DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY. Daniel A. West, MD I HAVE NO RELEVENT RELATIONSHIPS WITH ANY COMPANIES
|
|
|
- Michael Snow
- 5 years ago
- Views:
Transcription
1 DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Daniel A. West, MD I HAVE NO RELEVENT RELATIONSHIPS WITH ANY COMPANIES

2 The most likely diagnosis is: A. Allergic contact dermatitis B. Pemphigus vulgaris C. Psoriasis D. Tinea corporis E. Tinea versicolor



3
4 The most likely diagnosis is: A. Allergic contact dermatitis B. Pemphigus vulgaris C. Psoriasis D. Tinea corporis E. Tinea versicolor
5 Epidemiology All races Male = female Peak age of onset years 90% cases before 40 years

6
7 Arthritis Variable, but up to 20-40% Types: Asymmetric oligoarticular Symmetric polyarticular DIP Ankylosing spondylitis Arthritis mutilans
8 Type 1 and 2 psoriasis? Henseler and Christophers Type 1 psoriasis (onset age <40 y), and type 2 psoriasis (onset age >40 y) Type 1: increased in first-degree relatives, increased HLA linkage, more severe disease Type 2: sporadic, less familial, less HLA linkage, less severe
9 Infection HIV Triggers Trauma (physical, chemical, electrical, etc) Pregnancy Drugs (b-blockers, lithium, steroid withdrawal, NSAIDS, antimalarials) Smoking




10



11


12


13 Distractors Pemphigus vulgaris* Allergic contact dermatitis*


14 Tinea corporis* Incorrect Choices Tinea versicolor*
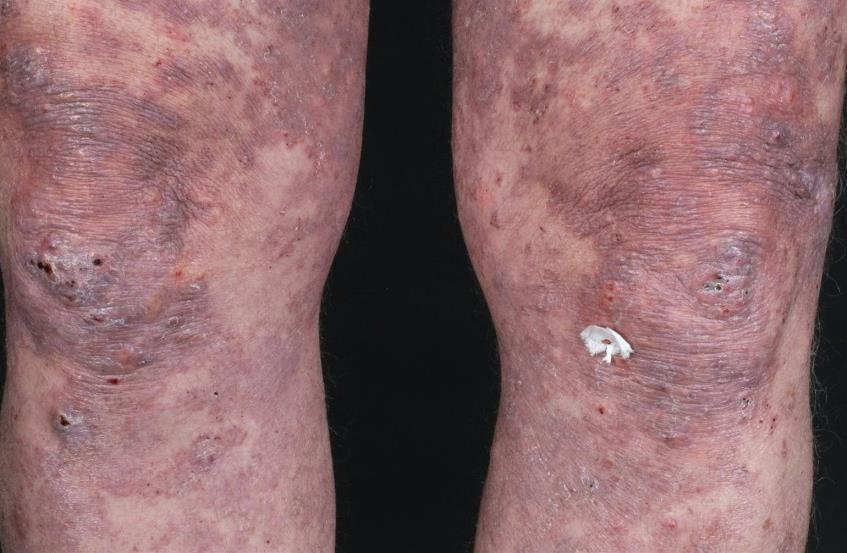
15 The most likely diagnosis is: A. Arterial ulcer B. Lipodermatosclerosis C. Livedoid vasculopathy D. Pyoderma gangrenosum E. Venous stasis ulcer

16
17 The most likely diagnosis is: A. Arterial ulcer B. Lipodermatosclerosis C. Livedoid vasculopathy D. Pyoderma gangrenosum E. Venous stasis ulcer
18 Pathergy Pyoderma gangrenosum Satellite purple papules will appear just distal to the edge of the ulcer and eventually ulcerate Painful with violaceous overhanging border Bullous forms 50% patients with underlying disease Inflammatory bowel disease is most common Therapy often difficult


19 Arterial ulcer Distractors Lipodermatosclerosis*


20 Distractors Livedoid vasculopathy* Venous stasis*
21 The most likely diagnosis is: A. Contact dermatitis B. Psoriasis C. Minocycline hyperpigmentation D. Phytophotodermatitis E. Photodrug eruption
22 The most likely diagnosis is:
23 The most likely diagnosis is: A. Contact dermatitis B. Psoriasis C. Minocycline hyperpigmentation D. Phytophotodermatitis E. Photodrug eruption
24 Photodrug eruption Broad types of photodrug eruptions Phototoxic Photoallergic
25 Phototoxic Photodrug eruption Does not require sensitization Resembles exaggerated sunburn Pain > itch Can develop quickly, i.e. within hours Photoallergic Requires sensitization Resembles contact dermatitis Itch > pain Potentially more delayed
26 Phototoxic Oral > topical Photodrug eruption Amiodarone, tetracyclines, quinolones, sulfonamides, NSAIDs, thiazides, psoralens, voriconazole, phenothiazines, hypericin Photoallergic Topical > oral Sunscreens, fragrances, chlorhexidine NSAIDs, phenothiazines, griseofulvin
27 Unique phototoxic reactions Psuedoporphyria Photo-onycholysis Slate-gray hyperpigmentation Phytophotodermatitis


28




29


30 Contact dermatitis* Distractors Psoriasis*


31 Minocycline hyperpigmentation Distractors Phytophotodermatitis
32 The most likely diagnosis is: A. Calciphylaxis B. Erythema induratum C. Erythema nodosum D. Leukocytoclastic vasculitis E. Toxic epidermal necrolysis

33
34 The most likely diagnosis is: A. Calciphylaxis B. Erythema induratum C. Erythema nodosum D. Leukocytoclastic vasculitis E. Toxic epidermal necrolysis

35


36
37 Calciphylaxis Rare disorder with high mortality rate Cutaneous ischemia and necrosis secondary to calcification, intimal fibroplasia and thrombosis of pannicular arterioles Commonly affects individuals with end-stage renal failure High levels of serum calcium and phosphate Risk factors include hyperparathyroidism, elevated calcium-phosphate product, diabetes mellitus, female gender, obesity, warfarin use and protein C or S deficiency, liver disease, systemic corticosteroid use Typical clinical presentation: painful ischemic purpura and necrotic ulceration



38 Distractors Erythema induratum Erythema nodosum*


39 Distractors Leukocytoclastic vasculitis Toxic epidermal necrolysis*
40 The most likely diagnosis is: A. Plasma cell balanitis B. Lichen planus C. Lichen sclerosus D. Herpes simplex infection E. Aphthosis
41

42 The most likely diagnosis is: A. Plasma cell balanitis B. Lichen planus C. Lichen sclerosus D. Herpes simplex infection E. Aphthosis


43

44

45
46 Lichen sclerosus Sclerotic and atrophic white patches and plaques with associated erosion or ulceration Occurs in all ages Genitalia most commonly affected Complications: scarring, phimosis, squamous cell carcinoma Pruritus common complaint


47 Plasma cell balanitis Distractors Lichen planus*

48 Distractors Herpes simplex infection*
49 A 48 year old woman presents with several months of a progressive itchy rash that started on the upper torso and spread to the lower torso and extremities including the palms and soles. The most likely diagnosis is: A. Ichthyosis vulgaris B. Lichen planus C. Pityriasis lichenoides D. Pityriasis rosea E. Pityriasis rubra pilaris

50

51 A 48 year old woman presents with several months of a progressive itchy rash that started on the upper torso and spread to the lower torso and extremities including the palms and soles. The most likely diagnosis is: A. Ichthyosis vulgaris B. Lichen planus C. Pityriasis lichenoides D. Pityriasis rosea E. Pityriasis rubra pilaris


52

53

54

55
56 Pityriasis rubra pilaris Coalescence of orange-red plaques with islands of sparing Cephalocaudad spread Orange-red waxy keratoderma of palms and soles Follicular papules on an erythematous base on dorsal fingers Varying degrees of exfoliation Thickened nail plate with subungual hyperkeratosis



57 Ichthyosis vulgaris* Distractors Lichen planus* Pityriasis lichenoides*

58 Distractors Pityriasis rosea*
59 The most likely diagnosis is: A. Eruptive xanthomas B. Erythema elevatum diutinum C. Lichen amyloidosis D. Lichen planus E. Necrobiosis lipoidica


60
61 The most likely diagnosis is: A. Eruptive xanthomas B. Erythema elevatum diutinum C. Lichen amyloidosis D. Lichen planus E. Necrobiosis lipoidica
62 Eruptive xanthomas Erythematous to yellow papules Extensor extremities, buttocks and hands May be accompanied by pruritus or tenderness Occur in setting of primary or secondary hypertriglyceridemia (>3000 to 4000mg/dL) Type I, IV and V hypertriglyceridemias

63


64


65


66 Distractors Erythema elevatum diutinum Lichen amyloidosis

67 Lichen planus* Distractors Necrobiosis lipoidica*
68 The most likely diagnosis is: A. Arsenical keratoses B. Keratoderma climactericum C. Erythema multiforme D. Punctate keratoderma E. Syphilis
69

70 The most likely diagnosis is: A. Arsenical keratoses B. Keratoderma climactericum C. Erythema multiforme D. Punctate keratoderma E. Syphilis
71 Syphilis Chronic infection caused by Treponema pallidum Intermittent disease with primary, secondary and tertiary stages Variety of clinical presentations Secondary syphillis is associated with systemic signs including fever, malaise and adenopathy




72 Syphilis


73 Distractors Arsenical keratoses Keratoderma climactericum


74 Erythema multiforme* Distractors Punctate keratoderma
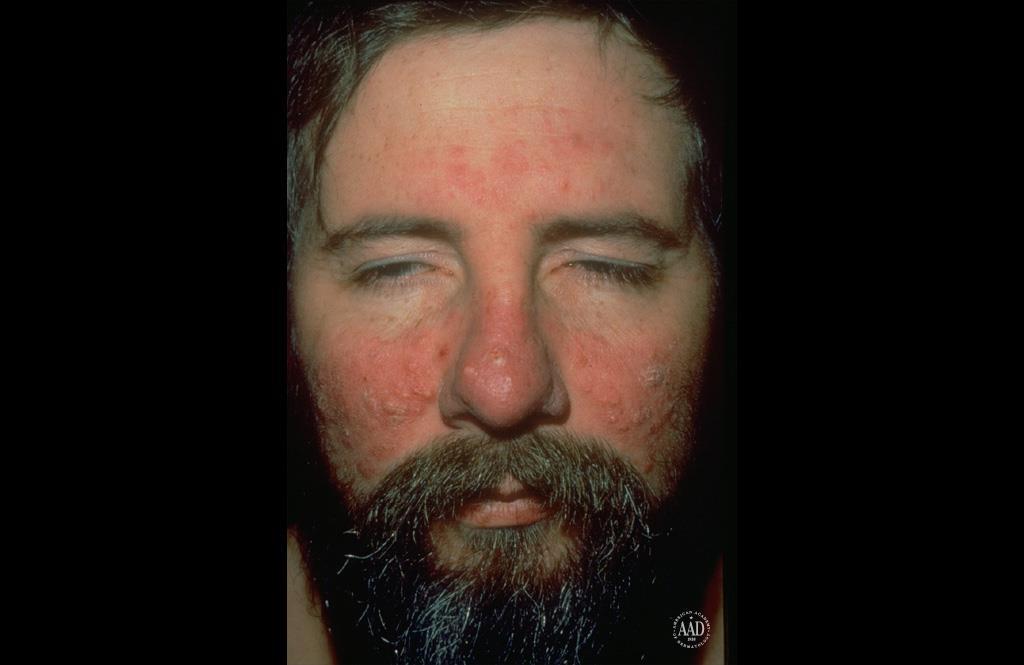
75 A 65 year-old man presented with this condition. He said it gets worse in the sun. The most likely diagnosis is: A. Allergic contact dermatitis B. Erysipelas C. Lupus erythematosus D. Rosacea E. Seborrheic dermatitis
76
77 A 65 year-old man presented with this condition. He said it gets worse in the sun. The most likely diagnosis is: A. Allergic contact dermatitis B. Erysipelas C. Lupus erythematosus D. Rosacea E. Seborrheic dermatitis
78 Rosacea Inflammatory condition of the pilosebaceous unit Exact cause unknown Known triggers UV light Alcohol Spicy food Extremes in temperature Stress
79 Clinical features Rosacea Erythematotelangiectatic (vascular): flushing, erythema, telangiectasia Papulopustular Phymatous: especially rhinophyma Ocular: dry or gritty sensation, blepharitis, conjuntivitis Rosacea fulminans (pyoderma faciale): very severe form
80 Treatement Avoid triggers Metronidazole Azeleic acid Sulfacetamide +/- sulfur Brimonidine Cyclosporine drops (ocular) Tetracyclines Azithromycin Isotretinoin Lasers Rosacea
81

82

83 Distractors Erysipelas Allergic contact dermatitis*


84 Distractors Lupus erythematosus* Seborrheic dermatitis*
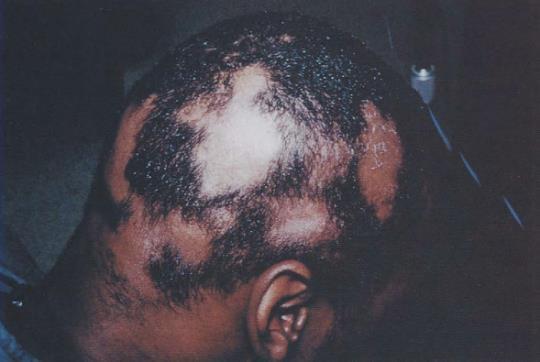
85 A. Sarcoidosis B. Leprosy C. Erysipelas D. Tinea E. Urticaria The most likely diagnosis is:



86

87 A. Sarcoidosis B. Leprosy C. Erysipelas D. Tinea E. Urticaria The most likely diagnosis is:

88
89 Leprosy Chronic, slowly progressive infectious disease caused by Mycobacterium leprae Predilection for peripheral nerves and skin Organism spread via nasal and oral droplets or breaks in skin barrier Affects all races and ages Peak incidences: yrs and yrs Three requirements for spread of disease Contagious person, susceptible person and close intimate contact
90 Leprosy Most common classification scheme used is by Ridley and Joplin (1966) LL: lepromatous leprosy TT: tuberculoid leprosy BB: borderline leprosy (BL, BB, BT) WHO classification (1997) Paucibacillary (single lesion) Paucibacillary (2-5 skin lesions) Multibacillary (more than 5 skin lesions)
91 Cutaneous manifestations: Leprosy Lepromatous leprosy: widespread, symmetric poorly defined erythematous macules, papules and plaques on face, buttocks, lower extremities Leonine facies, saddle nose deformities, bilateral earlobe infiltration, acquired icthyosis Borderline leprosy: asymmetric discrete erythematous plaques with alopecia Tuberculoid leprosy: few well-demarcated erythematous plaques

92 Distractors Sarcoidosis* Erysipelas


93 Distractors Tinea* Urticaria*
94 A 37 year-old woman presents with a 3 year history of painful erosions in the skin folds that heal leaving scars. The most likely diagnosis is: A. Hailey-Hailey disease B. Candidiasis C. Irritant dermatitis D. Lichen simplex chronicus E. Herpes simplex virus infection
95

96 A 37 year-old woman presents with a 3 year history painful erosions in the skin folds that heal leaving scars. The most likely diagnosis is: A. Hailey-Hailey disease B. Candidiasis C. Irritant dermatitis D. Lichen simplex chronicus E. Herpes simplex virus infection
97 Hailey-Hailey disease Familial benign chronic pemphigus AD, mutation in ATP2C1 gene, dysfunctional Ca2+ ATPase and intracellular Ca2+ signalling Second and third decade of life Flaccid blisters and erosions of neck and intertriginous areas axillae, groin, inframammary Easily ruptured blisters, macerated crusted erosions, chronic moist vegetative plaques with painful fissures common


