Tissue Conditions and the
|
|
|
- Marianna Webster
- 5 years ago
- Views:
Transcription
1 Management of Oral Soft Tissue Conditions and the Use of Medications 29 August 2017 Mike Brennan DDS, MHS Department of Oral Medicine Carolinas Medical Center Charlotte, NC
2 Objectives Differential diagnosis of soft tissue conditions Describe more common soft tissue conditions Diagnosis of soft tissue conditions Management strategies of mucosal lesions Treatment Prevention
3 Differential Diagnosis-NIRDS Neoplastic Infectious Reactive Developmental Systemic
4 NEOPLASTIC
5 Leukoplakia- White Clinical diagnosis only Histologically: hyperplasia, mild, moderate, or severe dysplasia, carcinoma in-situ, invasive carcinoma Thin leukoplakia: seldom malignant change Thick leukoplakia: 1-7% malignant change Granular or verruciform: 4-15% malignant change Erythroleukoplakia: 28% malignant change
6
7 Neoplastic: Red Lesions SCCA

8


9 Diagnosis: Incisional vs. Excisional Biopsies
10 Dysplasia Management Medical Systematic Review: 9 studies met criteria for low bias in prior review Three studies were reviewed based adequate study quality. topical bleomycin systemic retinoids systemic lycopene No therapeutic recommendations for bleomycin and cis-retinoic acid Lycopene (4 and 8 mg) may have some efficacy in patients with risk factors similar to those found in a subcontinental Indian population, for the shortterm resolution of oral epithelial dysplasia
11 Dysplasia Management Surgical Lack RCTs that would allow to assess the effectiveness of surgical treatment, including lasers In non-rcts the effectiveness of various surgical modalities in preventing malignant transformation of oral dysplasia have resulted in contradictory outcomes
12 INFECTIOUS
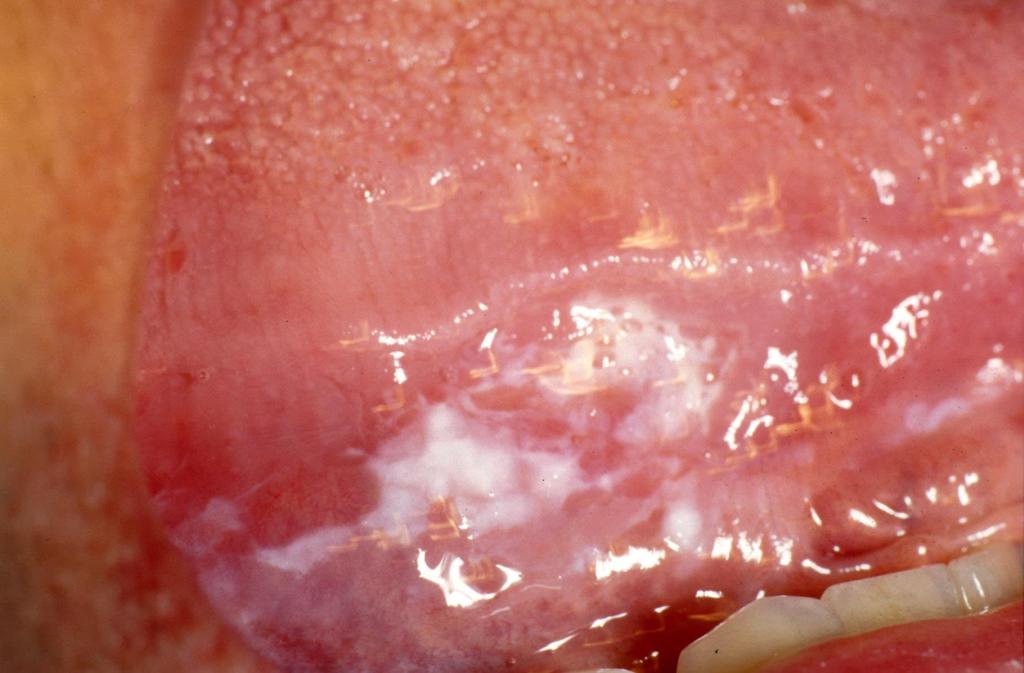
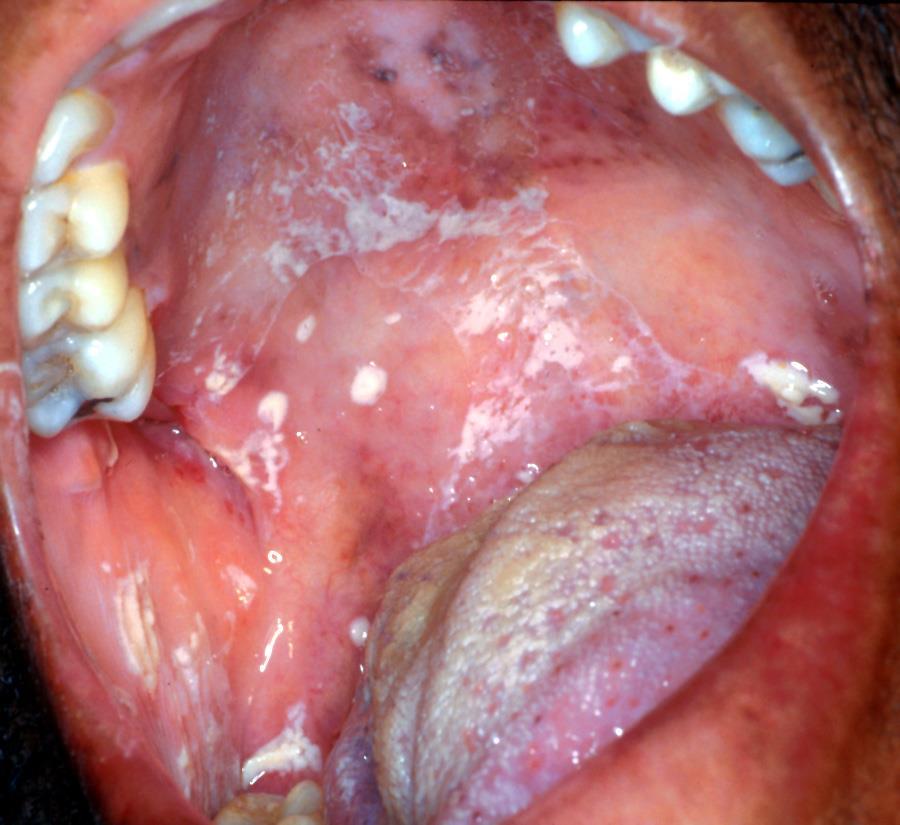
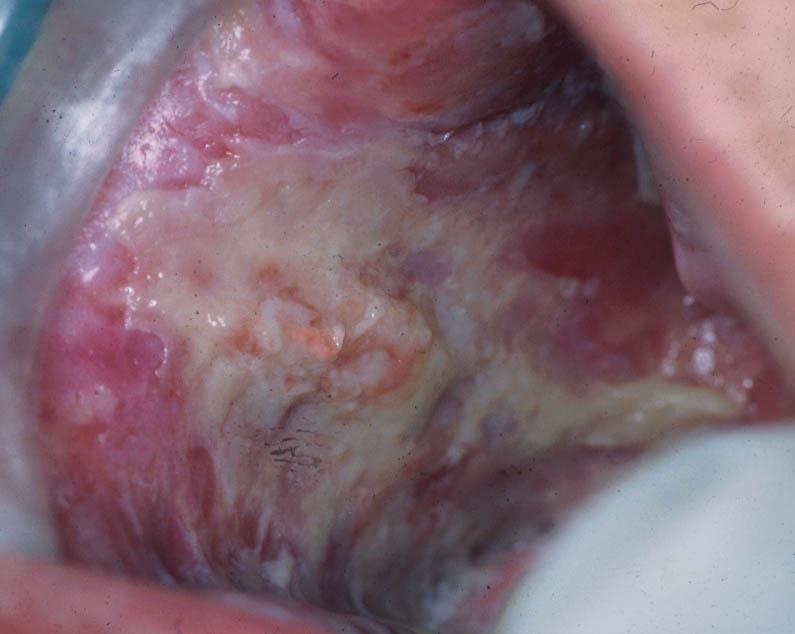
13 Candidiasis Psuedomembranous Erythematous Hyperplastic Angular cheilitis

