The State of Pregnancy-Related Depression Efforts in Colorado
|
|
|
- Pearl Gibbs
- 6 years ago
- Views:
Transcription

1 The State of Pregnancy-Related Depression Efforts in Colorado March 2014 Krista M. Beckwith, MSPH Colorado Department of Public Health and Environment
2 Contents Executive Summary... 3 Introduction... 4 Survey Respondents... 5 Current State of Pregnancy-Related Depression Efforts in Colorado... 6 Screening for Pregnancy-Related Depression... 6 Referring for Pregnancy-Related Depression Treatment... 9 Identifying and Cultivating Resources Providing Pregnancy-Related Depression Treatment or Support Professionals Who Do Not Directly Serve Pregnant or Postpartum Women Early Childhood Professionals Women s Health Providers Observations from the Data Conclusion Appendix A: Survey Methodology Survey Development Survey Dissemination Survey Question Analysis Known Limitations Appendix B: Survey
3 Executive Summary Pregnancy-related depression, occurring during pregnancy or for as long as a year postpartum, is the most common complication of pregnancy in Colorado. Over 10 percent of women giving birth in Colorado will experience signs and symptoms of depression (PRAMS, ). Identifying, referring and treating depression during the prenatal and postpartum periods is complex, requiring the commitment and coordination of diverse partners. The Colorado Department of Public Health and Environment (CDPHE) recognized the need to understand how systems in Colorado currently address both prenatal and postpartum depression. The team sought to identify how this issue is being addressed statewide along with resources for treatment or support. The best efforts and resources could be in vain, however, if women continue to fall through the cracks when it comes to appropriately identifying their depressive symptoms and effectively referring them to resources. Improvement in identifying pregnant and postpartum women in Colorado suffering from depression can best be achieved by first focusing on strengthening the screening and referral systems throughout the state, and then ensuring all Colorado providers use validated screening tools. Improvement to these systems must include a variety of community-based and clinical providers who interact with pregnant and postpartum women to ensure a wide safety net of support. Colorado has both significant strengths and opportunities for improvement in address pregnancy-related depression. To begin with, there is a strong awareness about pregnancy-related depression across the state, as witnessed by the response level to the survey. This awareness is also evident by the reporting of survey respondents that they are already screening for depression even with a lack of reimbursement for their time and effort. Colorado also has a strong early childhood system that is ready to address maternal mental health as part of the effort to improve a child s health and wellbeing. However, the state still experiences many challenges in improving care for women with pregnancy-related depression. For example, while the majority of the survey respondents noted that they use a screening tool validated for the pregnant and postpartum populations, 14 percent of respondents noted they did not use any sort of screening tool. And, when asked about screening practices, many noted that while they did use a screening tool, they did not use it consistently with all women. The survey results demonstrated a number of resources available for women experiencing pregnancy-related depression, however Colorado remains challenged in equitable resource access and services specifically tailored to the needs of pregnant and postpartum women. By engaging the whole community around screening and referral systems for pregnancy-related depression, those who serve pregnant and postpartum women can be accountable for their role in mental health awareness and follow-up, and feel prepared to incorporate this into their services. Women suffering from pregnancy-related depression need their health care providers and others they interact with in the community to be their advocates and let them know that they are not alone. 3
4 Introduction In 2011, Colorado registered 65,052 live births, with less than 8 percent of these births occurring among women age 20 and under. 1 Among all births, 16.4 percent were to women with less than a high school education, 24.0 percent were to unmarried women, and 7.4 percent were to women who reported smoking during their pregnancy. 1 Additionally, 20.6 percent of live births were to women who received prenatal care after the first trimester or who received no prenatal care, resulting in missed or delayed opportunities to address, reduce and prevent the development of pregnancy-associated morbidities. 1 According to the Pregnancy Risk Assessment Monitoring System (PRAMS) data for , the prevalence of postpartum depressive symptoms was higher among women who were unmarried, lacked resources or support (such as a stable income or health insurance) and/or had their prenatal care paid for by Medicaid. 2 Risk of depression during the postpartum period is significantly increased if the woman has a history of depression prior to becoming pregnant, has experienced postpartum depression with a previous pregnancy or has a family history of major depression. 3 Both health history and situational factors should be considered when assessing a woman s risk for pregnancy-related depression. Colorado s Maternal and Child Health Block Grant needs assessment identified pregnancy-related depression as one of nine priorities for Colorado s Maternal and Child Health program. This priority focuses on timely screening, referral and support for women with pregnancy-related depression through improvements to the health care system. It also aligns with Colorado s mental health and substance abuse winnable battle, one of 10 identified public health and environmental priorities in Colorado. The Maternal Wellness staffs at the Colorado Department of Public Health and Environment (CDPHE) are responsible for carrying out the state s pregnancy-related depression work. Early on, staff recognized the need to understand how pregnancyrelated depression is currently being addressed within communities. In the winter of 2013, Maternal Wellness staff implemented a survey across the state to further understand what screening efforts, referral processes and resources were being used by partners in the field. Further information on the survey methodology, distribution and analysis can be found in Appendix A Birth Certificate Data, Health Statistics Section, Colorado Department of Public Health and Environment Pregnancy Risk Assessment Monitoring System Data, Health Statistics Section, Colorado Department of Public Health and Environment 3 Miller, L., & LaRusso, E. (2011). Preventing postpartum depression. Psychiatric Clinics of North America, 34(1), doi: /j.psc
5 Survey Respondents A total of 580 unique responses were included in the data analysis. Approximately 86 percent completed the full survey, with the remaining respondents exiting part way through. All survey responses were included in the data analysis regardless of survey completion. As illustrated in Figure 1, responses were received from nearly every county across the state. Figure 1. Survey Respondents by County Respondents included a diverse representation of agencies, programs and health care practices, as noted in Figure 2. A majority of respondents stated they screened or talked with women about pregnancy-related depression, with a significant proportion also providing some sort of treatment or support once depressive symptoms were identified. Approximately 25 percent of respondents did not screen for or treat pregnancyrelated depression, but did provide services focused on young children or women s health. 5
6 Figure 2. Types of Agencies, Programs and Practices Responding to the Pregnancy-Related Depression Survey Note: Respondents could choose up to 3 descriptors to identify their work. Current State of Pregnancy-Related Depression Efforts in Colorado Screening for Pregnancy-Related Depression There were 352 respondents who said they discuss and/or screen for pregnancy-related depression. The screening process for each agency was assigned numerical values and categorized according to strength. These strength levels are represented by the following symbols on the map illustrated in Figure 3. A red dot represents a weak screening system. That means the agency or program talks with some women about how they are feeling, but may not converse with all women. A formal screening tool may or may not be used or may be used inconsistently. A yellow diamond represents a moderate screening system. That means the agency or program does consistently use a formal screening tool, but may only discuss results with women who they feel need it. An example of this may include only discussing screening results with a woman who screens at high risk for depression. A green star represents a strong screening system. The agency or program uses a formal screening tool with women and discusses all screening results. 6

7 Figure 3. Screening Processes for Pregnancy-Related Depression 7
8 For the purpose of this survey, a formal screening tool most commonly indicated the use of a validated tool, though a few agencies created a combined assessment where questions about depression were mixed in with other risk factor questions, such as with substance abuse, anxiety or intimate partner violence. An agency could improve the strength of its screening system by using a formal screening tool, improving standardized use and sharing results with all women regardless of score. Among agencies that reported they discuss or screen for pregnancy-related depression, 42 percent used the Edinburgh Postnatal Depression Scale (Figure 4), a screening tool designed specifically for the prenatal and postpartum population. A smaller number of respondents reported use of the Personal Health Questionnaire- 2 (PHQ-2) and Personal Health Questionnaire-9 (PHQ-9). While neither the PHQ-2 nor the PHQ-9 are specifically designed for the prenatal or postpartum population, both of these screening tools are commonly used to screen for depression in the non-pregnant adult population. The PHQ-9 also is commonly used as a diagnostic tool. These results align with national trends on the types of screening tools used and speak to the awareness many Colorado agencies and programs have of using screening tools designed for the pregnant and postpartum population. Figure 4: Screening Tools Used by Survey Respondents for Pregnant/Postpartum Women PHQ-2 PHQ-9 6% 7% Edinburgh Postnatal Depression Scale (EPDS) Postpartum Depression Screening Scale (PDSS) Center for Epidemiological Studies Depression Scale (CES-D) Beck Depression Inventory Developed Own Screening Tool 14% 4% 6% 1% 6% 13% Does Not Use a Screening Tool 42% However, while there is a high level of awareness regarding depression screens designed for the prenatal and postpartum population, 14 percent of respondents reported not using a screening tool (Figure 4). Use of a validated screening tool can appropriately and consistently identify depressive symptoms within the prenatal and postpartum population. Efforts to educate those who conduct depression screening about available tools should continue and should highlight those tools validated for the pregnant and postpartum population. 8
9 The majority of respondents reported they screen or talk to women about pregnancy-related depression more than once and as many as five times during pregnancy or the postpartum period. Additionally, respondents were asked whether they integrated the topic of depression with other relevant topics. This question was intentionally asked to identify the percentage of agencies that recognize the common risk factors among various health problems, as well as the co-occurrence. With regards to mental health during the pregnant and postpartum periods, tobacco use, substance use and anxiety commonly co-occur. Among agencies that integrate depression with other relevant topics, either in conversation or through a combined screening tool, almost half noted integration of depression with anxiety. Over one-third of respondents also integrate depression with intimate partner violence and/or substance use. Referring for Pregnancy-Related Depression Treatment There were 315 respondents who referred patients to external agencies for treatment or support of pregnancy-related depression. The referral processes for each agency were assigned numerical values and categorized according to strength. These strength levels are represented by the following symbols on the map in Figure 5. A red dot represents a weak referral system. The agency or program provides basic referral information, such as information on a local mental health agency, but not as a standard process. As a result, each woman may receive varying levels of referral information. A yellow diamond represents a moderate referral system. The agency or program provides basic referral information as well as a specific name to contact and/or instructions on how to set up an appointment. This is a standard process for at least all women who identify as high risk. A green star represents a strong referral system. The agency or program initiates all activities outlined for a moderate referral system and completes an active referral by calling on behalf of a woman and setting up an initial appointment. These activities are a standard practice for all women who identify as high risk. 9

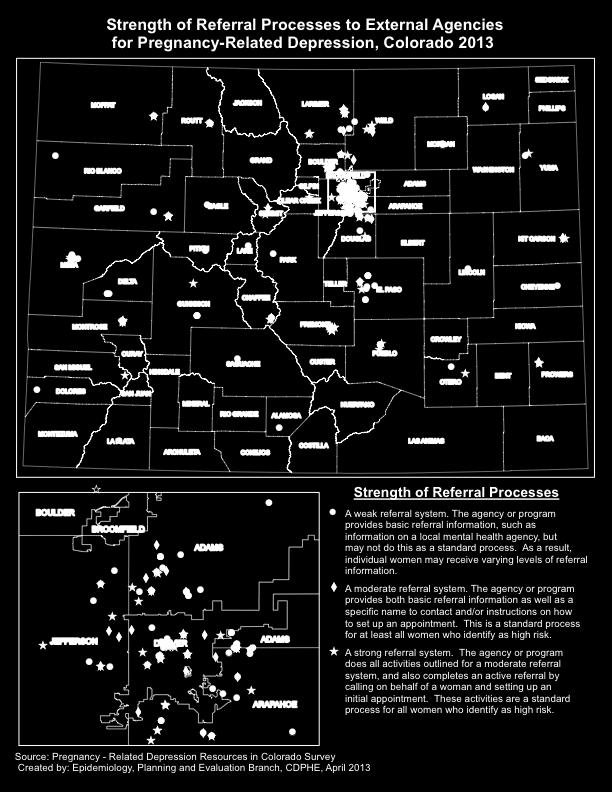
10 Figure 5. Referral Processes for Pregnancy-Related Depression 10
11 Identifying and Cultivating Resources Survey respondents who identify women with depressive symptoms through screening or conversation were asked to describe the referral resources within their communities, including mental health services, medication consultations, support groups, community education classes or other forms of support. Respondents were asked to provide both the address and services offered for the referral resource. As illustrated in Figure 6, 404 sites across Colorado were identified as referral resources. Individual or group counseling services were the most common types of referrals. Resources were grouped into four different categories to reflect the general type of support they provided, including hotlines, counseling, education/support and medication consultation/management. Many sites offer all four types of services and have potential as regional resource hubs where women can travel to receive multiple, diverse services. Hotlines were included for those sites that self-reported this resource or clearly advertised a hotline number on their agency website. While Figure 6 reflects a significant number of resources available for women experiencing pregnancy-related depression, Colorado remains challenged in equitable resource access and services specifically tailored to the needs of pregnant and postpartum women. Women living in rural and frontier communities have limited access to resources due to geographic barriers. Even when a resource is located within the community, access may not always be readily available, an observation not made as part of the survey but anecdotally noted by partners in the field. Pregnant and postpartum women continue to face delayed entry into mental health programs due to long wait lists, limited pro-bono or affordable sliding scale services for the uninsured, and loss of Medicaid coverage at six weeks postpartum. 11

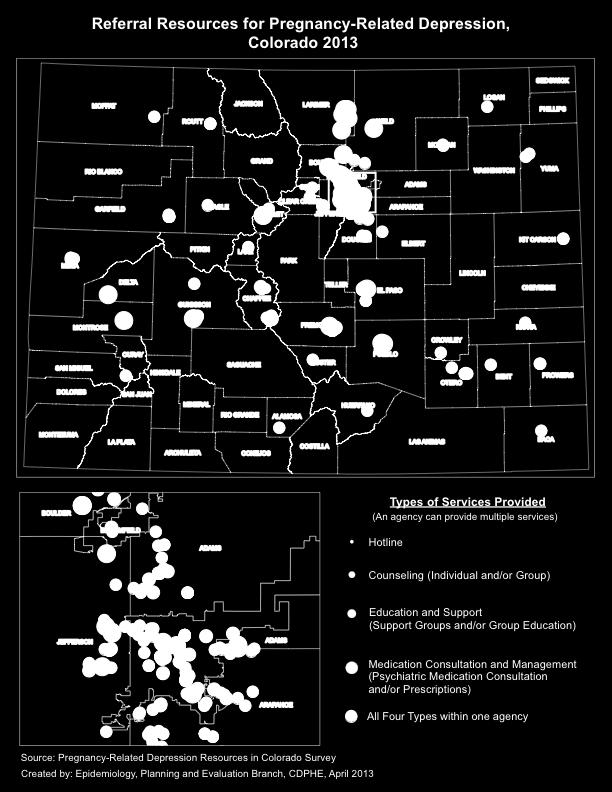
12 Figure 6. Referral Resources for Pregnancy-Related Depression 12
.")



13 Providing Pregnancy-Related Depression Treatment or Support As part of the survey, agencies that stated they provide treatment or support for pregnancy-related depression were asked about the source of referrals received. Of the 35 agencies that identified solely as treatment or support sites, self-referrals were most frequently noted as the referral source (74.3 percent). As noted in Figure 7, when treatment and support providers were asked whether they inquired about recent pregnancies during the intake process, 60 percent of respondents did not ask all women about recent pregnancies. Identifying whether a woman referred for mental health services has been pregnant in the past year may help assess pregnancy-related depression or another prenatal or postpartum mood disorder. Figure 7. Identification of a Recent Pregnancy Among Respondents Who Provide Treatment or Support for Pregnancy-Related Depression Yes- there is a 'recent pregnancy' question on our intake form or initial screening form Yes- we ask about recent pregnancies verbally with all women when we meet Yes- we ask about recent pregnancies verbally with some women when we feel it is appropriate We do not ask about a recent pregnancy 43% 17% 20% 20% Professionals Who Do Not Directly Serve Pregnant or Postpartum Women Part of the survey s intention was to reach those professionals who also may interact with pregnant or postpartum women, but not necessarily in connection with their pregnancy, such as those focused on early childhood services and women s health. The goal of reaching these professionals was to gain information about the type of work and services they provide to understand how pregnancy-related depression awareness could be effectively integrated and enhanced in their setting. 13
14 Early Childhood Professionals Early childhood professionals, such as pediatric health care providers, childcare providers, early childhood educators and early childhood council representatives were included in the survey with 125 individual responses recorded. As noted by Figure 8, most early childhood professionals predominantly interact with the mother about the child s progress or behavior, with fewer respondents interacting with the mother about her own risks. Additionally, early childhood professionals were asked to reflect on why their program or agency may not discuss pregnancy-related depression. More than 60 percent said they did not speak with mothers about this topic because they focus services on children. Figure 8. Types of Interaction with Mothers by Early Childhood Professionals Discussion of Developmental Progress of Child Discussion of Child's Behavior Discussion of Risk Behaviors of Mother Have Mother Complete a Screen for Risk Behaviors Women s Health Providers Those providing general women s health services, such as family planning, were included in the survey due to their interaction with women during the first 12 months postpartum. Family planning providers are in a unique position to check in with postpartum women during that first year, as these providers are likely one of the only non-urgent health services a new mother will seek out for herself. Yet, this sector represented the lowest percentage of survey respondents (4.1 percent). A low level of response by these providers may be due to not recognizing that they can support the follow-up care needed by postpartum women. The health sector commonly identifies postpartum follow-up care as ending at the six-week postpartum follow-up visit, and most family planning providers do not have contact with a new 14
15 mother until after that first six weeks. Yet, women s mental and behavioral health needs post-pregnancy extend beyond the first six weeks, putting family planning providers in a key position to follow up on their needs as new mothers. Observations from the Data Colorado has both significant strengths and opportunities for improvement in address pregnancy-related depression. To begin with, there is a strong awareness about pregnancy-related depression across the state, as witnessed by the response level to the survey. This awareness is also evident by the reporting of survey respondents that they are already screening for depression even with a lack of reimbursement for their time and effort. Colorado also has a strong early childhood system that is ready to address maternal mental health as part of the effort to improve a child s health and wellbeing. However, the state still experiences many challenges in improving care for women with pregnancy-related depression. For example, while the majority of the survey respondents noted that they use a screening tool validated for the pregnant and postpartum populations, almost 14 percent of respondents noted they did not use any sort of screening tool. And, when asked about screening practices, many noted that while they did use a screening tool, they did not use it consistently with all women. Thus, a gap exists in Colorado where not all providers are using a standard screening tool or using it consistently with all clients. The state also remains extremely limited in its ability to provide treatment for pregnancy-related depression. The state s mental health workforce cannot adequately meet the growing need for services, both in the general adult population and the sub-group of pregnant and postpartum women. There is limited access to mental health services in the rural and frontier regions of the state. And while a variety of resources were identified throughout the state, there is no method besides self-reporting that ensures those providing treatment for pregnancy-related depression or other perinatal mood disorders are adequately trained. Conclusion Health care and community partners working with pregnant and postpartum women cannot overlook asking a woman how she is dealing with her pregnancy and new motherhood, despite less than ideal referral resources. Not asking will not minimize the impact this debilitating health issue has on women, their families and the community. Use of a validated screening tool can appropriately and consistently identify depressive symptoms within the prenatal and postpartum population. Community-based and tele-health resources can be cultivated as appropriate referral options for those identified with mild depressive symptoms. Parenting classes, home visitation programs, infant groups and other community-based services are opportunities for education about pregnancy-related depression. They can act as a stepping stone for women in need of mental health services, but not ready or unable to access them right away. Colorado can develop ways to equip primary care providers with a level of knowledge and confidence to address the mental health needs of those who are not suffering severe diagnoses. Childcare and 15
16 family planning providers can be brought into community-level conversations on pregnancy-related depression, as their interactions with women during the first year postpartum can provide a key entry point for educating women. By engaging the whole community around screening and referral systems for pregnancy-related depression, those who serve pregnant and postpartum women can be accountable for their role in mental health awareness and follow-up, and feel prepared to incorporate this into their services. Women suffering from pregnancy-related depression need their health care providers and others they interact with in the community to be their advocates and let them know that they are not alone. 16
17 Appendix A: Survey Methodology Survey Development In Winter 2013, Maternal Wellness staff surveyed partners statewide to gather information on screening and referral behaviors, as well as referral resources used for pregnancy-related depression support. The survey required respondents to enter the address of the responding agency as well as the address of referral resources in order to link geographic coordinates to street addresses, a process known as geo-coding, to later create a visual representation of results. A copy of the survey can be found in Appendix B. Survey Dissemination To capture efforts across Colorado that address pregnancy-related depression, the survey was disseminated to a broad spectrum of medical and community partners. The survey focused on asking individuals to reflect on their program or agency s practices and procedures. Traditional prenatal and postpartum medical providers were included as well as professional medical associations, community-based programs, local public health agencies and mental health centers. Support services used during the prenatal and postpartum period were included, such as lactation consultants, social services, case management programs and substance use providers who serve pregnant women. Staff also identified and included those resources that pregnant or postpartum women access. As a result, the distribution included childcare centers, Head Start programs, certified childcare providers and family planning clinics. Approximately 5,000 individual addresses were obtained along with 27 distribution lists. In January 2013, the survey link was sent out via invitation with an introductory message describing the project s intention and a staff contact for follow-up questions or concerns. The survey remained open for two weeks, with as many as three reminder s sent to respondents. Respondents could answer the survey and then send the link to others whom they thought should answer. This sampling method gave multiple individuals within one agency the opportunity to give their input, allowing responses to reflect the diversity in policies and procedures that may exist between multiple programs housed within one agency. Survey Question Analysis Staff constructed the survey questions on screening and referral processes to allow for the identification of a system s strength in screening and referring pregnant or postpartum women for depressive symptoms. Screening and referral questions were developed as matrices, where respondents were asked to reflect on a group of activities and determine if they had done each activity with all women, some women or no women. Staff then assigned numerical values to each possible response/activity. Two total scores representing screening and referral strength were calculated based on the sums of the corresponding activities numerical values. Cut-off values were defined, which allowed each agency to be categorized based on the strength of its 17
18 screening and referral systems (weak, moderate or strong). These strength levels were then tied to specific symbols and mapped to give a visual representation of the strength of systems around the state. Staff could then use the data to describe how an agency could improve the strength of their system. Known Limitations While considerable effort was put forth by staff to reach as many respondents as possible across the state, the survey was not able to reach the entire population of agencies and practices that treat or provide support for pregnancy-related depression. Therefore, gaps in information and understanding still exist. Also, since those who received the survey were encouraged to forward it on to others, it is unknown how many individuals actually received an invite to complete the survey questions. Additionally, as with any questionnaire, using an individual s knowledge and opinion to collect information, individual interpretation may vary across respondents. This individual interpretation should be considered when making generalized statements about the results, as each respondent may have answered a question from a slightly varying viewpoint. This became evident when respondents were asked about referrals made within their own agencies, and resulted in this data not being included as part of the report. Furthermore, the survey required respondents to answer each question prior to moving on to the next, therefore not allowing them to skip questions. As a result, there were respondents who did not complete the entire survey, creating limitations in comparing individual responses. 18
19 Appendix B: Survey Beginning of survey Thank you for filling out this brief survey on behalf of the Maternal Wellness Team at the Colorado Department of Public Health and Environment. The Maternal Wellness Team is surveying organizations, programs and providers around the state to identify what screening and referral efforts are available for pregnancy related depression. This includes looking at programs and services not focused on depression that may be appropriate linkages for future work. Pregnancy related depression is defined as depression that occurs during pregnancy or up to one year after birth, including after a pregnancy loss/miscarriage. It is also commonly known as perinatal depression, postpartum depression and maternal depression. Information collected from this survey will be used in program planning. Survey findings will be made available; however individual level responses will remain anonymous. Please note that the publication of these findings are not intended to promote the use of, or referral to, specific services or agencies. Upon completion of this survey, your address will be entered into a drawing to win a $50 gift card to the restaurant of your choice. More information on the state s work with pregnancy related depression may be found at: PSD/CBON/
20 The survey should take between minutes to complete. Please note that the survey may prompt you to give address information both for yourself and those agencies you refer women to. Only your city and zip code is required. Additional information is optional. This information will not be made public, but will be used to create a visual map of the survey results. Questions may be referred to: Krista M. Beckwith, MSPH Maternal Wellness Program Colorado Department of Public Health and Environment I Krista.Beckwith@state.co.us
21 * 1. What is your address? ( addresses are requested to help identify unique responses, but will not be used in survey results.) * 2. What is the name of your agency or practice? * 3. What type of agency, program or practice most closely reflects where you work? (Please select no more than 3 options.) Child Care Doula Early Childhood Education Early Intervention Services Family Planning Home Visitation Local Public Health Agency Mental Health OB/GYN Pediatric Prenatal Plus Primary Care Social Services Substance Abuse WIC (please specify)
22 * 4. Where is your agency or practice located? If your agency has multiple locations, please put the location where you work. (If you are unable to provide your full address, please provide just city and zip. This information will be used to map survey results.) Address: Address 2: City/Town: ZIP:
23 5. What is your current level of knowledge on Colorado House Bill : Pregnancy and Evidence of Substance Use? This bill was passed during the 2012 legislature and prohibits the use of information about illegal drug use obtained through a pregnancy test or prenatal care in criminal court. I am not familiar with this I am vaguely familiar with I am adequately familiar I could educate a peer about this with this this The target population prioritized by HB The changes made to the use information on substance use obtained during pregnancy. How this legislation may impact my work with pregnant women. * 6. Does your agency or practice interact with any of the following? (Please select all that apply) Pregnant women New mothers up to 1 year postpartum Women who have recently experienced a pregnancy loss/miscarriage Children (ages birth up to at least age 1) Women seeking reproductive health or other women s health services My agency does not provide services or resources to any of the above
24 *7. Which description most appropriately reflects your agency or practice? We screen for or talk about pregnancy related depression, but do not provide treatment or support once it has been identified. We screen for or talk about pregnancy related depression and provide treatment or support once it has been identified. We provide treatment or support for pregnancy related depression when a woman is referred to us. We do not screen, treat or provide support for pregnancy related depression, but we do provide other women s health services. We do not screen, treat or provide treatment for pregnancy related depression but we do provide other children s services, such as daycare, health or other early childhood services.
25 Section 1 * 8. Does your agency or practice use any of the following formal screening tools for pregnant/postpartum women? (either verbally or in paper form) (Please select all that apply) PHQ 2 (often referred to as the "2 question screen") PHQ 9 Edinburgh Postnatal Depression Scale (EPDS) Postpartum Depression Screening Scale (PDSS) Center for Epidemiological Studies Depression Scale (CES D) Beck Depression Inventory We have developed our own screening tool We do not utilize a screening tool (please describe in the comment box below) * 9. Please identify the extent of your agency's or practice's screening process. If you do not partake in an activity, please select "We do not do this". Done with all women Done only with women we think need it We do not do this We ask a woman how she is feeling. We use a formal screening tool and have a short conversation when there is a positive screen. We use a formal screening tool and have a short conversation regardless of the screening results.
26 Section 1 * 10. How often does your agency or practice screen or talk to women about pregnancyrelated depression? 1 time during pregnancy 1 time during postpartum check up Up to 3 times either during pregnancy or postpartum Up to 5 times either during pregnancy or postpartum (please specify) * 11. Do you currently integrate the topic of pregnancy related depression with other topics? This may be through combining screening tools or combining topics in a conversation. (Select all that apply) Yes, with substance use Yes, with domestic violence Yes, with anxiety Yes, with a brief intervention tool that covers numerous topics No (please specify)
27 Section 1 * 12. Please identify the degree to which your organization/practice completes the following processes with women who need referrals to external agencies for pregnancyrelated depression treatment or support. If your agency or practice does not do a particular activity, please select We do not do this for that activity. Additional activities can be described in the box. Not a standard process, but Standard process with ALL Standard process for women done on occasion (or when a women who identify as high risk woman asks). We do not do this Provide information to take home, such as a flier or pamphlet Provide a list of local mental health services. Provide a specific name, contact information and instructions on how to schedule a visit at the referral agency Call and set up an initial intake visit at a referral agency Complete formal referral documents that are then sent to the referral agency Participate in a formal communication loop that allows referral follow up information to be shared back with our agency/practice (please specify)
28 Section 1 * 13. If able, please provide us with information about what organizations you most frequently refer women to who need support for pregnancy related depression. This may be done by selecting one of the options below. If you are unable to provide this information at this time please select "I am unable to provide this information at this time". This information is critical and will be utilized to help plan future programming and address resource gaps around the state. I will submit a referral contact list to the following address: COprdsurvey@gmail.com I will provide up to 4 referral resources as part of this survey I am unable to provide this information at this time I do not have referral resources available for women with pregnancy related depression
29 Four Referral Resources Please provide as much information as is readily available to you. You may skip over items you do not know. Please note, this information will be utilized to map the findings. (If there is no physical location for your referral, please enter none into the address, city and zip lines). Once finished, please press "Continue" at the bottom of the page. 14. Enter information about the first organization Name of Organization Address: Address 2: City/Town: ZIP: Website: Address: Phone Number: 15. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify) 16. Enter information about the second organization Name of Organization Address: Address 2: City/Town: ZIP: Website: Address: Phone Number:
30 17. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify) 18. Enter information about the third organization Name of Organization Address: Address 2: City/Town: ZIP: Website: Address: Phone Number: 19. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify)
31 20. Enter information about the fourth organization Name of Organization Address: Address 2: City/Town: ZIP: Website: Address: Phone Number: 21. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify) * 22. Please select "Continue" Continue
32 Unable to provide this information at this time 23. What types of organizations do you most frequently refer women to who need support for pregnancy related depression? (Please select all that apply) Support groups Mental/behavioral health center(s) Private counselor/psychotherapist Community based organization(s) Hotlines (local or national) Church(es) Blogs and/or websites Group counseling (please specify)
33 Section 2 * 24. Does your agency or practice use any of the following formal screening tools for pregnant/postpartum women? (either verbally or in paper form) (Please select all that apply) PHQ 2 (often referred to as the "2 question screen") PHQ 9 Edinburgh Postnatal Depression Scale (EPDS) Postpartum Depression Screening Scale (PDSS) Center for Epidemiological Studies Depression Scale (CES D) Beck Depression Inventory We have developed our own screening tool We do not utilize a screening tool (please describe in the comment box below) * 25. Please identify the extent of your agency's or practice's screening process. If you do not partake in an activity, please select "We do not do this". Done with all women Done only with women we think need it We do not do this We ask a woman how she is feeling. We use a formal screening tool and have a short conversation when there is a positive screen. We use a formal screening tool and have a short conversation regardless of the screening results.
34 Section 2 * 26. How often does your agency or practice screen or talk to women about pregnancyrelated depression? 1 time during pregnancy 1 time during postpartum check up Up to 3 times either during pregnancy or postpartum Up to 5 times either during pregnancy or postpartum (please specify) * 27. Do you currently integrate the topic of pregnancy related depression with other topics? This may be through combining screening tools or combining topics in a conversation. (Select all that apply) Yes, with substance use Yes, with domestic violence Yes, with anxiety Yes, with a brief intervention tool that covers numerous topics No (please specify)
35 Section If you make REFERRALS WITHIN YOUR OWN AGENCY please identify to what degree your agency or practice completes the following processes with women who need pregnancy related depression treatment or support. If your agency or practice does not do a particular activity, please select We do not do this for that activity. Additional activities can be described in the box. Not standard process, but Standard process with ALL Standard process for women done on occasion (or when a women who identify as high risk woman asks) We do not do this Provide information to take home, such as a flier or pamphlet Provide a specific name, contact information and instructions on how to schedule a visit Schedule up an appointment right then and there Complete formal referral documents that are then given to the staff member providing treatment services (please specify)
36 29. If you make REFERRALS TO EXTERNAL AGENCIES please identify to what degree your agency or practice completes the following processes with women who need pregnancy related depression treatment or support. If your agency or practice does not do a particular activity, please select We do not do this for that activity. Additional activities can be described in the box. Not standard process, but Standard process with ALL Standard process for women done on occasion (or when a women who identify as high risk woman asks) We do not do this Provide information to take home, such as a flier or pamphlet Provide a list of local mental health services Provide a specific name, contact information and instructions on how to schedule a visit at the referral agency Call and set up an initial intake visit at a referral agency Complete formal referral documents that are then sent to the referral agency Participate in a formal communication loop that allows referral follow up information to be shared back with our agency/practice (please specify)
37 Section 2 * 30. What forms of treatment or support does your agency or practice provide? (Please select all that apply) Information or resources to take home Individual counseling Group counseling Psychiatric medication consultations and/or prescriptions Support groups Hotline Group education classes (please specify)
38 Section 2 * 31. If able, please provide us with information about what organizations you most frequently refer women to who need support for pregnancy related depression. This may be done by selecting one of the options below. If you are unable to provide this information at this time please select "I am unable to provide this information at this time". This information is critical and will be utilized to help plan future programming and address resource gaps around the state. I will submit a referral contact list to the following address: COprdsurvey@gmail.com I will provide up to 4 referral resources as part of this survey I am unable to provide this information at this time I do not have referral resources available for women with pregnancy related depression My agency does not refer women externally for treatment services
39 Four Referral Resources Please provide as much information as is readily available to you. You may skip over items you do not know. Please note, this information will be utilized to map the findings. (If there is no physical location for your referral, please enter none into the address, city and zip lines). Once finished, please press "Continue" at the bottom of the page. 32. Enter information about the first organization Name of Organization Address: Address 2: City/Town: State: 6 ZIP: Website: Address: Phone Number: 33. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify)
40 34. Enter information about the second organization Name of Organization Address: Address 2: City/Town: State: 6 ZIP: Website: Address: Phone Number: 35. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify) 36. Enter information about the third organization Name of Organization Address: Address 2: City/Town: State: 6 ZIP: Website: Address: Phone Number:
41 37. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify) 38. Enter information about the fourth organization Name of Organization Address: Address 2: City/Town: State: 6 ZIP: Website: Address: Phone Number: 39. For the above organization, please select the type of service(s) you commonly refer for, if known. (please select all that apply) Individual counseling Group counseling Psychiatric medication consultation and/or prescriptions Support group Hotline (referral or information) Group education classes (please specify)
42 *40. Please select "Continue" Continue
43 Unable to provide this information at this time 41. What types of organizations do you most frequently refer women to who need services or support for pregnancy related depression? (Please select all that apply) Support groups Mental/behavioral health center(s) Private counselor/psychotherapist Community based organization(s) Hotlines (local or national) Church(es) Blogs and/or websites Group counseling (please specify)
44 Section 3 * 42. What types of agencies or individuals most frequently provide you with referrals? (Please select all that apply) Doulas NICU staff Early Childhood Councils OB/GYNs Early Intervention Services Patient navigators/care coordinators Family Planning Clinics Pediatricians Child care providers Prenatal Plus Child protective services Primary care providers Home visitation programs Self Referral Hospital Staff Special Connections Housing/TANF services Women, Infants and Children (WIC) Local public health departments Midwives (please specify) * 43. What forms of treatment or support does your agency or practice provide? (Please select all that apply) Information or resources to take home Individual counseling Group counseling Psychiatric medication consultations and/or prescriptions Support groups Hotline Group education classes (please specify)
45 Section 3 * 44. During a visit, do you identify whether a woman has been pregnant in the last year if she does not come to your agency via a referral for pregnancy related depression (or is a self referral)? Yes there is a 'recent pregnancy' question on our intake form or initial screening form Yes we ask about recent pregnancies verbally with ALL women when we meet Yes we ask about recent pregnancies verbally with some women when we feel it is appropriate No not at this time (please describe in the comments box)
46 Section 4 * 45. What type of services do you provide? (Please select all that apply) Women s reproductive or other health services Children s health services Children s daycare and/or other early childhood education services Both women's and children's services (please specify) * 46. Do you currently talk with women about, or provide a screening tool for, any of the following topics? (Please select all that apply) Yes, general depression screening Yes, anxiety level screening Yes, substance use screening Yes, domestic violence screening Yes, a brief intervention screening that covers numerous topics No (please specify)
47 Section 4 * 47. If you provide women s reproductive or other health services, do you currently ask whether the woman has had a baby in the past year? If you do not provide services to women, please only select "I do not provide women's reproductive or other health services". Yes there is a 'recent pregnancy' question on our intake or initial screening form Yes we ask about recent pregnancies verbally with ALL women Yes we ask about recent pregnancies verbally with some women when we feel it is appropriate No not at this time I do not provide women s reproductive or other health services (please specify) * 48. If you provide children s daycare, health or other early childhood education services, do you currently do any of the following? (Please select all that apply) If you do not provide services to children, please only select "I do not provide children's health, daycare or other early childhood education services". Talk with the child's mother about the developmental progress of the child (physical, social, emotional, etc.) Talk with the child's mother about the child s behavior and/or attitude Talk with the child's mother about their substance use, general depression or other risk behaviors Screen the mother for substance use, depression or other risk behaviors using some sort of screening tool I do not provide children's health, daycare or other early childhood education services. None of the above (please specify)
48 Section 4 * 49. In your opinion, why do you think your program/agency does not screen or converse with women about pregnancy related depression? (Please select all that apply) We do not serve pregnant women We do not serve new mothers up to 1 year postpartum We focus our services on children We do not have enough staff to conduct this type of conversation or screening We do not have adequate knowledge to provide this type of conversation or screening We do not have time to provide this type of service or conversation. We do not get reimbursed for this type of service, and therefore cannot provide it. (please specify)
MI MOM S MOUTH. Examining a Multifaceted Michigan Initiative and the Critical Role of FQHC s in Delivering Interprofessional Care
 MI MOM S MOUTH Examining a Multifaceted Michigan Initiative and the Critical Role of FQHC s in Delivering Interprofessional Care TODAY S OBJECTIVES Learning Objective 1: Develop an understanding of Michigan
MI MOM S MOUTH Examining a Multifaceted Michigan Initiative and the Critical Role of FQHC s in Delivering Interprofessional Care TODAY S OBJECTIVES Learning Objective 1: Develop an understanding of Michigan
Implementing Postpartum Depression Screening During Infant Well Child Checks:
 Implementing Postpartum Depression Screening During Infant Well Child Checks: Options and Resources to Address Logistical Barriers to Screening During Child and Teen Checkups (C&TC) Visits Maternal & Child
Implementing Postpartum Depression Screening During Infant Well Child Checks: Options and Resources to Address Logistical Barriers to Screening During Child and Teen Checkups (C&TC) Visits Maternal & Child
Postpartum Depression Screening
 Postpartum Depression Screening October 13, 2018 Deborah CowleyMD Psychiatrist Perinatal Consultant University of Washington Disclosures Perinatal Psychiatry Consultation Line/PAL for Moms UW Perinatal
Postpartum Depression Screening October 13, 2018 Deborah CowleyMD Psychiatrist Perinatal Consultant University of Washington Disclosures Perinatal Psychiatry Consultation Line/PAL for Moms UW Perinatal
COMMUNITY MATERNITY RESOURCE GUIDE
 COMMUNITY RESOURCE GUIDE At MetroPlus Health Plan, we want to make sure that you and your baby are as healthy as possible. Here is a list of community resources that are available to you through MetroPlus.
COMMUNITY RESOURCE GUIDE At MetroPlus Health Plan, we want to make sure that you and your baby are as healthy as possible. Here is a list of community resources that are available to you through MetroPlus.
Structured Guidance for Postpartum Retention in HIV Care
 An Approach to Creating a Safety Net for Individual Patients and for Programmatic Improvements 1. Problem statement and background: Pregnant women living with HIV (WLH) are a vulnerable population that
An Approach to Creating a Safety Net for Individual Patients and for Programmatic Improvements 1. Problem statement and background: Pregnant women living with HIV (WLH) are a vulnerable population that
The Roles Local Health Departments Play in the Organization and Provision of Perinatal Services
 The Roles Local Health Departments Play in the Organization and Provision of Perinatal Services Public health efforts to reduce maternal complications and poor pregnancy outcomes encompass a wide array
The Roles Local Health Departments Play in the Organization and Provision of Perinatal Services Public health efforts to reduce maternal complications and poor pregnancy outcomes encompass a wide array
The Aboriginal Maternal and Infant Health Service: a decade of achievement in the health of women and babies in NSW
 The Aboriginal Maternal and Infant Health Service: a decade of achievement in the health of women and babies in NSW Elisabeth Murphy A,B and Elizabeth Best A A Maternity, Children and Young People s Health
The Aboriginal Maternal and Infant Health Service: a decade of achievement in the health of women and babies in NSW Elisabeth Murphy A,B and Elizabeth Best A A Maternity, Children and Young People s Health
HHSC LAR Request. Substance Abuse Disorder Coalition. Contact Person: Will Francis Members:
 HHSC LAR Request Substance Abuse Disorder Coalition Contact Person: Will Francis wfrancis.naswtx@socialworkers.org Members: NAMI Texas Children s Defense Fund Texas Communities for Recovery National Association
HHSC LAR Request Substance Abuse Disorder Coalition Contact Person: Will Francis wfrancis.naswtx@socialworkers.org Members: NAMI Texas Children s Defense Fund Texas Communities for Recovery National Association
Baby Pediatric Symptom Checklist (BPSC) Scoring Guide
 Scoring Guide") Baby Pediatric Symptom Checklist (BPSC) Scoring Guide Scoring Instructions: 1. Determine the BPSC total score by assigning a 0 for each not at all response, a 1 for each somewhat response, and a 2 for
Baby Pediatric Symptom Checklist (BPSC) Scoring Guide Scoring Instructions: 1. Determine the BPSC total score by assigning a 0 for each not at all response, a 1 for each somewhat response, and a 2 for
Intake Form. Date: Referred By: Name: Phone Number: Religious Affiliation: Where are you currently staying? City?
 Intake Form Date: Referred By: Name: Phone Number: Email: Religious Affiliation: Where are you currently staying? City?: Birthdate: Age: Place of Birth: Citizenship: Race: Social Security Number: Marital
Intake Form Date: Referred By: Name: Phone Number: Email: Religious Affiliation: Where are you currently staying? City?: Birthdate: Age: Place of Birth: Citizenship: Race: Social Security Number: Marital
5.20 West Virginia BEST START Breastfeeding Program
 POLICY: West Virginia WIC The purpose of the West Virginia BEST START Breastfeeding Program is to increase the frequency and duration of breastfeeding among women in the WIC Program per set goals cited
POLICY: West Virginia WIC The purpose of the West Virginia BEST START Breastfeeding Program is to increase the frequency and duration of breastfeeding among women in the WIC Program per set goals cited
HIP Year 2020 Health Objectives related to Perinatal Health:
 PERINATAL HEALTH Perinatal health is the health and wellbeing of mothers and babies before, during, and after child birth. As described by Healthy People 2020, Pregnancy can provide an opportunity to identify
PERINATAL HEALTH Perinatal health is the health and wellbeing of mothers and babies before, during, and after child birth. As described by Healthy People 2020, Pregnancy can provide an opportunity to identify
Day-to-Day Activities
 Maternal and Child Health, Maternal and Child Health Massachusetts Department of Public Health, Bureau of Family Health and Nutrition/Office of Data Translation Boston, Massachusetts Assignment Description
Maternal and Child Health, Maternal and Child Health Massachusetts Department of Public Health, Bureau of Family Health and Nutrition/Office of Data Translation Boston, Massachusetts Assignment Description
Perinatal Depression: What We Know
 Enhanced Engagement and Behavioral Health Integrated Centralized Intake: Infusing Mental Health Services and Support Into Maternal and Child Health Home Visiting Programs Perinatal Depression: What We
Enhanced Engagement and Behavioral Health Integrated Centralized Intake: Infusing Mental Health Services and Support Into Maternal and Child Health Home Visiting Programs Perinatal Depression: What We
Child Welfare and MOMS: Building Partnerships to Improve Care
 Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Exploration of Child Sexual Abuse Prevention Efforts in Washington State
 Exploration of Child Sexual Abuse Prevention Efforts in Washington State Over the last two years, WCSAP has prioritized the issue of child sexual abuse (CSA) prevention in Washington State. Our initial
Exploration of Child Sexual Abuse Prevention Efforts in Washington State Over the last two years, WCSAP has prioritized the issue of child sexual abuse (CSA) prevention in Washington State. Our initial
HEALTHY BABIES: COLORADO COIIN Smoking Cessation Among Pregnant Women and other priorities
 HEALTHY BABIES: COLORADO COIIN Smoking Cessation Among Pregnant Women and other priorities Larry Wolk, M.D. M.S.P.H. Executive Director and Chief Medical Officer Smoking Prevalence Among Pregnant Women
HEALTHY BABIES: COLORADO COIIN Smoking Cessation Among Pregnant Women and other priorities Larry Wolk, M.D. M.S.P.H. Executive Director and Chief Medical Officer Smoking Prevalence Among Pregnant Women
Maternal Emotional Wellness Resource Guide
 2017 Maternal Emotional Wellness Resource Guide Page 0 Service Providers 2-1-1 is a collaborative effort and we need your partnership. Your agency is responsible to get your information to 2-1-1 and provide
2017 Maternal Emotional Wellness Resource Guide Page 0 Service Providers 2-1-1 is a collaborative effort and we need your partnership. Your agency is responsible to get your information to 2-1-1 and provide
EMPOWERING WOMEN. EXPANDING AWARENESS. ERADICATING VIOLENCE.
 JOIN ICADV Become a Friend today by submitting your application. Why Join ICADV? Policy Action Alerts Newsletters and Training Alerts Make a difference in the lives of survivors of domestic violence by
JOIN ICADV Become a Friend today by submitting your application. Why Join ICADV? Policy Action Alerts Newsletters and Training Alerts Make a difference in the lives of survivors of domestic violence by
Help for Pregnant Women to Quit Smoking and Stay Quit
 BABY & ME Tobacco Free Hendricks County Health Department 355 S. Washington St. #211 Danville, IN 46122 Phone: (317) 745-9222 Fax: (317) 745-9383 Help for Pregnant Women to Quit Smoking and Stay Quit UPDATED
BABY & ME Tobacco Free Hendricks County Health Department 355 S. Washington St. #211 Danville, IN 46122 Phone: (317) 745-9222 Fax: (317) 745-9383 Help for Pregnant Women to Quit Smoking and Stay Quit UPDATED
Learning Objectives. Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons
 Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons Marianna Corona Jennifer Foley September 12, 2017 Learning Objectives 2017 Improving Family Outcomes
Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons Marianna Corona Jennifer Foley September 12, 2017 Learning Objectives 2017 Improving Family Outcomes
Matrix Framework of PERINATAL DEPRESSION and RELATED DISORDERS
 Aim of the framework: Matrix Framework of PERINATAL DEPRESSION and RELATED DISORDERS Provide guidelines on the core skills required by health professionals predominantly involved in screening women for
Aim of the framework: Matrix Framework of PERINATAL DEPRESSION and RELATED DISORDERS Provide guidelines on the core skills required by health professionals predominantly involved in screening women for
5 Public Health Challenges
 5 Public Health Challenges The most recent Mecklenburg County Community Health Assessment (CHA) prioritized the prevention of premature death and disability from chronic disease as the number one public
5 Public Health Challenges The most recent Mecklenburg County Community Health Assessment (CHA) prioritized the prevention of premature death and disability from chronic disease as the number one public
Dental Public Health Activities & Practices
 Dental Public Health Activities & Practices Practice Number: 37002 Submitted By: North Dakota Department of Health, Family Health Division Submission Date: January 2010 Last Updated: January 2010 SECTION
Dental Public Health Activities & Practices Practice Number: 37002 Submitted By: North Dakota Department of Health, Family Health Division Submission Date: January 2010 Last Updated: January 2010 SECTION
Mississippi State Department of Health, Health Services / Office of Health Data and Research
 Maternal and Child Health Mississippi State Department of Health, Health Services / Office of Health Data and Research Jackson, Mississippi Assignment Description The Mississippi State Department of Health
Maternal and Child Health Mississippi State Department of Health, Health Services / Office of Health Data and Research Jackson, Mississippi Assignment Description The Mississippi State Department of Health
Preconception Health in North Carolina. February 13, 2012 Perinatal Health Committee Child Fatality Task Force
 Preconception Health in North Carolina February 13, 2012 Perinatal Health Committee Child Fatality Task Force What is Preconception Care? Identification of modifiable and non modifiable risk factors for
Preconception Health in North Carolina February 13, 2012 Perinatal Health Committee Child Fatality Task Force What is Preconception Care? Identification of modifiable and non modifiable risk factors for
Substance-Exposed Newborns
 Substance-Exposed Newborns State of Oklahoma 2017 Substance-Exposed Newborns State of Oklahoma 2017 Legal Background Oklahoma statute, Title 63, 1-550.3, states, "The Department of Human Services shall
Substance-Exposed Newborns State of Oklahoma 2017 Substance-Exposed Newborns State of Oklahoma 2017 Legal Background Oklahoma statute, Title 63, 1-550.3, states, "The Department of Human Services shall
WIC and WIC BFPC Local Agency Application FY 20XX-20XX
 WIC and WIC BFPC Local Agency Application FY 20XX-20XX Please submit all documents electronically to the ITCA WIC Director at mindy.jossefides@itcaonline.com. Required: All documents marked with an asterisk
WIC and WIC BFPC Local Agency Application FY 20XX-20XX Please submit all documents electronically to the ITCA WIC Director at mindy.jossefides@itcaonline.com. Required: All documents marked with an asterisk
Pre-Conception & Pregnancy in Ohio
 Pre-Conception & Pregnancy in Ohio Elizabeth Conrey, PhD 1 January 217 1 State Maternal and Child Health Epidemiologist, Ohio Department of Health EXECUTIVE SUMMARY The primary objective of the analyses
Pre-Conception & Pregnancy in Ohio Elizabeth Conrey, PhD 1 January 217 1 State Maternal and Child Health Epidemiologist, Ohio Department of Health EXECUTIVE SUMMARY The primary objective of the analyses
LOGIC MODEL TEMPLATE ACT EARLY SUMMIT -WA
 Autism Society of America Chapters-resource manuals (3 currently)-expand to all 12 counties Parent s next step DVD LEND (training at all levels) Title V Community Trainings Child Profile Resource Hotline
Autism Society of America Chapters-resource manuals (3 currently)-expand to all 12 counties Parent s next step DVD LEND (training at all levels) Title V Community Trainings Child Profile Resource Hotline
Chapter 5 Nutrition Education. Table of Contents
 Chapter 5 Nutrition Education Table of Contents This chapter describes WIC's nutrition education component, including required nutrition education topics, frequency of nutrition education contacts, providing
Chapter 5 Nutrition Education Table of Contents This chapter describes WIC's nutrition education component, including required nutrition education topics, frequency of nutrition education contacts, providing
Loving Support Award of Excellence Gold Award Application Instructions
 U.S. Department of Agriculture, Food and Nutrition Service (FNS), Special Supplemental Nutrition Program for Women, Infants and Children (WIC) Gold Award Application Instructions There are 3 Award Levels:
U.S. Department of Agriculture, Food and Nutrition Service (FNS), Special Supplemental Nutrition Program for Women, Infants and Children (WIC) Gold Award Application Instructions There are 3 Award Levels:
Substance-Exposed Newborns
 Substance-Exposed Newborns State of Oklahoma 2016 Substance-Exposed Newborns State of Oklahoma 2016 Legal Background Federal guidelines in the Child Abuse Prevention and Treatment Act (CAPTA) require states
Substance-Exposed Newborns State of Oklahoma 2016 Substance-Exposed Newborns State of Oklahoma 2016 Legal Background Federal guidelines in the Child Abuse Prevention and Treatment Act (CAPTA) require states
FLORIDA S NO WRONG DOOR (NWD) SYSTEM PLANNING PROJECT
 SYSTEM PLANNING PROJECT") FLORIDA S NO WRONG DOOR (NWD) SYSTEM PLANNING PROJECT Agenda No Wrong Door (NWD) Planning Project Update Agencies Inventory Stakeholder Survey Planning and Service Area (PSA) Visits NWD System State Plan
FLORIDA S NO WRONG DOOR (NWD) SYSTEM PLANNING PROJECT Agenda No Wrong Door (NWD) Planning Project Update Agencies Inventory Stakeholder Survey Planning and Service Area (PSA) Visits NWD System State Plan
MERCY HOUSE RESIDENT APPLICATION FORM
 MERCY HOUSE RESIDENT APPLICATION FORM PERSONAL INFORMATION Name: Date: Date of Birth: Age: Address: Email: Phone #: (Cell) (Alternitive) Marital status (please circle): Single Engaged Married Separated
MERCY HOUSE RESIDENT APPLICATION FORM PERSONAL INFORMATION Name: Date: Date of Birth: Age: Address: Email: Phone #: (Cell) (Alternitive) Marital status (please circle): Single Engaged Married Separated
WOMEN S HEALTH CLINIC STRATEGIC PLAN
 WOMEN S HEALTH CLINIC STRATEGIC PLAN Introduction Women s Health Clinic (WHC) is a pro-choice, feminist community health centre in Manitoba that offers a wide range of woman-centred services in the 4 key
WOMEN S HEALTH CLINIC STRATEGIC PLAN Introduction Women s Health Clinic (WHC) is a pro-choice, feminist community health centre in Manitoba that offers a wide range of woman-centred services in the 4 key
Suicide Prevention Strategic Plan
 Suicide Prevention Strategic Plan 2019 For more information visit dphhs.mt.gov/suicideprevention 2 Vision Zero suicide in the Big Sky State Mission Our Reduce suicide in Montana through a comprehensive,
Suicide Prevention Strategic Plan 2019 For more information visit dphhs.mt.gov/suicideprevention 2 Vision Zero suicide in the Big Sky State Mission Our Reduce suicide in Montana through a comprehensive,
Research and Best Practices in Domestic Violence. Julie Beck, LMSW Rose Brooks Center, Inc.
 Research and Best Practices in Domestic Violence Julie Beck, LMSW Rose Brooks Center, Inc. Who am I? Former Director of the Bridge Program for Rose Brooks Center, Inc. (8 years) Member of the Family Violence
Research and Best Practices in Domestic Violence Julie Beck, LMSW Rose Brooks Center, Inc. Who am I? Former Director of the Bridge Program for Rose Brooks Center, Inc. (8 years) Member of the Family Violence
Provider Training. Behavioral Health Screening, Referral, and Coding Requirements
 Provider Training Behavioral Health Screening, Referral, and Coding Requirements Training Outline I. Behavioral Health Screening Requirements and Referrals II. Healthy Behaviors Substance and Alcohol Abuse
Provider Training Behavioral Health Screening, Referral, and Coding Requirements Training Outline I. Behavioral Health Screening Requirements and Referrals II. Healthy Behaviors Substance and Alcohol Abuse
handouts for women 1. Self-test for depression symptoms in pregnancy and postpartum Edinburgh postnatal depression scale (epds) 2
 2") handouts for women 1. Self-test for depression symptoms in pregnancy and postpartum Edinburgh postnatal depression scale (epds) 2 2. The Cognitive-Behaviour Therapy model of depression 4 3. Goal setting
handouts for women 1. Self-test for depression symptoms in pregnancy and postpartum Edinburgh postnatal depression scale (epds) 2 2. The Cognitive-Behaviour Therapy model of depression 4 3. Goal setting
Journey to Truth Counseling
 ADULT / COUPLE INTAKE FORM (Please Print) Date: / / Social Security # Date of birth: Age: Mr. Ms. Dr. Mrs. Miss. Rev. Full Name (Last) (First) (Middle) Parent/Guardian/Power of Attorney: (if applicable)
ADULT / COUPLE INTAKE FORM (Please Print) Date: / / Social Security # Date of birth: Age: Mr. Ms. Dr. Mrs. Miss. Rev. Full Name (Last) (First) (Middle) Parent/Guardian/Power of Attorney: (if applicable)
Making the Connection: County Mental Health, Community Providers, and Other Campuses
 Making the Connection: County Mental Health, Community Providers, and Other Campuses Sally Jue, MSW, Facilitator Michele Renfrow, Clinical Psychologist, Resource Navigation and Crisis Specialist Sylvia
Making the Connection: County Mental Health, Community Providers, and Other Campuses Sally Jue, MSW, Facilitator Michele Renfrow, Clinical Psychologist, Resource Navigation and Crisis Specialist Sylvia
HIV Prevention Service Provider Survey 2014
 Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
Respondent Demographics This survey will help the Florida HIV Prevention Planning Group (PPG) establish the resources and unmet needs of the communities we serve. Please take a few minutes to complete
An Introduction to Southern Nevada's Homeless Continuum of Care and Regional Plan to end homelessness
 An Introduction to Southern Nevada's Homeless Continuum of Care and Regional Plan to end homelessness Today you will leave with An understanding of homelessness in Southern NV An understanding of Help
An Introduction to Southern Nevada's Homeless Continuum of Care and Regional Plan to end homelessness Today you will leave with An understanding of homelessness in Southern NV An understanding of Help
ACCOUNTABILITY AND QUALITY IMPROVEMENT FOR PERINATAL HEALTH
 ACCOUNTABILITY AND QUALITY IMPROVEMENT FOR PERINATAL HEALTH Attention to health system reforms of the past decade has focused on cost containment through efficiency, choice, and medical necessity controls.
ACCOUNTABILITY AND QUALITY IMPROVEMENT FOR PERINATAL HEALTH Attention to health system reforms of the past decade has focused on cost containment through efficiency, choice, and medical necessity controls.
Washington State Collaborative Oral Health Improvement Plan
 Washington State Collaborative Oral Health Improvement Plan 2009-2014 Prioritization Criteria (non-financial): Strategic Area I: System Infrastructure (Partnerships, Funding, Technology) Goal 1: Mobilize
Washington State Collaborative Oral Health Improvement Plan 2009-2014 Prioritization Criteria (non-financial): Strategic Area I: System Infrastructure (Partnerships, Funding, Technology) Goal 1: Mobilize
APPENDIX 26: RESULTS OF SURVEY OF ANTENATAL AND POSTNATAL MENTAL HEALTH PRIMARY CARE SERVICES IN ENGLAND AND WALES
 APPENDIX 26: RESULTS OF SURVEY OF ANTENATAL AND POSTNATAL MENTAL HEALTH PRIMARY CARE SERVICES IN ENGLAND AND WALES Background In order to inform the guideline development process, the guideline development
APPENDIX 26: RESULTS OF SURVEY OF ANTENATAL AND POSTNATAL MENTAL HEALTH PRIMARY CARE SERVICES IN ENGLAND AND WALES Background In order to inform the guideline development process, the guideline development
Women s Health Services at UNHS: Increasing Patient Education and Provider Knowledge of Supportive Community Resources.
 Women s Health Services at UNHS: Increasing Patient Education and Provider Knowledge of Supportive Community Resources Nykia Burke General Electric-National Medical Fellowships Primary Care Leadership
Women s Health Services at UNHS: Increasing Patient Education and Provider Knowledge of Supportive Community Resources Nykia Burke General Electric-National Medical Fellowships Primary Care Leadership
Implementing Bright Futures in Your Office. Shilpa Pai, MD FAAP Jeannette Mejias
 Implementing Bright Futures in Your Office Shilpa Pai, MD FAAP Jeannette Mejias Implementing Bright Futures In-depth look at pre-visit forms QIDA Quality Improvement Data Aggregation Data points to be
Implementing Bright Futures in Your Office Shilpa Pai, MD FAAP Jeannette Mejias Implementing Bright Futures In-depth look at pre-visit forms QIDA Quality Improvement Data Aggregation Data points to be
LOOKING FORWARD: 2017 UPDATE ON ORAL HEALTH IN MICHIGAN
 LOOKING FORWARD: 2017 UPDATE ON ORAL HEALTH IN MICHIGAN LOOKING FORWARD: 2017 ORAL HEALTH UPDATE If you want to go fast, go alone. If you want to go far, go together. -African Proverb OBJECTIVES 1. Overview
LOOKING FORWARD: 2017 UPDATE ON ORAL HEALTH IN MICHIGAN LOOKING FORWARD: 2017 ORAL HEALTH UPDATE If you want to go fast, go alone. If you want to go far, go together. -African Proverb OBJECTIVES 1. Overview
ADULT INTAKE QUESTIONNAIRE. Ok to leave message? Yes No. Present psychological difficulties please check any that apply to you at this time.
 ADULT INTAKE QUESTIONNAIRE Name: Today s Date: Age: Date of Birth: Address: Home phone: Work phone: Cell phone: Ok to leave message? Yes No Ok to leave message? Yes No Ok to leave message? Yes No Email:
ADULT INTAKE QUESTIONNAIRE Name: Today s Date: Age: Date of Birth: Address: Home phone: Work phone: Cell phone: Ok to leave message? Yes No Ok to leave message? Yes No Ok to leave message? Yes No Email:
Are You Ready to Sail. February 11, 2016
 Are You Ready to Sail your SHIP?! February 11, 2016 Acknowledgement and Disclaimer This webinar was supported by funds made available from the Centers for Disease Control and Prevention, Office for State,
Are You Ready to Sail your SHIP?! February 11, 2016 Acknowledgement and Disclaimer This webinar was supported by funds made available from the Centers for Disease Control and Prevention, Office for State,
City of Lawrence 2010 Alcohol Tax Funds Request for Proposals Calendar Year 2010 ( January December) Cover Page
 Cover Page") City of Lawrence 2010 Alcohol Tax Funds Request for Proposals Calendar Year 2010 ( January December) Cover Page Agency Name: Program Name: Contact Person: DCCCA, Inc First Step at Lake View Lisa Carter,
City of Lawrence 2010 Alcohol Tax Funds Request for Proposals Calendar Year 2010 ( January December) Cover Page Agency Name: Program Name: Contact Person: DCCCA, Inc First Step at Lake View Lisa Carter,
Moms Help Organization Helping Moms to be the best Moms they can be! West Sample Road, #24 Coral Springs, FL
 Moms Help Organization Helping Moms to be the best Moms they can be! 11471 West Sample Road, #24 Coral Springs, FL 33065 www.momshelp.org Application for Assistance Welcome to the Moms Help Organization.
Moms Help Organization Helping Moms to be the best Moms they can be! 11471 West Sample Road, #24 Coral Springs, FL 33065 www.momshelp.org Application for Assistance Welcome to the Moms Help Organization.
LPHA Contractor: Wright County Health Department. LPHA Administrator/Director or Designee: Tracy Hardcastle. Report Prepared By:
 LPHA Contractor: Wright County Health Department LPHA Administrator/Director or Designee: Tracy Hardcastle Report Prepared By: Contact Telephone Number: Date: 1. Please describe (summarize) the methodology
LPHA Contractor: Wright County Health Department LPHA Administrator/Director or Designee: Tracy Hardcastle Report Prepared By: Contact Telephone Number: Date: 1. Please describe (summarize) the methodology
PLANNED PARENTHOOD ADVOCATES OF MICHIGAN 2018 CANDIDATE QUESTIONNAIRE
 PLANNED PARENTHOOD ADVOCATES OF MICHIGAN 2018 CANDIDATE QUESTIONNAIRE Planned Parenthood Advocates of Michigan (PPAM) is the advocacy arm of Planned Parenthood in Michigan. We are committed to ensuring
PLANNED PARENTHOOD ADVOCATES OF MICHIGAN 2018 CANDIDATE QUESTIONNAIRE Planned Parenthood Advocates of Michigan (PPAM) is the advocacy arm of Planned Parenthood in Michigan. We are committed to ensuring
Prince George s County Health Department Health Report Findings
 Prince George s County Health Department 2018 Health Report Findings Our Residents Socioeconomic Factors Compared to Maryland, Prince George s residents: have a higher median household income, are employed
Prince George s County Health Department 2018 Health Report Findings Our Residents Socioeconomic Factors Compared to Maryland, Prince George s residents: have a higher median household income, are employed
Building a Comprehensive, Community-driven Prevention Approach to the Opioid Crisis in Maine
 Building a Comprehensive, Community-driven Prevention Approach to the Opioid Crisis in Maine Scott M. Gagnon, MPP, PS-C Director, AdCare Educational Institute of Maine, Inc. Co-Chair, Prevention & Harm
Building a Comprehensive, Community-driven Prevention Approach to the Opioid Crisis in Maine Scott M. Gagnon, MPP, PS-C Director, AdCare Educational Institute of Maine, Inc. Co-Chair, Prevention & Harm
NCACH RAPID CYCLE APPLICATION: OPIOID PROJECT North Central Accountable Community of Health - Medicaid Transformation Project
 NCACH RAPID CYCLE APPLICATION: OPIOID PROJECT North Central Accountable Community of Health - Introduction The North Central Accountable Community of Health (NCACH) is accepting applications from partners
NCACH RAPID CYCLE APPLICATION: OPIOID PROJECT North Central Accountable Community of Health - Introduction The North Central Accountable Community of Health (NCACH) is accepting applications from partners
PROCEDURES AND GUIDANCE
 PROCEDURES AND GUIDANCE Working with Substance Misusing Parents and those who come into Regular Contact with Children and Young People Date of original document July 2009 Date document reviewed April 2016
PROCEDURES AND GUIDANCE Working with Substance Misusing Parents and those who come into Regular Contact with Children and Young People Date of original document July 2009 Date document reviewed April 2016
Postnatal Depression in New Zealand and Feedback on Maternal Mental Health Services
 Postnatal Depression in New Zealand and Feedback on Maternal Mental Health Services Author: Kristina Paterson Published by: Mothers Helpers, 2015 First Survey of Mothers with Postnatal Depression From
Postnatal Depression in New Zealand and Feedback on Maternal Mental Health Services Author: Kristina Paterson Published by: Mothers Helpers, 2015 First Survey of Mothers with Postnatal Depression From
Response to the Language Equality and Acquisition for Deaf Kids (LEAD-K) Task Force Report
 Task Force Report") Response to the Language Equality and Acquisition for Deaf Kids (LEAD-K) Task Force Report Louisiana Department of Health Office of Public Health March 21, 2019 Report Title Version Number Version Date
Response to the Language Equality and Acquisition for Deaf Kids (LEAD-K) Task Force Report Louisiana Department of Health Office of Public Health March 21, 2019 Report Title Version Number Version Date
How to Design a Tobacco Cessation Insurance Benefit
 How to Design a Tobacco Cessation Insurance Benefit All tobacco users need access to a comprehensive tobacco cessation benefit to help them quit. A comprehensive tobacco cessation benefit includes: Nicotine
How to Design a Tobacco Cessation Insurance Benefit All tobacco users need access to a comprehensive tobacco cessation benefit to help them quit. A comprehensive tobacco cessation benefit includes: Nicotine
Ending HIV/AIDS in Southwest Minnesota
 Ending HIV/AIDS in Southwest Minnesota SUMMARY OF REGIONAL STAKEHOLDER INPUT July 2018 Prepared by Wilder Research ENDING HIV/AIDS IN SOUTHWEST MINNESOT A Ending HIV/AIDS in Southwest Minnesota Minnesota
Ending HIV/AIDS in Southwest Minnesota SUMMARY OF REGIONAL STAKEHOLDER INPUT July 2018 Prepared by Wilder Research ENDING HIV/AIDS IN SOUTHWEST MINNESOT A Ending HIV/AIDS in Southwest Minnesota Minnesota
New Jersey Department of Human Services Quarterly Newsletter Division of Mental Health Services June 2006
 Dear Mental Health Community, On February 10, 2006, the Division of Mental Health Services released a Wellness and Recovery Transformation Statement guiding the direction for future activities of New Jersey
Dear Mental Health Community, On February 10, 2006, the Division of Mental Health Services released a Wellness and Recovery Transformation Statement guiding the direction for future activities of New Jersey
Excerpt from Interim Report Health of Houston Survey 2010
 Excerpt from 2008-09 Interim Report July 2009 Assessing Health Information Priorities of Stakeholders and Community Groups in Houston STAKEHOLDER AND COMMUNITY GROUP ENGAGEMENT One of the central goals
Excerpt from 2008-09 Interim Report July 2009 Assessing Health Information Priorities of Stakeholders and Community Groups in Houston STAKEHOLDER AND COMMUNITY GROUP ENGAGEMENT One of the central goals
OUTPATIENT & RESIDENTIAL
 Substance Abuse OUTPATIENT & RESIDENTIAL SUBSTANCE ABUSE FACILITIES FOR PREGNANT & PARENTING WOMEN A Resource Guide for Providers Residential and Outpatient Substance Abuse Treatment Facilities in Philadelphia
Substance Abuse OUTPATIENT & RESIDENTIAL SUBSTANCE ABUSE FACILITIES FOR PREGNANT & PARENTING WOMEN A Resource Guide for Providers Residential and Outpatient Substance Abuse Treatment Facilities in Philadelphia
Strategic Plan
 2017-18 Strategic Plan 1 Strategic Planning Process The Summit County Opiate Task Force has made great strides in addressing the opiate crisis in the last few years. More than 100 Summit County citizens
2017-18 Strategic Plan 1 Strategic Planning Process The Summit County Opiate Task Force has made great strides in addressing the opiate crisis in the last few years. More than 100 Summit County citizens
Policy 61 Summary Report Page 1 of 5
 Policy 61 Summary Report Page 1 of 5 Summary of the ALA Task Force Survey on ALA Policy 61 Library Services for the Poor Policy 61 states: The American Library Association promotes equal access to information
Policy 61 Summary Report Page 1 of 5 Summary of the ALA Task Force Survey on ALA Policy 61 Library Services for the Poor Policy 61 states: The American Library Association promotes equal access to information
Keeping In Touch M A Y
 Inside this edition UNDERSTANDING DEPRESSION E d u c a t i o n a l & D e v e l o p m e n t a l I n t e r v e n t i o n S e r v i c e s ( E D I S ) Pe r s o n n e l D e v e l o p m e n t Resource 1 Article
Inside this edition UNDERSTANDING DEPRESSION E d u c a t i o n a l & D e v e l o p m e n t a l I n t e r v e n t i o n S e r v i c e s ( E D I S ) Pe r s o n n e l D e v e l o p m e n t Resource 1 Article
Mood Disorders Society of Canada Mental Health Care System Study Summary Report
 Mood Disorders Society of Canada Mental Health Care System Study Summary Report July 2015 Prepared for the Mood Disorders Society of Canada by: Objectives and Methodology 2 The primary objective of the
Mood Disorders Society of Canada Mental Health Care System Study Summary Report July 2015 Prepared for the Mood Disorders Society of Canada by: Objectives and Methodology 2 The primary objective of the
Effective Strategies for Addressing the Needs of Substance Exposed Newborns & their Families Dixie L. Morgese, BA, CAP, ICADC.
 Effective Strategies for Addressing the Needs of Substance Exposed Newborns & their Families Dixie L. Morgese, BA, CAP, ICADC Key Issues Significant increase in number of pregnant women addicted to prescription
Effective Strategies for Addressing the Needs of Substance Exposed Newborns & their Families Dixie L. Morgese, BA, CAP, ICADC Key Issues Significant increase in number of pregnant women addicted to prescription
National Center on Substance Abuse
 National Center on Substance Abuse and Child Welfare Bringing Systems Together for Family Recovery, Safety and Stability September 24, 2009 Presented by: Cathleen Otero, MSW, MPA Deputy Director, NCSACW
National Center on Substance Abuse and Child Welfare Bringing Systems Together for Family Recovery, Safety and Stability September 24, 2009 Presented by: Cathleen Otero, MSW, MPA Deputy Director, NCSACW
Peripartum Depression:
 Peripartum Depression: Organizing a Statewide System of Care Laura J. Miller MD Women s Mental Health Program University of Illinois at Chicago Peripartum depression (PPD) in Illinois In 2001, several
Peripartum Depression: Organizing a Statewide System of Care Laura J. Miller MD Women s Mental Health Program University of Illinois at Chicago Peripartum depression (PPD) in Illinois In 2001, several
Working with Public Officials
 Working with Public Officials Obtaining an official Resolution, Citation or Proclamation from a government body or official can bring a good bit of recognition to the work you're doing for Children's Grief
Working with Public Officials Obtaining an official Resolution, Citation or Proclamation from a government body or official can bring a good bit of recognition to the work you're doing for Children's Grief
Perinatal Health Strategic Plan Update
 Perinatal Health Strategic Plan Update Background and process Perinatal Health Committee, Child Fatality Task Force Preconception Health Strategic Plan Equity in Birth Outcomes Council CoIIN (Collaborative
Perinatal Health Strategic Plan Update Background and process Perinatal Health Committee, Child Fatality Task Force Preconception Health Strategic Plan Equity in Birth Outcomes Council CoIIN (Collaborative
The Blues Prior, During and After Labor: Es Dificil ser Mujer? The Health Education Action for Latinas (HEAL) Model
 Model") The Blues Prior, During and After Labor: Es Dificil ser Mujer? The Health Education Action for Latinas (HEAL) Model Maria Lourdes F. Reyes, MD, MPH Director of California programs, PCI National Healthy
The Blues Prior, During and After Labor: Es Dificil ser Mujer? The Health Education Action for Latinas (HEAL) Model Maria Lourdes F. Reyes, MD, MPH Director of California programs, PCI National Healthy
Certified Nurse-Midwives' Beliefs About and Screening Practices for Postpartum Depression: A Descriptive Study
 University of Connecticut DigitalCommons@UConn School of Nursing Scholarly Works School of Nursing 5-22-2006 Certified Nurse-Midwives' Beliefs About and Screening Practices for Postpartum Depression: A
University of Connecticut DigitalCommons@UConn School of Nursing Scholarly Works School of Nursing 5-22-2006 Certified Nurse-Midwives' Beliefs About and Screening Practices for Postpartum Depression: A
Survey Instrument. Appendix B
 Appendix B Survey Instrument As part of the 1992 assessment Cystic Fibrosis and DNA Tests: Implications of Carrier Screening, OTA surveyed the summer 1991 memberships of the International Society of Nurses
Appendix B Survey Instrument As part of the 1992 assessment Cystic Fibrosis and DNA Tests: Implications of Carrier Screening, OTA surveyed the summer 1991 memberships of the International Society of Nurses
This report examines the demographics and risk factors associated with maternal depression. It looks at the current
 Landscape Report August 2009 Maternal Depression in Los Angeles County: Current Screening Practices and Recommendations I. Introduction and Overview This report examines the demographics and risk factors
Landscape Report August 2009 Maternal Depression in Los Angeles County: Current Screening Practices and Recommendations I. Introduction and Overview This report examines the demographics and risk factors
PSYCHOLOGIST-PATIENT SERVICES
 PSYCHOLOGIST-PATIENT SERVICES PSYCHOLOGICAL SERVICES Welcome to my practice. Because you will be putting a good deal of time and energy into therapy, you should choose a psychologist carefully. I strongly
PSYCHOLOGIST-PATIENT SERVICES PSYCHOLOGICAL SERVICES Welcome to my practice. Because you will be putting a good deal of time and energy into therapy, you should choose a psychologist carefully. I strongly
Priority Area: 1 Access to Oral Health Care
 If you are unable to attend one of the CHARTING THE COURSE: Developing the Roadmap to Advance Oral Health in New Hampshire meetings but would like to inform the Coalition of activities and services provided
If you are unable to attend one of the CHARTING THE COURSE: Developing the Roadmap to Advance Oral Health in New Hampshire meetings but would like to inform the Coalition of activities and services provided
FASD Prevention and Health Promotion Resources
 FASD PREVENTION AND HEALTH PROMOTION RESOURCES FASD Prevention and Health Promotion Resources Module 3 Monitoring and Evaluating August 2017 Review Module 1: What is FASD? Module 1 aimed to increase: i.
FASD PREVENTION AND HEALTH PROMOTION RESOURCES FASD Prevention and Health Promotion Resources Module 3 Monitoring and Evaluating August 2017 Review Module 1: What is FASD? Module 1 aimed to increase: i.
Children and AIDS Fourth Stocktaking Report 2009
 Children and AIDS Fourth Stocktaking Report 2009 The The Fourth Fourth Stocktaking Stocktaking Report, Report, produced produced by by UNICEF, UNICEF, in in partnership partnership with with UNAIDS, UNAIDS,
Children and AIDS Fourth Stocktaking Report 2009 The The Fourth Fourth Stocktaking Stocktaking Report, Report, produced produced by by UNICEF, UNICEF, in in partnership partnership with with UNAIDS, UNAIDS,
FAMILIES IN HEALING - GUIDE FOR WOMEN RETURNING HOME AFTER AFE
 FAMILIES IN HEALING - GUIDE FOR WOMEN RETURNING HOME AFTER AFE If you have a loved one who has experienced amniotic fluid embolism (AFE) and they are about to or have returned home, we are here to help.
FAMILIES IN HEALING - GUIDE FOR WOMEN RETURNING HOME AFTER AFE If you have a loved one who has experienced amniotic fluid embolism (AFE) and they are about to or have returned home, we are here to help.
Outreach and Working With Your PEDIATRICIAN
 Outreach and Working With Your PEDIATRICIAN Studies show you get only about 15 minutes of face time with your pediatrician during an average well visit Finding A Pediatrician When trying to find local
Outreach and Working With Your PEDIATRICIAN Studies show you get only about 15 minutes of face time with your pediatrician during an average well visit Finding A Pediatrician When trying to find local
Early Childhood Mental Health and Homelessness
 Issue Brief No. 1 September, 2013 Early Childhood Mental Health and Homelessness A Brief Overview of Family Homelessness The United States has the highest number of children who experience homelessness
Issue Brief No. 1 September, 2013 Early Childhood Mental Health and Homelessness A Brief Overview of Family Homelessness The United States has the highest number of children who experience homelessness
Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health
 Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health Columbus, Ohio Assignment Description The rapid advance of the opiate crisis has had far
Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health Columbus, Ohio Assignment Description The rapid advance of the opiate crisis has had far
Recognizing Racial Ethnic Disparities in Maternity Care
 Recognizing Racial Ethnic Disparities in Maternity Care Louise Marie Roth, PhD Associate Professor of Sociology, University of Arizona Racial-Ethnic Disparities in Health Outcomes Black Americans suffer
Recognizing Racial Ethnic Disparities in Maternity Care Louise Marie Roth, PhD Associate Professor of Sociology, University of Arizona Racial-Ethnic Disparities in Health Outcomes Black Americans suffer
: STATE OF COLORADO. Colorado Department of Public Health. and Environment. May 20,2009. Dear Colleague,
 v Bill Ritter, Jr., Governor James B. Martin, Executive Director Dedicated to protecting and improving the health and environment of the people of Colorado 4300 Cherry Creek Dr. S. Laboratory Services
v Bill Ritter, Jr., Governor James B. Martin, Executive Director Dedicated to protecting and improving the health and environment of the people of Colorado 4300 Cherry Creek Dr. S. Laboratory Services
Policy brief 6. Integrating mental health into maternal care in South Africa. Perinatal Mental Health Project. Mental Health and Poverty Project
 Perinatal Mental Health Project Policy brief 6 Integrating mental health into maternal care in South Africa Caring for Mothers Caring for the Future Mental Health and Poverty Project Improving mental health,
Perinatal Mental Health Project Policy brief 6 Integrating mental health into maternal care in South Africa Caring for Mothers Caring for the Future Mental Health and Poverty Project Improving mental health,
Welcoming Services and Service Coordination for Women with SUD and/or Co-occurring Disorders
 FLORIDA CERTIFICATION BOARD Supervision Key The successful application of knowledge to practice is one of the most-needed and desired outcomes for behavioral health professionals, and others, involved
FLORIDA CERTIFICATION BOARD Supervision Key The successful application of knowledge to practice is one of the most-needed and desired outcomes for behavioral health professionals, and others, involved
natal Marijuana and Public Health: The Colorado Perspective
 natal Marijuana and Public Health: The Colorado Perspective Larry Wolk, MD MSPH Executive Director and CMO September 2015 1 natal 2 natal CDPHE Role Medical Marijuana Registry Medical Marijuana Research
natal Marijuana and Public Health: The Colorado Perspective Larry Wolk, MD MSPH Executive Director and CMO September 2015 1 natal 2 natal CDPHE Role Medical Marijuana Registry Medical Marijuana Research
IMPORTANT HEALTH INFORMATION
 IMPORTANT HEALTH INFORMATION SU-6523MI Page 1 of 8 Table of Contents Page What is an HIV test?..........................................1 Will the HIV test tell me if I have AIDS?............................1
IMPORTANT HEALTH INFORMATION SU-6523MI Page 1 of 8 Table of Contents Page What is an HIV test?..........................................1 Will the HIV test tell me if I have AIDS?............................1
Perinatal Depression For GA22
 For GA22 Who WIC Participants Why WIC Time 5-10 minutes Setup Chairs in clusters of 2 or 3. White board and pens Objectives By the end of this session, participants will: Identify the importance of attachment
For GA22 Who WIC Participants Why WIC Time 5-10 minutes Setup Chairs in clusters of 2 or 3. White board and pens Objectives By the end of this session, participants will: Identify the importance of attachment
Psychotherapy Services
 Psychotherapy Services Available now Free mental health services for people in Ontario experiencing mild to moderate depression and anxiety Funded by the Government of Ontario Meet Sarah. Sarah is 30
Psychotherapy Services Available now Free mental health services for people in Ontario experiencing mild to moderate depression and anxiety Funded by the Government of Ontario Meet Sarah. Sarah is 30
Center for Autism and Related Disabilities (CARD)
") Center for Autism and Related Disabilities (CARD) Providing Support and Assistance to Optimize Potential Dear Parents, Thank you for referring your child to the Center for Autism and Related Disabilities
Center for Autism and Related Disabilities (CARD) Providing Support and Assistance to Optimize Potential Dear Parents, Thank you for referring your child to the Center for Autism and Related Disabilities
Creating a Safety Net for HIV Exposed Infants in Illinois
 Creating a Safety Net for HIV Exposed Infants in Illinois Perinatal HIV Elimination Project Anne Statton BA, Laurie Ayala MPH, Yolanda Olszewski MS MPH National HIV Prevention Conference December 3, 2007
Creating a Safety Net for HIV Exposed Infants in Illinois Perinatal HIV Elimination Project Anne Statton BA, Laurie Ayala MPH, Yolanda Olszewski MS MPH National HIV Prevention Conference December 3, 2007
Babies in Emergency Housing
 Babies in Emergency Housing Is Philadelphia Doing All That It Should? Sara Shaw, Joe Willard June, 2016 Introduction More and more families are experiencing homelessness in Philadelphia. Some 1,500 families
Babies in Emergency Housing Is Philadelphia Doing All That It Should? Sara Shaw, Joe Willard June, 2016 Introduction More and more families are experiencing homelessness in Philadelphia. Some 1,500 families
Lorain County Community Health Improvement Plan Annual report
 Lorain County Community Health Improvement Plan 2017 Annual report Completed July 2, 2018 Introduction In December 2012, partner agencies used data from the 2011 Lorain County Community Health Assessment
Lorain County Community Health Improvement Plan 2017 Annual report Completed July 2, 2018 Introduction In December 2012, partner agencies used data from the 2011 Lorain County Community Health Assessment