CLASSIFICATIONS. Established in 1994 as a subcommittee of the. Prosthodontic Care Committee
|
|
|
- Philippa Reynolds
- 5 years ago
- Views:
Transcription
1 CLASSIFICATIONS Established in 1994 as a subcommittee of the Prosthodontic Care Committee
2 Committee Members Thomas J. McGarry, DDS, Chair Arthur Nimmo, DDS James F. Skiba, DDS Christopher R. Smith, DDS Robert H. Ahlstrom, DDS, MS Jack H. Koumjian, DDS, MSD Ronald P. Desjardins, DMD, MSD
3 The value of information and the cost of uncertainty: Who pays the bill? Lysle E. Johnston, Jr. DDS, Ph.D. The Angle Orthodontist Vol. 68 No In the long run, a willingness to treat without reference to evidence has a price that can be measured. Stated simply, it is the difference between what the patient actually gets and what he or she could have gotten from the best available treatment. The cost of this difference (the regret ) always comes due and is borne in full by the patient.
4 Perhaps because there is no obvious penalty for being wrong (or for not being as right as one might like), decision-making in the face of uncertainty (i.e., in the absence of data) is a time-honored prosthodontic tradition.
5 Diagnostic Classification of Complete Edentulism
6 Do different physical variations require a change in treatment procedures? Do different treatment procedures require additional education and training? Do patient mediated variables require a change in treatment procedure?
7 Evidence based treatment procedures require: Accurate diagnosis Differentiation of treatment procedures to a specific diagnosis Outcome assessment criteria
8 EDENTULOUS EDENTULISM
9 PHYSIOLOGY OR ABUSE? Resorption Increased osteoclastic activity, as in hyperparathyroidism and pressure mediated resorption
10 Establish the continual resorption/atrophy for the majority of edentulous patients Increasing dysfunction Residual Ridge Reduction Maxilla 0.1mm Mandible 0.4mm

11 Chronic progressive, irreversible and disabling disease process probably of multifactoral origin. At the present time, the relative importance of various cofactors is not known.
12 TREATMENT PROCEDURES PARAMETERS OF CARE SPECIALTY PROCEDURES CODING GENERAL CODING OUTCOME DATA CRITERIA PARAMETERS OF CARE SUCCESS COMPLICATIONS & KNOWN RISKS PARAMETERS OF CARE REVISION
13 DEFINITION OF SPECIALTY Diagnostic Coding Committee Computerized Patient Record Parameters of Care Outcome Data Assessment Quality Assurance Third Party Coverage Peer Review
14 American College of Pathologists SNOMED
15 Dental Diseases SNODENT
16 Diagnostic Code +Treatment Code Outcome Data
17 Complete Edentulism
18 Class I Ideal or minimally compromised Classification System for the Completely Edentulous Patient Class II Class III Moderately compromised Substantially compromised Diagnostic Criteria 1. Bone height--mandibular 2. Maxillomandibular relationship 3. Residual ridge morphologymaxilla 4. Muscle attachments Class IV Severely compromised
19 Diagnostic Criteria Addendum The diagnostic criteria are ordered by their objective nature and not in their rank of significance. Objective criteria will allow for the most accurate application of the classification system and measurement of its efficacy. Objectivity will also provide reliable outcome data and mechanisms for review by administrative panels.
20 Bone Height Mandibular
21 Quantity of the Underlying Bony Foundation Denture foundation area Tissues remaining for reconstruction Loss of facial muscle support/attachment Decrease in total facial height Residual ridge morphology

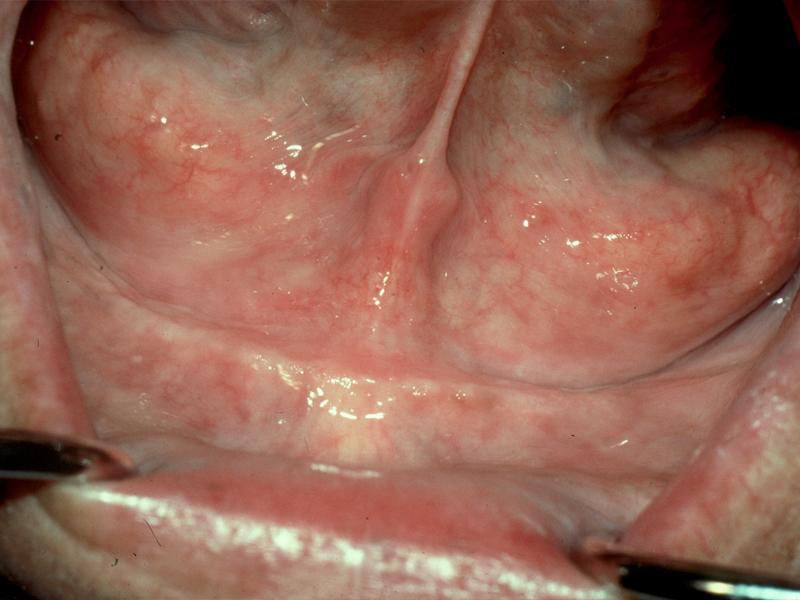
22 Classification of Alveolar Atrophy John H. Kent, D.D.S. LSU Medical Center, New Orleans Alveolar measurements Incisal edge to vestibule 19mm Alveolar crest to vestibule 10mm

23 Alveolar Measurements Occlusal plane to inferior border Mental nerve to inferior border Alveolar crest to inferior border 40mm 15mm 32mm

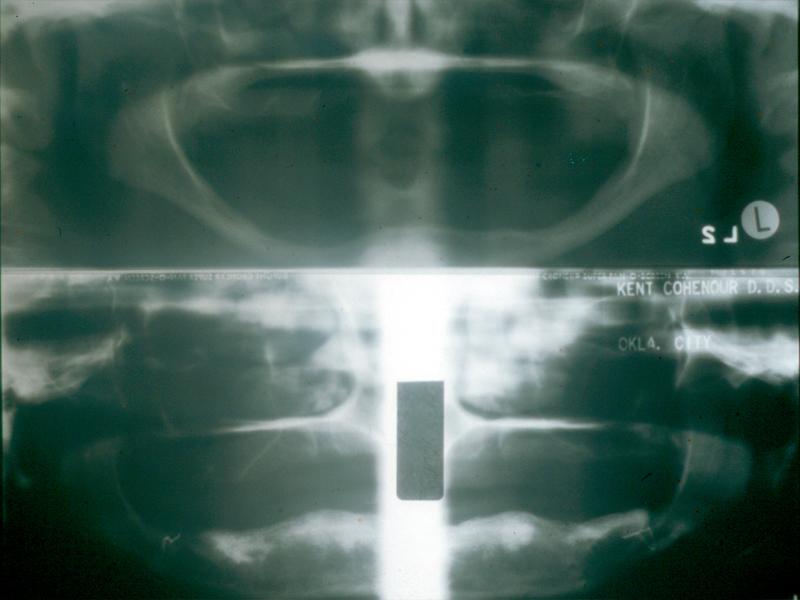
24 The objectivity of residual bone height measurement is affected by the magnification and variance of radiographic procedures and equipment of different manufacturers.

25 However, this diagnostic measurement reveals the most information of all the criteria. In order to minimize variance in techniques, the measurement should be made at that portion of the mandible of the least vertical height.

26 Type I Residual bone height of 21mm or greater measured at the least vertical height of the mandible.

27 Type II Residual bone height of mm measured at the least vertical height of the mandible.

28 Type III Residual alveolar bone height of mm measured at the least vertical height of the mandible

29 Type IV Residual vertical bone height of 10 mm or less measured at the least vertical height of the mandible

30
31 Functional Positioning of the Artificial Teeth Maxillomandibular relationship classification relates to the position of the artificial teeth to the residual ridge and to the opposing dentition.
32
33 Maxillomandibular Relationship

34 Class I Maxillomandibular relationship allows tooth position that has normal articulation with the teeth supported by the residual ridge.

35 Class II Maxillomandibular relationship requires tooth position outside the normal ridge relation in order to attain phonetics and articulation; i.e., anterior or posterior tooth position not supported by the residual ridge/anterior vertical overlap that exceeds the principles of articulation.

36 Class III Maxillomandibular relationship requires tooth position outside the normal ridge relation in order to attain phonetics and articulation; i.e., crossbite anterior or posterior, tooth position not supported by the residual ridge.
37 Complete Edentulism

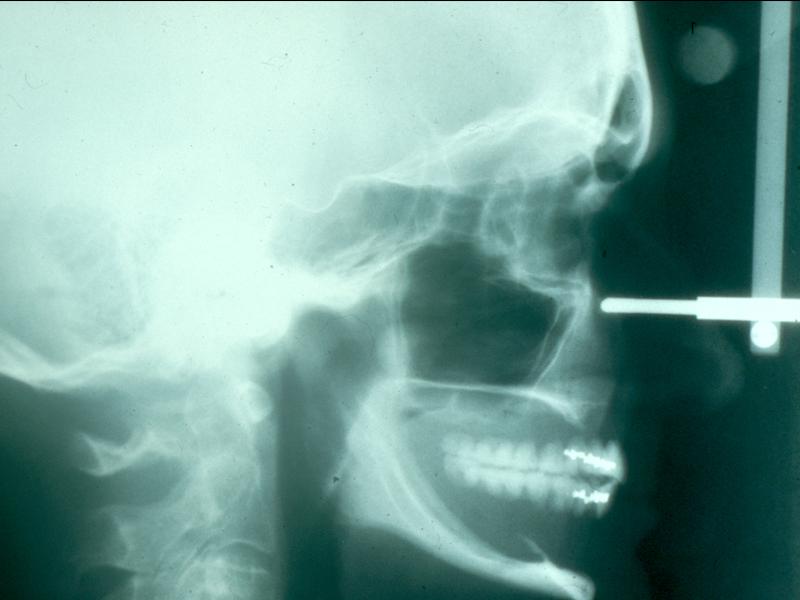
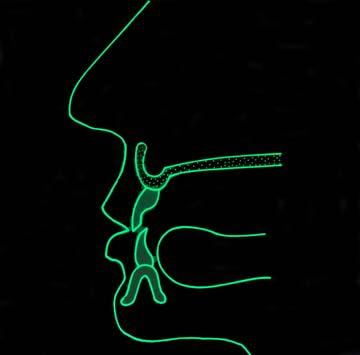
38 Position and Angulation of the Occlusal Plane
39 Residual Ridge Morphology: Maxilla Residual ridge morphology is the most objective criteria for the maxilla since measurement of the residual bone height by radiography is not reliable. The following descriptive scenario follows a logical progression to describe the effects of residual ridge morphology and muscular influence on the maxillary denture.
40 Type A Maxilla Hard Palate form Anterior Maxilla Maxillary Tuberosities

41 Anterior labial and posterior buccal vestibular depth that resists vertical and horizontal movement of the denture base Palatal morphology that resists vertical and horizontal movement of the denture base Sufficient tuberosity definition that resists vertical and horizontal movement of the denture base Hamular notch is well defined to establish the posterior extension of the denture base Absence of tori or exostoses
42 Type B Maxilla Hard Palate form Residual Alveolar Ridge Anterior Posterior Maxillary Tuberosities

43 Loss of posterior buccal vestibule Tuberosity and hamular notch are poorly defined compromising delineation of the posterior extension of the denture base Maxillary palatal and/or lateral tori are rounded and do not affect the posterior extension of the denture base Palatal vault morphology that resists vertical and horizontal movement of the denture base
44 Type C Maxilla Hard Palate form Anterior Maxilla Maxillary Tuberosities

45 Loss of anterior labial vestibule Prominent midline suture Maxillary palatal and/or lateral tori with bony undercuts that do not affect the posterior extension of the denture base Hyperplastic, mobile anterior ridge that offers minimum support and stability of the denture base Palatal vault morphology that offers minimal resistance to vertical and horizontal movement of the denture base Reduction of the post malar space by the coronoid process during mandibular opening and/or excursive movements
46 Type D Maxilla Hard Palate form Residual alveolar ridge Anterior Posterior Maxillary Tuberosities

47 Loss of anterior labial and posterior buccal vestibules Maxillary palatal and/or lateral tori-rounded or undercut- that interferes with the posterior border of the denture Hyperplastic, redundant anterior ridge Palatal vault morphology that does not resist vertical or horizontal movement of the denture base Prominent anterior nasal spine
48 The location and influence of the muscle attachments affecting a complete denture are most commonly associated with the mandibular denture. Although, arguably the most significant measurement, it is also the most difficult to quantify.
49 The following descriptive scenario follows a logical progression to describe the effects of muscular influence on the mandibular denture.
50 Anatomy that resists anterior (forward) movement of the denture base
51 Muscle Attachments

52 Type A Adequate attached mucosal base without undue muscular impingement during normal function in all regions.

53 Type B Adequate attached mucosal base in all regions except anterior buccal vestibule cuspid to cuspid High mentalis muscle attachment

54 Type C Adequate attached mucosal base in all regions except anterior buccal and lingual vestibules cuspid to cuspid High genioglossus and mentalis muscle attachments

55 Type D Adequate attached mucosal base only in the posterior lingual region All other regions are detached

56 Type E No attached mucosa in any region Cheek and lip movement = tongue movement
57 Diagnostic Classification of Complete Edentulism
58 Class I This classification level describes the stage of edentulism that is most apt to be successfully treated by conventional prosthodontic techniques with complete denture prosthesis. All four of the diagnostic criteria are favorable.

59 Class I Residual bone height of 21 mm or greater measured at the least vertical height of the mandible Class I maxillomandibular relationship

60 Class I Residual bone height of 21 mm or greater measured at the least vertical height of the mandible Class I maxillomandibular relationship

61 Residual ridge morphology that resists horizontal and vertical movement of the denture base Type A Maxilla Location of muscle attachments that are conducive to denture base stability and retention Type A, B--Mandible Class I

62 Residual ridge morphology that resists horizontal and vertical movement of the denture base Type A Maxilla Location of muscle attachments that are conducive to denture base stability and retention Type A, B--Mandible Class I
63 Class II This classification level distinguishes itself with the noted continuation of the physical degradation of the denture supporting structures and in addition is characterized with the early onset of systemic disease interactions, localized soft tissue factors and patient management/lifestyle considerations.

64 Residual bone height of mm measured at the least vertical height of the mandible Class II Class I maxillomandibular relationship Residual ridge morphology that resists horizontal and vertical movement of the denture base Type A, B--Maxilla

65 Residual bone height of mm measured at the least vertical height of the mandible Class II Class I maxillomandibular relationship Residual ridge morphology that resists horizontal and vertical movement of the denture base Type A, B--Maxilla

66 Location of muscle attachments with limited influence on denture base stability and retention Type A,B Mandible Class II Minor modifiers, psychosocial considerations, mild systemic disease with oral manifestations and localized soft tissue conditions

67 Location of muscle attachments with limited influence on denture base stability and retention Type A,B Mandible Class II Minor modifiers, psychosocial considerations, mild systemic disease with oral manifestations and localized soft tissue conditions
68 Class III This classification level is characterized by the need for surgical revision of denture supporting structures to allow for adequate prosthodontic function. Additional factors now play a significant role in treatment outcomes.

69 Residual bone height of mm measured at the least vertical height of the mandible Class III Class I, II and III maxillomandibular relationship Residual ridge morphology has minimum influence to resist horizontal or vertical movement of the denture base Type C Maxilla Location of muscle attachments with moderate influence on denture base stability and retention Type C--Mandible

70 Residual bone height of mm measured at the least vertical height of the mandible Class III Class I, II and III maxillomandibular relationship Residual ridge morphology has minimum influence to resist horizontal or vertical movement of the denture base Type C Maxilla Location of muscle attachments with moderate influence on denture base stability and retention Type C--Mandible

71 Residual bone height of mm measured at the least vertical height of the mandible Class III Class I, II and III maxillomandibular relationship Residual ridge morphology has minimum influence to resist horizontal or vertical movement of the denture base Type C Maxilla Location of muscle attachments with moderate influence on denture base stability and retention Type C--Mandible

72 Residual bone height of mm measured at the least vertical height of the mandible Class III Class I, II and III maxillomandibular relationship Residual ridge morphology has minimum influence to resist horizontal or vertical movement of the denture base Type C Maxilla Location of muscle attachments with moderate influence on denture base stability and retention Type C--Mandible
73 Conditions requiring preprosthetic surgery: Minor soft tissue procedures Minor hard tissue procedures Implant placement (simple)--no augmentation required Multiple extractions leading to complete edentulism for immediate denture placement Limited interarch space mm Moderate psychosocial considerations and/or moderate oral manifestations of systemic diseases or localized soft tissue conditions TMD symptoms present Large tongue with or without hyperactivity Hyperactive gag reflex
74 Class IV This classification level depicts the most debilitated edentulous condition. Surgical reconstruction is almost always indicated but can not always be accomplished due to the patient s health, desires, past dental history and financial considerations. When surgical revision is not selected, prosthodontic techniques of a specialized nature must be used in order to achieve an adequate treatment outcome.

75 Residual bone height of least vertical height of the mandible Class IV Class I, II and III maxillomandibular relationships Residual ridge offers no resistance to horizontal or vertical movement Type D Maxilla Location of muscle attachments with significant influence on denture base stability and retention Type D and E--Mandible

76 Residual bone height of least vertical height of the mandible Class IV Class I, II and III maxillomandibular relationships Residual ridge offers no resistance to horizontal or vertical movement Type D Maxilla Location of muscle attachments with significant influence on denture base stability and retention Type D and E--Mandible

77 Residual bone height of least vertical height of the mandible Class IV Class I, II and III maxillomandibular relationships Residual ridge offers no resistance to horizontal or vertical movement Type D Maxilla Location of muscle attachments with significant influence on denture base stability and retention Type D and E--Mandible

78 Residual bone height of least vertical height of the mandible Class IV Class I, II and III maxillomandibular relationships Residual ridge offers no resistance to horizontal or vertical movement Type D Maxilla Location of muscle attachments with significant influence on denture base stability and retention Type D and E--Mandible
79 Major conditions which require preprosthetic surgery Implant placement (complex) augmentation required Surgical correction of dentofacial deformities Hard tissue augmentation Major soft tissue revision, i.e., vestibular extensions with or without soft tissue grafting History of paresthesia or dysensthesia Insufficient interarch space with surgical correction required Acquired or congenital maxillofacial defects
80 Severe oral manifestation of systemic disease or conditions including sequelae from oncologic treatment Maxillomandibular ataxia (incoordination) Hyperactivity of tongue that can be associated with a retracted tongue position and/or its associated morphology Hyperactive gag reflex managed with medication Psychosocial conditions warranting professional intervention

81 Refractory patient (a patient who has chronic complaints following appropriate therapy). These patients continue to have difficulty in achieving their treatment expectations despite the thoroughness or frequency of the treatment provided.
82 Guidelines for use of the Complete Edentulism Classification System In those instances when a patient s diagnostic criteria are mixed between two classes, any single criteria of a more complex class will move the patient into that respective class. Utilization of this system is indicated for pre-treatment evaluation and classification of patients. Retrospective analysis on a post-treatment basis may alter a patient s final classification
83 Recognition by third-party payers of these special procedures and techniques Establish codes for procedures Establish codes for groups of procedures Establish that prosthodontists are the most common users of these codes/procedures
84 Target Audiences for this Edentulous Classification System Prosthodontic Educators Prosthodontic Researchers Prosthodontic Clinicians General Practitioners Oral & Maxillofacial Surgeons Third Party Payers Closed Panel Administrators
85 Improve Communication within Specialty Common language Standardize research Standardize terminology
86 Specialties with Classifications Systems Orthodontics Periodontics Oral and Maxillofacial Surgery Endodontics
87 Prosthodontic Classification System Being developed by the ACP for edentulous, partially edentulous and dentate patients Based upon diagnostic findings rather than treatment methods Education will decide what level is appropriate for the new dentist
88 The Next Step? Implementation of the Prosthodontic Classification System Outcome assessment measures for procedures at the competency skill level
89 Objective Criteria for Treatment Difficulty What makes a difficult patient? Measurable criteria Hard tissue Soft tissue Maxillomandibular relationship
Classification System for Partial Edentulism
 TOPICS OF INTEREST Classification System for Partial Edentulism Thomas J. McGarry, DDS, 1 Arthur Nimmo, DDS, 2 James F. Skiba, DDS, 3 Robert H. Ahlstrom, DDS, MS, 4 Christopher R. Smith, DDS, 5 Jack H.
TOPICS OF INTEREST Classification System for Partial Edentulism Thomas J. McGarry, DDS, 1 Arthur Nimmo, DDS, 2 James F. Skiba, DDS, 3 Robert H. Ahlstrom, DDS, MS, 4 Christopher R. Smith, DDS, 5 Jack H.
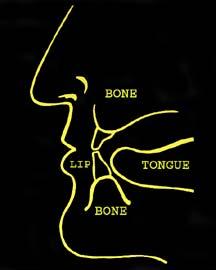
Upper arch. 1Prosthodontics. Dr.Bassam Ali Al-Turaihi. Basic anatomy & & landmark of denture & mouth
 1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
1Prosthodontics Lecture 2 Dr.Bassam Ali Al-Turaihi Basic anatomy & & landmark of denture & mouth Upper arch Palatine process of maxilla: it form the anterior three quarter of the hard palate. Horizontal
Pre prosthetic surgery
 Pre prosthetic surgery The surgical procedures designed to facilitate fabrication of a prosthesis or to improve the prognosis of prosthodontics care. AIMS OF PRE PROSTHETIC SURGERY 1-provide adequate bony
Pre prosthetic surgery The surgical procedures designed to facilitate fabrication of a prosthesis or to improve the prognosis of prosthodontics care. AIMS OF PRE PROSTHETIC SURGERY 1-provide adequate bony
Figure (2-6): Labial frenum and labial notch.
: Labial frenum and labial notch.") The anatomy of the edentulous ridge in the maxilla and mandible is very important for the design of a complete denture. The consistency of the mucosa and architecture of the underlying bone is different
The anatomy of the edentulous ridge in the maxilla and mandible is very important for the design of a complete denture. The consistency of the mucosa and architecture of the underlying bone is different
COMPLETELY DENTATE patients needing
 Classification System for the Completely Dentate Patient Thomas J. McGarry, DDS; 1 Arthur Nimmo, DDS; 2 James F. Skiba, DDS; 3 Robert H. Ahlstrom, DDS, MS; 4 Christopher R. Smith, DDS; 5 Jack H. Koumjian,
Classification System for the Completely Dentate Patient Thomas J. McGarry, DDS; 1 Arthur Nimmo, DDS; 2 James F. Skiba, DDS; 3 Robert H. Ahlstrom, DDS, MS; 4 Christopher R. Smith, DDS; 5 Jack H. Koumjian,
Diagnosis & treatment planning for implants!
 Diagnosis & treatment planning for implants Since implant therapy encompasses both surgical and prosthodontic procedures, integration of these two components of care is essential. The outcome of treatment
Diagnosis & treatment planning for implants Since implant therapy encompasses both surgical and prosthodontic procedures, integration of these two components of care is essential. The outcome of treatment
Samantha W. Chou, D.M.D N. Southport Ave. Chicago, Illinois Phone: Fax:
 Samantha W. Chou, D.M.D. 2325 N. Southport Ave. Chicago, Illinois 60614 Phone: 312-608-6881 Fax: 773-296-0601 Samanthawchou@gmail.com What is our role as the dentist? "We live in a culture in which people
Samantha W. Chou, D.M.D. 2325 N. Southport Ave. Chicago, Illinois 60614 Phone: 312-608-6881 Fax: 773-296-0601 Samanthawchou@gmail.com What is our role as the dentist? "We live in a culture in which people
Arrangement of the artificial teeth:
 Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Lecture Prosthodontic Dr. Osama Arrangement of the artificial teeth: It s the placement of the teeth on a denture with definite objective in mind or it s the setting of teeth on temporary bases. Rules
Oral cavity landmarks
 By: Dr. Ahmed Rabah Oral cavity landmarks The knowledge of oral anatomy and physiology will help the operator and provides enough landmarks to act as positive guide during denture construction. This subject
By: Dr. Ahmed Rabah Oral cavity landmarks The knowledge of oral anatomy and physiology will help the operator and provides enough landmarks to act as positive guide during denture construction. This subject
Prosthetic Options in Implant Dentistry. Hakimeh Siadat, DDS, MSc Associate Professor
 Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Prosthetic Options in Dentistry Hakimeh Siadat, DDS, MSc Associate Professor Dental Research Center, Department of Prosthodontics & Dental s Faculty of Dentistry, Tehran University of Medical Sciences
Dental Morphology and Vocabulary
 Dental Morphology and Vocabulary Palate Palate Palate 1 2 Hard Palate Rugae Hard Palate Palate Palate Soft Palate Palate Palate Soft Palate 4 Palate Hard Palate Soft Palate Maxillary Arch (Maxilla) (Uppers)
Dental Morphology and Vocabulary Palate Palate Palate 1 2 Hard Palate Rugae Hard Palate Palate Palate Soft Palate Palate Palate Soft Palate 4 Palate Hard Palate Soft Palate Maxillary Arch (Maxilla) (Uppers)
Complete denture impressions
 Lec.5 Complete denture impressions د. غسان الطائي Dental Impression: a negative imprint of an oral structure used to produce a positive replica of the structure to be used as a permanent record or in the
Lec.5 Complete denture impressions د. غسان الطائي Dental Impression: a negative imprint of an oral structure used to produce a positive replica of the structure to be used as a permanent record or in the
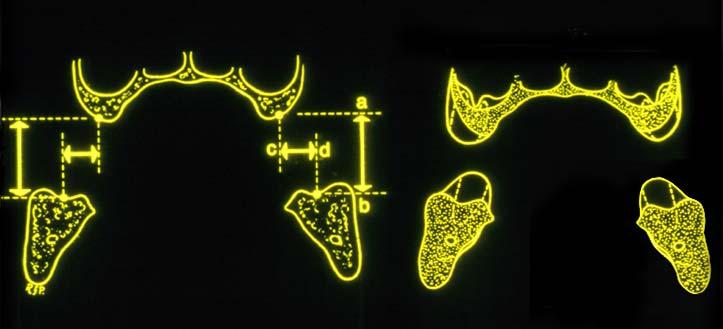
/TLv/ A classification of the edentulous jaws. Trauma; Preprosthetic Surgery. iiiii!iii!iii! ] BASAL
![/TLv/ A classification of the edentulous jaws. Trauma; Preprosthetic Surgery. iiiii!iii!iii! ] BASAL](/thumbs/72/66558540.jpg "/TLv/ A classification of the edentulous jaws. Trauma; Preprosthetic Surgery. iiiii!iii!iii! ] BASAL") Trauma; Preprosthetic Surgery A classification of the edentulous jaws J. I. awood ~ and R. A. Howell 2 ~Maxillofacial Unit, Royal Infirmary, hester, UK, 2Liverpool Dental Hospital, Liverpool, UK J. L awood
Trauma; Preprosthetic Surgery A classification of the edentulous jaws J. I. awood ~ and R. A. Howell 2 ~Maxillofacial Unit, Royal Infirmary, hester, UK, 2Liverpool Dental Hospital, Liverpool, UK J. L awood
Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report
 Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Research & Reviews: Journal of Dental Sciences Rehabilitating a Compromised Site for Restoring Form, Function and Esthetics- A Case Report Priyanka Prakash* Division of Periodontology, Department of Dental
Osseointegrated implant-supported
 CLINICAL SCREWLESS FIXED DETACHABLE PARTIAL OVERDENTURE TREATMENT FOR ATROPHIC PARTIAL EDENTULISM OF THE ANTERIOR MAXILLA Dennis Flanagan, DDS This is a case report of the restoration of a partially edentulous
CLINICAL SCREWLESS FIXED DETACHABLE PARTIAL OVERDENTURE TREATMENT FOR ATROPHIC PARTIAL EDENTULISM OF THE ANTERIOR MAXILLA Dennis Flanagan, DDS This is a case report of the restoration of a partially edentulous
م.م. طارق جاسم حممد REMOVABLE PARTIAL DENTURE INTRODUCTION
 Lec.1 م.م. طارق جاسم حممد REMOVABLE PARTIAL DENTURE INTRODUCTION االسنان طب Prosthodontics is the branch of dentistry pertaining to the restoration and maintenance of oral function, comfort, appearance,
Lec.1 م.م. طارق جاسم حممد REMOVABLE PARTIAL DENTURE INTRODUCTION االسنان طب Prosthodontics is the branch of dentistry pertaining to the restoration and maintenance of oral function, comfort, appearance,
ARAB AMERICAN UNIVERSITY. Lab. Manual. Prosthetic Dentistry1; Removable Prosthodontics. 3 rd year
 ARAB AMERICAN UNIVERSITY Lab. Manual Prosthetic Dentistry1; Removable Prosthodontics 3 rd year Department of Fixed and removable prosthetic Dentistry Faculty of Dentistry 2012/2013 Course Instructor Dr.
ARAB AMERICAN UNIVERSITY Lab. Manual Prosthetic Dentistry1; Removable Prosthodontics 3 rd year Department of Fixed and removable prosthetic Dentistry Faculty of Dentistry 2012/2013 Course Instructor Dr.
ORTHODONTIC INITIAL ASSESSMENT FORM (OIAF) w/ INSTRUCTIONS
 w/ INSTRUCTIONS") Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
Use the accompanying Tip Sheet and How to Score the Orthodontic Initial Assessment Form for guidance in completion of the assessment form. You will need this score sheet and a disposable ruler (or a Boley
Removable partial dentures
 Removable partial dentures Feb, 4, 2015 McCracken's Removable Partial Prosthodontics, Twelfth Edition Carr, Alan B 1 Prosthesis that replaces the missing teeth and associated supporting structures in a
Removable partial dentures Feb, 4, 2015 McCracken's Removable Partial Prosthodontics, Twelfth Edition Carr, Alan B 1 Prosthesis that replaces the missing teeth and associated supporting structures in a
APPENDIX A. MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge)
 You will need this scoresheet and a disposable ruler (or a Boley Gauge)") APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
APPENDIX A MEDICAID ORTHODONTIC INITIAL ASSESSMENT FORM (IAF) You will need this scoresheet and a disposable ruler (or a Boley Gauge) Name: _ I. D. Number: Conditions: 1. Cleft palate deformities 2. Deep
Appendix 4. Case Summary Template. Social history. Patient (Name and Date of birth): Presenting complaints. History Medical history
: Presenting complaints. History Medical history") Appendix 4 Case Summary Template Patient (Name and Date of birth): Presenting complaints Chief complaint Subsidiary complaints History of complaints Patient s expectations History Medical history Medical
Appendix 4 Case Summary Template Patient (Name and Date of birth): Presenting complaints Chief complaint Subsidiary complaints History of complaints Patient s expectations History Medical history Medical
Principles of. By: Dr. Ahmad Rabah
 Principles of By: Dr. Ahmad Rabah 1. Utilize what's present: Whenever possible, select a design that fits the teeth and soft tissues, rather than choosing one that requires tissue alteration. When minimal
Principles of By: Dr. Ahmad Rabah 1. Utilize what's present: Whenever possible, select a design that fits the teeth and soft tissues, rather than choosing one that requires tissue alteration. When minimal
Concepts of occlusion Balanced occlusion. Monoplane occlusion. Lingualized occlusion. Figure (10-1)
") Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Any contact between teeth of opposing dental arches; usually, referring to contact between the occlusal surface. The static relationship between the incising or masticatory surfaces of the maxillary or
Dental Anatomy and Occlusion
 CHAPTER 53 Dental Anatomy and Occlusion Ma Lou C. Sabino DDS, and Emily G. Smythe, DDS What numerical system is used most commonly in the United States for designating the adult dentition? Pediatric dentition?
CHAPTER 53 Dental Anatomy and Occlusion Ma Lou C. Sabino DDS, and Emily G. Smythe, DDS What numerical system is used most commonly in the United States for designating the adult dentition? Pediatric dentition?
Techniques of local anesthesia in the mandible
 Techniques of local anesthesia in the mandible The technique of choice for anesthesia of the mandible is the block injection and this is attributed to the absence of the advantages which are present in
Techniques of local anesthesia in the mandible The technique of choice for anesthesia of the mandible is the block injection and this is attributed to the absence of the advantages which are present in
Evaluation for Severe Physically Handicapping Malocclusion. August 23, 2012
 Evaluation for Severe Physically Handicapping Malocclusion August 23, 2012 Presenters: Office of Health Insurance Programs Division of OHIP Operations Lee Perry, DDS, MBA, Medicaid Dental Director Gulam
Evaluation for Severe Physically Handicapping Malocclusion August 23, 2012 Presenters: Office of Health Insurance Programs Division of OHIP Operations Lee Perry, DDS, MBA, Medicaid Dental Director Gulam
Archived SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS
 SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
SECTION 14 - SPECIAL DOCUMENTATION REQUIREMENTS 14.1 CERTIFICATE OF MEDICAL NECESSITY...2 14.2 OPERATIVE REPORT...2 14.2.A PROCEDURES REQUIRING A REPORT...2 14.3 PRIOR AUTHORIZATION REQUEST...2 14.3.A
Denture Troubleshooting Guide
 Denture Troubleshooting Guide Technical bulletin from National Dentex Comfort Sore spot in vestibule upper or lower denture Sore spot in upper post dam. (posterior limit of upper) Single sore spots on
Denture Troubleshooting Guide Technical bulletin from National Dentex Comfort Sore spot in vestibule upper or lower denture Sore spot in upper post dam. (posterior limit of upper) Single sore spots on
6610 NE 181st Street, Suite #1, Kenmore, WA
 660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
660 NE 8st Street, Suite #, Kenmore, WA 9808 www.northshoredentalacademy.com.08.900 READ CHAPTER The Professional Dental Assistant (p.-9) No Key Terms Recall Questions:,,,, and 6 CLASS SYLLABUS DAY READ
Module 2 Introduction to immediate full arch fixed implant treatment - surgical options
 Module 2 Introduction to immediate full arch fixed implant treatment - surgical options First Name Last Name Objectives Identify the need and opportunity to treat full arch patients with fixed detachable
Module 2 Introduction to immediate full arch fixed implant treatment - surgical options First Name Last Name Objectives Identify the need and opportunity to treat full arch patients with fixed detachable
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note
 Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Bone Reduction Surgical Guide for the Novum Implant Procedure: Technical Note Stephen M. Parel, DDS 1 /Steven L. Ruff, CDT 2 /R. Gilbert Triplett, DDS, PhD 3 /Sterling R. Schow, DMD 4 The Novum System
Dental Implants: A Predictable Solution for Tooth Loss. Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor
 Oral & Maxillofacial Surgeon Associate Clinical Professor") Dental Implants: A Predictable Solution for Tooth Loss Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor What are Dental Implants? Titanium posts used to replace missing
Dental Implants: A Predictable Solution for Tooth Loss Reena Talwar, DDS PhD FRCD(C) Oral & Maxillofacial Surgeon Associate Clinical Professor What are Dental Implants? Titanium posts used to replace missing
Uppers are from Mars, Lowers from Venus Clarifying Overdentures
 Uppers are from Mars, Lowers from Venus Clarifying Overdentures M. Nader Sharifi, D.D.S., M.S. Thomas P. Hinman Dental Meeting Atlanta, GA March 23, 2017 About Your Speaker: M. Nader Sharifi, D.D.S., M.S.
Uppers are from Mars, Lowers from Venus Clarifying Overdentures M. Nader Sharifi, D.D.S., M.S. Thomas P. Hinman Dental Meeting Atlanta, GA March 23, 2017 About Your Speaker: M. Nader Sharifi, D.D.S., M.S.
It has been proposed that partially edentulous maxillectomy
 CLASSICAL ARTICLE Basic principles of obturator design for partially edentulous patients. Part II: Design principles Mohamed A. Aramany, DMD, MS* Eye and Ear Hospital of Pittsburgh and University of Pittsburgh,
CLASSICAL ARTICLE Basic principles of obturator design for partially edentulous patients. Part II: Design principles Mohamed A. Aramany, DMD, MS* Eye and Ear Hospital of Pittsburgh and University of Pittsburgh,
Attachment G. Orthodontic Criteria Index Form Comprehensive D8080. ABBREVIATIONS CRITERIA for Permanent Dentition YES NO
 First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
First Review IL HFS Dental Program Models Second Review Ortho cad Attachment G Orthodontic Criteria Index Form Comprehensive D8080 Ceph Film X-Rays Photos Narrative Patient Name: DOB: ABBREVIATIONS CRITERIA
Contemporary Implant Dentistry
 Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Contemporary Implant Dentistry C H A P T ER 1 4 O F C O N T E M P OR A R Y O R A L A N D M A X I L L OFA C IA L S U R G E RY B Y : D R A R A S H K H O J A S T EH Dental implant is suitable for: completely
Nagri D et al. Linear occlusion and Neutral Zone recording for severely resorbed ridges
 Doi:10.21276/ledent.2018.02.01.02 Case Report LINEAR OCCLUSION AND NEUTRAL ZONE RECORDING USING TISSUE CONDITIONER REPORT OF A SEVERELY RESORBED RIDGE Divya Nagri, 1Ashish Kakkar, 2Neeraj Mittal, 3Lovely
Doi:10.21276/ledent.2018.02.01.02 Case Report LINEAR OCCLUSION AND NEUTRAL ZONE RECORDING USING TISSUE CONDITIONER REPORT OF A SEVERELY RESORBED RIDGE Divya Nagri, 1Ashish Kakkar, 2Neeraj Mittal, 3Lovely
Component parts of Chrome Cobalt Removable Partial Denture
 Lec. 5 د.بسام الطريحي Component parts of Chrome Cobalt Removable Partial Denture Major connectors: Are either bars or plates, the difference between them is in the amount of tissue covers. Plates are broad
Lec. 5 د.بسام الطريحي Component parts of Chrome Cobalt Removable Partial Denture Major connectors: Are either bars or plates, the difference between them is in the amount of tissue covers. Plates are broad
Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants. by Timothy F. Kosinski, DDS, MAGD
 Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants by Timothy F. Kosinski, DDS, MAGD Implant dentistry is undergoing some amazing transformations. With the
Utilizing Digital Treatment Planning and Guided Surgery in Conjunction with Narrow Body Implants by Timothy F. Kosinski, DDS, MAGD Implant dentistry is undergoing some amazing transformations. With the
Interview with Vincent KOKICH
 DOI: 10.1051/odfen/2010302 J Dentofacial Anom Orthod 2010;13:218-222 Ó RODF / EDP Sciences Interview with Vincent KOKICH Conducted by and translated by Sophie ROZENCWEIG Dr. Kokich, it has always been
DOI: 10.1051/odfen/2010302 J Dentofacial Anom Orthod 2010;13:218-222 Ó RODF / EDP Sciences Interview with Vincent KOKICH Conducted by and translated by Sophie ROZENCWEIG Dr. Kokich, it has always been
Diagnosis. overt Examination. Definitive Examination. History. atient interview. Personal History. Clinical Examination.
 Diagnosis overt Examination History Definitive Examination atient interview Personal History Mental Attitude Medical History Dental History Clinical Examination Extra Oral Oral Radiographic Evaluation
Diagnosis overt Examination History Definitive Examination atient interview Personal History Mental Attitude Medical History Dental History Clinical Examination Extra Oral Oral Radiographic Evaluation
ISPUB.COM. Habitual Centric: A Case Report. Manisha, N Kathuria, A Gupta, N Gupta INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Geriatrics and Gerontology Volume 6 Number 2 Habitual Centric: A Case Report Manisha, N Kathuria, A Gupta, N Gupta Citation Manisha, N Kathuria, A Gupta, N Gupta. Habitual
ISPUB.COM The Internet Journal of Geriatrics and Gerontology Volume 6 Number 2 Habitual Centric: A Case Report Manisha, N Kathuria, A Gupta, N Gupta Citation Manisha, N Kathuria, A Gupta, N Gupta. Habitual
Vertical relation: It is the amount of separation between the maxilla and
 Vertical relations Vertical relation: It is the amount of separation between the maxilla and the mandible in a frontal plane. Vertical dimension: It is the distance between two selected points, one on
Vertical relations Vertical relation: It is the amount of separation between the maxilla and the mandible in a frontal plane. Vertical dimension: It is the distance between two selected points, one on
Osseointegrated dental implant treatment generally
 Placement of Dental Implants Without Flap Surgery: A Clinical Report Bader H. Al-Ansari, BDS, MScD*/Robert R. Morris, DMD** Traditionally, the procedure of implant placement requires a surgical periosteal
Placement of Dental Implants Without Flap Surgery: A Clinical Report Bader H. Al-Ansari, BDS, MScD*/Robert R. Morris, DMD** Traditionally, the procedure of implant placement requires a surgical periosteal
CHAPTER 8 SECTION 1.4 ORAL SURGERY TRICARE/CHAMPUS POLICY MANUAL M DEC 1998 SPECIAL BENEFIT INFORMATION
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 SPECIAL BENEFIT INFORMATION CHAPTER 8 SECTION 1.4 Issue Date: October 8, 1986 Authority: 32 CFR 199.4(e)(10) I. DESCRIPTION There are certain oral surgical
Irecall my first course on titanium
 Dental Facial Aesthetics Botox with Implants Warren Roberts, DMD and Janet Roberts, BSc, DMD Botulinum Toxin type A (BoNT-A) has been used extensively cosmetically treating facial lines & therapeutically
Dental Facial Aesthetics Botox with Implants Warren Roberts, DMD and Janet Roberts, BSc, DMD Botulinum Toxin type A (BoNT-A) has been used extensively cosmetically treating facial lines & therapeutically
Post insertion problems in complete denture
 د. زينب الجمالي Lec. 3 Post insertion problems in complete denture Loss of natural teeth &subsequent alveolar resorption has a significant impact on appearance &function. CD fabrication techniques, &placement
د. زينب الجمالي Lec. 3 Post insertion problems in complete denture Loss of natural teeth &subsequent alveolar resorption has a significant impact on appearance &function. CD fabrication techniques, &placement
The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs.
 programs.") B.4.2.11 Orthodontic Services The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs. Orthodontic Consultation
B.4.2.11 Orthodontic Services The following standards and procedures apply to the provision of orthodontic services for children in the Medicaid/NJ FamilyCare (NJFC) programs. Orthodontic Consultation
Selection and arrangement of teeth in rpd
 Selection and arrangement of teeth in rpd upon completion of the articulator mounting and a thorough assessment of the occlusal requirements, the practitioner should be able to perform the proper arrangement
Selection and arrangement of teeth in rpd upon completion of the articulator mounting and a thorough assessment of the occlusal requirements, the practitioner should be able to perform the proper arrangement
Volume 22 No. 14 September Dentists, Federally Qualified Health Centers and Health Maintenance Organizations For Action
 State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 22 No. 14 September 2012 TO: Dentists, Federally Qualified Health Centers and Health Maintenance
State of New Jersey Department of Human Services Division of Medical Assistance & Health Services Volume 22 No. 14 September 2012 TO: Dentists, Federally Qualified Health Centers and Health Maintenance
ADEA COHAEP SYMPOSIA: TURF WARS
 ADEA COHAEP SYMPOSIA: TURF WARS October 30, 2015 8:00 9:30 a.m. Chicago, IL Saulius E. Drukteinis, D.M.D., M.S., Ph.D. Associate Professor, Director, Predoctoral Periodontology Nova Southeastern University
ADEA COHAEP SYMPOSIA: TURF WARS October 30, 2015 8:00 9:30 a.m. Chicago, IL Saulius E. Drukteinis, D.M.D., M.S., Ph.D. Associate Professor, Director, Predoctoral Periodontology Nova Southeastern University
Set the patient in up right position. For mandibular impression the dentist stand in front of the patient
 Set the patient in up right position For mandibular impression the dentist stand in front of the patient For maxillary impression the dentist stand behind the patient Denture retention relies on a number
Set the patient in up right position For mandibular impression the dentist stand in front of the patient For maxillary impression the dentist stand behind the patient Denture retention relies on a number
STANDARDS & GUIDELINES
 STANDARDS & GUIDELINES 3.1.1. Complete Dentures 2 APPENDIX A FOR 3.1.1 Complete Dentures.. 3 Patient History and Treatment Plan Impressions Centric and Protrusive Denture Try In Insertion 3.1.2. Partial
STANDARDS & GUIDELINES 3.1.1. Complete Dentures 2 APPENDIX A FOR 3.1.1 Complete Dentures.. 3 Patient History and Treatment Plan Impressions Centric and Protrusive Denture Try In Insertion 3.1.2. Partial
Prosthodontic Management of Combination Syndrome Case with Metal Reinforced Maxillary Complete Denture and Mandibular Teeth supported Overdenture
 Case Report imedpub Journals www.imedpub.com Periodontics and Prosthodontics DOI: 10.21767/2471-3082.100041 Prosthodontic Management of Combination Syndrome Case with Metal Reinforced Maxillary Complete
Case Report imedpub Journals www.imedpub.com Periodontics and Prosthodontics DOI: 10.21767/2471-3082.100041 Prosthodontic Management of Combination Syndrome Case with Metal Reinforced Maxillary Complete
Question #2: What range of options would you present to this patient?
 Question #2: What range of options would you present to this patient? Some highlights of different treatment planning perspectives 1 Tidy up orthodontic treatment before proceeding with any type of treatment,...implant/
Question #2: What range of options would you present to this patient? Some highlights of different treatment planning perspectives 1 Tidy up orthodontic treatment before proceeding with any type of treatment,...implant/
Severe Malocclusion: Appropriately Timed Treatment. This article discusses challenging issues clinicians face when treating
 Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
Severe Malocclusion: The Importance of Appropriately Timed Treatment A Synchronized and Simultaneous Interdisciplinary Plan Using Cosmetic Dentistry Principles David M. Sarver, DMD, MS Abstract This article
SCD Case Study. Implant-supported overdentures
 SCD Case Study Implant-supported overdentures An implant-retained overdenture may be indicated in patients with changed anatomy, neuromuscular disorders, significant gag reflex or considerable ridge resorption
SCD Case Study Implant-supported overdentures An implant-retained overdenture may be indicated in patients with changed anatomy, neuromuscular disorders, significant gag reflex or considerable ridge resorption
Mesial Step Class I or Class III Dependent upon extent of step seen clinically and patient s growth pattern Refer for early evaluation (by 8 years)
") Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Orthodontics and Dentofacial Development Overview Development of Dentition Treatment Retention and Relapse Growth of Naso-Maxillary Complex Develops postnatally entirely by intramenbranous ossification
Dr.Sepideh Falah-kooshki
 Dr.Sepideh Falah-kooshki MAXILLA Premaxillary/median palatal suture (radiolucent). Incisive fossa and foramen (radiolucent). Nasal passages (radiolucent). Nasal septum (radiopaque). Anterior nasal spine
Dr.Sepideh Falah-kooshki MAXILLA Premaxillary/median palatal suture (radiolucent). Incisive fossa and foramen (radiolucent). Nasal passages (radiolucent). Nasal septum (radiopaque). Anterior nasal spine
Occlusion in complete denture
 Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
Occlusion in complete denture Occlusion is a concept that is pertinent to all dental patients wheather they have their own teeth or not.it is a term used to describe the contact relationship between the
Methods of determining vertical dimension of occlusion
 Methods of determining vertical dimension of occlusion 1) Pre-extraction records a) Willis gauge This device could used to measure V D O before teeth extraction and then recorded in the patient record.
Methods of determining vertical dimension of occlusion 1) Pre-extraction records a) Willis gauge This device could used to measure V D O before teeth extraction and then recorded in the patient record.
Deep and cross bite (class II and class III) Special Edition
 Special Edition") Deep and cross bite (class II and class III) Special Edition Sandra Goergen Nancy Tomkins Challenging class II and class III bites This Special Edition highlights the T and K mould posterior tooth morphology
Deep and cross bite (class II and class III) Special Edition Sandra Goergen Nancy Tomkins Challenging class II and class III bites This Special Edition highlights the T and K mould posterior tooth morphology
REMOVABLE PROSTHODONTICS
 REMOVABLE PROSTHODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG020.03 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
REMOVABLE PROSTHODONTICS UnitedHealthcare Dental Coverage Guideline Guideline Number: DCG020.03 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...1 BENEFIT CONSIDERATIONS...1
Non-surgical management of skeletal malocclusions: An assessment of 100 cases
 Non-surgical management of skeletal malocclusions: An assessment of 100 cases In early 1970 s reduced risks associated with surgical procedures allowed the treatment planning process for skeletal malocclusions
Non-surgical management of skeletal malocclusions: An assessment of 100 cases In early 1970 s reduced risks associated with surgical procedures allowed the treatment planning process for skeletal malocclusions
Surveying. 3rd year / College of Dentistry/University of Baghdad ( ) Page 1
 Page 1") د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
د. فائزة Lec.3 Prosthodontics Surveying The ideal requirements for successful removable partial denture are: 1. Be easily inserted and removed by the patient. 2. Resist dislodging forces. 3. It should
Benefits of CBCT in Implant Planning
 10.5005/jp-journals-10012-1032 CLINICAL SCIENCE 1 Gregori M Kurtzman, 2 Douglas F Dompkowski 1 Private General Practice in Silver Spring, Maryland, USA 2 Private Periodontal Practice in Bethesda, Maryland,
10.5005/jp-journals-10012-1032 CLINICAL SCIENCE 1 Gregori M Kurtzman, 2 Douglas F Dompkowski 1 Private General Practice in Silver Spring, Maryland, USA 2 Private Periodontal Practice in Bethesda, Maryland,
Delta Dental of Colorado EXCLUSIVE PANEL OPTION (EPO) Schedule EPO 1B List of Patient Co-Payments. * See Special Provisions on Last Page
 Schedule EPO 1B List of Patient Co-Payments. * See Special Provisions on Last Page") List of Co-Payments Code edure Code Definition Co-Pay DIAGNOSTIC CODES D0120 Periodic oral evaluation - established patient $10.00 D0140 Limited oral evaluation - problem focused $10.00 D0145 Oral evaluation
List of Co-Payments Code edure Code Definition Co-Pay DIAGNOSTIC CODES D0120 Periodic oral evaluation - established patient $10.00 D0140 Limited oral evaluation - problem focused $10.00 D0145 Oral evaluation
ORTHOGNATHIC SURGERY
 ORTHOGNATHIC SURGERY MEDICAL POLICY Effective Date: February 1, 2017 Review Dates: 1/93, 7/95, 10/97, 4/99, 10/00, 8/01, 12/01, 4/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11,
ORTHOGNATHIC SURGERY MEDICAL POLICY Effective Date: February 1, 2017 Review Dates: 1/93, 7/95, 10/97, 4/99, 10/00, 8/01, 12/01, 4/02, 2/03, 1/04, 1/05, 12/05, 12/06, 12/07, 12/08, 12/09, 12/10, 12/11,
Much has been written about the success of various
 Simplified Guide for Precise Implant Placement: A Technical Note Brent D. Kennedy, MD, DDS*/Thomas A. Collins, Jr, DDS**/ Patrick C. W. Kline, DMD, MD** Ideal implant placement is ultimately determined
Simplified Guide for Precise Implant Placement: A Technical Note Brent D. Kennedy, MD, DDS*/Thomas A. Collins, Jr, DDS**/ Patrick C. W. Kline, DMD, MD** Ideal implant placement is ultimately determined
Conus Concept: A Rewarding Complete Denture Treatment
 Conus Concept: A Rewarding Complete Denture Treatment Complete dentures have largely become the domain of the denturist due to the dissatisfaction general dentists feel with this treatment. Multiple visits,
Conus Concept: A Rewarding Complete Denture Treatment Complete dentures have largely become the domain of the denturist due to the dissatisfaction general dentists feel with this treatment. Multiple visits,
For many years, patients with
 Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
Dr. Robert Lowe is one of the great teachers in dentistry. Recently, he received the Gordon J. Christensen Award from the Chicago Dental Society in recognition of his excellence in teaching. Some of my
SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015
 SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015 Dental Surveyor: It is a mechanical device used to determine the relative parallelism of the teeth surfaces and the undercuts areas in relation to
SURVEYING OF REMOVABLE PARITAL DENTURES FEB, 11, 2015 Dental Surveyor: It is a mechanical device used to determine the relative parallelism of the teeth surfaces and the undercuts areas in relation to
IMPRESSION MAKING (IN COMPLETE DENTURES)
") IMPRESSION MAKING (IN COMPLETE DENTURES) DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics), Adelaide, FRACDS 17.06.2007 Impressions An impression
IMPRESSION MAKING (IN COMPLETE DENTURES) DR ZURYATI AB GHANI BDS (WALES), Grad Dip Clin Dent (Adelaide), Doctor in Clinical Dentistry (prosthodontics), Adelaide, FRACDS 17.06.2007 Impressions An impression
Oral Health and Dentistry
 Page 107 to 118 Volume 1 Issue 2 2017 Case Report Oral Health and Dentistry ISSN: 2573-4989 Full Mouth Implants Rehabilitation of a Patient with Ectodermal Dysplasia After 3-Ds Ridge Augmentation and Bilateral
Page 107 to 118 Volume 1 Issue 2 2017 Case Report Oral Health and Dentistry ISSN: 2573-4989 Full Mouth Implants Rehabilitation of a Patient with Ectodermal Dysplasia After 3-Ds Ridge Augmentation and Bilateral
Post insertion problems in complete denture.
 Page1 Lect. 8 Prosthodontics Dr. Intisar J. Ismail 5 th class 22/11/2016 Post insertion problems in complete denture. Loss of natural teeth and subsequent alveolar resorption has a significant impact on
Page1 Lect. 8 Prosthodontics Dr. Intisar J. Ismail 5 th class 22/11/2016 Post insertion problems in complete denture. Loss of natural teeth and subsequent alveolar resorption has a significant impact on
Dr.Mikulás Krisztina. Fabrication of the trial denture, and the try in procedure
 Dr.Mikulás Krisztina Fabrication of the trial denture, and the try in procedure the correct shape for the labial, buccal and palatal surfaces Adjusting the upper record rim Before starting adjustment-upper
Dr.Mikulás Krisztina Fabrication of the trial denture, and the try in procedure the correct shape for the labial, buccal and palatal surfaces Adjusting the upper record rim Before starting adjustment-upper
DEVELOPING ANALOGUE SUBTITUTE FOR THE MAXILLARY DENTURE BEARING AREA. Dr Muhammad Rizwan Memon FCPS Assistant Professor
 DEVELOPING ANALOGUE SUBTITUTE FOR THE MAXILLARY DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor Mucous membrane Residual Ridge Incisive papilla Rugae area Mid palatine raphe Hard
DEVELOPING ANALOGUE SUBTITUTE FOR THE MAXILLARY DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor Mucous membrane Residual Ridge Incisive papilla Rugae area Mid palatine raphe Hard
CHAPTER. 1. Uncontrolled systemic disease 2. Retrognathic jaw relationship
 CHAPTER 7 Immediate Implant Supported Restoration of the Edentulous Arch Stephen G. Alfano and Robert M. Laughlin Department of Oral and Maxillofacial Surgery, Naval Medical Center San Diego, San Diego,
CHAPTER 7 Immediate Implant Supported Restoration of the Edentulous Arch Stephen G. Alfano and Robert M. Laughlin Department of Oral and Maxillofacial Surgery, Naval Medical Center San Diego, San Diego,
Indirect retainers. 1 i
 8 1 i Indirect retainers Factors Influencing Effectiveness Indirect Retainers Auxiliary Functions Indirect Retainers Forms Indirect Retainers Auxiliary occlusal rest Canine extensions fiom occlusal rests
8 1 i Indirect retainers Factors Influencing Effectiveness Indirect Retainers Auxiliary Functions Indirect Retainers Forms Indirect Retainers Auxiliary occlusal rest Canine extensions fiom occlusal rests
1- Implant-supported vs. implant retained distal extension mandibular partial overdentures and residual ridge resorption. Abstract Purpose: This
 1- Implant-supported vs. implant retained distal extension mandibular partial overdentures and residual ridge resorption. Abstract Purpose: This retrospective study in male patients sought to examine posterior
1- Implant-supported vs. implant retained distal extension mandibular partial overdentures and residual ridge resorption. Abstract Purpose: This retrospective study in male patients sought to examine posterior
Preserving the Integrity of Facial Structures with Implant-Retained Overdentures
 Preserving the Integrity of Facial Structures with Implant-Retained Overdentures Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD The Centers for Disease Control and Prevention (CDC) has
Preserving the Integrity of Facial Structures with Implant-Retained Overdentures Go online for in-depth content by Timothy F. Kosinski, DDS, MAGD The Centers for Disease Control and Prevention (CDC) has
Cephalometric Analysis
 Cephalometric Analysis of Maxillary and Mandibular Growth and Dento-Alveolar Change Part III In two previous articles in the PCSO Bulletin s Faculty Files, we discussed the benefits and limitations of
Cephalometric Analysis of Maxillary and Mandibular Growth and Dento-Alveolar Change Part III In two previous articles in the PCSO Bulletin s Faculty Files, we discussed the benefits and limitations of
OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC
 Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Oral Anatomy and Occlusion Prosthodontic Component OCCLUSION: PHYSIOLOGIC vs. NON-PHYSIOLOGIC By: Dr. Babak Shokati, DDS, MSc. MSc. Prosthodontics Definition of Masticatory System by The Academy of Prosthodontics
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults
 Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Evaluation of maxillary protrusion malocclusion treatment effects with prosth-orthodontic method in old adults Peicheng Xu, DDS, MSD, a and Honghu Liu, DDS, PhD b a Shanghai Xuhui Dental Hospital and b
Accu-Dent. impression system. Procedural guide. System 2 TM. For removable dentate impressions
 Accu-Dent impression system System 2 TM Procedural guide System 2 TM For removable dentate impressions The Complete System 2 TM Accu-Dent s System 2 is designed for partials, immediate dentures, orthodontics,
Accu-Dent impression system System 2 TM Procedural guide System 2 TM For removable dentate impressions The Complete System 2 TM Accu-Dent s System 2 is designed for partials, immediate dentures, orthodontics,
Dentistry continues to evolve. Esthetic Templates for Complex Restorative Cases: Rationale and Management
 Esthetic Templates for Complex Restorative Cases: Rationale and Management DEAN E. KOIS, DMD* KYLE K. SCHMIDT, DDS* ARIEL J. RAIGRODSKI, DMD, MS ABSTRACT Complex restorative cases require difficult clinical
Esthetic Templates for Complex Restorative Cases: Rationale and Management DEAN E. KOIS, DMD* KYLE K. SCHMIDT, DDS* ARIEL J. RAIGRODSKI, DMD, MS ABSTRACT Complex restorative cases require difficult clinical
Saudi Dental Licensure Examination Content Outline
 Saudi Dental Licensure Examination Content Outline This outline provides a common organization of SDLE content. SDLE central committee continually reviews the outline to ensure content is relevant to the
Saudi Dental Licensure Examination Content Outline This outline provides a common organization of SDLE content. SDLE central committee continually reviews the outline to ensure content is relevant to the
ORTHOGNATHIC SURGERY
 Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-16 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Status Active Medical and Behavioral Health Policy Section: Surgery Policy Number: IV-16 Effective Date: 10/22/2014 Blue Cross and Blue Shield of Minnesota medical policies do not imply that members should
Low-Force Mechanics Nonextraction. Estimated treatment time months (Actual 15 mos 1 week). Low-force mechanics.
. Low-force mechanics.") T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
T.S. Age: 43 Years 1 Month Diagnosis: Class I Nonextraction Adult (severe crowding, very flat profile with tissue-grafting indications) Background: This case is very similar to the previous case of a 14-year-old.
Benefit Changes for Texas Health Steps Orthodontic Dental Services Effective January 1, 2012
 Benefit Changes for Texas Health Steps Orthodontic Dental Services Effective January 1, 2012 Information posted November 14, 2011 Effective for dates of service on or after January 1, 2012, the following
Benefit Changes for Texas Health Steps Orthodontic Dental Services Effective January 1, 2012 Information posted November 14, 2011 Effective for dates of service on or after January 1, 2012, the following
DIAGNOSIS & TREATMENT PLANNING For RPD
 DIAGNOSIS & TREATMENT PLANNING For RPD Introduction Goals of Treatment a) Eliminate disease b) Preserve what remains c) Restore esthetics & function d) Make up of patient psychology Functions of a RPD
DIAGNOSIS & TREATMENT PLANNING For RPD Introduction Goals of Treatment a) Eliminate disease b) Preserve what remains c) Restore esthetics & function d) Make up of patient psychology Functions of a RPD
UNDERSTANDING DIGITAL DENTISTRY: CBCT AND INTRA-ORAL 30 SCANNING
 UNDERSTANDING DIGITAL DENTISTRY: CBCT AND INTRA-ORAL 30 SCANNING -=- & UNDERSTANDING DIGITAL DENTISTRY: CBCT AND INTRA-ORAL 30 SCANNING ----CBCTi-------iTERO------ NewTom VGi *Vertical Patient Positioning
UNDERSTANDING DIGITAL DENTISTRY: CBCT AND INTRA-ORAL 30 SCANNING -=- & UNDERSTANDING DIGITAL DENTISTRY: CBCT AND INTRA-ORAL 30 SCANNING ----CBCTi-------iTERO------ NewTom VGi *Vertical Patient Positioning
Exclusive Panel Option (EPO 1-B) a feature of the Delta Dental PPO Denver Public Schools- Group #
 a feature of the Delta Dental PPO Denver Public Schools- Group #") Exclusive Panel Option (EPO 1-B) a feature of the Delta Dental PPO Denver Public Schools- Group #6694 7.2011 MAXIMUM BENEFIT Calendar Year Orthodontic Lifetime CALENDAR YEAR DEDUCTIBLE WHO CAN BE COVERED
Exclusive Panel Option (EPO 1-B) a feature of the Delta Dental PPO Denver Public Schools- Group #6694 7.2011 MAXIMUM BENEFIT Calendar Year Orthodontic Lifetime CALENDAR YEAR DEDUCTIBLE WHO CAN BE COVERED
Prosthodontic Rehabilitation of a Partially Edentulous Hemiglossectomy Patient: A Clinical Report
 case report 10.5005/jp-journals-10031-1067 Prosthodontic Rehabilitation of a Partially Edentulous Hemiglossectomy Patient: A Clinical Report 1 Ragini Sudhakar Sanaye, 2 Sabita M Ram, 3 Naisargi Shah, 4
case report 10.5005/jp-journals-10031-1067 Prosthodontic Rehabilitation of a Partially Edentulous Hemiglossectomy Patient: A Clinical Report 1 Ragini Sudhakar Sanaye, 2 Sabita M Ram, 3 Naisargi Shah, 4
Mandibular ridge changes after adaptation. An issue of shortened dental arch to be considered from changes of soft tissues after unattended tooth loss
 (Journal of Dental Outlook, Vol.110, Vol.6:1021~1027, Japan 2007. An issue of shortened dental arch to be considered from changes of soft tissues after unattended tooth loss Dr. Jiro Abe Abe Dental Clinic
(Journal of Dental Outlook, Vol.110, Vol.6:1021~1027, Japan 2007. An issue of shortened dental arch to be considered from changes of soft tissues after unattended tooth loss Dr. Jiro Abe Abe Dental Clinic
TOOTH SUPPORTED MANDIBULAR OVERDENTURE: A FORGOTTEN CONCEPT
 TJPRC: International Journal of Prosthetic Dentistry & Research (TJPRC:IJPDR) Vol. 1, Issue 1, Jun 2017, 5-10 TJPRC Pvt. Ltd. TOOTH SUPPORTED MANDIBULAR OVERDENTURE: A FORGOTTEN CONCEPT ANSUIA GUPTA 1,
TJPRC: International Journal of Prosthetic Dentistry & Research (TJPRC:IJPDR) Vol. 1, Issue 1, Jun 2017, 5-10 TJPRC Pvt. Ltd. TOOTH SUPPORTED MANDIBULAR OVERDENTURE: A FORGOTTEN CONCEPT ANSUIA GUPTA 1,
Frequency of the Various Classes of Removable Partial Dentures and Selection of Major Connectors and Direct/Indirect Retainers
 Turk J Med Sci 31 (2001) 445-449 TÜB TAK Filiz KEYF Frequency of the Various Classes of Removable Partial Dentures and Selection of Major Connectors and Direct/Indirect Retainers Received: November 30,
Turk J Med Sci 31 (2001) 445-449 TÜB TAK Filiz KEYF Frequency of the Various Classes of Removable Partial Dentures and Selection of Major Connectors and Direct/Indirect Retainers Received: November 30,
DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA. Dr Muhammad Rizwan Memon FCPS Assistant Professor
 DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor Crest of Residual Ridge Buccal Shelf Shape of supporting structure Mylohyoid Ridge
DEVELOPING ANALOGUE/SUBTITUTE FOR THE MANDIBULAR DENTURE BEARING AREA Dr Muhammad Rizwan Memon FCPS Assistant Professor Crest of Residual Ridge Buccal Shelf Shape of supporting structure Mylohyoid Ridge
CASE REPORT. CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration
 Computer Aided Implantology Academy Newsletter - Newsletter 20 - July 2009 CASE REPORT CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration Case Report
Computer Aided Implantology Academy Newsletter - Newsletter 20 - July 2009 CASE REPORT CBCT-Assisted Treatment of the Failing Long Span Bridge with Staged and Immediate Load Implant Restoration Case Report
Removable Prosthodontics. Summative Evaluations
 Department of General Dentistry Division of Removable Prosthodontics Summative Evaluations For Competency #9 Rev. February 2010 Ronni A. Schnell, D.M.D., M.A.G.D. General Guidelines for the Removable Prosthodontics
Department of General Dentistry Division of Removable Prosthodontics Summative Evaluations For Competency #9 Rev. February 2010 Ronni A. Schnell, D.M.D., M.A.G.D. General Guidelines for the Removable Prosthodontics