14
15

16

17
18

19
20
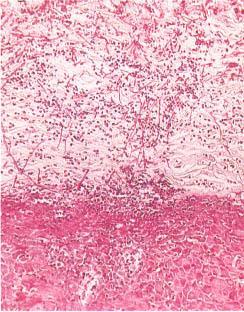
21 Soft tissue diagnostic tests Fungal Superficial: Smear potassium hydroxide or stained with PAS hyphae Culture Deep fungal: Biopsy
22 Treatment - Fungal Topical 10 mg clotrimazole troches 5x/d for 7-10 days Nystatin rinse- 100,000U/mL swish and spit 5mL 4x/d for 2 weeks Chlorhexidine rinse 10 ml bid Probiotics (reduced oral candida in elderly population- RCT J Dent Res x2) Nystatin/triamcinolone cream- dab on corners of mouth 4x/d Clotrimazole-betamethasone dipropionate (Lotrisone) cream Miconazole (Monistat 7) nitrate vaginal cream 2% Nystatin ointment (thin layer on denture) tid
23 Treatment - Fungal Systemic Fluconazole 200 mg day 1 followed by 100 mg/d 1-2 weeks Ketoconazole 200 mg/day for 14 days Both are potent inhibitors of cytochrome P- 450: Check Pharmacology Reference- Drugs.com: 149 major drug interactions- Warfarin, Xanax, Lipitor, Plavix, hydrocodone
24 Infectious: Red Lesions Fungal Erythematous candidiasis Immunocompromised Histoplasmosis, Coccidioidomycosis, Blastomycosis, Cryptococcus (Solitary painful ulceration of tongue, palate, buccal mucosa) Aspergillosis (sinus, after tooth extraction or endodontic treatment) Mucormycosis (Maxillary sinus infection, swelling of alveolar process and/or palate) Extensive tissue destruction due to preference for small blood vessels: infarction and necrosis disrupts blood flow


25
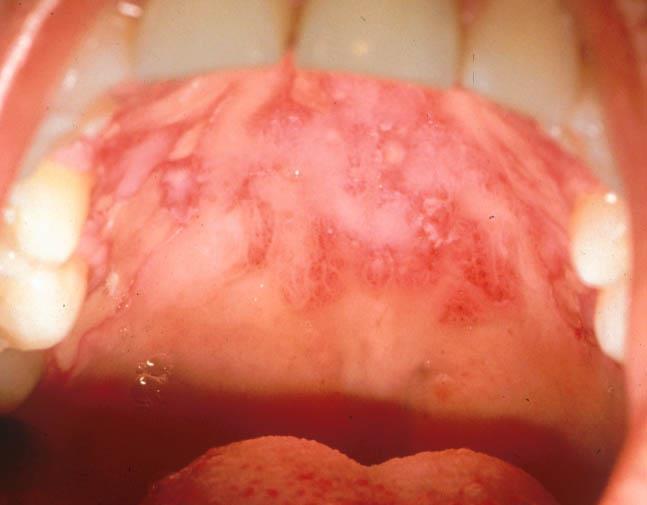
26 Infectious: Red Lesions Viral HSV HSV-1 vs. HSV-2 Children: Acute herpetic gingivostomatitis-both moveable and attached mucosa Adults: Pharyngotonsillitis- vesicles tonsils and posterior pharynx. Oral mucosa anterior to waldeyer s ring <10% of cases. Most common recurrent site: lip (herpes labialis)

27

28

29
30 Soft tissue diagnostic tests Viral Culture 2-4 days for + ID Cytology Virally damaged epithelial cells Serology Rising titre of antibody DNA in situ hybridization for specific virus identification Bacterial Aerobic and anaerobic culture
31 Infectious: Red Lesions Viral VZV Primary infection: chickenpox (oral lesion: palate and buccal mucosa most frequently involved: vesicles. Recurrence: Herpes Zoster 10-20% of older population. One dermatome affected Prodromal pain, fever, malaise 1-4 days before cutaneous/oral lesions.


32

33
34 Treatment- Viral Observe/supportive care Immunocompetent patient Maintain hydration and nutrition Topical MBX- care with lidocaine (esp. children and elderly) Aquaoral with SPF Penciclovir (Denavir) cream 1% Docosanol (Abreva)
35 Treatment - Viral Systemic Acyclovir caps 200 mg: 2 caps 3x/day for 7 days Valacyclovir 500 mg: 1 g 2x/day for 7-10 days (initial episode) Valacyclovir 500 mg: 4 caps when prodromal symptoms start Valacyclovir 500 mg: 1 cap 2x/day for 3 days
36 Prevention - Viral Systemic Acyclovir caps 200 mg: 2 caps 2x/day Valacyclovir 500 mg: 1 cap daily
37 REACTIVE
38 Reactive-White
39 Reactive lesions Focal (frictional) hyperkeratosis Response to low-grade irritation (sharp edge) Buccal mucosa along occlusal line No dysplastic changes

40
41 Reactive lesions Tobacco pouch keratosis Muccobuccal fold, granular to wrinkled appearance Gingival, periodontal destruction possible 15% chewing tobacco, 60% snuff users Malignant potential Nicotine stomatitis Palatal mucosa: elevated papules with red centers are inflammed minor ducts Not pre-malignant. May revert when discontinues smoking

42

43
44 Reactive-Red
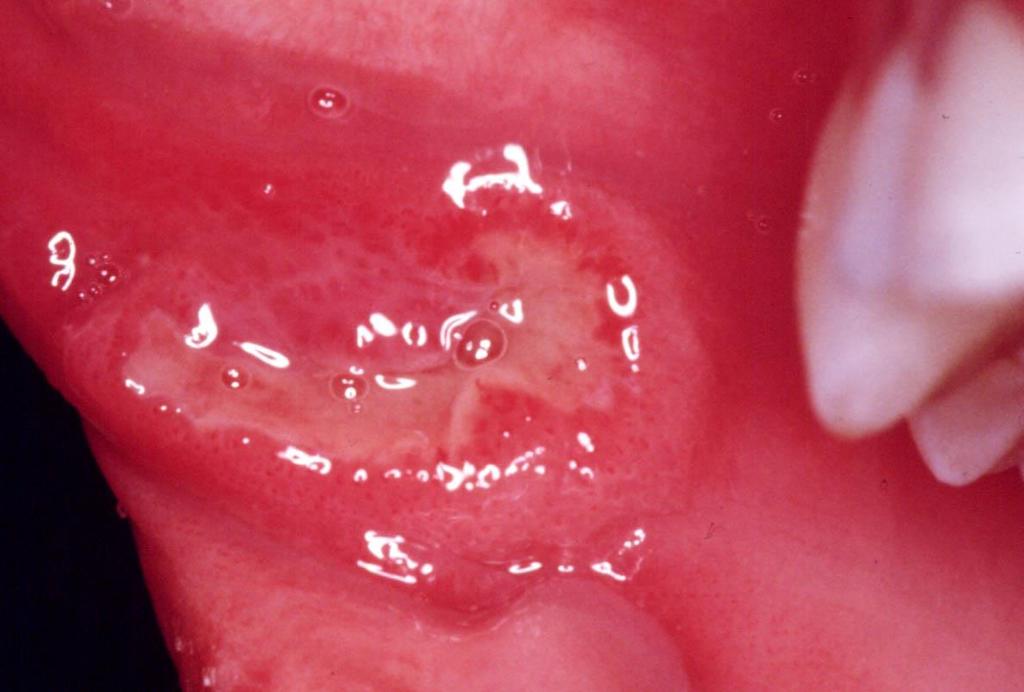
45 Reactive: Red Lesion Aphthae Unknown etiology, incidence 20-60% 3 Clinical forms (minor, major, herpetiform) Non-keratinized mucosa Diagnosis by elimination Rule out allergies, hematologic abnormalities, infectious agents, nutritional imbalances, trauma, stress.
46
47 Management/prevention of RAS Clobetasol (0.05% gel) on lesion immediately when first symptoms occur Chlorhexidine start 1-2x/day for 2 weeks and decrease to every other day or every 3 rd day Vitamin B12 supplement Alteration of diet?
48 Topical steroid by strength Ultrapotent Clobetasol 0.05% Halobetasol 0.05% Potent Dexamethasone 0.5 mg/5 ml Fluocinonide 0.05% Intermediate: Triamcinolone acetonide (Kenalog) 0.1% Low: Hydrocortisone 1% Gel, Ointment, Cream, Compounded
49 Topical Steroids for external use only High cost Atrophy of mucosa Fungal side effects
50 Topical Steroids and Fungal Infection: Study Objectives Primary Determine the incidence of oral candidiasis in patients treated with topical steroids for oral lichen planus (OLP) Secondary Determine if different antifungal therapies are more effective than others in preventing the development of clinical fungal infections Marable DR, Bowers LM, Stout T, Stewart CM, Berg KM, Sankar VS, DeRossi SS, Thoppay JR, Brennan MT. Oral candidiasis following steroid therapy for oral lichen planus. Oral Dis Mar;22(2):140-7.
51 Methods Multicenter, retrospective chart review of a well-characterized group of Lichen Planus patients Carolinas Medical Center (CMC) University of Florida College of Dentistry (UF) University of Texas Health Science Center at San Antonio (UTHSCSA) Georgia Regents University College of Dental Medicine (GRU) 51
52 Methods Inclusion Criteria Patients diagnosed with clinical oral lichen planus. Patients at CMC, UF, UTHSCSA, and GRU Patients treated for lichen planus with topical steroids for at least 2 weeks AND a follow-up visit within 5 weeks of the initiation of daily topical steroids. 52
53 Methods Treatment regimen for oral lichen planus Topical Steroid Used: Y/N Generic name and % of topical steroid Systemic Steroid Used: Y/N Antifungal Preventive Therapy Used: Y/N Generic name and % (if applicable) of antifungal therapy 53
54 Methods Follow-up Data Clinical appearance: Improved/Worsening/No change Clinical symptoms (burning/pain): Improved/Worsening/No change Oral Fungal Infection? Y/N If yes, describe appearance Treatment of oral fungal infection 54
 patients. Systemic steroids were used in 12 (3.8%).")
55 Results Topical steroids were used in 303 (96.2%) patients. Systemic steroids were used in 12 (3.8%). % patients 55
56 Results Objective improvement Clobetasol 91.1% with clobetasol 81.5% without clobetasol (p=0.02) Use of any preventive antifungal 90.6% with antifungal 80.5% without antifungal (p=0.02) Subjective improvement Clotrimazole 94.3% with clotrimazole 85.4% without clotrimazole (p=0.04)
57 Results Oral fungal infections at follow-up Total: 43 (13.7%) patients No significant difference between sites (p=0.36). CMC - 24/155 (15.5%) UF - 11/67 (16.4%) UTHSCSA - 6/59 (10.2%) GRU - 2/34 (5.9%) 57
58 Results Fungal infections at follow-up, by steroid treatment Clobetasol - 32/183 (17.5%), (p=0.02) Dexamethasone - 11/98 (11.2%), (p=0.39) Fluocinonide - 1/22 (4.6%), (p=0.33) Lotrisone - 4/20 (20%), (p=0.50) Preventive antimycotic agents were used in 203 patients and no antimycotic in 111, with fungal infections occurring in 29 (14.3%) and 14 (12.6%), respectively. 58
59 Results Salivary flow testing was completed in 51 patients of which 10 developed OFI. Low stimulated salivary flow group ( 0.7 ml/min) 9 (90%) OFI patients High stimulated salivary flow (>0.7 ml/min) 1 (10%) OFI patient No difference in unstimulated flow 59
60 Conclusions The incidence of oral fungal infections in OLP patients following steroid therapy was higher than anticipated (13.7%). Clobetasol had a significantly higher incidence of fungal infection compared to all other steroid therapies. Low saliva is a major risk factor for a fungal infection 60
61 Reactive: Red Lesion Allergic reaction to systemic drugs Erythema multiforme Lichenoid Lupus erythematous-like eruptions Pemphigus-like lesions
62 Reactive: Red Lesion Erythema Multiforme Immunologically mediated 50% of cases preceding infection or exposure to drug Oral: erythematous patches that develop shallow erosions and ulcerations. Target skin lesions in 50% of cases More severe: erythema multiforme major (Stevens-Johnson syndrome) and Toxic Epidermal Necrolysis (Drug involved)

63
64 Management Erythema Multiforme Prednisone start of lesions Preventive: Acyclovir 400 mg 2x/day Valacyclovir mg /day
65 DEVELOPMENTAL- White
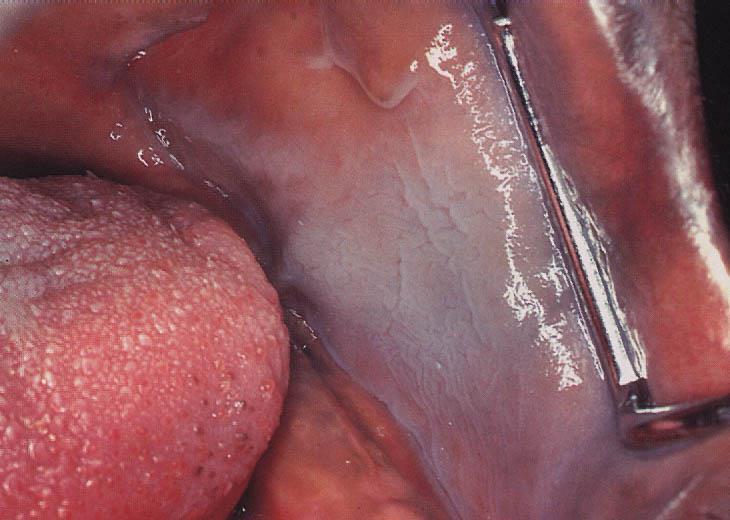
66 Hereditary conditions Leukoedema Natural variant. Asymptomatic, symmetric gray-white, filmy or milky surface Stretching removes clinical appearance More frequent in African Americans
67
68 Fordyce granules Sebaceous glands that occur on the oral mucosa. Normal variant Found in up to 80% of the population Multiple yellowish-white papular lesions. Most common buccal mucosa.

69
70 Developmental: Red Lesion Benign Migratory Glossitis (Geographic Tongue) Red Lesion with white border Usually asymptomatic Moves Diagnosis Elimination Rule out fungal etiology of symptoms

71
72 Management of Benign Migratory Glossitis Topical Steroids Antifungals Rule out hematinic deficiencies
73 SYSTEMIC
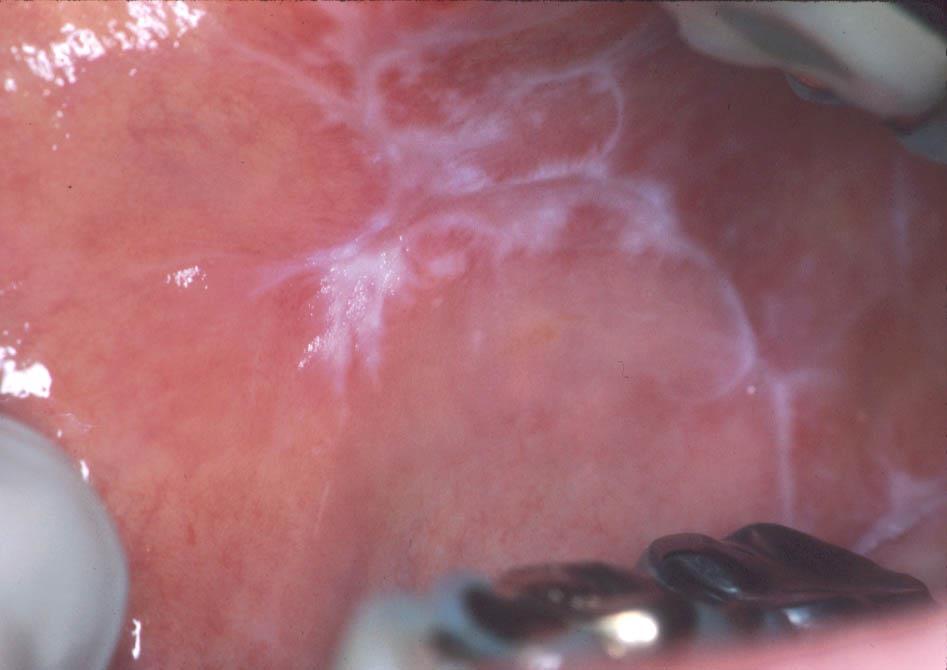
74 Lichen Planus The reported prevalence rates of oral lichen planus (OLP) vary from 0.5% to 2.2% of the population Often develops between years, and it is more frequently seen in women Intra-oral: Reticular, plaque-like, erosive, bullous forms, desquamative Extra-oral: PPPP: purple, polygonal, pruritic papules- Flexural surfaces, scalp, nails, genitals Etiology unknown Lichenoid reactions (drugs, amalgam, gold)
75

76

77

78
79 Treatment for symptomatic OLP- systematic review Topical corticosteroids (+/- topical anti-mycotics) are the first-line treatment for localized lesions Insufficient evidence regarding different dosages, formulations or modes of delivery of topical steroids (eg. paste, spray, mouthwash) to make an evidence based recommendation about which is best Systemic corticosteroids (+/- topical anti-mycotics) are the first-line treatment only for severe, wide-spread OLP and for lichen planus involving other muco-cutaneous sites (eg.: vaginal/vulval LP) recalcitrant /resistant to topical therapies Topical retinoids should be considered only as second line therapy for OLP; systemic retinoids are not recommended Topical calcineurin-inhibitors should be considered only as second-line therapy.
80 Management Lichen Planus Topical steroids Up to 2 weeks followed by 1 week break: repeat if needed Concern of atrophy of mucosa and adrenal suppression with long-term use Optimize oral care Chlorhexidine with poor plaque control Tacrolimus (protopic) 0.1% ointment No a steroid BUT- black box warning
81 LP malignant transformation The alleged annual malignant transformation rate for OLP is between 0.2% and 0.5% 10-50X increased risk of SCCA 2-4 /100 patients over 10 year follow up Patients should be encouraged to avoid or discontinue habits such as excessive tobacco and alcohol use, that are likely to increase the risk of malignant transformation Long-term monitoring may be problematic as this is resource intensive. At a minimum, annual monitoring of OLP is recommended

82
83 Oral Lichenoid Reactions Oral lichenoid contact lesions (OLCL s) are seen in direct topographic relationship to an offending agent This reaction is most often attributable to dental restorative materials, most commonly amalgam With the removal and replacement of the putative causative material, the majority of such OLCL s resolve within several months Patch testing?

84
85 Lupus Oral lesions approximately 25% of SLE. May appear lichenoid, ulcerative or granulomatous. May have more erosive quality.
86

87
88 Pemphigus Autoantibodies to desmosomes 50% have oral mucosal lesions prior to mucocutaneous lesions. Eventually all have intra-oral lesions. Prior to corticosteroids, 60-80% mortality

89
90 Pemphigoid Autoantibodies to basement membrane Average age 60 Oral lesions most patients. Begin as vesicles or bullae. Painful and persistent if untreated. Ocular lesions in 25% of pemphigoid patients with oral lesions


91
92 Management - Pemphigoid Avoid hard/sharp foods Optimal plaque control Chlorhexidine Topical steroids Doxycycline 100 mg daily long-term Refractory: dapsone, prednisone
93 Gingival Differential Desquamative Gingivitis Erosive LP (71%) Pemphigoid (14%) Pemphigus (13%) Linear IgA Disease Epidermolysis Bullosa Acquisita Plasma Cell Gingivitis Mass on Gingiva (4 Ps) Pyogenic Granuloma Peripheral Ossifying Fibroma Peripheral Giant Cell Granuloma Parulis
94 White Lesions Does lesion rub away? Yes No Infections Etiology Pseudomembranous candidiasis Secondary syphilis Diphtheria Reactive Etiology Thermal or chemical burn Allergy Mechanical trauma Keratosis Hereditary Frictional Smoker s Lichen Planus/ Lichenoid Reaction Lupus Erythematosus Infections etiology Hairy leukoplakia Fungal Dysplastic Tissue changes Mild, moderate, severe dysplasia Carcinoma in situ Squamous cell carcinoma
95 Erythematous Lesions Generalized? Yes No Dermatosis erosive lichen planus pemphigoid pemphigus epidermolysis bullosa acquisita psoriasis Nutritional Deficiency ferritin folate vitamin B12 Fungal Etiology Center of tongue: Median rhomboid glossitis Glossitis Palate: -Denture stomatitis -Fungal Bilateral corners of mouth: Angular cheilitis Fungal; candidosis Staph or strep Hematinic deficiency Oral Crohn s disease Immuno compromised state (e.g. Diabetes, HIV) Gingival: Plaque-associated gingivitis Dermatosis Allergy (plasma cell gingivitis) Dysplastic Tissue changes (solitary lesion) Mild, moderate, severe dysplasia Carcinoma in situ Squamous cell carcinoma
96 Management of Oral Lesions Acute lesions (i.e. < 2 weeks) Chronic lesions (> 2 weeks) Long term follow-up of chronic oral lesions Transformation of oral lesions to oral cancer
97 Management of Acute Lesions New onset lesions CHLORIDE Head and neck examination Evaluate for etiologic factors Social habit Change in medication or oral care product Parafunctional habits Trauma- sharp areas NIRDS
98 Management of Acute Lesions Eliminate potential etiologic factors Treat with antifungals if on differential Chlorhexidine 2x/day for 2 weeks Clotrimazole troches 10 mg 5x/d for 7-10 days Nystatin/triamcinolone cream dab corners of mouth 4x/d Probiotic yogurt Fluconazole 200 mg day 1 followed by 100 mg/d one week Nystatin ointment (thin layer on denture) tid Return for reassessment in 2 weeks Consider incisional biopsy for definitive diagnosis
99 Questions? Carolinas Center for Oral Health Carolinas Medical Center 1601 Abbey Place, Suite 220 Charlotte, NC Office number:
Oral Medicine. Dr. Qianming Ian CHEN
 Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
Oral Medicine Dr. Qianming Ian CHEN ORAL MEDICINE Oral medicine is the specialty of dentistry that is concerned with the oral health care of medically compromised patients and with the diagnosis and nonsurgical
TANYA A. WRIGHT, DDS OBJECTIVES
 TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
TANYA A. WRIGHT, DDS OBJECTIVES One will be able to recognize pathological entities One will be able to establish a reasonable differential diagnosis One will be able to identify various types of lesions
Index. Dent Clin N Am 49 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Dent Clin N Am 49 (2005) 273 278 Index Note: Page numbers of article titles are in boldface type. A Acanthosis nigricans, familial, 251 Amalgam tattoo, 197 198 Amphotericin B, 62 Ankyloglossia, 11 Anti-inflammatory
Dent Clin N Am 49 (2005) 273 278 Index Note: Page numbers of article titles are in boldface type. A Acanthosis nigricans, familial, 251 Amalgam tattoo, 197 198 Amphotericin B, 62 Ankyloglossia, 11 Anti-inflammatory
LESIONS OF THE ORAL CAVITY ORAL CAVITY. Oral Cavity Subsites 4/10/2013 LIPS TEETH GINGIVA ORAL MUCOUS MEMBRANES PALATE TONGUE ORAL LYMPHOID TISSUES
 LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
LESIONS OF THE ORAL CAVITY David I. Kutler, MD, FACS Associate Professor Division of Head and Neck Surgery Department of Otolaryngology HNS Weill Cornell Medical Center ORAL CAVITY LIPS TEETH GINGIVA ORAL
That. Name QUIZ. 60 SEPTEMBER 2017 // dentaltown.com
 QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
QUIZ Name That General dentists are first in the line of practitioners that patients see for an oral lesion evaluation; therefore, a sound understanding of oral mucosal diseases and their clinical presentation
Contents. 3 Diagnostic Tests and Studies Introduction Examination... 27
 Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Contents 1 Normal Anatomy... 1 1.1 Introduction... 1 1.2 Surface Landmarks... 1 1.3 Oral Mucosa... 3 1.4 Tongue... 5 1.5 Floor of Mouth... 6 1.6 Palate... 6 1.7 Dentition... 7 1.8 Temporomandibular Joint...
Oral Health & HIV. Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape
 Oral Health & HIV Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape Importance & relevance of Oral HIV Lesions >70% of HIV+ve patients present with oral manifestations
Oral Health & HIV Professor Sudeshni Naidoo Department of Community Dentistry University of the Western Cape Importance & relevance of Oral HIV Lesions >70% of HIV+ve patients present with oral manifestations
2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD
 2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD Course 9148: Diagnosis and Treatment of Recurrent Oral Ulcers Friday, April 6 9 am - 12 pm Diagnosis and Treatment of Recurrent Oral Ulcers
2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD Course 9148: Diagnosis and Treatment of Recurrent Oral Ulcers Friday, April 6 9 am - 12 pm Diagnosis and Treatment of Recurrent Oral Ulcers
Lesions & Lifestyles
 Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Lesions & Lifestyles attended a 3 hour Continuing Education Seminar on Oral Pathology presented by Nancy Dewhirst, RDH,BS on (date) at (location):. Course material is directly related patient care. Notes:
Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients
 Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients Siri Beier Jensen Associate Professor, DDS, PhD Aarhus University Faculty Disclosure X No, nothing to disclose
Case presentations: The pitfalls in diagnosis and management of oral lesions in cancer patients Siri Beier Jensen Associate Professor, DDS, PhD Aarhus University Faculty Disclosure X No, nothing to disclose
Vascular. Extravasated blood. Melanocytic. Tattoo. Epidermolysis bullosa. Lichen planus. Pemphigoid Pemphigus Lupus. Candidosis. Surface Epithelial
 Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Oral Soft Tissue Pathology Epithelial Thickening (white) Combination Erythema migrans Epithelial atrophy (red) Surface Lesions Clinical Impression Enlargements Surface Debris Pigmented Vesicular Ulcerated
Contents. 1 Normal Anatomy Introduction... 17
 Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
Contents 1 Normal Anatomy... 1 Introduction... 1 Surface Landmarks... 1 Oral Mucosa... 1 Tongue... 4 Floor of Mouth... 6 Palate... 7 Dentition... 7 Temporomandibular Joint... 9 Innervation... 10 Jaws and
REF: Chap 1 (Pemphigus vulgaris/etiology and
 Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
ANS: C REF: Chap 1 (Pemphigus vulgaris/etiology and pathogenesis), p 11
, p 11") Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
Chapter 1: Vesiculobullous Diseases Test Bank MULTIPLE CHOICE 1. Intercellular deposits of IgG are consistently found in oral epithelium in which of the following? a. Cicatricial pemphigoid b. Lichen planus
Squamous Cell Neoplasia and Precursor Lesions
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
04/09/2018. Squamous Cell Neoplasia and Precursor Lesions. Agenda. Squamous Dysplasia. Squamo-proliferative lesions. Architectural features
 Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Squamous Cell Neoplasia and Precursor Lesions Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical
Stomatitis.
 Stomatitis http://www.entusa.com/oral_photographs/20080102-stomatitis-palate_small.jpg Oral inflammation and ulcers, known as stomatitis, may be mild and localized or severe and widespread. They are invariably
Stomatitis http://www.entusa.com/oral_photographs/20080102-stomatitis-palate_small.jpg Oral inflammation and ulcers, known as stomatitis, may be mild and localized or severe and widespread. They are invariably
Oral infections. Siri Beier Jensen Associate Professor, DDS, PhD
 Oral infections Siri Beier Jensen Associate Professor, DDS, PhD Oral mucosa Covers and protects underlying structures Barrier to bacterial, fungal and viral infection Resistant to: Temperature ph Mechanical
Oral infections Siri Beier Jensen Associate Professor, DDS, PhD Oral mucosa Covers and protects underlying structures Barrier to bacterial, fungal and viral infection Resistant to: Temperature ph Mechanical
APHTHOUS STOMATITIS ADULT & PEDIATRIC
 DEFINITION Aphthous stomatitis or canker sores are described as ulcers and inflammation of the tissues of the mouth, including the lips, buccal mucosa, tongue, gingiva, and posterior pharyngeal wall. These
DEFINITION Aphthous stomatitis or canker sores are described as ulcers and inflammation of the tissues of the mouth, including the lips, buccal mucosa, tongue, gingiva, and posterior pharyngeal wall. These
Differential Diagnosis of Oral Ulcerations
 Differential Diagnosis of Oral Ulcerations Dr. Nagamani Narayana Department of Oral Biology University of Nebraska Medical Center College of Dentistry Objectives Differential diagnosis of oral ulcerations
Differential Diagnosis of Oral Ulcerations Dr. Nagamani Narayana Department of Oral Biology University of Nebraska Medical Center College of Dentistry Objectives Differential diagnosis of oral ulcerations
VIRUS. Viral infection causing, or associated with diseases of the oral mucosa : Herpes Simpleks 1 & 2
 VIRUS Viral infection causing, or associated with diseases of the oral mucosa : VIRUS Herpes Simpleks 1 & 2 Varicella - Zoster Coxsakie A PENYAKIT Primary Gingivostomatitis Herpetica Herpes Labialis Recurrent
VIRUS Viral infection causing, or associated with diseases of the oral mucosa : VIRUS Herpes Simpleks 1 & 2 Varicella - Zoster Coxsakie A PENYAKIT Primary Gingivostomatitis Herpetica Herpes Labialis Recurrent
Useful Medications for Oral Conditions *
 Useful Medications for Oral Conditions * DISCLAIMER: Drug information is constantly changing and is often subject to interpretation. While care has been taken to ensure the accuracy of the information
Useful Medications for Oral Conditions * DISCLAIMER: Drug information is constantly changing and is often subject to interpretation. While care has been taken to ensure the accuracy of the information
The Oral Cavity. Image source:
 The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
The Oral Cavity Anatomy Image source: http://anatomyforlayla.blogspot.co.za/2007/04/blog-post.html The major structures of the oral cavity are the lips, the teeth, the alveolar ridges (bony areas that
Autoimmune Diseases with Oral Manifestations
 Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Autoimmune Diseases with Oral Manifestations Martin S. Greenberg DDS, FDS RCSEd Professor Emeritus Department of Oral Medicine University of Pennsylvania Disclosure Statement I have no actual or potential
Useful Prescriptions for Common Oral Diseases
 Useful Prescriptions for Common Oral Diseases John R. Kalmar, DMD, PhD The Ohio State University College of Dentistry Oral and Maxillofacial Pathology The following are examples of prescriptions for medications
Useful Prescriptions for Common Oral Diseases John R. Kalmar, DMD, PhD The Ohio State University College of Dentistry Oral and Maxillofacial Pathology The following are examples of prescriptions for medications
الطلاوة = Leukoplakia LEUKOPLAKIA
 LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Leukoplakia is a clinical term that refers to a predominantly white lesion of the oral mucosa that cannot be rubbed off or characterized by any other definable lesion or known disease. 130
LEUKOPLAKIA Definition Epidemiology Clinical presentation
 LEUKOPLAKIA Definition Leukoplakia is the most common premalignant or "potentially malignant" lesion of the oral mucosa. Leukoplakia is a predominantly white lesion of the oral mucosa than cannot be clinicopathologically
LEUKOPLAKIA Definition Leukoplakia is the most common premalignant or "potentially malignant" lesion of the oral mucosa. Leukoplakia is a predominantly white lesion of the oral mucosa than cannot be clinicopathologically
Diagnostic sieve. Looking Beyond the Vermillion Border. Time bombs for medical GPs! Normal oral mucosa
 Sat 12 June 2010 Millennium WS 28 + 38 2.00-2.55; 3.05-4.00 PM Looking Beyond the Vermillion Border Laurence J. Walsh BDSc, PhD, DDSc, FFOP(RCPA), GCEd, FICD, FPFA, FADI, FIADFE The University of Queensland
Sat 12 June 2010 Millennium WS 28 + 38 2.00-2.55; 3.05-4.00 PM Looking Beyond the Vermillion Border Laurence J. Walsh BDSc, PhD, DDSc, FFOP(RCPA), GCEd, FICD, FPFA, FADI, FIADFE The University of Queensland
Diagnosis and management of COMMON NON-VIRAL ORAL ULCERATIONS
 and management of COMMON NON-VIRAL ORAL ULCERATIONS Van Heerden WFP, BChD, MChD (Oral Path), FC Path(SA) Oral Path, PhD, DSc Department of Oral Pathology, University of Pretoria Boy SC, BChD, MChD (Oral
and management of COMMON NON-VIRAL ORAL ULCERATIONS Van Heerden WFP, BChD, MChD (Oral Path), FC Path(SA) Oral Path, PhD, DSc Department of Oral Pathology, University of Pretoria Boy SC, BChD, MChD (Oral
WHITE LESIONS OF THE UPPER AIRWAY
 WHITE LESIONS OF THE UPPER AIRWAY WHITE LESION CONFIGURATIONS Solitary vrs Multifocal Flat Plaque Verrucous/rippled Lacey White with red component Papular (curdled milk plaques) Pseudomembranous PLAQUES
WHITE LESIONS OF THE UPPER AIRWAY WHITE LESION CONFIGURATIONS Solitary vrs Multifocal Flat Plaque Verrucous/rippled Lacey White with red component Papular (curdled milk plaques) Pseudomembranous PLAQUES
Society of Dermatology Physicians Assistants Orocutaneous Disease: Review and Update June 29, 2018
 Society of Dermatology Physicians Assistants Orocutaneous Disease: Review and Update June 29, 2018 John M Wright DDS, MS Regents Professor and Chair Diagnostic Sciences Texas A&M College of Dentistry Dallas,
Society of Dermatology Physicians Assistants Orocutaneous Disease: Review and Update June 29, 2018 John M Wright DDS, MS Regents Professor and Chair Diagnostic Sciences Texas A&M College of Dentistry Dallas,
3. Acyclovir 5% ointment with Dyclonine HCl 1% or Lidocaine 1% Compound Sig: Apply to affected area q2h (start applying prodromal stage)
") Cincinnati Dental Association Great Cases with New Faces November 17, 2010 THERAPEUTIC REGIMENS FOR SELECTED ORAL MUCOSAL DISEASES John A. Svirsky, DDS, MEd Virginia Commonwealth University (804) 828-0547
Cincinnati Dental Association Great Cases with New Faces November 17, 2010 THERAPEUTIC REGIMENS FOR SELECTED ORAL MUCOSAL DISEASES John A. Svirsky, DDS, MEd Virginia Commonwealth University (804) 828-0547
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients. Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology
 Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
Oral Cancer and Common Oral Lesions seen in HIV Seropositive Patients Gwen Cohen Brown DDS, FAAOMP Professor New York City College of Technology Program Objectives Recognize the oral health needs of the
Benign Oral cavity lesions. Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery
 Benign Oral cavity lesions Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery Anatomy Histology Physiology Pathology Clinical cases Introduction The oral cavity
Benign Oral cavity lesions Mohammed ALESSA MBBS,FRCSC Assistant Professor Consultant Otolaryngology, Head & Neck Surgery Anatomy Histology Physiology Pathology Clinical cases Introduction The oral cavity
Oral Medicine Update for the dental practitioner Oral white patches
 IN BRIEF Most white lesions in the mouth are inconsequential and caused by friction or trauma. However, cancer and some systemic diseases such as lichen planus and candidosis may present in this way. Biopsy
IN BRIEF Most white lesions in the mouth are inconsequential and caused by friction or trauma. However, cancer and some systemic diseases such as lichen planus and candidosis may present in this way. Biopsy
Oral Pathology With a Twist and a Number of Crusts
 2016 CDA Presents in Anaheim Oral Pathology With a Twist and a Number of Crusts John A. Svirsky, DDS, MEd Friday, May 13, 2016 9---11:30 a.m. Please visit the C.E. Pavilion to validate your course attendance
2016 CDA Presents in Anaheim Oral Pathology With a Twist and a Number of Crusts John A. Svirsky, DDS, MEd Friday, May 13, 2016 9---11:30 a.m. Please visit the C.E. Pavilion to validate your course attendance
Oral Medicine in 2011
 Oral Medicine in 2011 and Denis P. Lynch, D.D.S., Ph.D. denis.lynch@marquette.edu Outline Recurrent human herpes virus, Type 1 Aphthous ulcers Lichen planus Oral cancer Candidiasis Xerostomia 1 Synopsis
Oral Medicine in 2011 and Denis P. Lynch, D.D.S., Ph.D. denis.lynch@marquette.edu Outline Recurrent human herpes virus, Type 1 Aphthous ulcers Lichen planus Oral cancer Candidiasis Xerostomia 1 Synopsis
Red and White Tissue Reactions: A white appearance of the oral mucosa may be caused by: An increased production of keratin (hyperkeratosis).
.") Burket, chapter 4 Red and White Tissue Reactions: A white appearance of the oral mucosa may be caused by: An increased production of keratin (hyperkeratosis). An abnormal but benign thickening o stratum
Burket, chapter 4 Red and White Tissue Reactions: A white appearance of the oral mucosa may be caused by: An increased production of keratin (hyperkeratosis). An abnormal but benign thickening o stratum
Useful Medications for Oral Conditions *
 AMERICAN ACADEMY OF PEDIATRIC DENTISTRY Useful Medications for Oral Conditions * DISCLAIMER: Drug information is constantly changing and is often subject to interpretation. While care has been taken to
AMERICAN ACADEMY OF PEDIATRIC DENTISTRY Useful Medications for Oral Conditions * DISCLAIMER: Drug information is constantly changing and is often subject to interpretation. While care has been taken to
INFLAMMATORY DISEASES PART I. Immunopathology Part I
 INFLAMMATORY DISEASES PART I Immunopathology Part I Nonspecific & T Cell Mediated Mucosal Inflammatory Lesions Nonspecific and Idiopathic Mucositis Hypersensitivity and Autoimmune T cell mediated Immunoglobulin
INFLAMMATORY DISEASES PART I Immunopathology Part I Nonspecific & T Cell Mediated Mucosal Inflammatory Lesions Nonspecific and Idiopathic Mucositis Hypersensitivity and Autoimmune T cell mediated Immunoglobulin
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem.
 Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Oral cavity cancer accounts for approximately 3% of all malignancies and is a significant worldwide health problem. Majority are SCC ( 5-year survival rate only about 50-60% ) Many SCC arrive from premalignant
Sign In: pemphigus.org/form
 Pemphigus and Pemphigoid The Unique Role of the Dental Professional Dr. Carol Anne Murdoch Kinch Sign In: pemphigus.org/form The International Pemphigus & Pemphigoid Foundation (IPPF) kindly asks all attendees
Pemphigus and Pemphigoid The Unique Role of the Dental Professional Dr. Carol Anne Murdoch Kinch Sign In: pemphigus.org/form The International Pemphigus & Pemphigoid Foundation (IPPF) kindly asks all attendees
I. CHRONIC NON-MICROBIAL MUCOSITIS (aphthous stomatitis, erosive lichen planus, mucous membrane pemphigoid, pemphigus, erythema multiforme)
") Therapeutic Agents and Treatment Strategies for the Management of Selected Mucosal Diseases February 2017 Faculty, Dept. of Oral Pathology, Radiology & Medicine The University of Iowa College of Dentistry
Therapeutic Agents and Treatment Strategies for the Management of Selected Mucosal Diseases February 2017 Faculty, Dept. of Oral Pathology, Radiology & Medicine The University of Iowa College of Dentistry
MUCOCUTANEOUS LESIONS Normal structures in epithelium cell adhesion to each other and to underlying connective tissue:
 ORAL DERMATOSES AND MUCOSAL/GINGIVAL LESIONS MUCOCUTANEOUS LESIONS Normal structures in epithelium cell adhesion to each other and to underlying connective tissue: Diagram taken from: Oral and Maxillofacial
ORAL DERMATOSES AND MUCOSAL/GINGIVAL LESIONS MUCOCUTANEOUS LESIONS Normal structures in epithelium cell adhesion to each other and to underlying connective tissue: Diagram taken from: Oral and Maxillofacial
Premalignant lesions may expose to a promoting. factor & may be induced to undergo malignant. Carcinoma in situ displays the cytologic features of
 بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
بسم رلاهللا Def. Premalignant lesions may expose to a promoting factor & may be induced to undergo malignant transformation. Carcinoma in situ displays the cytologic features of malignancy without invasion
Vulval dermatoses. Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough
 Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
Vulval dermatoses Dr Fiona Lewis, Consultant Dermatologist St John s Institute of Dermatology, London & Heatherwood & Wexham Park Hospital, Slough Pigmentation Vulvodynia Ulcers Genetic Pruritus VULVAL
I. CHRONIC NON-MICROBIAL MUCOSITIS (aphthous stomatitis, erosive lichen planus, mucous membrane pemphigoid, pemphigus, erythema multiforme)
") Therapeutic Agents and Treatment Strategies for the Management of Selected Mucosal Diseases January 2019 Cindy Marek, PharmD & Faculty, Dept. of Oral Pathology, Radiology & Medicine The University of Iowa
Therapeutic Agents and Treatment Strategies for the Management of Selected Mucosal Diseases January 2019 Cindy Marek, PharmD & Faculty, Dept. of Oral Pathology, Radiology & Medicine The University of Iowa
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease:
 4. Associated with systemic disease:") Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Classification: 1. Infective: 2. Traumatic: 3. Idiopathic: Recurrent Aphthous Stomatitis (RAS) 4. Associated with systemic disease: Hematological GIT Behcet s HIV 5. Associated with dermatological diseases:
Role of the Dental Hygienist in Oral Pathology. Role of the Dental Hygienist in Oral Pathology. Cancers of the Oral Cavity.
 Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Gum Gardeners Study Club April 25, 2016 Early Detection of Oral Cancer Cindy Kleinegger, DDS, MS NW Oral Pathology Tigard, OR nworalpathology.com Role of the Dental Hygienist in Oral Pathology Work closely
Therapeutic Management of Oral Mucosal Diseases and Xerostomia
 Therapeutic Management of Oral Mucosal Diseases and Xerostomia Cindy Kleinegger, DDS, MS NW Oral Pathology, Tigard, OR www.nworalpathology.com This handout is intended to offer guidance in the management
Therapeutic Management of Oral Mucosal Diseases and Xerostomia Cindy Kleinegger, DDS, MS NW Oral Pathology, Tigard, OR www.nworalpathology.com This handout is intended to offer guidance in the management
Oral Manifestations of HIV: Case Studies
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Oral Manifestations of HIV: Case Studies David Spach, MD Principal Investigator and Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Oral Manifestations of HIV: Case Studies David Spach, MD Principal Investigator and Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious
2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD
 2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD Course 9121: Infectious Hazards in Dentistry or What You Never Thought You'd Have to Worry about after You Passed National Boards Thursday,
2018 Oregon Dental Conference Course Handout Denis Lynch, DDS, PhD Course 9121: Infectious Hazards in Dentistry or What You Never Thought You'd Have to Worry about after You Passed National Boards Thursday,
Differential Diagnosis of Oral Lesions. An Interactive Lecture Using Audience Response Polling. John L. Alonge, MS, DDS
 Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
Differential Diagnosis of Oral Lesions An Interactive Lecture Using Audience Response Polling John L. Alonge, MS, DDS Goals 1. Review the diagnostic process needed to formulate a differential diagnosis
O RAL H EALTH C OMPLICATIONS IN THE HIV-INFECTED PATIENT
 CHAPTER 8 O RAL H EALTH C OMPLICATIONS IN THE HIV-INFECTED PATIENT Oral health care is a critical component of comprehensive HIV medical management. Development of oral pathology is frequently associated
CHAPTER 8 O RAL H EALTH C OMPLICATIONS IN THE HIV-INFECTED PATIENT Oral health care is a critical component of comprehensive HIV medical management. Development of oral pathology is frequently associated
IN THE NAME OF GOD. Dr.kheirandish DDS,MSC Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr.kheirandish DDS,MSC Oral and maxillofacial pathology Dermatologic Diseases Chapter 16 ECTODERMAL DYSPLASIA o Two or more ectodermally derived anatomic structures fail to develop o
IN THE NAME OF GOD Dr.kheirandish DDS,MSC Oral and maxillofacial pathology Dermatologic Diseases Chapter 16 ECTODERMAL DYSPLASIA o Two or more ectodermally derived anatomic structures fail to develop o
A CASE REPORT OF: PSEUDOMEMBRANOUS CANDIDIASIS INDUCED BY LONG TERM SYSTEMIC CORTICOSTEROIDS THERAPY
 Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 A CASE REPORT OF: PSEUDOMEMBRANOUS CANDIDIASIS INDUCED BY LONG TERM SYSTEMIC CORTICOSTEROIDS THERAPY Ziad Salim Abdul
Case Report International Journal of Dental and Health Sciences Volume 02, Issue 02 A CASE REPORT OF: PSEUDOMEMBRANOUS CANDIDIASIS INDUCED BY LONG TERM SYSTEMIC CORTICOSTEROIDS THERAPY Ziad Salim Abdul
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES)
") NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline
 Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
Oral Lesions & Oral Cancer Dr Rodney Itaki Lecturer Division of Pathology Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Overview
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School
 Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Chapter 2 Variants of Normal and Common Benign Conditions
 Chapter 2 Variants of Normal and Common Benign Conditions Summary Fundamental to diagnosing oral pathologic conditions is the ability to recognize the spectrum of clinical findings that represents variation
Chapter 2 Variants of Normal and Common Benign Conditions Summary Fundamental to diagnosing oral pathologic conditions is the ability to recognize the spectrum of clinical findings that represents variation
CAMOSUN COLLEGE School of Health & Human Services Dental Programs. DHYG 321 Oral Science COURSE OUTLINE
 CAMOSUN COLLEGE School of Health & Human Services Dental Programs 2013 COURSE OUTLINE 1. Instructor Information (a) Instructor Lynne Viczko (b) Office hours Posted on office door (c) Location Dental Building
CAMOSUN COLLEGE School of Health & Human Services Dental Programs 2013 COURSE OUTLINE 1. Instructor Information (a) Instructor Lynne Viczko (b) Office hours Posted on office door (c) Location Dental Building
Conflicts of interest
 Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
Vulvar Cases 2 nd PANHELLANIC CONGRESS on Lower Genital Tract Disorders December 14-16 Grand Hyatt Athens Lynette J. Margesson MD FRCPC Assistant Professor of Obstetrics & Gynecology and Surgery(Dermatology)
PACIFIC JOURNAL OF MEDICAL SCIENCES {Formerly: Medical Sciences Bulletin} ISSN:
 PACIFIC JOURNAL OF MEDICAL SCIENCES {Formerly: Medical Sciences Bulletin} ISSN: 2072 1625 Pac. J. Med. Sci. (PJMS) www.pacjmedsci.com. Email: pacjmedsci@gmail.com. EROSIVE LICHEN PLANUS A CASE REPORT *Prathima
PACIFIC JOURNAL OF MEDICAL SCIENCES {Formerly: Medical Sciences Bulletin} ISSN: 2072 1625 Pac. J. Med. Sci. (PJMS) www.pacjmedsci.com. Email: pacjmedsci@gmail.com. EROSIVE LICHEN PLANUS A CASE REPORT *Prathima
Let s start from the basics for a little review. The Mouth Is Like a Black Hole. But he s friendly at home. Always Wear Gloves!
 The Mouth Is Like a Black Hole Seek and ye shall find: Recognition of Oral Lesions in the Exam Room Lisa Fink, DVM, DAVDC Dentistry & Oral Surgery Service October 4, 2015 But he s friendly at home Part
The Mouth Is Like a Black Hole Seek and ye shall find: Recognition of Oral Lesions in the Exam Room Lisa Fink, DVM, DAVDC Dentistry & Oral Surgery Service October 4, 2015 But he s friendly at home Part
Medical History. Oral Medicine and General Medicine
 Medical History Oral Medicine and General Medicine Gingivitis herpetica acuta NECROTIZÁLÓ SIALOMETAPLASIA SOOR Medical History The life expectancy has recently increased and increasing By dental prevention
Medical History Oral Medicine and General Medicine Gingivitis herpetica acuta NECROTIZÁLÓ SIALOMETAPLASIA SOOR Medical History The life expectancy has recently increased and increasing By dental prevention
Diagnostic difficulties with lesions of the oral mucosa
 BDIAP London, November 2010 School of Clinical Dentistry University of Sheffield Diagnostic difficulties with lesions of the oral mucosa Paul M Speight Dept Oral & Maxillofacial Pathology University of
BDIAP London, November 2010 School of Clinical Dentistry University of Sheffield Diagnostic difficulties with lesions of the oral mucosa Paul M Speight Dept Oral & Maxillofacial Pathology University of
Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions. Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX
 1 Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX Susan Müller, DMD, MS Professor Department of Pathology
1 Oral Manifestations of Dermatologic Disease: A Focus on Lichenoid Lesions Proceedings of the NASHNP Companion Meeting, March, 2011, San Antonio, TX Susan Müller, DMD, MS Professor Department of Pathology
THE TONGUE. In Clinical Diagnosis
 THE TONGUE In Clinical Diagnosis A Colour Atlas of The Tongue in Clinical Diagnosis D.W. BEAVEN S.E. BROOKS BATES Guide to Physical Examination Lynn s. Bickley רויטל רחימי, תום כספי פנימית ב', תל-השומר
THE TONGUE In Clinical Diagnosis A Colour Atlas of The Tongue in Clinical Diagnosis D.W. BEAVEN S.E. BROOKS BATES Guide to Physical Examination Lynn s. Bickley רויטל רחימי, תום כספי פנימית ב', תל-השומר
a. viral INFECTIONS OF ORAL MUCOSA HERPETIC STOMATITIS HERPETIC STOMATITIS
 a. viral INFECTIONS OF ORAL MUCOSA laboratory confirmation rather long diagnosis based mainly on clinical features basic diagnostic methods: (1) culture of viral particles; (2) morphologic changes and
a. viral INFECTIONS OF ORAL MUCOSA laboratory confirmation rather long diagnosis based mainly on clinical features basic diagnostic methods: (1) culture of viral particles; (2) morphologic changes and
Oral problems. Mouth Ulcer and Cold sore. Lec-2
 Oral problems Mouth Ulcer and Cold sore Lec-2 By: Dr.Khanda Taifwr 1 Mouth ulcers Mouth ulcers are extremely common, and are a recurrent problem in some people. Common sites are the tongue margin and inside
Oral problems Mouth Ulcer and Cold sore Lec-2 By: Dr.Khanda Taifwr 1 Mouth ulcers Mouth ulcers are extremely common, and are a recurrent problem in some people. Common sites are the tongue margin and inside
Oral Cancer- Improving Early Detection
 Oral Cancer- Improving Early Detection GDC Recommended Subject Aims: To give an overview of the dental team's role in detecting the early signs of oral cancer; to give an overview of the risk factors associated
Oral Cancer- Improving Early Detection GDC Recommended Subject Aims: To give an overview of the dental team's role in detecting the early signs of oral cancer; to give an overview of the risk factors associated
Proceedings of the Southern European Veterinary Conference - SEVC -
 Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
Close this window to return to IVIS www.ivis.org Proceedings of the Southern European Veterinary Conference - SEVC - Sep. 30-Oct. 3, 2010, Barcelona, Spain Next SEVC Conference: Sep. 30-Oct. 2, 2011 -
OH I CAN GUIDELINES FOR ORAL HEALTH PROTOCOLS
 OH I CAN GUIDELINES FOR ORAL HEALTH PROTOCOLS THIS PAGE INTENTIONALLY LEFT BLANK OH I CAN Guidelines Based on Oral Health Signs and Symptoms Symptoms Likely Cause Initial Management Ongoing Care Brief
OH I CAN GUIDELINES FOR ORAL HEALTH PROTOCOLS THIS PAGE INTENTIONALLY LEFT BLANK OH I CAN Guidelines Based on Oral Health Signs and Symptoms Symptoms Likely Cause Initial Management Ongoing Care Brief
Pattern of oral lesions Cytohistopathological study in tertiary care centre.
 International Journal of Current Research in Medical Sciences ISSN: 2454-5716 P-ISJN: A4372-3064, E -ISJN: A4372-3061 www.ijcrims.com Original Research Article Volume 3, Issue 10-2017 Pattern of oral lesions
International Journal of Current Research in Medical Sciences ISSN: 2454-5716 P-ISJN: A4372-3064, E -ISJN: A4372-3061 www.ijcrims.com Original Research Article Volume 3, Issue 10-2017 Pattern of oral lesions
A Guide to Clinical Differential Diagnosis of Oral Mucosal Lesions
 Continuing Education Brought to you by A Guide to Clinical Differential Diagnosis of Oral Mucosal Lesions Course Author(s): Michael W. Finkelstein, DDS, MS; Emily Lanzel, DDS, MS; John W. Hellstein, DDS,
Continuing Education Brought to you by A Guide to Clinical Differential Diagnosis of Oral Mucosal Lesions Course Author(s): Michael W. Finkelstein, DDS, MS; Emily Lanzel, DDS, MS; John W. Hellstein, DDS,
Infection Causing Oral Ulceration
 TITLE: Ulcerations of the Oral Cavity SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 RESIDENT PHYSICIAN: David Gleinser, MD FACULTY ADVISOR: Susan McCammon, MD SERIES
TITLE: Ulcerations of the Oral Cavity SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: March 31, 2009 RESIDENT PHYSICIAN: David Gleinser, MD FACULTY ADVISOR: Susan McCammon, MD SERIES
Kings College London Dental Institute. Guy s & St Thomas NHS Foundation Trust Oral Medicine Unit. Disease Activity Scoring sheets
 Kings College London Dental Institute Guy s & St Thomas NHS Foundation Trust ral Medicine Unit Disease Activity Scoring sheets Clinical scoring systems for oral mucosal Diseases The routine clinical management
Kings College London Dental Institute Guy s & St Thomas NHS Foundation Trust ral Medicine Unit Disease Activity Scoring sheets Clinical scoring systems for oral mucosal Diseases The routine clinical management
Disorders of the vulva
 Vulval lesions Disorders of the vulva Terminology standardised by the International Society for the Study of Vulvovaginal Disease(ISSVD) Classification 1.Nonneoplastic epithelial disorders of vulva Lichen
Vulval lesions Disorders of the vulva Terminology standardised by the International Society for the Study of Vulvovaginal Disease(ISSVD) Classification 1.Nonneoplastic epithelial disorders of vulva Lichen
Oral Manifestation in Patients diagnosed with Dermatological Diseases
 JCDP ORIGINAL RESEARCH Oral Manifestation in Patients diagnosed 10.5005/jp-journals-10024-2191 with Dermatological Diseases Oral Manifestation in Patients diagnosed with Dermatological Diseases 1 Sanjay
JCDP ORIGINAL RESEARCH Oral Manifestation in Patients diagnosed 10.5005/jp-journals-10024-2191 with Dermatological Diseases Oral Manifestation in Patients diagnosed with Dermatological Diseases 1 Sanjay
GROUP 15 TOPICAL PREPARATIONS
 - 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
- 105 - GROUP 15 15.1 DERMATOLOGICAL PREPARATIONS 15.1.1 TOPICAL ANTIFUNGALS CLOTRIMAZOLE Indication: Treatment of susceptible fungal infections, dermatophytoses, superficial mycoses, and cutaneous candidiasis
Allergic contact stomatitis is a rare disorder,
 Allergic Contact Stomatitis: A Case Report and Review of Literature P Lokesh, T Rooban, Joshua Elizabeth, K Umadevi, K Ranganathan Abstract Allergic contact stomatitis is a well-recognized entity, which
Allergic Contact Stomatitis: A Case Report and Review of Literature P Lokesh, T Rooban, Joshua Elizabeth, K Umadevi, K Ranganathan Abstract Allergic contact stomatitis is a well-recognized entity, which
A New Approach to the Pharmacological Treatment. of Oral Lichen Planus: Case Report
 Case Report 57 Copyright University of Medicine, Tirana AJMHS Vol. 47 (2/3): 57-65 2016 A New Approach to the Pharmacological Treatment of Oral Lichen Planus: Case Report Besian Abazi 1, Joana Mihani 2
Case Report 57 Copyright University of Medicine, Tirana AJMHS Vol. 47 (2/3): 57-65 2016 A New Approach to the Pharmacological Treatment of Oral Lichen Planus: Case Report Besian Abazi 1, Joana Mihani 2
A. Erythema multiforme and related diseases
 Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
Go Back to the Top To Order, Visit the Purchasing Page for Details Chapter Erythema, Erythroderma (Exfoliative Dermatitis) Erythema is caused by telangiectasia or hyperemia in the papillary and reticular
=ﻰﻤاﻤﺤﻠا ﺔﻴﻘﻠﺤﻠا ﺔذﺒاﻨﻠا
 1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
1 / 15 Erythema Annulare Centrifugum and Other Figurate Erythemas The figurate erythemas include a variety of eruptions characterized by annular and polycyclic lesions. Classification of this group has
DENIS P. LYNCH, DDS, PHD
 140 TH ANNUAL MEETING MAY 6 MAY 7, 2010 JEWEL OF THE GREAT LAKES DENIS P. LYNCH, DDS, PHD FRIDAY, MAY 7, 2010 9:00 A.M. TO 12:00 NOON ORAL CANCER AND RELATED PREMALIGNANCY Oral Cancer and Premalignancy
140 TH ANNUAL MEETING MAY 6 MAY 7, 2010 JEWEL OF THE GREAT LAKES DENIS P. LYNCH, DDS, PHD FRIDAY, MAY 7, 2010 9:00 A.M. TO 12:00 NOON ORAL CANCER AND RELATED PREMALIGNANCY Oral Cancer and Premalignancy
BLOCK 12 Viruses of the ENT
 BLOCK 12 Viruses of the ENT Acute infections Introduction Pharyngitis, Common cold, Sinusitis, Otitis media Recurrent infections Herpes zoster oticus Chronic infections HIV and ENT manifestations Neoplasms
BLOCK 12 Viruses of the ENT Acute infections Introduction Pharyngitis, Common cold, Sinusitis, Otitis media Recurrent infections Herpes zoster oticus Chronic infections HIV and ENT manifestations Neoplasms
Dental Care and Health An Update. Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI
 Dental Care and Health An Update Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI WHO s Definition of Health? Health is a state of complete physical, mental, and social wellbeing and not merely the absence of
Dental Care and Health An Update Dr. Ranjini Pillai, DDS, MPH, FAGD, FICOI WHO s Definition of Health? Health is a state of complete physical, mental, and social wellbeing and not merely the absence of
Inflammatory Disease. Part I. Infections
 Inflammatory Disease Part I Infections Bacterial, Fungal and Viral Infections of the Head and Neck Sexually Transmitted Diseases Lomaki, Middle Mesa Petroglyphs Northern Arizona Herpesviruses I, II Clamydia
Inflammatory Disease Part I Infections Bacterial, Fungal and Viral Infections of the Head and Neck Sexually Transmitted Diseases Lomaki, Middle Mesa Petroglyphs Northern Arizona Herpesviruses I, II Clamydia
Leukoplakia is a white patch on the oral mucous membrane, which is undeliable and can not diagnose neither clinically nor pathologically as an other
 Leukoplakia Leukoplakia is a white patch on the oral mucous membrane, which is undeliable and can not diagnose neither clinically nor pathologically as an other disease. (Pindborg. 1978) Precancerous lesion
Leukoplakia Leukoplakia is a white patch on the oral mucous membrane, which is undeliable and can not diagnose neither clinically nor pathologically as an other disease. (Pindborg. 1978) Precancerous lesion
In India among the 1027 million populations about 72% people live in rural areas
 1 INTRODUCTION 2 In India among the 1027 million populations about 72% people live in rural areas India produces 9000 dentists per annum-dentist population ratio is 1:30,000 Only 10%of the dentists are
1 INTRODUCTION 2 In India among the 1027 million populations about 72% people live in rural areas India produces 9000 dentists per annum-dentist population ratio is 1:30,000 Only 10%of the dentists are
Rashes Not To Be Missed In Children
 May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
May 2016 Rashes Not To Be Missed In Children Dr Chan Yuin Chew Dermatologist Dermatology Associates Gleneagles Medical Centre Scope of presentation Focus on rashes May lead to significant morbidity if
Premalignant lesion is a morphologically altered tissue in which cancer is more likely to occur, than its apparently normal counter parts.
 Oral Premalignancy Premalignant lesion is a morphologically altered tissue in which cancer is more likely to occur, than its apparently normal counter parts. Premalignant condition is a generalized state
Oral Premalignancy Premalignant lesion is a morphologically altered tissue in which cancer is more likely to occur, than its apparently normal counter parts. Premalignant condition is a generalized state
Diseases of oral cavity
 Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Diseases of oral cavity Diseases of Teeth and Supporting Structures Inflammatory/Reactive Lesions Infections Oral Manifestations of Systemic Disease Precancerous and Cancerous Lesions Odontogenic Cysts
Tanzania Dental Journal Vol. 15 No. 1, May 2008
 Diagnosis of Oral Lesions associated with HIV/AIDS Hamza O. Department of Oral Surgery and Oral Pathology, MUHAS Hamza O: Diagnosis of Oral Lesions associated with HIV/AIDS. Tanz Dent J 2008; 15 (1): 22-26
Diagnosis of Oral Lesions associated with HIV/AIDS Hamza O. Department of Oral Surgery and Oral Pathology, MUHAS Hamza O: Diagnosis of Oral Lesions associated with HIV/AIDS. Tanz Dent J 2008; 15 (1): 22-26
Proliferative Verrucous Leukoplakia of the Gingiva, Report of two Cases with Malignant Transformation
 Journal of Clinical and Anatomic Pathology Case Report Open Access Proliferative Verrucous Leukoplakia of the Gingiva, Report of two Cases with Malignant Transformation Nadereh Ghanee DMD, Selene Saraf
Journal of Clinical and Anatomic Pathology Case Report Open Access Proliferative Verrucous Leukoplakia of the Gingiva, Report of two Cases with Malignant Transformation Nadereh Ghanee DMD, Selene Saraf
Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases
 Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases Abstract Aim: The aim of this article is to present a brief review of plasma cell gingivitis (PCG) along with reports of three
Plasma Cell Gingivitis Among Herbal Toothpaste Users: A Report of Three Cases Abstract Aim: The aim of this article is to present a brief review of plasma cell gingivitis (PCG) along with reports of three
We re Passionate About
 Oral Health Training Marie Burgum Oral Health Advisor Tees Community Dental Service We re Passionate About Putting patients first Quality, safety and patient experience Transforming services to meet the
Oral Health Training Marie Burgum Oral Health Advisor Tees Community Dental Service We re Passionate About Putting patients first Quality, safety and patient experience Transforming services to meet the