98 Distractors Irritant dermatitis* Candidiasis*


99 Distractors Lichen simplex chronicus* Herpes simplex virus Infection*
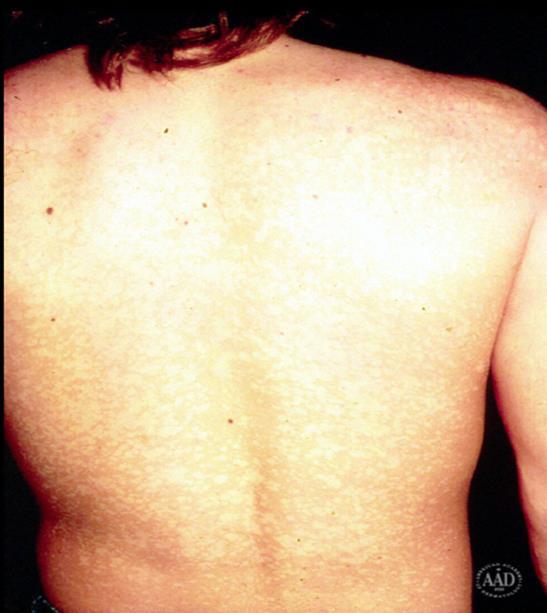
100 The most likely diagnosis is: A. Tinea versicolor B. Psoriasis C. Parapsoriasis D. Tinea corporis E. Granuloma annulare

101
102 The most likely diagnosis is: A. Tinea versicolor B. Psoriasis C. Parapsoriasis D. Tinea corporis E. Granuloma annulare
103 Controversial entity Parapsoriasis Clonal dermatitis transition point between chronic polyclonal dermatitis and mycosis fungoides? 2 types: small plaque, large plaque
104 Small plaque parapsoriasis Parapsoriasis Considered minimal to no chance of evolving to MF Less than 5 cm diameter Round to oval variably pinkish to hyperpigmented patches, thin plaques Digitate variant Large plaque parapsoriasis Considered to have potential for evolution to MF vs just early stage MF Larger than 5 cm diameter Often more irregular Retiform variant




105


106 Tinea versicolor* Distractors Psoriasis*


107 Distractors Tinea corporis* Granuloma annulare*
108 The most likely diagnosis is: A. Cutaneous anthrax B. Gonococcemia C. Reactive arthritis D. Sweet syndrome E. Syphilis
109
110 The most likely diagnosis is: A. Cutaneous anthrax B. Gonococcemia C. Reactive arthritis D. Sweet syndrome E. Syphilis
111 Gonococcemia Characteristic cutaneous lesions: Scattered papules or pustules (often hemorrhagic) with necrotic centers on distal acral sites Embolic septic vasculitis Acute arthritis-dermatosis syndrome Most common clinical manifestation of gonoccocal bacteremia Fever, joint pain, rash

*")
112 Distractors Reactive arthritis (Reiter s)* Sweet s syndrome*
113 Distractors Syphilis*
114 The most likely diagnosis is: A. Aphthous stomatitis B. Contact dermatitis C. Erythema multiforme D. Paraneoplastic pemphigus E. Squamous cell carcinoma

115

116 The most likely diagnosis is: A. Aphthous stomatitis B. Contact dermatitis C. Erythema multiforme D. Paraneoplastic pemphigus E. Squamous cell carcinoma
117 Aphthous stomatitis Oval, shallow, discrete painful ulcers with yellowish base and erythematous halo Commonly involves labial or buccal mucosa Most often heal within 7-10 days Peak prevalence occurs during second decade



118 Distractors Erythema multiforme* Paraneoplastic pemphigus

119 Distractors Squamous cell carcinoma*
120 The most likely diagnosis is: A. Chronic radiation dermatitis B. Coumadin necrosis C. Leukocytoclastic vasculitis D. Squamous cell carcinoma E. Toxic epidermal necrolysis
121
122 The most likely diagnosis is: A. Chronic radiation dermatitis B. Coumadin necrosis C. Leukocytoclastic vasculitis D. Squamous cell carcinoma E. Toxic epidermal necrolysis

123
124 Coumadin necrosis Develops within 2-5 days of starting warfarin in the absence of heparin especially with loading doses of coumadin Early drop in protein C levels Incidence is higher in women; peak incidence in 6 th and 7 th decades of life
125 Coumadin necrosis Begins as intense pain, with subsequent development of sharply demarcated erythema with overlying hemorrhage and necrosis. Retiform branching purpura seen at periphery of cutaneous lesions Peak incidence in women >50 years of age. Typical in sites with abundant subcutaneous tissue, such as the breasts, hips, buttocks or thighs.


126 Chronic radiation dermatitis* Distractors Leukocytoclastic vasculitis

127 Distractors Squamous cell carcinoma* Toxic epidermal necrolysis*

128 A 60 year old man presents with severely itchy blisters on the elbows, knees and upper back. The most likely diagnosis is: A. Neurotic excoriations B. Erythema elevatum diutinum C. Pemphigoid D. Scabies infestation E. Dermatitis herpetiformis


129
130 The most likely diagnosis is: A. Neurotic excoriations B. Erythema elevatum diutinum C. Bullous pemphigoid D. Scabies infestation E. Dermatitis herpetiformis
131 Dermatitis Herpetiformis Cutaneous manifestation of celiac disease and is associated with gluten sensitivity in most cases IgA antiendomysial antibodies are directed against tissue transglutaminase Mean age of onset: 4 th decade of life M>F:2:1
132 Dermatitis Herpetiformis Symmetric distribution: extensor elbows, forearms, nape of neck, back, buttocks and extensor knees Pleomorphic primary lesions: urticarial papules, plaques and vesicles Classic presentation: grouped excoriated papulovesicles on an erythematous base

133




134 Distractors Neurotic excoriations Erythema elevatum diutinum




135 Distractors Pemphigoid* Scabies infestation*
136 A 31 year-old female got this eruption shortly after using a topical steroid for a rash. The most likely diagnosis is: A. Perioral dermatitis B. Perleche C. Actinic cheilitis D. Contact dermatitis E. Herpes simplex virus
137
138 A 31 year-old female got this eruption shortly after using a topical steroid for a rash. The most likely diagnosis is: A. Perioral dermatitis B. Perleche C. Actinic cheilitis D. Contact dermatitis E. Herpes simplex virus


139
140 Perioral dermatitis (AKA periorificial dermatitis) Common in young adult women Cause unknown, but can be triggered by topical steroids Papules, pustules, erythema, scale; primary lesions often monomorphic Commonly spares vermillion border Can be periocular Can have burning, itching Treat similar to rosacea


141 Perleche (angular cheilitis) Distractors Actinic cheilitis


142 Distractors Contact dermatitis* Herpes simplex*
143 Thank You
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
An Approach to Common and not so Common Rashes in the Office FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc 1 Common Rashes Tinea Corporis: Annular- this is not the only criteria Advancing erythematous
Cutanous Manifestation of Lupus Erythematosus. Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university
 Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Cutanous Manifestation of Lupus Erythematosus Presented By: Dr. Naif S. Al Shahrani Salman Bin Abdaziz university A 50-year old lady, who is otherwise healthy, presented to the dermatology clinic with
Table of Contents: Part 1 Medical Dermatology. Chapter 1 Acneiform Disorders. Acne. Acne Vulgaris. Pomade Acne. Steroid Acne
 Table of Contents: Part 1 Medical Dermatology Chapter 1 Acneiform Disorders Acne Acne Vulgaris Pomade Acne Steroid Acne Infantile Acne Pediatric Perspectives Neonatal Acne (Acne Neonatorum) Pediatric Perspectives
Table of Contents: Part 1 Medical Dermatology Chapter 1 Acneiform Disorders Acne Acne Vulgaris Pomade Acne Steroid Acne Infantile Acne Pediatric Perspectives Neonatal Acne (Acne Neonatorum) Pediatric Perspectives
Rash Decisions Approach to the patient with a skin condition
 National Conference for Nurse Practitioners April 25, 2014 Rash Decisions Approach to the patient with a skin condition Margaret A. Bobonich, DNP, FNP C, DCNP, FAANP Assistant Professor, Case Western Reserve
National Conference for Nurse Practitioners April 25, 2014 Rash Decisions Approach to the patient with a skin condition Margaret A. Bobonich, DNP, FNP C, DCNP, FAANP Assistant Professor, Case Western Reserve
Index. derm.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abatacept for DLE, 493 for SLE, 497 Ablative therapies, localized, for cutaneous T-cell lymphoma, 502 506. See also Cutaneous T-cell lymphoma,
Note: Page numbers of article titles are in boldface type. A Abatacept for DLE, 493 for SLE, 497 Ablative therapies, localized, for cutaneous T-cell lymphoma, 502 506. See also Cutaneous T-cell lymphoma,
Index. Angiosarcoma diagnosis, 47 lymphedema-related vs. non-lymphedemarelated, 48
 A Acneiform rash biopsy, 134 cetuximab, EGFR, 132 133 diagnosis, 131 patient history, 131 134 treatment, 134 135 Acne vulgaris, 109 AGA. See Androgenetic alopecia Alopecia areata, 148 American Joint Committee
A Acneiform rash biopsy, 134 cetuximab, EGFR, 132 133 diagnosis, 131 patient history, 131 134 treatment, 134 135 Acne vulgaris, 109 AGA. See Androgenetic alopecia Alopecia areata, 148 American Joint Committee
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Time to Learn. 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service
 Time to Learn 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service The Red Face Rosacea Acne Seborrhoeic eczema eczema Psoriasis Slapped cheek syndrome Fungal infection Erysipelas...
Time to Learn 6 th March 2018 Dr. Shirin Chakera GPwSI Integrated Dermatology Service The Red Face Rosacea Acne Seborrhoeic eczema eczema Psoriasis Slapped cheek syndrome Fungal infection Erysipelas...
My Algorithm. Questions to ask. Do you or your family have a history of?... Allergic rhinitis, Sensitive skin, Asthma Skin Cancer
 Tracey C. Vlahovic, DPM Associate Professor, Temple University School of Podiatric Medicine My Algorithm Inflammatory Skin Disorder on Feet Family hx, clinical exam, look at hands! Defined plaques: Psoriasis
Tracey C. Vlahovic, DPM Associate Professor, Temple University School of Podiatric Medicine My Algorithm Inflammatory Skin Disorder on Feet Family hx, clinical exam, look at hands! Defined plaques: Psoriasis
Objectives. Terminology. Recognize common pediatric dermatologic conditions. Review treatment plans Identify skin manifestations of systemic disease
 Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Pediatric Visual Dermatological Diagnosis Fernando Vega, M.D. Objectives Recognize common pediatric dermatologic conditions Expand differential diagnosis Review treatment plans Identify skin manifestations
Dermatology GP Referral Guidelines
 Austin Health Dermatology Department holds 5 Clinic sessions to discuss and plan the treatment of with Dermatology conditions. Department of Health clinical urgency categories for specialist clinics Urgent:
Austin Health Dermatology Department holds 5 Clinic sessions to discuss and plan the treatment of with Dermatology conditions. Department of Health clinical urgency categories for specialist clinics Urgent:
DERMATOLOGICAL EMERGENCIES. DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE
, DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE") DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
DERMATOLOGICAL EMERGENCIES DR. Ian Hoyle MBBS DIP IMC RCS (Ed), DA (UK),FRACGP,FACRRM,DIP DERM(Wales) TASMANIAN SKIN AND BODY CENTRE Dermatological Emergencies INFECTIONS ERYTHRODERMA DRUG ERUPTIONS STEVENS-JOHNSON
Recognizing common Dermatologic conditions. Case presentations. CAPA 2015 Annual Conference. Tanya Nino, MD St. Joseph Heritage Medical Group
 Recognizing common Dermatologic conditions Tanya Nino, MD St. Joseph Heritage Medical Group Case presentations 65 year old female referred for rule out melanoma a lesion on back 30 year old female has
Recognizing common Dermatologic conditions Tanya Nino, MD St. Joseph Heritage Medical Group Case presentations 65 year old female referred for rule out melanoma a lesion on back 30 year old female has
Common Cutaneous Signs of Medical Illnesses
 Common Cutaneous Signs of Medical Illnesses DR COLIN THENG MBBS, MMED (FAM. MED), MRCP(UK), FAMS SENIOR CONSULTANT DERMATOLOGIST THE SKIN SPECIALISTS & LASER CLINIC MOUNT ALVERNIA MEDICAL CENTRE D, #07-61
Common Cutaneous Signs of Medical Illnesses DR COLIN THENG MBBS, MMED (FAM. MED), MRCP(UK), FAMS SENIOR CONSULTANT DERMATOLOGIST THE SKIN SPECIALISTS & LASER CLINIC MOUNT ALVERNIA MEDICAL CENTRE D, #07-61
COPYRIGHTED MATERIAL. Introduction CHAPTER 1. Introduction
 CHAPTER 1 Introduction OVERVIEW The clinical features of skin lesions are related to the underlying pathological processes. Broadly skin conditions fall into three clinical groups: (a) those with a well-defined
CHAPTER 1 Introduction OVERVIEW The clinical features of skin lesions are related to the underlying pathological processes. Broadly skin conditions fall into three clinical groups: (a) those with a well-defined
CONDITIONS OF THE SKIN
 CONDITIONS OF THE SKIN UCSF/SFGH Family & Community Medicine Residency Program Educational Objectives I. Knowledge The resident will be able to discuss the definition, diagnosis, and initial management
CONDITIONS OF THE SKIN UCSF/SFGH Family & Community Medicine Residency Program Educational Objectives I. Knowledge The resident will be able to discuss the definition, diagnosis, and initial management
Contents. QAaptm-2. CAaptei-3. CAaptm-4. Cftapte%-5. Qfiaptvt-6. QhapteK-7. Qkaptefc-8 Clinical Immunology and Allergy 71
 Contents Ckaptm-1 Aaatomy, Physiology, Embryology, Bacteriology and Pathology ~ 1 Anatomy 1 Physiology 10 Embryology 14 Pathology 19 Bacteriology 22 Laboratory and other aids in dermatological pratice
Contents Ckaptm-1 Aaatomy, Physiology, Embryology, Bacteriology and Pathology ~ 1 Anatomy 1 Physiology 10 Embryology 14 Pathology 19 Bacteriology 22 Laboratory and other aids in dermatological pratice
Site and distribution: symmetrical, asymmetrical. Surface characteristics: smooth, scaly, warty
 B I O T E R R O R I S M PRINCIPLES AND PRACTICE OF DERMATOLOGY Dr Matthew Ng Joo Ming INTRODUCTION Medical schools and textbooks teach us dermatology by subjects such as eczema and psoriasis. This is useful
B I O T E R R O R I S M PRINCIPLES AND PRACTICE OF DERMATOLOGY Dr Matthew Ng Joo Ming INTRODUCTION Medical schools and textbooks teach us dermatology by subjects such as eczema and psoriasis. This is useful
Rosacea Rosacea: how I hates ya! Richard Castillo, OD, DO The Oklahoma College of Optometry Northeastern State University Tahlequah, OK
