Melanoma and Mimickers
|
|
|
- Laureen Blake
- 6 years ago
- Views:
Transcription
1 Melanoma and Mimickers Kara Walton, MD Assistant Professor of Dermatology and Dermatopathology Medical College of Wisconsin Disclosures No relevant financial disclosures 1
2 Objectives Recognize common benign melanocytic and nonmelanocytic lesions that may mimic melanoma Know when to be concerned about nail pigmentation or dystrophy Understand the limitations of biopsies of melanocytic lesions and how to biopsy suspicious lesions Identify when to refer patients to a specialist and who to refer to Epidemiology Lifetime incidence of melanoma: 1 in 49* Incidence has increased 5-7 fold over the past four decades, primarily in Caucasian population Mortality rates continue to increase in Caucasian males but are stable in females Leads to >90% of skin cancer deaths Median age at diagnosis: 61 years 82-85% present with localized disease, 10-13% with regional disease, 2-5% with metastatic disease *NCI SEER Database; NCCN melanoma guidelines,
3 Risk Factors for Melanoma Genetic Factors Family history of cutaneous melanoma Environmental Factors Intense intermittent sun exposure Phenotypic expressions of gene/environment interactions >100 acquired melanocytic nevi (8-10x increased relative risk) Lightly pigmented skin Chronic sun exposure >5 atypical nevi (4-6x increased relative risk) Tend to burn, unable to tan Residence near equator Multiple solar lentigines (3-4x increased relative risk) Red hair color PUVA (possible) Personal history of cutaneous melanoma DNA repair defects (eg. XP) Giant congenital nevus Tanning bed (esp <35 yo) Immunosuppression Diagnosis Early detection key in improving survival Clinical diagnosis based on visual inspection and dermoscopy In high risk patients, dermoscopic image storing and lesional or total body photography helpful Histopathology remains the gold standard for melanoma diagnosis Diagnostically difficult lesions may require additional molecular studies such as comparative genomic hypridization (CGH), fluorescence in situ hybridization (FISH) or gene expression profiling (GEP) 3

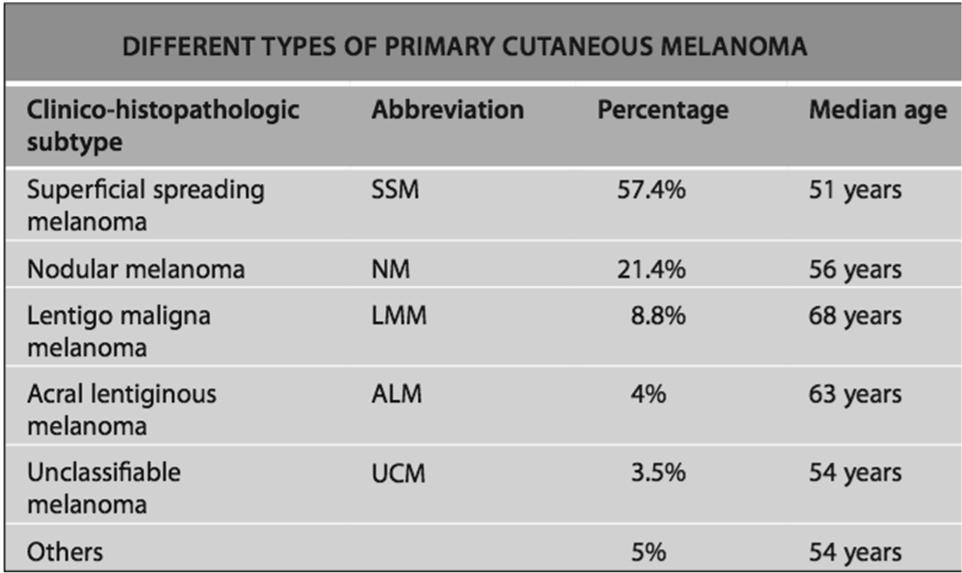
4 Types of Melanoma 4



5 Superficial spreading melanoma 60-70% of melanomas Females- lower extremities/upper back Males- upper back ~50% arise in a pre-existing nevus BRAF mutations common Most common variant in young individuals Mean age of diagnosis- 5 th decade Nodular melanoma 15-30% of melanomas Mean age: 6th decade Most commonly on trunk, head and neck Men>women No radial growth phase Rapid progression Poor prognosis 5
 Chronically sun damaged skin (face, dorsal hands) 5-20 year radial")

