Resistance is not futile: working with refractory depression and anxiety
|
|
|
- Hester Moody
- 6 years ago
- Views:
Transcription

1 Resistance is not futile: working with refractory depression and anxiety
2 Divulgation des conflits d intérêts Conseil consultatif ou comité analogue Essais cliniques ou études Honoraires ou autres revenus Valeant, BMS, Otsuka, Eli Lilly, Lundbeck, Janssen, Shire Subventions de recherche
3 Objectives: Define risk and evaluation factors in psychiatric resistance Review the canadian guidelines (CANMAT) in pharmacologically dealing with treatment resistance To know which modalities of intervention are more effective Review the new modalities, some controversial, in dealing with refractory illness Review the risk/benefit factors in augmentation and switching strategies

4
5 How common is treatment resistant depression (trd)? Corey-Lisle and colleagues reported that approximately 22% of patients who received treatment for depression by their primary-care physicians remitted following 6 months of treatment, 32% were responders, while 45% were nonresponders University and speciality clinic studies not much better, listing resistance at 50% or more. Longer term follow up is slightly more positive
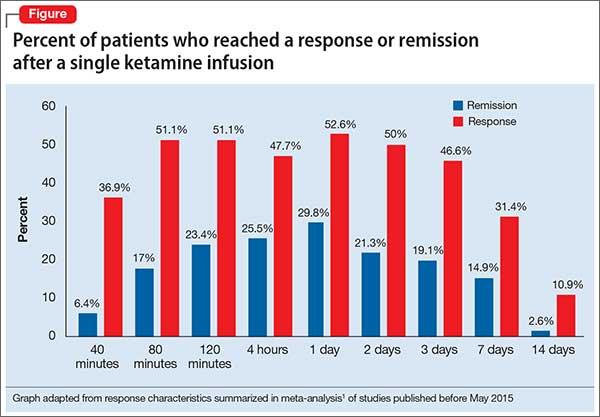
6 Achieving remission: Evidence of phyisiological resistance 50 Percent remission remission rate % Time after start of episode (months)
7 The price of resistance: Depressives smoke at 3 times the popn rate; even when well they have greater difficulty quitting Chronic depression doubles the risk of a heart attack and, if it persists, increases the short term mortality by 5 times Depression is the biggest risk factor for angina and death shortly after heart attack 87% of diagnosed breast cancer patients had severe depressive and anxiety symptoms in the 2 years prior
8 Further evidence; Treated depressives spend 59% of the next decades in a state of low grade depression By 3 rd episode of depression, relapse rate exceeds 90% 4 11/22/17
9
10 The natural progression of depression: evidence for biologica resistance Major depression lifetime prevalance: 17% Dysthymia: 8% DSM low grade symptoms:25% response rate: 50-70% once treated: 25-35% remission continue residual illness: >50% risk of recurrence with residua: 5 times normal rate only 25% risk if patient put into remission 11/22/17
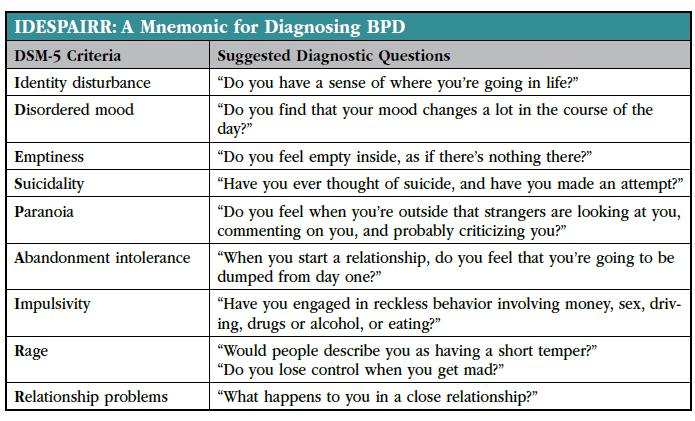
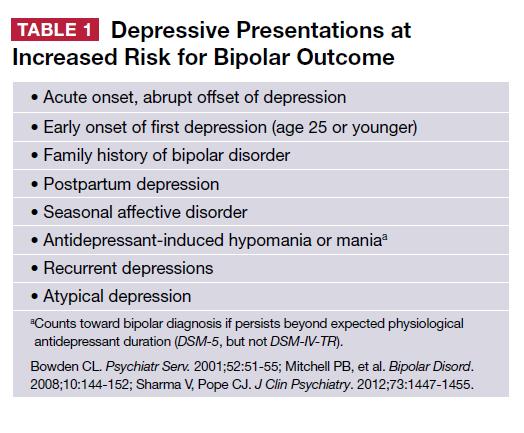
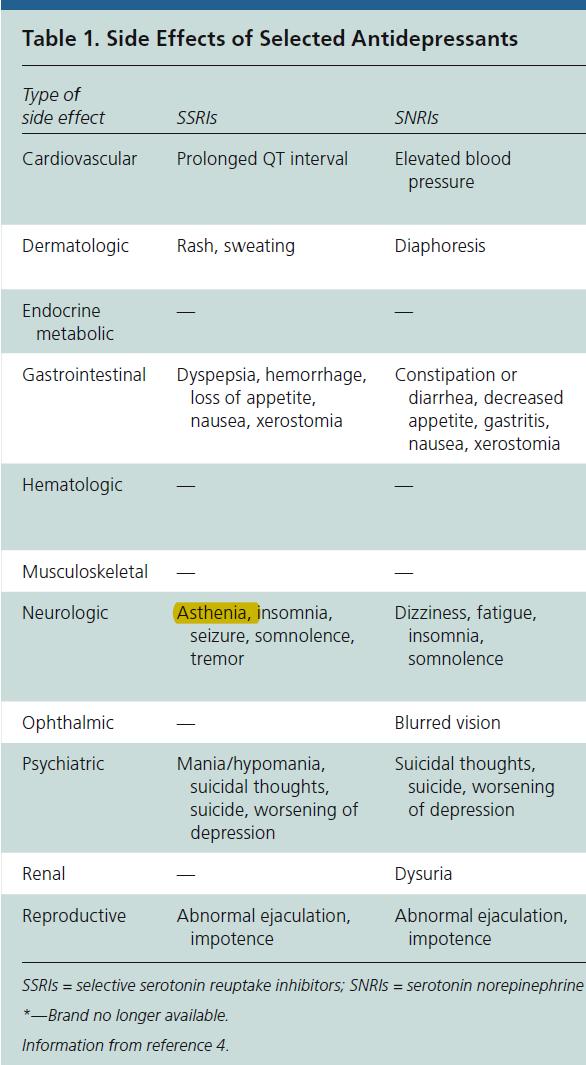
11 How to short circuit depression resistance Apply scales, labs, and good history to rule out other treatable co-morbidity: Borderline personality +/- dependent, narcissistic Workplace and adjustment dynamics: work role, stress, strain, interpersonal, secondary gain Hypothyroidism and metabolic imbalances, sleep apnea Bipolar depression: see criteria Comorbid anxiety +/- insomnia: careful use of benzos Substance overuse or abuse: even low grade alcohol, THC, hard drugs, benzos Do not wait: start pharmacotherapy +/- atypicals and go to next steps quickly: Rapid dose optimization with new generation drugs: easily dosed, effective, minimal SFX Knowledge of effective boosting strategies and their doses Use scale score guided depression treatment (PHQ ( and others) Optimize cognition quickly Weight gain early: switch; check for sleep, anxiety, sexual side effects: antidotes Comorbid atypical boosters: vitamins, light therapy, ketamine(?) Use adjunctive behavioral and cognitive strategies from the start, even if book or internet based: Behavioral activation framework Antidepressant skills workbook: slant towards employment and staying employed Exercise daily Whole foods diet/ Mediterranean: Viva L Italia!!!
12 How to short circuit depression resistance Apply scales, labs, and good history to rule out other treatable comorbidity: Borderline personality +/- dependent, narcissistic Workplace and adjustment dynamics: work role, stress, strain, interpersonal, secondary gain Hypothyroidism and metabolic imbalances, sleep apnea Bipolar depression: see criteria Comorbid anxiety +/- insomnia: careful use of benzos Substance overuse or abuse: even low grade alcohol, THC, hard drugs, benzos
13
14
15
16 How to short circuit depression resistance Do not wait: start pharmacotherapy +/- atypicals and go to next steps quickly: Rapid dose optimization with new generation drugs: easily dosed, effective, minimal SFX crucial role of asthenia, sexual dysfunction Knowledge of effective boosting strategies and their doses Use scale score guided depression treatment (PHQ ( and others) Optimize cognition quickly Weight gain early: switch; check for sleep, anxiety, sexual side effects: antidotes Comorbid atypical boosters: vitamins, light therapy, ketamine(?)
17 MAX DOSE
18
19 Antidepressants With Evidence for Superior Efficacy Based on Meta-Analyses Level 1 Antidepressant Escitalopram Comparators Citalopram, duloxetine, fluoxetine, fluvoxamine, paroxetine Mirtazapine Sertraline Venlafaxine Duloxetine, fluoxetine, fluvoxamine, paroxetine, sertraline, venlafaxine Duloxetine, fluoxetine, fluvoxamine, paroxetine Duloxetine, fluoxetine, fluvoxamine, paroxetine Level 2 Antidepressant Agomelatine Citalopram Comparators Fluoxetine, sertraline Paroxetine Return to algorithm SECTION 3 - Pharmacological Treatments Kennedy SH et al. Can J Psychiatry 2016;61(9):540-60
20
21
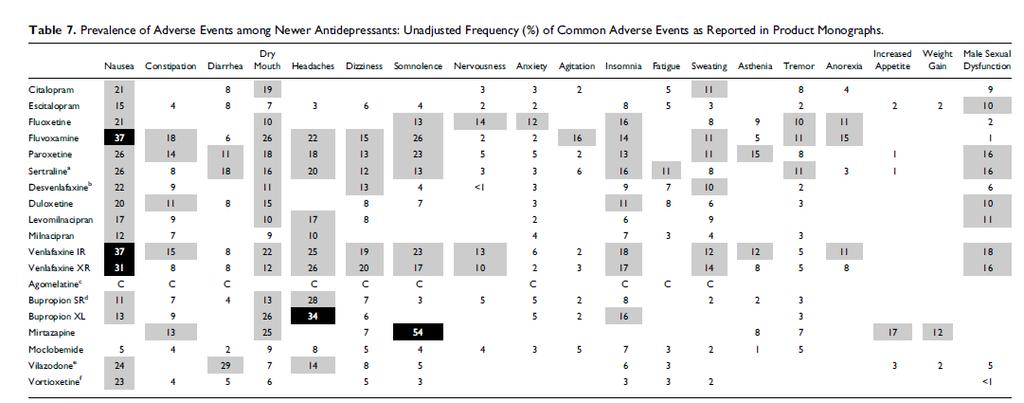
22 Modern Antidepressants: What u really don t want: The Culprits: More Culprits: Lethality in overdose Tricyclics, effexor, wellbutrin, celexa (generally rare) Sexual side effects All cause except Trintellix, Wellbutrin, Remeron Blood pressure changes Effexor, wellbutrin, fetzima Metabolic/weight gain Paxil, Remeron Withdrawal syndrome (often severe) Effexor, Paxil, Pristiq, Cymbalta Worsening Anxiety Wellbutrin, prozac, fetzima Huge dosage ranges Effexor, zoloft Medication interactions Prozac, paxil, luvox Headache Celexa, prozac Oversedation Paxil, remeron, luvox

23 Modern Antidepresssants: What you want
24
25
26
27


28 Newly Approved Antidepressants Antidepressant Mode of action Acute efficacy Maintenance therapy Vortioxetine Multimodal: Ø SRI Ø 5-HT 1A agonist Ø 5-HT 1B partial agonist Ø Antagonist at 5-HT 1D, 5-HT 3A, 5- HT 7 Meta-analysis of 12 RCTs was superior to PBO for response, remission Positive effects on multiple cognitive domains in MDD Superior to PBO for relapse prevention Vilazodone Multimodal: Ø SRI Ø 5-HT 1A partial agonist 12 RCTs 5 early trials failed 4 Phase 3 or 4 studies positive for 20 and 40 mg vs PBO None available Levomilnacipran SNRI Pooled analysis of 5 PBO-controlled RCTs was positive for response, remission No significant difference vs PBO for relapse prevention RCT, randomized controlled trial; SNRI, serotonin-noradrenaline reuptake inhibitor; SRI, serotonin reuptake inhibitor; PBO, placebo; MDD, major depressive disorder; GI, gastrointestinal SECTION 3 - Pharmacological Treatments Lam RW et al. Can J Psychiatry 2016;61(9):506-9
29 Adjuncts: General Considerations High doses of the adjunct often (Lithium) The response is seldom miraculously fast: 2-3 week trials needed; but atypicals often act in one week There will be side effects: tremor, weight gain, sexual dysfunction Adjuncts used too late, after biological resistance has crystallized Cost and compliance are issues Modern meds dosed correctly and quickly is a good start
30
31
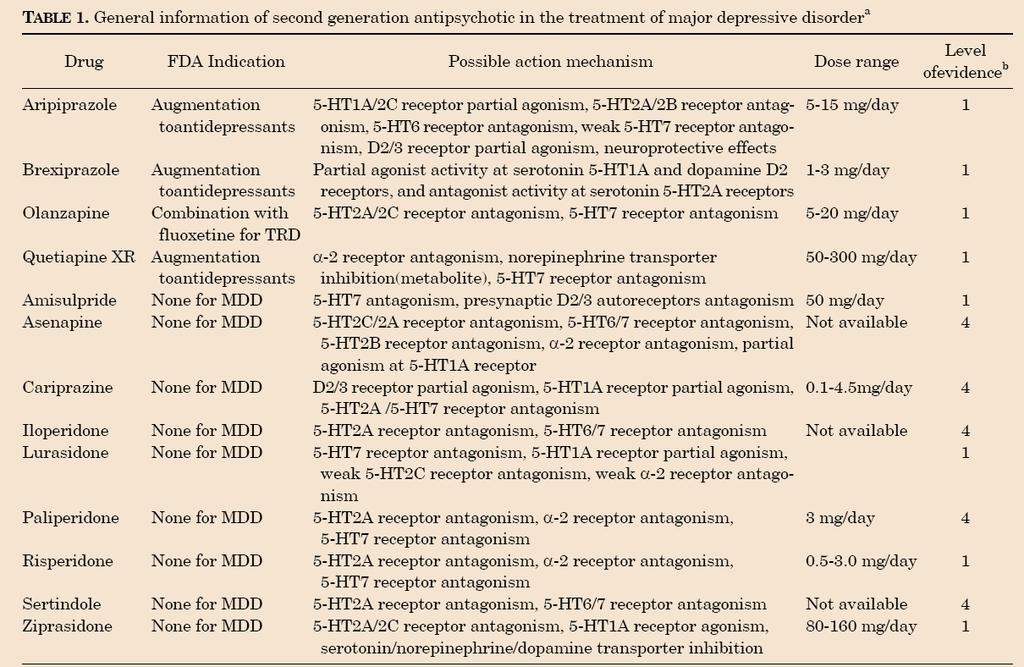
32 Adjunctive Strategies for Non or Partial Response 1 st LINE Aripiprazole (2-15 mg) Quetiapine ( mg) Risperidone (1-3 mg) 2 nd LINE Brexpiprazole* (1-3 mg) Olanzapine ( mg) Bupropion ( mg) Lithium ( mg [therapeutic serum levels]) Mirtazapine/mianserin (30-60 mg) Modafinil ( mg) Triiodothyronine (25-50 mcg) 3 rd LINE TCAs (e.g. desipramine) (various) Other antidepressants (various) Other stimulants (methylphenidate, lisdexamfetamine, etc) Ziprasidone (20-80 mg bid) *Newly approved since the 2009 CANMAT guidelines. TCA, tricyclic antidepressant; IV, intravenous; N/A, not applicable Return to algorithm SECTION 3 - Pharmacological Treatments Kennedy SH et al. Can J Psychiatry 2016;61(9):540-60
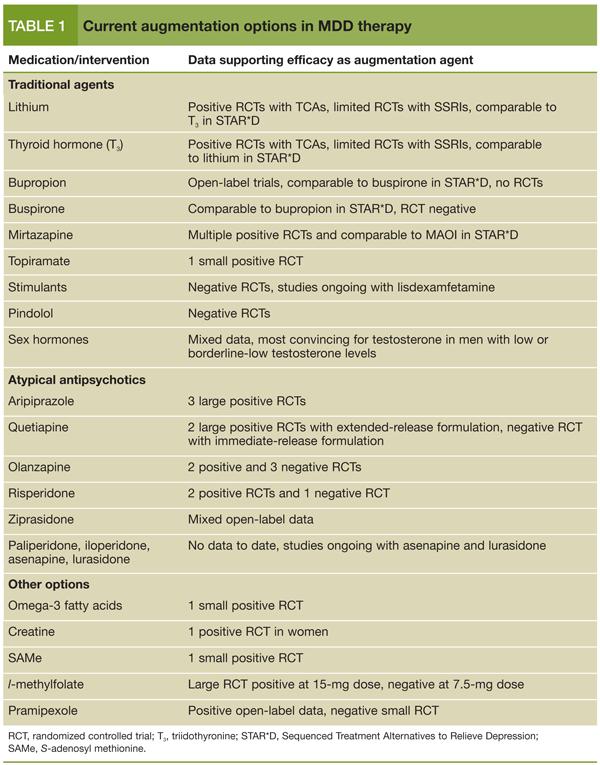
33 Preferential augmentation strategies Atypical antipsychotics Greatest knowledge base and effect sizes Low doses needed, except for Seroquel (at or greater than 150 mg po qhs) Metabolic/neurological side effects more marked in a depressed versus schizophrenic population Lithium Works as booster for all classes of antidepressant Rule out bipolarity if it does work! Doses needed: high; knowledge base: good Weight gain, renal monitoring, polyuria cognitive effects Combination antidepressants Do not start from beginning of therapy Use drugs with different mechanisms of action Proven inferior to the other 2 booster categories listed here
34
35

36

37
38
39 What not to regularly use: St John s wart (sorry, wort) Liver toxicity, interactions, phototoxicity Kava Potentially addictive, hepatotoxicity Omega 3 oils Large number of pills: dyspepsia, fish smell, medication interactions Effect size?


40 MDD criteria: mood, physical, and cognitive symptoms 2 weeks in which a person has 5 symptoms that must include: Depressed mood and/or Loss of interest or pleasure plus 4 of: Significant changes in weight and/or appetite Insomnia or hypersomnia Psychomotor agitation or retardation Fatigue or loss of energy Feelings of worthlessness or excessive/inappropriate guilt Diminished ability to think or concentrate, or indecisiveness Recurring thoughts of death or suicide, including plans and attempts DSM-5, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed

41 MDD is a multidimensional disease
42 Cognitive Impact of MDD Cognitive deficits are associated with significant impact on daily functioning and quality of life Cognitive dysfunction Is more strongly associated with loss of workplace productivity than ratings of depression severity Is a common symptom that can persist even after mood symptoms have remitted Clinical assessment and monitoring of cognitive symptoms during management of MDD is critical MDD, major depressive disorder SECTION 1 Principles of Care Lam R., et al., Can J Psychiatry 2016;61(9):
43 FDA Panel Backs Vortioxetine for Cognitive Dysfunction in MDD The US Food and Drug Administration's (FDA's) Psychopharmacologic Drug Advisory Committee has determined that there is substantial evidence to support claims that vortioxetine (Brintellix) is effective in the treatment of cognitive dysfunction in patients with major depressive disorder (MDD). The prevalence of cognitive dysfunction associated with depression is high, according to background information in the press release. In a 3-year prospective study of people treated for depression, cognitive symptoms (defined as diminished ability to think or concentrate and/or indecisiveness) was reported 94% of the time during acute major depressive episodes and 44% of the time during remission. Only vortioxetine shown to increase functionality in a series of objective measures of cognitive function.
44 The role of ECT Currently severely underused 75-80% effective in resistance where there is no severe personality disorder comorbidly if ect maintenance not continued past the initial remission period, 50% relapse rate in the next 2-3 years with antidepressants alone 93% maintenance rate if ect chronically administrated
45
46
47

48
49
50
51
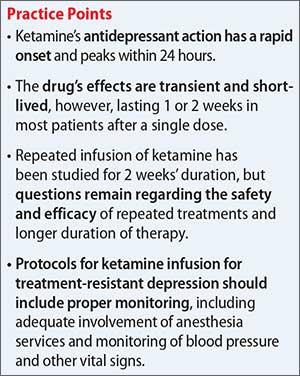
52 Ketamine improves suicidal thoughts in depression Wilkinson ST, et al. Am J Psychiatry. October 5, 2017 Meta-analysis results indicated a single dose of ketamine significantly and quickly improved suicidal ideation. To assess efficacy of a single dose of IV ketamine for suicidal ideation, researchers conducted a systematic review and individual participant data meta-analysis Studies used either saline or midazolam as a control treatment. At baseline, participants had a mean Montgomery-Åsberg Depression Rating Scale (MADRS) score of Analysis showed that within 1 day, ketamine significantly reduced suicidal ideation Effect sizes were moderate to large at all time points after dosing, according to results. Ketamine s effect on suicidal ideation remained significant when adjusting for concurrent changes in depression symptom severity.
53
54
55
56
57
58
59 Patterns of marijuana use among psychiatry patients with depression and its impact on recovery. J Affect Disord. March 2017;312: Six-month recovery trajectories showed that marijuana use was significantly associated with worse recovery for depression symptoms (P = <.001) and anxiety symptoms (P =.025), and mental health functioning (P =.010) compared with patients not using marijuana. No significant differences in symptoms or mental health functioning outcomes (P's >.05) were found between patients who reported recreational or medicinal marijuana use Other research: Association between cannabis use (particularly frequent use) and the development of psychoses, including schizophrenia (substantial evidence). Increased suicidality and symptoms in Bipolar disorder.
60 How to short circuit depression resistance Use adjunctive behavioral and cognitive strategies from the start, even if book or internet based: Behavioral activation framework Antidepressant skills workbook (free online resource): slant towards employment and staying employed Exercise daily Whole foods diet/ Mediterranean: Viva L Italia!!! Keep abreast of employment-work friends, developments, relationships
61 Psychological Treatments for Acute Treatment of MDD Recommendation 1 st LINE 1 st LINE 1 st LINE 2 nd LINE 2 nd LINE 2 nd LINE 2 nd LINE 2 nd LINE 2 nd LINE 3 rd LINE 3 rd LINE 3 rd LINE 3 rd LINE Psychological Treatment Level of Evidence Cognitive-behavioural therapy (CBT) 1 Interpersonal therapy (IPT) 1 Behavioural activation (BA) 1 Mindfulness-based cognitive therapy (MBCT) 2 Cognitive-behavioural analysis system of psychotherapy (CBASP) 2 Problem-solving therapy (PST) 2 Short-term psychodynamic psychotherapy (STPP) 2 Telephone-delivered CBT, IPT 2 Internet- and computer-assisted therapy 2 Long-term psychodynamic psychotherapy (PDT) 3 Acceptance and commitment therapy (ACT) 3 Videoconferenced psychotherapy 3 Motivational interviewing (MI) 4 SECTION 2 - Psychological Treatments Parikh, S., et al., Can J Psychiatry 2016;61(9):524-39
62
63


64 Site Password:
65 Preventing resistance:
66 Basics of avoiding or dealing with resistance Compliance measurement or repeated questioning (25% of resistant depression due to this) Comorbid drugs, THC, alcohol use: even 2-3 drinks/weekly can create resistance Comprehensive labs: including iron studies, testosterone, a.m. cortisol, ferritin, transferrin binding, thyroid studies, and the regular culprits Rule out bipolar illness Rule out borderline, dependent, and narcissistic personalities Role of stress, work problems, secondary gain Comorbid diagnoses, especially generalized anxiety disorder The use of low dose benzos and/or sleep agents temporarily early on appears to effectively combat much resistance and aid compliance Vital role for atypicals as augmentation strategies
Psychiatry curbside: Answers to a primary care doctor s top mental health questions
 Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Psychiatry curbside: Answers to a primary care doctor s top mental health questions April 27, 2018 Laurel Ralston, DO Psychiatrist, Taussig Cancer Institute Objectives Review current diagnostic and prescribing
Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University
 Associate Professor, McMaster University") APPROACH TO DEPRESSION IN PRIMARY CARE Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University DISCLOSURE Speaker/Presenter Disclosure
APPROACH TO DEPRESSION IN PRIMARY CARE Family Medicine Forum November 10, 2017 Montreal., Quebec. Jon Davine, CCFP, FRCP(C) Associate Professor, McMaster University DISCLOSURE Speaker/Presenter Disclosure
Diagnosis & Management of Major Depression: A Review of What s Old and New. Cerrone Cohen, MD
 Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Diagnosis & Management of Major Depression: A Review of What s Old and New Cerrone Cohen, MD Why You re Treating So Much Mental Health 59% of Psychiatrists Are Over the Age of 55 AAMC 2014 Physician specialty
Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Disclosure Information
 Disclosure Information I have no financial relationships to disclose. I will discuss the off label use of several depression and anxiety medications in pediatric population Pediatric Depression & Anxiety
Disclosure Information I have no financial relationships to disclose. I will discuss the off label use of several depression and anxiety medications in pediatric population Pediatric Depression & Anxiety
9/20/2011. Integrated Care for Depression & Anxiety: Psychotropic Medication Management for PCPs. Presentation is Being Recorded
 Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Integrated Care for Depression & Anxiety Psychotropic Medication Management for Primary Care Providers Los Angeles County Department of Mental Health September 20, 2011 Presentation is Being Recorded Please
Depression & Anxiety in Adolescents
 Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Depression & Anxiety in Adolescents Objectives 1) Review diagnosis of anxiety and depression in adolescents 2) Provide overview of evidence-based treatment options 3) Increase provider comfort level with
Adult Depression - Clinical Practice Guideline
 1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
1 Adult Depression - Clinical Practice Guideline 05/2018 Diagnosis and Screening Diagnostic criteria o Please refer to Attachment A Screening o The United States Preventative Services Task Force (USPSTF)
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression
 Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Where to from Here? Evidence-Based Strategies for Treatment of Refractory Depression Michael D. Jibson, MD, PhD Professor of Psychiatry University of Michigan Major Depression #1 WHO cause of disability
Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School
 Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School of Psychology, Fuller Theological Seminary Medical
Daniel Suzuki, MD Adjunct Clinical Associate Professor of Psychiatry, USC Keck School of Medicine Clinical Adjunct Professor/Faculty, Graduate School of Psychology, Fuller Theological Seminary Medical
Objectives. Objectives. A practice review. 02-Nov-16 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS
 MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
MAJOR DEPRESSIVE DISORDER: NEW DEVELOPMENTS AND PRACTICAL IMPLICATIONS Jon-Paul Khoo What is treatment resistance really? Database review 328 consecutive non-remitted MDD patients referred for private
Children s Hospital Of Wisconsin
 Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Children s Hospital Of Wisconsin Co-Management Guidelines To support collaborative care, we have developed guidelines for our community providers to utilize when referring to, and managing patients with,
Psychiatry in Primary Care: What is the Role of Pharmacist?
 Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
Psychiatry in Primary Care: What is the Role of Pharmacist? Benjamin Chavez, PharmD, BCPP, BCACP Clinical Associate Professor Director of Behavioral Health Pharmacy Services January 12, 2019 Disclosure
How to treat depression with medication: Some rules of thumb
 How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
How to treat depression with medication: Some rules of thumb R. Hamish McAllister-Williams, MD, PhD, FRCPsych Reader in Clinical Psychopharmacology Newcastle University Hon. Consultant Psychiatrist Regional
The Pharmacist's Role in Major Depressive Disorder: Optimizing Care. Welcome We will begin shortly.
 The Pharmacist's Role in Major Depressive Disorder: Optimizing Care Welcome We will begin shortly. The Canadian Pharmacists Association is pleased to be partnering with Pfizer to highlight the role of
The Pharmacist's Role in Major Depressive Disorder: Optimizing Care Welcome We will begin shortly. The Canadian Pharmacists Association is pleased to be partnering with Pfizer to highlight the role of
A Brief Overview of Psychiatric Pharmacotherapy. Joel V. Oberstar, M.D. Chief Executive Officer
 A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
A Brief Overview of Psychiatric Pharmacotherapy Joel V. Oberstar, M.D. Chief Executive Officer Disclosures Some medications discussed are not approved by the FDA for use in the population discussed/described.
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Depression in Late Life
 Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Depression in Late Life Robert Madan MD FRCPC Geriatric Psychiatrist Key Learnings Robert Madan MD FRCPC Key Learnings By the end of the session, participants will be able to List the symptoms of depression
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Who Writes Prescriptions for Psychotropic Medications. Biological Psychiatry
 Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient
 Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
Recognizing Depression and Restoring Mood and Well- Being in the Older Patient Andreea L. Seritan, MD UC Davis Mini Medical School February 22, 2014 Objectives Review late life depression symptoms Review
MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE
 MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE Reviewed and Updated by the Behvioral Health Subcommittee 7/20/2017 Topic Purpose Access Assessment 7/2017 Recommendations SummaCare Health Plan bases its Clinical
MAJOR DEPRESSION CLINICAL PRACTICE GUIDELINE Reviewed and Updated by the Behvioral Health Subcommittee 7/20/2017 Topic Purpose Access Assessment 7/2017 Recommendations SummaCare Health Plan bases its Clinical
Quick Guide to Common Antidepressants-Adults
 Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Quick Guide to Common Antidepressants-Adults Medication Therapeutic Range (mg/day) Initial Suggested Serotonin Reuptake Inhibitors (SSRIs) All available as generic FLUOXETINE (Prozac) CITALOPRAM (Celexa
Depression and Anxiety. What is Depression? What is Depression? By Christopher Okiishi, MD Spring Not just being sad A syndrome of symptoms
 Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Depression and Anxiety By Christopher Okiishi, MD Spring 2016 What is Depression? Not just being sad A syndrome of symptoms Depressed mood Sleep disturbance Decreased interest in usual activities (anhedonia)
Joel V. Oberstar, M.D. 1
 Diagnosis and Treatment of Depressive Disorders in Children and Adolescents Joel V. Oberstar, M.D. CEO & Chief Medical Officer Adjunct Assistant Professor of Psychiatry University of Minnesota Medical
Diagnosis and Treatment of Depressive Disorders in Children and Adolescents Joel V. Oberstar, M.D. CEO & Chief Medical Officer Adjunct Assistant Professor of Psychiatry University of Minnesota Medical
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
Treatment-resistant depression in primary care
 Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
Treatment-resistant depression in primary care Interprofessional CME, October 2017 Brian J. Mickey, MD, PhD Associate Professor School of Medicine Department of Psychiatry Disclosures Speakers bureau:
Consultant Pharmacist Approach to Major Depressive Disorder
 Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO
 Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Consultant Pharmacist Approach to Major Depressive Disorder ALAN OBRINGER RPH, CPH, CGP PRESIDENT/OWNER GUARDIAN PHARMACY OF ORLANDO Objectives What is Depression? Discuss the epidemiology of depression
Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association
 Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association Our clinical advisor adds updated advice on electroconvulsive therapy, transcranial magnetic
Practice Guideline for the Treatment of Patients With Major Depressive Disorder: American Psychiatric Association Our clinical advisor adds updated advice on electroconvulsive therapy, transcranial magnetic
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Depression. University of Illinois at Chicago College of Nursing
 Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
Depression University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this session, participants will be better able to: 1. Recognize depression, its symptoms and behaviors
New Patient Questionnaire
 4 Embarcadero Center, Suite 1400, San Francisco, CA 94111 (415) 926-7774 phone; (415) 591-7760 office@sanfranciscopsych.com New Patient Questionnaire Thank you for trusting San Francisco Psychiatry with
4 Embarcadero Center, Suite 1400, San Francisco, CA 94111 (415) 926-7774 phone; (415) 591-7760 office@sanfranciscopsych.com New Patient Questionnaire Thank you for trusting San Francisco Psychiatry with
Treatment of Depression in the Primary Care Office
 Treatment of Depression in the Primary Care Office Paul E.A. Glaser, MD, PhD Departments of Psychiatry, Pediatrics and Anatomy & Neurobiology University of Kentucky November 5, 2010 Disclosures of Potential
Treatment of Depression in the Primary Care Office Paul E.A. Glaser, MD, PhD Departments of Psychiatry, Pediatrics and Anatomy & Neurobiology University of Kentucky November 5, 2010 Disclosures of Potential
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 6. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
MEDICATION ALGORITHM FOR ANXIETY DISORDERS
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences MEDICATION ALGORITHM FOR ANXIETY DISORDERS RYAN KIMMEL, MD MEDICAL DIRECTOR HOSPITAL PSYCHIATRY UNIVERSITY OF WASHINGTON
Treatment of Major Depressive Disorder
 Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
Treatment of Major Depressive Disorder Sarah Mullowney, MD PGY3 Psychiatry Resident, University of Utah Paula Gibbs, MD Medical Director of 5 West at UUMC Clerkship Director MS III Psychiatric Rotation
Augmentation and Combination Strategies in Antidepressants treatment of Depression
 Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Augmentation and Combination Strategies in Antidepressants treatment of Depression Byung-Joo Ham, M.D. Department of Psychiatry Korea University College of Medicine Background The response rates reported
Child & Adolescent Psychiatry (a brief overview)
") Child & Adolescent Psychiatry (a brief overview) Lance Feldman, MD, FAPA, MBA, BSN Vice Chair Clinical Affairs, Department of Psychiatry Affiliate Clinical Assistant Professor, University of South Carolina
Child & Adolescent Psychiatry (a brief overview) Lance Feldman, MD, FAPA, MBA, BSN Vice Chair Clinical Affairs, Department of Psychiatry Affiliate Clinical Assistant Professor, University of South Carolina
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Mixing and Matching: Layering Medications as Family Physicians
 Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
Mixing and Matching: Layering Medications as Family Physicians Family Medicine Forum Vancouver, B.C. November 9-12, 2016. Jon Davine, CCFP, FRCP(C) McMaster University Objectives Discuss different examples
FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD OF ANXIETY
 13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
13 th Pearl Leibovitch Clinical Day November 18th, 2014 Mounir H. Samy, MD, FRCP(C) Associate Professor of Psychiatry McGill University (ret.) FROM MEDICATION TO MINDFULNESS: NEW INSIGHTS INTO THE WORLD
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*
 DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications*") COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
COMMONLY PRESCRIBED PSYCHOTROPIC MEDICATIONS NAME Generic (Trade) DOSAGE KEY CLINICAL INFORMATION Antidepressant Medications* Bupropion (Wellbutrin) Start: IR-100 mg bid X 4d then to 100 mg tid; SR-150
Clinical Update on Management of Depression and Anxiety in the Primary Care Setting. Objectives: Why Is This Important?
 Clinical Update on Management of Depression and Anxiety in the Primary Care Setting Kirstyn Kameg, DNP, PMHNP, BC University Professor PMHNP Program Coordinator Robert Morris University November 4, 2017
Clinical Update on Management of Depression and Anxiety in the Primary Care Setting Kirstyn Kameg, DNP, PMHNP, BC University Professor PMHNP Program Coordinator Robert Morris University November 4, 2017
Treat mood, cognition, and behavioral disturbances associated with psychological disorders. Most are not used recreationally or abused
 Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Psychiatric Drugs Psychiatric Drugs Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally or abused Benzodiazepines
Realities of Depression in Primary Care Setting
 Realities of Depression in Primary Care Setting Jaroslava Salman, MD Department of Supportive Care Medicine Division of Psychiatry Click to edit Master Presentation Date August 4 th 2018 Disclosure I have
Realities of Depression in Primary Care Setting Jaroslava Salman, MD Department of Supportive Care Medicine Division of Psychiatry Click to edit Master Presentation Date August 4 th 2018 Disclosure I have
It is the policy of health plans affiliated with Centene Corporation that Seroquel XR is medically necessary when the following criteria are met:
 Clinical Policy: (Seroquel XR) Reference Number: CP.PMN.64 Effective Date: 12.01.14 Last Review Date: 02.18 Line of Business: Commercial, Health Insurance Marketplace, Medicaid Revision Log See Important
Clinical Policy: (Seroquel XR) Reference Number: CP.PMN.64 Effective Date: 12.01.14 Last Review Date: 02.18 Line of Business: Commercial, Health Insurance Marketplace, Medicaid Revision Log See Important
A Basic Approach to Mood and Anxiety Disorders in the Elderly
 A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
A Basic Approach to Mood and Anxiety Disorders in the Elderly November 1 2013 Sarah Colman MD FRCPC Clinical Fellow, Geriatric Psychiatry Mount Sinai Hospital, University of Toronto Disclosure No conflict
Non-A, non-b=hcv; IFN/RBV; DSM-5/Ham-D, OLT; SSRI, P450
 James A. Bourgeois, O.D., M.D. Vice Chair Clinical Affairs and Director, CL Service University of California San Francisco Non-A, non-b=hcv; IFN/RBV; DSM-5/Ham-D, OLT; SSRI, P450 Localize! Sequence! 1
James A. Bourgeois, O.D., M.D. Vice Chair Clinical Affairs and Director, CL Service University of California San Francisco Non-A, non-b=hcv; IFN/RBV; DSM-5/Ham-D, OLT; SSRI, P450 Localize! Sequence! 1
Depression: Assessment and Treatment For Older Adults
 Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Tool on Depression: Assessment and Treatment For Older Adults Based on: National Guidelines for Seniors Mental Health: the Assessment and Treatment of Depression Available on line: www.ccsmh.ca www.nicenet.ca
Depression major depressive disorder. Some terms: Major Depressive Disorder: Major Depressive Disorder:
 Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Guilt Suicidality. Depression Co-Occurs with Medical Illness The rate of major depression among those with medical illness is significant.
 1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
1-800-PSYCH If you are obsessive-compulsive, dial 1 repeatedly If you are paranoid-delusional, dial 2 and wait, your call is being traced If you are schizophrenic, a little voice will tell you what number
PSYCHIATRIC DRUGS. Mr. D.Raju, M.pharm, Lecturer
 PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
PSYCHIATRIC DRUGS Mr. D.Raju, M.pharm, Lecturer PSYCHIATRIC DRUGS Treat mood, cognition, and behavioral disturbances associated with psychological disorders Psychotropic in nature Most are not used recreationally
Antidepressant Medication Therapy in Primary Care July 25, 2013
 New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
New York State Collaborative Care Initiative Antidepressant Medication Therapy in Primary Care July 25, 2013 http://uwaims.org Presenter Building on 25 years of Research and Practice in Integrated Mental
Managing Late Life Depression
 Managing Late Life Depression Maria I. Lapid, M.D, Professor of Psychiatry Program Director, Geriatric Psychiatry Fellowship Simon Kung, M.D. Associate Professor of Psychiatry Medical Director, Mood Disorders
Managing Late Life Depression Maria I. Lapid, M.D, Professor of Psychiatry Program Director, Geriatric Psychiatry Fellowship Simon Kung, M.D. Associate Professor of Psychiatry Medical Director, Mood Disorders
Department of Psychiatry & Behavioral Sciences. University of Texas Medical Branch
 Depression in Childhood: Advances and Controversies in Treatment Karen Dineen Wagner, MD, PhD Marie B. Gale Centennial Professor & Vice Chair Department of Psychiatry & Behavioral Sciences Director, Division
Depression in Childhood: Advances and Controversies in Treatment Karen Dineen Wagner, MD, PhD Marie B. Gale Centennial Professor & Vice Chair Department of Psychiatry & Behavioral Sciences Director, Division
Major Depressive Disorder (MDD) in Children under Age 6
 in Children under Age 6") in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
in Children under Age 6 Level 0 Comprehensive assessment. Refer to Principles of Practice on page 5. Level 1 Psychotherapeutic intervention (e.g., dyadic therapy) for 6 to 9 months; assessment of parent/guardian
Depression: Identification, Evaluation and Management in Primary Care
 Depression: Identification, Evaluation and Management in Primary Care Primary Care Medicine: Update 2010 Rena K. Fox, M.D. Associate Professor of Clinical Medicine University of California, San Francisco
Depression: Identification, Evaluation and Management in Primary Care Primary Care Medicine: Update 2010 Rena K. Fox, M.D. Associate Professor of Clinical Medicine University of California, San Francisco
Major Depression and Anxiety in Adolescents and Adults
 Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine greenbml@slu.edu *NO DISCLOSURES* OBJECTIVES * Recognize
Major Depression and Anxiety in Adolescents and Adults Miggie Greenberg, M.D. Associate Professor of Psychiatry St. Louis University School of Medicine greenbml@slu.edu *NO DISCLOSURES* OBJECTIVES * Recognize
Medication for Anxiety and Depression. PJ Cowen Department of Psychiatry, University of Oxford
 Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
Medication for Anxiety and Depression PJ Cowen Department of Psychiatry, University of Oxford Topics Medication for anxiety disorders Medication for first line depression treatment Medication for resistant
The Context: Why is this so important to treat?
 Depression for PG1s Ian A. Cook, M.D. UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience & Human Behavior DepressionLA.com PsychiatryGuidelines.com
Depression for PG1s Ian A. Cook, M.D. UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience & Human Behavior DepressionLA.com PsychiatryGuidelines.com
Dr.Rahiminejad Roozbeh Hospital TUMS
 Dr.Rahiminejad Roozbeh Hospital TUMS Psychiatric disorders, particularly depression, anxiety and eating disorders, are prevalent in diabetes. Mental illness increases risk of diabetes and diabetic complications.
Dr.Rahiminejad Roozbeh Hospital TUMS Psychiatric disorders, particularly depression, anxiety and eating disorders, are prevalent in diabetes. Mental illness increases risk of diabetes and diabetic complications.
Focusing on Depression in the Community. Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy
 Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Disclosure and Conflict of Interest Dr. Gable declares no conflicts of interest, real
Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Disclosure and Conflict of Interest Dr. Gable declares no conflicts of interest, real
Partners in Care Quick Reference Cards
 Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
Partners in Care Quick Reference Cards Supported by the Agency for Healthcare Research and Quality MR-1198/8-AHRQ R This project was funded by the Agency for Healthcare Research and Quality (AHRQ), formerly
THE CHOICE D PATIENT AND FAMILY GUIDE TO DEPRESSION TREATMENT
 THE CHOICE D PATIENT AND FAMILY GUIDE TO DEPRESSION TREATMENT PRACTICAL INFORMATION FROM CANMAT AND MDAO THE CHOICE D PATIENT AND FAMILY GUIDE TO DEPRESSION TREATMENT PRACTICAL INFORMATION FROM CANMAT
THE CHOICE D PATIENT AND FAMILY GUIDE TO DEPRESSION TREATMENT PRACTICAL INFORMATION FROM CANMAT AND MDAO THE CHOICE D PATIENT AND FAMILY GUIDE TO DEPRESSION TREATMENT PRACTICAL INFORMATION FROM CANMAT
BRIEF ANTIDEPRESSANT OVERVIEW. Casey Gallimore, Pharm.D., M.S.
 BRIEF ANTIDEPRESSANT OVERVIEW Casey Gallimore, Pharm.D., M.S. Antidepressant Medication Classes First Generation Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Second Generation
BRIEF ANTIDEPRESSANT OVERVIEW Casey Gallimore, Pharm.D., M.S. Antidepressant Medication Classes First Generation Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Second Generation
CHILD & ADOLESCENT PSYCHIATRY ALERTS, VOLUME XIV, 2012 INDEX
 A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
A Adderall Counterfeit, 31 addiction, internet CBT, 55 ADHD Adjunctive Guanfacine, 11 Counterfeit Adderall, 31 Developmental Trajectory and Risk Factors, 5 Dopamine Transporter Alterations, 14 Extended-Release
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D.
 Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Depression: Identification, Evaluation and Management in Primary Care
 Depression: Identification, Evaluation and Management in Primary Care Primary Care Medicine: Update 2012 Rena K. Fox, M.D. Associate Professor of Clinical Medicine University of California, San Francisco
Depression: Identification, Evaluation and Management in Primary Care Primary Care Medicine: Update 2012 Rena K. Fox, M.D. Associate Professor of Clinical Medicine University of California, San Francisco
Mental Health Practice Support
 Initial Screening and Triage for Follow-up HEALTH TEAM Depression is suspected: Perform two-question screen 1,2 (box 1)* Review risk factors 1-3 (box 2) Diagnose and characterize MDE with clinical interview:
Initial Screening and Triage for Follow-up HEALTH TEAM Depression is suspected: Perform two-question screen 1,2 (box 1)* Review risk factors 1-3 (box 2) Diagnose and characterize MDE with clinical interview:
#CHAIR2016. September 16 17, 2016 The Biltmore Hotel Miami, FL. Sponsored by
 #CHAIR2016 September 16 17, 2016 The Biltmore Hotel Miami, FL Sponsored by Depression in Children and Adolescents Karen Dineen Wagner, MD, PhD University of Texas Medical Branch Galveston, TX Karen Dineen
#CHAIR2016 September 16 17, 2016 The Biltmore Hotel Miami, FL Sponsored by Depression in Children and Adolescents Karen Dineen Wagner, MD, PhD University of Texas Medical Branch Galveston, TX Karen Dineen
Depression in adults: treatment and management
 1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
1 2 3 4 Depression in adults: treatment and management 5 6 7 8 Appendix V3: recommendations that have been deleted of changed from 2009 guideline Depression in adults: Appendix V3 1 of 22 1 Recommendations
Depression Workshop 26 January 2007
 Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
%, # Southern Medical Association July / 01/ /7 23 #, 2 3
 Southern Medical Association July 2011 Robert A. Bashford, M.D., Professor Associate Dean for Admissions University of North Carolina Professor of Psychiatry and OB-GYN!" #! $ %&'(%&) $ * &+ %&, ' ) #
Southern Medical Association July 2011 Robert A. Bashford, M.D., Professor Associate Dean for Admissions University of North Carolina Professor of Psychiatry and OB-GYN!" #! $ %&'(%&) $ * &+ %&, ' ) #
Judges Reference Table for the March 2016 Psychotropic Medication Utilization Parameters for Foster Children
 Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Judges Reference Table for the Psychotropic Medication Utilization Parameters for Foster Children Stimulants for treatment of ADHD Preschool (Ages 3-5 years) Child (Ages 6-12 years) Adolescent (Ages 13-17
Disclosures - None. Learning Objectives. Emerging Issues Prevalence of Mood Disorders. Update on Depression-2012
 Disclosures - None Update on Depression-2012 Russell G. Vasile, M. D. Associate Professor of Psychiatry Beth Israel Deaconess Medical Center Harvard Medical School Learning Objectives Understand the spectrum
Disclosures - None Update on Depression-2012 Russell G. Vasile, M. D. Associate Professor of Psychiatry Beth Israel Deaconess Medical Center Harvard Medical School Learning Objectives Understand the spectrum
Illuminating the Black Box: Antidepressants, Youth and Suicide
 Illuminating the Black Box: Antidepressants, Youth and Suicide David H. Rubin, M.D. Executive Director, MGH Psychiatry Academy Director, Postgraduate Medical Education Director, Child and Adolescent Psychiatry
Illuminating the Black Box: Antidepressants, Youth and Suicide David H. Rubin, M.D. Executive Director, MGH Psychiatry Academy Director, Postgraduate Medical Education Director, Child and Adolescent Psychiatry
The Context: Why is this so important to treat?
 ER Management of Depression for PGY1s Ian A. Cook, M.D. Director, UCLA Depression Research Program UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience
ER Management of Depression for PGY1s Ian A. Cook, M.D. Director, UCLA Depression Research Program UCLA Department of Psychiatry Laboratory of Brain, Behavior, and Pharmacology Semel Institute for Neuroscience
Pharmacy Technician Objectives. Pharmacist Objectives. Pre-Test Question 2. Pre-Test Question 1 9/27/2016. Disclosure and Conflict of Interest
 Disclosure and Conflict of Interest Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Dr. Gable declares no conflicts of interest, real
Disclosure and Conflict of Interest Focusing on Depression in the Community Kelly N. Gable, Pharm.D., BCPP Associate Professor SIUE School of Pharmacy Dr. Gable declares no conflicts of interest, real
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist
 and Glutamate (NMDA) Receptor Antagonist") Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Dementia Medications Acetylcholinesterase Inhibitors (AChEIs) and Glutamate (NMDA) Receptor Antagonist Medication Dosage Indication for Use Aricept (donepezil) Exelon (rivastigmine) 5mg 23mg* ODT 5mg Solution
Manual of Clinical Psychopharmacology
 Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Manual of Clinical Psychopharmacology Fourth Edition Alan F. Schatzberg, M.D. Kenneth T. Norris, Jr., Professor and Chairman, Department of Psychiatry and Behavioral Sciences, Stanford University School
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Steps for Initiating Electroconvulsive Therapy Treatment
 Steps for Initiating Electroconvulsive Therapy Treatment PSYCHIATRISTS CAN REFER PATIENTS FOR ECT TREATMENT AT EL CAMINO HOSPITAL BY CALLING THE ECT NURSE COORDINATOR AT 650-962-5795. Once the referral
Steps for Initiating Electroconvulsive Therapy Treatment PSYCHIATRISTS CAN REFER PATIENTS FOR ECT TREATMENT AT EL CAMINO HOSPITAL BY CALLING THE ECT NURSE COORDINATOR AT 650-962-5795. Once the referral
Review of Psychotrophic Medications. (An approved North Carolina Division of Health Services Regulation Continuing Education Course)
") Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Review of Psychotrophic Medications (An approved North Carolina Division of Health Services Regulation Continuing Education Course) Common Psychiatric Disorders *Schizophrenia *Depression *Bipolar Disorder
Disclosures. Learning Objectives. Psychopharmacology of Pediatric Anxiety and Depression 5/4/2017
 Psychopharmacology of Pediatric Anxiety and Depression Susan Sharp, DO Clinical Assistant Professor of Child and Adolescent Psychiatry Kansas University Medical Center The Children's Mercy Hospital, 2017
Psychopharmacology of Pediatric Anxiety and Depression Susan Sharp, DO Clinical Assistant Professor of Child and Adolescent Psychiatry Kansas University Medical Center The Children's Mercy Hospital, 2017
Summary of guideline for the. treatment of depression RANZCP CLINICAL PRACTICE GUIDELINES ASSESSMENT
 RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
Depression. There are several forms of depression (depressive disorders). Major depressive disorder and dysthymic disorder are the most common.
. Major depressive disorder and dysthymic disorder are the most common.") Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Diabetes and Depression. Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C
 Diabetes and Depression Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C 2008 Learning Objectives State the risk factors for depression Identify the vulnerability
Diabetes and Depression Roshini Pinto-Powell, MD Stephen Noyes, LICSW, LADC William Gunn, PhD Beverly Bean, RN, C 2008 Learning Objectives State the risk factors for depression Identify the vulnerability
The Latest in Treating Depression and Anxiety in Primary Care
 The Latest in Treating Depression and Anxiety in Primary Care Wendy L. Wright MS, ANP-BC, FNP-BC, FAANP, FAAN, FNAP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare @ Amherst
The Latest in Treating Depression and Anxiety in Primary Care Wendy L. Wright MS, ANP-BC, FNP-BC, FAANP, FAAN, FNAP Adult/Family Nurse Practitioner Owner Wright & Associates Family Healthcare @ Amherst
Management of SSRI Induced Sexual Dysfunction. Serotonin Reuptake Inhibitors*
 Management of SSRI Induced Sexual Dysfunction John J. Miller, M.D. Medical Director, Center for Health and WellBeing Exeter, NH Serotonin Reuptake Inhibitors* fluoxetine clomipramine sertraline paroxetine
Management of SSRI Induced Sexual Dysfunction John J. Miller, M.D. Medical Director, Center for Health and WellBeing Exeter, NH Serotonin Reuptake Inhibitors* fluoxetine clomipramine sertraline paroxetine
Depression: Identification, Evaluation and Management in Primary Care
 Depression: Identification, Evaluation and Management in Primary Care Primary Care Update: 2013 I have nothing to disclose Rena K. Fox, M.D. Associate Professor of Clinical Medicine University of California,
Depression: Identification, Evaluation and Management in Primary Care Primary Care Update: 2013 I have nothing to disclose Rena K. Fox, M.D. Associate Professor of Clinical Medicine University of California,
Setting ambitious goals for patients with depression with a focus on functional recovery
 Setting ambitious goals for patients with depression with a focus on functional recovery The role of the overlooked cognitive symptoms in the treatment of depression Dr Andreas Papadopoulos Locum Consultant
Setting ambitious goals for patients with depression with a focus on functional recovery The role of the overlooked cognitive symptoms in the treatment of depression Dr Andreas Papadopoulos Locum Consultant
Professional Practice Minutes September 7 th, 2016
 Professional Practice Minutes September 7 th, 2016 1. Lung Cancer Screening : Fast Facts Number 1 killer of both men and women in the US (The Global Burden of Cancer 2013) More people die from lung cancer
Professional Practice Minutes September 7 th, 2016 1. Lung Cancer Screening : Fast Facts Number 1 killer of both men and women in the US (The Global Burden of Cancer 2013) More people die from lung cancer
CANMAT Guidelines. *Co-first authors.
 Canadian Psychiatric Association CANMAT Guidelines Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section
Canadian Psychiatric Association CANMAT Guidelines Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section
Medication management of anxiety & depression. Dr Katie Simpson GP Mental health lead East Berks CCG
 Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
Medication management of anxiety & depression Dr Katie impson GP Mental health lead East Berks CCG NICE guidelines for Anxiety tepped Care RIs and NRIs in Anxiety disorders RI ertraline Citalopram Fluoxetine
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES
 PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
Depression: A Darker Shade of Blue. CareOregon Pharmacy
 Depression: A Darker Shade of Blue CareOregon Pharmacy Today s Agenda Welcome and Introduction 8:00 Clinical & In Real Life Aspects 8:05 Break 9:15 Medication Review 9:30 Questions 10:30 Closing 10:55
Depression: A Darker Shade of Blue CareOregon Pharmacy Today s Agenda Welcome and Introduction 8:00 Clinical & In Real Life Aspects 8:05 Break 9:15 Medication Review 9:30 Questions 10:30 Closing 10:55
Schedule FDA & literature based indications
 Psychotropic Medication List Recommended dosages are intended to serve only as a guide for children. Recommended doses are literature based. Clinicians should consult package insert of medications for
Psychotropic Medication List Recommended dosages are intended to serve only as a guide for children. Recommended doses are literature based. Clinicians should consult package insert of medications for