 Rosacea Rosacea: how I hates ya! Richard Castillo, OD, DO The Oklahoma College of Optometry Northeastern State University Tahlequah, OK Introduction Clinical Features Flushing Telangiectasia Erythema Papules
Rosacea Rosacea: how I hates ya! Richard Castillo, OD, DO The Oklahoma College of Optometry Northeastern State University Tahlequah, OK Introduction Clinical Features Flushing Telangiectasia Erythema Papules
My ear won t stop hurting!
 This month: 1. My ear won t stop hurting! 5. Cortisone Cream Didn t Help! 2. What are these red bumps? 6. Can my girlfriend get it? 3. Why won t this rash leave? 7. My wife noticed it! 4. What s the cause
This month: 1. My ear won t stop hurting! 5. Cortisone Cream Didn t Help! 2. What are these red bumps? 6. Can my girlfriend get it? 3. Why won t this rash leave? 7. My wife noticed it! 4. What s the cause
Diagnose dermatologic conditions based on physical examination (visual recognition). The majority of the items will come from Group 1.
. The majority of the items will come from Group 1.") This document was developed by a committee of the American Board of Dermatology (ABD) for the purpose of preparing the BASIC Examination. The BASIC Exam is assessment of fundamental knowledge and skills.
This document was developed by a committee of the American Board of Dermatology (ABD) for the purpose of preparing the BASIC Examination. The BASIC Exam is assessment of fundamental knowledge and skills.
DESCRIPTIONS FOR MED 3 ROTATIONS Dermatology A3S
 Regardless of your future field of practice, you will be exposed to a considerable amount of dermatology and this rotation provides you the chance to see a range of skin diseases. You will have the opportunity
Regardless of your future field of practice, you will be exposed to a considerable amount of dermatology and this rotation provides you the chance to see a range of skin diseases. You will have the opportunity
Eczema. By:- Dr. Naif Al-Shahrani Salman bin Abdazziz University
 Eczema By:- Dr. Naif Al-Shahrani Salman bin Abdazziz University Dermatitis= Eczema =Spongiosis Eczema Atopic Seborrheic Contact Allergic Irritant Nummular Asteatotic Stasis Neurodermatitis/Lichen Simplex
Eczema By:- Dr. Naif Al-Shahrani Salman bin Abdazziz University Dermatitis= Eczema =Spongiosis Eczema Atopic Seborrheic Contact Allergic Irritant Nummular Asteatotic Stasis Neurodermatitis/Lichen Simplex
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
Contents. Part I Genodermatoses
 Contents Part I Genodermatoses 1 Hyperkeratotic Palms and Soles with Periorificial Keratosis............... 3 2 Indurated, Dark, Hairy Plaques, with Arthritis and Deafness.............. 9 3 Cleft Palate,
Contents Part I Genodermatoses 1 Hyperkeratotic Palms and Soles with Periorificial Keratosis............... 3 2 Indurated, Dark, Hairy Plaques, with Arthritis and Deafness.............. 9 3 Cleft Palate,
Emergency Dermatology Dr Melissa Barkham
 Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
Emergency Dermatology Dr Melissa Barkham Spotlight Seminar 30 th September 2010 Why is this important? Urgent recognition and treatment of dermatologic emergencies can be life saving and prevent long term
4. Pityriasis lichenoides
 Go Back to the Top To Order, Visit the Purchasing Page for Details usually more than 5 cm in diameter and accompanied by poikiloderma. Some but not all patients may develop mycosis fungoides (Fig. 22.35).
Go Back to the Top To Order, Visit the Purchasing Page for Details usually more than 5 cm in diameter and accompanied by poikiloderma. Some but not all patients may develop mycosis fungoides (Fig. 22.35).
Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level
 Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level Dr Ng Su Yuen Paediatrician and Paediatric Dermatologist Hospital Pulau Pinang Outline Common inflammatory
Diagnosis and Management of Common and Infective Skin Diseases in Children at primary care level Dr Ng Su Yuen Paediatrician and Paediatric Dermatologist Hospital Pulau Pinang Outline Common inflammatory
Topographical dermatology
 Chapter 12: Topographical dermatology page: 332 Topographical dermatology Alopecia page: 333 12.1 Alopecia Alopecia areata Alopecia areata of the scalp is characterized by the appearance of round or oval,
Chapter 12: Topographical dermatology page: 332 Topographical dermatology Alopecia page: 333 12.1 Alopecia Alopecia areata Alopecia areata of the scalp is characterized by the appearance of round or oval,
Oral Medicine. Dr. Qianming Ian CHEN
 Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
Phototherapy and Photochemotherapy Treatment (Ultraviolet A [PUVA] and B [UBV])
![Phototherapy and Photochemotherapy Treatment (Ultraviolet A [PUVA] and B [UBV])](/thumbs/89/99382632.jpg "Phototherapy and Photochemotherapy Treatment (Ultraviolet A [PUVA] and B [UBV])") Origination: 09/27/07 Revised: 08/2/17 Annual Review: 11/2/17 Purpose: To provide Phototherapy and Photochemotherapy Treatment (PUVA and UBV) guidelines for the Medical Department staff to reference when
Origination: 09/27/07 Revised: 08/2/17 Annual Review: 11/2/17 Purpose: To provide Phototherapy and Photochemotherapy Treatment (PUVA and UBV) guidelines for the Medical Department staff to reference when
Cutaneous Drug Reactions
 Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Cutaneous Drug Reactions Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada Copyright 2017 by Sea Courses
Inflammatory Dermatopathology
 Inflammatory Dermatopathology Steven D. Billings Jenny Cotton Inflammatory Dermatopathology A Pathologist s Survival Guide Second Edition Steven D. Billings, MD Professor of Pathology and Co-Director
Inflammatory Dermatopathology Steven D. Billings Jenny Cotton Inflammatory Dermatopathology A Pathologist s Survival Guide Second Edition Steven D. Billings, MD Professor of Pathology and Co-Director
Proceedings of the Southern European Veterinary Conference - SEVC -
 Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Learning Objectives. History 8/1/2016. An Approach to Pediatric Rashes
 An Approach to Pediatric Rashes Neethi Patel, D.O. Learning Objectives 1.To identify common features of rashes seen in the pediatric population as well as pathognomonic features of certain pathologies
An Approach to Pediatric Rashes Neethi Patel, D.O. Learning Objectives 1.To identify common features of rashes seen in the pediatric population as well as pathognomonic features of certain pathologies
Cutaneous reactions to targeted therapies. Stavonnie Patterson, MD, FAAD Northwestern University Feinberg School of Medicine March 6, 2017
 Cutaneous reactions to targeted therapies Stavonnie Patterson, MD, FAAD Northwestern University Feinberg School of Medicine March 6, 2017 Disclosures I have no relevant disclosures Papulopustular Eruption
Cutaneous reactions to targeted therapies Stavonnie Patterson, MD, FAAD Northwestern University Feinberg School of Medicine March 6, 2017 Disclosures I have no relevant disclosures Papulopustular Eruption
Subspecialty Rotation: Dermatology
 Subspecialty Rotation: Dermatology Faculty: Wesley Galen, M.D. GOAL: Prevention, Counseling and Screening (Dermatology). Understand the pediatrician's role in preventing illness and dysfunction related
Subspecialty Rotation: Dermatology Faculty: Wesley Galen, M.D. GOAL: Prevention, Counseling and Screening (Dermatology). Understand the pediatrician's role in preventing illness and dysfunction related
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
HEADS UP. IT S OUR BIRTHDAY. Photo Diagnosis
 An illustrated quiz on problems seen in everyday practice Case 1 A 57-year-old male presented with a history of recurrent abdominal pain and weight loss over the last three months. A computed tomography
An illustrated quiz on problems seen in everyday practice Case 1 A 57-year-old male presented with a history of recurrent abdominal pain and weight loss over the last three months. A computed tomography
page: 582 alphabetical Index by Causes picture cause basic lesion search contents print last screen viewed back next
 page: 582 Index by Causes basic lesion cause picture alphabetical Index by Causes page: 583 Mechanical factors Acquired digital fibrokeratoma,393 Angioma,418 Atopic dermatitis in the adult: xerosis, lichenification
page: 582 Index by Causes basic lesion cause picture alphabetical Index by Causes page: 583 Mechanical factors Acquired digital fibrokeratoma,393 Angioma,418 Atopic dermatitis in the adult: xerosis, lichenification
My Method for Approaching Skin Biopsies
 My Method for Approaching Skin Biopsies P A U L H A U N, MD, MS, F A A D A S S I S T A N T P R O F E S S O R D E R M A T O L O G Y A N D D E R M A T O P A T H O L O G Y D E P A R T M E N T O F D E R M
My Method for Approaching Skin Biopsies P A U L H A U N, MD, MS, F A A D A S S I S T A N T P R O F E S S O R D E R M A T O L O G Y A N D D E R M A T O P A T H O L O G Y D E P A R T M E N T O F D E R M
Some skin conditions
 Some skin conditions Some skin conditions Acute Inflammatory Dermatoses Chronic Inflammatory Dermatoses Blistering (Bullous) Diseases Panniculitis Disorders of Epidermal Appendages -Urticaria -Acute eczematous
Some skin conditions Some skin conditions Acute Inflammatory Dermatoses Chronic Inflammatory Dermatoses Blistering (Bullous) Diseases Panniculitis Disorders of Epidermal Appendages -Urticaria -Acute eczematous
Chapter 8 Skin Disorders and Diseases
 Chapter 8 Skin Disorders and Diseases Attitude is more important than the past, than education, than money, than circumstances, than what people do or say. It is more important than appearance, giftedness,
Chapter 8 Skin Disorders and Diseases Attitude is more important than the past, than education, than money, than circumstances, than what people do or say. It is more important than appearance, giftedness,
What is Psoriasis? Common Areas Affected. Type Who Does it Affect Characteristics
 What is? is a term derived from the Greek word psōra which means itch and is a common, long lasting, inflammatory skin condition which affects 1-3% of the UK population and about 80 million people worldwide.
What is? is a term derived from the Greek word psōra which means itch and is a common, long lasting, inflammatory skin condition which affects 1-3% of the UK population and about 80 million people worldwide.
الاكزيماتيد= Eczematid
 1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
1 / 7 2 / 7 Pityriasis Debate confusing of hypopigmentation characterized increasing surrounded differ hypomelanotic "progressive exists alba misnomer extensive a to observed term the applied term derived
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Granuloma annulare is a benign self-limited disease, first described by Colcott-Fox 1 in 1895 and Radcliffe-Crocker in 1902.
 Granuloma Annulare Granuloma annulare is a benign self-limited disease, first described by Colcott-Fox 1 in 1895 and Radcliffe-Crocker in 1902. EPIDEMIOLOGY Granuloma annulare is a relatively common disorder.
Granuloma Annulare Granuloma annulare is a benign self-limited disease, first described by Colcott-Fox 1 in 1895 and Radcliffe-Crocker in 1902. EPIDEMIOLOGY Granuloma annulare is a relatively common disorder.
Skin Disorders of the Nose in Dogs
 Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Skin Disorders of the Nose in Dogs (Canine Nasal Dermatoses) Basics OVERVIEW Conditions
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Skin Disorders of the Nose in Dogs (Canine Nasal Dermatoses) Basics OVERVIEW Conditions
Commonly Coded Conditions in Dermatology
 Commonly Coded Conditions in Dermatology No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or mechanically, including photocopying,
Commonly Coded Conditions in Dermatology No part of this presentation may be reproduced or transmitted in any form or by any means (graphically, electronically, or mechanically, including photocopying,
COURSE DESCRIPTION AND STUDY REGULATIONS
 COURSE DESCRIPTION AND STUDY REGULATIONS Course: SKIN AND VENEREAL DISEASES Course type: COMPULSORY ELECTIVE ECTS credits: 6 Nominated teacher(s): prof. dr. Tomaž Lunder, izr. prof. dr. Mateja Dolenc-Voljč
COURSE DESCRIPTION AND STUDY REGULATIONS Course: SKIN AND VENEREAL DISEASES Course type: COMPULSORY ELECTIVE ECTS credits: 6 Nominated teacher(s): prof. dr. Tomaž Lunder, izr. prof. dr. Mateja Dolenc-Voljč
Evidence-based Clinical Practice Guidelines for Treatment of Acne and Rosacea in Canada. Catherine Zip Nov 10, 2016
 Evidence-based Clinical Practice Guidelines for Treatment of Acne and Rosacea in Canada Catherine Zip Nov 10, 2016 Acne Acne Classification Type Comedonal Mild-to-moderate papulopustular acne Severe Description
Evidence-based Clinical Practice Guidelines for Treatment of Acne and Rosacea in Canada Catherine Zip Nov 10, 2016 Acne Acne Classification Type Comedonal Mild-to-moderate papulopustular acne Severe Description
Herbal and homeopathic products, often considered natural and non-toxic, can also cause adverse drug reactions.
 Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Idiosyncratic and potentially serious cutaneous adverse drug reactions (CADRs), although relatively rare, account for significant morbidity and mortality. RANNAKOE J LEHLOENYA, BSc, MB ChB, FCDerm (SA)
Cutaneous Adverse Drug Reactions in Domestic Animals. Katherine Doerr, DVM, Dip. ACVD. Veterinary Dermatology Center
 Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Cutaneous Adverse Drug Reactions in Domestic Animals Katherine Doerr, DVM, Dip. ACVD Veterinary Dermatology Center Maitland, Rockledge, Waterford Lakes, FL Not highly studied in veterinary medicine Unknown
Course Regime. Course: SKIN AND VENEREAL DISEASES. Study Programme: Medicine. Year of the Course: 4 th study year.
 Komisija za študijske zadeve UL Medicinske fakultete Vrazov trg 2 SI-1000 Ljubljana E: ksz@mf.uni-lj.si T: +386 1 543 7700 Course Regime Course: SKIN AND VENEREAL DISEASES Study Programme: Medicine Year
Komisija za študijske zadeve UL Medicinske fakultete Vrazov trg 2 SI-1000 Ljubljana E: ksz@mf.uni-lj.si T: +386 1 543 7700 Course Regime Course: SKIN AND VENEREAL DISEASES Study Programme: Medicine Year
Skin lesions & Abrasions
 Skin lesions & Abrasions What Are Skin Lesions? A skin lesion is a part of the skin that has an abnormal growth or appearance compared to the skin around it Types of Skin Lesions Two types of skin lesions
Skin lesions & Abrasions What Are Skin Lesions? A skin lesion is a part of the skin that has an abnormal growth or appearance compared to the skin around it Types of Skin Lesions Two types of skin lesions
GOOD MORNING! AUGUST 5, 2014
 GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
GOOD MORNING! AUGUST 5, 2014 PREP QUESTION During the health supervision visit of a term newborn boy, his mother relates that a cousins child died at age 4 months from sudden infant death syndrome. She
Questions. Answers. Share your photos and diagnoses with us!
 Illustrated quizzes on problems seen in everyday practice Case 1 A 56-year-old woman presented with a two-week history of pruritic urticarial plaques and tense bullae on both erythematous and normal skin.
Illustrated quizzes on problems seen in everyday practice Case 1 A 56-year-old woman presented with a two-week history of pruritic urticarial plaques and tense bullae on both erythematous and normal skin.
Skin Manifestations of Systemic Disease. Approach to Dermatalogic Diagnosis 9/6/2016. Go Ahead---Judge a Book by its Cover!
 Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Go Ahead---Judge a Book by its Cover! Skin Manifestations of Systemic Disease Amelie Hollier, DNP, FNP-BC, FAANP Lafayette, LA President, APEA Objectives Compare diseases of the skin with reactions of
Rashes in the elderly
 Clinical practice 29 Rashes in the elderly In this article we aim to highlight some of the commoner skin conditions one might expect to see in an elderly population, their typical features and treatments.
Clinical practice 29 Rashes in the elderly In this article we aim to highlight some of the commoner skin conditions one might expect to see in an elderly population, their typical features and treatments.
Paul K. Shitabata, M.D. Dermatopathology Institute
 Paul K. Shitabata, M.D. Dermatopathology Institute Key Points Subtle dermatologic signs may suggest significant gastrointestinal and systemic disease Check family history Several dermatologic disorders
Paul K. Shitabata, M.D. Dermatopathology Institute Key Points Subtle dermatologic signs may suggest significant gastrointestinal and systemic disease Check family history Several dermatologic disorders
Treatments used Topical including cleansers and moisturizer Oral medications:
 Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
Discipline: Dermatology Extended Topic: Acne & Rosacea : Onset: Location: Face Chest Back Menses if female: Regular Irregular PCOS Treatments used Topical including cleansers and moisturizer Oral medications:
Misdiagnosed Case of Lepromatous Leprosy
 Bahrain Medical Bulletin, Vol. 36, No. 3, September 2014 Misdiagnosed Case of Lepromatous Leprosy Ahmed Anwer Aljowder, BSc, MD* Azad Kareem Kassim FRCPI, FRCP (Glasg), FAAD** Mazen Raees MB, BCh, BAO,
Bahrain Medical Bulletin, Vol. 36, No. 3, September 2014 Misdiagnosed Case of Lepromatous Leprosy Ahmed Anwer Aljowder, BSc, MD* Azad Kareem Kassim FRCPI, FRCP (Glasg), FAAD** Mazen Raees MB, BCh, BAO,
DERMCASE. Doc, my baby s all spotty! Case 1
 Test Your Knowledge With Multiple-Choice Cases This month 5 cases: Case 1 1. Doc, my baby s all spotty! 2. A Mediterranean Matter 3. Mommy, what s wrong with my head? 4. Armed with Lesions 5. It s spreading!
Test Your Knowledge With Multiple-Choice Cases This month 5 cases: Case 1 1. Doc, my baby s all spotty! 2. A Mediterranean Matter 3. Mommy, what s wrong with my head? 4. Armed with Lesions 5. It s spreading!
Dermclinic
 Dermclinic /Dermclinic A Photo Quiz to Hone Dermatologic Skills DAVID L. KAPLAN, MD Series Editor University of Missouri Kansas City, University of Kansas Case 1: Upon his return from a summer visit to
Dermclinic /Dermclinic A Photo Quiz to Hone Dermatologic Skills DAVID L. KAPLAN, MD Series Editor University of Missouri Kansas City, University of Kansas Case 1: Upon his return from a summer visit to
PAPULOSQUAMOUS DISEASE AND VESICULOBULLOUS DISEASE
 PAPULOSQUAMOUS DISEASE AND VESICULOBULLOUS DISEASE NOPPANUN CHALERMROJ; MD. DEPARTMENT OF MEDICINE MAHARAT NAKORN RATCHASIMA HOSPITAL PAPULOSQUAMOUS ERUPTIONS Group of skin diseases that share similar
PAPULOSQUAMOUS DISEASE AND VESICULOBULLOUS DISEASE NOPPANUN CHALERMROJ; MD. DEPARTMENT OF MEDICINE MAHARAT NAKORN RATCHASIMA HOSPITAL PAPULOSQUAMOUS ERUPTIONS Group of skin diseases that share similar
DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY
 DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Nicole Burkemper, MD Associate Professor of Dermatology and Pathology Saint Louis University I HAVE NO RELEVENT RELATIONSHIPS WITH ANY COMPANIES The most
DISCLOSURE OF RELEVANT RELATIONSHIPS WITH INDUSTRY Nicole Burkemper, MD Associate Professor of Dermatology and Pathology Saint Louis University I HAVE NO RELEVENT RELATIONSHIPS WITH ANY COMPANIES The most
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation. Dermatopathology Specialists Needed. Changing Trends
 Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Five things not to miss in Dermatology. Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine
 Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Five things not to miss in Dermatology Dr Judy Wismer Associate Clinical Professor Michael G DeGroote School of Medicine Key Descriptives Fever, skin pain Purpura, necrosis Bullae, Mucosal, Skin sloughing
Clinic Clinic Information Suitable for Referral Not Suitable for Referral
 PBC Services Clinic Clinic Information Suitable for Referral Not Suitable for Referral Diabetes One Off Clinic Donnington Medical The Health Centre, Wrekin Drive Donnington TF2 8EA Contact: Bryan Henshall
PBC Services Clinic Clinic Information Suitable for Referral Not Suitable for Referral Diabetes One Off Clinic Donnington Medical The Health Centre, Wrekin Drive Donnington TF2 8EA Contact: Bryan Henshall
2) Disorders of Abnormal Keratinization - Dr. Ali
 Disorders of Abnormal Keratinization - Dr. Ali") 2) Disorders of Abnormal Keratinization - Dr. Ali Disorder of Keratinization In the normal epidermis, as the keratinocytes move from the basal-cell layer to the surface, the process of terminal differentiation
2) Disorders of Abnormal Keratinization - Dr. Ali Disorder of Keratinization In the normal epidermis, as the keratinocytes move from the basal-cell layer to the surface, the process of terminal differentiation
The side effects of prolonged used of systemic Corticosteroids
 The side effects of prolonged used of systemic Corticosteroids -Lowering the resistance to many infections. -Metabolic disturbance, particularly in regard to electrolytes and carbohydrates leading to fluid
The side effects of prolonged used of systemic Corticosteroids -Lowering the resistance to many infections. -Metabolic disturbance, particularly in regard to electrolytes and carbohydrates leading to fluid
Inflammatory Dermatoses of the Vulva for the General/Gyn Pathologist with emphasis in the lichenoid pattern
 Inflammatory Dermatoses of the Vulva for the General/Gyn Pathologist with emphasis in the lichenoid pattern By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor
Inflammatory Dermatoses of the Vulva for the General/Gyn Pathologist with emphasis in the lichenoid pattern By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor
Introduction. A Short Review of Cutaneous Vasculitis. Introduction. Introduction. Introduction. Introduction
 A Short Review of Cutaneous Vasculitis Uma Sundram, MD, PhD Professor of Pathology, William Beaumont Oakland University School of Medicine Staff Dermatopathologist Beaumont Hospital-Royal Oak, MI September
A Short Review of Cutaneous Vasculitis Uma Sundram, MD, PhD Professor of Pathology, William Beaumont Oakland University School of Medicine Staff Dermatopathologist Beaumont Hospital-Royal Oak, MI September
Dermatology for the PCP
 Dermatology for the PCP Laura S. Winterfield, MD MPH Associate Professor Medical University of South Carolina I have no relevant conflicts of interest. 1 Learning Objectives Identify common skin conditions
Dermatology for the PCP Laura S. Winterfield, MD MPH Associate Professor Medical University of South Carolina I have no relevant conflicts of interest. 1 Learning Objectives Identify common skin conditions
Emergent and Urgent Dermatology, Eruptions, and Wound Care
 Emergent and Urgent Dermatology, Eruptions, and Wound Care G. Scott Drew, DO, FAAD, FAOCD Smith Clinic Department of Dermatology Tucson Osteopathic Medical Foundation April 27, 2018 Acute Cutaneous Lupus
Emergent and Urgent Dermatology, Eruptions, and Wound Care G. Scott Drew, DO, FAAD, FAOCD Smith Clinic Department of Dermatology Tucson Osteopathic Medical Foundation April 27, 2018 Acute Cutaneous Lupus
Pathology of the skin. Dr Fónyad László, 1sz. Patológiai és Kísérleti Rákkutató Intézet, SE
 Pathology of the skin Dr Fónyad László, 1sz. Patológiai és Kísérleti Rákkutató Intézet, SE The skin Biggest organ Kb. 1.8 nm Kb. 10 kg Most frequent site for tumor development (BCC) Pathology of the skin
Pathology of the skin Dr Fónyad László, 1sz. Patológiai és Kísérleti Rákkutató Intézet, SE The skin Biggest organ Kb. 1.8 nm Kb. 10 kg Most frequent site for tumor development (BCC) Pathology of the skin
Inflammatory skin disease I Jade Wititsuwannakul, MD Chulalongkorn University, Thailand
 Inflammatory skin disease I Jade Wititsuwannakul, MD Chulalongkorn University, Thailand Superficial Perivascular Dermatitis Interface Dermatitis Vacuolar Dermatitis Lichenoid Dermatitis Barnhill Textbook
Inflammatory skin disease I Jade Wititsuwannakul, MD Chulalongkorn University, Thailand Superficial Perivascular Dermatitis Interface Dermatitis Vacuolar Dermatitis Lichenoid Dermatitis Barnhill Textbook
Facial Rash. Facial Rash 10/14/2013. Ten Look Alike Rashes Michelle DiBaise, MPAS, PA-C, DFAAPA Associate Clinical Professor NAU PA Program
 Ten Look Alike Rashes Michelle DiBaise, MPAS, PA-C, DFAAPA Associate Clinical Professor NAU PA Program Facial Rash Facial Rash Case 1 28 year female Progressive development of erythematous facial lesions