 Incidence similar across all ethnic groups Diagnosed")
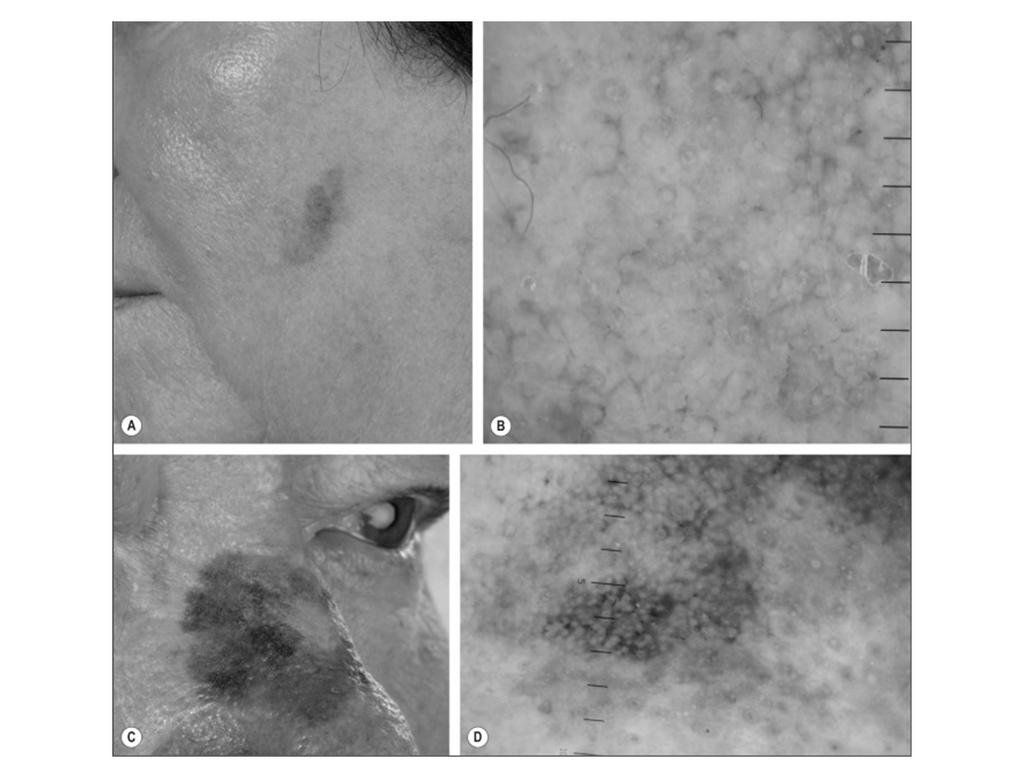
6 Lentigo maligna melanoma 10% of melanomas Older individuals (7 th decade), M=F ckit mutations (17%) Chronically sun damaged skin (face, dorsal hands) 5-20 year radial growth phase Lentigo maligna is precursor lesion: 5% progress to invasive melanoma Acral lentiginous melanoma 5% of melanomas Most in 7 th decade of life ckit mutations (>20%) Palms, soles, nails Most common type of MM in blacks and Asians (b/c low frequency of others) Incidence similar across all ethnic groups Diagnosed at advanced stage 6


7 MELANOMA VARIANTS Amelanotic melanoma Amelanotic variants for all melanoma subtypes Prognosis and therapy do not differ from pigmented subtypes Diagnosis often delayed More commonly seen in patients with OCA 7


8 Desmoplastic melanoma AKA spindled or neurotropic melanoma Skin colored, red, brown plaque Often occurs within lentigo maligna, acral lentiginous or mucosal melanoma Deep biopsy necessary Locally aggressive but mets are uncommon Ocular Melanoma Conjunctival or Uveal melanoma 5% of all melanomas Most common primary intraocular tumor in adults Uveal activating mutations in GNA11 or GNAQ Increased risk in nevus of Ota (esp Caucasians) 8




9 Melanocytic mimickers Clinically and histologically distinctive May occur sporadically or in a familial form Patients with multiple dysplastic nevi have increased risk of melanoma Clinically larger than acquired nevi, irregular in shape and uneven in color Important to document clinical stability Often have a benign dermoscopic pattern 9


10 Dysplastic Nevus Syndrome van der Rhee et al (2011) 10

 Biopsy lesions that appear de novo, are multinodular or plaque like or have")
11 Blue nevi Blue to blue-black, firm papule, nodule or plaque Small and wellcircumscribed, rarely larger than 1 cm Most common on dorsal aspects of hands and feet, face and scalp Often onset during childhood or adolescence Lesions that are clinically stable, small and in typical location can be monitored Malignant Blue Nevus Rare tumor of dermal melanocytes Most commonly arise in a cellular blue nevus; also within nevus of Ota or Ito, or de novo Scalp most common site >1cm High rate of recurrence and metastasis (LNs and lungs) Biopsy lesions that appear de novo, are multinodular or plaque like or have changed 11



12 Spitz nevi Red or pigmented papule or nodule, avg 8mm Can mimic melanoma clinically and histologically Generally homogenous color and well defined margins with smooth or verrucous surface Most common on lower extremities and head/neck region Usually in children or young adults; rare beyond years Pigmented spindle cell nevus Spindle cell variant of spitz nevus Dark brown to black macule or papule, usually <6mm Found in children or young adults Most common on extremities, esp thigh of young women Rare transformation to melanoma Rarely recur unless incompletely excised 12


13 Atypical spitz tumors and spitzoid melanoma Some shared histologic features of a Spitz nevus but more atypia, expansile growth, mitotic activity Can do FISH for diagnosis and/or prognostication 13


14 Halo nevi White halo around a nevus; nevus may be flat or raised and have surface scale or crusting Usually preceding erythema; lesions regress over months to years Most common on trunk in teenagers with increased number of nevi; up to 50% will have two or more Histologically lymphocytes infiltrate nevus Most often benign dermoscopic pattern ~20% of pts with halo nevi have vitiligo New onset of multiple halo nevi can be a sign of an ocular melanoma or cutaneous melanoma elsewhere, esp in older adults May appear following immunotherapy for melanoma, eg imatinib, tocilizumab, nivolumab Recurrent nevi Fairly common following shave biopsy May clinically and histologically resemble melanoma Most common on trunk of young females Often within 6 mos Pigment confined to area of scar and stable over yrs Concerning dermoscopic features Repeat biopsy if progressive enlargement, extension beyond scar or longer time interval before recurrence* 14


15 Melanoma with regression Usually asymmetric white areas or irregular halo as compared with halo nevi Well-circumscribed, round to oval, brown to black macules; 3mm-2cm Homogenous pigment or mottled appearance Almost always multiple; sun exposed sites Indicates chronic UV exposure and risk for cutaneous carcinomas Lentigo maligna shows greater pigment variation, irregular borders, atypical dermoscopic features Solar lentigines 15
16 Non-melanocytic mimickers 16

17 Seborrheic keratoses Appear 4 th decade of life Can be anywhere excepth mucous membranes, palms and soles Tan to black, macular, papular or verrucous lesions; waxy stuck-on appearance Some lesions difficult or impossible to differentiate clinically from melanoma Can usually differentiate with dermoscopy Can have collision tumors 17

