Atypical Nevi When to Re-excise. Catherine Barry, DO Dermatopathologist
|
|
|
- Arron Barber
- 5 years ago
- Views:
Transcription

1 Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist

2 Why talk about skin cancer? Because it s the most common type of cancer!
3 Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell Carcinoma Leiomyosarcoma Dermatofibrosarcoma Protuberans Sebaceous Carcinoma Merkel Cell Carcinoma Microcystic Adnexal Carcinoma There are even more than these!
4 Non Melanoma Skin Cancer > 1,300,000 per year 20% lifetime risk in fair-skinned individuals Incidence rising Increased leisure time? Increased UV radiation? Increased awareness?
5 Most Common Skin Cancers Basal Cell Carcinoma 1 million/year Squamous Cell Carcinoma 250,000/year Malignant Melanoma 50,000/year

6 Cells of Origin Basal keratinocyte Keratinocyte Melanocyte
7 Skin Cancer Deaths 10,000 deaths/year in U.S. 7,000 from Melanoma
8 Etiology Ultraviolet Light induced mutations BCC PTCH gene mutations p53 mutations SCC P53 mutations Melanoma Less clear
9 Introduction Melanocytes Overview of benign nevi Selected benign pigmented lesions Aypical Melanocytic Lesions /Melanoma precursors Malignant melanoma
10 Overview Selected benign pigmented lesions Freckle (ephelides) Labial melanotic macule Solar lentigo Lentigo simplex Lentiginous junctional melanocytic nevus Lentiginous compound melanocytic nevus Aypical Melanocytic Lesions /Melanoma precursors Dysplastic nevi / Clark s nevus / B-K mole Mild Moderate Severe Margins Treatment and re-exision Malignant melanoma Margins Re-excision
11 The Melanocyte

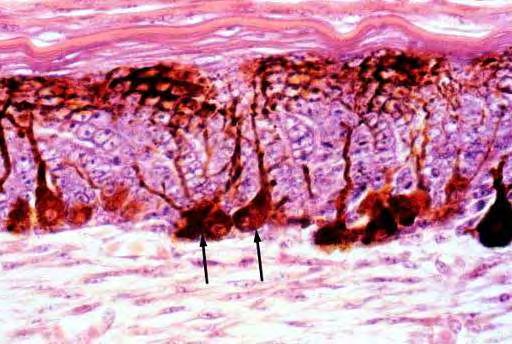
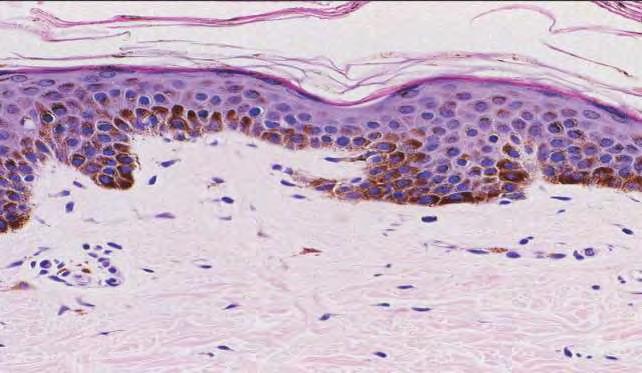
12 Normal Melanocytes Melan-A (Mart-1) Dispersed within the basal layer approximately one melanocyte per 10 keratinocytes Varies with location Highest face and male genitailia Lowest trunk
13 Melanocytes Overview Melan-A highly branched connected to approximately 36 keratinocytes through dendritic processes The number of melanocytes is the same between all races In African Americans the melanocytes are larger and contain more highly dendritic melanocytes The color of your skin is determined by the number of melanosomes contained within the melanocytes The number of melanosomes is greater in the basal layer and they get degraded within the keratinocytes as they move upwards and are shed