Ten Look Alike Rashes Michelle DiBaise, MPAS, PA-C, DFAAPA Associate Clinical Professor NAU PA Program Facial Rash Facial Rash Case 1 28 year female Progressive development of erythematous facial lesions
Spongiotic Dermatitis
 Prepared by Kurt Schaberg Introduction to Inflammatory Dermpath Spongiotic Dermatitis intraepidermal intercellular edema (spongiosis) - presence of widened intercellular spaces between keratinocytes, with
Prepared by Kurt Schaberg Introduction to Inflammatory Dermpath Spongiotic Dermatitis intraepidermal intercellular edema (spongiosis) - presence of widened intercellular spaces between keratinocytes, with
The Leonine Face of Leprosy: An International Exploration
 The Leonine Face of Leprosy: An International Exploration Leela Athalye Dermatology Resident Western University/College Medical Center Program Director: Dr. Navid Nami International Exploration India,
The Leonine Face of Leprosy: An International Exploration Leela Athalye Dermatology Resident Western University/College Medical Center Program Director: Dr. Navid Nami International Exploration India,
Principi ed Aggiornamenti in Dermatologia Roma, 6-7 Aprile Grand rounds. Lorenzo Cerroni, Graz
 Principi ed Aggiornamenti in Dermatologia Roma, 6-7 Aprile 2018 Grand rounds Lorenzo Cerroni, Graz "Computer palms" Described in patient using computer keyboards for long periods; similar features described
Principi ed Aggiornamenti in Dermatologia Roma, 6-7 Aprile 2018 Grand rounds Lorenzo Cerroni, Graz "Computer palms" Described in patient using computer keyboards for long periods; similar features described
OCCUPATIONAL DERMATOSES
 OCCUPATIONAL DERMATOSES Part II Liz Clark, D.O., MPH & TM, FAOCOPM Learning Objectives: To better understand the epidemiology and economic impact of Occupational Dermatoses To review medical definitions
OCCUPATIONAL DERMATOSES Part II Liz Clark, D.O., MPH & TM, FAOCOPM Learning Objectives: To better understand the epidemiology and economic impact of Occupational Dermatoses To review medical definitions
Dr Emmy Babor GPSI Dermatology
 Dr Emmy Babor GPSI Dermatology Wrinkles Sagging Thin skin (not all areas think about soles of feet) Loss of elasticity Pigmentary changes Dryness Loss of luminosity Baldness/ grey hair Increased nose
Dr Emmy Babor GPSI Dermatology Wrinkles Sagging Thin skin (not all areas think about soles of feet) Loss of elasticity Pigmentary changes Dryness Loss of luminosity Baldness/ grey hair Increased nose
Patterns and mechanisms of inflammatory skin conditions: the pathologist s survival kit SALVADOR J. DIAZ-CANO BAHRAIN, APRIL 2017
 Patterns and mechanisms of inflammatory skin conditions: the pathologist s survival kit SALVADOR J. DIAZ-CANO 0000-0003-1245-2859 BAHRAIN, APRIL 2017 Basic Elements of Lesions Repair Injury Time & Intensity
Patterns and mechanisms of inflammatory skin conditions: the pathologist s survival kit SALVADOR J. DIAZ-CANO 0000-0003-1245-2859 BAHRAIN, APRIL 2017 Basic Elements of Lesions Repair Injury Time & Intensity
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
9/9/17. Disclosures" Dermatology in Primary Care: Recognition and treatment of common disorders of the skin" A preview" Classic skin infections"
 Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
Disclosures Dermatology in Primary Care: Recognition and treatment of common disorders of the skin I have no conflicts of interest to disclose. I may discuss off-label use of treatments for cutaneous disease.
Dermatology Pearls. Leah Layman, ARNP Jefferson Healthcare Dermatology June 21, 2018
 Dermatology Pearls Leah Layman, ARNP Jefferson Healthcare Dermatology June 21, 2018 What s on the agenda? Common skin conditions and where to start with treatment Gentle skin care regimen PCP and Biologics
Dermatology Pearls Leah Layman, ARNP Jefferson Healthcare Dermatology June 21, 2018 What s on the agenda? Common skin conditions and where to start with treatment Gentle skin care regimen PCP and Biologics
OCCUPATIONAL DERMATOSES
 OCCUPATIONAL DERMATOSES OCCUPATIONAL MEDICINE Liz Clark, D.O., MPH & TM, FAOCOPM, FAIMA Learning Objectives: To better understand the epidemiology and economic impact of Occupational Dermatoses To review
OCCUPATIONAL DERMATOSES OCCUPATIONAL MEDICINE Liz Clark, D.O., MPH & TM, FAOCOPM, FAIMA Learning Objectives: To better understand the epidemiology and economic impact of Occupational Dermatoses To review
Pediatric Dermatology
 Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
Pediatric Dermatology --------- Emergencies & Urgencies Nicholas V. Nguyen, M.D. Director, Pediatric Dermatology Disclosures In the past 12 months, I have had the following financial relationships with
2017 All right reserved Bellomo Consulting, Inc RECOGNIZING COMMON SKIN CONDITIONS
 RECOGNIZING COMMON SKIN CONDITIONS Perioral Dermatitis Perioral Dermatitis Predominately seen in females ranging in age from 16 to 45 years old. Also seen in infants and toddlers due to excess moisture
RECOGNIZING COMMON SKIN CONDITIONS Perioral Dermatitis Perioral Dermatitis Predominately seen in females ranging in age from 16 to 45 years old. Also seen in infants and toddlers due to excess moisture
Angioedema. Dermatographism. Fernando Vega, M.D. 1. Fernando Vega, M.D. Seattle Healing Arts
 Common Dermatological Dilemmas Itchy Wheals Fernando Vega, M.D. Seattle Healing Arts Itchy Wheals When is it Urticaria? When is it angioedema? When is it allergic? When is it non-allergic? Wheals, superficial
Common Dermatological Dilemmas Itchy Wheals Fernando Vega, M.D. Seattle Healing Arts Itchy Wheals When is it Urticaria? When is it angioedema? When is it allergic? When is it non-allergic? Wheals, superficial
ExtraintestinalManifestations of IBD
 ExtraintestinalManifestations of IBD Hyun Kim, M.D. San Diego Digestive Disease Consultants Associate Professor, UCSD School of Medicine Why Other Organs Involved in IBD? Organ Involvement Bones, Joints
ExtraintestinalManifestations of IBD Hyun Kim, M.D. San Diego Digestive Disease Consultants Associate Professor, UCSD School of Medicine Why Other Organs Involved in IBD? Organ Involvement Bones, Joints
CPC. Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand
 CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
CPC Chutika Srisuttiyakorn, M.D. Kobkul Aunhachoke, M.D. Phramongkutklao Hospital Bangkok, Thailand A 53 year-old woman with fever, facial swelling and rashes on face, trunk and upper extremities for 3
Conflicts. Objectives. University of Texas Health Science Center at San Antonio. Pediatrics Grand Rounds 24 August Pediatric Dermatology 101
 Pediatric Dermatology 101 John C. Browning, MD, FAAD, FAAP Conflicts Investigator: ViroXis Advisor: ViroXis Advisory Board: TopMD Speaker: Galderma Objectives Understand the meaning and importance of cutaneous
Pediatric Dermatology 101 John C. Browning, MD, FAAD, FAAP Conflicts Investigator: ViroXis Advisor: ViroXis Advisory Board: TopMD Speaker: Galderma Objectives Understand the meaning and importance of cutaneous
PHLEBOLOGY AND DERMATOLOGY COMPETITIVE OR COMPLEMENTARY?
 PHLEBOLOGY AND DERMATOLOGY COMPETITIVE OR COMPLEMENTARY? Dr Inga Vanhandenhove AZ Monica - Antwerp Disclosure Speaker name:... X Inga Vanhandenhove I have the following potential conflicts of interest
PHLEBOLOGY AND DERMATOLOGY COMPETITIVE OR COMPLEMENTARY? Dr Inga Vanhandenhove AZ Monica - Antwerp Disclosure Speaker name:... X Inga Vanhandenhove I have the following potential conflicts of interest
CME Derm Quiz. Share your photos and diagnoses with us! Case 1
 Case 1 A 21-year-old woman presents with brownish, linear lesions on her forearm and thigh. She mentions she applied lime to insect bites during the days preceding this visit to your office. Phytophotodermatitis.
Case 1 A 21-year-old woman presents with brownish, linear lesions on her forearm and thigh. She mentions she applied lime to insect bites during the days preceding this visit to your office. Phytophotodermatitis.
Thursday 21 st August Skin Problems
 Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic