A CLASSIFICATION SYSTEM FOR THE MANAGEMENT OF BIOMECHANICAL FACTORS IN DENTISTRY
|
|
|
- Carmella Clark
- 5 years ago
- Views:
Transcription
1 A CLASSIFICATION SYSTEM FOR THE MANAGEMENT OF BIOMECHANICAL FACTORS IN DENTISTRY I. INTRODUCTION Virtually all Masticatory System structural breakdowns are a result of either microbial or biomechanical factors. Microbial factors primarily affect the teeth and periodontium and cause caries and periodontal disease. Both of these disease processes are well documented, and much attention is given to their evaluation and treatment. In contrast, biomechanical factors affect not only the periodontium and teeth (or restorations and prostheses upon the teeth) but also the masticatory muscles and TM-Joints. Because biomechanical issues impact upon each component of the Masticatory System, they affect nearly every type of dental treatment. Despite this fact, biomechanical issues in dentistry do not seem to be as well documented or understood as those caused by microbial factors. This is of particular concern because of the possibility that this will lead to inappropriate or inadequate patient treatment. To contribute to a better understanding of biomechanical issues and their improved management, the Integrated Classification System (of Biomechanical Factors) has been developed. It does so by separating the entire spectrum of biomechanical issues into its fundamental components and then considers each in a way that guides both their evaluation and treatment. It is the purpose of this article to introduce the concept of the Integrated Classification System to all dentists, but especially those that are involved with the restorative and esthetic rehabilitation of teeth. II. RATIONALE A good classification system should be simple to understand, while providing insight to treatment selection. In addition, the more specific the classification system is, the more meaningful it is. The Integrated Classification System is intended to provide guidance to the evaluation, diagnosis, and treatment of biomechanical issues for dentists in a manner that fulfills these requirements. The following statements are the guiding principles of design of the Integrated Classification System: I. Biomechanical factors play a significant role in the predictable success of restorative and esthetic dental treatment, as well as the comfort and quality of life of our patients. II. Biomechanical factors are most effectively evaluated if separated into their three primary components: 1. TM-Joint Stability 2. Functional Occlusion 3. Parafunctional Activity III. Disorders resulting from biomechanical factors are most effectively treated if all three components are evaluated and treated, first individually in the order presented in statement II above, then in relation to each other component. The most important quality of the Integrated Classification System is that it requires consideration of all three biomechanical components during patient evaluation. Considering all components assures not only a comprehensive biomechanical assessment, but also a highly specific classification and diagnosis. A specific diagnosis makes possible the most appropriate and focused treatment. Although designed from a restorative dentist s perspective, because of its wide-ranging biomechanical considerations and applications, it is useful for 1
2 all dentists and dental specialists. It was inspired largely by Dr. Peter Dawson s Classification of Occlusion, which considers both Occlusal and TM-Joint factors, and also by Dr. John Kois s Classification of Occlusion, which considers both functional and parafunctional occlusal factors 1,2. III. DESCRIPTION The Integrated Classification System is divided into three parts. Each one classifies the status of a primary biomechanical component. Each component is classified in a way that is most meaningful for Restorative Dentists. Although not detailed in this article, it is important to understand that evaluative processes used to determine the classification of each component do exist and can be learned by any dentist choosing to do so. The following are descriptions of each component of The Integrated Classification System (see insert). TM-Joint Stability Classification The Integrated Classification System classifies TM-Joint Status based on the orthopedic stability of the joint(s), as it is this quality that best predicts the effect of the joint(s) on treatment provided by Restorative Dentists. Orthopedic stability of a joint considers not only anatomic alterations of structures within the joint, but also the structure, physiology, and pathology of all other components of the musculoskeletal system associated with that joint 3. These include supporting ligaments, muscles, and other joints. The Integrated Classification System considers all orthopedic factors because the status of joint anatomy alone is not always predictive of the joint s long-term stability or its effect on other Masticatory System structures. For example, a TM-Joint that is anatomically damaged with complete disc displacement without reduction (Piper Stage IV B) may be actively breaking down and placing the teeth and joint at considerable biomechanical risk. However, another damaged joint with a non-reducing completely displaced disc may be one that is well adapted and placing the teeth and joint at very little risk. Analysis of TM-Joint orthopedic stability should be based on the fact that it is a synovial joint of the human body. Therefore, it should be evaluated and managed similar to other synovial joints. A fundamental orthopedic characteristic of synovial joints is that their stability involves both structural and mechanical qualities 4. Structural stability is a pure joint anatomy or morphology consideration, referring to volumetric or dimensional stability of joint structures e.g. is the condyle breaking down or getting smaller with time. Breakdown of joint structures results in a positional shift of the entire mandible that directly affects maxillomandibular relationships 5. This most frequently results in a hyper-occlusion of the posterior teeth on the side of structural breakdown. Another effect of joint structure breakdown is on the mechanical stability of the joint. In contrast to structural stability, mechanical stability is a result of the anatomy and physiology of the joint and also the anatomy and physiology of structures associated with the joint. It considers the effectiveness of reciprocating joint surfaces, supporting capsule and ligaments, and muscles to allow smooth, yet controlled and limited joint movement 6,7. Structural breakdown of the condyle results in an incongruity of joint surfaces that contributes to a redistribution of stresses on the joint as well as altered mechanical stability 7,8. However, the resultant mechanical stability of a damaged TM-Joint is also affected by the status of supporting masticatory muscles, ligaments, the other TM-Joint, and the teeth. Reduced mechanical stability leads to added biomechanical demands on all Masticatory System structures. This bi-directional cause and effect relationship between structural and mechanical elements may lead to additional breakdown of the joints as well as added stresses on the masticatory muscles and teeth (or restorations and prostheses supported by the teeth). Each TM-Joint is classified as Stable, Manageably Adapted, Transitioning, or Unstable. Patients are classified and managed according to their more problematic joint. 2
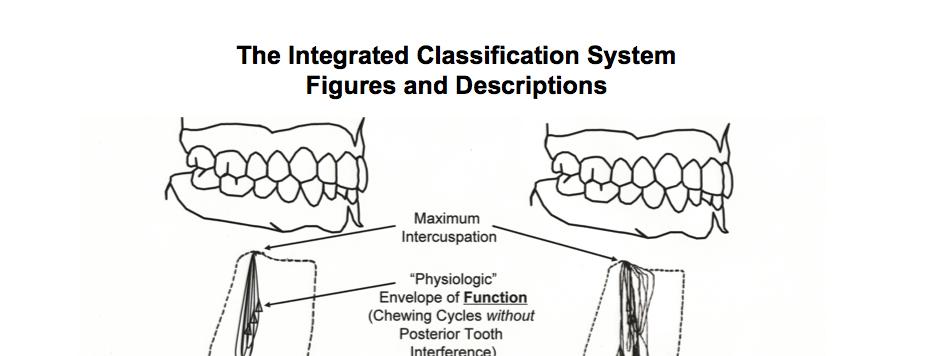
3 DESCRIPTION OF TM-JOINT STABILITY TYPES : STABLE - TM-Joint is healthy. It is structurally and mechanically stable. The condyle-disc assembly is intact and no degenerative processes have thus far affected the joint. Care should be taken to not create biomechanical stresses that might change this status. MANAGEABLY ADAPTED - TM-Joint is damaged and has undergone favorable adaptation. It has manageable levels of mechanical and structural stability. Future structural changes are anticipated, however at a rate and magnitude that will allow management of Functional Occlusion and Parafunctional Activity. Maintenance of an acceptable biomechanical stress level is dependant upon continuous monitoring and management of the Functional Occlusion and Parafunctional Activity. TRANSITIONING - TM-Joint is damaged and has not yet adapted. It is structurally unstable and experiencing a rate and/or magnitude of structural breakdown that makes management of the Functional Occlusion or Parafunctional Activity impossible. Management of patients with transitioning joints is directed toward stimulating a favorable adaptive response of the TM-Joints into a Manageably Adapted status. UNSTABLE - TM-Joint is damaged and has adapted poorly. It is mechanically unstable, and is not expected to become Manageably Adapted. Orthopedic rehabilitation may improve mechanical joint stability, however control of biomechanical issues is still unpredictable. While management of the Functional Occlusion and Parafunctional Activity may be helpful, definitive restorative or prosthetic treatment should only be done with great caution and with the patient s acceptance of risk. Functional Occlusion Classification The Functional Occlusion is the component of the Integrated Classification System that Restorative Dentists most directly (positively or negatively) impact. It considers the relationship of maxillary to mandibular teeth during all mandibular movements involved with mastication. These include straight closure as well as all lateral and protrusive functional movements. Collectively, these movements make up the Envelope of Function. In the Integrated Classification System, the Envelope of Function is defined as the three-dimensional space contained within the Envelope of Motion that defines mandibular movement during masticatory function 9. It is the world in which our mandible and teeth live in the normal chewing cycle. Functional Occlusion disorders occur when teeth interfere with this Envelope of Function. The Envelope of Function is best understood and managed if viewed as having two elements: 1) The Available Envelope of Function 2) The Required Envelope of Function The Available Envelope of Function represents the horizontal anterior-posterior spatial relationship that exists between lower central and lateral incisal edges and upper central and lateral lingual surfaces, with the teeth in maximum intercuspation. It is static and a purely structural component. The Required Envelope of Function represents the horizontal anterior-posterior dimension that is needed between these same tooth surfaces to allow a non-interfering, mechanically benign relationship between these surfaces in function. Unlike the purely structural and static nature of the Available Envelope of Function, the Required Envelope of Function is dynamic and is affected by a number of factors including Functional Occlusion relationships. It is described as physiologic if no posterior teeth interfere with closure of the mandible into maximum intercuspation while the condyles are in their Physiologically Seated Condylar Position (PSCP/CR). It is expanded if posterior teeth do interfere with physiologic closure, causing the mandible to deviate outside its physiologic path. (Figs. 1, 2, 3) (Author s note: The research of Lundeen and Gibbs was among the first to show 3
4 actual patient plots of the envelope of motion and envelope of function ( Chewing Plots ). Although portions of Figs. 1 and 2 are adapted from their work, they are not intended to show actual patient plots from their research. Rather, they are intended to illustrate the affect of posterior tooth interferences on physiologic closure of the mandible on a theoretical patient s envelope of function.) 10 Each patient is classified as having Benign Function, Posterior Dysfunction, or Anterior Dysfunction. DESCRIPTION OF FUNCTIONAL OCCLUSION TYPES: BENIGN FUNCTION No functionally induced occlusal disease is present. Structural damage, pain, and dysfunction resulting from Functional Occlusion relationships are either absent or present to a degree that currently are not, and whose implications will not adversely affect patient quality of life. POSTERIOR DYSFUNCTION Posterior tooth relationships are interfering with a physiologic Envelope of Function and are causing disease. Structural damage, pain, and/or dysfunction from posterior tooth relationships currently are, or their implications may adversely affect patient quality of life. Posterior Dysfunction is divided into two types: Type I (Simple) Posterior tooth interferences to the Envelope of Function are not damaging the teeth or are damaging only posterior teeth. Type II (Compound) Pseudo Anterior Dysfunction Posterior tooth interferences to the Envelope of Function are damaging posterior and anterior teeth. ANTERIOR DYSFUNCTION - Anterior tooth relationships are interfering with a physiologic Envelope of Function and are causing disease. Structural damage, pain, and/or dysfunction from anterior tooth relationships currently are, or their implications may adversely affect patient quality of life. Anterior Dysfunction is divided into two types: Type I (Primary) Anterior tooth relationships are interfering with straight closure of mandible with condyles in PSCP/CR and are also interfering with other movements of a physiologic Envelope of Function. Type II (Secondary) Anterior tooth relationships are not interfering straight closure of mandible with condyles in PSCP/CR, but are interfering with other movements of a physiologic Envelope of Function. Parafunctional Activity Classification The final component classifies patient Parafunctional Activity. In the Integrated Classification System, parafunctional activity is defined as all mandibular movements involved with non-physiologic movement the mandible. These include all movements except the normal chewing cycle, swallowing, breathing, or speech. Parafunctional Activity classification is based upon two clinical criteria. The first is whether or not the parafunctional activity is causing any damage, pain, or dysfunction to any part of the Masticatory System. The second is the etiology or etiologies of the parafunctional activity. Each patient is classified as having Benign Parafunctional Activity, Structural Parafunctional Activity, CNS Parafunctional Activity, or Secondary Parafunctional Activity. 4
5 DESCRIPTION OF PARAFUNCTIONAL ACTIVITY TYPES: BENIGN PARAFUNCTION No disease from parafunctional activity is present. Parafunctional activity is either absent, or structural damage, pain, and dysfunction from parafunctional activity are absent or present to a degree which currently is not, and whose implications will not adversely affect patient quality of life. STRUCTURAL PARAFUNCTION Parafunctional activity is causing disease in the form of structural damage, pain, or dysfunction and structural elements of the Masticatory System are the primary initiators. Functional Occlusion relationships quantitatively and/or qualitatively do affect Structural Parafunctional Activity. CNS PARAFUNCTION Parafunctional activity is causing disease in the form of structural damage, pain, or dysfunction and Brain Stem activity of the Central Nervous System is the primary initiator. Functional Occlusion relationships do not quantitatively or qualitatively affect CNS Parafunctional Activity. SECONDARY PARAFUNCTION - Parafunctional activity is causing disease in the form of structural damage, pain, or dysfunction and is initiated by extrinsic or intrinsic factors not included in Structural or CNS Parafunctional Activity. Functional Occlusion relationships do not quantitatively or qualitatively affect Structural Parafunctional Activity. Extrinsic initiators include Amphetamines, Extacy, and Selective Serotonin Reuptake Inhibitors (SSRI s). Intrinsic initiators include Basal Ganglion tumors. IV. DISCUSSION Collectively, the TM-Joint Stability, Functional Occlusion, and Parafunctional Activity component classifications make up the Integrated Classification System. Proper selection of biomechanical treatment is a two-step process that begins with classifying each of these three components. In the first step, after each component is classified, a Patient Type is assigned to the patient. Each combination of TM-Joint, Functional Occlusion, and Parafunctional Activity classifications defines a unique Patient Type. Each Patient Type has a unique set of treatment options and/or restrictions that may be appropriate for treating that patient s biomechanical issues. The Integrated Classification System includes Patient Types and guides treatment of patients with all four TM- Joint classes. However, because this article is primarily designed for dentists involved with restorative and esthetic treatment, only treatment details for Patient Types with Stable and Manageably Adapted joints have been included. Definitive treatment and management options considered in the Integrated Classification System for patients with these joint types include: 1. Additive Reshaping 2. Reductive Reshaping 3. Orthodontic/Orthognathic Tooth Movement 4. Night Guard Appliance Management For those dentists who choose to treat patients with Transitioning and Unstable joint classifications, treatment must begin with rehabilitation of the joints - the goal of which is to assist the joint(s) in becoming Manageably Adapted. It is not until the time that both joints become Manageably Adapted that definitive restorative or esthetic treatment should be performed. It should be noted that even though all dentists do not need to treat patients with Transitioning or Unstable TM- Joints, it is critical that they are able to identify them and make an appropriate referral. Fortunately, the vast 5
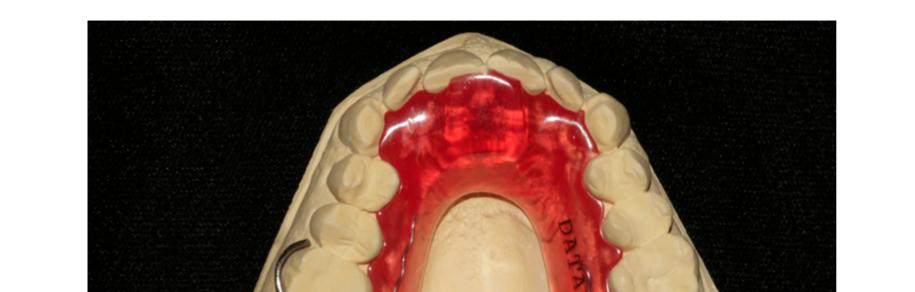
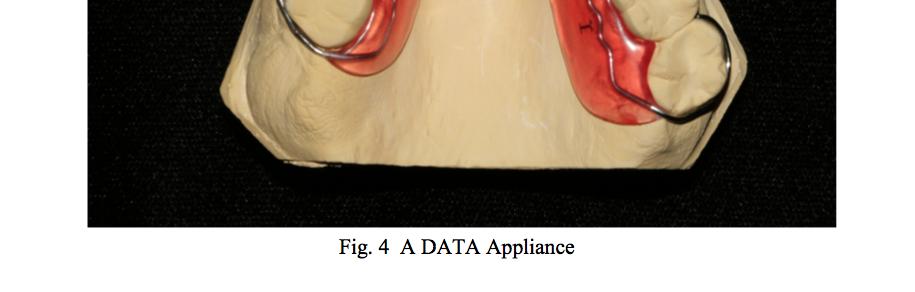
6 majority of patients seeking restorative or esthetic treatment have either Stable or Manageably Adapted joints. It is this large group of patients who can most benefit from correction of biomechanical problems with clinical skills that all dentists treating these patients should possess. The second step of proper biomechanical treatment selection involves identifying which one or combination of potentially acceptable options is most appropriate for a specific patient. This requires consideration of both biomechanical Patient Type and patient wants and needs independent of biomechanical issues. Patients wants and needs to consider include: 1. Improved Function 2. Improved Esthetics 3. Needed Restorations 4. Elimination of Pain 5. Maintainable Dental Health The option or combination of options that most conservatively achieves biomechanical harmony, and is also consistent with all other patient wants and needs should be utilized. With the proper selection and execution of the above listed options, there are virtually no patients with Stable or Manageably Adapted TM-Joints that cannot become biomechanically healthy. V. UTILIZATION Utilization of the Integrated Classification System is best understood when it is viewed as being part of another larger system. This larger system, hereafter referred to as the Physiologically Driven Treatment System (PDTS), consists of three parts: the Integrated Classification System (ICS), the DATA Appliance (Diagnosis And Treatment Assisting Appliance), and a Stable Biomechanical Platform. Details of this system were described in a previous three part series of article published in Spectrum Dialogue 12,12,13. The series of articles, entitled A Systematic Approach to Esthetic and Functional Treatment, described a clinical case in which both the functional and esthetic evaluation and treatment of a patient were guided by this system. The following is a brief review of a part of these articles that demonstrated utilization of the ICS and the PDTS. Demonstrating their utilization in a clinical case may be helpful for readers to better appreciate both their use and advantages. A critical part of the PDTS, the DATA Appliance is a removable appliance with an anterior stop that is used to assist in both evaluating and treating biomechanical force issues. It is used to provide patient information regarding each biomechanical element of the ICS 14,15 (Fig. 4). In the case described in the previous article, initial patient evaluation of biomechanical force issues revealed generalized moderate to severe excessive tooth wear, painful masticatory muscles, and damaged TMJ s. Both joints could accept firm loading with no sign of tension or tenderness, although clicking sounds that had been present for many years were noted in the left joint. Range of motion measurements were within normal limits. These findings were consistent with damaged, but well adapted (Manageably Adapted), TMJ s. To confirm this, a DATA Appliance was fabricated and seated. The DATA Appliance anterior stop was adjusted to allow contact of one lower incisor with closure, perpendicular to the arc of closure, allowing approximately 2mm interocclusal space between the most posterior teeth. The patient was initially re-evaluated after wearing the DATA Appliance twenty-four hours a day for ten days (except during eating and oral home care). Three significant responses were noted: 1) There was a near complete elimination of facial pain and joint sounds. 2) There was no evidence of parafunctional activity on the DATA Appliance acrylic anterior stop. 3) The patient reported that after seven days of wearing the DATA Appliance, tooth # s 15 and 18 were in contact if he closed with the appliance in place. 6
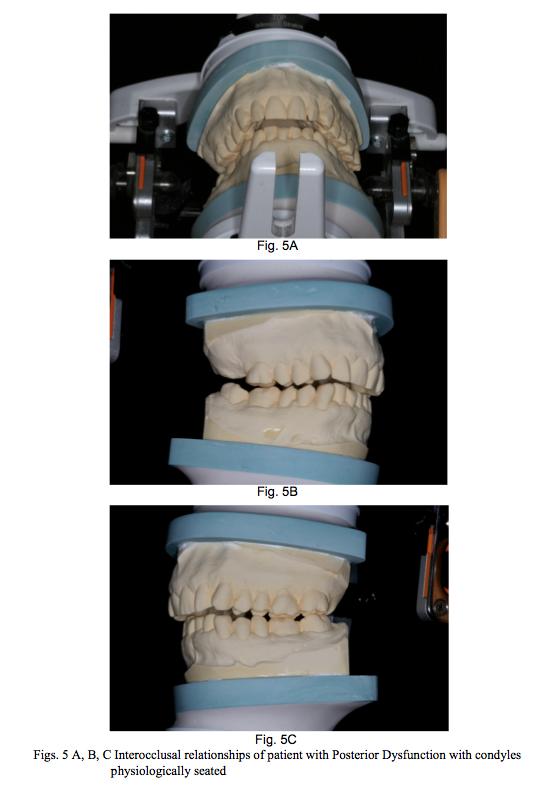
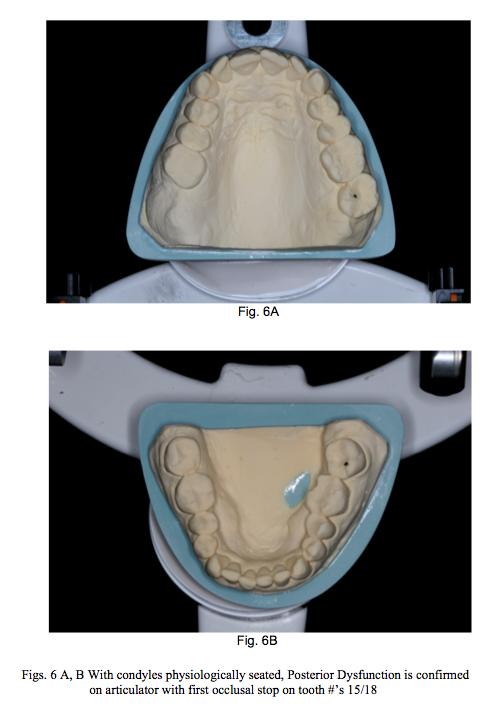
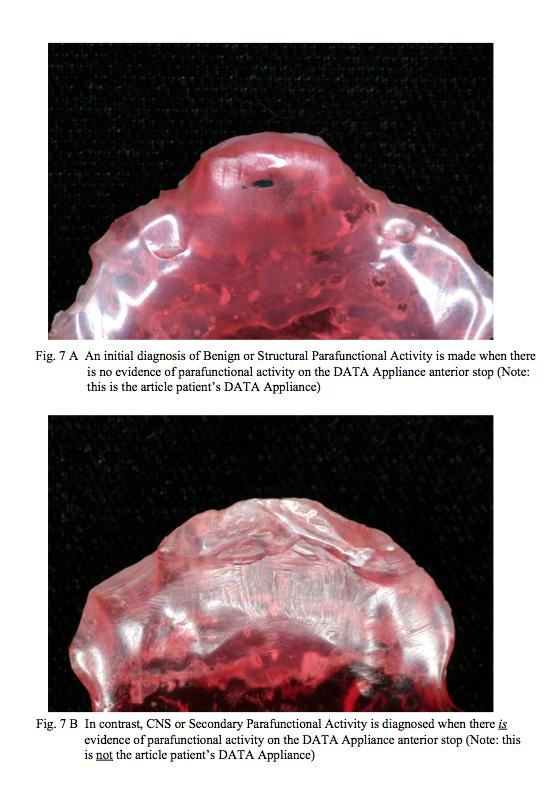
7 A bite registration using Futar D Occlusion bite registration material (Kettenbach GmbH & Co.; Eschenburg, Germany) with the DATA Appliance in place confirmed tooth # s 15 and 18 were in contact. At that time, additional acrylic was added to the anterior stop to once again allow approximately 2mm posterior tooth interocclusal space. The patient was next seen twenty-one days later. He reported a continued near complete absence of facial pain, with no joint sounds, and there was no evidence of parafunctional activity on the DATA Appliance anterior stop. Another bite registration was made and revealed tooth # s 15 and 18 nearly in contact again. Subsequent identical bite registrations were made over the next two weeks, and stabilization of maxillomandibular relationships was confirmed. A facebow registration to record the hinge axis was made and the maxillary cast mounted. The mandibular cast was then mounted using a Futar bite registration (Figs. 5 A, B, C). In this patient s case, information from DATA Appliance response, along with history and clinical examination findings, confirmed an ICS TM-Joint Stability diagnosis of Manageably Adapted. Significant history and examination findings included unchanging joint sounds, a normal ROM, and joints that could accept firm loading with no sign of tension or tenderness. These findings combined with a patient DATA Appliance response resulting in masticatory muscle pain elimination and stabilization of condylar position (as evidenced by precisely reproducible bite registrations) confirmed a Manageably Adapted TMJ status. DATA Appliance response also confirmed a Functional Occlusion diagnosis of Posterior Dysfunction and an initial Parafunctional Activity diagnosis of Benign or Structural Parafunctional Activity. A diagnosis of Posterior dysfunction was confirmed when posterior teeth (in this case, tooth # s 15 and 18) were found to interfere with closure of the mandible after the condyles were physiologically seated (Figs. 6 A, B). Because damage to the dentition involved both anterior and posterior teeth, a specific diagnosis of Posterior Dysfunction Type II was made. An initial diagnosis of either Structural or Benign Parafunctional Activity was made when no evidence of parafunctional activity was found on the DATA Appliance s anterior stop (Figs. 7 A, B). This combination of TM-Joint Stability, Functional Occlusion, and Parafunctional Activity diagnoses is common and one that can predictably benefit from occlusal correction. For this ICS classification (Patient Type 3M), occlusal correction may include additive reshaping, reductive reshaping, and/or orthodontic/orthognathic treatment (see insert Patient Type 3M). As stated in the previous section of this article, for any given patient, the proper choice of potential treatment modalities is dependent upon all their wants and needs including functional, esthetic, and restorative considerations. In this patient s case, occlusal correction was most appropriately accomplished with a combination of reductive and additive reshaping. As in most cases, not only did this patient benefit from occlusal correction, but the occlusal correction was a fundamental requirement for developing a Stable Biomechanical Platform. A Stable Biomechanical Platform is achieved when interocclusal relationships are in harmony with masticatory muscle function, together with healthy or well-adapted TMJ s, at the final treatment vertical dimension of occlusion. It requires that maximum intercuspation occurs with equal intensity contact of all teeth with both condyles physiologically seated. It also requires an anterior guidance that allows disclusion of the posterior teeth and one that is in harmony with the Envelope of Function. Creating this platform will not only assure patient comfort, but also serve as a foundation upon which ideal esthetic and functional design can be effectively developed and delivered. VI. CONCLUSION It is difficult to imagine a dentist who has not experienced the affects of failing to properly manage a patient s biomechanical issues - whether they are a cosmetic dentist, restorative dentist, prosthodontist, orthodontist, or any dentist wanting to help their patients achieve comfort and maintainable dental health. However, only after 7
8 the status of each biomechanical component of the Integrated Classification System is determined is it possible to predictably manage these issues. Failure to properly evaluate and address even one component may result in inappropriate or inadequate dental treatment. Inappropriate or inadequate treatment, in turn, often results in undesirable consequences for both the patient and dentist. Countless hours of time and dollars are wasted by dentists each year repairing or replacing restorations that have failed because of harmful biomechanical stresses. Many patients suffer daily with facial pain or tooth loss resulting from biomechanical disharmony within their Masticatory System. These common occurrences are most disturbing because in the majority of cases, they could have been avoided. A primary objective of the Integrated Classification System is to help prevent such problems. It does so most effectively by working in conjunction with the DATA Appliance and the concept of a Stable Biomechanical Platform. Combined, they are intended to help achieve biomechanical stability by providing guidance to appropriate evaluation and treatment. The Integrated Classification System is a tool for dentists to use to improve the quality of their dental treatment and the quality of life of their patients. This is only predictably accomplished with attention to both microbial and biomechanical issues. Regardless of their background or training, it is the goal of the Integrated Classification System to encourage and assist all dentists to improve their skills in recognizing and managing biomechanical problems. 8
9 9
10 10
11 11
12 12
13 13
14 Acknowledgments: I would like to acknowledge the following individuals for their contributions to the creation of the Integrated Classification System. First are Dr. Peter Dawson and Dr. John Kois for opening the minds of dentists around the world to the true nature of biomechanical factors in dentistry. Next are Dr. Mark Piper, Dr. John Droter, and Dr. Edward Zebovitz for their relentless pursuit of a better understanding of the Temporomandibular Joint. Finally are the late Drs. Harry Lundeen and Hudson (Hud) Heidorf for their unselfish encouragement and support of my efforts to help my profession and my patients. References: 1. Dawson PE. A Classification of Occlusion that Relates Maximal Intercuspation to the Position and Condition of the Temporomandibular Joints. J Prosthet Dent. 75: Kois J. Functional Occlusion: Science Driven Management. The Journal of Cosmetic Dentistry Fall; 23(3) p Salter RB, Textbook of Disorders and Injuries of the Musculoskeletal System, 3 rd Edition. Baltimore (Maryland): Lippincott, Williams and Wilkins; P 2,3. 4. Droter JR November. An Orthopedic Approach to the Diagnosis and Treatment of Disorders of the Temporomandibular Joint. Dentistry Today. < Clinical+Articles&type=Publishing&mod=Publications%3A%3AArticle&mid=8F3A F1 8BE895F87F791&tier=4&id=0394C8842E1744D681E036C599243D0C> Accessed 2009 May Dawson PE. Evaluation, Diagnosis, and Treatment of Occlusal Problems. St. Louis (Missouri): Mosby Elsevier; p Salter RB, Textbook of Disorders and Injuries of the Musculoskeletal System, 3 rd Edition. Baltimore (Maryland): Lippincott, Williams and Wilkins; P Salter RB, Textbook of Disorders and Injuries of the Musculoskeletal System, 3 rd Edition. Baltimore (Maryland): Lippincott, Williams and Wilkins; P Dawson PE. Functional Occlusion: From TMJ to Smile Design. St. Louis (Missouri): Mosby Elsevier; P The Glossary of Prosthodontic Terms. The Journal of Prosthetic Dentistry. Mosby Elsevier. 2005; 94.1: Lundeen HC, Gibbs CH. The Function of Teeth. Earleton, FL; L and G Publishers LLC; Hegyi KE, Csapo A. A Systematic Approach to Functional and Esthetic Treatment. Spectrum Dialogue Hegyi KE, Csapo A. Spectrum Dialogue. 13. Hegyi KE, Csapo A. Spectrum Dialogue 14. Hegyi KE. The DATA Appliance Part I: Appliance Seating Protocol, A printed version of this document is available via mail by contacting Karl E Hegyi DDS, Ridge Rd., North Royalton, OH 44133; or via phone at Hegyi KE. The DATA Appliance Part II: Appointment Management and Interpretation, A printed version of this document is available via mail by contacting Karl E Hegyi DDS, Ridge Rd., North Royalton, OH 44133; or via phone at Karl E Hegyi DDS Copyright
OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC
 Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Principle of Occlusion
 Principle of Occlusion Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Overview Principle of Occlusion Overview Principle of Occlusion Point centric Long centric Freedom
Principle of Occlusion Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Overview Principle of Occlusion Overview Principle of Occlusion Point centric Long centric Freedom
Restoring Severe Anterior Wear Cases; A Step by step Process
 0 Restoring Severe Anterior Wear Cases; Solving the Most Difficult Cases: A Step by Step Process" A Step by step Process Friday, February 6, 2015 Glenn E. DuPont, D.D.S. 1 The presence of worn dentition,
0 Restoring Severe Anterior Wear Cases; Solving the Most Difficult Cases: A Step by Step Process" A Step by step Process Friday, February 6, 2015 Glenn E. DuPont, D.D.S. 1 The presence of worn dentition,
Occlusion & Prosthodontics
 Occlusion & Prosthodontics Occlusion and Prosthodontic Treatments Babak Shokati DDS, MSc. MSc. Candidate (Prosthodontics) Occlusion: A Controversial Issue Occlusion related issues and contradictory debates:
Occlusion & Prosthodontics Occlusion and Prosthodontic Treatments Babak Shokati DDS, MSc. MSc. Candidate (Prosthodontics) Occlusion: A Controversial Issue Occlusion related issues and contradictory debates:
Occlusion in complete denture
 Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
INSIGHT & INNOVATION. Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been
 Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been employed in regard to treatment planning and correct restorative sequence. Assuming that the patient has healthy
Envelope of Parafunction: 7 Steps of Treatment Planning Many methods and theories have been employed in regard to treatment planning and correct restorative sequence. Assuming that the patient has healthy
Prosthetic Management of TMJ Disorders
 Prosthetic Management of TMJ Disorders Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Mohd@DrMohdAlfarsi.com @DrMohdAlfarsi DrMohdAlfarsi 056 224 2227 Overview Overview
Prosthetic Management of TMJ Disorders Mohammed Alfarsi BDS, MDSc(Pros), PhD www.drmohdalfarsi.com com.+*()ا&%$ر"!. www Mohd@DrMohdAlfarsi.com @DrMohdAlfarsi DrMohdAlfarsi 056 224 2227 Overview Overview
Full mouth occlusal rehabilitation; by Pankey Mann Schuyler philosophy
 Case Report DOI: 10.18231/2455-8486.2017.0006 Jinsa P. Devassy 1, Ankitha Sivadas 2, Shabas Muhammed 3 1 Consultant Prosthodontist, Ernakulam, Kerala, 2 Assistant Professor, 3 PG Student, Dept. of Prosthodontics,
Case Report DOI: 10.18231/2455-8486.2017.0006 Jinsa P. Devassy 1, Ankitha Sivadas 2, Shabas Muhammed 3 1 Consultant Prosthodontist, Ernakulam, Kerala, 2 Assistant Professor, 3 PG Student, Dept. of Prosthodontics,
Dr Mohammed Alfarsi Page 1 9 December Principles of Occlusion
 Dr Mohammed Alfarsi Page 1 9 December 2013 Principles of Occlusion Overview: The occlusion is a very large, yet easy to manage once properly understood, topic. Thus, no one handout is enough to fully understand
Dr Mohammed Alfarsi Page 1 9 December 2013 Principles of Occlusion Overview: The occlusion is a very large, yet easy to manage once properly understood, topic. Thus, no one handout is enough to fully understand
NORTH COAST 2017 INTERDISCIPLINARY OROFACIAL PAIN SYMPOSIUM OROFACIAL PAIN: A SYSTEMATIC METHOD OF
 NORTH COAST 2017 INTERDISCIPLINARY OROFACIAL PAIN SYMPOSIUM OROFACIAL PAIN: A SYSTEMATIC METHOD OF EVALUATION, DIAGNOSIS, AND TREATMENT... AS A PART OF COMPLETE DENTISTRY Karl E. Hegyi DDS FAGD North Royalton,
NORTH COAST 2017 INTERDISCIPLINARY OROFACIAL PAIN SYMPOSIUM OROFACIAL PAIN: A SYSTEMATIC METHOD OF EVALUATION, DIAGNOSIS, AND TREATMENT... AS A PART OF COMPLETE DENTISTRY Karl E. Hegyi DDS FAGD North Royalton,
Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure
 Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure Saurav Banerjee, Nabarun Chakraborty, Rajwinder Singh, Tapas Gupta Abstract Excessive occlusal wear can
Full-mouth rehabilitation of a patient with severe attrition using the Hobo twin-stage procedure Saurav Banerjee, Nabarun Chakraborty, Rajwinder Singh, Tapas Gupta Abstract Excessive occlusal wear can
Jaw relation registration in RPD
 Jaw relation registration in RPD Why to Record the Jaw Relations? To establish and maintain a harmonious relationship with all oral structures and to provide a masticatory apparatus that is efficient and
Jaw relation registration in RPD Why to Record the Jaw Relations? To establish and maintain a harmonious relationship with all oral structures and to provide a masticatory apparatus that is efficient and
Methods of determining vertical dimension of occlusion
 Methods of determining vertical dimension of occlusion 1) Pre-extraction records a) Willis gauge This device could used to measure V D O before teeth extraction and then recorded in the patient record.
Methods of determining vertical dimension of occlusion 1) Pre-extraction records a) Willis gauge This device could used to measure V D O before teeth extraction and then recorded in the patient record.
Maximizing Insurance Benefits
 Maximizing Insurance Benefits For Splint Patients This guide contains dental insurance information and dental codes to assist you in processing insurance claims for splint treatment. Reference: American
Maximizing Insurance Benefits For Splint Patients This guide contains dental insurance information and dental codes to assist you in processing insurance claims for splint treatment. Reference: American
Case Report Prosthodontic Rehabilitation of the Patient with Severely Worn Dentition: A Case Report
 Case Reports in Dentistry Volume 2012, Article ID 961826, 4 pages doi:10.1155/2012/961826 Case Report Prosthodontic Rehabilitation of the Patient with Severely Worn Dentition: A Case Report Mahnaz Hatami,
Case Reports in Dentistry Volume 2012, Article ID 961826, 4 pages doi:10.1155/2012/961826 Case Report Prosthodontic Rehabilitation of the Patient with Severely Worn Dentition: A Case Report Mahnaz Hatami,
Definition and History of Orthodontics
 In the name of GOD Definition and History of Orthodontics Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 1 William R. Proffit, Henry W. Fields, David M.Sarver.
In the name of GOD Definition and History of Orthodontics Presented by: Dr Somayeh Heidari Orthodontist Reference: Contemporary Orthodontics Chapter 1 William R. Proffit, Henry W. Fields, David M.Sarver.
Aesthetic and functional restoration of the severely worn dentition
 A SYSTEMATIC APPROACH TO FULL-MOUTH RECONSTRUCTION OF THE SEVERELY WORN DENTITION JAY LERNER Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge.
A SYSTEMATIC APPROACH TO FULL-MOUTH RECONSTRUCTION OF THE SEVERELY WORN DENTITION JAY LERNER Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge.
DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION
 DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION WHO IS PETER DAWSON? WHO IS PETER DAWSON? Peter Dawson is a dentist that specializes in the treatment of the exposed exterior surfaces of the teeth.
DR. PETER DAWSON S PHILOSOPHY OF FUNCTIONAL OCCLUSION WHO IS PETER DAWSON? WHO IS PETER DAWSON? Peter Dawson is a dentist that specializes in the treatment of the exposed exterior surfaces of the teeth.
Reestablishment of Occlusion with Prosthesis and Composite Resin Restorations
 Bull Tokyo Dent Coll (2009) 50(2): 91 96 91 Case Report Reestablishment of Occlusion with Prosthesis and Composite Resin Restorations Alício Rosalino Garcia, Renato Herman Sundfeld* and Rodrigo Sversut
Bull Tokyo Dent Coll (2009) 50(2): 91 96 91 Case Report Reestablishment of Occlusion with Prosthesis and Composite Resin Restorations Alício Rosalino Garcia, Renato Herman Sundfeld* and Rodrigo Sversut
Introduction to Occlusion and Mechanics of Mandibular Movement
 Introduction to Occlusion and Mechanics of Mandibular Movement Dr. Pauline Hayes Garrett Department of Endodontics, Prosthodontics, and Operative Dentistry University of Maryland, Baltimore Assigned reading
Introduction to Occlusion and Mechanics of Mandibular Movement Dr. Pauline Hayes Garrett Department of Endodontics, Prosthodontics, and Operative Dentistry University of Maryland, Baltimore Assigned reading
Shadeguides Finding the Centric Relation The Kois Deprogrammer
 Maciej Zarow Shadeguides Finding the Centric Relation The Kois Deprogrammer 21 Jun 2018 Finding the centric relation might sometimes seem hard, but with appropriate devices, such as the Kois Deprogrammer
Maciej Zarow Shadeguides Finding the Centric Relation The Kois Deprogrammer 21 Jun 2018 Finding the centric relation might sometimes seem hard, but with appropriate devices, such as the Kois Deprogrammer
CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration
 Reality or Resin; Free Hand Artistry with Anterior Bonding Dennis B. Hartlieb, DDS CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration Wish List: 1. Reversible (no prep/ minimal
Reality or Resin; Free Hand Artistry with Anterior Bonding Dennis B. Hartlieb, DDS CPR for Complex Dental Treatment; From Concept, to Prototype, to Restoration Wish List: 1. Reversible (no prep/ minimal
Articulators. 5- Wax up and refining the occlusion for dental restorations.
 Articulators It is a mechanical device represents the TMJ, maxillary and mandibular arches. It can be used to hold the upper and lower casts according to their relationships to facilitate the purposes
Articulators It is a mechanical device represents the TMJ, maxillary and mandibular arches. It can be used to hold the upper and lower casts according to their relationships to facilitate the purposes
Nine Steps To Occlusal Harmony
 Nine Steps To Occlusal Harmony Dr. Ali Tunkiwala has graduated from Nair Hospital Dental College in 1996 & completed his Masters Degree in Prosthetic Dentistry from Mumbai University (GDC, Mumbai) in 1998.
Nine Steps To Occlusal Harmony Dr. Ali Tunkiwala has graduated from Nair Hospital Dental College in 1996 & completed his Masters Degree in Prosthetic Dentistry from Mumbai University (GDC, Mumbai) in 1998.
AN EVALUATION OF MANDIBULAR BORDER MOVEMENTS THEIR CHARACTER AND SIGNIFICANCE
 AN EVALUATION OF MANDIBULAR BORDER MOVEMENTS THEIR CHARACTER AND SIGNIFICANCE HARRY C. LUNDEEN, D.D.S. EDWIN F. SHRYOCK, D.D.S.,M.S. and CHARLES H. GIBBS, PhD. The University of Florida, College of Dentistry,
AN EVALUATION OF MANDIBULAR BORDER MOVEMENTS THEIR CHARACTER AND SIGNIFICANCE HARRY C. LUNDEEN, D.D.S. EDWIN F. SHRYOCK, D.D.S.,M.S. and CHARLES H. GIBBS, PhD. The University of Florida, College of Dentistry,
JAMSS Speed-to-Treat Protocol For treatment of jaw joint and muscle sprain/strain injuries
 JAMSS Speed-to-Treat Protocol For treatment of jaw joint and muscle sprain/strain injuries INTRODUCTION What is Jaw Joint and Muscle Sprain/Strain (JAMSS)? Jaw Joint and Muscle Sprain/Strain (JAMSS) is
JAMSS Speed-to-Treat Protocol For treatment of jaw joint and muscle sprain/strain injuries INTRODUCTION What is Jaw Joint and Muscle Sprain/Strain (JAMSS)? Jaw Joint and Muscle Sprain/Strain (JAMSS) is
Deprogrammers made. Deprogrammers can be used for... How do deprogrammers work?
 Deprogrammers made asy Easy Deprogrammers made Deprogrammers can be used for... Headache sufferers Bruxers and/or clenchers Muscle relaxation Determining proper joint position Protection against wear Diagnosis
Deprogrammers made asy Easy Deprogrammers made Deprogrammers can be used for... Headache sufferers Bruxers and/or clenchers Muscle relaxation Determining proper joint position Protection against wear Diagnosis
Occlusal rehabilitation of posterior fixed prostheses: A clinical report
 J Korean Acad Prosthodont : Volume 39, Number 3, 2001 Occlusal rehabilitation of posterior fixed prostheses: A clinical report In-Sung Yeo, DDS a, and Jae-Ho Yang, DDS, MSD, PhD b College of Dentistry,
J Korean Acad Prosthodont : Volume 39, Number 3, 2001 Occlusal rehabilitation of posterior fixed prostheses: A clinical report In-Sung Yeo, DDS a, and Jae-Ho Yang, DDS, MSD, PhD b College of Dentistry,
See the end from the beginning
 Staub Cranial See the end from the beginning with Staub Cranial Recently a new technology was introduced to the United States that will revolutionize the way our industry restores teeth. The Staub Cranial
Staub Cranial See the end from the beginning with Staub Cranial Recently a new technology was introduced to the United States that will revolutionize the way our industry restores teeth. The Staub Cranial
Selection and arrangement of teeth in rpd
 Selection and arrangement of teeth in rpd upon completion of the articulator mounting and a thorough assessment of the occlusal requirements, the practitioner should be able to perform the proper arrangement
Selection and arrangement of teeth in rpd upon completion of the articulator mounting and a thorough assessment of the occlusal requirements, the practitioner should be able to perform the proper arrangement
Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique
 10.5005/JP-Journals-10012-1099 Koshika Tandon et al CASE REPORT Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique Koshika Tandon, Ajay Singh, Himanshu Gupta, Rajdeep
10.5005/JP-Journals-10012-1099 Koshika Tandon et al CASE REPORT Implant and Tooth Supported Full-Mouth Rehabilitation with Hobo Twin-Stage Technique Koshika Tandon, Ajay Singh, Himanshu Gupta, Rajdeep
Aesthetic and functional restoration of
 A systematic approach to full-mouth reconstruction of the severely worn dentition Jay Lerner demonstrates a procedure that allows the clinician to obtain the space required for the restoration of severely
A systematic approach to full-mouth reconstruction of the severely worn dentition Jay Lerner demonstrates a procedure that allows the clinician to obtain the space required for the restoration of severely
Horizontal jaw relations: The relationship of mandible to maxilla in a
 Horizontal relations Horizontal jaw relations: The relationship of mandible to maxilla in a horizontal plane (in anteroposterior and side to side direction). a- Protruded or forward relation. b-lateral
Horizontal relations Horizontal jaw relations: The relationship of mandible to maxilla in a horizontal plane (in anteroposterior and side to side direction). a- Protruded or forward relation. b-lateral
529-A Treatment and Management of the Edentulous Patient. Upon completion of this course the student should be able to:
 Course & Title: Session & Topic: 529-A Treatment and Management of the Edentulous Patient Jaw Relations General Goal: To understand the principles of orientational, horizontal and vertical jaw relations
Course & Title: Session & Topic: 529-A Treatment and Management of the Edentulous Patient Jaw Relations General Goal: To understand the principles of orientational, horizontal and vertical jaw relations
Case Report Use of Zirconia to Restore Severely Worn Dentition: A Case Report
 Volume 2012, Article ID 324597, 4 pages doi:10.1155/2012/324597 Case Report Use of Zirconia to Restore Severely Worn Dentition: A Case Report Manish Agrawal, 1 Banashree Sankeshwari, 1 and Channaveer V.
Volume 2012, Article ID 324597, 4 pages doi:10.1155/2012/324597 Case Report Use of Zirconia to Restore Severely Worn Dentition: A Case Report Manish Agrawal, 1 Banashree Sankeshwari, 1 and Channaveer V.
Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report
 J. Adv Oral Research Case Report All Rights Res Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report Hemal S. Agrawal
J. Adv Oral Research Case Report All Rights Res Full mouth rehabilitation of a patient with enamel hypoplasia using hobo s twin-tables technique for occlusal rehabilitation-a case Report Hemal S. Agrawal
SPLINT THERAPY: WHAT WORKS, WHAT DOESN T AND WHY?
 Clinical Research Foundation (A non-profit Foundation for Research and Charitable Endeavors) SPLINT THERAPY: WHAT WORKS, WHAT DOESN T AND WHY? Terry T. Tanaka, DDS Clinical Professor, Advanced Education
Clinical Research Foundation (A non-profit Foundation for Research and Charitable Endeavors) SPLINT THERAPY: WHAT WORKS, WHAT DOESN T AND WHY? Terry T. Tanaka, DDS Clinical Professor, Advanced Education
Dzakovich Conclusions
 Definitions Attrition Tooth wear resulting from contact between opposing teeth. Erosion A gradual tooth-surface loss process caused by an electrolytic or chemical mechanism without bacteria being involved.
Definitions Attrition Tooth wear resulting from contact between opposing teeth. Erosion A gradual tooth-surface loss process caused by an electrolytic or chemical mechanism without bacteria being involved.
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Ready to crown. McReynolds, David. Journal of the Irish Dental Association. Download date 12/10/ :52:38.
 Ready to crown Item Type Article Authors McReynolds, David Publisher Journal of the Irish Dental Association Journal Journal of the Irish Dental Association Download date 12/10/2018 03:52:38 Link to Item
Ready to crown Item Type Article Authors McReynolds, David Publisher Journal of the Irish Dental Association Journal Journal of the Irish Dental Association Download date 12/10/2018 03:52:38 Link to Item
Case report: Lingualized occlusion -A better way for enhancing function & esthetic
 Case report: Lingualized occlusion -A better way for enhancing function & esthetic 1Dr. Vishrut Shah, 2 Dr. Sunil Dhaded, 3 Dr. Chandrashekar Sajjan 1Post graduate student, Department of Prosthodontics,
Case report: Lingualized occlusion -A better way for enhancing function & esthetic 1Dr. Vishrut Shah, 2 Dr. Sunil Dhaded, 3 Dr. Chandrashekar Sajjan 1Post graduate student, Department of Prosthodontics,
How to Design an Ideal Maxillary Plane of Occlusion For Fixed or Removeable Prosthetics
 How to Design an Ideal Maxillary Plane of Occlusion For Fixed or Removeable Prosthetics By James R. Neuber RDT Full Mouth Rehabilitation Ceramist There are several techniques to establish a new plane of
How to Design an Ideal Maxillary Plane of Occlusion For Fixed or Removeable Prosthetics By James R. Neuber RDT Full Mouth Rehabilitation Ceramist There are several techniques to establish a new plane of
Samantha W. Chou, D.M.D N. Southport Ave. Chicago, Illinois Phone: Fax:
 Samantha W. Chou, D.M.D. 2325 N. Southport Ave. Chicago, Illinois 60614 Phone: 312-608-6881 Fax: 773-296-0601 Samanthawchou@gmail.com What is our role as the dentist? "We live in a culture in which people
Samantha W. Chou, D.M.D. 2325 N. Southport Ave. Chicago, Illinois 60614 Phone: 312-608-6881 Fax: 773-296-0601 Samanthawchou@gmail.com What is our role as the dentist? "We live in a culture in which people
Splint Appliance. Selection Guide. Great Lakes. See inside...
 Great Lakes Splint Appliance Selection Guide This guide includes helpful tips on how to choose the right splint for your patient and information on standard function and specifications for Great Lakes
Great Lakes Splint Appliance Selection Guide This guide includes helpful tips on how to choose the right splint for your patient and information on standard function and specifications for Great Lakes
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL
 MANUAL") AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
AD2 MEASURES CONDYLE DISPLACEMENT (MCD) MANUAL Dr. Jorge Ayala Puente, DDS* Dr. Gonzalo Gutiérrez Álvarez, DDS* Dr. José Miguel Obach M., DDS Translation: Dr. Barbara Fernández Lübbert, DDS Edited: Dr.
Active Clinical Treatment Case 48
 Active Clinical Treatment Case 48 Treating Clinicians: Drs. Jung Nam, Scott G. Cohen and Soojin Kim Initial smile Final smile Initial Presentation: January 2004 Age at Initial Presentation: 59 Active Treatment
Active Clinical Treatment Case 48 Treating Clinicians: Drs. Jung Nam, Scott G. Cohen and Soojin Kim Initial smile Final smile Initial Presentation: January 2004 Age at Initial Presentation: 59 Active Treatment
Parafunction poses a risk for any. Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion
 Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion BRIAN S. VENCE, DDS* ABSTRACT The goal of this clinical report is to describe and illustrate the principles for achieving
Predictable Esthetics through Functional Design: The Role of Harmonious Disclusion BRIAN S. VENCE, DDS* ABSTRACT The goal of this clinical report is to describe and illustrate the principles for achieving
Symposium on Occlusal Articulation. Mandibular Movement Recordings and Articulator Adjustments Simplified. Harry C. Lundeen, D.D.S.
 Symposium on Occlusal Articulation Mandibular Movement Recordings and Articulator Adjustments Simplified Harry C. Lundeen, D.D.S. Judging from the volume of writing that has appeared in the dental literature
Symposium on Occlusal Articulation Mandibular Movement Recordings and Articulator Adjustments Simplified Harry C. Lundeen, D.D.S. Judging from the volume of writing that has appeared in the dental literature
Application of ARCUS digma I, II systems for full mouth reconstruction: a case report
 https://doi.org/10.14368/jdras.2016.32.4.345 ISSN 2384-4353 eissn 2384-4272 Case Report Application of ARCUS digma I, II systems for full mouth reconstruction: a case report Chan Park* Department of Prosthodontics,
https://doi.org/10.14368/jdras.2016.32.4.345 ISSN 2384-4353 eissn 2384-4272 Case Report Application of ARCUS digma I, II systems for full mouth reconstruction: a case report Chan Park* Department of Prosthodontics,
Prosthodontics. Dental articulator. 1-Allow most of the prosthetic work to be done in the absence of the patient.
 Prosthodontics Dental articulator Definition: It is a mechanical instrument that represents the TMJ and jaw members to which the maxillary and mandibular casts are attached to simulate some or all mandibular
Prosthodontics Dental articulator Definition: It is a mechanical instrument that represents the TMJ and jaw members to which the maxillary and mandibular casts are attached to simulate some or all mandibular
Introduction to the Panadent System
 Prosthodontics has changed significantly over the years to the point where patient s acceptance or requests for complete removable dentures has been replaced with requests to save the natural dentition
Prosthodontics has changed significantly over the years to the point where patient s acceptance or requests for complete removable dentures has been replaced with requests to save the natural dentition
Avoiding Restorative Failure
 Avoiding Restorative Failure Lee Ann Brady, DMD Dr. Brady has no relevant financial relationships to disclose. Presentation partially sponsored by DMG and GC America Friday, June 15, 2018 1:30pm 4:30pm
Avoiding Restorative Failure Lee Ann Brady, DMD Dr. Brady has no relevant financial relationships to disclose. Presentation partially sponsored by DMG and GC America Friday, June 15, 2018 1:30pm 4:30pm
A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture
 Rita Zarina et al Mini Review 10.5005/jp-journals-10052-0097 A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture 1 Rita Zarina, 2 JL Jaini, 3 Rajan S Raj ABSTRACT Long-term success
Rita Zarina et al Mini Review 10.5005/jp-journals-10052-0097 A Systematic Approach for Rehabilitation of Occlusion in Fixed Partial Denture 1 Rita Zarina, 2 JL Jaini, 3 Rajan S Raj ABSTRACT Long-term success
Horizontal Jaw Relation
 Horizontal Jaw Relation Horizontal Jaw Relation It is the relationship of the mandible to the maxilla in a horizontal plane. It can also be described as the relationship of the mandible to the maxilla
Horizontal Jaw Relation Horizontal Jaw Relation It is the relationship of the mandible to the maxilla in a horizontal plane. It can also be described as the relationship of the mandible to the maxilla
Complex Occlusal Rehabilitation: A Case Report
 Complex Occlusal Rehabilitation: A Case Report DR. ALI TUNKIWALA INTRODUCTION The most difficult problems in clinical practice are those where there is interaction of various pathogenic factors with consequent
Complex Occlusal Rehabilitation: A Case Report DR. ALI TUNKIWALA INTRODUCTION The most difficult problems in clinical practice are those where there is interaction of various pathogenic factors with consequent
Interdisciplinary Treatment Planning in Transitioning Periodontally Hopeless Dentition
 Interdisciplinary Treatment Planning in Transitioning Periodontally Hopeless Dentition A clinical case review I NTRODUCTION Decreasing risk in an advanced periodontally diseased dentition presents a great
Interdisciplinary Treatment Planning in Transitioning Periodontally Hopeless Dentition A clinical case review I NTRODUCTION Decreasing risk in an advanced periodontally diseased dentition presents a great
Dentistry continues to evolve. Esthetic Templates for Complex Restorative Cases: Rationale and Management
 Esthetic Templates for Complex Restorative Cases: Rationale and Management DEAN E. KOIS, DMD* KYLE K. SCHMIDT, DDS* ARIEL J. RAIGRODSKI, DMD, MS ABSTRACT Complex restorative cases require difficult clinical
Esthetic Templates for Complex Restorative Cases: Rationale and Management DEAN E. KOIS, DMD* KYLE K. SCHMIDT, DDS* ARIEL J. RAIGRODSKI, DMD, MS ABSTRACT Complex restorative cases require difficult clinical
Jaw relations and jaw relation records
 Lecture 11 Prosthodontics Dr. Osama Jaw relations and jaw relation records Jaw relations can be classified into 3 categories 1-Orientation jaw relation 2-Vertical jaw relation 3-Horizontal jaw relation
Lecture 11 Prosthodontics Dr. Osama Jaw relations and jaw relation records Jaw relations can be classified into 3 categories 1-Orientation jaw relation 2-Vertical jaw relation 3-Horizontal jaw relation
Muscles of mastication [part 1]
![Muscles of mastication [part 1]](/thumbs/76/73586850.jpg "Muscles of mastication [part 1]") Muscles of mastication [part 1] In this lecture well have the muscles of mastication, neuromuscular function, and its relationship to the occlusion morphology. The fourth determinant of occlusion is the
Muscles of mastication [part 1] In this lecture well have the muscles of mastication, neuromuscular function, and its relationship to the occlusion morphology. The fourth determinant of occlusion is the
TMJ UNDERSTANDING SYNDROME SPECIAL REPORT By Paul R. White, D.D.S. Special Report: Understanding TMJ Syndrome
 SPECIAL REPORT Special Report: Understanding TMJ Syndrome UNDERSTANDING TMJ SYNDROME By Paul R. White, D.D.S. 804.715.1647 www.smilerichmond.com 804.715.1647 www.smilerichmond.com 1 UNDERSTANDING TMJ SYNDROME
SPECIAL REPORT Special Report: Understanding TMJ Syndrome UNDERSTANDING TMJ SYNDROME By Paul R. White, D.D.S. 804.715.1647 www.smilerichmond.com 804.715.1647 www.smilerichmond.com 1 UNDERSTANDING TMJ SYNDROME
Anatomy and physiology of Temporomandibular Joint
 Anatomy and physiology of Temporomandibular Joint Temporomandibular joint (TMJ): It is the articulation of the condyle of the mandible, and the inter-articular disc; with the mandibular fossa (glenoid
Anatomy and physiology of Temporomandibular Joint Temporomandibular joint (TMJ): It is the articulation of the condyle of the mandible, and the inter-articular disc; with the mandibular fossa (glenoid
Featured Patient Case #1: Complete Mouth Reconstruction with Hybrid Restorations
 Philip L. Fava II, DMD, MDSc Robert A. Levine, DDS, FCPP, FISPPS 9880 Bustleton Ave, Suite 211 Philadelphia, PA 19115 PADentalImplants.com 215-677-8686 Featured Patient Case #1: Complete Mouth Reconstruction
Philip L. Fava II, DMD, MDSc Robert A. Levine, DDS, FCPP, FISPPS 9880 Bustleton Ave, Suite 211 Philadelphia, PA 19115 PADentalImplants.com 215-677-8686 Featured Patient Case #1: Complete Mouth Reconstruction
TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE
 TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics( prosthodontics), Adelaide, FRACDS
TOOTH SELECTION & ARRANGEMENT IN REMOVABLRE PARTIAL DENTURE DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics( prosthodontics), Adelaide, FRACDS
STANDARDS & GUIDELINES
 STANDARDS & GUIDELINES 3.1.1. Complete Dentures 2 APPENDIX A FOR 3.1.1 Complete Dentures.. 3 Patient History and Treatment Plan Impressions Centric and Protrusive Denture Try In Insertion 3.1.2. Partial
STANDARDS & GUIDELINES 3.1.1. Complete Dentures 2 APPENDIX A FOR 3.1.1 Complete Dentures.. 3 Patient History and Treatment Plan Impressions Centric and Protrusive Denture Try In Insertion 3.1.2. Partial
OCCLUSION IN NEWLY FABRICATED BRIDGE*
 15 OCCLUSION IN NEWLY FABRICATED BRIDGE* (OKLUSI PADA GIGI TIRUAN JEMBATAN YANG BARU DIBUAT) Natasya Ahmad Tarib, Marlynda Ahmad Department of Prosthodontics, Faculty of Dentistry, University Kebangsaan
15 OCCLUSION IN NEWLY FABRICATED BRIDGE* (OKLUSI PADA GIGI TIRUAN JEMBATAN YANG BARU DIBUAT) Natasya Ahmad Tarib, Marlynda Ahmad Department of Prosthodontics, Faculty of Dentistry, University Kebangsaan
ESTHETIC AND FUNCTIONAL REHABILITATION OF THE PATIENT WITH SEVERELY WORN DENTITION USING TWIN STAGE PROCEDURE: A CASE REPORT
 ESTHETIC AND FUNCTIONAL REHABILITATION OF THE PATIENT WITH SEVERELY WORN DENTITION USING TWIN STAGE PROCEDURE: A CASE REPORT Naresh HG Shetty 1, Manoj Shetty 2, Krishna Prasad D. 3 ijcrr Vol 04 issue 03
ESTHETIC AND FUNCTIONAL REHABILITATION OF THE PATIENT WITH SEVERELY WORN DENTITION USING TWIN STAGE PROCEDURE: A CASE REPORT Naresh HG Shetty 1, Manoj Shetty 2, Krishna Prasad D. 3 ijcrr Vol 04 issue 03
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note
 Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Surveying. 3rd year / College of Dentistry/University of Baghdad ( ) Page 1
 Page 1") د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
2015 Member Speaker Forum. Chair: L. Scott Brooksby, DDS, BS. Friday, October 23, :30 AM 3:45 PM. Coral Ballroom. 3.
 2015 Member Speaker Forum Chair: L. Scott Brooksby, DDS, BS Friday, October 23, 2015 11:30 AM 3:45 PM Coral Ballroom 3.25 CE Credits 11:30 a.m. 3:45 p.m. Member Speaker Forum 11:30 11:40 a.m. Introduction
2015 Member Speaker Forum Chair: L. Scott Brooksby, DDS, BS Friday, October 23, 2015 11:30 AM 3:45 PM Coral Ballroom 3.25 CE Credits 11:30 a.m. 3:45 p.m. Member Speaker Forum 11:30 11:40 a.m. Introduction
Case Report Replacement of Missing Anterior Teeth in a Patient with Temporomandibular Disorder
 Case Reports in Dentistry, Article ID 393627, 4 pages http://dx.doi.org/10.1155/2014/393627 Case Report Replacement of Missing Anterior Teeth in a Patient with Temporomandibular Disorder Satheesh B. Haralur
Case Reports in Dentistry, Article ID 393627, 4 pages http://dx.doi.org/10.1155/2014/393627 Case Report Replacement of Missing Anterior Teeth in a Patient with Temporomandibular Disorder Satheesh B. Haralur
OCCLUSION. Principles & Treatment. José dos Santos, Jr, DDS, PhD. São Paulo, Brazil
 OCCLUSION Principles & Treatment José dos Santos, Jr, DDS, PhD São Paulo, Brazil Former Professor Division of Occlusion Department of Restorative Dentistry University of Texas Health Science Center at
OCCLUSION Principles & Treatment José dos Santos, Jr, DDS, PhD São Paulo, Brazil Former Professor Division of Occlusion Department of Restorative Dentistry University of Texas Health Science Center at
#45 Ortho-Tain, Inc PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT
 #45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
#45 Ortho-Tain, Inc. 1-800-541-6612 PREVENTIVE ERUPTION GUIDANCE -- PREVENTIVE OCCLUSAL DEVELOPMENT Analysis and Diagnosis of Occlusion: The ideal child of 5 y ears of age that probably has the best chance
UNLV School of Dental Medicine Advanced Education in Orthodontics and Dentofacial Orthopedics Course Descriptions, updated Dec.
 UNLV School of Dental Medicine Advanced Education in and Dentofacial Orthopedics Course Descriptions, updated Dec. 2012 Year 1 Summer Courses Intro to 8001 8011 8201 Cephlometrics Year 1 Fall Courses 1.
UNLV School of Dental Medicine Advanced Education in and Dentofacial Orthopedics Course Descriptions, updated Dec. 2012 Year 1 Summer Courses Intro to 8001 8011 8201 Cephlometrics Year 1 Fall Courses 1.
Interview with Vincent KOKICH
 DOI: 10.1051/odfen/2010302 J Dentofacial Anom Orthod 2010;13:218-222 Ó RODF / EDP Sciences Interview with Vincent KOKICH Conducted by and translated by Sophie ROZENCWEIG Dr. Kokich, it has always been
DOI: 10.1051/odfen/2010302 J Dentofacial Anom Orthod 2010;13:218-222 Ó RODF / EDP Sciences Interview with Vincent KOKICH Conducted by and translated by Sophie ROZENCWEIG Dr. Kokich, it has always been
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
AVADENT-WAGNER EZ GUIDE PROTOCOL
 APPOINTMENT A. Final Impressions 1 APPOINTMENT 2 APPOINTMENT 3 D. Seat Wagner EZ Guide Try-In B. Papillameter Measurement E. Refine Anterior Teeth C. Tooth Mould Selection F. Interocclusal Record G. Deliver
APPOINTMENT A. Final Impressions 1 APPOINTMENT 2 APPOINTMENT 3 D. Seat Wagner EZ Guide Try-In B. Papillameter Measurement E. Refine Anterior Teeth C. Tooth Mould Selection F. Interocclusal Record G. Deliver
Annals and Essences of Dentistry
 doi:10.5368/aedj.2013.5.4.3.1 DEVELOPMENT OF HARMONIOUS OCCLUSION FOR COMPLETE DENTURE PATIENT USING FUNCTIONALLY GENERATED PATH TECHNIQUE- A CASE REPORT 1 Ravi Rakesh Dev J 2 swetha Hima Bindu O 3 Aparna
doi:10.5368/aedj.2013.5.4.3.1 DEVELOPMENT OF HARMONIOUS OCCLUSION FOR COMPLETE DENTURE PATIENT USING FUNCTIONALLY GENERATED PATH TECHNIQUE- A CASE REPORT 1 Ravi Rakesh Dev J 2 swetha Hima Bindu O 3 Aparna
Occlusion and removable prosthodontics
 12 Occlusion and removable prosthodontics R. Jagger Synopsis Occlusal considerations for removable prostheses are essentially the same as for fixed restorations. The approach to establishing occlusion
12 Occlusion and removable prosthodontics R. Jagger Synopsis Occlusal considerations for removable prostheses are essentially the same as for fixed restorations. The approach to establishing occlusion
Significant improvement with limited orthodontics anterior crossbite in an adult patient
 VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
VARIA Significant improvement with limited orthodontics anterior crossbite in an adult patient Arzu Ari-Demirkaya Istanbul, Turkey Summary Objectives. Orthodontic treatment is known to last as long as
Removable Partial Dentures
 Removable Partial Dentures Replacement of missing teeth Fixed partial denture Removable partial denture Complete removable Transitional denture Partial removable Implant retained prosthodontics No prosthetic
Removable Partial Dentures Replacement of missing teeth Fixed partial denture Removable partial denture Complete removable Transitional denture Partial removable Implant retained prosthodontics No prosthetic
Mutilated Occlusion Fixed-Removable Approach- A Case Report
 Int. J. Life. Sci. Scienti. Res. eissn: 2455-1716 Case Report Mutilated Occlusion Fixed-Removable Approach- A Case Report 1* 2 3 Nami Sheth, Rubina Ali, Gaurang Mistry, Omkar Shetty 4 1 Post Graduate Student,
Int. J. Life. Sci. Scienti. Res. eissn: 2455-1716 Case Report Mutilated Occlusion Fixed-Removable Approach- A Case Report 1* 2 3 Nami Sheth, Rubina Ali, Gaurang Mistry, Omkar Shetty 4 1 Post Graduate Student,
Tooth preparation for posterior fi xed partial denture (FPD) Tooth preparation for anterior fi xed partial denture (FPD)
 Tooth preparation for anterior fi xed partial denture (FPD)") CHAPTER 17 Tooth preparation for posterior fi xed partial denture (FPD) 1 Defi nition and feature of FPD 2 Actual sequence of tooth preparation for posterior FPD Verify abutment teeth Occlusal guide groove
CHAPTER 17 Tooth preparation for posterior fi xed partial denture (FPD) 1 Defi nition and feature of FPD 2 Actual sequence of tooth preparation for posterior FPD Verify abutment teeth Occlusal guide groove
The Goal: Esthetics & Function. Occlusion In Dentistry. The Engineering= Occlusion
 Occlusion In Dentistry The Goal: Esthetics & Function Presented by: Dr. George Arvanitis DDS, DABOI, FAAID, etc.. Director of the Ti-Max Institute for Continuing Dental Education and the Ti-Max AAID Implant
Occlusion In Dentistry The Goal: Esthetics & Function Presented by: Dr. George Arvanitis DDS, DABOI, FAAID, etc.. Director of the Ti-Max Institute for Continuing Dental Education and the Ti-Max AAID Implant
COURSE CURRICULUM FOR AESTHETIC DENTISTRY
 COURSE CURRICULUM FOR AESTHETIC DENTISTRY Esthetic Dentistry is actually the fourth dimension in clinical dentistry. In addition to biologic, Physiologic, and mechanical factors, all of which must be understood
COURSE CURRICULUM FOR AESTHETIC DENTISTRY Esthetic Dentistry is actually the fourth dimension in clinical dentistry. In addition to biologic, Physiologic, and mechanical factors, all of which must be understood
Immediate Complete Denture: A Case Report
 Human Journals Case Report July 2018 Vol.:10, Issue:1 All rights are reserved by Ruby et al. Immediate Complete Denture: A Case Report Keywords: immediate denture, dental prosthesis ABSTRACT Ruby*, Manish
Human Journals Case Report July 2018 Vol.:10, Issue:1 All rights are reserved by Ruby et al. Immediate Complete Denture: A Case Report Keywords: immediate denture, dental prosthesis ABSTRACT Ruby*, Manish
ORTHODONTIC INITIAL ASSESSMENT FORM (OIAF) w/ INSTRUCTIONS
 w/ INSTRUCTIONS") Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
PATIENT INSTRUCTIONS FOR BRACE REMOVAL
 McNamara Orthodontics Specialists in Orthodontics and Dentofacial Orthopedics 321 N. Ingalls Street, Ann Arbor, MI 48104 (734) 668-8288 www.mcnamaraortho.com PATIENT INSTRUCTIONS FOR BRACE REMOVAL As the
McNamara Orthodontics Specialists in Orthodontics and Dentofacial Orthopedics 321 N. Ingalls Street, Ann Arbor, MI 48104 (734) 668-8288 www.mcnamaraortho.com PATIENT INSTRUCTIONS FOR BRACE REMOVAL As the
ALTERNATE OCCLUSAL SCHEMES
 ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
ALTERNATE OCCLUSAL SCHEMES The same basic concepts need to be applied to all occlusal schemes. Some challenges include missing teeth, transposed teeth, crossbites, and anterior open bites. POSTERIOR CROSSBITES
The De Vreugd Occlusal Compass
 The De Vreugd Occlusal Compass A Guide to Creating Functional Morphology in Wax Each color on the DeVreugd Occlusal Compass represents directions in which the mandibular buccal cusps travel during chewing
The De Vreugd Occlusal Compass A Guide to Creating Functional Morphology in Wax Each color on the DeVreugd Occlusal Compass represents directions in which the mandibular buccal cusps travel during chewing
Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants. by Timothy F. Kosinski, DDS, MAGD
 Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants by Timothy F. Kosinski, DDS, MAGD Implant dentistry is undergoing some amazing transformations. With the
Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants by Timothy F. Kosinski, DDS, MAGD Implant dentistry is undergoing some amazing transformations. With the
Special Report. Top Ten Things You should consider Before Choosing Your Orthodontist
 Special Report Top Ten Things You should consider Before Choosing Your Orthodontist Welcome note from Dr. Richard M. Hesby Dear Friend, If you are researching orthodontists or investigating the various
Special Report Top Ten Things You should consider Before Choosing Your Orthodontist Welcome note from Dr. Richard M. Hesby Dear Friend, If you are researching orthodontists or investigating the various
Jaw relation (Maxillomandibular relationship): any one of the infinite
: any one of the infinite") Maxillo-mandibular Relationship Jaw relation (Maxillomandibular relationship): any one of the infinite spatial relationships of the mandible to the maxilla. Jaw relation record: It is a registration of
Maxillo-mandibular Relationship Jaw relation (Maxillomandibular relationship): any one of the infinite spatial relationships of the mandible to the maxilla. Jaw relation record: It is a registration of
Treatment Agreement for Oral Appliance Therapy: Temporomandibular Disorder (TMD)
") Treatment Agreement for Oral Appliance Therapy: Temporomandibular Disorder (TMD) What is TMD? Temporomandibular Disorders (TMD) are a group of conditions that cause pain and dysfunction in the jaw joint
Treatment Agreement for Oral Appliance Therapy: Temporomandibular Disorder (TMD) What is TMD? Temporomandibular Disorders (TMD) are a group of conditions that cause pain and dysfunction in the jaw joint
AAO Meeting Mutilated Dentition in Aging Population
 AAO Meeting 2018 Mutilated Dentition in Aging Population 1. Introduction & Presentation 2. Anterior Missing Teeth 3. Posterior Missing Teeth 4. Analyze, Visualize and Optimize 5. Case Presentation 6. Challenge
AAO Meeting 2018 Mutilated Dentition in Aging Population 1. Introduction & Presentation 2. Anterior Missing Teeth 3. Posterior Missing Teeth 4. Analyze, Visualize and Optimize 5. Case Presentation 6. Challenge
Occlusion and Attachments
 THE VOICE OF TECHNO-CLINICAL DENTISTRY Occlusion and Attachments The Underlying Scheme for Successful Overdentures Dennis Urban, CDT Vol. 9 No. 4 - April 2010 - Reprint 2 Spectrum dialogue Vol. 9 No. 4
THE VOICE OF TECHNO-CLINICAL DENTISTRY Occlusion and Attachments The Underlying Scheme for Successful Overdentures Dennis Urban, CDT Vol. 9 No. 4 - April 2010 - Reprint 2 Spectrum dialogue Vol. 9 No. 4
TEMPORO-MANDIBULAR JOINT DISORDERS
 Disclaimer This movie is an educational resource only and should not be used to manage your dental health. All decisions about the management of TMJ Disorders must be made in conjunction with your Dental
Disclaimer This movie is an educational resource only and should not be used to manage your dental health. All decisions about the management of TMJ Disorders must be made in conjunction with your Dental
Complex esthetic and functional rehabilitation using glass-ceramic materials - long-term documentation of a restoration
 C L I N I C A L Complex esthetic and functional rehabilitation using glass-ceramic materials - long-term documentation of a restoration Daniel Edelhoff 1 and Oliver Brix 2 1 Prof. Dr Daniel Edelhoff, Munich
C L I N I C A L Complex esthetic and functional rehabilitation using glass-ceramic materials - long-term documentation of a restoration Daniel Edelhoff 1 and Oliver Brix 2 1 Prof. Dr Daniel Edelhoff, Munich
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults
 Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Safety and esthetics with
 Safety and esthetics with dental implants A guide for patients Dear reader, Implant restorations follow nature's example. You can have the functions of natural teeth completely restored and thus maintain
Safety and esthetics with dental implants A guide for patients Dear reader, Implant restorations follow nature's example. You can have the functions of natural teeth completely restored and thus maintain