18 Sign of Leser-Trelát 18



19 Pyogenic granuloma Rapidly growing, friable red papule or polyp of skin or mucosa May occur following minor trauma; associated with some medications More common in children, young adults, pregnant women (esp gingiva) Some consider reactive vascular hyperplasia rather than neoplasm May mimic amelanotic melanoma Angiokeratoma Small, warty, black papule, most common on LE Due to chronic irritation or injury to the wall of venules Dermoscopy can distinguish between angiokeratoma and melanoma 19
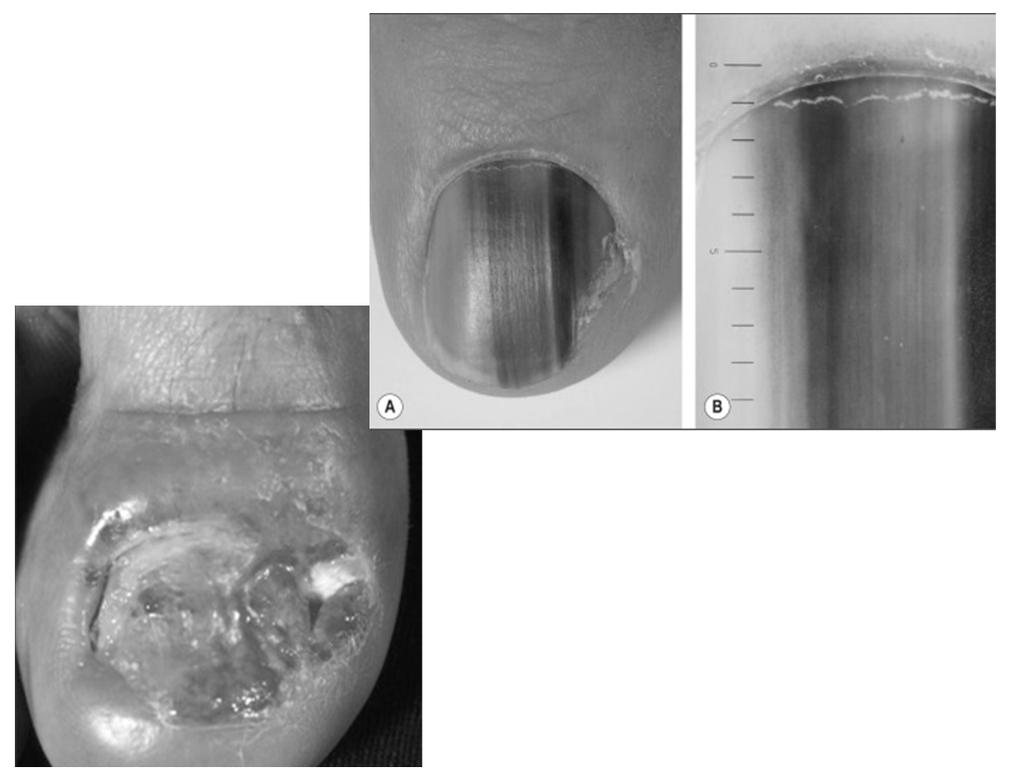
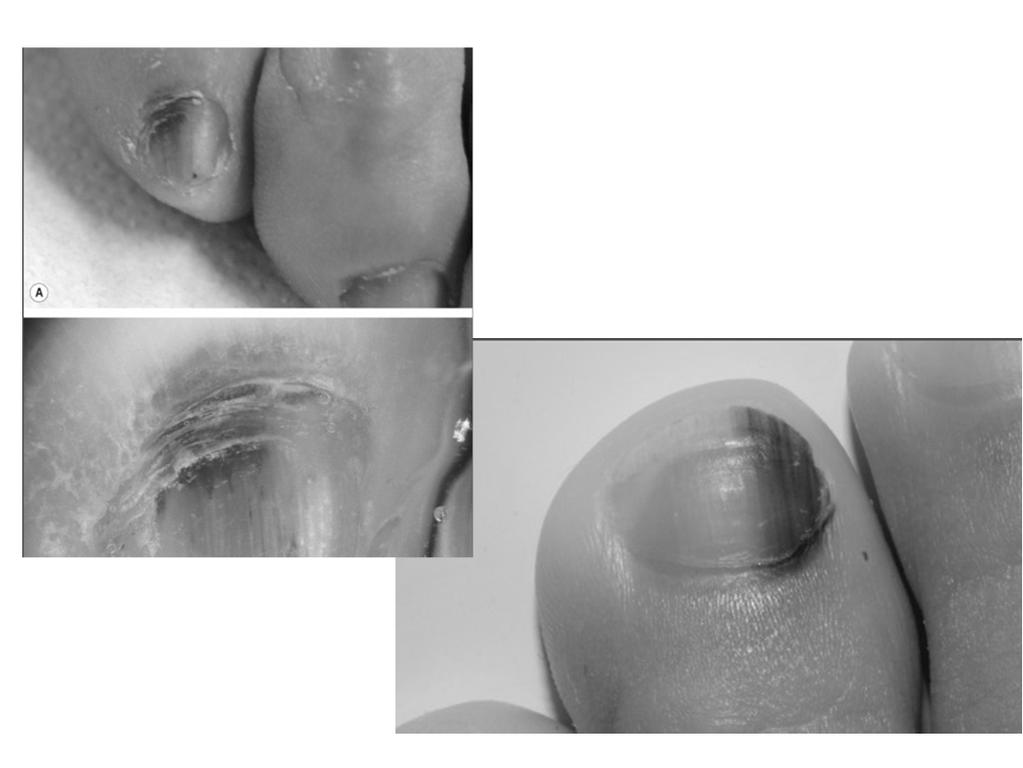
20 Nail lesions Nail melanoma Nail melanoma most commonly presents with longitudinal melanonychia In ~25 % of pts, the lesion is amelanotic Most frequently involves the thumb, index finger and great toe Diagnosis often delayed and 5 yr survival only 15% Peak incidence 5 th -7 th decades Africans, Asians and native americans up to 1/3 of cases Width of band usually greater than 3 mm and may have Hutchinson s sign 20
21 21
22 In general Rule out exogenous pigment Fungal, hematoma, pyocyanin Only one nail affected in an adult (even if amelanotic) biopsy In child usually due to nevus; if rapidly enlarging or whole nail involved need to biopsy Many nails Drugs Racial melanonychia Medications Inflammatory Evaluation of patient with suspected melanoma Medical history Risk factors History of lesion ROS TBSE and lymph node exam If suspect melanoma Excisional biospy with narrow margins recommended (1-2mm) Deep saucerization many be used for flat lesions or low suspicion for melanoma Thoroughly document site of biopsy Communicate size of lesion and type of biopsy to the pathologist 22

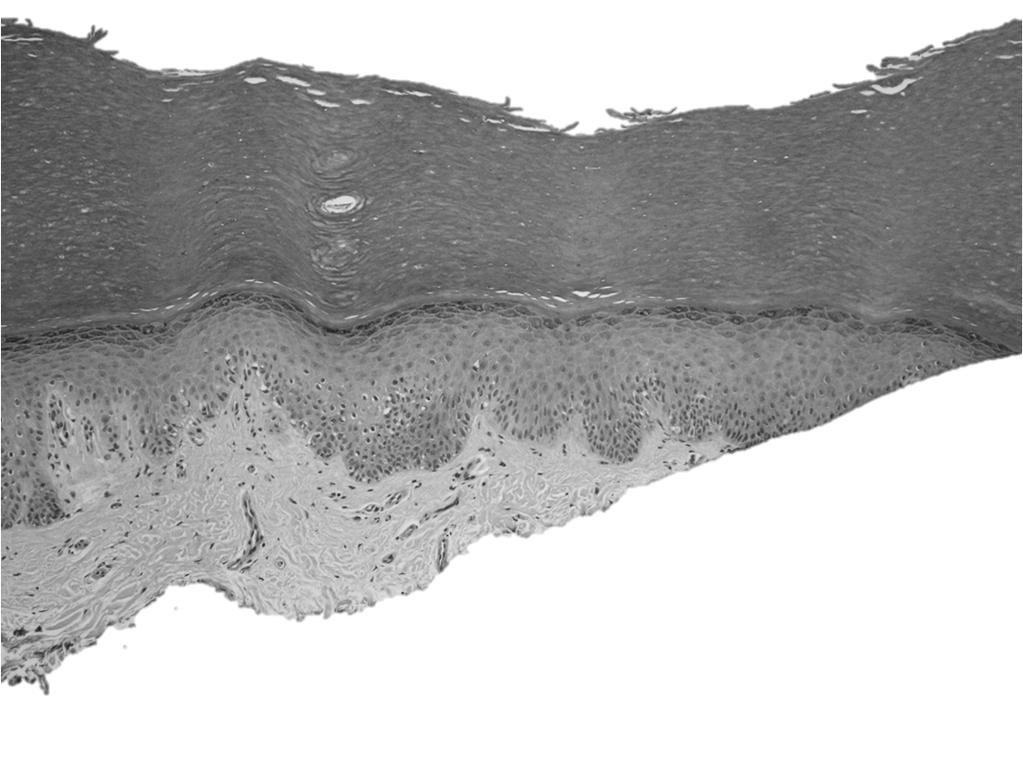
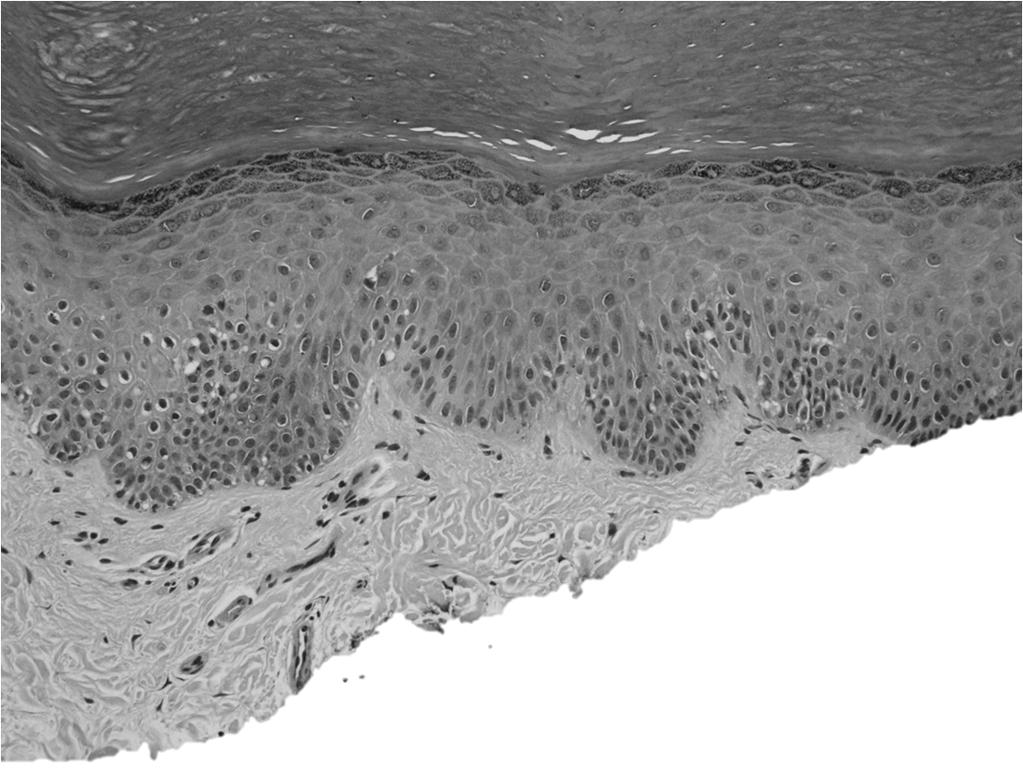
23 The gold standard The gold standard 23

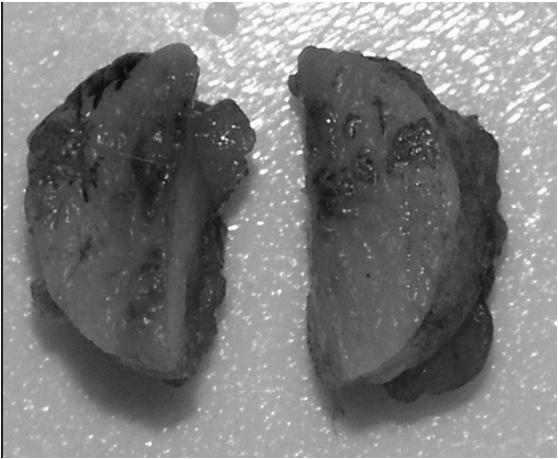
24 Lesion A 24
25 25

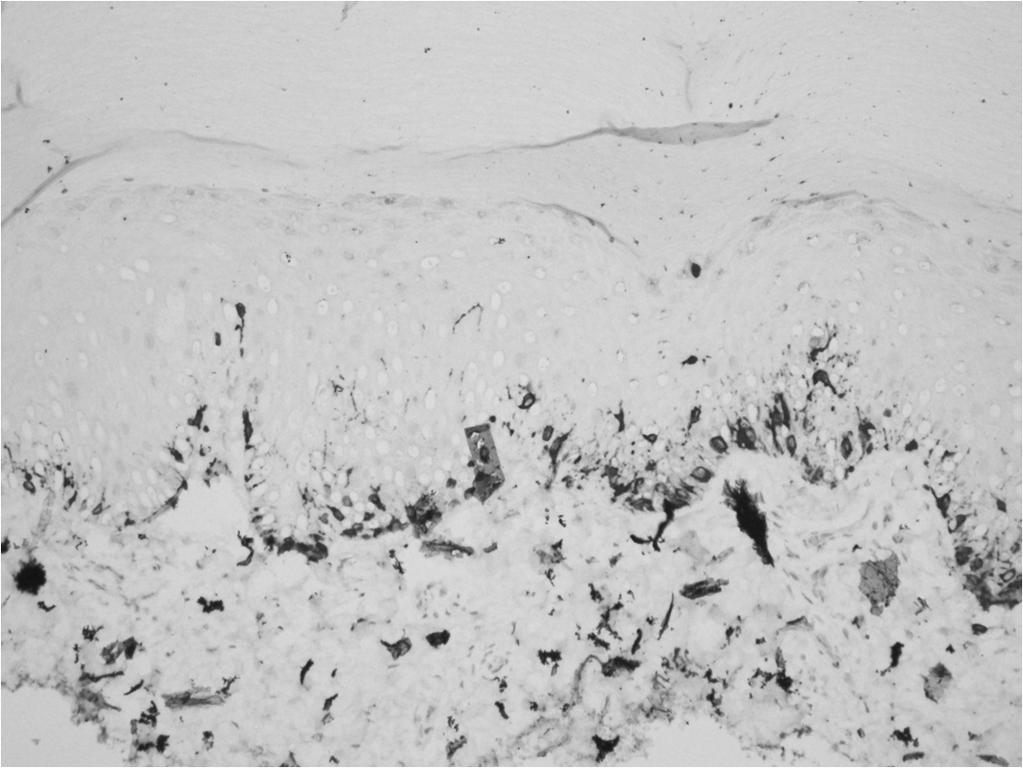
26 1/16/2018 MELAN-A MELAN-A 26

27 Lesion B 27

28 1/16/
29 Which is the melanoma? A B Lesion A Further clinical history obtained from the clinician Lesion 3 mm in size Present for years, stable in size but possibly darker per patient 29


30 Lesion B Spoke to clinician s office Offered to photo 30
31 Treatment Staging of Melanoma American Joint Committee on Cancer (AJCC) New guidelines (version 8) to take effect Jan 1,
32 Staging- TNM N 32

33 M Clinical Staging Melanoma AJCC T N M Stage T1a N0 M0 IA T1b N0 M0 IB T2a N0 M0 IB T2b N0 M0 IIA T3a N0 M0 IIA T3b N0 M0 IIB T4a N0 M0 IIB T4b N0 M0 IIC Any T >/= N1 M0 III Any T Any N M1 IV 33
- 52% Stage III C (T1-4b/N1b or N2b/Mo OR any T and N3)- 26% Stage IV- any T/N with M1-6-18% Management of Melanoma National Comprehensive Cancer Network")
34 Prognosis (5 year survival) Stage IA/B (T1a-T2a/N0/M0)- >90% Stage IIA (T2b-T3a/N0/M0)-78% Stage IIB (T3b-T4a/No/Mo)- 65% Stage IIC (T4b/No/Mo)-45% Stage III A (T1-4a/N1a-N2a/M0)- 66% Stage III B(T1-4B/N1a or N2a/Mo OR T1-4a/N1b or N2b)- 52% Stage III C (T1-4b/N1b or N2b/Mo OR any T and N3)- 26% Stage IV- any T/N with M1-6-18% Management of Melanoma National Comprehensive Cancer Network (NCCN guidelines): 2016 version 34
35 Surgical management for primary melanoma Tumor Thickness In situ 1 mm Recommended Margins 0.5 cm 1.0 cm 1.01 mm- 2mm 1-2 cm mm 2.0 cm >4 mm 2.0 cm -- Margins may be modified to accommodate individual anatomic or functional considerations. --Excision recommendations are based on clinical margins taken at the time of surgery and not gross or histologic margins, as measured by the pathologist Sentinel Lymph Node Biopsy Sentinel node = 1st to receive metastases Identifies patients with subclinical nodal metastases, at high risk for recurrence, who should receive CLND and adjuvant therapy Useful for staging Impact on overall survival has not been proven 5-30% patients with Stage I-II are upstaged to Stage III after SLNB 35
36 Sentinel Lymph Node Biopsy 2013 NCCN recommendations/asco Indicated for melanomas >1mm thick <1mm Breslow, risk of regional node mets is 5% SLNB recommended if high risk features (ulceration, mitoses) Clinically apparent regional lymph nodes Surgical lymphadenectomy Management of Melanoma Stage 0 in situ- wide excision Stage Ia: WLE Stage Ib ( 0.75mm, ±ulceration, ±mitotic rate >1/mm2)- wide excision, consider SLNB, CT/PET/MRI only if symptomatic Stage IIa (0.76mm-1mm, no ulceration, mitotic rate< 1/mm2)- wide excision, consider SLNB, CT/PET/MRI only if symptomatic 36
37 Melanoma Surveillance No standard guidelines Risk of secondary primary cutaneous melanomas Risk of local recurrence (4%, greatest in first 2-5 years) Risk of late recurrence (>15 years) Risk of other cutaneous and noncutaneous malignancies Most recommend 4x/year visit with derm for 2 years then Q6-12 months for life Summary Diagnostic accuracy for clinical diagnosis of melanoma does not exceed 75%, may be increased to 90% with expert use of dermoscopy History of change in color, size or shape of pigmented lesion most sensitive clinical sign; clinical context important If one pigmented or dystrophic nail in adult biopsy When possible, excisional biopsy is the preferred method for sampling lesions concerning for melanoma; communicate with dermatopathologist Patients with dysplastic nevus syndrome and/or high risk for melanoma should be referred to dermatology for close dermatologic surveillance 37
38 References Bolognia, Jean L., MD; Schaffer, Julie V., MD; Cerroni, Lorenzo, MD. Dermatology, 4 th Edition, 2018, Elsevier. Garbe C, and Leiter U: Melanoma epidemiology and trends. Clin Dermatol 2009; 27: pp. 3-9 Siegel RL, Miller KD, and Jemal A: Cancer statistics, CA Cancer J Clin 2017; 67: pp Meyle KD, and Guldberg P: Genetic risk factors for melanoma. Hum Genet 2009; 126: pp Geller AC, Clapp RW, Sober AJ, et al: Melanoma epidemic: an analysis of six decades of data from the Connecticut Tumor Registry. J Clin Oncol 2013; 31: pp Wellbrock C: Melanoma and the microenvironment age matters. N Engl J Med 2016; 375: pp Lasithiotakis K, Leiter U, Meier F, et al: Age and gender are significant independent predictors of survival in primary cutaneous melanoma. Cancer 2008; 112: pp Goldstein AM, Chan M, Harland M, et al: Features associated with germline CDKN2A mutations: a GenoMEL study of melanoma-prone families from three continents. J Med Genet 2007; 44: pp Bauer J, and Garbe C: Risk estimation for malignant transformation of melanocytic nevi. Arch Dermatol 2004; 140: pp. 127 Tsao H, Bevona C, Goggins W, and Quinn T: The transformation rate of moles (melanocytic nevi) into cutaneous melanoma. A population based estimate. Arch Dermatol 2003; 139: pp Paradela S, Fonseca E, Pita S, et al: Spitzoid melanoma in children: clinicopathological study and application of immunohistochemistry as an adjunct diagnostic tool. J Cutan Pathol 2009; 36: pp Cerroni L, and Kerl H: Simulators of malignant melanoma of the skin. Eur J Dermatol 1998; 8: pp AJCC Cancer Staging Manual : American Joint Committee on Cancer. New York: Springer, pp Bichakjian CK, Halpern AC, Johnson TM, et al: Guidelines of care for the management of primary cutaneous melanoma. American Academy of Dermatology. J Am Acad Dermatol 2011; 65: pp aries MB, Thompson JF, Cochran AJ, et al: Completion dissection or observation for sentinel-node metastasis in melanoma. N Engl J Med 2017; 376: pp
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
MELANOMA IN ADOLESCENTS AND YOUNG ADULTS
 Cancer in Adolescents and Young Adults (AYA) Working Group MELANOMA IN ADOLESCENTS AND YOUNG ADULTS Emmanouil Saloustros MD, DSc General Hospital of Heraklion Venizelio Heraklion, Crete, Greece ESMO Preceptorship
Cancer in Adolescents and Young Adults (AYA) Working Group MELANOMA IN ADOLESCENTS AND YOUNG ADULTS Emmanouil Saloustros MD, DSc General Hospital of Heraklion Venizelio Heraklion, Crete, Greece ESMO Preceptorship
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
LENTIGO SIMPLEX. Epidemiology
 LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Corporate Medical Policy
 Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Clinicopathologic Self- Assessment S003 AAD 2017
 Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
Professor Michael Eccles
 Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Practical Tips for Caring for Melanoma Patients
 Practical Tips for Caring for Melanoma Patients Caroline C. Kim, MD, Director Assistant Professor, Department of Dermatology Harvard Medical School Director, Pigmented Lesion Clinic Associate Director,
Practical Tips for Caring for Melanoma Patients Caroline C. Kim, MD, Director Assistant Professor, Department of Dermatology Harvard Medical School Director, Pigmented Lesion Clinic Associate Director,
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision
 Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MALIGNANT MELANOMA. Dr D. Tenea Department of Dermatology University of Pretoria
 MALIGNANT MELANOMA Dr D. Tenea Department of Dermatology University of Pretoria BACKGROUND History MM. of the skin is a malignant neoplasm of the epidermal melanocytes The incidence rates show considerable
MALIGNANT MELANOMA Dr D. Tenea Department of Dermatology University of Pretoria BACKGROUND History MM. of the skin is a malignant neoplasm of the epidermal melanocytes The incidence rates show considerable
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Skin Tumors in Children
 AAD San Diego S021 2018 Skin Tumors in Children Jane M. Grant-Kels, MD,FAAD grant@uchc.edu Founding Chair Emeritus, Derm Dept, UCONN Vice Chair Dept of Dermatology Professor of Dermatology, Pathology and
AAD San Diego S021 2018 Skin Tumors in Children Jane M. Grant-Kels, MD,FAAD grant@uchc.edu Founding Chair Emeritus, Derm Dept, UCONN Vice Chair Dept of Dermatology Professor of Dermatology, Pathology and
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper:
 This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma.
 Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham
 Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham Classifying melanoma Melanoma (site of origin, thickness,
Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham Classifying melanoma Melanoma (site of origin, thickness,
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines
 CLINICAL GUIDANCE The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines Julia Newton Bishop, Veronique Bataille, Alice Gavin, Marko Lens, Jerry Marsden, Tania Mathews
CLINICAL GUIDANCE The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines Julia Newton Bishop, Veronique Bataille, Alice Gavin, Marko Lens, Jerry Marsden, Tania Mathews
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Poor prognosis for thin ulcerated melanomas and implications for a more aggressive approach to treatment
 Poor prognosis for thin ulcerated melanomas and implications for a more aggressive approach to treatment Makenzie L. Hawkins, MSPH 1 Matthew J. Rioth, MD 1,2 Megan M. Eguchi, MPH 1 Myles Cockburn, Phd
Poor prognosis for thin ulcerated melanomas and implications for a more aggressive approach to treatment Makenzie L. Hawkins, MSPH 1 Matthew J. Rioth, MD 1,2 Megan M. Eguchi, MPH 1 Myles Cockburn, Phd
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern
 Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons
 Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Challenges in Melanoma Diagnosis and Management
 Challenges in Melanoma Diagnosis and Management Winter Clinical Dermatology Conference - Hawaii Darrell S. Rigel, MD MS Clinical Professor of Dermatology New York University Medical Center DISCLOSURE OF
Challenges in Melanoma Diagnosis and Management Winter Clinical Dermatology Conference - Hawaii Darrell S. Rigel, MD MS Clinical Professor of Dermatology New York University Medical Center DISCLOSURE OF
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre
 Malaysian J Pathol 202; (2) : 97 0 ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre Jayalakshmi PAILOOR, Kein-Seong
Malaysian J Pathol 202; (2) : 97 0 ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre Jayalakshmi PAILOOR, Kein-Seong
Dr. Brent Doolan, BSc MBBS MPH
 Impact of partial biopsies on the need for complete excisional surgery in the management of cutaneous melanomas: A multi-centre review Dr. Brent Doolan, BSc MBBS MPH Peter MacCallum Cancer Centre, Melbourne
Impact of partial biopsies on the need for complete excisional surgery in the management of cutaneous melanomas: A multi-centre review Dr. Brent Doolan, BSc MBBS MPH Peter MacCallum Cancer Centre, Melbourne
World Articles of Ear, Nose and Throat Page 1
 World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Katsuhiro Yamada, Natsuko Noguti, Masaaki Tsuda, Hazime Nagato, Naoko Hasunuma, Yoshihiro Umebayashi and Motomu Manabe
 Akita J Med 36 : 45-52, 2009 45 Katsuhiro Yamada, Natsuko Noguti, Masaaki Tsuda, Hazime Nagato, Naoko Hasunuma, Yoshihiro Umebayashi and Motomu Manabe (Received 22 December 2008, Accepted 15 January 2009)
Akita J Med 36 : 45-52, 2009 45 Katsuhiro Yamada, Natsuko Noguti, Masaaki Tsuda, Hazime Nagato, Naoko Hasunuma, Yoshihiro Umebayashi and Motomu Manabe (Received 22 December 2008, Accepted 15 January 2009)
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures