Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars
|
|
|
- Bertina Bradley
- 6 years ago
- Views:
Transcription

1 IJOI 35 iaoi CASE REPORT Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars Abstract An 8y2mo female presented a Class II Division 2 malocclusion associated with typical dental alignment problems: retroclined upper central incisors, labially flared maxillary lateral incisors, deep overbite, and severe crowding. Skeletally the malocclusion was complicated by a retrognathic mandible (ANB of 9 ) steep mandibular plane angle (MPA 34 ) and severe facial convexity (24 ). Despite the Class II/2 pattern, the molars were Class I due to ectopic eruption and mesial migration of the mandibular first molars, which resulted in the second premolars being blocked out. The Discrepancy Index (DI) was 37. Treatment mechanics were passive self-ligating brackets, early light short elastics (ELSE), anterior bite turbos, and extra-alveolar (E-A) miniscrews in the infrazygomatic crests to retract the entire maxillary arch. Nonextraction treatment for 32 months resulted in an acceptable skeletal compromises (4 increase in the MPA and lower incisor to mandibular plane angle of 9 ), but dental alignment was excellent, as documented with Cast-Radiograph (CRE) score of 22 and a Pink and White (P&W) dental esthetics score of 3. (Int I Ortho Implantol 24;35:64-78 ) Key words: Class II division 2 malocclusion, self-ligating appliance, bite turbo, bone screw anchorage History and Etiology It is more difficult to finish severe malocclusions well. Of the common malocclusions, Class II Division 2 (Class II/2) malocclusions are the most challenging, 2 and extended treatment times (>36 months) contribute to an inferior result. 3 The traditional treatment approaches involves headgear, functional appliances and/or orthognathic surgery. However, these methods are all problematic with respect to compliance, extended treatment time and/or postoperative complications. -3 The present patient is a 8-year-and-2-monthold female who presented with her mother for orthodontics evaluation (Figs. -3). Chief complaints were crooked teeth and flared upper lateral incisors. Despite a distinct Class II/2 skeletal and dental pattern with bimaxillary crowding, the molars were Class I and both lower second premolars were blocked in to the lingual. The etiology of this complex malocclusion is multifactorial. 3 Developmentally the patient had a severely retrusive mandible which is a growth deficit that usually involves both polygenetic genetic traits and environmental factors. 4 The subsequent development of the dental aspects of the malocclusion appears to be environmental based on the following scenario. Maintaining lip competence in the present of a Class II skeletal pattern results in lingual tipping of the maxillary central incisors, which blocks out the lateral incisors to the labial. The Class I molar relationship is probably due to the ectopic eruption in the mandibular arch: st molars erupted mesially into a Class I relationship, causing premature loss of the 2 nd deciduous molars, which in turn resulted in blocked in 2 nd premolars. Thus, the Class I molar relationship is actually a complicating factor for a Class II/2 skeletal malocclusion. The patient was treated to a pleasing result in 23 months as documented in Figs Radiographs 64




















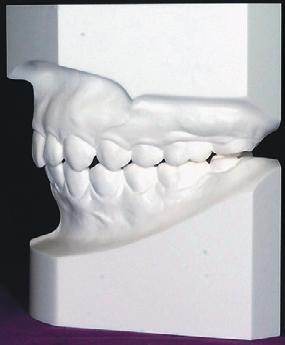


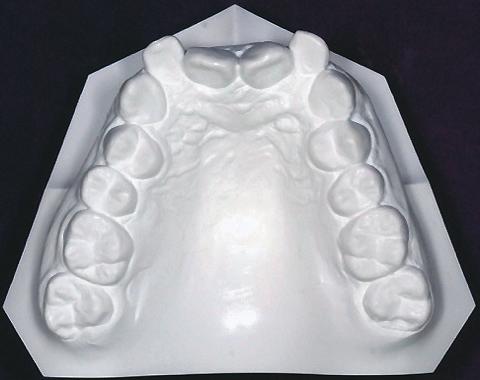

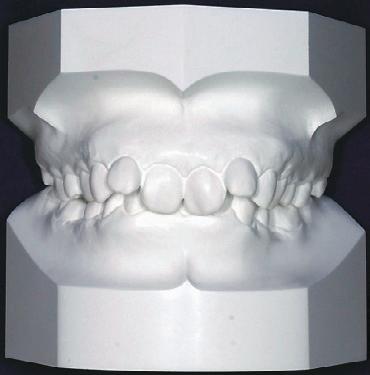
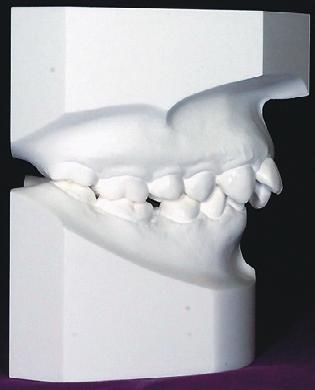
2 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 Dr. Sophia Pei-Wen Shu, Instructor Beethoven Orthodontic Course (left) Dr. Hsin Yin Yeh, Diplomate International Association for Orthodontists & Implantologists (middle) Dr. Chris Chang, Publisher International Journal of Orthodontics& Implantology (middle) W. Eugene Roberts, Consultant International Journal of Orthodontics & Implantology (right) Fig. : Pre-treatment facial photographs Fig. 4: Post-treatment facial photographs Fig. 2: Pre-treatment intraoral photographs Fig. 5: Post-treatment intraoral photographs Fig. 3: Pre-treatment study models (casts) Fig. 6: Post-treatment study models (casts) 65




3 IJOI 35 iaoi CASE REPORT Fig. 7: Pre-treatment lateral cephalometric and panoramic radiographs Fig. 8: Post-treatment lateral cephalometric and panoramic radiographs Fig. 9: Cephalometric tracings are superimposed on the anterior cranial base, maxilla and mandible. 66
4 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 Specific Objectives of Treatment before and after treatment are shown in Figs. 7 & 8, respectively. Fig. 9 documents the treatment with superimposed cephalometric tracings. Maxilla (all three planes): A - P: Maintain Vertical: Maintain Transverse: Maintain Diagnosis. Angle Classification: Class I molar relationship (due to lingually blocked-in of 2 nd premolars) 2. Tooth Size Arch Length Discrepancy: Maxillary: 6 mm, Mandibular: mm 3. Crossbite: Bilateral lingual crossbite of mandibular second premolars 4. Facial: Gummy smile, convex profile, and mandibular retrusion 5. Radiographic\Cephalometric: a. Skeletal: Class II (SNA 84, SNB 75, ANB 9 ); increased mandibular plane angle (SN-MP 34 ) b. Dental: % overbite; lingually tipped upper central incisors 6. Radiographic\Panoramic: Three impacted 3 rd molars (UL, LL, LR) As shown in the subsequent worksheet, the American Board of Discrepancy Index (DI) was 37. Mandible (all three planes): A - P: Maintain Vertical: Maintain if possible, but posterior rotation is likely with efficient mechanics for treatment in < 36 mo. Transverse: Maintain Maxillary Dentition A - P: a. Molars: Retract b. Incisors: Tip labially Vertical: Maintain a. Molars: Maintain b. Incisors: Intrude Inter-molar Width: Increase Inter-canine Width: Maintain Buccolingual Inclination: Maintain Mandibular Dentition A - P: a. Molars: Retract b. Incisors: Maintain Vertical: a. Molars: Extrude b. Incisors: Intrude Inter-molar Width: Increase Inter-canine Width: Maintain Buccolingual Inclination: Maintain 67

5 IJOI 35 iaoi CASE REPORT Facial Esthetics: Correct relatively protrusive upper lip, maintain lip competence Other: Correct the gummy smile by improving upper incisor alignment; consider follow-up gingivetomy if needed M Treatment Plan Smooth the facial surface of upper left central incisor before bonding. Bond both arches with a full fixed appliance. Place upper anterior bite turbos on the lingual surface of both central incisors and correct the deepbite with extrusion of the other teeth in the arch. Place early light short elastics (2 oz) to correct Class II buccal segments. Treat the lingual crossbite of the lower 2 nd premolars with cross elastics (3.5 oz). Place miniscrews in the infrazygomatic crests bilaterally, to retract the upper posterior segments to attain Class I buccal segments. Apply Class II and posterior vertical elastics as needed. Detail the final occlusion and remove all fixed appliances. Retain the corrected dentition with upper 2-2 and lower 3-3 fixed retainers plus a clear overlay retainer for the maxillary arch. Extraction of all 3 rd molars is recommended. Appliances and Treatment Progress A.22 slot Damon Clear bracket system (Ormco, Glendora, CA) was selected. The maxillary arch was bonded with standard torque brackets except for high torque brackets on the canines. The upper arch was fitted with a.4 CuNiTi archwire (Fig. Fig. : The maxillary arch was bonded with Damon Q Clear with standard torque brackets on the incisors and high torque brackets on the canines. A.3 CuNiTi archwire was inserted. ), followed by the sequence for.8 CuNiTi, rectangular.4x.25 CuNiTi,.7x.25 TMA, and.9x.25 pre-torqued CuNiTi. One month later, the lower arch was bonded with low torque brackets and an.4 CuNiTi archwire was placed. The subsequent archwire sequence was.8 CuNiTi, rectangular.4x.25 CuNiTi, and.7x.25 TMA for detailing. In order to open space for the lower 2 nd premolars, open coil springs were applied bilaterally between the st premolars and st molars (Fig. ). Drop in hooks were inserted into the brackets of the upper st premolars. The patient was instructed to wear Class II early light short elastics (Parrot 5/6, 2 oz) bilaterally full time. The elastics extended from the upper st premolar to the lower st molar bilaterally to retract the upper anterior teeth and reduce the overjet (Fig. 2). Anterior bite turbos were bonded on both upper central incisors to help correct the deep bite (Fig. 3). After 8 th months of initial alignment and leveling in 68

.")


 were used to reduce the overjet.")
6 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 both arches, 2x2 mm stainless steel mini-screws (OrthoBoneScrew, Newton s A Ltd., Hsinchu, Taiwan) were inserted in the infrazygomatic crests bilaterally. Elastometric chains from the bone screws to the upper canines were used to retract the maxillary anterior segment (Fig. 4). M Fig. : Open coil springs were applied bilaterally between the st premolars and st molars to open the space for the 2 nd premolars. One year after the initiation of treatment, spaces between the st premolars and st molars was created with open coil springs, and brackets were bonded on the lower 2 nd premolars (Fig. 5). Since M Fig. 2: Class II elastics (Parrot 5/6, 2 oz) were used to reduce the overjet. 8M Fig. 4: OrthoBoneScrew mini-screws were implanted bilaterally in the infrazygomatic crests as anchorage to retract the maxillary dentition. 3M Fig. 3: After the initial alignment of the maxillary arc, anterior bite turbos were bonded on both upper central incisors to correct the deep bite. 2M Fig. 5: The 2 nd premolars brackets were bonded once adequate space was obtained. A lingual button was bonded on the lower right 2 nd premolar. 69

 In the 22 month, a maxillary.9x.")
.")
 was applied from the upper 2nd premolar to the lower 2nd premolar to correct the buccal crossbite. 3M 22M 7 Fig. 7: An.9x.")
7 IJOI 35 iaoi CASE REPORT the lower right 2nd premolar was still tilted lingually, (Fig. 8). Brackets were repositioned to achieve the a lingual button was bonded on it. A cross elastic desired outcome. (Chipmunk /8, 3.5 oz ) was applied from upper 2 nd premolar to lower 2nd premolar to correct the buccal One month before removing all fixed appliances, the crossbite (Fig. 6). upper archwire was sectioned distal to the canines, and continuous vertical elastics (Ostrich 3/4, 2 oz) In the 22 month, a maxillary.9x.25 pre-torqued were utilized to settle the occlusion (Fig. 9).5 Once archwire was inserted to apply lingual root torque to an optimal finished occlusion was achieved, all fixed the anterior segment (Fig. 7). A progress panoramic appliances were removed. The total active treatment radiograph was taken to evaluate axial inclinations time was 32 months. nd 29M 2M Fig. 6: A cross elastic (Chipmunk /8, 3.5 oz) was applied from the upper 2nd premolar to the lower 2nd premolar to correct the buccal crossbite. 3M 22M 7 Fig. 7: An.9x.25 maxillary pre-torqued archwire was uses to apply lingual root torque in the anterior segment. Fig. 8: A progress panoramic radiography was taken to evaluate axial inclinations: brackets were repositioned on teeth marked with blue lines. Fig. 9: To settle the posterior occlusion, the upper archwire was sectioned distal to the canine, continuous intermaxillary elastics (Ostrich 3/4, 2 oz) were prescribed.
8 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 Results Achieved Maxilla (all three planes): A - P: Maintained Vertical: Maintained Transverse: Maintained Mandible (all three planes): A - P: Retracted Vertical: Increased with a clockwise rotation of the mandible Transverse: Maintained Maxillary Dentition A - P: a. Molars: Retracted b. Incisors: Tipped labially Vertical: a. Molars: Maintained b. Incisors: Maintained Inter-molar Width: Expanded Inter-canine Width: Maintained Buccolingual Inclination: Maintained Mandibular Dentition A - P: a. Molars: Retracted b. Incisors: Tipped labially (9 to mandibular plane) Vertical: a. Molars: Maintained b. Incisors: Maintained Inter-molar Width: Expanded Inter-canine Width: Maintained Buccolingual Inclination: Uprighted Facial Esthetics: Lip profile retracted, despite posterior mandibular rotation, facial convexity was unchanged Retention Fixed retainers were bonded to each tooth in the upper 2-2 and lower 3-3 areas. Upper and lower clear overlay retainers were delivered with instructions to wear them full time for the first 6 months and nights only thereafter. Home hygiene and retainer care instructions were provided. Final Evaluation of Treatment The ABO Cast-Radiograph Evaluation (CRE) score was 22 points, which indicated an optimal dental alignment for this challenging malocclusion. The large overjet and deep bite were corrected, but significant discrepancies were noted for occlusal relationships (Fig. 2) and alignment of second molars (Fig. 2). The dental esthetics were good as documented by the IBOI Pink & White Esthetic score of 3. However, there was a minor deficiencies in maxillary middling papilla, incisal curvature (smile arc) axial inclination of incisors. Overall, the lingually tipped upper central incisors and the flared lateral incisors were well aligned, considering the skeletal 7

.")
 because the excellent dental result (CRE 22), treatment was completed in 32 months, and an")


9 IJOI 35 iaoi CASE REPORT Fig. 2: The occlusal relationships for canines and premolars were still slightly Class II on the finish casts. Fig. 22: The excessive gingival display when smiling was improved and the patient is satisfied with her smile. the increase in the vertical dimension of occlusion would probably increase the treatment time and result in an inferior overall outcome. -3 Discussion Fig. 2: The second molars were not well aligned. limitations (ANB 9 ). Improved axial inclination of the maxillary incisors resulted in less gingival exposure when smiling: gingivectomy was not necessary (Fig. 22). The 4 posterior rotation of the mandible did not compromise the facial profile, but it did require excessive inclination of the lower incisor to correct the overjet. However, the treatment was considered optimal for this difficult malocclusion (DI 37) because the excellent dental result (CRE 22), treatment was completed in 32 months, and an acceptable facial result was achieved. Attempting to avoid The Class II/2 pattern of malocclusion exhibits complex characteristics such as severe anterior crowding, with retroclined maxillary central incisors/ lateral incisors and flared maxillary lateral incisors/ canines, deep overbite, and retrusive mandibular or short lower anterior face height. 6 Class II/2 malocclusion is relatively rare in the Chinese population, with an incidence of.5%-5%, 7 but it is a very challenging to treat and has a high risk of relapse. 8 Treatment for Class II/2 requires careful diagnosis and a treatment plan involving esthetics, occlusion, and function. It is critical to analyze patient s facial profile, skeletal pattern, and severity of dental malocclusion carefully in the treatment plan as well. 9 The objective of treatment for Class II/2 usually involves correcting the intrusion of the 72


10 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 upper incisors and deep overbite and achieving a satisfactory skeletal, dental, and soft tissue relationship. Depending on the patient s age and growth potential, there are several options for treating this Class II/2 malocclusion, e.g., fixed and functional appliances, headgears, and orthognathic surgery. However, it is important to choose an efficient option to complete the correction in <36 months to avoid compromises associated with extended treatment times. -3 The present patient preferred nonsurgical orthodontic treatment to minimize the risk of facial compromise. Extraction treatment for Class II/2 has a tendency to flatten the facial profile and deepen the bite. Pitts 2 suggests: Only extract for the face, not for the space! The patient s pre-treatment cephalometric radiograph (Fig. 7) showed a slightly protruded profile for both lips due to the flaring of the upper lateral incisors and fairly narrow arches. A non-extraction treatment plan was indicated and the Damon self-ligating system was selected. Using Damon self-ligating brackets and NiTi archwires, the variable torque control brackets allow the roots of the teeth to begin to upright during the leveling phase. With variable torque brackets, the upper anterior teeth are readily leveled and aligned. 3 This preliminary alignment provided space for the lower segment to be bonded (Fig. 2). At the same appointment, anterior bite turbos were placed on the upper central incisors (Fig. 3). Anterior bite turbos are excellent tools for the correction of deep bite if opening the bite and posterior mandibular rotation are acceptable mechanics. They are easy to use and decrease the treatment time for many patients. However, for lingually tipped upper central incisors, the line of occlusal force may be lingual to the center of resistance (CR) which can result in more lingual tipping. Thavarungkul 4 suggests bonding the anterior bite turbos after both central incisors have been proclined slightly. This allows the force vector to pass in anterior of CR in order to correct the deep bite (Fig. 23). Cr Cr Cr Cr Fig. 23: Left: If anterior bite turbos are applied before the initial alignment of the incisors, the line of occlusal force may be distal to the center of resistance (CR) resulting in more lingual tipping. Right: After some labial movement of the maxillary central incisor crowns, the line of force (green) is labial to CR which is a preferable force system. (Diagram Courtesy of Dr. Rungsi Thavarungkul) 4 73
11 IJOI 35 iaoi CASE REPORT In addition, early light elastics also play an important role in correcting deep bite and aligning the anterior teeth. Using early light short elastics has the advantage of controlling the vertical dimension without decreasing the smile arch and sagittal correction in the early stage of treatment for deep bite. The light force reduces the side effects of the horizontal component of force which can produce unnecessary tipping of the teeth. Pitts 5 also suggests, keeping the elastics distal to facilitate posterior extrusion for the deep bite case. For the present patient, anterior bite turbos and Class II elastics resolved the overjet problem, but extruded the mandibular molars, which increased the mandibular plane angle due to posterior rotation of the mandible. However, this skeletal compromise was indicated to meet the patient s objectives and control the duration of treatment. Extended treatment times for difficult malocclusions often result in inferior results. -3 For Class II/2 malocclusion, anchorage control is one of the most difficult problems. En masse movement of the anterior segment and improvement in the facial profile can be accomplished with E-A miniscrew anchorage. 6 Miniscrew anchorage is an effective tool for improving maxillary incisor inclination consistent with a proper molar relationship. 7-9 It is also a minimally intrusive method that reduces treatment time and simplifies mechanics for managing dentoalveolar protrusion. 2 Studies have shown miniscrew anchorage or headgear can achieve acceptable results for the retraction of incisors. However, with miniscrew anchorage, it does not require patient cooperation SKELETAL ANALYSIS CEPHALOMETRIC PRE-Tx POST-Tx DIFF. SNA SNB ANB 9 9 SN-MP FMA DENTAL ANALYSIS U TO NA mm -3 mm - mm 2 mm U TO SN L TO NB mm 4 mm 7 mm 3 mm L TO MP FACIAL ANALYSIS E-LINE UL 2 mm mm 2 mm E-LINE LL mm mm mm Table : Cephalometric summary and minimal pain is associated E-A miniscrew can improve the facial profile of Class II/2 patients without wearing an inconvenient and embarrassing headgear device. Conclusion Skeletal Class II/2 with a deep bite and severe crowding is a challenging malocclusion that may require facial compromise to attain an optimal result in minimal treatment time. Infrazygomatic crest miniscrew anchorage is effective for retracting the maxillary arch. Moreover, anterior bite turbos are effective appliances for resolving deep bite, but they increase the vertical dimension of occlusion, which increases overjet and the mandibular plane. 74


12 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 Combined miniscrew anchorage and anterior bite turbos are an efficient option for treating Class II/2, but judicious application of the mechanics and management of side effects are required. References. Campbell CL, Roberts WE, Hartsfield JK Jr, Qi R. Treatment outcomes in a graduate orthodontics clinic for cases defined by the American Board of Orthodontics malocclusion categories. Am J Orthod Dentofacial Orthop 27;32: Knierim K, Roberts WE, Hartsfield JK Jr. Assessing treatment outcomes for a graduate orthodontics program: Follow-up study for the classes of Am J Orthod Dentofacial Orthop 26;3: Pinskaya YB, Hsieh T-J, Roberts WE, Hartsfield JK Jr. Comprehensive clinical evaluation as an outcome assessment for a graduate orthodontics program. Am J Orthod Dentofacial Orthop 24;26: Hartsfield JK. Genetics and orthodontics. Chapter 3 in Orthodontics: Current principles & techniques, Graber TM, Vanarsdall RL Jr, Vig KWL, Elsevier Mosby, St. Louis, 25, pp Steffen JM, Haltom FT. The five-cent tooth positioner. J Clin Ortho 987 Aug;2(8): Garlapati Y, Jadav CL, Kolasani SR, Mummidi B. Management of sever class II division II malocclusion using simplified MPA A case report. APOS Trends Orthod 23;3: Lin JJ. Prevalence of malocclusion in Chinese children age 9-5. Taiwan Clin Dent 985;5: Canut JA, Arias S. A long-term evaluation of treated Class II division 2 malocclusions: a retrospective study model analysis. European Journal of Orthodontics 999;2: Flavio U, Ravindra N. Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations. Journal of Clinic Orthodontics 23;37(): Chen YJ, Yao CC, Chang JF. Nonsurgical correction of skeletall deep overbite and class II division 2 malocclusion in an adult patient. Am J Orthod & Dentolfacial Orthop 24 Sep;26(3): Lee TH. Cephalometric predictor variables for treatment o f C l a s s I I D iv i s i o n 2 m a l o c c l u s i o n s. J D e n t S c i 26;(): Pitts T. The Secrets of Excellent Finishing. News & Trends in Orthod 29 Apr.;4: Kozlowski J. Honing Damon System Mechanics for the Ultimate in Efficiency and Excellence. Clinical Impression 23;9(): Thavarungkul R. Correcting Deep-bite with Fixed Bite Ramps. News & Trends in Orthod 29 Oct. ;6: Chang CH. Advanced Damon Course No. 7: Deep bite correction. Beethoven Podcast Encyclopedia in Orthodontics. Hsinchu: Newton s A Ltd; Chang CH. Damon Q Course No. 3-2: Class II Mechanics. Beethoven Podcast Encyclopedia in Orthodontics. Hsinchu: Newton s A Ltd; Chang CH, Roberts WE. Stability of Mini-screws on Buccal Shelves: A Retrospective Study of 68 Mini-screw Insertions by the Same Orthodontist. Int J Orthod Implantol 23;3: Chang CH, Roberts WE. A Retrospective Study of the Extraalveolar Screw Placement on Buccal Shelves. Int J Orthod Implantol 23;32: Park HS, Kwon OW, Sung JH. Microscrew implant anchorage sliding mechanics. World Journal of Orthodontics 25;6(3): Kuroda S, Yamada K, Deguchi T, Kyung HM, Yamamoto TT. Class II malocclusion treated with miniscrew anchorage: Comparison with traditional orthodontic mechanics outcomes. Am J Orthod & Dentofacial Orthopedics 29 Mar;35(3): Chang CH. Advanced Damon Course No. 4,5 : DI & CRE Workshop ()(2). BeethovenPodcast Encyclopedia in Orthodontics. Hsinchu: Newton s A Ltd; Chang CH, Roberts WE. Orthodontics, 3D i-ortho encyclopedia. Hsinchu: Newton s A Ltd;
13 IJOI 35 iaoi CASE REPORT Discrepancy Index Worksheet (Rev. 9/22/8) TOTAL D.I. SCORE 25 OVERJET mm. (edge-to-edge) = pt. Ð 3 mm. = pts. 3. Ð 5 mm. = 2 pts. 5. Ð 7 mm. = 3 pts. 7. Ð 9 mm. = 4 pts. > 9 mm. = 5 pts. Negative OJ (x-bite) pt. per mm. per tooth = OVERBITE Total = 5 Ð 3 mm. = pts. 3. Ð 5 mm. = 2 pts. 5. Ð 7 mm. = 3 pts. Impinging (%) = 5 pts. Total = 5 ANTERIOR OPEN BITE 37 mm. (edge-to-edge), pt. per tooth then pt. per additional full mm. per tooth 4 5 Total = LINGUAL POSTERIOR X-BITE pt. per tooth Total = BUCCAL POSTERIOR X-BITE 2 pts. per tooth Total = 2 CEPHALOMETRICS (See Instructions) ANB 6 or -2 = 4 pts. Each degree < -2 x pt. = Each degree > 6 x pt. = SN-MP 38 = 2 pts. Each degree > 38 x 2 pts. = 26 = pt. Each degree < 26 4 x pt. = 4 to MP 99 = pt. Each degree > 99 2 x pt. = LATERAL OPEN BITE 2 pts. per mm. per tooth OTHER (See Instructions) 7 Total = 8 76 CROWDING (only one arch) Ð 3 mm. = pt. 3. Ð 5 mm. = 2 pts. 5. Ð 7 mm. = 4 pts. > 7 mm. = 7 pts. OCCLUSION Total = Total = Class I to end on = pts. End on Class II or III = 2 pts. per side pts. Full Class II or III = 4 pts. per side pts. Beyond Class II or III = pt. per mm. pts. additional Total = 7 Supernumerary teeth x pt. = Ankylosis of perm. teeth x 2 pts. = Anomalous morphology x 2 pts. = Impaction (except 3 rd molars) x 2 pts. = Midline discrepancy ( 2 pts. = Missing teeth (except 3 rd molars) x pts. = Missing teeth, congenital x 2 pts. = Spacing (4 or more, per arch) x 2 pts. = 2 Spacing (Mx cent. diastema 2 pts. = 2 Tooth transposition x 2 pts. = Skeletal asymmetry (nonsurgical 3 pts. 2 = Addl. treatment complexities x 2 pts. = Identify: Irregular facial surface was found on the upper left central incisor. 2. Molar relationship was supposed to be full Class II on both side but the mandibular st molars mesially shifted due to the mandibular 2 nd premolars were lingual blocked-in. Total = 4 6





14 Crowded Class II Division 2 Malocclusion with Class I Molars Due to Blocked In Lower Second Premolars IJOI 35 Cast-Radiograph Evaluation Occlusal Contacts 3 Total Score: 22 Alignment/Rotations Marginal Ridges 4 Occlusal Relationships 6 Buccolingual Inclination 4 Interproximal Contacts Overjet Root Angulation INSTRUCTIONS: Place score beside each deficient tooth and enter total score for each parameter in the white box. Mark extracted teeth with ÒXÓ. Second molars should be in occlusion. 77
15 IJOI 35 iaoi CASE REPORT IBOI Pink & White Esthetic Score Total Score: = 3. Pink Esthetic Score Total = M & D Papillae 2 2. Keratinized Gingiva 2 3. Curvature of Gingival Margin 2 4. Level of Gingival Margin 2 5. Root Convexity ( Torque ) 2 6. Scar Formation 2. M & D Papillae 2 2. Keratinized Gingiva 2 3. Curvature of Gingival Margin 2 4. Level of Gingival Margin 2 5. Root Convexity ( Torque ) 2 6. Scar Formation 2 2. White Esthetic Score ( for Micro-esthetics ) Total = 2. Midline 2 2. Incisor Curve Axial Inclination (5, 8, ) 2 4. Contact Area (5%, 4%, 3%) 2 5. Tooth Proportion (:.8) 2 6. Tooth to Tooth Proportion 2. Midline 2 2. Incisor Curve 2 3. Axial Inclination (5, 8, ) 2 4. Contact Area (5%, 4%, 3%) 2 5. Tooth Proportion (:.8) 2 6. Tooth to Tooth Proportion 2 78
Crowded Class II Division 2 Malocclusion
 Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Class II Division 2 Malocclusion Crowded Class II Division 2 Malocclusion Clinicians: Drs. Chris Chang, Hsin-Yin Yeh, Sophia Pei-Wen Shu, W. Eugene Roberts Patient: Miss Jhan Pre-treatment Diagnosis An
Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction
 Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Case Report Case Report: Long-Term Outcome of Class II Division 1 Malocclusion Treated with Rapid Palatal Expansion and Cervical Traction Roberto M. A. Lima, DDS a ; Anna Leticia Lima, DDS b Abstract:
Class II Malocclusion with Crowding, Missing LR2 and Ectopic Eruption of UR3 is Treated Conservatively with Maxillary Retraction
 JDO 50 iaoi CASE REPORT Class II Malocclusion with Crowding, Missing LR and Ectopic Eruption of UR3 is Treated Conservatively with Maxillary Retraction Abstract Introduction: A -year-old female presented
JDO 50 iaoi CASE REPORT Class II Malocclusion with Crowding, Missing LR and Ectopic Eruption of UR3 is Treated Conservatively with Maxillary Retraction Abstract Introduction: A -year-old female presented
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER:44 CASE NUMBER: 2 Year: 2010 ESLO 01 RÉSUMÉ OF CASE 5 CASE CATEGORY: CLASS II DIVISION 1 MALOCCLUSION A MALOCCLUSION WITH SIGNIFICANT MANDIBULAR
Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction Treatment?
 TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
TURKISH JOURNAL of DOI: 10.5152/TurkJOrthod.2017.17034 CASE REPORT Treatment of Class II, Division 2 Malocclusion with Miniscrew Supported En-Masse Retraction: Is Deepbite Really an Obstacle for Extraction
Trans-Alveolar Uprighting of a Horizontally Impacted Lower Canine with a Mandibular Buccal Shelf Bone Screw
 IJOI 6 iaoi CASE REPORT Trans-Alveolar Uprighting of a Horizontally Impacted Lower Canine with a Mandibular Buccal Shelf Bone Screw Abstract A yr 6m female presented with an unerupted mandibular left canine
IJOI 6 iaoi CASE REPORT Trans-Alveolar Uprighting of a Horizontally Impacted Lower Canine with a Mandibular Buccal Shelf Bone Screw Abstract A yr 6m female presented with an unerupted mandibular left canine
Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results.
 SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
SM 3M Health Care Academy Lingual correction of a complex Class III malocclusion: Esthetic treatment without sacrificing quality results. Christopher S. Riolo, DDS, M.S, Ph.D. Dr. Riolo received his DDS
The Tip-Edge appliance and
 Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
Figure 1: Internal surfaces of the edgewise archwire slot are modified to create the Tip-Edge archwire slot. Tipping surfaces (T) limit crown tipping during retraction. Uprighting surfaces (U) control
A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
 Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Dhaval Ranjitbhai Lekhadia, Gautham Hegde RESEARCH ARTICLE 10.5005/jp-journals-10029-1149 A Modified Three-piece Base Arch for en masse Retraction and Intrusion in a Class II Division 1 Subdivision Case
Angle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy*
 O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
O C a s e R e p o r t ngle Class II, division 2 malocclusion with severe overbite and pronounced discrepancy* Daniela Kimaid Schroeder** bstract This article reports the treatment of a young patient at
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER: 44 CASE NUMBER: 1 Year: ESLO 01 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME: K.N BORN: 03/03/1980 SEX: Male PRE-TREATMENT RECORDS:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS CANDIDATE NUMBER : 13 Dr. Masatoshi Sana CASE NUMBER : Year : ESLO 01 RÉSUMÉ OF CASE 2 CASE CATEGORY: CLASS I MALOCCLUSION NAME: BORN: SEX: Yukari K. 08/03/1979
Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics
 Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Case Report Nonsurgical Treatment of Adult Open Bite Using Edgewise Appliance Combined with High-Pull Headgear and Class III Elastics Isao Saito, DDS, PhD a ; Masaki Yamaki, DDS, PhD b ; Kooji Hanada,
Angle Class II, division 2 malocclusion with deep overbite
 BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
BBO Case Report Angle Class II, division 2 malocclusion with deep overbite Arno Locks 1 Angle Class II, division 2, malocclusion is characterized by a Class II molar relation associated with retroclined
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1*
 UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
UNILATERAL UPPER MOLAR DISTALIZATION IN A SEVERE CASE OF CLASS II MALOCCLUSION. CASE PRESENTATION. 1* Department of Orthodontics and Pedodontics 1 Faculty of Dental Medicine, University of Medicine and
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth
 Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
Angle Class I malocclusion with anterior open bite treated with extraction of permanent teeth Matheus Melo Pithon 1 This clinical case reports the orthodontic treatment of a Class I malocclusion with anterior
The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain
 Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
Welcome Ron Not Ron? Click here. My Account The Tip-Edge Concept: Eliminating Unnecessary Anchorage Strain VOLUME 26 : NUMBER 03 : PAGES (165-178) 1992 CHRISTOPHER K. KESLING, DDS, MS Tooth movement in
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTISTS Dr. Masatoshi Sana Year: ESLO 01 RÉSUMÉ OF CASE 8 CASE CATEGORY: TRANS / VERTICAL DISCREPANCY NAME: Akiko T. BORN : 15/03/1973 SEX: F PRE-TREATMENT RECORDS: AGE:
Intraoral molar-distalization appliances that
 2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
2014 JCO, Inc. May not be distributed without permission. www.jco-online.com Distalization with the Miniscrew- Supported EZ Slider Auxiliary ENIS GÜRAY, DDS, PHD FARUK IZZET UCAR, DDS, PHD NISA GUL, DDS
Correction of Crowding using Conservative Treatment Approach
 Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
Case Report Correction of Crowding using Conservative Treatment Approach Dr Tapan Shah, 1 Dr Tarulatha Shyagali, 2 Dr Kalyani Trivedi 3 1 Senior Lecturer, 2 Professor, Department of Orthodontics, Darshan
ORTHODONTICS Treatment of malocclusion Assist.Lec.Kasem A.Abeas University of Babylon Faculty of Dentistry 5 th stage
 Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
Lec: Treatment of class I malocclusion Class I occlusion can be defined by Angles, classification as the mesiobuccal cusp of the upper 1 st permanent molar occlude with the developmental groove of the
The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding
 B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
B B O C a s e R e p o r t The conservative treatment of Class I malocclusion with maxillary transverse deficiency and anterior teeth crowding Lincoln I. Nojima* Abstract This report describes the treatment
Gentle-Jumper- Non-compliance Class II corrector
 15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
15 CASE REPORT Gentle-Jumper- Non-compliance Class II corrector Amit Prakash 1,O.P.Mehta 2, Kshitij Gupta 3 Swapnil Pandey 4 Deep Kumar Suryawanshi 4 1 Senior lecturer Bhopal - INDIA 2 Professor Bhopal
Simple Mechanics to Upright Horizontally Impacted Molars with Ramus Screws
 Simple Mechanics to Upright Horizontally Impacted Molars with Ramus Screws Abstract Simplified mechanics are reported for uprighting horizontally impacted mandibular molars with ramus bone screws. A 27-year-old
Simple Mechanics to Upright Horizontally Impacted Molars with Ramus Screws Abstract Simplified mechanics are reported for uprighting horizontally impacted mandibular molars with ramus bone screws. A 27-year-old
Correction of Class II Division 2 Malocclusion by Fixed Functional Class II Corrector Appliance: Case Report
 Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
Case Report To cite: Kumar M, Sharma H, Bohara P. Correction of class II division 2 malocclusion by fixed functional class II corrector appliance: case report. Journal of contemporary orthodontics, February
The ASE Example Case Report 2010
 The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
The ASE Example Case Report 2010 The Requirements for Case Presentation in The Angle Society of Europe are specified in the Appendix I to the Bylaws. This example case report exemplifies how these requirements
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD
 REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
REPRINTED FROM JOURNAL OF CLINICAL ORTHODONTICS 1828 PEARL STREET, BOULDER, COLORADO 80302 Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS
ORTHODONTIC CORRECTION Of OCCLUSAL CANT USING MINI IMPLANTS:A CASE REPORT. Gupta J*, Makhija P.G.**, Jain V***
 ORTHODONTIC CORRECTION Of OCCLUSAL CANT USING MINI IMPLANTS:A CASE REPORT Gupta J*, Makhija P.G.**, Jain V*** Abstract: The inability of orthodontists to change the cant of the maxillary occlusal plane
ORTHODONTIC CORRECTION Of OCCLUSAL CANT USING MINI IMPLANTS:A CASE REPORT Gupta J*, Makhija P.G.**, Jain V*** Abstract: The inability of orthodontists to change the cant of the maxillary occlusal plane
Case Report n 2. Patient. Age: ANB 8 OJ 4.5 OB 5.5
 Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Case Report n 2 Patient Age: 12.11 Diagnosis Angle cl.ii div.2 ANB 8 OJ 4.5 OB 5.5 Author: Dr. Case History The patient is a thirteen year old girl who exhibits delayed development, both physically and
Bimaxillary Protrusion Treated with Insignia System Customized Brackets and Archwires
 IJOI 48 iaoi CASE REPORT Bimaxillary Protrusion Treated with Insignia System Customized Brackets and Archwires Abstract Introduction: Correction of bimaxillary protrusion is challenging, particularly without
IJOI 48 iaoi CASE REPORT Bimaxillary Protrusion Treated with Insignia System Customized Brackets and Archwires Abstract Introduction: Correction of bimaxillary protrusion is challenging, particularly without
Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm.
 Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Chapter 16 Clinical cases: mixed dentition and adolescent, CLII non-extraction 219 Full CLII div I OJ = 15 OB = 8 SNA = 82 SNB = 75 Mx1 to NA = 34 & 10 mm. Md1 to NB = 21 & 3 mm. Md1 to A-pog = -2 GO-GN
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
ortho case report Sagittal First international magazine of orthodontics By Dr. Luis Carrière Special Reprint
 Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Cover image courtesy of K Line Europe GmbH (www.kline-europe.de) ortho Special Reprint international magazine of orthodontics 1 2017 case report Sagittal First By Dr. Luis Carrière Sagittal First Author:
Class III malocclusion occurs in less than 5%
 CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
CDABO CASE REPORT Orthodontic correction of a Class III malocclusion in an adolescent patient with a bonded RPE and protraction face mask Steven W. Smith, DDS, a and Jeryl D. English, DDS, MS b Dallas,
SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 SURGICAL - ORTHODONTIC TREATMENT OF CLASS II DIVISION 1 MALOCCLUSION IN AN ADULT PATIENT: A CASE REPORT Amit Dahiya 1,Minakshi
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
ISW for the treatment of moderate crowding dentition with unilateral second molar impaction
 International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
International Research Journal of Public and Environmental Health Vol.5 (6),pp. 90-103, September 2018 Available online at https://www.journalissues.org/irjpeh/ https://doi.org/10.15739/irjpeh.18.013 Copyright
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: Dr. Stefan Blasius Year: 2010 WBLO 01 RÉSUMÉ
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D
 by Masatada Koga, D.D.S., Ph.D") MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
MBT System as the 3rd Generation Programmed and Preadjusted Appliance System (PPAS) by Masatada Koga, D.D.S., Ph.D Dr. Masatada Koga, D.D.S., Ph.D, is an assistant professor in the Department of Orthodontics
Case Report. profile relaxed relaxed smiling. How would you treat this malocclusion?
 Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
Pre-Treatment profile relaxed relaxed smiling How would you treat this malocclusion? Case R. C. 16 years, 9 months introduction This female adolescent with bilabial protrusion and flared upper anterior
KJLO. A Sequential Approach for an Asymmetric Extraction Case in. Lingual Orthodontics. Case Report INTRODUCTION DIAGNOSIS
 KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
KJLO Korean Journal of Lingual Orthodontics Case Report A Sequential Approach for an Asymmetric Extraction Case in Lingual Orthodontics Ji-Sung Jang 1, Kee-Joon Lee 2 1 Dream Orthodontic Clinic, Gimhae,
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 1 Year: 2010 WBLO 01 RESUME OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME : IOANNIS.G BORN: 03.01.1989 SEX:
The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions
 Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Journal of Orthodontics/Vol. 28/2001/271 280 The Modified Twin Block Appliance in the Treatment of Class II Division 2 Malocclusions F. M. V. DYER H. F. MCKEOWN P. J. SANDLER Department of Orthodontics,
Case Report Unilateral Molar Distalization: A Nonextraction Therapy
 Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Case Reports in Dentistry Volume 2012, Article ID 846319, 4 pages doi:10.1155/2012/846319 Case Report Unilateral Molar Distalization: A Nonextraction Therapy M. Bhanu Prasad and S. Sreevalli Department
Low-Force Mechanics Nonextraction. Estimated treatment time months (Actual 15 mos 1 week). Low-force mechanics.
. Low-force mechanics.") T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report
 Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
Case Report Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/506 Class II Correction using Combined Twin Block and Fixed Orthodontic Appliances: A Case Report Ahmed Alassiry Assistant
2008 JCO, Inc. May not be distributed without permission. Correction of Asymmetry with a Mandibular Propulsion Appliance
 2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
2008 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT Correction of Asymmetry with a Mandibular Propulsion Appliance JOSÉ AUGUSTO MENDES MIGUEL, DDS, MSC, PHD GUSTAVO
Treatment of a severe class II division 1 malocclusion with twin-block appliance
 2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
2018; 4(5): 167-171 ISSN Print: 2394-7500 ISSN Online: 2394-5869 Impact Factor: 5.2 IJAR 2018; 4(5): 167-171 www.allresearchjournal.com Received: 27-03-2018 Accepted: 28-04-2018 Dr. Sheetal Bohra Resident
Keeping all these knowledge in mind I will show you 3 cases treated with the Forsus appliance.
 Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Due to technical difficulties there were some audio problems with the webinar recording. Starting at 27:54, please use this guide to follow along with Dr. Kercelli s presentation. Keeping all these knowledge
Early Mixed Dentition Period
 REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
REVIEW ARTIC CLE AODMR The Effects of a Prefabricated Functional Appliance in Early Mixed Dentition Period Toshio Iwata 1, Takashi Usui 2, Nobukazu Shirakawa 2, Toshitsugu Kawata 3 1 Doctor of Philosophy
Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment
 The Angle Orthodontist: Vol. 78, No. 1, pp. 181 188. Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment Eiji Tanaka; a Akiko Nishi-Sasaki;
The Angle Orthodontist: Vol. 78, No. 1, pp. 181 188. Skeletal Anchorage for Orthodontic Correction of Severe Maxillary Protrusion after Previous Orthodontic Treatment Eiji Tanaka; a Akiko Nishi-Sasaki;
OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS CANDIDATE NUMBER: KDr. KP. kanarelis CASE NUMBER: 2 Year: 2010 WBLO 01 RESUME OF CASE 2 CASE CATEGORY: ADULT MALOCCLUSION NAME : MARIA A. BORN: 18.04.1983 SEX:
Correction of a maxillary canine-first premolar transposition using mini-implant anchorage
 CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
CASE REPORT Correction of a maxillary canine-first premolar transposition using mini-implant anchorage Mehmet Oguz Oztoprak, DDS, MSc, a Cigdem Demircan, DDS, b Tulin Arun, PhD, DDS, MSc c Transposition
Experience with Contemporary Tip-Edge plus Technique A Case Report.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 13, Issue 3 Ver. I. (Mar. 2014), PP 12-17 Experience with Contemporary Tip-Edge plus Technique A Case
Class I. Clear Fixed Appliance vs. Aligner Treatment for Arch Development. Clinician: Dr. Stuart Frost, Phoenix, AZ Patient: A.M.
 Clear Fixed Appliance vs. Aligner Treatment for Arch Development Class I End-to-End Molar Clinician: Dr. Stuart Frost, Phoenix, AZ Patient: A.M. Pretreatment Diagnosis Class I (end-to-end molar on right),
Clear Fixed Appliance vs. Aligner Treatment for Arch Development Class I End-to-End Molar Clinician: Dr. Stuart Frost, Phoenix, AZ Patient: A.M. Pretreatment Diagnosis Class I (end-to-end molar on right),
Orthodontic Treatment Using The Dental VTO And MBT System
 Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Orthodontic Treatment Using The Dental VTO And MBT System by Dr. Hideyuki Iyano Dr. Hideyuki Iyano, Department of Orthodontics, Ohu University School of Dentistry, Japan. He is also a member of the Japan
Clinical efficacy of Invisalign treatment with weekly aligner changes: Two case reports
 Clinical efficacy of Invisalign treatment with weekly aligner changes: Two case reports Class II and deep bite correction with the Invisalign System and weekly aligner changes. Dr Schupp and Dr Haubrich
Clinical efficacy of Invisalign treatment with weekly aligner changes: Two case reports Class II and deep bite correction with the Invisalign System and weekly aligner changes. Dr Schupp and Dr Haubrich
Sample Case #1. Disclaimer
 ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
ABO Sample Cases Disclaimer Sample Case #1 The following sample questions and answers were composed and vetted by a panel of experts in orthodontics and are intended to provide an example of the types
An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case
 10.5005/jp-journals-10021-1127 CASE REPORT An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case 1 Anil Miglani, 2 Reena R Kumar, 3 Ashish Chopra,
10.5005/jp-journals-10021-1127 CASE REPORT An Innovative Treatment Approach with Atypical Orthodontic Extraction Pattern in Bimaxillary Protrusion Case 1 Anil Miglani, 2 Reena R Kumar, 3 Ashish Chopra,
Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report
 Journal oforthodontîcz^ol 40, 2013, 256-263! CLINICAL SECTION Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report Marcel Marchiori Farret^
Journal oforthodontîcz^ol 40, 2013, 256-263! CLINICAL SECTION Skeletal class III maloeclusion treated using a non-surgieal approach supplemented with mini-implants: a case report Marcel Marchiori Farret^
Orthodontic mini-implants have revolutionized
 CASE REPORT Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II Division 2 patient Tae-Woo Kim, a Hyewon Kim, b and Shin-Jae Lee c Seoul, South
CASE REPORT Correction of deep overbite and gummy smile by using a mini-implant with a segmented wire in a growing Class II Division 2 patient Tae-Woo Kim, a Hyewon Kim, b and Shin-Jae Lee c Seoul, South
ADOLESCENT TREATMENT. Thomas J. Cangialosi. Stella S. Efstratiadis. CHAPTER 18 Pages CLASS II DIVISION 1 WHY NOW?
 ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
ADOLESCENT By Thomas J. Cangialosi and Stella S. Efstratiadis From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice, EFOP Press of EFOP, LLC. Ann Arbor and Grand Haven, Michigan, U.S.A.,
2007 JCO, Inc. May not be distributed without permission.
 2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
2007 JCO, Inc. May not be distributed without permission. www.jco-online.com CSE REPORT Correction of an symmetrical Class II Malocclusion Using Predictable Force Systems PIERO PLCIOS, DDS, MDS FLVIO URIBE,
Treatment of a malocclusion characterized
 CONTINUING EDUCATION ARTICLE Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics Nazan Küçükkeleș, DDS, PhD, a Ahu Acar, DDS, PhD, b Arzu A. Demirkaya, DDS, c Berna
CONTINUING EDUCATION ARTICLE Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics Nazan Küçükkeleș, DDS, PhD, a Ahu Acar, DDS, PhD, b Arzu A. Demirkaya, DDS, c Berna
The treatment options for nongrowing skeletal Class
 CASE REPORT Total distalization of the maxillary arch in a patient with skeletal Class II malocclusion Yoon Jeong Choi, a Jong-Suk Lee, b Jung-Yul Cha, c and Young-Chel Park d Seoul, Korea In nongrowing
CASE REPORT Total distalization of the maxillary arch in a patient with skeletal Class II malocclusion Yoon Jeong Choi, a Jong-Suk Lee, b Jung-Yul Cha, c and Young-Chel Park d Seoul, Korea In nongrowing
Transverse malocclusion, posterior crossbite and severe discrepancy*
 O C a s e R e p o r t Transverse malocclusion, posterior crossbite and severe discrepancy* Roberto Carlos odart randão** bstract This article reports the orthodontic treatment of a 14 years and 2 months
O C a s e R e p o r t Transverse malocclusion, posterior crossbite and severe discrepancy* Roberto Carlos odart randão** bstract This article reports the orthodontic treatment of a 14 years and 2 months
Treatment planning of nonskeletal problems. in preadolescent children
 In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
In the name of GOD Treatment planning of nonskeletal problems in preadolescent children Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 7 William R. Proffit,
Class II. Bilateral Cleft Lip and Palate. Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Cleft Lip and Palate.
 Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Bilateral Cleft Lip and Palate Clinician: Dr. Mike Mayhew, Boone, NC Patient: R.S. Class II Cleft Lip and Palate Pretreatment Diagnosis Class II dolichofacial female, age 22 years 11 months, presented
Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars*
 B B O C a s e R e p o r t Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars* Aldino Puppin Filho** Abstract This case report describes the orthodontic treatment
B B O C a s e R e p o r t Angle Class I malocclusion with bimaxillary dental protrusion and missing mandibular first molars* Aldino Puppin Filho** Abstract This case report describes the orthodontic treatment
TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION
 Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
Case Report NUJHS Vol. 5, No.2, June 2015, ISSN 2249-7110 TWO PHASE FOR A BETTER FACE!! TWIN BLOCK AND HEADGEAR FOLLOWED BY FIXED THERAPY FOR CLASS II CORRECTION 1 2 3 4 U S Krishna Nayak, Ashutosh Shetty,
ORTHOdontics SLIDING MECHANICS
 ORTHOdontics PGI/II SLIDING MECHANICS FOCUS ON TARGETED SPACE GAINING AND ITS APPLICATIONS, INCLUDING WITH RAPID PALATAL EXPANDIONS. ALSO INCLUDES RETENTION AND CLINICAL PEARLS FACULTY: Joseph Ghafari,
ORTHOdontics PGI/II SLIDING MECHANICS FOCUS ON TARGETED SPACE GAINING AND ITS APPLICATIONS, INCLUDING WITH RAPID PALATAL EXPANDIONS. ALSO INCLUDES RETENTION AND CLINICAL PEARLS FACULTY: Joseph Ghafari,
Simple Mechanics to Upright Horizontally Impacted Molars with Ramus Screws
 Case Report Simple Mechanics to Upright Horizontally Impacted Molars with Ramus Screws Dr Shih-Yung Lin, 1 Dr Chris Chang, 2 W. Eugene Roberts 3 1I BOI Diplomate, 2 Founder, Beethoven Orthodontic Center,
Case Report Simple Mechanics to Upright Horizontally Impacted Molars with Ramus Screws Dr Shih-Yung Lin, 1 Dr Chris Chang, 2 W. Eugene Roberts 3 1I BOI Diplomate, 2 Founder, Beethoven Orthodontic Center,
Sliding Mechanics with Microscrew Implant Anchorage
 Clinical Report Sliding Mechanics with Microscrew Implant Anchorage Hyo-Sang Park, DDS, MSD, PhD a ; Tae-Geon Kwon, DDS, MSD, PhD b Abstract: Three cases are illustrated. One was treated with maxillary
Clinical Report Sliding Mechanics with Microscrew Implant Anchorage Hyo-Sang Park, DDS, MSD, PhD a ; Tae-Geon Kwon, DDS, MSD, PhD b Abstract: Three cases are illustrated. One was treated with maxillary
Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient
 Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Case Report Maxillary Expansion and Protraction in Correction of Midface Retrusion in a Complete Unilateral Cleft Lip and Palate Patient Masayoshi Kawakami, DDS, PhD a ; Takakazu Yagi, DDS, PhD b ; Kenji
Dr Robert Drummond. BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015
, FDC(SA) Ortho. Canad Inn Polo Park Winnipeg 2015") Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
Dr Robert Drummond BChD, DipOdont Ortho, MChD(Ortho), FDC(SA) Ortho Canad Inn Polo Park Winnipeg 2015 Severely compromised FPM with poor prognosis Children often present with a developing dentition affected
An Effectiv Rapid Molar Derotation: Keles K
 An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
An Effectiv ective e and Precise Method forf Rapid Molar Derotation: Keles K TPA Ahmet Keles, DDS, DMSc 1 /Sedef Impar, DDS 2 Most of the time, Class II molar relationships occur due to the mesiopalatal
ISW for the treatment of adult anterior crossbite with severe crowding combined facial asymmetry case
 International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
International Research Journal of Medicine and Biomedical Sciences Vol.3 (2),pp. 15-29, November 2018 Available online at http://www.journalissues.org/irjmbs/ https://doi.org/10.15739/irjmbs.18.004 Copyright
Hypodontia is the developmental absence of at
 CASE REPORT Orthodontic treatment for a patient with hypodontia involving the maxillary lateral incisors Saud A. Al-Anezi Kuwait City, Kuwait Developmental absence of maxillary lateral incisors is not
CASE REPORT Orthodontic treatment for a patient with hypodontia involving the maxillary lateral incisors Saud A. Al-Anezi Kuwait City, Kuwait Developmental absence of maxillary lateral incisors is not
Different Non Surgical Treatment Modalities for Class III Malocclusion
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 9, Issue 6 (Sep.- Oct. 2013), PP 48-52 Different Non Surgical Treatment Modalities for Class III Malocclusion
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861. Volume 9, Issue 6 (Sep.- Oct. 2013), PP 48-52 Different Non Surgical Treatment Modalities for Class III Malocclusion
Non Extraction philosophy: Distalization using Jone s Jig appliance- a case report
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 36-41 Non Extraction philosophy: Distalization using Jone s Jig appliance-
6. Timing for orthodontic force
 6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
6. Timing for orthodontic force Orthodontic force is generally less than 300gm, so early mechanical stability is enough for immediate orthodontic force. There is no actually difference in success rate
The practice of orthodontics is faced with new
 CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
CLINICIAN S CORNER A new approach to correction of crowding William Randol Womack, DDS, a Jae H. Ahn, DDS, MSD, b Zahra Ammari, DDS, MDSc, c and Anamaría Castillo, DDS, MS c Phoenix, Ariz, and Santa Clara,
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile. Background:
 S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
S.H. Age: 15 Years 3 Months Diagnosis: Class I Nonextraction Severe crowding, very flat profile Background: This case was selected to illustrate the long-term impact of treatment planning on the face and
Treatment of Class II non-extraction using the Bioprogressive method
 DOI: 10.1051/odfen/2014013 J Dentofacial Anom Orthod 2014;17:407 Ó RODF / EDP Sciences Treatment of Class II non-extraction using the Bioprogressive method P. Guezenec CD SQODF, membre titulaire de la
DOI: 10.1051/odfen/2014013 J Dentofacial Anom Orthod 2014;17:407 Ó RODF / EDP Sciences Treatment of Class II non-extraction using the Bioprogressive method P. Guezenec CD SQODF, membre titulaire de la
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases
 Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
Forsus Class II Correctors as an Effective and Efficient Form of Anchorage in Extraction Cases by Lisa Alvetro, DDS, MSD After receiving her DDS summa cum laude from Ohio State University, Dr. Alvetro
3D Cortical Bone Anatomy of the Mandibular Buccal Shelf: a CBCT study to define sites for extra-alveolar bone screws to treat Class III malocclusion
 3D Cortical Bone Anatomy of the Mandibular Buccal Shelf: a CBCT study to define sites for extra-alveolar bone screws to treat Class III malocclusion Abstract Objective: Assess the feasibility of a proposed
3D Cortical Bone Anatomy of the Mandibular Buccal Shelf: a CBCT study to define sites for extra-alveolar bone screws to treat Class III malocclusion Abstract Objective: Assess the feasibility of a proposed
Checklist with summary points
 Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Checklist with summary points Question 1: Are your doctor Invisalign preferences on your home page up to date? Go to your doctor home page and open up your doctor preferences pages. Be sure to update item
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion.
 Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Tips from your peers to help you treat with confidence. Anterior Open Bite Correction with Invisalign Anterior Extrusion and Posterior Intrusion. Dr. Linda Crawford DDS, MS, P.C. Anterior Open Bite Correction
Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year Follow-Up
 Hindawi Case Reports in Dentistry Volume 2017, Article ID 4206435, 9 pages https://doi.org/10.1155/2017/4206435 Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year
Hindawi Case Reports in Dentistry Volume 2017, Article ID 4206435, 9 pages https://doi.org/10.1155/2017/4206435 Case Report Orthodontic Replacement of Lost Permanent Molar with Neighbor Molar: A Six-Year
Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports
 Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
Case Report Use of a Tip-Edge Stage-1 Wire to Enhance Vertical Control During Straight Wire Treatment: Two Case Reports Helen Taylor, BDS, MScD, DOrth, MOrth, FDSRCS(Eng) a Abstract: Vertical control is
Research & Reviews: Journal of Dental Sciences
 Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Research & Reviews: Journal of Dental Sciences Orthodontic Camouflage of Skeletal Class I, Class II and Class III Malocclusion in Borderline Cases Report of Three Cases Dr. Seema Kapil Lahoti 1 *, Dr.
Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique
 Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
Case Report Unilateral Horizontally Impacted Maxillary Canine and First Premolar Treated with a Double Archwire Technique Chien-Lun Peng a ; Yu-Yu Su b ; Sheng-Yang Lee c Abstract: A patient with a unilateral
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS
 EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS EUROPEAN SOCIETY OF LINGUAL ORTHODONTICS KANARELIS PANAGIOTIS (TAKIS) CASE NUMBER: 1 Year: 2012 WBLO 1 RÉSUMÉ OF CASE 1 CASE CATEGORY: ADULT MALOCCLUSION NAME:
Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report
 Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Case Report Ortho-surgical Management of Severe Vertical Dysplasia: A Case Report 1 Vinni Arora, 2 Rekha Sharma, 3 Sachin Parashar 1 Senior Resident, 2 Professor and Head of Department, 3 Former Resident
Effective and efficient orthodontic management of
 CASE REPORT Interdisciplinary approach for increasing the vertical dimension of occlusion in an adult patient with several missing teeth Flavio Uribe, a Nandakumar Janakiraman, b and Ravindra Nanda c Farmington,
CASE REPORT Interdisciplinary approach for increasing the vertical dimension of occlusion in an adult patient with several missing teeth Flavio Uribe, a Nandakumar Janakiraman, b and Ravindra Nanda c Farmington,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Smile attractiveness has been regarded as a standard
 CASE REPORT Nonsurgical correction of a Class III malocclusion in an adult by miniscrew-assisted mandibular dentition distalization Yan Jing, a Xianglong Han, b Yongwen Guo, a Jingyu Li, c and Ding Bai
CASE REPORT Nonsurgical correction of a Class III malocclusion in an adult by miniscrew-assisted mandibular dentition distalization Yan Jing, a Xianglong Han, b Yongwen Guo, a Jingyu Li, c and Ding Bai
Class II correction with Invisalign - Combo treatments. Carriere Distalizer.
 Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Tips from your peers to help you treat with confidence. Class II correction with Invisalign - Combo treatments. Carriere Distalizer. Dr. Clark D. Colville. Carriere Distalizer and Invisalign Combo. A distalization
Comprehensive Orthodontic Diagnosis Align upper and lower arches is not a treatment plan!
 Engineering Your Invisalign Treatment Plan To Conquer a Wide Variety of Cases Dr. Willy Dayan drwillydayan@gmail.com www.orthoclined.com Orthodontics is not just Straight Teeth Skeletal Foundation Posterior
Engineering Your Invisalign Treatment Plan To Conquer a Wide Variety of Cases Dr. Willy Dayan drwillydayan@gmail.com www.orthoclined.com Orthodontics is not just Straight Teeth Skeletal Foundation Posterior