DEPRESSION IN CHILDHOOD AND ADOLECENCE
|
|
|
- Nathaniel Greene
- 6 years ago
- Views:
Transcription

1 DEPRESSION IN CHILDHOOD AND ADOLECENCE Bob Salo
2 Mood Disorders Childhood Depression Major Depressive Disorder Disruptive Mood Dysregulation Disorder Bipolar Affective Disorder Mainly Depressive Mainly Hypomanic Mixed Mood Disorders complicating other psychiatric disorders
3 Depression PREVALENCE OF MAJOR DEPRESSION 2% of children 5-8% of adolescents Upto 15% of adolescents have mood disorders: (dysthymia, Depressive Disorder, Depressive adjustment disorder)
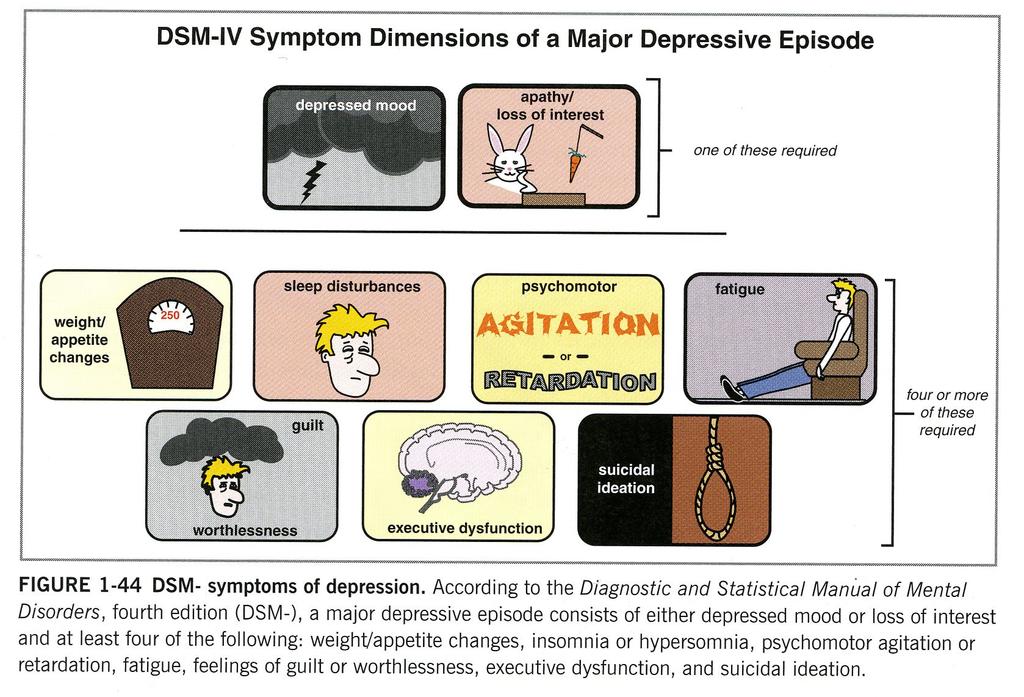
4 Depression Depressed mood, or irritable mood every day Diminished interest in play, work, activities which usually afford pleasure or interest, apathy Diminished ability to concentrate, indecisiveness, clinginess Weight loss or gain, or failure to grow because of diminished food intake. Insomnia or hypersomnia Agitation or retardation of activity levels Feelings of worthlessness, guilt or hopelessness Recurrent thoughts of death or dying, or recurrent suicidal thoughts.
5
6 Depressive Disorders DSM5 Field Trials - Diagnostic Reliability Mixed Anxiety-depressive Disorder Colorado Unacceptable Stanford Unacceptable Pooled Unacceptable Major Depressive Disorder Colorado Questionable Stanford Questionable Pooled Questionable
7
8
9
10
11 Depression Differences between Children and Adolescents Younger children unable accurately to describe their inner mental states Irritability common Somatic symptoms common Reduced weight gain rather than weight loss
12 Clinical Signs and Symptoms of Child vs Adolescent Depression Signs and Symptoms Child Adolescent Anhedonia Hopelessness Sleep Weight /- - Appearance Somatic Complaints Fears and Worries Suicide Ryan et al. (1987) and Rosenberg et al (1992, 1994)
13 Genetics and Depressive Disorders Twin studies: MZ : DZ = 4:1 Twin studies suggest that Genetic effect = 60% of variance Family studies Familial aggregation Heritability =30-40% Environmental influences important Depression is a complex disorder Consistency of findings
14 Depression: Risks Upto age 10: After age 10: Females = Males Females > Males More 1st and 2nd degree relatives have depression Risk of depression before 18: 1 Depressed Parent = 2x risk. 2 Depressed Parents = 4x risk Males whose fathers die, before the age of 13, are more likely to develop depression
15 Depression and Temperament Characteristic ways of interacting with the world which is moulded by both genetically transmitted traits and interactions with the environment that begin at birth or before and may influence the development of depression in the following ways Direct Indirect Mediate the role of factors such as stress Moderate the role of temperament (related to coping styles)
16 Depression and Temperament Vulnerability - temperament places the individual at risk of a disorder Pathoplastic - temperament shapes the course of the disorder Scarring - experience of a disorder changes personality and increases vulnerability Spectrum disorder is endpoint of a trait expression
17 Depression High Hormonal levels Cortisol, Dehydroepiandosterone Increase in rates of depression after puberty Rate increases more rapidly mid puberty Higher rates in females than males
18 Depression Environmental Stresses Attachment General Family functioning Conflict Losses and Life Events Adolescence Gender socialisation
19
20 Depression Suicide: 3rd leading cause of death in adolescents Suicide and suicidal ideation frequent in depressed adolescents Males more at risk.
21 Individual Predisposition Alcohol abuse Depression Character Disorder -aggressive/impulsive -perfectionistic/rigid Proximate (Trigger) Stress Event Altered state of mind (hopelessness; fear/dread, rage etc) Opportunity: available method, privacy etc Social Milieu High or Low community rates Taboos Media Display Inhibit or facilitate SUICIDE Case finding and treatment Hotlines Firearm education Preventions Media Guidance Enhance Taboos
22 Age Specific Suicide Rates 2010 Males 13.4 per 100,000 Females 5.2 per 100,000

23 Age Specific Suicide Rates: 2010
24 Suicide rates by State/Territory Deaths Standardised death rate (per 100,000) State Males FemalesPersons New South Wales Victoria Queensland South Australia Western Australia Tasmania Northern Territory Australian Capital Territory Total 1, ,
25 Assessing Risk
26 4 Rs Recognising the signs Raising the issue Risk Assessment Responding
27 Establish Rapport Non Judgmental Unhurried Active listening Confidentiality issues Individual Assessment Family involvement Make some positive comments
28 Depression Self harm Substance abuse Recent Loss Recognising the signs: Antisocial Aggressive behaviour possession of a firearm. Antecedents
29 Numerous Accidents Recognising the signs: Behaviours Dangerous Risky Behaviours Morbid thoughts Giving away favoured possessions
30 Other Risk Factors Psychiatric disorders Poor social adjustment Physical health problems Family and Environmental Factors
31 Raising the issue Ask directly about suicidal, self harming thoughts Talk to the young person alone Do not swear secrecy
32 Factors that impede disclosure Clinician not prepared Anxiety / fear about mismanagement Anger with repeated self harmers Denial of possibility of suicide because of personal views
33 Depression >17% of adolescents with depression present with substance abuse Somatic complaints are common Behaviour problems, grouchiness, aggression are common Social withdrawal, school difficulties Neglect of personal hygiene Increased emotionality and sensitivity to feelings of rejection Depressive Delusions and Hallucinations uncommon (rare before puberty)
34 Assessing Suicide Risk : 1 1. Have you been feeling depressed for several days at a time? 2. When you feel this way, have you ever had thoughts of killing yourself? 3. When did these thoughts occur? 4. What did you think you might do to yourself? 5. Did you act on these thoughts in any way? 6. How often do these thoughts occur? 7. When was the last time you had these thoughts?
35 Assessing Suicide Risk : 2 8. Have your thoughts ever included harming someone else as well as yourself? 9. Recently, what specifically have you thought about doing to yourself? 10. Have you taken any steps towards doing this? (e.g., getting pills / buying a gun) 11. Have you thought about when and where you would do this? 12. Have you made any plans for your possessions or left any instructions for people for after your death, such as a note or a will?
36 Assessing Suicide Risk : Have you thought about the effect your death would have upon your family or friends? 14. What has stopped you from acting on your thoughts so far? 15. What are your thoughts about staying alive? 16. What help could make it easier for you to cope with your problems at the moment? 17. How does talking about all this make you feel?
37 Attempted Suicide Risk Factors Male gender Poor Communication History of Previous Attempts Depressive Symptoms Sense of Hopelessness Persistent Suicidal Ideation
38 Suicide and Attempted Suicide Psychopathology: psychiatric disorder common amongst suicides High rates of behaviour disorder High rates of Substance abuse especially amongst males Parent - Adolescent Communication less good in suicides
39 Attempted Suicide Suicidal ideation : 27% thought of suicide in the last 12 mths; (ages 14-17) Lethal Intent: 16% had made a plan; 8% had made an attempt; 2% an attempt which required medical attention 70% certainly survivable, 26% lethal potential 4% death a distinct possibility Females more likely to attempt suicide than males ( but less so as ascertained by community samples) Low SES associated with suicide attempts
40 F:M = 6:1 Attempted Suicide Usually only return for a few sessions therefore brief intervention strategies are important Cognitive problem solving strategies Identify potentially stressful situations Improve family communications and support, reduce conflictual situations
41 Attempted Suicide Attempters : low rates of affective disorders, high rates of Disruptive disorders, and substances abuse Cognitive Factors: Outcome: sense of hopelessness; poor problem solving strategies, negative attributional style, impulsive style 50% will repeat attempts within the first 2 yr... 10% (approx.)will complete suicide
42 DEVELOPING A MANAGEMENT PLAN 1. Establish a Therapeutic Alliance 2. Be systematic in your assessment 3. Where feasible, remove all obvious means of self harm. 4. Ensure appropriate supervision for the individual 5. Ensure immediate 24 hour access to suitable clinical care 6. Where feasible, neutralise the precipitating problem 7. Try to make a contract to keep themselves safe 8. Try to delay the individuals suicidal impulses: offer strategies 9. Identify supportive people or services who can be contacted 10. Engage in ongoing consultation with colleagues
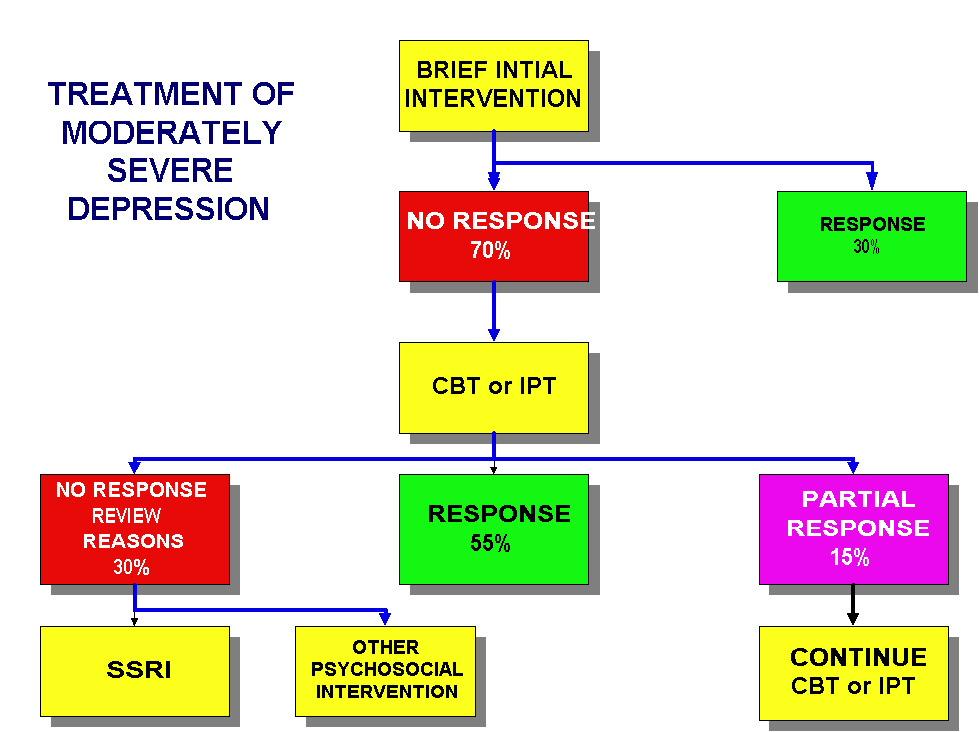
43 Treatment Options
44 Treatment Options Empathic listening, monitoring. Psychotherapy: CBT, IPT, Psychodynamic, other psychotherapies Antidepressants Referral Education Liaison Coordination of ongoing care
45
46 Evidence bases: Psychological Interventions INTERVENTION STRENGTH OF RECOMMENDATION QUALITY OF EVIDENCE COGNITVE BEHAVIOURAL THERAPY B+ INTERPERSONAL THERAPY B- FAMILY THERAPY B
47 Mild Depression Listen Are there any high risk factors Watch and Wait Review
48 Moderate Depression Assessment risk of self harm Assessment of protective factors Assessment of severity of depression and co-morbidities If low risk: Assess severity and risk Provide Client & Carer education Develop safety plan Develop treatment plan Inform about treatment options Inform about medication risks and side effects and benefits Establish a review and emergency procedure & educate what to look for. If psychological support initiated, if after 6-8 weeks no improvement consider adding antidepressant
49 Severe Depression Actively suicidal Psychotic features Requires immediate admission Consider CAT assessment if not willing to go to hospital with a view to involuntary admission
50 Referral Actively suicidal Depression Severe Psychotic Symptoms Bipolar disorder Worsening despite treatment No response to treatment after 2-3 weeks
51 Other Options CBT, IPT Psychotherapy etc Refining Antidepressant therapy Phototherapy Hospitalisation ECT
52 Treatments Unipolar: Bipolar:» Antidepressants» CBT» Antidepressants,» Mood Stabilisers,» CBT, Psychotherapy» ECT
53 Antidepressants SSRIs preferably because of lower cardiotoxicity esp. in overdose All SSRIs carry a Black Box warning at least weekly supervision required for the first six weeks Fluoxetine has the strongest evidence base Adverse effects are not uncommon Lack of response: increase dose Lack of response to increased dose change to another SSRI If medication effective then treatment should continue for at least 12 months
54
55
56 Adverse Effects Increase in suicidality; actual suicide rates are reduced by antidepressants Agitation Nausea, gastric irritation. Weight gain Sedation Serotonergic Syndrome esp. in overdose
57 Response to Antidepressants 30-50% will respond to first antidepressant If there are residual symptoms then relapse is high Of those that do not respond to the first antidepressant about 30-50% will respond to a second antidepressant. After four trials of antidepressants only ⅔ will have responded Response rates can be increased by including psychotherapy CBT or IPT Psychotherapy reduces relapse rates
58 Disruptive Mood Dysregulation Disorder Diagnostic criteria The four criteria listed below should be met: Severe, recurrent, disproportionate temper outbursts On average, three or more times per week. Temper outbursts are inconsistent with developmental level. Between outbursts, mood is persistently irritable or angry, most of the day and nearly every day.
59 Disruptive Mood Dysregulation Disorder POSITIVE CONDITIONS Onset of symptoms must be before age 10 Symptoms must have been present for 12 or more months Symptoms must not be absent for three or more consecutive months Children must be between 6 and 18 years of age Symptoms should be present in at least two of three settings (home, school, social situations) and are severe in at least one setting NEGATIVE CONDITIONS Symptoms are not better explained by another mental disorder e.g. ODD, CD, ADHD. Symptoms are not the manifestation of a substance or medical condition Full symptom criteria for manic/hypomanic episode have not been met for more than one day Behaviours do not occur solely during an episode of major depressive disorder
60 Disruptive Mood Dysregulation Disorder DSM5 Field Trials : Site reliability of diagnosis Baystate Colorado Columbia Unacceptable Good Unacceptable Pooled Questionable
Screening for Depression and Suicide
 Screening for Depression and Suicide Christa Smith, PsyD Western Interstate Commission for Higher Education Boulder, Colorado 10/2/2008 Background My background A word about language Today stopics Why
Screening for Depression and Suicide Christa Smith, PsyD Western Interstate Commission for Higher Education Boulder, Colorado 10/2/2008 Background My background A word about language Today stopics Why
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School
 More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School Keep in Mind In the U.S., approximately 10-15% of children/adolescents
More Than Just Moody Blaise Aguirre, MD Child and Adolescent Psychiatrist McLean Hospital Assistant Professor of Psychiatry Harvard Medical School Keep in Mind In the U.S., approximately 10-15% of children/adolescents
Depression in the Eldery Handout Package
 Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression in the Eldery Handout Package Depression in the Elderly 1 Learning Objectives Upon completion of this module, you should be able to: 1. State the prevalence and describe the consequences of
Depression and Bipolar Disorder
 The Canadian Mental Health Association (CMHA) is a nation-wide, charitable organization that promotes the mental health of all and supports the resilience and recovery of people experiencing mental illness.
The Canadian Mental Health Association (CMHA) is a nation-wide, charitable organization that promotes the mental health of all and supports the resilience and recovery of people experiencing mental illness.
Safeguarding Our Youth Parent Information Night
 Safeguarding Our Youth Parent Information Night SEPTEMBER 14, 2016 PRESENTED BY DCC MIDDLE SCHOOL COUNSELORS JESS HALL, KRISTIN JARAMILLO, AND JENNIFER SCOTT Tonight s Agenda Welcome and introductions
Safeguarding Our Youth Parent Information Night SEPTEMBER 14, 2016 PRESENTED BY DCC MIDDLE SCHOOL COUNSELORS JESS HALL, KRISTIN JARAMILLO, AND JENNIFER SCOTT Tonight s Agenda Welcome and introductions
Session outline. Introduction to depression Assessment of depression Management of depression Follow-up Review
 Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
DSM5: How to Understand It and How to Help
 DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
DSM5: How to Understand It and How to Help Introduction: The DSM5 is a foreign language! Three Questions: I. The first was, What the key assumptions made to determine the organization of the DSM5? A. Mental
Depression: what you should know
 Depression: what you should know If you think you, or someone you know, might be suffering from depression, read on. What is depression? Depression is an illness characterized by persistent sadness and
Depression: what you should know If you think you, or someone you know, might be suffering from depression, read on. What is depression? Depression is an illness characterized by persistent sadness and
Depression Workshop 26 January 2007
 Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Depression Workshop 26 January 2007 Leslie G Walker Professor of Cancer Rehabilitation Donald M Sharp Senior Lecturer in Behavioural Oncology Mary B Walker Senior Clinical and Research Nurse Specialist
Reading the Signs. Risk Factors and Warning Signs for Suicide
 Reading the Signs Risk Factors and Warning Signs for Suicide 14.7.14 Welcome Jennifer Fisher headspace School Support Consultant jfisher@headspace.org.au 0447 001 612 Anxiety Warren Jones headspace Nowra
Reading the Signs Risk Factors and Warning Signs for Suicide 14.7.14 Welcome Jennifer Fisher headspace School Support Consultant jfisher@headspace.org.au 0447 001 612 Anxiety Warren Jones headspace Nowra
Suicide Risk Factors
 Suicide Prevention Suicide Risk Factors Mental Health disorders, in particular: o Depression or bipolar (manic-depressive) disorder o Alcohol or substance abuse or dependence o Schizophrenia o Post Traumatic
Suicide Prevention Suicide Risk Factors Mental Health disorders, in particular: o Depression or bipolar (manic-depressive) disorder o Alcohol or substance abuse or dependence o Schizophrenia o Post Traumatic
PSYCH 235 Introduction to Abnormal Psychology. Agenda/Overview. Mood Disorders. Chapter 11 Mood/Bipolar and Related disorders & Suicide
 PSYCH 235 Introduction to Abnormal Psychology Chapter 11 Mood/Bipolar and Related disorders & Suicide 1 Agenda/Overview Mood disorders Major depression Persistent Depressive Disorder (Dysthymia) Bipolar
PSYCH 235 Introduction to Abnormal Psychology Chapter 11 Mood/Bipolar and Related disorders & Suicide 1 Agenda/Overview Mood disorders Major depression Persistent Depressive Disorder (Dysthymia) Bipolar
Suicide Prevention in the Older Adult
 Suicide Prevention in the Older Adult Nina R. Ferrell, MA Geriatric Outreach Professional Relations Salt Lake Behavioral Health Hospital Presentation Content Credits 1. Addressing Suicidal Thoughts and
Suicide Prevention in the Older Adult Nina R. Ferrell, MA Geriatric Outreach Professional Relations Salt Lake Behavioral Health Hospital Presentation Content Credits 1. Addressing Suicidal Thoughts and
UPMC SAFE-T Training Adapted for Pediatric Primary Care. Sheri L. Goldstrohm, Ph.D.
 UPMC SAFE-T Training Adapted for Pediatric Primary Care Sheri L. Goldstrohm, Ph.D. Prevalence of Suicide in the U.S. 10th most frequent cause of death for all ages 2nd leading cause of death for individuals
UPMC SAFE-T Training Adapted for Pediatric Primary Care Sheri L. Goldstrohm, Ph.D. Prevalence of Suicide in the U.S. 10th most frequent cause of death for all ages 2nd leading cause of death for individuals
Suicide Awareness & Prevention The Silent Epidemic Kristin A. Drake Cell:
 Suicide Awareness & Prevention The Silent Epidemic Kristin A. Drake Cell: 915 525 8937 What is Suicidality? ~According to Dr. Osvaldo Gaytan, Child and Adolescent Psychiatrist for El Paso Behavioral, Suicidality
Suicide Awareness & Prevention The Silent Epidemic Kristin A. Drake Cell: 915 525 8937 What is Suicidality? ~According to Dr. Osvaldo Gaytan, Child and Adolescent Psychiatrist for El Paso Behavioral, Suicidality
Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders
 Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Page 1 Extremes in Normal Mood Chapter 6 Mood Disorders and Suicide An Overview of Mood Disorders Nature of depression Nature of mania and hypomania Types of DSM-IV Depressive Disorders Major depressive
Suicide: Starting the Conversation. Jennifer Savner Levinson Bonnie Swade SASS MO-KAN Suicide Awareness Survivors Support
 Suicide: Starting the Conversation Jennifer Savner Levinson Bonnie Swade SASS MO-KAN Suicide Awareness Survivors Support What We Do Know About Suicide Suicidal thoughts are common. Suicidal acts, threats
Suicide: Starting the Conversation Jennifer Savner Levinson Bonnie Swade SASS MO-KAN Suicide Awareness Survivors Support What We Do Know About Suicide Suicidal thoughts are common. Suicidal acts, threats
4. Definition, clinical diagnosis and diagnostic criteria
 4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
4. Definition, clinical diagnosis and diagnostic criteria 4.1. Definition Major depression is a mood disorder consisting of a set of symptoms, which include a predominance of the affective type (pathological
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Major Depressive Disorder. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Major Depressive Disorder. These podcasts are designed to give medical students an overview of key topics in pediatrics.
A basic approach to a suicidal patient
 A basic approach to a suicidal patient With Dr Joanne Ferguson, Staff Specialist Psychiatry and Addiction Medicine, Royal Prince Alfred Hospital Introduction Talking about suicide is regarded as one of
A basic approach to a suicidal patient With Dr Joanne Ferguson, Staff Specialist Psychiatry and Addiction Medicine, Royal Prince Alfred Hospital Introduction Talking about suicide is regarded as one of
Treating Childhood Depression in Pediatrics. Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences
 Treating Childhood Depression in Pediatrics Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences Objectives The learner will: Describe the signs and symptoms of childhood
Treating Childhood Depression in Pediatrics Martha U. Barnard, Ph.D. University of Kansas Medical Center Pediatrics/Behavioral Sciences Objectives The learner will: Describe the signs and symptoms of childhood
Depression. Content. Depression is common. Depression Facts. Depression kills. Depression attacks young people
 Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Content Depression Dr. Anna Lam Associate Consultant Department of Psychiatry, Queen Mary Hospital Honorary Clinical Assistant Professor Li Ka Shing Faculty of Medicine, The University of Hong Kong 1.
Youth Depression & Suicide
 Youth Depression & Suicide Hatim Omar, M.D. Professor, Pediatrics & Ob\Gyn. Chief, Division of Adolescent Medicine & Young Parent Program Department of Pediatrics University of Kentucky Email: haomar2@uky.edu
Youth Depression & Suicide Hatim Omar, M.D. Professor, Pediatrics & Ob\Gyn. Chief, Division of Adolescent Medicine & Young Parent Program Department of Pediatrics University of Kentucky Email: haomar2@uky.edu
Your journal: how can it help you?
 Journal Your journal: how can it help you? By monitoring your mood along with other symptoms like sleep, you and your treatment team will be better able to follow the evolution of your symptoms and therefore
Journal Your journal: how can it help you? By monitoring your mood along with other symptoms like sleep, you and your treatment team will be better able to follow the evolution of your symptoms and therefore
Announcements. Grade Query Tool+ PsychPortal. Final Exam Wed May 9, 1-3 pm
 Grade Query Tool+ Announcements This tool is the definitive source for your final grade! Now includes Grade Estimator Tool PsychPortal Technical glitches in Learning Curves for Chapters 5, 14, and 15 are
Grade Query Tool+ Announcements This tool is the definitive source for your final grade! Now includes Grade Estimator Tool PsychPortal Technical glitches in Learning Curves for Chapters 5, 14, and 15 are
Mood Disorders. Gross deviation in mood
 Mood Disorders Gross deviation in mood Depression u Affective: Depressed mood (kids-irritability), or anhedonia for 2 weeks minimum. u Cognitive: worthlessness/ guilt, hopelessness, indecisiveness/ concentration,
Mood Disorders Gross deviation in mood Depression u Affective: Depressed mood (kids-irritability), or anhedonia for 2 weeks minimum. u Cognitive: worthlessness/ guilt, hopelessness, indecisiveness/ concentration,
Guidelines MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD)
") MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
MANAGEMENT OF MAJOR DEPRESSIVE DISORDER (MDD) Guidelines CH Lim, B Baizury, on behalf of Development Group Clinical Practice Guidelines Management of Major Depressive Disorder A. Introduction Major depressive
Depressive, Bipolar and Related Disorders
 Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Depressive, Bipolar and Related Disorders Robert Kelly, MD Assistant Professor of Psychiatry Weill Cornell Medical College White Plains, New York Lecture available at www.robertkelly.us Financial Conflicts
Class Objectives. Depressive Disorders 10/7/2013. Chapter 7. Depressive Disorders. Next Class:
 Chapter 7 Class Objectives Depressive Disorders - Major Depressive Disorder - Persistent Depressive Disorder - Disruptive Mood Dysregulation Disorder - Premenstrual Dysphoric Disorder (PMDD) Next Class:
Chapter 7 Class Objectives Depressive Disorders - Major Depressive Disorder - Persistent Depressive Disorder - Disruptive Mood Dysregulation Disorder - Premenstrual Dysphoric Disorder (PMDD) Next Class:
Mood Disorders Workshop Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland
 Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Mood Disorders Workshop 2010 Dr Andrew Howie / Dr Tony Fernando Psychological Medicine Faculty of Medical and Health Sciences University of Auckland Goals To learn about the clinical presentation of mood
Dr Carmelo Aquilina Senior Staff Specialist & Service Director Sydney West Area Health Service Clinical Senior Lecturer, University of Sydney
 Dr Carmelo Aquilina Senior Staff Specialist & Service Director Sydney West Area Health Service Clinical Senior Lecturer, University of Sydney A suicide Outline Part 1: understanding suicide Part 2: What
Dr Carmelo Aquilina Senior Staff Specialist & Service Director Sydney West Area Health Service Clinical Senior Lecturer, University of Sydney A suicide Outline Part 1: understanding suicide Part 2: What
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS
 DISORDERS and ANXIETY DISORDERS") MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
MOOD (AFFECTIVE) DISORDERS and ANXIETY DISORDERS Shelley Klipp AS91 Spring 2010 TIP 42 Pages 226-231 and 369-379 DSM IV-TR APA 2000 Co-Occurring Substance Abuse and Mental Disorders by John Smith Types
Chapter 7 - Mood Disorders
 Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
Chapter 7 - Mood Disorders I. DEPRESSION A. Description Symptoms: 5+ constant over 2 weeks - sadness/depressed mood - guilt/remorse/worthlessness - suicidal thoughts - anhedonia (lack of pleasure) - fatigue/lethargy
Depression in Adolescents PREMA MANJUNATH, MD CHILD AND ADOLESCENT PSYCHIATRIST
 Depression in Adolescents PREMA MANJUNATH, MD CHILD AND ADOLESCENT PSYCHIATRIST Francis Bacon Children sweeten labors, but they make misfortunes bitter. They increase the cares of life, but they mitigate
Depression in Adolescents PREMA MANJUNATH, MD CHILD AND ADOLESCENT PSYCHIATRIST Francis Bacon Children sweeten labors, but they make misfortunes bitter. They increase the cares of life, but they mitigate
Phone Screen. Beginning the Psychoeducational Process: The Intake. The Psychoeducational Process and Elements throughout Care
 Brian McKain, RN, MSN Christina Hanna, MS 1. Identify and explain the components used to assess and diagnose depression 2. How to share the wealth with both patients and their parents 3. Understand that
Brian McKain, RN, MSN Christina Hanna, MS 1. Identify and explain the components used to assess and diagnose depression 2. How to share the wealth with both patients and their parents 3. Understand that
Overview. Part II: Part I: Screening for Depression and Anxiety Risk Assessment Diagnosis of Depressive Disorders
 1 Learning Objectives 1. Providers will become familiar with methods of screening for depression and anxiety. 2. Providers will become more comfortable with diagnosis and management of these common pediatric
1 Learning Objectives 1. Providers will become familiar with methods of screening for depression and anxiety. 2. Providers will become more comfortable with diagnosis and management of these common pediatric
Summary of guideline for the. treatment of depression RANZCP CLINICAL PRACTICE GUIDELINES ASSESSMENT
 RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
RANZCP CLINICAL PRACTICE GUIDELINES Summary of guideline for the RANZCP CLINICAL PRACTICE GUIDELINES treatment of depression Pete M. Ellis, Ian B. Hickie and Don A. R. Smith for the RANZCP Clinical Practice
Depression Management
 Depression Management Ulka Agarwal, M.D. Adjunct Psychiatrist Pine Rest Christian Mental Health Disclosures The presenter and all planners of this education activity do not have a financial/arrangement
Depression Management Ulka Agarwal, M.D. Adjunct Psychiatrist Pine Rest Christian Mental Health Disclosures The presenter and all planners of this education activity do not have a financial/arrangement
Bipolar Disorder 4/6/2014. Bipolar Disorder. Symptoms of Depression. Mania. Depression
 Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Bipolar Disorder J. H. Atkinson, M.D. Professor of Psychiatry HIV Neurobehavioral Research Programs University of California, San Diego KETHEA, Athens Slides courtesy of John Kelsoe, M.D. Bipolar Disorder
Suicide Prevention: How to Keep Someone Safe & Alive. January 2017
 Suicide Prevention: How to Keep Someone Safe & Alive January 2017 Goals & Objectives Define Mental Illness, Age of Onset Discuss Statistics of Suicide, Nonfatal Suicidal Thoughts & Behaviors, Racial &
Suicide Prevention: How to Keep Someone Safe & Alive January 2017 Goals & Objectives Define Mental Illness, Age of Onset Discuss Statistics of Suicide, Nonfatal Suicidal Thoughts & Behaviors, Racial &
CRPS and Suicide Prevention
 1 CRPS and Suicide Prevention Jill Harkavy Friedman, PhD June 23, 2012 RSDSA Board Meeting 2 What we know about suicidal ideation and behavior Majority of people have thought about suicide at some point
1 CRPS and Suicide Prevention Jill Harkavy Friedman, PhD June 23, 2012 RSDSA Board Meeting 2 What we know about suicidal ideation and behavior Majority of people have thought about suicide at some point
Contemporary Psychiatric-Mental Health Nursing Third Edition. Introduction. Introduction 9/10/ % of US suffers from Mood Disorders
 Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 17 Mood Disorders Introduction 12% of US suffers from Mood Disorders MD are a group of psychiatric DO characterized by physical, emotional
Running head: DEPRESSIVE DISORDERS 1
 Running head: DEPRESSIVE DISORDERS 1 Depressive Disorders: DSM-5 Name: Institution: DEPRESSIVE DISORDERS 2 Abstract The 2013 update to DSM-5 saw revisions of the psychiatric nomenclature, diagnostic criteria,
Running head: DEPRESSIVE DISORDERS 1 Depressive Disorders: DSM-5 Name: Institution: DEPRESSIVE DISORDERS 2 Abstract The 2013 update to DSM-5 saw revisions of the psychiatric nomenclature, diagnostic criteria,
KEY MESSAGES. It is often under-recognised and 30-50% of MDD cases in primary care and medical settings are not detected.
 KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
KEY MESSAGES Major depressive disorder (MDD) is a significant mental health problem that disrupts a person s mood and affects his psychosocial and occupational functioning. It is often under-recognised
HELPING TEENS COPE WITH GRIEF AND LOSS RESPONDING TO SUICIDE
 HELPING TEENS COPE WITH GRIEF AND LOSS RESPONDING TO SUICIDE HOW TEENS COPE WITH LOSS & GRIEVE Grief is personal There is no right or wrong way to grieve Influenced by developmental level, cultural traditions,
HELPING TEENS COPE WITH GRIEF AND LOSS RESPONDING TO SUICIDE HOW TEENS COPE WITH LOSS & GRIEVE Grief is personal There is no right or wrong way to grieve Influenced by developmental level, cultural traditions,
Teen Suicide 2013 Kmcfarlane 10/3/13
 1 2 3 4 5 6 7 Teen Suicide Kevin McFarlane BSN,RN,CEN,EMT University of New Mexico Hospital Suicide The spectrum of suicide Suicide Defined Suicide: Intentionally causing one s own death. Sometimes difficult
1 2 3 4 5 6 7 Teen Suicide Kevin McFarlane BSN,RN,CEN,EMT University of New Mexico Hospital Suicide The spectrum of suicide Suicide Defined Suicide: Intentionally causing one s own death. Sometimes difficult
PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS. Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA
 CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
CASE #1 PRACTICAL MANAGEMENT OF DEPRESSION IN OLDER ADULTS Lee A. Jennings, MD MSHS Assistant Professor Division of Geriatrics, UCLA OBJECTIVES Epidemiology Presentation in older adults Assessment Treatment
AMPS : A Quick, Effective Approach To The Primary Care Psychiatric Interview
 AMPS : A Quick, Effective Approach To The Primary Care Psychiatric Interview February 7, 2012 Robert McCarron, D.O. Assosicate Clinical Professor Internal Medicine / Psychiatry / Pain Medicine UC Davis,
AMPS : A Quick, Effective Approach To The Primary Care Psychiatric Interview February 7, 2012 Robert McCarron, D.O. Assosicate Clinical Professor Internal Medicine / Psychiatry / Pain Medicine UC Davis,
https://www.glyndewis.com/wp-content/uploads/2014/12/sos.jpg Recognizing and Responding to Signs in Ourselves or Others
 https://www.glyndewis.com/wp-content/uploads/2014/12/sos.jpg Recognizing and Responding to Signs in Ourselves or Others Purpose of the SOS Suicide Prevention Program To help students and trusted adults
https://www.glyndewis.com/wp-content/uploads/2014/12/sos.jpg Recognizing and Responding to Signs in Ourselves or Others Purpose of the SOS Suicide Prevention Program To help students and trusted adults
Announcements. The final Aplia gauntlet: Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+
 The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
The final Aplia gauntlet: Announcements Chapter 12 Aplia due tonight Chapter 13 Aplia due Wednesday Final Exam is May 14, 3:30 pm Still more experiments going up daily! Enhanced Grade-query Tool+ Now includes
FIREARMS AND SUICIDE PREVENTION
 FIREARMS AND SUICIDE PREVENTION WHAT LEADS TO SUICIDE? There s no single cause. Suicide most often occurs when several stressors and health issues converge to create an experience of hopelessness and despair.
FIREARMS AND SUICIDE PREVENTION WHAT LEADS TO SUICIDE? There s no single cause. Suicide most often occurs when several stressors and health issues converge to create an experience of hopelessness and despair.
Handout 3: Mood Disorders
 Handout 3: Mood Disorders Mood disorders are called affective (emotional) disorders. There are two categories of mood disorders: Depressive Disorders Bipolar Affective Disorders Depressive Disorders Minor
Handout 3: Mood Disorders Mood disorders are called affective (emotional) disorders. There are two categories of mood disorders: Depressive Disorders Bipolar Affective Disorders Depressive Disorders Minor
Chapter 10 Suicide Assessment
 Chapter 10 Suicide Assessment Dr. Rick Grieve PSY 442 Western Kentucky University Not this: Suicide is man s way of telling God, You can t fire me, I quit. Bill Maher 1 Suicide Assessment Personal Reactions
Chapter 10 Suicide Assessment Dr. Rick Grieve PSY 442 Western Kentucky University Not this: Suicide is man s way of telling God, You can t fire me, I quit. Bill Maher 1 Suicide Assessment Personal Reactions
Depression, Anxiety, and the Adolescent Athlete: Introduction to Identification and Treatment
 Depression, Anxiety, and the Adolescent Athlete: Introduction to Identification and Treatment Jamie E. Pardini, PhD Sports Medicine and Concussion Specialists Banner University Medical Center-Phoenix University
Depression, Anxiety, and the Adolescent Athlete: Introduction to Identification and Treatment Jamie E. Pardini, PhD Sports Medicine and Concussion Specialists Banner University Medical Center-Phoenix University
Depression & Suicidality. Project Success+ & CAPE
 Depression & uicidality Project uccess+ & CAPE Introduction Project uccess-tudent upport Program Assess and Refer to ervices Group and Individual Counseling Education Windsor O Clinic CAPE-(Crisis Assessment
Depression & uicidality Project uccess+ & CAPE Introduction Project uccess-tudent upport Program Assess and Refer to ervices Group and Individual Counseling Education Windsor O Clinic CAPE-(Crisis Assessment
Suicide Prevention Carroll County Public Schools
 Suicide Prevention Carroll County Public Schools 2012-13 The Facts Statistics 3 rd leading cause of death for adolescents (15-24 yrs. old) 6 th leading cause of death for children (5-14 yrs. old) 11 th
Suicide Prevention Carroll County Public Schools 2012-13 The Facts Statistics 3 rd leading cause of death for adolescents (15-24 yrs. old) 6 th leading cause of death for children (5-14 yrs. old) 11 th
Primary Care: Referring to Psychiatry
 Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Primary Care: Referring to Psychiatry Carol Capitano, PhD, APRN-BC Assistant Professor, Clinical Educator University of New Mexico College of Nursing University of New Mexico Psychiatric Center Objectives
Warning Signs of Mental Illness in Children/Adolescents. Beth Confer, MA, LPC Director, Community Relations Clarity Child Guidance Center
 Warning Signs of Mental Illness in Children/Adolescents Beth Confer, MA, LPC Director, Community Relations Clarity Child Guidance Center Identify At least 5 warning signs of mental illness in children
Warning Signs of Mental Illness in Children/Adolescents Beth Confer, MA, LPC Director, Community Relations Clarity Child Guidance Center Identify At least 5 warning signs of mental illness in children
Geriatric Depression; Not a Normal Part of Growing Older. Cherie Warriner, LCSW
 1 Geriatric Depression; Not a Normal Part of Growing Older Cherie Warriner, LCSW What is Depression? While it is normal to feel sad or blue on occasion, these feelings are often transient. Depression is
1 Geriatric Depression; Not a Normal Part of Growing Older Cherie Warriner, LCSW What is Depression? While it is normal to feel sad or blue on occasion, these feelings are often transient. Depression is
Patient Management Tools
 Patient Management Tools Many concrete and easy-to-use tools are available to assist you and your staff in preventing suicide. This section includes pocket-sized tools to facilitate assessment and intervention
Patient Management Tools Many concrete and easy-to-use tools are available to assist you and your staff in preventing suicide. This section includes pocket-sized tools to facilitate assessment and intervention
RANZCP 2010 AUCKLAND, NEW ZEALAND
 RANZCP 2010 AUCKLAND, NEW ZEALAND Dr Veronica Stanganelli et al. RANZCP 2010 1 INTRODUCTION Bipolar disorder within young people has been debated for years. It is still controversial in DSM V (1), whether
RANZCP 2010 AUCKLAND, NEW ZEALAND Dr Veronica Stanganelli et al. RANZCP 2010 1 INTRODUCTION Bipolar disorder within young people has been debated for years. It is still controversial in DSM V (1), whether
Low mood and depression
 Section 1 Low mood and depression Flow chart for the management of low mood or depression from Primary Care to Specialist CAMHS Child/young person presents to Tier 1 professional with signs of low mood/depression
Section 1 Low mood and depression Flow chart for the management of low mood or depression from Primary Care to Specialist CAMHS Child/young person presents to Tier 1 professional with signs of low mood/depression
Suicide Spectrum Assessment and Interventions. Welcome to RoseEd Academy. Disclaimer
 RoseEd Module 7 Suicide Spectrum Assessment and Interventions Suicide Spectrum Assessment and Interventions J. Scott Nelson MA NCC LPC CRADC Staff Education Coordinator Welcome to RoseEd Academy Disclaimer
RoseEd Module 7 Suicide Spectrum Assessment and Interventions Suicide Spectrum Assessment and Interventions J. Scott Nelson MA NCC LPC CRADC Staff Education Coordinator Welcome to RoseEd Academy Disclaimer
Class Objectives 10/19/2009. Chapter 5 Mood Disorders. Depressive Disorders. What are Unipolar Mood Disorders?
 Chapter 5 Mood Disorders Class Objectives Depressive Disorders What are Mood Disorders? What is Major Depressive Disorder? What is Post Partum Disorder? What are Unipolar Mood Disorders? What is Mania?
Chapter 5 Mood Disorders Class Objectives Depressive Disorders What are Mood Disorders? What is Major Depressive Disorder? What is Post Partum Disorder? What are Unipolar Mood Disorders? What is Mania?
Module Objectives 10/28/2009. Chapter 6 Mood Disorders. Depressive Disorders. What are Unipolar Mood Disorders?
 Chapter 6 Mood Disorders Module Objectives Depressive Disorders What are Mood Disorders? What is Major Depressive Disorder? What is Post Partum Disorder? What are Unipolar Mood Disorders? What is Mania?
Chapter 6 Mood Disorders Module Objectives Depressive Disorders What are Mood Disorders? What is Major Depressive Disorder? What is Post Partum Disorder? What are Unipolar Mood Disorders? What is Mania?
BDS-2 QUICK SCORE SCHOOL VERION PROFILE SAMPLE
 BEHAVIOR DIMENSIONS SCALE-2 Name of student: Andrea Thomas School: Midvale High School Class: Science City: Midvale SCHOOL VERSION RATING FORM PROFILE SHEET Gender: Female Grade: State: NY Subscales SUMMARY
BEHAVIOR DIMENSIONS SCALE-2 Name of student: Andrea Thomas School: Midvale High School Class: Science City: Midvale SCHOOL VERSION RATING FORM PROFILE SHEET Gender: Female Grade: State: NY Subscales SUMMARY
Referral guidance for Lincolnshire CAMHS
 Referral guidance for Lincolnshire CAMHS The service is designed to meet a wide range of mental health needs in children and young people. This includes mild to moderate emotional wellbeing and mental
Referral guidance for Lincolnshire CAMHS The service is designed to meet a wide range of mental health needs in children and young people. This includes mild to moderate emotional wellbeing and mental
Suicide Prevention in Children and Adolescents. November 9, Note: Listen to the Webinar using your computer s speakers. There is no phone line.
 Suicide Prevention in Children and Adolescents November 9, 2016 Note: Listen to the Webinar using your computer s speakers. There is no phone line. Continuing Education Children s Hospital of Philadelphia
Suicide Prevention in Children and Adolescents November 9, 2016 Note: Listen to the Webinar using your computer s speakers. There is no phone line. Continuing Education Children s Hospital of Philadelphia
BAPTIST HEALTH SCHOOL OF NURSING NSG 3037: PSYCHIATRIC MENTAL HEALTH. Safety: Suicidal Crisis
 F 1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3037: PSYCHIATRIC MENTAL HEALTH Safety: Suicidal Crisis Lecture Objectives: 1. Discuss epidemiological statistics and risk factors related to suicide. 2. Describe
F 1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3037: PSYCHIATRIC MENTAL HEALTH Safety: Suicidal Crisis Lecture Objectives: 1. Discuss epidemiological statistics and risk factors related to suicide. 2. Describe
Depression among Older Adults. Prevalence & Intervention Strategies
 Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Depression among Older Adults Prevalence & Intervention Strategies Definition Depression is a complex syndrome complex characterized by mood disturbance plus variety of cognitive, psychological, and vegetative
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults
 Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Are All Older Adults Depressed? Common Mental Health Disorders in Older Adults Cherie Simpson, PhD, APRN, CNS-BC Myth vs Fact All old people get depressed. Depression in late life is more enduring and
Depression major depressive disorder. Some terms: Major Depressive Disorder: Major Depressive Disorder:
 Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Depression major depressive disorder Oldest recognized disorder: melancholia It is a positive and active anguish, a sort of psychical neuralgia wholly unknown to normal life. - William James "I am now
Evolve: Avita Community Partners. Emerging Adults Support Services
 Evolve: Avita Community Partners Emerging Adults Support Services About Avita: Avita s mission is to improve quality of life for persons with behavioral health and developmental disabilities. Our goal
Evolve: Avita Community Partners Emerging Adults Support Services About Avita: Avita s mission is to improve quality of life for persons with behavioral health and developmental disabilities. Our goal
ROBBINSVILLE SCHOOL DISTRICT
 ROBBINSVILLE SCHOOL DISTRICT Working Together to Help Our Children A Candid Discussion About Recovering from Loss A Community Conversation September 12, 2017 Tonight is intended to be a serious and important
ROBBINSVILLE SCHOOL DISTRICT Working Together to Help Our Children A Candid Discussion About Recovering from Loss A Community Conversation September 12, 2017 Tonight is intended to be a serious and important
Depressive and Bipolar Disorders
 Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
Depressive and Bipolar Disorders Symptoms Associated with Depressive and Bipolar Disorders Characteristics of mood symptoms Affects a person s well being, school, work, or social functioning Continues
LINEHAN RISK ASSESSMENT AND MANAGEMENT PROTOCOL (LRAMP)
") Client: Person Completing: LINEHAN RISK ASSESSMENT AND MANAGEMENT PROTOCOL (LRAMP) Date Contacted: Date Created: SECTION 1: REASON FOR COMPLETION LRAMP 1. Reason for completing: History of suicide ideation,
Client: Person Completing: LINEHAN RISK ASSESSMENT AND MANAGEMENT PROTOCOL (LRAMP) Date Contacted: Date Created: SECTION 1: REASON FOR COMPLETION LRAMP 1. Reason for completing: History of suicide ideation,
Mental Health Disorders in 22q11 DS
 Mental Health Disorders in 22q11 DS Give yourself plenty of time to read this leaflet and do get in touch with us if you have any queries or concerns. The purpose of this leaflet is to give you a broad
Mental Health Disorders in 22q11 DS Give yourself plenty of time to read this leaflet and do get in touch with us if you have any queries or concerns. The purpose of this leaflet is to give you a broad
Mental Health and Stress
 Mental Health and Stress Learning Objectives Ø Define mental health and discuss the characteristics of mentally healthy and selfactualized people Ø Describe the various mental disorders and appropriate
Mental Health and Stress Learning Objectives Ø Define mental health and discuss the characteristics of mentally healthy and selfactualized people Ø Describe the various mental disorders and appropriate
Jonathan Haverkampf BIPOLAR DISORDR BIPOLAR DISORDER. Dr. Jonathan Haverkampf, M.D.
 BIPOLAR DISORDER Dr., M.D. Abstract - Bipolar disorder is a condition affecting an individual s affective states (mood). The different flavors of bipolar disorder have in common that there are alterations
BIPOLAR DISORDER Dr., M.D. Abstract - Bipolar disorder is a condition affecting an individual s affective states (mood). The different flavors of bipolar disorder have in common that there are alterations
depression and anxiety in later life clinical challenges and creative research
 2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
2 nd Annual MARC Symposium Critical Themes in Ageing Melbourne, 10 th August 2018 depression and anxiety in later life clinical challenges and creative research Nicola T Lautenschlager, MD, FRANZCP Professor
Introduction into Psychiatric Disorders. Dr Jon Spear- Psychiatrist
 Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
Overview. Classification, Assessment, and Treatment of Childhood Disorders. Criteria for a Good Classification System
 Classification, Assessment, and Treatment of Childhood Disorders Dr. K. A. Korb University of Jos Overview Classification: Identifying major categories or dimensions of behavioral disorders Diagnosis:
Classification, Assessment, and Treatment of Childhood Disorders Dr. K. A. Korb University of Jos Overview Classification: Identifying major categories or dimensions of behavioral disorders Diagnosis:
MENTAL HEALTH DISEASE CLASSIFICATIONS
 MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
MENTAL HEALTH DISEASE CLASSIFICATIONS DIAGNOSIS OF MENTAL DISORDERS DSM-IV-TR Published by APA ( 2000 ) Multiaxial system 5 categories called axes Facilitate holistic assessment for care Is a great resource
Mood Disorders for Care Coordinators
 Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
Mood Disorders for Care Coordinators David A Harrison, MD, PhD Assistant Professor, Dept of Psychiatry & Behavioral Sciences University of Washington School of Medicine Introduction 1 of 3 Mood disorders
WHAT IS DEPRESSION? Persistent Condition Abnormal Functioning 9/28/2011
 Developmental Resources Proudly Presents Kim Tip Frank, Ed.S., LPC School Counselor Rock Hill School District Three Author of: Battling the Blues Available @ www.youthlightbooks.com Please Ask Questions
Developmental Resources Proudly Presents Kim Tip Frank, Ed.S., LPC School Counselor Rock Hill School District Three Author of: Battling the Blues Available @ www.youthlightbooks.com Please Ask Questions
3/9/2017. A module within the 8 hour Responding to Crisis Course. Our purpose
 A module within the 8 hour Responding to Crisis Course Our purpose 1 What is mental Illness Definition of Mental Illness A syndrome characterized by clinically significant disturbance in an individual
A module within the 8 hour Responding to Crisis Course Our purpose 1 What is mental Illness Definition of Mental Illness A syndrome characterized by clinically significant disturbance in an individual
Directions: Use your mouse or the arrows on your keyboard to click through this tutorial.
 Directions: Use your mouse or the arrows on your keyboard to click through this tutorial. Diamond Healthcare Corporation Suicide Risk Assessment For Outpatient Programs 2009 Objectives 1. Identify the
Directions: Use your mouse or the arrows on your keyboard to click through this tutorial. Diamond Healthcare Corporation Suicide Risk Assessment For Outpatient Programs 2009 Objectives 1. Identify the
Recovery From Depression
 Recovery From Depression Optimising Primary Care Management Dr Andrew Smithers Mental Health and LD Lead Coventry & Rugby CCG CLINICAL TRIALS EXCELLENCE THE PHYSICIAN - LED NETWORK Introduction Primarily
Recovery From Depression Optimising Primary Care Management Dr Andrew Smithers Mental Health and LD Lead Coventry & Rugby CCG CLINICAL TRIALS EXCELLENCE THE PHYSICIAN - LED NETWORK Introduction Primarily
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia
 Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
Condensed Clinical Practice Guideline Treatment Of Patients With Schizophrenia I. Key Points a. Schizophrenia is a chronic illness affecting all aspects of person s life i. Treatment Planning Goals 1.
ACOEM Commercial Driver Medical Examiner Training Program
 ACOEM Commercial Driver Medical Examiner Training Program Module 7: Psychological Psychological 49 CFR 391.41(b)(9) "A person is physically qualified to drive a commercial motor vehicle if that person
ACOEM Commercial Driver Medical Examiner Training Program Module 7: Psychological Psychological 49 CFR 391.41(b)(9) "A person is physically qualified to drive a commercial motor vehicle if that person
Psychosis, Mood, and Personality: A Clinical Perspective
 Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
Psychosis, Mood, and Personality: A Clinical Perspective John R. Chamberlain, M.D. Assistant Director, Psychiatry and the Law Program Assistant Clinical Professor University of California San Francisco
5/2/2017. By Pamela Pepper PMH, CNS, BC. DSM-5 Growth and Development
 By Pamela Pepper PMH, CNS, BC DSM-5 Growth and Development The idea that diagnosis is based on subjective criteria and that those criteria should fall neatly into a set of categories is not sustainable,
By Pamela Pepper PMH, CNS, BC DSM-5 Growth and Development The idea that diagnosis is based on subjective criteria and that those criteria should fall neatly into a set of categories is not sustainable,
The Difficult Patient. Psychiatric Dilemmas in the Primary Care Setting. No Disclosures. Objectives 10/12/17. Erick K. Hung, MD
 Psychiatric Dilemmas in the Primary Care Setting No Disclosures Erick K. Hung, MD Associate Professor of Clinical Psychiatry University of California, San Francisco Objectives Describe approaches to the
Psychiatric Dilemmas in the Primary Care Setting No Disclosures Erick K. Hung, MD Associate Professor of Clinical Psychiatry University of California, San Francisco Objectives Describe approaches to the
DURING A SUICIDAL CRISIS
 DURING A SUICIDAL CRISIS 1 UTAH RANKS 5 TH IN THE NATION 1 6 7 5 3 9 10 4 8 2 Data Source: WONDER 2016 Suicide Fatality Rates ages 10+ 2 Crude Rate of Suicides per 100,000 UTAH AND U.S. SUICIDE TREND Rate
DURING A SUICIDAL CRISIS 1 UTAH RANKS 5 TH IN THE NATION 1 6 7 5 3 9 10 4 8 2 Data Source: WONDER 2016 Suicide Fatality Rates ages 10+ 2 Crude Rate of Suicides per 100,000 UTAH AND U.S. SUICIDE TREND Rate
Parental Depression: The Elephant in the room with us
 Parental Depression: The Elephant in the room with us Ardis Olson, MD Dartmouth Medical School UPIQ Screening for Maternal Depression Learning Collaborative September 15, 2006 Ardis.Olson@dartmouth.edu
Parental Depression: The Elephant in the room with us Ardis Olson, MD Dartmouth Medical School UPIQ Screening for Maternal Depression Learning Collaborative September 15, 2006 Ardis.Olson@dartmouth.edu
HERTFORDSHIRE PARTNERSHIP UNIVERSITY NHS FOUNDATION TRUST. Referral Criteria for Specialist Tier 3 CAMHS
 Referral Criteria for Specialist Tier 3 CAMHS Specialist CAMHS provides mental health support, advice and guidance and treatment for Children and Young People with moderate or severe mental health difficulties,
Referral Criteria for Specialist Tier 3 CAMHS Specialist CAMHS provides mental health support, advice and guidance and treatment for Children and Young People with moderate or severe mental health difficulties,
Operation S.A.V.E Campus Edition
 Operation S.A.V.E Campus Edition 1 Suicide Prevention Introduction Objectives: By participating in this training you will learn: The scope and importance of suicide prevention The negative impact of myths
Operation S.A.V.E Campus Edition 1 Suicide Prevention Introduction Objectives: By participating in this training you will learn: The scope and importance of suicide prevention The negative impact of myths
Mental Health First Aid at a Glance
 Mental Health First Aid at a Glance Candice M. Haines, LCPC Program Supervisor Mental Health First Aid Instructor Pilsen Wellness Center chaines@pilsenmh.org Overview Address myths vs facts Warning signs
Mental Health First Aid at a Glance Candice M. Haines, LCPC Program Supervisor Mental Health First Aid Instructor Pilsen Wellness Center chaines@pilsenmh.org Overview Address myths vs facts Warning signs
2018 Texas Focus: On the Move! Let s Talk: Starting the Mental Health Conversation with Your Teen Saturday, March 3, :45-11:15 AM
 Texas School for the Blind & Visually Impaired Outreach Programs www.tsbvi.edu 512-454-8631 1100 W. 45 th St. Austin, TX 78756 2018 Texas Focus: On the Move! Let s Talk: Starting the Mental Health Conversation
Texas School for the Blind & Visually Impaired Outreach Programs www.tsbvi.edu 512-454-8631 1100 W. 45 th St. Austin, TX 78756 2018 Texas Focus: On the Move! Let s Talk: Starting the Mental Health Conversation