14 With exposure to UV light melanocytes increase in size and functional activity but not in number Specialized organelles of the melanocytes called melanosomes. Melanosomes develop in four stages and move from the cytoplasm to the dendritic processes Receptors on keratinocytes is a key receptor involved in the melanosome transfer These are transferred to the keratinocytes by a receptor on the keratinocyte (proteaseactivated receptor 2, PAR-2) Pinocytotic process where they fuse with acid lysosomes. With time the keratinocytes and melanocytes migrate to the surface of the skin and are shed

15 Melanin granules (Warthin-Starry Stain) Melanin gets impregnanted by silver nitrate solutions. When reduced to silver it turns black
16 Increased Melanin in Keratinocytes Freckle (ephelides) Labial melanotic macule Lentigo simplex Solar lentigo

17 Freckle (ephelides)


18 Labial and Genital Melanotic Macules


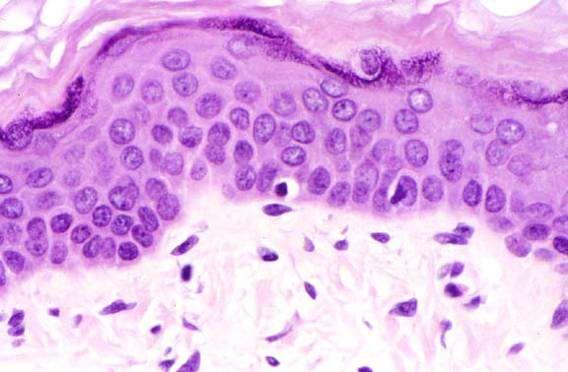
19 Lentigo Simplex (Simple Lentigo) Variable basal hyperpigmentation Increased number of single melanocytes in the basal layer Elongation of rete ridges
20 Multiple Lentigines Xeroderma pigmentosum Peutz-Jeghers Laugier-Hunziker Myxoma Syndromes LAMB NAME Carney LEOPARD Syndrome
")

21 Solar (Senile) Lentigo
 Especially in sun protected areas PUVA")
22 Clinical Occurs after exposure to psoralens (methoxsalen) and ultraviolet-a radiation (PUVA) Especially in sun protected areas PUVA Lentigo
23 Increased Melanin in Keratinocytes and nests of melanocytes Lentiginous nevus Lentiginous junctional melanocytic nevus Lentiginous compound melanocytic nevus Nevus spilius

24 Lentiginous Nevus


25 Speckled Lentiginous Nevus Present at birth or appear in childhood Considered a variant of congenital nevus (Nevus Spilus)
26 Immunohistochemistry S100 stains dermal melanocytes that other stains may not, also stains Langerhan s cells Mel-A (Mart-1) HMB45 Tyrosinase MITF - Microphthalmia Transcription Factor NKI/C-3 Melan-A
27 Melanocytic Nevi Junctional Nevus Compound Nevus Most common Intradermal Nevus Meyerson s Nevus Ancient Nevus Deep Penetrating Nevus Balloon Cell Nevus Halo Nevus Cockarde Nevus Eccrine Centered Nevus Recurrent Nevus Spitz Nevus (Spindled and Epitheliod Cell Nevus) Pigmented Spindled Cell Nevus Congenital Nevus



28 Benign Proliferation of Melanocytes= Nevus Compound nevus Junctional nevus Intradermal nevus


29 Junctional Nevus Clinical Well circumscribed, brown black macule, develops anywhere on the body surface Usually appears during childhood or adolescence Skin lines are preserved


30 Compound Nevus Clinical Most common in children and adolescents Dome shaped to polypoid and may be tan or dark brown


31 Intradermal Nevus Clinical most common type of nevi, the majority are found in adults Dome shaped, nodular or polypoid, pink or slightly pigmented Coarse hairs may protrude from the surface
32 Other Dermal Melanocytic Lesions Mongolian Spot Nevus of Ota and Nevus of Ito Blue Nevus Cellular Blue Nevus Blue Nevus-like Metastatic Melanoma Malignant Blue Nevus Dermal Melanocytic Hamartoma Phakomatosis Pigmentovascularis Cutaneous Neurocristic Hamartoma
33 Aypical Melanocytic Lesions Melanoma precursors Dysplastic nevi / Clark s nevus / B-K mole Margins Treatment and re-exision



