 3 IBD Lip/oral cavity/pharynx Crude non -antitnf 1.24 ( ) =51,593 Adjusted 1.47 ( ) Adjusted for use of azathioprine 1.08 ( ) ADA=3,160 1 CD Oral cavity SCC ADA=494 1 UC Oral cavity 1 of total 35 Ca on ADA <0.1% of the cohort AZA=7, IBD 15 ear-nose-throat Ca 3.6% of all Ca (n=428) AZA (any use pre- or combo- to IFX)=501 1 IBD Lip SCC patient on combo AZA+IFX AZA=174 2 IBD Lip AZA =725 0 IBD No oral cancer (1 BCC in UC on AZA and 1 SCC in UC not on AZA) AZA= IBD 1 SCC oral on AZA 1 SCC oral not on AZA 31 Ca in AZA 77 Ca not in AZA
55
56 CONCLUSIONS The list of oral lesions is extensive. may have devastating consequences most lesions are easily handled and respond to the treatment of intestinal IBD A multidisciplinary approach is essential for the correct diagnosis and management.


57








58 + JAN 12 th, 2016 The Henry D. Janowitz Division of Gastroenterology at Mt Sinai, NY, USA

59
60

61

62

63

64
The Oral Cavity. Image source:
 The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
Contents. 3 Diagnostic Tests and Studies Introduction Examination... 27
 Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Oral Health & HIV. Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape
 Oral Health & HIV Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape Importance & relevance of Oral HIV Lesions >70% of HIV+ve patients present with oral manifestations
Oral Health & HIV Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape Importance & relevance of Oral HIV Lesions >70% of HIV+ve patients present with oral manifestations
Contents. 1 Normal Anatomy Introduction... 17
 Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
Dental Care and Health An Update. Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI
 Dental Care and Health An Update Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI WHO s Definition of Health? Health is a state of complete physical, mental, and social wellbeing and not merely the absence of
Dental Care and Health An Update Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI WHO s Definition of Health? Health is a state of complete physical, mental, and social wellbeing and not merely the absence of
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School
 Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
Oral Medicine. Dr. Qianming Ian CHEN
 Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
How do I evaluate a patient with a swollen lip?
 How do I evaluate a patient with a swollen lip? Yang Gu, BDS, MSc; Michele Williams, BSN, DMD, FRCD(C); Catherine F. Poh, DDS, PhD, FRCD(C) Tags: diagnosis oral pathology Cite this as: J Can Dent Assoc
How do I evaluate a patient with a swollen lip? Yang Gu, BDS, MSc; Michele Williams, BSN, DMD, FRCD(C); Catherine F. Poh, DDS, PhD, FRCD(C) Tags: diagnosis oral pathology Cite this as: J Can Dent Assoc
TANYA A. WRIGHT, DDS OBJECTIVES
 TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
Index. Dent Clin N Am 49 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Dent Clin N Am 49 (2005) 273 278 Index Note: Page numbers of article titles are in boldface type. A Acanthosis nigricans, familial, 251 Amalgam tattoo, 197 198 Amphotericin B, 62 Ankyloglossia, 11 Anti-inflammatory
Dent Clin N Am 49 (2005) 273 278 Index Note: Page numbers of article titles are in boldface type. A Acanthosis nigricans, familial, 251 Amalgam tattoo, 197 198 Amphotericin B, 62 Ankyloglossia, 11 Anti-inflammatory
Diseases of oral cavity
 Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
That. Name QUIZ. 60 SEPTEMBER 2017 // dentaltown.com
 QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
Kings College London Dental Institute. Guy s & St Thomas NHS Foundation Trust Oral Medicine Unit. Disease Activity Scoring sheets
 Kings College London Dental Institute Guy s & St Thomas NHS Foundation Trust ral Medicine Unit Disease Activity Scoring sheets Clinical scoring systems for oral mucosal Diseases The routine clinical management
Kings College London Dental Institute Guy s & St Thomas NHS Foundation Trust ral Medicine Unit Disease Activity Scoring sheets Clinical scoring systems for oral mucosal Diseases The routine clinical management
CHEILITIS GRANULOMATOSA
 CHEILITIS GRANULOMATOSA Report of two Cases with Clinical and Diagnostic Implications Presented By Dr. Amar Sholapurkar Under the guidance of Dr.Ausaf Ahsan Department of Oral Medicine & Radiology, MCODS,
CHEILITIS GRANULOMATOSA Report of two Cases with Clinical and Diagnostic Implications Presented By Dr. Amar Sholapurkar Under the guidance of Dr.Ausaf Ahsan Department of Oral Medicine & Radiology, MCODS,
Role of the Dental Hygienist in Oral Pathology. Role of the Dental Hygienist in Oral Pathology. Cancers of the Oral Cavity.
 Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients. Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology
 Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
THE TONGUE. In Clinical Diagnosis
 THE TONGUE In Clinical Diagnosis A Colour Atlas of The Tongue in Clinical Diagnosis D.W. BEAVEN S.E. BROOKS BATES Guide to Physical Examination Lynn s. Bickley רויטל רחימי, תום כספי פנימית ב', תל-השומר
THE TONGUE In Clinical Diagnosis A Colour Atlas of The Tongue in Clinical Diagnosis D.W. BEAVEN S.E. BROOKS BATES Guide to Physical Examination Lynn s. Bickley רויטל רחימי, תום כספי פנימית ב', תל-השומר
Differential Diagnosis of Oral Ulcerations
 Differential Diagnosis of Oral Ulcerations Dr. Nagamani Narayana Department of Oral Biology University of Nebraska Medical Center College of Dentistry Objectives Differential diagnosis of oral ulcerations
Differential Diagnosis of Oral Ulcerations Dr. Nagamani Narayana Department of Oral Biology University of Nebraska Medical Center College of Dentistry Objectives Differential diagnosis of oral ulcerations
Lesions & Lifestyles
 Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Case 1 History. William Tremaine, M.D. CP
 Extraintestinal Manifestations of IBD Case Studies William Tremaine, M.D. Case 1 History 18 year-old woman with Crohn s disease Onset at age 5: colonic & perianal Sulfasalazine, prednisone, mercaptopurine
Extraintestinal Manifestations of IBD Case Studies William Tremaine, M.D. Case 1 History 18 year-old woman with Crohn s disease Onset at age 5: colonic & perianal Sulfasalazine, prednisone, mercaptopurine
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem.
 Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Benign Oral cavity lesions. Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery
 Benign Oral cavity lesions Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery Anatomy Histology Physiology Pathology Clinical cases Introduction The oral cavity
Benign Oral cavity lesions Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery Anatomy Histology Physiology Pathology Clinical cases Introduction The oral cavity
Oral Cancer FAQs. What is oral cancer? How many people are diagnosed with oral cancer each year?
 Oral Cancer FAQs What is oral cancer? Oral cancer or oral cavity cancer, is cancer that starts in the mouth. Areas affected by this type of cancer are the lips, the inside lining of the lips and cheeks
Oral Cancer FAQs What is oral cancer? Oral cancer or oral cavity cancer, is cancer that starts in the mouth. Areas affected by this type of cancer are the lips, the inside lining of the lips and cheeks
Beyond the Bowel: Extraintestinal Manifestations of Inflammatory Bowel Disease
 Beyond the Bowel: Extraintestinal Manifestations of Inflammatory Bowel Disease Robert Isfort, M.D. TriHealth Digestive Institute IBD Family Education Day 2019 Learning Objectives Review manifestations
Beyond the Bowel: Extraintestinal Manifestations of Inflammatory Bowel Disease Robert Isfort, M.D. TriHealth Digestive Institute IBD Family Education Day 2019 Learning Objectives Review manifestations
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
Stomatitis.
 Stomatitis http://www.entusa.com/oral_photographs/20080102-stomatitis-palate_small.jpg Oral inflammation and ulcers, known as stomatitis, may be mild and localized or severe and widespread. They are invariably
Stomatitis http://www.entusa.com/oral_photographs/20080102-stomatitis-palate_small.jpg Oral inflammation and ulcers, known as stomatitis, may be mild and localized or severe and widespread. They are invariably
Dental Management of the Organ or Stem Cell Transplant Patient
 Dental Management of the Organ or Stem Cell Transplant Patient KEY POINTS Before and after organ or stem cell transplantation, patients require specialized dental management. Optimal dental management
Dental Management of the Organ or Stem Cell Transplant Patient KEY POINTS Before and after organ or stem cell transplantation, patients require specialized dental management. Optimal dental management
More Non-infectious Granulomatous Diseases! Karolyn Wanat, MD Assistant Professor, Dermatology & Pathology University of Iowa
 More Non-infectious Granulomatous Diseases! Karolyn Wanat, MD Assistant Professor, Dermatology & Pathology University of Iowa Conflicts of Interest/Disclosure None Classification/Overview 1) Necrobiotic/Palisading
More Non-infectious Granulomatous Diseases! Karolyn Wanat, MD Assistant Professor, Dermatology & Pathology University of Iowa Conflicts of Interest/Disclosure None Classification/Overview 1) Necrobiotic/Palisading
Cases of Non-Infectious Vulvovaginitis
 Cases of Non-Infectious Vulvovaginitis 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology
Cases of Non-Infectious Vulvovaginitis 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology
A Prospective Study of the Oral Manifestations of Crohn s Disease
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:886 891 A Prospective Study of the Oral Manifestations of Crohn s Disease SINEAD HARTY,* PADRAIG FLEMING, MARION ROWLAND,* ELLEN CRUSHELL,* MICHAEL MCDERMOTT,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:886 891 A Prospective Study of the Oral Manifestations of Crohn s Disease SINEAD HARTY,* PADRAIG FLEMING, MARION ROWLAND,* ELLEN CRUSHELL,* MICHAEL MCDERMOTT,*
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Diagnostic sieve. Looking Beyond the Vermillion Border. Time bombs for medical GPs! Normal oral mucosa
 Sat 12 June 2010 Millennium WS 28 + 38 2.00-2.55; 3.05-4.00 PM Looking Beyond the Vermillion Border Laurence J. Walsh BDSc, PhD, DDSc, FFOP(RCPA), GCEd, FICD, FPFA, FADI, FIADFE The University of Queensland
Sat 12 June 2010 Millennium WS 28 + 38 2.00-2.55; 3.05-4.00 PM Looking Beyond the Vermillion Border Laurence J. Walsh BDSc, PhD, DDSc, FFOP(RCPA), GCEd, FICD, FPFA, FADI, FIADFE The University of Queensland
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
SYSTEMIC DISEASES IN THE HEAD AND NECK REGION
 SYSTEMIC DISEASES IN THE HEAD AND NECK REGION DEFINITION OF SYSTEMIC DISEASE More organs involved in the process of disease Very often combined with developmental disorders 1000-1500 syndromes written
SYSTEMIC DISEASES IN THE HEAD AND NECK REGION DEFINITION OF SYSTEMIC DISEASE More organs involved in the process of disease Very often combined with developmental disorders 1000-1500 syndromes written
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Medical History. Oral Medicine and General Medicine
 Medical History Oral Medicine and General Medicine Gingivitis herpetica acuta NECROTIZÁLÓ SIALOMETAPLASIA SOOR Medical History The life expectancy has recently increased and increasing By dental prevention
Medical History Oral Medicine and General Medicine Gingivitis herpetica acuta NECROTIZÁLÓ SIALOMETAPLASIA SOOR Medical History The life expectancy has recently increased and increasing By dental prevention
Internal Medicine Correlations in Oral Health
 Internal Medicine Correlations in Oral Health Mark D. Baldwin D.O., FACOI Chair, Department of Internal Medicine Professor of Medicine LEARN. CARE. COMMUNITY. None, just working for The Man Disclosures
Internal Medicine Correlations in Oral Health Mark D. Baldwin D.O., FACOI Chair, Department of Internal Medicine Professor of Medicine LEARN. CARE. COMMUNITY. None, just working for The Man Disclosures
Oral Ulceration (Ulcers of the Mouth) Basics
 Basics") Oral Ulceration (Ulcers of the Mouth) Basics OVERVIEW Oral ulceration is the term for ulcers of the mouth ; ulcers are lesions on the moist tissues, characterized by the loss of the top layer(s) of tissue,
Oral Ulceration (Ulcers of the Mouth) Basics OVERVIEW Oral ulceration is the term for ulcers of the mouth ; ulcers are lesions on the moist tissues, characterized by the loss of the top layer(s) of tissue,
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Head and Neck Cancer How to recognize it in your office
 Head and Neck Cancer How to recognize it in your office Peter M Hunt, MD, FACS Associates in ENT/Head & Neck Surgery Director CHI Memorial Head & Neck and Melanoma Centers of Excellence September 8, 2018
Head and Neck Cancer How to recognize it in your office Peter M Hunt, MD, FACS Associates in ENT/Head & Neck Surgery Director CHI Memorial Head & Neck and Melanoma Centers of Excellence September 8, 2018
W. R. TYLDESLEY, D.D.s., PH.D., F.D.S.R.C.S.
 British Journal of Oral Surgery 17 (I 979~80), 1-9 ORAL CROHN S DISEASE AND RELATED CONDITIONS School W. R. TYLDESLEY, D.D.s., PH.D., F.D.S.R.C.S. of Dental Surger,y, Pembroke Place, P.O. Box 147, Liverpool,
British Journal of Oral Surgery 17 (I 979~80), 1-9 ORAL CROHN S DISEASE AND RELATED CONDITIONS School W. R. TYLDESLEY, D.D.s., PH.D., F.D.S.R.C.S. of Dental Surger,y, Pembroke Place, P.O. Box 147, Liverpool,
RISK FACTORS OF BURNING MOUTH SYNDROME: UN UPDATE
 RISK FACTORS OF BURNING MOUTH SYNDROME: UN UPDATE Cristina Popa, Carmen Stelea, Eugenia Popescu Department of Oral and Maxilo-facial Surgery Abstract: Burning mouth syndrome has never been associated with
RISK FACTORS OF BURNING MOUTH SYNDROME: UN UPDATE Cristina Popa, Carmen Stelea, Eugenia Popescu Department of Oral and Maxilo-facial Surgery Abstract: Burning mouth syndrome has never been associated with
Vitamins Minerals Chapter 12
 DH 250 Water soluble B1 Thiamin B2 Riboflavin B3 Niacin Vitamins Minerals Chapter 12 Role RDA Source Deficiency Toxicity Clinical Use intermediary coenzymes 1.2mg 1.1mg 1.2mg 1.1mg 16mg 14mg dairy B6 Pyridoxine
DH 250 Water soluble B1 Thiamin B2 Riboflavin B3 Niacin Vitamins Minerals Chapter 12 Role RDA Source Deficiency Toxicity Clinical Use intermediary coenzymes 1.2mg 1.1mg 1.2mg 1.1mg 16mg 14mg dairy B6 Pyridoxine
IBD in teenagers Biological and Transition
 IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients
 Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients Siri Beier Jensen Associate Professor, DDS, PhD Aarhus University Faculty Disclosure X No, nothing to disclose
Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients Siri Beier Jensen Associate Professor, DDS, PhD Aarhus University Faculty Disclosure X No, nothing to disclose
We re Passionate About
 Oral Health Training Marie Burgum Oral Health Advisor Tees Community Dental Service We re Passionate About Putting patients first Quality, safety and patient experience Transforming services to meet the
Oral Health Training Marie Burgum Oral Health Advisor Tees Community Dental Service We re Passionate About Putting patients first Quality, safety and patient experience Transforming services to meet the
2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD
 2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD Course 9148: Diagnosis and Treatment of Recurrent Oral Ulcers Friday, April 6 9 am - 12 pm Diagnosis and Treatment of Recurrent Oral Ulcers
2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD Course 9148: Diagnosis and Treatment of Recurrent Oral Ulcers Friday, April 6 9 am - 12 pm Diagnosis and Treatment of Recurrent Oral Ulcers
Slide 1 Medications in inflammatory bowel disease a primer for health care providers. Slide 2. Slide 3 Theory of pathogenesis. IBD - epidemiology
 Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
Slide 1 Medications in inflammatory bowel disease a primer for health care providers Athos Bousvaros, MD Associate director Inflammatory Bowel Disease Center Boston Children s Hospital 617 355 2962 Slide
PREVENTION OF ORAL CANCER
 PREVENTION OF ORAL CANCER Oral cancer is increasing in incidence worldwide. Throughout the world, malignant neoplasms of the mouth and pharynx rate as the fifth most common cancer in men and the seventh
PREVENTION OF ORAL CANCER Oral cancer is increasing in incidence worldwide. Throughout the world, malignant neoplasms of the mouth and pharynx rate as the fifth most common cancer in men and the seventh
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
The Spectrum of IBD. Inflammatory Bowel Disease. Symptoms. Epidemiology. Tests for IBD. CD or UC? Inflamatory Bowel Disease. Fernando Vega, M.D.
 The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
The Spectrum of IBD Inflammatory Bowel Disease Fernando Vega, M.D. Epidemiology CD and UC together 1:400 UC Prevalence 1:500 UC Incidence 6-12K/annum CD Prevalence 1:1000 CD Incidence 3-6K/annum Symptoms
CAMOSUN COLLEGE School of Health & Human Services Dental Programs. DHYG 321 Oral Science COURSE OUTLINE
 CAMOSUN COLLEGE School of Health & Human Services Dental Programs 2013 COURSE OUTLINE 1. Instructor Information (a) Instructor Lynne Viczko (b) Office hours Posted on office door (c) Location Dental Building
CAMOSUN COLLEGE School of Health & Human Services Dental Programs 2013 COURSE OUTLINE 1. Instructor Information (a) Instructor Lynne Viczko (b) Office hours Posted on office door (c) Location Dental Building
Manifestations of gastrointestinal diseases in the oral cavity. Nabil El-Lababidi
 Manifestations of gastrointestinal diseases in the oral cavity Nabil El-Lababidi Types of mouth affections in conjunction with GIT diseases I. Glossitis: Crohn s disease Coeliac disease Kwashiorkhor Malabsorption
Manifestations of gastrointestinal diseases in the oral cavity Nabil El-Lababidi Types of mouth affections in conjunction with GIT diseases I. Glossitis: Crohn s disease Coeliac disease Kwashiorkhor Malabsorption
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Clinical Implications Of Treating PWD
 Clinical Implications Of Treating PWD Xerostomia- Antihypertensive Medications Hyperglycemic xerostomia Neuropathic Association? Clinical Significance: Caries Mucositis Impaired Denture Retention Candida
Clinical Implications Of Treating PWD Xerostomia- Antihypertensive Medications Hyperglycemic xerostomia Neuropathic Association? Clinical Significance: Caries Mucositis Impaired Denture Retention Candida
APHTHOUS STOMATITIS ADULT & PEDIATRIC
 DEFINITION Aphthous stomatitis or canker sores are described as ulcers and inflammation of the tissues of the mouth, including the lips, buccal mucosa, tongue, gingiva, and posterior pharyngeal wall. These
DEFINITION Aphthous stomatitis or canker sores are described as ulcers and inflammation of the tissues of the mouth, including the lips, buccal mucosa, tongue, gingiva, and posterior pharyngeal wall. These
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
INFLAMMATORY DISEASES PART I. Immunopathology Part I
 INFLAMMATORY DISEASES PART I Immunopathology Part I Nonspecific & T Cell Mediated Mucosal Inflammatory Lesions Nonspecific and Idiopathic Mucositis Hypersensitivity and Autoimmune T cell mediated Immunoglobulin
INFLAMMATORY DISEASES PART I Immunopathology Part I Nonspecific & T Cell Mediated Mucosal Inflammatory Lesions Nonspecific and Idiopathic Mucositis Hypersensitivity and Autoimmune T cell mediated Immunoglobulin
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Oral Pathology Syllabus for English-Speaking Students
 Oral Pathology Syllabus for English-Speaking Students Academic Hours Academic Hours in Years and Semesters I year II year III year IV year V year DISCIPLINE Semester Exam Total Lectures Practicals I II
Oral Pathology Syllabus for English-Speaking Students Academic Hours Academic Hours in Years and Semesters I year II year III year IV year V year DISCIPLINE Semester Exam Total Lectures Practicals I II
ORAL MANIFESTATIONS IN LIVER DISEASES
 ORAL MANIFESTATIONS IN LIVER DISEASES Rodica Ghiuru, D.Munteanu Department of Internal Medicine Abstract: Chronic hepatitis C infection is a worldwide health problem because it causes chronic hepatitis,
ORAL MANIFESTATIONS IN LIVER DISEASES Rodica Ghiuru, D.Munteanu Department of Internal Medicine Abstract: Chronic hepatitis C infection is a worldwide health problem because it causes chronic hepatitis,
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Oral Signs of Systemic Diseases
 Oral Signs of Systemic Diseases American Academy of Dermatology San Diego, California February 17, 2018 Oral Signs of Gastrointestinal Diseases Roy S. Rogers, III, M.D. Professor of Dermatology Mayo Clinic
Oral Signs of Systemic Diseases American Academy of Dermatology San Diego, California February 17, 2018 Oral Signs of Gastrointestinal Diseases Roy S. Rogers, III, M.D. Professor of Dermatology Mayo Clinic
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease:
 4. Associated with systemic disease:") Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
In India among the 1027 million populations about 72% people live in rural areas
 1 INTRODUCTION 2 In India among the 1027 million populations about 72% people live in rural areas India produces 9000 dentists per annum-dentist population ratio is 1:30,000 Only 10%of the dentists are
1 INTRODUCTION 2 In India among the 1027 million populations about 72% people live in rural areas India produces 9000 dentists per annum-dentist population ratio is 1:30,000 Only 10%of the dentists are
Principles of Management of Head & Neck Cancer. Jinka Sathya Associate professor of Oncology
 Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Burning Mouth Syndrome. Nurdiana, drg., Sp.PM
 Burning Mouth Syndrome Nurdiana, drg., Sp.PM DEFINITION Burning Mouth Syndrome (BMS) oral burning tongue/other mucous membranes no detectable cause, anatomic pathways, mucosal lesions, neurologic disorders
Burning Mouth Syndrome Nurdiana, drg., Sp.PM DEFINITION Burning Mouth Syndrome (BMS) oral burning tongue/other mucous membranes no detectable cause, anatomic pathways, mucosal lesions, neurologic disorders
Differential Diagnosis of Oral Lesions. An Interactive Lecture Using Audience Response Polling. John L. Alonge, MS, DDS
 Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
VIRUS. Viral infection causing, or associated with diseases of the oral mucosa : Herpes Simpleks 1 & 2
 VIRUS Viral infection causing, or associated with diseases of the oral mucosa : VIRUS Herpes Simpleks 1 & 2 Varicella - Zoster Coxsakie A PENYAKIT Primary Gingivostomatitis Herpetica Herpes Labialis Recurrent
VIRUS Viral infection causing, or associated with diseases of the oral mucosa : VIRUS Herpes Simpleks 1 & 2 Varicella - Zoster Coxsakie A PENYAKIT Primary Gingivostomatitis Herpetica Herpes Labialis Recurrent
Vascular. Extravasated blood. Melanocytic. Tattoo. Epidermolysis bullosa. Lichen planus. Pemphigoid Pemphigus Lupus. Candidosis. Surface Epithelial
 Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Sign In: pemphigus.org/form
 Pemphigus and Pemphigoid The Unique Role of the Dental Professional Dr. Carol Anne Murdoch Kinch Sign In: pemphigus.org/form The International Pemphigus & Pemphigoid Foundation (IPPF) kindly asks all attendees
Pemphigus and Pemphigoid The Unique Role of the Dental Professional Dr. Carol Anne Murdoch Kinch Sign In: pemphigus.org/form The International Pemphigus & Pemphigoid Foundation (IPPF) kindly asks all attendees
Oral Hygiene. Dental hygiene disorders: Dental Caries Gingivitis Halitosis Teething discomfort Aphthous (mouth) ulcer
 ulcer") Oral Hygiene Dental hygiene disorders: Dental Caries Gingivitis Halitosis Teething discomfort Aphthous (mouth) ulcer Anatomy of the tooth Dental caries Incidence: It decreases especially in children
Oral Hygiene Dental hygiene disorders: Dental Caries Gingivitis Halitosis Teething discomfort Aphthous (mouth) ulcer Anatomy of the tooth Dental caries Incidence: It decreases especially in children
Oral infections. Siri Beier Jensen Associate Professor, DDS, PhD
 Oral infections Siri Beier Jensen Associate Professor, DDS, PhD Oral mucosa Covers and protects underlying structures Barrier to bacterial, fungal and viral infection Resistant to: Temperature ph Mechanical
Oral infections Siri Beier Jensen Associate Professor, DDS, PhD Oral mucosa Covers and protects underlying structures Barrier to bacterial, fungal and viral infection Resistant to: Temperature ph Mechanical
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline
 Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
PEDIATRIC INFLAMMATORY BOWEL DISEASE
 PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
PEDIATRIC INFLAMMATORY BOWEL DISEASE Alexis Rodriguez, MD Pediatric Gastroenterology Advocate Children s Hospital Disclosers Abbott Nutrition - Speaker Inflammatory Bowel Disease Chronic inflammatory disease
Ammara ismail, Fatima Javed, Memoona Ismail
 International Journal of Scientific & Engineering Research Volume 9, Issue 4, April-2018 1542 Oral manifestations of exam/prof induced stress ABSTRACT Ammara ismail, Fatima Javed, Memoona Ismail Stress
International Journal of Scientific & Engineering Research Volume 9, Issue 4, April-2018 1542 Oral manifestations of exam/prof induced stress ABSTRACT Ammara ismail, Fatima Javed, Memoona Ismail Stress
Allergic contact stomatitis is a rare disorder,
 Allergic Contact Stomatitis: A Case Report and Review of Literature P Lokesh, T Rooban, Joshua Elizabeth, K Umadevi, K Ranganathan Abstract Allergic contact stomatitis is a well-recognized entity, which
Allergic Contact Stomatitis: A Case Report and Review of Literature P Lokesh, T Rooban, Joshua Elizabeth, K Umadevi, K Ranganathan Abstract Allergic contact stomatitis is a well-recognized entity, which
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
The Role of Oral Health in Successful Care Transitions: How AAAs Can Address Oral Health Issues to Improve Health Outcomes
 The Role of Oral Health in Successful Care Transitions: How AAAs Can Address Oral Health Issues to Improve Health Outcomes 1 ADS Case Management Training June 27, 2012 Mary Pat O Leary, RN To understand
The Role of Oral Health in Successful Care Transitions: How AAAs Can Address Oral Health Issues to Improve Health Outcomes 1 ADS Case Management Training June 27, 2012 Mary Pat O Leary, RN To understand
MODULE 5 IMPACTS OF DRY MOUTH. Welcome to. Module 5. Impacts of Dry Mouth
 Welcome to Module Impacts of Dry Mouth IMPACTS OF DRY MOUTH According to Oralieve research, nearly 90% of Dental Professionals believe that the incidence of the cases of dry mouth is on the rise. 1 * Living
Welcome to Module Impacts of Dry Mouth IMPACTS OF DRY MOUTH According to Oralieve research, nearly 90% of Dental Professionals believe that the incidence of the cases of dry mouth is on the rise. 1 * Living
MELKERSSON-ROSENTHAL SYNDROME AND CROHN S DISEASE
 British Journal of Oral Surgery (1980) 18, 254-258 @ The British Association of Oral Surgeons OOO7-117X/80/00370254$02.00 MELKERSSON-ROSENTHAL SYNDROME AND CROHN S DISEASE N. WORSAAE,~* K. C. CHRISTENSEN,2
British Journal of Oral Surgery (1980) 18, 254-258 @ The British Association of Oral Surgeons OOO7-117X/80/00370254$02.00 MELKERSSON-ROSENTHAL SYNDROME AND CROHN S DISEASE N. WORSAAE,~* K. C. CHRISTENSEN,2
REF: Chap 1 (Pemphigus vulgaris/etiology and
 Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
ANS: C REF: Chap 1 (Pemphigus vulgaris/etiology and pathogenesis), p 11
, p 11") Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
WOMEN'S INTERAGENCY HIV STUDY ORAL PROTOCOL FORM OP 4: ORAL MUCOSAL TISSUE EXAM
 WOMEN'S INTERAGENCY HIV STUDY ORAL PROTOCOL FORM OP 4: ORAL MUCOSAL TISSUE EXAM COMPLETING THE FORM GENERAL INFORMATION Affix the Participant ID label in the space indicated. Record the visit number. Be
WOMEN'S INTERAGENCY HIV STUDY ORAL PROTOCOL FORM OP 4: ORAL MUCOSAL TISSUE EXAM COMPLETING THE FORM GENERAL INFORMATION Affix the Participant ID label in the space indicated. Record the visit number. Be
DURATION OF THE STUDY: JUNE-OCTOBER 2008 COST OF STUDY; 9400KSH SOURCE OF FUNDS: SELF INVESTIGATOR: GIKUNDA MARY KATHURE
 J ORAL MANIFESTATIONS OF HIV INFECTION/AIDS AND THEIR INFLUENCE ON ORAL FUNCTIONS AND ORAL HYGIENE PRACTICES AMONG ADULT PATIENTS IN KENYATTA NATIONAL HOSPITAL COMPREHENSIVE CARE CENTRE. INVESTIGATOR:
J ORAL MANIFESTATIONS OF HIV INFECTION/AIDS AND THEIR INFLUENCE ON ORAL FUNCTIONS AND ORAL HYGIENE PRACTICES AMONG ADULT PATIENTS IN KENYATTA NATIONAL HOSPITAL COMPREHENSIVE CARE CENTRE. INVESTIGATOR:
Clinical Oral Manifestation in Gastrointestinal Disorders
 LKN JOURNL OF STOMTOLOGY ISSN 1107-1141 STOMTOLOGICL SOCIETY Clinical Oral Manifestation in Gastrointestinal Disorders SUMMRY im: to evidence extraoral and intraoral, subjective and objective, symptoms
LKN JOURNL OF STOMTOLOGY ISSN 1107-1141 STOMTOLOGICL SOCIETY Clinical Oral Manifestation in Gastrointestinal Disorders SUMMRY im: to evidence extraoral and intraoral, subjective and objective, symptoms
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Diagnosis and management of COMMON NON-VIRAL ORAL ULCERATIONS
 and management of COMMON NON-VIRAL ORAL ULCERATIONS Van Heerden WFP, BChD, MChD (Oral Path), FC Path(SA) Oral Path, PhD, DSc Department of Oral Pathology, University of Pretoria Boy SC, BChD, MChD (Oral
and management of COMMON NON-VIRAL ORAL ULCERATIONS Van Heerden WFP, BChD, MChD (Oral Path), FC Path(SA) Oral Path, PhD, DSc Department of Oral Pathology, University of Pretoria Boy SC, BChD, MChD (Oral
Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases
 Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases Abstract Aim: The aim of this article is to present a brief review of plasma cell gingivitis (PCG) along with reports of three
Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases Abstract Aim: The aim of this article is to present a brief review of plasma cell gingivitis (PCG) along with reports of three
Image: Blend Images/Punchstock Image: Blend Images/Punchstock Image: Ablestock/Punchstock. Copyright STFM
 Image: Blend Images/Punchstock Image: Blend Images/Punchstock Image: Ablestock/Punchstock Copyright STFM 2005-2014 Third Edition June 2010 www.smilesforlifeoralhealth.org Last Modified: April, 2014 2 Course
Image: Blend Images/Punchstock Image: Blend Images/Punchstock Image: Ablestock/Punchstock Copyright STFM 2005-2014 Third Edition June 2010 www.smilesforlifeoralhealth.org Last Modified: April, 2014 2 Course
Oral Medicine FULL Referral Guide (FRG)
") Oral Medicine FULL Referral Guide (FRG) Yorkshire & the Humber February 2017 Version 1 Contents Introduction... 1 Oral Medicine Referral Decision Process 1 Step 1. Oral Medicine Condition?... 2 A. Soft
Oral Medicine FULL Referral Guide (FRG) Yorkshire & the Humber February 2017 Version 1 Contents Introduction... 1 Oral Medicine Referral Decision Process 1 Step 1. Oral Medicine Condition?... 2 A. Soft