PATIENT NAME: FIRST MIDDLE LAST ADDRESS: ADDRESS: PERSON TO NOTIFY IN CASE OF EMERGENCY: RELATIONSHIP: PHONE NUMBER(S):
|
|
|
- Nigel Dennis
- 5 years ago
- Views:
Transcription
1 PATIENT REGISTRATION PATIENT NAME: FIRST MIDDLE LAST INITIALS: (first, middle, last) GENDER: MALE FEMALE (circle one) BIRTHDATE: / / AGE: ADDRESS: HOME PHONE: ( ) - EMPLOYER: CELL/PAGER: ( ) - WORK PHONE: ( ) - ADDRESS: PERSON TO NOTIFY IN CASE OF EMERGENCY: RELATIONSHIP: PHONE NUMBER(S): HOW DID YOU HEAR ABOUT OUR PROGRAM?
2 DEMOGRAPHIC INVENTORY Today s Date / / M M D D Y Y Y Y 1. Race/Ethnicity Ethnicity Hispanic Non-Hispanic Race American Indian or Alaskan Native Asian Black or African American White Native Hawaiian or Other Pacific Islander Other 2. Current marital status (Check one): Single, never married Married, living together Separated Widowed Cohabiting with partner Married, not living together Divorced 3. If you are married or cohabitating with partner, how long has this been? Years Months 4. Number of previous marriages? 5. How many children do you have? 6. TOTAL number of persons including yourself in your household? 7. How many years of formal education have you completed? 8. Highest degree obtained: (Check only one) Years High school graduate M.B.A./M.A./M.S./M.P.H. G.E.D. J.D./LL.B. Junior college degree or M.D. technical school diploma Ph.D. 4 year college degree Other: 9. What best describes your current employment status? (Check one from each category a, b, & c) a. Employment Status b. Student Status c. Volunteer Status Unemployed, not looking for employment Part-time Volunteer Part-time Unemployed, looking for employment Full-time Volunteer Full-time Full-time employed Not a student No Volunteer Work Part-time employed Retired, not working Self-employed for pay
3 10. Type of occupation? (Check only one) Professional specialty Service, except private households & protective Technical and related support Precision production, craft and repair Sales Machine operators, assemblers and inspectors Administrative support, including clerical Transportation and material moving occupations Private Household Handlers, equipment cleaners, helpers and laborers Protective Service Farming, forestry and fishing Spousal Information 11. How many years of formal education has your spouse completed? 12. Highest degree your spouse has obtained: (Check only one) Years High school graduate M.B.A./M.A./M.S./M.P.H. G.E.D. J.D./LL.B. Junior college degree or M.D. technical school diploma Ph.D. 4 year college degree Other: 13. What best describes your spouse s current employment status? (Check one from each a, b, & c) a. Employment Status b. Student Status c. Volunteer Status Unemployed, not looking for employment Part-time Volunteer Part-time Unemployed, looking for employment Full-time Volunteer Full-time Full-time employed Not a student No Volunteer Work Part-time employed Retired, not working Self-employed for pay 14. Spouse s type of occupation? (Check only one) Professional specialty Service, except private households & protective Technical and related support Precision production, craft and repair Sales Machine operators, assemblers and inspectors Administrative support, including clerical Transportation and material moving occupations Private Household Handlers, equipment cleaners, helpers and laborers Protective Service Farming, forestry and fishing Household: income 0 - $24,999 $50,000-$74,999 $100,000+ Zip Code : $25,000-$49,999 $75,000-$99,999 Current residence : What is the major mode of Detached house Retirement complex transportation that you use? Rooming house or hotel or senior housing (check one) Rowhouse or townhouse Healthcare facility Bus/rail system Train Mobile home or nursing home Car Walk Apartment or condominium Homeless
4 MEDICAL & MENTAL HEALTH HISTORY Have you ever had any of the following (check all that apply): Chest pain/pressure/tightening High Blood Pressure Heart attack Stroke Headaches Head injury Paralysis Seizures or Convulsions Memory loss Dizzy Spells Difficulty hearing Asthma Shortness of breath TB / Lung disorder History of cancer or tumors Ulcers Colitis Digestive problems Diabetes Thyroid problems Glaucoma Cataracts Hepatitis (Liver Disease) Anemia Mononucleosis Arthritis Kidney infections Allergies Skin rash Other (list) Please list current or past medications you have taken for the treatment of any medical problem. Medical Problem Medication (name/dose) Start Date Stop Date Currently Taking? What kind of birth control are you using? How much alcohol, including beer, do you drink per week?
5 Mental Health History Have you ever had a problem with any of the following (check all that apply): Depression Anxiety Panic Attacks Post Traumatic Stress Bipolar (Manic / Depressive) Disorder Schizophrenia Alcohol Problems (including AA) Drug Problems Other (list) Please list current or past medications you have taken for treatment of any mental health problem. Problem (e.g. Depression, Anxiety) Medication (name and highest dose) Start Date Stop Date Why stopped (e.g. felt better, didn t help) Has anyone in your family ever been treated for any of the following (check all that apply): Mother Father Aunt Uncle Brother Sister Children Depression Anxiety Panic Attacks Post Traumatic Stress Bipolar (Manic / Depressive) Disorder Schizophrenia Alcohol Problems (including AA) Drug Problems Are you currently seeing a counselor or therapist? Are you having problems concentrating or problems remembering things?
6 Additional Medications Please list any medications you are taking that have not been listed above, including birth control pills, any over the counter medications and herbal remedies (i.e. decongestants, St. John's Wart, vitamins). Medication (name/dose) Start Date Stop Date Physician Medication Allergies Medication (name/dose) Type of Reaction Physical Activity YES NO Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor? YES NO Do you feel pain in your chest when you do physical activity? YES NO In the past month, have you had chest pain when you were doing physical activity? YES NO Do you lose you balance because of dizziness or do you ever lose consciousness? YES NO Do you have a bone or joint problem (for example, back, knee or hip) that could be made worse by a change in your physical activity? YES NO Is you doctor currently prescribing drugs (for example, water pills) for your blood pressure or heart condition? YES NO Do you know of any other reason why you should not do physical activity? How much do you exercise each week?
7 UTSW Antidepressant Treatment History Evaluation Have you taken any of the anti-depressant medications listed below? If yes, please indicated: 1) What dosage did you take? 2) How many weeks did you take the medication? 3) Did it result in 50% reduction of depressive symptoms? 4) Did you have any troubling side effects that made it difficult to take the medication? Anti-Depressant Medication Dose Taken Weeks Taken 50% Reduction in Symptoms Troubling Side Effects Citalopram or CELEXA mg Yes No Yes No Fluoxetine or PROZAC mg Yes No Yes No Paroxetine or PAXIL mg Yes No Yes No Escitalopram or LEXAPRO mg Yes No Yes No Sertraline or ZOLOFT mg Yes No Yes No Paroxetine CR or PAXIL CR mg Yes No Yes No Fluvoxamine or LUVOX mg Yes No Yes No Duloxetine or CYMBALTA mg Yes No Yes No Venlafaxine XR or EFFEXOR XR mg Yes No Yes No Mirtazapine or REMERON mg Yes No Yes No Bupropion or WELLBUTRIN mg Yes No Yes No Nortriptyline or PAMELOR mg Yes No Yes No Protriptyline or VIVACTIL mg Yes No Yes No Amitriptyline or ELAVIL mg Yes No Yes No Amoxapine or MOXADIL mg Yes No Yes No Imipramine or TOFRANIL mg Yes No Yes No Desipramine or NORPRAMINE mg Yes No Yes No Trimipramine or SURMONTIL mg Yes No Yes No Clomipramine or ANAFRAMIL mg Yes No Yes No Maprotilene or LUDIOMIL mg Yes No Yes No Doxepin or SINEQUAN mg Yes No Yes No Nomifensine or MERITAL mg Yes No Yes No Isocarboxazid or MARPLAN mg Yes No Yes No Tranylcypromine or PARNATE mg Yes No Yes No Phenelzine or NARDIL mg Yes No Yes No Trazodone or DESYREL mg Yes No Yes No Nefazodone or SERZONE mg Yes No Yes No Selegiline or EMSAM mg Yes No Yes No
8 DIAGNOSTIC SCREENING QUESTIONNAIRE (DSQ) Name: Age: Gender: M OR F Date: 1. YES NO There have been times when I felt down, depressed, or sad for several weeks in a row. 2. YES NO There have been times when I lost interest or pleasure in things I usually enjoyed, and it lasted for several weeks in a row. If you answered YES to questions 1 or 2, when you felt that way did you also notice. YES NO Not feeling like eating...or the opposite, eating more than usual. YES NO Not getting enough sleep...or the opposite, sleeping too much. YES NO Feeling restless and couldn't sit still...or the opposite, feeling slowed down. YES NO Feeling low in energy or getting tired for no reason. YES NO Feeling guilty most of the time or feeling worthless. YES NO Having trouble concentrating or trouble making decisions. YES NO Thinking that life is not worth living or thinking about dying. YES NO Have you been feeling this way the last 2 weeks? If YES, how long have you felt this way? YES NO Have you felt this way before? If YES, how many times have you felt this way? How old were you when you first felt this way?
9 3. YES NO I have had a period of six months or more when I worried excessively and found it difficult to control my anxiety. If you answered YES to question 3 please answer the following questions. More days than not during the last 6 months: YES NO I worried excessively and found it difficult to control my anxiety. YES NO I felt tense or keyed-up, or felt restless. YES NO I have had trouble concentrating or my mind goes blank at times. YES NO I have felt easily annoyed or irritable. YES NO I have had tense or sore muscles. YES NO I have not been getting enough sleep. 4. YES NO I have had a panic attack when I suddenly felt frightened or anxious or suddenly developed a lot of physical symptoms. The symptoms may have included some of the following: heart pounding or racing, sweating, shaking or trembling, shortness of breath, choking feeling, chest pain, upset stomach, feeling dizzy or faint, feeling spaced-out, fear of losing control, fear of dying, numbness or tingling, chills or hot flushes. If you answered YES to question 4 please answer the following questions. The month after this happened did you: YES NO I had a lot of concern about this happening again. (For example you may have been concerned that if it happened again you might lose control, or have a heart attack.) YES NO I changed what I was doing or where I was going because I was concerned that this might happen again. YES NO This only happens to me in certain situations. Some of the situations are things such as: seeing a snake or a dog; being in a storm; being in high places; going swimming; seeing blood; being in places that are small and enclosed; driving the car; having to talk or perform in front of people; going to crowded places; etc. 5. YES NO I have been bothered by thoughts that did not make any sense and kept coming back even when I tried not to have them. 6. YES NO I cannot resist doing some things over and over again, like washing my hands repeatedly, or checking the same thing repeatedly, or counting things. 7. YES NO I keep thinking about, or dreaming about a traumatic event that involved me or someone I cared about. The event(s) were life threatening, such as a serious accident, a physical assault, or seeing someone killed or badly injured.
10 8. YES NO There have been days when I was feeling so good, high, excited, irritable, or hyper that other people thought I was not my normal self or I got into trouble. 9. YES NO There have been days when I felt so good about myself that I thought I could do just about anything. 10. YES NO There have been times when I only needed a couple of hours of sleep each night. 11. YES NO There have been days when other people noticed that I was talking a lot more than usual. 12. YES NO There have been days when my thoughts seemed to be racing through my head. 13. YES NO There have been days when I was easily distracted and had trouble paying attention. 14. YES NO There have been times when I started so many projects that I could never finish them all. 15. YES NO There have been times when I did a lot or reckless things such as, spending a lot of money on things I didn t need, or getting sexually involved with people I normally would not get involved with. If you answered YES any of the questions 8 through 15, please answer the following questions. YES NO Did this last for more than 4 days in a row? YES NO Did this last for a week or more? YES NO I have felt some of these things in the last week? 16. YES NO I have heard things that other people couldn t hear, such as noises, or the voices of people whispering or talking. 17. YES NO I have seen visions or have seen things that other people couldn t see. 18. YES NO I have had a problem with alcohol or drug use...or my friends, family, or employers have told me they thought I had a problem with alcohol or drug use. Comments:
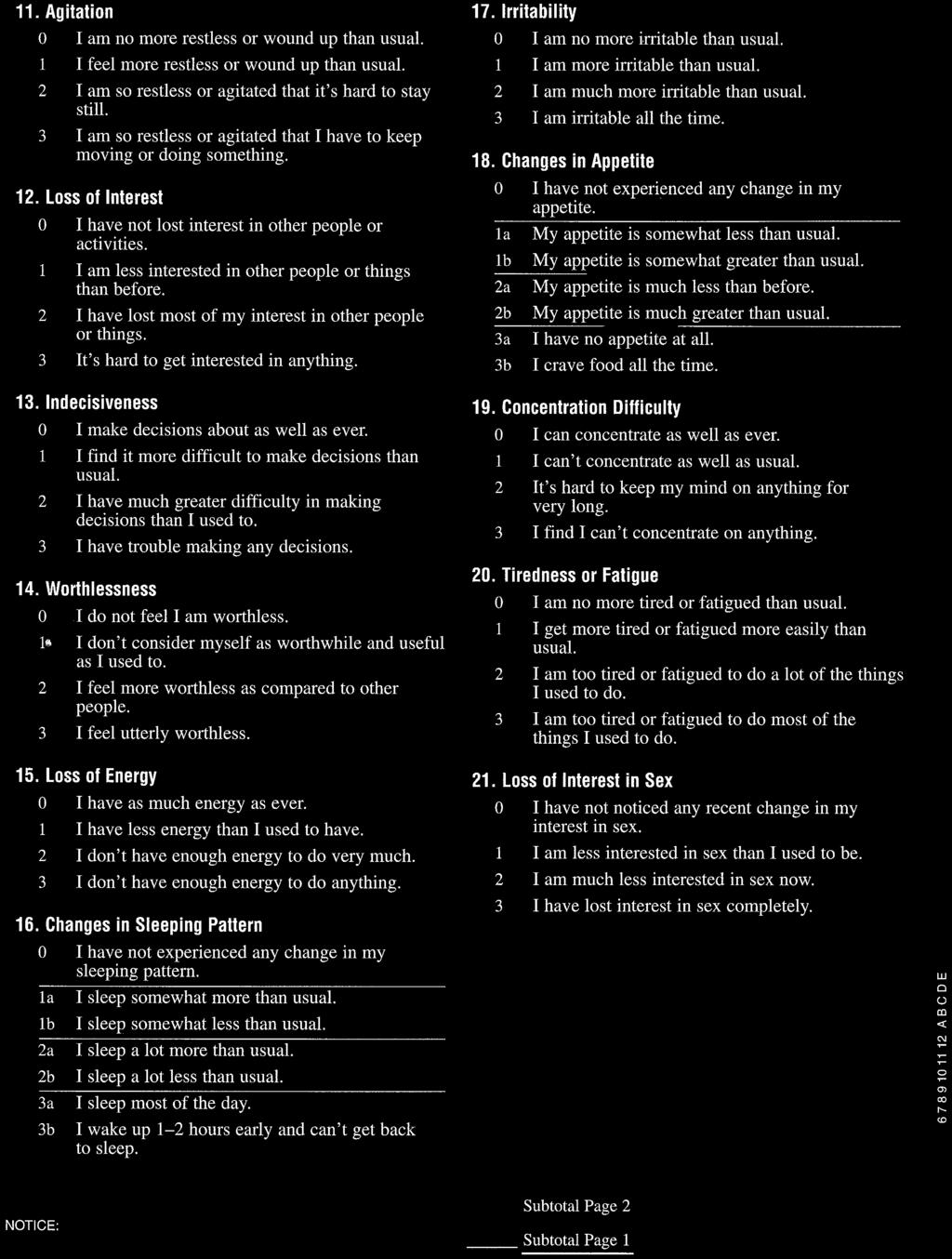
11 QUICK INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY (SELF-REPORT) (QIDS-SR 16 ) Subject ID Date Please circle the one response to each item that best describes you for the past seven days. 1. Falling Asleep: 0 I never take longer than 30 minutes to fall asleep. 1 I take at least 30 minutes to fall asleep, less than half the time. 2 I take at least 30 minutes to fall asleep, more than half the time. 3 I take more than 60 minutes to fall asleep, more than half the time. 2. Sleep During the Night: 0 I do not wake up at night. 1 I have a restless, light sleep with a few brief awakenings each night. 2 I wake up at least once a night, but I go back to sleep easily. 3 I awaken more than once a night and stay awake for 20 minutes or more, more than half the time. 6. Decreased Appetite: 0 There is no change in my usual appetite. 1 I eat somewhat less often or lesser amounts of food than usual. 2 I eat much less than usual and only with personal effort. 3 I rarely eat within a 24-hour period, and only with extreme personal effort or when others persuade me to eat. 7. Increased Appetite: 0 There is no change from my usual appetite. 1 I feel a need to eat more frequently than usual. 2 I regularly eat more often and/or greater amounts of food than usual. 3 I feel driven to overeat both at mealtime and between meals. 3. Waking Up Too Early: 0 Most of the time, I awaken no more than 30 minutes before I need to get up. 1 More than half the time, I awaken more than 30 minutes before I need to get up. 2 I almost always awaken at least one hour or so before I need to, but I go back to sleep eventually. 3 I awaken at least one hour before I need to, and can't go back to sleep. 4. Sleeping Too Much: 0 I sleep no longer than 7-8 hours/night, without napping during the day. 1 I sleep no longer than 10 hours in a 24-hour period including naps. 2 I sleep no longer than 12 hours in a 24-hour period including naps. 3 I sleep longer than 12 hours in a 24-hour period including naps. 5. Feeling Sad: 0 I do not feel sad 1 I feel sad less than half the time. 2 I feel sad more than half the time. 3 I feel sad nearly all of the time. 8. Decreased Weight (Within the Last Two Weeks): 0 I have not had a change in my weight. 1 I feel as if I've had a slight weight loss. 2 I have lost 2 pounds or more. 3 I have lost 5 pounds or more. 9. Increased Weight (Within the Last Two Weeks): 0 I have not had a change in my weight. 1 I feel as if I've had a slight weight gain. 2 I have gained 2 pounds or more. 3 I have gained 5 pounds or more. 10. Concentration/Decision Making: 0 There is no change in my usual capacity to concentrate or make decisions. 1 I occasionally feel indecisive or find that my attention wanders. 2 Most of the time, I struggle to focus my attention or to make decisions. 3 I cannot concentrate well enough to read or cannot make even minor decisions.
12 11. View of Myself: 0 I see myself as equally worthwhile and deserving as other people. 1 I am more self-blaming than usual. 2 I largely believe that I cause problems for others. 3 I think almost constantly about major and minor defects in myself. 12. Thoughts of Death or Suicide: 0 I do not think of suicide or death. 1 I feel that life is empty or wonder if it's worth living. 2 I think of suicide or death several times a week for several minutes. 3 I think of suicide or death several times a day in some detail, or I have made specific plans for suicide or have actually tried to take my life. 13. General Interest: 0 There is no change from usual in how interested I am in other people or activities. 1 I notice that I am less interested in people or activities. 2 I find I have interest in only one or two of my formerly pursued activities. 3 I have virtually no interest in formerly pursued activities. 14. Energy Level: 0 There is no change in my usual level of energy. 1 I get tired more easily than usual. 2 I have to make a big effort to start or finish my usual daily activities (for example, shopping, homework, cooking or going to work). 3 I really cannot carry out most of my usual daily activities because I just don't have the energy. 15. Feeling slowed down: 0 I think, speak, and move at my usual rate of speed. 1 I find that my thinking is slowed down or my voice sounds dull or flat. 2 It takes me several seconds to respond to most questions and I'm sure my thinking is slowed. 3 I am often unable to respond to questions without extreme effort. 16. Feeling restless: 0 I do not feel restless. 1 I'm often fidgety, wringing my hands, or need to shift how I am sitting. 2 I have impulses to move about and am quite restless. 3 At times, I am unable to stay seated and need to pace around. To Score: 1. Enter the highest score on any 1 of the 4 sleep items (1-4) 2. Item 5 3. Enter the highest score on any 1 appetite/ weight item (6-9) 4. Item Item Item Item Item Enter the highest score on either of the 2 psychomotor items (15 and 16) TOTAL SCORE (Range 0-27)
13 National Network of Depression Centers Common Assessment Package: Self-Rated Patient Health Questionnaire (PHQ-9) Instructions: Please circle one number for each statement. Over the last 2 weeks, how often have you been bothered by any of the following problems? 1. Little interest or pleasure in doing things 2. Feeling down, depressed, or hopeless 3. Trouble falling or staying asleep, or sleeping too much 4. Feeling tired or having little energy 5. Poor appetite or overeating 6. Feeling bad about yourself- or that you are a failure or have let yourself or your family down 7. Trouble concentrating on things, such as reading the newspaper or watching television 8. Moving or speaking so slowly that other people could have noticed. Or the opposite being so fidgety or restless that you have been moving around a lot more than usual. 9. Thoughts that you would be better off dead, or of hurting yourself. Not at all Several days More than half the days Nearly every day 10. If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people? Not difficult at all Somewhat difficult Very difficult Extremely difficult PHQ-9 Copyright 1999 Pfizer Inc. All rights reserved. NNDC Common Assessment Package: Self-Rated (January 25, 2011)
14 National Network of Depression Centers Common Assessment Package: Self-Rated Generalized Anxiety Disorder Scale (GAD-7) Instructions: Please circle one number for each statement. Over the last 2 weeks, how often have you been bothered by any of the following problems? Not at all Several days More than half the days Nearly every day 1. Feeling nervous, anxious, or on edge 2. Not being able to stop or control worrying 3. Worrying too much about different things 4. Trouble relaxing 5. Being so restless it is hard to sit still 6. Becoming easily annoyed or irritable 7. Feeling afraid as if something awful might happen If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people? Not difficult at all Somewhat difficult Very difficult Extremely difficult Spitzer RL, Kroenke K, Williams JBW, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Intern Med 2006;166: Arch NNDC Common Assessment Package: Self-Rated (January 25, 2011)
15 National Network of Depression Centers Common Assessment Package: Self-Rated Altman Self-Rating Mania Scale (ASRM) Instructions: On this questionnaire are groups of 5 statements; read each group of statements carefully. Choose the one statement in each group that best describes the way you have been feeling for the past week. Circle the number next to the statement you picked. Please note: The word occasionally when used here means once or twice;; often means several times or more;; frequently means most of the time ) I do not feel happier or more cheerful than usual. 2) I occasionally feel happier or more cheerful than usual. 3) I often feel happier or more cheerful than usual. 4) I feel happier or more cheerful than usual most of the time. 5) I feel happier or more cheerful than usual all of the time. 1) I do not feel more self-confident than usual. 2) I occasionally feel more self-confident than usual. 3) I often feel more self-confident than usual. 4) I feel more self-confident than usual most of the time. 5) I feel extremely self-confident all of the time. 1) I do not need less sleep than usual. 2) I occasionally need less sleep than usual. 3) I often need less sleep than usual. 4) I frequently need less sleep than usual. 5) I can go all day or night without any sleep and still not feel tired. 1) I do not talk more than usual. 2) I occasionally talk more than usual. 3) I often talk more than usual. 4) I frequently talk more than usual. 5) I talk constantly and cannot be interrupted. 1) I have not been more active (either socially, sexually, at work, home or school) than usual. 2) I have occasionally been more active than usual. 3) I have often been more active than usual. 4) I have frequently been more active than usual. 5) I am constantly active or on the go all the time. NNDC Common Assessment Package: Self-Rated (January 25, 2011)
16 National Network of Depression Centers Common Assessment Package: Self-Rated (Baseline) Work and Social Adjustment Scale (WSAS) Instructions: Rate each of the following questions on a 0 to 8 scale: 0 indicates no impairment at all and 8 indicates very severe impairment. Please circle your responses below. 1. Because of my mood problems, my ability to work is impaired. 0 means not at all impaired and 8 means very severely impaired to the point I can t work Because of my mood problems, my home management (cleaning, tidying, shopping, cooking, looking after home or children, paying bills) is impaired. 0 means not at all impaired and 8 means very severely impaired Because of my mood problems, my social leisure activities (with other people, such as parties, bars, clubs, outings, visits, dating, home entertainment) are impaired. 0 means not at all impaired and 8 means very severely impaired Because of my mood problems, my private leisure activities (done alone, such as reading, gardening, collecting, sewing, walking alone) are impaired. 0 means not at all impaired and 8 means very severely impaired Because of my mood problems, my ability to form and maintain close relationships with others, including those I live with, is impaired. 0 means not at all impaired and 8 means very severely impaired Mundt, J.C., Marks, I.M., Shear, M.K., & Greist, J.H. (2002). The Work and Social Adjustment Scale: a simple measure of impairment in functioning. Br J Psychiatry, 180, NNDC Common Assessment Package, Baseline: Self-Rated (February 14, 2011)

17
18
USF Mood & Anxiety Disorders Program
 QUICK INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY (SELF-REPORT)(QIDS-SR16) Please circle the one response to each item that best describes you for the past seven days. 1. Falling Asleep: 0 I never take longer
QUICK INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY (SELF-REPORT)(QIDS-SR16) Please circle the one response to each item that best describes you for the past seven days. 1. Falling Asleep: 0 I never take longer
Depression Fact Sheet
 Depression Fact Sheet Please feel free to alter and use this fact sheet to spread awareness of depression, its causes and symptoms, and what can be done. What is Depression? Depression is an illness that
Depression Fact Sheet Please feel free to alter and use this fact sheet to spread awareness of depression, its causes and symptoms, and what can be done. What is Depression? Depression is an illness that
Height: Weight: Neck Size: Does your work involve shift work? Yes No. Where did you hear about us: Physician Media Friend Other
 Personal Information Name: Date of birth: Sex: Male Female Marital Status: Nationality: MRN(for KAUH Patients): Height: Weight: Neck Size: Address: Occupation: Length of work day: Does your work involve
Personal Information Name: Date of birth: Sex: Male Female Marital Status: Nationality: MRN(for KAUH Patients): Height: Weight: Neck Size: Address: Occupation: Length of work day: Does your work involve
CBT Intake Form. Patient Name: Preferred Name: Last. First. Best contact phone number: address: Address:
 Patient Information CBT Intake Form Patient Name: Preferred Name: Last Date of Birth: _// Age: _ First MM DD YYYY Gender: Best contact phone number: Email address: _ Address: _ Primary Care Physician:
Patient Information CBT Intake Form Patient Name: Preferred Name: Last Date of Birth: _// Age: _ First MM DD YYYY Gender: Best contact phone number: Email address: _ Address: _ Primary Care Physician:
PATIENT NAME: DATE OF DISCHARGE: DISCHARGE SURVEY
 PATIENT NAME: DATE OF DISCHARGE: DISCHARGE SURVEY Please indicate whether you feel Living Hope Eating Disorder Treatment Center provided either Satisfactory or Unsatisfactory service for each number listed
PATIENT NAME: DATE OF DISCHARGE: DISCHARGE SURVEY Please indicate whether you feel Living Hope Eating Disorder Treatment Center provided either Satisfactory or Unsatisfactory service for each number listed
Problem Summary. * 1. Name
 Problem Summary This questionnaire is an important part of providing you with the best health care possible. Your answers will help in understanding problems that you may have. Please answer every question
Problem Summary This questionnaire is an important part of providing you with the best health care possible. Your answers will help in understanding problems that you may have. Please answer every question
Westminster IAPT Primary Care Psychology Service. Opt-In Questionnaire
 Westminster IAPT Primary Care Psychology Service Opt-In Questionnaire In order to get a better idea of your difficulties, we would be grateful if you could complete the attached registration form and questionnaire.
Westminster IAPT Primary Care Psychology Service Opt-In Questionnaire In order to get a better idea of your difficulties, we would be grateful if you could complete the attached registration form and questionnaire.
PHARMACY INFORMATION:
 Patient Name: Date of Birth: Referred by: Reason for Visit: Current psychiatric medications and doses: PHARMACY INFORMATION: Name of Pharmacy: Phone Number: Fax Number: Address: PRIMARY CARE PHYSICIAN
Patient Name: Date of Birth: Referred by: Reason for Visit: Current psychiatric medications and doses: PHARMACY INFORMATION: Name of Pharmacy: Phone Number: Fax Number: Address: PRIMARY CARE PHYSICIAN
ADULT QUESTIONNAIRE. Date of Birth: Briefly describe the history and development of this issue from onset to present.
 ADULT QUESTIONNAIRE Name: Address: Preferred phone number to reach you: Is it okay to leave a message? Yes No (Please check one) Date of Birth: Reason(s) for seeking treatment at this time? Briefly describe
ADULT QUESTIONNAIRE Name: Address: Preferred phone number to reach you: Is it okay to leave a message? Yes No (Please check one) Date of Birth: Reason(s) for seeking treatment at this time? Briefly describe
Christina Pucel Counseling 416 W. Main St Monongahela, PA /
 ADULT INTAKE Name: Gender: M F DOB: Address: City: State: Zip: Telephone: Home Mobile Highest Level Education: Occupation: Emergency Contact: Relationship: Phone: Referred by: Family Members: Name Gender
ADULT INTAKE Name: Gender: M F DOB: Address: City: State: Zip: Telephone: Home Mobile Highest Level Education: Occupation: Emergency Contact: Relationship: Phone: Referred by: Family Members: Name Gender
If you have any difficulties in filling out the forms, please contact our team administrator on
 Westminster IAPT Primary Care Psychology Service Lisson Grove Health Centre Gateforth Street London NW8 8EG Team Administrator Tel: 07971315596 Dear Sir/Madam Thank you for requesting this opt-in pack
Westminster IAPT Primary Care Psychology Service Lisson Grove Health Centre Gateforth Street London NW8 8EG Team Administrator Tel: 07971315596 Dear Sir/Madam Thank you for requesting this opt-in pack
INSOMNIA SEVERITY INDEX
 Name: Date: INSOMNIA SEVERITY INDEX For each of the items below, please circle the number that most closely corresponds to how you feel. 1. Please rate the CURRENT (i.e. last 2 weeks) severity of your
Name: Date: INSOMNIA SEVERITY INDEX For each of the items below, please circle the number that most closely corresponds to how you feel. 1. Please rate the CURRENT (i.e. last 2 weeks) severity of your
Brief Pain Inventory (Short Form)
") Brief Pain Inventory (Short Form) Study ID# Hospital# Do not write above this line Date: Time: Name: Last First Middle Initial 1) Throughout our lives, most of us have had pain from time to time (such
Brief Pain Inventory (Short Form) Study ID# Hospital# Do not write above this line Date: Time: Name: Last First Middle Initial 1) Throughout our lives, most of us have had pain from time to time (such
did you feel sad or depressed? did you feel sad or depressed for most of the day, nearly every day?
 Name: Age: Date: PDSQ This form asks you about emotions, moods, thoughts, and behaviors. For each question, circle YES in the column next to that question, if it describes how you have been acting, feeling,
Name: Age: Date: PDSQ This form asks you about emotions, moods, thoughts, and behaviors. For each question, circle YES in the column next to that question, if it describes how you have been acting, feeling,
Adult ADHD Screening Packet
 Adult ADHD Screening Packet Adult ADHD Screening Packet...1 Medical History...2 Primary Care Provider:...2 Local Pharmacy:...2 Mail Order Pharmacy:...2 Current medications:...2 Allergies to medications:...2
Adult ADHD Screening Packet Adult ADHD Screening Packet...1 Medical History...2 Primary Care Provider:...2 Local Pharmacy:...2 Mail Order Pharmacy:...2 Current medications:...2 Allergies to medications:...2
Sleep Health Center. You have been scheduled for an Insomnia Treatment Program consultation to further discuss your
 Sleep Health Center You have been scheduled for an Insomnia Treatment Program consultation to further discuss your sleep. In the week preceding your appointment, please take the time to complete the enclosed
Sleep Health Center You have been scheduled for an Insomnia Treatment Program consultation to further discuss your sleep. In the week preceding your appointment, please take the time to complete the enclosed
GENERAL BEHAVIOR INVENTORY Self-Report Version Never or Sometimes Often Very Often
 GENERAL BEHAVIOR INVENTORY Self-Report Version Here are some questions about behaviors that occur in the general population. Think about how often they occur for you. Using the scale below, select the
GENERAL BEHAVIOR INVENTORY Self-Report Version Here are some questions about behaviors that occur in the general population. Think about how often they occur for you. Using the scale below, select the
ALLIANCE COMMUNITY HOSPITAL SLEEP DISORDERS CENTER PATIENT QUESTIONNAIRE/HISTORY PLEASE COMPLETE AND BRING WITH YOU ON THE NIGHT OF YOUR TEST.
 ALLIANCE COMMUNITY HOSPITAL SLEEP DISORDERS CENTER PATIENT QUESTIONNAIRE/HISTORY PLEASE COMPLETE AND BRING WITH YOU ON THE NIGHT OF YOUR TEST. NAME DATE: HEIGHT: WEIGHT: DOB: SEX: HOME PHONE #: REFERRING
ALLIANCE COMMUNITY HOSPITAL SLEEP DISORDERS CENTER PATIENT QUESTIONNAIRE/HISTORY PLEASE COMPLETE AND BRING WITH YOU ON THE NIGHT OF YOUR TEST. NAME DATE: HEIGHT: WEIGHT: DOB: SEX: HOME PHONE #: REFERRING
Jessica Gifford, LICSW Mental Health Educator Jessica Gifford, LICSW Mental Health Educator
 Alleviating Depression and Anxiety through Wellness Promotion Jessica Gifford, LICSW Mental Health Educator Jessica Gifford, LICSW Mental Health Educator Public Health Approach Mental Health is a public
Alleviating Depression and Anxiety through Wellness Promotion Jessica Gifford, LICSW Mental Health Educator Jessica Gifford, LICSW Mental Health Educator Public Health Approach Mental Health is a public
Medical condition SELF Mother Father Sibling (list brother or sister) Anxiety Bipolar disorder Heart Disease Depression Diabetes High Cholesterol
 Anxiety Bipolar disorder Heart Disease Depression Diabetes High Cholesterol") PRE-EVALUATION FORM Medical condition SELF Mother Father Sibling (list brother or sister) Anxiety Bipolar disorder Heart Disease Depression Diabetes High Cholesterol High Blood Pressure Obesity Heart Defect
PRE-EVALUATION FORM Medical condition SELF Mother Father Sibling (list brother or sister) Anxiety Bipolar disorder Heart Disease Depression Diabetes High Cholesterol High Blood Pressure Obesity Heart Defect
PSYCHIATRY INTAKE FORM
 Please complete all information on this form. PSYCHIATRY INTAKE FORM Name Date Date of Birth Primary Care Physician Current Therapist/Counselor What are the problem(s) for which you are seeking help? 1.
Please complete all information on this form. PSYCHIATRY INTAKE FORM Name Date Date of Birth Primary Care Physician Current Therapist/Counselor What are the problem(s) for which you are seeking help? 1.
Schodack Internal Medicine and Pediatrics. Annual Physical-Female
 Schodack Internal Medicine and Pediatrics Annual Physical-Female Please Fill out this form (or have your caregiver complete it) and discuss with your medical provider. Thank you! Please Mark the preferred
Schodack Internal Medicine and Pediatrics Annual Physical-Female Please Fill out this form (or have your caregiver complete it) and discuss with your medical provider. Thank you! Please Mark the preferred
Short Clinical Guidelines: General Anxiety Disorder (GAD)
") Definition is one of the most prevalent psychiatric disorders seen in the primary care office and is characterized by excessive anxiety and worry about a number of events that cause clinically significant
Definition is one of the most prevalent psychiatric disorders seen in the primary care office and is characterized by excessive anxiety and worry about a number of events that cause clinically significant
STEP 1: Forms Please complete all the attached forms and bring them with you on the day of your visit.
 PATIENT HEALTH HISTORY FORM DIRECTIONS AND VISIT DAY INSTRUCTIONS Prior to your Appointment: STEP 1: Forms Please complete all the attached forms and bring them with you on the day of your visit. STEP
PATIENT HEALTH HISTORY FORM DIRECTIONS AND VISIT DAY INSTRUCTIONS Prior to your Appointment: STEP 1: Forms Please complete all the attached forms and bring them with you on the day of your visit. STEP
Medicare Wellness Visit
 of Birth: Today s : Medicare Wellness Visit Dear Patient, Your Medicare benefits include an Annual Wellness Visit to assist in preventing illness or detect illness at an early stage. Your Annual Wellness
of Birth: Today s : Medicare Wellness Visit Dear Patient, Your Medicare benefits include an Annual Wellness Visit to assist in preventing illness or detect illness at an early stage. Your Annual Wellness
SCL-90. Backaches 0 (T) In this case, the respondent experienced backaches a little bit (1). Please proceed with the questionnaire.
 In this case, the respondent experienced backaches a little bit (1). Please proceed with the questionnaire.") 4-79 Name Date SCL-90 Below is a list of problems and complaints that people sometimes have. Please read each one carefully. After you have done so, select one of the numbered descriptors that best describes
4-79 Name Date SCL-90 Below is a list of problems and complaints that people sometimes have. Please read each one carefully. After you have done so, select one of the numbered descriptors that best describes
Client s Name: Today s Date: Partner s Name (if being seen as a couple): Address, City, State, Zip: Home phone: Work phone: Cell phone:
: Address, City, State, Zip: Home phone: Work phone: Cell phone:") Client s Name: Today s Date: Partner s Name (if being seen as a couple): Address, City, State, Zip: Home phone: Work phone: Cell phone: Private email address: Student? If yes, where and major? May we leave
Client s Name: Today s Date: Partner s Name (if being seen as a couple): Address, City, State, Zip: Home phone: Work phone: Cell phone: Private email address: Student? If yes, where and major? May we leave
Southeastern Rehabilitation Medicine Initial (New) Outpatient Information Questionnaire
 Outpatient Information Questionnaire") Southeastern Rehabilitation Medicine Initial (New) Outpatient Information Questionnaire Name: MR#:_ Date: Date of Injury: Referred By: Age: Date of Birth: Handed: R L Ambidextrous Male Female **** Mark
Southeastern Rehabilitation Medicine Initial (New) Outpatient Information Questionnaire Name: MR#:_ Date: Date of Injury: Referred By: Age: Date of Birth: Handed: R L Ambidextrous Male Female **** Mark
FMS Psychology, PLLC Adult Intake Form. Phone Number (Day): Phone Number (Evening):
: Phone Number (Evening):") FMS Psychology, PLLC Adult Intake Form General Information: Name: Date of Birth: / / Age: Gender: Address: Phone Number (Day): Phone Number (Evening): Primary Care Physician: Highest Level of Formal Education:
FMS Psychology, PLLC Adult Intake Form General Information: Name: Date of Birth: / / Age: Gender: Address: Phone Number (Day): Phone Number (Evening): Primary Care Physician: Highest Level of Formal Education:
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D.
 Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
Prepared by: Elizabeth Vicens-Fernandez, LMHC, Ph.D. Sources: National Institute of Mental Health (NIMH), the National Alliance on Mental Illness (NAMI), and from the American Psychological Association
These questionnaires are used by psychology services to help us understand how people feel. One questionnaire measures how sad people feel.
 ADAPTED PHQ-9 & GAD-7 QUESTIONNAIRES How to fill in these questionnaires: These questionnaires are used by psychology services to help us understand how people feel. One questionnaire measures how sad
ADAPTED PHQ-9 & GAD-7 QUESTIONNAIRES How to fill in these questionnaires: These questionnaires are used by psychology services to help us understand how people feel. One questionnaire measures how sad
Seek, Test, Treat and Retain for Vulnerable Populations: Data Harmonization Measure
 Seek, Test, Treat and Retain for Vulnerable Populations: Measure MENTAL HEALTH Center for Epidemiologic Studies Depression Scale (CES-D) Reference: Radloff, L.S. (1977). The CES-D Scale: a self-report
Seek, Test, Treat and Retain for Vulnerable Populations: Measure MENTAL HEALTH Center for Epidemiologic Studies Depression Scale (CES-D) Reference: Radloff, L.S. (1977). The CES-D Scale: a self-report
Welcome to NHS Highland Pain Management Service
 Welcome to NHS Highland Pain Management Service Information from this questionnaire helps us to understand your pain problem better. It is important that you read each question carefully and answer as
Welcome to NHS Highland Pain Management Service Information from this questionnaire helps us to understand your pain problem better. It is important that you read each question carefully and answer as
To be completed by Patient. Client Questionnaire
 Date: To be completed by Patient Client Questionnaire Client(s) Name: SSN#: - - Name of Person Completing Form: Relationship to Patient: (if other than client) Marital Status of Client Race/Ethnic Origin
Date: To be completed by Patient Client Questionnaire Client(s) Name: SSN#: - - Name of Person Completing Form: Relationship to Patient: (if other than client) Marital Status of Client Race/Ethnic Origin
Measurement of Psychopathology in Populations. William W. Eaton, PhD Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
WELCOME TO AGEWELL MEDICAL ASSOCIATES
 WELCOME TO AGEWELL MEDICAL ASSOCIATES We offer the following checklist and suggestions to help make your first visit as easy and pleasant as possible. What to bring with you: [ ] All of your medications
WELCOME TO AGEWELL MEDICAL ASSOCIATES We offer the following checklist and suggestions to help make your first visit as easy and pleasant as possible. What to bring with you: [ ] All of your medications
ALVIN C. BURSTEIN, MD PATIENT CLIENT INFORMATION
 ALVIN C. BURSTEIN, MD PATIENT CLIENT INFORMATION LEGAL Name Date of Birth (must match insurance card) Address City State Zip Mailing Address City State Zip (If different) Phone: Cell Home Appt. reminders
ALVIN C. BURSTEIN, MD PATIENT CLIENT INFORMATION LEGAL Name Date of Birth (must match insurance card) Address City State Zip Mailing Address City State Zip (If different) Phone: Cell Home Appt. reminders
COUPLE & FAMILY INSTITUTE OF TRI-CITIES AMEN ADULT GENERAL SYMPTOM CHECKLIST
 COUPLE & FAMILY INSTITUTE OF TRI-CITIES AMEN ADULT GENERAL SYMPTOM CHECKLIST Please rate yourself on each symptom listed below. Please use the following scale: 0--------------------------1---------------------------2--------------------------3--------------------------4
COUPLE & FAMILY INSTITUTE OF TRI-CITIES AMEN ADULT GENERAL SYMPTOM CHECKLIST Please rate yourself on each symptom listed below. Please use the following scale: 0--------------------------1---------------------------2--------------------------3--------------------------4
A1a. Have you ever had a time in your life when you felt sad, blue, or depressed for two weeks or more in a row?
 PhenX Measure: General Psychiatric Assessment (#120100) PhenX Protocol: General Psychiatric Assessment - Adult (#120101) Date of Interview/Examination (MM/DD/YYYY): SECTION A: [Major Depressive Episode]
PhenX Measure: General Psychiatric Assessment (#120100) PhenX Protocol: General Psychiatric Assessment - Adult (#120101) Date of Interview/Examination (MM/DD/YYYY): SECTION A: [Major Depressive Episode]
Richard Heidenfelder M.D. Child, Adolescent and Adult Psychiatry 447 9th Ave San Diego, CA
 *We are not accepting any New Patients who are currently taking any controlled pain medications *We are *Note: not completion accepting of the any following New Patients paperwork who and Initial are Screening
*We are not accepting any New Patients who are currently taking any controlled pain medications *We are *Note: not completion accepting of the any following New Patients paperwork who and Initial are Screening
Do not write below this line DSM IV Code: Primary Secondary. Clinical Information
 New Client Registration Today s date Name Age Sex Address Social security # Date of birth Home phone May I call you at this number? y / n Leave a message? y / n Other numbers at which I can call you Can
New Client Registration Today s date Name Age Sex Address Social security # Date of birth Home phone May I call you at this number? y / n Leave a message? y / n Other numbers at which I can call you Can
USF Health Psychiatry Clinic. New Patient Questionnaire Adult
 USF Health Psychiatry Clinic New Patient Questionnaire Adult Please mail or fax the completed forms to the address/fax number on the bottom of this page. Completed forms must be received five (5) days
USF Health Psychiatry Clinic New Patient Questionnaire Adult Please mail or fax the completed forms to the address/fax number on the bottom of this page. Completed forms must be received five (5) days
EMOTIONAL SUPPORT ANIMAL (ESA) PSYCHOLOGICAL EVALUATION PART I: PERSONAL INFORMATION STREET ADDRESS CITY/STATE
 PSYCHOLOGICAL EVALUATION PART I: PERSONAL INFORMATION STREET ADDRESS CITY/STATE") EMOTIONAL SUPPORT ANIMAL (ESA) PSYCHOLOGICAL EVALUATION PART I: PERSONAL INFORMATION FIRST NAME LAST NAME EMAIL PHONE # STREET ADDRESS CITY/STATE ZIP GENDER: MALE FEMALE TRANSGENER MARITAL STATUS: MARRIED
EMOTIONAL SUPPORT ANIMAL (ESA) PSYCHOLOGICAL EVALUATION PART I: PERSONAL INFORMATION FIRST NAME LAST NAME EMAIL PHONE # STREET ADDRESS CITY/STATE ZIP GENDER: MALE FEMALE TRANSGENER MARITAL STATUS: MARRIED
GENERAL INFORMATION PROFESSIONAL REFERRAL INFORMATION
 SO THAT WE MAY BETTER SERVE YOU, PLEASE COMPLETE THE FOLLOWING FORM AND EITHER BRING THE COMPLETED FORM WITH YOU TO YOUR FIRST APPOINTEMNT OR SCAN IT AND EMAIL IT TO OFFICE, PRIOR TO YOUR APPOINTMENT LORRAINE@ANALIPSONMD.COM
SO THAT WE MAY BETTER SERVE YOU, PLEASE COMPLETE THE FOLLOWING FORM AND EITHER BRING THE COMPLETED FORM WITH YOU TO YOUR FIRST APPOINTEMNT OR SCAN IT AND EMAIL IT TO OFFICE, PRIOR TO YOUR APPOINTMENT LORRAINE@ANALIPSONMD.COM
Baptist Health Floyd 1850 State Street New Albany, IN Sleep Disorders Center Lung & Sleep Specialists. Date of Birth: Age:
 Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
EMOTIONAL SUPPORT ANIMAL (ESA) PSYCHOLOGICAL EVALUATION. Important Information
 PSYCHOLOGICAL EVALUATION. Important Information") EMOTIONAL SUPPORT ANIMAL (ESA) PSYCHOLOGICAL EVALUATION Important Information The primary purpose of an Emotional Support Animal (ESA) is to help his or her owner by decreasing symptoms that are associated
EMOTIONAL SUPPORT ANIMAL (ESA) PSYCHOLOGICAL EVALUATION Important Information The primary purpose of an Emotional Support Animal (ESA) is to help his or her owner by decreasing symptoms that are associated
Initial Patient Self Assessment Demographics:
 Initial Patient Self Assessment Demographics: Name: Address: E mail: Phone Number: Date of Birth: Gender: Male Female Other Primary Language: English Spanish Other Occupation: Education: Clerical Skilled
Initial Patient Self Assessment Demographics: Name: Address: E mail: Phone Number: Date of Birth: Gender: Male Female Other Primary Language: English Spanish Other Occupation: Education: Clerical Skilled
Major Depressive Disorder Wellness Workbook
 Framing Major Depressive Disorder Major Depressive Disorder Wellness Workbook This Workbook belongs to you and you decide how to use it. You decide who to show it to and whether or not you want someone
Framing Major Depressive Disorder Major Depressive Disorder Wellness Workbook This Workbook belongs to you and you decide how to use it. You decide who to show it to and whether or not you want someone
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
Date of Birth (mm/dd/year): 2. How much would you like to weigh (desired weight)?
: 2. How much would you like to weigh (desired weight)?") MFA Weight Management Practice Initial Consultation Survey Name: Date of Birth (mm/dd/year): I. Weight History 1. What is the main reason you want to lose weight? _ 2. How much would you like to weigh
MFA Weight Management Practice Initial Consultation Survey Name: Date of Birth (mm/dd/year): I. Weight History 1. What is the main reason you want to lose weight? _ 2. How much would you like to weigh
Peer Support / Social Activities Overview and Application Form
 Peer Support / Social Activities Overview and Application Form What is Peer Support? Peer support is when people use their own experiences to help each other. What happens during peer support sessions
Peer Support / Social Activities Overview and Application Form What is Peer Support? Peer support is when people use their own experiences to help each other. What happens during peer support sessions
Psychiatric Evaluation Intake Form
 Psychiatric Evaluation Intake Form Patient Contact Information Patient Name: Date of Birth: Age: Last First MI Address: Contact phone number: Email address: Emergency Contact/Number/Relationship: Primary
Psychiatric Evaluation Intake Form Patient Contact Information Patient Name: Date of Birth: Age: Last First MI Address: Contact phone number: Email address: Emergency Contact/Number/Relationship: Primary
Psychological Sleep Services Sleep Assessment
 Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Conscious Living Counseling & Education Center 3239 Oak Ridge Loop East, West Fargo ND (701)
") Conscious Living Counseling & Education Center 3239 Oak Ridge Loop East, West Fargo ND 58078 (701) 478-7199 INTAKE FORM BIRTH DATE: / / Age: Email: YOUR NAME FIRST: MIDDLE INITIAL: LAST: YOUR ADDRESS COMPLETE
Conscious Living Counseling & Education Center 3239 Oak Ridge Loop East, West Fargo ND 58078 (701) 478-7199 INTAKE FORM BIRTH DATE: / / Age: Email: YOUR NAME FIRST: MIDDLE INITIAL: LAST: YOUR ADDRESS COMPLETE
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
Psychiatric Evaluation Intake Form
 Patient Contact Information Psychiatric Evaluation Intake Form Patient Name: Date of Birth: Age: Last First MI Address: Contact phone number: Email address: Emergency Contact/Number/Relationship: Primary
Patient Contact Information Psychiatric Evaluation Intake Form Patient Name: Date of Birth: Age: Last First MI Address: Contact phone number: Email address: Emergency Contact/Number/Relationship: Primary
CUMMINS BEHAVIORAL HEALTH SYSTEMS, INC. CONSUMER MEDICAL HISTORY SELF-REPORT
 Page 1 of 5 CUMMINS BEHAVIORAL HEALTH SYSTEMS, INC. CONSUMER MEDICAL HISTORY SELF-REPORT Please describe what problems you/consumer are having and why you are seeking treatment at this time. PRIOR MENTAL
Page 1 of 5 CUMMINS BEHAVIORAL HEALTH SYSTEMS, INC. CONSUMER MEDICAL HISTORY SELF-REPORT Please describe what problems you/consumer are having and why you are seeking treatment at this time. PRIOR MENTAL
Joseph M. Sharpe, M.D Church St, Suite# 513 Nashville, TN Phone Fax
 Joseph M. Sharpe, M.D. 2010 Church St, Suite# 513 Nashville, TN 37203 Phone 615.284.3850 Fax 615.284.4350 Patient Name Referred by What is your main problem? List difficulties/symptoms/issues which have
Joseph M. Sharpe, M.D. 2010 Church St, Suite# 513 Nashville, TN 37203 Phone 615.284.3850 Fax 615.284.4350 Patient Name Referred by What is your main problem? List difficulties/symptoms/issues which have
If you arrive at the office without these forms, your visit may need to be rescheduled.
 Dear, Your Appointment for the Welcome to Medicare Visit OR Annual Wellness Visit is scheduled on at There is NO CO-PAY for this visit, so it is free for you. The goal of this visit is to provide time
Dear, Your Appointment for the Welcome to Medicare Visit OR Annual Wellness Visit is scheduled on at There is NO CO-PAY for this visit, so it is free for you. The goal of this visit is to provide time
Depression. There are several forms of depression (depressive disorders). Major depressive disorder and dysthymic disorder are the most common.
. Major depressive disorder and dysthymic disorder are the most common.") Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Depression Depression is a state of low mood and aversion to activity that can affect a person's thoughts, behavior, feelings and sense of well-being. People with depressed mood can feel sad, anxious,
Happy Daisy Ltd. New Client intake Form. What are the issues for which you are seeking care?
 Happy Daisy Ltd. New Client intake Form Name Date Preferred name Pronouns Referred by Date of birth Age Race What are the issues for which you are seeking care? 1. 2. 3. Please check of any of the symptoms
Happy Daisy Ltd. New Client intake Form Name Date Preferred name Pronouns Referred by Date of birth Age Race What are the issues for which you are seeking care? 1. 2. 3. Please check of any of the symptoms
ANTI-DEPRESSANT MEDICATIONS
 ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
ANTI-DEPRESSANT MEDICATIONS This information is not intended to be a substitute for medical advice. It s purpose is solely informative. If your client or yourself are taking antidepressants, do not change
Sleep History Questionnaire B/P / Pulse: Neck Circum Wgt: Pulse Ox
 2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
ADULT HISTORY QUESTIONNAIRE
 ADULT HISTORY QUESTIONNAIRE Date: Full Name: Date of Birth: If applicable, please complete the following: Partner s Name: Partner s Age: Partner s Occupation: IF YOU HAVE CHILDREN PLEASE LIST THEIR NAMES
ADULT HISTORY QUESTIONNAIRE Date: Full Name: Date of Birth: If applicable, please complete the following: Partner s Name: Partner s Age: Partner s Occupation: IF YOU HAVE CHILDREN PLEASE LIST THEIR NAMES
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES
 PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
PHYSICIAN REFERENCE ANTIDEPRESSANT DOSING GUIDELINES Table of Contents Print TABLE OF CONTENTS Drug Page Number Anafranil... 2 Asendin... 4 Celexa... 4 Cymbalta... 6 Desyrel... 8 Effexor...10 Elavil...14
Part I. Demographics. Part II. Presenting Problem. Who referred you to WellStar Psychological Services?
 Part I. Demographics Today s Date Current Time : Patient s Name (Last) (First) (MI) Patient s Date of Birth Patient s Gender Female Male Patient s Address Primary Phone Ok to leave a message? Email Address
Part I. Demographics Today s Date Current Time : Patient s Name (Last) (First) (MI) Patient s Date of Birth Patient s Gender Female Male Patient s Address Primary Phone Ok to leave a message? Email Address
Single Married Divorced Widowed Male Female
 Annual Physical Form General Information Name Birth Date Phone Email Address Street Address City State Zip Marital Status Gender Single Married Divorced Widowed Male Female Employment Information Position
Annual Physical Form General Information Name Birth Date Phone Email Address Street Address City State Zip Marital Status Gender Single Married Divorced Widowed Male Female Employment Information Position
The role of stabilizing and communicating symptoms given overlapping. communities in psychopathology networks
 The role of stabilizing and communicating symptoms given overlapping communities in psychopathology networks Tessa F. Blanken a,b,1,* Marie K. Deserno a,c,1 Jonas Dalege a Denny Borsboom a Peter Blanken
The role of stabilizing and communicating symptoms given overlapping communities in psychopathology networks Tessa F. Blanken a,b,1,* Marie K. Deserno a,c,1 Jonas Dalege a Denny Borsboom a Peter Blanken
Mental Health Intake Form
 Current Symptoms Checklist: (check once for any symptoms present, twice for major symptoms) ( ) ( ) Depressed mood ( ) ( ) Racing thoughts ( ) ( ) Excessive worry ( ) ( ) Unable to enjoy activities ( )
Current Symptoms Checklist: (check once for any symptoms present, twice for major symptoms) ( ) ( ) Depressed mood ( ) ( ) Racing thoughts ( ) ( ) Excessive worry ( ) ( ) Unable to enjoy activities ( )
Memory & Aging Clinic Questionnaire
 Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Memory & Aging Clinic Questionnaire The answers you give to the questions below will assist us with our evaluation. Each section is equally important so please be sure to complete the entire questionnaire.
Psychiatric Nurse Practitioner Intake Form. General Information. 1. Name. 2. Date of Birth. 3. Age. 4. Gender. 5. Referred by
 Psychiatric Nurse Practitioner Intake Form General Information 1. Name 2. Date of Birth 3. Age 4. Gender 5. Referred by 6. Emergency Contact & Phone Number 7. Please State your Main Reason for Coming in
Psychiatric Nurse Practitioner Intake Form General Information 1. Name 2. Date of Birth 3. Age 4. Gender 5. Referred by 6. Emergency Contact & Phone Number 7. Please State your Main Reason for Coming in
Sonja Benson, Ph.D., PLLC Licensed Psychologist
 Sonja Benson, Ph.D., PLLC Licensed Psychologist Date_ Referred by Name Date of Birth Social Security # Address_ City State Zip code Daytime Phone Nighttime Phone Cell Phone Email Male( ) Female ( ) Ethnicity
Sonja Benson, Ph.D., PLLC Licensed Psychologist Date_ Referred by Name Date of Birth Social Security # Address_ City State Zip code Daytime Phone Nighttime Phone Cell Phone Email Male( ) Female ( ) Ethnicity
MEDICAL HISTORY QUESTIONNAIRE
 MEDICAL HISTORY QUESTIONNAIRE NAME: SEX: DATE: DOB: AGE: Primary Doctor / Care Manager: Additional doctors to receive sleep study results: Chief sleep related complaint: What made you decide to have this
MEDICAL HISTORY QUESTIONNAIRE NAME: SEX: DATE: DOB: AGE: Primary Doctor / Care Manager: Additional doctors to receive sleep study results: Chief sleep related complaint: What made you decide to have this
SLEEP DISORDERS CENTER QUESTIONNAIRE
 Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Preferred Name (s): Local Address: City: State: Zip: Permanent Address: City: State: Zip: Years of Education: Occupation: Gender: M F
: Local Address: City: State: Zip: Permanent Address: City: State: Zip: Years of Education: Occupation: Gender: M F") Today Date: Client Name(s) : Psychological Consultants Northgate Center 1210 ½ -7 th Street NW, Suite 216 Rochester, MN 55901 www.psychologicalconsultants1.com Office: (507) 252-9292 Fax: (507) 252-9203
Today Date: Client Name(s) : Psychological Consultants Northgate Center 1210 ½ -7 th Street NW, Suite 216 Rochester, MN 55901 www.psychologicalconsultants1.com Office: (507) 252-9292 Fax: (507) 252-9203
* CC* PATIENT QUESTIONNAIRE
 Pain Center of Michigan *0290341CC* PATIENT QUESTIONNAIRE Patient Name Birthdate Age Home Address City State Zip Home Phone Alternate Phone Referring Physician Primary Care Physician MEDICAL HISTORY Please
Pain Center of Michigan *0290341CC* PATIENT QUESTIONNAIRE Patient Name Birthdate Age Home Address City State Zip Home Phone Alternate Phone Referring Physician Primary Care Physician MEDICAL HISTORY Please
Fear of Vomiting Questionnaire. Please complete this questionnaire as best as you can to help us understand as much as possible about your fear.
 Page 1 Fear of Vomiting Questionnaire Name: Date: Please complete this questionnaire as best as you can to help us understand as much as possible about your fear. 1) How old were you when you first became
Page 1 Fear of Vomiting Questionnaire Name: Date: Please complete this questionnaire as best as you can to help us understand as much as possible about your fear. 1) How old were you when you first became
PRE-VISIT QUESTIONNAIRE FOR NEW PATIENTS
 UF Health Senior Care PO Box 100383 Gainesville, FL 32608 352-265-0615 Fax 352-294-5803 PRE-VISIT QUESTIONNAIRE FOR NEW PATIENTS Please complete this questionnaire at home and bring it with you to the
UF Health Senior Care PO Box 100383 Gainesville, FL 32608 352-265-0615 Fax 352-294-5803 PRE-VISIT QUESTIONNAIRE FOR NEW PATIENTS Please complete this questionnaire at home and bring it with you to the
Occupation: Leisure Activities: ALLERGIES Are you latex-sensitive? Y N List any medication(s) you are allergic to:
 you are allergic to:") Hello and thank you for choosing Fusion Physical Therapy as the provider for your current healthcare need(s)! We look forward to working with you to help make your day a little easier! To ensure you receive
Hello and thank you for choosing Fusion Physical Therapy as the provider for your current healthcare need(s)! We look forward to working with you to help make your day a little easier! To ensure you receive
Kelowna Sleep Clinic Dr. Ronald Cridland Inc Sleep Questionnaire
 Dr. Ronald Cridland Inc Sleep Questionnaire Name: Date: d/m/yr Date of Birth: d/m/yr Age: Marital Status: Sex: M F Address: City: Province: Postal Code: Health Care #: Home Phone #: Work Phone #: _ Cell
Dr. Ronald Cridland Inc Sleep Questionnaire Name: Date: d/m/yr Date of Birth: d/m/yr Age: Marital Status: Sex: M F Address: City: Province: Postal Code: Health Care #: Home Phone #: Work Phone #: _ Cell
Integrating older age, disability and mental health issues into household surveys: progress and outstanding gaps
 Integrating older age, disability and mental health issues into household surveys: progress and outstanding gaps Annex Emma Samman and Laura K. Rodriguez-Takeuchi 1. Selected survey questions: disability
Integrating older age, disability and mental health issues into household surveys: progress and outstanding gaps Annex Emma Samman and Laura K. Rodriguez-Takeuchi 1. Selected survey questions: disability
Medicare Annual Wellness Visit HEALTH RISK ASSESSMENT
 Patient Name: Date of Birth: GENERAL HEALTH 1. How is your overall health? Excellent Good Fair Poor 2. How many different prescriptions are you taking? 0-3 4-6 7-10 10+ 3. Do you take all of your mediations
Patient Name: Date of Birth: GENERAL HEALTH 1. How is your overall health? Excellent Good Fair Poor 2. How many different prescriptions are you taking? 0-3 4-6 7-10 10+ 3. Do you take all of your mediations
A 15-Minute Psychiatric Assessment
 A 15-Minute Psychiatric Assessment The following questions have been adapted from several sources (see references) and are intended to screen for the following psychiatric conditions: MDE Alcohol Misuse
A 15-Minute Psychiatric Assessment The following questions have been adapted from several sources (see references) and are intended to screen for the following psychiatric conditions: MDE Alcohol Misuse
BACKGROUND HISTORY QUESTIONNAIRE
 BACKGROUND HISTORY QUESTIONNAIRE Name: Sex M F Address: Home Number: Work Number: Cell Number: Email: SSN: Name and Address of Employer: Date of Birth: Age: Ethnicity: Referred By: Referral Question or
BACKGROUND HISTORY QUESTIONNAIRE Name: Sex M F Address: Home Number: Work Number: Cell Number: Email: SSN: Name and Address of Employer: Date of Birth: Age: Ethnicity: Referred By: Referral Question or
Please complete this form before your Doctor visit. We will review this together and make any changes needed.
 1 Medical History Please complete this form before your Doctor visit. We will review this together and make any changes needed. Name Date of Birth Date of visit What is your height? weight? Medical History,
1 Medical History Please complete this form before your Doctor visit. We will review this together and make any changes needed. Name Date of Birth Date of visit What is your height? weight? Medical History,
RESEARCH DIAGNOSTIC CRITERIA FOR TEMPOROMANDIBULAR DISORDERS: REVIEW, CRITERIA, EXAMINATIONS AND SPECIFICATIONS, CRITIQUE
 RESEARCH DIAGNOSTIC CRITERIA FOR TEMPOROMANDIBULAR DISORDERS: REVIEW, CRITERIA, EXAMINATIONS AND SPECIFICATIONS, CRITIQUE Edited by: Samuel F. Dworkin, DDS, PhD and Linda LeResche, ScD A. HISTORY QUESTIONNAIRE
RESEARCH DIAGNOSTIC CRITERIA FOR TEMPOROMANDIBULAR DISORDERS: REVIEW, CRITERIA, EXAMINATIONS AND SPECIFICATIONS, CRITIQUE Edited by: Samuel F. Dworkin, DDS, PhD and Linda LeResche, ScD A. HISTORY QUESTIONNAIRE
MERLE MULLINS COUNSELING REGISTRATION FORM (Please Print) CLIENT INFORMATION
 CLIENT INFORMATION") MERLE MULLINS COUNSELING REGISTRATION FORM (Please Print) CLIENT INFORMATION Last Name: First: Middle:! Mr.! Mrs. Today s date: / /! Miss! Ms. Marital status (circle one) Single / Mar / Div / Sep / Wid
MERLE MULLINS COUNSELING REGISTRATION FORM (Please Print) CLIENT INFORMATION Last Name: First: Middle:! Mr.! Mrs. Today s date: / /! Miss! Ms. Marital status (circle one) Single / Mar / Div / Sep / Wid
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA SLEEP HISTORY QUESTIONNAIRE
 604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
Allina Health United Lung and Sleep Clinic
 Medical History Form Date Allina Health United Lung and Sleep Clinic Name Last First MI Date of birth What lung problem do you want us to help you with: Who is your primary care provider? Social History
Medical History Form Date Allina Health United Lung and Sleep Clinic Name Last First MI Date of birth What lung problem do you want us to help you with: Who is your primary care provider? Social History
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE
 VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
GASTROINTESTINAL CANCER PREVENTION PROGRAM INTAKE FORM Page 1 of 6
 Full Name Today s date Referred by: Primary Care Provider: What is the reason for your visit? Date of Birth FOR CLINIC USE ONLY HT (cm) WT (kg) Questions you would like addressed at this visit: Personal
Full Name Today s date Referred by: Primary Care Provider: What is the reason for your visit? Date of Birth FOR CLINIC USE ONLY HT (cm) WT (kg) Questions you would like addressed at this visit: Personal
Treating Chronic Illness in the PCMH Handout - Depression. A. Guidelines. 1. Control of Symptoms:
 Treating Chronic Illness in the PCMH Handout - Depression A. Guidelines A quick note on diagnosis: Note: For a major depressive episode a person must have experienced at least five of the nine symptoms
Treating Chronic Illness in the PCMH Handout - Depression A. Guidelines A quick note on diagnosis: Note: For a major depressive episode a person must have experienced at least five of the nine symptoms
New Client Information. address: Date of Birth:
 Milwaukee Area Psychological Services, S.C. (MAPS) 401 E. Kilbourn Avenue, Suite 402 Milwaukee, WI 52302 414-269-8660 (phone) 414-269-8656 (fax) New Client Information Your responses to the following questions
Milwaukee Area Psychological Services, S.C. (MAPS) 401 E. Kilbourn Avenue, Suite 402 Milwaukee, WI 52302 414-269-8660 (phone) 414-269-8656 (fax) New Client Information Your responses to the following questions
EPWORTH SLEEPINESS SCALE
 EPWORTH SLEEPINESS SCALE Name: Sponsors last 4 of SSN#: DOB: Today s Date: Age (years): Gender (circle): MALE FEMALE How likely are you to doze off or fall asleep in the following situation, in contrast
EPWORTH SLEEPINESS SCALE Name: Sponsors last 4 of SSN#: DOB: Today s Date: Age (years): Gender (circle): MALE FEMALE How likely are you to doze off or fall asleep in the following situation, in contrast
Lambeth Psychological Therapies
 Complaints procedure: If you are not happy about your experience with our service, you can speak to a member of staff directly; alternatively, you can contact the PALS Office. To make a formal complaint,
Complaints procedure: If you are not happy about your experience with our service, you can speak to a member of staff directly; alternatively, you can contact the PALS Office. To make a formal complaint,
To: Our Medicare Patients. Subject: Your Welcome to Medicare Exam
 To: Our Medicare Patients Subject: Your Welcome to Medicare Exam Medicare covers a one-time Welcome to Medicare visit. The Welcome to Medicare visit must occur during your first twelve months as a Medicare
To: Our Medicare Patients Subject: Your Welcome to Medicare Exam Medicare covers a one-time Welcome to Medicare visit. The Welcome to Medicare visit must occur during your first twelve months as a Medicare
Medicare Annual Wellness Visit Patient History
 Grace Health Medicare Annual Wellness Visit Patient History Name Date Birthdate Languages Spoken Date of Last Wellness Visit Do you have an advance directive or living will? Yes Don t Know Want Information
Grace Health Medicare Annual Wellness Visit Patient History Name Date Birthdate Languages Spoken Date of Last Wellness Visit Do you have an advance directive or living will? Yes Don t Know Want Information
Patient Scheduled Letter Thunderbird Internal Medicine Sleep Center 5620 W. Thunderbird Rd., Suite C-1 Glendale, AZ (602)
") Patient Scheduled Letter Thunderbird Internal Medicine Sleep Center 5620 W. Thunderbird Rd., Suite C-1 Glendale, AZ 85306 (602) 938 6960 Dear Patient, Your Doctor has requested you be scheduled for a sleep
Patient Scheduled Letter Thunderbird Internal Medicine Sleep Center 5620 W. Thunderbird Rd., Suite C-1 Glendale, AZ 85306 (602) 938 6960 Dear Patient, Your Doctor has requested you be scheduled for a sleep
FATIGUE ASSESSMENT SCALE
 WORKSHEET #1 FATIGUE ASSESSMENT SCALE Please indicate how true each statement has been for you during the past 7 days Not at all A little bit Some what Quite a lot Very much I feel fatigued I feel weak
WORKSHEET #1 FATIGUE ASSESSMENT SCALE Please indicate how true each statement has been for you during the past 7 days Not at all A little bit Some what Quite a lot Very much I feel fatigued I feel weak
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Who Writes Prescriptions for Psychotropic Medications. Biological Psychiatry
 Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free
Antidepressant Medication Strategies We ve Come a Long Way or Have We? Joe Wegmann, PD, LCSW The PharmaTherapist Joe@ThePharmaTherapist.com 504.587.9798 www.pharmatherapist.com Are you receiving our free