34 Correct terminology Dated termonology Dysplastic nevi originally described in 1978 by Wallace H. Clark Clark s nevus B-K mole Correct (Compound/Junctional) melanocytic nevus with architectural disorder and (mild/moderate/severe) atypia
 syndrome Lifetime risk for melanoma 10% Familial or sporadic occurrence of multiple dysplastic (atypical) nevi in an individual May have up")
35 Atypical Nevus 10% of melanocytic lesions received by pathology Dysplastic nevus syndrome In 1820 Norris reported the first case of what was originally called BK mole syndrome is now recognized as familial atypical mole/malignant melanoma syndrome (FAMM) syndrome Lifetime risk for melanoma 10% Familial or sporadic occurrence of multiple dysplastic (atypical) nevi in an individual May have up to 80 or more nevi that appear normal in childhood
36 ABCDE s Not all of these criteria need to be met Some melanomas only have one strike against them! A= Asymmetry B= Border C= Color D= Diameter > 6mm E= Evolution our newest and perhaps most important criteria!
37 E= Evolution My mole is changing My mole is growing My mole is itching This is a new mole


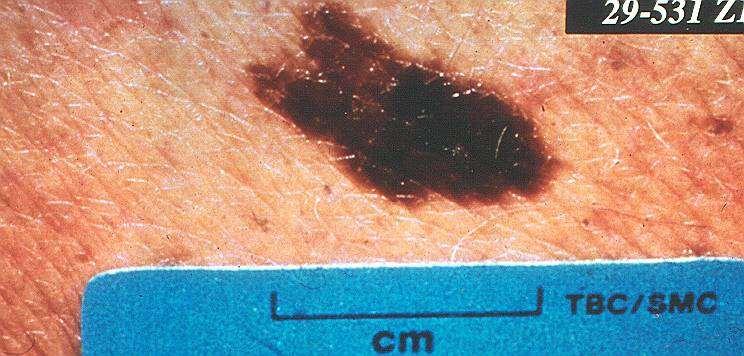
38 Atypical Nevus Clinical Larger than ordinary nevi Mixture of colors Pebbly surface
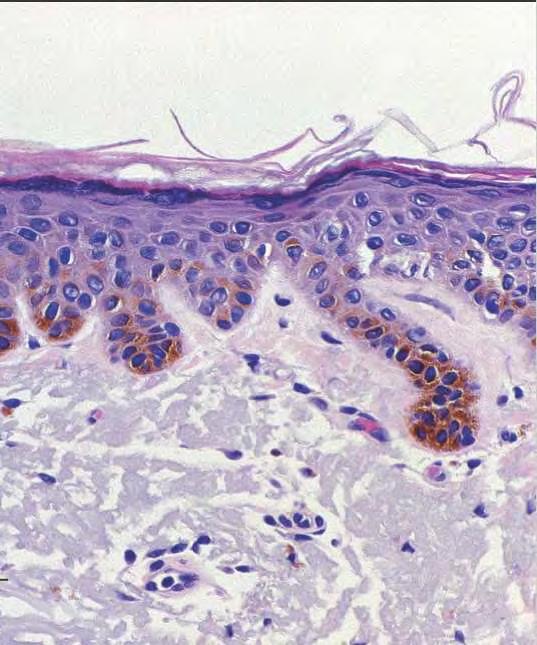
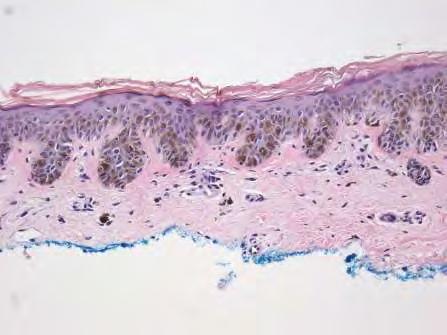
39 Atypical Nevus Junctional and compound melanocytic nevi can be atypical Histologically there are two components Architectural disorder Cytological atypia Mild Moderate re-excise if margin involved Severe re-excise if margin involved


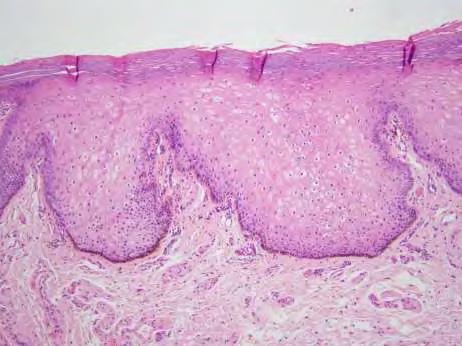
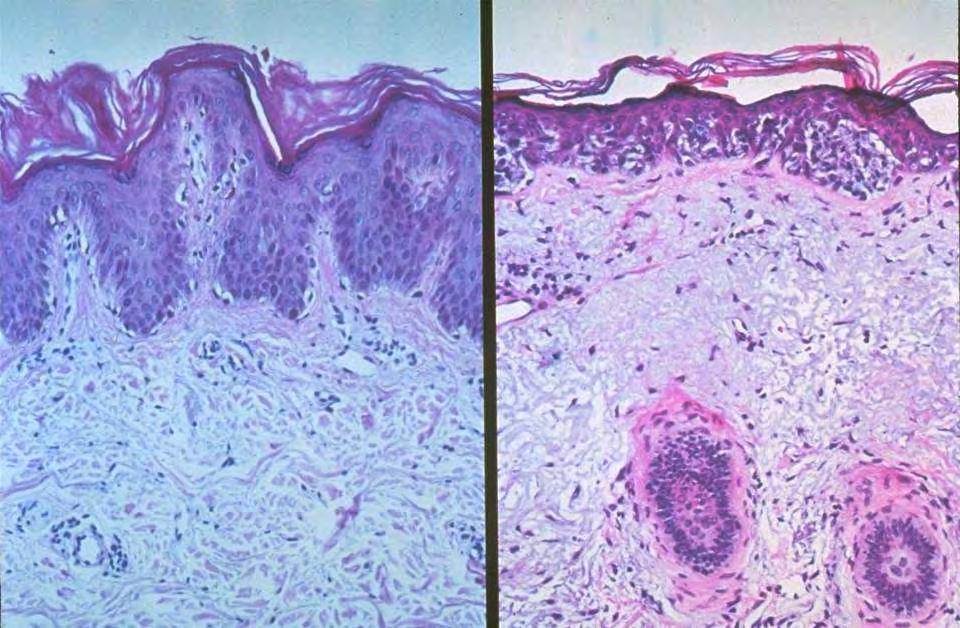
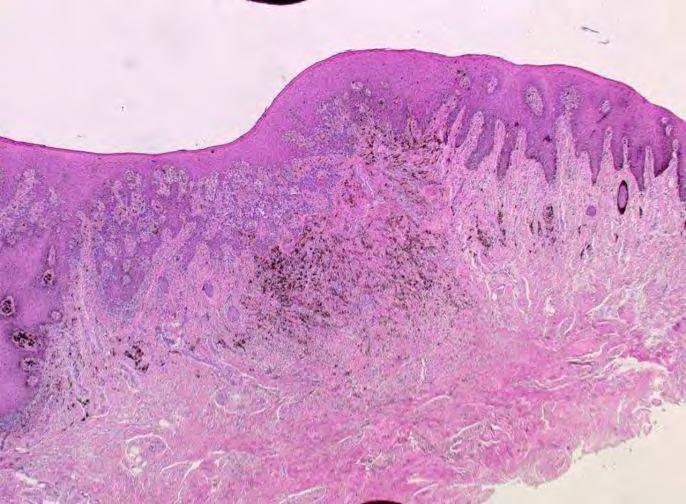
40 Atypical Nevus Architectural Disorder Poorly circumscribed Broad extension


41 Atypical Nevus Architectural Disorder Shouldering junctional nests of melanocytes extending beyond the dermal component Bridging of the rete ridges


42 Single and nested melanocytes along the sides and tips of the rete ridges Chronic inflammation Fibroplasia Pigment incontinence
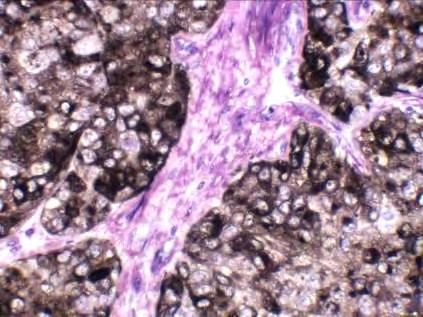
43 Atypical Nevus Cytological Atypia Mild Nucleus approximates size of keratinocyte nucleus Fine dusty cytoplasm Hyperchromatic nucleus, with mild pleomorphism Absent nucleolus Moderate re-excise 1-2x keratinocyte nucleus Fine dusty cytoplasm Hyperchromatic nucleus, with moderate pleomorphism Absent nucleus Severe re-excise 2x or greater keratinocyte nucleus Fine dusty cytoplasm Vesicular nucleus, with severe pleomorphism Prominent nucleolus Abundant cytoplasm
44 Atypical Nevus 1. Architectural disorder Shouldering proliferation of junctional nests of melanocytes extending beyond the dermal component Intraepidermal lentiginous hyperplasia of melanocytes Proliferation of melanocytes singly and in nests along the basal layer (sides and tips of rete ridges) 2. Cytological atypia Large hyperchromatic cells with prominent nucleoli (nuclei equal or larger than the nucleus of the overlying keratinocytes) Spindled Large epitheliod Stromal response Concentric lamellar fibroplasia Proliferation of dermal dendrocytes Patchy lymphocytic infiltrate Small vessel proliferation
45 Bottom line SAMPLE PATHOLOGY REPORT SKIN, RIGHT ARM, SHAVE BIOPSY: Compound melanocytic nevus with architectural disorder and mild cytological atypia Margins involved No re-excision necessary Close clinical follow up. If the lesion returns in 6 months re-excision may be necessary
46 Bottom line SAMPLE PATHOLOGY REPORT SKIN, RIGHT ARM, SHAVE BIOPSY: Compound melanocytic nevus with architectural disorder and moderate/severe cytological atypia Margins involved RE-EXCISE 2-5mm clinical margins

47 Malignant proliferation of melanocytes= Melanoma
48 Melanoma 1 in 80 Americans Incidence increased 1000% in past 50 years Risks Light complexions Light eyes Blond or red hair Blistering sunburns Heavy freckling Tanning poorly
49 Melanoma Most often begin from melanocytes at dermal-epidermal junction About half evolve from pre-existing nevi Horizontal and vertical growth phase Survival nearly ensured if lesion caught early!

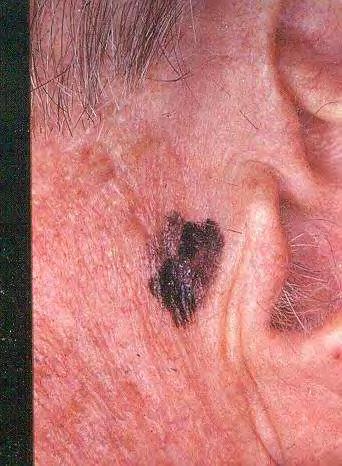
50 Confined to the epidermis Often found on face of elderly patients with sun damage Melanoma caught early has the best prognosis Melanoma in situ

51 Melanoma in situ= confined to the epidermis
52
53 Melanoma in situ Bottm line Re-excision with 5mm clincial margins

54 Invasive Melanoma Melanoma which has grown into the dermis This happens quickly in some patients but slowly in others Prognosis based on depth of invasion and presence of ulceration Sentinel node biopsy is a newer prognostic test

55 Invasive Melanoma Biopsy Critical Need to sample the entire lesion if possible Often requires excision either with sutures or deep shave If excision is not possible, do an incisional biopsy But tell your pathologist you are sending a piece of a very large lesion!
56 How to biopsy this lesion? Remove entire lesion with a margin, deep to fat

57
58

59
60

61

62

63 Amelanotic melanoma- difficult to diagnose
64
65

66 Acral lentiginous melanoma Most common type of melanoma in darker skinned patients Which famous singer died of this?

67

68
69 Invasive melanoma Breslow Depth <1mm Re-excision with 1cm clincal margins results in 90% survival

70 ABCDE s of Melanoma Not all of these criteria need to be met Some melanomas only have one strike against them! A= Asymmetry B= Border C= Color D= Diameter > 6mm E= Evolution our newest and perhaps most important criteria!
71 E= Evolution My mole is changing My mole is growing My mole is itching This is a new mole
72 Primary Melanoma: What factors influence prognosis? Depth of invasion is the single most important factor in survival --ulceration is next


73 Excision and FNA of Left Groin Mass

74 BRAF V600E mutation BRAF is a proto-oncogene. Mutations result in activation of signaling pathways that lead to uncontrolled cell growth and oncogenesis Roughly 50% of melanomas carry one of these mutations, most commonly a single amino acid change at position 600, V600E.
75 Treatment Surgical metastasectomy Immunotherapy High dose IL-2 Ipilimumab Monoclonal antibodies against programmed death 1 protein (PD-1) and its ligand (PD1-L1) MAPK pathway inhibition for BRAF positive patients Vemurafenib Dahrafenib Radiation Chemotherapy
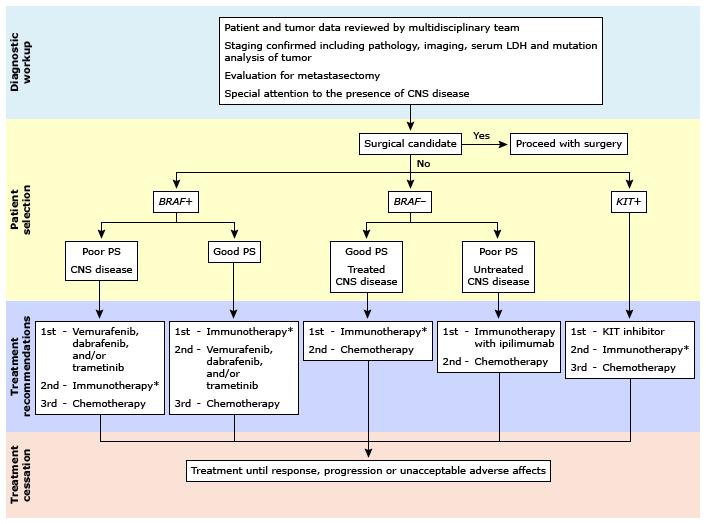
76 Treatment

77 Melanoma Survival

78 Melanoma Prevention Wear broad-spectrum sunblock! UVA and UVB blockers like titanium dioxide, zinc oxide, and mexoryl- and REAPPLY! Avoid mid-day sun exposure
LENTIGO SIMPLEX. Epidemiology
 LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Associate Clinical Professor of Dermatology MUSC
 Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Index. Springer-Verlag Berlin Heidelberg 2017 J.A. Plaza, V.G. Prieto, Pathology of Pigmented Skin Lesions, DOI /
 A Acral lentiginous (mucosal lentiginous) melanoma, 483 Acral lentiginous melanoma (ALM) asymmetric and irregular lentiginous junctional growth, 431 clinical features, 427 428 differential diagnosis, 428
A Acral lentiginous (mucosal lentiginous) melanoma, 483 Acral lentiginous melanoma (ALM) asymmetric and irregular lentiginous junctional growth, 431 clinical features, 427 428 differential diagnosis, 428
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Guy Perrot (Ги Перро)
") НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Sun Safety and Skin Cancer Prevention. Maryland Skin Cancer Prevention Program
 Sun Safety and Skin Cancer Prevention Maryland Skin Cancer Prevention Program Do You Know the Facts About Skin Cancer? Skin cancer is the most common cancer but also the most preventable Childhood sunburn
Sun Safety and Skin Cancer Prevention Maryland Skin Cancer Prevention Program Do You Know the Facts About Skin Cancer? Skin cancer is the most common cancer but also the most preventable Childhood sunburn
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
PATHOLOGY OF THE SKIN 2. Tumours of the skin
 PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College Tumour (Neoplasia) Benign or
PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College Tumour (Neoplasia) Benign or
MELANOMA. 4 Fitzroy Square, London W1T 5HQ Tel: Fax: Registered Charity No.
 MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Cancer Reporting for Dermatologists. Florida Department of Health Florida Cancer Data System. March 9, Agenda
 Cancer Reporting for Dermatologists Florida Department of Health Florida Cancer Data System March 9, 2011 Agenda Welcome Introductions Cancer Reporting in Florida BETA Participation Expectations Review
Cancer Reporting for Dermatologists Florida Department of Health Florida Cancer Data System March 9, 2011 Agenda Welcome Introductions Cancer Reporting in Florida BETA Participation Expectations Review
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma.
 Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
SKIN. 3. How is the skin structured around the finger joints to allow for flexible movement of the fingers?
 SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
SKIN Objectives for Exam #1: 1. List various skin structures and describe their functions. 2. Describe skin responses to increases and decreases in body temperature. 3. Provide examples of various skin
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Case Report Clear Cell Basal Cell Carcinoma
 SAGE-Hindawi Access to Research Volume 2011, Article ID 386921, 4 pages doi:10.4061/2011/386921 Case Report Clear Cell Basal Cell Carcinoma Deba P. Sarma, 1 Daniel Olson, 1 Jennifer Olivella, 1 Tracey
SAGE-Hindawi Access to Research Volume 2011, Article ID 386921, 4 pages doi:10.4061/2011/386921 Case Report Clear Cell Basal Cell Carcinoma Deba P. Sarma, 1 Daniel Olson, 1 Jennifer Olivella, 1 Tracey
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Talking to Your Clients About Skin Cancer. Objectives 9/9/2017. Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017
 Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
ARTICLE INFO ABSTRACT
 Melanocytic Pigmentation: A Single Manifestation of Myriad of Pathologies [PP: 05-09] Dr. Swapna Honwad Department of Oral Pathology dr.swapnahonwad@gmail.com Dr. Elsy P. Simon Department of Endodontics
Melanocytic Pigmentation: A Single Manifestation of Myriad of Pathologies [PP: 05-09] Dr. Swapna Honwad Department of Oral Pathology dr.swapnahonwad@gmail.com Dr. Elsy P. Simon Department of Endodontics
Appendix : Dermoscopy
 Go Back to the Top To Order, Visit the Purchasing Page for Details APP Appendix : Dermoscopy Dermoscopy, also known as dermatoscopy, epiluminoscopy and epiluminescent microscopy, is an effective non-invasive
Go Back to the Top To Order, Visit the Purchasing Page for Details APP Appendix : Dermoscopy Dermoscopy, also known as dermatoscopy, epiluminoscopy and epiluminescent microscopy, is an effective non-invasive
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Gross Appearance & Histology of Skin Cancer. Kyle Mannion M.D. January 21, 2005
 Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Melanoma what is it? Most aggressive and lifethreatening
 SUN,SURF AND MELANOMA Judy Brincat Dorevitch Pathology Heidelberg Victoria Melanoma what is it? Most aggressive and lifethreatening of cutaneous malignancies Develops from melanocytes. Adults and elderly
SUN,SURF AND MELANOMA Judy Brincat Dorevitch Pathology Heidelberg Victoria Melanoma what is it? Most aggressive and lifethreatening of cutaneous malignancies Develops from melanocytes. Adults and elderly
Lichenoid Tissue Reaction in Malignant Melanoma A Potential Diagnostic Pitfall
 natomic Pathology / LICHENOID TISSUE RECTION IN MLIGNNT MELNOM Lichenoid Tissue Reaction in Malignant Melanoma Potential Diagnostic Pitfall CPT Scott R. Dalton, MC, US, 1,3 Capt Matt. aptista, USF, MC,
natomic Pathology / LICHENOID TISSUE RECTION IN MLIGNNT MELNOM Lichenoid Tissue Reaction in Malignant Melanoma Potential Diagnostic Pitfall CPT Scott R. Dalton, MC, US, 1,3 Capt Matt. aptista, USF, MC,
Pigmented lesions of the Oral cavity
 Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Integumentary System
 Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Regression 2/3/18. Histologically regression is characterized: melanosis fibrosis combination of both. Distribution: partial or focal!
 Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Steven Robinson. Steven Robinson Memorial Endowment at
 fchwmt.org Steven Robinson Steven Robinson Memorial Endowment at Fair hair and skin Steven s story Grew up around water and loved being outdoors Experienced several sunburns as a child and young adult
fchwmt.org Steven Robinson Steven Robinson Memorial Endowment at Fair hair and skin Steven s story Grew up around water and loved being outdoors Experienced several sunburns as a child and young adult
Skin Cancers Emerging Trends and Treatment Approaches
 Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Brief Report. Shivanand Gundalli 1, Smita Kadadavar 1, Somil Singhania 1, Rutuja Kolekar 2 INTRODUCTION. Melanocytic Nevus
 Our Dermatology Online Histopathological spectrum of benign melanocytic nevi our experience in a tertiary care centre Shivanand Gundalli 1, Smita Kadadavar 1, Somil Singhania 1, Rutuja Kolekar 2 1 Department
Our Dermatology Online Histopathological spectrum of benign melanocytic nevi our experience in a tertiary care centre Shivanand Gundalli 1, Smita Kadadavar 1, Somil Singhania 1, Rutuja Kolekar 2 1 Department
EXCESSIVE SUN EXPOSURE A DANGER FACTOR FOR THE SKIN
 EXCESSIVE SUN EXPOSURE A DANGER FACTOR FOR THE SKIN When the weather warms up, we all like to get more sunshine. While better weather can make us feel brighter, we must also be aware of the dangers as
EXCESSIVE SUN EXPOSURE A DANGER FACTOR FOR THE SKIN When the weather warms up, we all like to get more sunshine. While better weather can make us feel brighter, we must also be aware of the dangers as
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Skin Cancer Awareness
 Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
EARLY ONLINE RELEASE
 EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Skin Malignancies. Presented by Dr. Douglas Paauw
 Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Associate Professor Amanda Oakley. Professor H. Peter Soyer. Academic Dermatologist The University of Queensland Brisbane. Dermatologist Hamilton
 Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-10:30 WS #3: Dermoscopy Workshop Part 1 11:00-13:00 WS
Associate Professor Amanda Oakley Dermatologist Hamilton Professor H. Peter Soyer Academic Dermatologist The University of Queensland Brisbane 8:30-10:30 WS #3: Dermoscopy Workshop Part 1 11:00-13:00 WS
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Disclosures. I have no conflicts of interest to disclose
 Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
CH 05 THE INTEGUMENTARY SYSTEM
 CH 05 THE INTEGUMENTARY SYSTEM This system consists of skin and its derivatives. The skin is one of the largest organs of the body in terms of surface area. The functions of the integumentary system include:
CH 05 THE INTEGUMENTARY SYSTEM This system consists of skin and its derivatives. The skin is one of the largest organs of the body in terms of surface area. The functions of the integumentary system include:
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations
 F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
MELANOMA IN ADOLESCENTS AND YOUNG ADULTS
 Cancer in Adolescents and Young Adults (AYA) Working Group MELANOMA IN ADOLESCENTS AND YOUNG ADULTS Emmanouil Saloustros MD, DSc General Hospital of Heraklion Venizelio Heraklion, Crete, Greece ESMO Preceptorship
Cancer in Adolescents and Young Adults (AYA) Working Group MELANOMA IN ADOLESCENTS AND YOUNG ADULTS Emmanouil Saloustros MD, DSc General Hospital of Heraklion Venizelio Heraklion, Crete, Greece ESMO Preceptorship
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest